barbed sutures and wound complications in plastic surgery
TRANSCRIPT
Barbed Sutures and Wound Complications in Plastic
Surgery: An Analysis of Outcomes
Roberto Cortez, BS, Eric Lazcano, BS, Travis Miller, BS, Rachel E. Hein, BS, Ryan
S. Constantine, BS, Kendall Anigian, BS, Kathryn E. Davis, PhD, Jeffrey M. Kenkel,
MD
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
Barbed Sutures and Wound Complicationsin Plastic Surgery: An Analysis of Outcomes
Roberto Cortez, BS; Eric Lazcano, BS; Travis Miller, BS;Rachel E. Hein, BS; Ryan S. Constantine, BS; Kendall Anigian, BS;Kathryn E. Davis, PhD; and Jeffrey M. Kenkel, MD
AbstractBackground: Barbed sutures may expedite dermal approximation and improve tissue support while requiring less time and material than conventionalsutures. Several types of barbed sutures are available, each with unique advantages.Objectives: The authors sought to determine whether the incidence of complications differed after wound approximation in plastic surgery whenvarious brands of barbed vs nonbarbed traditional sutures were employed.Methods: The authors conducted a retrospective review of outcomes in body contouring, free flap, and breast reconstruction. Suture type and closuremethod were noted for each case. The number of complications after traditional 2-layer closure with nonbarbed sutures was compared with the number of com-plications after closure via 1- and 2-layer techniques with several brands of barbed sutures, and the brands of barbed sutures were compared with each other.Results: A total of 1011 unique surgical procedures, including 298 procedures with barbed sutures and 713 procedures with nonbarbed sutures, wereperformed by 5 members of the plastic surgery faculty. The 2-layer technique with barbed sutures was associated with significantly higher rates of woundseparation than traditional methods. Excessive erythema along the incision site was significantly more frequent with Quill barbed sutures than with V-Locbarbed sutures.Conclusions: Barbed sutures were associated with significantly higher rates of minor wound complications, specifically when the 2-layer closure tech-nique was performed. Significantly higher rates of erythema were associated with Quill barbed sutures than with V-Loc barbed sutures.
Level of Evidence: 4
RiskAccepted for publication June 18, 2014.
Technological advancements aimed at reducing operatingtimes and complications have substantially increased thenumber of wound closure tools available to the plasticsurgeon. An example of this is the emergence of barbedsutures in the 1960s and their modifications over subsequentdecades.1 Early barbed suture models were intended forlifting and shaping of tissue; however, when maintenance oflong-term outcomes was unsatisfactory, the utility of barbedsutures was reevaluated as a knot-free device for expeditioussoft-tissue approximation. Subsequent clinical researchsupported the advantages claimed by suture manufacturers,including significantly reduced operating times3,4 withminimal sacrifice of closure strength and scar cosmesis.5,6
Contrary findings have included higher costs, complications
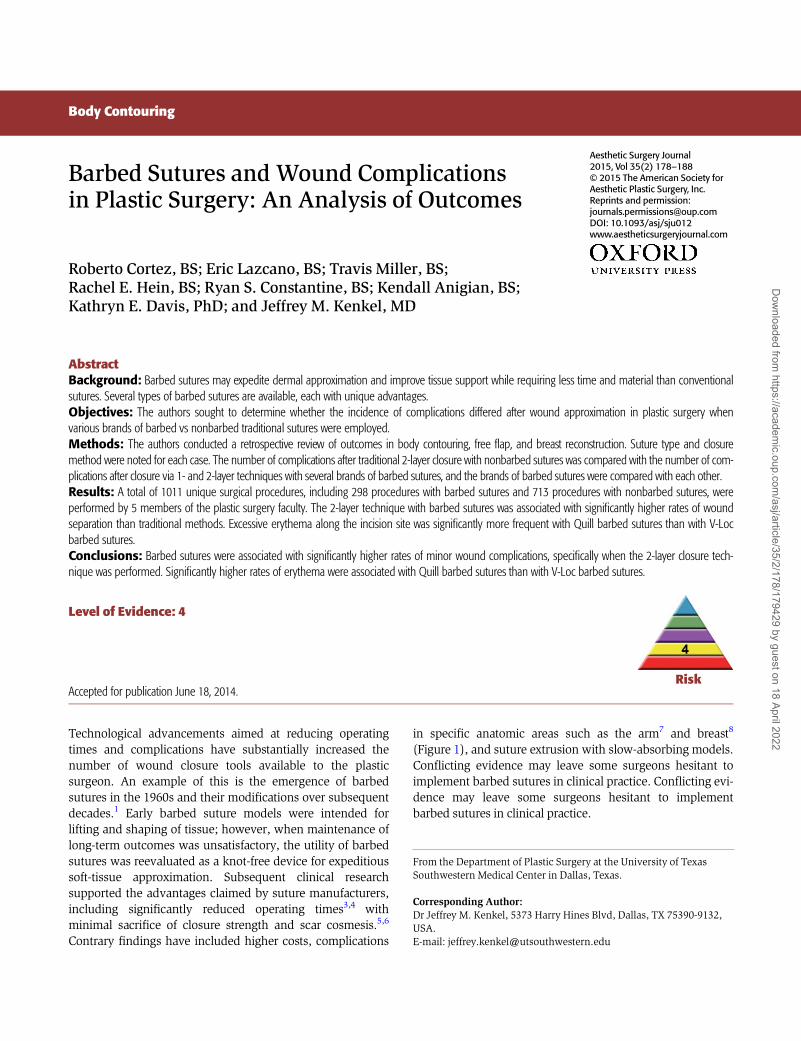
in specific anatomic areas such as the arm7 and breast8
(Figure 1), and suture extrusion with slow-absorbing models.Conflicting evidence may leave some surgeons hesitant toimplement barbed sutures in clinical practice. Conflicting evi-dence may leave some surgeons hesitant to implementbarbed sutures in clinical practice.
From the Department of Plastic Surgery at the University of TexasSouthwestern Medical Center in Dallas, Texas.
