advances in topical drug delivery system: micro to nanofibrous structures
TRANSCRIPT

Copyright © 2014 American Scientific PublishersAll rights reservedPrinted in the United States of America
ReviewJournal of
Nanoscience and NanotechnologyVol. 14, 853–867, 2014
www.aspbs.com/jnn
Advances in Topical Drug Delivery System:Micro to Nanofibrous Structures
Mangala Joshi∗, B. S. Butola, and Kasturi SahaDepartment of Textile Technology, Indian Institute of Technology Delhi, New Delhi 110016, India
This paper is a review of the latest developments in the field of topical drug delivery via which thedrug is directly applied onto the skin with high selectivity and efficiency. Advances in microfiber-based medical textiles such as sutures and wound dressings, especially those containing a drugor an antimicrobial agent, have been covered briefly. A special focus is on recent developments inthe area of nanofibrous drug delivery systems, which have several advantages due to their largesurface area to volume ratio, high porosity and flexibility. The electrospinning technique to producenanofibers has also been discussed with reference to latest advances such as multiple needles,needleless and coaxial forms of electrospinning. The applications of nanofibers in different areassuch as wound dressing, periodontal and anticancer treatment have also been discussed.
Keywords: Sutures, Nanofibrous Webs, Topical Drug Delivery, Wound Dressings,Electrospinning.
CONTENTS1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8532. Drug Delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8543. Topical Drug Delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8554. Topical Drug Delivery via Microfibrous Structures . . . . . . . . . . 855
4.1. Sutures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8554.2. Wound Dressing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 856
5. Topical Drug Delivery via Nanofibrous Structures . . . . . . . . . . . 8585.1. Advantages of Nanofibers . . . . . . . . . . . . . . . . . . . . . . . . . 8585.2. Electrospinning: Producing Nanofibers . . . . . . . . . . . . . . . 8585.3. Advances in Electrospun Nanofibrous
Systems for Drug Delivery . . . . . . . . . . . . . . . . . . . . . . . . 8596. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 864
References and Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 865
1. INTRODUCTIONAdvances in medical textiles and polymer science have ledto the development of a variety of novel drug delivery sys-tems. The aim is to deliver pharmaceutical agent to theaction site and consequently to the systemic circulation toproduce the desired pharmacological effect. The accom-plishment of predictable and consistent release of an activetherapeutic agent into a target site over a long periodhas much significant merit. It creates specific surround-ings with optimal release, minimum adverse effects andlong-term efficiency. Controlled drug release forms also
∗Author to whom correspondence should be addressed.
enhance safety, efficiency and reliability of drug therapy.Therefore, there is a need to develop suitable drug deliverysystems that not only administer the active therapeuticagents to the action site without affecting healthy tissuesbut also release drug in appropriate amount and over pro-longed periods. In a topical system, a drug is applieddirectly onto the skin and thus protects it from degradationduring systemic circulation. Advantages of topical drugdelivery systems include high efficacy with very little doseto a specific site, improving physiological and pharmaco-logical response and patient compliance, convenience andease of application along with the option of termination ofthe medication whenever required.Fibrous textile structures are popularly used in design-
ing topical drug delivery systems such as sutures, wounddressings, bandages etc. Conventional textile fibers orfilaments generally have a diameter in the micron(10–100 �m) range. They are converted to different typesof structures, such as monofilament or multifilament yarns,which can be twisted or braided and then converted todifferent fabric forms, such as woven, nonwoven andknitted. These textile structures have a wide range ofproperties such as flexibility, elasticity, strength, etc., andtherefore are used in a variety of biomedical applica-tions. Textiles used for medical purposes need to benon-allergic, non-carcinogenic, non-toxic, biocompatible,
J. Nanosci. Nanotechnol. 2014, Vol. 14, No. 1 1533-4880/2014/14/853/015 doi:10.1166/jnn.2014.9083 853

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
flameproof, antistatic in nature and should have optimumfatigue endurance. Antimicrobial property is also one ofthe important attributes for medical textiles as they remainin intimate contact of human body for most of the timeduring use and provide congenial environment and surfacerequired for growth of microbes, leading to infection.Recent developments in the field of nanomaterials and
their possible application in a wide variety of productsincluding nanomedicine and targeted drug delivery areevident from the current literature.1�2 Nano-biotechnologyresearchers are actively focused towards drug deliveryat a controlled and sustained rate to the site of actionusing nanoparticles.3–5 Such nanoparticle-based drug deliv-ery systems not only reduce the number of doses requiredbut also makes the treatment a better experience witha reduction in treatment expenses. With the advent ofnanotechnology, there is increased interest in nanofibers,which are typically 50–500 nm in diameter. Advantagesof nanofibrous delivery systems include the possibility ofdelivering uniform, large and controlled doses of phar-maceutical agents at the action site as a result of highsurface area to volume ratio, high porosity and high
Mangala Joshi is a Professor in the Department of Textile Technology at IIT Delhi. She isan alumnus of IIT Delhi having obtained her M.Tech. and Ph.D. degrees in Polymer Sci-ence and Technology, and she has 13 years of teaching experience in the area of fiberscience and technology. Her current research interests include nanotechnology applica-tions in textiles, polymer nanocomposites, nano-biomaterials, nanocoatings and nanofibers,bioactive and functional textiles. She is a member of a nano research group at IIT Delhiand is associated with an interdisciplinary team researching nanobiotechnology with afocus on bioactive nanocomposites.
B. S. Butola is a Ph.D. from and currently working as Assistant Professor in the Depart-ment of Textile Technology, IIT Delhi. He has around four years of working experiencein the industry of melt spinning area and around 11 years’ experience in teaching andresearch. His areas of interest include Protective textiles, Enzymatic processing of tex-tiles and Polymeric nanocomposites. Currently he is also working in the area of durableantimicrobial textiles and drug loaded textile structure for wound healing applications.
Kasturi Saha obtained her M.Tech. and B.Tech. degrees in Polymer Science and Engi-neering in India. She started her research in polymer-clay nanocomposites in 2009 underjoint supervision of Professor Mangala Joshi and Dr. B. S. Butola in Indian Institute ofTechnology, Delhi. Her research field is mainly focusing towards wound dressing and drugdelivery application employing film and nanofibrous nanocomposites.
flexibility of the lightweight nanofibrous system as com-pared to conventional topical drug delivery systems basedon microstructures.6
2. DRUG DELIVERYA drug is recognized as a substance, used in the diagnosis,treatment or prevention of a disease, or as a component ofmedication according to Federal Food, Drug and CosmeticAct (FD&C Act). Drug delivery is the process of adminis-tering a pharmaceutical compound to achieve a therapeuticeffect in humans or animals.7 An optimal drug deliverysystem assures availability of the active drug molecule atthe site of action for the appropriate time and duration.Drug concentration at the correct site must remain abovethe minimal effective concentration (MEC) and below theminimal toxic concentration (MTC). This concentrationinterval is known as the therapeutic range as shown inFigure 1.Most preferred routes of drug delivery include oral,
injection, transmucosal, inhalation and topical routes.8
Oral route (through the mouth) is the most familiar route
854 J. Nanosci. Nanotechnol. 14, 853–867, 2014

Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
Figure 1. Different ranges of drug delivery.
for drug administration.9 Another drug administrationroute directly into the body via the injection or infu-sion route is known as parenteral drug delivery. Mucosalmembrane is the most important route of drug adminis-tration into the body. The gastrointestinal tract is one ofthe most common mucosal membranes, allowing oral drugdelivery.10 Other mucosal absorption sites include buccal,sublingual, ocular, rectal, vaginal, lung and nasal. Inhala-tion route is an effective way of delivering medicationlocally to the lungs and is used extensively to treat respi-ratory conditions such as asthma and chronic obstructivepulmonary disease. Another preferred route of drug admin-istration is through the skin, commonly known as topicaldelivery system. This drug delivery system is designed togive a local drug effect and is not exposed to systemiccirculation. This will be discussed in more depth in thesubsequent sections.
3. TOPICAL DRUG DELIVERYTopical drug delivery is defined as the application of adrug containing formulation to the skin to treat cutaneousdisorders (e.g., acne) directly or for the treatment of anyother wound and wound-related infection. This is achievedin two ways: external and internal topicals. External top-icals are sprayed, spread or dispersed directly on to thecutaneous tissues to cover the affected site. However, inter-nal topicals are applied to the mucous membrane via oral,vaginal or on anorectal route for local activity. The advan-tages of topical drug delivery over more popular oral routeare summarized below:11
(a) avoids metabolic route(b) avoids risk and issues of intravenous medication undervarious situations of absorption, like changes of pH, pres-ence of enzymes, stomach emptying time etc.(c) high efficiency using very low total daily dosage viacontinuous input of drug(d) avoids fluctuations in drug level and inter- and intra-patient variations
(e) easy to terminate the medication whenever needed(f) availability of larger application area in comparisonwith nasal or buccal cavity(g) delivers drug to the appropriate action site with higherselectively(h) easy route of application(i) avoid gastro-intestinal incompatibility(j) better utilization of short biological half-life drug withnarrow therapeutic range(k) improves the physiological and pharmacologicalresponse and patient compliance.
Few disadvantages associated with topical drug deliveryare as listed below:12
(a) Occurrence of contact dermatitis or skin irritation dueto the drug and/or excipient(b) possibility of allergic reactions(c) denaturation of drug due to presence of enzyme in epi-dermal skin layer(d) difficulty of absorbing bigger particle size drug throughthe skin.
Various forms of topical therapeutic agents are mostly usedon wound sites for cleansing and debridement (surgicalremoval of foreign material and dead tissue from a wound)with antiseptic and antibacterial action. But for highly exu-dating wounds, topical formulating agents are not veryeffective in staying in contact with the wound area as itcan rapidly absorb fluid, lose its rheological features andbecome mobile. So, new generations of medicated prod-ucts with superior therapeutic value have come into play.These are active directly or indirectly either as cleansingor debriding agent for removal of necrosis tissue or asantimicrobials, which can prevent or treat infection or mayalso has active growth agents to assist in regeneration oftissue in the wound healing process.
