a prospective study of estimated glomerular filtration rate and outcomes in patients with atrial...
TRANSCRIPT
Online First articles are not copyedited prior to posting.
©American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the
American College of Chest Physicians. See online for more details.
ONLINE FIRST
This is an Online First, unedited version of this article. The final, edited version will appear in a numbered issue of CHEST and may contain substantive
changes. We encourage readers to check back for the final article. Online First papers are indexed in PubMed and by search engines, but the information, including the final title and author list, may be updated on final publication.
http://journal.publications.chestnet.org/
Page 1 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

1
A prospective study of estimated glomerular filtration rate and outcomes in
patients with atrial fibrillation: The Loire Valley Atrial Fibrillation Project
Amitava Banerjee MPH DPhil1 [email protected]
Laurent Fauchier MD PhD4 [email protected]
Patrick Vourc'h PhD3 [email protected]
Christian R. Andres MD, PhD3
Sophie Taillandier MD4
Jean Michel Halimi* MD PhD2
Gregory Y. H. Lip* MD1 [email protected]
[*joint senior authors]
1 University of Birmingham Centre for Cardiovascular Sciences, City Hospital, Birmingham B18
7QH, UK; 2Service de Nephrologie-Immunologie Clinique, Hðpital Bretonneau and Université
François Rabelais, Tours, France; 3Laboratoire de Biochimie et Biologie moléculaire, Hôpital
Bretonneau, Centre Hospitalier régional et Universitaire de Tours; 4
Service de Cardiologie, Pôle
Coeur Thorax Vasculaire, Centre Hospitalier, Universitaire Trousseau et Faculté de Médecine,
Université François Rabelais, Tours, France
Corresponding author
Prof GYH Lip ([email protected]), University of Birmingham Centre for Cardiovascular
Sciences, City Hospital, Birmingham B18 7QH, UK
Running title: Estimated glomerular filtration rate in patients with AF
Page 2 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
2
Abstract
Background: Patients with chronic kidney disease (CKD) are more likely to develop atrial
fibrillation(AF) than individuals with normal renal function, and are more likely to suffer ischaemic
stroke(IS)/thromboembolism(TE). No prior study has considered the impact of eGFR on bleeding.
We investigated the relationship of eGFR to IS/TE, mortality and bleeding in an AF population,
unrestricted by age or comorbidity.
Methods: Patients with non-valvular AF (NVAF) were stratified into five categories according to
eGFR(ml/min/1.73 m2): ≥90,60-89,30-59,15-29 and <15, analysing risk factors, all-cause mortality,
bleeding and IS/TE. Of 8962 eligible individuals, 5912 had NVAF and available serum creatinine
data, with 14499 patient-years of follow-up.
Results: In non-anticoagulated and anticoagulated individuals, the incidence rates of IS/TE were
7.4 and 7.2 per 1000 person-years, respectively. Rates of all-cause mortality were 13.4 and 9.4 per
1000 person-years, respectively, and of major bleeding, 6.2 and 9.0 per 1000 person-years,
respectively.
Rates increased with decreasing eGFR with IS/TE rates being lower in individuals receiving OAC.
eGFR was not an independent predictor of IS/TE on multivariate analyses. When the benefit of IS
reduction is balanced against the increased risk of haemorrhagic stroke, the net clinical benefit
(NCB) was clearly positive in favour of OAC use.
Conclusion: Incidence rates of IS/TE, mortality and bleeding increased with reducing eGFR, across
the whole range of renal function. OAC use was associated with a lower incidence of IS/TE and
mortality at 1 year, compared with non-anticoagulated individuals in all categories of renal function
as measured by eGFR. The NCB balancing IS against serious bleeding was positive, in favour of
OAC use amongst patients with renal impairment.
Key words:
estimated glomerular filtration rate, atrial fibrillation, stroke, bleeding, renal impairment, survival
Page 3 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
3
Abbreviations and Acronyms
NVAF Non-valvular atrial fibrillation
TE Thromboembolism
IS Ischaemic stroke
CHADS2 Acronym for Congestive heart failure, Hypertension, Age ≥75 years,
Diabetes, previous Stroke
CHA2DS2-VASc Acronym for Congestive heart failure, Hypertension, Age ≥75 years,
Diabetes, previous Stroke, Vascular disease, Age 65-74 years, Sex
category (female)
HAS-BLED Hypertension, Abnormal renal/liver function, Stroke, Bleeding history
or predisposition, Labile international normalized ratio, Elderly (> 65
years), Drugs/alcohol concomitantly
VKA Vitamin K antagonist
OAC Oral anticoagulation
eGFR Estimated glomerular filtration rate
Page 4 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
4
Introduction
Impairment of renal function and atrial fibrillation (AF) are both independently associated with
poor cardiovascular outcomes and all-cause mortality, presenting a growing global burden of
disease1-12
. Moreover, AF and chronic kidney disease (CKD) share several risk factors, including
age, hypertension, history of vascular disease and diabetes mellitus. Thus, improved understanding
of the associations between renal function and AF may lead to new approaches in risk stratification,
management and prevention.
Individuals with CKD are more likely to develop AF13-14
, ischaemic stroke(IS) and
thromboembolism(TE)15
than patients with normal renal function. In a large prospective study of
132,372 Danish individuals with AF, where 3587 individuals had CKD, the latter was associated
with increased risk of IS/TE and bleeding16
, thus confirming observations of previous smaller
studies17-21
. However, the study by Olesen et al16
was a nationwide registry cohort, which only
categorised patients as “no renal disease”, “non-end stage CKD” and “renal replacement therapy”.
In clinical practice, renal function is quantified by urinary creatinine clearance or by the estimated
glomerular filtration rate (eGFR)22-24
. Only two previous studies have considered the association
between eGFR and stroke/TE15, 25
, including only time off oral anticoagulation (OAC). No
epidemiologic studies have considered the impact of eGFR on major bleeding and all long-term
outcomes concurrently, nor included individuals with AF regardless of OAC use2-4, 16, 26
. Therefore
the balance between risk of IS/TE and bleeding has not been quantified by eGFR in a large ‘real
world’ population of individuals with AF.
Of note, renal failure is included as a dichotomous variable in risk prediction tools for bleeding but
is rarely included in guideline-recommended risk prediction tools for IS/TE21, 25, 27-30
, which is
supported by a recent analysis in our cohort which proved that renal impairment and eGFR do not
improve risk prediction of IS/TE31
. However, this analysis also showed that renal impairment was
associated with higher rates of IS/TE, compared to normal renal function. Better understanding of
the impact of renal function and eGFR on clinical outcomes in AF is required.
In a population of individuals with AF, unrestricted by age or comorbidity, we conducted the first
prospective study of renal function, as measured by eGFR, on IS/TE, mortality and bleeding.
Page 5 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

5
Among patients with renal impairment taking OAC, we also assessed the net clinical benefit (NCB)
of ischaemic stroke reduction balanced against the increased risk of haemorrhagic stroke.
Methods
The methods of the Loire Valley Atrial Fibrillation Project have been previously reported31-32
.
Extended methods for the present paper are shown in the Web-only Appendix.
Patients with non-valvular AF (NVAF) or atrial flutter diagnosed by the cardiology department
between 2000-2010 were identified (Figure 1). The CHADS228
and CHA2DS2-VASc29
scores were
calculated following the first diagnosis of AF during hospital admission, as was the HAS-BLED21
score. During follow-up, information on outcomes of TE, stroke (ischaemic or haemorrhagic),
major bleeding, and all-cause mortality were recorded by active surveillance of hospital
administrative data. The study was approved by the Review Board of the Pole Coeur Thorax
Vaisseaux from the Trousseau University Hospital in 2010 (December 7th, 2010).
Assessment of renal function
Renal failure was defined as reported history of renal failure, or baseline serum creatinine level
of >133µmol/L in men and >115µmol/L in women33
. In order to convert serum creatinine from
µmol/L to mg/dL, the former was divided by a conversion factor of 88.4. Current consensus
guidelines state that prediction equations have greater consistency and accuracy than serum
creatinine in the assessment of GFR22-24, 34-36
. In addition, prediction equations are equivalent or
better than 24-hour urine creatinine clearance in all but one study22-24, 37
. In adults, the most widely-
used and validated method for estimating GFR from serum creatinine level is the isotope dilution
mass spectrometry (IDMS)-traceable Modification of Diet in Renal Disease (MDRD) Study
equation22-24
. The laboratories where biochemical analysis of creatinine levels was conducted were
calibrated to be IDMS-traceable. The MDRD equation was preferred to the more recently validated
“CKD-Epi” equation38
because there were very few patients aged≥75 years in cohorts used to
validate this equation whereas the current study population was unrestricted by age.
eGFR = 175 x (Scr)-1.154 x (Age)-0.203 x (0.742 if female) x (1.212 if African American)
Page 6 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
6
where eGFR is the estimated glomerular filtration rate in mL/min/1.73 m2, Scr is serum creatinine
level in mg/dL. The African population in the study population was <1% and therefore no
correction factor for ethnicity was required in the MDRD calculation of eGFR.
