abcs of dietary guidelines 2000 for clinicians
TRANSCRIPT

© 2000 Tufts University, 1096-6781/00/$15.00/0 Nutrition in Clinical Care,Volume 3, Number 6, 2000 359–370
ABCs of Dietary Guidelines 2000 for Clinicians
Johanna Dwyer, DSc, RD
j
Alice H. Lichtenstein, DSc
School of Nutrition Science and Policy and Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University, Boston, Massachusetts
j
A
BSTRACT
The Dietary Guidelines for Americans are the ABCs forgood health. They urge that all Americans Aim for fit-ness, Build a healthy base, and Choose sensibly. Actionsteps include the following:
Aim for fitness:
Aim for ahealthy weight. Be physically active everyday.
Build ahealthy base:
Let the food pyramid guide your foodchoices. Choose a variety of grains daily, especiallywhole grains. Choose a variety of fruits and vegetablesdaily. Keep food safe to eat.
Choose sensibly:
Choosea diet that is low in saturated fat and cholesterol andmoderate in total fat. Choose beverages and foods tomoderate your intake of sugars. Choose and preparefoods with less salt. If you drink alcoholic beverages, doso in moderation.
Nutr Clin Care.
2000;3:359–370
j
K
EY
W
ORDS
:
dietary guidelines, nutrition policy
The Dietary Guidelines for Americans, 2000
1
repre-sent the best current thinking about what Ameri-cans should eat to stay healthy. This article reviewswhy these guidelines exist, how they are formu-lated, and the rationale for this latest revision. Wethen note some key changes that will affect yourpatients, as well as practical steps you can take ineveryday practice to help your patients lead fuller,healthier lives through good nutrition.
WHY DIETARY GUIDELINES EXIST
The most recent dietary guidelines can best be un-derstood within the context of their history. It be-
gins in the 1970s, when it had become increasinglyapparent that nutritional advice that focused simplyon getting enough food to eat was not sufficient tomake Americans healthy. Too much food, as well asimbalances between the types and amounts of foodand the nutrients they contained, was creatinghealth problems, including increased risks of severaldiet-related chronic, degenerative diseases. Pressuremounted for more authoritative advice on healthyeating that dealt with these issues.
By this time, Congress and many leading healthexperts had become increasingly convinced thatnational planning required closer synchronizationbetween agricultural and health policies involvingnutrition, especially in those areas involving risksfor chronic degenerative diseases linked to diet. Itwas also noted that authoritative and comprehen-sive dietary guidance to reduce risks of chronic, de-generative diseases was not available. These con-cerns gave rise to a document addressing both issues,
entitled
Dietary Goals for the United States
, whichemerged from hearings of the Senate Select Commit-tee on Nutrition and Human Needs held in the mid1970s. This was a start, but it was evident that amore careful review of the scientific evidence wasneeded before national nutrition goals or guide-lines for individuals could be formulated in a soundmanner.
HOW THE GUIDELINES WERE DEVELOPED
During the Carter administration, the Departmentof Health, Education and Welfare built on theseearly efforts by convening a working group to re-view evidence for associations between certain nu-
Reprint requests to Johanna Dwyer, DSc, RD, New England MedicalCenter, Box 783, 750 Washington Street, Boston, MA 02111. E-mail:[email protected]

360
j
DWYER AND LICHTENSTEIN Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
trients and chronic degenerative disease risks. Thesefindings were published in the peer-reviewed litera-ture. Later on, the Secretaries of Health, Educationand Welfare and the US Department of Agriculture,the cabinet departments with the most direct re-sponsibilities in the area of nutrition, appointed anexpert committee. The committee was asked touse the findings of the conference to craft a docu-ment consumers could use for modifying their indi-vidual diets. The document also was envisioned asbeing potentially useful to policymakers as a guidefor planning nutrition policy. The first set of dietaryguidelines was issued in 1980. By federal mandate,these guidelines are revised every 5 years to keepthe recommendations in step with current science.
In 1998, the Secretaries of Agriculture and Healthand Human Services appointed an Advisory Commit-tee to review the 1995 Dietary Guidelines for Ameri-cans, to determine if a revision was needed and, ifso, to provide recommendations for possible revi-sions. The Dietary Guidelines Advisory Committeeconsisted of American biomedical scientists withspecial expertise in nutrition (Table 1).
After a review of the data, the Advisory Commit-tee determined that the 1995 report did need revi-sion. The process included an exhaustive literaturereview and 4 public meetings to hear testimony,gather evidence, and discuss recent research find-ings. A public comment period was open duringthe entire review process. Consumer focus groupswere commissioned to determine how members ofthe general public interpreted the current (1995)guidelines. The committee then set about to inte-grate all the accumulated material to develop an
updated report that would provide evidence-basedrecommendations for any proposed revisions.
The draft report, which consisted of suggestionsfor revision of the consumer guidance booklet anddocumentation of the rationale for each change, wassubmitted for consideration to the 2 cabinet secretar-ies (Agriculture and Health and Human Services) inDecember of 1999 and posted in the
Federal Regis-ter
for public comment. The comments were re-viewed and the document revised as deemed neces-sary by the cabinet secretaries. The final documentwas issued at the National Nutrition Summit held inWashington, DC, in May 2000. The Dietary Guide-lines are now being disseminated to the public andto government decision makers. The process of har-monizing the report with other federally-issued foodguidance material, such as the Nutrient Label andthe Food Guide Pyramid, has begun.