4. TOPICAL DRUG DELIVERY VIAMICROFIBROUS STRUCTURES
The two most common examples of topical drug deliveryproducts are medicated sutures and wound dressings wheremicrofibrous structures are used.
4.1. SuturesCurrently used suture materials are mainly polymeric innature. The ideal suture should be strong in nature, ableto form a secure knot and should be easy to handle.13�14
Moreover, it is important that it causes minimal tissueinflammation and infection. Additionally it must be capa-ble of stretching up to a certain length, accommodatewound edema and undergo recoiling to the original lengthalong with contraction of wound. Sutures are generallymade from synthetic or natural micron-sized polymericfibers. Sutures are either monofilament, multifilament orbraided textile structures made up of non-biodegradablepolymers (non-absorbable) or biodegradable polymers
J. Nanosci. Nanotechnol. 14, 853–867, 2014 855

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
(absorbable). The common methods for manufacturingsutures are: wet spinning, dry spinning, melt spinningand gel spinning.15–18 The current trend in direction ofdeveloping bioactive surgical and radioactive sutures hasbeen covered in detail. A recent research activity reportsfabrication of drug-loaded sutures via blend or coaxialelectrospinning.19
Antimicrobial surgical sutures, with the antibioticsembedded in their structure, are utilized for treat-ment of operative sepsis. Sutures with anesthetic andanti-cancerous properties are also important. Antibiotics(clindamycin, gentamycin, lincomycin etc.), anesthetics(lidocaine, novocaine, trimecaine and pyrocaine), prote-olytic enzymes (tripsin and pepsin) and anti-tumor medi-cations (prospydin, 5-fluorocyl, sarcolysin, etc.) have beenincorporated into sutures to meet specific requirement.20
Antimicrobial agents such as Triclosan have been addedin some sutures i.e., Monocryl Plus, PDS Plus and CoatedVicryl Plus to impart additional antimicrobial functionalityto the suture material.21
Radioactive surgical suture is another modern kind ofbiologically active fiber that can act by the emission ofionizing irradiation from radioactive isotopes settled inits structure.22 Isotopes of sulphur-35 emitting soft beta-rays and phosphorus-32 isotopes emanating much harderrays have been incorporated in polypropylene, polyamide,polyvinyl alcohol and polyethylene terephthalate fibers bystrong covalent bonds and can be used as radioactive sur-gical sutures. This kind of suture has found an applicationin treating advanced malignancy of the head and neck andalso in ophthalmology.23�24
4.2. Wound DressingDressing is a material applied onto a wound with or with-out medication, to give it protection and also assist in heal-ing. An ideal wound dressing should have the ability to:(a) absorb exudates and toxic substances from wound site(b) maintain sufficient humidity at the interface of woundand dressing(c) provide gaseous permeability (both water vapor andair)(d) allow thermal insulation(e) protect the damaged site from penetration ofmicroorganisms(f) should be non-toxic and non-traumatic in nature.25�26
Other assessed parameters desired are(a) it must have satisfactory handling qualities; i.e., shouldbe tear-resistant and should not disintegrate in both wetand dry conditions(b) should be comfortable and sterilizable(c) cost effectiveness (needing low frequency of dressingchange).
Wound dressing materials are placed in the physiologicaland biological environment of a wound.
4.2.1. ClassificationDressings are categorized into primary, secondary andisland dressings.27 Primary dressings remain in physicalcontact with the affected site while secondary dressingslead to complete coverage of the primary dressing, suchas adsorbent pad or bandage. Island dressing consists ofa central absorbent region that is further encircled byan adhesive component. Another route of classificationincludes Passive, Interactive and Bioactive dressings.28�29
Passive dressings only provide coverage over the woundsite; e.g., gauze and tulle dressings. Interactive dressingscomprising various polymeric forms are largely transpar-ent, can permeate water vapor and oxygen, but are imper-meable to bacteria, e.g., hydrogels, hyaluronic acid orfoam dressings. Bioactive dressings deliver active com-ponents needed for wound treatment, e.g., hydrocolloids,alginates, collagens, chitosan, etc.
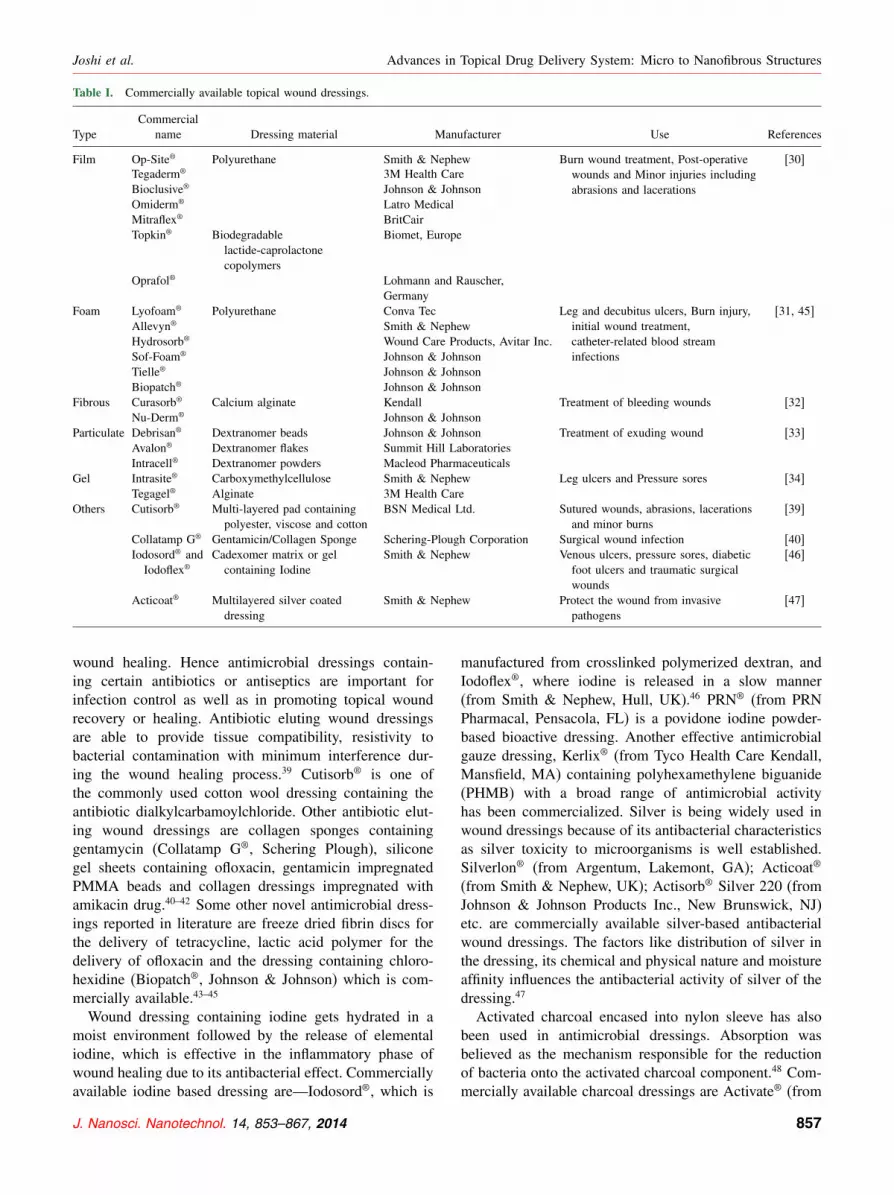
4.2.2. Advances in Wound DressingVarious forms of wound dressing available for topical drugdelivery are film, foam, fibrous, particulate and gel.30–34
Table I summarizes the various topical wound dressingscommercially available in the market. However, currenttrends in development of natural polymer-based as well asbioactive wound dressing is being discussed in detail inthe following sections:4.2.2.1. Natural Polymer Based Dressings. Naturally
occurring materials such as alginates and chitins, themain members of the polysaccharide group are becom-ing popular in making fibrous dressings. These dress-ings are generally hydrophilic (absorptive) in nature andsuitable for the treatment of bleeding wounds. Alginatedressings in fibrous forms are derived from alginic acidsalts obtained from algae Phaeophyceae found in sea-weed. Their best use is for moderate to heavily exudingwounds. This dressing is haemostatic, hydrophilic (absorbsup to 20 to 30 times its weight) and non-traumatic innature.35 It provides a moist environment that leads torapid granulation and reepithelialization helping in thewound healing process.36 Curasorb®, Nu-Derm® etc. arecommercially available alginate-based wound dressings.32
Chitin is a polymeric N-octyl-D glucosamine, one ofthe main constituents of the skeletal substances of crus-taceans and insects. Chitin non-woven fabric has beendirectly used as a dressing exhibiting excellent propertywith respect to pain relief, wound adherence and dryingwithout dissolution even in cases of deep dermal burnsthat contain a large number of exudates.32 This dressing iseffective for treatment of superficial burns, relief of painand epidermalization, and also provides effective barrieragainst bacterial infection.37�38 The dressing is also appli-cable as a mesh or patch for skin grafting with good adhe-sive quality.4.2.2.2. Bioactive Dressings. Infection and bacterial
colonization is the most important factor in delayed
856 J. Nanosci. Nanotechnol. 14, 853–867, 2014
Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
Table I. Commercially available topical wound dressings.