Corresponding Author:Dr Jeffrey M. Kenkel, 5373 Harry Hines Blvd, Dallas, TX 75390-9132,USA.E-mail: [email protected]
Body Contouring
Aesthetic Surgery Journal2015, Vol 35(2) 178–188© 2015 The American Society forAesthetic Plastic Surgery, Inc.Reprints and permission:[email protected]: 10.1093/asj/sju012www.aestheticsurgeryjournal.com
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
Currently manufactured barbed sutures include theQuill Self-Retaining System (SRS; Angiotech, Vancouver,BC, Canada), the V-Loc (Covidien, Dublin, Ireland), andthe Stratafix (Ethicon, Somerville, NJ). Results of recentstudies demonstrated that barbed sutures are markedlymore expensive than traditional wound-closure methods,with V-Loc 90 sutures costing approximately 6 times morethan Vicryl sutures and twice as much as Monocryl sutures(both from Ethicon) per strand.3 Quill polydioxanone(PDO) sutures may cost 7-fold more than Biosyn sutures(Covidien), but have been shown to be more cost effectiveoverall due to a reduction in operating room and anesthesia-related fees.8
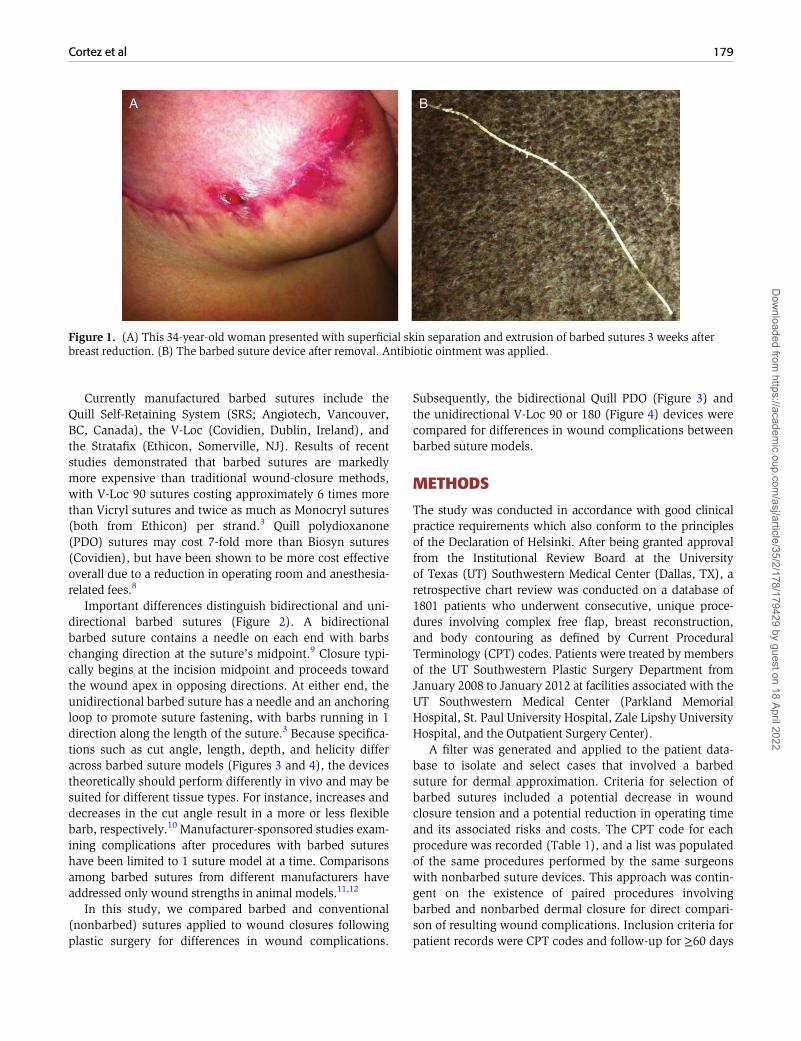
Important differences distinguish bidirectional and uni-directional barbed sutures (Figure 2). A bidirectionalbarbed suture contains a needle on each end with barbschanging direction at the suture’s midpoint.9 Closure typi-cally begins at the incision midpoint and proceeds towardthe wound apex in opposing directions. At either end, theunidirectional barbed suture has a needle and an anchoringloop to promote suture fastening, with barbs running in 1direction along the length of the suture.3 Because specifica-tions such as cut angle, length, depth, and helicity differacross barbed suture models (Figures 3 and 4), the devicestheoretically should perform differently in vivo and may besuited for different tissue types. For instance, increases anddecreases in the cut angle result in a more or less flexiblebarb, respectively.10 Manufacturer-sponsored studies exam-ining complications after procedures with barbed sutureshave been limited to 1 suture model at a time. Comparisonsamong barbed sutures from different manufacturers haveaddressed only wound strengths in animal models.11,12
In this study, we compared barbed and conventional(nonbarbed) sutures applied to wound closures followingplastic surgery for differences in wound complications.
Subsequently, the bidirectional Quill PDO (Figure 3) andthe unidirectional V-Loc 90 or 180 (Figure 4) devices werecompared for differences in wound complications betweenbarbed suture models.
METHODS
The study was conducted in accordance with good clinicalpractice requirements which also conform to the principlesof the Declaration of Helsinki. After being granted approvalfrom the Institutional Review Board at the Universityof Texas (UT) Southwestern Medical Center (Dallas, TX), aretrospective chart review was conducted on a database of1801 patients who underwent consecutive, unique proce-dures involving complex free flap, breast reconstruction,and body contouring as defined by Current ProceduralTerminology (CPT) codes. Patients were treated by membersof the UT Southwestern Plastic Surgery Department fromJanuary 2008 to January 2012 at facilities associated with theUT Southwestern Medical Center (Parkland MemorialHospital, St. Paul University Hospital, Zale Lipshy UniversityHospital, and the Outpatient Surgery Center).
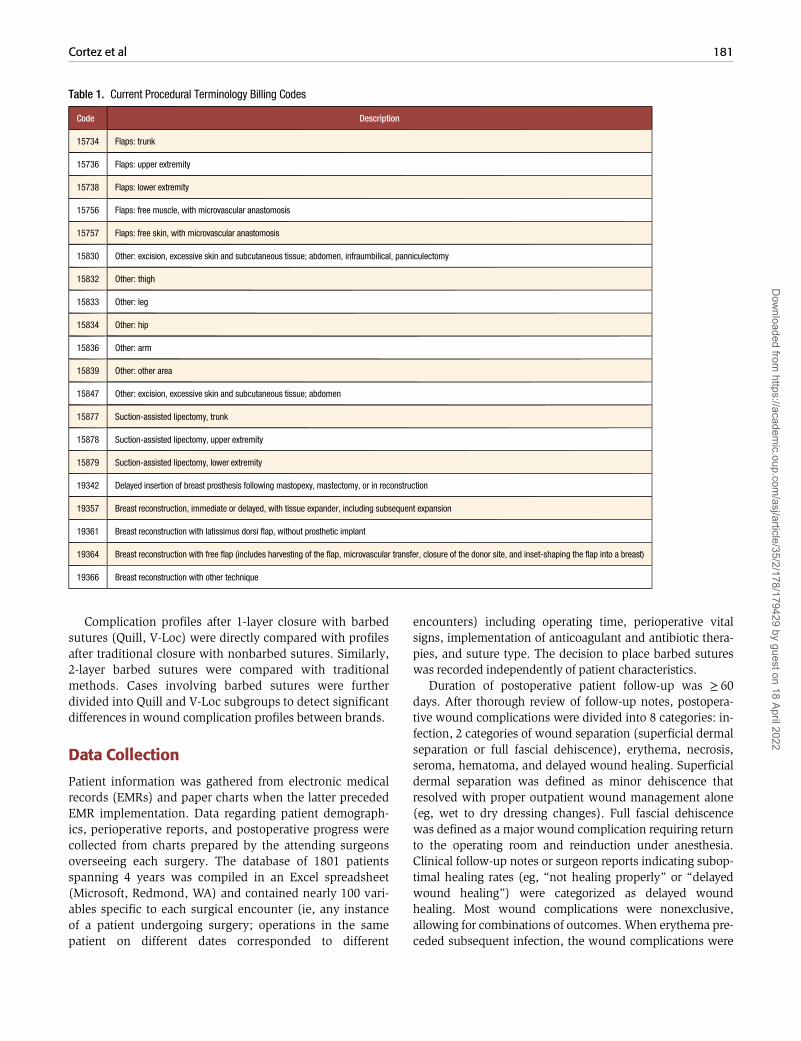
A filter was generated and applied to the patient data-base to isolate and select cases that involved a barbedsuture for dermal approximation. Criteria for selection ofbarbed sutures included a potential decrease in woundclosure tension and a potential reduction in operating timeand its associated risks and costs. The CPT code for eachprocedure was recorded (Table 1), and a list was populatedof the same procedures performed by the same surgeonswith nonbarbed suture devices. This approach was contin-gent on the existence of paired procedures involvingbarbed and nonbarbed dermal closure for direct compari-son of resulting wound complications. Inclusion criteria forpatient records were CPT codes and follow-up for ≥60 days
Figure 1. (A) This 34-year-old woman presented with superficial skin separation and extrusion of barbed sutures 3 weeks afterbreast reduction. (B) The barbed suture device after removal. Antibiotic ointment was applied.
Cortez et al 179
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
to allow for sufficient assessment postoperatively. Patientrecords with <60 days of follow-up were excluded fromthe study. Age, body mass index (BMI), and other comor-bidities were not considered in the chart selection process.
