bacterial diversity in aortic aneurysms determined by 16s ribosomal rna gene analysis
TRANSCRIPT

BASIC RESEARCH STUDIES
Bacterial diversity in aortic aneurysms determinedby 16S ribosomal RNA gene analysisRafael Marques da Silva, DDS,a Dominique A. Caugant, PhD,a,b Emenike R. K. Eribe, PhD,a
Jørn A. Aas, DDS, PhD,a Per S. Lingaas, MD,c Odd Geiran, MD, PhD,c Leif Tronstad, DMD, PhD,a
and Ingar Olsen, DDS, PhD,a Oslo, Norway
Background: Aortic aneurysms are common vascular conditions that cause considerable morbidity and mortality.Understanding of the mechanisms involved in the pathogenesis of the condition remains limited. Recently, infection hasbeen suggested as possible contributor in the development of the disease. The aim of the present study was to examineaortic aneurysms for the presence of bacterial DNA using polymerase chain reaction (PCR) targeting the 16S ribosomalRNA (rRNA) gene, followed by cloning and sequencing.Methods: Universal eubacterial primers were used to amplify 16S rRNA bacterial genes in 10 specimens from arterial wallsof aortic aneurysms. Subsequently, PCR amplicons were cloned into Escherichia coli and sequencing of the cloned insertswas used to determine species identity or closest relatives by comparison with known sequences in GenBank.Results: Sequences of Stenotrophomonas spp., including S. maltophilia (formerly Pseudomonas homology group V) weredetected in six aneurysm samples. Propionibacterium acnes was identified in five samples, and Brevundimonas diminuta(formerly P. diminuta) in four samples. Other species previously assigned to the Pseudomonas genus such as Comamonastestosteroni, Delftia acidovorans, Burkholderia cepacia, Herbaspirillum sp., and Acidovorax sp. were also detected. Someclones fell into other environmental species, including Methylobacterium sp. and Bradyrhizobium elkanii, and othersrepresented bacteria that have not yet been cultivated. DNA sequences from oral bacteria, including Streptococcussanguinis, Tannerella forsythia, and Leptotrichia buccalis were detected. Sequences from Prevotella melaninogenica andLactobacillus delbrueckii, which are commonly found in both mouth and gastrointestinal tract, were also detected.Additional species included Dermacoccus spp. and Corynebacterium vitaeruminis.Conclusions: A wide variety of bacteria, including oral bacteria, was found to colonize aortic aneurysms and may play a rolein their development. Several of these microorganisms have not yet been cultivated. (J Vasc Surg 2006;44:1055-60.)
Clinical Relevance: Although Chlamydophila pneumoniae has been detected in aneurysmal walls, its exact role in thecondition remains inconclusive. Overall, there is scarce information about the role of microorganisms in aneurysmaldisease. In the present study, we used molecular genetics to detect a diversity of bacteria in arterial walls of aorticaneurysms. The presence of multiple microorganisms in aneurysmal disease may have implications for chemoprophylaxis
and antibiotic treatment if directed only at C. pneumoniae.Aortic aneurysms are life-threatening conditions asso-ciated with significant morbidity and mortality. The hall-marks in the pathogenesis of aortic aneurysms are destruc-tion of elastin and collagen combined with medial andadventitial inflammation, and their etiology is complex and
From the Institute of Oral Biology, Faculty of Dentistry, University ofOslo,a Division of Infectious Disease Control, Norwegian Institute ofPublic Health,b and Department of Thoracic and Cardiovascular Sur-gery, Faculty Division Rikshospitalet.c
Supported in part by research grants from the foundations of Professor Halland Stokbak, National Hospital, Oslo, and by the Faculty of Dentistry,University of Oslo, Oslo, Norway.
Competition of interest: none.Reprint requests: Rafael Marques da Silva, DDS, Institute of Oral Biology,
Faculty of Dentistry, University of Oslo, PO Box 1052 Blindern, N-0316Oslo, Norway (e-mail: [email protected]).