CommercialType name Dressing material Manufacturer Use References
Film Op-Site® Polyurethane Smith & Nephew Burn wound treatment, Post-operativewounds and Minor injuries includingabrasions and lacerations
[30]Tegaderm® 3M Health CareBioclusive® Johnson & JohnsonOmiderm® Latro MedicalMitraflex® BritCairTopkin® Biodegradable
lactide-caprolactonecopolymers
Biomet, Europe
Oprafol® Lohmann and Rauscher,Germany
Foam Lyofoam® Polyurethane Conva Tec Leg and decubitus ulcers, Burn injury,initial wound treatment,catheter-related blood streaminfections
[31, 45]Allevyn® Smith & NephewHydrosorb® Wound Care Products, Avitar Inc.Sof-Foam® Johnson & JohnsonTielle® Johnson & JohnsonBiopatch® Johnson & Johnson
Fibrous Curasorb® Calcium alginate Kendall Treatment of bleeding wounds [32]Nu-Derm® Johnson & Johnson
Particulate Debrisan® Dextranomer beads Johnson & Johnson Treatment of exuding wound [33]Avalon® Dextranomer flakes Summit Hill LaboratoriesIntracell® Dextranomer powders Macleod Pharmaceuticals
Gel Intrasite® Carboxymethylcellulose Smith & Nephew Leg ulcers and Pressure sores [34]Tegagel® Alginate 3M Health Care
Others Cutisorb® Multi-layered pad containingpolyester, viscose and cotton
BSN Medical Ltd. Sutured wounds, abrasions, lacerationsand minor burns
[39]
Collatamp G® Gentamicin/Collagen Sponge Schering-Plough Corporation Surgical wound infection [40]Iodosord® andIodoflex®
Cadexomer matrix or gelcontaining Iodine
Smith & Nephew Venous ulcers, pressure sores, diabeticfoot ulcers and traumatic surgicalwounds
[46]
Acticoat® Multilayered silver coateddressing
Smith & Nephew Protect the wound from invasivepathogens
[47]
wound healing. Hence antimicrobial dressings contain-ing certain antibiotics or antiseptics are important forinfection control as well as in promoting topical woundrecovery or healing. Antibiotic eluting wound dressingsare able to provide tissue compatibility, resistivity tobacterial contamination with minimum interference dur-ing the wound healing process.39 Cutisorb® is one ofthe commonly used cotton wool dressing containing theantibiotic dialkylcarbamoylchloride. Other antibiotic elut-ing wound dressings are collagen sponges containinggentamycin (Collatamp G®, Schering Plough), siliconegel sheets containing ofloxacin, gentamicin impregnatedPMMA beads and collagen dressings impregnated withamikacin drug.40–42 Some other novel antimicrobial dress-ings reported in literature are freeze dried fibrin discs forthe delivery of tetracycline, lactic acid polymer for thedelivery of ofloxacin and the dressing containing chloro-hexidine (Biopatch®, Johnson & Johnson) which is com-mercially available.43–45
Wound dressing containing iodine gets hydrated in amoist environment followed by the release of elementaliodine, which is effective in the inflammatory phase ofwound healing due to its antibacterial effect. Commerciallyavailable iodine based dressing are—Iodosord®, which is
manufactured from crosslinked polymerized dextran, andIodoflex®, where iodine is released in a slow manner(from Smith & Nephew, Hull, UK).46 PRN® (from PRNPharmacal, Pensacola, FL) is a povidone iodine powder-based bioactive dressing. Another effective antimicrobialgauze dressing, Kerlix® (from Tyco Health Care Kendall,Mansfield, MA) containing polyhexamethylene biguanide(PHMB) with a broad range of antimicrobial activityhas been commercialized. Silver is being widely used inwound dressings because of its antibacterial characteristicsas silver toxicity to microorganisms is well established.Silverlon® (from Argentum, Lakemont, GA); Acticoat®
(from Smith & Nephew, UK); Actisorb® Silver 220 (fromJohnson & Johnson Products Inc., New Brunswick, NJ)etc. are commercially available silver-based antibacterialwound dressings. The factors like distribution of silver inthe dressing, its chemical and physical nature and moistureaffinity influences the antibacterial activity of silver of thedressing.47
Activated charcoal encased into nylon sleeve has alsobeen used in antimicrobial dressings. Absorption wasbelieved as the mechanism responsible for the reductionof bacteria onto the activated charcoal component.48 Com-mercially available charcoal dressings are Activate® (from
J. Nanosci. Nanotechnol. 14, 853–867, 2014 857

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
3M Center, St. Paul, MN); Actisorb® (from Johnson &Johnson Products Inc., New Brunswick, NJ); CarboFlex®
(from ConvaTec Ltd, USA) and Lyoform® (from SetonHealthcare Group plc, Oldham, UK).49 Suggested advan-tages of these activated dressings are: they provide amoist atmosphere needed for autolytic debridement, effec-tively prevents bacterial colonization via absorption, pre-vent the growth of granulating tissue and minimizes thewound odor.
5. TOPICAL DRUG DELIVERY VIANANOFIBROUS STRUCTURES
5.1. Advantages of NanofibersElectrospun nanofibers exhibit interesting characteristics;e.g., high surface area and flexibility for surface func-tionalization; at the same time the as-spun fibrous matexhibits high porosity with pore size in sub-micrometerlength scale.50 Therefore, the overall drug release from thenanofibrous web is much higher than that of bulk films.Electrospun mats also demonstrate a good combinationof mechanical and physical properties with controlledrelease of antibiotic drug from the porous binding matrixand are also able to prevent bacterial colonization andinfection.51�52 Specific degradation characteristics andadjustable drug delivery profile by variation of fiber char-acteristics make the nonwoven nanofibrous mat a potentdrug delivery route as compared to polymeric films andparticles. These unique properties make electrospun fibermats as excellent candidates for the potential use inbiomedical field such as tissue engineering, DNA deliveryand drug delivery systems.53
Nanofibrous systems used directly as wound dress-ing show controlled evaporative water loss, excellentoxygen permeability and promote fluid drainage ability.Nanofibrous non-woven mat was also found to be use-ful for preventing post-surgery-induced abdominal adhe-sion. Maximum benefit is achieved when the release ofan antibiotic is conjugated with the nanofibrous barrier.Recent studies report that nanofibrous web in combinationwith drug release therapy is useful for specific applica-tion, such as anticancer treatment via the topical appli-cation route.53 The nanofibers have several advantages ascompared to other microsystems for applications in wounddressing as listed below:54 Hemostasis: This is the firststage of wound healing and plays a protective role. Smalldiameter nanofibers with a large effective surface area canpromote a hemostasis phase by absorbing the maximumamount of wound exudates without using any additionalhemostatic agent during topical application.Absorbability: Nanofibers with high surface area to vol-
ume ratio are able to absorb and retain extremely largeamounts of a liquid relative to their own mass. Nanofibrousdressings exhibit water absorption in the range of 18–213%as compared to conventional film dressings which showonly limited water absorption of around 2–3%.55
Semi-permeability: A semi-permeable nanofibrousstructure allows selective permeation of fluids or gasesthrough it but acts as a barrier to others (e.g., bacteria).High porosity of a nanofibrous web is ideal for the cellrespiration and it also appropriately controls the moist sur-roundings suitable for the wound healing. Moreover, smallpore size can efficiently protect the affected site fromany bacterial infection. Conformability: Conformability,defined as the ability to conform to the actual shape ofthe wound, is one of the characteristics related to the flex-ibility and resiliency during topical application. Accordingto theory of textile structures, the fabric conformability isdirectly associated with the fiber fineness.56 Finer fabricscan fit easily around the complicated three-dimensionalcontours. Therefore, ultrafine fibers are able to furnishexcellent conformability, better coverage and maximumprotection against bacterial contamination suitable for thetopical application.Surface modification: Modification of electrospun fibers
by incorporating therapeutic compounds is mainly accom-plished by post processing routes via conjugating activemolecules onto the nanofibrous surface.57 Various sur-face modification techniques to make polymeric nanofiberssuitable for drug delivery application are plasma treat-ment, wet chemical method and graft polymerization. Co-electrospinning is another route in which surface activeagents are integrated into the dope used for spinning.Active compounds including pharmaceutical agents suchas antiseptics, antifungal and vasodilators that cause dila-tion of blood vessels, etc., can be incorporated into thenanofibrous system depending on the treatment route andspecified role of the active agents. Other active additivesintegrated into nanofibrous structures are the growth fac-tor proteins that are involved in cell differentiation andgrowth, and other cells like keratinocytes which consti-tute 95% of the cells in the outermost epidermis layer ofhuman skin. Further, to achieve multi-functionality (all-in-one wound dressing), medication and growth factorstogether can be incorporated into single blended layervia electrospinning, which helps to avoid use of commer-cial dressings with a multilayered configuration. This con-tributes to extra benefits such as cost reduction and cuttingdown frequency of change in the dressing that otherwisehinders the regeneration of neotissues.Scar-free: Nanofibers also promote wound healing with-
out leaving any scar marks. For example, they assist in thegrowth of normal skin without any scarring due to goodcell connectivity.57 They also facilitate blood and tissuecompatibility that in turn leads to healing and regenera-tion of skin and provides better road map to skin cells forself-repair.