Statistical analysis
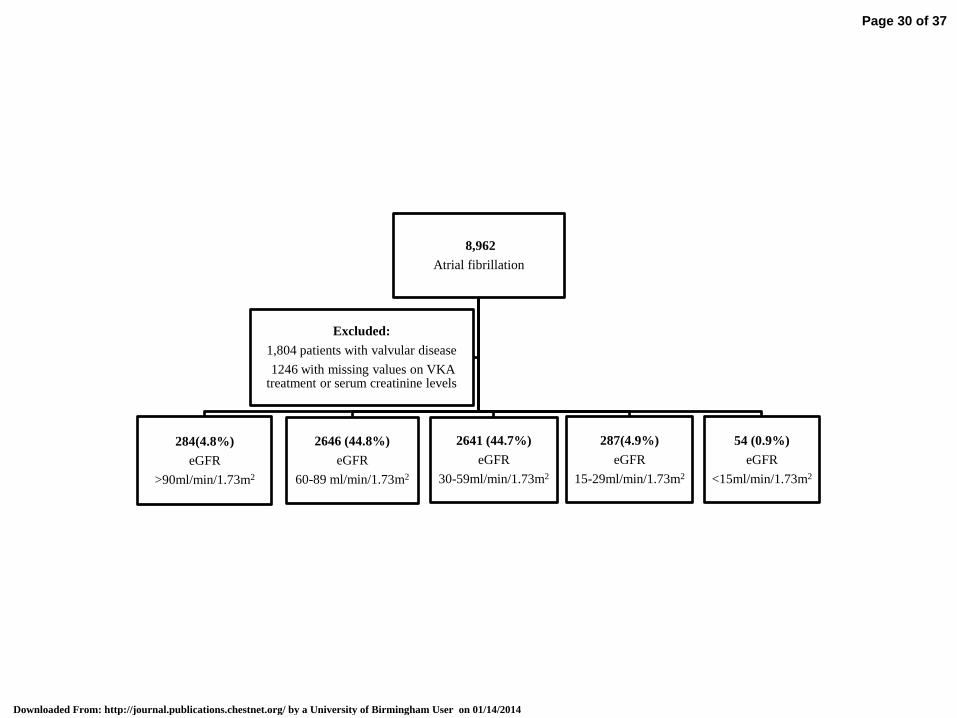
The study population was stratified into five categories according to eGFR (in ml/min/1.73 m2),
corresponding to the stages of CKD: ≥90, 60-89, 30-59, 15-29, and <15 (Figure 1)22-24
. Since data
regarding proteinuria was not available, stage of renal impairment could not be defined. Baseline
characteristics were determined separately for the five eGFR strata, and differences were
investigated using chi-squared test for categorical covariates and Kruskal-Wallis test for continuous
covariates. Age-adjustment was performed by including age as a covariate in a logistic regression
model.
Cumulative incidence rates of IS/TE, bleeding and all-cause mortality were calculated for all
patients by eGFR category, stratifying by presence or absence of VKA therapy. Since VKA therapy
was the only form of OAC used during the study period, the terms, “VKA” and “OAC” are used
interchangeably in the analyses. Due to low numbers of patients and outcomes in the categories
with eGFR≥90 and <15 ml/min/1.73m2, rates were calculated for categories with eGFR≥60, 30-59
and <30 ml/min/1.73m2. Haemorrhagic strokes were excluded from analyses of “stroke” or
“stroke/TE”. Event rates were also calculated by age and sex categories. In each eGFR category,
Cox-proportional hazards analyses were performed to calculate 1-year survival for IS/TE, bleeding
and all-cause mortality. Bivariate analyses of event rates in different subgroups were used to
calculate hazard ratios associated with renal impairment and eGFR category.
Cox proportional-hazard regression models were constructed to investigate whether renal
impairment and eGFR were independent predictors of IS/TE. The risk associated with renal
impairment and eGFR were estimated in a univariate analysis, as well as a sex- and age-adjusted
analysis, an analysis adjusted for the risk factors included in the CHADS2 score, and a multivariate
analysis adjusted for all baseline characteristics in Table 1. All analyses were repeated by eGFR
category, and by combined stratification by renal impairment and eGFR. Further, to test whether the
results were influenced by patients initiating treatment with VKA, we performed additional
analyses excluding patients at the initiation of such treatment.
Page 7 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
7
Finally, the net clinical benefit (NCB) was calculated, as originally proposed by Singer and
colleagues39
using the formula:
Net clinical benefit (NCB) = IS rate on no treatment- IS rate on anticoagulant)-1.5(ICH rate on no
treatment- ICH rate on anticoagulant
…. where IS=ischaemic stroke and ICH=intracerebral haemorrhage, which is the most serious form
of bleeding associated with OAC use. A modified formula with “haemorrhagic stroke” instead of
“ICH” was used to calculate NCB for the different eGFR categories. The NCB is used by clinicians
and researchers as a validated method of balancing risk of ischaemic stroke against intracerebral
haemorrhage.
A two-sided p-value <0.05 was considered statistically significant.
Page 8 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
8
Results
Of 8962 eligible individuals, 5912 (66.0%) had non-valvular AF and available serum creatinine
data, allowing the eGFR to be calculated (Figure 1). Thus, 14499 patient-years of follow-up were
included in the analysis, with mean follow-up of 2.45 (SD 3.56) years. We focused on the 1-year
outcomes in our analyses.
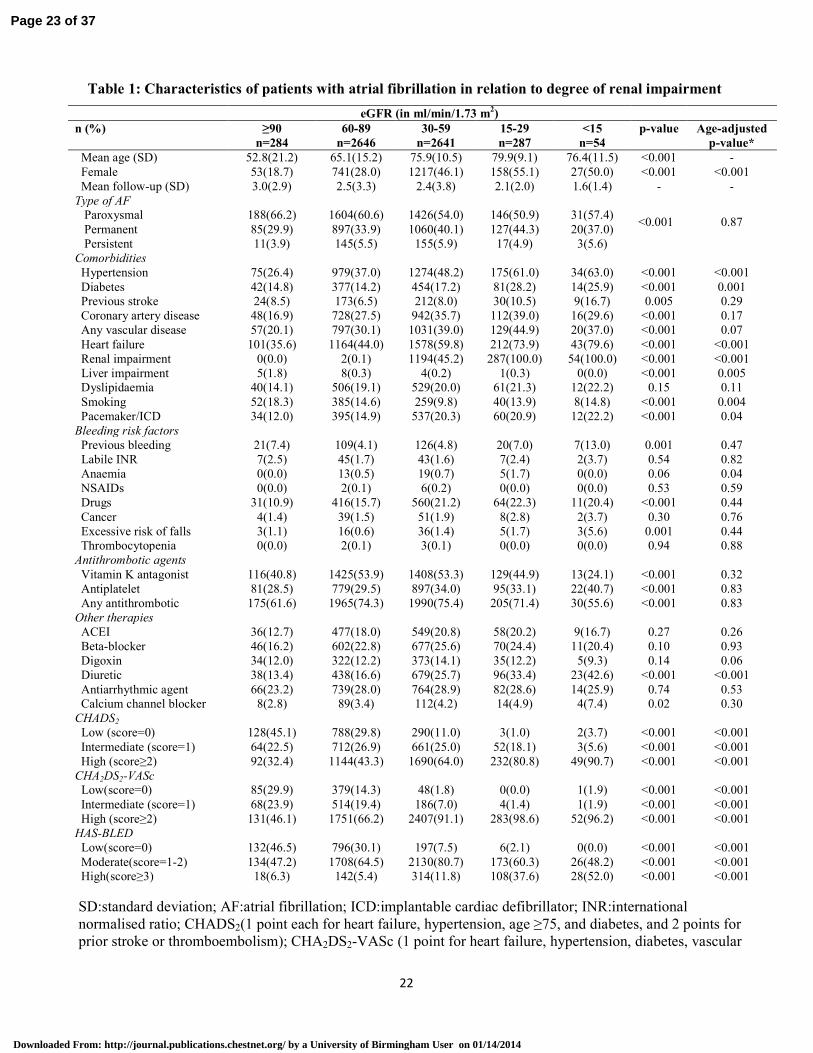
Baseline characteristics are shown in Table 1. Individuals with eGFR<15 mL/min/1.73m2 were
older, and more likely to be female and have paroxysmal AF, compared with individuals with
eGFR>90mL/min/1.73m2. After age-adjustment, individuals with eGFR<15 mL/min/1.73 m
2 were
more likely to have hypertension, heart failure (p<0.001), diabetes mellitus (p=0.001), liver
impairment (p=0.005), pacemaker/ICD (p=0.004), smoking history (p=0.04), diuretic therapy
(p<0.001) and higher CHADS2, CHA2DS2-VASc and HAS-BLED scores (p<0.001), when
compared with individuals with eGFR>90mL/min/1.73 m2, but there were no significant differences
in rates of OAC or antithrombotic therapies.
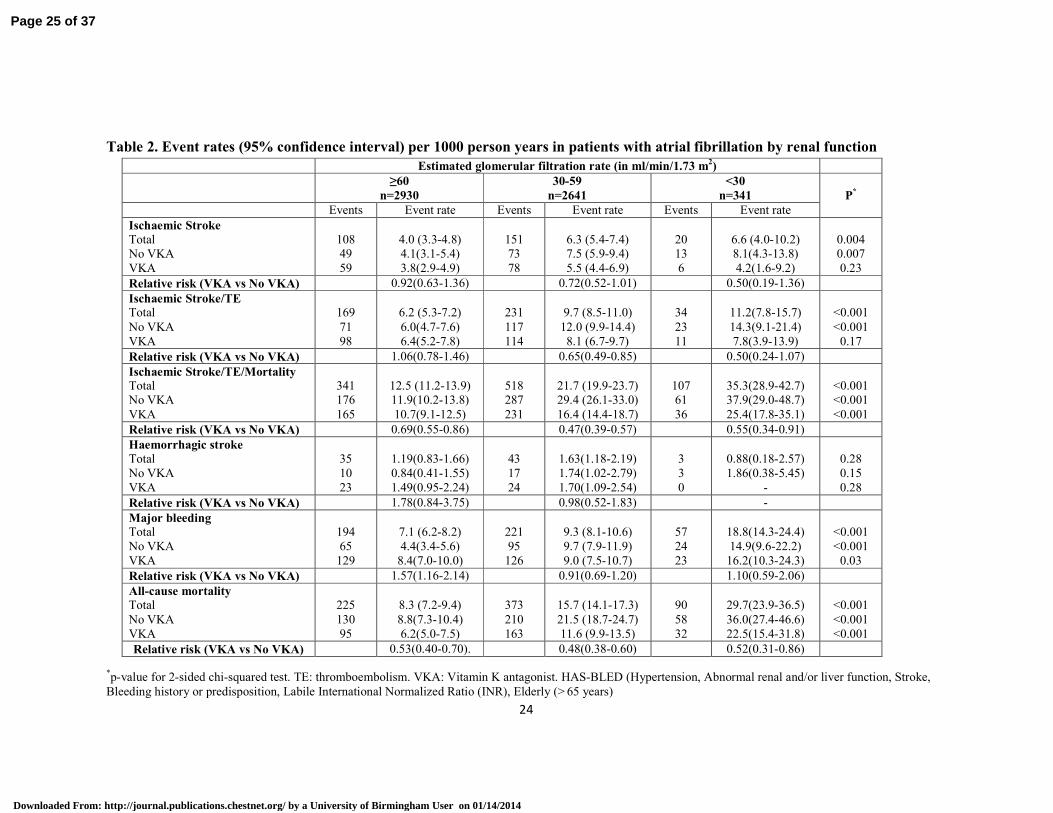
Rates of the composite of ‘stroke and all-cause mortality’ were lower in individuals on OAC,
compared with those individuals not on OAC. In non-anticoagulated and anticoagulated individuals,
rates of IS/TE were 7.4 (95% CI 6.3-8.6) and 7.2 (6.3-8.2) per 1000 person years, respectively.
