bevacizumab plus chemotherapy versus chemotherapy alone as second-line treatment for patients with...
TRANSCRIPT
www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5 1
Articles
Bevacizumab plus chemotherapy versus chemotherapy alone as second-line treatment for patients with HER2-negative locally recurrent or metastatic breast cancer after fi rst-line treatment with bevacizumab plus chemotherapy (TANIA): an open-label, randomised phase 3 trialGunter von Minckwitz, Fabio Puglisi, Javier Cortes, Eduard Vrdoljak, Norbert Marschner, Christoph Zielinski, Cristian Villanueva, Gilles Romieu, István Lang, Eva Ciruelos, Michele De Laurentiis, Corinne Veyret, Sabine de Ducla, Ulrich Freudensprung, Stefanie Srock, Joseph Gligorov
SummaryBackground Combining bevacizumab with fi rst-line or second-line chemotherapy improves progression-free survival in HER2-negative locally recurrent or metastatic breast cancer. We assessed the effi cacy and safety of further bevacizumab therapy in patients with locally recurrent or metastatic breast cancer whose disease had progressed after treatment with bevacizumab plus chemotherapy.
Methods In this open-label, randomised, phase 3 trial, we recruited patients who had HER2-negative locally recurrent or metastatic breast cancer that had progressed after receiving 12 weeks or more of fi rst-line bevacizumab plus chemotherapy from 118 centres in 12 countries. Patients were randomly assigned (1:1) by use of a central interactive voice response system using a block randomisation schedule (block size four) stratifi ed by hormone receptor status, fi rst-line progression-free survival, selected chemotherapy, and lactate dehydrogenase concentration, to receive second-line single-agent chemotherapy either alone or with bevacizumab (15 mg/kg every 3 weeks or 10 mg/kg every 2 weeks). Second-line therapy was continued until disease progression, unacceptable toxicity, or consent withdrawal. At progression, patients randomly assigned to chemotherapy alone received third-line chemotherapy without bevacizumab; those randomly assigned to bevacizumab continued bevacizumab with third-line chemotherapy. The primary endpoint was progression-free survival from randomisation to second-line progression or death in the intention-to-treat population. This trial is ongoing, and registered with ClinicalTrials.gov, number NCT01250379.
Findings Between Feb 17, 2011, and April 3, 2013, 494 patients were randomly assigned to treatment (247 in each group). The median duration of follow-up at the time of this prespecifi ed primary progression-free survival analysis was 15·9 months (IQR 9·1–21·7) in the chemotherapy-alone group and 16·1 months (10·6–22·7) in the combination group. Progression-free survival was signifi cantly longer for those patients treated with bevacizumab plus chemotherapy than for those with chemotherapy alone (median: 6·3 months [95% CI 5·4–7·2] vs 4·2 months [3·9–4·7], respectively, stratifi ed hazard ratio [HR] 0·75 [95% CI 0·61–0·93], two-sided stratifi ed log-rank p=0·0068). The most common grade 3 or more adverse events were hypertension (33 [13%] of 245 patients receiving bevacizumab plus chemotherapy vs 17 [7%] of 238 patients receiving chemotherapy alone), neutropenia (29 [12%] vs 20 [8%]), and hand-foot syndrome (27 [11%] vs 25 [11%]). Grade 3 proteinuria occurred in 17 (7%) of 245 patients receiving combination therapy and one (<1%) of 238 patients receiving chemotherapy alone. Serious adverse events were reported in 61 (25%) of 245 patients receiving bevacizumab plus chemotherapy versus 44 (18%) of 238 patients receiving chemotherapy alone.
Interpretation These results suggest that continued VEGF inhibition with further bevacizumab is a valid treatment option for patients with locally recurrent or metastatic HER2-negative breast cancer whose disease was stabilised or responded to fi rst-line bevacizumab with chemotherapy.
Funding F Hoff mann-La Roche.
IntroductionThe anti-angiogenic VEGF-inhibitor bevacizumab has been extensively assessed in breast cancer. In randomised, phase 3 trials in HER2-negative locally recurrent or metastatic breast cancer, bevacizumab increased progression-free survival but not overall survival when combined with fi rst-line1–3 or second-line4 chemotherapy. However, because patients pretreated
with bevacizumab were ineligible for the second-line therapy trial,4 the eff ect of further bevacizumab given after fi rst-line bevacizumab-containing therapy for locally recurrent or metastatic breast cancer was unknown.
The crucial role of VEGF throughout the angiogenic pathway5,6 suggests the potential importance of sustained VEGF inhibition for long-term disease control. Various preclinical models suggest that continuous VEGF
Lancet Oncol 2014
Published OnlineSeptember 28, 2014http://dx.doi.org/10.1016/S1470-2045(14)70439-5
See Online/Commenthttp://dx.doi.org/10.1016/ S1470-2045(14)70454-1
German Breast Group, Neu-Isenburg, and University Women’s Hospital, Frankfurt, Germany (Prof G von Minckwitz MD); University Hospital of Udine, Udine, Italy (F Puglisi MD); Vall d’Hebron Institute of Oncology and Vall d’Hebron University Hospital, Barcelona, Spain (J Cortes MD); Center of Oncology, University Hospital Split, Split, Croatia (Prof E Vrdoljak MD); Outpatient Cancer Center, Freiburg, Germany (N Marschner MD); Department of Medicine I and Comprehensive Cancer Center, Medical University Vienna, Vienna, Austria (Prof C Zielinski MD); Central European Cooperative Oncology Group, Vienna, Austria (Prof C Zielinski); Centre Hospitalier-Universitaire de Besançon, Besançon, France (C Villanueva MD); Institut du Cancer Montpellier, Val d’Aurelle, France (G Romieu MD); National Institute of Oncology, Budapest, Hungary (Prof I Lang MD); Hospital Universitario 12 Octubre, Madrid, Spain (E Ciruelos MD); Istituto Nazionale Tumori Fondazione G Pascale, Naples, Italy (M De Laurentiis MD); Centre Henri Becquerel, Rouen, France (Prof C Veyret MD); F Hoff mann-La Roche Ltd, Basel, Switzerland (S de Ducla DEA, U Freudensprung MSc,

Articles
2 www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5
S Srock MD); and Assistance-Publique Hôpitaux de
Paris-Tenon, Institut Universitaire de Cancerologie
Université Pierre et Marie Curie, Sorbonne Université, Paris,
France (J Gligorov MD)
Correspondence to:Prof Gunter von Minckwitz, GBG Forschungs GmbH, 63263 Neu-
Isenburg, [email protected]
suppression is required to maximise the activity of bevacizumab as monotherapy, combined with chemotherapy, or as post-chemotherapy maintenance.6 In patients with colorectal cancer, exploratory analyses of single-group observational cohort and registry studies suggested improved post-progression or overall survival in patients receiving further bevacizumab after disease progression on fi rst-line bevacizumab-containing therapy.7–9 In a randomised phase 3 trial (ML18147) that assessed bevacizumab with second-line chemotherapy versus second-line chemotherapy alone after progression on fi rst-line bevacizumab plus chemotherapy in patients with colorectal cancer, patients treated with bevacizumab and chemotherapy had signifi cantly longer progression-free survival and overall survival than those treated with chemotherapy alone.10 Similarly, another phase 3 trial in colorectal cancer showed signifi cantly longer progression-free survival with continued bevacizumab after disease progression on fi rst-line bevacizumab-containing therapy, despite premature recruitment discontinuation after the positive results from ML18147.11
We therefore designed the TANIA trial to explore the eff ect of second-line bevacizumab after disease progression on or after fi rst-line bevacizumab plus chemotherapy in locally recurrent or metastatic breast cancer.