5.2. Electrospinning: Producing NanofibersWith emerging new areas of nanoscience and nanotech-nology, electrospinning has generated a lot of interest in
858 J. Nanosci. Nanotechnol. 14, 853–867, 2014

Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
producing nanofibers not only on the laboratory scale butalso for mass production of continuous nanofibers fromvarious polymers. This process of using electrostatic forcesto spin fibers was first patented by Formhals in 1934 andlater developed by Reneker et al. of University of Akron,USA.58�59
A number of synthetic polymers; e.g., nylon, polyester,polyacrylonitrile, cellulose acetate, polyurethane, poly-caprolactone, poly(lactic acid) as well as natural poly-mers; e.g., chitin, collagen, silk fibroin, etc. have been usedto produce nanofibers through electrospinning.60�61 In lastdecade, there has been significant progress in the devel-opment of electrospinning technology, such as producingnanofibrous webs at a faster rate or making modificationsin spinneret design to make different morphology (core-sheath, hollow fibers or side-by-side) structures. A briefoverview of these developments is given in the followingsection.(i) Depending upon the nature of the precursor, elec-trospinning process can be subdivided into solution andmelt electrospinning. In solution electrospinning, a poly-mer solution is held at the end of a capillary tube by sur-face tension which is further subjected to an electric field.When the electric field reaches a critical value, a chargedjet of solution is ejected from the tip of the Taylor cone andcontinuous fibers are collected onto the grounded collector.In melt electrospinning, instead of solution, a polymer meltis introduced into the capillary tube and spun into nano-fibers. Unlike for solutions, the electrospinning processfor a polymer melt has to be performed under a vacuum.Advantages associated with this process are high through-put rate, no need to eliminate harsh organic solvents andeasy preparation of nanofibers from those polymers that donot have appropriate solvents at room temperature such asPolypropylene, Polyethylene etc.(ii) Depending upon the feed system and its distributionmanner, the electrospinning system can be categorized intoconfined or unconfined feed systems.62 Confined feed sys-tem (CFS) includes a syringe and a syringe pump whichcan control the flow rate for stable electrospinning. Butclogging of the electrospinning setup is the main draw-back of this system. This system can be further subdividedinto needle or needleless systems. In conventional singleneedle electrospinning (SNE), one single jet is formed dur-ing the application of electrostatic force. Apart from this,multi-jets from the single needle are formed when thepolymeric jet undergoes interaction with the broad elec-trostatic field.63 Multi-jet formation has been attributedeither to discrepancy in electric field distribution or occur-rence of solution blockage at the needle tip. There areseveral reports on multiple needle electrospinning (MNE)systems in which needles are designed either in a lin-ear or two dimensional arrays such as elliptical, triangu-lar, square or hexagonal.64�65 Work has also been reportedto increase the productivity of electrospinning process
using needleless arrangement.66 In this system, when theelectric field intensity reaches a threshold value, multiplejets from the free liquid surface eject onto a grounded col-lector. Successful commercialization of this process hasbeen done by Elmarco Company’s “NanospiderTM.” In caseof unconfined feed system (UFS), flow of the polymericmelt or solution over the surface of another material isunrestricted in nature.67 This system includes bubble elec-trospinning, electroblowing, roller electrospinning, elec-trospinning from porous hollow tube and microfluidicmanifold.68–72 Advantage of the unconfined system is theability to form more jets without using any fine engineeredparts which require maintenance.62 But this kind of elec-trospinning leads to the formation of larger diameter fiberswith a broad distribution.(iii) Depending upon the spinneret modification and sol-vent evaporation rate, electrospun bicomponent nanofiberscan adopt either a core–shell, porous, hollow or side-by-side structure. In coaxial electrospinning, one solution isinjected into another at the tip of the spinneret.73 If the twosolutions are immiscible in nature then a core–shell struc-ture is formed. However, miscible solutions are reportedto form porous morphology due to phase segregation dur-ing solidification of the nanofibers. Emulsion electrospin-ning is another way to form continuous core-sheath fibersif the volume fraction of inner fluid in the emulsiondroplet is sufficiently high.74 Hollow fibers can also beproduced by using coaxial spinneret. Core sheath fiberscan be transformed into hollow fibers by extracting thecore using an appropriate solvent.75 Side-by-side bicompo-nent fibers are fabricated by using dual-opposite-spinneretelectrospinning.76
5.3. Advances in Electrospun NanofibrousSystems for Drug Delivery
In the following section various ongoing research activi-ties both in the academia as well as in the industry relatedto topical drug delivery are discussed, focusing mainlyon release kinetics and area of application. Various mod-ified fabrication techniques are also taken into account soas to improve the site-specific drug delivery with highefficiency.
5.3.1. According to Release KineticsThe main advantage of solution electrospun nanofibroussystem is the deliberate avoidance of melt processing routethat is not suitable for heat-sensitive drugs. It also mini-mizes the immediate burst release of a drug as observed inconventional topical drug delivery forms based on microfi-brous structures. The drug-release pattern (controlled,burst or sustained) from polymeric system is related tofiber diameter, efficiency of drug loading, drug–polymercompatibility, polymer degradation rate, addition of sur-factants and polymer biodegradability.
J. Nanosci. Nanotechnol. 14, 853–867, 2014 859

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
The release rate of drug from electrospun ultrafine fibermat depends upon the immersion time, molecular weightof the drug, nature of drug (hydrophobic or hydrophilic)etc. Other release controlling factors are drug solubility inthe polymer matrix and medium of testing, swelling abil-ity and solvability of the polymeric matrix in the elutingmedium, drug diffusion rate from the matrix, etc.77
Peng et al. studied in vitro paracetamol release profilesfor biodegradable poly(d,l-lactide) and poly(ethyleneglycol)-co-poly(d,l-lactide) electrospun nanofibrousmats.78 The results indicate an initial burst release whichdepends on drug–polymer compatibility whereas sustaineddelivery which follows is related to the polymer degrada-tion behavior. Paracetamol release and matrix degradationof poly(d,l-lactide) nanofiber was studied by Xiaohonget al.79 Larger diameter fibers exhibited a zero-orderkinetic profile for a longer period and a higher concentra-tion of drug encapsulation was also responsible for initialburst release after initial incubation in the phosphate buffersolution. Nanofibrous mat showed no molecular weightdecrease while remarkable mass reduction was found insmall and medium-size fibers due to surface erosion.Release of tetracycline hydrochloride drug from elec-
trospun poly(lactic acid), polyethylene-co-vinylacetate andtheir blends (50:50) was first examined by Kenawy et al.80
The release pattern showed continuous release for upto 120 days of the examination. Zhiwei et al.81 loadedtetracycline or chlorotetracycline in poly(D,L-lactide) byelectrospinning and demonstrated that electrospun fibersexhibited controlled drug delivery. Kanawung et al.53
investigated the delivery of diclofenac sodium and tetracy-cline hydrochloride from polycaprolactone and poly(vinylalcohol) nanofibrous mats. Drug release was increased ina monotonical way with increasing submerging time andexhibited constancy at long immersion times.Zong et al.82 fabricated bioabsorbable amorphous
poly(D,L-lactic acid) and semi-crystalline poly(L-lacticacid) non-woven membranes containing Mefoxin antibi-otic by electrospinning. Initial burst drug release due tothe concentration gradient was observed, which is use-ful for prevention of post-operative infection becausemost infections occur within the first few hours aftersurgery. Kim et al.83 confirmed the controlled release ofa hydrophilic antibiotic Mefoxin® from electrospun nano-fibers composed of poly(lactide-co-glycolide) (PLGA) andpoly(ethylene glycol)–poly(L-lactic acid) (PEG-b-PLA).Ketoprofen, a non-steroidal anti-inflammatory drug
(NSAID) release was studied by Kenawy et al.84 Fiberswere derived either from biodegradable polycaprolactoneor non-biodegradable polyurethane polymer or from theblending of the two. Results indicate that release ratesfrom all the systems are almost similar. In another study,release of ketoprofen from partially and fully hydrolyzedelectrospun poly(vinyl alcohol) fibers showed that uponthe treatment of electrospun PVA with methanol, the initial
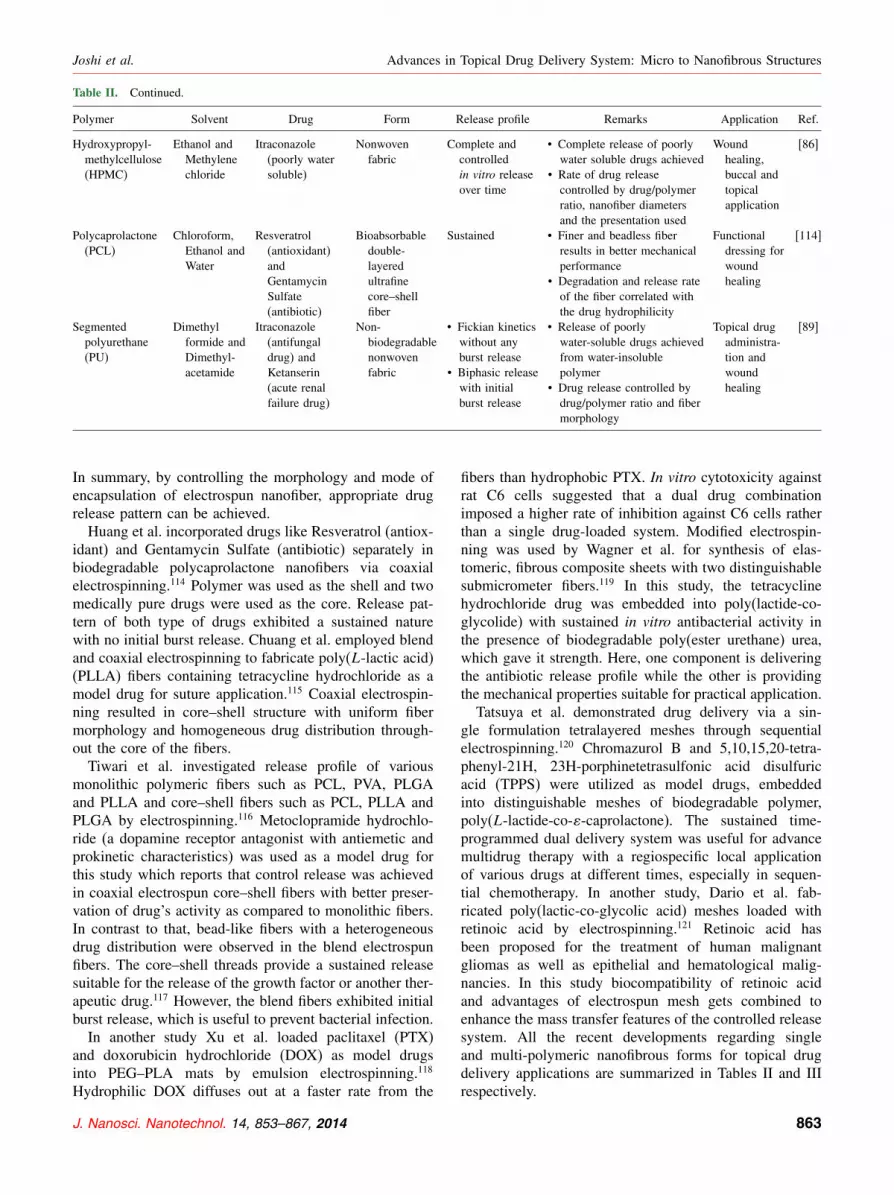
burst release was eliminated.85 Geert et al. also preparedwater-soluble polymers; i.e., hydroxylpropylmethylcellu-lose (HPMC) based nanofibers with poorly water-solubledrug, itraconazole by electrospinning.86 Here, completeand controlled release of drugs was achieved.
