abc's of treatment strategies for upper extremity instabilities
TRANSCRIPT
1
ABCrsquos of Treatment Strategies for Upper Extremity Instabilities
Tambra Marik OTD OTL CHT
Secrets to Stabilization Part 1 1
Objectivesbull Describe the basic functional anatomy and
biomechanics of the shoulder wrist and elbow
bull Implement the concepts of functional rehabilitation
bull Assess pathomechanics of instabilities of the shoulder elbow and wrist
bull Utilize evaluation tests and interpret diagnostic values of tests for application to daily clinical practice
bull Implement neuromuscular training and core strengthening to treatment strategies
Secrets to Stabilization Part 1 2
THEMES
bull Rehabilitation concepts
ndash Themes of stabilization functional rehabilitation
ndash Rest and immobilization required for healing
ndash Specific structures require protection
ndash Gradual ROM progressions based on soft tissue healing
ndash The core matters
ndash Gradual progression towards strengthening and return to previous level of function
ndash Proximal and distal joint movement patterns addressed to avoid further injury
ndash Proprioception trainingsensorimotor activities
Secrets to Stabilization Part 1 3
2
THEMES Secrets to Stabilization
Functional Rehabilitation
Core
Motor Control
Dynamic Stability
Static StabilitySecrets to Stabilization Part 1 4
Secrets to Stabilization Part 1 5
Function
Rehabilitation
Core Stability
Static Stability
Motor Control
DynamicStability
Local
Stabilizers
Global
Stabilizers
Global Mobilizers
bull Abnormal
movement at 1
segment
bull Reflex inhibition
bull Poor response to
load
bull Poor movement
patterns at
segment
Dysfunction
bull Decreased force
production
bull Reflex inhibition
bull Dysfunctional
recruitment
pattern
Secrets to Stabilization Part 1 6
Local
StabilizersGlobal
Stabilizers
Global
Mobilizers
bull Overactive amp
tight muscles
bull Spasms
bull Results in
decreased
movement
patterns at
several joints
3
GLENOHUMERAL STABILIZERS
STATIC
bull LigamentsCapsule
bull Geometry of GH joint
bull Glenoid Labrum
bull Negative intra-articular
pressures
7
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and
Rebab Clinics of N Amer 200415575-605Secrets to Stabilization Part 1
Static Stability
Motor Control
Pacinian Ruffini
Extreme Motion
Compressive Strength
Extreme Motion
Tensile Strength
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
8Secrets to Stabilization Part 1
Static Stability
Ligaments of the Shoulder Girdle
bull Sternoclavicular (SC)ndash Anterior Posterior
ndash Costoclavicular
bull Acromio-clavicular (AC)ndash Coracoacromial
ndash Coracoclavicular (conoid trapzoid)
bull Superior Transverse Ligament
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
9
httpuploadwikimediaorgwik
ipediacommons33bGray326
pngSecrets to Stabilization Part 1
4
Ligaments of the Shoulder Girdle
Sternoclavicular
bull Interclavicular inferior displacement
(holds shoulder up)
bull Anteriorposterior antpost displacement
bull Costoclavicular excessive rotation and
mediallateral displacement
Retrieved on 81515 from httpclassconnections3amazonawscom535flashcards3547535pngsternoclavicular_j
14105C8D3116E509030png
restrains
restrains
restrains
Secrets to Stabilization Part 1
Mechanism of Injury SC ligament
Direct or Indirect force
Anterior dislocationbull 8 wks in sling
bull Elbowwrist ROM
8 wks ROM below 90deg(gradual reduce sling wear)
12 wks Full ROM and strengtheningGuan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Posterior dislocation
bull Posterior dislocation 6-8
wks figure of eight clavicle
strap and gentle
pendelums Avoid flex and
abduction above 90
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic
posterior sternoclavicular dislocations Journal of Shoulder and Elbow Surgery
20(1) 107-113
Secrets to Stabilization Part 1 11
Ligaments of the Shoulder Girdle
bull Acromio-clavicular
12
Retrieved on 81515 from
httpssyimgcomfzapires12nRAxT99C962Y7olZJXIcWw--
YXBwaWQ9c3JjaGRkO2g9NjEyO3E9OTU7dz02MjU-
httpclassconnections3amazonawscom184flashcards1904184jpg
11353982940540jpg
bull Acromoclavicular antpost
translation provides horizontal stabilization
bull Coracoacromial antpost translation
bull Coracoclavicular vertical
displacement
restrains
restrains
restrains
Secrets to Stabilization Part 1
5
Mechanism of Injury AC ligament
Fall directly on shoulder
Types I amp IIbull 1 to 3 wks wear sling
(discharge as pain subsides)
bull ROM and strengthening
Type III (conservative)
bull 3 to 4 wks wear sling
bull Progress ROM amp strength
Types IV V (Reconstruction
Procedures)
bull 6-8 wks Gunslinger Shoulder Orthosis
bull AROM elbow wrist and hand
bull 7 to 10 days PROM to 90deg flexion supine
bull AROM 6 to 8 wks
bull Strengthening at 12 wks if no pain with
arom
bull 12 to 16 wks gradual return to pre-
injury activity levelJohansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries indications
for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82Secrets to Stabilization Part 1 13
Glenohumeral
Ligaments
14
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
bull Coracohumeral ligament (CHL)
bull Superior glenohumeral ligament (SGHL)
bull Middle glenohumeral ligament (MGHL)
bull Inferior glenohumeral ligament (IGHL)
bull Posterior band glenohumeral ligament
httpuploadwikimediaorg
wikiped
Iacommons33bGray326
png
15Secrets to Stabilization Part 1
6
Ligaments of the Glenohumeral
JointCoracohumeral
bull Coracohumeral ligament (CHL)
Connects coracoid process to greater and lesser
tuberosities of the humerus
httpuploadwikimediaorgwikipediacommons33bGray326png
16Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
(SGHL MGHL IGHL)bull Superior glenohumeral ligament
(SGHL)
Connects anterosuperior edge of the glenoid to the lesser tubercle of the humerus
bull Middle glenohumeral ligament (MGHL)
Connects supra-glenoid tubercle superior labrum or scapular neck to lesser tuberosity
bull Inferior glenohumeral ligament (IGHL)
Connects anteroinferior labrum and glenoid lip to lesser tuberosity
httpuploadwikimediaorgwikipediacom
mons33bGray326png
Axillary
Pouch
SGHL
MGHL
IGHL
17Secrets to Stabilization Part 1
Stabilizers Against Anterior Translations
bull Humerus adducted Subscapularis
bull Humerus abducted 45deg Subscapularis middle
anterior GH ligament and superior portion of
inferior anterior GH ligament
bull Humerus at 90deg abduction Inferior anterior GH
ligament
18Turkel et al 1981
Retrieved from httpwwwradsource
us_images0909_6jpgSecrets to Stabilization Part 1
7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
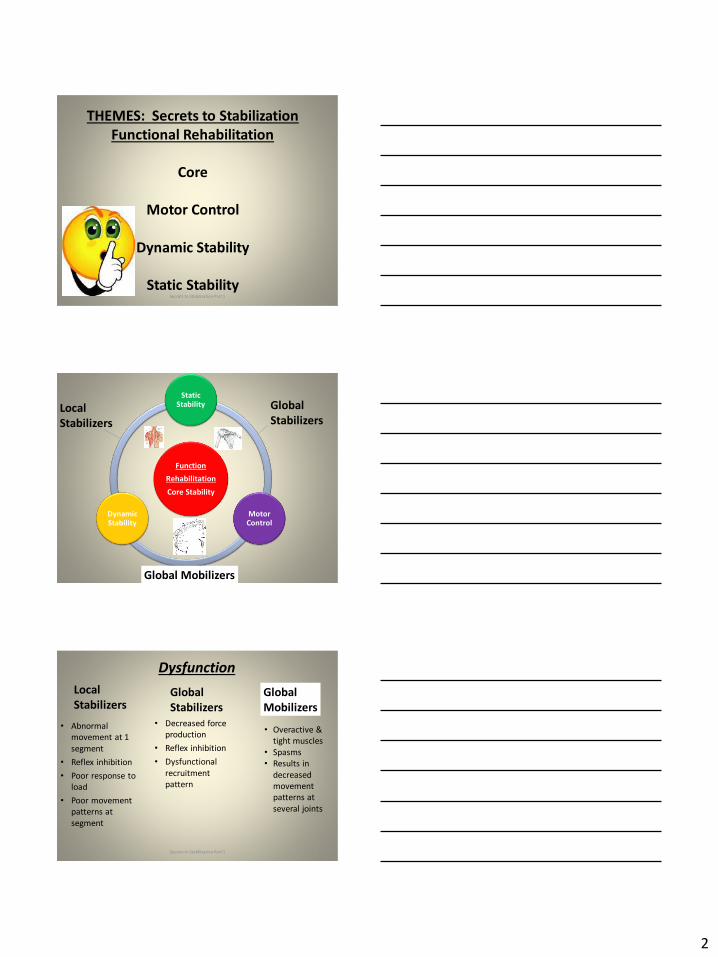
2
THEMES Secrets to Stabilization
Functional Rehabilitation
Core
Motor Control
Dynamic Stability
Static StabilitySecrets to Stabilization Part 1 4
Secrets to Stabilization Part 1 5
Function
Rehabilitation
Core Stability
Static Stability
Motor Control
DynamicStability
Local
Stabilizers
Global
Stabilizers
Global Mobilizers
bull Abnormal
movement at 1
segment
bull Reflex inhibition
bull Poor response to
load
bull Poor movement
patterns at
segment
Dysfunction
bull Decreased force
production
bull Reflex inhibition
bull Dysfunctional
recruitment
pattern
Secrets to Stabilization Part 1 6
Local
StabilizersGlobal
Stabilizers
Global
Mobilizers
bull Overactive amp
tight muscles
bull Spasms
bull Results in
decreased
movement
patterns at
several joints
3
GLENOHUMERAL STABILIZERS
STATIC
bull LigamentsCapsule
bull Geometry of GH joint
bull Glenoid Labrum
bull Negative intra-articular
pressures
7
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and
Rebab Clinics of N Amer 200415575-605Secrets to Stabilization Part 1
Static Stability
Motor Control
Pacinian Ruffini
Extreme Motion
Compressive Strength
Extreme Motion
Tensile Strength
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
8Secrets to Stabilization Part 1
Static Stability
Ligaments of the Shoulder Girdle
bull Sternoclavicular (SC)ndash Anterior Posterior
ndash Costoclavicular
bull Acromio-clavicular (AC)ndash Coracoacromial
ndash Coracoclavicular (conoid trapzoid)
bull Superior Transverse Ligament
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
9
httpuploadwikimediaorgwik
ipediacommons33bGray326
pngSecrets to Stabilization Part 1
4
Ligaments of the Shoulder Girdle
Sternoclavicular
bull Interclavicular inferior displacement
(holds shoulder up)
bull Anteriorposterior antpost displacement
bull Costoclavicular excessive rotation and
mediallateral displacement
Retrieved on 81515 from httpclassconnections3amazonawscom535flashcards3547535pngsternoclavicular_j
14105C8D3116E509030png
restrains
restrains
restrains
Secrets to Stabilization Part 1
Mechanism of Injury SC ligament
Direct or Indirect force
Anterior dislocationbull 8 wks in sling
bull Elbowwrist ROM
8 wks ROM below 90deg(gradual reduce sling wear)
12 wks Full ROM and strengtheningGuan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Posterior dislocation
bull Posterior dislocation 6-8
wks figure of eight clavicle
strap and gentle
pendelums Avoid flex and
abduction above 90
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic
posterior sternoclavicular dislocations Journal of Shoulder and Elbow Surgery
20(1) 107-113
Secrets to Stabilization Part 1 11
Ligaments of the Shoulder Girdle
bull Acromio-clavicular
12
Retrieved on 81515 from
httpssyimgcomfzapires12nRAxT99C962Y7olZJXIcWw--
YXBwaWQ9c3JjaGRkO2g9NjEyO3E9OTU7dz02MjU-
httpclassconnections3amazonawscom184flashcards1904184jpg
11353982940540jpg
bull Acromoclavicular antpost
translation provides horizontal stabilization
bull Coracoacromial antpost translation
bull Coracoclavicular vertical
displacement
restrains
restrains
restrains
Secrets to Stabilization Part 1
5
Mechanism of Injury AC ligament
Fall directly on shoulder
Types I amp IIbull 1 to 3 wks wear sling
(discharge as pain subsides)
bull ROM and strengthening
Type III (conservative)
bull 3 to 4 wks wear sling
bull Progress ROM amp strength
Types IV V (Reconstruction
Procedures)
bull 6-8 wks Gunslinger Shoulder Orthosis
bull AROM elbow wrist and hand
bull 7 to 10 days PROM to 90deg flexion supine
bull AROM 6 to 8 wks
bull Strengthening at 12 wks if no pain with
arom
bull 12 to 16 wks gradual return to pre-
injury activity levelJohansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries indications
for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82Secrets to Stabilization Part 1 13
Glenohumeral
Ligaments
14
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
bull Coracohumeral ligament (CHL)
bull Superior glenohumeral ligament (SGHL)