MethodsStudy design and patientsTANIA is an ongoing, open-label parallel-group randomised multicentre phase 3 trial. Eligible women were those aged 18 years or older, who had HER2-negative, measurable or non-measurable, locally recurrent or metastatic breast cancer. Disease had to have progressed (according to investigator assessment) after 12 weeks or more of fi rst-line bevacizumab plus chemotherapy for locally recurrent or metastatic breast cancer. Maintenance bevacizumab, maintenance endocrine therapy, or both, before enrolment was allowed. All patients had to have an Eastern Cooperative Oncology Group performance status of 0–2 and an estimated life expectancy of 12 weeks or more. Patients were ineligible if they had previously received fi rst-line anti-angiogenic therapy (except bevacizumab) for locally recurrent or metastatic breast cancer; positive or unknown HER2 status; inadequately controlled hypertension; serious non-healing wound or active ulcer; history of nephrotic syndrome, hypertensive crisis, hypertensive encephalopathy, bleeding diathesis, clinically relevant coagulopathy, or grade 3 or 4 venous thromboembolism; a history of myocardial infarction, unstable angina, signifi cant vascular disease, gastrointestinal perforation, abdominal fi stula, intra-abdominal abscess, or active gastrointestinal bleeding within 6 months preceding study treatment; or a major surgical procedure within 28 days preceding study treatment; or known CNS disease, except treated brain metastases. Patients were also ineligible if they had
inadequate haematological function (absolute neutrophil count <1·5× 10⁹ cells per L, platelet count <75× 10⁹ cells per L, or haemoglobin <80 g/L [transfusion or approved haemopoietic growth factors allowed]), coagulation parameters (international normalised ratio >1·5, except for patients on stable anticoagulation therapy, activated partial thromboplastin time ≥1·5 × upper limit of normal [ULN], or above the lower limit of the therapeutic range), hepatic function (total bilirubin >1·5 × ULN, aspartate aminotransferase and alanine aminotransferase >2 × ULN, or >5 × ULN in patients with known liver involvement, alkaline phosphatase >2 × ULN, or >5 × ULN in patients with known liver involvement, or >7 × ULN in patients with known bone involvement), or renal function (creatinine clearance <50 mL/min, urine dipstick for proteinuria >2+ unless 24 h protein was ≤1 g). Patients were also ineligible if they were participating, or had recently participated (within 4 weeks or two half-lives of the investigational drug, whichever was greater), or were planning to participate in, an experimental drug study other than previous participation in a study of bevacizumab for breast cancer.
All patients provided written informed consent. The study was done in full accordance with Good Clinical Practice guidelines and the Declaration of Helsinki. The protocol and all modifi cations were approved by independent ethics committees at all participating sites. An independent data monitoring committee undertook ongoing review of all safety data and effi cacy of the bevacizumab plus vinorelbine combination in view of exploratory analyses of RIBBON-2, in which the progression-free survival hazard ratio (HR) was less favourable for the subgroup of 76 patients receiving this combination (HR 1·42, 95% CI 0·78–2·59) compared with the overall HR (0·78, 0·64–0·93).
Randomisation and maskingPatients were randomly assigned (1:1) to receive second-line chemotherapy either alone or with bevacizumab by investigators using a central interactive voice response system with an allocation sequence generated by Parexel Informatics (Nottingham, UK). Randomisation was by stratifi ed blocks (block size of four) within the following strata: hormone receptor status (triple negative vs oestrogen receptor [ER] or progesterone receptor [PR] or both positive); fi rst-line progression-free survival from the time of diagnosis of locally recurrent or metastatic breast cancer (<6 months vs ≥6 months); selected second-line chemotherapy (taxane vs vinorelbine vs other non-taxane); and lactate dehydrogenase concentration (≤1·5 × ULN vs >1·5 × ULN). Neither the patients nor the investigators were masked to treatment assignment, but the steering committee and all representatives of the funder (including the lead biostatistician) only had access to data pooled from across both treatment groups until the database was locked and the treatment code was revealed.
Articles
www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5 3
ProceduresBefore randomisation, investigators selected the single-agent chemotherapy for each patient from prespecifi ed standard options: intravenous paclitaxel (80–90 mg/m² weekly), intravenous nanoparticle albumin-bound paclitaxel (260 mg/m² every 3 weeks, or 100 mg/m² weekly), intravenous docetaxel (75–100 mg/m², or 60 mg/m² for Japanese patients, every 3 weeks), oral capecitabine (1000 mg/m² twice daily for 14 days followed by a 7-day rest period), intravenous gemcitabine (1000 mg/m² on days 1, 8, and 15 every 4 weeks), intravenous pegylated liposomal doxorubicin (40–50 mg/m² every 4 weeks), intravenous non-pegylated liposomal doxorubicin (60 mg/m² every 3 weeks), intravenous doxorubicin (60–75 mg/m² every 3 weeks, or 20–25 mg/m² weekly), intravenous epirubicin (75–90 mg/m² every 3 weeks, or 25–30 mg/m² weekly), vinorelbine (weekly 30 mg/m² administered intravenously, or weekly 80 mg/m² administered orally), cyclophos phamide (500–700 mg/m² administered intravenously every 3 weeks, or 50 mg/m² administered orally every day), or intravenous ixabepilone (40 mg/m² administered every 3 weeks). Patients assigned to bevacizumab received 15 mg/kg every 3 weeks, or 10 mg/kg every 2 weeks, depending on the chosen chemotherapy regimen. Second-line therapy was continued until disease progression, unacceptable toxicity, or patient withdrawal. If patients allocated to combination therapy discontinued bevacizumab or chemotherapy for any reason before disease progression, the other treatment was continued as monotherapy until disease progression, unacceptable toxicity, or patient withdrawal. If chemo therapy-related toxicity necessitated chemotherapy discontinuation before disease progression, patients received standard of care (potentially switching to another chemotherapy drug) until disease progression. Maintenance endocrine therapy was allowed in both groups (with bevacizumab in the combination arm). In the event of toxicity, dose reduction or modifi cation of bevacizumab was not allowed, but bevacizumab was to be interrupted or permanently discontinued for hyper tension, proteinuria, thrombosis, embolism, haemorrhage, congestive heart failure, or wound-healing complications (appendix).
After disease progression on second-line therapy, patients initially assigned to chemotherapy alone received third-line chemotherapy without bevacizumab (no crossover), whereas those assigned to combination therapy continued to receive bevacizumab with third-line chemotherapy (unless prevented by unacceptable toxicity). Investigators chose the third-line chemo therapy for each patient from the prespecifi ed standard options listed above, or intravenous eribulin (1·23 mg/m² on days 1 and 8 every 3 weeks) as an additional option following a protocol amendment in September, 2013. After third-line disease progression, fourth-line treatment (with or without bevacizumab) was at the investigator’s discretion in all patients.
Tumour assessment was based on limited Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 with CT, MRI, bone scans, and x-rays done at baseline and at 8-week or 9-week intervals, depending on the chosen chemotherapy. No independent review of tumour assessment was done; clinical examinations were done as clinically indicated before starting every cycle. Safety was assessed using Common Terminology Criteria for Adverse Events (version 4.0). All grade 3–5 adverse events, serious adverse events (any grade), and adverse events of special interest for bevacizumab (any grade) were recorded at every study visit. All laboratory assess-ments were done locally according to local standards. Unless a patient withdrew consent, was lost to follow-up, or the investigator withdrew the patient—eg, because of another illness, adverse event, treatment failure after a prescribed procedure, protocol violation, cure, or administrative reason—all patients remained in the study with continued follow-up for overall survival. Patient-reported outcomes were assessed with the Functional Assessment of Cancer Therapy–Breast questionnaire (FACT-B).