Incidence rates of all-cause mortality were 13.4 (12.0-15.0) and 9.4 (8.3-10.5), respectively, and of
major bleeding were 6.2 (5.2-7.3) and 9.0 (8.0-10.1) per 1000 person years, respectively. Rates of
all events increased with decreasing eGFR, regardless of OAC therapy (Table 2). Bleeding rates
were higher in individuals on OAC, compared with non-anticoagulated individuals.
VKA was associated with approximately 50% relative risk reduction for stroke/TE/all-cause
mortality and all-cause mortality in all eGFR categories (Table 2). There was a trend towards
relative risk reduction for stroke and IS/TE with VKA, but this was not statistically significant. In
patients with eGFR≥60 mL/min/1.73 m2, VKA was associated with higher risk of bleeding (RR
1.57, 1.16-2.14), but there was no statistically significant increase in bleeding risk in other eGFR
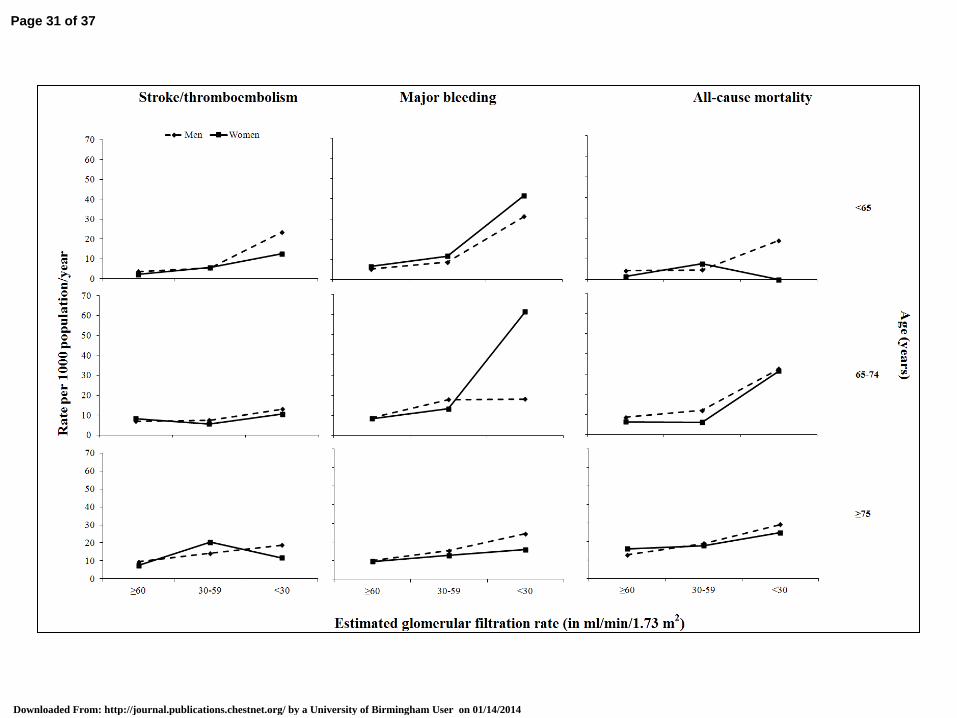
categories (Table 2). After stratification by age and sex, the reduction in eGFR was associated with
increased rates of all-cause mortality, IS/TE and bleeding in men and women and in all age groups
(figure 2).
Page 9 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
9
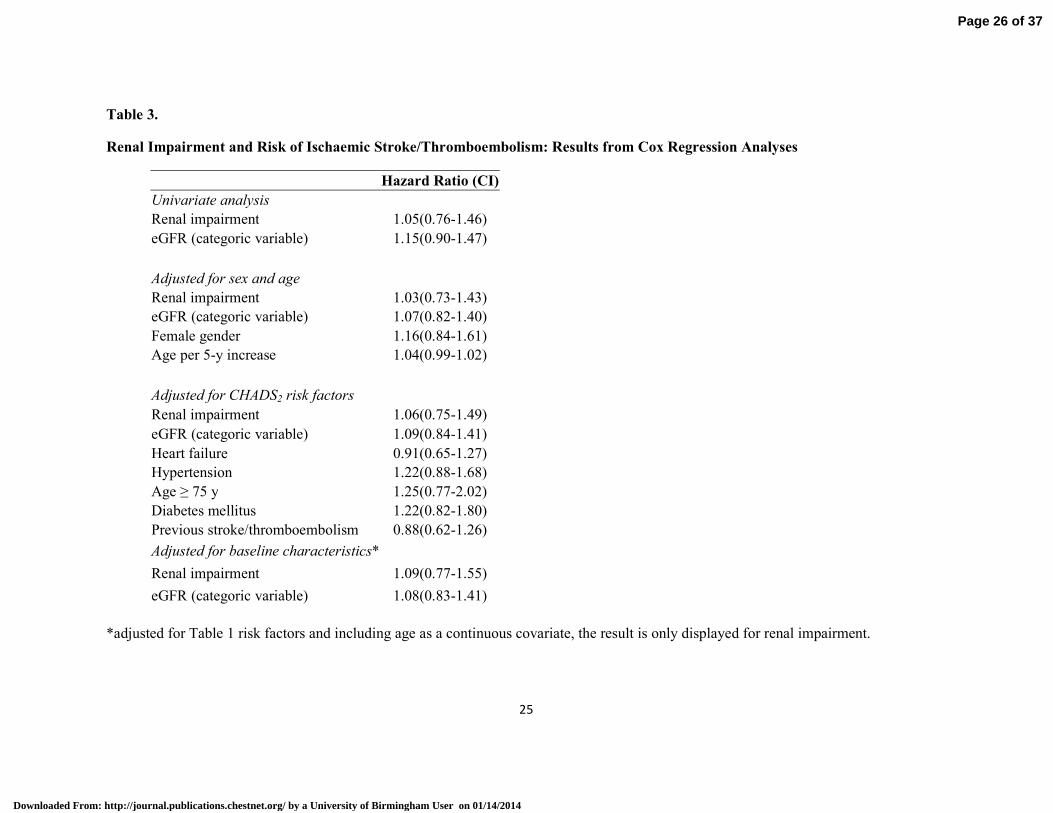
Table 3 shows the results from the Cox regression analyses. Neither renal impairment nor eGFR
were independent predictors of IS/TE in AF at 1 year follow-up in univariate or multivariate
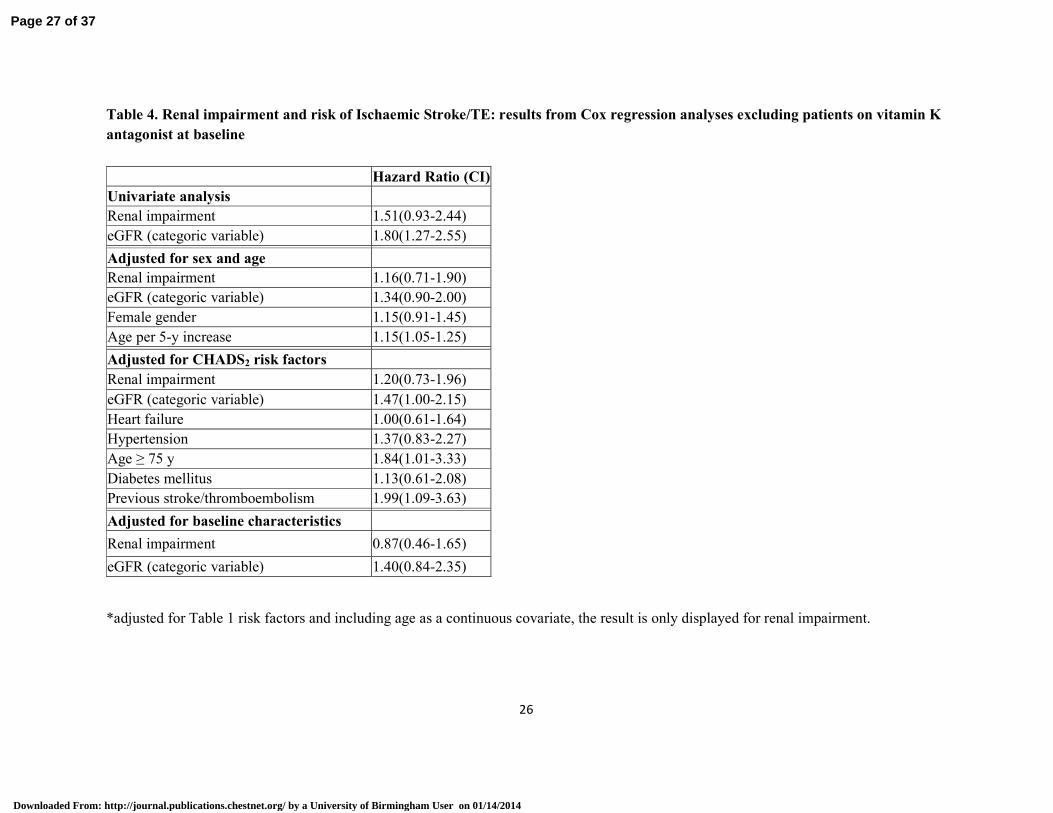
analyses, after adjustment for age, sex, CHADS2 risk factors or baseline characteristics. Table 4
shows analogous results from Cox regression analyses after excluding patients on vitamin K
antagonists at baseline (n=3592; 60.8%). As a categoric variable, eGFR was an independent
predictor for IS/TE on univariate analysis (HR 1.80;1.27-2.55), but not after adjustment for age,
sex, CHADS2 risk factors or baseline characteristics at 1 year follow-up.
When the benefit of ischaemic stroke reduction is balanced against the increased risk of
haemorrhagic stroke amongst patients with renal impairment, the net clinical benefit (NCB) was
clearly positive in favour of VKA use, for example, in individuals with a eGFR=30-59,
NCB=2.06(95%CI 1.40-2.88), as well as those with eGFR<30, NCB=6.69(3.27-12.78).