0741-5214/$32.00Copyright © 2006 by The Society for Vascular Surgery.
doi:10.1016/j.jvs.2006.07.021multifactorial. The mechanisms behind the pathogenesis ofthe disease are yet not fully understood.1
Recently, infection has been proposed as a contributingfactor in the development of the disease. So far, mostexperimental and clinical studies examining aortic aneu-rysms have focused on a possible etiologic role of chronicinfection with Chlamydophila (formerly Chlamydia) pneu-moniae.2 Little is known about the role of other microor-ganisms in the development and progression of aneurysms.If infection does play a causal role, it would seem highlylikely that various and multiple pathogens are causallyinvolved and that hematogenous spreading may be likely.
Although culture-based methods may be useful toidentify possible pathogens, they usually do not enableprediction of the associated clinical burden, because lessnumerous or difficult-to-cultivate species may not be de-tected. Advances in molecular biology in the last decade
have permitted the study of microbial communities based1055

JOURNAL OF VASCULAR SURGERYNovember 20061056 Marques da Silva et al
on typing of nucleic acids. In particular, polymerase chainreaction (PCR) amplification of the bacterial 16S ribosomalRNA (rRNA) gene, followed by cloning and sequencing ofthe inserts, have resulted in improved information of bac-terial diversity from clinical and environmental samples.3
The 16S rRNA molecule is a basic constituent of thebacterial ribosome, which is a highly conserved structurewith an important function in protein synthesis. The rRNAmolecules contain several functionally different regions,some of which have highly conserved sequences, and othershave regions of highly variable sequence.4 By designingPCR primers complementary to conserved regions of therRNA gene, the approach may be useful in identifyingfastidious, uncultivable, and novel microorganisms.5,6 Af-ter cloning and sequencing of the PCR products, the 16SrRNA sequences are compared with other known 16SrRNA sequences to establish phylogenetic affinities andplace the organism of interest within a phylogenetic tree.4
The purpose of the present study was to examine thepresence of bacterial DNA in aortic aneurysms by usingPCR technique targeting the 16S rRNA gene, followed bycloning and sequencing.
METHODS
Patients and specimens. Specimens from arterial wallsof 56 consecutive aortic aneurysm samples were examinedfor bacterial DNA and DNA of putative periodontal patho-gens using the PCR technique as described in a previousstudy.7 A set of universal primers was used to examine thepresence of bacterial DNA, and 50 (89.2%) of the 56samples were positive. In the present study, 10 aneurysmspecimens from nine patients were randomly selected fromthe 50 PCR-positive specimens to investigate bacterial spe-cies present in aortic aneurysms by means of cloning and16S rDNA sequencing analysis. The characteristics of thepatients are summarized in the Table. Informed consentwas obtained from the patients, and the study was approvedby the Regional Committee on Medical Ethics.
DNA preparation from the tissue samples. The tis-sue samples (approximately 25 mg) were homogenized in asterile mortar with liquid nitrogen in a laminar flow hood,under strict aseptic conditions. Before homogenization,the aortic specimens were washed with sterile TE buffer toensure no contamination with blood-borne bacteria.DNA was extracted as previously described 7 using acommercial kit (QIAamp Mini Kit, Qiagen GmbH,Hilden, Germany) according to the manufacturer’s instruc-tions. Control extraction samples containing sterile dis-tilled water (Ultrapure quality, PCR-grade, Qiagen) in-stead of tissue samples were run in parallel in order to checkthe sterility of the solutions and buffers used in the DNAextraction method.
PCR amplification of 16S rDNA and purification ofPCR products. Amplification of 16S rDNA occurred un-der standardized conditions using previously publisheduniversal eubacterial primers.8 The primers used were PA5=-AGA GTT TGA TCC TGG CTC AG-3= and PD 5=-
GTA TTA CCG CGG CTG CTG-3=. PCR was performedin thin-walled tubes using the GeneAmp PCR System 2700(Applied Biosystems, Foster City, Calif), with a master mixsolution (HotStarTaq Master Mix, Qiagen GmbH) con-taining 2.5 units of Taq DNA polymerase, 1� PCR bufferwith 1.5 mM MgCl2, 200 �M of each deoxynucleosidetriphosphates, 0.2 �M of primer PA, 0.2 �M of primer PD,and 10 �L of the template DNA, in a total volume of50 �L.