OutcomesThe primary endpoint was second-line progression-free survival, defi ned as the time from randomisation to disease progression or death on second-line treatment. See Online for appendix
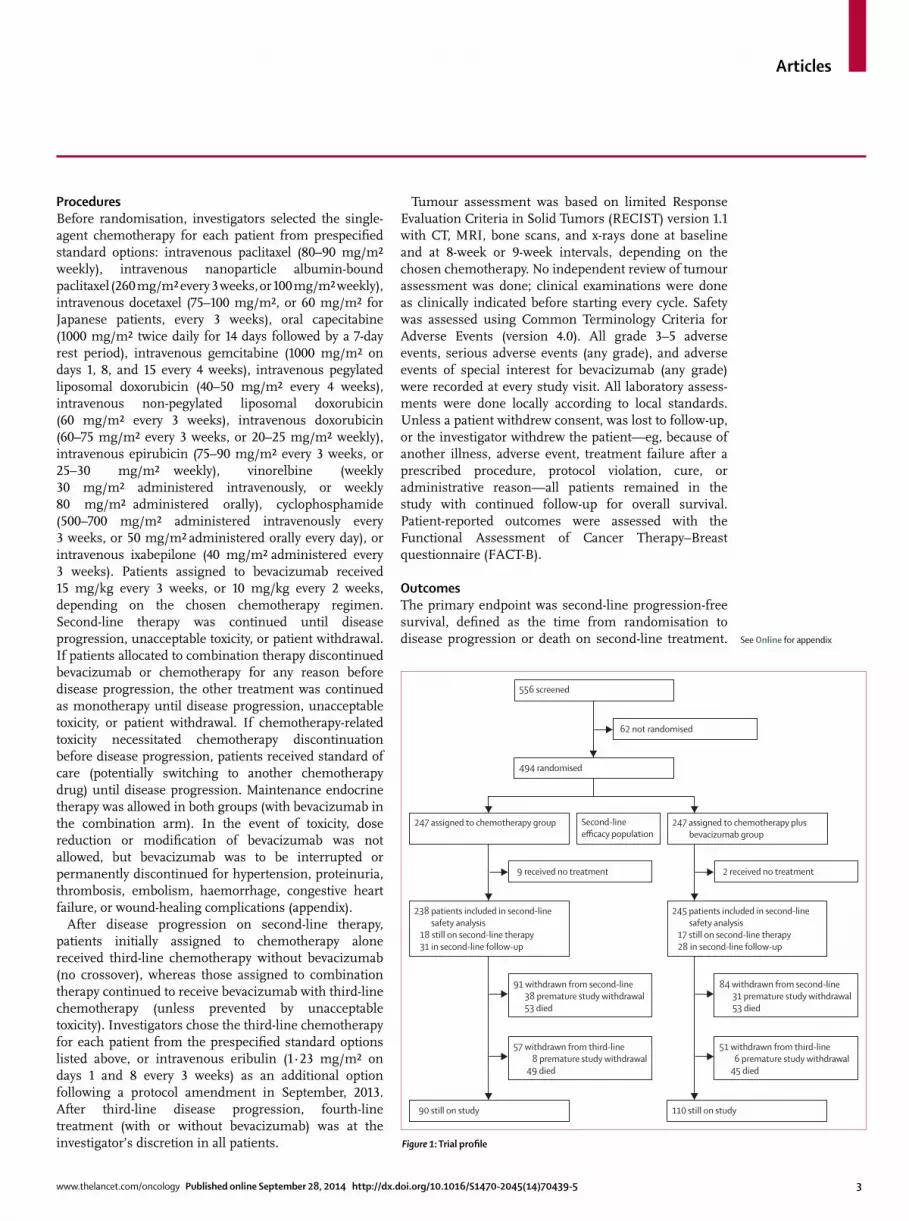
Figure 1: Trial profi le
247 assigned to chemotherapy group
9 received no treatment
238 patients included in second-line safety analysis 18 still on second-line therapy 31 in second-line follow-up
91 withdrawn from second-line 38 premature study withdrawal 53 died
90 still on study
57 withdrawn from third-line 8 premature study withdrawal 49 died
247 assigned to chemotherapy plus bevacizumab group
2 received no treatment
245 patients included in second-line safety analysis 17 still on second-line therapy 28 in second-line follow-up
84 withdrawn from second-line 31 premature study withdrawal 53 died
110 still on study
51 withdrawn from third-line 6 premature study withdrawal 45 died
556 screened
62 not randomised
494 randomised
Second-lineefficacy population

Articles
4 www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5
Secondary endpoints included second-line progression-free survival assessed in prespecifi ed stratifi cation subgroups, rate of best objective response to second-line therapy (defi ned as complete or partial tumour response), progression-free survival from randomisation until disease progression or death on third-line therapy, overall survival from randomisation to death from any cause, 1-year overall survival (defi ned as the number of patients alive 1 year after randomisation), safety, and patient-reported outcomes.
Statistical analysisWe calculated a sample size of 488 patients based on a log-rank test that assumed median progression-free survival of 7 months with chemotherapy alone and 9·3 months with combination therapy (representing a HR of 0·75), 30 months’ recruitment, and 5% dropout. For the primary analysis, second-line progression-free survival events were required in 384 of 488 patients for 80% power with a two-sided α of 0·05. Progression-free survival was compared between treatment groups with a two-sided log-rank test, stratifi ed by stratifi cation factors. Median progression-free survival was estimated by the Kaplan-Meier method. A stratifi ed Cox proportional hazards model was used to estimate the HR with 95% CIs.12 Planned sensitivity analyses included an unstratifi ed approach and analyses accounting for change of therapy before disease progression (the fi rst censoring patients at the last tumour assessment preceding initiation of new chemotherapy before any progression-free survival event, the second using a similar approach but censoring for any anti-cancer therapy, including endocrine therapy). Duration of follow-up was estimated with the reverse Kaplan-Meier method.13
We analysed effi cacy in the intent-to-treat population (all patients randomly assigned to treatment groups) and safety in all patients who received at least one dose of study therapy (bevacizumab or chemotherapy; safety population). All adverse events occurring during second-line therapy were included in the second-line safety analysis reported here, irrespective of any switch to another chemotherapy, endocrine therapy, or both before disease progression. This approach was chosen to avoid under-reporting. A sensitivity analysis with every patient analysed according to actual treatment received was also done.
The fi nal overall survival analysis is planned for when all patients have been followed for at least 24 months since randomisation, died, withdrawn consent, or been lost to follow-up. Results regarding outcomes of third-line treatment (eg, third-line progression-free survival and third-line safety) will be reported at the same time. Analyses of patient-reported outcomes and translational research (an exploratory endpoint within the optional biomarker substudy) will be reported separately. Statistical analyses were done with SAS version 9.2.
This trial is registered with ClinicalTrials.gov, NCT01250379.
Chemotherapy alone (n=247)
Chemotherapy plus bevacizumab (n=247)
Age (years) 54 (30–77) 56 (24–81)
≥65 51 (21%) 64 (26%)
≥70 21 (9%) 28 (11%)
Hormone receptor status
Triple negative 57 (23%) 49 (20%)
ER or PgR positive or both positive 188 (76%) 198 (80%)
Locally recurrent or metastatic disease at fi rst diagnosis 49 (20%) 37 (15%)
Disease-free interval*
≤12 months 24 (10%) 18 (7%)
≤24 months 58 (23%) 53 (21%)
Previous (neo)adjuvant chemotherapy†
Taxane 97 (39%) 100 (40%)
Anthracycline 139 (56%) 155 (63%)
Other 144 (58%) 162 (66%)
Previous (neo)adjuvant bevacizumab 3 (1%) 4 (2%)
Previous endocrine therapy for locally recurrent/metastatic breast cancer
112 (45%) 125 (51%)
Timing of fi rst-line progression in relation to fi rst-line chemotherapy plus bevacizumab
During bevacizumab 48 (19%) 45 (18%)
After bevacizumab 198 (80%) 196 (79%)
Unknown/missing/other 1 (<1%) 6 (2%)
Invasive ductal 204 (83%) 199 (81%)
Invasive lobular 30 (12%) 37 (15%)
Metastatic organ sites at baseline
Visceral 190 (77%) 186 (75%)
Liver 151 (61%) 143 (58%)
Lung 75 (30%) 70 (28%)
≥3 metastatic organ sites 88 (36%) 80 (32%)
Bone only 16 (6%) 15 (6%)
First-line chemotherapy with bevacizumab†
Paclitaxel 180 (73%) 182 (74%)
Docetaxel 27 (11%) 33 (13%)
Capecitabine 46 (19%) 39 (16%)
First-line progression-free survival‡
Median, months (IQR) 14·1 (8·5–23·3) 14·9 (9·2–24·3)
<6 32 (13%) 25 (10%)
≥6 213 (86%) 221 (89%)
History of hypertension§ 115 (47%) 141 (57%)
Bevacizumab-free interval before study therapy
≤6 weeks 165 (67%) 149 (60%)
>6 weeks 81 (33%) 98 (40%)
Missing 1 (<1%) 0
LDH concentration
≤1·5 × ULN 207 (84%) 210 (85%)
>1·5 × ULN 40 (16%) 37 (15%)
Data are median (range or IQR) or number of patients (%). ER=oestrogen receptor. PgR=progesterone receptor. LDH=lactate dehydrogenase. ULN=upper limit of normal. *Patients with both early and locally recurrent or metastatic breast cancer; defi ned as the time from diagnosis of early breast cancer to diagnosis of locally recurrent or metastatic disease, whichever is earlier. †More than one answer possible. ‡Defi ned as the time from diagnosis of locally recurrent or metastatic disease, whichever is later, to the date of disease progression following fi rst-line therapy; missing from the case report form for two patients in the chemotherapy-alone group and one patient in the chemotherapy plus bevacizumab group. §Recorded in bevacizumab-related medical history in the case report form.
Table 1: Baseline characteristics (intent-to-treat population, n=494) as recorded in the electronic case report form
Articles
www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5 5
Role of the funding sourceF Hoff mann-La Roche funded the trial, and was responsible for the statistical analyses, which were done by Paraxel International (Berlin, Germany). The trial was designed by the trial steering committee in collaboration with the funder. The funder was not involved in the collection or interpretation of data but was involved in the (blinded) querying process—eg, to ensure progression-free survival data were recorded in accordance with RECIST version 1.1. The funder was involved, together with the steering committee and co-authors, in interpreting the results after database lock and unblinded analysis. The funder supported third-party medical writing assistance for this paper and had the opportunity to review the content. GvM, SdD, UF, and SS had full access to all the data in the study. GvM had the fi nal responsibility for the decision to submit for publication, in agreement with the trial steering committee and coauthors.
ResultsBetween Feb 17, 2011, and April 3, 2013, 494 patients recruited from 118 centres in France, Hungary, Spain, Italy, Austria, Croatia, Germany, Switzerland, Slovakia, Greece, Israel, and Argentina were randomly assigned to treatment (247 in each group; fi gure 1). Baseline characteristics were well balanced between treatment groups (table 1). Most patients had received fi rst-line bevacizumab with a taxane, typically paclitaxel. The most frequently chosen second-line chemotherapy was capecitabine (table 2).
