367.full.pdf - british journal of ophthalmology
TRANSCRIPT

PostScript..............................................................................................
LETTERS
Intravitreal injection oftriamcinolone acetonide astreatment for chronic uveitisChronic intraocular inflammation such aschronic uveitis can lead to cystoid macularoedema, papilloedema, and vitreous opacitiestemporarily or permanently reducing visualacuity. Chronic uveitis has usually beentreated by topical or systemic application ofsteroids. Topical treatment, however, often hasnot been sufficiently effective to suppressintraocular inflammation and to reduce cyst-oid macular oedema. Systemic treatment withsteroids inevitably leads to secondary sideeffects such as systemic suppression of thewhole immune system and Cushing’s syn-drome. Taking into account that the eye com-prises only 0.01% of the whole body volume,and considering that for achieving highconcentrations of a drug at its site of action itis best to apply it directly into the region ofrequired action, we describe the clinicaloutcome in a patient receiving an intravitrealinjection of a crystalline cortisone.
Case reportA 17 year old woman suffering from chronicidiopathic uveitis in both eyes for 5 years hadbeen treated topically, peribulbarly, and sys-temically with corticosteroids. As a steroidresponder, she had developed secondary ocu-lar hypertension. Steroid induced cataract inher right eye was operated on by phacoaspira-tion, transpupillary anterior vitrectomy, andposterior chamber lens implantation. To re-duce the systemic side effects of steroid treat-ment, systemic cyclosporin A had been addedto the treatment scheme since January 1998.In February 2000, she presented again with asevere uveitis with papilloedema and cystoidmacular oedema. Despite intensive topicaltreatment with steroids given hourly, and sys-temic acetazolamide, visual acuity remainedin the range 0.10–0.16. To avoid the sideeffects of systemic steroid treatment and toachieve high and longstanding concentrationsof steroids in the eye, we injected 20 mg crys-talline triamcinolone acetonide into the vitre-ous cavity of the right eye in July 2000 withtopical anaesthesia.
Within the next 5 weeks, visual acuityincreased to 0.5. Intraocular pressure in-creased to a maximum of 38 mm Hg, and wasreduced to the normal range with topicalantiglaucomatous medication. Four monthsafter the injection, the steroid crystals wereresorbed, visual acuity returned to the preop-erative level of 0.1, and with topical steroidsgiven, intraocular pressure decreased tovalues of less than 23 mm Hg without furtherantiglaucomatous medication.
CommentIn ophthalmology, corticosteroids appliedtopically or systemically are well known andhave widely been used to suppress intraocularinflammation. Based on experimental studiesperformed by Machemer, Peyman and others,as well as on clinical observations, intravitrealinjections of triamcinolone acetonide haveincreasingly been reported as treatment for
intraocular neovascular, oedematous, or in-flammatory diseases. These include diffusediabetic macular oedema, proliferate diabeticretinopathy, neovascular glaucoma, exudativeage related macular degeneration, anduveitis.1–5 In agreement with these previousstudies, the results of the present report sug-gest that the intravitreal injection of triamci-nolone acetonide may be an additional optionin the treatment of chronic uveitis. Futurestudies may address which types of uveitisintravitreal steroid injection are best for, andwhether the use of intravitreally implantedslow release devices6 can decrease the recur-rence rate of uveitis for a longer period than asingle intravitreal injection dose.
Proprietary interest: none.
R F Degenring, J B JonasDepartment of Ophthalmology, Faculty for Clinical
Medicine Mannheim, Ruprecht-Karls-UniversityHeidelberg, Germany
Correspondence to: Dr R Degenring,Universitäts-Augenklinik, Theodor-Kutzer-Ufer 1–3,
68167 Mannheim, Germany;[email protected]
Accepted for publication 17 June 2002
References1 Machemer R, Sugita G, Tano Y. Treatment of
intraocular proliferations with intravitrealsteroids. Trans Am Ophthalmol Soc1979;77:171–80.
2 Jonas JB, Söfker A. Intraocular injection ofcrystalline cortisone as adjunctive treatment ofdiabetic macular edema. Am J Ophthalmol2001;132:425–7.
3 Antcliff RJ, Spalton DJ, Stanford MR, et al.Intravitreal triamcinolone for uveitic cystoidmacular edema: an optical coherencetomography study. Ophthalmology2001;108:765–72.
4 Young S, Larkin G, Branley M, et al. Safetyand efficacy of intravitreal triamcinolone forcystoid macular edema in uveitis. Clin ExpOphthalmol 2001;29:2–6.
5 Martidis A, Duker JS, Puliafito CA. Intravitrealtriamcinolone for refractory cystoid macularedema secondary to birdshotretinochoroidopathy. Arch Ophthalmol2001;119:1380–3
6 Jaffe GJ, Ben-nun J, Guo H, et al.Fluocinolone acetonide sustained drugdelivery device to treat severe uveitis.Ophthalmology 2000;107:2024–33.
Ophthalmodynamometricestimation of cerebrospinal fluidpressure in pseudotumourcerebriMeasurement of the cerebrospinal fluid pres-sure usually requires a lumbar puncture orcraniotomy to get direct access to the cerebro-spinal fluid space. These techniques, however,are invasive and so carry the risk of complica-tions such as infections and damage to theneural structures. Furthermore, owing to theleakage of cerebrospinal fluid during thepuncture, the cerebrospinal fluid pressure willbe altered in the moment the measurement isperformed. It is, therefore, desirable to have anon-invasive method allowing the estimationof the intracerebral pressure without requir-ing a direct access to the brain or spinal cord.We describe a patient in whom ophthalmody-namometry strongly suggested an increased
intracerebral pressure which was confirmedby eventual direct measurement.
Case reportA 12 year old female patient presented withacute vomiting, massive headache, and bilat-eral abducens nerve palsy. Visual acuity was20/20 in both eyes, and visual fields wereunremarkable, except for an enlarged blindspot. Both optic discs showed a prominence of0.5 mm (right eye) and 0.6 mm (left eye) asmeasured by confocal laser scanning tomo-graphy. Intraocular pressure measured 18 mmHg. With topical anaesthesia, a Goldmanncontact lens fitted with a pressure sensormounted into its holding ring was put ontothe cornea (Fig 1). Pressure was asserted ontothe globe by slightly pressing the contact lens,and the pressure value at the time when thecentral retinal vein started pulsating wasnoted. The measurements of this new tech-nique of ophthalmodynamometry were re-peated nine times in both eyes.
The central retinal vein collapse pressure asthe sum of the ophthalmodynamometricvalue plus the intraocular pressure, measured103 relative units right eye and 98 relativeunits left eye. These values were significantlyhigher than normal values (6.1 (SD 8.4) rela-tive units) determined previously in normalsubjects (own data). Direct measurement ofcerebrospinal fluid pressure by lumbar punc-ture performed about 5 hours later revealed avalue of 107 cm water column (equivalent to82.3 mm Hg). In combination with otherclinical findings, the diagnosis of pseudotu-mour cerebri was made.
CommentThe central retinal vein is the only structurewhose appearance depends on its inner pres-sure, and which runs through the cerebro-spinal fluid space and which is accessible fromoutside the body without any invasive proce-dure being performed. After exiting the eyethrough the optic disc, the central retinal veingoes through the retrobulbar part of the opticnerve before it traverses the subarachnoidaland subdural spaces of the optic nerve andpierces the optic nerve meninges. The pres-sure in the central retinal vein is thus at leastas high as the cerebrospinal fluid pressure.The central retinal vein collapse pressure maybe measurable by ophthalmodynamometrysince the vein will start to pulsate, if the sum
Figure 1 Photograph showing theGoldmann contact lens with a pressuresensor mounted into the holding ring of thecontact lens and connected to a display.
Br J Ophthalmol 2003;87:361–377 361
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from
of intraocular pressure plus an external pres-sure exerted onto the eye equals the diastolicpressure of the central retinal vein.1–4 Theintraocular pressure can be determined byapplanation tonometry, and the additionalpressure exerted onto the globe can bemeasured by the ophthalmodynamometer. Inthe ophthalmodynamometers used in the1960s and 1970s, determinations of thecentral retinal vein pressure were oftendifficult or almost impossible so that the cen-tral retinal vein pressure has usually not beenmeasured.5 The new ophthalmodynamometerused in the present study (Fig 1) mayovercome some of the problems associatedwith the old ophthalmodynamometers. In aprevious study on the reproducibility of thenew technique, the variation of the centralretinal vein collapse pressure was 15.9% (SD11.9%). The present study suggests that, inpatients with markedly increased intracer-ebral pressure, the new, Goldmann lens asso-ciated, ophthalmodynamometer may provideinformation about the intracerebral pressureby estimating the central retinal vein collapsepressure. It may be helpful for the neuro-ophthalmological diagnosis of diseases asso-ciated with increased intracerebral pressure.
Proprietary interest: none.
J B Jonas, B HarderDepartment of Ophthalmology, Faculty of Clinical
Medicine Mannheim, University of Heidelberg,68167 Mannheim, Germany
Correspondence to: Dr J Jonas,Universitäts-Augenklinik, Theodor-Kutzer-Ufer 1-3,
68167 Mannheim, Germany;[email protected]
Accepted for publication 14 July 2002
References1 Meyer-Schwickerath R, Kleinwachter T,
Firsching R, et al. Central retinal venousoutflow pressure. Graefes Arch Clin ExpOphthalmol 1995;233:783–8.
2 Morgan WH, Yu DY, Cooper RL, et al.Retinal artery and vein pressures in the dogand their relationship to aortic, intraocularand cerebrospinal fluid pressures. MicrovascRes 1997;53:211–21.
3 Firsching R, Schutze M, Motschmann M, etal. Venous opthalmodynamometry: anoninvasive method for assessment ofintracranial pressure. J Neurosurg2000;93:33–6.
4 Draeger J, Rumberger E, Hechler B.Intracranial pressure in microgravityconditions: non-invasive assessment byophthalmodynamometry. Aviat Space EnvironMed 1999;70:1227–9.
5 Wunsh SE. Ophthalmodynamometry. N EnglJ Med 1969;281:446.
6 Jonas JB. Reproducibility ofophthalmodynamometric measurements of thecentral retinal artery and vein collapsepressure. Br J Ophthalmol 2003 (in press).
