a consensus introduction to serum replacements and serum
TRANSCRIPT

REVIEW ARTICLE
A consensus introduction to serum replacements and serum-freemedia for cellular therapies
OHAD KARNIELI1, ORYAN MAKLER FRIEDNER2, JULIE G. ALLICKSON3,NAN ZHANG4, SUNGHOON JUNG5, DAVID FIORENTINI6, EYTAN ABRAHAM5,SHANNON S. EAKER7, TAN KAH YONG8, ALLAN CHAN8, SARAH GRIFFITHS9,AMY K. WHEN10, STEVE OH8 & OHAD KARNIELI1
1Karnieli Ltd and ATVIO Biotech,Ticon, Israel, 2PluristemTherapeutics,Matam Park,Haifa, Israel, 3RegenerativeMedicine Clinical Center,Wake Forest Institute for Regenerative Medicine,Wake Forest University School of Medicine,Winston-Salem,North Carolina, USA, 4Hematology Branch,National Heart, Lung, and Blood Institute NationalInstitute of Health, Bethesda,Maryland, USA, 5Cell Therapy Research &Technology LonzaWalkersville,Walkersville,Maryland, USA, 6Biological Industries Ltd., Beit Haemek, Israel, 7GE Healthcare Cell Therapy Division,Marlborough,Massachusetts, USA, 8BioprocessingTechnology Institute, Singapore, 9Stimlabs, Roswell, Georgia, USA,and 10Irvine Scientific, Santa Ana, California, USA
AbstractThe cell therapy industry is a fast-growing industry targeted toward a myriad of clinical indications. As the cell therapyindustry matures and clinical trials hit their pivotal Phase 3 studies, there will be a significant need for scale-up, processvalidation, and critical raw material quality assurance. Part of the well discussed challenges of upscaling manufacturing pro-cesses there is a less discussed issue relating to the availability of raw materials in the needed quality and quantities. TheFDA recently noted that over 80% of the 66 investigational new drug (IND) applications for mesenchymal stem cell (MSC)products analyzed described the use of FBS during manufacturing. Accumulated data from the past years show an accel-eration in serum consumption by at least 10%-15% annually, which suggests that the global demand for serum may soonexceed the supply. Ongoing concerns of safety issues due to risks of various pathogen contaminations, as well as issues relatedto the aforementioned serum variability that can affect final product reproducibility, are strong motivators to search for serumsubstitutes or serum-free media. it is important to note that there are no accepted definitions for most of these terms whichleads to misleading’s and misunderstandings, where the same term might be defined differently by different vendors, man-ufacturer, and users. It is the drug developer’s responsibility to clarify what the supplied labels mean and to identify thecorrect questions and audits to ensure quality.The paper reviews the available serum replacements, main components, basicstrategies for replacement of serum and suggests definitions.
KeyWords: serum replacement, serum free, defined media, cell therapy, animal component free, platelet lysate, cGMP media, fetalbovine serum, human serum, xeno free
Introduction
The cell therapy industry is a fast-growing industrytargeted toward myriad clinical indications. Most celltherapy companies are currently conducting clinicaltrials in phase 1 or 2 with several that are more maturein phase 3 or even early market approvals [1]. As thecell therapy industry matures and clinical trials hit theirpivotal phase 3 studies, there will be a significant needfor scale-up, process validation and critical raw material
quality assurance [1]. Addressing this need might resultin changes to culturing technologies, methods, raw ma-terial sourcing and testing. Because of the sensitivityof cells to their microenvironment, any change inculture conditions can affect cellular physiology, therebyaltering physical and performance characteristics andcritical quality attributes. Thus, uncontrolled scale-up may affect the final product’s activity or attributesand prevent it from being comparable to the originalsmaller-scale product [2,3]. Other challenges of
Correspondence:Ohad Karnieli, PhD, MBA, Karnieli Ltd and ATVIO Biotech, 57 Tamar Street,Ticon 36015, Israel. E-mail: [email protected]
(Received 8 April 2016; accepted 9 November 2016)
ISSN 1465-3249 Copyright © 2017 Published by Elsevier Inc. on behalf of International Society for Cellular Therapy.http://dx.doi.org/10.1016/j.jcyt.2016.11.011
Cytotherapy, 2017; 19: 155–169

upscaling manufacturing processes relate to the avail-ability of raw materials in the needed quality andquantities. Difficulties in keeping up with the supplyof raw materials while maintaining their quality andminimizing variability may prevent progression of large-scale production.
One of the most critical raw materials in the celltherapy industry is serum.Serum serves as a media sup-plement used for culture and enables cell growthstimulation.The most common type of serum used inthe cell therapy industry is fetal bovine serum (FBS).The U.S. Food and Drug Administration (FDA) re-cently noted that more than 80% of the 66 investiga-tional new drug applications for mesenchymal stromalcell (MSC) products analyzed described the use of FBSduring manufacturing [4]. The concentration of FBSin media ranged from approximately 2 to 20%, with10% FBS the most common concentration.The mostcommon alternative noted for these MSC investiga-tional new drugs was human platelet lysate. However,there are also other sources for bovine sera, such asnewborn calf serum or donor bovine serum, which areobtained from animals by repeated bleeding.Serum fromother animals (e.g., horse, sheep) are also in use [5].
Serum manufacturing
Currently, 90% of all serum used in the cell therapyindustry is supplied from three countries: the UnitedStates, Australia and New Zealand [2]. A large quan-tity of serum may be derived from any number ofanimals and can range from a few hundred liters toseveral thousand liters [2].Therefore, serum will oftenbe derived from a large number of animals.The pro-duction of FBS begins with removal of the calf fetusfrom the slaughtered pregnant cow in the abattoir [6].Next, blood is removed from the heart to prevent mi-crobial contamination and then centrifuged to removethe clot and blood cells from the serum. The serumis then passed through a 0.1-µ filter to remove eventhe smallest bacterial or fungal contaminants andmycoplasmas, effectively “sterilizing” the product. Ad-ditionally, the serum may undergo gamma irradiationsterilization to eradicate viruses and other pathogenssmall enough to pass through the filter. Between allmanufacturing steps, the serum is stored frozen tomaintain potency by minimizing degradation of bio-logical moieties. Representative samples from pooledbatches of serum are taken for various testing, in-cluding sterility to ensure safety of the product. Thefinal FBS product is also frozen until sampling forquality control release to buyers [7]. For current GoodManufacturing Practices (cGMP) applications, regu-lators including theWorld Health Organization requirethat serum be traceable throughout the supply chain,and it must originate from cattle that are free of bovine
spongiform encephalopathy and have not have in-gested prohibited animal feeds [8]. Several ethical issuescentered on potential suffering of the fetus have alsobeen raised regarding the production of FBS [6,9].Additionally, because the serum industry is a byproductof the meat industry, there is no real apparent eco-nomic incentive for cattle ranchers to increase herdsto source more FBS, limiting again the quantities.
Future availability of serum
In 2002, an estimated 600 000 L of FBS were pro-duced, of which only one-third met the regulatoryrequirements in cell therapy [6,9]. Accumulated datafrom the past years show an acceleration in serum con-sumption by at least 10–15% annually, which suggeststhat the global demand for serum may soon exceed thesupply [2,10,11]. Evidence of this growing demand isa threefold price increase in clinically used serum overthe past few years [2]. As already noted, FBS is cur-rently a byproduct of the cattle industry, and it wouldnot be economical for cattle to be bred solely for theproduction of serum. Currently, approximately 15 com-panies are audited and certified by the InternationalSerum Industry Association for theTraceability AuditChecklist that supports use of serum for the cell therapyindustry [2]. Therefore, it is unlikely that serum pro-duction in its current form will be able to keep up withfuture demand, which may be a key limitation in thecommercialization of cell-based medicine.
Inherited serum variation andquality assurance
Although FBS has been used for more than 50 years,the knowledge is incomplete regarding the connec-tions between serum components and cell productattributes influenced by culturing in the presence ofserum [11]. FBS is a complex medium supplement;subtle variation in its composition can influence keyproperties of cells due to their sensitivity to cultureconditions and might even cause alterations in the finalproduct [12]. This variation in serum compositiontherefore becomes a challenge for generating consis-tent and quality-assured cells in clinical-scaleproduction [2]. Potential causes of serum variationinclude genetic diversity of source herds and animaldiet as well as the serum manufacturing process itselfand the fact that there are about some 1800 pro-teins and 4000 metabolites present in serum [11].Furthermore, the current specifications for serummanufacturing and release are under a broad accept-able range, leading to inherent variation. Additionalmodifications and optimizations are needed to narrowthe ranges of these respective specifications and stan-dardize manufacturing methodologies. A procedureof serum screening from various lots before purchas-
156 O. Karnieli et al.

ing a lot of cGMP manufacturing is necessary and wellknown in the industry.