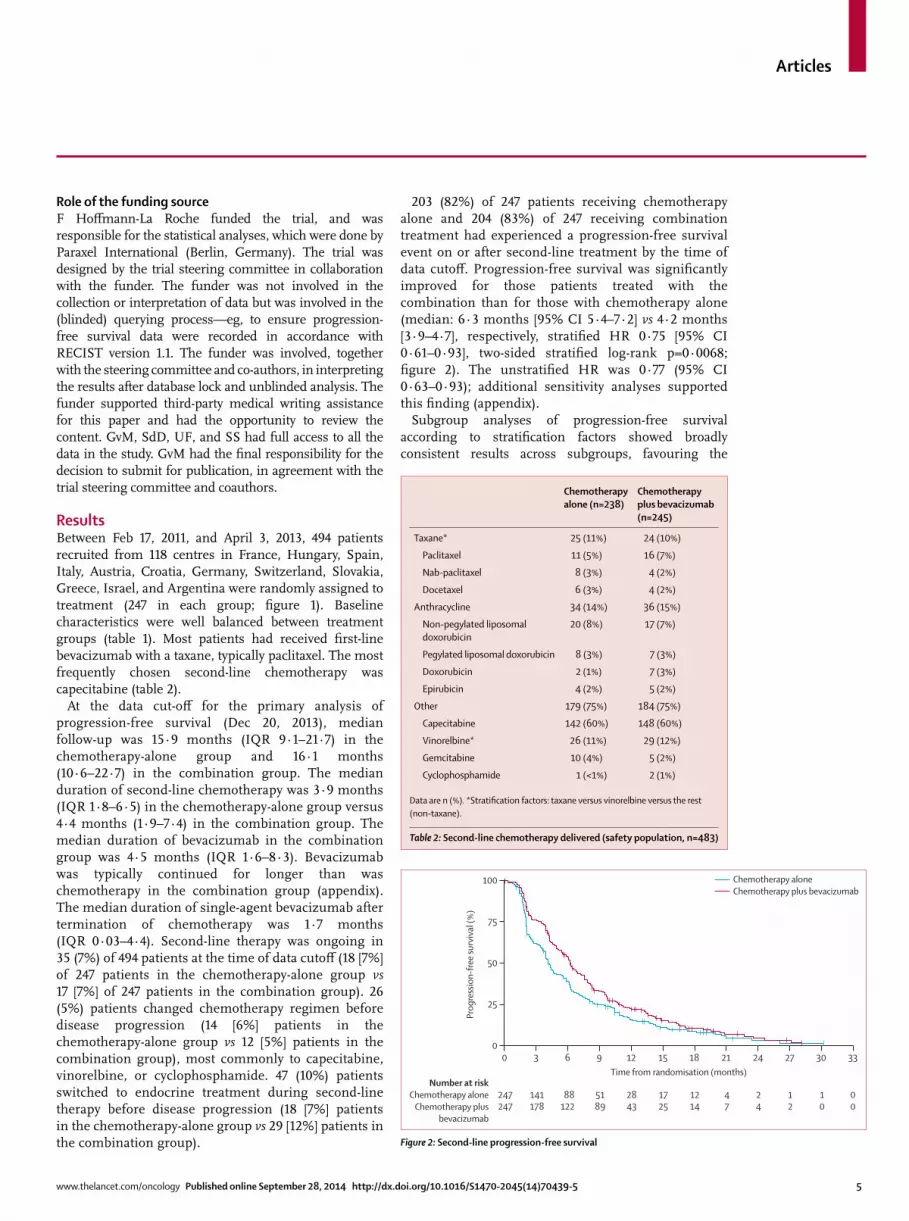
At the data cut-off for the primary analysis of progression-free survival (Dec 20, 2013), median follow-up was 15·9 months (IQR 9·1–21·7) in the chemotherapy-alone group and 16·1 months (10·6–22·7) in the combination group. The median duration of second-line chemotherapy was 3·9 months (IQR 1·8–6·5) in the chemotherapy-alone group versus 4·4 months (1·9–7·4) in the combination group. The median duration of bevacizumab in the combination group was 4·5 months (IQR 1·6–8·3). Bevacizumab was typically continued for longer than was chemotherapy in the combination group (appendix). The median duration of single-agent bevacizumab after termination of chemotherapy was 1·7 months (IQR 0·03–4·4). Second-line therapy was ongoing in 35 (7%) of 494 patients at the time of data cutoff (18 [7%] of 247 patients in the chemotherapy-alone group vs 17 [7%] of 247 patients in the combination group). 26 (5%) patients changed chemotherapy regimen before disease progression (14 [6%] patients in the chemotherapy-alone group vs 12 [5%] patients in the combination group), most commonly to capecitabine, vinorelbine, or cyclo phos phamide. 47 (10%) patients switched to endocrine treatment during second-line therapy before disease progression (18 [7%] patients in the chemotherapy-alone group vs 29 [12%] patients in the combination group).
203 (82%) of 247 patients receiving chemotherapy alone and 204 (83%) of 247 receiving combination treatment had experienced a progression-free survival event on or after second-line treatment by the time of data cutoff . Progression-free survival was signifi cantly improved for those patients treated with the combination than for those with chemotherapy alone (median: 6·3 months [95% CI 5·4–7·2] vs 4·2 months [3·9–4·7], respectively, stratifi ed HR 0·75 [95% CI 0·61–0·93], two-sided stratifi ed log-rank p=0·0068; fi gure 2). The unstratifi ed HR was 0·77 (95% CI 0·63–0·93); additional sensitivity analyses supported this fi nding (appendix).
Subgroup analyses of progression-free survival according to stratifi cation factors showed broadly consistent results across subgroups, favouring the
Chemotherapy alone (n=238)
Chemotherapy plus bevacizumab (n=245)
Taxane* 25 (11%) 24 (10%)
Paclitaxel 11 (5%) 16 (7%)
Nab-paclitaxel 8 (3%) 4 (2%)
Docetaxel 6 (3%) 4 (2%)
Anthracycline 34 (14%) 36 (15%)
Non-pegylated liposomal doxorubicin
20 (8%) 17 (7%)
Pegylated liposomal doxorubicin 8 (3%) 7 (3%)
Doxorubicin 2 (1%) 7 (3%)
Epirubicin 4 (2%) 5 (2%)
Other 179 (75%) 184 (75%)
Capecitabine 142 (60%) 148 (60%)
Vinorelbine* 26 (11%) 29 (12%)
Gemcitabine 10 (4%) 5 (2%)
Cyclophosphamide 1 (<1%) 2 (1%)
Data are n (%). *Stratifi cation factors: taxane versus vinorelbine versus the rest (non-taxane).
Table 2: Second-line chemotherapy delivered (safety population, n=483)
Figure 2: Second-line progression-free survival
Prog
ress
ion-
free
surv
ival
(%)
100
75
50
25
0
Number at riskChemotherapy alone
Chemotherapy plusbevacizumab
Time from randomisation (months)0 3 6 9 12 15 18 21 24 27 30 33
247 141 88 51 28 17 12 4 2 1 1 0247 178 122 89 43 25 14 7 4 2 0 0
Chemotherapy aloneChemotherapy plus bevacizumab
Articles
6 www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5
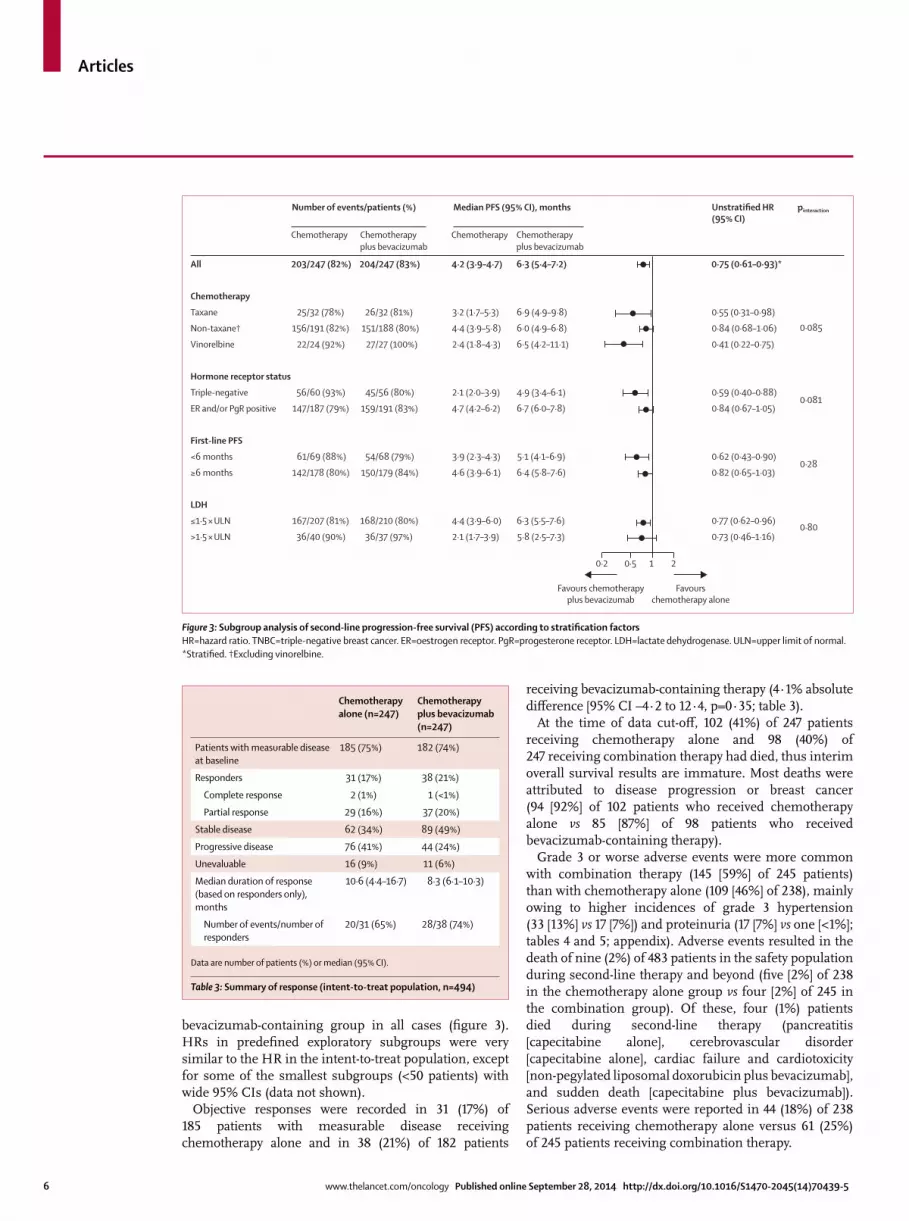
bevacizumab-containing group in all cases (fi gure 3). HRs in predefi ned exploratory subgroups were very similar to the HR in the intent-to-treat population, except for some of the smallest subgroups (<50 patients) with wide 95% CIs (data not shown).
