au psyc706 final
TRANSCRIPT
Running head: MEDICINAL ISSUES: AIDS1
Medicinal Issues: AIDS
Shon Powell
PSYC 706-2 Medical Issues and Introduction to Pharmacology
Bill Heusler, Psy.D.
Antioch University Seattle
December 17, 2010
MEDICINAL ISSUES: AIDS 2
Abstract
Human Immunodeficiency Virus (HIV) is a disease that has risen to
epidemic proportions. Acquired Immunodeficiency Syndrome (AIDS)
is a secondary disorder and a direct result of exposure to the
HIV infection. HIV and AIDS are transmitted between individuals
through bodily fluids via mucous membranes. Opportunistic
infections account for the majority of deaths from AIDS.
Homosexuality has traditionally been associated with the disease,
however, heterosexual intimacy carries equal risk. Heterosexual
men generally do not feel the need to protect themselves from the
disease with condoms during heterosexual intercourse and this
leads to their vulnerability. Although different treatment
modalities are available, the current crop of antiretroviral
drugs are most effective in offering patients longer, healthier
lives.
MEDICINAL ISSUES: AIDS 3
Medicinal Issues: AIDS The world first became aware of the Human Immunodeficiency
Virus (HIV) in 1981 (Rathbun, Lockhart, & Stephens, 2006). The
disease is now considered a pandemic due to its dispersal through
human populations across the globe. According to Rathbun,
Lockhart, & Stephens (2006), the World Health Organization
estimates that approximately 38 million individuals worldwide had
been infected with HIV in 2003. An additional 4.8 million new
infections occurred in that same year alone. At present an
estimated 20 million persons have died from the HIV infection.
Since the first cases of AIDS were diagnosed more than 25 years
ago, women from the global south came to represent the primary
face of the disease. Conversely, men who have sex with women
remain a forgotten group in the pandemic, and are almost entirely
unaddressed in HIV prevention programs (Higgins, Hoffman, and
Dworkin, 2010).
Symptoms of a Presenting Patient
Tank, Heusser, Schroeder, Luft, & Jordon (2010) discussed a case
study:
MEDICINAL ISSUES: AIDS 4
A 43 year old man was referred to our syncope–and–
hypotension service because of recurrent “dizziness and
passing out” after a few seconds standing. According to the
patient’s history, a prescription for fludrocortisones and
midodrine had not helped him. He also reported erectile
dysfunction, complete anhidrosis, early satiety, and gastric
distention. His symptoms began 10 years earlier and worsened
gradually. The patient tested positive for human
immunodeficiency virus (HIV) in 1994. (p. 263)
According to Rathbun, Lockhart, & Stephens (2006) the
Acquired Immunodeficiency Syndrome (AIDS) is a disorder in which
the body’s immune system is suppressed as a direct result of
exposure to the human immunodeficiency virus (HIV) infection,
which is transmitted between individuals through bodily fluids
(for example, blood, semen, or vaginal fluids) via mucous
membranes. The vast majority of individuals with an HIV infection
develop AIDS within an average of seven to ten years. Moreover,
Hudson, Kirksey, & Holzemer (2004) reported that HIV positive
women presented with the following most frequently occurring
MEDICINAL ISSUES: AIDS 5
symptoms: (a) anxiety/fear (17.3%); (b) diarrhea (16.6%); (c)
neuropathy (11.6%); (d) nausea/vomiting (9.7%); (e) depression
(8.1%); and (f) fatigue (7.3%).
Tank, Heusser, Schroeder, Luft, & Jordon (2010) discussed:
The patient was normal weight with warm and dry skin. His
pupils responded slowly to light. Otherwise, his
neurological status was unremarkable. Cardiovascular
autonomic reflex testing was conducted with continuous
finger blood pressure, respiration, heart rate, and cardiac
stroke volume measurements. Respiratory sinus arrhythmia,
which is mediated through vagal modulation of heart rate,
was severely depressed. Blood pressure decreased profoundly
during phase II of the Valsalva manoeuvre and during phase
IV the pressure overshoot was absent. Hand grip and cold
pressure decreased dramatically. He became unconscious after
standing 30 s, which was not enough time to measure upper
arm blood pressure. Systolic and diastolic blood pressure
measured at the finger decreased by -95 and -40 mmHg,
respectively. Heart rate increased insufficiently by 4 beats
MEDICINAL ISSUES: AIDS 6
per minute. In response to 6.25 µg phenylephrine given
intravenously, his systolic blood pressure increased 20 mmHg
(normal ~ 3 mmHg) suggesting that resistance vessels hyper-
responded to adrenergic stimulation. Together, these
observations are consistent with severe autonomic failure
involving the parasympathetic and sympathetic nervous system
(p. 263)
Patient History
In 1993, the patient had been working as a commercial
trucker driver, and although married, the patient stated that
long periods of time away from his wife made him anxious for
female companionship. Adding to the patient’s restless feelings
was the fact that his marriage was suffering due to his
employment as a truck driver. Because of these circumstances the
patient solicited a commercial sex worker at a truck stop along
his regular route. The patient paid the commercial sex worker an
additional fee to forgo a condom during sexual intercourse. The
patient states that this was the only time that he had had
intercourse with anyone outside of his marriage.