THE YEAR 2000 DIETARY GUIDELINES
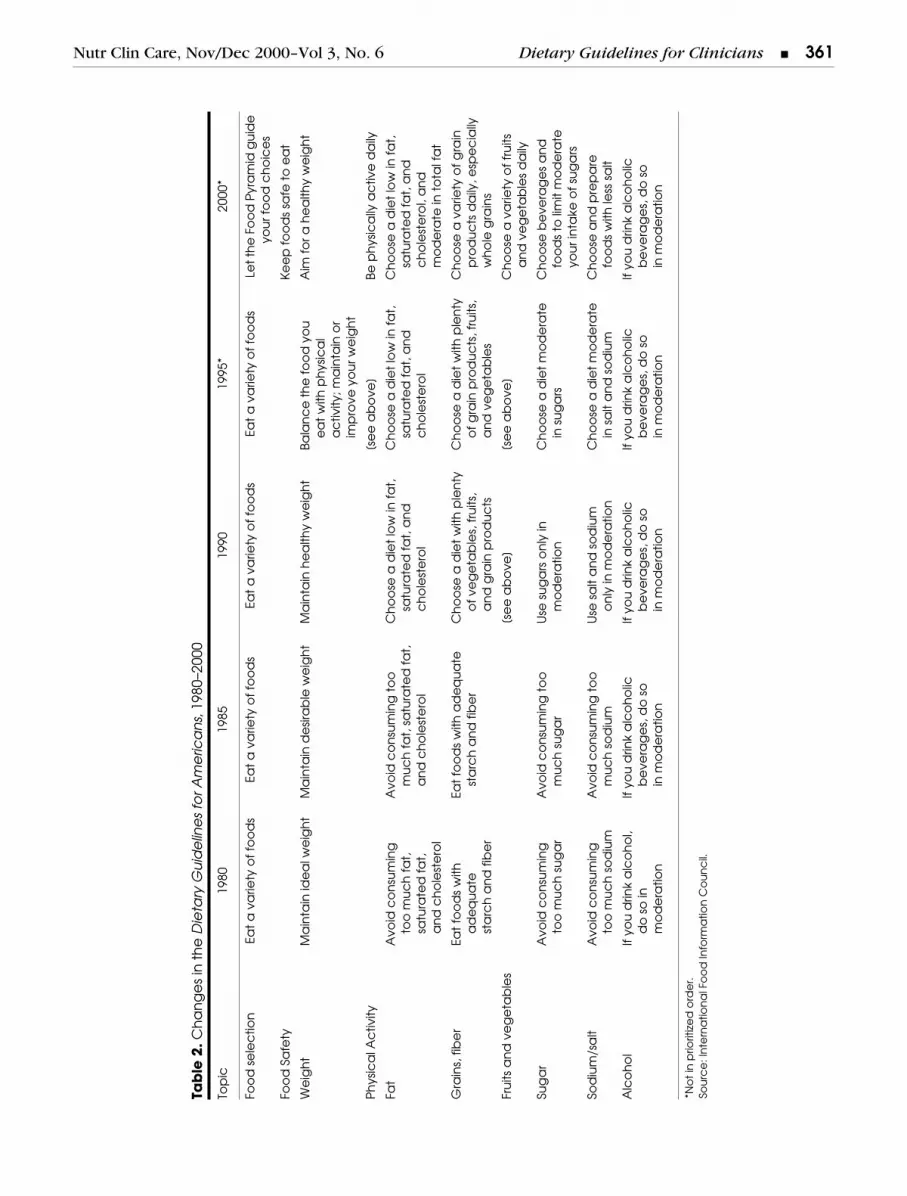
Table 2 allows a comparison of the 2000 guide-lines—the latest step in this evolutionary process—with those of previous years. As the science haschanged over the past two decades, the substanceof the guidelines has changed considerably. Theirtone has also changed; the current guidelines havefewer “don’ts” and more “do’s” than their forebears.
The fundamental message of the 2000 guidelinesis that eating well and regular exercise are essentialfor maintaining good health—and that doing so canbe enjoyable. These messages are summarized inthe guidelines’ “ABCs for good health”—Aim for fit-
Table 1.
Dietary Guidelines 2000 Advisory Committe
Chair Cutberto Garza, MD, PhD, Cornell University, Ithaca, New York
Vice Chair Suzanne Murphy, PhD, RD, University of Hawaii, Honolulu, Hawaii
Members
•
Richard Deckelbaum, MD, College of Physicians and Surgeons of Columbia University, New York, New York
•
Johanna Dwyer, DSc, RD, Tufts University and New England Medical Center, Boston, Massachusetts
•
Scott Grundy, MD, PhD, The University of Texas Southwestern Medical Center at Dallas, Dallas, Texas
•
Rachel Johnson, PhD, MPH, RD, The University of Vermont, Burlington, Vermont
•
Shiriki Kumanyika, PhD, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania
•
Alice H. Lichtenstein, DSc, Tufts University, Boston, Massachusetts
•
Meir Stampfer, MD, DrPH, Harvard University, Boston, Massachusetts
•
Lesley Fels Tinker, PhD, RD, Fred Hutchinson Cancer Research Center, Seattle, Washington
•
Roland Weinsier, MD, DrPH, University of Alabama at Birmingham, Birmingham, Alabama
Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Dietary Guidelines for Clinicians
j
361
Tab
le 2
.