Objective responses were recorded in 31 (17%) of 185 patients with measurable disease receiving chemotherapy alone and in 38 (21%) of 182 patients
receiving bevacizumab-containing therapy (4·1% absolute diff erence [95% CI –4·2 to 12·4, p=0·35; table 3).
At the time of data cut-off , 102 (41%) of 247 patients receiving chemotherapy alone and 98 (40%) of 247 receiving combination therapy had died, thus interim overall survival results are immature. Most deaths were attributed to disease progression or breast cancer (94 [92%] of 102 patients who received chemotherapy alone vs 85 [87%] of 98 patients who received bevacizumab-containing therapy).
Grade 3 or worse adverse events were more common with combination therapy (145 [59%] of 245 patients) than with chemotherapy alone (109 [46%] of 238), mainly owing to higher incidences of grade 3 hypertension (33 [13%] vs 17 [7%]) and proteinuria (17 [7%] vs one [<1%]; tables 4 and 5; appendix). Adverse events resulted in the death of nine (2%) of 483 patients in the safety population during second-line therapy and beyond (fi ve [2%] of 238 in the chemotherapy alone group vs four [2%] of 245 in the combination group). Of these, four (1%) patients died during second-line therapy (pancreatitis [capecitabine alone], cerebro vascular disorder [capecitabine alone], cardiac failure and cardiotoxicity [non-pegylated liposomal doxorubicin plus bevacizumab], and sudden death [capecitabine plus bevacizumab]). Serious adverse events were reported in 44 (18%) of 238 patients receiving chemotherapy alone versus 61 (25%) of 245 patients receiving combination therapy.
Figure 3: Subgroup analysis of second-line progression-free survival (PFS) according to stratifi cation factorsHR=hazard ratio. TNBC=triple-negative breast cancer. ER=oestrogen receptor. PgR=progesterone receptor. LDH=lactate dehydrogenase. ULN=upper limit of normal. *Stratifi ed. †Excluding vinorelbine.
All 203/247 (82%) 204/247 (83%) 4·2 (3·9–4·7) 6·3 (5·4–7·2) 0·75 (0·61–0·93)*
Chemotherapy
Taxane 25/32 (78%) 26/32 (81%) 3·2 (1·7–5·3) 6·9 (4·9–9·8) 0·55 (0·31–0·98)
Non-taxane† 156/191 (82%) 151/188 (80%) 4·4 (3·9–5·8) 6·0 (4·9–6·8) 0·84 (0·68–1·06)
Vinorelbine 22/24 (92%) 27/27 (100%) 2·4 (1·8–4·3) 6·5 (4·2–11·1) 0·41 (0·22–0·75)
Hormone receptor status
Triple-negative 56/60 (93%) 45/56 (80%) 2·1 (2·0–3·9) 4·9 (3·4–6·1) 0·59 (0·40–0·88)
ER and/or PgR positive 147/187 (79%) 159/191 (83%) 4·7 (4·2–6·2) 6·7 (6·0–7·8) 0·84 (0·67–1·05)
First-line PFS
<6 months 61/69 (88%) 54/68 (79%) 3·9 (2·3–4·3) 5·1 (4·1–6·9) 0·62 (0·43–0·90)
≥6 months 142/178 (80%) 150/179 (84%) 4·6 (3·9–6·1) 6·4 (5·8–7·6) 0·82 (0·65–1·03)
LDH
≤1·5 × ULN 167/207 (81%) 168/210 (80%) 4·4 (3·9–6·0) 6·3 (5·5–7·6) 0·77 (0·62–0·96)
>1·5 × ULN 36/40 (90%) 36/37 (97%) 2·1 (1·7–3·9) 5·8 (2·5–7·3) 0·73 (0·46–1·16)
0·2 0·5 1 2
0·085
0·081
0·28
0·80
Favours chemotherapyplus bevacizumab
Favourschemotherapy alone
Number of events/patients (%) Median PFS (95% CI), months
Chemotherapy Chemotherapyplus bevacizumab
Chemotherapy Chemotherapyplus bevacizumab
pinteraction Unstratified HR (95% CI)
Chemotherapy alone (n=247)
Chemotherapy plus bevacizumab (n=247)
Patients with measurable disease at baseline
185 (75%) 182 (74%)
Responders 31 (17%) 38 (21%)
Complete response 2 (1%) 1 (<1%)
Partial response 29 (16%) 37 (20%)
Stable disease 62 (34%) 89 (49%)
Progressive disease 76 (41%) 44 (24%)
Unevaluable 16 (9%) 11 (6%)
Median duration of response (based on responders only), months
10·6 (4·4–16·7) 8·3 (6·1–10·3)
Number of events/number of responders
20/31 (65%) 28/38 (74%)
Data are number of patients (%) or median (95% CI).