MEDICINAL ISSUES: AIDS 7
Lee, Salman, and Fitzpatrick (2008) stated that depression
probably diminishes or indirectly affects an individual’s self-
efficacy, which is believed to be a significant factor in the
prediction of condom use during sexual intercourse and refusing
unsafe sexual practices. Furthermore, Solomon et al. (2000) found
that truck drivers are at particular high risk for acquiring HIV
due to long periods at work away from home without access to a
regular sex partner (see Appendix). Of additional note, HIV
infected truck drivers moving along their routes have long been
seen as a root factor in the international spread of HIV.
Higgins, Hoffman, & Dworkin (2010) established that men generally
do not feel the need to protect themselves with condom usage
during unprotected heterosexual intercourse. Moreover, men may be
at a great risk of contracting HIV through sexual intercourse
with small networks of high-risk women, though some other pattern
of sexual behavior may be at play.
Approximately nine months after his encounter with the
commercial sex worker, the patient began to complain of
persistent flu-like symptoms and aching joints. He saw a general
MEDICINAL ISSUES: AIDS 8
practitioner who did a routine blood screen. After the return of
these test results, the patient was told that he was HIV
positive. The patient confessed to his wife that he contracted
HIV, at which point she underwent testing and received a negative
result. The disclosure of the patient’s condition resulted in a
divorce from his wife and the termination of his employment.
According to Lyketos et al. (1995), there are a number of
findings showing that depressive symptoms develop in the early
and middle stages of HIV infection.
Physiological
The typical course of an HIV infection is defined by three
distinct phases: 1) primary infection phase, 2) chronic
asymptomatic and 3) latency phase/overt AIDS phase (Porth, 2007).
In most cases, the phases present themselves within an eight to
twelve year timeframe.
According to Porth (2007), once an individual is infected
with HIV, an acute mononucleosis will commonly occur much like
the syndrome known as the primary infection phase. The symptoms
of the first phase are often fever, fatigue, myalgias, sore
MEDICINAL ISSUES: AIDS 9
throat, night sweats, gastrointestinal problems, lymphadenopathy,
maculopapular rash, and headache. In addition, the primary
infection phase will be marked with an increase in viral
replication leading to high viral loads, which sometimes consist
of over 1,000,000 copies/mL and a decrease in CD4+ cell count.
This initial phase usually appears two to four weeks after
exposure to HIV, will usually last for a few days to two weeks,
and is marked by phase signs and the symptoms of the primary HIV
infection. Several weeks later, the immune system acts to curtail
viral replication reducing the viral load to a lesser degree.
This phase often remains at the same level for several years. If
the disease is caught in its beginning stage (primary infection),
infected individuals who are diagnosed with HIV seem to benefit
from early treatment, perhaps reducing the number of long living
HIV infected cells or CD4+ memory cells in their systems. The
latency phase is possibly the most dangerous phase for
transmission of the virus. During this period, individuals
present no outward signs of the virus. Median period for the
latent stage is approximately ten years. During this phase, the
MEDICINAL ISSUES: AIDS 10
CD4+ cell count falls until it reaches a critically low level
below which there is considerable risk of opportunistic infection
(see Patient Course). Lymphadenopathy develops in some HIV
positive individuals during this phase. Persistent generalized
lymphadenopathy is defined as lymph nodes that are chronically
swollen for more than three months in at least two locations, not
including the groin. The lymph nodes may be sore and/or be
visible externally.