bull Middle glenohumeral ligament (MGHL)
bull Inferior glenohumeral ligament (IGHL)
bull Posterior band glenohumeral ligament
httpuploadwikimediaorg
wikiped
Iacommons33bGray326
png
15Secrets to Stabilization Part 1
6
Ligaments of the Glenohumeral
JointCoracohumeral
bull Coracohumeral ligament (CHL)
Connects coracoid process to greater and lesser
tuberosities of the humerus
httpuploadwikimediaorgwikipediacommons33bGray326png
16Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
(SGHL MGHL IGHL)bull Superior glenohumeral ligament
(SGHL)
Connects anterosuperior edge of the glenoid to the lesser tubercle of the humerus
bull Middle glenohumeral ligament (MGHL)
Connects supra-glenoid tubercle superior labrum or scapular neck to lesser tuberosity
bull Inferior glenohumeral ligament (IGHL)
Connects anteroinferior labrum and glenoid lip to lesser tuberosity
httpuploadwikimediaorgwikipediacom
mons33bGray326png
Axillary
Pouch
SGHL
MGHL
IGHL
17Secrets to Stabilization Part 1
Stabilizers Against Anterior Translations
bull Humerus adducted Subscapularis
bull Humerus abducted 45deg Subscapularis middle
anterior GH ligament and superior portion of
inferior anterior GH ligament
bull Humerus at 90deg abduction Inferior anterior GH
ligament
18Turkel et al 1981
Retrieved from httpwwwradsource
us_images0909_6jpgSecrets to Stabilization Part 1
7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
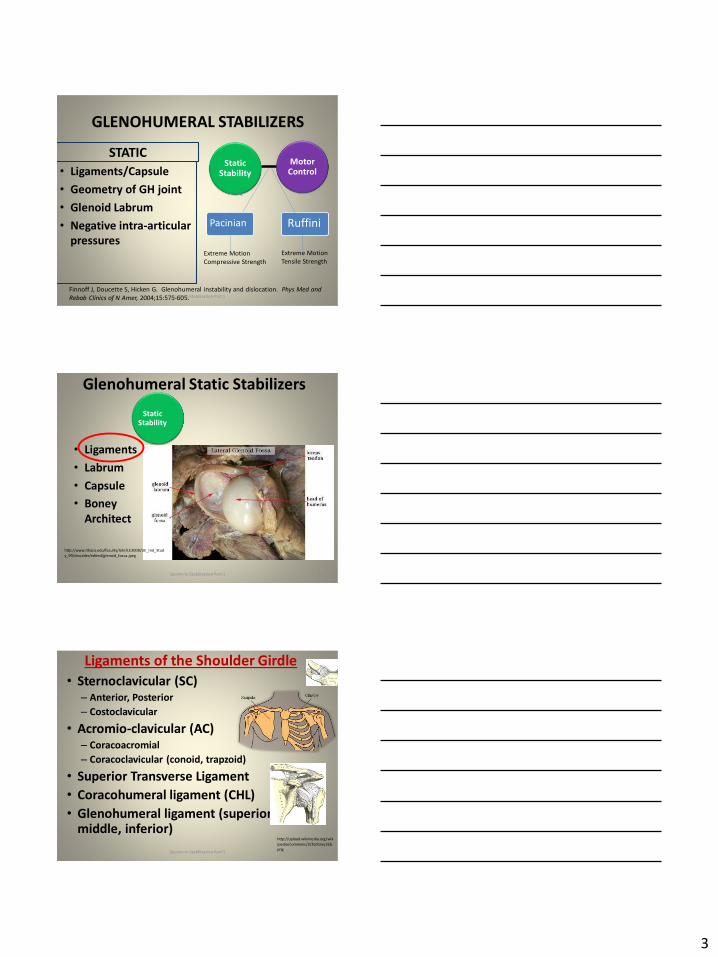
3
GLENOHUMERAL STABILIZERS
STATIC
bull LigamentsCapsule
bull Geometry of GH joint
bull Glenoid Labrum
bull Negative intra-articular
pressures
7
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and
Rebab Clinics of N Amer 200415575-605Secrets to Stabilization Part 1
Static Stability
Motor Control
Pacinian Ruffini
Extreme Motion
Compressive Strength
Extreme Motion
Tensile Strength
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
8Secrets to Stabilization Part 1
Static Stability
Ligaments of the Shoulder Girdle
bull Sternoclavicular (SC)ndash Anterior Posterior
ndash Costoclavicular
bull Acromio-clavicular (AC)ndash Coracoacromial
ndash Coracoclavicular (conoid trapzoid)
bull Superior Transverse Ligament
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
9
httpuploadwikimediaorgwik
ipediacommons33bGray326
pngSecrets to Stabilization Part 1
4
Ligaments of the Shoulder Girdle
Sternoclavicular
bull Interclavicular inferior displacement
(holds shoulder up)
bull Anteriorposterior antpost displacement
bull Costoclavicular excessive rotation and
mediallateral displacement
Retrieved on 81515 from httpclassconnections3amazonawscom535flashcards3547535pngsternoclavicular_j
14105C8D3116E509030png
restrains
restrains
restrains
Secrets to Stabilization Part 1
Mechanism of Injury SC ligament
Direct or Indirect force
Anterior dislocationbull 8 wks in sling
bull Elbowwrist ROM
8 wks ROM below 90deg(gradual reduce sling wear)
12 wks Full ROM and strengtheningGuan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Posterior dislocation
bull Posterior dislocation 6-8
wks figure of eight clavicle
strap and gentle
pendelums Avoid flex and
abduction above 90
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic
posterior sternoclavicular dislocations Journal of Shoulder and Elbow Surgery
20(1) 107-113
Secrets to Stabilization Part 1 11
Ligaments of the Shoulder Girdle
bull Acromio-clavicular
12
Retrieved on 81515 from
httpssyimgcomfzapires12nRAxT99C962Y7olZJXIcWw--
YXBwaWQ9c3JjaGRkO2g9NjEyO3E9OTU7dz02MjU-
httpclassconnections3amazonawscom184flashcards1904184jpg
11353982940540jpg
bull Acromoclavicular antpost
translation provides horizontal stabilization
bull Coracoacromial antpost translation
bull Coracoclavicular vertical
displacement
restrains
restrains
restrains
Secrets to Stabilization Part 1
5
Mechanism of Injury AC ligament
Fall directly on shoulder
Types I amp IIbull 1 to 3 wks wear sling
(discharge as pain subsides)
bull ROM and strengthening
Type III (conservative)
bull 3 to 4 wks wear sling
bull Progress ROM amp strength
Types IV V (Reconstruction
Procedures)
bull 6-8 wks Gunslinger Shoulder Orthosis
bull AROM elbow wrist and hand
bull 7 to 10 days PROM to 90deg flexion supine
bull AROM 6 to 8 wks
bull Strengthening at 12 wks if no pain with
arom
bull 12 to 16 wks gradual return to pre-
injury activity levelJohansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries indications
for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82Secrets to Stabilization Part 1 13
Glenohumeral
Ligaments
14
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
bull Coracohumeral ligament (CHL)
bull Superior glenohumeral ligament (SGHL)
bull Middle glenohumeral ligament (MGHL)
bull Inferior glenohumeral ligament (IGHL)
bull Posterior band glenohumeral ligament
httpuploadwikimediaorg
wikiped
Iacommons33bGray326
png
15Secrets to Stabilization Part 1
6
Ligaments of the Glenohumeral
JointCoracohumeral
bull Coracohumeral ligament (CHL)
Connects coracoid process to greater and lesser
tuberosities of the humerus
httpuploadwikimediaorgwikipediacommons33bGray326png
16Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
(SGHL MGHL IGHL)bull Superior glenohumeral ligament
(SGHL)
Connects anterosuperior edge of the glenoid to the lesser tubercle of the humerus
bull Middle glenohumeral ligament (MGHL)
Connects supra-glenoid tubercle superior labrum or scapular neck to lesser tuberosity
bull Inferior glenohumeral ligament (IGHL)
Connects anteroinferior labrum and glenoid lip to lesser tuberosity
httpuploadwikimediaorgwikipediacom
mons33bGray326png
Axillary
Pouch
SGHL
MGHL
IGHL
17Secrets to Stabilization Part 1
Stabilizers Against Anterior Translations
bull Humerus adducted Subscapularis
bull Humerus abducted 45deg Subscapularis middle
anterior GH ligament and superior portion of
inferior anterior GH ligament
bull Humerus at 90deg abduction Inferior anterior GH
ligament
18Turkel et al 1981
Retrieved from httpwwwradsource
us_images0909_6jpgSecrets to Stabilization Part 1
7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
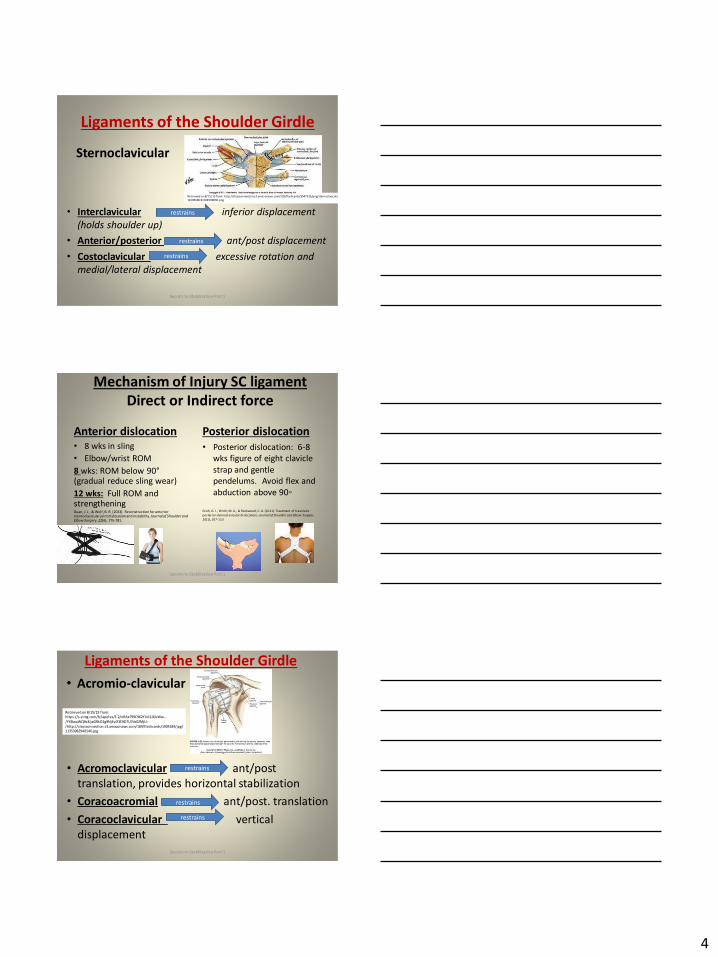
4
Ligaments of the Shoulder Girdle
Sternoclavicular
bull Interclavicular inferior displacement
(holds shoulder up)
bull Anteriorposterior antpost displacement
bull Costoclavicular excessive rotation and
mediallateral displacement
Retrieved on 81515 from httpclassconnections3amazonawscom535flashcards3547535pngsternoclavicular_j
14105C8D3116E509030png
restrains
restrains
restrains
Secrets to Stabilization Part 1
Mechanism of Injury SC ligament
Direct or Indirect force
Anterior dislocationbull 8 wks in sling
bull Elbowwrist ROM
8 wks ROM below 90deg(gradual reduce sling wear)
12 wks Full ROM and strengtheningGuan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Posterior dislocation
bull Posterior dislocation 6-8
wks figure of eight clavicle
strap and gentle
pendelums Avoid flex and
abduction above 90
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic
posterior sternoclavicular dislocations Journal of Shoulder and Elbow Surgery
20(1) 107-113
Secrets to Stabilization Part 1 11
Ligaments of the Shoulder Girdle
bull Acromio-clavicular
12
Retrieved on 81515 from
httpssyimgcomfzapires12nRAxT99C962Y7olZJXIcWw--
YXBwaWQ9c3JjaGRkO2g9NjEyO3E9OTU7dz02MjU-
httpclassconnections3amazonawscom184flashcards1904184jpg
11353982940540jpg
bull Acromoclavicular antpost
translation provides horizontal stabilization
bull Coracoacromial antpost translation
bull Coracoclavicular vertical
displacement
restrains
restrains
restrains
Secrets to Stabilization Part 1
5
Mechanism of Injury AC ligament
Fall directly on shoulder
Types I amp IIbull 1 to 3 wks wear sling
(discharge as pain subsides)
bull ROM and strengthening
Type III (conservative)
bull 3 to 4 wks wear sling
bull Progress ROM amp strength
Types IV V (Reconstruction
Procedures)
bull 6-8 wks Gunslinger Shoulder Orthosis
bull AROM elbow wrist and hand
bull 7 to 10 days PROM to 90deg flexion supine
bull AROM 6 to 8 wks
bull Strengthening at 12 wks if no pain with
arom
bull 12 to 16 wks gradual return to pre-
injury activity levelJohansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries indications
for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82Secrets to Stabilization Part 1 13
Glenohumeral
Ligaments
14
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
bull Coracohumeral ligament (CHL)
bull Superior glenohumeral ligament (SGHL)
bull Middle glenohumeral ligament (MGHL)
bull Inferior glenohumeral ligament (IGHL)
bull Posterior band glenohumeral ligament
httpuploadwikimediaorg
wikiped
Iacommons33bGray326
png
15Secrets to Stabilization Part 1
6
Ligaments of the Glenohumeral
JointCoracohumeral
bull Coracohumeral ligament (CHL)
Connects coracoid process to greater and lesser
tuberosities of the humerus
httpuploadwikimediaorgwikipediacommons33bGray326png
16Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
(SGHL MGHL IGHL)bull Superior glenohumeral ligament
(SGHL)
Connects anterosuperior edge of the glenoid to the lesser tubercle of the humerus
bull Middle glenohumeral ligament (MGHL)
Connects supra-glenoid tubercle superior labrum or scapular neck to lesser tuberosity
bull Inferior glenohumeral ligament (IGHL)
Connects anteroinferior labrum and glenoid lip to lesser tuberosity
httpuploadwikimediaorgwikipediacom
mons33bGray326png
Axillary
Pouch
SGHL
MGHL
IGHL
17Secrets to Stabilization Part 1
Stabilizers Against Anterior Translations
bull Humerus adducted Subscapularis
bull Humerus abducted 45deg Subscapularis middle
anterior GH ligament and superior portion of
inferior anterior GH ligament
bull Humerus at 90deg abduction Inferior anterior GH
ligament
18Turkel et al 1981
Retrieved from httpwwwradsource
us_images0909_6jpgSecrets to Stabilization Part 1
7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
5
Mechanism of Injury AC ligament
Fall directly on shoulder
Types I amp IIbull 1 to 3 wks wear sling
(discharge as pain subsides)
bull ROM and strengthening
Type III (conservative)
bull 3 to 4 wks wear sling
bull Progress ROM amp strength
Types IV V (Reconstruction
Procedures)
bull 6-8 wks Gunslinger Shoulder Orthosis
bull AROM elbow wrist and hand
bull 7 to 10 days PROM to 90deg flexion supine
bull AROM 6 to 8 wks
bull Strengthening at 12 wks if no pain with
arom
bull 12 to 16 wks gradual return to pre-
injury activity levelJohansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries indications
for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82Secrets to Stabilization Part 1 13
Glenohumeral