5.3.2. According to Application AreaRecent ongoing research activities aim to develop electro-spun ultrafine fibers containing drug formulations, whichcan be used as potential drug carriers for wound dress-ing applications, periodontal disease and anticancer treat-ment. One advantage of using the drug-loaded nanofibersincludes a biomaterial with nanoscale dimension and opti-mum porosity that can be designed for desirable drugdelivery.87 Katti et al. studied electrospun biodegrad-able polymer poly(lactide-co-glycolide) (PLGA) with cefa-zolin, a broad spectrum antibiotic.88 This system showspotential as antibiotic delivery system for the treatmentof wound. Geert et al. applied electrostatic spinning forincorporating poorly water-soluble drug, itraconazole andketanserin into nonbiodegradable segmented polyurethane(PU) nanofiber mainly used in topical drug delivery andwound healing.89 Itraconazole was released as a linearfunction of the square root of time, suggesting Fickiankinetics with no initial burst release. For ketanserin,a biphasic release pattern with two sequential linear com-ponents was observed.In another study, Bolgen et al. performed in vivo
studies to examine nanofibrous drug delivery systemfor intra-abdominal treatment.90 Both ornidazole (activeantibiotic against anaerobic intestinal bacteria) and bit-eral antibiotic were embedded into biodegradable poly-caprolactone by simply dropping antibiotic solution ontothe membranes. They reported that due to the combinedsynergistic effect of membrane and the antibiotic, thehealing process becomes better and faster. Supaphol et al.successfully prepared ultra-fine fiber mats of celluloseacetate comprising of four model drugs, i.e., naproxen,indomethacin, ibuprofen and sulindac by electrospinning.77
Mats of poly(vinyl alcohol) nanofibers with four differenttypes of non-steroidal anti-inflammatory drug with vari-able water solubility; e.g., sodium salicylate, diclofenacsodium, naproxen, and indomethacin were also developedby them for transdermal drug delivery systems.91 Resultsindicate that with an increasing molecular weight of adrug, the rate and amount of drug release decreases. Alsothe drug-loaded mats exhibited better release character-istics as compared to solvent cast films due to a highporosity of the electrospun nonwoven mats. Khil et al.reported that electrospun polyurethane (PU) membranesare useful as wound dressing material because it is ableto absorb wound exudates well, as it does not accumu-late under the covering and does not lead to any type ofwound desiccation.92�93 Histological examination suggeststhat the epithelialization rate is increased when wounds arecovered with nanofibrous PU membrane.
860 J. Nanosci. Nanotechnol. 14, 853–867, 2014

Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
Natural biopolymers such as chitosan, collagen, andsilk fibroin are also being used in combination to makenanofibrous mats. These natural polymeric materials arereported to have inherent properties helpful in wounddressing.94–96 Chitosan, a natural polysaccharide derivedfrom chitin provides bacteriostatic and fungistatic activ-ities. It therefore finds use in various biomedical appli-cations, such as surgical sutures, drug delivery carriers,bone healing and wound dressing materials, etc. It is ableto speed up healing of wound injury by accelerating thefibroblastic generation via collagen, promotes hemosta-sis phase and achieve natural tissue regeneration. Due tothe abovementioned reasons, chitosan in membrane formis currently considered as one of the most efficient bio-materials for wound healing.97 Other reported electrospundrug delivery systems using chitosan nanofibrous mem-branes include a chitosan-polyvinyl alcohol blend with ananofibrous membrane, biocompatible carboxyethyl chi-tosan/poly(vinyl alcohol) composite membrane, blendedchitosan and silk fibroin nanofibrous membrane, chitosan-coated poly(vinyl alcohol) nanofibrous matrix, etc., whichcan be directly used as a wound dressing material.98–101
In another study, Chen et al. fabricated compositenanofibrous membranes (NFM) composed of collagen andchitosan by electrospinning.102 Use of these membranespromoted wound curing and induced migration and pro-liferation phase. NFM are also able to attract fibroblastscell to the dermis layer, which can egest extracellularcomponents, such as collagen, growth and angiogenic fac-tors to repair the injured tissues. Liu et al. reported thatnanofibrous PLGA/collagen membranes were effective inresponse to human fibroblasts functionally and also act asearly stage wound-healing accelerators.103
There are some reports of herbal extracts and antimi-crobial peptide being introduced in nanofibers which helpin wound management and drug delivery.104 RecentlySupaphol et al. studied release characteristics of Cen-tella asiatica herbal extract which is familiar for itswound healing ability from electrospun gelatin fibers.105
According to the unit weight of wound-healing agentpresent in the samples, total amount releasing from thefilm was higher than the fiber mat; whereas depend-ing upon the unit weight of the sample, an inversetrend was noticed. Another study reports the perfor-mance of electrospun hyperbranched polyglycerol nano-fibers containing Calendula officinalis as a wound-healingand anti-inflammatory agent suitable for wound dressingapplications.106 Other than suture or wound-dressing appli-cations, electrospun nanofibrous systems are also efficientin facilitating targeted drug delivery for treatment of can-cer cells. Xie et al. developed Poly(lactide-co-glycolide)based microfibers and nanofibers which are suitable forsustained release of anticancer drug (paclitaxel) for treat-ing brain tumors.107 Zeng et al. studied electrospun matscontaining paclitaxel (lipophilic anticancer drug), dox-orubicin hydrochloride (hydrophilic drug with antitumor
activity) and doxorubicin base (lipophilic in nature) asmodel drugs. Release of drugs followed zero-order kinet-ics with no burst release, along with degradation of PLLAfibers in the presence of enzyme proteinase K added as alyophilized powder.108
In another study, anticancer drug doxorubicinhydrochloride was electrospun in a solution ofpoly(ethylene glycol)–poly(L-lactic acid) copolymer(PEG–PLLA) with homogeneous distribution of the anti-cancer agent within the nanofiber.109 Results indicatethat the initial burst release was diminished in case ofwater-in-oil emulsion electrospun fiber as compared withthe suspension electrospun nanofibers. Here release kinet-ics followed a combined mechanism of diffusion andenzymatic degradation. Chen et al. studied the potentialapplication of blends of nano-TiO2 and PLA nanofiberswith the anticancer drug doxorubicin to facilitate efficientdelivery in targeted cancer cells.110 Another drug, 1,3-bis(2-chloroethyl)-1-nitrosourea (BCNU) was encapsulatedin PEG–PLLA diblock copolymeric fibers by Xu et al.to treat malignant glioma. Drug release from the fiberswas dependent on the initial drug-loading and primarilyfollowed a diffusion route.111
Zing et al. studied the effect of addition of threetypes of surfactants (anionic, cationic, and nonionic) intopoly(L-lactic acid) electrospun fibers.112 These surfactantswere able to reduce the diameter size (from 4.2 �m to0.5 �m) and distribution of ultrafine fibers. For this study,Rifampin (tuberculosis drug) and paclitaxel (anti-cancerdrug) were employed as model drugs. The drugs werereleased constantly from fibers with no initial burst releaseassociated with degradation of such ultrafine fiber mats.This study thus established that the nanofibrous nonwovenmat is superior to polymer films and particles as a poten-tial drug delivery system for cancer treatment. Maedehet al. successfully electrospun PCL nanofibers contain-ing metronidazole benzoate (MET), which is useful forperiodontal disease treatment.113 Sustained release of drugthrough the nanofibers was achieved for at least 19 dayswith a low burst release, which could be an ideal treatmentperiod for periodontal diseases.
5.3.3. According to Different Morphology viaModified Electrospinning
Electrospinning is a versatile method for generating mono-lithic fibers from a variety of polymers. In addition tothe conventional single needle electrospinning, variousother modified electrospinning techniques such as coax-ial, blend, emulsion and sequential electrospinning havebeen studied for controlled drug delivery applications.Core–shell nanofibers are able to minimize burst releaseeffects whereas blend fibers are able to prevent bacterialcolonization and infection due to initial burst release. Alsoadvanced multi-drug therapy with specific application isachieved either by emulsion or sequential electrospinning.
J. Nanosci. Nanotechnol. 14, 853–867, 2014 861

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
Table II. Comparative chart of various single polymeric nanofibrous forms for topical application.
Polymer Solvent Drug Form Release profile Remarks Application Ref.
Poly(lactide-co-glycolide)(PLGA)
Tetrahydro-furan andDimethylformide
Cefazolin, (broadspectrumantibiotic)
Biodegradablenonwovennanofiber
Not mentioned • Used as antibiotic deliverysystems
• Drug loading caused anincrease in nanofiberdiameter
Woundtreatment
[88]
Poly(L-lacticacid) (PLLA)
ChloroformandAcetone
Lipophilic drugs:Rifampin andPaclitaxel;Hydrophilic drug:Doxorubicinhydrochloride
Ultrafinenonwoven fiber
Zero orderkineticsindicateconstantrelease withno initial burstrelease
• Addition of surfactants canreduce diameter size anddistribution of electrospunfibers
• Rifampin and Paclitaxelcompatible with PLLA butphase separation takesplace in case ofDoxorubicin hydrochloride
Clinicalapplication
[112]
Poly(L-lacticacid) (PLLA)
1,1,1,3,3,3-Hexafluoro-2-propanol
Tetracyclinehydrochloride(antibiotic drug)
Core-shell fibreby co-axial andblend fiber byblendelectrospinning
Sustained releasefromcore–shellfiber and burstrelease fromblend fiber
• Blend fibers showedsmaller diameter whereascore–shell fibers showedlarger average diameter
• Core–shell fiber suitablefor releasing the growthfactor or therapeutic drugsbut blend fiber useful toprevent bacterial infection
Tissuesuturingand tissueregenerationapplications
[115]
Poly(D,L-lactide)(PDLLA)
ChloroformandMethanol
Tetracycline andChlorotetracycline(antibiotic)
Nanofiber web Controlled • Different in vitro releaseprofiles and swellingbehaviors showed differentdrug release mechanisms
• Choice of solvent systemused to control the drugrelease
Biomedicalapplication
[81]
Poly(D,L-lactide)(PDLLA)
Acetone andChloroform
Paracetanol Fiber mat Burst releasefollowed bysustainedrelease
• Degradation behavior anddrug release kineticsrelated with variation offiber characteristic
Drug delivery [79]
Polyvinyl alcohol(PVA)
Methanol andWater
Ketoprofen Biodegradablenanofiber
Controlled • Release medium withhigher temperature showedhigher release rates
• Methanol treated matsshowed lower release thanuntreated ones
Drug delivery [85]
Poly(vinylalcohol) (PVA)
Water NSAID: Sodiumsalicylate (SS)(water soluble),Diclofenac sodium(DS) (sparinglywater soluble),Naproxen (NAP)and Indomethacin(IND) (both waterinsoluble)
Ultrafine fiber mat SS exhibits burstrelease butothers followmonotonousincrease withimmersiontime andbecome levelat longimmersiontime
• Electrospinning did notalter the chemical integrityof the drugs
• Drug release rate andamount decreasing withincreasing molecularweight of the drug
Transdermaldrugdeliverysystem
[91]
Celluloce acetate(CA)
Acetone/N ,Ndimethyl-acetamide(DMAc)
NSAID: Naproxen(NAP)Indomethacin(IND) Ibuprofen(IBU) Sulindac(SUL)
Ultrafine fiber mat Drug to releasefrom matrixmaintainingthe followingorder:IBU> NAP>
IND> SUL
• Absence of drugaggregates on the fibersurface indicated wellencapsulation of drugswithin the fibers
• Smaller the difference insolubility parametersbetween the drug andpolymer, greater is theirmiscibility and lower isthe drug release mainlyoccur by diffusion
Managementof painfuland inflam-matoryconditions
[77]
862 J. Nanosci. Nanotechnol. 14, 853–867, 2014
Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
Table II. Continued.