Ch
an
ge
s in
th
e
Die
tary
Gu
ide
line
s fo
r Am
eric
an
s
, 198
0–20
00
Top
ic19
8019
8519
9019
95*
2000
*
Foo
d s
ele
ctio
nEa
t a
va
riety
of
foo
ds
Eat
a v
arie
ty o
f fo
od
sEa
t a
va
riety
of
foo
ds
Eat
a v
arie
ty o
f fo
od
sLe
t th
e F
oo
d P
yra
mid
gu
ide
yo
ur f
oo
d c
ho
ice
s
Foo
d S
afe
tyK
ee
p f
oo
ds
safe
to
ea
t
We
igh
tM
ain
tain
ide
al w
eig
ht
Ma
inta
in d
esir
ab
le w
eig
ht
Ma
inta
in h
ea
lthy
we
igh
tBa
lan
ce
th
e f
oo
d y
ou
ea
t w
ith p
hys
ica
l a
ctiv
ity; m
ain
tain
or
imp
rove
yo
ur w
eig
ht
Aim
fo
r a h
ea
lthy
we
igh
t
Ph
ysic
al A
ctiv
ity[s
ee
ab
ove
]Be
ph
ysic
ally
ac
tive
da
ily
Fat
Avo
id c
on
sum
ing
too
mu
ch
fa
t,
satu
rate
d f
at,
a
nd
ch
ole
ste
rol
Avo
id c
on
sum
ing
to
o
mu
ch
fa
t, s
atu
rate
d f
at,
a
nd
ch
ole
ste
rol
Ch
oo
se a
die
t lo
w in
fa
t,
satu
rate
d f
at,
an
d
ch
ole
ste
rol
Ch
oo
se a
die
t lo
w in
fa
t,sa
tura
ted
fa
t, a
nd
c
ho
lest
ero
l
Ch
oo
se a
die
t lo
w in
fa
t,sa
tura
ted
fa
t, a
nd
c
ho
lest
ero
l, a
nd
m
od
era
te in
to
tal f
at
Gra
ins,
fib
er
Eat
foo
ds
with
a
de
qu
ate
st
arc
h a
nd
fib
er
Eat
foo
ds
with
ad
eq
ua
te
sta
rch
an
d f
ibe
rC
ho
ose
a d
iet
with
ple
nty
o
f ve
ge
tab
les,
fru
its,
an
d g
rain
pro
du
cts
Ch
oo
se a
die
t w
ith p
len
tyo
f g
rain
pro
du
cts
, fru
its,
an
d v
eg
eta
ble
s
Ch
oo
se a
va
riety
of
gra
inp
rod
uc
ts d
aily
, esp
ec
ially
wh
ole
gra
ins
Fru
its a
nd
ve
ge
tab
les
[se
e a
bo
ve]
[se
e a
bo
ve]
Ch
oo
se a
va
riety
of
fru
its
an
d v
eg
eta
ble
s d
aily
Sug
ar
Avo
id c
on
sum
ing
too
mu
ch
su
ga
rA
void
co
nsu
min
g t
oo
m
uc
h s
ug
ar
Use
su
ga
rs o
nly
in
mo
de
ratio
nC
ho
ose
a d
iet
mo
de
rate
in
su
ga
rsC
ho
ose
be
vera
ge
s a
nd
fo
od
s to
lim
it m
od
era
teyo
ur i
nta
ke o
f su
ga
rs
Sod
ium
/sa
ltA
void
co
nsu
min
g
too
mu
ch
so
diu
mA
void
co
nsu
min
g t
oo
m
uc
h s
od
ium
Use
sa
lt a
nd
so
diu
m
on
ly in
mo
de
ratio
nC
ho
ose
a d
iet
mo
de
rate
in s
alt
an
d s
od
ium
Ch
oo
se a
nd
pre
pa
re
foo
ds
with
less
sa
lt
Alc
oh
ol
If yo
u d
rink
alc
oh
ol,
do
so
in
mo
de
ratio
n
If yo
u d
rink
alc
oh
olic
b
eve
rag
es,
do
so
in
mo
de
ratio
n
If yo
u d
rink
alc
oh
olic
be
vera
ge
s, d
o s
oin
mo
de
ratio
n
If yo
u d
rink
alc
oh
olic
b
eve
rag
es,
do
so
in m
od
era
tion
If yo
u d
rink
alc
oh
olic
b
eve
rag
es,
do
so
in m
od
era
tion
*No
t in
prio
ritiz
ed
ord
er.
Sou
rce
: In
tern
atio
na
l Fo
od
Info
rma
tion
Co
un
cil.

362
j
DWYER AND LICHTENSTEIN Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Figure 1. ABC’s for Good Health.

Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Dietary Guidelines for Clinicians
j
363
ness, Build a healthy base, and Choose sensibly.(Figure 1)
AIM FOR FITNESS
Aim for a Healthy Weight
Rationale
There is extensive evidence that excess weight isrelated to increased mortality risk. Overweight isalso associated with morbidity. These risks start torise at more moderate degrees of overweight thanwere previously thought. Even the loss of modestamounts of weight, 10 to 20 pounds, or about 10%to 20% of body weight, can have very striking healthbenefits. The evidence for clinical guidelines on treat-ing obesity has been summarized recently and is con-sistent with these messages.
2
Key Points
Every patient needs to have his or her weight eval-uated to determine if he or she is in the healthyrange. Then he or she should strive to attain ormaintain a healthy weight.
Steps to Take
Calculate your patient’s BMI and measure waist cir-cumference. Multiply weight in pounds by 705. Di-vide by height in inches. Then divide by height ininches again to get the BMI. Be sure also to assessother factors that increase disease risks with over-weight. These include a family or personal historyof heart disease, middle age (males older than 45years or postmenopausal females), smoking, seden-tary lifestyle, high blood pressure, abnormal bloodcholesterol (high LDL-cholesterol, low HDL-choles-terol, and/or high triglycerides), and diabetes. Thepresence of any of these additional factors increasesthe urgency of managing weight or avoiding furthergains. Weight gain (gain of 1 BMI unit or 5 to 10pounds) is also a sign for action to manage weight.
Next, discuss a healthy weight goal that fallswithin the healthy range for the patient. For non-pregnant adults, this healthy range is a BMI from18.5 to 25, with a waist circumference of no morethan 35 inches for women or 40 inches for men. In-dividuals with BMIs greater than 25 should be ad-
vised to lose weight, especially if other risk factorsor a high waist circumference are present; peoplewith BMIs under 25 but with high waist circumfer-ences should be advised to watch their weights.
New in the 2000 guidelines is the goal for everyindividual to achieve a
healthy
weight, not someimpossible-to-reach ideal. The healthy BMI rangeapplies to adults of
all
ages. Most patients have un-realistically low weight goals that may need modifi-cation. Remind patients that small losses, even as lit-tle as 10 to 15 pounds, will make a big difference inhealth risks, and that even a small loss will improveappearance and feelings of wellbeing. Encouragepatients to pick an
achievable
weight goal they canwork toward achieving over the next 6 months.
For patients who don’t feel they can lose weight,the first goal should be to help them to stop gain-ing. Discuss a plan to help them avoid further gains.Once weight gain has stopped, you can help themlose weight gradually. Overweight people with eat-ing disorders and children who are overweightneed special attention.
All overweight patients need suggestions to helpthem get started. The Food Guide Pyramid is a goodguide for building a healthy pattern of meals andsnacks. Stress sensible portion sizes using the FoodGuide Pyramid portions as a starter—these portionsizes are much smaller than most people typicallyeat. Remind your patients that high-fat, high-caloriefoods and alcoholic beverages are easy to consumein excess, so these need special attention. At thesame time, remind patients of the importance ofreading labels: low-fat doesn’t always mean low incalories. Finally, stress a physically active life-stylethat involves moving the body at least 30 minutes aday at moderate activity levels.
Be Physically Active Each Day
Rationale
A sedentary lifestyle increases risks of many chronicdiseases, even for individuals whose weights are atappropriate levels. Regular physical activity not onlyincreases physical fitness but has positive effects onbone health, endurance and muscle strength, well-being, and helps control weight. A recent report ofthe Surgeon General, entitled
Physical Activity andHealth
, provides further support for the importanceof these measures.