Ligaments
14
bull Coracohumeral ligament (CHL)
bull Glenohumeral ligament (superior middle inferior)
Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
bull Coracohumeral ligament (CHL)
bull Superior glenohumeral ligament (SGHL)
bull Middle glenohumeral ligament (MGHL)
bull Inferior glenohumeral ligament (IGHL)
bull Posterior band glenohumeral ligament
httpuploadwikimediaorg
wikiped
Iacommons33bGray326
png
15Secrets to Stabilization Part 1
6
Ligaments of the Glenohumeral
JointCoracohumeral
bull Coracohumeral ligament (CHL)
Connects coracoid process to greater and lesser
tuberosities of the humerus
httpuploadwikimediaorgwikipediacommons33bGray326png
16Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
(SGHL MGHL IGHL)bull Superior glenohumeral ligament
(SGHL)
Connects anterosuperior edge of the glenoid to the lesser tubercle of the humerus
bull Middle glenohumeral ligament (MGHL)
Connects supra-glenoid tubercle superior labrum or scapular neck to lesser tuberosity
bull Inferior glenohumeral ligament (IGHL)
Connects anteroinferior labrum and glenoid lip to lesser tuberosity
httpuploadwikimediaorgwikipediacom
mons33bGray326png
Axillary
Pouch
SGHL
MGHL
IGHL
17Secrets to Stabilization Part 1
Stabilizers Against Anterior Translations
bull Humerus adducted Subscapularis
bull Humerus abducted 45deg Subscapularis middle
anterior GH ligament and superior portion of
inferior anterior GH ligament
bull Humerus at 90deg abduction Inferior anterior GH
ligament
18Turkel et al 1981
Retrieved from httpwwwradsource
us_images0909_6jpgSecrets to Stabilization Part 1
7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
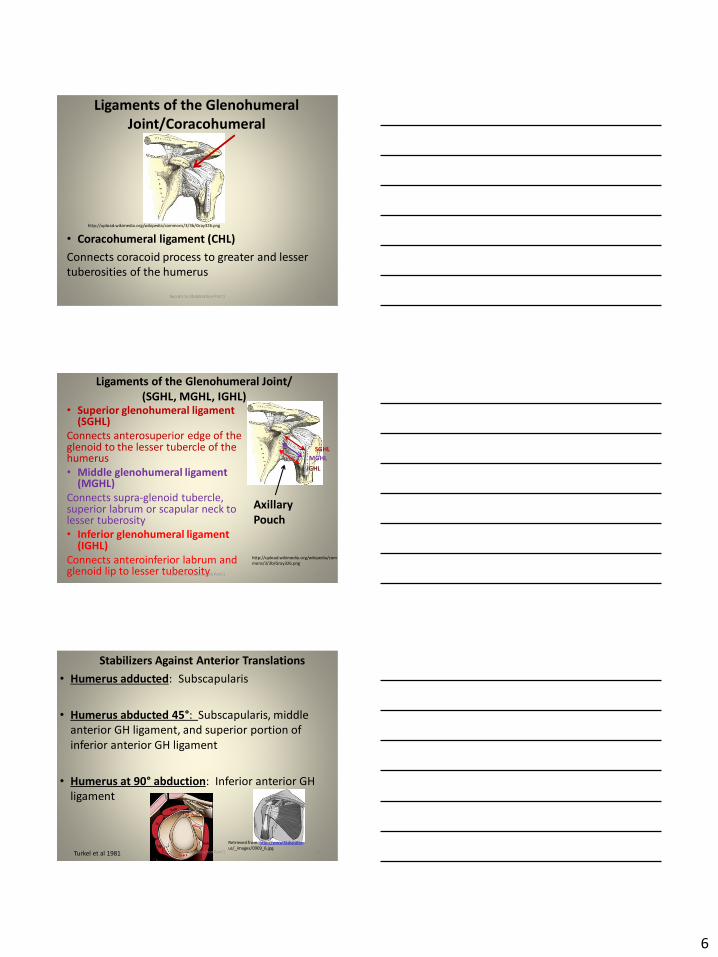
6
Ligaments of the Glenohumeral
JointCoracohumeral
bull Coracohumeral ligament (CHL)
Connects coracoid process to greater and lesser
tuberosities of the humerus
httpuploadwikimediaorgwikipediacommons33bGray326png
16Secrets to Stabilization Part 1
Ligaments of the Glenohumeral Joint
(SGHL MGHL IGHL)bull Superior glenohumeral ligament
(SGHL)
Connects anterosuperior edge of the glenoid to the lesser tubercle of the humerus
bull Middle glenohumeral ligament (MGHL)
Connects supra-glenoid tubercle superior labrum or scapular neck to lesser tuberosity
bull Inferior glenohumeral ligament (IGHL)
Connects anteroinferior labrum and glenoid lip to lesser tuberosity
httpuploadwikimediaorgwikipediacom
mons33bGray326png
Axillary
Pouch
SGHL
MGHL
IGHL
17Secrets to Stabilization Part 1
Stabilizers Against Anterior Translations
bull Humerus adducted Subscapularis
bull Humerus abducted 45deg Subscapularis middle
anterior GH ligament and superior portion of
inferior anterior GH ligament
bull Humerus at 90deg abduction Inferior anterior GH
ligament
18Turkel et al 1981
Retrieved from httpwwwradsource
us_images0909_6jpgSecrets to Stabilization Part 1
7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1

7
0 to 30 degrees
45 to 60 degrees
90 degrees
Antero-medial force
Boney Architect
Secrets to Stabilization Part 1 19
Secrets to Stabilization Part 1 20
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
21Secrets to Stabilization Part 1
Static Stability
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
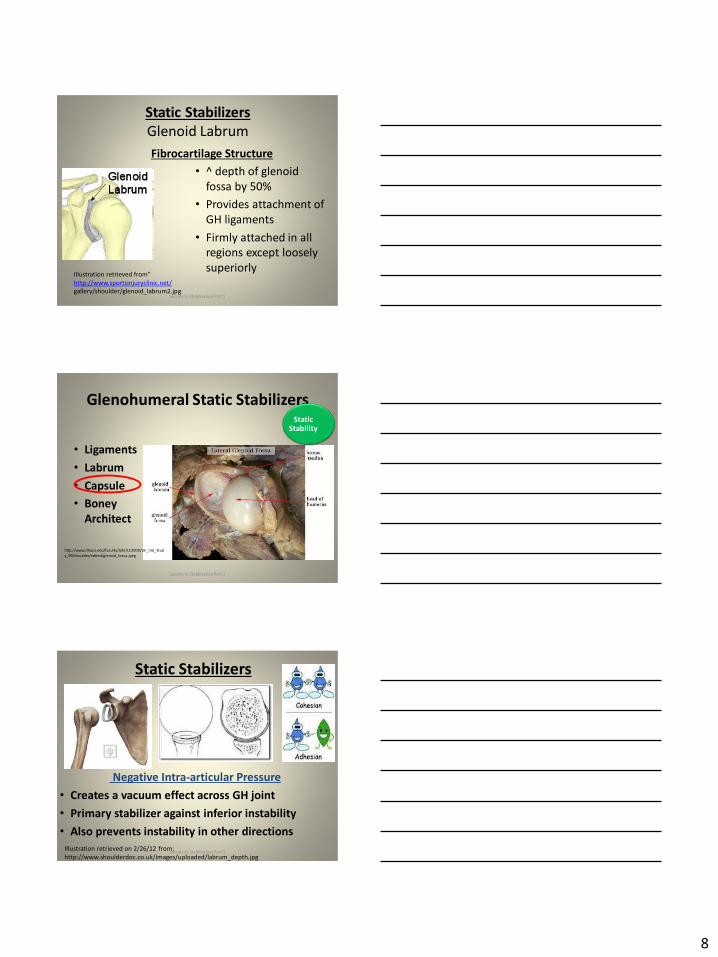
8
Static Stabilizers
Glenoid Labrum
Fibrocartilage Structure
bull ^ depth of glenoid
fossa by 50
bull Provides attachment of
GH ligaments
bull Firmly attached in all
regions except loosely
superiorly
22
Illustration retrieved fromrdquohttpwwwsportsinjuryclinicnet
galleryshoulderglenoid_labrum2jpgSecrets to Stabilization Part 1
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
23Secrets to Stabilization Part 1
Static Stability
Static Stabilizers
Negative Intra-articular Pressure
bull Creates a vacuum effect across GH joint
bull Primary stabilizer against inferior instability
bull Also prevents instability in other directions
24Illustration retrieved on 22612 from
httpwwwshoulderdoccoukimagesuploadedlabrum_depthjpgSecrets to Stabilization Part 1
9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1

9
Glenohumeral Static Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
httpwwwithacaedufacultylahrLE2000UE_Ind_Stud
y_99shouldereditedglenoid_fossajpeg
25Secrets to Stabilization Part 1
Static Stability
26
Glenohumeral Static
Stabilizers
bull Ligaments
bull Labrum
bull Capsule
bull Boney
Architect
Il lustration retrieved on 41110 from
httpwwwacta-orthogrv57t3U1jpg
Secrets to Stabilization Part 1
bull Humeral
head to
shaft angle
130deg to
150deg
bull Retroverted
30deg
Defining Shoulder Instability
bull Shoulder instability is the inability to maintain
the humeral head in the glenoid fossa
Dislocation the humeral head is forced
completely out of its normal position in the
glenoid fossa
Subluxation the humeral head slips partially out
of glenoid fossa causing symptoms
Laxity partial lost of glenohumeral articulation
without symptoms
Secrets to Stabilization Part 1 27
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
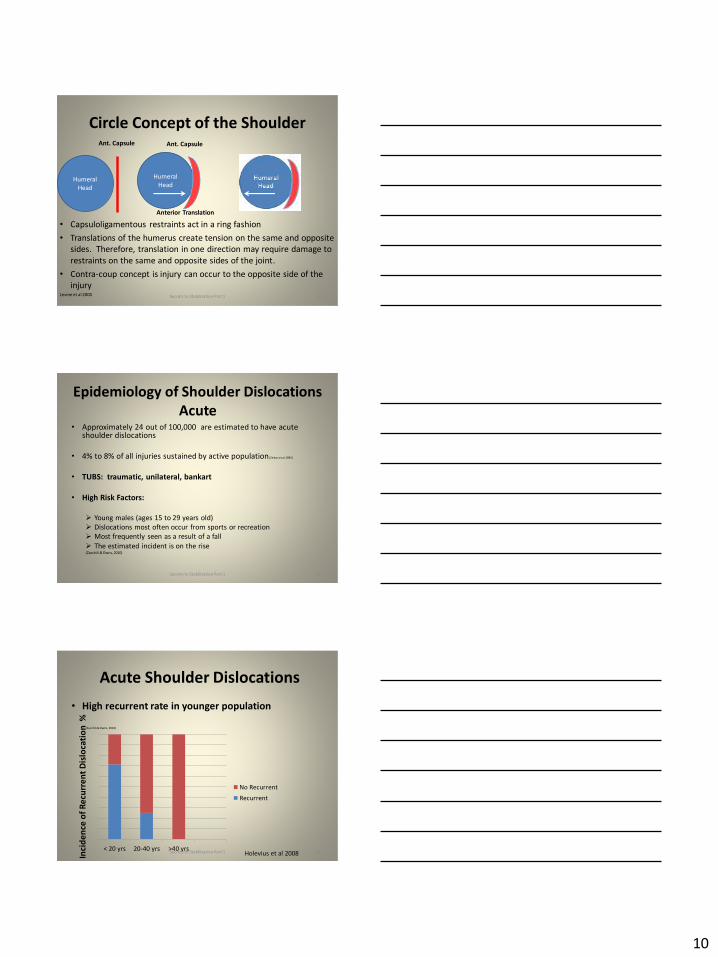
10
Circle Concept of the Shoulder
bull Capsuloligamentous restraints act in a ring fashion
bull Translations of the humerus create tension on the same and opposite
sides Therefore translation in one direction may require damage to
restraints on the same and opposite sides of the joint
bull Contra-coup concept is injury can occur to the opposite side of the
injuryLevine et al 2000
Humeral
Head
Ant Capsule
Humeral
Head
Anterior Translation
Ant Capsule
Secrets to Stabilization Part 1 28
Epidemiology of Shoulder Dislocations
Acutebull Approximately 24 out of 100000 are estimated to have acute
shoulder dislocations
bull 4 to 8 of all injuries sustained by active population (Zebas et al 1995)
bull TUBS traumatic unilateral bankart
bull High Risk Factors
Young males (ages 15 to 29 years old)
Dislocations most often occur from sports or recreation
Most frequently seen as a result of a fall
The estimated incident is on the rise(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 29
Acute Shoulder Dislocations
bull High recurrent rate in younger population
(Zacchili amp Owns 2010)
lt 20 yrs 20-40 yrs gt40 yrs
No Recurrent
Recurrent
Inci
de
nce
of
Re
curr
en
t D
islo
cati
on
Holevius et al 2008Secrets to Stabilization Part 1 30
11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1

11
Sensorimotor Insufficiencies
bull Recurrent anterior instability sensorimotor
insufficiency increase with dominant side
involvement (Edouard Gasq Calmes amp Degache 2014)
Secrets to Stabilization Part 1 31
Etiology of Traumatic Shoulder
Dislocationsbull Unidirectional from traumatic event (anterior is the most
common)
Most commonly caused by a fall on an outstretched hand or a sudden forceful motion in the abder position
Bankhart
Superior Labrum Anterior Posterior (SLAP)
Most common direction of instability is anteriorinferior from falling in 9090 position (ABDER)
(Zacchili amp Owns 2010)
Secrets to Stabilization Part 1 32
Special Tests Anterior Instability
Apprehension amp Relocation
Sensitivity 81 Specificity 98 (Farber et al 2006)
Apprehension Test Relocation Test
Secrets to Stabilization Part 1 33
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
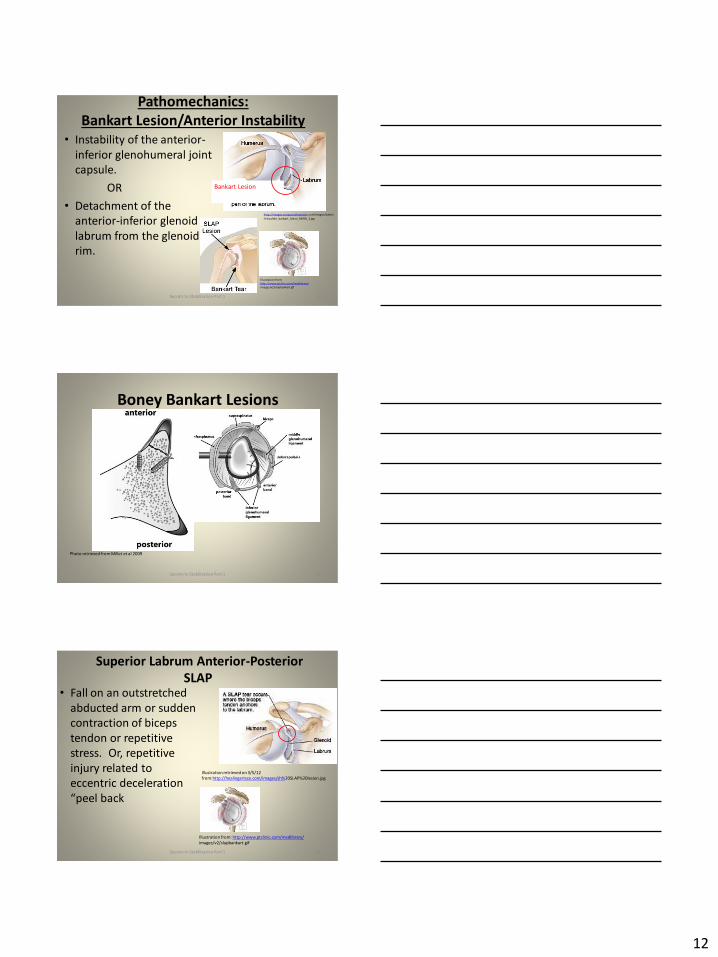
12
Pathomechanics
Bankart LesionAnterior Instability
bull Instability of the anterior-
inferior glenohumeral joint
capsule
OR
bull Detachment of the
anterior-inferior glenoid
labrum from the glenoid
rim
34
httpimagesconquestchroniclescomimagesadmin
shoulder_bankart_lesion_85905_2jpg
Bankart Lesion
I l lustration from
httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
Boney Bankart Lesions
Photo retrieved from Millet et al 2009
Secrets to Stabilization Part 1 35
Superior Labrum Anterior-Posterior
SLAPbull Fall on an outstretched
abducted arm or sudden
contraction of biceps
tendon or repetitive
stress Or repetitive
injury related to
eccentric deceleration
ldquopeel back
36
Illustration retrieved on 3512
fromhttphealingartscecomimagessh20SLAP20lesionjpg
Illustration from httpwwwptcliniccommedlibrary
imagesv2slapbankartgif
Secrets to Stabilization Part 1
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
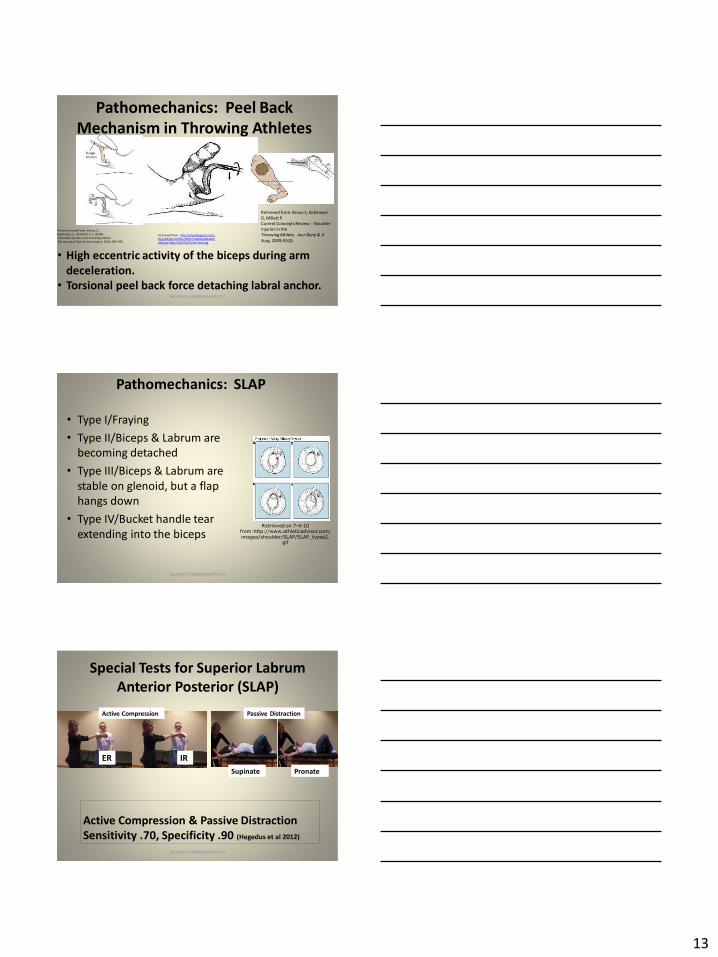
13
Pathomechanics Peel Back
Mechanism in Throwing Athletes
37
Retrieved from http2bpblogspotcom_
BsgqbRhgCnQSRtejHI0PvIAAAAAAAAANA
vMjopqYdgrss400SLAP-peel-backjpg
Retrieved from Braun S Kokmeyer
D Millett P
Current Concepts Review Shoulder
Injuries in the
Throwing Athlete Jour Bone amp Jt
Surg 200991(4)
bull High eccentric activity of the biceps during arm
deceleration
bull Torsional peel back force detaching labral anchor
Photo retrieved from Braun S
Kokmeyer D amp Mi llett P J (2009)
Shoulder injuries in the throwing athlete
The Journal of Bone amp Joint Surgery 91(4) 966-978
Secrets to Stabilization Part 1
Pathomechanics SLAP
bull Type IFraying
bull Type IIBiceps amp Labrum are
becoming detached
bull Type IIIBiceps amp Labrum are
stable on glenoid but a flap
hangs down
bull Type IVBucket handle tear
extending into the bicepsRetrieved on 7-4-10
fromhttpwwwathleticadvisorcomimagesshoulderSLAPSLAP_types2
gif
Secrets to Stabilization Part 1 38
Special Tests for Superior Labrum
Anterior Posterior (SLAP)
Active Compression amp Passive Distraction
Sensitivity 70 Specificity 90 (Hegedus et al 2012)
ER
Supinate Pronate
Passive Distraction
IR
Active Compression
Secrets to Stabilization Part 1 39
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
14
Secrets to Stabilization Part 1 40
Secrets to Stabilization Part 1 41
Etiology Atraumatic Shoulder
Multidirectional Instabilities
bull Instability from mirco-trauma from repetitive motions in one direction or multi-directional
Voluntary Individual subluxes or dislocates volitionally
AMBRI atraumatic multidirectional bilateral rehabilitation inferior shift
Involuntary Subluxes or dislocates involuntary
Secrets to Stabilization Part 1 42
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
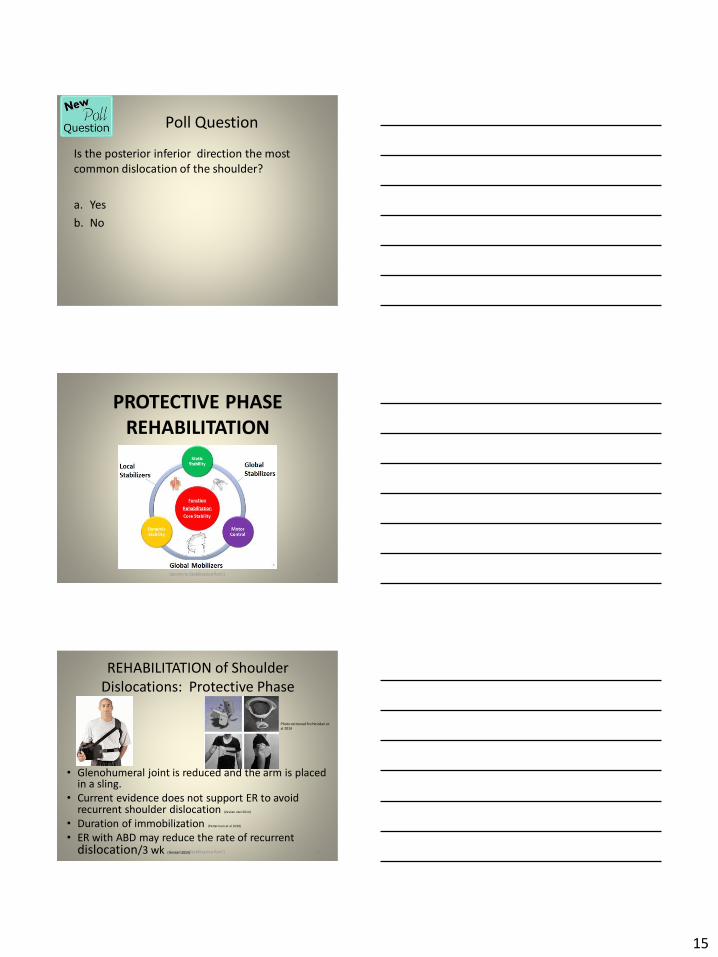
15
Poll Question
Is the posterior inferior direction the most
common dislocation of the shoulder
a Yes
b No
43
PROTECTIVE PHASE
REHABILITATION
Secrets to Stabilization Part 1 44
REHABILITATION of Shoulder
Dislocations Protective Phase
bull Glenohumeral joint is reduced and the arm is placed in a sling
bull Current evidence does not support ER to avoid recurrent shoulder dislocation (Vavken etal 2014)
bull Duration of immobilization (Patternson et al 2010)
bull ER with ABD may reduce the rate of recurrent dislocation3 wk (Heidari 2014)