It is important to note that the commonly used“cGMP-grade” serum is misleading because Europe-an Union (EU) regulators argue that raw materials arenot manufactured under cGMP guidelines.The EU onlylicenses facilities making active substances and drugproducts, but not raw materials, as cGMP compliant.Nevertheless, a quality system is important to ensurethat the manufacturing process is well documented andreproducible with a change control mechanism. It isalso important to clarify that this quality system doesnot necessarily ensure the quality of the material manu-factured, and the responsibility for the safety and efficacyof the drug product lies in the hands of the cell therapymanufacturer; therefore, this quality system must beaudited and approved by the customer (cell therapymanufacturer). Critical process design elements needto be considered to ensure good quality, for example,inclusion as necessary for viral reduction/eliminationsteps, temperature control, in process control, andprocess validation up-to-date studies.Additionally, a sup-plier’s quality control (QC) testing may not cover allaspects required by the developer. In many cases, thesupplier’s QC process may need to be confirmed and/or supplemented with functional assessments such asgrowth, marker expression or activity profiling becausethe usual QC consists of tests such as total protein, im-munoglobulin, sterility, pH and osmolality. It isimportant to note that in many cases, the QC is doneafter manufacturing and before irradiation. The irra-diation can affect the serum’s performance; therefore,it is important to establish a quality assurance strate-gy for the post-irradiation testing. In addition to a qualitysystem, relevant QC and validation, it is critical to havea European Directorate for the Quality of Medicinesand Healthcare (EDQM) Certificate of suitability fortransmissible spongiform encephalopathies risk and acertificate of origin. Each local health authority may haveadditional tests and specifications; therefore, it is im-portant to understand where the product is intendedto be used and meet the relevant local regulatoryguidelines.
Alternative serum replacements
Human platelet lysate
The essential physiological role of platelets in woundhealing and tissue repair builds the rationale for theuse of human platelet derivatives in regenerative med-icine. Abundant growth factors and cytokines storedin platelet granules can be naturally released by throm-bin activation and clotting or artificially by freeze/thaw-mediated platelet lysis, sonication or chemicaltreatment. Human platelet lysate (HPL) prepared bythe various release strategies has been established as
a suitable alternative to FBS as culture mediumsupplement, enabling efficient propagation of humancells under animal serum-free conditions for a mul-tiplicity of applications in advanced somatic cell therapyand tissue engineering. In parallel with the spread ofin vivo use of platelet-derived preparations, the use ofplatelet lysates for in vitro cell proliferation was initi-ated in the 1980s. After lysis of outdated plateletconcentrates or platelet rich plasma, the lysates wereefficiently used for in vitro culture of fibroblasts, en-dothelial cells or tumor cell lines [13,14]. It isconsidered that approximately 15–20% of whole blooddonations that are driven by the need for red bloodcells are currently used to prepare platelet concen-trates and that 5–20% of those expire and can serveas raw material for HPL. Considering that an esti-mated 100 million whole blood donations are collectedeach year in the world [15], these figures suggest apotential for approximately 100 000–250 000 L of HPLper year from outdated platelet concentrates.
Human serum
A promising alternative for culture of human cells isthe substitution of FBS with converted human ABserum (HABS), which is routinely tested for viral con-tamination. HABS supports the propagation of humanosteoblasts, chondrocytes and bone marrow cells[16–19] as well as glioma and melanoma cancer celllines [20,21]. These studies suggest that HABS maybe a good candidate to replace FBS as a supplementfor cell culture. The main limitation of this alterna-tive is the amount that can be collected and the riskof using human blood products and distributingunknown and new human pathogens.
Serum free, xeno free and chemically defined
In the past several years, efforts were made both byacademia and industry to develop serum replacementsfor cell culture. Such replacements are commonly calledserum-free media, xeno-free media and chemicallydefined media. The terminology has evolved duringthe years, resulting in confusion and lack of clear-ness. We have attempted to suggest the followingterminology to better define the space.
Recommended terms and definitions
Before defining any of the generally used terms in thecell therapy industry, it is important to note that thereare no accepted definitions for most of these terms,and the following definitions are our recommenda-tions only.The same term might be defined differentlyby different vendors, manufacturer and users. It is thetherapies developer’s responsibility to clarify what the
Serum replacements and serum-free media for cellular therapies 157

supplied labels mean and to identify the correct ques-tions and audits to ensure quality.
In general, a complete cell culture medium con-sists of a defined basal medium plus growth supplementsthat are often classified by their source (i.e., animalserum, human serum or platelet lysates, animal or planthydrolysates or recombinant proteins) and the degreeof their characterization and traceability. For example,“ill-defined” would apply to serum, platelet lysates,animal/plant hydrolysates or soy phospholipids; all ofthese are more defined then serum but still consist ofunknown factors and quantities. “Semi-defined” wouldapply to partially purified/enriched serum proteins, whichmay still be associated with unidentified trace ele-ments such as pooled human serum albumin (HSA);“chemically defined” would apply to synthetic mate-rials or purified recombinant proteins.
Consequently, cell culture media are normally clas-sified by the source and characterization of suchsupplements. Impurities in media supplements alsoneed to be taken into consideration; for example,plasma or plasma-derived materials are likely to containanticoagulants, and it was found that heparin affect-
ed colony formation of MSCs [22]. Some developershave chosen to collect autologous serum as a byproductof apheresis, but the amount of citrate added is highlyvariable. Our recommended classification of cell culturemedia, and their definitions and examples are sum-marized in Table I and Figure 1.
Of note, medium formulations are not often fullydisclosed. Consequently, even though there are com-mercial products advertised as “chemically defined,” itcan be ambiguous as to whether they really containdefined components only. Moreover, this term is some-times misused in the field. For example, human serumalbumin is often considered to be “chemically defined”in its natural (non-recombinant) form; however, itcannot fit the chemically defined term as we suggestbecause it can have many undefined contaminants, suchas hormones, lipids and trace elements, associatedwith it.
Main active components
Typical serum-free culture media consist of basalculture medium supplemented with defined and/or
Figure 1. An exemplified schematic to demonstrate the classification of cell culture media: serum-based (SB), serum-free (SF), xeno-free(XF), animal component–free (ACF), protein-free (PF), and chemically defined (CD). Serum-based media typically contain animal sera.Media containing human serum or plasma are not serum-free but xeno-free. Serum-free media typically contain purified proteins that arederived from animals or humans and are likely associated with other defined and undefined factors. Media containing purified humanproteins and/or human platelet lysate are serum-free and xeno-free. Animal component-free media do not contain human- and animal-derived components and often contain plant hydrolysates. Chemically defined media are typically made up of human recombinant proteinsand synthetic components. Protein-free media do not contain proteins but often include hydrolyzed proteins and ill-defined native lipids.
158 O. Karnieli et al.
undefined ingredients. Basal culture media such asAlpha-Minimum Essential Medium, Dulbecco’sModified Eagle’s Medium/F12 (1:1), Iscove’sModified Dulbecco’s Medium, and RPMI contain amixture of inorganic and organic salts and buffers,amino acids, vitamins, carbohydrates and trace ele-ments. These basal culture media are essentiallydeficient of most nutritional content, so additionalcomponents are required to support the in vitrogrowth of human cells. Such components includeantioxidants, additional trace elements, lipids, fattyacids (cholesterol, phospholipids), and, in addition,carrier proteins (albumin, transferrin), insulin and/
or insulin-like growth factor (IGF)-1, hormones andgrowth factors.
Depending on the intended application, availabil-ity, and the developer’s preferences, the culture mediummay contain human-derived components (xeno-free, XF) or be chemically defined and/or animalcomponent-free (ACF).The requirements (e.g., per-formance, quality and source) for these main growthpromoting raw materials such as growth factors varyand depend on the cell type, matrix, culture system(two- [2D] and three-dimensional), intended use,classification of the final medium (serum-free, xeno-free, ACF) and regulatory requirements.