3
364
j
DWYER AND LICHTENSTEIN Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Key Points
Adults should aim for 30 minutes of moderate phys-ical activity most days a week. There are even morehealth benefits from increasing the amount of timespent in physical activity, particularly vigorous phys-ical activity, strength and resistance training, andactivities that increase flexibility. Physical activityshould be a regular part of daily life for
everyone
, re-gardless of age.
Steps to Take
Your highest priority should be patients who areextremely sedentary, because such patients run veryhigh risks of health problems as a result of their ha-bitual inactivity. People who walk less than 15 min-utes a day are extremely sedentary. Many older peo-ple are very inactive and individuals with chronicdiseases may feel that physical activity is unsafe forthem; they will need special help.
First, make sure the patient’s medical impedimentsor related risks (eg, heart disease, diabetes, hyperten-sion, or obesity) are taken into account. Then discusswhy physical activity is important and suggest a safeand workable physical-activity plan. For individualswho are very inactive, walking clubs or other struc-tured activities may be useful and even as little as 15minutes a day of walking is a good start.
Gradually increase the exercise recommendationonce the patient becomes more active. Ask your pa-tient to increase his or her daily physical activity by15 minutes; this might include a brisk walk, addi-tional work involving moving objects, or sports suchas dancing, biking, or swimming.
Urge patients who are already active to increaseor maintain their physical activity. Make sure theyinclude not only aerobic physical activity that speedsthe heart rate and breathing and contributes to car-diovascular fitness, but also strength building andflexibility.
Check to see if your patient is doing any strengthor resistance training; if not, suggest some simplesteps such as lifting small weights. Discuss waysthe patient can set a good example for spouses, sig-nificant others, and children by being active. Mostpatients find it easiest to choose structured physi-cal activities that fit into their daily routines. Sug-gest low-cost, structured exercise programs avail-able in your community for those who like groupactivities, or a sound self-help book for those wholike to do things solo. Ask your patient to keep a
physical activity diary for the week before his orher next visit, and go over it together to developfurther suggestions.
A goal for progressing in a more physically ac-tive life is to try to walk 2 miles in 30 minutes. Peo-ple who are trying to lose weight or maintain weightloss may need even more physical activity than this.Patients can increase the health benefits of physicalactivity by spending more time in vigorous physicalactivities.
BUILD A HEALTHY BASE
Let the Pyramid Guide your Food Choices
Rationale
Provide the dietary context in which to assemblespecific guidance on food-based recommendations.
Key Points
Regardless of a patient’s specific eating pattern, agood way to provide general advice on construct-ing a healthy eating plan is to start with the 3 groupsof food at the base of the Food Guide Pyramid (Figure2)—grains, fruits, and vegetables. Within this generalframework, people can make choices that will ac-commodate their cultural, religious, or personal pref-erences. Eating upward from the bottom of the pyra-mid will provide a nutrient-dense foundation for aneating pattern that is moderate in saturated fat,cholesterol, salt, and sugars. In epidemiologic stud-ies, dietary patterns high in grains, fruits, and vege-tables are associated with decreased incidence ofcommon chronic diseases.
Steps to Take
Urge patients to consume foods from the differentcategories within the Food Guide Pyramid. Empha-size a broad range of grain products, fruits, and veg-etables.
Remember that there are many different health-ful eating patterns. People who are unwilling, or un-able, to consume foods from one of the food groupsshould be encouraged to choose alternatives. For ex-ample, if a patient does not, or cannot, consume milkand milk products, he or she should choose alternatesources of dietary calcium (ie, soy-based beverageswith added calcium, tofu made with calcium sulfate,breakfast cereals with added calcium, canned fishwith bones, fruit juice with added calcium, and dark-

Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Dietary Guidelines for Clinicians
j
365
green leafy vegetables). Guidance for such accom-modations can be found in the Dietary Guidelinesdocument.
Explain that many individual foods can makemultiple contributions to helping patients reachthe recommended number of daily servings in a va-riety of food groups in the Food Guide Pyramid.For example, a chicken sandwich may include serv-ings of bread, meat, and vegetables (eg, lettuce).
Often, serving sizes for commonly consumed foodsare larger than that defined as a “serving size” withinthe Food Guide Pyramid. It is important to emphasizethat in order to stay in energy balance, your patientsneed to moderate both number of servings and serv-ing size. Too much of anything, even “healthy” foods,can result in weight gain.
Typical serving sizes, USDA Pyramid serving sizes,serving sizes as defined on food labels, and servingsizes of common foods served in restaurants are of-ten different. For example, on the label, one servingof pasta is defined as 1 cup. But on the Food GuidePyramid, one serving of pasta is defined as just 1/2cup—far less than most people eat at a single meal.Table 3 lists Food Guide Pyramid serving sizes for anumber of foods from each food group.
The consumer document has specific, practicaladvice on food sources of nutrients that are fre-quently low in the diet. Individuals in certain vul-nerable groups should consult this advice. For ex-ample, adolescents and adults over the age of 50
years have especially high needs for calcium. How-ever, dairy products and other sources of calciumshould be low fat or fat free to keep saturated fatintakes low. Additional and/or alternative sourcesof calcium should be encouraged (see above).
Other nutrients of concern to specific groups ofindividuals include iron in young children, teenagegirls, and women of childbearing age; folate in womenof childbearing age; and vitamin D and B
12
in olderadults. Most of these needs can be met through diet.However, women who could become pregnant mayneed folate supplements or folate-fortified foods. Simi-larly, older adults and people with little exposure tosunlight may need supplementary vitamin D; peoplewho seldom eat dairy products or other rich sourcesof calcium need calcium-fortified foods or supple-ments; and people who eat no animal foods or whoare over 50 years old, may require Vitamin B
12
sup-plements. However, nobody should depend onsupplements to meet basic nutritional needs. Stressfoods first.
Choose a Variety of Grains Daily, Especially Whole Grains
Rationale
Grain products form the foundation of the diet, be-cause they provide vitamins, minerals, carbohydrates(starch and dietary fiber), and other substances thatare important for good health.
Figure 2. Food Guide Pyramid: a guide to dailyfood choices.