Photo retrieved fro Heirdari et
al 2014
Secrets to Stabilization Part 1 45
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
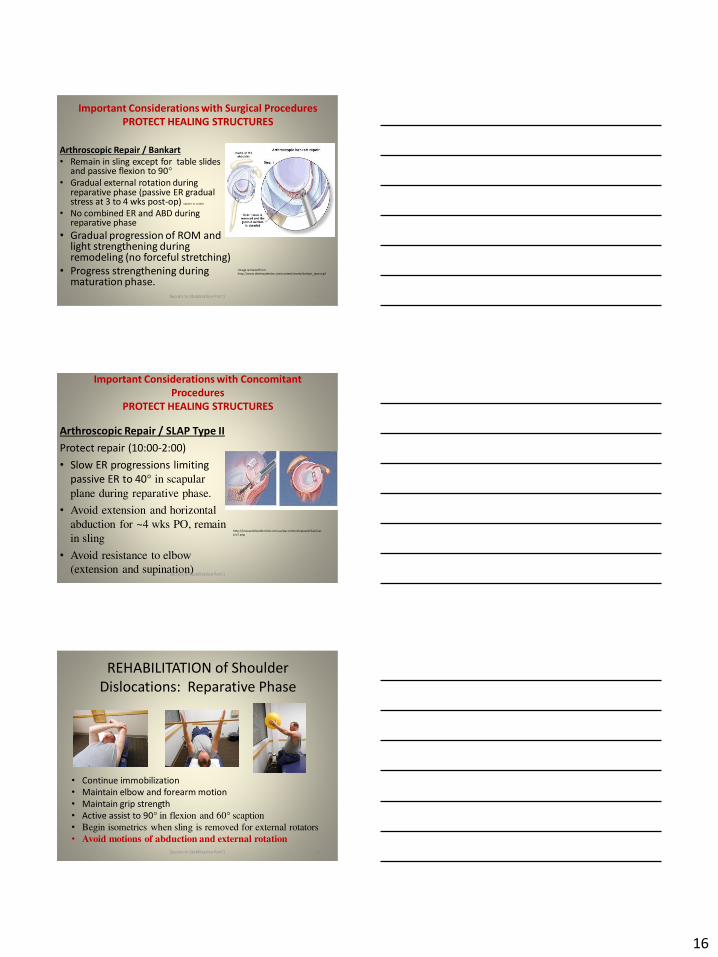
16
Important Considerations with Surgical Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair Bankart
bull Remain in sling except for table slides and passive flexion to 90deg
bull Gradual external rotation during reparative phase (passive ER gradual stress at 3 to 4 wks post-op) Sperber et al 2001
bull No combined ER and ABD during reparative phase
bull Gradual progression of ROM and light strengthening during remodeling (no forceful stretching)
bull Progress strengthening during maturation phase
Image retrieved from
httpwwwtheshoulderdoccomcontentassetsbankart_layoutgif
Secrets to Stabilization Part 1 46
Important Considerations with Concomitant
Procedures
PROTECT HEALING STRUCTURES
Arthroscopic Repair SLAP Type II
Protect repair (1000-200)
bull Slow ER progressions limiting
passive ER to 40deg in scapular
plane during reparative phase
bull Avoid extension and horizontal
abduction for ~4 wks PO remain
in sling
bull Avoid resistance to elbow
(extension and supination)
httpkneeandshouldercliniccomauwp-contentuploadsSlapTear-
pic2png
Secrets to Stabilization Part 1 47
REHABILITATION of Shoulder
Dislocations Reparative Phase
bull Continue immobilization
bull Maintain elbow and forearm motion
bull Maintain grip strength
bull Active assist to 90deg in flexion and 60deg scaption
bull Begin isometrics when sling is removed for external rotators
bull Avoid motions of abduction and external rotation
Secrets to Stabilization Part 1 48
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
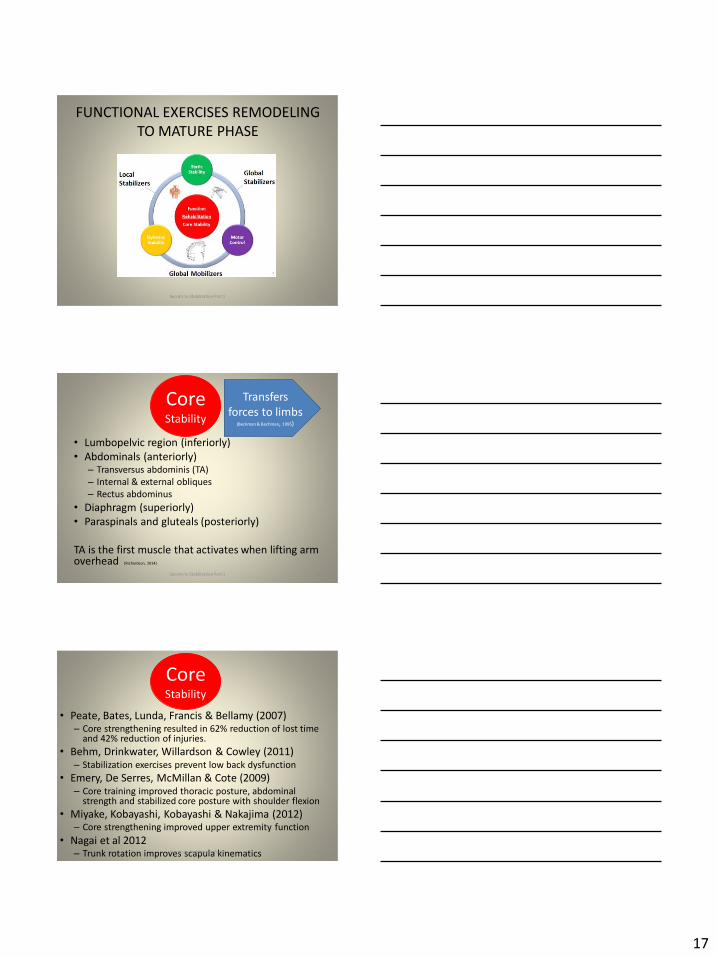
17
FUNCTIONAL EXERCISES REMODELING
TO MATURE PHASE
Secrets to Stabilization Part 1 49
bull Lumbopelvic region (inferiorly)
bull Abdominals (anteriorly)ndash Transversus abdominis (TA)
ndash Internal amp external obliques
ndash Rectus abdominus
bull Diaphragm (superiorly)
bull Paraspinals and gluteals (posteriorly)
TA is the first muscle that activates when lifting arm overhead (Richardson 2014)
Secrets to Stabilization Part 1 50
Core Stability
Transfers
forces to limbs(Beckman amp Bachman 1995)
bull Peate Bates Lunda Francis amp Bellamy (2007)ndash Core strengthening resulted in 62 reduction of lost time
and 42 reduction of injuries
bull Behm Drinkwater Willardson amp Cowley (2011)ndash Stabilization exercises prevent low back dysfunction
bull Emery De Serres McMillan amp Cote (2009)ndash Core training improved thoracic posture abdominal
strength and stabilized core posture with shoulder flexion
bull Miyake Kobayashi Kobayashi amp Nakajima (2012)ndash Core strengthening improved upper extremity function
bull Nagai et al 2012ndash Trunk rotation improves scapula kinematicsSecrets to Stabilization Part 1 51
Core Stability
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
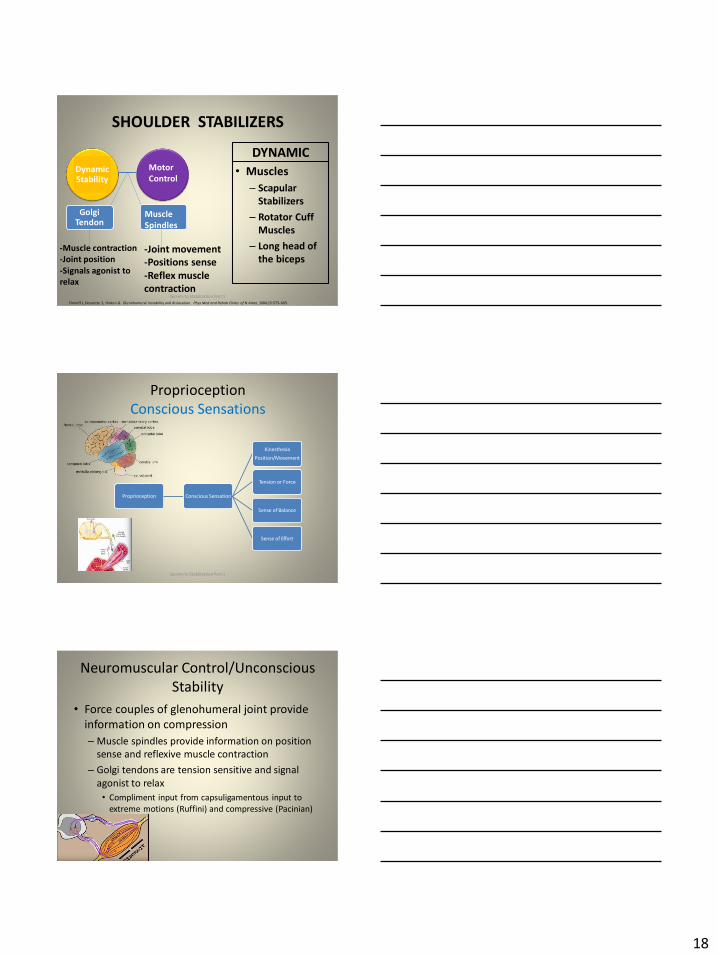
18
SHOULDER STABILIZERS
DYNAMIC
bull Muscles
ndash Scapular
Stabilizers
ndash Rotator Cuff
Muscles
ndash Long head of
the biceps
52
Finnoff J Doucette S Hicken G Glenohumeral instability and dislocation Phys Med and Rebab Clinics of N Amer 200415575-605
Secrets to Stabilization Part 1
DynamicStability
Motor
Control
Golgi Tendon
-Muscle contraction
-Joint position
-Signals agonist to
relax
Muscle
Spindles
-Joint movement
-Positions sense
-Reflex muscle
contraction
Proprioception
Conscious Sensations
Proprioception Conscious Sensation
Kinesthesia
PositionMovement
Tension or Force
Sense of Balance
Sense of Effort
Secrets to Stabilization Part 1 53
Neuromuscular ControlUnconscious
Stability
bull Force couples of glenohumeral joint provide
information on compression
ndash Muscle spindles provide information on position
sense and reflexive muscle contraction
ndash Golgi tendons are tension sensitive and signal
agonist to relax
bull Compliment input from capsuligamentous input to
extreme motions (Ruffini) and compressive (Pacinian)
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
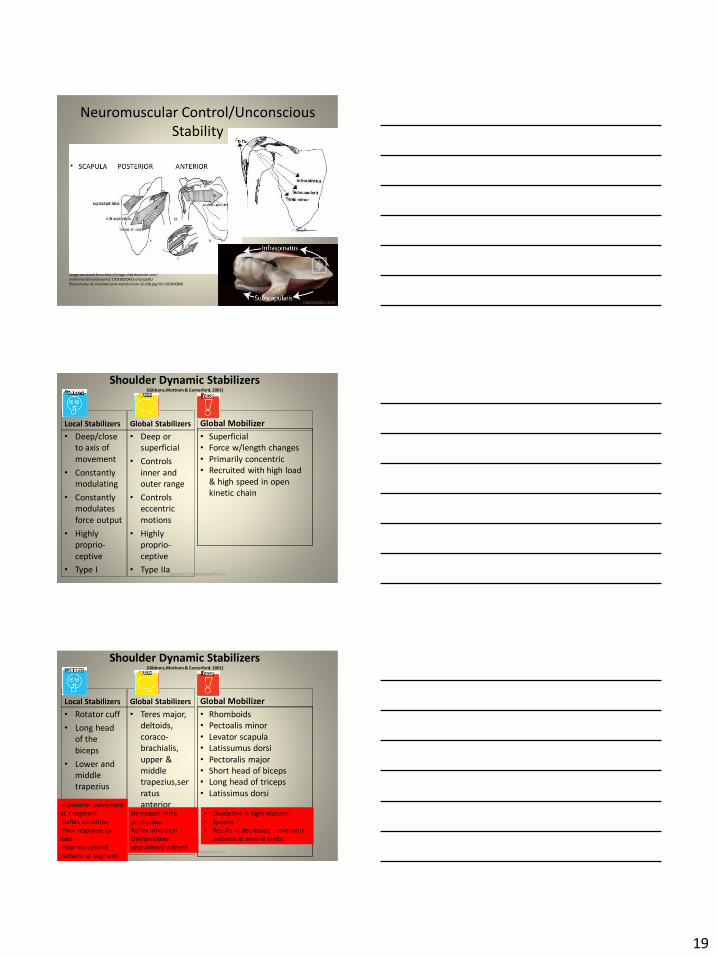
19
Neuromuscular ControlUnconscious
Stability
Image retrieved fromhttpimageslidesharecdncom
anatomyofshoulderjoint2-130318210432-phpapp01
95anatomy-of-shoulder-joint-vamshi-kiran-32-638jpgcb=1363640800
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Deepclose
to axis of
movement
bull Constantly
modulating
bull Constantly
modulates
force output
bull Highly
proprio-
ceptive
bull Type I
Global Stabilizers
bull Deep or
superficial
bull Controls
inner and
outer range
bull Controls
eccentric
motions
bull Highly
proprio-
ceptive
bull Type IIaSecrets to Stabilization Part 1 56
Global Mobilizer
bull Superficial
bull Force wlength changes
bull Primarily concentric
bull Recruited with high load
amp high speed in open
kinetic chain
Shoulder Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Rotator cuff
bull Long head
of the
biceps
bull Lower and
middle
trapezius
Global Stabilizers
bull Teres major
deltoids
coraco-
brachialis
upper amp
middle
trapeziusser
ratus
anterior
Secrets to Stabilization Part 1 57
Global Mobilizer
bull Rhomboids
bull Pectoalis minor
bull Levator scapula
bull Latissumus dorsi
bull Pectoralis major
bull Short head of biceps
bull Long head of triceps
bull Latissimus dorsi
-Abnormal movement
at 1 segment
-Reflex inhibition
-Poor response to
load
-Poor movement
patterns at segment
Decreased force
production
Reflex inhibition
Dysfunctional
recruitment pattern
bull Overactive amp tight muscles
bull Spasms
bull Results in decreased movement
patterns at several joints
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
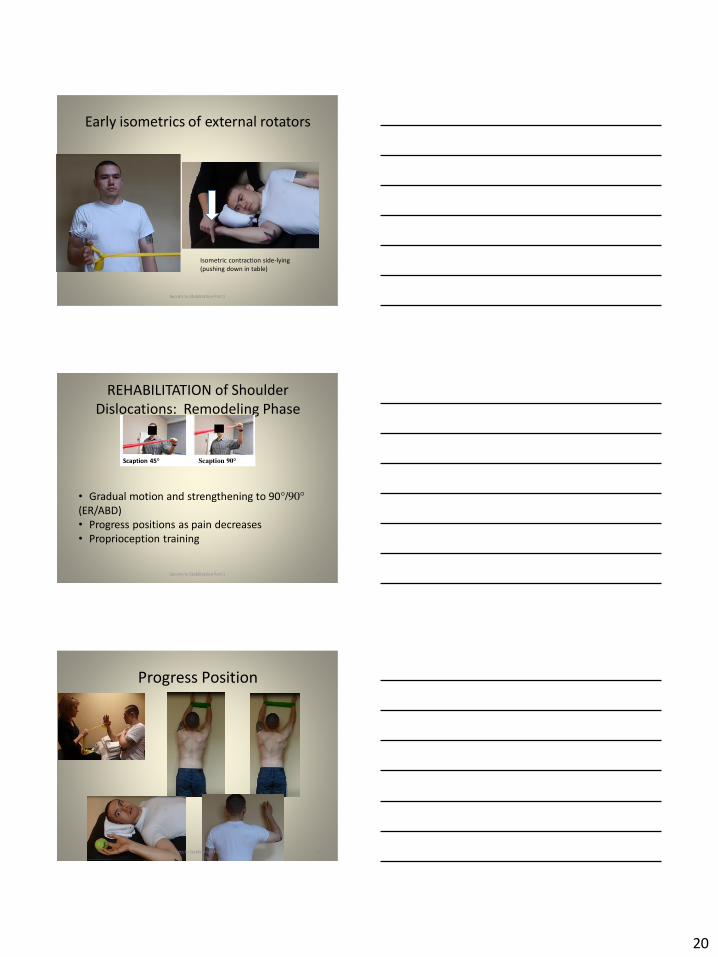
20
Early isometrics of external rotators
Secrets to Stabilization Part 1 58
Isometric contraction side-lying
(pushing down in table)
REHABILITATION of Shoulder
Dislocations Remodeling Phase
bull Gradual motion and strengthening to 90deg90deg(ERABD)
bull Progress positions as pain decreases
bull Proprioception training
Scaption 45deg Scaption 90deg
Secrets to Stabilization Part 1 59
Progress Position
Secrets to Stabilization Part 1 60
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
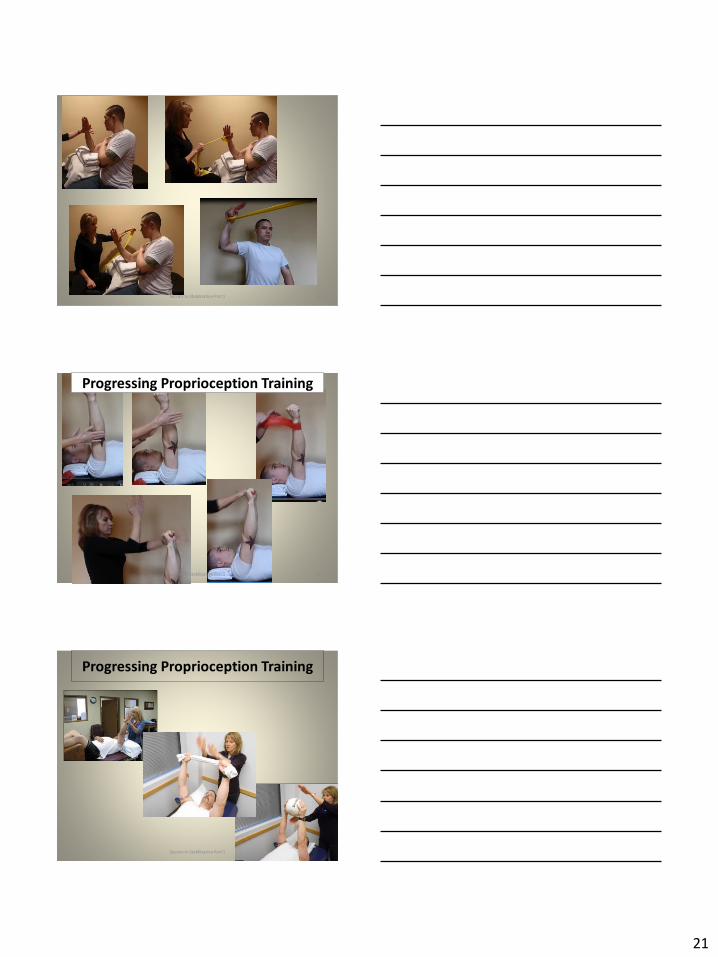
21
Secrets to Stabilization Part 1 61
Secrets to Stabilization Part 1 62
Progressing Proprioception Training
Progressing Proprioception Training
Secrets to Stabilization Part 1 63
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
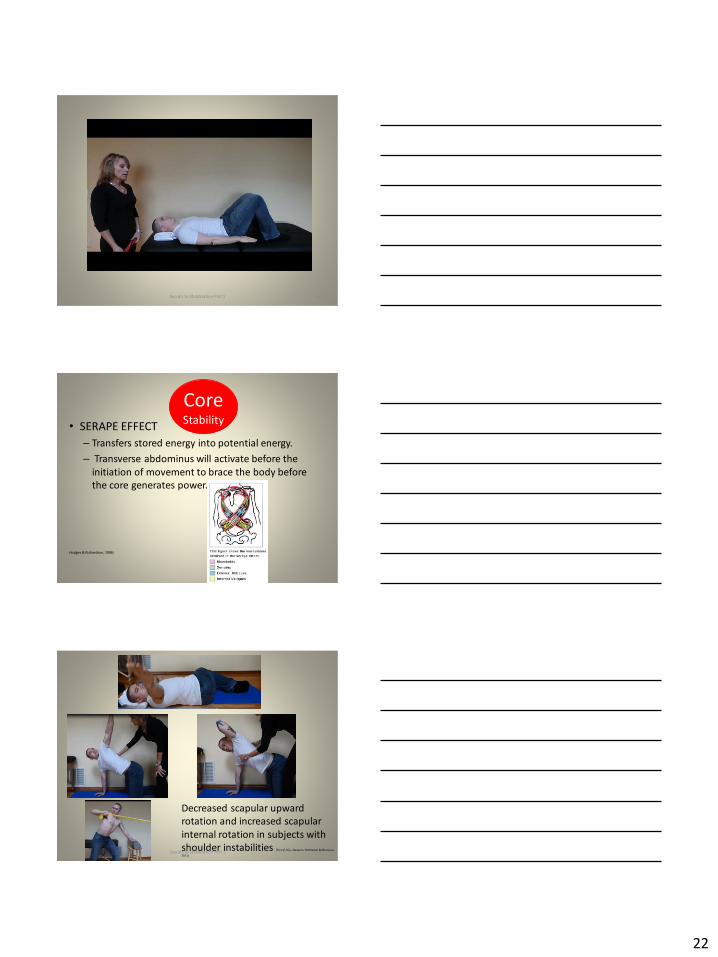
22
Secrets to Stabilization Part 1 64
bull SERAPE EFFECT
ndash Transfers stored energy into potential energy
ndash Transverse abdominus will activate before the
initiation of movement to brace the body before
the core generates power
Hodges amp Richardson 1996)
Core Stability
Secrets to Stabilization Part 1 66
Decreased scapular upward
rotation and increased scapular
internal rotation in subjects with
shoulder instabilities (Struyf Ni js Baeyens Mottaram amp Meeusen
2011)
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
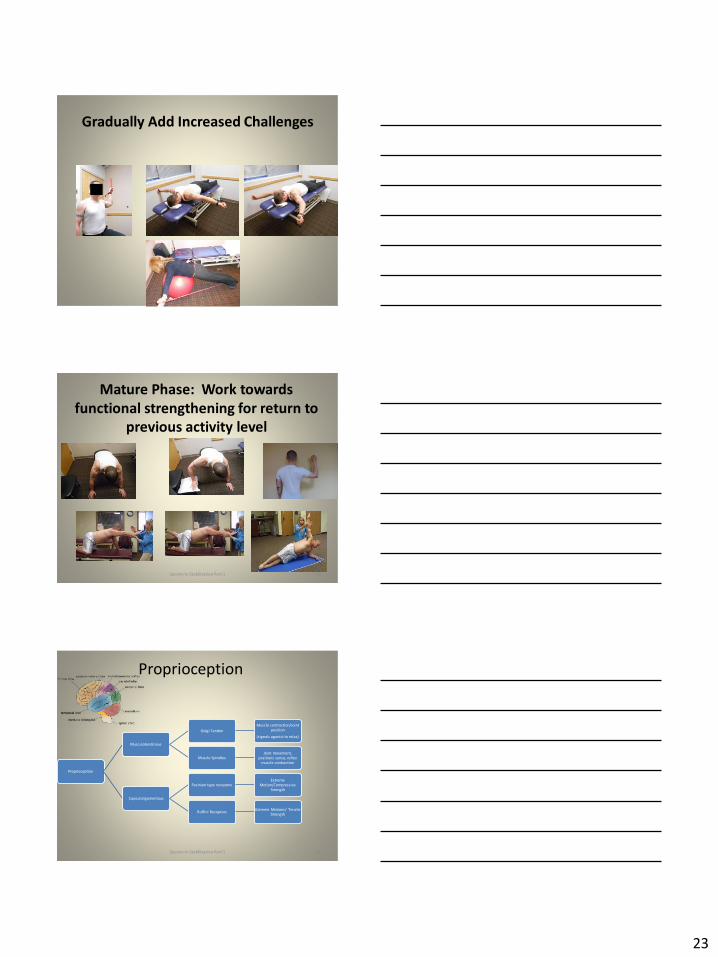
23
Gradually Add Increased Challenges
Secrets to Stabilization Part 1 67
Mature Phase Work towards
functional strengthening for return to
previous activity level
Secrets to Stabilization Part 1 68
Proprioception
Proprioception
Musculotendinous
Golgi Tendon
Muscle contractionJoint
position
(signals agonist to relax)
Muscle SpindlesJoint movement
positions sense reflex
muscle contraction
Capsuloligamentous
Pacinian type receptorsExtreme
MotionCompressive
Strength
Ruffini ReceptorsExtreme Motions Tensile
Strength
Secrets to Stabilization Part 1 69
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
24
Secrets to Stabilization Part 1 70
Poll Question
1 Is limiting passive external rotation
appropriate after a SLAP or Bankart surgery
a Yes
b No
71
ELBOW INSTABILITIES
Secrets to Stabilization Part 1 72
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
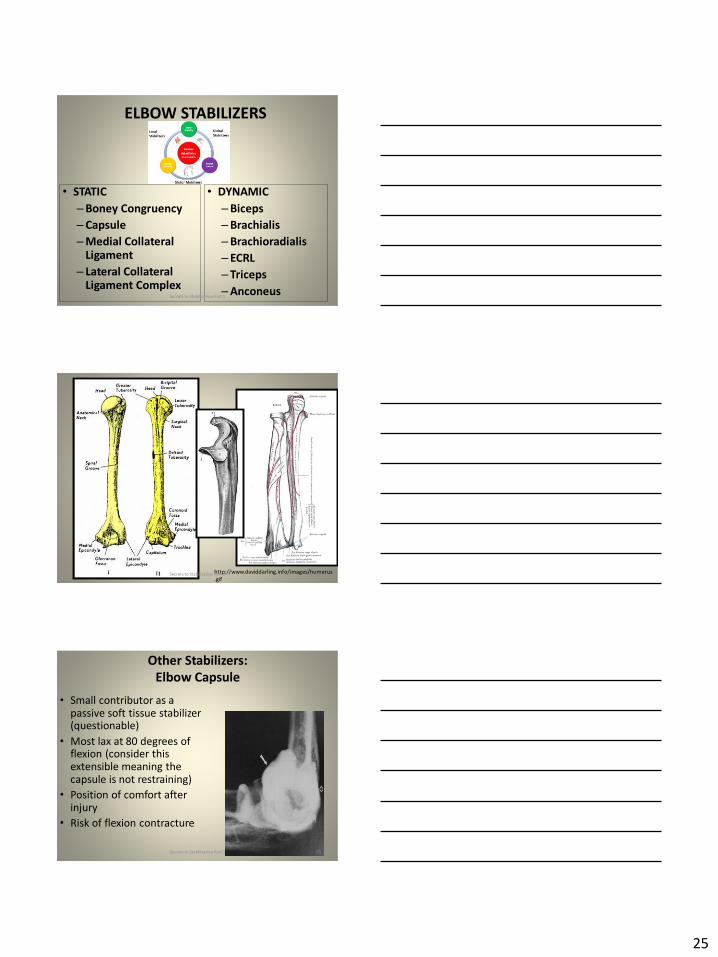
25
ELBOW STABILIZERS
bull STATIC
ndashBoney Congruency
ndashCapsule
ndashMedial Collateral Ligament
ndash Lateral Collateral Ligament Complex
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashBrachioradialis
ndashECRL
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 73
httpwwwdaviddarlinginfoimageshumerus
gifSecrets to Stabilization Part 1 74
Other Stabilizers
Elbow Capsule
bull Small contributor as a passive soft tissue stabilizer (questionable)
bull Most lax at 80 degrees of flexion (consider this extensible meaning the capsule is not restraining)
bull Position of comfort after injury
bull Risk of flexion contracture
Secrets to Stabilization Part 1 75
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
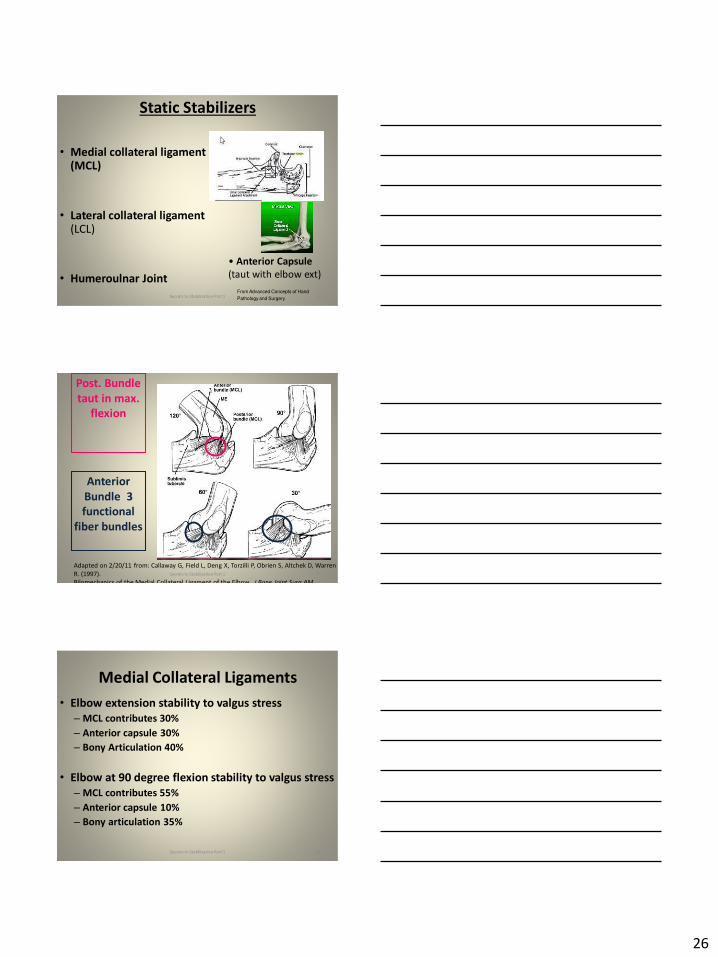
26
Static Stabilizers
bull Medial collateral ligament (MCL)
bull Lateral collateral ligament(LCL)
bull Humeroulnar JointFrom Advanced Concepts of Hand
Pathology and Surgery
Subliime tubercle
of proximal ulna
bull Anterior Capsule
(taut with elbow ext)
Secrets to Stabilization Part 1 76
Adapted on 22011 from Callaway G Field L Deng X Torzilli P Obrien S Altchek D Warren
R (1997)
Bilomechanics of the Medial Collateral Ligament of the Elbow J Bone Joint Surg AM
Post Bundle
taut in max
flexion
Anterior
Bundle 3
functional
fiber bundles
Secrets to Stabilization Part 1 77
Medial Collateral Ligaments
bull Elbow extension stability to valgus stress
ndash MCL contributes 30
ndash Anterior capsule 30
ndash Bony Articulation 40
bull Elbow at 90 degree flexion stability to valgus stress
ndash MCL contributes 55
ndash Anterior capsule 10
ndash Bony articulation 35
Secrets to Stabilization Part 1 78
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
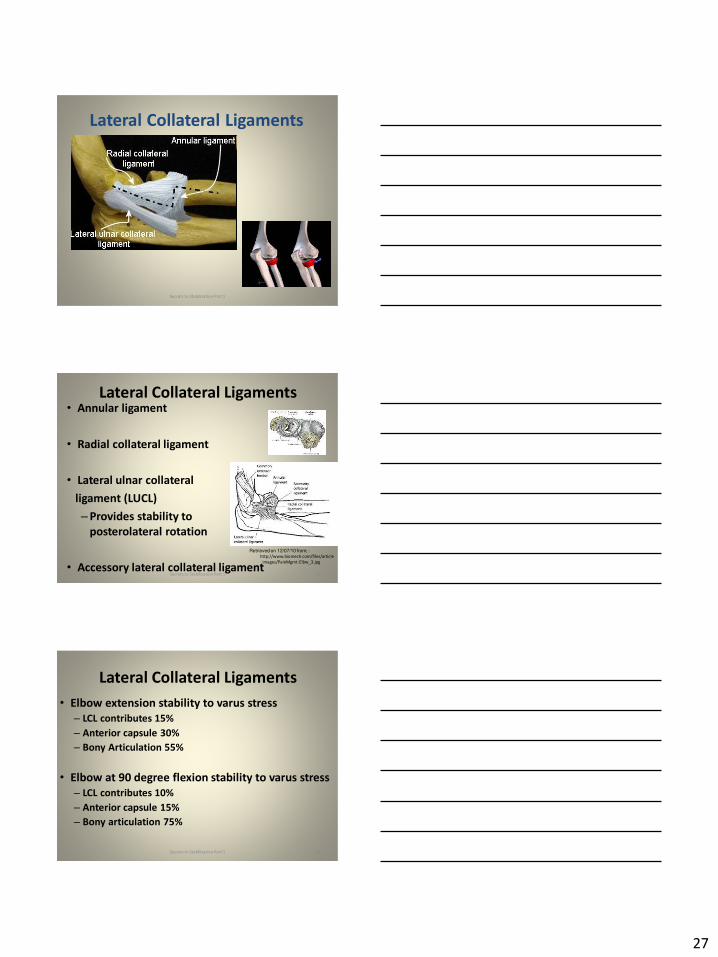
27
Lateral Collateral Ligaments
Secrets to Stabilization Part 1 79
Lateral Collateral Ligaments bull Annular ligament
bull Radial collateral ligament
bull Lateral ulnar collateral
ligament (LUCL)
ndashProvides stability to
posterolateral rotation
bull Accessory lateral collateral ligament
Retrieved on 120710 from
httpwwwbiomechcomfilesarticle
_imagesPainMgmt-Elbw_3jpg
Secrets to Stabilization Part 1 80
Lateral Collateral Ligaments
bull Elbow extension stability to varus stress
ndash LCL contributes 15
ndash Anterior capsule 30
ndash Bony Articulation 55
bull Elbow at 90 degree flexion stability to varus stress
ndash LCL contributes 10
ndash Anterior capsule 15
ndash Bony articulation 75
Secrets to Stabilization Part 1 81