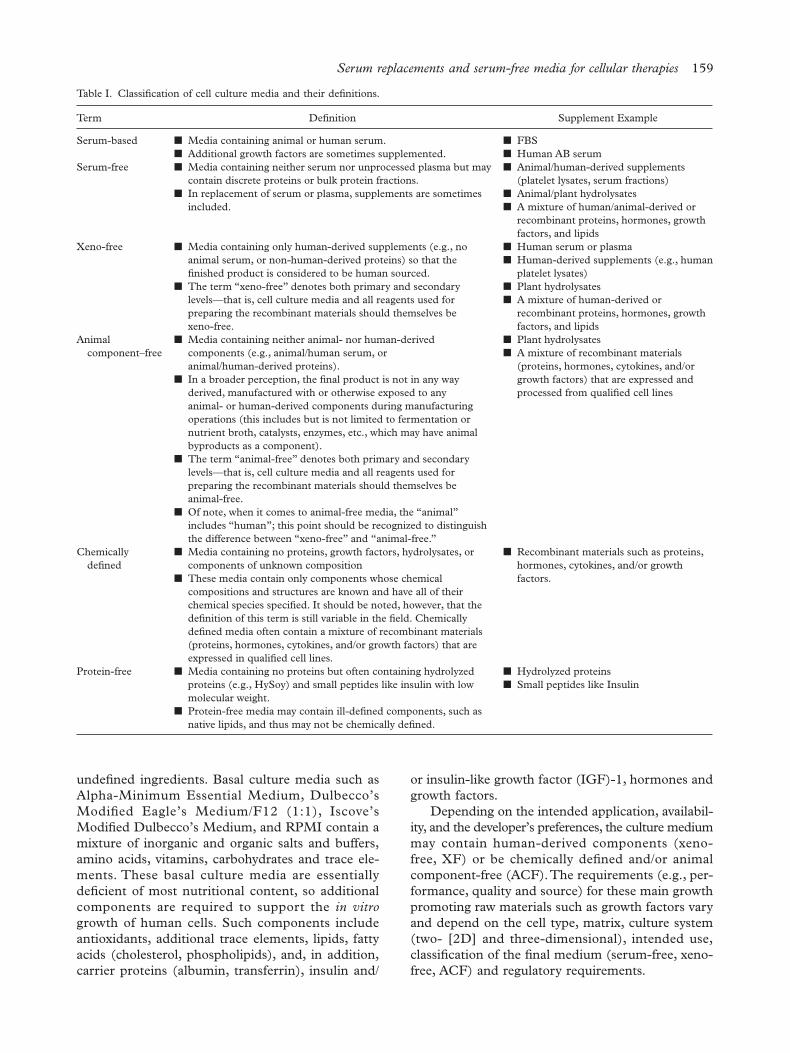
Table I. Classification of cell culture media and their definitions.
Term Definition Supplement Example
Serum-based ■ Media containing animal or human serum.■ Additional growth factors are sometimes supplemented.
■ FBS■ Human AB serum
Serum-free ■ Media containing neither serum nor unprocessed plasma but maycontain discrete proteins or bulk protein fractions.
■ In replacement of serum or plasma, supplements are sometimesincluded.
■ Animal/human-derived supplements(platelet lysates, serum fractions)
■ Animal/plant hydrolysates■ A mixture of human/animal-derived or
recombinant proteins, hormones, growthfactors, and lipids
Xeno-free ■ Media containing only human-derived supplements (e.g., noanimal serum, or non-human-derived proteins) so that thefinished product is considered to be human sourced.
■ The term “xeno-free” denotes both primary and secondarylevels—that is, cell culture media and all reagents used forpreparing the recombinant materials should themselves bexeno-free.
■ Human serum or plasma■ Human-derived supplements (e.g., human
platelet lysates)■ Plant hydrolysates■ A mixture of human-derived or
recombinant proteins, hormones, growthfactors, and lipids
Animalcomponent–free
■ Media containing neither animal- nor human-derivedcomponents (e.g., animal/human serum, oranimal/human-derived proteins).
■ In a broader perception, the final product is not in any wayderived, manufactured with or otherwise exposed to anyanimal- or human-derived components during manufacturingoperations (this includes but is not limited to fermentation ornutrient broth, catalysts, enzymes, etc., which may have animalbyproducts as a component).
■ The term “animal-free” denotes both primary and secondarylevels—that is, cell culture media and all reagents used forpreparing the recombinant materials should themselves beanimal-free.
■ Of note, when it comes to animal-free media, the “animal”includes “human”; this point should be recognized to distinguishthe difference between “xeno-free” and “animal-free.”
■ Plant hydrolysates■ A mixture of recombinant materials
(proteins, hormones, cytokines, and/orgrowth factors) that are expressed andprocessed from qualified cell lines
Chemicallydefined
■ Media containing no proteins, growth factors, hydrolysates, orcomponents of unknown composition
■ These media contain only components whose chemicalcompositions and structures are known and have all of theirchemical species specified. It should be noted, however, that thedefinition of this term is still variable in the field. Chemicallydefined media often contain a mixture of recombinant materials(proteins, hormones, cytokines, and/or growth factors) that areexpressed in qualified cell lines.
■ Recombinant materials such as proteins,hormones, cytokines, and/or growthfactors.
Protein-free ■ Media containing no proteins but often containing hydrolyzedproteins (e.g., HySoy) and small peptides like insulin with lowmolecular weight.
■ Protein-free media may contain ill-defined components, such asnative lipids, and thus may not be chemically defined.
■ Hydrolyzed proteins■ Small peptides like Insulin
Serum replacements and serum-free media for cellular therapies 159

Serum albumin
Bovine serum albumin is commonly used in serum-free medium formulations. Albumin is a carrier proteinfor fatty acids, lipids and trace elements. In addi-tion, albumin is able to bind toxic components inthe culture medium and can protect cells from shearstress. HSA is typically used in xeno-free formula-tions and is available as pooled serum of clinical-grade preparations. The performance of the HSA isvery much dependent on the source because themethod of isolation from blood might have an impacton the final product’s quality and characteristics. Itis necessary to screen HSA suppliers for the opti-mized product for a specific cell culture system. Inaddition, testing and approval of a specific lot isrequired to avoid lot-to-lot variations. In ACF mediumformulations, fatty acids, lipids, phospholipids andtrace elements can be added as a replacement forthe use of albumin.
In recent years, a variety of recombinant forms ofhuman albumin have become commercially avail-able. Recombinant human albumin is more likely tobe compliant with regulatory requirements and mayserve as an ACF ancillary product for cell therapy andregenerative medicine applications. Regulatory re-quirements include screening of the various materialsavailable (e.g., from recombinant Saccharomycescerevisiae or recombinant rice), production methodsas well as the supplier’s quality system.
Human transferrin
Human transferrin is a carrier protein required to trans-port iron into animal cells for optimal cell growth andexpansion. Human transferrin is extracted from humanplasma, and the source plasma is collected for clini-cal blood donations tested and approved for humanuse.
Recombinant analogues of human transferrin arecommercially available and have equivalent perfor-mance as the native form but at the moment are moreexpensive and limited in scale. For recombinant humanalbumin, it is necessary to screen the various mate-rials available (recombinant yeast, recombinant rice)as well as the available suppliers.
Alternatively, iron salts such as iron citrate, ironethylenediaminetetraacetic acid, and other iron ch-elators have been used in ACF media.The performanceof these alternatives is very much dependent on thecells and culture system used. Iron salts may have neg-ative effects on cell growth due to the formation offree radicals as well as limited availability of iron tothe cells. The type and concentration of iron saltshould be optimized for each cell type and culturesystem.
Insulin
Insulin is involved in glucose uptake, lipid metabo-lism, and DNA synthesis.As clinical grade recombinantinsulin is currently available and is widely used in mostserum-free formulations in the concentration range of2–10 mg/L.
Alternatively, recombinant IGF-1 may be used inXF or ACF formulations yielding enhanced perfor-mance with some cell types due to the direct activationof IGF-1 receptor. IGF-1 is typically used in muchlower concentrations than insulin.
Hormones
Commonly used hormones in serum-free media for-mulations are glucocorticoids, thyroid hormones andestrogens. Hydrocortisone, progesterone and dexa-methasone have been shown to increase proliferationof adherent cells. Hormone combinations may be akey component of ACF media, taking into account theirspecificity, particularly for certain cell types used incell therapy applications.