In some cases, multiple CPT codes were associated withthe same chart (eg, liposuction combined with other proce-dures). However, no charts employing barbed sutures fordermal closure involved liposuction alone.
Figure 2. (A) The Covidien V-Loc unidirectional barbed suture, with anchoring loop and needle at opposite ends. (B) Magnifiedanchoring loop. (C) The Angiotech Quill bidirectional barbed suture, with barb orientation change at the suture midpoint. (D)Magnified device showing change in barb orientation.
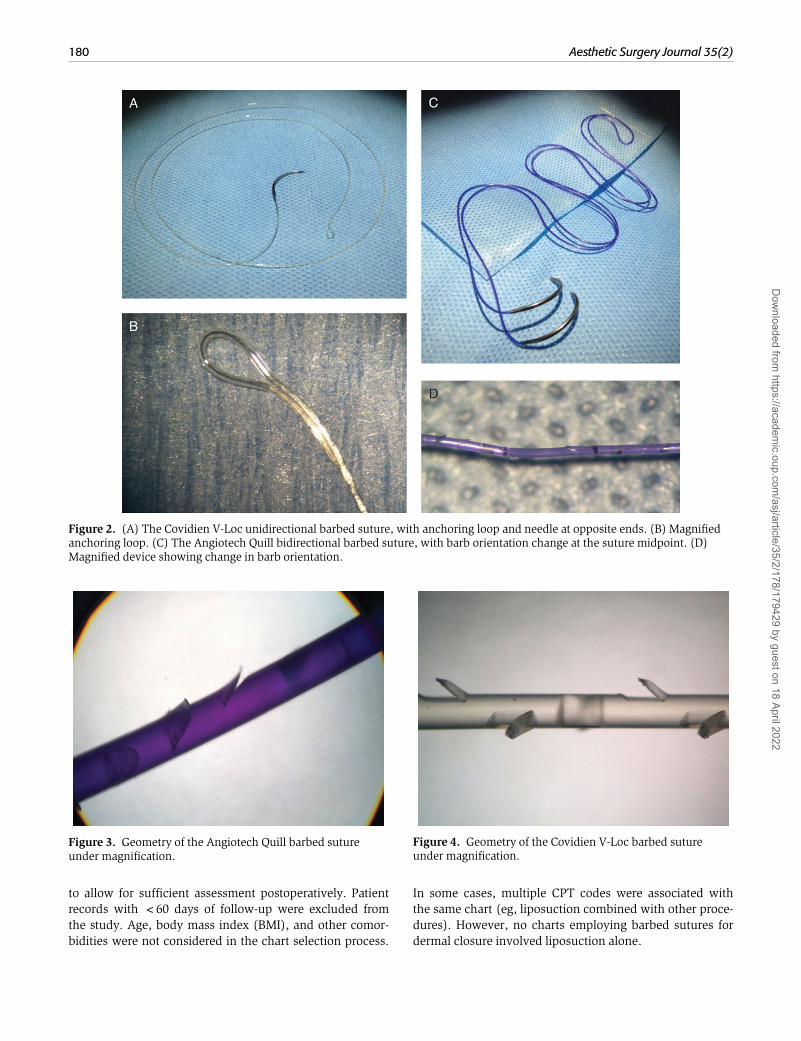
Figure 3. Geometry of the Angiotech Quill barbed sutureunder magnification.
Figure 4. Geometry of the Covidien V-Loc barbed sutureunder magnification.
180 Aesthetic Surgery Journal 35(2)
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
Complication profiles after 1-layer closure with barbedsutures (Quill, V-Loc) were directly compared with profilesafter traditional closure with nonbarbed sutures. Similarly,2-layer barbed sutures were compared with traditionalmethods. Cases involving barbed sutures were furtherdivided into Quill and V-Loc subgroups to detect significantdifferences in wound complication profiles between brands.
Data Collection
Patient information was gathered from electronic medicalrecords (EMRs) and paper charts when the latter precededEMR implementation. Data regarding patient demograph-ics, perioperative reports, and postoperative progress werecollected from charts prepared by the attending surgeonsoverseeing each surgery. The database of 1801 patientsspanning 4 years was compiled in an Excel spreadsheet(Microsoft, Redmond, WA) and contained nearly 100 vari-ables specific to each surgical encounter (ie, any instanceof a patient undergoing surgery; operations in the samepatient on different dates corresponded to different
encounters) including operating time, perioperative vitalsigns, implementation of anticoagulant and antibiotic thera-pies, and suture type. The decision to place barbed sutureswas recorded independently of patient characteristics.
Duration of postoperative patient follow-up was ≥ 60days. After thorough review of follow-up notes, postopera-tive wound complications were divided into 8 categories: in-fection, 2 categories of wound separation (superficial dermalseparation or full fascial dehiscence), erythema, necrosis,seroma, hematoma, and delayed wound healing. Superficialdermal separation was defined as minor dehiscence thatresolved with proper outpatient wound management alone(eg, wet to dry dressing changes). Full fascial dehiscencewas defined as a major wound complication requiring returnto the operating room and reinduction under anesthesia.Clinical follow-up notes or surgeon reports indicating subop-timal healing rates (eg, “not healing properly” or “delayedwound healing”) were categorized as delayed woundhealing. Most wound complications were nonexclusive,allowing for combinations of outcomes. When erythema pre-ceded subsequent infection, the wound complications were
Table 1. Current Procedural Terminology Billing Codes
Code Description
15734 Flaps: trunk
15736 Flaps: upper extremity
15738 Flaps: lower extremity
15756 Flaps: free muscle, with microvascular anastomosis
15757 Flaps: free skin, with microvascular anastomosis
15830 Other: excision, excessive skin and subcutaneous tissue; abdomen, infraumbilical, panniculectomy
15832 Other: thigh
15833 Other: leg
15834 Other: hip
15836 Other: arm
15839 Other: other area
15847 Other: excision, excessive skin and subcutaneous tissue; abdomen
15877 Suction-assisted lipectomy, trunk
15878 Suction-assisted lipectomy, upper extremity
15879 Suction-assisted lipectomy, lower extremity
19342 Delayed insertion of breast prosthesis following mastopexy, mastectomy, or in reconstruction
19357 Breast reconstruction, immediate or delayed, with tissue expander, including subsequent expansion
19361 Breast reconstruction with latissimus dorsi flap, without prosthetic implant
19364 Breast reconstruction with free flap (includes harvesting of the flap, microvascular transfer, closure of the donor site, and inset-shaping the flap into a breast)
19366 Breast reconstruction with other technique
Cortez et al 181
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
exclusive. Erythema was defined as a markedly increasedinflammatory response that prompted documentation in themedical record and that resolved without antibiotic treat-ment. Patients requiring antibiotics or explicitly demonstrat-ing signs of infection (eg, purulence along incision site,cellulitis, or marked tenderness) as described in the medicalrecord were recorded as infection rather than erythema.Because superficial dermal separation and full fascial dehis-cence could not occur simultaneously in 1 patient, thesewound complications were exclusive.
Statistical Analysis
Contingency tables (2× 2) were constructed for each ofthe 8 types of wound complications along with the pres-ence or absence of a barbed suture. Outcomes reported asdichotomous variables (ie, yes or no) were analyzed withthe Fisher exact test, with statistical significance defined asP< .05. Differences in continuous variables such as ageand BMI were ascertained by means of the t test.