When the CD4+ cell count reach a threshold less than 200
cells/µL, the overt AIDS phase is said to occur and is the
defining point for AIDS as an illness. Porth (2007) assert that
without antiretroviral therapy, this phase can lead to death
within two to three years. The risk of opportunistic (see Patient
Course) infections and death is increased significantly when the
CD4+ cell count reaches this level. In the United States, the
typical adult with overt AIDS presents with fever, diarrhea,
weight loss and the wasting syndrome, generalized
lymphadenopathy, multiple opportunistic infections, and in many
cases, secondary neoplasms.
MEDICINAL ISSUES: AIDS 11
According to Porth (2007), the clinical course of HIV varies
from person to person. Most (60% to 70%) of those infected with
HIV develop overt AIDS ten to eleven years after the infection -
these people are the typical progressors. Another 10% to 20% of
those infected experience more rapid progression. These
individuals develop overt AIDS in less than five years and are
called rapid progressors. The final 5% to 15% are slow
progressors, who do not experience progression to overt AIDS for
more than 15 years. There is subset of slow progressors, called
long-term nonprogressors, who account for 1% of all HIV
infections. These people have been infected for at least 8 years,
are antiretroviral naïve, have high CD4+ counts, and usually have
very low viral loads.
Patient Course
Opportunistic infections account for the majority of deaths
from AIDS (Porth, 2007). In the United States, the most common
opportunistic infections are Pneumocystis carinii pneumonia
(PCP), oropharyngeal or esophageal candidiasis (thrush),
MEDICINAL ISSUES: AIDS 12
cytomegalovirus (CMV) infection, and infections caused by
Mycobacterium avium-intracellulare complex (MAC). Additionally,
according to Marcus, Kerns, Rosenfeld, and Breitbart (2000),
HIV/AIDS related pain is a significant clinical problem
associated with functional impairment and psychological distress.
Currently, there is little empirical information available to
guide practitioners in the treatment of patients with HIV/AIDS
related pain. Furthermore, empirical investigations have
indentified numerous barriers to the adequate assessment and
treatment of AIDS pain (Bottonari, Safren, McQuaid, Hsiao, and
Roberts, 2010).
Patient Treatment
Tank, Heusser, Schroeder, Luft, & Jordon (2010) remarked
that patient autonomic failure may be caused by central nervous
system disorders or dysfunction of peripheral autonomic nerves.
They stated:
When we probed the peroneal nerve with a microneurography
electrode, we were unable to record efferent skin or muscle
sympathetic nerve activity. Venous plasma norepinephrine was
MEDICINAL ISSUES: AIDS 13
profoundly reduced (0.22 nM =37 ng/l; normal ~ 1.18 nM
= 200ng/l). Blood pressure failed to increase with ingestion
of the alph-2 adrenoreceptor antagonist yohimbine, which
normally raises sympathetic activity. These observations and
lack of additional neurological symptoms point to a lesion
involving peripheral autonomic neurons. He had no antibodies
against ganglionic nicotinergic acetylcholine receptors,
which is a rare potentially treatable cause of peripheral
autonomic dysfunction. An earlier report suggested that
orthostatic hypotension can also result from central nervous
system degeneration in HIV patients. (p. 263)
In this case study (Tank, Heusser, Schroeder, Luft, &
Jordon, 2010), the patient was encouraged to drink water
regularly before meals. He was also instructed to elevate the
head of his bed which decreased nocturia and increased
orthostatic symptoms. Additionally, he apply water to his skin to
increase heat tolerance. Finally, the patient continued on the
drug midodrine, which was tailored by the patient to accommodate
his daily activities. At the conclusion of his current battery of
MEDICINAL ISSUES: AIDS 14
treatment, the patient registered a supine blood pressure of
133/91 and a standing blood pressure of 66/36 mmHg while standing
for 10 minutes, thus affecting a cure for his fainting spells.