Growth factors
Growth factors are mitogens that stimulate cell pro-liferation and are crucial in maintenance of cellcharacteristics. The most commonly used growthfactors in XF/ACF media include basic fibroblastgrowth factor, epidermal growth factor, transform-ing growth factor beta, vascular endothelial growthfactor, and platelet-derived growth factor.These growthfactors are available as recombinant proteins and arewidely used for cell therapy applications.The specif-ic growth factors, concentrations and synergistic effectsplay a crucial role in achieving an optimized, cell spe-cific, serum-free ACF medium. Several growth factorsare manufactured under current cGMP, but they areless commonly used due to their premium pricing.
Serum-free, xeno-free and ACF media are highlycell and culture system specific. Medium develop-ment should involve screening and testing appropriatefactors for their effects on cell growth, maintenanceand characteristics for a safer, optimized and regulatory-compliant cell culture system.
Scientific experience with the use ofserum-free
The strategy of how to approach the use of serum-free media, FBS replacements or serum reductionstrategies for cell culture, either in the academic settingor in the commercial setting, is of critical impor-tance.The first line of assistance can be found in theliterature, which can provide a baseline of scientificevidence discussing the protocols and challenges inusing specific serum replacements with specific cell
160 O. Karnieli et al.

types and the resulting advantages and disadvan-tages of the approach. Herein we bring several examplesof such evidence, mostly on the use of serum-freemedia. In most cases, serum-free media can be furtheroptimized for specific cell types and processes.
Efforts have been made to develop serum-freemedia for various cell types in regenerative medi-cine, including human MSCs (hMSCs), inducedpluripotent stem cells and T cells. Some of the opti-mized serum-free media have even demonstratedenhanced growth-promoting performance com-pared to conventional serum-containing counterparts[23–25]. For instance, a systematically developedserum-free medium supported a significantly highercell growth in the primary and subsequent culturesof BM-hMSCs compared to a classical serum-containing medium (Dulbecco’s Modified Eagle’sMedium supplemented with 10% FBS), while main-taining the critical characteristics of BM-hMSCs [22].Moreover, the use of the serum-free medium led tothe consistent production of a more homogeneoushMSC population, which was smaller in size than thosein the serum-containing medium [23]. Serum-free,xeno-free media for hMSC culture have also been com-mercialized by numerous manufacturers (BiologicalIndustries, Irvine Scientific, LifeTechnologies, MiltenyiBiotec, StemCell Technologies, GE and others), andsimilar results have been reported using some com-mercial media [26].The size of cells to be administeredto patients could be an important factor from a ther-apeutic viewpoint because several studies with animalmodels demonstrated that most hMSCs grown in FBS-supplemented media were trapped in the lung [27–29].The generation of small hMSCs in an optimizedserum-free condition may offer a significant benefitin different therapies if the small cells can travel throughthe lung and home to the site of injury or disease athigh efficiencies [30]. Moreover, the ability to producehighly proliferative cells at a smaller size might providea benefit from the cell manufacturing standpointbecause this could reduce the cell culture process timeand the number of culture vessels required tomanufacture a large size of lot and thus save in costof goods.
There are a variety of serum-free media either com-mercially available or reported in the literature. Mediumformulations can significantly affect cell characteris-tics (i.e., growth pattern, gene expression, phenotypeand functional properties); therefore, it is crucial toevaluate media for the intended therapeutic applica-tions, which can only be done once the cells arecharacterized and the critical quality attributes and ex-pected mechanism of action (MoA) are defined.Further optimization of a selected medium formula-tion may be needed for the development of a robustcell-manufacturing platform. As pointed out earlier,
in vitro studies conducted by different investigators haveoften demonstrated conflicting results. An encourag-ing set of in vivo and in vitro data for the use of serum-free media was recently reported [31]. In this study,umbilical cord–derived MSCs (UC-hMSCs) grownin a commercial serum-free medium exhibited strongimmunosuppressive activities and secreted high levelsof immunomodulatory cytokines at similar levels com-pared with those expanded in a control serum-containing medium. Moreover, to evaluate the in vivotherapeutic properties of culture-expanded UC-hMSCs in the commercial serum-free medium, theauthors administered the cells into a rat model of pul-monary arterial hypertension induced by monocrotalineand observed a substantial reduction in the thick-ness of the pulmonary arterial wall and an increasedsurvival rate compared with control cases with no treat-ment. The degree of in vivo therapeutic activities(presumably via immunomodulation) was compara-ble in the serum-free culture-expanded cells and cellsgrown in the serum-containing medium. Several studiesin the recent years had shown success in culturing Tcells in a serum-free-based medium showed compa-rable proliferation capability and efficacy [24].
Since 2005, initiated by a study of [32] describ-ing the preparation and efficient use of human plateletlysate (HPL) for expanding MSC, a series of reportshave shown that both allogeneic and autologous HPLare superior to FBS for stimulation of cell prolifera-tion [33–35]. This highly efficient stimulation of cellproliferation enabled large-scale of MSC for clinicaluse in a single culture period of 11–16 days withoutfurther passage, while maintaining genomic stability.
Additionally, use of AB serum complemented withplatelet-rich plasma for cell therapy was shown to beaffective in 2007 for culturing of MSCs isolated formadipose tissue [36].
Serum replacement and reduction strategies
Taken together, commercial-scale cell therapy manu-facturing is expected to demand higher amounts ofserum than what is currently or potentially available.Ongoing concerns of safety issues due to risks of variouspathogen contaminations, as well as issues related tothe aforementioned serum variability that can affect finalproduct reproducibility, are strong motivators to searchfor serum substitutes or serum-free media [2,37,38].However, a serum replacement strategy is not alwaysthe only measure or the best measure that can be taken.Alternative strategies such as serum reduction or useof human-based serum can and should be investi-gated to better ensure the supply availability. In casesof small-scale manufacturing for rare diseases where theinitial active cell therapy was developed using serum,the cost-effectiveness, feasibility and risk of changing
Serum replacements and serum-free media for cellular therapies 161
from serum may hinder the ability to bring the treat-ment to patients in need. In such cases, ensuringserum supply may be feasible, and additional safetymeasures such as viral testing in activation steps couldbe a more relevant and preferred strategy. Each caseshould be investigated separately, taking into accountthe aforementioned limitations and risks, and devel-opers should try to reduce or eliminate serum use ifpossible.
Strategies for media and serum replacements
Culture media and their supplements aim to providemost or all of the cells’ essential requirements andwould ideally mimic the in vivo situation as much aspossible. The following list covers some of the func-tions required of culture media:
1. Isotonic environment, basic salts, metal ions,osmolality
2. Buffer system to maintain pH (may be CO2 de-pendent or independent)
3. Essential amino acids4. Carbon source, typically sugar (e.g., glucose,
galactose)5. Lipids essential for cell growth/maintenance6. Iron carrier (e.g., transferrin)7. Growth factors/hormones (e.g., platelet-derived
growth factor, insulin-like growth factor-1,hydrocortisone)
8. Attachment factors (e.g., vitronectin, collagen)9. Other factors to maintain phenotype/differentiation
state, which can include specific growth factors10. Protection from shear forces (e.g., passaging/
handling, especially in bioreactors which includesurfactants or albumin)
When evaluating media, developers must take intoconsideration the following factors in addition to spe-cific cell type functionality:
1. Attachment potential during primary isolation andduring the expansion phase to ensure that thereare no population shifts due to different attach-ment potentials
2. Population doubling time, which is the durationin which the cell population doubles
3. Population doubling level, which is the amountof population doublings from isolation to senes-cence or change in phenotypic and activitycharacterization
4. Cell and population phenotypic stability andin relevant cases differentiation potential andstate
5. Genetic stability of the cell population in the dif-ferent population doubling levels, which can be
demonstrated for example by karyology changesand transformations.
6. Cell fragility and cell size are a good indirect mea-surement that can imply changes in the cell qualityand stability.
7. Relevant biological functions to the intendeduse (need to understand likely MoA; e.g.,biodistribution [chemokines], differentiationcapacity, immune modulation/stimulation,etc.)
8. Donor variation because autologous healthy vol-unteer cells may behave differently to cells frompatients with disease
Although rapid cell proliferation might be desir-able from a manufacturing and cost of goodsperspective, it needs to be balanced against genetic,phenotypic and functional stability. Media plays a rolein cell proliferation capability and function and canlead to genetic instability or senescence of part or allof the cell population.