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
28
ELBOW STABILIZERS
bull DYNAMIC
ndashBiceps
ndashBrachialis
ndashPronators
ndash Supinatos
ndashBrachioradialis
ndashWristdigit extensors amp flexors
ndashTriceps
ndashAnconeusSecrets to Stabilization Part 1 82
Elbow Dynamic Stabilizers(GibbonsMottram amp Comerford 2001)
Local Stabilizers
bull Anconeus(deep fibers)
bull Pronator
Quadratus(deep fibers)
bull Supinator(deep fibers)
Global Stabilizers
bull Brachialis
bull Brachioradialis
bull Triceps (medial amp
lateral heads)
bull Anconeous
(superficial fibers)
bull Supinator
(superficial fibers)
bull Pronator
Quadratus(superficial fibers)
bull ECU (ulnar head)
bull FCU (ulnar head)
bull APL
Secrets to Stabilization Part 1 83
Global Mobilizer
Biceps Brachii (long amp short heads)
Triceps Brachii (long head)
Wrist amp Digit Extensors
Pronator Teres
Wrist amp Digit Flexors
I Elbow Pathology Ligamentous
Lateral Collateral Ligament (LCL)
bull Ligamentous
ndash Lateral collateral ligament sprain
or tear is also associated with trauma
and often occurs with a fracture
ndashMechanism of injury
bull Fall on outstretched hand (FOOSH)
bull Forced twisting of the arm with varus
(lateral) forces
OrsquoDriscoll 1992Secrets to Stabilization Part 1 84
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
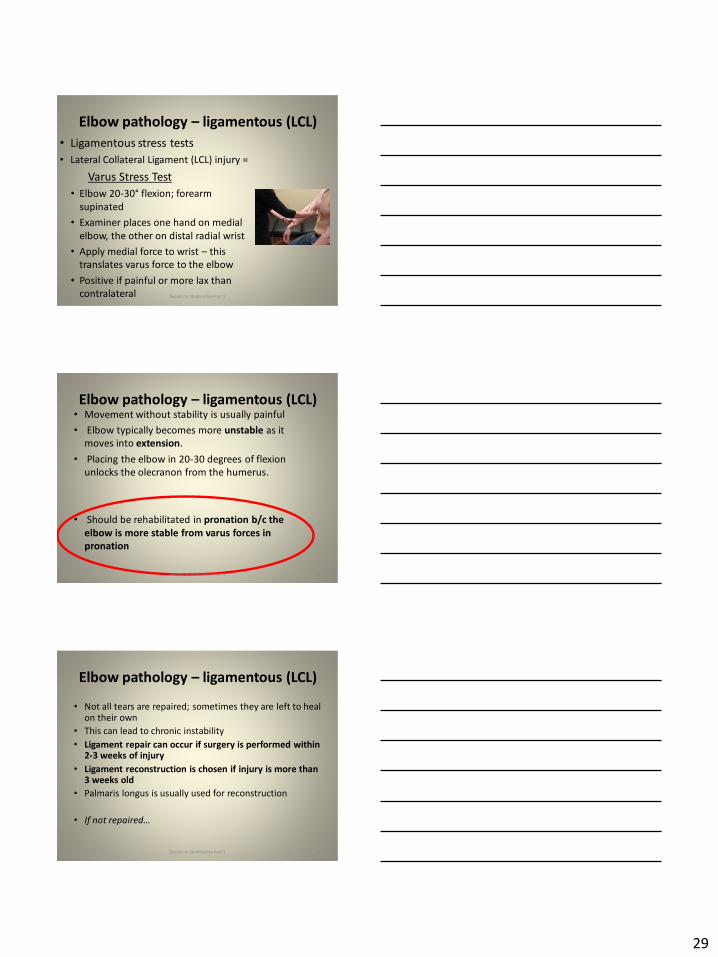
29
Elbow pathology ndash ligamentous (LCL)
bull Ligamentous stress tests
bull Lateral Collateral Ligament (LCL) injury =
Varus Stress Test
bull Elbow 20-30deg flexion forearm
supinated
bull Examiner places one hand on medial
elbow the other on distal radial wrist
bull Apply medial force to wrist ndash this
translates varus force to the elbow
bull Positive if painful or more lax than
contralateral Secrets to Stabilization Part 1 85
Elbow pathology ndash ligamentous (LCL)bull Movement without stability is usually painful
bull Elbow typically becomes more unstable as it
moves into extension
bull Placing the elbow in 20-30 degrees of flexion
unlocks the olecranon from the humerus
bull Should be rehabilitated in pronation bc the
elbow is more stable from varus forces in
pronation
Secrets to Stabilization Part 1 86
Elbow pathology ndash ligamentous (LCL)
bull Not all tears are repaired sometimes they are left to heal on their own
bull This can lead to chronic instability
bull Ligament repair can occur if surgery is performed within 2-3 weeks of injury
bull Ligament reconstruction is chosen if injury is more than 3 weeks old
bull Palmaris longus is usually used for reconstruction
bull If not repairedhellip
Secrets to Stabilization Part 1 87
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
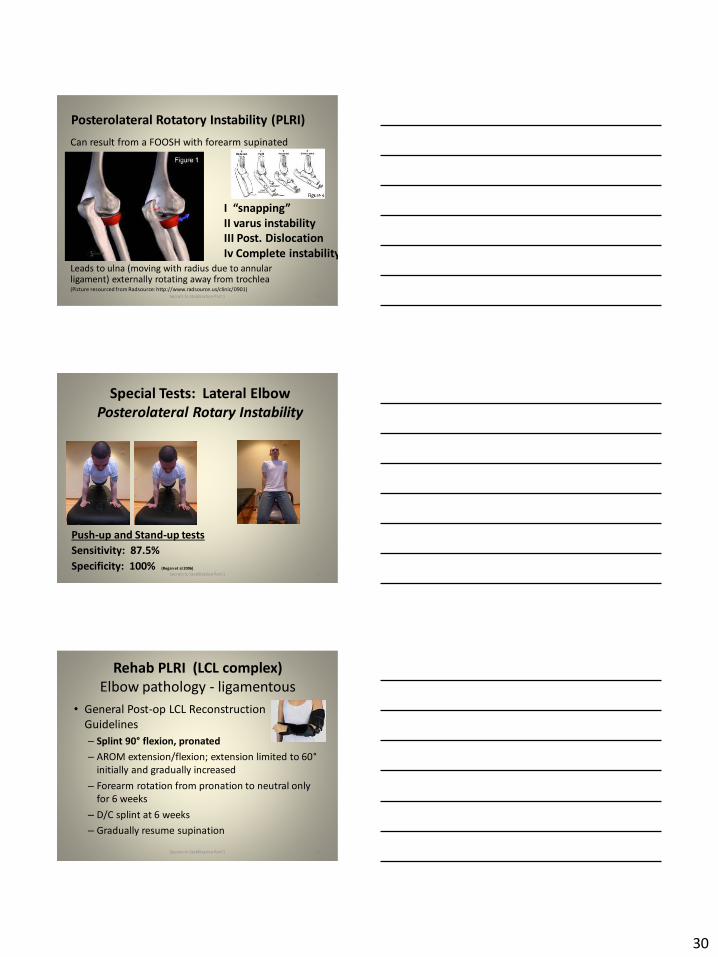
30
Posterolateral Rotatory Instability (PLRI)
Can result from a FOOSH with forearm supinated
Leads to ulna (moving with radius due to annular ligament) externally rotating away from trochlea(Picture resourced from Radsource httpwwwradsourceusclinic0901)
Secrets to Stabilization Part 1 88
I ldquosnappingrdquoII varus instability
III Post Dislocation
Iv Complete instability
Special Tests Lateral Elbow
Posterolateral Rotary Instability
Push-up and Stand-up tests
Sensitivity 875
Specificity 100 (Regan et al 2006)
Secrets to Stabilization Part 1 89
Rehab PLRI (LCL complex)
Elbow pathology - ligamentous
bull General Post-op LCL Reconstruction
Guidelines
ndash Splint 90deg flexion pronated
ndash AROM extensionflexion extension limited to 60deg
initially and gradually increased
ndash Forearm rotation from pronation to neutral only
for 6 weeks
ndash DC splint at 6 weeks
ndash Gradually resume supination
Secrets to Stabilization Part 1 90
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
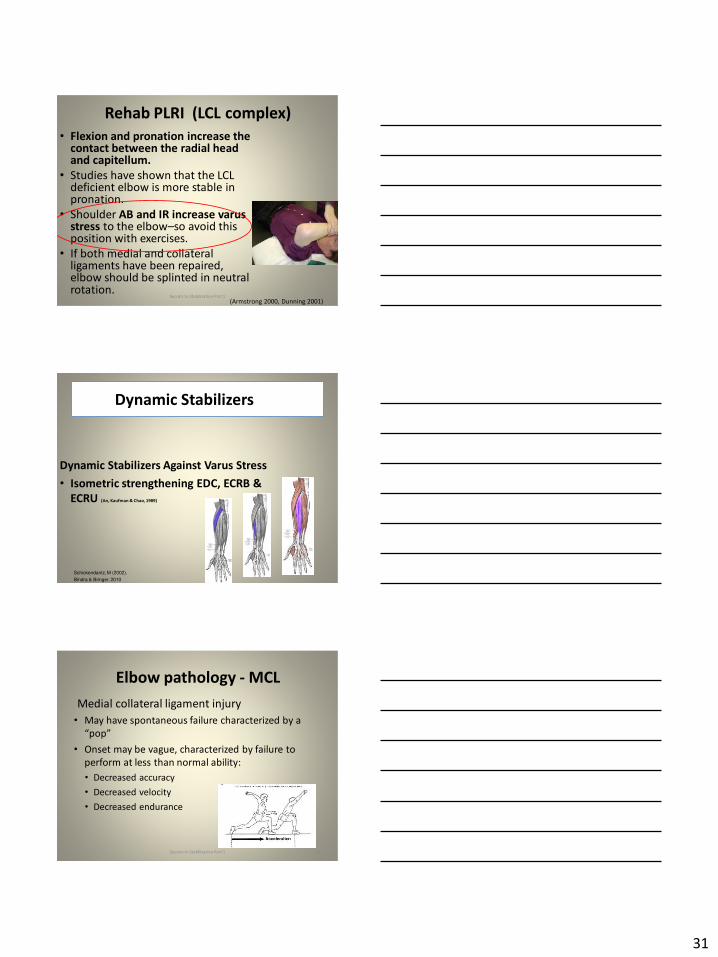
31
Rehab PLRI (LCL complex)
bull Flexion and pronation increase the contact between the radial head and capitellum
bull Studies have shown that the LCL deficient elbow is more stable in pronation
bull Shoulder AB and IR increase varus stress to the elbowndashso avoid this position with exercises
bull If both medial and collateral ligaments have been repaired elbow should be splinted in neutral rotation
(Armstrong 2000 Dunning 2001)Secrets to Stabilization Part 1 91
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Dynamic Stabilizers ent
Elbow pathology - MCL
Medial collateral ligament injury
bull May have spontaneous failure characterized by a
ldquopoprdquobull Onset may be vague characterized by failure to
perform at less than normal ability
bull Decreased accuracy
bull Decreased velocity
bull Decreased endurance
Secrets to Stabilization Part 1 93
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
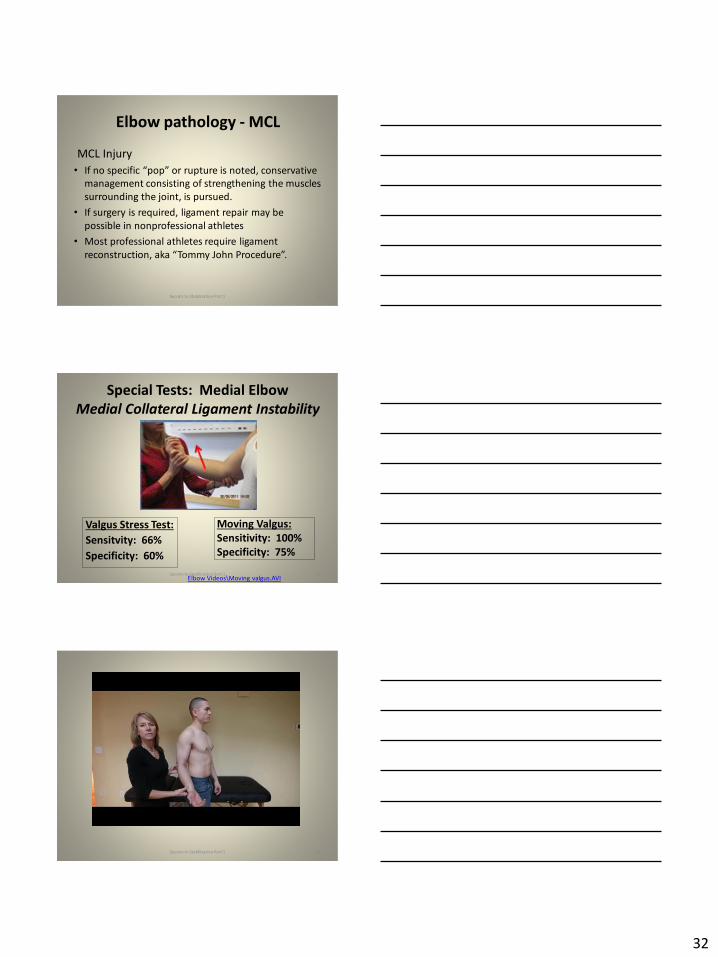
32
Elbow pathology - MCL
MCL Injury
bull If no specific ldquopoprdquo or rupture is noted conservative management consisting of strengthening the muscles
surrounding the joint is pursued
bull If surgery is required ligament repair may be
possible in nonprofessional athletes
bull Most professional athletes require ligament
reconstruction aka ldquoTommy John Procedurerdquo
Secrets to Stabilization Part 1 94
Special Tests Medial Elbow
Medial Collateral Ligament Instability
Moving Valgus
Sensitivity 100
Specificity 75
Valgus Stress Test
Sensitvity 66
Specificity 60
Elbow VideosMoving valgusAVISecrets to Stabilization Part 1 95
Secrets to Stabilization Part 1 96
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
33
Secrets to Stabilization Part 1 97
Elbow pathology - ligamentous
Conservative Management MCL Injury
bull Protect ndash no overhead activity
bull AROM - sagittal plane
bull Strengthening - core shoulder elbow and wrist
bull Throwerrsquos Ten Program for shoulder elbow
forearm and wrist
bull Evaluation of throwing technique
bull Advanced Throwerrsquos Ten Program
Secrets to Stabilization Part 1 98
Elbow pathology - ligamentous
bull Post-operative management of MCL injury
bull Splint in neutral rotation 90deg flexion
bull Active elbow extension and flexion with full extension limited initially
bull AROM digits and wrist ok to grip
bull Isometric strengthening of shoulder No external rotation of shoulder as it creates valgus stress at elbow
bull Splint DCrsquod at 6 weeksbull Progress through full ROM and into Throwerrsquos Ten
Secrets to Stabilization Part 1 99
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
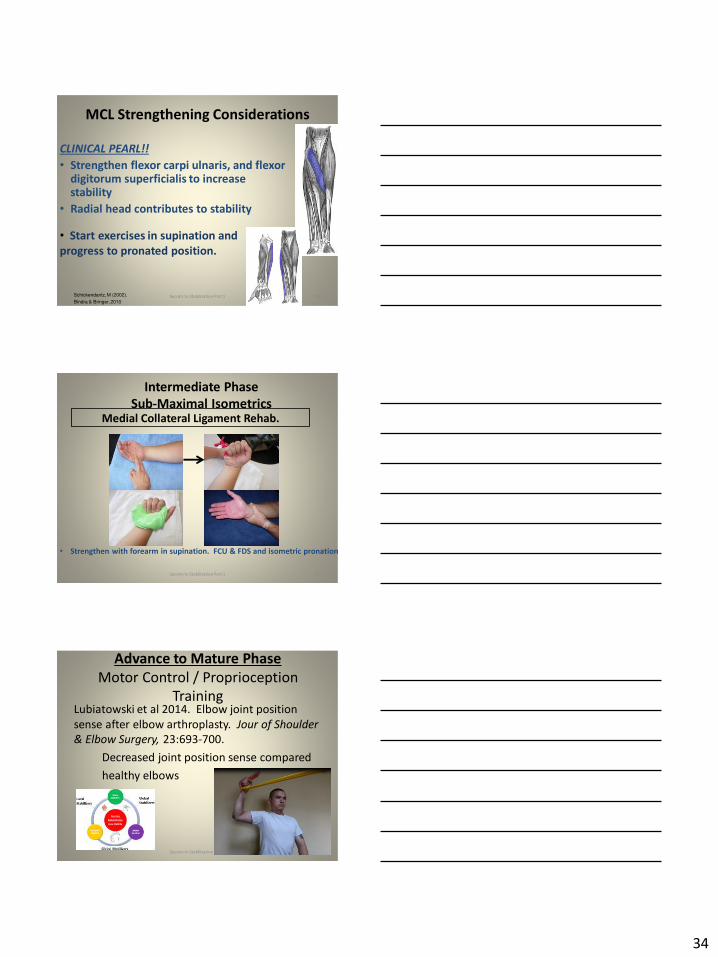
34
MCL Strengthening Considerations
CLINICAL PEARL
bull Strengthen flexor carpi ulnaris and flexor digitorum superficialis to increase stability
bull Radial head contributes to stability
Schickendantz M (2002)
Bindra amp Bringer 2010
bull Start exercises in supination and
progress to pronated position
Secrets to Stabilization Part 1 100
Intermediate Phase
Sub-Maximal IsometricsMedial Collateral Ligament Rehab
bull Strengthen with forearm in supination FCU amp FDS and isometric pronation
Secrets to Stabilization Part 1 101
Advance to Mature Phase
Motor Control Proprioception
TrainingLubiatowski et al 2014 Elbow joint position
sense after elbow arthroplasty Jour of Shoulder
amp Elbow Surgery 23693-700
Decreased joint position sense compared
healthy elbows
Secrets to Stabilization Part 1 102
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
35
Elbow Trauma
Dislocations amp
Fractures
Dislocation Classification bull Simple
ndash Small osseous fractures not affecting joint stability
ndashDescribed as posterior anterior medial lateral
bull Complex
ndashDescribed as posterior anterior medial lateral or divergent
bull Acute (less than 2 weeks)
bull Subacute (2 to 4 weeks)
bull Chronic (6 weeks ore more)
Sheps et al 2004
Medial Lateral DivergentRetrieved on 22211 fromhttpboneandspinecomwp-contentuploads200902lateral-dislocation-elbowgif
PosteriorNormalRetrieved on 22211 fromhttpimgmedscapecompiemedckbemergency_medicine756148-821994-823277-1671248jpg
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
36
Evidence for Early Motion in Simple
Posterior Dislocations
bull Loss of extension is the most frequent
complication
bull Ross et al protocol Immediate active motion
combined with modalities to reduce pain and
swelling and UE strengthening Results of
nearly full ROM within 5 degrees of extensionRoss et al (1999)
Sheps et al 2004
ELBOW TRAUMA
Secrets to Stabilization Part 1 107
Radial Head Fractures in Elbow
Trauma
bull Terrible Triadndash Posterior or posterolateral dislocation of ulnohumeral
joint with fractures of the radial head and coronoid process Avulsion of medial collateral ligament (MCL) and lateral collateral ligament (LCL)
ndash Coronoid process provides stabilitybull Buttress against posterior displacement of the ulna and
contributes to varus stability (Budoff 2012)
bull Essex Lopresti radial head fracture rupture of the interosseous membrane (IOM) resulting in forearm instability and proximal migration of the radius
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
37
Radial Head Fractures
Internal Fixation or Radial Head
Replacement
bull Fragmentation of less than 3 fragments have improved results with fixation (Ring amp Jupiter 2001)
bull Lateral collateral ligament protection may be required if ligament re-attached or involved reattached after surgery (pronation) at 2 days post-op allow prosup with elbow flexed at 90
Internal Fixationbull Phase I
ndash Early mobilization 3 to 5 days post-opPROM gentle
ndash Posterior elbow orthosis 90deg flexion with forearm
neutral
ndash Regain motion 1 to 3 wks post-op AAROM (flexext
prosup)
ndash CPM
bull Phase II (4 to 6 wks post-op)
ndash Regain full motion and gradual strengthening
bull Phase III (6 to 12 wks)
ndash Advance strengthening and closed chain exercises
ndash Joint mobilizations
ndash End range strengthening
Radial Head Replacementbull Phase I (Week 1 to 3 post-op)
ndash Early mobilization (orthosis CPM (forearm pronated or neutral) AROM wrist and hand during 1st week
ndash Hinged elbow orthosis worn at all times
ndash Advance elbow and forearm motion exercises Elbow AAROM with gravity assisted extension Position elbow at 90deg flexion during forearm exercises
ndash Consider edema glove for hand
bull Phase II (Week 3-6 post-op)
ndash Begin AAROM prosup PROM elbow stretching to tolerance initiate orthosis to increase flexext if needed advance to AROM forearm rotation and elbow motion
bull Phase III (Week 6-8 post-op)
ndash Discharge hinged orthosis begin isometrics continue
mobilization orthosis
bull Phase IV (Week 8-12 post-op)ndash Light resistance gradually upgrade strengthening