Table 3: Summary of response (intent-to-treat population, n=494)
Articles
www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5 7
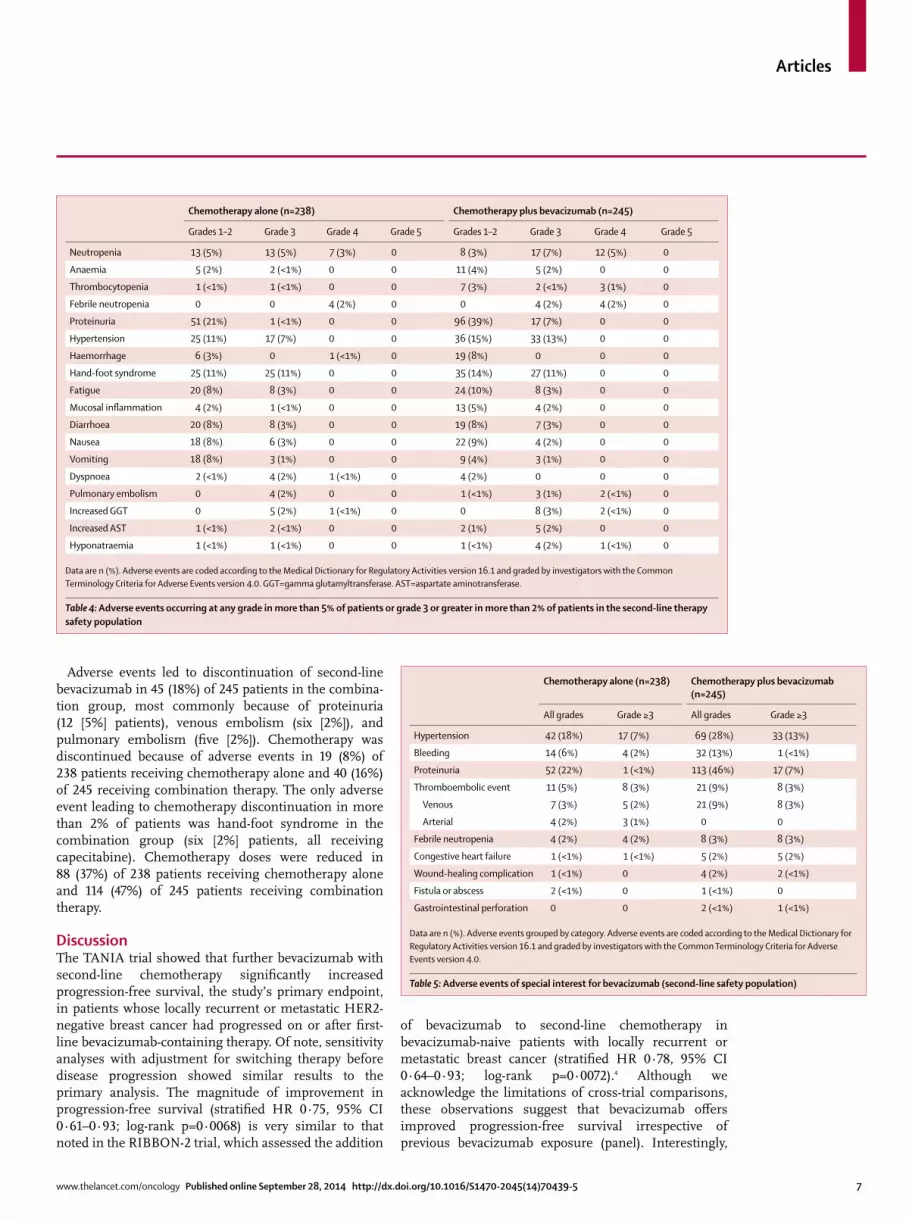
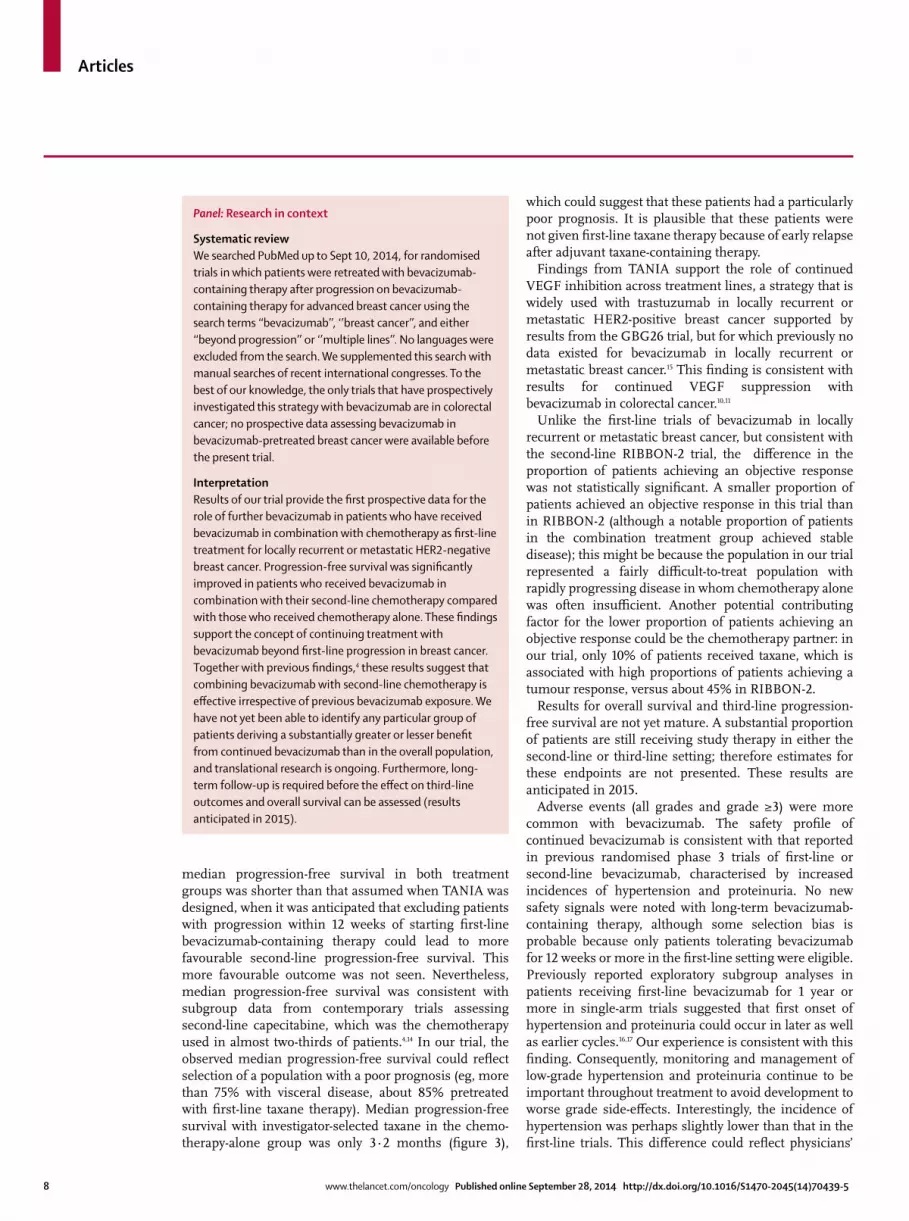
Adverse events led to discontinuation of second-line bevacizumab in 45 (18%) of 245 patients in the combina-tion group, most commonly because of proteinuria (12 [5%] patients), venous embolism (six [2%]), and pulmonary embolism (fi ve [2%]). Chemotherapy was discontinued because of adverse events in 19 (8%) of 238 patients receiving chemotherapy alone and 40 (16%) of 245 receiving combination therapy. The only adverse event leading to chemotherapy discontinuation in more than 2% of patients was hand-foot syndrome in the combination group (six [2%] patients, all receiving capecitabine). Chemotherapy doses were reduced in 88 (37%) of 238 patients receiving chemotherapy alone and 114 (47%) of 245 patients receiving combination therapy.
DiscussionThe TANIA trial showed that further bevacizumab with second-line chemotherapy signifi cantly increased progression-free survival, the study’s primary endpoint, in patients whose locally recurrent or metastatic HER2-negative breast cancer had progressed on or after fi rst-line bevacizumab-containing therapy. Of note, sensitivity analyses with adjustment for switching therapy before disease progression showed similar results to the primary analysis. The magnitude of improvement in progression-free survival (stratifi ed HR 0·75, 95% CI 0·61–0·93; log-rank p=0·0068) is very similar to that noted in the RIBBON-2 trial, which assessed the addition
of bevacizumab to second-line chemotherapy in bevacizumab-naive patients with locally recurrent or metastatic breast cancer (stratifi ed HR 0·78, 95% CI 0·64–0·93; log-rank p=0·0072).4 Although we acknowledge the limitations of cross-trial comparisons, these observations suggest that bevacizumab off ers improved progression-free survival irrespective of previous bevacizumab exposure (panel). Interestingly,
Chemotherapy alone (n=238) Chemotherapy plus bevacizumab (n=245)
Grades 1–2 Grade 3 Grade 4 Grade 5 Grades 1–2 Grade 3 Grade 4 Grade 5
Neutropenia 13 (5%) 13 (5%) 7 (3%) 0 8 (3%) 17 (7%) 12 (5%) 0
Anaemia 5 (2%) 2 (<1%) 0 0 11 (4%) 5 (2%) 0 0
Thrombocytopenia 1 (<1%) 1 (<1%) 0 0 7 (3%) 2 (<1%) 3 (1%) 0
Febrile neutropenia 0 0 4 (2%) 0 0 4 (2%) 4 (2%) 0
Proteinuria 51 (21%) 1 (<1%) 0 0 96 (39%) 17 (7%) 0 0
Hypertension 25 (11%) 17 (7%) 0 0 36 (15%) 33 (13%) 0 0
Haemorrhage 6 (3%) 0 1 (<1%) 0 19 (8%) 0 0 0
Hand-foot syndrome 25 (11%) 25 (11%) 0 0 35 (14%) 27 (11%) 0 0
Fatigue 20 (8%) 8 (3%) 0 0 24 (10%) 8 (3%) 0 0
Mucosal infl ammation 4 (2%) 1 (<1%) 0 0 13 (5%) 4 (2%) 0 0
Diarrhoea 20 (8%) 8 (3%) 0 0 19 (8%) 7 (3%) 0 0
Nausea 18 (8%) 6 (3%) 0 0 22 (9%) 4 (2%) 0 0
Vomiting 18 (8%) 3 (1%) 0 0 9 (4%) 3 (1%) 0 0
Dyspnoea 2 (<1%) 4 (2%) 1 (<1%) 0 4 (2%) 0 0 0
Pulmonary embolism 0 4 (2%) 0 0 1 (<1%) 3 (1%) 2 (<1%) 0
Increased GGT 0 5 (2%) 1 (<1%) 0 0 8 (3%) 2 (<1%) 0
Increased AST 1 (<1%) 2 (<1%) 0 0 2 (1%) 5 (2%) 0 0
Hyponatraemia 1 (<1%) 1 (<1%) 0 0 1 (<1%) 4 (2%) 1 (<1%) 0
Data are n (%). Adverse events are coded according to the Medical Dictionary for Regulatory Activities version 16.1 and graded by investigators with the Common Terminology Criteria for Adverse Events version 4.0. GGT=gamma glutamyltransferase. AST=aspartate aminotransferase.