RESULTS
A total of 1075 unique surgical encounters were included inthe study. From the 1801 original surgical encounters, 726encounters consisted of cosmetic cases to include fat injec-tion, liposuction, and rhinoplasty where barbed sutureswere not used. Following exclusion of these cases, a totalof 1075 unique surgical encounters were included in thestudy. Of these, 64 were excluded due to lack of sufficientdata (eg, no suture type specified, no barbed/nonbarbedCPT codes). Of the remaining 1011 patients, 298 receivedbarbed and 713 received nonbarbed sutures. Quill barbedsutures were employed in 62 surgical encounters (34[55.6%] PDO, 16 [25.4%] Monoderm, 12 [19.0%] combi-nation), whereas V-Loc sutures were utilized in 228 cases(200 [87.7%] V-Loc 90, 10 [4.4%] V-Loc 180, 18 [7.9%]combination). The larger percentage of V-Loc cases com-pared with Quill cases was attributed to the emergence andsteadily increasing popularity of the former from late 2008until 2009. The distribution of procedures employingbarbed vs nonbarbed sutures are listed in Table 2.
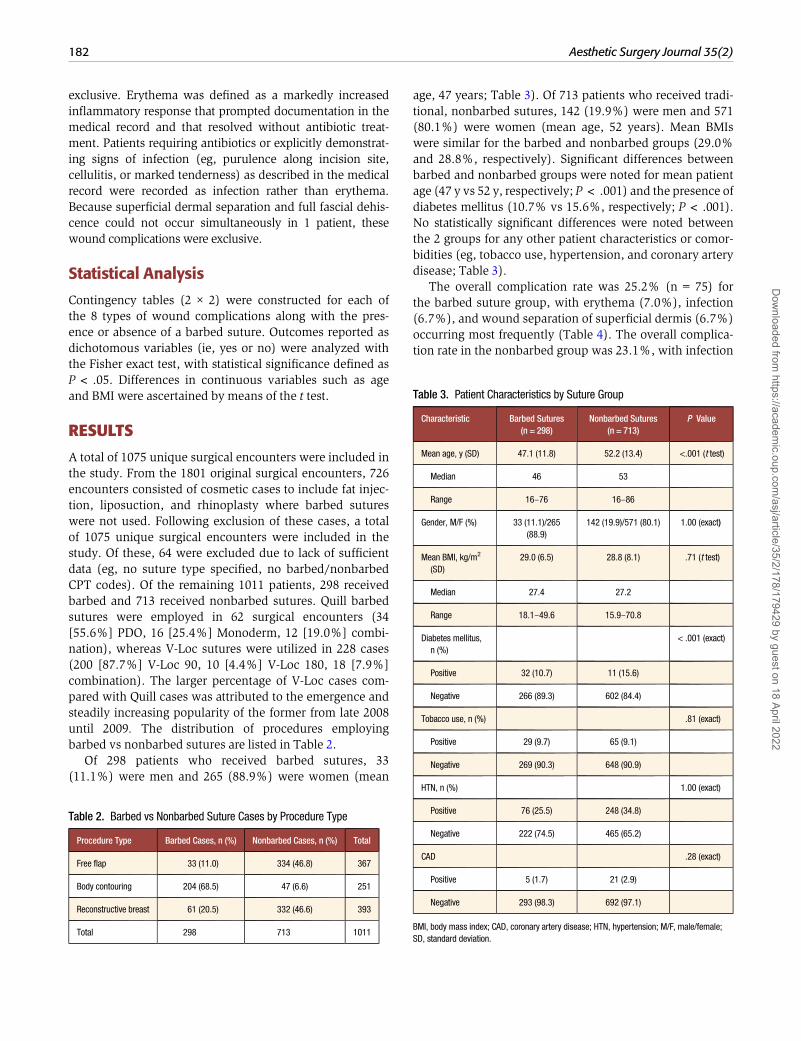
Of 298 patients who received barbed sutures, 33(11.1%) were men and 265 (88.9%) were women (mean
age, 47 years; Table 3). Of 713 patients who received tradi-tional, nonbarbed sutures, 142 (19.9%) were men and 571(80.1%) were women (mean age, 52 years). Mean BMIswere similar for the barbed and nonbarbed groups (29.0%and 28.8%, respectively). Significant differences betweenbarbed and nonbarbed groups were noted for mean patientage (47 y vs 52 y, respectively; P< .001) and the presence ofdiabetes mellitus (10.7% vs 15.6%, respectively; P< .001).No statistically significant differences were noted betweenthe 2 groups for any other patient characteristics or comor-bidities (eg, tobacco use, hypertension, and coronary arterydisease; Table 3).
The overall complication rate was 25.2% (n= 75) forthe barbed suture group, with erythema (7.0%), infection(6.7%), and wound separation of superficial dermis (6.7%)occurring most frequently (Table 4). The overall complica-tion rate in the nonbarbed group was 23.1%, with infection
Table 2. Barbed vs Nonbarbed Suture Cases by Procedure Type
Procedure Type Barbed Cases, n (%) Nonbarbed Cases, n (%) Total
Free flap 33 (11.0) 334 (46.8) 367
Body contouring 204 (68.5) 47 (6.6) 251
Reconstructive breast 61 (20.5) 332 (46.6) 393
Total 298 713 1011
Table 3. Patient Characteristics by Suture Group
Characteristic Barbed Sutures(n = 298)
Nonbarbed Sutures(n = 713)
P Value
Mean age, y (SD) 47.1 (11.8) 52.2 (13.4) <.001 (t test)
Median 46 53
Range 16–76 16–86
Gender, M/F (%) 33 (11.1)/265(88.9)
142 (19.9)/571 (80.1) 1.00 (exact)
Mean BMI, kg/m2
(SD)29.0 (6.5) 28.8 (8.1) .71 (t test)
Median 27.4 27.2
Range 18.1–49.6 15.9–70.8
Diabetes mellitus,n (%)
< .001 (exact)
Positive 32 (10.7) 11 (15.6)
Negative 266 (89.3) 602 (84.4)
Tobacco use, n (%) .81 (exact)
Positive 29 (9.7) 65 (9.1)
Negative 269 (90.3) 648 (90.9)
HTN, n (%) 1.00 (exact)
Positive 76 (25.5) 248 (34.8)
Negative 222 (74.5) 465 (65.2)
CAD .28 (exact)
Positive 5 (1.7) 21 (2.9)
Negative 293 (98.3) 692 (97.1)
BMI, body mass index; CAD, coronary artery disease; HTN, hypertension; M/F, male/female;SD, standard deviation.