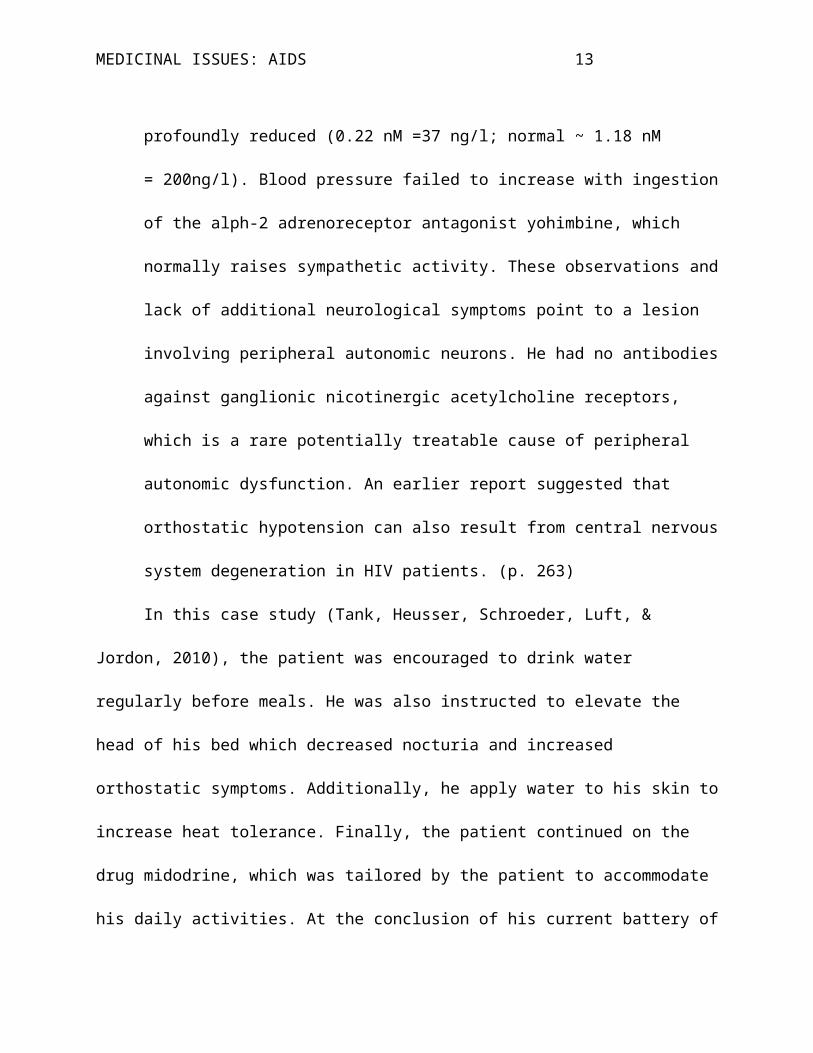
Although the patient in the case study did not use any
antiretroviral treatment, there are currently, pharmaceutical
treatments which include twenty antiretroviral medications,
comprised of four classes of antiretroviral (ARV) agents:
nucleoside/tide reverse transcriptase inhibitors (NRTIs), non-
nucleoside reverse transcriptase inhibitors (NNRTIs), protease
inhibitors (PIs) and fusion inhibitors (FIs). (See Table 1
through Table 4.)
Table 1.
Currently Available NRTIsBrand Name Generic Name Abbreviation Manufacturer
Emtriva® Emtricitabine FTC Gilead
Epivir® Lamivudine 3TC GlaxoSmithKline
Hivid® Zalcitabine ddC Roche
Retrovir® Zidovudine AZT ZDV GlaxoSmithKlineVidex EC® Didanosine ddI EC BristolMyersSqu
ibb
Viread® Tenofovir TDF Gilead
MEDICINAL ISSUES: AIDS 15
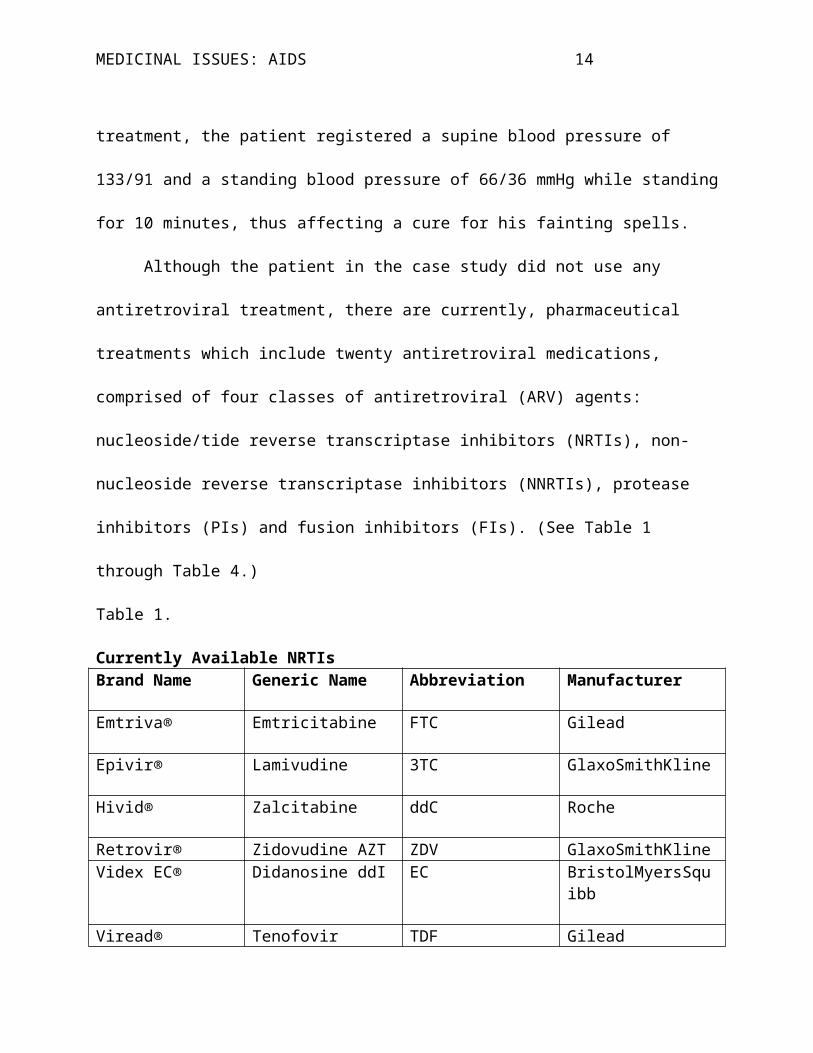
Zerit® Stavudine d4T BristolMyersSquibb