Table 4: Adverse events occurring at any grade in more than 5% of patients or grade 3 or greater in more than 2% of patients in the second-line therapy safety population
Chemotherapy alone (n=238) Chemotherapy plus bevacizumab (n=245)
All grades Grade ≥3 All grades Grade ≥3
Hypertension 42 (18%) 17 (7%) 69 (28%) 33 (13%)
Bleeding 14 (6%) 4 (2%) 32 (13%) 1 (<1%)
Proteinuria 52 (22%) 1 (<1%) 113 (46%) 17 (7%)
Thromboembolic event 11 (5%) 8 (3%) 21 (9%) 8 (3%)
Venous 7 (3%) 5 (2%) 21 (9%) 8 (3%)
Arterial 4 (2%) 3 (1%) 0 0
Febrile neutropenia 4 (2%) 4 (2%) 8 (3%) 8 (3%)
Congestive heart failure 1 (<1%) 1 (<1%) 5 (2%) 5 (2%)
Wound-healing complication 1 (<1%) 0 4 (2%) 2 (<1%)
Fistula or abscess 2 (<1%) 0 1 (<1%) 0
Gastrointestinal perforation 0 0 2 (<1%) 1 (<1%)
Data are n (%). Adverse events grouped by category. Adverse events are coded according to the Medical Dictionary for Regulatory Activities version 16.1 and graded by investigators with the Common Terminology Criteria for Adverse Events version 4.0.
Table 5: Adverse events of special interest for bevacizumab (second-line safety population)
Articles
8 www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5
median progression-free survival in both treatment groups was shorter than that assumed when TANIA was designed, when it was anticipated that excluding patients with progression within 12 weeks of starting fi rst-line bevacizumab-containing therapy could lead to more favourable second-line progression-free survival. This more favourable outcome was not seen. Nevertheless, median progression-free survival was consistent with subgroup data from contemporary trials assessing second-line capecitabine, which was the chemotherapy used in almost two-thirds of patients.4,14 In our trial, the observed median progression-free survival could refl ect selection of a population with a poor prognosis (eg, more than 75% with visceral disease, about 85% pretreated with fi rst-line taxane therapy). Median progression-free survival with investigator-selected taxane in the chemo-therapy-alone group was only 3·2 months (fi gure 3),
which could suggest that these patients had a particularly poor prognosis. It is plausible that these patients were not given fi rst-line taxane therapy because of early relapse after adjuvant taxane-containing therapy.
Findings from TANIA support the role of continued VEGF inhibition across treatment lines, a strategy that is widely used with trastuzumab in locally recurrent or metastatic HER2-positive breast cancer supported by results from the GBG26 trial, but for which previously no data existed for bevacizumab in locally recurrent or metastatic breast cancer.15 This fi nding is consistent with results for continued VEGF suppression with bevacizumab in colorectal cancer.10,11
Unlike the fi rst-line trials of bevacizumab in locally recurrent or metastatic breast cancer, but consistent with the second-line RIBBON-2 trial, the diff erence in the proportion of patients achieving an objective response was not statistically signifi cant. A smaller proportion of patients achieved an objective response in this trial than in RIBBON-2 (although a notable proportion of patients in the combination treatment group achieved stable disease); this might be because the population in our trial represented a fairly diffi cult-to-treat population with rapidly progressing disease in whom chemotherapy alone was often insuffi cient. Another potential contributing factor for the lower proportion of patients achieving an objective response could be the chemotherapy partner: in our trial, only 10% of patients received taxane, which is associated with high proportions of patients achieving a tumour response, versus about 45% in RIBBON-2.
Results for overall survival and third-line progression-free survival are not yet mature. A substantial proportion of patients are still receiving study therapy in either the second-line or third-line setting; therefore estimates for these endpoints are not presented. These results are anticipated in 2015.
Adverse events (all grades and grade ≥3) were more common with bevacizumab. The safety profi le of continued bevacizumab is consistent with that reported in previous randomised phase 3 trials of fi rst-line or second-line bevacizumab, characterised by increased incidences of hypertension and proteinuria. No new safety signals were noted with long-term bevacizumab-containing therapy, although some selection bias is probable because only patients tolerating bevacizumab for 12 weeks or more in the fi rst-line setting were eligible. Previously reported exploratory subgroup analyses in patients receiving fi rst-line bevacizumab for 1 year or more in single-arm trials suggested that fi rst onset of hypertension and proteinuria could occur in later as well as earlier cycles.16,17 Our experience is consistent with this fi nding. Consequently, monitoring and management of low-grade hypertension and proteinuria continue to be important throughout treatment to avoid development to worse grade side-eff ects. Interestingly, the incidence of hypertension was perhaps slightly lower than that in the fi rst-line trials. This diff erence could refl ect physicians’
Panel: Research in context
Systematic reviewWe searched PubMed up to Sept 10, 2014, for randomised trials in which patients were retreated with bevacizumab-containing therapy after progression on bevacizumab-containing therapy for advanced breast cancer using the search terms ‘‘bevacizumab’’, ‘’breast cancer’’, and either ‘‘beyond progression’’ or ‘’multiple lines’’. No languages were excluded from the search. We supplemented this search with manual searches of recent international congresses. To the best of our knowledge, the only trials that have prospectively investigated this strategy with bevacizumab are in colorectal cancer; no prospective data assessing bevacizumab in bevacizumab-pretreated breast cancer were available before the present trial.
InterpretationResults of our trial provide the fi rst prospective data for the role of further bevacizumab in patients who have received bevacizumab in combination with chemotherapy as fi rst-line treatment for locally recurrent or metastatic HER2-negative breast cancer. Progression-free survival was signifi cantly improved in patients who received bevacizumab in combination with their second-line chemotherapy compared with those who received chemotherapy alone. These fi ndings support the concept of continuing treatment with bevacizumab beyond fi rst-line progression in breast cancer. Together with previous fi ndings,4 these results suggest that combining bevacizumab with second-line chemotherapy is eff ective irrespective of previous bevacizumab exposure. We have not yet been able to identify any particular group of patients deriving a substantially greater or lesser benefi t from continued bevacizumab than in the overall population, and translational research is ongoing. Furthermore, long-term follow-up is required before the eff ect on third-line outcomes and overall survival can be assessed (results anticipated in 2015).

Articles
www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5 9
experience with bevacizumab in the fi rst-line treatment of each patient: notably 141 (57%) of patients in the combination group had a history of hypertension during previous bevacizumab. Those patients with problematic or uncon trollable hypertension during previous bevacizumab were not considered for our trial. Therefore, the patient population represented a group of patients with well-managed hypertension, making the likelihood of an indication for more intensive anti-hypertensive therapy (one of the criteria defi ning grade 3 hyper-tension) less probable.
Choice of chemotherapy in our trial was at the investigator’s discretion, enabling physicians to select the most appropriate chemotherapy for every individual based on clinical judgement and factors including disease and patient characteristics, previous treatment, and patient preference. This pragmatic approach refl ects clinical practice, but the heterogeneity of the chemo-therapy backbone might be considered a limitation of the trial, as could be the open-label design. Most patients (about 60%) received capecitabine as their second-line therapy, as might be expected in a population treated mainly with fi rst-line bevacizumab plus taxane therapy. In the small subgroup of patients (51 [10%] of 494) receiving second-line vinorelbine, the progression-free survival HR was 0·41 (95% CI 0·22–0·75). The small sample size and investigator-selected chemotherapy preclude any fi rm conclusion about the effi cacy of bevacizumab plus vinorelbine, but this fi nding at least allays potential concerns or hypotheses about a putative antagonistic eff ect. The contrasting vinorelbine subgroup fi ndings between RIBBON-2 and our trial also emphasise the limitations and risks of over-interpretation of post-hoc exploratory analyses in small subgroups, particularly in an open-label trial with chemotherapy chosen by the investigator and thus infl uenced by a wide range of factors that might aff ect prognosis.
An important strength of the design of our trial is the continuation of allocated treatment (bevacizumab vs non-bevacizumab) from the second-line setting into the third-line setting. Crossover to bevacizumab after disease progression on second-line therapy was not allowed in the chemotherapy-alone group and, conversely, patients randomly assigned to second-line bevacizumab could continue to receive bevacizumab in the third-line setting (unless toxicity prevented further bevacizumab). Although this continuation has no eff ect on the results of second-line progression-free survival, the eff ect of such a trial design might become apparent when the fi nal overall survival results and the secondary endpoint of progression-free survival from randomisation until third-line disease progression or death are available. Mandating whether or not a patient could receive bevacizumab in subsequent treatment lines was not considered reasonable.