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
38
Distal Humerus Intra-articular
FracturesFixation Plating (post-op 1 week)
bull Edema control
bull Long arm orthosis alternating between elbow flexion daily and elbow extension nightly
bull Elbow shoulder forearm wrist hand AROM every 1 to 2 hours
Post-op 2 weeks
bull Initiate scar management
bull Progress ROM each week
bull Non-weight-bearing until fracture healed
bull Strengthening when fractured healed
CHALLENGE
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
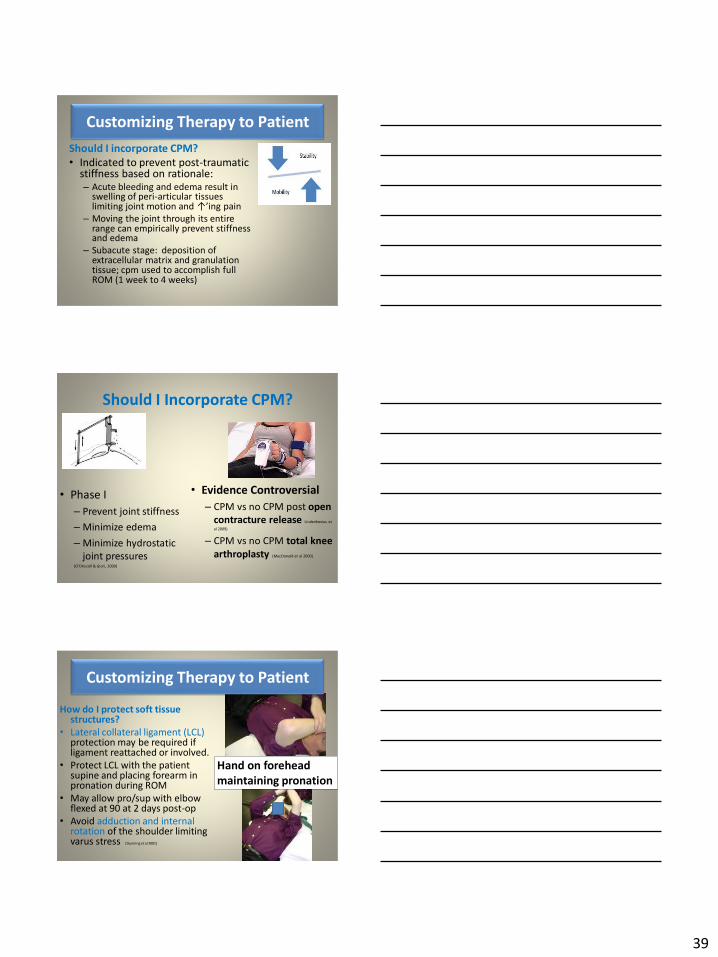
39
Customizing Therapy to Patient
Should I incorporate CPM
bull Indicated to prevent post-traumatic stiffness based on rationale ndash Acute bleeding and edema result in
swelling of peri-articular tissues limiting joint motion and uarrrsquoing pain
ndash Moving the joint through its entire range can empirically prevent stiffness and edema
ndash Subacute stage deposition of extracellular matrix and granulation tissue cpm used to accomplish full ROM (1 week to 4 weeks)
Should I Incorporate CPM
bull Phase I
ndash Prevent joint stiffness
ndash Minimize edema
ndash Minimize hydrostatic
joint pressures(OrsquoDriscoll amp Giori 2000)
bull Evidence Controversial
ndash CPM vs no CPM post open
contracture release Lindenhovius et
al 2009)
ndash CPM vs no CPM total knee
arthroplasty (MacDonald et al 2000)
How do I protect soft tissue structures
bull Lateral collateral ligament (LCL) protection may be required if ligament reattached or involved
bull Protect LCL with the patient supine and placing forearm in pronation during ROM
bull May allow prosup with elbow flexed at 90 at 2 days post-op
bull Avoid adduction and internal rotation of the shoulder limiting varus stress (Dunning et al 2001)
Hand on forehead
maintaining pronation
Customizing Therapy to Patient
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
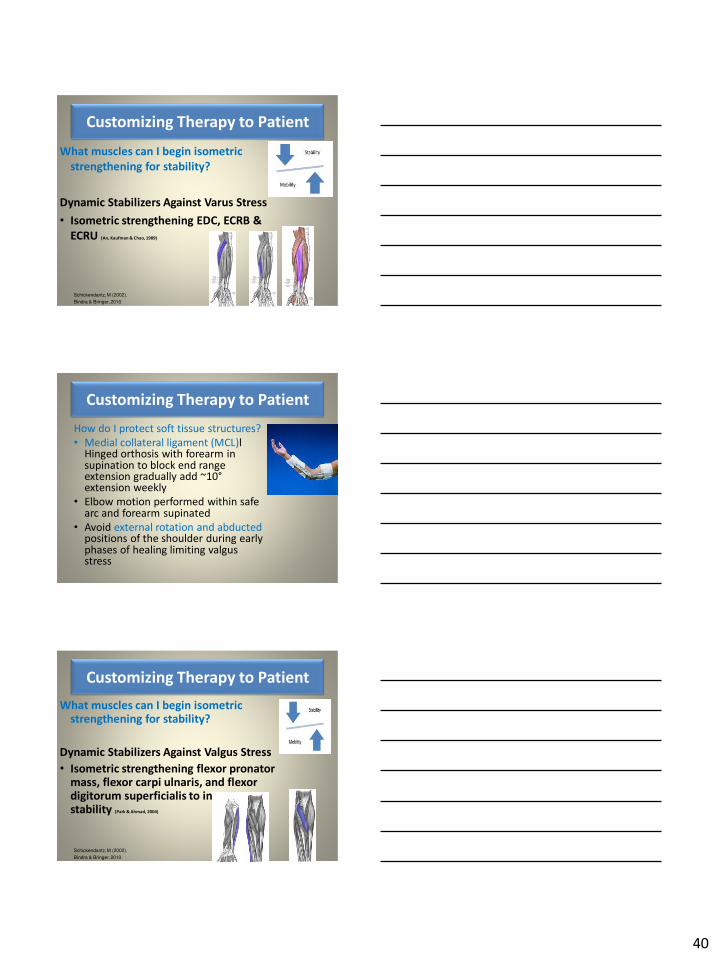
40
What muscles can I begin isometric
strengthening for stability
Dynamic Stabilizers Against Varus Stress
bull Isometric strengthening EDC ECRB amp
ECRU (An Kaufman amp Chao 1989)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
How do I protect soft tissue structures
bull Medial collateral ligament (MCL)l Hinged orthosis with forearm in supination to block end range extension gradually add ~10degextension weekly
bull Elbow motion performed within safe arc and forearm supinated
bull Avoid external rotation and abducted positions of the shoulder during early phases of healing limiting valgus stress
Customizing Therapy to Patient
What muscles can I begin isometric strengthening for stability
Dynamic Stabilizers Against Valgus Stress
bull Isometric strengthening flexor pronator mass flexor carpi ulnaris and flexor digitorum superficialis to increase stability (Park amp Ahmad 2004)
Schickendantz M (2002)
Bindra amp Bringer 2010
Customizing Therapy to Patient
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
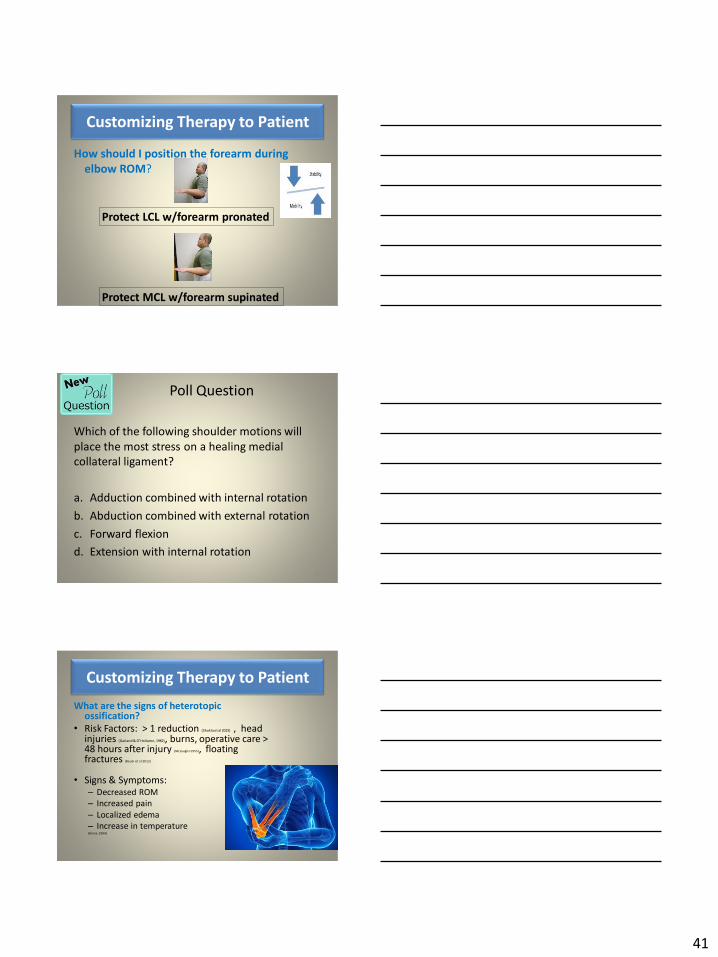
41
How should I position the forearm during
elbow ROM
Customizing Therapy to Patient
Protect LCL wforearm pronated
Protect MCL wforearm supinated
Poll Question
Which of the following shoulder motions will
place the most stress on a healing medial
collateral ligament
a Adduction combined with internal rotation
b Abduction combined with external rotation
c Forward flexion
d Extension with internal rotation
122
What are the signs of heterotopic ossification
bull Risk Factors gt 1 reduction (Shukla et al 2015) head injuries (Garland amp OrsquoHollaren 1982) burns operative care gt 48 hours after injury (McLauglin1955) floating fractures (Bauer et al 2012)
bull Signs amp Symptoms ndash Decreased ROM
ndash Increased pain
ndash Localized edema
ndash Increase in temperature (Hinck 1994)
Customizing Therapy to Patient
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
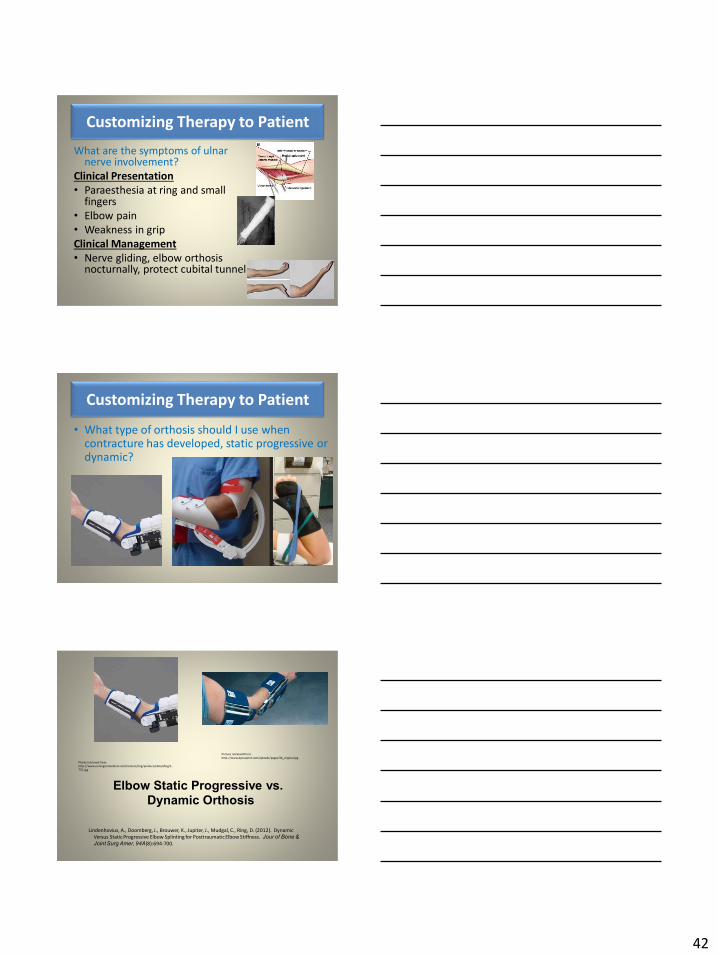
42
What are the symptoms of ulnar nerve involvement
Clinical Presentation
bull Paraesthesia at ring and small fingers
bull Elbow pain
bull Weakness in grip
Clinical Management
bull Nerve gliding elbow orthosis nocturnally protect cubital tunnel
Customizing Therapy to Patient
bull What type of orthosis should I use when contracture has developed static progressive or dynamic
Customizing Therapy to Patient
Elbow Static Progressive vs Dynamic Orthosis
Lindenhovius A Doomberg J Brouwer K Jupiter J Mudgal C Ring D (2012) Dynamic
Versus Static Progressive Elbow Splinting for Posttraumatic Elbow Stiffness Jour of Bone amp
Joint Surg Amer 94A(8)694-700
Picture retreived from
httpwwwdynasplintcomuploadspages36_originaljpg
Photo retrieved from
httpwwwremingtonmedicalcomContentimgproductsdetailbig1-
T55jpg
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
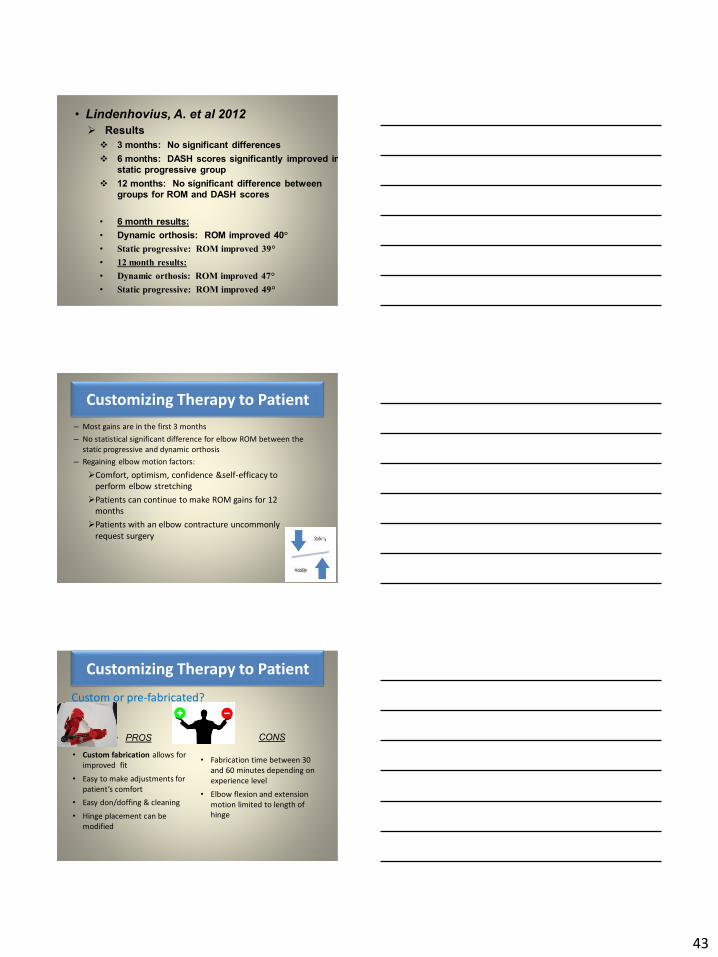
43
bull Lindenhovius A et al 2012
Results
3 months No significant differences
6 months DASH scores significantly improved in static progressive group
12 months No significant difference between groups for ROM and DASH scores
bull 6 month results
bull Dynamic orthosis ROM improved 40degbull Static progressive ROM improved 39degbull 12 month results
bull Dynamic orthosis ROM improved 47degbull Static progressive ROM improved 49deg
ndash Most gains are in the first 3 months
ndash No statistical significant difference for elbow ROM between the
static progressive and dynamic orthosis
ndash Regaining elbow motion factors
Comfort optimism confidence ampself-efficacy to
perform elbow stretching
Patients can continue to make ROM gains for 12
months
Patients with an elbow contracture uncommonly
request surgery
Customizing Therapy to Patient
bull PROS
129
bull Custom fabrication allows for
improved fit
bull Easy to make adjustments for
patientrsquos comfortbull Easy dondoffing amp cleaning
bull Hinge placement can be
modified
CONS
bull Fabrication time between 30
and 60 minutes depending on
experience level
bull Elbow flexion and extension
motion limited to length of
hinge
Customizing Therapy to Patient
Custom or pre-fabricated
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
44
d
bull PROS
130
bull Pre-fab short wearing time
bull Light weight amp easy fitting with
measurements
bull Easy dondoffing amp cleaning
bull Results can reach up to 170deg of
flexion and -10deg of extension
bull Patient can track progress on
CONS
bull Could be limited by insurance
authorization
bull Modifications to orthosis could
be more timely
bull Can be high profile depending
on order
Customizing Therapy to Patient
Custom or pre-fabricated
Customizing Therapy to Patient
Poll Question
Is it safe to begin early ROM in a type one radial
head fracture that is minimally displaced
a Yes
b No
132
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
45
WRISTHAND INSTABILITIES
Bony Anatomy
bull 2 long bones
ndashRadius amp Ulna
bull 8 carpal bones
ndashProximal amp distal rows
bull 14 phalanges
bull 5 metacarpals 134
FUNCTIONAL MOTIONS
bull FLEXION
bull EXTENSION
bull RADIAL DEVIATION
bull ULNAR DEVIATION
bull CIRCUMDUCTION
bull DART THROW AXIS Retrieved on 050109 from
wwwdkimagescomDarts
Darts-15html
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
46
Carpal Row Movements during
FlexionExtensionbull Distal carpal row follows the
direction of movement of metacarpals 23
bull Proximal row moves with the distal row but there is more motion between the individual bones
bull Flexion Proximal row glides dorsally and capitate glides dorsally on lunate
bull Extension Proximal row glides volarly and capitate glide volarly
Retrieved on 050109 from
httpwwwandysleighcom
WristAndForearmtutorial
wristpage5ahtml
Carpal Row Movements during
RadialUlnar Deviation
Reciprocal Motion
bull Ulnar Deviation Distal row moves ulnarly and the proxmialrow extends and translate radially
bull Radial deviation Distal row moves radially and the proximal row flexes and translate ulnarly Retrieved on 050109 from
wwwdavidlnelsonmd
Lichtman_talkhtm
Berger 1996
Osseous Morphology amp Kinematics
Radius amp Ulna
bull Distal radius articulates with proximal row at scaphoid fossa and lunate fossa
bull Ulna does not articulate with the carpus Triangular disc articulates with carpus at distal ulna
Retrieved on 050109
fromwwwanswerscomtopicu
lna
Retrieved on 50309From wwwhughstoncom
hhaa_13_3_1htm
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
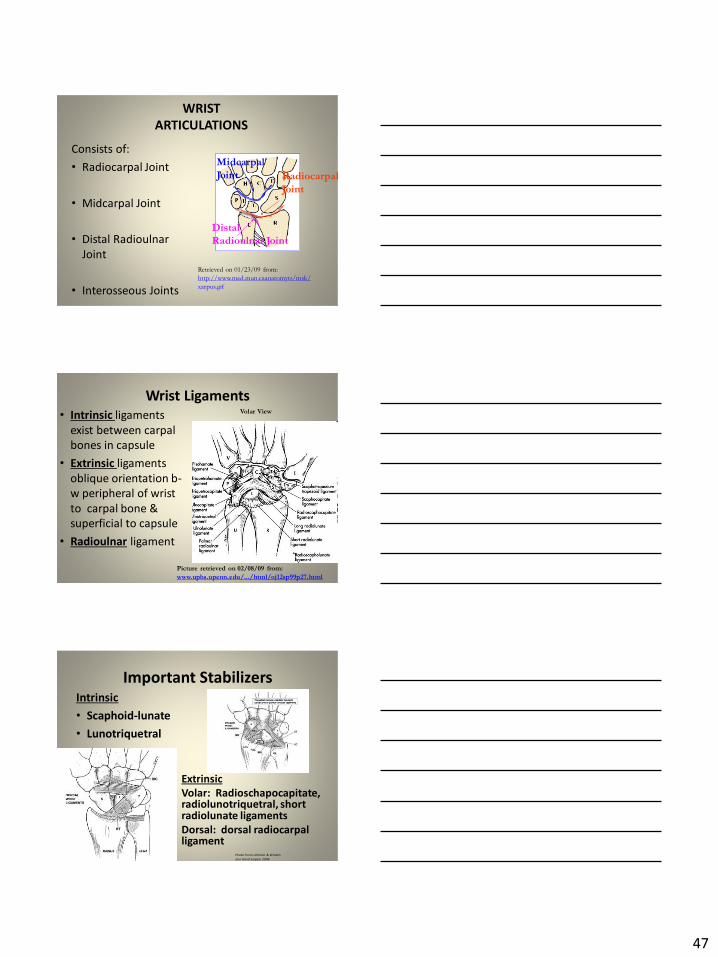
47
WRIST
ARTICULATIONS
Consists of
bull Radiocarpal Joint
bull Midcarpal Joint
bull Distal Radioulnar
Joint
bull Interosseous Joints
Retrieved on 012309 from
httpwwwmedmuncaanatomytsmsk
xarpusgif
Radiocarpal
Joint
Midcarpal
Joint
Distal
Radioulnar Joint
Wrist Ligaments
bull Intrinsic ligaments
exist between carpal
bones in capsule
bull Extrinsic ligaments
oblique orientation b-
w peripheral of wrist
to carpal bone amp
superficial to capsule
bull Radioulnar ligament
Volar View
Picture retrieved on 020809 from
wwwuphsupenneduhtmloj12sp99p27html
Important StabilizersIntrinsic
bull Scaphoid-lunate
bull Lunotriquetral
Extrinsic
Volar Radioschapocapitate radiolunotriquetral short radiolunate ligaments
Dorsal dorsal radiocarpal ligament
Photo from Lichtmen amp Wroten
Jour Hand Surgery 2006
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
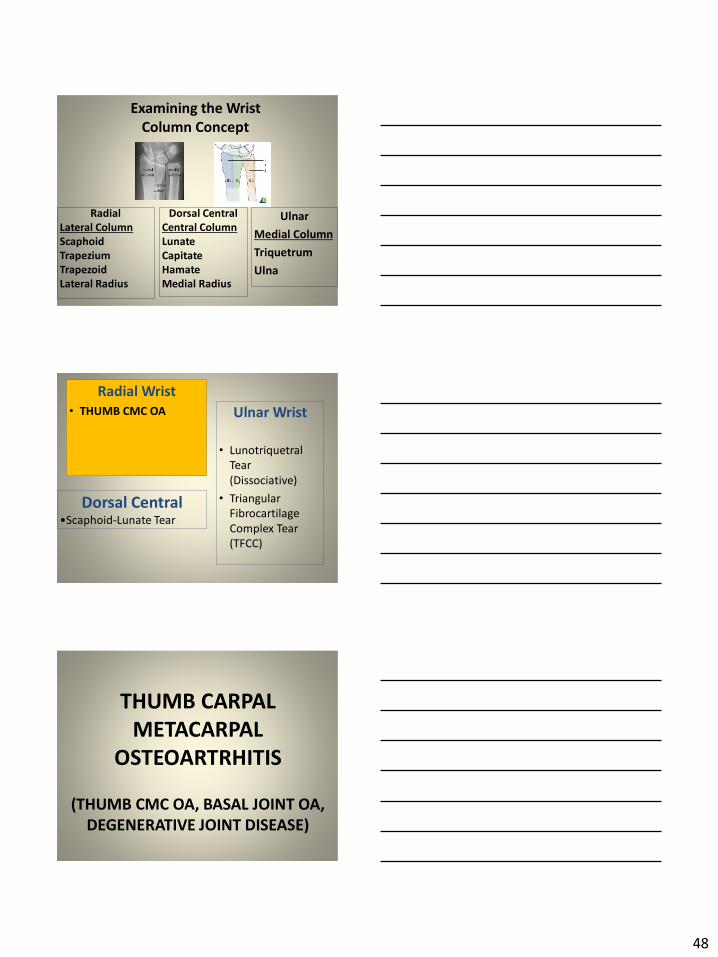
48
Examining the Wrist
Column Concept
Radial
Lateral Column
Scaphoid
Trapezium
Trapezoid
Lateral Radius142
Dorsal Central
Central Column
Lunate
Capitate
Hamate
Medial Radius
Ulnar
Medial Column
Triquetrum
Ulna
Radial Wrist
bull THUMB CMC OA Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
THUMB CARPAL
METACARPAL
OSTEOARTRHITIS
(THUMB CMC OA BASAL JOINT OA
DEGENERATIVE JOINT DISEASE)
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
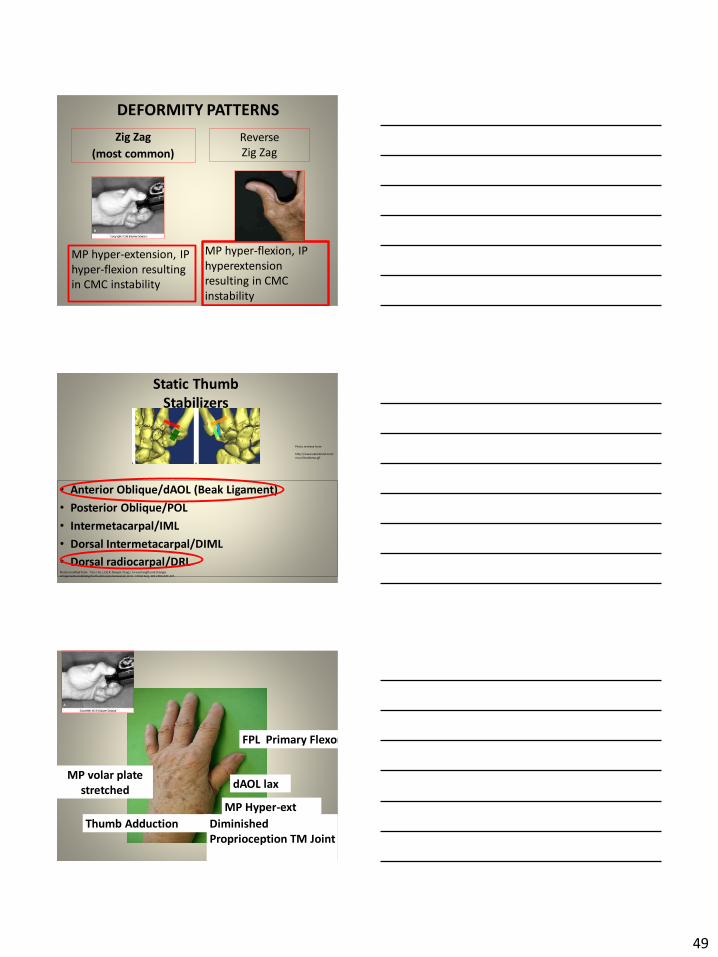
49
DEFORMITY PATTERNS
Zig Zag
(most common)
MP hyper-extension IP
hyper-flexion resulting
in CMC instability
MP hyper-flexion IP
hyperextension
resulting in CMC
instability
Reverse
Zig Zag
Static Thumb
Stabilizers
bull Anterior ObliquedAOL (Beak Ligament)
bull Posterior ObliquePOL
bull IntermetacarpalIML
bull Dorsal IntermetacarpalDIML
bull Dorsal radiocarpalDRLPhoto modified from Tan J Xu J Zie R Deng A Tang J In vivo length and changes
of l igaments stabilizing the thumb carpometacarpal joint J Hand Surg 201136A420-427
Photo retrieve from
httpwwweatonhandcom
musthumbmusgif
Thumb Adduction
MP Hyper-ext
FPL Primary Flexor
MP volar plate
stretcheddAOL lax
Diminished
Proprioception TM Joint
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