In a hot start protocol, samples were denatured at 95°Cfor 15 minutes, followed by amplification consisting of adenaturation step at 95°C for 40 seconds, annealing at58°C for 1 minute, and elongation at 72°C for 1 minute. Atotal of 32 cycles was performed, followed by a final elon-gation step at 72°C for 10 minutes.
Each set of experiments included negative controlswith sterile distilled water instead of template DNA andpositive controls containing purified DNA from Escherichiacoli. The results of PCR amplification were examined byelectrophoresis in a 1% agarose gel. DNA was visualized andphotographed under ultraviolet light after ethidium bro-mide staining (Fig 1). Before cloning, amplicons werepurified using the QIAquick Gel Extraction Kit (Qiagen)according to the manufacturer’s instructions.
Cloning and 16S rDNA sequencing. The ampliconswere ligated into the pCR4-TOPO vector (Invitrogen,Carlsbad, Calif) and transformed into competent E. coliTOP10 cells (Invitrogen) according to instructions of themanufacturer. The transformed cells were then plated ontoLuria-Bertani agar plates supplemented with kanamycin(50 �g/mL), and incubated overnight at 37°C. Ninety-sixcolonies containing the insert were then placed into 40 �Lof 10 mM Tris. Correct sizes of the inserts were determinedby PCR with an M13 (-20) forward primer and an M13reverse primer (Invitrogen), followed by electrophoresis ona 1% agarose gel.
PCR products were purified by adding 1 �L of shrimpalkaline phosphatase and 1 �L of exonuclease I to 7 �L ofthe PCR product according to the manufacturer’s instruc-tions (Amersham Pharmacia Biotech, Oslo, Norway).
Purified DNA was sequenced on both strands using theABI Prism BigDye Terminator Cycle Sequencing ReadyReaction kit with AmpliTaq DNA polymerase FS (AppliedBiosystems). The primers PB and PC (PB 5=-TAA CACATG CAA GTC GAA CG-3= and PC 5’- CCC ACT GCTGCC TCC CGT AG-3=) were used for sequencing.8 Se-quencing reactions were run on an ABI Prism 3100 DNAsequencer (Applied Biosystems).
Data analyses of 16S rDNA sequences. DNA se-quences were assembled with the SEQUENCHER 4.0.5program (Gene Codes Corp, Ann Arbor, Mich) and ana-lyzed for the presence of chimeric sequences using theChimera Check program from the Ribosomal DatabaseProject II.9 After elimination of suspected chimeric se-quences, the partial 16S rDNA sequences of approximately500 bp were used to determine identity or nearest phylo-genetic position. For identification of closest relatives, theconsensus sequences were compared with 16S rDNA se-
quences in GenBank databases using the NCBI BLAST
cedureary art
JOURNAL OF VASCULAR SURGERYVolume 44, Number 5 Marques da Silva et al 1057
search tool (http://www.ncbi.nlm.nih.gov/BLAST/).The sequences were aligned by the ClustalV (Higgins andSharp, 1988 and 1989) method, with aligned fragmentscorresponding to E. coli nucleotide positions 50-361.8
Phylogenetic trees were constructed using the MegAlignprogram (DNASTAR, Inc, Madison, Wisc).