The vast number of considerations, combined withfactors needed for cell growth and maintenance, meansthat identifying the optimal culture media requires ahuge number of experimental conditions to be con-sidered. Additionally, the optimal concentration of thecomponents must be identified, especially growthfactors and cytokines that might have undesirableeffects such as cell transformation at the wrong con-centrations. Undertaking such a task is likely to requirestatistical approaches such as design of experiments.Because of this complexity, most developers have takenan empirical approach and test a limited number ofpublished or proprietary formulations to identify whichappear to be suitable. Once an available formulationseems to perform in a similar or reasonable activity,there is an option to further optimize the media toperform more efficiently. A further confounding factoris that the optimal media may be different at variousstages of manufacturing giving, for example, an ad-vantage to one subpopulation in the initial selectionstage by that changing the product if used in the earlystages but allowing growth to both subpopulations andcan be used efficiently after the selection had accruedresulting in reduction in the amount of serum usedduring the manufacturing process.
When choosing other alternatives for FBS for cellculture, previous data on growth and expansion of spe-cific cells in serum replacement media is helpful andshould be investigated via literature and discussionswith the vendor.
The second aspect supporting the use of serum-free media is the need for scientific and practicalculture support from the serum-free media manufac-turer. In many cases, manufacturers will be familiarwith their custom media formulations and how to avoid
162 O. Karnieli et al.

or overcome some of the issues that may arise fromthe use of a non-optimized media. Examples of issuesthat may need to be addressed and for which man-ufacturer’s support can be available include thefollowing:
• Requirement for selecting a serum-free mediumformulation for a specific target cell population
• Factors to enhance or reduce cell growth ratesand doubling times
• Use of attachment factors to facilitate cell at-tachment during the initial culture period aftercell seeding
• Matching serum-free medium attachmentsupplements/protocols to culture surface and cells
• Cell seeding densities• Alteration in the biological properties of the cells
(secretome, differentiation, cell size, immune-related properties)
• Alteration of surface marker composition orfrequency
• Adaptation methods of cells to serum-free culture• Primary isolation of cells using serum-free
media• Shelf-life of media, storage conditions (temp, light,
etc.)• Changing culturing systems, which can affect ad-
herence or/and sheer force
For some of these issues, manufacturers should beable to refer users to papers and protocols and tosupply advice on how to avoid and/or deal with theseissues. End users should be proactive in requesting as-sistance from manufactures both before using themedia and after purchase.
Attachment substrates for adherent culture
Serum contains attachment substrates that initiate cellattachment and spreading on culture ware surfaces.When using a serum-free culture system, a separateattachment substrate is required for MSC culture inaddition to published and commercially availableserum-free media.
Human plasma fibronectin is a common attach-ment substrate used in serum-free culture systems.Plasma source and viral safety, as well as regulatoryacceptance, should be considered with regard to cellsaimed for cell therapy.
Synthetic surfaces, such as synthetic peptides con-taining the Arg-Gly-Asp (RGD) motif for cellattachment, are still fairly new. Recent reports dem-onstrated some success in the use synthetic peptidesduring cell expansion [39,40]. Synthetic peptidesand surfaces offer the advantage of being animal-components free and having potential for scalability.
Additionally, the coating procedure that is neededfor the culture dishes adds additional stamps and ma-nipulations to the culturing process, thereby increasingprocessing time and adding risk of contamination dueto open manipulations. The preceding process stepsmight be achievable in small scale but could add sig-nificant challenges and cost in a cGMP large-scalesetting.
The main objective in the switch from serum-containing media to an alternative culture media optionis to retain the desired biological functions, most im-portantly those required for the intended clinical effect.Some understanding of the hypothesized MoA is nec-essary to retain the biological functions; however, theMoA is often not well understood early in develop-ment when this change would be made. The attemptto switch culture media must be done only if a goodactivity/potency assay is available and will require re-testing of the material to prove comparability. As anexample, many developers of MSC products focus onretaining the International Society for CellularTherapy–defined MSC characteristics, including phenotype andchondrogenic, adipogenic and osteogenic capacity [41].However, these are the characteristics of freshly iso-lated MSCs, and not all of these activities are likely tobe involved in the intended clinical use and have beendeveloped as the consensus phenotype and not neces-sarily related to the specific activity.The criteria we havedescribed are not considered sufficient to prove com-parability but serve as a minimal base for consensusphenotype of MSCs. Consequently, media optimiza-tion does not require that all in situ functions of an MSCpopulation are retained but that the critical MoA relatedproperties are present, which have to be judged indi-vidually case by case. As an example, if the product isbeing developed to modulate immune responses, suchas autoimmune disease, then osteogenic and adipogenicactivity are unlikely to be required and might also beseen as undesirable and risk factors.The comparabil-ity criteria must be predefined and tested to ensure thatchanges due to different media conditions do not affectthe safety and efficacy of the product. Therefore, it isimportant to define the main critical quality and bio-logical attributes that relate to the biological activity andensure that they are not negatively affected.
The approach to identifying the appropriatemedium depends on whether it is intended for an initialmanufacturing strategy or change to an existingmedium composition when development is already un-derway. In preclinical development, the focus wouldbe to optimize cell function and growth. Mid-development, the safest approach would be to mimicthe properties of the existing media performancebecause it may be difficult to justify that differencesin performance are not significant (i.e., do not altersafety and efficacy of the product).
Serum replacements and serum-free media for cellular therapies 163

Main issues to be considered in choosing the source ofand developing a product
Currently, serum provides several functions in cellculture. Development and use of a serum-free mediadepends on finding acceptable substitutes for eachfunction, as well as reliable and certified sources ofindividual components. At each stage of medium de-velopment, removing an undefined animal-derivedcomponent requires the identification of active com-ponents (such as albumin-bound signaling lipids),identification of a suitable biological substitute and re-liable sourcing of the material. Xeno-free culturemedium does not contain non-human-derived com-ponents. Human serum albumin, transferrin or platelet-derived lysate are potential good substitutes, but theymight be the restricted in terms of sourcing, differ-ent regional regulations and quality assurance. Achemically defined media could address this issue.Lessons could be learned from Chinese Hamster Ovary(CHO) cell culture, where chemically defined mediumhas been used in industry for a long time, but no ex-amples of MSC chemically defined media exist as ofwriting.
A number of xeno-free serum-free medium for-mulations are currently published and/or commerciallyavailable [10] with new formulations coming to marketfrequently as the science progress. The next genera-tion of medium is ACF, which eliminates the use ofanimal-derived components such as human serumalbumin. The identification and use of relevant re-combinant proteins may be considered as a step towardchemically defined medium.
Regulatory requirements
For substances prepared from blood, an additional reg-ulatory barrier exists: the blood needs to meet specificquality and safety standards. In the EU, a plasmamaster file can be helpful to ensure that isolation andpreparation are under a suitable quality system to thenincorporate appropriate viral clearance and urification,for example.The nature of media and the quality andregulatory aspect is still being defined, and theregulation is not clear of the exact testing and manu-facturing requirements.These will probably evolve andbecome clearer once the industry matures, but it willstill be process-, product- and regulatory agency–dependent and might change between products andterritories.
Replacement of other solutions during cell cultureWhen transforming to a serum-free media, the culturebehavior might change and require optimization. Suchsolutions might include trypsinization, neutraliza-tion solution after the trypsinization procedure (ifneeded) and cryopreservation. Because the adherence
of the cells might change, the trypsinization might needto be optimized in duration and concentration of theenzyme. Additionally, the neutralization potential ofthe media and the serum replacements should be assetsand tested with potential new neutralization solu-tions such as albumin. Additionally, as the mediumcomposition changes, it is important to test the cells,their survival and recovery post-cryopreservation andoptimize the media for this purpose.
As the medium becomes more defined duringdevelopment, it becomes more cell type–specific as well asexpansion process–specificAs culture media becomes increasingly defined (ACFmedia and chemically defined media that contain re-combinant or synthetic proteins/peptides), they becomemore cell- and process-specific.The same medium andattachment substrate that support successful growthwith MSCs from certain tissues may fail with MSCsfrom different tissue sources [42,43].This also holdstrue for the specific expansion process because theculture system may introduce additional require-ments from the medium. For example, culture of cellson static microcarriers may already introduce differ-ent medium requirements compared to 2D monolayerculture. Six sources of MSCs behaved differently invarious commercial serum free media in 2D versusmicrocarrier cultures [44]. Furthermore, microcarrierculture of cells in bioreactors introduces shear forcesthat stress the cells and may induce phenotypic changes[45,46]. FBS contains certain factors that protectagainst shear forces [47], which may have to be sub-stituted for during adaptation of serum-free media tobioreactor cultures (such as addition of Pluronics) [48].SeeThompson et al. and Pagliara et al. [49,50] for ex-amples of the effects of pluronics on cells. Theseeffects of pluronics may be fine for biotech manufac-ture of CHO cells but not for cell therapy products(CTP).