Treatment of atopic blepharitisby controlling eyelid skin waterretention ability with ceramidegel applicationAtopic blepharitis is one of the major ocularcomplications of atopic dermatitis (AD).1 2 Ithas been pointed out that atopic patients havedry skin accompanied by barrier disruptionand water deficiency. Previously, we assessedthe water retention ability of eyelid skin bymeasuring the water content and waterevaporation rate from the eyelid in patientswith atopic blepharitis.3 The water contentpositively correlated and water evaporation
from the eyelid negatively correlated with theseverity of blepharitis.3
Ceramide comprises about 30% of stratumcorneum lipids, which have an important rolein both the water retention and barrier func-tion of the skin.4 Ceramide abnormalities inseveral skin disorders, such as AD, have beenreported.5 6 Decreased levels of ceramides maybe attributable to the insufficient water reten-tion of the skin in AD. Apytt Gel (ZenyakuKogyo, Tokyo, Japan) is a product containinggalactosyl ceramides extracted from horses asa major moisturising ingredient. In this study,we assessed the efficacy and safety of this gelproduct in patients with mild atopic blephari-tis by measuring the water retention ability ofthe eyelid skin before and after prescription.
Methods and resultsSixteen lids of eight patients (five males andthree females, 7∼35 years old, average age 16.0(SEM 8.4) years) diagnosed as having AD bydermatologists, according to Hanifin and Raj-ka’s criteria,7 were examined. Because cera-mide gel has no anti-inflammatory effect,cases with severe inflammation were ex-cluded from this investigation. After informedconsent was obtained, patients were in-structed to place Apytt Gel on their eyelidstwo to five times a day after washing theirfaces. Assessment of clinical findings usingmeasurement of water retention ability wereperformed as previously described3 before and4 weeks after the beginning of application.Statistical analysis was carried out by non-parametric tests (Wilcoxon test). A p value of0.05 or less was considered statisticallysignificant.
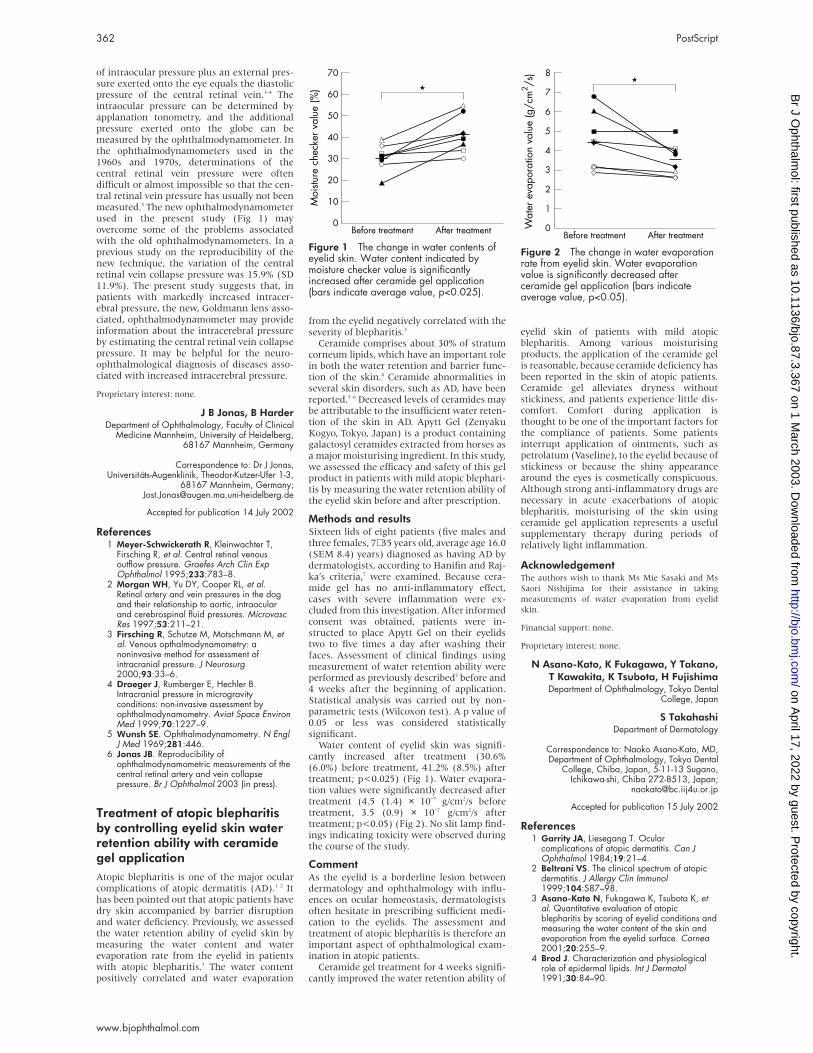
Water content of eyelid skin was signifi-cantly increased after treatment (30.6%(6.0%) before treatment, 41.2% (8.5%) aftertreatment; p<0.025) (Fig 1). Water evapora-tion values were significantly decreased aftertreatment (4.5 (1.4) × 10−7 g/cm2/s beforetreatment, 3.5 (0.9) × 10−7 g/cm2/s aftertreatment; p<0.05) (Fig 2). No slit lamp find-ings indicating toxicity were observed duringthe course of the study.
CommentAs the eyelid is a borderline lesion betweendermatology and ophthalmology with influ-ences on ocular homeostasis, dermatologistsoften hesitate in prescribing sufficient medi-cation to the eyelids. The assessment andtreatment of atopic blepharitis is therefore animportant aspect of ophthalmological exam-ination in atopic patients.
Ceramide gel treatment for 4 weeks signifi-cantly improved the water retention ability of
eyelid skin of patients with mild atopicblepharitis. Among various moisturisingproducts, the application of the ceramide gelis reasonable, because ceramide deficiency hasbeen reported in the skin of atopic patients.Ceramide gel alleviates dryness withoutstickiness, and patients experience little dis-comfort. Comfort during application isthought to be one of the important factors forthe compliance of patients. Some patientsinterrupt application of ointments, such aspetrolatum (Vaseline), to the eyelid because ofstickiness or because the shiny appearancearound the eyes is cosmetically conspicuous.Although strong anti-inflammatory drugs arenecessary in acute exacerbations of atopicblepharitis, moisturising of the skin usingceramide gel application represents a usefulsupplementary therapy during periods ofrelatively light inflammation.
AcknowledgementThe authors wish to thank Ms Mie Sasaki and Ms
Saori Nishijima for their assistance in taking
measurements of water evaporation from eyelid
skin.
Financial support: none.
Proprietary interest: none.
N Asano-Kato, K Fukagawa, Y Takano,T Kawakita, K Tsubota, H FujishimaDepartment of Ophthalmology, Tokyo Dental
College, Japan
S TakahashiDepartment of Dermatology
Correspondence to: Naoko Asano-Kato, MD,Department of Ophthalmology, Tokyo Dental
College, Chiba, Japan, 5-11-13 Sugano,Ichikawa-shi, Chiba 272-8513, Japan;
Accepted for publication 15 July 2002
References1 Garrity JA, Liesegang T. Ocular
complications of atopic dermatitis. Can JOphthalmol 1984;19:21–4.
2 Beltrani VS. The clinical spectrum of atopicdermatitis. J Allergy Clin Immunol1999;104:S87–98.
3 Asano-Kato N, Fukagawa K, Tsubota K, etal. Quantitative evaluation of atopicblepharitis by scoring of eyelid conditions andmeasuring the water content of the skin andevaporation from the eyelid surface. Cornea2001;20:255–9.
4 Brod J. Characterization and physiologicalrole of epidermal lipids. Int J Dermatol1991;30:84–90.
Figure 1 The change in water contents ofeyelid skin. Water content indicated bymoisture checker value is significantlyincreased after ceramide gel application(bars indicate average value, p<0.025).
Figure 2 The change in water evaporationrate from eyelid skin. Water evaporationvalue is significantly decreased afterceramide gel application (bars indicateaverage value, p<0.05).
362 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from
5 Imokawa G, Abe A, Jin K, et al. Decreasedlevel of ceramides in stratum corneum ofatopic dermatitis: an etiologic factor in atopicdry skin? J Invest Dermatol 1991;96:523–6.
6 Jin K, Higaki Y, Takagi Y, et al. Analysis ofbeta-glucocerebrosidase and ceramidaseactivities in atopic and aged dry skin. ActaDerm Venereol (Stockh) 1994;74: 337–40.
7 Hanifin JM, Rajka G. Diagnostic features ofatopic dermatitis. Acta Derm Venereol(Stockh) 1980;92:44–7.
An unusual tumour of thelacrimal glandLacrimal gland swelling is usually due to aninflammatory or neoplastic process. We reportan oncocytoma as the cause of lacrimal glandswelling and review the literature. Oncocy-toma of the lacrimal gland is extremely rareand has been described only three timesbefore.
Case reportA 72 year old man experienced periodic swell-ing of his right eyelid over a period of 9months. For 2 months he complained of verti-cal diplopia. He had a past medical history ofchronic obstructive airways disease and a pastocular history of early cataract, asteroidhyalosis of the vitreous body, and primaryopen angle glaucoma.