Renal failure vs normal renal function
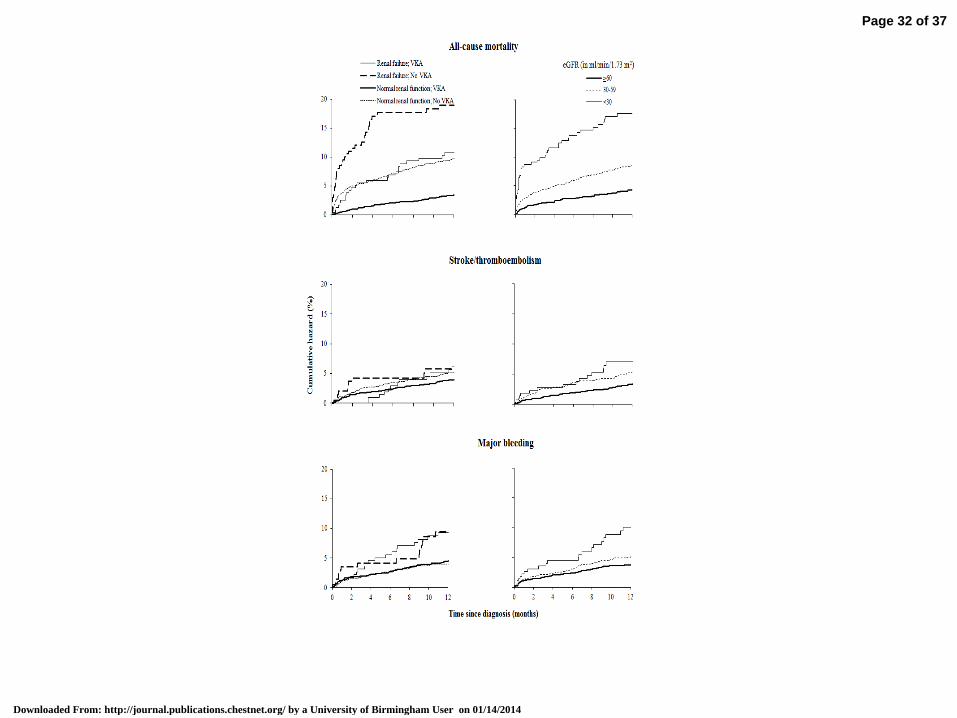
In the presence of VKA, rates of IS/TE were 6.2% and 3.9% at 1 year in individuals with renal
failure and with normal renal function respectively. The corresponding rates of all-cause mortality
were 10.8% and 3.4% at 1 year, and rates of bleeding were 9.3% and 4.5% at 1 year respectively
(Figure 3). In non-anticoagulated individuals, at 1 year, rates of IS/TE, all-cause mortality and
bleeding were 5.8% and 5.1%, 18.9% and 9.6%, and 9.4% and 3.9% with renal failure and with
normal renal function respectively (Figure 3).
Individuals with eGFR≥60mL/min/1.73m2 compared with eGFR <30 mL/min/1.73m
2
Rates of IS/TE were 3.3% and 7.0% at 1 year in individuals with eGFR≥60mL/min/1.73m2and with
eGFR <30 mL/min/1.73m2 respectively. At 1 year, the corresponding rates of all-cause mortality
were 4.2% and 17.6%, and the rates of bleeding were 3.8% and 10.0% (Figure 3).
VKA was associated with reduced hazard of mortality, increased hazard of bleeding and a trend
towards reduced risk of IS/TE, regardless of renal function (Figure 3).
In both anticoagulated and non-anticoagulated individuals, incidence rates of IS/TE, mortality and
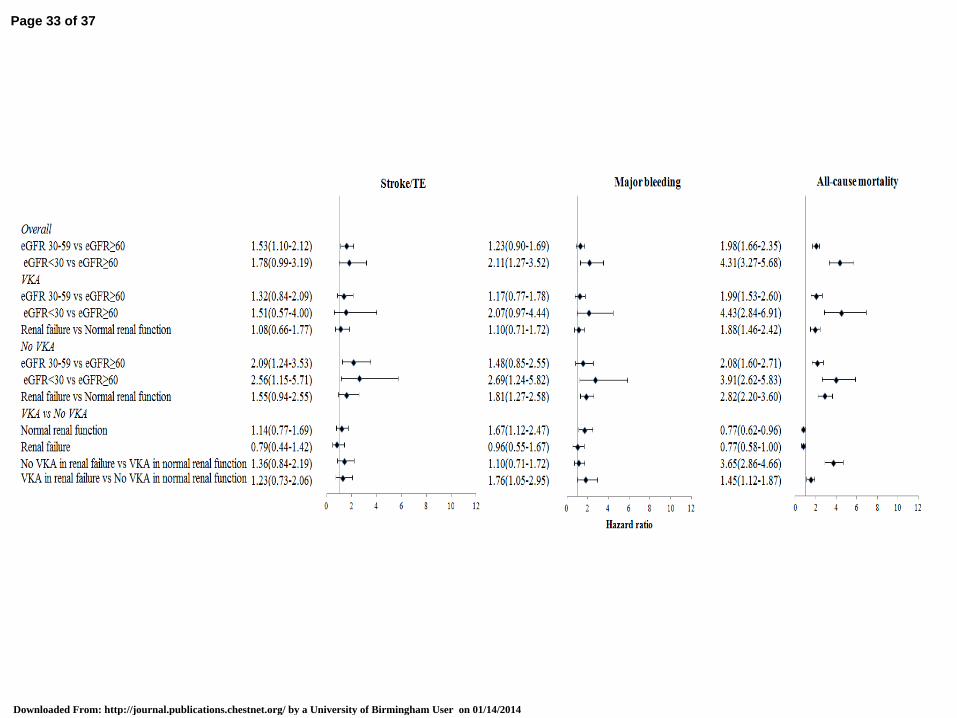
bleeding increased with reducing eGFR. In non-anticoagulated individuals with renal failure, the
risk of mortality was 4-fold greater than in anti-coagulated individuals with normal renal function
(HR 3.65, 95%CI 2.86-4.66) (Figure 4).
Page 10 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
10
Discussion
This is the first prospective study of the impact of renal function, as measured by eGFR, on IS/TE,
mortality and bleeding in the same population of individuals with AF, with four major findings.
First, in AF patients, renal failure and reduced eGFR were associated with a more severe risk factor
profile, higher rates of permanent AF, higher risk of IS/TE and bleeding as measured by validated
risk stratification schemes and worse outcomes. Second, individuals receiving OAC had lower
incidence of IS/TE and mortality, compared with non-anticoagulated individuals in all categories of
renal function measured by eGFR. Indeed, the net clinical benefit (NCB) balancing ischaemic
stroke reduction against the increased risk of haemorrhagic stroke was clearly positive in favour of
OAC use amongst patients with renal impairment. Third, rates of IS/TE, mortality and bleeding
increased with reducing eGFR, regardless of gender, age or OAC therapy. Fourth, renal impairment,
whether as a dichotomous variable or measured by eGFR, was not a significant predictor of IS/TE
at 1 year after adjustment for baseline characteristics.
The 1-year risks for stroke/TE and mortality were significantly increased by renal failure and
absence of OAC. When eGFR was <30mL/min/1.73m2, 1-year mortality was 17.6%. Our data
confirm that in addition to its growing global burden8-10
, the outcomes of AF are at least as severe
as in contemporary data for atherosclerotic vascular diseases40
.
The rates of IS/TE in non-anticoagulated individuals in this population (12.0 and 14.3 per 1000
person years with eGFR stage 30-59 and <30 mL/min/1.73m2 respectively) were lower than the
ATRIA study (4.2 per 100 person years in patients with eGFR <45mL/min/1.73 m2)15
. Although the
ATRIA cohort and our study population have similar comorbidities and similar rates of OAC, the
older age of patients in the former study may explain the higher IS/TE rates. Our data suggest that
the association between low eGFR and IS/TE is explained by confounding since there was no
independent association after adjustment for baseline characteristics, and moreover, we have
already shown that eGFR does not add incremental value to risk prediction in IS/TE. Indeed, renal
impairement is commonly associated with many of the individual components of CHADS2 and
CHA2DS2-VASc scores and thus, our observation that neither renal impairment nor eGFR were
independent predictors of IS/TE in AF is perhaps unsurprising. Two recent analyses found that
renal function (as measured by eGFR) was independently predictive of IS/TE25,41
. However, our
Page 11 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
11
study is a contemporary ‘real-world’ population whilst the ATRIA cohort stopped recruiting in
2003 and therefore may not represent contemporary clinical practice in AF populations.
In this study, individuals with renal failure and AF, as measured by eGFR were less likely to be on
OAC than individuals with normal renal function (Table 1). Current consensus guidelines do not
recommend routine OAC in patients on haemodialysis (which may explain the low rates of OAC in
patients with renal impairment in our population) although limited data already suggest a reduction
in stroke/TE with OAC in patients with CKD42-45
.
Our observations illustrate the high bleeding risk associated with increasing renal impairment in a
series of patients with one of the longest follow-up periods in the literature to-date. Indeed, the
latter may have implications for future risk stratification schemes for major bleeding which
currently classify renal failure as a dichotomous variable21
. Trials of OAC (including novel
anticoagulants) are urgently required in patients with renal impairment in order to establish the
balance of efficacy vs safety of OAC in this patient group, especially because the majority of AF
trials have excluded patients with CKD and most do not even analyse the effect of renal function22,
45-50. However, the moderate-high renal clearance of most novel anticoagulants probably limits their
use in moderate/severe renal impairment, although the oral Factor Xa inhibitor, betrixaban is
minimally renally cleared and is the only novel agent that could be studied in individuals with
severe renal impairment51
.
In our NCB analysis balancing ischaemic stroke reduction against the increased risk of
haemorrhagic stroke amongst patients with renal impairment, there was a positive NCB in favour of
OAC use. The original NCB analysis for warfarin by Singer and colleagues39
in patients with AF
showed greatest benefit in patients with the highest untreated risk for stroke. The NCB of warfarin
may be greatest in patients with highest bleeding risk who also have high stroke risk (as measured
by validated risk stratification scoring systems)52
, and extrapolation of available clinical trial data
suggests the same trends for novel anticoagulants53
. In the present study, we clearly show for the
first time that warfarin may have greatest NCB, when balancing ischaemic stroke against
haemorrhagic stroke, in individuals with AF and renal failure.