Serum replacement media screening before substitutionfrom media containing FBSExpansion medium used can affect cell prolifera-tion, time to senescence, and differentiation ability [51].These effects of expansion medium may have a greatimpact on manufacturing yields and the final thera-peutic product.Therefore, it is necessary to prototypeand test the final medium version in early-stage de-velopment, using the specific cell line to avoid majorchanges to production that may introduce variabilityin cell production. A media screening to better un-derstand the effects of expansion medium on cellproduct is vital before substitution of the originalmedia. Time and resources invested in this processshould be taken under consideration.
164 O. Karnieli et al.

Sourcing of individual componentsIndividual components of serum-free media may beanimal-derived, or ideally recombinant (if available).Animal- or human-derived components should becGMP processed. For large-scale production of cells,sufficient quantities of clinical grade raw materials mustbe available. Cost can be an issue with animal- andhuman-derived sources of product, such as plasma-derived albumin or fibronectin. The use of a clinicalgrade human plasma (meeting Pharmacopeia andmedical grade guidelines) as a source for humanfibronectin is required. Production processes shouldbe in accordance with a defined and audited qualitysystem and meet all required safety regulations. Meetingthese production processes may in turn lead to lim-itation in availability of the material as the need forlarger quantities grow.
Certain medium components, such as transfer-rin, have the disadvantage of lacking a reliable sourceof GMP raw material, which will be problematic asthe industry continues to grow. Recombinant ver-sions of proteins have been developed, such asfibronectin and laminin, offering the potential of a trulyACF component. However, at present, recombinantproteins are cost-prohibitive for large-scale cellproduction.
ConsistencySerum is a highly complex mixture of lipids, pro-teins and cytokines and is variable depending on thevendor, source and production methods. Becauseserum is a biological material, there will be lot-to-lotvariability. In many applications, serum lots must bepre-screened and qualified for use to eliminate processvariability. This process can be time-consuming andexpensive. Manufacturing processes involving the useof well-characterized media with raw materials that aresynthetically produced or made from highly consis-tent expression system seem to be ideal. Alternatively,efforts have been made to develop media supplementedwith a mixture of purified proteins (i.e., attachment-and growth-promoting proteins and carrier pro-teins), hormones, growth factors and additionalnutrients [22]. Although these media are not chem-ically defined, their “semi-defined” nature may helpreduce the potential for variability and streamline themanufacturing process.
Security of supplyCurrent global demand for serum is high, and the pro-duction levels of high-quality serum are generally fixed.Therefore, the market is highly volatile, and prices canfluctuate greatly [2]. Switching to alternative raw ma-terials may help reduce this risk because multiplevendors can be established to set up a secure supply
chain. However, consideration must be given to thedevelopment of serum-free media, in that some of therecombinant proteins or growth factors that are nec-essary for biological activity of the therapy of interestmay also hold particular manufacturing limitations.Supply and quality agreements with vendors shouldbe in place to ensure the product’s long-term avail-ability and quality.
Product efficacyChanging medium formulations may changevarious aspects of the biology of cells, such as theirsecretory and immunomodulatory properties, differ-entiation potentials and growth kinetics. However,the experimental outcomes in the literature haveoften demonstrated conflicting data. A good exampleis the use of human platelet lysate (hPL) in replace-ment of FBS for the culture of hMSCs. Numerousstudies reported that the use of allogeneic hPL re-sulted in a significant increase in hMSC growth whilemaintaining the immunomodulatory properties anddifferentiation potentials. By contrast, other studiesreported that hMSCs showed a reduced osteogenicor adipogenic differentiation property [52,53] andan altered expression profile of surface moleculesand a decreased immunosuppressive capacity [54]when cultured in hPL-containing media. In recentyears, HPL has been manufactured under GMP con-ditions by several vendors including companies suchas Akron Biotech, Regentec, Compass Biomedical,Mill Creek, Macopharma, Helios, ZenBio, Trinovaand PL BioScience. One major drawback to date ofHPL is the limited batch size, when pooled at suffi-cient scale, 3.0–3.5 L of HPL can be obtained bymixing the platelet concentrates from up to 50 donors.Pooling, however, increases the risks of contamina-tion with human bloodborne pathogens, a risk thatcan be greatly reduced by the current donor screen-ing and testing strategies applied in licensed bloodcenters, as well as by pathogen inactivation [55]. Forcases in which MoA has been relatively well definedor the clinical data are clear, such as chimeric antigenreceptorT-cell (CAR-T) therapies, correlations betweenchange of medium formulations and therapeutic ef-ficacy may be readily evaluated. However, for othercases in which the MoA has not yet been clarified,such as hMSC therapies, it is challenging but notinsurmountable to assess the product’s efficacywhen trying to change medium formulations, partic-ularly when switching from serum-based to serum-free medium. In this regard, it is crucial for thecell therapy product developers to start their re-search and clinical studies with a medium type thatis favorable in regulatory and manufacturing perspec-tives as early as possible in their development stages.Clearly, this should represent a serum-free medium
Serum replacements and serum-free media for cellular therapies 165

formulation (or ideally, chemically defined) de-signed for the culture of a specific cell type.
Regulatory and quality issues
For cell therapy products that use serum, regulatoryguidelines are in place that make manufacturers re-sponsible for ensuring and documenting the impactof sera on the quality, safety and efficacy of the finalproduct (lot-to-lot performance, sterility, etc.).To date,there are no specific guidelines on using serum-freeproducts or other materials such as HPL in cell therapyapplications. Specifically, within FDA, cell culturemedia, with and without serum, are considered an-cillary materials, raw materials and/or reagents. Eachcomponent must be properly qualified for serum-free media, similar to any additive used in cell culturemedia or any other reagent used under cGMP manu-facturing guidelines.
In any serum-free formulation that is based onhuman components sourced from blood, a criticalelement of safety is added due to the nature of thematerial. Because these components are usually derivedfrom a pool of several donors, the safety testing ofviral infections, donor screening procedures andviral inactivation during the process becomes criti-cal. Different regulatory agencies have differentsafety requirements for blood-derived products,which adds complexity and might limit the availabil-ity of such materials. For example, the followingrequirements may be necessary for a serum-freeformula to be used:
1. Plasma donor acceptance criteria such asthose defined in the “Guidance for Industry:Revised Preventive Measures to Reduce the Pos-sible Risk of Transmission of Creutzfeldt-JakobDisease (CJD) and vCJD by Blood and BloodProducts” [56].
2. Tested pathogens, test methodology and testingprocedures.
3. Source material country of origin including fulltractability.
4. Licensed plasma collection facility (FDA, Euro-pean Medicines Agency, Pharmaceutical andMedical Devices Agency of Japan); plasmaMasterfile in the EU; European Directorate forthe Quality of Medicines certificate if bovine.
5. Viral testing (as per USP <1240 > ) [57].6. Virus inactivation and removal steps (pathogen-
reduction steps) incorporated into the manu-facturing processes.
When working with human primary cells, addi-tives such as albumin and hydrolysates can vary lot-to-lot. Still, the variability in these additives is usually
less than the variability present when using sera. Suchvariability might affect the cells; therefore, it is criti-cal to test the quality and performance of eachincoming lot. It is also important to consider the avail-ability of each material in the quality process. Atminimum, dual sourcing needs to be achieved but isnot always possible because of the limited source andnature of the product.
Main lessons learned from thebiotech industry
The cell therapy industry is still developing and is rel-atively immature compared with other established fieldssuch as bio-therapeutics and vaccine productionmarkets. However, many advanced cellular therapiesare on a solid path to commercialization. As the pro-gression from early research to clinical trials and finalproduct approval continues, several lessons can belearned and applied from the biopharmaceutical in-dustry. One such area is raw material selection criteriaand management, most notably the selection of cellculture media and reagents used in the productionprocess. Most cellular therapies were developed in theresearch/preclinical setting using available systems usingtraditional serum-containing cell culture media frombovine or human sources (or others). Recently therehas been a push to transition to serum-free media formany reasons, and many proposals submitted toregulatory agencies for cell therapies have indicatedprocess development to replace animal serum withother alternatives for their manufacturing processes[4]. Furthermore, there is a strong move in thebiopharmaceutical industry to replace serum, andseveral drugs are now manufactured with serum-free media.