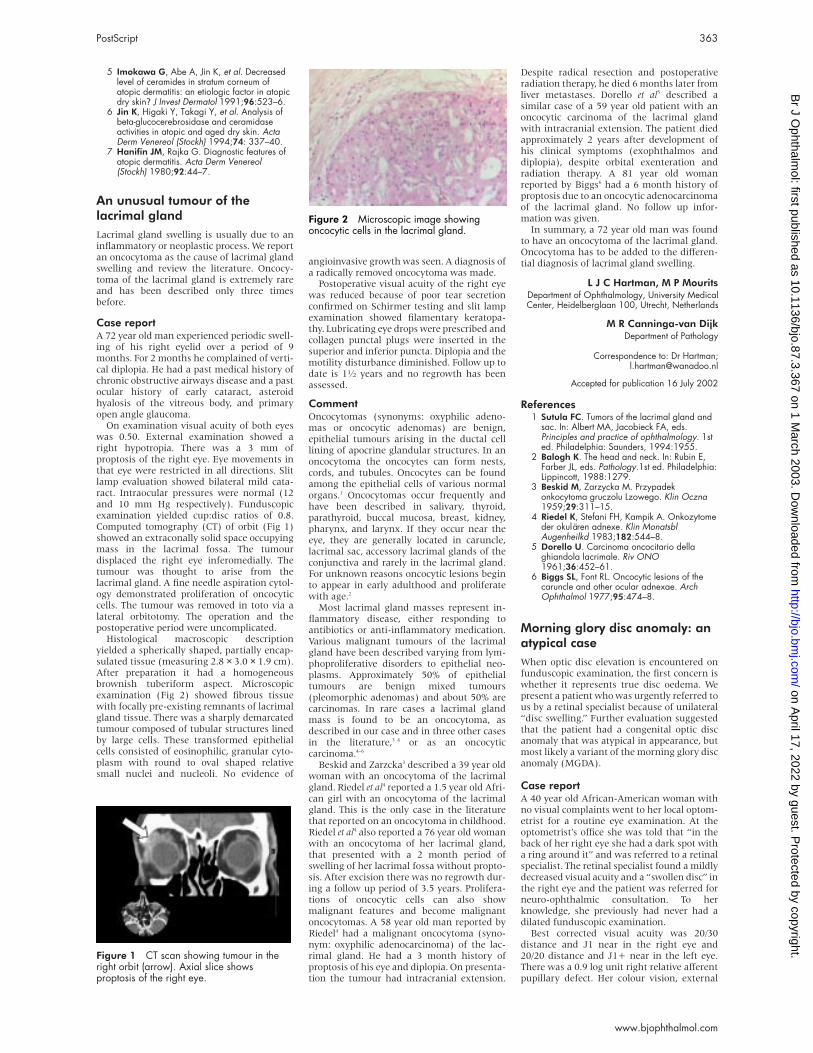
On examination visual acuity of both eyeswas 0.50. External examination showed aright hypotropia. There was a 3 mm ofproptosis of the right eye. Eye movements inthat eye were restricted in all directions. Slitlamp evaluation showed bilateral mild cata-ract. Intraocular pressures were normal (12and 10 mm Hg respectively). Funduscopicexamination yielded cup:disc ratios of 0.8.Computed tomography (CT) of orbit (Fig 1)showed an extraconally solid space occupyingmass in the lacrimal fossa. The tumourdisplaced the right eye inferomedially. Thetumour was thought to arise from thelacrimal gland. A fine needle aspiration cytol-ogy demonstrated proliferation of oncocyticcells. The tumour was removed in toto via alateral orbitotomy. The operation and thepostoperative period were uncomplicated.
Histological macroscopic descriptionyielded a spherically shaped, partially encap-sulated tissue (measuring 2.8 × 3.0 × 1.9 cm).After preparation it had a homogeneousbrownish tuberiform aspect. Microscopicexamination (Fig 2) showed fibrous tissuewith focally pre-existing remnants of lacrimalgland tissue. There was a sharply demarcatedtumour composed of tubular structures linedby large cells. These transformed epithelialcells consisted of eosinophilic, granular cyto-plasm with round to oval shaped relativesmall nuclei and nucleoli. No evidence of
angioinvasive growth was seen. A diagnosis ofa radically removed oncocytoma was made.
Postoperative visual acuity of the right eyewas reduced because of poor tear secretionconfirmed on Schirmer testing and slit lampexamination showed filamentary keratopa-thy. Lubricating eye drops were prescribed andcollagen punctal plugs were inserted in thesuperior and inferior puncta. Diplopia and themotility disturbance diminished. Follow up todate is 11⁄2 years and no regrowth has beenassessed.
CommentOncocytomas (synonyms: oxyphilic adeno-mas or oncocytic adenomas) are benign,epithelial tumours arising in the ductal celllining of apocrine glandular structures. In anoncocytoma the oncocytes can form nests,cords, and tubules. Oncocytes can be foundamong the epithelial cells of various normalorgans.1 Oncocytomas occur frequently andhave been described in salivary, thyroid,parathyroid, buccal mucosa, breast, kidney,pharynx, and larynx. If they occur near theeye, they are generally located in caruncle,lacrimal sac, accessory lacrimal glands of theconjunctiva and rarely in the lacrimal gland.For unknown reasons oncocytic lesions beginto appear in early adulthood and proliferatewith age.2
Most lacrimal gland masses represent in-flammatory disease, either responding toantibiotics or anti-inflammatory medication.Various malignant tumours of the lacrimalgland have been described varying from lym-phoproliferative disorders to epithelial neo-plasms. Approximately 50% of epithelialtumours are benign mixed tumours(pleomorphic adenomas) and about 50% arecarcinomas. In rare cases a lacrimal glandmass is found to be an oncocytoma, asdescribed in our case and in three other casesin the literature,3 4 or as an oncocyticcarcinoma.4–6
Beskid and Zarzcka3 described a 39 year oldwoman with an oncocytoma of the lacrimalgland. Riedel et al4 reported a 1.5 year old Afri-can girl with an oncocytoma of the lacrimalgland. This is the only case in the literaturethat reported on an oncocytoma in childhood.Riedel et al4 also reported a 76 year old womanwith an oncocytoma of her lacrimal gland,that presented with a 2 month period ofswelling of her lacrimal fossa without propto-sis. After excision there was no regrowth dur-ing a follow up period of 3.5 years. Prolifera-tions of oncocytic cells can also showmalignant features and become malignantoncocytomas. A 58 year old man reported byRiedel4 had a malignant oncocytoma (syno-nym: oxyphilic adenocarcinoma) of the lac-rimal gland. He had a 3 month history ofproptosis of his eye and diplopia. On presenta-tion the tumour had intracranial extension.
Despite radical resection and postoperativeradiation therapy, he died 6 months later fromliver metastases. Dorello et al5 described asimilar case of a 59 year old patient with anoncocytic carcinoma of the lacrimal glandwith intracranial extension. The patient diedapproximately 2 years after development ofhis clinical symptoms (exophthalmos anddiplopia), despite orbital exenteration andradiation therapy. A 81 year old womanreported by Biggs6 had a 6 month history ofproptosis due to an oncocytic adenocarcinomaof the lacrimal gland. No follow up infor-mation was given.
In summary, a 72 year old man was foundto have an oncocytoma of the lacrimal gland.Oncocytoma has to be added to the differen-tial diagnosis of lacrimal gland swelling.
L J C Hartman, M P MouritsDepartment of Ophthalmology, University MedicalCenter, Heidelberglaan 100, Utrecht, Netherlands
M R Canninga-van DijkDepartment of Pathology
Correspondence to: Dr Hartman;[email protected]
Accepted for publication 16 July 2002
References1 Sutula FC. Tumors of the lacrimal gland and
sac. In: Albert MA, Jacobieck FA, eds.Principles and practice of ophthalmology. 1sted. Philadelphia: Saunders, 1994:1955.
2 Balogh K. The head and neck. In: Rubin E,Farber JL, eds. Pathology.1st ed. Philadelphia:Lippincott, 1988:1279.
3 Beskid M, Zarzycka M. Przypadekonkocytoma gruczolu Lzowego. Klin Oczna1959;29:311–15.
4 Riedel K, Stefani FH, Kampik A. Onkozytomeder okulären adnexe. Klin MonatsblAugenheilkd 1983;182:544–8.
5 Dorello U. Carcinoma oncocitario dellaghiandola lacrimale. Riv ONO1961;36:452–61.
6 Biggs SL, Font RL. Oncocytic lesions of thecaruncle and other ocular adnexae. ArchOphthalmol 1977;95:474–8.
Morning glory disc anomaly: anatypical caseWhen optic disc elevation is encountered onfunduscopic examination, the first concern iswhether it represents true disc oedema. Wepresent a patient who was urgently referred tous by a retinal specialist because of unilateral“disc swelling.” Further evaluation suggestedthat the patient had a congenital optic discanomaly that was atypical in appearance, butmost likely a variant of the morning glory discanomaly (MGDA).
Case reportA 40 year old African-American woman withno visual complaints went to her local optom-etrist for a routine eye examination. At theoptometrist’s office she was told that “in theback of her right eye she had a dark spot witha ring around it” and was referred to a retinalspecialist. The retinal specialist found a mildlydecreased visual acuity and a “swollen disc” inthe right eye and the patient was referred forneuro-ophthalmic consultation. To herknowledge, she previously had never had adilated funduscopic examination.
Best corrected visual acuity was 20/30distance and J1 near in the right eye and20/20 distance and J1+ near in the left eye.There was a 0.9 log unit right relative afferentpupillary defect. Her colour vision, external
Figure 1 CT scan showing tumour in theright orbit (arrow). Axial slice showsproptosis of the right eye.
Figure 2 Microscopic image showingoncocytic cells in the lacrimal gland.
PostScript 363
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

examination, slit lamp biomicroscopy, in-traocular pressures, and motility were all nor-mal in both eyes. Funduscopic examinationwas normal in the left eye with an optic nervecup to disc ratio of 0.4. The appearance of herright optic nerve (Fig 1) was that of anelevated ring around the centre of the disc,interrupted from about 7 o’clock to 9 o’clockby an area of pigmentation. The vasculaturewas mildly obscured as it crossed the eleva-tion. There was no venous engorgement,haemorrhage, cotton wool spots, or exudate.Funduscopic examination gave the appear-ance of a peripapillary excavation of retinaand retinal pigment epithelium surroundingthe elevated ring from about 12 o’clock to 7o’clock. The macula and periphery werenormal. Automated perimetry showed anenlarged blind spot and a relative superioraltitudinal defect on the right and a full fieldon the left.
Fluorescein angiography showed stainingof optic nerve tissue but no leakage of fluores-cein outside the disc margin, confirming theabsence of true disc swelling (Fig 2). Magneticresonance imaging of the brain and orbitswith gadolinium showed no pathology. B-scanultrasonography excluded optic disc drusen.Optical coherence tomography (OCT) of theoptic nerve showed the elevated annulus oftissue seen on fundus examination and alsoshowed a peripapillary excavation of the reti-nal pigment epithelium (RPE) adjacent to theoptic nerve (Fig 3). This was thought to bemost consistent with MGDA.
CommentMorning glory disc anomaly is a congenitalanomaly of the optic disc that is typically uni-
lateral (for review see Brodsky1). The majorityof patients have a visual acuity between20/200 and counting fingers in the affectedeye, although cases with 20/20 vision and nolight perception have been reported. It is morecommon in females than males and is lesscommon in African-Americans than whitepeople.2–4 This condition is not typically aninherited condition or part of a multisystemgenetic disorder, although it has been re-ported as part of the renal-colobomasyndrome5 and trisomy 4q.6
The term “morning glory syndrome” wascoined for its ophthalmoscopic resemblanceto the morning glory flower.7 In MGDA theoptic nerve lies centrally within an excavationof the posterior globe. The size of the excava-tion varies from being relatively small, as inthis particular case, to cases in which theexcavation encompasses the macula, termedmacular capture. In most cases there is a cen-tral fibrous tuft that obscures the central partof the disc8 and a variable amount of peripap-illary pigment.