366
j
DWYER AND LICHTENSTEIN Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Key Points
Grain products tend to be low in fat, unless fat isadded during the processing. Therefore, they arenot calorie dense. Whole-grain products, as well asfruits and vegetables, are especially rich in dietaryfiber and, possibly, in other protective substances.Federal regulations ensure that refined-grain prod-ucts are enriched with added thiamin, riboflavin,niacin, and iron, and, more recently, fortified withfolic acid.
Steps to Take
Encourage the use of a variety of grain products,both whole grain and fortified. Emphasize whole
grains because consumption of such products typi-cally is low, and increasing it may confer specialhealth benefits. In additional to whole wheat, you canencourage consumption of a wide variety of whole-grain products, including brown rice, bulgur (crackedwheat), graham flour, oatmeal or whole oats, popcornor other whole corn products, pearl barley, and wholerye. Ingredient labels on packaged foods can help pa-tients select products made with whole grains. Thosethat list whole wheat or whole grain first, or as thesole grain ingredient, are high in whole grains. TheNutrient Facts panel can help patients comparethe relative amounts of fiber per serving of commonfoods.
Choose a Variety of Fruits and Vegetables Daily
Rationale
A diet high in fruits and vegetables may protectagainst chronic disease, promote healthy bowel func-tion, and provide essential vitamins and minerals, fi-ber, and other substances that are important for goodhealth.
Key Points
Each category of fruits and vegetables is rich in dif-ferent nutrients, but none is rich in all nutrients.For example, citrus fruits are a good source of vita-min C, while winter squash is a good source of vita-min A (carotenoids). Therefore, it is best to eat arange of fruits and vegetables.
Steps to Take
Fruits and vegetables aren’t good for you only whenfresh; fresh, frozen, dried, or canned fruits and veg-etables, as well as juice, are healthful also. How-ever, it is important to note that juice lacks the fi-ber normally present in the other forms of fruitsand vegetables and often is high in calories. Whenbuying prepared vegetable and fruit items, the Nu-trient Facts panel and ingredient statement on foodlabels can help patients determine whether the prod-uct is high in added sugar, fat, or salt. Since manyAmericans’ fruit and vegetable intakes are low, pa-tients should be encouraged to try new ways of eat-ing these foods (eg, incorporated into food mixturessuch as meat loaf or soup, or as toppings on pizza).Tell patients to make it a habit to include fruits andvegetables with meals and to use them as snacks.
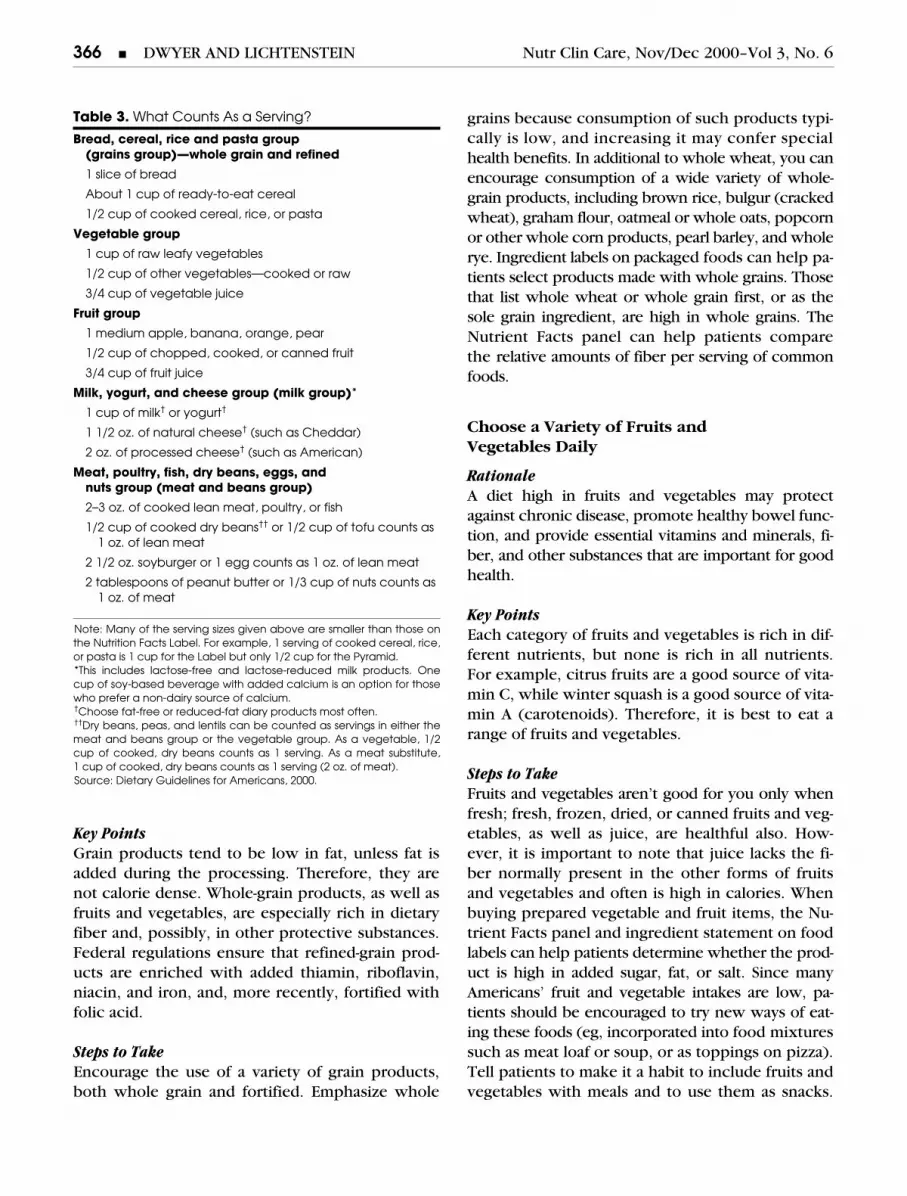
Table 3.
What Counts As a Serving?