Page 12 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

12
Study limitations.
This study is based on a ‘real world’ registry with inherent limitations of diagnostic coding and case
ascertainment, as previously reported31, 32
. Despite stratification and adjustment for several risk
factors, the non-randomized design leaves a risk of residual confounding factors, but as already
stated, the majority of randomised trials to-date in AF patients have excluded analyses of the effect
of renal function. If a resident moved away from the area or died or had a stroke diagnosed
elsewhere, information on the event was not available. However, the relatively high number of
deaths in our study suggests a high proportion of ascertainment of events. The study population was
hospital-based and therefore may not be representative of all patients with AF, many of whom are
not hospitalized for their arrhythmia. The study was not ethnically diverse and our findings may not
be generalisable to other populations.
In the randomised trials, anticoagulation reduces stroke (by 64%) and all cause mortality (by
26%)54
. In our study, although VKA was associated with a relative risk reduction in
stroke/TE/mortality and all-cause mortality, there was not a statistically significant relative risk
reduction for ischaemic stroke, despite lower event rates in patients on VKA versus patients not on
VKA. A possible explanation may be that in such ‘real world’ registries, some recorded deaths may
be due to strokes, as not all patients had routine post mortems or detailed cerebral imaging,
therefore leading to the our findings of a higher-than-predicted risk reduction for all-cause mortality
and a non-statistically significant risk reduction for ischaemic stroke, compared with clinical trials.
The data regarding OAC use are only regarding baseline therapy and do not reflect any changes in
prescribed therapy or adherence to therapy. Also, data regarding the “time in therapeutic range”
(TTR) are not available for our study population. Our study population was a prospective cohort
design and not a randomised clinical trial, therefore, confounding by indication is a possibility55
.
However, the effect of this confounding is likely to be minimal since the individuals at highest risk
of study outcomes (based on risk prediction scores) were least likely to be taking OAC. Only
baseline creatinine measurements and eGFR calculations are available and therefore, we are unable
to comment on change or progression of renal impairment, nor the need for renal replacement
therapy. We used a categoric eGFR variable analysis as this would be more useful in terms of
incorporating eGFR into a risk prediction score; there was no appreciable difference with eGFR
analysed as a continuous variable. However, eGFR is probably the most important indicator of renal
function to take into account, since OAC doses are usually lower in patients with CKD than in those
Page 13 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

13
without CKD and changes are more often necessary in this situation56
. Finally, the number of
individuals with eGFR<30 mL/min/1.73 m2 in the study population was small (as were the number
on dialysis) and therefore, the statistical power of analysis in this subgroup may be limited.
Conclusions
Renal impairment is associated with poor outcomes at 1 year in individuals with NVAF across the
whole range of renal function, as measured by eGFR. OAC use was associated with a lower
incidence of IS/TE and mortality, compared with non-anticoagulated individuals in all categories of
renal function as measured by eGFR. Indeed, the NCB balancing ischaemic stroke against major
bleeding was positive, in favour of OAC use amongst patients with renal impairment, suggesting
that bleeding risk is not the most important variable in stroke prevention treatment decisions in
these individuals. Therefore, full anticoagulation is recommended in patients with at least moderate
renal impairment, with improved attention to good quality INR control (as reflected by a high time
in therapeutic range, which is associated with lower event rates57
). Whilst eGFR was not an
independent predictor of IS/TE in patients with AF, these patients are still ‘high risk’ and regular
checks on eGFR would be recommended, especially since normal or mild renal impairment at
baseline does not preclude some patients deteriorating to severe renal impairment58
. These
observations have implications for future risk prediction tools of outcomes in NVAF as well as
future clinical trials.
Page 14 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
14
Acknowledgments
Author Contributions - AB, GYHL, and LF contributed to the study conception and design. LF, ST,
JMH and PV made the primary contribution to data collection. AB performed the analyses and
produced the initial manuscript. All authors contributed to interpretation of results, revising the
manuscript critically for important intellectual content, and all approved the final manuscript.
LF had full access to all the data in the study and takes responsibility for the integrity of the data
and the accuracy of the data analysis.
All authors – no conflicts of interest pertaining directly to this paper. No funding (commercial/non-
commercial) was received for this study.
Page 15 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
15
References
1. Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA,
Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW;
American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood
Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Kidney disease
as a risk factor for development of cardiovascular disease: a statement from the American
Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure
Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension
2003;42:1050-65.
2. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks
of death, cardiovascular events, and hospitalization. N Engl J Med 2004;351:1296-305.
3. Weiner DE, Tighiouart H, Amin MG, Stark PC, MacLeod B, Griffith JL, Salem DN, Levey
AS, Sarnak MJ. Chronic kidney disease as a risk factor for cardiovascular disease and all-
cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol
2004;15:1307-15.
4. Coresh J, Astor B, Sarnak MJ. Evidence for increased cardiovascular disease risk in patients
with chronic kidney disease. Curr Opin Nephrol Hypertens 2004;13:73-81.
5. Couser WG, Remuzzi G, Mendis S, Tonelli M. The contribution of chronic kidney disease
to the global burden of major noncommunicable diseases. Kidney Int. 2011;8:1258-70.
6. McCullough K, Sharma P, Ali T, Khan I, Smith WC, Macleod A, Black C. Measuring the
population burden of chronic kidney disease: a systematic literature review of the estimated
prevalence of impaired kidney function.Nephrol Dial Transplant. 2012;27:1812-21.
7. Nugent RA, Fathima SF, Feigl AB, Chyung D.The burden of chronic kidney disease on
developing nations: a 21st century challenge in global health.Nephron Clin Pract.
2011;118:c269-77.
8. Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, , Vasan RS, D'Agostino RB,
Massaro JM, Beiser A, Wolf PA, Benjamin EJ. Lifetime risk for development of atrial
fibrillation: the Framingham Heart Study. Circulation. 2004; 110:1042-6.
9. Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, Stricker BH Stijnen T,
Lip GY, Witteman JC. Prevalence, incidence and lifetime risk of atrial fibrillation: the
Rotterdam Study. Eur Heart J 2006; 27: 949–53.
Page 16 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
16
10. Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB,
Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota,
1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;
114: 119–25.
11. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for
stroke: the Framingham Study. Stroke. 1991; 22: 983–88.
12. Kurth T, de Jong PE, Cook NR, Buring JE, Ridker PM. Kidney function and risk of
cardiovascular disease and mortality in women: a prospective cohort study. BMJ. 2009 Jun
29;338:b2392. doi: 10.1136/bmj.b2392.
13. Alonso A, Lopez FL, Matsushita K, Loehr LR, Agarwal SK, Chen LY, Soliman EZ, Astor
BC, Coresh J. Chronic kidney disease is associated with the incidence of atrial fibrillation:
the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123:2946-53.
14. Horio T, Iwashima Y, Kamide K, Tokudome T, Yoshihara F, Nakamura S, Kawano Y.
Chronic kidney disease as an independent risk factor for new-onset atrial fibrillation in
hypertensive patients. J Hypertens. 2010;28:1738-44.
15. Go AS, Fang MC, Udaltsova N, Chang Y, Pomernacki NK, Borowsky L, Singer DE;
ATRIA Study Investigators. Impact of proteinuria and glomerular filtration rate on risk of
thromboembolism in atrial fibrillation: the anticoagulation and risk factors in atrial
fibrillation (ATRIA) study. Circulation. 2009;119:1363-9.
16. Olesen JB, Lip GY, Kamper AL, Hommel K, Køber L, Lane DA, Lindhardsen J, Gislason
GH, Torp-Pedersen C. Stroke and bleeding in atrial fibrillation with chronic kidney disease.
N Engl J Med. 2012;367:625-35.
17. Nakagawa K, Hirai T, Takashima S, Fukuda N, Ohara K, Sasahara E, Taguchi Y, Dougu N,
Nozawa T, Tanaka K, Inoue H. Chronic kidney disease and CHADS(2) score independently
predict cardiovascular events and mortality in patients with nonvalvular atrial fibrillation.
Am J Cardiol. 2011;107:912-6.
18. Vázquez E, Sánchez-Perales C, Lozano C, García-Cortés MJ, Borrego F, Guzmán M, Pérez
P, Pagola C, Borrego MJ, Pérez V. Comparison of prognostic value of atrial fibrillation
versus sinus rhythm in patients on long-term hemodialysis. Am J Cardiol. 2003;92:868-71.
19. Fox KA, Piccini JP, Wojdyla D, Becker RC, Halperin JL, Nessel CC, Paolini JF, Hankey
GJ, Mahaffey KW, Patel MR, Singer DE, Califf RM. Prevention of stroke and systemic
embolism with rivaroxaban compared with warfarin in patients with non-valvular atrial
fibrillation and moderate renal impairment Eur Heart J. 2011;32:2387-94.
Page 17 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
17
20. Abdelhafiz AH, Myint MP, Tayek JA, Wheeldon NM. Anemia, hypoalbuminemia, and
renal impairment as predictors of bleeding complications in patients receiving
anticoagulation therapy for nonvalvular atrial fibrillation: a secondary analysis. Clin Ther.
2009;31:1534-9.
21. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY.A novel user-friendly
score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation:
the Euro Heart Survey. Chest. 2010;138:1093-100. Epub 2010 Mar 18.
22. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney
disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39(2 Suppl
1):S1-266.
23. Archibald G, Bartlett W, Brown A, Christie B, Elliott A, Griffith K, Pound S, Rappaport I,
Robertson D, Semple Y, Slane P, Whitworth C, Williams B. UK consensus conference on
early chronic kidney disease. Edinburgh: Royal College of Physicians; 2007.
http://www.rcpe.ac.uk/clinical-standards/standards/UK-Consensus-Conference-on-Early-
Chronic-Kidney-Disease-Feb-2007.pdf [accessed 12 June 2013]
24. National Institute for Health and Clinical Excellence (NICE). CG73 Chronic kidney disease:
Early identification and management of chronic kidney disease in adults in primary and
secondary care. NICE clinical guidelines Issued: September 2008
25. Piccini JP, Stevens SR, Chang Y, Singer DE, Lokhnygina Y, Go AS, Patel MR, Mahaffey
KW, Halperin JL, Breithardt G, Hankey GJ, Hacke W, Becker RC, Nessel CC, Fox KA,
Califf RM; ROCKET AF Steering Committee and Investigators. Renal dysfunction as a
predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation:
validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral,
direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke
and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In
Atrial fibrillation) study cohorts. Circulation. 2013;127:224-32
26. Marinigh R, Lane DA, Lip GY. Severe renal impairment and stroke prevention in atrial
fibrillation: implications for thromboprophylaxis and bleeding risk. J Am Coll Cardiol.