RESULTS
Sequencing was used to analyze 83 clones. All 16S
Table. Characteristic features of patients’ aneurysm samplreaction, cloning and 16S rDNA sequencing and their Gen
Subject Age/Sex Location in aorta Etiology/associated con
Ac 39/M Ascendingc Congenital/Marfan’ssyndrome
Bd 32/M Ascending, arch Mechanical/CoA
C 43/M Ascending MechanicalD 73/M Ascending Mechanical
E 22/F Descending Inflammatory
F 67/F Ascending Degenerative/atherosc
Ge 70/F Descendinge Degenerative/atherosc
H 75/F Abdominal Degenerative/atherosc
I 77/F Abdominal Degenerative/atherosc
Jd 32/M Descending Postoperative/previou
CoA, Aortic coarctation.aThe number of clones is given in parenthesis (for each sample if �1).bAccession number of the nearest 16S rDNA sequences is given for each straifor values �98%.cPatient previously operated in the same location.dB and J refer to the same subject operated in two locations in separate proePatient previously operated in a different location with concomitant coron
rDNA sequences, except for two (uncultured clostridia
bacterium and uncultured Weissella sp), showed �98%similarity to sequences deposited to GenBank (Table). Thedetected 16S rDNA sequences were represented by twomajor clusters at 10% nucleotide difference (Fig 2). All butone specimen harbored several bacterial species. The 10analyzed clones from patient C were all identical, showing92% identity to an uncultured Weissella sp. (Lactobacillus-like organism). The sample from patient I was the mostheterogeneous, with 10 different bacterial species identified
d bacteria detected analyzed by polymerase chaink accession numbers
BacteriaaGenBank accession
numbersb
Comamonas testosteroniHerbaspirillum sp.Uncultured clostridia bacteriumLeptotrichia buccalis (2)Tannerella forsythia (2)
AY653219AY953141AY607222 [96%]L37788AB053940
B-proteobacterium B6�-proteobacterium MBIC3025Propionibacterium acnes (7)
AF035052AB016980AY458863
Uncultured Weissella sp. (10) AY421855 [92%]Methylobacterium sp (5)Brevundimonas diminuta (2)
AY468371AY730717
Stenotrophomonas sp. JRL-2Methylobacterium sp. (3)Brevundimonas diminuta (2)Bradyrhizobium elkanii (2)Lactobacillus delbrueckii ss bulgaricusPropionibacterium acnes
AF181569AY468371AY730717AY568513AY568513AY458863
is Stenotrophomonas sp. dune 276S. maltophilia SM14UDermacoccus sp. Ellin183 (3)Propionibacterium acnes (5)
AJ884482AF533952AF409025AY458863
is Stenotrophomonas sp. dune 276Methylobacterium sp.Uncultured Bradyrhizobium
AJ884482AY468371AY437440
is Stenotrophomonas maltophilia SM14UPropionibacterium acnes (4)Streptococcus sanguinis (2)Dermacoccus sp. Ellin183 (2)
AF533952AY458863AF543281AF409025
is Delftia acidovorans (2)Acidovorax sp.Burkholderia cepacia (2)Stenotrophomonas sp. JRL-2S. maltophilia E2Brevundimonas diminutaDermacoccus sp. L560Corynebacterium vitarumenPropionibacterium acnesPrevotella melaninogenica (2)Uncultured Bacteroidetes bacterium
AY178541AJ012071AY268149AF181569AY841799AY730717AY367751X84680AY458863L16469DQ06661
Stenotrophomonas sp. JRL-2Uncultured bacterium 227ds5S maltophilia SM14UDermacoccus sp. Ellin183
AF181569AY212674AF533952AF409025
centage of 16S rDNA sequence similarity is indicated in brackets, given only
s.ery bypass surgery.
es anBan
dition
leros
leros
leros
leros
s CoA
n. Per
among the 16 clones sequenced. DNA of Stenotrophomonas

JOURNAL OF VASCULAR SURGERYNovember 20061058 Marques da Silva et al
spp, including S. maltophilia (formerly Pseudomonas ho-mology group V) was detected in six aneurysm samples.Propionibacterium acnes DNA was identified in five speci-mens, and Brevundimonas diminuta (formerly classified asa member of the group IV of the genus Pseudomonas) wasfound in four specimens. Other species previously assignedto the Pseudomonas genus, such as Comamonas testosteroni,Delftia acidovorans, Burkholderia cepacia, Herbaspirillumsp. and Acidovorax sp. were also detected. Some clones fellinto other environmental species, such as Methylobacte-rium sp. and Bradyrhizobium elkanii, and others repre-sented not-yet-cultivable bacteria (cluster I). Additionalspecies found in this cluster included Dermacoccus spp. andCorynebacterium vitaeruminis.
DNA from a putative periodontal pathogen, Tan-nerella forsythia, was detected in one sample (A). DNAcorresponding to other oral bacteria, including Streptococ-cus sanguinis and Leptotrichia buccalis were detected. DNAof Prevotella melaninogenica and Lactobacillus delbrueckiisubsp. bulgaricus, which are commonly found in bothmouth and gastrointestinal tract, was also detected in onepatient each (cluster II).