Bread, cereal, rice and pasta group(grains group)—whole grain and refined
1 slice of bread
About 1 cup of ready-to-eat cereal
1/2 cup of cooked cereal, rice, or pasta
Vegetable group
1 cup of raw leafy vegetables
1/2 cup of other vegetables—cooked or raw
3/4 cup of vegetable juice
Fruit group
1 medium apple, banana, orange, pear
1/2 cup of chopped, cooked, or canned fruit
3/4 cup of fruit juice
Milk, yogurt, and cheese group (milk group)
*
1 cup of milk
†
or yogurt
†
1 1/2 oz. of natural cheese
†
(such as Cheddar)
2 oz. of processed cheese
†
(such as American)
Meat, poultry, fish, dry beans, eggs, and nuts group (meat and beans group)
2–3 oz. of cooked lean meat, poultry, or fish
1/2 cup of cooked dry beans
††
or 1/2 cup of tofu counts as 1 oz. of lean meat
2 1/2 oz. soyburger or 1 egg counts as 1 oz. of lean meat
2 tablespoons of peanut butter or 1/3 cup of nuts counts as 1 oz. of meat
Note: Many of the serving sizes given above are smaller than those onthe Nutrition Facts Label. For example, 1 serving of cooked cereal, rice,or pasta is 1 cup for the Label but only 1/2 cup for the Pyramid.*This includes lactose-free and lactose-reduced milk products. Onecup of soy-based beverage with added calcium is an option for thosewho prefer a non-dairy source of calcium.
†
Choose fat-free or reduced-fat diary products most often.
††
Dry beans, peas, and lentils can be counted as servings in either themeat and beans group or the vegetable group. As a vegetable, 1/2cup of cooked, dry beans counts as 1 serving. As a meat substitute,1 cup of cooked, dry beans counts as 1 serving (2 oz. of meat).Source: Dietary Guidelines for Americans, 2000.

Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
Dietary Guidelines for Clinicians
j
367
The goal is at least 2 servings of fruit and 3 servingsof vegetables per day. The more colorful fruits andvegetables frequently are the most nutrient dense,and, thus, deserve special attention.
Keep Food Safe to Eat
Rationale
Food-borne disease is a major source of preventableillness. Although food-safety problems often arise far-ther back in the food chain, recent evidence showsthat food preparation and storage practices at home,as well as lack of precautions when eating out, alsocontribute to risks of food-borne illness.
Key Points
People need to keep foods safe to eat at home andwhen eating out. Table 4 provides a home food-safety checklist. Some people are at special risk,and they need to take extra precautions.
Steps to Take
Focus first on your patients who are at highest riskof food-borne illness. These include pregnant women,older persons, and those with weakened immune sys-tems, such as those undergoing chemotherapy and in-dividuals who are HIV positive. Urge these patients todo a safety check on the way their food is handled athome—especially perishable foods such as eggs,meats, poultry, fish, shellfish, milk products, andfresh fruits and vegetables. The Dietary Guidelinesconsumer booklet provides some specific points tocheck. Suggest that high-risk patients buy anduse food thermometers to make sure that foods arecooked to safe temperatures. People at high risk alsoshould avoid unpasteurized juices and milk products,raw sprouts, undercooked or raw meat, poultry, eggs,
fish, and shellfish. They also should be especially care-ful when eating out to make sure that foods are thor-oughly cooked and served piping hot. All patientsneed to remember to play it safe; if they have doubtswhen shopping or eating out, they should choosesomething else.
CHOOSE SENSIBLY
Choose a Diet that Is Low in Saturated Fat and Cholesterol and Moderate in Total Fat
Rationale
Fats are important sources of energy and essentialfatty acids. They are critical for the absorption offat-soluble vitamins (vitamins A [carotenoids], D, Eand K). Saturated fat intake has been steadily declin-ing in the US, but it is still higher than currently rec-ommended (
,
10% of energy from saturates,
,
30%of energy from all sources of fat). In some individu-als, very low-fat diets (
,
20% of energy from fats)may result in increased blood triglycerides and de-creased HDL-cholesterol levels. This is why the cur-rent Dietary Guidelines shifted the emphasis fromlow-total-fat diets to low-
saturated-
fat and low-cho-lesterol diets.
Key Points
It is the
type
of fat (ie, saturated fat) and choles-terol, rather than the total
amount
of fat, that ismost closely related to the risk of developing car-diovascular disease. “Fat-free” or “low-fat” does notnecessarily indicate products that are more nutri-tious or, for that matter, lower in calories than theirfull-fat counterparts. Exceptions are low-fat and fat-free dairy and meat products, where the reductionin fat is primarily in saturated fat, and where othercaloric sources (ie, sugars) are not added.
Steps to Take
Make sure your patient understands that not all fatsare the same—foods high in saturated fats,
trans
fats, and cholesterol increase blood cholesterol lev-els. Saturated fats and cholesterol are found prima-rily in fats of animal origin (meat and dairy prod-ucts), and saturated fats are also present in tropicaloils (coconut, palm, and palm kernel oils). Dietarycholesterol is found only in foods of animal origin,especially eggs.
Trans
fatty acids are found in lowlevels in meat and dairy products and at variable
Table 4.
Home Food-Safety Checklist
Clean:
Wash hands and surfaces often when preparing food
Separate:
Separate raw, cooked, and ready-to-eat foods while shopping, preparing, or storing
Cook:
Cook foods to safe temperatures
Chill: Refrigerate perishable foods promptly
Follow the label: Food labels have instructions that can help keep foods safe
Serve safely: Keep hot foods hot and cold foods cold when serving
If in doubt, throw it out
368 j DWYER AND LICHTENSTEIN Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
levels in hydrogenated fats or products made fromthem (such as vegetable shortening and some stickmargarines, which are high in trans fats). Commer-cially fried foods and baked products account formost trans fatty acids consumed in the UnitedStates.
Unsaturated, fat-rich foods (high monounsaturatedor polyunsaturated fat) decrease blood cholesterollevels, especially polyunsaturates. Unsaturated fats arefound mainly in vegetable oils (except tropical oils)and products made from these oils, such as full-fatsalad dressings. Oils high in monounsaturated fatty ac-ids include canola and olive oils; oils high in polyun-saturated fatty acids are soybean and corn oils.