182 Aesthetic Surgery Journal 35(2)
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
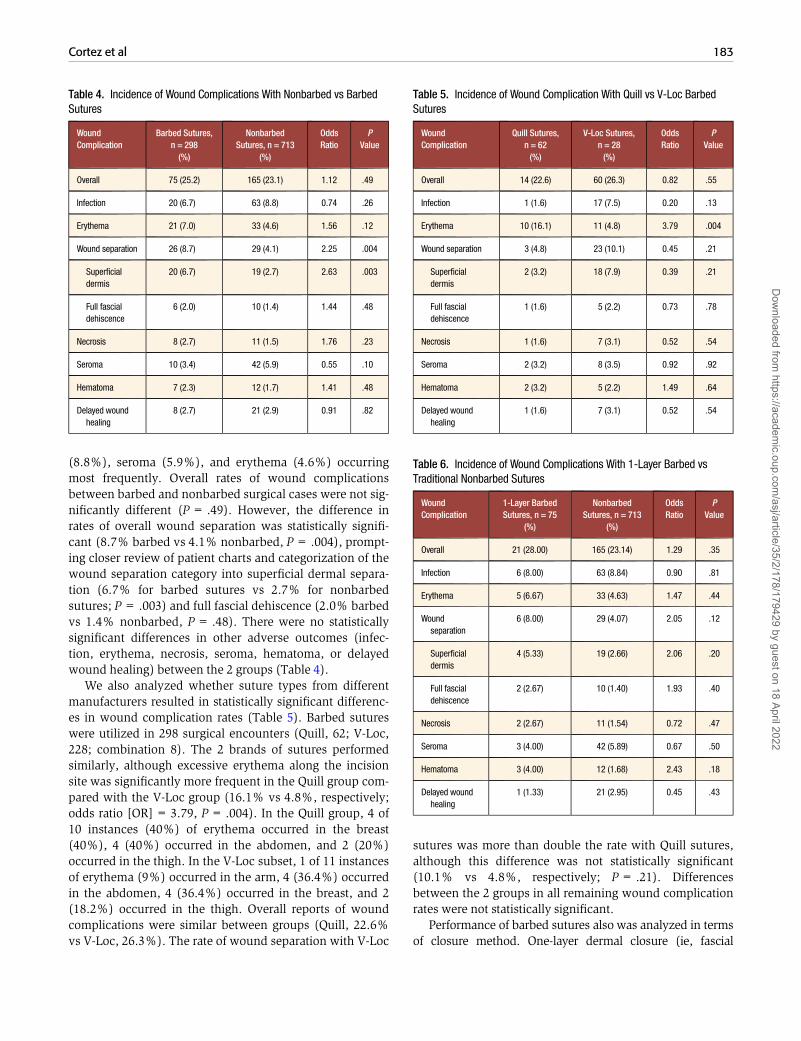
(8.8%), seroma (5.9%), and erythema (4.6%) occurringmost frequently. Overall rates of wound complicationsbetween barbed and nonbarbed surgical cases were not sig-nificantly different (P= .49). However, the difference inrates of overall wound separation was statistically signifi-cant (8.7% barbed vs 4.1% nonbarbed, P= .004), prompt-ing closer review of patient charts and categorization of thewound separation category into superficial dermal separa-tion (6.7% for barbed sutures vs 2.7% for nonbarbedsutures; P= .003) and full fascial dehiscence (2.0% barbedvs 1.4% nonbarbed, P= .48). There were no statisticallysignificant differences in other adverse outcomes (infec-tion, erythema, necrosis, seroma, hematoma, or delayedwound healing) between the 2 groups (Table 4).
We also analyzed whether suture types from differentmanufacturers resulted in statistically significant differenc-es in wound complication rates (Table 5). Barbed sutureswere utilized in 298 surgical encounters (Quill, 62; V-Loc,228; combination 8). The 2 brands of sutures performedsimilarly, although excessive erythema along the incisionsite was significantly more frequent in the Quill group com-pared with the V-Loc group (16.1% vs 4.8%, respectively;odds ratio [OR]= 3.79, P= .004). In the Quill group, 4 of10 instances (40%) of erythema occurred in the breast(40%), 4 (40%) occurred in the abdomen, and 2 (20%)occurred in the thigh. In the V-Loc subset, 1 of 11 instancesof erythema (9%) occurred in the arm, 4 (36.4%) occurredin the abdomen, 4 (36.4%) occurred in the breast, and 2(18.2%) occurred in the thigh. Overall reports of woundcomplications were similar between groups (Quill, 22.6%vs V-Loc, 26.3%). The rate of wound separation with V-Loc
sutures was more than double the rate with Quill sutures,although this difference was not statistically significant(10.1% vs 4.8%, respectively; P= .21). Differencesbetween the 2 groups in all remaining wound complicationrates were not statistically significant.
Performance of barbed sutures also was analyzed in termsof closure method. One-layer dermal closure (ie, fascial
Table 4. Incidence of Wound Complications With Nonbarbed vs BarbedSutures
WoundComplication
Barbed Sutures,n = 298(%)
NonbarbedSutures, n = 713
(%)
OddsRatio
PValue
Overall 75 (25.2) 165 (23.1) 1.12 .49
Infection 20 (6.7) 63 (8.8) 0.74 .26
Erythema 21 (7.0) 33 (4.6) 1.56 .12
Wound separation 26 (8.7) 29 (4.1) 2.25 .004
Superficialdermis
20 (6.7) 19 (2.7) 2.63 .003
Full fascialdehiscence
6 (2.0) 10 (1.4) 1.44 .48
Necrosis 8 (2.7) 11 (1.5) 1.76 .23
Seroma 10 (3.4) 42 (5.9) 0.55 .10
Hematoma 7 (2.3) 12 (1.7) 1.41 .48
Delayed woundhealing
8 (2.7) 21 (2.9) 0.91 .82
Table 5. Incidence of Wound Complication With Quill vs V-Loc BarbedSutures
WoundComplication
Quill Sutures,n = 62(%)
V-Loc Sutures,n = 28(%)
OddsRatio
PValue
Overall 14 (22.6) 60 (26.3) 0.82 .55
Infection 1 (1.6) 17 (7.5) 0.20 .13
Erythema 10 (16.1) 11 (4.8) 3.79 .004
Wound separation 3 (4.8) 23 (10.1) 0.45 .21
Superficialdermis
2 (3.2) 18 (7.9) 0.39 .21
Full fascialdehiscence
1 (1.6) 5 (2.2) 0.73 .78
Necrosis 1 (1.6) 7 (3.1) 0.52 .54
Seroma 2 (3.2) 8 (3.5) 0.92 .92
Hematoma 2 (3.2) 5 (2.2) 1.49 .64
Delayed woundhealing
1 (1.6) 7 (3.1) 0.52 .54
Table 6. Incidence of Wound Complications With 1-Layer Barbed vsTraditional Nonbarbed Sutures
WoundComplication
1-Layer BarbedSutures, n = 75
(%)
NonbarbedSutures, n = 713
(%)
OddsRatio
PValue
Overall 21 (28.00) 165 (23.14) 1.29 .35
Infection 6 (8.00) 63 (8.84) 0.90 .81
Erythema 5 (6.67) 33 (4.63) 1.47 .44
Woundseparation
6 (8.00) 29 (4.07) 2.05 .12
Superficialdermis
4 (5.33) 19 (2.66) 2.06 .20
Full fascialdehiscence
2 (2.67) 10 (1.40) 1.93 .40
Necrosis 2 (2.67) 11 (1.54) 0.72 .47
Seroma 3 (4.00) 42 (5.89) 0.67 .50
Hematoma 3 (4.00) 12 (1.68) 2.43 .18
Delayed woundhealing
1 (1.33) 21 (2.95) 0.45 .43
Cortez et al 183
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
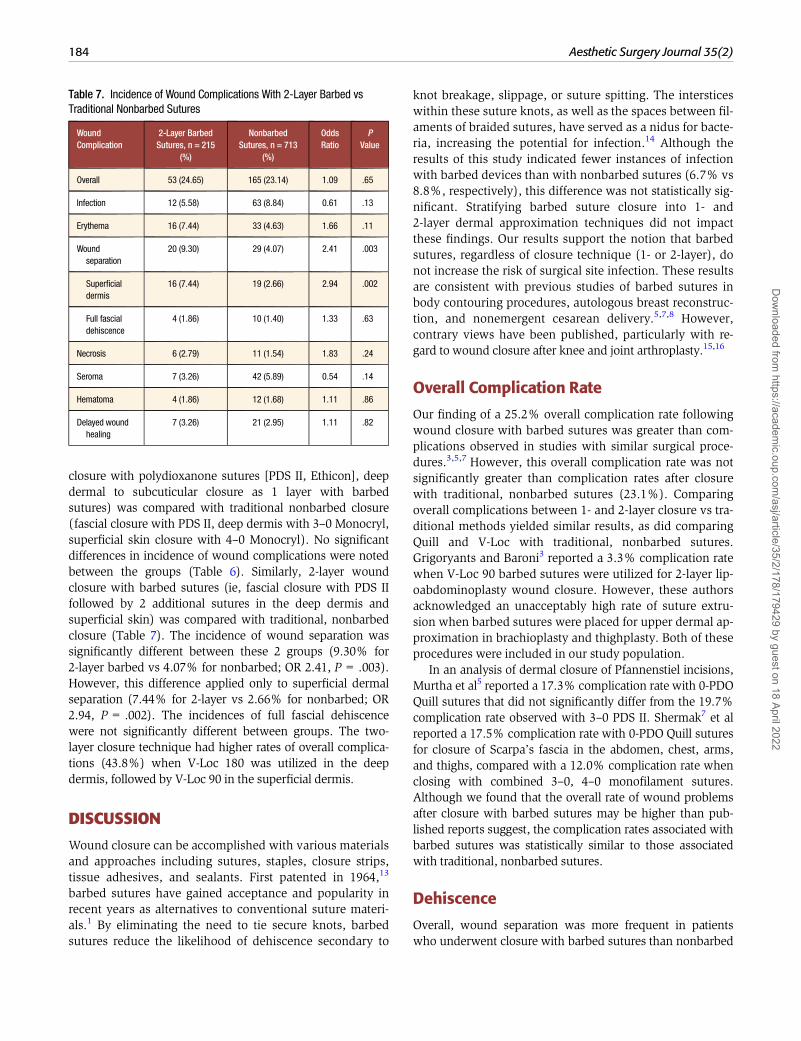
closure with polydioxanone sutures [PDS II, Ethicon], deepdermal to subcuticular closure as 1 layer with barbedsutures) was compared with traditional nonbarbed closure(fascial closure with PDS II, deep dermis with 3–0 Monocryl,superficial skin closure with 4–0 Monocryl). No significantdifferences in incidence of wound complications were notedbetween the groups (Table 6). Similarly, 2-layer woundclosure with barbed sutures (ie, fascial closure with PDS IIfollowed by 2 additional sutures in the deep dermis andsuperficial skin) was compared with traditional, nonbarbedclosure (Table 7). The incidence of wound separation wassignificantly different between these 2 groups (9.30% for2-layer barbed vs 4.07% for nonbarbed; OR 2.41, P=.003).However, this difference applied only to superficial dermalseparation (7.44% for 2-layer vs 2.66% for nonbarbed; OR2.94, P=.002). The incidences of full fascial dehiscencewere not significantly different between groups. The two-layer closure technique had higher rates of overall complica-tions (43.8%) when V-Loc 180 was utilized in the deepdermis, followed by V-Loc 90 in the superficial dermis.