While MGDA is usually diagnosed byfunduscopic examination alone, our case wasatypical and not diagnosed immediately forseveral reasons: the patient had good visualacuity in the affected eye; she was African-American; there was no central fibrous tuft;and there was only a mild amount of peripap-illary pigmentation. It is likely that ourpatient’s visual acuity was spared because ofrelative sparing of the papillomacular bundle(Fig 1). Indeed, the peripapillary annulus oftissue surrounding the optic nerve spared asmall area temporally from about 7 to 9o’clock. In this region there was somepigment disturbance, but little if any apparentfibrosis, compared to the rest of the opticnerve. While a previous study of eightpatients9 suggested there was “no correlationbetween optic disc configuration and visualacuity” there was no patient in that studywith a documented visual acuity better than20/100.
Another atypical feature of our patient isthe small amount of peripapillary pigmentseen in the affected eye. The only area of pig-mentation is between 7 and 9 o’clock. Theremaining clock hours have elevated fibrovas-cular tissue but no visible pigment. This find-ing is not unexpected, as the visible peripapil-lary pigment in MGDA dissipates over time.This decrease in peripapillary pigment overtime is believed to be secondary to a metapla-sia of hamartomatous RPE into fibroglialtissue and hyperplasia of the fibroglial tissue.Our patient was 40 years old at diagnosis ofMGDA and it is possible that she had moreperipapillary pigment when she was younger.It is also possible that the peripapillaryexcavation of this patient was larger when shewas younger, as the glial hyperplasia tends toprogressively elevate the disc over time.10
There is controversy regarding the aetiologyof MGDA. Some believe it is a form of opticdisc coloboma.11 12 This theory is supported byevidence that MGDA is seen along a con-tinuum of other optic disc anomalies includ-ing coloboma in the renal colobomasyndrome.5 Based on the findings of a scleraldefect, vascular anomalies, central glial tuft,and adipose and smooth muscle tissue in his-topathological specimens, it has been hypoth-esised that MGDA may be a primary mesen-chymal disorder or an abnormality in therelative growth between the mesoderm andectoderm.8 9 Another theory proposes that anabnormal enlargement of the distal optic stalkduring eye development allows the inner layerof the optic cup to enter, causing an excava-tion at the entry site.3 One problem withdetermining the aetiology has been the lack ofclinical confirmation (primarily a lack of fun-dus photography) in previous histopathologi-cal reports.8 13–16 In this report we present OCTdata that confirm these pathological findingsin MGDA. Common to all of the histopatho-logical reports is a layer of RPE that lines theperipapillary excavation. This histological fea-ture is confirmed in the present case withOCT, which shows RPE extending posteriorlywithin the peripapillary scleral excavation asit approaches the optic nerve (Fig 3). We arecurrently evaluating other patients withMGDA using OCT and comparing these find-ings with the OCT appearances of other opticnerve anomalies, including optic disc colo-boma.
MGDA is sometimes associated with a basalencephalocele17–21 and up to a third of patientswith MGDA will develop a retinaldetachment.2 4 22 Hence, the first step in themanagement of MGDA is recognising theseassociated conditions. Our patient did nothave the characteristic facial features (flat-tened nasal bridge or cleft lip) nor did shehave any neurological, endocrine, or respira-tory symptoms to suggest she had a basalencephalocele and an magnetic resonanceimaging confirmed its absence. Funduscopicexamination showed no evidence of retinaldetachment, and she will be followed care-fully for this potential complication.
Although this is an atypical case, with nocentral fibrous tuft and little peripapillarypigment, this patient demonstrates the peri-papillary excavation characteristic of MGDA.To our knowledge this is the first report ofOCT of an eye with MGDA and confirms pre-vious histopathological reports of MGDAshowing RPE lining the central peripapillaryexcavation. Ongoing studies at our institutionare using OCT to quantify the changes thatoccur with MGDA over time and to comparethe features of MGDA with those of otheroptic nerve anomalies, including optic disccoloboma.
Figure 1 Photograph of the patient’s rightoptic disc. An elevated annulus of apparentfibroglial tissue surrounds most of the discalthough it appears to spare part of thepapillomacular bundle. An excavation ofretina and retinal pigment epitheliumsurrounding the optic disc can beappreciated from about 12 o’clock to 7o’clock.
Figure 2 Fluorescein angiography of the patient’s right eye. Both early (left; 32.6 secondsafter injection) and late (right; 6 minutes and 14 seconds after injection) images show noevidence of fluorescein leakage outside the disc margin.
Figure 3 Optical coherence tomography(OCT) of the patient’s right optic nerve.Representative OCT shows retinal pigmentepithelium lining an excavation surroundingthe optic nerve, characteristic of morningglory syndrome.
364 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

AcknowledgementsThis manuscript was supported in part by a depart-
mental grant (Department of Ophthalmology) from
Research to Prevent Blindness, Inc, New York, New
York, and by core grant P30-EY06360 (Department
of Ophthalmology) from the National Institute of
Health, Bethesda, Maryland. NJN is a recipient of a
Research to Prevent Blindness Lew R Wasserman
Merit Award.
Some of the data in this paper have been
previously published in abstract form at the Associ-
ation for Research in Vision and Ophthalmology
(ARVO) annual conference in 2002.
C A Baer, T M Aaberg SrDepartment of Ophthalmology, Emory University
School of Medicine, Atlanta, GA, USA
N J NewmanDepartments of Ophthalmology, Neurology, and
Neurological Surgery
Correspondence to: Nancy J Newman, MD,Neuro-ophthalmology Unit, Emory Eye Center,1365B Clifton Road, NE, Atlanta, GA 30322,
USA; [email protected]
Accepted for publication 5 July 2002
References1 Brodsky MC. Congenital optic disc
anomalies. Surv Ophthalmol1994;39:89–112.
2 Haik BG, Greenstein SH, Smith ME, et al.Retinal detachment in the morning glorysyndrome. Ophthalmology1984;91:1638–47.
3 Pollock, S. The morning glory disc anomaly:contractile movement, classification, andembryogenesis. Doc Ophthalmol1987;65:439–60.
4 Steinkuller PG. The morning glory discanomaly: case report and literature review. JPediatr Ophthalmol Strabismus1980;17:81–7.
5 Dureau P, Attie-Bitach T, Salomon R, et al.Renal coloboma syndrome. Ophthalmology2001;108:1912–6.
6 Nucci P, Mets MB, Babianelli EB. Trisomy 4qwith morning glory anomaly. OphthalmicPediatr Genet 1990;2:143–5.
7 Kindler P. Morning glory syndrome: unusualcongenital optic disc anomaly. Am JOphthalmol 1970;69:376–84.
8 Dempster AG, Lee WR, Forrester JV, et al.The ‘morning glory syndrome’: a mesodermaldefect? Ophthalmologica 1983;187:222–30.
9 Traboulsi EI, O’Neill JF. The spectrum in themorphology of the so-called “morning glorydisc anomaly”. J Pediatr OphthalmolStrabismus 1988;25:93–8.
10 Beyer WB, Quencer RM, Osher RH. Morningglory syndrome: a functional analysisincluding fluorescein angiography,ultrasonography, and computerizedtomography. Ophthalmology1982;89:1364–7.
11 Gardner TW, Zaparackas ZG, Naidich TP.Congenital optic nerve colobomas: CTdemonstration. J Comp Ass Tomog1984;8:95–102.
12 Mafee MF, Jampol LM, Langer BG, et al.Computed tomography of optic nervecolobomas, morning glory anomaly, andcolobomatous cyst. Radiol Clin N Am1987;25:693–9.
13 Cogan, DG. Coloboma of the optic nervewith overlay of the peripapillary retina. Br JOphthalmol 1978;62:347–50.
14 Manschot WA. Morning glory syndrome: ahistopathological study. Br J Ophthalmol1990;74:56–8.
15 Pedler, C. Unusual coloboma of the opticnerve entrance. Br J Ophthalmol1961;45:803–7.
16 Rack JH, Wright GF. Coloboma of the opticnerve entrance. Br J Ophthalmol1966;50:705–9.
17 Caprioli J, Lesser RL. Basal encephaloceleand morning glory syndrome. Br J Ophthalmol1971;71:423–5.
18 Goldhammer Y, Smith JL. Optic nerveanomalies in basal encephalocele. ArchOphthalmol 1975;93:115–18.
19 Hope-Ross M, Hohnston SS. The morningglory syndrome associated withsphenoethmoidal encephalocele. OphthalPediatr Genet 1990;2:147–53.
20 Koenig SP, Naidich TP, Lissner G. Themorning glory syndrome associated withsphenoidal encephalocele. Ophthalmology1982;89:1368–72.
21 Pollock JA, Newton TH, Hoyt WF.Transsphenoidal and transethmoidalencephaloceles: a review of clnical androentgen features in 8 cases. Radiology1968;90:442–53
22 Takeda A, Hida T, Kimura C, et al. A case ofbilateral morning glory syndrome with totalretinal detachment. Folia Ophthalmol Jap1981;32:1179–81.
Idiopathic anterior hyaloidvesselsAnterior hyaloidal fibrovascular proliferation(AHFP), the growth of vessels across theanterior hyaloid face from an origin inanterior retina,1 was first described in phakiceyes after diabetic vitrectomy surgery,2 but isalso reported following cataract surgery indiabetics.3 Complications include cataracts,vitreous haemorrhage, tractional retinal de-tachment, ciliary body detachment, andphthisis bulbi.1 We present the first report ofthis entity occurring in a non-diabetic patientwithout previous ophthalmic surgery.
Case reportA 20 year old Asian man presented with acuteright sided visual loss. There was no history ofocular trauma or family history of note. Hewas systemically well. Visual acuity was 6/12right eye, 6/5 left. Vessels were visible on theright posterior lens capsule, associated withlocalised cataract and anterior vitreous opac-ity (Fig 1A). Clinical examination revealed noother ocular abnormality, but the temporalperiphery of the right retina was obscured.Anterior segment fluorescein angiographyconfirmed perfusion of the vessels (Fig 1B).Posterior segment fluorescein angiography
was of poor quality in the right eye andrevealed no fundus or peripheral abnormalityin the left eye. Fluorescein angiography of thepatient’s only surviving parent was normal.Fasting blood glucose, Toxocara/Toxoplasmaserology, haemoglobin electrophoresis, andskull/chest radiographs were normal. Dopplerstudies indicated a probable feeder vesselderived from anterior retina but no evidenceof tumour or other pathology (Fig 2).