2011;57:1339-48.
27. Gage BF, Yan Y, Milligan PE, Waterman AD, Culverhouse R, Rich MW, Radford MJ.
Clinical classification schemes for predicting hemorrhage: results from the National
Registry of Atrial Fibrillation (NRAF). Am Heart J. 2006;151:713-9.
Page 18 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

18
28. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of
clinical classification schemes for predicting stroke: results from the National Registry of
Atrial Fibrillation". JAMA 2001; 285:2864–70.
29. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for
predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based
approach: the Euro Heart Survey on atrial fibrillation. Chest. 2010; 137:263-72.
30. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic
stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial
Fibrillation cohort study. Eur Heart J. 2012;33:1500-10.
31. Banerjee A, Fauchier L, Vourc'h P, Andres CR, Taillandier S, Halimi JM, Lip GY. Renal
impairment and ischaemic stroke risk assessment in patients with atrial fibrillation: The
Loire Valley Atrial Fibrillation Project. J Am Coll Cardiol. 2013 Mar 21. [Epub ahead of
print]
32. Banerjee A, Taillandier S, Olesen JB, Lane DA, Lallemand B, Lip GY, Fauchier L. Ejection
fraction and outcomes in patients with atrial fibrillation and heart failure: the Loire Valley
Atrial Fibrillation Project. Eur J Heart Fail. 2012;14:295-301.
33. Couchoud C, Pozet N, Labeeuw M, Pouteil-Noble C. Screening early renal failure: cut-off
values for serum creatinine as an indicator of renal impairment. Kidney Int. 1999;55:1878-
84.
34. Van Den Noortgate NJ, Janssens WH, Delanghe JR, Afschrift MB, Lameire NH. Serum
cystatin C concentration compared with other markers of glomerular filtration rate in the old
old. J Am Geriatr Soc 2002;50:1278-82.
35. Daniel JP, Chantrel F, Offner M, Moulin B, Hannedouche T. Comparison of cystatin C,
creatinine and creatinine clearance vs. GFR for detection of renal failure in renal transplant
patients. Ren Fail 2004;26:253-7.
36. Schuck O, Gottfriedova H, Maly J, Jabor A, Stollova M, Bruzkova I, , Skibova J, Ryska M,
Spicak J, Trunecka P, Novakova J. Glomerular filtration rate assessment in individuals after
orthotopic liver transplantation based on serum cystatin C levels. Liver Transpl 2002;8:594-
9.
37. Mariat C, Alamartine E, Barthelemy JC, De Filippis JP, Thibaudin D, Berthoux P, , Laurent
B, Thibaudin L, Berthoux F. Assessing renal graft function in clinical trials: can tests
predicting glomerular filtration rate substitute for a reference method? Kidney Int
2004;65:289-97.
Page 19 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
19
38. Botev R, Mallié JP, Wetzels JF, Couchoud C, Schück O. The clinician and estimation of
glomerular filtration rate by creatinine-based formulas: current limitations and quo vadis.
Clin J Am Soc Nephrol. 2011;6:937-50.
39. Singer DE, Chang Y, Fang MC, Borowsky LH, Pomernacki NK, Udaltsova N, Go AS. The
net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med 2009;
151: 297–305.
40. Rothwell PM, Coull AJ, Silver LE, Fairhead JF, Giles MF, Lovelock CE, Redgrave JN, Bull
LM, Welch SJ, Cuthbertson FC, Binney LE, Gutnikov SA, Anslow P, Banning AP, Mant D,
Mehta Z; Oxford Vascular Study. Population-based study of event-rate, incidence, case
fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular
Study). Lancet. 2005;366:1773-83.
41. Singer DE, Chang Y, Borowsky LH, Fang MC, Pomernacki NK, Udaltsova N, Reynolds K,
Go AS. A New Risk Scheme to Predict Ischemic Stroke and Other Thromboembolism in
Atrial Fibrillation: The ATRIA Study Stroke Risk Score. J Am Heart Assoc. 2013;2:
e000250.
42. Herzog CA, Asinger RW, Berger AK, Charytan DM, Díez J, Hart RG, Eckardt KU, Kasiske
BL, McCullough PA, Passman RS, DeLoach SS, Pun PH, Ritz E. Cardiovascular disease in
chronic kidney disease. A clinical update from Kidney Disease: Improving Global
Outcomes (KDIGO). Kidney Int. 2011;80:572-86.
43. Hart RG, Pearce LA, Asinger RW, Herzog CA. Warfarin in atrial fibrillation patients with
moderate chronic kidney disease.Clin J Am Soc Nephrol 2011;6(11):2599-604). Clin J Am
Soc Nephrol. 2011;6:2599-604.
44. Wizemann V, Tong L, Satayathum S, Disney A, Akiba T, Fissell RB, Kerr PG, Young EW,
Robinson BM. Atrial fibrillation in hemodialysis patients: clinical features and associations
with anticoagulant therapy. Kidney Int. 2010;77:1098-106.
45. Winkelmayer WC, Liu J, Setoguchi S, Choudhry NK. Effectiveness and safety of warfarin
initiation in older hemodialysis patients with incident atrial fibrillation. Clin J Am Soc
Nephrol. 2011;6:2662-8.
46. Morocutti C, Amabile G, Fattapposta F, Nicolosi A, Matteoli S, Trappolini M, Cataldo G,
Milanesi G, Lavezzari M, Pamparana F, Coccheri S. Indobufen versus warfarin in the
secondary prevention of major vascular events in nonrheumatic atrial fibrillation. SIFA
(Studio Italiano Fibrillazione Atriale) Investigators. Stroke. 1997;28:1015-21.
Page 20 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
20
47. Hellemons BS, Langenberg M, Lodder J, Vermeer F, Schouten HJ, Lemmens TG, van Ree
JW, Knottnerus JA. Primary prevention of arterial thromboembolism in nonrheumatic atrial
fibrillation: the PATAF trial study design. Control Clin Trials. 1999;20:386-93.
48. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly
PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius
H, Diener HC, Joyner CD, Wallentin L; RE-LY Steering Committee and Investigators.
Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139-
51.
49. Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, Al-Khalidi HR,
Ansell J, Atar D, Avezum A, Bahit MC, Diaz R, Easton JD, Ezekowitz JA, Flaker G, Garcia
D, Geraldes M, Gersh BJ, Golitsyn S, Goto S, Hermosillo AG, Hohnloser SH, Horowitz J,
Mohan P, Jansky P, Lewis BS, Lopez-Sendon JL, Pais P, Parkhomenko A, Verheugt FW,
Zhu J, Wallentin L; ARISTOTLE Committees and Investigators. Apixaban versus warfarin
in patients with atrial fibrillation. N Engl J Med. 2011;365:981-92.
50. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL,
Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KA, Califf
RM; ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial
fibrillation. N Engl J Med. 2011;365:883-91.
51. Ahrens I, Peter K, Lip GY, Bode C. Development and clinical applications of novel oral
anticoagulants. Part II. Drugs under clinical investigation. Discov Med. 2012;13:445-50.
52. Olesen JB, Lip GY, Lindhardsen J, Lane DA, Ahlehoff O, Hansen ML, Raunsø J, Tolstrup
JS, Hansen PR, Gislason GH, Torp-Pedersen C. Risks of thromboembolism and bleeding
with thromboprophylaxis in patients with atrial fibrillation: A net clinical benefit analysis
using a 'real world' nationwide cohort study. Thromb Haemost. 2011;106:739-49.
53. Banerjee A, Lane DA, Torp-Pedersen C, Lip GY. Net clinical benefit of new oral
anticoagulants (dabigatran, rivaroxaban, apixaban) versus no treatment in a 'real world' atrial
fibrillation population: a modelling analysis based on a nationwide cohort study. Thromb
Haemost. 2012;107:584-9.
54. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in
patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857-67.
55. Signorello LB, McLaughlin JK, Lipworth L, Friis S, Sørensen HT, Blot WJ. Confounding
by indication in epidemiologic studies of commonly used analgesics. Am J Ther.
2002;9:199-205.
Page 21 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
21
56. Limdi NA, Beasley TM, Baird MF, Goldstein JA, McGwin G, Arnett DK, Acton RT, Allon
M. Kidney function influences warfarin responsiveness and hemorrhagic complications. J
Am Soc Nephrol. 2009;20:912-21.
57. Gallagher AM, Setakis E, Plumb JM, Clemens A, van Staa TP. Risks of stroke and mortality
associated with suboptimal anticoagulation in atrial fibrillation patients. Thromb Haemost.
2011;106:968-77.
58. Roldán V, Marín F, Fernández H, Manzano-Fernández S, Gallego P, Valdés M, Vicente V,
Lip GY. Renal impairment in a "real-life" cohort of anticoagulated patients with atrial
fibrillation (implications for thromboembolism and bleeding). Am J Cardiol.
2013;111:1159-64.