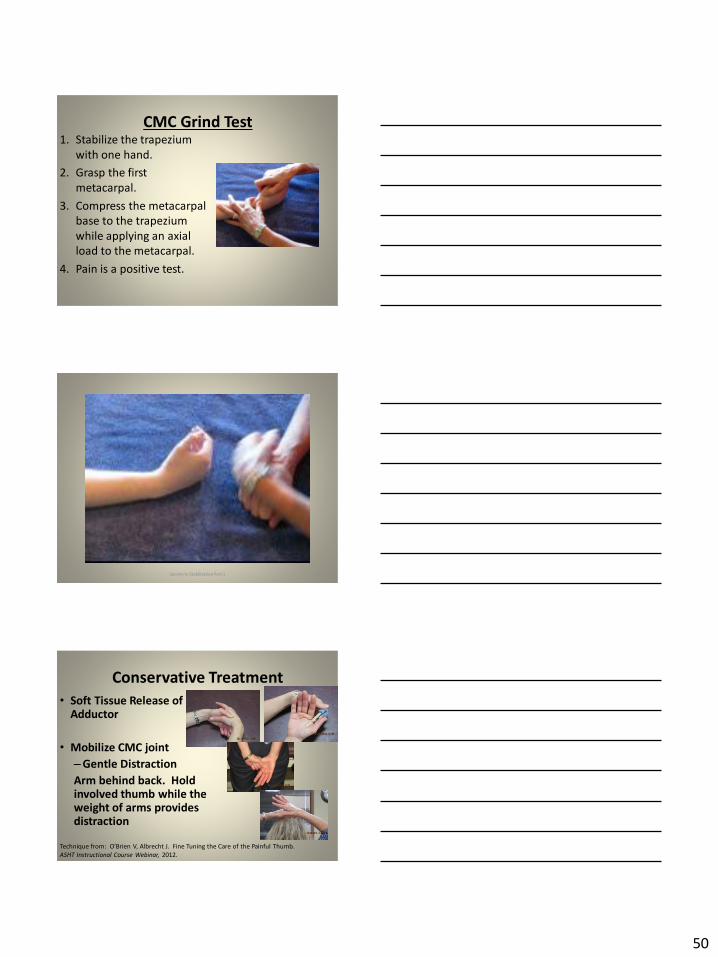
50
CMC Grind Test1 Stabilize the trapezium
with one hand
2 Grasp the first
metacarpal
3 Compress the metacarpal
base to the trapezium
while applying an axial
load to the metacarpal
4 Pain is a positive test
Secrets to Stabilization Part 1 149
Conservative Treatment
bull Soft Tissue Release of Adductor
bull Mobilize CMC joint
ndashGentle Distraction
Arm behind back Hold involved thumb while the weight of arms provides distraction
Technique from OrsquoBrien V Albrecht J Fine Tuning the Care of the Painful Thumb ASHT Instructional Course Webinar 2012
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
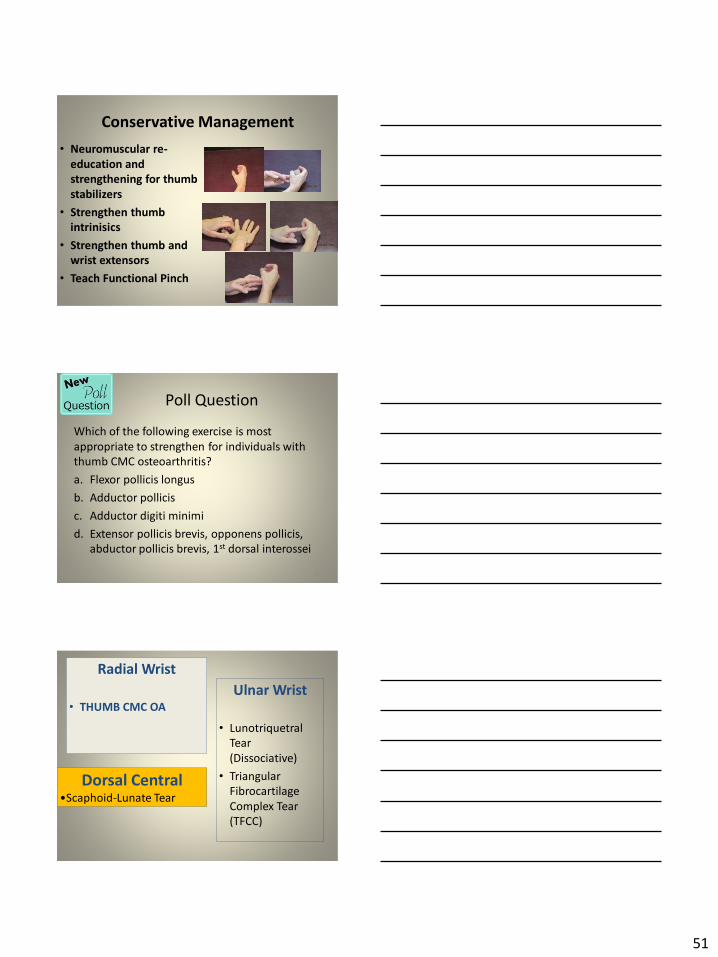
51
Conservative Management
bull Neuromuscular re-
education and
strengthening for thumb
stabilizers
bull Strengthen thumb
intrinisics
bull Strengthen thumb and
wrist extensors
bull Teach Functional Pinch
Poll Question
Which of the following exercise is most
appropriate to strengthen for individuals with
thumb CMC osteoarthritis
a Flexor pollicis longus
b Adductor pollicis
c Adductor digiti minimi
d Extensor pollicis brevis opponens pollicis
abductor pollicis brevis 1st dorsal interossei
152
Radial Wrist
bull THUMB CMC OA
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
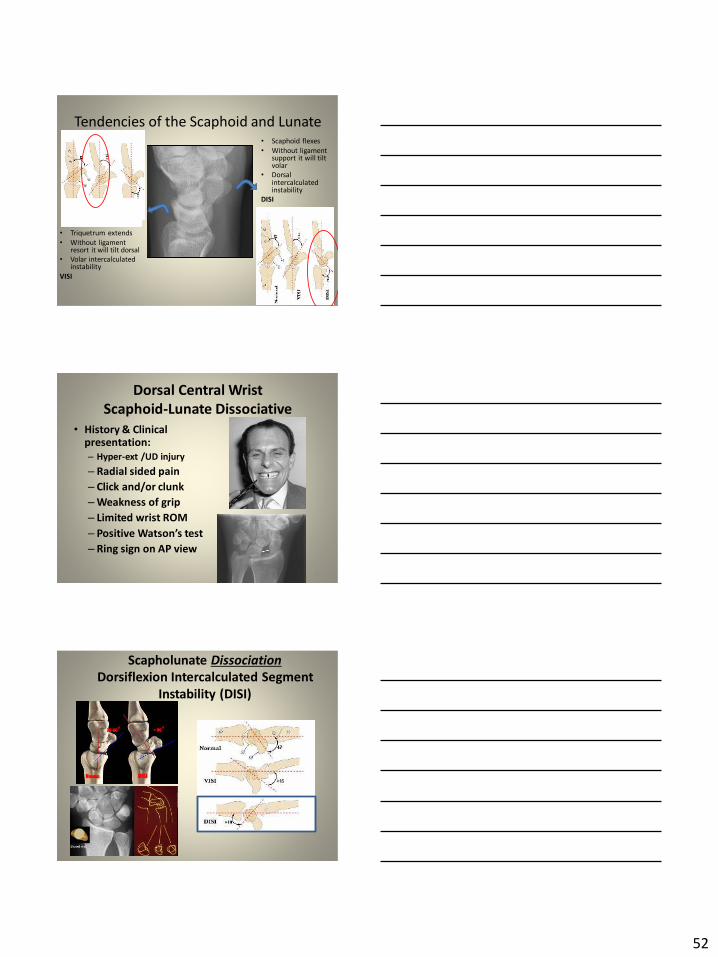
52
Tendencies of the Scaphoid and Lunate
bull Triquetrum extends
bull Without ligament resort it will tilt dorsal
bull Volar intercalculated instability
VISI
bull Scaphoid flexes
bull Without ligament support it will tilt volar
bull Dorsal intercalculated instability
DISI
Dorsal Central Wrist
Scaphoid-Lunate Dissociative
bull History amp Clinical presentation
ndash Hyper-ext UD injury
ndash Radial sided pain
ndash Click andor clunk
ndashWeakness of grip
ndash Limited wrist ROM
ndash Positive Watsonrsquos testndash Ring sign on AP view
155
Scapholunate Dissociation
Dorsiflexion Intercalculated Segment
Instability (DISI)
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
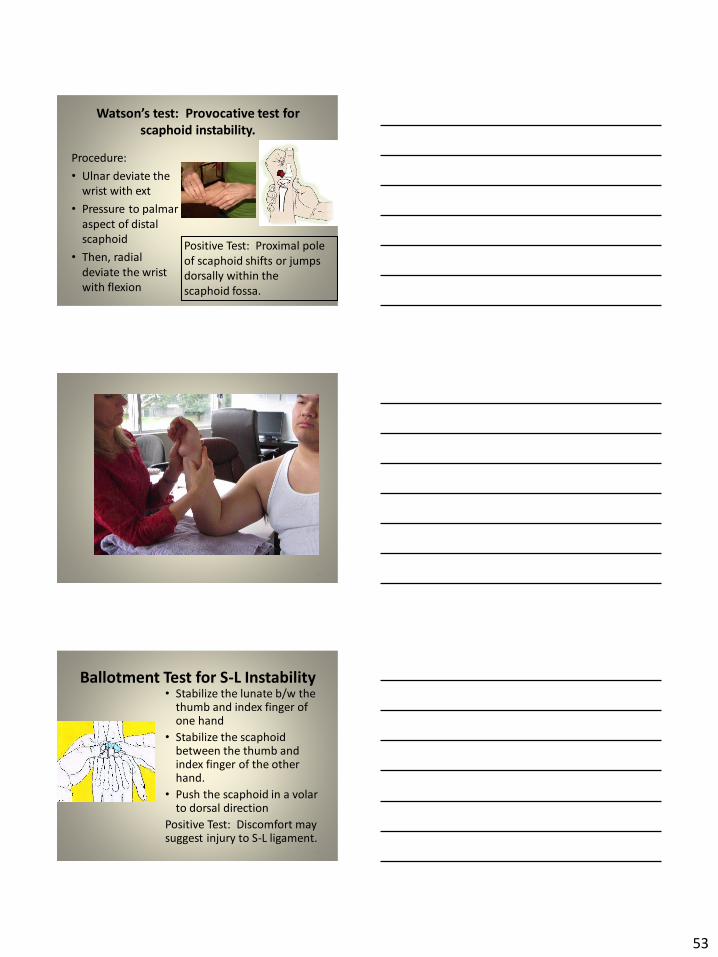
53
Watsonrsquos test Provocative test for scaphoid instability
Procedure
bull Ulnar deviate the
wrist with ext
bull Pressure to palmar
aspect of distal
scaphoid
bull Then radial
deviate the wrist
with flexion
Positive Test Proximal pole
of scaphoid shifts or jumps
dorsally within the
scaphoid fossa
158
Ballotment Test for S-L Instabilitybull Stabilize the lunate bw the
thumb and index finger of one hand
bull Stabilize the scaphoid between the thumb and index finger of the other hand
bull Push the scaphoid in a volar to dorsal direction
Positive Test Discomfort may suggest injury to S-L ligament
159
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
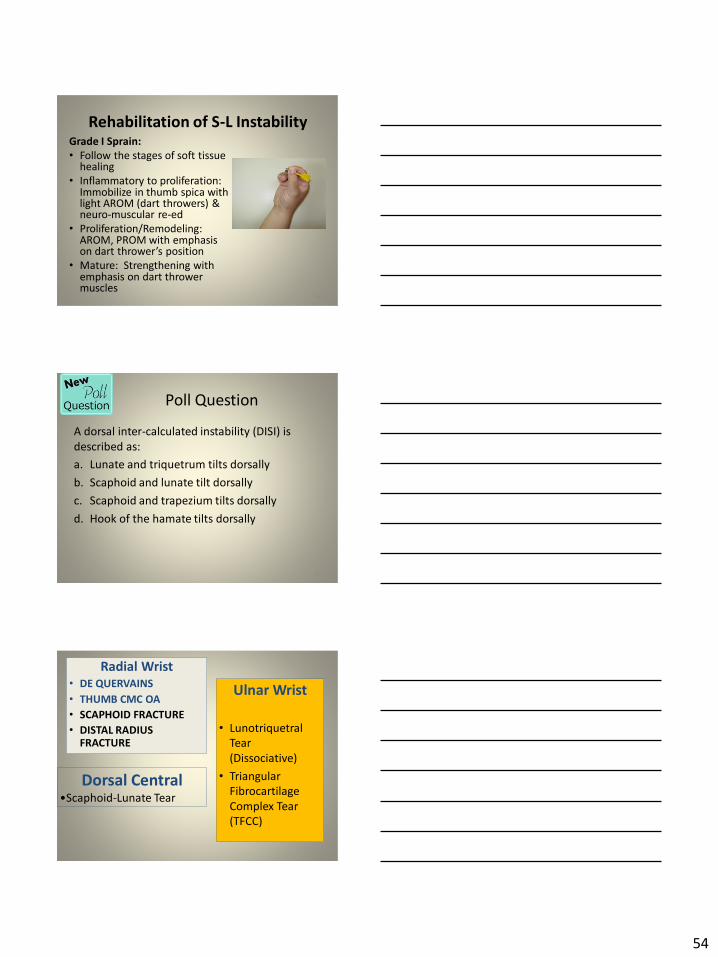
54
Rehabilitation of S-L InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in thumb spica with light AROM (dart throwers) amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
160
Poll Question
A dorsal inter-calculated instability (DISI) is
described as
a Lunate and triquetrum tilts dorsally
b Scaphoid and lunate tilt dorsally
c Scaphoid and trapezium tilts dorsally
d Hook of the hamate tilts dorsally
161
Radial Wrist
bull DE QUERVAINS
bull THUMB CMC OA
bull SCAPHOID FRACTURE
bull DISTAL RADIUS FRACTURE
Ulnar Wrist
bull Lunotriquetral
Tear
(Dissociative)
bull Triangular
Fibrocartilage
Complex Tear
(TFCC)
Dorsal CentralbullScaphoid-Lunate Tear
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
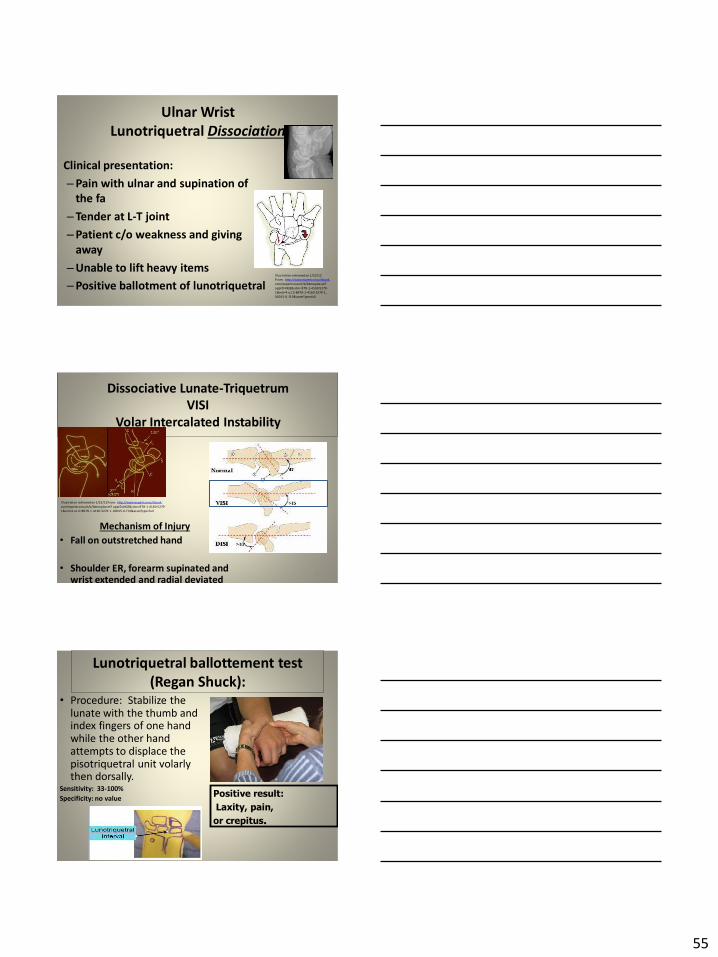
55
Ulnar Wrist
Lunotriquetral Dissociation
bull Clinical presentation
ndashPain with ulnar and supination of
the fa
ndashTender at L-T joint
ndashPatient co weakness and giving
away
ndashUnable to lift heavy items
ndashPositive ballotment of lunotriquetralIl lustration retrieved on 12212
From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset
appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-1
00015-0f19ampassetType=full
Dissociative Lunate-Triquetrum
VISI
Volar Intercalated Instability
Mechanism of Injury
bull Fall on outstretched hand
bull Shoulder ER forearm supinated and wrist extended and radial deviated
164
Il lustration retrieved on 12212From httpwwwexpertconsultbook
comexpertconsultbbbmapAsset appID=NGEampisbn=978-1-4160-5279-
1ampeid=4-u10-B978-1-4160-5279-100015-0f19ampassetType=full
Lunotriquetral ballottement test
(Regan Shuck)bull Procedure Stabilize the
lunate with the thumb and index fingers of one hand while the other hand attempts to displace the pisotriquetral unit volarly then dorsally
Sensitivity 33-100
Specificity no valuePositive result
Laxity pain
or crepitus
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
56
Secrets to Stabilization Part 1 166
Rehabilitation of LT InstabilityGrade I Sprain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp
bull neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM with emphasis on dart throwerrsquos position
bull Mature Strengthening with emphasis on dart thrower muscles
Consider taping for neuromuscular re-ed
167
Ulnar Sided Wrist Pain
Clinical Presentation of TFCC Tearbull Ulnar sided wrist pain
bull Pain with palpation in region of TFCC
bull Pain with active ulnar deviation
bull Positive TFCC load test
bull Pain with forearm rotation
bull Audible click with rotation
bull Pain with pronated grip
168
Retrieved from
wwwhughstoncom
hhaa_13_3_1htm
57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1

57
bull Normal axial load of radius is 80 and ulna is 20
bull The TFCC functions to transmit 20 of the axially applied load from the ulnar carpus to the distal ulna It is a major stabilizer of the distal radial ulnar joint
169
Illustration from Palmer A Bille B Anderson A
Acute Injuries of the Distal Radioulnar Joint
Tears by the Triangular Fibrocartilage
Distal Radiouulnar Joint Chapter 24
TRIANGULAR FIBROCARTILAGE COMPLEX
(TFCC)
Stabilizers of the Ulnar Wrist
bull Static Stabilizers
ndash Sigmoid Notch
ndashDorsalVolar radioulnar ligaments
ndashTFCC
bull Dynamic Stabilizers
ndashPronator Quadratus
ndashECU
ndash FCU
170Image fromhttpuploadwikimediaorgwikipedia
commons115Gray424png
Triangular Fibrocartilage Complex
(TFCC)
bull Palpate for
tenderness
171
Fovea sign Tenderness bw
FCU tendon and ulnar styloid
process
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
58
TFCC or Ulnocarpal Abutment
TESTING
Ulnocarpal Stress
Test
bull Axial load compression
with wrist in ulnar
deviation Glide volar
and dorsally
Positive Test
Reproduction of pain
clicking or crepitus
173
Poll Question
Which is the following best describes the triangular fibro-cartilage complex
a Redistributes force from the ulna to the radius
b Is highly vascular in the central portion
c Re-distributes 20 of the force from the ulnar carpus to the distal ulna and is contributor to the stability of the distal radioulnar joint
d Clinically presents as radial wrist pain174
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
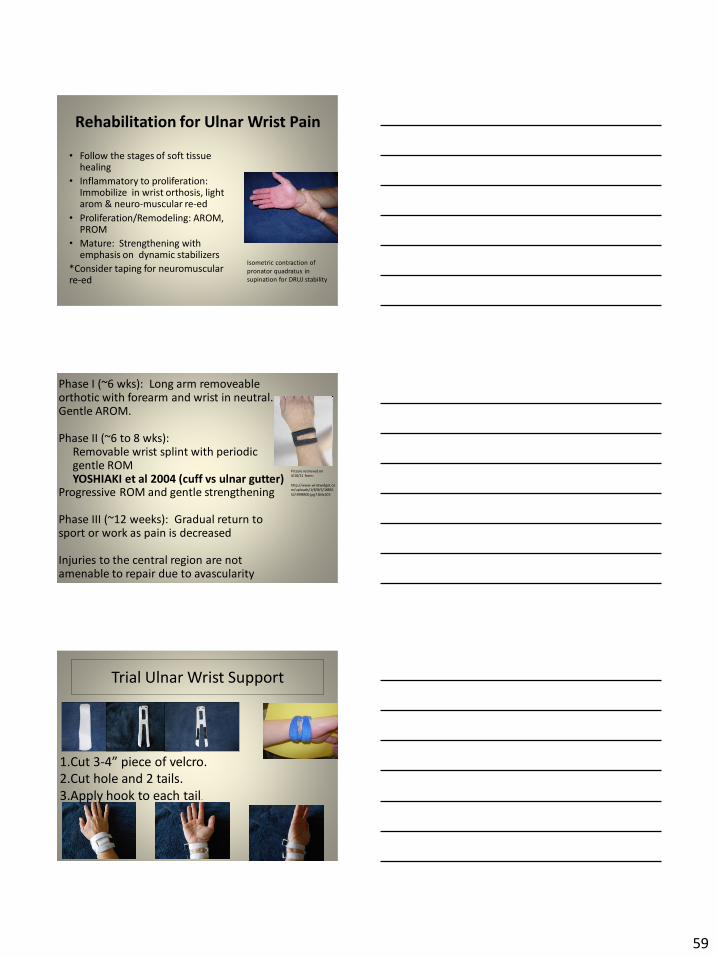
59
Rehabilitation for Ulnar Wrist Pain
bull Follow the stages of soft tissue healing
bull Inflammatory to proliferation Immobilize in wrist orthosis light arom amp neuro-muscular re-ed
bull ProliferationRemodeling AROM PROM
bull Mature Strengthening with emphasis on dynamic stabilizers
Consider taping for neuromuscular re-ed
175
Isometric contraction of
pronator quadratus in
supination for DRUJ stability
Picture retrieved on
41011 from
httpwwwwristwidgetco
muploads188518855
523998400jpg164x203
Phase I (~6 wks) Long arm removeable orthotic with forearm and wrist in neutral Gentle AROM
Phase II (~6 to 8 wks) Removable wrist splint with periodic gentle ROMYOSHIAKI et al 2004 (cuff vs ulnar gutter)
Progressive ROM and gentle strengthening
Phase III (~12 weeks) Gradual return to sport or work as pain is decreased
Injuries to the central region are not amenable to repair due to avascularity
Trial Ulnar Wrist Support
1Cut 3-4rdquo piece of velcro2Cut hole and 2 tails
3Apply hook to each tail
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
60
Procedures for Distal Radial
Ulnar Joint (DRUJ) Instability
bull Soft tissue reconstruction
bull Suave Kapandje
bull Darrah
bull Hemiresection-Interposition Arthroplasty (HIT)
bull Implant arthroplasty
Retrieved on 112711 from
httpwwworthoteersorg
imagesuploadedSauvejpg
Retrieved on 121011f from Fornalski S Hay Q Gupta R Chronic Instability of the
Dis tal Radioulnar Joint A Review Univ Of Penn Ortho Jour 20001343-52
Photo retrieved from Ka iser et a l 2008
General Progression Concepts with
Stabilization
ProliferationRegeneration Phases
bull Gradual return to AROM and gentle PROM at wrist and forearm (gradual progression to end range prosup)
Maturation Phase (6 to 12 weeks)
bull Gentle strengthening and activity as tolerated
bull Full activity as tolerated
GENERAL REHAB CONSIDERATIONS
bull Which orthotic limits forearm rotation best
ndashMuenster
ndashSugartong
ndashAntipronationSlaughter et al 2010
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
61
Conclusionbull Sugartong restricts pronation significantly better
than all other orthotics
bull Anti-pronation demonstrated significantly better
results limiting forearm pronation as compared to
the wrist orthotic
bull Anti-pronation splint may be uncomfortable due
to placement on ulnar styloid
bull Neither Muenster or Sugartong completely
immobilized rotation
bull 3 subjects reported Sugartong most comfortable
and 2 reported Muenster most comfortableSlaughter et al 2010
Poll Question
Should forearm rotatiion strength and ROM be
phased in gradually as the patient gains strength
following a surgical reconstruction of the distal
radial ulnar joint
a Yes
b No
182
General Concepts for
Wrist Rehabilitation
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
62
Proprioception Training
Conscious RehabilitationPhase I Conscious joint control
Phase II Sense joint motion without audiovisual
cues
Phase III Strengthening specific muscles to enhance
joint stability
Phase IV Unconscious RehabilitationHagert E (2010)
bull Edema Control
bull Pain Control (visual analog scale)
bull Promote Safe Motion
Conscious Rehabilitation
Phase I
Diagram retrieved on 71511 from http0tqncomdergonomics10C---
painscalejpg
Conscious Rehabilitation
Phase II amp III
Conscious joint controlbull Mirror therapy
bull Active reproduction of joint angle accuracy of joint re-positioning
Hagert E (2010)
63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1

63
Conscious Rehabilitation
Phase IV
Sense Joint Motion without