Progressive cataract reduced visual acuityto 6/24 within 2 weeks of presentation.Phacoemulsification surgery was performed,followed by closure of the abnormal vesselswith krypton laser (568 nm). Nd:YAG cap-sulotomy was performed 6 weeks after sur-gery. Two weeks later, fibrinous anterior uvei-tis and vitritis developed which resolved withtopical steroid medication. A year later, vesselspersisted in the rolled capsular edge, andopacification of the anterior hyaloid necessi-tated Nd:YAG laser discission. Two and a halfyears after presentation, he is asymptomaticwith 6/9 visual acuity in the right eye.
CommentIn most instances of retinal neovascularisa-tion, an angiogenic stimulus, such as capillarynon-perfusion or inflammation, can beidentified.4 In this case, no evidence wasfound of capillary non-perfusion, or any, otherthan postoperative, inflammation.
A number of specific diagnoses were con-sidered. No temporal traction on vasculararcades or optic disc was seen in the affectedeye, and peripheral retinal vasculature wasnormal, where seen in the affected eye, and inthe fellow eye. There was no history of lowbirth weight or prematurity as in retinopathyof prematurity. There was no family history,and the retinal peripheries of the parent werenormal, which makes dominant exudativevitreoretinopathy unlikely. No inflammation,other than post-surgical, was identified inanterior or posterior segment, and visible parsplana appeared normal. Toxocara and Toxo-plasma serology was negative. There was novisible peripheral retinal vasculitis or systemicevidence of sarcoidosis or multiple sclerosis.No evidence of ocular trauma was found, andno foreign body was identified radiographi-cally. The patient is not diabetic, screening forhaemoglobinopathy was negative, and therewere no ophthalmoscopic or angiographicsigns of retinal vascular occlusion. No evi-dence of a hyperviscosity syndrome wasfound.
The patient’s age, sex, and race are typical ofpatients suffering from idiopathic peripheralvaso-occlusive retinopathy (Eales’ disease),but the absence of retinal vasculitis, vitreousand retinal haemorrhage, and the unilateralnature of disease, are less characteristic. Nosign of tumour was apparent on ultrasonogra-phy, and no evidence of arteriovenous malfor-mation was found in the eye or body. He had
Figure 1 Right eye. (A) Abnormal vesselson temporal aspect of posterior capsuleassociated with localised cataract andanterior vitreous opacity. (B) Anteriorsegment fluorescein angiography confirmingperfusion of vessels.
Figure 2 B-scan ultrasonography withDoppler showing a feeder vessel.
PostScript 365
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

no features of incontinentia pigmenti orfacioscapulohumeral muscular dystrophy. Thediagnosis therefore remains uncertain.
Treatment was mandated on the basis ofvisual loss. Vitreoretinal opinion preferredphacoemulsification surgery to pars plana vit-reolensectomy because of the absence ofdefinable vitreous or peripheral retinal dis-ease. The vessels were closed with laser beforecapsulotomy to avoid haemorrhage, as hasoccurred after capsulotomy in diabetic pa-tients with AHFP.3
J G F Dowler, J S Mehta, A M Landers,A M P Hamilton
Medical Retinal Service, Moorfields Eye Hospital,City Road, London EC1V 2PD, UK
Correspondence to: Mr J S Mehta;[email protected]
Accepted for publication 8 July 2002
References1 Lewis H, Abrams GW, Foos RY.
Clinicopathologic findings in anteriorhyaloidal fibrovascular proliferation afterdiabetic vitrectomy. Am J Ophthalmol1987;104:614–8.
2 Lewis H, Abrams GW, Williams GA.Anterior hyaloidal fibrovascular proliferationafter diabetic vitrectomy. Am J Ophthalmol1987;104:607–13.
3 Ulbig MR, Hykin PG, Foss AJ, et al. Anteriorhyaloidal fibrovascular proliferation afterextracapsular cataract extraction in diabeticeyes. Am J Ophthalmol 1993;115:321–6.
4 Jampol LM, Ebroon DA, Goldbaum MH.Peripheral proliferative retinopathies: anupdate on angiogenesis, etiologies andmanagement. Surv Ophthalmol1994;38:519–40.
Iris pigment epithelial cystinduced by topicaladministration of latanoprostLatanoprost is an ester prodrug analogue ofprostaglandin F2α that enhances uveoscleraloutflow and reduces intraocular pressure.1
Several adverse side effects associated withtopical administration of latanoprost havebeen described.2 3 Iris cyst can be primary orsecondary; the secondary iris cysts are usuallycaused by trauma, intraocular surgery, inflam-mation, and prolonged use of strong mioticagents, etc.4 We report one female patient,with advanced chronic angle closure glau-coma, who developed an iris cyst in her lefteye 9 months after topical administration oflatanoprost in both her eyes.
Case reportA 67 year old female patient initially pre-sented with advanced chronic angle closureglaucoma in 1994. Laser iridotomy wasperformed on both her eyes in April 1994.After then, both eyes were treated with 2%pilocarpine and β blocker to maintain herintraocular pressures in the low teens. Be-cause she preferred to use monotherapy,latanoprost had been used once a day at bed-time since July 2000. The intraocular pres-sures were maintained between 12 and 15mm Hg with latanoprost monotherapy. Noabnormal responses except mild hyperaemiaof the conjunctiva were noticed during followup examinations. Unfortunately, in May 2001(about 9+ months after latanoprost mono-therapy), it was noticed that the iris of her lefteye bulged forward between 7 o’clock and 8o’clock. The lesion was gradually increasingits size, and in September 2001 an iris
pigment epithelial cyst was found at the pos-terior iris surface through a mid-dilated pupil(Fig 1). Latanoprost was then discontinuedand her antiglaucomatous medication waschanged to dorzolamide and β blocker twice aday in both eyes. The iris cyst graduallydecreased in size and completely disappearedfrom the pupil margin in February 2002 (Fig2). During the follow up period of 4 months,there have been no visual complications orsigns of recurring cyst.
CommentOur report demonstrates another case of rareadverse side effects of latanoprost involvingthe iris. Although no ultrasonic biomicroscopywas used to follow up this case, the slit lampbiomicroscopy strongly suggested that thepatient had a secondary pigment epithelialcyst arising from the posterior surface of theiris. The iris cyst developed in her left eyeabout 9+ months after topical administrationof latanoprost in her both eyes, and itprogressively decreased in size and completelydisappeared 5 months after topical latano-prost was discontinued. The iris cyst in ourcase took more time to develop and a longertime to disappear than previously reported.3
We propose that if it took more time todevelop an iris cyst after topical administra-tion of latanoprost, it would need more timefor the iris cyst to regress.
The topical latanoprost was administered toher both eyes, but only her left eye developedthe iris cyst. We propose that both her eyesmight have different sensitivity to the devel-opment of an iris cyst when exposed to topicallatanoprost. (If her right eye was exposed tolatanoprost for a longer time, an iris cystmight occur later.) Although cysts of uvealtissue might occur after uveitis,5 no definite
symptoms and signs of uveitis were noticed inour patient during the follow up period. Themost likely cause of this adverse side effectmay be the increasing uveoscleral outflow ontopical use of latanoprost; increasing uveo-scleral outflow leads to an enhanced aqueousflow through the ciliary muscle and theintraepithelial space of the posterior iris. Theiris cyst can occur at anytime during topicaladministration of latanoprost. Ophthalmolo-gists should be aware of this possible rare sideeffect of topical administration of latanoprost.
I C Lai, M T Kuo, l M C TengDepartment of Ophthalmology, Chang-Gung
Memorial Hospital, Kaohsiung, 123 Tai-Pei Road,Niao-Sung Hsiang, Kaohsiung Asien, Taiwan
Correspondence to: Ing-Chou Lai;[email protected]
Accepted for publication 17 July 2002
References1 Toris CB, Camras CB, Yablonski ME. Effects
of PHXA41, a new prostaglandin F2α analog,on aqueous humor dynamics in human eyes.Ophthalmology 1993;100:1297–304.
2 Rowe JA, Hattenhauer MG, Herman DC.Adverse side effects associated withlatanoprost. Am J Ophthalmol1997;124:683–5.
3 Krohn J, Hove VK. Iris cyst associated withtopical administration of latanoprost. Am JOphthalmol 1999;127:91–3.
4 Eagle JR, RC. Congenital, developmental anddegenerative disorders of the iris and ciliarybody. In Albert DM, Jacobiec FA, eds.Principle and pratice of ophthalmology:clinical pratice. 1st ed. Philadephia:Saunders, 1994:367–88.
5 Gentile RC, Leibmann JM, TelloC, et al.Ciliary body enlargement and cyst formationin uveitis. Br J Ophthalmol 1996;80:895–9.
Paravertebral primitiveneuroectodermal tumourpresenting with Horner’ssyndromeWe describe a peripheral primitive neuroecto-dermal tumour (PPNET) arising from the cer-vical paravertebral region of a 34 year oldwoman, who presented with Horner’s syn-drome and a cervical radiculopathy. PPNETsare rare malignant small round cell tumours.This appears to be the first documented caseof localised PPNET with Horner’s syndrome atinitial presentation.
Case reportA 34 year old woman presented with acute leftscapula pain, numbness of her left forearm, aleft upper lid ptosis, and left hemifacial anhy-drosis. Her symptoms disappeared spontane-ously within a fortnight, but returned 2months later with greater intensity. Examina-tion then revealed wasting of the smallmuscles of her left hand with reduced powerin the distribution of C8 and T1; there was lossof light touch and pinprick in the C8dermatome. The presence of left 1 mm upperlid ptosis, miosis, hemifacial anhydrosis, and 1mm lower lid (“upside down”) ptosis washighly suggestive of a preganglionic leftHorner’s syndrome (Fig 1A). Magnetic reso-nance imaging (MRI) of the neck showed alarge mass arising from the T1, T2 interverte-bral foramen extending into the root of theleft side of the neck and the region of the apexof the left lung (Fig 1B).