Page 22 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
22
Table 1: Characteristics of patients with atrial fibrillation in relation to degree of renal impairment
eGFR (in ml/min/1.73 m2)
n (%) ≥90
n=284
60-89
n=2646
30-59
n=2641
15-29
n=287
<15
n=54
p-value Age-adjusted
p-value*
Mean age (SD) 52.8(21.2) 65.1(15.2) 75.9(10.5) 79.9(9.1) 76.4(11.5) <0.001 -
Female 53(18.7) 741(28.0) 1217(46.1) 158(55.1) 27(50.0) <0.001 <0.001
Mean follow-up (SD) 3.0(2.9) 2.5(3.3) 2.4(3.8) 2.1(2.0) 1.6(1.4) - -
Type of AF
Paroxysmal
Permanent
Persistent
188(66.2)
85(29.9)
11(3.9)
1604(60.6)
897(33.9)
145(5.5)
1426(54.0)
1060(40.1)
155(5.9)
146(50.9)
127(44.3)
17(4.9)
31(57.4)
20(37.0)
3(5.6)
<0.001 0.87
Comorbidities
Hypertension 75(26.4) 979(37.0) 1274(48.2) 175(61.0) 34(63.0) <0.001 <0.001
Diabetes 42(14.8) 377(14.2) 454(17.2) 81(28.2) 14(25.9) <0.001 0.001
Previous stroke 24(8.5) 173(6.5) 212(8.0) 30(10.5) 9(16.7) 0.005 0.29
Coronary artery disease 48(16.9) 728(27.5) 942(35.7) 112(39.0) 16(29.6) <0.001 0.17
Any vascular disease 57(20.1) 797(30.1) 1031(39.0) 129(44.9) 20(37.0) <0.001 0.07
Heart failure 101(35.6) 1164(44.0) 1578(59.8) 212(73.9) 43(79.6) <0.001 <0.001
Renal impairment 0(0.0) 2(0.1) 1194(45.2) 287(100.0) 54(100.0) <0.001 <0.001
Liver impairment 5(1.8) 8(0.3) 4(0.2) 1(0.3) 0(0.0) <0.001 0.005
Dyslipidaemia 40(14.1) 506(19.1) 529(20.0) 61(21.3) 12(22.2) 0.15 0.11
Smoking 52(18.3) 385(14.6) 259(9.8) 40(13.9) 8(14.8) <0.001 0.004
Pacemaker/ICD 34(12.0) 395(14.9) 537(20.3) 60(20.9) 12(22.2) <0.001 0.04
Bleeding risk factors
Previous bleeding 21(7.4) 109(4.1) 126(4.8) 20(7.0) 7(13.0) 0.001 0.47
Labile INR 7(2.5) 45(1.7) 43(1.6) 7(2.4) 2(3.7) 0.54 0.82
Anaemia 0(0.0) 13(0.5) 19(0.7) 5(1.7) 0(0.0) 0.06 0.04
NSAIDs 0(0.0) 2(0.1) 6(0.2) 0(0.0) 0(0.0) 0.53 0.59
Drugs 31(10.9) 416(15.7) 560(21.2) 64(22.3) 11(20.4) <0.001 0.44
Cancer 4(1.4) 39(1.5) 51(1.9) 8(2.8) 2(3.7) 0.30 0.76
Excessive risk of falls 3(1.1) 16(0.6) 36(1.4) 5(1.7) 3(5.6) 0.001 0.44
Thrombocytopenia 0(0.0) 2(0.1) 3(0.1) 0(0.0) 0(0.0) 0.94 0.88
Antithrombotic agents
Vitamin K antagonist 116(40.8) 1425(53.9) 1408(53.3) 129(44.9) 13(24.1) <0.001 0.32
Antiplatelet 81(28.5) 779(29.5) 897(34.0) 95(33.1) 22(40.7) <0.001 0.83
Any antithrombotic 175(61.6) 1965(74.3) 1990(75.4) 205(71.4) 30(55.6) <0.001 0.83
Other therapies
ACEI 36(12.7) 477(18.0) 549(20.8) 58(20.2) 9(16.7) 0.27 0.26
Beta-blocker 46(16.2) 602(22.8) 677(25.6) 70(24.4) 11(20.4) 0.10 0.93
Digoxin 34(12.0) 322(12.2) 373(14.1) 35(12.2) 5(9.3) 0.14 0.06
Diuretic 38(13.4) 438(16.6) 679(25.7) 96(33.4) 23(42.6) <0.001 <0.001
Antiarrhythmic agent 66(23.2) 739(28.0) 764(28.9) 82(28.6) 14(25.9) 0.74 0.53
Calcium channel blocker 8(2.8) 89(3.4) 112(4.2) 14(4.9) 4(7.4) 0.02 0.30
CHADS2
Low (score=0) 128(45.1) 788(29.8) 290(11.0) 3(1.0) 2(3.7) <0.001 <0.001
Intermediate (score=1) 64(22.5) 712(26.9) 661(25.0) 52(18.1) 3(5.6) <0.001 <0.001
High (score≥2) 92(32.4) 1144(43.3) 1690(64.0) 232(80.8) 49(90.7) <0.001 <0.001
CHA2DS2-VASc
Low(score=0) 85(29.9) 379(14.3) 48(1.8) 0(0.0) 1(1.9) <0.001 <0.001
Intermediate (score=1) 68(23.9) 514(19.4) 186(7.0) 4(1.4) 1(1.9) <0.001 <0.001
High (score≥2) 131(46.1) 1751(66.2) 2407(91.1) 283(98.6) 52(96.2) <0.001 <0.001
HAS-BLED
Low(score=0) 132(46.5) 796(30.1) 197(7.5) 6(2.1) 0(0.0) <0.001 <0.001
Moderate(score=1-2) 134(47.2) 1708(64.5) 2130(80.7) 173(60.3) 26(48.2) <0.001 <0.001
High(score≥3) 18(6.3) 142(5.4) 314(11.8) 108(37.6) 28(52.0) <0.001 <0.001
SD:standard deviation; AF:atrial fibrillation; ICD:implantable cardiac defibrillator; INR:international
normalised ratio; CHADS2(1 point each for heart failure, hypertension, age ≥75, and diabetes, and 2 points for
prior stroke or thromboembolism); CHA2DS2-VASc (1 point for heart failure, hypertension, diabetes, vascular
Page 23 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

23
disease, age 65-74, and female gender; 2 points for prior stroke or thromboembolism and age ≥75); HAS-BLED
(Hypertension, Abnormal renal and/or liver function, Stroke, Bleeding history or predisposition, Labile
International Normalized Ratio (INR), Elderly (> 65 years)
*Age adjustment was performed by including age as a covariate in a logistic regression model
Page 24 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
24
Table 2. Event rates (95% confidence interval) per 1000 person years in patients with atrial fibrillation by renal function
*p-value for 2-sided chi-squared test. TE: thromboembolism. VKA: Vitamin K antagonist. HAS-BLED (Hypertension, Abnormal renal and/or liver function, Stroke,
Bleeding history or predisposition, Labile International Normalized Ratio (INR), Elderly (> 65 years)
Estimated glomerular filtration rate (in ml/min/1.73 m2)
≥60
n=2930
30-59
n=2641
<30
n=341
P*
Events Event rate Events Event rate Events Event rate
Ischaemic Stroke
Total
No VKA
VKA
108
49
59
4.0 (3.3-4.8)
4.1(3.1-5.4)
3.8(2.9-4.9)
151
73
78
6.3 (5.4-7.4)
7.5 (5.9-9.4)
5.5 (4.4-6.9)
20
13
6
6.6 (4.0-10.2)
8.1(4.3-13.8)
4.2(1.6-9.2)
0.004
0.007
0.23
Relative risk (VKA vs No VKA) 0.92(0.63-1.36) 0.72(0.52-1.01) 0.50(0.19-1.36)
Ischaemic Stroke/TE
Total
No VKA
VKA
169
71
98
6.2 (5.3-7.2)
6.0(4.7-7.6)
6.4(5.2-7.8)
231
117
114
9.7 (8.5-11.0)
12.0 (9.9-14.4)
8.1 (6.7-9.7)
34
23
11
11.2(7.8-15.7)
14.3(9.1-21.4)
7.8(3.9-13.9)
<0.001
<0.001
0.17
Relative risk (VKA vs No VKA) 1.06(0.78-1.46) 0.65(0.49-0.85) 0.50(0.24-1.07)
Ischaemic Stroke/TE/Mortality Total
No VKA
VKA
341
176
165
12.5 (11.2-13.9)
11.9(10.2-13.8)
10.7(9.1-12.5)
518
287
231
21.7 (19.9-23.7)
29.4 (26.1-33.0)
16.4 (14.4-18.7)
107
61
36
35.3(28.9-42.7)
37.9(29.0-48.7)
25.4(17.8-35.1)
<0.001
<0.001
<0.001
Relative risk (VKA vs No VKA) 0.69(0.55-0.86) 0.47(0.39-0.57) 0.55(0.34-0.91)
Haemorrhagic stroke
Total
No VKA
VKA
35
10
23
1.19(0.83-1.66)
0.84(0.41-1.55)
1.49(0.95-2.24)
43
17
24
1.63(1.18-2.19)
1.74(1.02-2.79)
1.70(1.09-2.54)
3
3
0
0.88(0.18-2.57)
1.86(0.38-5.45)
-
0.28
0.15
0.28
Relative risk (VKA vs No VKA) 1.78(0.84-3.75) 0.98(0.52-1.83) -
Major bleeding
Total
No VKA
VKA
194
65
129
7.1 (6.2-8.2)
4.4(3.4-5.6)
8.4(7.0-10.0)
221
95
126
9.3 (8.1-10.6)
9.7 (7.9-11.9)
9.0 (7.5-10.7)
57
24
23
18.8(14.3-24.4)
14.9(9.6-22.2)
16.2(10.3-24.3)
<0.001
<0.001
0.03
Relative risk (VKA vs No VKA) 1.57(1.16-2.14) 0.91(0.69-1.20) 1.10(0.59-2.06)
All-cause mortality
Total
No VKA
VKA
225
130
95
8.3 (7.2-9.4)
8.8(7.3-10.4)
6.2(5.0-7.5)
373
210
163
15.7 (14.1-17.3)
21.5 (18.7-24.7)
11.6 (9.9-13.5)
90
58
32
29.7(23.9-36.5)
36.0(27.4-46.6)
22.5(15.4-31.8)
<0.001
<0.001
<0.001
Relative risk (VKA vs No VKA) 0.53(0.40-0.70). 0.48(0.38-0.60) 0.52(0.31-0.86)
Page 25 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
25
Table 3.