Polymer Solvent Drug Form Release profile Remarks Application Ref.
Hydroxypropyl-methylcellulose(HPMC)
Ethanol andMethylenechloride
Itraconazole(poorly watersoluble)
Nonwovenfabric
Complete andcontrolledin vitro releaseover time
• Complete release of poorlywater soluble drugs achieved
• Rate of drug releasecontrolled by drug/polymerratio, nanofiber diametersand the presentation used
Woundhealing,buccal andtopicalapplication
[86]
Polycaprolactone(PCL)
Chloroform,Ethanol andWater
Resveratrol(antioxidant)andGentamycinSulfate(antibiotic)
Bioabsorbabledouble-layeredultrafinecore–shellfiber
Sustained • Finer and beadless fiberresults in better mechanicalperformance
• Degradation and release rateof the fiber correlated withthe drug hydrophilicity
Functionaldressing forwoundhealing
[114]
Segmentedpolyurethane(PU)
Dimethylformide andDimethyl-acetamide
Itraconazole(antifungaldrug) andKetanserin(acute renalfailure drug)
Non-biodegradablenonwovenfabric
• Fickian kineticswithout anyburst release
• Biphasic releasewith initialburst release
• Release of poorlywater-soluble drugs achievedfrom water-insolublepolymer
• Drug release controlled bydrug/polymer ratio and fibermorphology
Topical drugadministra-tion andwoundhealing
[89]
In summary, by controlling the morphology and mode ofencapsulation of electrospun nanofiber, appropriate drugrelease pattern can be achieved.Huang et al. incorporated drugs like Resveratrol (antiox-
idant) and Gentamycin Sulfate (antibiotic) separately inbiodegradable polycaprolactone nanofibers via coaxialelectrospinning.114 Polymer was used as the shell and twomedically pure drugs were used as the core. Release pat-tern of both type of drugs exhibited a sustained naturewith no initial burst release. Chuang et al. employed blendand coaxial electrospinning to fabricate poly(L-lactic acid)(PLLA) fibers containing tetracycline hydrochloride as amodel drug for suture application.115 Coaxial electrospin-ning resulted in core–shell structure with uniform fibermorphology and homogeneous drug distribution through-out the core of the fibers.Tiwari et al. investigated release profile of various
monolithic polymeric fibers such as PCL, PVA, PLGAand PLLA and core–shell fibers such as PCL, PLLA andPLGA by electrospinning.116 Metoclopramide hydrochlo-ride (a dopamine receptor antagonist with antiemetic andprokinetic characteristics) was used as a model drug forthis study which reports that control release was achievedin coaxial electrospun core–shell fibers with better preser-vation of drug’s activity as compared to monolithic fibers.In contrast to that, bead-like fibers with a heterogeneousdrug distribution were observed in the blend electrospunfibers. The core–shell threads provide a sustained releasesuitable for the release of the growth factor or another ther-apeutic drug.117 However, the blend fibers exhibited initialburst release, which is useful to prevent bacterial infection.In another study Xu et al. loaded paclitaxel (PTX)
and doxorubicin hydrochloride (DOX) as model drugsinto PEG–PLA mats by emulsion electrospinning.118
Hydrophilic DOX diffuses out at a faster rate from the
fibers than hydrophobic PTX. In vitro cytotoxicity againstrat C6 cells suggested that a dual drug combinationimposed a higher rate of inhibition against C6 cells ratherthan a single drug-loaded system. Modified electrospin-ning was used by Wagner et al. for synthesis of elas-tomeric, fibrous composite sheets with two distinguishablesubmicrometer fibers.119 In this study, the tetracyclinehydrochloride drug was embedded into poly(lactide-co-glycolide) with sustained in vitro antibacterial activity inthe presence of biodegradable poly(ester urethane) urea,which gave it strength. Here, one component is deliveringthe antibiotic release profile while the other is providingthe mechanical properties suitable for practical application.Tatsuya et al. demonstrated drug delivery via a sin-
gle formulation tetralayered meshes through sequentialelectrospinning.120 Chromazurol B and 5,10,15,20-tetra-phenyl-21H, 23H-porphinetetrasulfonic acid disulfuricacid (TPPS) were utilized as model drugs, embeddedinto distinguishable meshes of biodegradable polymer,poly(L-lactide-co-�-caprolactone). The sustained time-programmed dual delivery system was useful for advancemultidrug therapy with a regiospecific local applicationof various drugs at different times, especially in sequen-tial chemotherapy. In another study, Dario et al. fab-ricated poly(lactic-co-glycolic acid) meshes loaded withretinoic acid by electrospinning.121 Retinoic acid hasbeen proposed for the treatment of human malignantgliomas as well as epithelial and hematological malig-nancies. In this study biocompatibility of retinoic acidand advantages of electrospun mesh gets combined toenhance the mass transfer features of the controlled releasesystem. All the recent developments regarding singleand multi-polymeric nanofibrous forms for topical drugdelivery applications are summarized in Tables II and IIIrespectively.
J. Nanosci. Nanotechnol. 14, 853–867, 2014 863

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
Table III. Comparative chart of various multi-polymeric nanofibrous forms for topical application.
Polymer Solvent Drug Form Release profile Remarks Application Ref.
Poly(lactic acid)(PLA) andPoly(ethylene-co-vinyl acetate)(PEVA)
ChloroformandMethanol
Tetracyclinehydrochloride(antibiotic)
Nonwovenfabric sheet
Smooth release • Crystallinity of PLAinhibited drug delivery forshort times
• Total drug release percentagefrom the cast film is lowerthan the electrospun matsdue to much lower surfacearea of the film
Controlledreleasetechnology
[80]
Poly(lactide-co-glycolide)(PLGA) anddiblockcopolymer(PEG-b-PLA)
Dimethylformide
Mefoxin®,(hydrophilicantibiotic)
Biodegradablenonwovennanofibrousscaffolds
Sustained • Used as local antibioticdelivery systems
• Morphology and density ofthe scaffold dependent onthe drug concentration
Prevention ofpostsurgicaladhesionandinfections
[83]
Poly(d,l-lactide)(PDLLA) andpoly(ethyleneglycol)-co-poly(d,l-lactide)(PELA)
Acetone Paracetanol(analgesicandantipyretic)
Fiber mat Burst releasefollowed bysustainedrelease
• Polymer degradation anddrug release adjusted bycontrolling fiber diameterand its porosity
Drug delivery [78]
Poly(ester urethane)urea (PEUU) andPoly(lactide-co-glycolide)(PLGA)
1,1,1,3,3,3-Hexafluoro-2-propanol
Tetracyclinehydrochloride(antibiotic)
Biodegradablefibrouscompositesheet by twostream elec-trospinning
Controlled • One component allowingantibiotic release whetherthe other responsible formechanical support
Abdominalwall closureandinfectioncontrol
[119]
Poly-l-lactide(PLLA)Polycaprolactone(PCL)Poly(lactide-coglycolide)(PLGA)Polyvinyl alcohol(PVA)
Chloroform,Dimethylformide andWater
Metoclopramidehydrochloride(dopaminereceptorantagonistwithantiemeticandprokineticproperties)
Core–shell andmonolithicelectrospunfibre
Controlled releasefrom core–shellfiber
• For effective drug release,sufficient hydrophilicitydifference and interfacialcompatibility between thecore and shell polymersmust exist
• Drug must have highersolubility in the core ratherthan in the shell
Drug deliveryapplication
[116]
Polycaprolactone(PCL) andPoly(vinylalcohol) (PVA)
Dichlorome-thane,Chloroformand Water
Diclofenacsodium andTetracyclinehydrochloride
Fiber mat Monotonousincrease indrug releasewith increasingimmersion timeand releasebecomeconstant at longimmersion time
• Fiber diameter increasedwith increasing solutionconcentration, amount ofdrug incorporation anddecreased with increasingapplied voltage and thecollection distance
– [53]
Polycaprolactone(PCL) andPolyurethane(PU)
ChloroformandMethanol
Ketoprofen,(non-steroidalanti-inflammatorydrug)
Nonwovennanofiber(Biodegrad-able andnon-biodegradable)
Initial burstreleasefollowed byslow release
• Release rates from the neatpolymers and their blend arealmost similar
• Drug released increased withincrease in temperature
Controllingpain andinflamma-tion inrheumaticdiseases
[84]
6. SUMMARYThe current trends in drug delivery research and de-velopment clearly show that nanomaterials, especiallynanofibers are increasingly being explored for possibleapplications in targeted drug delivery through topicalroute. Drug delivery via nanofibrous systems has manyadvantages compared to conventional microfibrous sys-tems such as improved therapeutic efficiency with lower
dosage, reduced toxicity by delivering drug to the specificsite, availability of large application area and minimalside effects. A variety of polymers, mostly biodegrad-able and a few non-biodegradables have been electrospunwith a range of drugs, including those meant for infec-tion control in wound dressing to anticancer drugs. Theseelectrospun nanostructures have several advantages overother forms of drug delivery such as films, foams, sponges,
864 J. Nanosci. Nanotechnol. 14, 853–867, 2014

Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
hydrogels, etc., in terms of high surface area to volumeratio, low density, flexibility and high porosity. Immediateburst release of drugs is observed in conventional microfi-brous systems such as sutures. This kind of release pro-file is advantageous for treating surgical infection whereimmediate action of a drug is necessary to inhibit thegrowth of bacteria. For acquiring long-term activity withhigh efficiency, such as oral and wound related infection,nanofibrous drug delivery systems are preferable. Nanofi-brous delivery systems are also desirable for site-specificactions, such as periodontal infection and anticancer treat-ment. The release kinetics of nanofibrous systems can becontrolled by controlling the nanofiber diameter or con-trolling mode of encapsulation of therapeutic agents orchanging the morphology to core–shell type. For exam-ple, monolithic and blend nanofibers exhibit burst releasekinetics whereas core–shell fibers are responsible for sus-tained release kinetics.However, there are still several challenges in upscal-
ing the electrospinning process. The first one is controlof the pore size and elimination of bead defects fromelectrospun nanofibers. The second one is maintaining theconsistency of the nanofiber diameter. Measurement ofmechanical properties of nanofibers poses technical diffi-culties and very few literature reports target this aspect.Electrospinning, the fabrication technique for nanofiberproduction is also quite expensive due to slow productionrate and high cost of technology as compared to conven-tional microfibrous systems. In addition to that, inhalationof nanofibers and solvent vapor also leads to health haz-ards. Due to these limitations, there are not many com-mercialized nanofibrous products in the market; althoughnanofibrous systems hold great promise and potential fornovel drug delivery applications. The limited speed of pro-duction of nanofibers via electrospinning is presently themajor bottleneck in taking the technology to commercialscale. Several companies like Donaldson, Elmarco, NanoFMG, SurModics are actively working toward upscalingelectrospinning technologies in terms of faster produc-tion rates as well as larger area coverage. A new venturecalled “The Electrospinning Company Limited,” foundedin 2010, has initiated design and commercial manufac-turing of nanofibrous scaffolding that supports the cellgrowth in a 3D structure. Finally, future collaborationsand greater communication between various disciplines,including medicine, engineering, material science, infor-mation technology and physics, will be instrumental inaddressing these issues and taking this technology to com-mercial success.