These clinical results are consistent with preclinical models suggesting that continuous VEGF suppression is
necessary to maximise the benefi t of bevacizumab6 and restrict regrowth after bevacizumab.18
The strategy of continued VEGF inhibition has changed clinical practice in colorectal cancer based on an improvement in median progression-free survival from 4·1 months to 5·7 months and in median overall survival from 22·5 months to 23·9 months.10 This approach is under evaluation in ongoing randomised phase 3 trials in platinum-sensitive ovarian cancer, non-small-cell lung cancer,19 and glioblastoma.20 Another important aspect in evaluation of this strategy in locally recurrent or metastatic breast cancer is identifi cation of those patients who might benefi t most from continued bevacizumab, because the benefi t is unlikely to be considered universally as clinically meaningful. Subgroup analyses did not indicate a particular population of patients that derive greater or smaller benefi t from continued bevacizumab with respect to the HRs, although absolute diff erences vary according to prognosis. Ongoing translational research and fi nal effi cacy results could provide greater insight. Nevertheless, our results show that in the overall study population, further bevacizumab signifi cantly improves progression-free survival; additionally, the results show that second-line bevacizumab increases progression-free survival irrespective of previous bevacizumab exposure, suggesting that this could be a valid option for patients responding to and tolerating fi rst-line bevacizumab-containing therapy.
ContributorsGvM, FP, JC, EV, NM, CZ, and JG designed the trial together with
representatives of the study funder. GvM, FP, JC, EV, NM, CZ, CVi, GR,
IL, EC, MDL, CVe, and JG were involved in data collection. UF was
involved in data analysis. All authors participated in data interpretation,
and revision and fi nalisation of the report for submission.
Declaration of interestsGvM reports grants from Roche for parts of the present study conduct
and honoraria from Roche for advisory board meetings and lectures. FP
has received honoraria from Roche, Eisai, and GlaxoSmithKline. JC
reports personal fees from Roche during the conduct of the study, and
personal fees from Celgene, Novartis, and Eisai outside the submitted
work. EV reports grants and personal fees from Roche and Pfi zer, and
personal fees from Novartis, AstraZeneca, and Astellas, all outside the
submitted work. NM has received research grants and honoraria for
advisory boards from Roche. CZ has received honoraria from Roche for
advisory boards. GR reports personal fees from Roche, outside the
submitted work. MDL has received honoraria for lectures and advisory
boards from Roche, Eisai, GlaxoSmithKline, and Celgene. CVe reports
personal fees and non-fi nancial support from Roche and Novartis,
personal fees from GlaxoSmithKline, and non-fi nancial support from
Eisai, all outside the submitted work. SdD and SS own shares and are
employees of F Hoff mann-La Roche. UF is an employee of F Hoff mann-
La Roche. JG has received a travel grant and consultancy and speaker
honoraria from Roche, Eisai, Teva, and Genomic Health, consultancy
honoraria from Sanofi -Aventis, consultancy and speaker honoraria from
Novartis, and speaker honoraria from GlaxoSmithKline. CVi, IL, and EC
have nothing to disclose.
AcknowledgmentsWe thank all the patients who participated in the TANIA trial, the study
teams, and the investigators. We are also grateful to members of the
independent data monitoring committee (Marc Buyse [Chair],
Matti Aapro, Paul Ellis), Anja-Alexandra Duenne, Gill Hales, and
Kerstin Ebel (all from F Hoff mann-La Roche), the clinical operations
team (F Hoff mann-La Roche: Ciaran Murphy, Sophie Clavelin, and

Articles
10 www.thelancet.com/oncology Published online September 28, 2014 http://dx.doi.org/10.1016/S1470-2045(14)70439-5
Isabelle Statovci; Parexel International: Judith Ruijter and
Robert Carrington), and the biostatisticians (F Hoff mann-La Roche:
Lada Mitchell and Corrado Bernasconi; Parexel International:
Thomas Boulet, Silke Hochstaedter, and Benjamin Piske). Support for
third-party writing assistance for this report, supplied by Jennifer Kelly
(Medi-Kelsey Ltd, Ashbourne, UK) was provided by F Hoff mann-La
Roche Ltd.
References1 Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab
versus paclitaxel alone for metastatic breast cancer. N Engl J Med 2007; 357: 2666–76.
2 Miles DW, Chan A, Dirix LY, et al. Phase III study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the fi rst-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol 2010; 28: 3239–47.
3 Robert NJ, Diéras V, Glaspy J, et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for fi rst-line treatment of human epidermal growth factor receptor 2-negative locally recurrent or metastatic breast cancer. J Clin Oncol 2011; 29: 1252–60.
4 Brufsky AM, Hurvitz S, Perez E, et al. RIBBON-2: a randomized, double-blind, placebo-controlled, phase III trial evaluating the effi cacy and safety of bevacizumab in combination with chemotherapy for second-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol 2011; 29: 4286–93.
5 Crawford Y, Ferrara N. VEGF inhibition: insights from preclinical and clinical studies. Cell Tissue Res 2009; 335: 261–69.
6 Bagri A, Berry L, Gunter B, et al. Eff ects of anti-VEGF treatment duration on tumor growth, tumor regrowth, and treatment effi cacy. Clin Cancer Res 2010; 16: 3887–900.
7 Grothey A, Sugrue MM, Purdie DM, et al. Bevacizumab beyond fi rst progression is associated with prolonged overall survival in metastatic colorectal cancer: results from a large observational cohort study (BRiTE). J Clin Oncol 2008; 26: 5326–34.
8 Grothey A, Flick ED, Cohn AL, et al. Bevacizumab exposure beyond fi rst disease progression in patients with metastatic colorectal cancer: analyses of the ARIES observational cohort study. Pharmacoepidemiol Drug Saf 2014; 23: 726–34.
9 Cartwright TH, Yim YM, Yu E, Chung H, Halm M, Forsyth M. Survival outcomes of bevacizumab beyond progression in metastatic colorectal cancer patients treated in US community oncology. Clin Colorectal Cancer 2012; 11: 238–46.
10 Bennouna J, Sastre J, Arnold D, et al; ML18147 Study Investigators. Continuation of bevacizumab after fi rst progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trial. Lancet Oncol 2013; 14: 29–37.
11 Masi G, Loupakis F, Salvatore L, et al. A randomized phase III study evaluating the continuation of bevacizumab (BV) beyond progression in metastatic colorectal cancer (mCRC) patients (pts) who received BV as part of fi rst-line treatment: results of the BEBYP trial by the Gruppo Oncologico Nord Ovest (GONO). Ann Oncol 2012; 23: ixe9 (LBA17).
12 Fleming TR, Rothmann MD, Lu HL. Issues in using progression-free survival when evaluating oncology products. J Clin Oncol 2009; 27: 2874–80.
13 Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials 1996; 17: 343–46.
14 Baselga J, Segalla JG, Roché H, et al. Sorafenib in combination with capecitabine: an oral regimen for patients with HER2-negative locally advanced or metastatic breast cancer. J Clin Oncol 2012; 30: 1484–91.
15 von Minckwitz G, du Bois A, Schmidt M, et al. Trastuzumab beyond progression in human epidermal growth factor receptor 2-positive advanced breast cancer: a German Breast Group 26/Breast International Group 03-05 study. J Clin Oncol 2009; 27: 1999–2006.
16 Smith I, Pierga JY, Biganzoli L, et al. Final overall survival results and eff ect of prolonged (≥ 1 year) fi rst-line bevacizumab-containing therapy for metastatic breast cancer in the ATHENA trial. Breast Cancer Res Treat 2011; 130: 133–43.
17 Aogi K, Masuda N, Ohno S, et al. First-line bevacizumab in combination with weekly paclitaxel for metastatic breast cancer: effi cacy and safety results from a large, open-label, single-arm Japanese study. Breast Cancer Res Treat 2011; 129: 829–38.
18 Ellis LM, Reardon DA. Cancer: the nuances of therapy. Nature 2009; 458: 290–92.
19 Gridelli C, Bennouna J, de Castro J, et al. Randomized phase IIIb trial evaluating the continuation of bevacizumab beyond disease progression in patients with advanced non-squamous non-small-cell lung cancer after fi rst-line treatment with bevacizumab plus platinum-based chemotherapy: treatment rationale and protocol dynamics of the AvaALL (MO22097) trial. Clin Lung Cancer 2011; 12: 407–11.
20 Brandes AA, Mason W, Pichler J, et al. Can bevacizumab prolong survival for glioblastoma patients through multiple lines of therapy? Future Oncol 2014; 10: 1137–45.