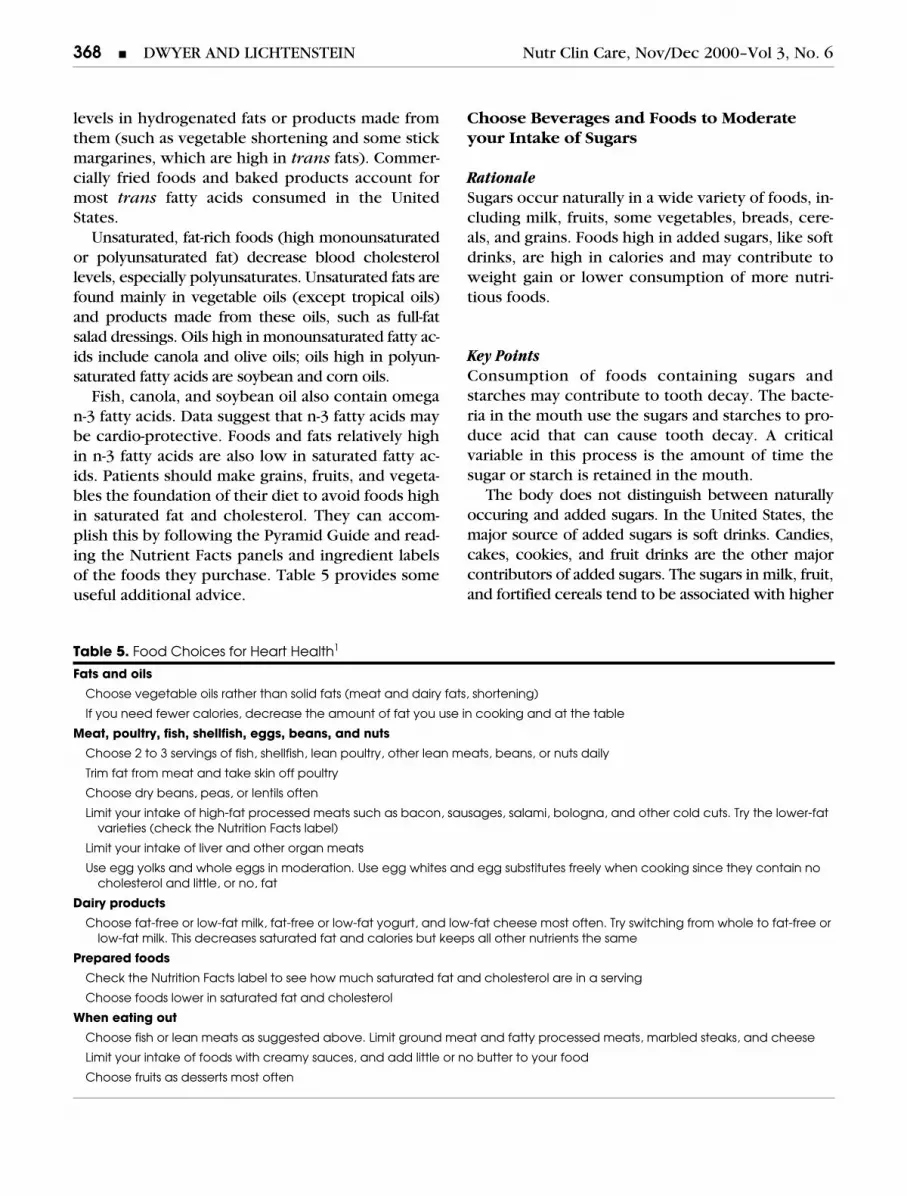
Fish, canola, and soybean oil also contain omegan-3 fatty acids. Data suggest that n-3 fatty acids maybe cardio-protective. Foods and fats relatively highin n-3 fatty acids are also low in saturated fatty ac-ids. Patients should make grains, fruits, and vegeta-bles the foundation of their diet to avoid foods highin saturated fat and cholesterol. They can accom-plish this by following the Pyramid Guide and read-ing the Nutrient Facts panels and ingredient labelsof the foods they purchase. Table 5 provides someuseful additional advice.
Choose Beverages and Foods to Moderate your Intake of Sugars
RationaleSugars occur naturally in a wide variety of foods, in-cluding milk, fruits, some vegetables, breads, cere-als, and grains. Foods high in added sugars, like softdrinks, are high in calories and may contribute toweight gain or lower consumption of more nutri-tious foods.
Key PointsConsumption of foods containing sugars andstarches may contribute to tooth decay. The bacte-ria in the mouth use the sugars and starches to pro-duce acid that can cause tooth decay. A criticalvariable in this process is the amount of time thesugar or starch is retained in the mouth.
The body does not distinguish between naturallyoccuring and added sugars. In the United States, themajor source of added sugars is soft drinks. Candies,cakes, cookies, and fruit drinks are the other majorcontributors of added sugars. The sugars in milk, fruit,and fortified cereals tend to be associated with higher
Table 5. Food Choices for Heart Health1
Fats and oils
Choose vegetable oils rather than solid fats (meat and dairy fats, shortening)
If you need fewer calories, decrease the amount of fat you use in cooking and at the table
Meat, poultry, fish, shellfish, eggs, beans, and nuts
Choose 2 to 3 servings of fish, shellfish, lean poultry, other lean meats, beans, or nuts daily
Trim fat from meat and take skin off poultry
Choose dry beans, peas, or lentils often
Limit your intake of high-fat processed meats such as bacon, sausages, salami, bologna, and other cold cuts. Try the lower-fat varieties (check the Nutrition Facts label)
Limit your intake of liver and other organ meats
Use egg yolks and whole eggs in moderation. Use egg whites and egg substitutes freely when cooking since they contain no cholesterol and little, or no, fat
Dairy products
Choose fat-free or low-fat milk, fat-free or low-fat yogurt, and low-fat cheese most often. Try switching from whole to fat-free or low-fat milk. This decreases saturated fat and calories but keeps all other nutrients the same
Prepared foods
Check the Nutrition Facts label to see how much saturated fat and cholesterol are in a serving
Choose foods lower in saturated fat and cholesterol
When eating out
Choose fish or lean meats as suggested above. Limit ground meat and fatty processed meats, marbled steaks, and cheese
Limit your intake of foods with creamy sauces, and add little or no butter to your food
Choose fruits as desserts most often

Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6 Dietary Guidelines for Clinicians j 369
amounts of other nutrients than the sugars in theseother foods.