DISCUSSION
The main finding in this study was the presence ofbacterial DNA from a diversity of species in aortic aneu-rysms of different clinical etiologies. Moreover, most spec-imens contained multiple species, pointing to a less specificrelationship between single species and the development ofinflammation in the aortic wall as well as subsequent pro-gression to aneurysmal disease. This agrees with our previ-ous demonstration of multiple bacteria on the walls ofaortic aneurysms by means of electron microscopy andanaerobic cultivation.10 Coaggregating and dividing bacte-rial cells inside tissue with different morphologies wereobserved, often organized in biofilm structures. Some ofthe bacteria identified in our study cannot yet be cultured.Because a great part of human microflora still is estimatedto resist cultivation,11,12 it is conceivable that aortic aneu-rysms also harbor uncultivable species, as demonstratedhere. Taken together, these findings suggested that aorticaneurysms contain a much more diverse bacterial burden
Fig 1. Polymerase chain reaction products from aortic aneurysmsamples using eubacterial primers to amplify approximately 500 bpof the 16S rRNA gene. Lane M, Molecular weight marker (1KbDNA Ladder, Invitrogen). Lanes 1 to 10, DNA extracted frompatients’ aneurysm samples. Lanes N, negative controls (sterilewater). Lane P, positive control (purified DNA from E. coli).
than previously estimated.
To our knowledge, our findings in aortic aneurysmsare original. Therefore, questions about sampling andmethodology must be raised. It should be emphasizedthat strict aseptic conditions were imposed to avoidcontamination both during surgery and in the labora-tory. However, biologic material from control sampleswas not included in our study. Instead, control extrac-tion samples with sterile water were used to test thesterility of solutions and buffers used during DNA prep-aration, which gave negative results.7 In addition, noamplification of bacterial DNA was seen in the PCRexperiments using sterile water instead of templateDNA, which also argued against contamination of thePCR reagents (Fig 1). It is also unlikely that DNAsequences detected from oral bacteria, including obli-gate anaerobes, such as T. forsythia, P. melaninogenicaand L. buccalis, could have been introduced duringsample preparation.
Most of the bacteria detected in the present study,including the many environmental species, have been re-ported as either opportunists or true pathogens in differenthuman diseases. B. cepacia, for instance, is known as atypical pathogen in patients with cystic fibrosis.13 Otherorganisms detected, including C testosteroni and Herbaspi-rillum sp., have also been identified from cystic fibrosis spu-tum by fatty acids analysis and 16S rDNA sequencing.14 Bdiminuta, which was formerly classified as a member ofPseudomonas group IV (P. diminuta) has been isolated fromclinical samples, particularly from blood in cancer pa-tients.15,16 Another example is S. maltophilia, which hasrecently emerged as an important multidrug-resistantnosocomial pathogen associated with significant mortal-ity, especially in immunocompromised patients. S. mal-tophilia is now the second most frequently isolated nos-ocomial bacterium after Pseudomonas aeruginosa.17
The spectrum of the infections includes pneumonia,urinary and wound infections, infections in cystic fibrosispatients, bacteremia, and endocarditis.13,18,19 Infective en-docarditis of a prosthetic aortic valve associated with adissecting aneurysm of the ascending aorta due to S. mal-tophilia has been reported.20 Of interest is a recent stud y b yOtt et al21 who, using the same methodology, havereported a very similar bacterial composition and a broadvariety of bacteria in atherosclerotic tissue obtainedthrough atherectomy of patients with coronary heartdisease, clearly supporting our findings. Therefore, thepresence of these organisms in aortic aneurysms shouldnot be considered as contamination.