References and Notes1. N. Jain, R. Jain, N. Thakur, B. P. Gupta, D. K. Jain, J. Banveer,
and S. Jain, Asian J. Pharm. Clin. Res. 3, 159 (2010).2. K. Savolainen, L. Pylkkänen, H. Norppa, G. Falck, H. Lindberg,
T. Tuomi, M. Vippola, H. Alenius, K. Hämeri, J. Koivisto,D. Brouwer, D. Mark, D. Bard, M. Berges, E. Jankowska,
M. Posniak, P. Farmer, R. Singh, F. Krombach, P. Bihari, G. Kasper,and M. Seipenbusch, Safety Sci. 48, 957 (2010).
3. R. Misra, M. Upadhyay, and S. Mohanty, J. NanopharmaceuticsDrug Delivery 1, 103 (2013).
4. M. Vallet-Regí, E. Ruiz-Hernández, B. González, and A. Baeza,J. Biomater. Tissue Eng. 1, 6 (2011).
5. Y. Liu, S. Shah, and J. Tan, Rev. Nanosci. Nanotechnol. 1, 66(2012).
6. C. P. Caracciolo, R. C. P. Tornello, M. F. Ballarin, M. Florencia,and A. G. Abraham, J. Biomater. Tissue Eng. 3, 39 (2013).
7. M. N. V. Ravi Kumar (ed.), Handbook of Particulate Drug Deliv-ery, American Scientific Publishers, Los Angeles, USA (2008),Vols. 1–2.
8. M. E. Aulton, Aulton’s Pharmaceutics: The Design, and Manufac-ture of Medicines, Elsevier Health Sciences, London, UK (2007).
9. R. L. Carrier and K. C. Waterman, Handbook of Biodegrad-able Polymeric Materials and Their Applications, edited by S. K.Mallapragada and B. Narasimhan, American Scientific Publishers,Los Angeles, USA (2005), Vol. 2.
10. A. T. Florence and D. Attwood, Physicochemical Principles ofPharmacy, Pharmaceutical Press, London (2008).
11. A. N. Misra, Controlled and Novel Drug Delivery, CBS Publishersand Distributors, New Delhi (1997).
12. B. Mishra, J. K. Pandit, and S. K. Bhattacharya, Ind. J. Exp. Biol.28, 1001 (1990).
13. R. L. Moy, B. Waldman, and D. W. Hein, J. Dermatol. Surg. Oncol.18, 785 (1992).
14. M. H. Kudur, S. B. Pai, H. Sripathi, and S. Prabhu, Indian J. Der-matol. Venereol. Leprol. 75, 425 (2009).
15. S. W. Ha, A. E. Tonelli, and S. M. Hudson, Biomacromolecules6, 1722 (2005).
16. N. Kojic, M. Kojic, S. Gudlavalleti, and G. McKinley,Biomacromolecules 5, 1698 (2004).
17. L. Fambri, S. Bragagna, and C. Migliaresi, Macromolecules Symp.234, 20 (2006).
18. K. Yamaura and R. Kumakura, J. Appl. Polym. Sci. 77, 2872 (2000).19. L. H. Chuang, M. H. Zheng, and J. H. Xiao, J. Biomed. Mater.
Res. A 89A, 80 (2009).20. K. Y. Lin, H. M. Farinholt, V. R. Reddy, R. F. Edlich, and G. T.
Rodeheaver, J. Long-Term Eff. Med. Implants 11, 29 (2001).21. W. van Winkle, Jr and J. C. Hastings, Surg. Gynecol. Obstet.
135, 113 (1972).22. V. Zhukovsky, Autex Research Journal 3, 41 (2003).23. L. G. Richard, F. Willard, Jr, G. Donald, and M. Alvaro,
Laryngoscope 89, 349 (1979).24. K. Gündüz, J. S. Pulido, P. D. Yeakel, M. King, K. L. Classic, and
K. M. Furutani, Clin. Ophthalmol. 4, 159 (2010).25. T. D. Turner, Pharma. J. 222, 421 (1979).26. M. Choucair and T. Phillips, Skin Aging J. Geriatr. Dermatol. 6, 37
(1998).27. L. van Rijswijk, J. Wound Care 15, 11 (2006).28. D. Queen, H. Orsted, H. Sanada, and G. Sussman, Int. Wound J.
1, 59 (2004).29. A. F. Falabella, Dermatol. Ther. 19, 317 (2006).30. S. Ganlanduik, W. R. Wrigtson, S. Young, S. Myers, and H. C.
Polk, Jr, Am. Surgeon. 63, 831 (1997).31. D. A. Morgan, Pharma. J. 263, 820 (1999).32. W. Paul and C. P. Sharma, Trends Biomater. Artif. Organs. 18, 18
(2004).33. T. D. Turner, Vet. Dermatol. 8, 235 (1997).34. K. Lay-Flurrie, Prof. Nurse 19, 269 (2004).35. W. Paul and C. P. Sharma, Encyclopedia of Surface and Colloid
Science, edited by P. Somasundaran, Taylor and Francis, New York(2006).
36. I. Yuvarani, S. Senthil Kumar, V. Jayachandran, S. K. Kim, andP. N. Sudha, J. Biomater. Tissue Eng. 2, 53 (2012).
J. Nanosci. Nanotechnol. 14, 853–867, 2014 865

Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures Joshi et al.
37. P. T. S. Kumar, V. K. Lakshmanan, R. Biswas, S. V. Nair, andR. Jayakumar, J. Biomed. Nanotechnol. 8, 891 (2012).
38. R. Ramya, J. Venkatesan, K. S. Kim, and P. N. Sudha, J. Biomater.Tissue Eng. 2, 100 (2012).
39. C. J. Doillon and F. H. Silver, Biomaterials 7, 3 (1986).40. H. J. T. Rutten and P. H. A. Nijhuis, Eur. J. Surg. 578, 31 (1997).41. Y. Sawada, M. Ara, T. Yotsuyanagi, and K. Sone, Burns 16, 347
(1990).42. J. Grzybowski, W. Kolodziez, E. A. Trafny, and S. Jerzy, J. Biomed.
Mater. Res. A 36, 163 (1997).43. T. R. Kumar, M. V. Bai, and L. K. Krishnan, Biologicals 32, 49
(2004).44. Y. Sawada, O. Tadashi, K. Masazumi, S. Kazunobu, O. Koichi, and
J. Sasaki, Brit. J. Plast. Surg. 47, 158 (1994).45. B. L. Roberts and D. Cheung, Aust. Crit. Care 11, 16 (1998).46. K. Moore, A. Thomas, and K. G. Harding, Int. J. Biochem. Cell
Biol. 29, 163 (1997).47. I. Chopra, J. Antimicrob. Chemother. 59, 587 (2007).48. M. R. Frost, S. W. Jackson, and P. J. Stevens, Microbios Lett.
13, 135 (1980).49. J. C. Kerihuel, Wounds 5, 87 (2009).50. Z. M. Huang, Y. Z. Zhang, M. Kotaki, and S. Ramakrishna,
Compos. Sci. Technol. 63, 2223 (2003).51. S. Zhang, M.S. Dissertation, North Carolina State University
(2009).52. M. Gorji, A. A. Jeddi, and A. A. Gharehaghaji, J. Appl. Polym. Sci.
125, 4135 (2012).53. K. Kanawung, K. Panitchanapan, S. Puangmalee, W. Utok,
N. Kreua-ongarjnukool, R. Rangkupan, C. Meechaisue, andP. Supaphol, Polym. J. 39, 369 (2007).
54. Y. Zhang, C. T. Lim, S. Ramakrishna, and Z. M. Huang, J. Mater.Sci. Mater. Med. 16, 933 (2005).
55. S. E. Dabney, Ph.D. Dissertation, University of Akron, Akron, USA(2002).
56. P. Zahedi, I. Rezaeian, S. Siadatb, S. Jafari, and P. Supaphol, Poly-mer. Adv. Tech. 21, 77 (2010).
57. Q. P. Pham, U. Sharma, and A. G. Mikos, Tissue Eng. 12, 1197(2006).
58. A. Formhals, U.S. Patent, 1-975-504 (1934).59. D. H. Reneker and A. L. Yarin, Polymer 49, 2387 (2008).60. N. Bhardwaj and S. C. Kundu, Biotechnol. Adv. 28, 325 (2010).61. Z. Huang, Y. Z. Zhang, M. Kotaki, and S. Ramakrishna, Compos.