A diagnostic biopsy was performed througha posterolateral approach, excising the extra-dural component of the tumour within the
Figure 1 Slit lamp photography of thepatient’s left eye was taken after 12+ monthsof topical administration of latanoprost. In theinferonasal quadrant (see the arrow), an iriscyst appeared as a dark brown massbetween the pupillary border and theanterior surface of the lens.
Figure 2 Slit lamp photography of thepatient’s left eye was taken 5 months afterdiscontinuation of latanoprost. The iris cysthas disappeared and the anterior chamber isof normal depth.
366 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

nerve root canal. Histology revealed a malig-nant round cell tumour consistent with a per-ipheral primitive neuroectodermal tumour(PPNET, Fig 2). Immunohistochemical studiesdemonstrated positivity for focal vimentin,cytokeratins, synaptophysin, and MIC-2, butwere negative for GFAP (glial fibrillary acidicprotein), S100, desmin, and the lymphoidmarkers LCA, CD3, and CD20. Staging investi-gations showed no evidence of metastatic dis-ease and therefore the diagnosis of localisedPPNET was made.
The patient received chemotherapy as pri-mary treatment followed by radiotherapy andhas been in remission since. A year later shewas referred to our unit for correction of herleft ptosis, and underwent left anterior levatorresection with a satisfactory result. Four yearsfollowing her initial diagnosis she remainsfree of recurrent disease.
CommentHorner’s syndrome is caused by an oculosym-pathetic deficit to the pupillodilator and supe-rior and inferior tarsal retractor muscles.1–3 Itis manifest by upper lid ptosis, ipsilateralmiosis, apparent enophthalmos due to lowerlid (“upside down”) ptosis, and often facialanhydrosis.4 The presence of all these featuresin our patient, together with the left facialanhydrosis, was indicative of a preganglioniclesion, since the sympathetic facial sweatfibres branch distal to the superior cervicalsympathetic ganglion and central neurologi-cal tract signs were absent.2 3 PreganglionicHorner’s syndrome is frequently associatedwith neoplasms of the pulmonary apex,mediastinum, or neck, as illustrated by thelocation of the PPNET seen in our patient (Fig1B).
PPNET is a rare malignant small round celltumour that can affect any age group but isthought to peak in adolescence, with no sexpredilection.5 The most common location isthe thoracopulmonary region, followed by thehead and neck. Extraosseous Ewing’s sarcomais now considered a form of PNET, throughimmunohistochemical, ultrastructural, andhistogenetical similarities.6 Both tumours ex-press elevated levels of glycoprotein p30–32, a
product of the MIC-2 gene, in a unique andhighly selected fashion, as well as specifictranslocations involving a gene on chromo-some 22q12. Indeed, the tumour cells of ourpatient exhibited immunohistochemical reac-tivity for MIC-2, consistent with a PPNET.
The association of Horner’s syndrome withC8/T1 cervical radiculopathy is classically seenin Pancoast’s syndrome, which is due to supe-rior sulcus tumours of the lung that involvethe chest wall and spinal column.7 Thepresentation of PPNET with Pancoast’s syn-drome has been reported previously, but inthis case the tumour had massively infiltratedthe left thorax with widespread metastases,resulting in death at 17 weeks following initialdiagnosis.8 In contrast, our patient presentedwith Horner’s syndrome at a relatively earlystage of the disease, since the PPNET waslocalised with no evidence of metastaticspread. The malignant nature of this tumourhighlights the importance of comprehensivelyinvestigating any patient with Horner’s syn-drome, especially when associated with cervi-cal radiculopathy.
AcknowledgementWe thank Dr Maria Thom, MRCPath, Division of
Pathology, Institute of Neurology, London, for her
assistance and permission in the preparation of
pathological figures.
D N Parmar, N Lim, N JoshiChelsea and Westminster Hospital, 369 Fulham
Road, London SW10 9NH, UK
Correspondence to: D N Parmar, Moorfields EyeHospital, City Road, London EC1V 2PD, UK
Accepted for publication 22 July 2002
References1 Kawasaki A. Physiology, assessment, and
disorders of the pupil. Curr Opin Ophthalmol1999;10:394–400.
2 Amonoo-Kuofi HS. Horner’s syndromerevisited: with an update of the centralpathway. Clin Anat 1999;12:345–61.
3 Wilhelm H. Neuro-ophthalmology ofpupillary function—practical guidelines. JNeurol 1998;245:573–83.
4 Nielsen PJ. Upside down ptosis in patientswith Horner’s syndrome. Acta Ophthalmol(Copenh) 1983;61:952–7.
5 Jones JE, McGill T. Peripheral primitiveneuroectodermal tumors of the head and neck.Arch Otolaryngol Head Neck Surg1995;121:1392–5.
6 Batsakis JG, Mackay B, el-Naggar AK.Ewing’s sarcoma and peripheral primitiveneuroectodermal tumor: an interim report. AnnOtol Rhinol Laryngol 1996;105:838–43.
7 York JE, Walsh GL, Lang FF, et al. Combinedchest wall resection with vertebrectomy andspinal reconstruction for the treatment ofPancoast tumors. J Neurosurg 1999;91(1Suppl):74–80.
8 Meyer T, Herrmann C, Hiddemann W, et al.Pathology and clinical aspects of peripheralneuroectodermal tumours. Deutsch MedWochenschr 1993;118:1442–6.
Association of keratoconus andAvellino corneal dystrophyKeratoconus is an idiopathic, progressive,non-inflammatory ectasia of the axial cornea.Its association of other systemic disorders orocular disease have been reported, but its spe-cific origin remains unknown. Recently, Mu-nier and associates detected that four types ofautosomal dominant corneal dystrophy resultfrom mutation in the human transforminggrowth factor β induced gene (βigH3), theproduct of which has shown to be the proteinkeratoepithelin (R555W for granular cornealdystrophy, R555Q mutation for Reis-Bückler’scorneal dystrophy, R124C mutation for latticecorneal dystrophy type I, and R124H mutationfor Avellino corneal dystrophy).1 Moleculargenetic analysis of various corneal dystro-phies, which had previously presented aninsuperable challenge to clinical diagnosis,now clearly demonstrates the distinctphenotypes.2 We report a rare case of bilateralkeratoconus in association with Avellinocorneal dystrophy diagnosed by moleculargenetic analysis.
Case reportA 35 year old man had complained blurredvision in both eyes for several years. Hisgeneral health was good and there was nohistory of atopic disease, connective tissuedisease, or ocular trauma. His familial historywas unknown.
His best corrected visual acuity was RE20/50 and LE 20/100. Slit lamp examinationrevealed bilateral non-inflammatory cornealthinning with protrusion of the centralthinning areas. Fleischer ring was found inboth corneas. Central corneal thickness was428 µm on the right and 421 µm on the leftmeasured by ultrasonic pachymetry. Therewas also clinical evidence of granular cornealdystrophy in both eyes. Discrete grey-whiteopacities and star-shaped spicular opacities
Figure 1 (A) Left Horner’s syndrome withleft upper lid ptosis, miosis, and “upsidedown” lower lid ptosis. (B) Magneticresonance imaging of neck (coronal section),showing a mass arising from between thefirst and second thoracic intervertebralforamen, extending into the root of the leftside of the neck and the left pulmonaryapical region (arrow).
Figure 2 Histology of excisedcervicothoracic extradural mass takenJanuary 1998 showing (A) round tumourcells with numerous frequent mitosesinfiltrating fibrovascular stroma(haematoxylin and eosin ×140); (B)immunohistochemical reactivity of tumour cellcytoplasm with vimentin stain (Dako Ltd, UK;1:40) ×710; (C) focal cytoplasmic dot-likestaining with synaptophysinimmunohistochemistry (arrowheads) (DakoLtd, UK; 1:100).
PostScript 367
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from
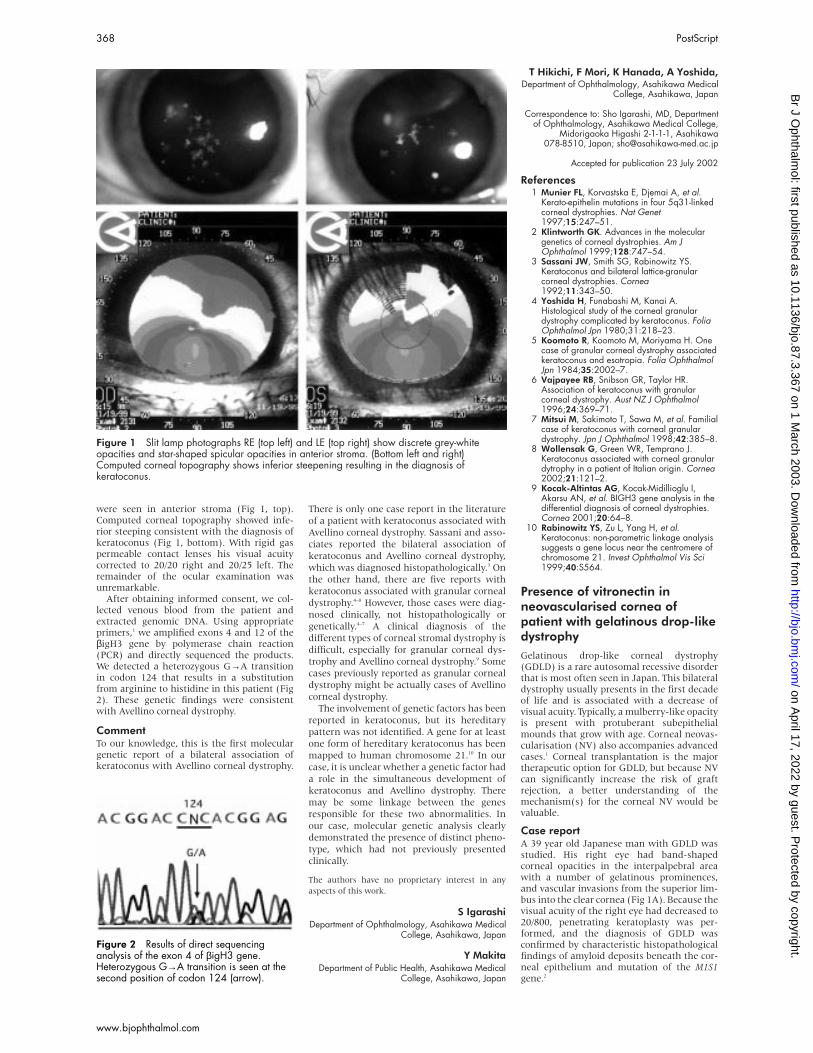
were seen in anterior stroma (Fig 1, top).Computed corneal topography showed infe-rior steeping consistent with the diagnosis ofkeratoconus (Fig 1, bottom). With rigid gaspermeable contact lenses his visual acuitycorrected to 20/20 right and 20/25 left. Theremainder of the ocular examination wasunremarkable.