DISCUSSION
Wound closure can be accomplished with various materialsand approaches including sutures, staples, closure strips,tissue adhesives, and sealants. First patented in 1964,13
barbed sutures have gained acceptance and popularity inrecent years as alternatives to conventional suture materi-als.1 By eliminating the need to tie secure knots, barbedsutures reduce the likelihood of dehiscence secondary to
knot breakage, slippage, or suture spitting. The intersticeswithin these suture knots, as well as the spaces between fil-aments of braided sutures, have served as a nidus for bacte-ria, increasing the potential for infection.14 Although theresults of this study indicated fewer instances of infectionwith barbed devices than with nonbarbed sutures (6.7% vs8.8%, respectively), this difference was not statistically sig-nificant. Stratifying barbed suture closure into 1- and2-layer dermal approximation techniques did not impactthese findings. Our results support the notion that barbedsutures, regardless of closure technique (1- or 2-layer), donot increase the risk of surgical site infection. These resultsare consistent with previous studies of barbed sutures inbody contouring procedures, autologous breast reconstruc-tion, and nonemergent cesarean delivery.5,7,8 However,contrary views have been published, particularly with re-gard to wound closure after knee and joint arthroplasty.15,16
Overall Complication Rate
Our finding of a 25.2% overall complication rate followingwound closure with barbed sutures was greater than com-plications observed in studies with similar surgical proce-dures.3,5,7 However, this overall complication rate was notsignificantly greater than complication rates after closurewith traditional, nonbarbed sutures (23.1%). Comparingoverall complications between 1- and 2-layer closure vs tra-ditional methods yielded similar results, as did comparingQuill and V-Loc with traditional, nonbarbed sutures.Grigoryants and Baroni3 reported a 3.3% complication ratewhen V-Loc 90 barbed sutures were utilized for 2-layer lip-oabdominoplasty wound closure. However, these authorsacknowledged an unacceptably high rate of suture extru-sion when barbed sutures were placed for upper dermal ap-proximation in brachioplasty and thighplasty. Both of theseprocedures were included in our study population.
In an analysis of dermal closure of Pfannenstiel incisions,Murtha et al5 reported a 17.3% complication rate with 0-PDOQuill sutures that did not significantly differ from the 19.7%complication rate observed with 3–0 PDS II. Shermak7 et alreported a 17.5% complication rate with 0-PDO Quill suturesfor closure of Scarpa’s fascia in the abdomen, chest, arms,and thighs, compared with a 12.0% complication rate whenclosing with combined 3–0, 4–0 monofilament sutures.Although we found that the overall rate of wound problemsafter closure with barbed sutures may be higher than pub-lished reports suggest, the complication rates associated withbarbed sutures was statistically similar to those associatedwith traditional, nonbarbed sutures.
Dehiscence
Overall, wound separation was more frequent in patientswho underwent closure with barbed sutures than nonbarbed
Table 7. Incidence of Wound Complications With 2-Layer Barbed vsTraditional Nonbarbed Sutures
WoundComplication
2-Layer BarbedSutures, n = 215
(%)
NonbarbedSutures, n = 713
(%)
OddsRatio
PValue
Overall 53 (24.65) 165 (23.14) 1.09 .65
Infection 12 (5.58) 63 (8.84) 0.61 .13
Erythema 16 (7.44) 33 (4.63) 1.66 .11
Woundseparation
20 (9.30) 29 (4.07) 2.41 .003
Superficialdermis
16 (7.44) 19 (2.66) 2.94 .002
Full fascialdehiscence
4 (1.86) 10 (1.40) 1.33 .63
Necrosis 6 (2.79) 11 (1.54) 1.83 .24
Seroma 7 (3.26) 42 (5.89) 0.54 .14
Hematoma 4 (1.86) 12 (1.68) 1.11 .86
Delayed woundhealing
7 (3.26) 21 (2.95) 1.11 .82
184 Aesthetic Surgery Journal 35(2)
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022

sutures, specifically for superficial skin separation.Theoretically, the benefits of barbed sutures for woundclosure include evenly distributed tension across suture lines,avoiding excessive amounts of pressure, and preventing ne-crosis caused by tissue strangulation and microinfarction.17,18
Our findings contradict previous studies reporting similarrates of wound dehiscence with barbed sutures comparedwith nonbarbed traditional sutures.8,19
Comparing V-Loc to Quill barbed sutures yielded differingrates of wound separation, though this differencewas not stat-istically significant. The Quill barbed suture (Figure 3) con-tains a 1-cut angle, with the 2–0 PDO device containing 12barbs per cm and 1 helix every 5.59 mm. The V-Loc barbedsuture (Figure 4) has a dual-cut angle, with the 3–0 devicecontaining 17 barbs per cm and 1 helix every 1.78 mm.Zaruby et al12 reported a significant difference in mode offailure when comparing V-Loc with Quill barbed sutures,with V-Loc sutures primarily failing due to suture breakageand Quill sutures failing due to barb slippage. Zaruby et al12
also compared biomechanical load to failure data, and foundthat Biosyn sutures demonstrated a significantly higher tensileload before failure compared with V-Loc at day 0 and Quill atday 3. Leung et al20 demonstrated that barb escarpment intotraditional PDO monofilament sutures reduced the suture’seffective diameter and straight-pull tensile strength by asmuch as 60%, rendering the strength equivalent to a monofil-ament suture 1 size smaller. In a comparison of dermal tissueclosure of Pfannenstiel incisions with conventional PDS IIsutures placed in the running intradermal pattern vs Quillsutures placed in the intradermal subcuticular pattern,Murtha et al5 found no incidence of full-wound dehiscenceduring 5 weeks of follow-up. These authors noted marginalseparation in only 1.6% of barbed cases, representing a non-significant difference.5 In autologous reconstructive breastprocedures, Jandali et al8 did not find significant differencesin dehiscence rates when comparing Biosyn and PDO QuillSRS to Biosyn alone. In a subset analysis of patients who un-derwent body contouring procedures, Shermak et al7 foundthat barbed sutures were associated with significantly higherwound complication rates in the arm than in the abdomen orthigh (OR, 8.4; P=.046). However, this was attributed topoor skin quality, mobility, and vulnerability to shearingforces in the area of surgical incision and has been furthersupported in the brachioplasty literature.21–23
We revealed a significantly greater risk of wound separa-tion after procedures with barbed sutures, particularly inthe superficial dermis. When groups who received barbedsutures were stratified into 1- and 2-layer dermal closuretechniques, superficial skin separation was significantly in-creased in the 2-layer dermal closure group. We believethat stratification of our barbed suture group into 1- and2-layer closure techniques and subsequent comparisonwith traditional closure methods helped to elucidate differ-ences in outcomes with various methods of wound closure.