Audiovisual Cuesbull Motion detection (detection of passive motion)
ndash Degree of joint angle at which motion is detected
Hagert E (2010)
Conscious Rehabilitation
Phase V
Strengthen specific muscles to enhance joint
stability
bull Eccentric training
bull Co-activation training
Hagert E (2010)
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION
Reactive muscle activation
Hagert E (2010)
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
64
Phase VIUNCONSCIOUS NEUROMUSCULAR
REHABILITATION Hagert E (2010)
Reactive muscle activation
Oscillating Technique Isometric
Stabilization
Light Ball Toss
Gentle Oscillations
Sensori-motor Re-training
191
Image retrieved from httpniveapsychouniv-paris5fr
CogSysZurich2010How20to20build20a20robot20t
hat20feels_
fichiersimage153png
Sensorimotor Retraining
1 Use chopsticks to pickup varying items and separate items
2 Finding dry beans in putty
3 Molding specific shapes
4 Card turning
5 Rhythmic stabilization
Research pediatric sensorimotor activities for more ideas
192
65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1

65
THANK YOU
Secrets to Stabilization Part 1 193
References1 Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult shoulder function Disabilities of
the Arm Shoulder and Hand Questionnaire (DASH) and its short version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American
Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder Test (SST)
Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario Shoulder Instability Index (WOSI) Arthritis care amp
research 63(S11) S174-S188
2 Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W (2004) Clinimetric evaluation of shoulder
disability questionnaires a systematic review of the literature Annals of the rheumatic diseases 63(4) 335-341
3 Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of Bone amp Joint Surgery 91(4) 966-978
4 Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist are oriented obliquely to the
anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
5 Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications on the Rehabilitation of the Wrist Jour
Hand Ther 2010232-17
6 Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M (2014) Immobilization in external rotation
combined with abduction reduces the risk of recurrence after primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery
23(6) 759-766
7 Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new method of immobilization after
traumatic anterior dislocation of the shoulder a preliminary study Journal of shoulder and elbow surgery 12(5) 413-415
8 Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of sports medicine 28(6) 910-917
9 Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005) Reliability validity and responsiveness of the
American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral
arthritis The Journal of Bone amp Joint Surgery 87(9) 2006-2011
10 Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a
bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp Related Surgery 25(1) 102-105
11 Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in internal or external
rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(1) 13-19
12 Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization after primary
anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
13 Paschos N K Mitsionis G I Vasiliadis H S amp Georgoulis A D (2013) Comparison of early mobilization protocols in radial head fractures
Journal of orthopaedic trauma 27(3) 134-139
14 Slaughter A Miles L Fleming J amp McPhail S (2010) A comparative study of splint effectiveness in limiting forearm rotation Journal of Hand
Therapy 23(3) 241-248
15 Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic Surgeons 18(7)
436-444
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 195
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
66
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 196
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 197
References Angst F Schwyzer H K Aeschlimann A Simmen B R amp Goldhahn J (2011) Measures of adult
shoulder function Disabilities of the Arm Shoulder and Hand Questionnaire (DASH) and its short
version (QuickDASH) Shoulder Pain and Disability Index (SPADI) American Shoulder and Elbow Surgeons
(ASES) Society standardized shoulder assessment form Constant (Murley) Score (CS) Simple Shoulder
Test (SST) Oxford Shoulder Score (OSS) Shoulder Disability Questionnaire (SDQ) and Western Ontario
Shoulder Instability Index (WOSI) Arthritis care amp research 63(S11) S174-S188
Bot S D M Terwee C B Van der Windt D A W M Bouter L M Dekker J amp De Vet H C W
(2004) Clinimetric evaluation of shoulder disability questionnaires a systematic review of the literature
Annals of the rheumatic diseases 63(4) 335-341
Braun S Kokmeyer D amp Millett P J (2009) Shoulder injuries in the throwing athlete The Journal of
Bone amp Joint Surgery 91(4) 966-978
Crisco J J Heard W M Rich R R Paller D J amp Wolfe S W (2011) The mechanical axes of the wrist
are oriented obliquely to the anatomical axes The Journal of Bone amp Joint Surgery 93(2) 169-177
Groh G I Wirth M A amp Rockwood C A (2011) Treatment of traumatic posterior sternoclavicular
dislocations Journal of Shoulder and Elbow Surgery 20(1) 107-113
Guan J J amp Wolf B R (2013) Reconstruction for anterior sternoclavicular joint dislocation and
instability Journal of Shoulder and Elbow Surgery 22(6) 775-781
Hagert E Proprioception of the Wrist Joint A ReviewmOf Current Concepts and Possible Impllications
on the Rehabilitation of the Wrist Jour Hand Ther 2010232-17
Heidari K Asadollahi S Vafaee R Barfehei A Kamalifar H Chaboksavar Z A amp Sabbaghi M
(2014) Immobilization in external rotation combined with abduction reduces the risk of recurrence after
primary anterior shoulder dislocation Journal of Shoulder and Elbow Surgery 23(6) 759-766Secrets to Stabilization Part 1 198
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
67
bull Hodges P W amp Richardson C A (1996) Inefficient muscular stabilization of the lumbar spine
associated with low back pain a motor control evaluation of transversus abdominis Spine 21(22) 2640-
2650
bull Itoi E Hatakeyama Y Kido T Sato T Minagawa H Wakabayashi I amp Kobayashi M (2003) A new
method of immobilization after traumatic anterior dislocation of the shoulder a preliminary study
Journal of shoulder and elbow surgery 12(5) 413-415
bull Johansen J A Grutter P W McFarland E G amp Petersen S A (2011) Acromioclavicular joint injuries
indications for treatment and treatment options Journal of Shoulder and Elbow Surgery 20(2) S70-S82
bull Levine W N amp Flatow E L (2000) The pathophysiology of shoulder instability The American journal of
sports medicine 28(6) 910-917
bull Liemohn WP Baumgartner TA Gagnon LH (2005) Measuring core stability J Strength Cond Res
19(3)583-6
bull Lubiatowski P Olczak I Lisiewicz E Ogrodowicz P Bręborowicz M amp Romanowski L (2014) Elbow
joint position sense after total elbow arthroplasty Journal of Shoulder and Elbow Surgery 23(5) 693-
700
bull Kocher M S Horan M P Briggs K K Richardson T R OHolleran J amp Hawkins R J (2005)
Reliability validity and responsiveness of the American Shoulder and Elbow Surgeons subjective
shoulder scale in patients with shoulder instability rotator cuff disease and glenohumeral arthritis The
Journal of Bone amp Joint Surgery 87(9) 2006-2011
bull Millett P J amp Braun S (2009) The ldquobony Bankart bridgerdquo procedure A new arthroscopic technique for reduction and internal fixation of a bony Bankart lesion Arthroscopy The Journal of Arthroscopic amp
Related Surgery 25(1) 102-105
bull Miyake Y Kobayashi R Kelepecz D amp Nakajima M (2013) Core exercises elevate trunk stability to
facilitate skilled motor behavior of the upper extremities Journal of bodywork and movement therapies
17(2) 259-265 Secrets to Stabilization Part 1 199
bull Nagai K Tateuchi H Takashima S Miyasaka J Hasegawa S Arai R amp Ichihashi N (2013) Effects of trunk rotation
on scapular kinematics and muscle activity during humeral elevation Journal of Electromyography and Kinesiology 23(3)
679-687
bull Paterson W H Throckmorton T W Koester M Azar F M amp Kuhn J E (2010) Position and duration of immobilization
after primary anterior shoulder dislocation The Journal of Bone amp Joint Surgery 92(18) 2924-2933
bull Peate W F Bates G Lunda K Francis S amp Bellamy K (2007) Core strength a new model for injury prediction and
prevention J Occup Med Toxicol 2(3) 1-9
bull Pizzari T Wickham J Balster S Ganderton C amp Watson L (2014) Modifying a shrug exercise can facilitate the upward
rotator muscles of the scapula Clinical Biomechanics 29(2) 201-205
bull Potvin JR Brown SH An equation to calculate individual muscle contributions to joint stability (2005) J Biomech 38(5)973-
80
bull Struyf F Nijs J Baeyens J P Mottram S amp Meeusen R (2011) Scapular positioning and movement in unimpaired
shoulders shoulder impingement syndrome and glenohumeral instability Scandinavian journal of medicine amp science in
sports 21(3) 352-358
bull Vavken P Sadoghi P Quidde J Lucas R Delaney R Mueller A M amp Valderrabano V (2014) Immobilization in
internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation Journal of
Shoulder and Elbow Surgery 23(1) 13-19
bull Wright R W amp Baumgarten K M (2010) Shoulder outcomes measures Journal of the American Academy of Orthopaedic
Surgeons 18(7) 436-444
Secrets to Stabilization Part 1 200
Patient Function and Goals
bull Patientrsquos functional activity ndash Validated outcome assessments for shoulder
instabilities include
bull Oxford shoulder instability questionnaire
bull Shoulder instability questionnaire
bull Western Ontario shoulder instability index
bull The American Shoulder and Elbow Surgeons subjective
scale
bull Disability of the arm shoulder and hand (DASH)
bull Constant Murley shoulder assessment
bull Shoulder pain and disability indexSecrets to Stabilization Part 1 201
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1
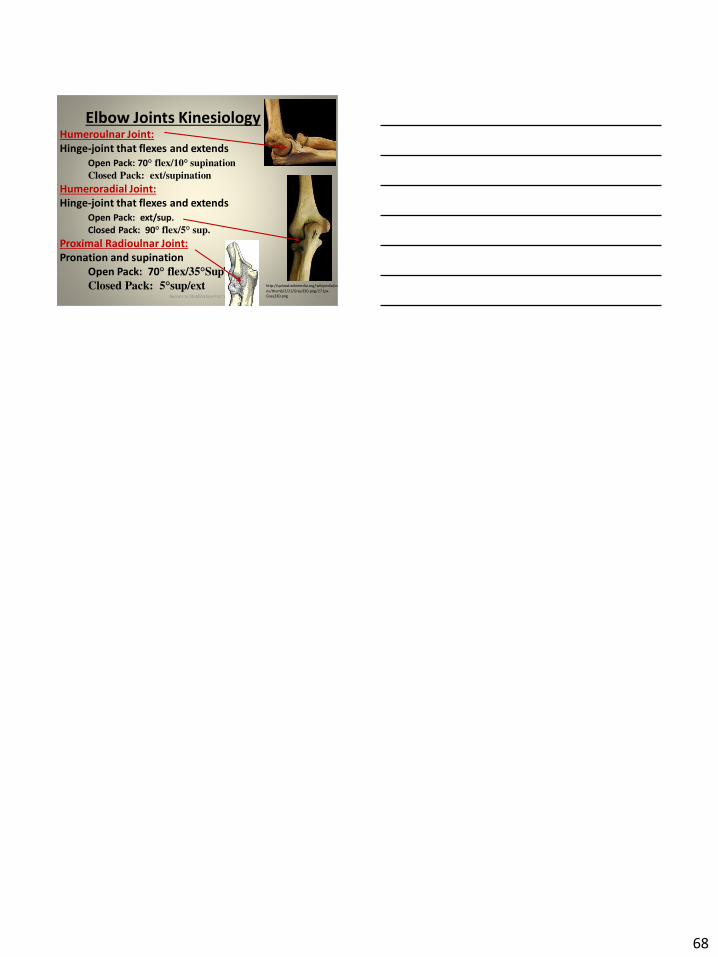
68
Elbow Joints KinesiologyHumeroulnar Joint
Hinge-joint that flexes and extends
Open Pack 70deg flex10deg supination
Closed Pack extsupination
Humeroradial Joint
Hinge-joint that flexes and extends
Open Pack extsup
Closed Pack 90deg flex5deg sup
Proximal Radioulnar Joint
Pronation and supination
Open Pack 70deg flex35degSup
Closed Pack 5degsupext httpuploadwikimediaorgwikipediacom
nsthumb221Gray330png271px-
Gray330png 202Secrets to Stabilization Part 1