Ziagen® Abacavir ABC GlaxoSmithKline
Shibuyama et al., 2000
Table 2.
Currently available NNRTIsBrand Name Generic Name Abbreviation Manufacturer
Sustiva® Efavirenz EFV BristolMyersSquibb
Viramune® Nevirapine NVP Boehringer - Ingelheim
Rescriptor® Delavirdine DLV Pfizer - Agouron
Shibuyama et al., 2000
Table 3.
Currently available PIsBrand Name Generic Name Abbreviation Manufacturer
Lexiva® Fosamprenavir fAPV GlaxoSmithKline-Vertex
Crixivan® Indinavir IDV MerckFortovase® Saquinavir
soft gel SQV- sgc Roche
Invirase® Saquinavir- hard gel
SQV- hgc Roche
Kaletra® Lopinavir + ritonavir
LPV/r Abbott
Norvir® Ritonavir RTV AbbottReyataz® Atazanavir ATV BristolMyersSqu
ibb
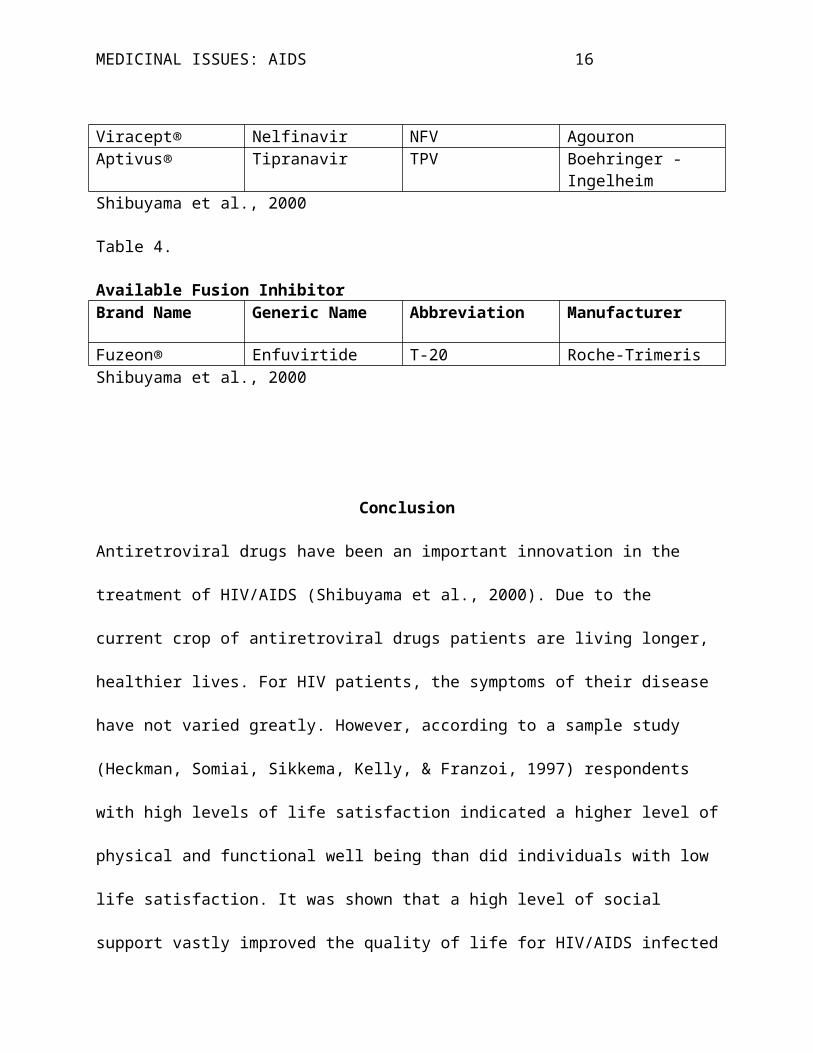
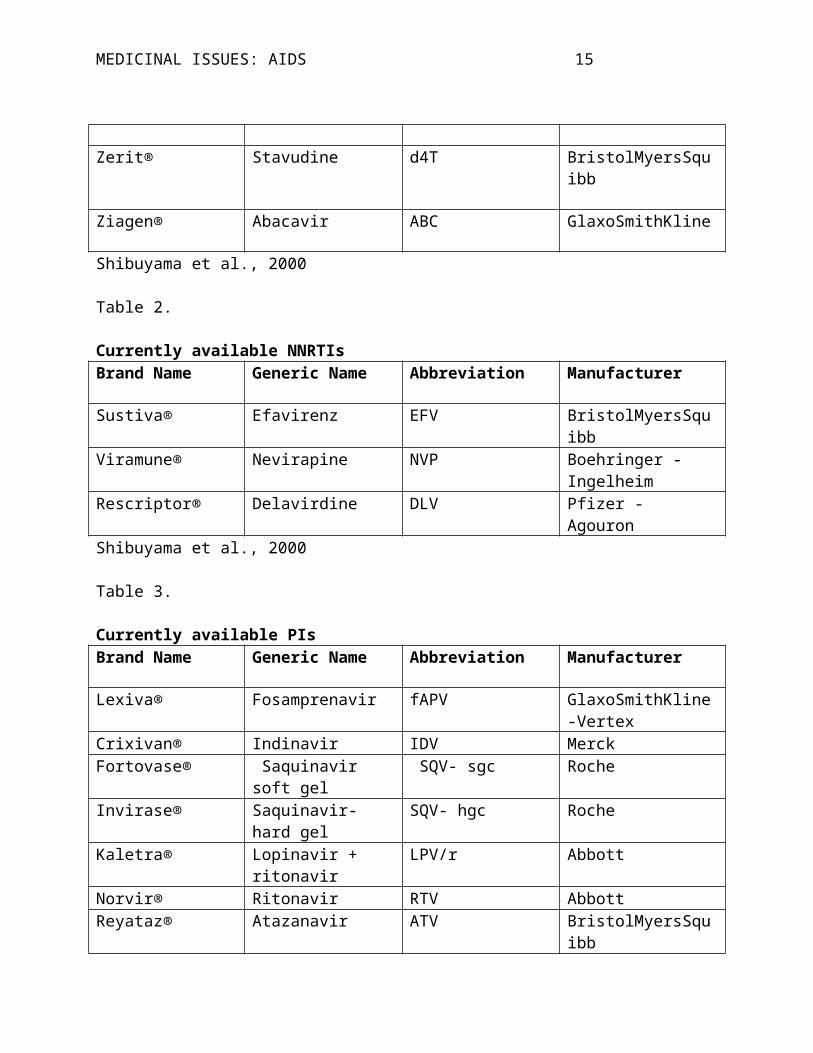
MEDICINAL ISSUES: AIDS 16
Viracept® Nelfinavir NFV AgouronAptivus® Tipranavir TPV Boehringer -
IngelheimShibuyama et al., 2000
Table 4.
Available Fusion InhibitorBrand Name Generic Name Abbreviation Manufacturer
Fuzeon® Enfuvirtide T-20 Roche-TrimerisShibuyama et al., 2000
Conclusion
Antiretroviral drugs have been an important innovation in the
treatment of HIV/AIDS (Shibuyama et al., 2000). Due to the
current crop of antiretroviral drugs patients are living longer,
healthier lives. For HIV patients, the symptoms of their disease
have not varied greatly. However, according to a sample study
(Heckman, Somiai, Sikkema, Kelly, & Franzoi, 1997) respondents
with high levels of life satisfaction indicated a higher level of
physical and functional well being than did individuals with low
life satisfaction. It was shown that a high level of social
support vastly improved the quality of life for HIV/AIDS infected
MEDICINAL ISSUES: AIDS 17
individuals. Yet, the stigma of homosexuality looms large in the
psychosocial aspects of HIV/AIDS within world culture.