Renal Impairment and Risk of Ischaemic Stroke/Thromboembolism: Results from Cox Regression Analyses
Hazard Ratio (CI)
Univariate analysis
Renal impairment 1.05(0.76-1.46)
eGFR (categoric variable) 1.15(0.90-1.47)
Adjusted for sex and age
Renal impairment 1.03(0.73-1.43)
eGFR (categoric variable) 1.07(0.82-1.40)
Female gender 1.16(0.84-1.61)
Age per 5-y increase 1.04(0.99-1.02)
Adjusted for CHADS2 risk factors
Renal impairment 1.06(0.75-1.49)
eGFR (categoric variable) 1.09(0.84-1.41)
Heart failure 0.91(0.65-1.27)
Hypertension 1.22(0.88-1.68)
Age ≥ 75 y 1.25(0.77-2.02)
Diabetes mellitus 1.22(0.82-1.80)
Previous stroke/thromboembolism 0.88(0.62-1.26)
Adjusted for baseline characteristics*
Renal impairment 1.09(0.77-1.55)
eGFR (categoric variable) 1.08(0.83-1.41)
*adjusted for Table 1 risk factors and including age as a continuous covariate, the result is only displayed for renal impairment.
Page 26 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
26
Table 4. Renal impairment and risk of Ischaemic Stroke/TE: results from Cox regression analyses excluding patients on vitamin K
antagonist at baseline
Hazard Ratio (CI)
Univariate analysis
Renal impairment 1.51(0.93-2.44)
eGFR (categoric variable) 1.80(1.27-2.55)
Adjusted for sex and age
Renal impairment 1.16(0.71-1.90)
eGFR (categoric variable) 1.34(0.90-2.00)
Female gender 1.15(0.91-1.45)
Age per 5-y increase 1.15(1.05-1.25)
Adjusted for CHADS2 risk factors
Renal impairment 1.20(0.73-1.96)
eGFR (categoric variable) 1.47(1.00-2.15)
Heart failure 1.00(0.61-1.64)
Hypertension 1.37(0.83-2.27)
Age ≥ 75 y 1.84(1.01-3.33)
Diabetes mellitus 1.13(0.61-2.08)
Previous stroke/thromboembolism 1.99(1.09-3.63)
Adjusted for baseline characteristics
Renal impairment 0.87(0.46-1.65)
eGFR (categoric variable) 1.40(0.84-2.35)
*adjusted for Table 1 risk factors and including age as a continuous covariate, the result is only displayed for renal impairment.
Page 27 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
27
FIGURE LEGENDS
Figure 1: Study population by stage of renal impairment
Figure 2: Event rates for stroke/thromboembolism, major bleeding and all-cause mortality by age and sex
Figure 3: All-cause mortality, stroke/thromboembolism and major bleeding by renal failure, oral anticoagulation and stage of renal impairment
Figure 4: Hazard ratios for stroke/thromboembolism, major bleeding and all-cause mortality
Page 28 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
8,962
Atrial fibrillation
284(4.8%)
eGFR
>90ml/min/1.73m2
2646 (44.8%)
eGFR
60-89 ml/min/1.73m2
2641 (44.7%)
eGFR
30-59ml/min/1.73m2
287(4.9%)
eGFR
15-29ml/min/1.73m2
54 (0.9%)
eGFR
<15ml/min/1.73m2
Excluded:
1,804 patients with valvular disease
1246 with missing values on VKA treatment or serum creatinine levels
Page 30 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
Page 31 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
Page 32 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
Page 33 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

WEB ONLY APPENDIX
Extended Methods
Study population
The methods of the Loire Valley Atrial Fibrillation Project have been previously reported30-
31. At the Centre Hospitalier Régional et Universitaire in Tours (France), all patients
diagnosed with non-valvular AF (NVAF) or atrial flutter by the cardiology department
between 2000-2010 were identified, thus excluding patients with mitral stenosis, valve
replacement or other valvular pathology which might explain AF. The institution includes
four hospitals covering all medical and surgical specialties; the only public institution in an
area of around 4,000 km², serving approximately 400,000 inhabitants. Patients were followed
from the first record of NVAF after 1 January 2000 (i.e. index date) up to the latest data
collection at the time of study (December 2010). Treatment at discharge was obtained by
screening hospitalisation reports, and information on comorbidities was obtained from the
computerised coding system. Patients were excluded from the study if there was no available
data regarding the baseline serum creatinine level (Figure 1).
For each patient, the CHADS227
and CHA2DS2-VASc28
scores (which are the most commonly
used and validated risk stratification schemes for IS/TE in patients with AF) were calculated
following the first diagnosis of AF during hospital admission. The CHADS2 score was the
sum of points obtained after adding one point for congestive heart failure, hypertension, age
≥75, and diabetes, and two points for previous stroke or TE27
. The CHA2DS2-VASc score
was the sum of points after adding one point for congestive heart failure, hypertension,
diabetes, vascular disease (including history of coronary, cerebrovascular or peripheral
vascular disease), age 65-74, and female gender, and two points for previous stroke or TE and
age ≥7528
. According to the two risk scores, patients with a score of 0 on either schema were
considered as ‘low risk’, 1 as ‘intermediate risk’, and ≥2 as ‘high risk’ of stroke and TE.
The HAS-BLED (Hypertension, Abnormal renal and/or liver function, Stroke, Bleeding
history or predisposition, Labile International Normalized Ratio (INR), Elderly (> 65 years),
Drugs (antiplatelet drugs or NSAIDS)/alcohol excess concomitantly) score is a validated
scoring system for bleeding risk stratification in AF patients21
. For each patient, the HAS-
BLED score was also calculated as the sum of the points obtained after adding one point for
Page 34 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
the presence of each individual factor). For this analysis, patients with HAS-BLED score of 0
were deemed to have ‘low’ bleeding risk, those with HAS-BLED scores of 1-2 and ≥3 were
classified as “moderate” and ‘high’ bleeding risk respectively.
During follow-up, information on outcomes of TE, stroke (ischaemic or haemorrhagic),
major bleeding, and all-cause mortality were recorded by active surveillance of hospital
administrative data. Major bleeding was defined as bleeding with a reduction in the
haemoglobin level of at least 2g per litre, or with transfusion of at least 1 unit of blood, or
symptomatic bleeding in a critical area or organ (e.g., intracranial, intraspinal, intraocular,
retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome)
or bleeding that causes death. All bleeding data were identified with the diagnosis coded in a
subsequent hospitalization during follow-up – thus, we recorded all 'hospitalizations with a
bleed' as an additional criterion for major bleeding.
Assessment of renal function
Renal failure was defined as reported history of renal failure, or baseline serum creatinine
level of >133 µmol/L in men and >115 µmol/L in women32
. In order to convert serum
creatinine from µmol/L to mg/dL, the former was multiplied by a conversion factor of 88.4.
Current consensus guidelines state that prediction equations have greater consistency and
accuracy than serum creatinine in the assessment of GFR22-24, 33-35
. In addition, prediction
equations are equivalent or better than 24-hour urine creatinine clearance in all but one
study22-24, 36
. In adults, the most widely-used and validated method for estimating GFR from
serum creatinine level is the isotope dilution mass spectrometry (IDMS)-traceable
Modification of Diet in Renal Disease (MDRD) Study equation22-24
. The laboratories where
biochemical analysis of creatinine levels was conducted were calibrated to be IDMS-
traceable. The MDRD equation was preferred to the more recently validated “CKD-Epi”
equation37
because there were very few patients aged≥75 years in cohorts used to validate this
equation whereas the current study population was unrestricted by age.
eGFR = 175 x (Scr)-1.154 x (Age)-0.203 x (0.742 if female) x (1.212 if African American)
where eGFR is the estimated glomerular filtration rate in mL/min/1.73 m2, Scr is serum
creatinine level in mg/dL. The African population in the study population was <1% and
therefore no correction factor for ethnicity was required in the MDRD calculation of eGFR.
Page 35 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014
Statistical analysis
The study population was stratified into five categories according to eGFR (in ml/min/1.73
m2), corresponding to the stages of CKD: ≥90, 60-89, 30-59, 15-29, and <15 (Figure 1)
22-24.
Since data regarding proteinuria was not available, stage of renal impairment could not be
defined. Baseline characteristics were determined separately for the five eGFR strata, and
differences were investigated using chi-squared test for categorical covariates and Kruskal-
Wallis test for continuous covariates. Age-adjustment was performed by including age as a
covariate in a logistic regression model.
Event rates of IS/TE, bleeding and all-cause mortality were calculated for all patients by
eGFR category, stratifying by presence or absence of VKA therapy. Since VKA therapy was
the only form of OAC used during the study period, the terms, “VKA” and “OAC” are used
interchangeably in the analyses. Due to low numbers of patients and outcomes in the
categories with eGFR≥90 and <15 ml/min/1.73m2, rates were calculated for categories with
eGFR≥60, 30-59 and <30 ml/min/1.73m2. Haemorrhagic strokes were excluded from
analyses of “stroke” or “stroke/TE”. Event rates were also calculated by age and sex
categories. In each eGFR category, Cox-proportional hazards analyses were performed to
calculate 1-year survival for IS/TE, bleeding and all-cause mortality. Bivariate analyses of
event rates in different subgroups were used to calculate hazard ratios associated with renal
impairment and eGFR category.
Cox proportional-hazard regression models were constructed to investigate whether renal
impairment and eGFR were independent predictors of IS/TE. The risk associated with renal
impairment and eGFR were estimated in a univariate analysis, as well as a sex- and age-
adjusted analysis, an analysis adjusted for the risk factors included in the CHADS2 score, and
a multivariate analysis adjusted for all baseline characteristics in Table 1. All analyses were
repeated by eGFR category, and by combined stratification by renal impairment and eGFR.
Further, to test whether the results were influenced by patients initiating treatment with VKA,
we performed additional analyses excluding patients at the initiation of such treatment.
Finally, the net clinical benefit (NCB) was calculated, as originally proposed by Singer and
colleagues38
using the formula:
Page 36 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014

Net clinical benefit (NCB) = IS rate on no treatment- IS rate on anticoagulant)-1.5(ICH rate
on no treatment- ICH rate on anticoagulant
…. where IS=ischaemic stroke and ICH=intracerebral haemorrhage, which is the most
serious form of bleeding associated with OAC use. A modified formula with “haemorrhagic
stroke” instead of “ICH” was used to calculate NCB for the different eGFR categories. The
NCB is used by clinicians and researchers as a validated method of balancing risk of
ischaemic stroke against intracerebral haemorrhage.
A two-sided p-value <0.05 was considered statistically significant. All analyses were
performed with SPSS statistical software version 18.0 (IBM,USA).
Page 37 of 37
Downloaded From: http://journal.publications.chestnet.org/ by a University of Birmingham User on 01/14/2014