P. acnes, which was detected in 50% of the specimens,can clearly act as a primary pathogen. The organism haspreviously been isolated from soft tissue abscesses, endo-carditis, prosthetic hip infections, patients with sarcoidosis,and also from mycotic aortic aneurysms.22-28 Endocarditiscaused by P. acnes may follow a very aggressive course,especially in the setting of a prosthetic valve.28
Another interesting finding was the sole detection ofsequences related to an uncultured Weissella sp. in subject
C (Table). The genus Weissella is proposed to accommo-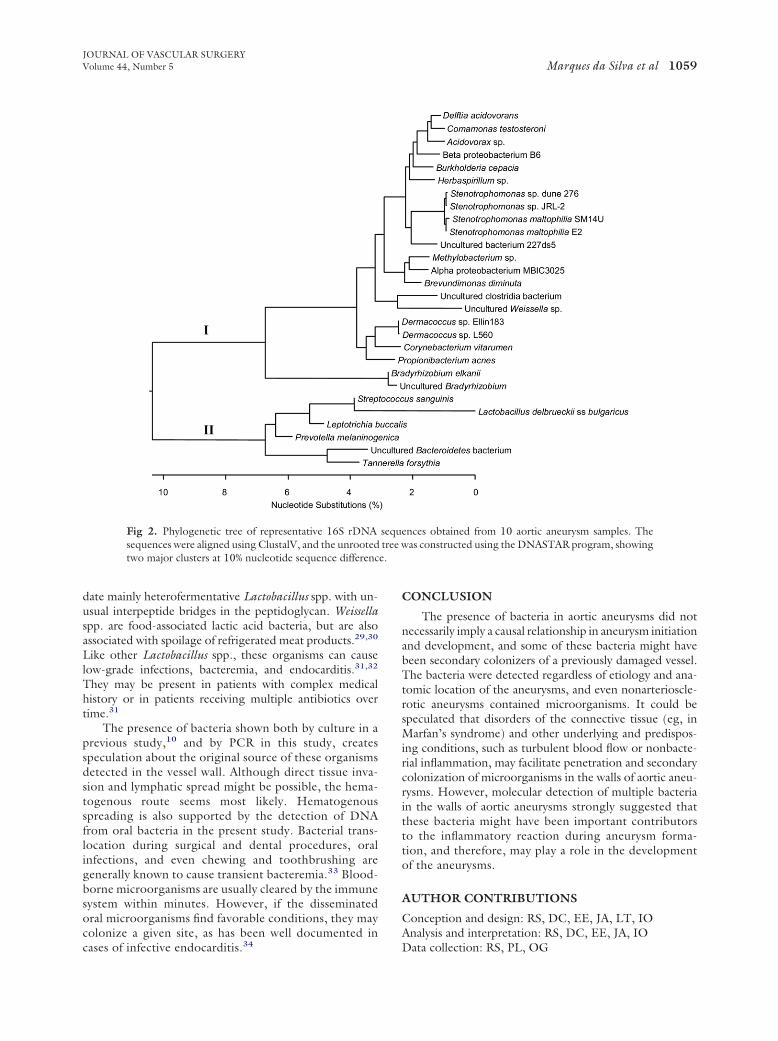
e.
JOURNAL OF VASCULAR SURGERYVolume 44, Number 5 Marques da Silva et al 1059
date mainly heterofermentative Lactobacillus spp. with un-usual interpeptide bridges in the peptidoglycan. Weissellaspp. are food-associated lactic acid bacteria, but are alsoassociated with spoilage of refrigerated meat products.29,30
Like other Lactobacillus spp., these organisms can causelow-grade infections, bacteremia, and endocarditis.31,32
They may be present in patients with complex medicalhistory or in patients receiving multiple antibiotics overtime.31
The presence of bacteria shown both by culture in aprevious study,10 and by PCR in this study, createsspeculation about the original source of these organismsdetected in the vessel wall. Although direct tissue inva-sion and lymphatic spread might be possible, the hema-togenous route seems most likely. Hematogenousspreading is also supported by the detection of DNAfrom oral bacteria in the present study. Bacterial trans-location during surgical and dental procedures, oralinfections, and even chewing and toothbrushing aregenerally known to cause transient bacteremia.33 Blood-borne microorganisms are usually cleared by the immunesystem within minutes. However, if the disseminatedoral microorganisms find favorable conditions, they maycolonize a given site, as has been well documented in
Fig 2. Phylogenetic tree of representative 16S rDNAsequences were aligned using ClustalV, and the unrootedtwo major clusters at 10% nucleotide sequence differenc
cases of infective endocarditis.34
CONCLUSION
The presence of bacteria in aortic aneurysms did notnecessarily imply a causal relationship in aneurysm initiationand development, and some of these bacteria might havebeen secondary colonizers of a previously damaged vessel.The bacteria were detected regardless of etiology and ana-tomic location of the aneurysms, and even nonarterioscle-rotic aneurysms contained microorganisms. It could bespeculated that disorders of the connective tissue (eg, inMarfan’s syndrome) and other underlying and predispos-ing conditions, such as turbulent blood flow or nonbacte-rial inflammation, may facilitate penetration and secondarycolonization of microorganisms in the walls of aortic aneu-rysms. However, molecular detection of multiple bacteriain the walls of aortic aneurysms strongly suggested thatthese bacteria might have been important contributorsto the inflammatory reaction during aneurysm forma-tion, and therefore, may play a role in the developmentof the aneurysms.