Sci. Technol. 63, 2223 (2003).62. R. Nayak, R. Padhye, I. L. Kyratzis, Y. B. Truong, and L. Arnold,
Text. Res. J. 82, 129 (2011).63. A. Yarin, W. Kataphinan, and D. Reneker, J. Appl. Phys. 98, 64501
(2005).64. W. Tomaszewski and M. Szadkowski, Fibers Text. East. Eur. 13, 22
(2005).65. S. Theron, A. Yarin, E. Zussman, and E. Kroll, Polymer 46, 2889
(2005).66. H. Niu, T. Lin, and X. Wang, J. Appl. Polym. Sci. 114, 3524 (2009).67. N. M. Thoppeya, J. R. Bochinski, L. I. Clarke, and R. E. Gorga,
Polymer 51, 4928 (2010).68. J. H. He, H. Y. Kong, R. R. Yang, H. Dou, N. Faraz, L. Wang, and
C. Feng, Them. Sci. 16, 1263 (2012).69. Y. M. Kim, K. R. Ahn, Y. B. Sung, and R. S. Jang, U.S. Patent,
7618579 (2009).70. F. Cengiz, T. A. Dao, and O. Jirsak, Polym. Eng. Sci. 50, 936
(2010).71. G. G. Chase, J. S. Varabhas, and D. H. Reneker, J. Eng. Fibr. Fabr.
6, 32 (2011).72. Y. Srivastava, I. Loscertales, M. Marquez, and T. Thorsen,
Microfluid. Nanofluid. 4, 245 (2008).73. A. V. Bazilevsky, A. L. Yarin, and C. M. Megaridis, Langmuir
23, 2311 (2007).
74. X. Xu, X. Zhuang, X. Chen, X. Wang, L. Yang, and X. Jing, Macro-mol. Rapid Commun. 27, 1637 (2006).
75. D. Li, J. T. McCann, and Y. Xia, Small 1, 83 (2005).76. F. Xu, L. Li, and X. Cui, J. Nanomater. 2012, 1 (2012).77. T. Santi, J. Ittipol, and P. Supaphol, Polymer 48, 5030 (2007).78. P. Hongsen, Z. G. Shaobing, L. Yanshan, L. Xiaohong, W. Jianxin,
and W. Jie, Colloids Surf. B 66, 206 (2008).79. C. Wenguo, L. Xiaohong, Z. Xinli, Y. Guo, Z. Shaobing, and W. Jie,
Biomacromolecules 7, 1623 (2006).80. E. Kenawy, G. L. Bowlin, K. Mansfield, J. Layman, D. G. Simpson,
E. H. Sanders, and G. E. Wnek, J. Control. Release 81, 57(2002).
81. X. Zhiwei and B. Gisela, J. Appl. Polym. Sci. 115, 1 (2009).82. X. H. Zong, K. Kim, D. F. Fang, S. F. Ran, B. S. Hsiao, and B. Chu,
Polymer 43, 4403 (2002).83. K. Kim, Y. K. Luu, C. Chang, D. Fang, B. S. Hsiao, B. Chu, and
M. Hadjiargyrou, J. Control. Release 98, 47 (2004).84. E. R. Kenawy, I. A. H. Fouad, H. E. N. Mohamed, and E. W. Gary,
Mater. Chem. Phys. 113, 296 (2009).85. E. R. Kenawy, I. A. H. Fouad, H. E. N. Mohamed, and E. W. Gary,
Mat. Sci. Eng. A-Struct. 459, 390 (2007).86. V. Geert, C. Iksoo, R. Joel, P. Jef, and E. B. Marcus, Pharmaceut.
Res. 20, 810 (2003).87. M. Jaiswal, A. Gupta, A. K. Agrawal, M. Jassal, A. K. Dinda, and
V. Koul, J. Biomed. Nanotechnol. 9, 1495 (2013).88. D. S. Katti, K. W. Robinson, F. K. Ko, and C. T. Laurencin,
J. Biomed. Mater. Res. Part B Appl. Biomater. 70, 286 (2004).89. V. Geert, C. Iksoo, R. Joel, P. Jef, V. D. Alex, M. Jurgen, N. Marc,
and E. B. Marcus, J. Control. Release 92, 349 (2003).90. N. Bölgen, I. Vargel, P. Korkusuz, Y. Z. Menceloglu, and E. Piskin,
J. Biomed. Mater. Res. Part B Appl. Biomater. 81, 530 (2007).91. P. Taepaiboon, U. Rungsardthong, and P. Supaphol, Nanotech-
nology 17, 2317 (2006).92. M. S. Khil, D. I. Cha, H. Y. Kim, I. S. Kim, and N. Bhattarai,
J. Biomed. Mater. Res. Part B Appl. Biomater. 67, 675 (2003).93. D. N. Heo, D. H. Yang, J. B. Lee, M. S. Bae, J. H. Kim, S. H.
Moon, J. H. Chun, C. H. Kim, H. Lim, and K. Kwon, J. Biomed.Nanotechnol. 9, 511 (2013).
94. K. Tomihata and Y. Ikada, Biomaterials 18, 567 (1997).95. S. P. Victor, W. Paul, and P. C. Sharma, J. Nanopharmaceutics
Drug Delivery 1, 193 (2013).96. R. Deepa, W. Paul, T. V. Anilkumar, and P. C. Sharma, J. Biomater.
Tissue Eng. 3, 261 (2013).97. L. Y. Chung, R. J. Schmidt, P. F. Hamlyn, B. F. Sagar, A. M.
Andrews, and T. D. Turner, J. Biomed. Mater. Res. 28, 463(1994).
98. A. G. Kanani, S. H. Bahrami, H. A. Taftei, S. Rabbani, andM. Sotoudeh, IET Nanobiotechnol. 4, 109 (2010).
99. Y. Zhou, D. Yang, X. Chen, Q. Xu, F. Lu, and J. Nie,Biomacromolecules 9, 349 (2008).
100. Z. Cai, X. Mo, K. Zhang, L. Fan, A. Yin, C. He, and H. Wang, Int.J. Mol. Sci. 11, 3529 (2010).
101. Y. O. Kang, I. Yoon, S. Y. Lee, D. Kim, S. J. Lee, W. H. Park,and S. M. Hudson, J. Biomed. Mater. Res. Part B Appl. Biomater.92, 568 (2010).
102. J. P. Chen, G. Y. Chang, and J. K. Chen, Colloids Surf., A 313, 183(2008).
103. S. Liu, Y. Kau, C. Chou, J. Chen, R. Wu, and W. Yeh, J. Membr.Sci. 355, 53 (2010).
104. T. H. B. Eriksen, E. Skovsen, and P. Fojan, J. Biomed. Nanotechnol.9, 492 (2013).
105. P. Sikareepaisan, A. Suksamrarn, and P. Supaphol, Nanotechnology19, 1 (2008).
106. V. E. A. Torres, N. C. Baracho, J. D. Brito, and A. A. A. Queiroz,Acta Biomater 6, 1069 (2010).
107. J. Xie and C. H. Wang, Pharmaceut. Res. 23, 1817 (2006).
866 J. Nanosci. Nanotechnol. 14, 853–867, 2014

Joshi et al. Advances in Topical Drug Delivery System: Micro to Nanofibrous Structures
108. Z. Jing, Y. Lixin, L. Qizhi, Z. Xuefei, G. Huili, X. Xiuling,C. Xuesi, and J. Xiabin, J. Control. Release 105, 43 (2005).
109. X. Xu, L. Yang, X. Xu, X. Wang, X. Chen, Q. Liang, J. Zeng, andX. Jing, J. Control. Release 108, 33 (2005).
110. C. Chen, L. Gang, P. Chao, S. Min, W. Chunhui, G. Dadong,W. Xuemei, C. Baoan, and G. Zhongze, Biomed. Mater. 2, L1(2007).
111. X. Xu, X. Chen, X. Xu, T. Lu, X. Wang, L. Yang, and X. Jing,J. Control. Release 114, 307 (2006).
112. Z. Jing, X. Xiaoyi, C. Xuesi, L. Qizhi, B. Xinchao, Y. Lixin, andJ. Xiabin, J. Control. Release 92, 227 (2003).
113. Z. Maedeh, M. Mohammad, V. Jaleh, and J. Marziyeh, Eur.J. Pharm. Biopharm. 75, 179 (2010).
114. Z. M. Huang, C. L. He, A. Yang, Y. Zhang, X. J. Han, and J. Yin,J. Biomed. Mater. Res. A 77A, 169 (2006).
115. L. H. Chuang, M. H. Zheng, and J. H. Xiao, J. Biomed. Mater.Res. A 89A, 80 (2009).
116. S. K. Tiwari, R. Tzezana, E. Zussman, and S. S. Venkatraman, Int.J. Pharm. 392, 209 (2010).
117. X. Ji, W. Yang, T. Wang, C. Mao, L. Guo, J. Xiao, and N. He,J. Biomed. Nanotechnol. 9, 1672 (2013).
118. X. Xiuling, C. Xuesi, W. Zhanfeng, and J. Xiabin, Eur. J. Pharm.Biopharm. 72, 18 (2009).
119. Y. Hong, K. Fujimoto, R. Hashizume, J. Guan, J. J. Stankus,K. Tobita, and W. R. Wagner, Biomacromolecules 9, 1200(2008).
120. O. Tatsuya, T. Kengo, and K. Satoru, J. Control. Release 143, 258(2010).
121. P. Dario, M. P. Anna, D. Nicola, D. Dinuccio, and C. Federica,Acta Biomater. 6, 1258 (2010).
Received: 29 August 2013. Accepted: 15 September 2013.
J. Nanosci. Nanotechnol. 14, 853–867, 2014 867