Timing for FBS replacement in thedevelopment plan
As detailed here, the replacement of FBS is recom-mended if possible, but the timing of this change isimportant.Theoretically, a cell therapy developer shouldconsider replacing the FBS as soon as possible evenbefore initial preclinical studies. Nevertheless, this the-oretical recommendation is not practical because mostof the therapies have been developed in academia andare based on data created using FBS and the cGMPissues of product development, and these are too earlyin development and too expensive for consideration.Therefore, a therapy developer should consider theissue as soon as possible and try to build a productdevelopment plan that includes the FBS replace-ment. Usually, this stage will take place during clinicalstudies after the initial safety and trends of efficacyhave been shown. At this stage the product charac-terization and potency tests must be clearly defined
166 O. Karnieli et al.

to ensure that any critical change to the culture con-ditions will not affect the cells MoA. Nevertheless,when looking at clinical trial design, the phase 3 trialis the pivotal trial in which all critical parameters inthe process must be defined, validated and lockeddown. Any critical change done to the process thatmight affect the product, such as FBS replacement,will require that the developer show comparability ofthe product. It is reasonable to predict that if such achange is done during or after phase 3, there mightbe a requirement for a bridging clinical study to ensurethe safety and efficacy. Therefore, we highly recom-mend assuming this change as early as possible oncethe product is defined and discussing with the regu-lator the development plan and where and how to dosuch a change.
Summary
Future growth of the cell therapy industry requires anincreasing focus on large-scale manufacturing strat-egies combined with a critical raw material control andquality strategy. FBS serves as a crucial raw materialused during cell culture growth in the majority of celltherapy manufacturing processes and therefore has agreat impact on the commercial-scale production ofthe industry. Limitations in the availability of FBS dueto increased demands and decreased production abilityfor the high amounts and quality needed may causea significant barrier to the commercial success of theindustry as a whole. Other disadvantages in the useof FBS are variability between batches that can affectend-product reproducibility, risks of contaminationsand ethical issues.Therefore, there is a great need tosearch for alternatives to serum, such as serum sub-stitutes or serum-free media.
In recent years, significant progress has been madeto generate various serum-free media alternatives andFBS replacements. However, because growth mediahave a great influence on cells’ characteristics and safetyand efficacy properties, it is crucial to understand thedifferences, advantages and challenges that come withthe different types of serum-free/xeno free media. Abetter understanding of these issues will influence thechoice of the most appropriate alternative to a com-pany’s cell product in terms of process conditions (2D,3D), cells requirements, etc. An optimization step isrequired when transforming a culture medium to aserum-free one. This process requires time and re-sources and may also involve other changes to beimplemented into the original production process. Fullcharacterization of the end product is vital after re-placement with a serum-free medium to verifycomparability to the original product. It is also crit-ical to carefully examine the quality, safety andavailability of the specific components to ensure that
the media selection meets the needs for further mat-uration of the process and resulting product.
In view of the discussion here, we propose takinginto account all aspects of availability, regulation, safety,cost, indication size and expected markets when de-fining the process and choosing the serum source.Werecommend considering the use of serum-free mediaor other FBS replacements for a new product devel-opment program as early as possible (taking in toconsideration the limits and challenges with suchoption) to save time and significant resources thatwould be required to convert a product culture mediumto serum-free in mid- to late-stage clinical develop-ment. Furthermore, we suggest the use of the termsand definitions provided in this article to ensure clarityand harmonization between end users, regulators andvendors. Serum replacements are often overlooked inearly development but should definitely be consid-ered during the development plan.
References
[1] Culme-Seymour EJ, Davie NL, Brindley DA, Edwards-PartonS, Mason C. A decade of cell therapy clinical trials (2000–2010). Regen Med 2012;7:455–62.
[2] Brindley DA, Davie NL, Culme-Seymour EJ, Mason C, SmithDW, Rowley JA. Peak serum: implications of serumsupply for cell therapy manufacturing. Regen Med 2012;7:7–13.
[3] Davie NL, Brindley DA, Culme-Seymour EJ, Mason C.Sreamlining cell therapy manufacture. BioprocessInternational; 2014. http://www.bioprocessintl.com/manufacturing/cell-therapies/streamlining-cell-therapy-manufacture-328083.
[4] Mendicino M, Bailey AM, Wonnacott K, Puri RK, Bauer SR.MSC-based product characterization for clinical trials: an FDAperspective. Cell Stem Cell 2014;14:141–5.
[5] Siegel W, Leland F. Fetal bovine serum: the impactof geography. Bioprocess J 2013;12:28–30. http://www.serumindustry.org/documents/J123-Siegel-Foster.pdf.
[6] Jochems CE, van der Valk JB, Stafleu FR, Baumans V. Theuse of fetal bovine serum: ethical or scientific problem? AlternLab Anim 2002;30:219–27.
[7] Zuliani T, David J, Bercegeay S, Pandolfino MC, Rodde-AstierI, Khammari A, et al. Value of large scale expansion of tumorinfiltrating lymphocytes in a compartmentalised gas-permeablebag: interests for adoptive immunotherapy. J Transl Med2011;9:63.
[8] da Silva CL. In: Devices, editor. Draft guidance for industryand food and drug administration staff medical devicescontaining materials derived from animal sources (except forin vitro diagnostic devices). 2014.
[9] Gstraunthaler G. Alternatives to the use of fetal bovine serum:serum-free cell culture. ALTEX 2003;20:275–81.
[10] Gottipamula S, Muttigi MS, Kolkundkar U, Seetharam RN.Serum-free media for the production of human mesenchymalstromal cells: a review. Cell Prolif 2013;46:608–27.
[11] Gstraunthaler G, Lindl T, van der Valk J. A plea to reduceor replace fetal bovine serum in cell culture media.Cytotechnology 2013;65:791–3.
[12] Boone CW, Mantel N, Caruso TD Jr, Kazam E, StevensonRE. Quality control studies on fetal bovine serum used in tissueculture. In Vitro 1971;7:174–89.
Serum replacements and serum-free media for cellular therapies 167
[13] Alden A, Gonzalez L, Persson A, Christensson K, HolmqvistO, Ohlson S. Porcine platelet lysate as a supplement for animalcell culture. Cytotechnology 2007;55:3–8.
[14] Holmovist OWB. Blood platelet lysate, method of itspreparation and a cell culture medium containing bloodplatelet lysate (WO 89/10398 PCT/SE89/00232). EuropeanPatent Office; 1989. p. 15.
[15] World Health Organization. Global database on blood safety.Summary report 2011. 2011. http://www.who.int/bloodsafety/global_database/GDBS_Summary_Report_2011.pdf.
[16] Munirah S, Ruszymah BH, Samsudin OC, Badrul AH, AzmiB, Aminuddin BS. Autologous versus pooled human serumfor articular chondrocyte growth. J Orthop Surg (Hong Kong)2008;16:220–9.
[17] Hankey DP, McCabe RE, Doherty MJ, Nolan PC, McAlindenMG, Nelson J, et al. Enhancement of human osteoblastproliferation and phenotypic expression when cultured inhuman serum. Acta Orthop Scand 2001;72:395–403.
[18] Thuresson K, Hoglund P, Hagmar L, Sjodin A, Bergman A,Jakobsson K. Apparent half-lives of hepta- to decabrominateddiphenyl ethers in human serum as determined inoccupationally exposed workers. Environ Health Perspect2006;114:176–81.
[19] Yamamoto N, Isobe M, Negishi A, Yoshimasu H, ShimokawaH, Ohya K, et al. Effects of autologous serum on osteoblasticdifferentiation in human bone marrow cells. J Med Dent Sci2003;50:63–9.
[20] Clavreul A, Jean I, Preisser L, Chassevent A, Sapin A, MichalakS, et al. Human glioma cell culture: two FCS-free media couldbe recommended for clinical use in immunotherapy. In VitroCell Dev Biol Anim 2009;45:500–11.
[21] Pandolfino MC, Saiagh S, Knol AC, Dreno B. Comparisonof three culture media for the establishment of melanoma celllines. Cytotechnology 2010;62:403–12.