AUTHOR CONTRIBUTIONS
Conception and design: RS, DC, EE, JA, LT, IOAnalysis and interpretation: RS, DC, EE, JA, IO
ences obtained from 10 aortic aneurysm samples. Theas constructed using the DNASTAR program, showing
sequtree w
Data collection: RS, PL, OG

JOURNAL OF VASCULAR SURGERYNovember 20061060 Marques da Silva et al
Writing the article: RSCritical revision of the article: RS, DC, EE, JA, PL, OG,
LT, IOFinal approval of the article: RS, DC, EE, JA, PL, OG, LT,
IOStatistical analysis: Not applicableObtained funding: RS, DC, OG, LT, IOOverall responsibility: RS
REFERENCES
1. Wassef M, Baxter BT, Chisholm RL, Dalman RL, Fillinger MF, Hei-necke J, et al. Pathogenesis of abdominal aortic aneurysms: a multidis-ciplinary research program supported by the National Heart, Lung, andBlood Institute. J Vasc Surg 2001;34:730-8.
2. Lindholt JS, Shi GP. Chronic inflammation, immune response, andinfection in abdominal aortic aneurysms. Eur J Vasc Endovasc Surg2006;31:453-63.
3. Olsen GJ, Lane DJ, Giovannoni SJ, Pace NR, Stahl DA. Microbialecology and evolution: a ribosomal RNA approach. Annu Rev Micro-biol 1986;40:337-65.
4. Woese CR. Bacterial evolution. Microbiol Rev 1987;51:221-71.5. Marchesi JR, Sato T, Weightman AJ, Martin TA, Fry JC, Hiom SJ, et al.
Design and evaluation of useful bacterium-specific PCR primers thatamplify genes coding for bacterial 16S rRNA. Appl Environ Microbiol1998;64:795-9.
6. Wilson KH, Blitchington RB, Greene RC. Amplification of bacterial16S ribosomal DNA with polymerase chain reaction. J Clin Microbiol1990;28:1942-6.
7. Marques da Silva R, Caugant DA, Lingaas PS, Geiran O, Tronstad L,Olsen I. Detection of Actinobacillus actinomycetemcomitans but notbacteria of the red complex in aortic aneurysms by multiplex polymerasechain reaction. J Periodontol 2005;76:590-4.
8. Edwards U, Rogall T, Blocker H, Emde M, Bottger EC. Isolation anddirect complete nucleotide determination of entire genes. Characteriza-tion of a gene coding for 16S ribosomal RNA. Nucleic Acids Res1989;17:7843-53.
9. Cole JR, Chai B, Farris RJ, Wang Q, Kulam SA, McGarrell DM, et al.The Ribosomal Database Project (RDP-II): sequences and tools forhigh-throughput rRNA analysis. Nucleic Acids Res 2005;33:D294-6.
10. Marques da Silva R, Lingaas PS, Geiran O, Tronstad L, Olsen I.Multiple bacteria in aortic aneurysms. J Vasc Surg 2003;38:1384-9.
11. Paster BJ, Boches SK, Galvin JL, Ericson RE, Lau CN, Levanos VA,et al. Bacterial diversity in human subgingival plaque. J Bacteriol 2001;183:3770-83.
12. Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L, SargentM, et al. Diversity of the human intestinal microbial flora. Science2005;308:1635-8.
13. Gilligan PH. Microbiology of airway disease in patients with cysticfibrosis. Clin Microbiol Rev 1991;4:35-51.
14. Coenye T, Goris J, Spilker T, Vandamme P, LiPuma JJ. Characteriza-tion of unusual bacteria isolated from respiratory secretions of cysticfibrosis patients and description of Inquilinus limosus gen. nov., sp. nov.J Clin Microbiol 2002;40:2062-9.