Erythema
Although the incidence of erythema along incision lineswas elevated in the group who received barbed suturescompared with those who received nonbarbed sutures, thedifference was not statistically significant. However, whencomparing Quill and V-Loc sutures directly, we observed asignificantly increased incidence in the Quill group.Differences in inflammatory responses from each groupmay be attributed to differences in suture composition,namely barb geometry, helicity, and needle structure. In aporcine study, Zaruby et al12 noted statistical differences inhistologic analyses of barbed and nonbarbed sutures (QuillMonoderm, V-Loc 90, and Biosyn). Specifically, the V-Loc90 device consistently demonstrated the least amount of in-flammation at days 3 and 10. In addition, the V-Loc 90device was the least reactive of the 3 suture devices at day10, demonstrating a significant difference compared withQuill Monoderm (P= .017). Trauma secondary to needlegeometry and greater radial compression in the tissues mayhave contributed to these results, as the latter increases lo-calized inflammation surrounding the suture.
The rate of erythema along incision lines observed withthe Quill population was >3 times that of the V-Loc popu-lation in our study. One explanation may be a propensityfor entrapment of foreign materials within the barbs of thesutures (Figure 5) when compared with traditional monofil-aments. Adoption of Quill sutures (and barbed sutures ingeneral) for wound closure began before a mainstreamawareness of this potential complication. As the implemen-tation of barbed sutures in wound closure has expandeddramatically to include body contouring, breast, gynecolog-ic, and tendon repair procedures, avoidance of immunereactions to foreign bodies has become increasinglyimportant. Results support decreased bacterial adherenceto barbed sutures, which is further reinforced with the
Figure 5. Foreign materials trapped by the suture barbs, asshown, may induce an undesired immune response in thepatient.
Cortez et al 185
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
recent release of antibiotic-coated barbed sutures.24 However,foreign-body reactions are a problem intrinsic to the barbedsutures, as their tendency to grasp soft tissue extends tosterile equipment intraoperatively. Implementation of severalsurgical techniques may help minimize these events, includ-ing avoiding direct suture contact with laparotomy pads orsterile drapes, placing barrier dressings (ie, polyethylene 1010surgical drapes) over the sterile field, and placing sutures inthe mid-dermis rather than the superficial dermis.
Operating Time
Although assessing time savings was not an objective ofthis study, the literature supports this as a major advantageof barbed sutures in wound approximation. Differences inoperating times may be more evident depending on thetype of surgery and closure methods. In progressive tensionclosure during abdominoplasty, a 1-PDO Quill barbedsuture allowed Warner and Gutowski25 to reduce closuretime for abdominal flap plication to nine minutes from 15to 20 minutes placing interrupted sutures. Grigoryants andBaroni3 demonstrated statistically significant time savingsin closure times for 2-layer closure of Scarpa’s fascia andthe upper dermis with V-Loc 90 sutures compared withstandard 3-layer closure with Vicryl and Monocryl. Theseauthors noted no obvious difference in scar appearancewhen both techniques were performed on the same patientby the same surgeon.3 Jandali et al8 noted similar findingsin a study of patients undergoing autologous unilateralbreast reconstruction.
Recent Literature
Various authors have proposed techniques for the applica-tion of barbed sutures to wound closures of the face, arms,thighs, abdomen, and breasts;26–29 however, few authorshave directly compared their optimal techniques for barbedsutures with conventional sutures. In September 2013,Aesthetic Surgery Journal published a supplement onbarbed sutures that was funded by the manufacturer ofQuill sutures, regarding the advent and release of this newtechnology.30,31 Most of the authors in the supplement re-ported a positive attitude toward outcomes with barbedsutures and the future potential of these devices, but theseaccounts were based on anecdotal, albeit extensive, experi-ence.30,31 The supplement was a valuable contribution tothe literature regarding barbed sutures, but it highlightedthe need for independent, systematic, outcomes-basedstudies to support adopting barbed sutures in evidence-based practice. Matarasso30 alludes to the lack of level 1 to3 evidence in this field, and Rosen28 notes that the publica-tion of data supporting barbed sutures currently lagsbehind the pace of technological development. Barbedsutures represent an innovative advance that reportedly
reduces operative time, eliminates or reduces the need fordrains, and improves cosmesis;28 however, evidence-basedguidance regarding the role of barbed sutures in woundclosure is limited. Our enthusiasm for these new tech-niques should be tempered with caution.
The aforementioned supplement included a retrospec-tive series of 360 patients in which Hurwitz and Reuben31
compared barbed sutures with running absorbable braidedsutures in body contouring and found reduced complica-tions in the arm and trunk, but not the thigh, among pa-tients who received barbed sutures. The authors cited ahigh complication rate (71.2%) for suture-line woundhealing with traditional sutures,31 whereas the results ofour study show an overall complication rate of only 23.1%.The findings of Hurwitz and Reuben31 contrast with earlierfindings by Shermak et al,7 who showed that barbed suturesincrease wound complications and do not decrease operativetimes compared with traditional running sutures, particularlyin brachioplasty. Hurwitz and Reuben’s31 retabulation ofdata reported by Shermak et al7 shows a positive associationbetween barbed sutures and complications. In addition,Hurwitz and Reuben31 explain why operative times were notreduced in the study by Shermak et al,7 but their explanationis based solely on speculation about the methods of Shermaket al.7 Our results corroborate those of Shermak et al.7
Limitations
The direct comparison of barbed with nonbarbed sutureswithout standardization of specific material types (eg, PDO,polyglactin) is a limitation of this study. The retrospectivenature of our study also limits postoperative analyses to phy-sician records. We attempted to expand upon the appropri-ateness of barbed sutures for deep layers vs superficial layersby further separating the study cohort into subpopulations.However, the resulting cohorts were very small, limiting theeffective statistical power of these groups. Subsequent largeprospective studies could avoid these limitations.
A failure in deep-layer closure could have contributedwound complications in the present study. We plan toaddress this concern in future studies. Attempts to compareobserved complications after superficial dermal closurewith PDO vs Quill Monoderm (2–0 and 3–0) suturesyielded sample sizes that were too small to draw significantconclusions; thus, we could not determine whether PDOsutures were associated with increased incidences of ery-thema and extrusion.
Suboptimal standardization of patient charts is a poten-tial limitation in this study, particularly with regard tominor complications (eg, erythema). The surgeries wereperformed at a teaching institution with residents andfellows assisting in wound closure under supervision bythe attending faculty. Several surgeons with differentfollow-up protocols performed procedures on the patients
186 Aesthetic Surgery Journal 35(2)
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022
in our study group. This could have influenced the occur-rence and the reporting of postoperative complications.