[22] Jung S, Sen A, Rosenberg L, Behie LA. Identification ofgrowth and attachment factors for the serum-free isolationand expansion of human mesenchymal stromal cells.Cytotherapy 2010;12:637–57.
[23] Jung S, Panchalingam KM, Rosenberg L, Behie LA. Ex vivoexpansion of human mesenchymal stem cells in definedserum-free media. Stem Cells Int 2012;2012:123030.
[24] Smith C, Okern G, Rehan S, Beagley L, Lee SK, Aarvak T,et al. Ex vivo expansion of human T cells for adoptiveimmunotherapy using the novel Xeno-free CTS Immune CellSerum Replacement. Clin Transl Immunology 2015;4:e31.
[25] Wang Y, Cheng L, Gerecht S. Efficient and scalable expansionof human pluripotent stem cells under clinically compliantsettings: a view in 2013. Ann Biomed Eng 2014;42:1357–72.
[26] Chase LG, Lakshmipathy U, Solchaga LA, Rao MS, VemuriMC. A novel serum-free medium for the expansion of humanmesenchymal stem cells. Stem Cell Res Ther 2010;1:8.
[27] Fischer UM, Harting MT, Jimenez F, Monzon-Posadas WO,Xue H, Savitz SI, et al. Pulmonary passage is a major obstaclefor intravenous stem cell delivery: the pulmonary first-passeffect. Stem Cells Dev 2009;18:683–92.
[28] Lee RH, Pulin AA, Seo MJ, Kota DJ, Ylostalo J, Larson BL,et al. Intravenous hMSCs improve myocardial infarction inmice because cells embolized in lung are activated to secretethe anti-inflammatory protein TSG-6. Cell Stem Cell2009;5:54–63.
[29] Schrepfer S, Deuse T, Reichenspurner H, Fischbein MP,Robbins RC, Pelletier MP. Stem cell transplantation: the lungbarrier. Transplant Proc 2007;39:573–6.
[30] Bartosh TJ, Ylostalo JH, Mohammadipoor A, Bazhanov N,Coble K, Claypool K, et al. Aggregation of humanmesenchymal stromal cells (MSCs) into 3D spheroids
enhances their antiinflammatory properties. Proc Natl AcadSci USA 2010;107:13724–9.
[31] Wu M, Han ZB, Liu JF, Wang YW, Zhang JZ, Li CT, et al.Serum-free media and the immunoregulatory properties ofmesenchymal stem cells in vivo and in vitro. Cell PhysiolBiochem 2014;33:569–80.
[32] Doucet C, Ernou I, Zhang Y, Llense JR, Begot L, Holy X,et al. Platelet lysates promote mesenchymal stem cellexpansion: a safety substitute for animal serum incell-based therapy applications. J Cell Physiol 2005;205:228–36.
[33] King GL, Buchwald S. Characterization and partialpurification of an endothelial cell growth factor from humanplatelets. J Clin Invest 1984;73:392–6.
[34] Chen B, Sun HH, Wang HG, Kong H, Chen FM, Yu Q. Theeffects of human platelet lysate on dental pulp stem cellsderived from impacted human third molars. Biomaterials2012;33:5023–35.
[35] Atashi F, Jaconi ME, Pittet-Cuenod B, Modarressi A.Autologous platelet-rich plasma: a biological supplement toenhance adipose-derived mesenchymal stem cell expansion.Tissue Eng Part C Methods 2015;21:253–62.
[36] Kocaoemer A, Kern S, Kluter H, Bieback K. Human ABserum and thrombin-activated platelet-rich plasma are suitablealternatives to fetal calf serum for the expansion ofmesenchymal stem cells from adipose tissue. Stem Cells2007;25:1270–8.
[37] Cantisan Bohorquez S, Navarro Ortega D. Immunologicalmonitoring strategies for cytomegalovirus infection. Immune-based therapies. Enferm Infecc Microbiol Clin 2011;29(Suppl.6):28–32 [in Spanish].
[38] Jung S, Sen A, Rosenberg L, Behie LA. Human mesenchymalstem cell culture: rapid and efficient isolation and expansionin a defined serum-free medium. J Tissue Eng Regen Med2012;6:391–403.
[39] Dolley-Sonneville PJ, Romeo LE, Melkoumian ZK. Syntheticsurface for expansion of human mesenchymal stem cells inxeno-free, chemically defined culture conditions. PLoS ONE2013;8:e70263.
[40] Hervy M, Weber JL, Pecheul M, Dolley-Sonneville P,Henry D, Zhou Y, et al. Long term expansion of bonemarrow-derived hMSCs on novel synthetic microcarriersin xeno-free, defined conditions. PLoS ONE 2014;9:e92120.
[41] Ishikawa E, Takano S, Ohno T, Tsuboi K. Adoptive celltransfer therapy for malignant gliomas. Adv Exp Med Biol2012;746:109–20.
[42] Guillot PV, Gotherstrom C, Chan J, Kurata H, Fisk NM.Human first-trimester fetal MSC express pluripotency markersand grow faster and have longer telomeres than adult MSC.Stem Cells 2007;25:646–54.
[43] Wegmeyer H, Broske AM, Leddin M, Kuentzer K, NisslbeckAK, Hupfeld J, et al. Mesenchymal stromal cell characteristicsvary depending on their origin. Stem Cells Dev 2013;22:2606–18.
[44] Laport GG, Sheehan K, Baker J, Armstrong R, Wong RM,Lowsky R, et al. Adoptive immunotherapy with cytokine-induced killer cells for patients with relapsed hematologicmalignancies after allogeneic hematopoietic cell transplantation.Biol Blood Marrow Transplant 2011;17:1679–87.
[45] Papa S, van Schalkwyk M, Maher J. Clinical evaluation ofErbB-targeted CAR T-cells, following intracavity delivery inpatients with ErbB-expressing solid tumors. Methods Mol Biol2015;1317:365–82.
[46] Park TS, Rosenberg SA, Morgan RA. Treating cancer withgenetically engineered T cells. Trends Biotechnol 2011;29:550–7.
168 O. Karnieli et al.

[47] Ozturk SS, Palsson BO. Examination of serum and bovineserum albumin as shear protective agents in agitated culturesof hybridoma cells. J Biotechnol 1991;18:13–28.
[48] Murhammer DW, Goochee CF. Sparged animal cellbioreactors: mechanism of cell damage and Pluronic F-68protection. Biotechnol Prog 1990;6:391–7.
[49] Thompson PA, Rezvani K, Hosing CM, Oran B, Olson AL,Popat UR, et al. Umbilical cord blood graft engineering:challenges and opportunities. Bone Marrow Transplant2015;50(Suppl. 2):S55–62.
[50] Pagliara D, Savoldo B. Cytotoxic T lymphocytes forthe treatment of viral infections and posttransplantlymphoproliferative disorders in transplant recipients. CurrOpin Infect Dis 2012;25:431–7.
[51] Apel A, Groth A, Schlesinger S, Bruns H, Schemmer P,Buchler MW, et al. Suitability of human mesenchymal stemcells for gene therapy depends on the expansion medium. ExpCell Res 2009;315:498–507.
[52] Gruber R, Karreth F, Kandler B, Fuerst G, Rot A, FischerMB, et al. Platelet-released supernatants increase migrationand proliferation, and decrease osteogenic differentiation of
bone marrow-derived mesenchymal progenitor cells under invitro conditions. Platelets 2004;15:29–35.
[53] Lange C, Cakiroglu F, Spiess AN, Cappallo-Obermann H,Dierlamm J, Zander AR. Accelerated and safe expansion ofhuman mesenchymal stromal cells in animal serum-freemedium for transplantation and regenerative medicine. J CellPhysiol 2007;213:18–26.
[54] Abdelrazik H, Spaggiari GM, Chiossone L, Moretta L.Mesenchymal stem cells expanded in human platelet lysatedisplay a decreased inhibitory capacity on T- and NK-cellproliferation and function. Eur J Immunol 2011;41:3281–90.
[55] Schmidl C, Hansmann L, Andreesen R, Edinger M, HoffmannP, Rehli M. Epigenetic reprogramming of the RORC locusduring in vitro expansion is a distinctive feature of humanmemory but not naiveTreg. Eur J Immunol 2011;41:1491–8.
[56] http://www.fda.gov/downloads/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Blood/UCM307137.pdf.
[57] http://www.usp.org/usp-manufacturers/biologics/usp-documentary-standardsbiologics.
Serum replacements and serum-free media for cellular therapies 169