15. Chi CY, Fung CP, Wong WW, Liu CY. Brevundimonas bacteremia: two
case reports and literature review. Scand J Infect Dis 2004;36:59-61.16. Han XY, Andrade RA. Brevundimonas diminuta infections and itsresistance to fluoroquinolones. J Antimicrob Chemother 2005;55:853-9.
17. Minkwitz A, Berg G. Comparison of antifungal activities and 16Sribosomal DNA sequences of clinical and environmental isolates ofStenotrophomonas maltophilia. J Clin Microbiol 2001;39:139-45.
18. Marshall WF, Keating MR, Anhalt JP, Steckelberg JM. Xanthomonasmaltophilia: an emerging nosocomial pathogen. Mayo Clin Proc 1989;64:1097-104.
19. Crum NF, Utz GC, Wallace MR. Stenotrophomonas maltophilia endo-carditis. Scand J Infect Dis 2002;34:925-7.
20. Mehta NJ, Khan IA, Mehta RN, Gulati A. Stenotrophomonas malto-philia endocarditis of prosthetic aortic valve: report of a case and reviewof literature. Heart Lung 2000;29:351-5.
21. Ott SJ, El Mokhtari NE, Musfeldt M, Hellmig S, Freitag S, Rehman A,et al. Detection of diverse bacterial signatures in atherosclerotic lesionsof patients with coronary heart disease. Circulation 2006;113:929-37.
22. Cummins CS, Johnson JL. Corynebacterium parvum: a synonym forPropionibacterium acnes. J Gen Microbiol 1974;80:433-42.
23. Felner JM, Dowell VR Jr. Anaerobic bacterial endocarditis. N EnglJ Med 1970;283:1188-92.
24. Tunney MM, Patrick S, Curran MD, Ramage G, Hanna D, Nixon JR,et al. Detection of prosthetic hip infection at revision arthroplasty byimmunofluorescence microscopy and PCR amplification of the bacterial16S rRNA gene. J Clin Microbiol 1999;37:3281-90.
25. Eishi Y, Suga M, Ishige I, Kobayashi D, Yamada T, Takemura T, et al.Quantitative analysis of mycobacterial and propionibacterial DNA inlymph nodes of Japanese and European patients with sarcoidosis. J ClinMicrobiol 2002;40:198-204.
26. Galema L, Overbosch EH, Schrander-van der Meer AM, Brom HL,Roggeveen C, van Dorp WT. Mycotic aneurysm after aortic bifurcationprosthesis. Neth J Med 1996;48:105-8.
27. Brook I, Frazier EH. Aerobic and anaerobic microbiology of mycoticaortic aneurysm. Clin Infect Dis 1999;28:928-9.
28. Lazar JM, Schulman DS. Propionibacterium acnes prosthetic valveendocarditis: a case of severe aortic insufficiency. Clin Cardiol 1992;15:299-300.
29. Collins MD, Samelis J, Metaxopoulos J, Wallbanks S. Taxonomicstudies on some leuconostoc-like organisms from fermented sausages:description of a new genus Weissella for the Leuconostoc paramesen-teroides group of species. J Appl Bacteriol 1993;75:595-603.
30. Borch E, Kant-Muermans ML, Blixt Y. Bacterial spoilage of meat andcured meat products. Int J Food Microbiol 1996;33:103-20.
31. Olano A, Chua J, Schroeder S, Minari A, La Salvia M, Hall G. Weissellaconfusa (basonym: Lactobacillus confusus) bacteremia: a case report.J Clin Microbiol 2001;39:1604-7.
32. Flaherty JD, Levett PN, Dewhirst FE, Troe TE, Warren JR, Johnson S.Fatal case of endocarditis due to Weissella confusa. J Clin Microbiol2003;41:2237-9.
33. Heimdahl A, Hall G, Hedberg M, Sandberg H, Soder PO, Tuner K,et al. Detection and quantitation by lysis-filtration of bacteremia afterdifferent oral surgical procedures. J Clin Microbiol 1990;28:2205-9.
34. Li X, Kolltveit KM, Tronstad L, Olsen I. Systemic diseases caused byoral infection. Clin Microbiol Rev 2000;13:547-58.
Submitted May 25, 2006; accepted Jul 6, 2006.