After obtaining informed consent, we col-lected venous blood from the patient andextracted genomic DNA. Using appropriateprimers,1 we amplified exons 4 and 12 of theβigH3 gene by polymerase chain reaction(PCR) and directly sequenced the products.We detected a heterozygous G→A transitionin codon 124 that results in a substitutionfrom arginine to histidine in this patient (Fig2). These genetic findings were consistentwith Avellino corneal dystrophy.
CommentTo our knowledge, this is the first moleculargenetic report of a bilateral association ofkeratoconus with Avellino corneal dystrophy.
There is only one case report in the literature
of a patient with keratoconus associated with
Avellino corneal dystrophy. Sassani and asso-
ciates reported the bilateral association of
keratoconus and Avellino corneal dystrophy,
which was diagnosed histopathologically.3 On
the other hand, there are five reports with
keratoconus associated with granular corneal
dystrophy.4–8 However, those cases were diag-
nosed clinically, not histopathologically or
genetically.4–7 A clinical diagnosis of the
different types of corneal stromal dystrophy is
difficult, especially for granular corneal dys-
trophy and Avellino corneal dystrophy.9 Some
cases previously reported as granular corneal
dystrophy might be actually cases of Avellino
corneal dystrophy.
The involvement of genetic factors has been
reported in keratoconus, but its hereditary
pattern was not identified. A gene for at least
one form of hereditary keratoconus has been
mapped to human chromosome 21.10 In our
case, it is unclear whether a genetic factor had
a role in the simultaneous development of
keratoconus and Avellino dystrophy. There
may be some linkage between the genes
responsible for these two abnormalities. In
our case, molecular genetic analysis clearly
demonstrated the presence of distinct pheno-
type, which had not previously presented
clinically.
The authors have no proprietary interest in any
aspects of this work.
S IgarashiDepartment of Ophthalmology, Asahikawa Medical
College, Asahikawa, Japan
Y MakitaDepartment of Public Health, Asahikawa Medical
College, Asahikawa, Japan
T Hikichi, F Mori, K Hanada, A Yoshida,Department of Ophthalmology, Asahikawa Medical
College, Asahikawa, Japan
Correspondence to: Sho Igarashi, MD, Departmentof Ophthalmology, Asahikawa Medical College,
Midorigaoka Higashi 2-1-1-1, Asahikawa078-8510, Japan; [email protected]
Accepted for publication 23 July 2002
References1 Munier FL, Korvastska E, Djemai A, et al.
Kerato-epithelin mutations in four 5q31-linkedcorneal dystrophies. Nat Genet1997;15:247–51.
2 Klintworth GK. Advances in the moleculargenetics of corneal dystrophies. Am JOphthalmol 1999;128:747–54.
3 Sassani JW, Smith SG, Rabinowitz YS.Keratoconus and bilateral lattice-granularcorneal dystrophies. Cornea1992;11:343–50.
4 Yoshida H, Funabashi M, Kanai A.Histological study of the corneal granulardystrophy complicated by keratoconus. FoliaOphthalmol Jpn 1980;31:218–23.
5 Koomoto R, Koomoto M, Moriyama H. Onecase of granular corneal dystrophy associatedkeratoconus and esotropia. Folia OphthalmolJpn 1984;35:2002–7.
6 Vajpayee RB, Snibson GR, Taylor HR.Association of keratoconus with granularcorneal dystrophy. Aust NZ J Ophthalmol1996;24:369–71.
7 Mitsui M, Sakimoto T, Sawa M, et al. Familialcase of keratoconus with corneal granulardystrophy. Jpn J Ophthalmol 1998;42:385–8.
8 Wollensak G, Green WR, Temprano J.Keratoconus associated with corneal granulardytrophy in a patient of Italian origin. Cornea2002;21:121–2.
9 Kocak-Altintas AG, Kocak-Midillioglu I,Akarsu AN, et al. BIGH3 gene analysis in thedifferential diagnosis of corneal dystrophies.Cornea 2001;20:64–8.
10 Rabinowitz YS, Zu L, Yang H, et al.Keratoconus: non-parametric linkage analysissuggests a gene locus near the centromere ofchromosome 21. Invest Ophthalmol Vis Sci1999;40:S564.
Presence of vitronectin inneovascularised cornea ofpatient with gelatinous drop-likedystrophyGelatinous drop-like corneal dystrophy(GDLD) is a rare autosomal recessive disorderthat is most often seen in Japan. This bilateraldystrophy usually presents in the first decadeof life and is associated with a decrease ofvisual acuity. Typically, a mulberry-like opacityis present with protuberant subepithelialmounds that grow with age. Corneal neovas-cularisation (NV) also accompanies advancedcases.1 Corneal transplantation is the majortherapeutic option for GDLD, but because NVcan significantly increase the risk of graftrejection, a better understanding of themechanism(s) for the corneal NV would bevaluable.
Case reportA 39 year old Japanese man with GDLD wasstudied. His right eye had band-shapedcorneal opacities in the interpalpebral areawith a number of gelatinous prominences,and vascular invasions from the superior lim-bus into the clear cornea (Fig 1A). Because thevisual acuity of the right eye had decreased to20/800, penetrating keratoplasty was per-formed, and the diagnosis of GDLD wasconfirmed by characteristic histopathologicalfindings of amyloid deposits beneath the cor-neal epithelium and mutation of the M1S1gene.2
Figure 1 Slit lamp photographs RE (top left) and LE (top right) show discrete grey-whiteopacities and star-shaped spicular opacities in anterior stroma. (Bottom left and right)Computed corneal topography shows inferior steepening resulting in the diagnosis ofkeratoconus.
Figure 2 Results of direct sequencinganalysis of the exon 4 of βigH3 gene.Heterozygous G→A transition is seen at thesecond position of codon 124 (arrow).
368 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

It was recently reported that vitronectin, amultifunctional extracellular matrix adhesionmolecule, is often a component of the abnor-mal extracellular deposits in various agerelated human diseases such as age relatedmacular degeneration and amyloidosis. Thissuggested that similar pathways may beinvolved in the aetiologies of other age relateddiseases.3 Because the disease state of GDLDdeteriorates with age, we hypothesised thatsimilar vitronectin related pathways may alsobe associated with GDLD, and examinedwhether vitronectin was expressed in theGDLD cornea by immunohistochemistry.
An antibody directed against vitronectin(Santa Cruz Biotechnology, Santa Cruz, CA,USA) exhibited intense reactivity with theinfiltrating leucocytes and corneal epitheliumaround the deposits. Substantial levels of vit-ronectin protein were also present in thedeposits (Fig 1B, C).
Because the production of new extracellu-lar matrix proteins has a crucial role insupporting cell proliferations that are neces-sary for new blood vessel growth,4 andbecause vitronectin receptors, such as integrinαvβ3 and αvβ5, are involved in angiogenesis,4
we further hypothesised that the accumulatedvitronectin in the GDLD cornea may also havea role in the accompanying corneal NV.
We therefore examined the angiogenicpotential of vitronectin using an in vivocorneal assay.5 Five µl hydron pellets (Inter-
feron Sciences, New Brunswick, NJ, USA)
containing 1 µg of mouse vitronectin (Invitro-
gen, Carlsbad, CA, USA) were implanted into
the cornea of anaesthetised male Sprague-
Dawley (S-D) rats and, after 7 days, the
animals were killed, and the corneal vessels
were photographed. Vitronectin elicited a
strong angiogenic response, but administra-
tion of phosphate buffered saline (PBS) alone
did not (Fig 2).
CommentThese results provide the first evidence for the
expression of vitronectin in the cornea with
GDLD, and for the in vivo inducement of ang-
iogenesis by vitronectin. The results indicate
that vitronectin may have a role in corneal NV
in patients with GDLD. Therefore, further
studies exploring mechanisms of corneal NV
mediated by vitronectin-integrin system, and
how mutation of M1S1 leads to accumulation
of vitronectin with more samples, may even-
tually offer a novel insight in understanding
the aetiology of corneal NV associated with
GDLD.
AcknowledgementsThis work was supported in part by grants from
Sumitomo Life Social Welfare Services Foundation
(SY), Japan National Society for the Prevention of
Blindness (AY), and Japan Eye Bank Association
(AY).
S Yoshida, A Yoshida, T IshibashiDepartment of Ophthalmology, Kyushu University
Graduate School of Medicine, Fukuoka,812–8582, Japan
Y Kumano, T MatsuiOhshima Hospital of Ophthalmology, Fukuoka,
812–0036, Japan.
Correspondence to: Shigeo Yoshida, MD, PhD,Department of Ophthalmology, Kyushu University
Graduate School of Medicine, Fukuoka, 812–582,Japan; [email protected]
Accepted for publication 12 August 2002
References1 Smolin G. Corneal dystrophies and
degenerations. In: Smolin G, Thoft RA, eds.The cornea. Boston: Little, Brown,1995:499–533.
2 Yoshida S, Kumano Y, Yoshida A, et al. Twobrothers with gelatinous drop-like dystrophy atdifferent stages of the disease: role ofmutational analysis. Am J Ophthalmol2002;133:830–2.
3 Mullins RF, Russell SR, Anderson DH, et al.Drusen associated with aging and age-relatedmacular degeneration contain proteinscommon to extracellular deposits associatedwith atherosclerosis, elastosis, amyloidosis,and dense deposit disease. Faseb J2000;14:835–46.
4 Stupack DG, Cheresh DA. ECM remodelingregulates angiogenesis: endothelial integrinslook for new ligands. Sci STKE2002;2002:PE7.
5 Yoshida S, Ono M, Shono T, et al.Involvement of interleukin-8, vascularendothelial growth factor, and basic fibroblastgrowth factor in tumor necrosis factoralpha-dependent angiogenesis. Mol Cell Biol1997;17:4015–23.