Repudiation of homosexuality is a fundamental characteristic of
masculinity that can place men at greater risk for HIV (Higgins,
Hoffman, and Dworkin, 2010).
MEDICINAL ISSUES: AIDS 18
References
Bottonari, K. A., Safren, S. A., McQuaid, J. R., Hsiao, C., &
Roberts, J. E. (2009). A longitudinal investigation of the
impact of life stress on HIV treatment adherence. Journal of
Behavioral Medicine, 33, 486-495. doi:10.1007/s10865-010-9273-9
Heckman, T. G., Somlai, A. M., Sikkema, K. J., Kelly, J. A., &
Franzoi, S. L. (1997). Psychosocial predictors of life
satisfaction among persons living with HIV infection and
AIDS. Journal of the Association of Nurses in AIDS Care, 8(5), 21-30.
Higgins, J. A., Hoffman, S., & Dworkin, S. L. (2010). Rethinking
gender, heterosexual men, and women’s vulnerability to
HIV/AIDS. American Journal of Public Health, 100(3), 435-445.
doi:10.2105/AJPH.2009.159723
Hudson, A., Kirksey, K., & Holzemer, W. (2004). The influence of
symptoms on quality of life among HIV-infected women. Western
Journal of Nursing Research, 26(1), 9-23.
doi:10.1177/0193945903259221
Lee, Y., Salman A., & Fitzpatrick, J. J. (2009). HIV/AIDS
preventive self-efficacy, depressive symptoms, and risky
MEDICINAL ISSUES: AIDS 19
sexual behavior in adolescents: A cross-sectional
questionnaire survey. International Journal of Nursing Studies, 46, 653-
660. doi:10.1016/j.ijnurstu.2008.11.007
Lyketsos, C. G.., Hoover, D. R., Guccione, M., Dew, M. A., Wesch,
J., Bing, E. G., & Treisman, G. J. (1996). Depressive
symptoms over the course of HIV infection before AIDS. Social
Psychiatry and Psychiatric Epidemiology, 31, 212-219.
Marcus, K. S., Kerns, R. D., Rosenfeld, B., & Breitbart, W.
(2000). HIV/AIDS-related pain as a chronic pain condition:
Implications of a biopsychosocial model for comprehensive
assessment and effective management. Pain Medicine, 1(3), 260-
263.
Porth, C. M. (2007). Essentials of pathophysiology: Concepts of altered health
states. USA: Lippincott, Williams, & Wilkins
Rathbun, R. C., Lockhart, S. M., & Stephens, J. R. (2006).
Current HIV treatment guidelines – An overview. Current
Pharmaceutical Design, 12, 1045-1063.
Shibuyama, S., Gevorkyan, A., Yoo, U., Tim, S., Dzhangiryan, K.,
& Scott, J. (2006). Understanding and avoiding
MEDICINAL ISSUES: AIDS 20
antiretroviral adverse events. Current Pharmaceutical Design,
12,1075-1090.
Solomon, S., Ganesh, Al, Ekstrand, M., Barclay, J., Kumarasamy,
N., Mandel, J., & Lindan, C. (2000). High HIV seropositivity
at an anonymous testing site in Chennai, India: Client
profile and trends over time. AIDS and Behavior, 4(1), 71-81.
Tank, J., Heusser, K., Schroeder, C., Luft, F. C., & Jordan, J.
(2009). Automatic failure in a HIV-infected patient. Clinical
Autonomic Research, 20(4), 263-265. doi:10.1007/s10286-010-0063-
9
MEDICINAL ISSUES: AIDS 21
Critique
Bottonari, K. A., Safren, S. A., McQuaid, J. R., Hsiao, C., &
Roberts, J. E. (2009). A longitudinal investigation of the
impact of life stress on HIV treatment adherence. Journal of
Behavioral Medicine, 33, 486-495. doi:10.1007/s10865-010-9273-9
Participants were 87 treatment seeking HIV positive clients from an inner-city health clinic. Life stress is associated with poor outcomes in HIV treatment. Study seeks to example effects of psychosocial factors on life stress, depression, and coping skills. This article is valuable in its demonstration of patient’s ability to affect treatment outcomes.