CONCLUSIONS
Our results showed significantly increased rates of minorwound complications in patients who received barbedsutures compared with nonbarbed sutures. Mild dehis-cence, specifically superficial skin separation, was signifi-cantly higher in the group who received barbed sutures. Inour subgroup analysis of 1- vs 2-layer dermal closure withbarbed sutures, only the 2-layer technique was associatedwith significantly higher rates of superficial skin separation.With only minor differences detected between Quill andV-Loc sutures, it appears that surgeon preference, perceivedease, and convenience may be the deciding factors whenchoosing a barbed suture for soft-tissue approximation.
AcknowledgmentsThe authors thank Debby Noble for her outstanding support inassisting with the organization, completion, and maintenanceof the plastic surgery patient database. In addition, specialthanks are due to Georgette Oni, Jessica Bills, Min-Jeong Cho,James Jewell, Daniel Zhang, Bhavani Gannavarapu, NatalieSciano, Matthew Kenkel, Ashley Kenkel, and Allan Wang fortheir assistance throughout this investigation.
DisclosuresDr Davis receives grants from ConvaTec (Skillman, NJ),Innovative Therapies (Pompano Beach, FL), Unilever(Englewood Cliffs, NJ), Andrew Technologies (Tustin, CA),and Kensey Nash (Exton, PA). Dr Kenkel is an unpaid investi-gator for Allergan (Irvine, CA) and Ultrashape (Synernon;Irvine, CA), and serves as a paid member of the AdvisoryBoards of Kythera (Calabasas, CA) and Ulthera (Mesa, AZ).The other authors have nothing to disclose.
FundingThe authors received no financial support for the research,authorship, and publication of this article.
REFERENCES1. Matarasso A, Pfeifer TM. The use of modified sutures in
plastic surgery. Plast Reconstr Surg. 2008;122(2):652-658.2. Sulamanidze M, Sulamanidze G, Vozdvizhensky I,
Sulamanidze C. Avoiding complications with Aptossutures. Aesthet Surg J. 2011;31(8):863-873.
3. Grigoryants V, Baroni A. Effectiveness of wound closurewith V-Loc 90 sutures in lipoabdominoplasty patients.Aesthet Surg J. 2013;33(1):97-101.
4. Einarsson JI, Chavan NR, Suzuki Y, Jonsdottir G,Vellinga TT, Greenberg JA. Use of bidirectional barbedsuture in laparoscopic myomectomy: evaluation ofperioperative outcomes, safety, and efficacy. J MinimInvasive Gynecol. 2011;18(1):92-95.
5. Murtha AP, Kaplan AL, Paglia MJ, Mills BB, Feldstein ML,Ruff GL. Evaluation of a novel technique for wound closureusing a barbed suture. Plast Reconstr Surg. 2006;117(6):1769-1780.
6. Oni G, Brown SA, Kenkel JM. A comparison betweenbarbed and nonbarbed absorbable suture for fascialclosure in a porcine model. Plast Reconstr Surg. 2012;130(4):535e-540e.
7. Shermak MA, Mallalieu J, Chang D. Barbed sutureimpact on wound closure in body contouring surgery.Plast Reconstr Surg. 2010;126(5):1735-1741.
8. Jandali S, Nelson JA, Bergey MR, Sonnad SS, Serletti JM.Evaluating the use of a barbed suture for skin closureduring autologous breast reconstruction. J ReconstrMicrosurg. 2011;27(5):277-286.
9. Ruff G. Technique and uses for absorbable barbedsutures. Aesthet Surg J. 2006;26(5):620-628.
10. Ingle NP, King MW. Optimizing the tissue anchoring per-formance of barbed sutures in skin and tendon tissues.J Biomech. 2010;43(2):302-309.
11. Gingras K, Zaruby J, Maul D. Comparison of V-Loc 180wound closure device and Quill PDO knotless tissue-closuredevice for intradermal closure in a porcine in vivo model:evaluation of biomechanical wound strength. J BiomedMater Res B Appl Biomater. 2012;100(4):1053-1058.
12. Zaruby J, Gingras K, Taylor J, Maul D. An in vivo com-parison of barbed suture devices and conventional mono-filament sutures for cosmetic skin closure: biomechanicalwound strength and histology. Aesthet Surg J. 2011;31(2):232-240.
13. Alcamo JH. Surgical Suture. U.S. Patent 3,123,077, 1964.14. Katz S, Izhar M, Mirelman D. Bacterial adherence to sur-
gical sutures. A possible factor in suture induced infec-tion. Ann Surg. 1981;194(1):35-41.
15. Campbell AL, Patrick DA Jr, Liabaud B, Geller JA.Superficial wound closure complications with barbedsutures following knee arthroplasty. J Arthroplasty.2014;29(5):966-969.
16. Patel RM, Cayo M, Patel A, Albarillo M, Puri L. Woundcomplications in joint arthroplasty: comparing traditionaland modern methods of skin closure. Orthopedics. 2012;35(5):e641-646.
17. Myers MB, Cherry G. Functional and angiographic vascu-lature in healing wounds. Am Surg. 1970;36(12):750-756.
18. Bartlett LC. Pressure necrosis is the primary cause ofwound dehiscence. Can J Surg. 1985;28(1):27-30.
19. Hansen J. A Prospective, Randomized Study to EvaluateDermal Closure with an Absorbable Barbed Suture(V-Loc 90 Device or V-Loc 180 Device) as Compared to aConventional Absorbable Suture. 2011.
20. Leung JC, Ruff GL, Megaro MA. Barbed, bi-directionalmedical sutures: Biomechanical properties and woundclosure efficacy study. In Society for Biomaterials 28thAnnual Meeting Transactions, Tampa, Fla., April 24-27,2002.
21. Knoetgen J 3rd, Moran SL. Long-term outcomes andcomplications associated with brachioplasty: a retrospec-tive review and cadaveric study. Plast Reconstr Surg.2006;117(7):2219-2223.
Cortez et al 187
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022

22. Aly A, Soliman S, Cram A. Brachioplasty in the massiveweight loss patient. Clin Plast Surg. 2008;35(1):141-147.
23. Hurwitz DJ, Neavin T. L brachioplasty correction ofexcess tissue of the upper arm, axilla, and lateral chest.Clin Plast Surg. 2008;35(1):131-140.
24. Fowler JR, Perkins TA, Buttaro BA, Truant AL.Bacteria Adhere Less to Barbed Monofilament ThanBraided Sutures in a Contaminated Wound Model.Clin Orthop. 2013;471(2):665-671.
25. Warner JP, Gutowski KA. Abdominoplasty with progres-sive tension closure using a barbed suture technique.Aesthet Surg J. 2009;29(3):221-225.
26. Gutowski KA, Warner JP. Incorporating barbed suturesin abdominoplasty. Aesthet Surg J. 2013;33(3 Suppl):76S-81S.
27. Hammond DC. Barbed sutures in plastic surgery: a per-sonal experience. Aesthet Surg J. 2013;33(3 Suppl):32S-39S.
28. Rosen AD. New and emerging uses of barbed suturetechnology in plastic surgery. Aesthet Surg J. 2013;33(3Suppl):90S-95S.
29. Salzberg CA. Barbed sutures in breast reconstruction.Aesthet Surg J. 2013;33(3 Suppl):40S-43S.
30. Matarasso A. Introduction to the barbed sutures supple-ment: the expanding applications of barbed sutures.Aesthet Surg J. 2013;33(3 Suppl):7S-11S.
31. Hurwitz DJ, Reuben B. Quill barbed sutures in bodycontouring surgery: a 6-year comparison with runningabsorbable braided sutures. Aesthet Surg J. 2013;33(3 Suppl):44S-56S.
188 Aesthetic Surgery Journal 35(2)
Dow
nloaded from https://academ
ic.oup.com/asj/article/35/2/178/179429 by guest on 18 April 2022