Steps to TakeUrge patients to choose foods and drinks sensiblyto limit their intake of sugars. This can be accom-plished by getting the majority of calories from grains(especially whole grains), fruits and vegetables, low-fat and fat-free dairy products, and lean meats ormeat substitutes. Foods and drinks high in added sug-ars, such as soft drinks and sweets, should not besubstituted for foods that are high in other nutrientsas well (ie, milk, fruit). Patients of all ages should befamiliar with oral hygiene techniques to maintainhealthy gums and teeth (ie, minimize between-mealsnacks containing sugars and starches, swish aftereating, brush at least twice per day, discuss dental hy-giene with dentist). Patients should be made awareof the synonyms for added sugar used on food labels.These include: brown sugar, corn sweetener, cornsyrup, dextrose, fructose, fruit juice concentrate, glu-cose, high-fructose corn syrup, honey, invert sugar,lactose, maltose, malt syrup, molasses, raw sugar, su-crose, syrup, and table sugar.
Choose and Prepare Foods with Less Salt
RationaleSalt intake is associated with high blood pressureand with calcium excretion in the urine.
Key PointsThere is good evidence that some people are saltsensitive—that is, their blood pressure increaseswith increased salt intake. Unfortunately, there isno simple laboratory test that can identify truly salt-sensitive individuals. However, since consuming lesssalt is good for everyone, in addition to having spe-cial benefits for some, it is a good idea for everyoneto consume less salt. (For hypertensive individualswho are overweight, weight reduction can also help,but many individuals who are hypertensive are notoverweight.)
Since most Americans already get more sodiumthan they need, it is healthier to learn to eat foodswith more of their natural flavor, without addingsalt. However, much of the salt we eat comes hid-den in prepared foods. Therefore, it is also criticalto choose and prepare foods that are low in salt.
Steps to TakeUrge patients who still salt their foods to cut downon how much they use and to use herbs, spices,and fruits to flavor their foods instead. Salt is foundmainly in processed and prepared foods, so eatingless of these can help reduce salt in the diet. Manyprepared foods are now available in reduced-or low-salt versions and are the preferable choices. In addi-tion to the front of the food package, the NutritionFacts label on processed foods can help to identifyfoods that are lower in sodium.
One of the major sources of sodium in most Ameri-can diets is restaurant food or fast foods. Some restau-rants now have identified “healthier” selections thatare low in sodium and saturated fat; these menu itemsare good choices. The DASH (Dietary Approaches toStop Hypertension) diet, which is high in fruit andvegetables and low in fat, has been shown to havepositive effects on blood pressure lowering, espe-cially when it includes lowered sodium intakes.4–6
If You Drink Alcoholic Beverages, Do So in Moderation
RationaleAlcohol can be considered both a food—in that itprovides food energy and few other nutrients—anda drug that can have powerful effects, particularlyin some individuals.
Key Points“Moderation” in alcohol intake is defined as no morethan 1 drink per day for women and 2 for men; thedifferences in tolerance are mainly due to sex differ-ences in body size and water (lean muscle mass).
Steps to TakeSome patients should not drink at all, and theyshould be advised accordingly. Patients who shouldnot drink fall in two categories. First are patientswith certain easily identifiable characteristics. Thesepersons include children, adolescents, individualswho cannot restrict their drinking to moderate lev-els, and women who may become pregnant or whoare pregnant. Older persons have a reduced toler-ance for alcohol since their lean muscle mass islower, and they should be counseled to be moder-ate in their drinking. A second category of patients

370 j DWYER AND LICHTENSTEIN Nutr Clin Care, Nov/Dec 2000–Vol 3, No. 6
who need to take special care with alcohol arethose taking certain prescription drugs or over-the-counter medications that interact with alcohol.Check to make sure that these patients recognizethat they are at risk, and do a quick review of theprimary over-the-counter medications that com-monly cause interactions with alcohol. All patientsneed to understand that alcohol can affect their at-tention span and motor skills, and that they shouldnot drink when they plan to drive, operate machin-ery, or engage in other activities that require atten-tion and skill.
CONCLUSIONS
The Dietary Guidelines consumer booklet, the Nu-trient Facts label and the Food Guide Pyramid arethree essential tools for good nutrition and healththat can be recommended to all of your patients.Patients who need additional dietary modificationsshould be referred to a registered dietitian. Freecopies of the Dietary Guidelines are available bycalling 1-888-878-3256. It can also be downloadedfrom the USDA Web site.7 The evidence-based ra-tionale for the Guidelines is also available.8
Johanna Dwyer, DSc, RD is a member of the Scien-tific Advisory Board, Ocean Spray Inc. Alice H. Lich-tenstein, DSc has indicated no significant relation-ships with commercial supporters.
This article was funded in part by a contract betweenthe US Department of Agriculture and Tufts Univer-sity under contract 58-1950-9. Any opinions, find-ings, conclusions, or recommendations expressed inthis publication are those of the authors and do not
necessarily reflect the views of the US Department ofAgriculture.
REFERENCES
1. US Department of Agriculture, US Department ofHealth and Human Services. Nutrition and Your Health:Dietary Guidelines for Americans. Home and GardenBulletin No 232, 5th ed. Washington, DC: US Depart-ment of Agriculture; 2000.
2. National Institute of Health, National Heart, Lung,and Blood Institute. Clinical Guidelines on the Identifi-cation, Evaluation, and Treatment of Overweight andObesity in Adults: The Evidence Report. Bethesda, MD:National Heart, Lung, and Blood Institute, National Insti-tute of Health, US Public Health Service; 1998.
3. US Department of Health and Human Services.Physical Activity and Health: A Report of the SurgeonGeneral US Department of Health and Human Ser-vices. Publication S/N 017-023-00196-5. Washington, DC:US Government Printing Office, 1996.
4. Appel LJ, Moore TJ, Obarzanek E, et al. A clinicaltrial of the effects of dietary patterns on blood pressures:DASH Collaborative Research Group. N Engl J Med. 1997:336;1117–1124.
5. McCarron DA. Diet and blood pressure: The para-digm shift. Sci. 1998:281;933–934.
6. Svetky LP, Sacks FM, Obarzanek EP, et al. TheDASH diet, sodium intake and blood pressure trail(DASH-Sodium): Rationale and design. J Am Diet Assoc.1999;99:596–604.
7. USDA Dietary Guidelines for Americans 2000Available at: http://www.usda.gov/cnpp/Pubs/DG2000/Index.htm. +-, 2000.
8. Dietary Guidelines Advisory Committee 2000. Re-port of the Dietary Guidelines Advisory Committee onthe Dietary Guidelines for Americans, 2000. Beltsville,MD: US Department of Agriculture, Agricultural ResearchService; 2000.