Lyketsos, C. G.., Hoover, D. R., Guccione, M., Dew, M. A., Wesch,
J., Bing, E. G., & Treisman, G. J. (1996). Depressive
symptoms over the course of HIV infection before AIDS. Social
Psychiatry and Psychiatric Epidemiology, 31, 212-219.
Study describes the prevalence and course of symptoms before AIDSin HIV-infected homosexual men. The Center for Epidemiologic Studies Depression Scale (CES-D) is addressed in its primary roleas the measure of depressive symptoms. Depressive symptoms suffered most often by homosexual men are investigated. This article was used to describe the stigma felt by all men diagnosedwith AIDS.
Tank, J., Heusser, K., Schroeder, C., Luft, F. C., & Jordan, J.
(2009). Automatic failure in a HIV-infected patient. Clinical
MEDICINAL ISSUES: AIDS 22
Autonomic Research, 20(4), 263-265. doi:10.1007/s10286-010-0063-
9
Case report of severe autonomic failure in a 43-year-old well-controlled HIV patient was showcased. Clinical and pharmacological autonomic function testing and diagnosis of peripheral autonomic failure were demonstrated. Physiological maneuvers required to improve patient’s symptoms was addressed. This case study was the actual one used to complete the assignment.
MEDICINAL ISSUES: AIDS 23
Appendix
Solomon, S., Ganesh, Al, Ekstrand, M., Barclay, J., Kumarasamy,
N., Mandel, J., & Lindan, C. (2000). High HIV seropositivity
at an anonymous testing site in Chennai, India: Client
profile and trends over time. AIDS and Behavior, 4(1), 71-
81.
The study took place in Chennai, India, between the years of
1994 to 1998, during a rapidly escalating epidemic, and looked at
trends of various demographic groups among the sample of 1,745
male and female clients. It was found that 74% of the infections
were due to heterosexual transmission, but this figure was likely
skewed due to the social stigma and illegality of homosexual and
bisexual conduct in India.
The clients that were most often defined as HIV-seropositive
were commercial sex workers and their husbands, truck drivers and
their wives, migrant workers and their wives, and children who
were at risk primarily from prenatal transmission or blood
transfusions. The majority of clients were at risk due to their
sexual behavior, such as low condom use with the 64% having never
MEDICINAL ISSUES: AIDS 24
used one. Only a fraction of those infected were aware of their
condition. Absent from the study’s list of health center clients
were intravenous drug users.
In 1998, the U.S. Agency for International Development
community-based survey documented overall community HIV infection
rates of 1.8%. Higher documented rates were recorded in rural
areas (21%) than in urban areas (0.7%). Correlates of being HIV-
positive included occasional condom use, being married, being
referred by an HIV-positive sex partner, working as a truck
driver or migrant, or having a spouse in these professions.
Differing rates of infection have resulted from male migrant
workers who brought the epidemic back to their wives in rural
villages. Tamil Nadu accounted for 15% reported HIV infections
and 32% of its reported AIDS cases in India.
Forty three percent of the women came to the center after
exposure through an HIV-positive partner. HIV prevalence among
housewives (47%) was greater than amongst women who admitted to
being a commercial sex worker (32%) and was contrasted by only 4%
of men who sought testing because of partner referral. Women were
MEDICINAL ISSUES: AIDS 25
more likely to be infected by a regular partner, while the men
had been engaging in behaviors that they were aware would have
placed them at risk for HIV infection. Commercial sex workers
were the most likely to use condoms regularly but the study still
speculated that husbands of these commercial sex workers were
still at risk due to their wives employment.
Several factors may have contributed to the high rural
prevalence of HIV found in Tamil Nadu. It was found that the
occupational groups in which men were most likely to be HIV-
infected were truck drivers (82% HIV seropositive) and migrant
workers (68%). It was theorized that HIV infections moved along
the truck routes where drivers sought out commercial sex workers
or non-regular sex partners. Migrant workers sought out
alternative partners because they were often working in urban
centers for long periods away from their regular sex partners.
The prevalence of HIV in this sample was 51%, indicating
that the clinics had been successful in their outreach to at-risk
individuals. The increasing number of clients over time as well
as the change in demographic (most notably HIV-uninfected woman
MEDICINAL ISSUES: AIDS 26
and pregnant woman as well as older, married and uneducated men)
suggested that the clinic had been well-received by the
community. The success of the clinic served as a model for
similar centers in India, and signaled the widespread need for
anonymous testing and counseling.