Factor XII deficiency andrecurrent sixth nerve palsyFactor XII deficiency is associated withthrombosis.1–3 Severe deficiency increases anindividual’s prothrombotic tendency but witha mild reduction in levels there is lesscertainty.4 We present a case of recurrent sixthcranial nerve palsy due to severe factor XIIdeficiency. To our knowledge, this is the firstreported case of a recurrent cranial nervepalsy associated with factor XII deficiency.
Case reportA 58 year old white male presented with anacquired constant incomitant horizontal di-plopia. He had had a previous episode of hori-zontal diplopia of 3 weeks’ duration 6 monthspreviously with spontaneous resolution and afurther similar episode 18 years before thatbut had been otherwise well. He was nothypertensive or diabetic, of normal weightand a non-smoker, and without any cardio-vascular disease. There was no family orpersonal history of venous or arterial throm-bosis. On examination he was found to havebilateral sixth nerve palsies without any asso-ciated headache or papilloedema. Detailedmagnetic resonance imaging with contrastand lumbar puncture opening pressure andinvestigation was normal.
Owing to the recurrent nature of the nervepalsy and the initial young age of presenta-tion, a further prothrombotic examinationwas undertaken. Laboratory investigationsshowed a normal full blood count, plasma vis-cosity, liver function tests, glucose, homo-cysteine, prothrombin time, and fibrinogenassay. There was a significantly prolongedactivated partial thromboplastin time of 74.7seconds (normal range 24–32), which wasstill abnormal on repeat testing (90 seconds).Further laboratory studies demonstrated se-vere factor XII deficiency which was consist-ent on repeated testing (<1% of normallevels) but otherwise normal levels of proteinS, protein C, antiphospholipid antibodies, fac-tor VIII, von Willebrand factor, and the factorV Leiden mutation or prothrombin G20210Aallele were not found.
Figure 1 (A) Slit lamp photographs of theright cornea of a 39 year old man withgelatinous drop-like dystrophy (GDLD),demonstrating subepithelial raised lesionswith a mulberry-like appearance andband-shaped opacities occupying the inferiorcornea. There is also neovascular infiltrationfrom the superior limbus of the cornea, someof the vessels are indicated by arrows. (B)Light microscopic photograph of a cornealbutton section surgically excised from the 39year old man. Histological section of thiscornea shows eosinophilic amorphousmaterial in the subepithelial region, and theoverlying epithelium was degenerated. Notethe prominent inflammatory infiltrate(haematoxylin and eosin, originalmagnification ×200). (C) Immunostaining ofGDLD cornea with vitronectin showingimmunopositivity in the infiltrating leucocytesand basal epithelial cell layer. Diffusestaining for vitronectin is also found in thedeposits. Anti-vitronectin also appears tostain the superficial layer of corneal epithelialcells, although we cannot totally rule out thepossibility that this might represent an edgeartefact (haematoxylin counterstain, originalmagnification ×200).
Figure 2 Representative photographsshowing the effect of vitronectin on in vivoangiogenesis in rat cornea. Hydron pelletswere formulated and implanted into ratcorneas. After 7 days, vessels in the regionof the pellet implant were photographed.Pellets contained PBS (A) or vitronectin (B). Sixrats were used to assess the effect ofvitronectin and neovascularisation wasobserved in all six replicates.
PostScript 369
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

He was fitted with Fresnel prisms to relievehis diplopia and was followed up 3 weekslater. By that time his diplopia had completelyresolved and he had full abduction in botheyes.
CommentWith this recurrent and resolving pattern ofcranial nerve palsy in a patient with no otherrisk factors for arteriosclerosis and a normalmagnetic resonance image and lumbar punc-ture, the most likely predisposing factor inthis case is his prothrombotic state associatedwith severe factor XII deficiency.
Severe factor XII deficiency is a geneticdeterminant for thrombosis.2 3 It is not associ-ated with any other clinical manifestations andprolonged activated thromboplastin time is aconsistent finding in any level of factor XIIdeficiency. The only previously reported oph-thalmic complications of factor XII deficiencyare two cases of central retinal vein occlusion inpatients without any vasculopathic riskfactors.5 Assay for factor XII is not routinelydone on thrombophilia screening protocols. Ithas been suggested that the frequency of factorXII deficiency (1.5–3%)6 is high enough towarrant the inclusion of factor XII assays inroutine thrombophilia screening.7 Detailedthrombophilia screening of healthy popula-tions may produce an identifiable abnormalityin 10% but clearly 10% of the population arenot clinically affected in their lifetime. There-fore the need for additional managementshould be assessed according to the presence ofconcurrent risk factors in an algorithmicfashion.8 Since his cranial nerve palsy resolvedquickly and there was no family history of vas-cular thrombosis he was treated empiricallywith aspirin, although there is no evidence tosupport its benefit in this condition.
A Kipioti, O C Backhouse, P M Jacobs,M R Howard
Department of Ophthalmology, York DistrictHospital NHS Trust, York, UK
Correspondence to: A Kipioti, Eye Department,Clarendon Wing, Leeds General Infirmary,
LS2 9NS, UK; [email protected]
Accepted for publication 12 August 2002
References1 Lee GR. Wintrobe’s clinical haematology.
10th ed. Philadelphia: Williams and Wilkins,1999:688–9, 1708–9.
2 Halbmayer WM, Mannhalter c, FeichtingerC, et al. The prevalence of factor XIIdeficiency in 103 orally anticoagulatedoutpatients suffering from recurrent venousand/or arterial thromboembolism. ThrombHaemost 1992;68:285–90.
3 Mannhalter C, Fischer M, Hopmeier D, et al.Factor XII activity and antigen concentrationsin patients suffering from recurrent thrombosis.Fibrinolysis 1987;1:259–63.
4 Zeerleder S, Schloesser M, Redondo M, etal. Revaluation of the incidence ofthromboembolic complications in congenitalFactor XII deficiency—a study on 73 subjectsfrom 14 Swiss families. Thromb Haemost1999;82:1240–6.
5 Speicher L, Philipp W, Kunz FJ. Factor XIIdeficiency and central retinal vein occlusion.Lancet 1992;340:237.
6 Halbmayer WM, Haushofer A, Schon R, etal. The prevalence of moderate and severeFXII (factor XII) deficiency among the normalpopulation: evaluation of the incidence of FXIIdeficiency among 300 healthy blood donors.Thromb Haemost 1994;71:68–72.
7 Winter M, Gallimore M, Jones DW, et al.Should factor XII assays be included inthrombophilia screening? Lancet1995;346:52.
8 Laffan M, Tuddenham E. Assessingthrombotic risk. BMJ 1998;317:520–3.
Unilateral proptosis: the role ofmedical historyThe most common cause of bilateral and uni-lateral exophthalmus among adults is Graves’disease. Unilateral exophthalmus, althoughfrequently seen in connection with thyroiddiseases, has a much larger differentialdiagnosis than bilateral exophthalmus. Withunilateral presentation one should think oforbital pseudotumour, orbital cellulitis, cav-ernous sinus thrombosis, or intraorbitalneoplasms.1
Graves’ ophthalmopathy (GO) usually isassociated with Graves’ hyperthyroidism(GH) although the temporal relation tothyroid disease is not consistent. It has beenestimated that 77% of GO patients are hyper-thyroid, 21% euthyroid, and 2% hypothyroid.2
The mean absolute interval between GH andGO is 3.3 years in men and 3.6 years inwomen. Two thirds of patients present withorbital symptoms within 18 months of diag-nosis of thyroid disease.3
The following cases of Graves’ ophthal-mopathy are described because of theirunusual presentation: a long interval betweenthyroid disease and the development ofpredominantly unilateral Graves’ ophthal-mopathy. Both cases were seen at the depart-ment of ophthalmology of the UniversityHospital Groningen, Netherlands.
Case 1A female patient born in 1922 became hyper-thyroid with minimal eye signs with possiblysome lid retraction in 1948. She was treatedby thyroidectomy and became clinically eu-thyroid. In 1980 her thyroid function andantibodies were tested because of complaintsof dizziness. Thyroid hormones were withinnormal ranges and thyroperoxidase (TPO)colloid and antiparietal cell antibodies(APCA) were negative.
In January 1983 she presented with com-plaints of sharp pains in both eyes, a feeling ofpressure, and an exophthalmus of her righteye. On ocular examination there were noabnormalities except for exophthalmus of theright eye. Hertel exophthalmometer valueswere 24 mm right eye and 19 mm left eye. InDecember 1983 signs and symptoms wors-ened. Examination at that time showed anobvious retraction of the upper eyelid of theright eye. The exophthalmus was stable. Therewas diplopia caused by a right hypotropia inprimary position of 1.5 degrees with restric-tion of elevation. A computed tomograph (CT)scan showed enlargement of all external eyemuscles of the right eye without involvementof the tendons. During this exacerbation labo-ratory testing showed thyroid hormone levelswithin normal ranges and again TPO and col-loid antibodies tests were negative. The diplo-pia resolved without treatment.
Case 2A male patient born in 1944 was diagnosedwith hypothyroidism in 1979. Thyroid hor-mones were abnormal. FT4 was decreased,TSH was increased, antibodies against colloidwere positive, and APCA and TPO antibodieswere negative. Because of this primary hypo-thyroidism levothyroxine therapy was startedand he gradually became euthyroid. Hisocular history mentioned a disorder of thecentral retinal pigment epithelium and glau-coma which was treated with timolol.
In August 2000 he presented with unilat-
eral proptosis and progressive loss of vision.
Ocular examination showed chemosis and
oedema of the eyelids in both eyes. Visual
acuity was 20/60 right eye and 20/30 left eye.
Pupillary reflexes were normal and symmetri-
cal. Clinically and biochemically he presented
as euthyroid. A CT scan showed bilateral
enlargement of the eye muscles, more marked
on the right side. He was treated with 60 mg
prednisone daily.
One month later visual acuity of the right
eye dropped further and he was referred to
our hospital. Ocular examination showed
marked soft tissue signs, worse in the right
eye, bilateral chemosis, and unilateral exoph-
thalmus of 26 mm in the right eye. Visual
acuity was reduced to counting fingers in the
right eye. Colour vision was diminished and
there was a relative afferent pupillary defect
in the right eye. He had restrictions of the eye
movements of the right eye when looking
upwards, downwards, and in adduction. Thy-
roid hormone levels were again within normal
ranges. He was admitted and methylpred-
nisone 250 mg four times a day intravenouslyand radiotherapy (10 × 2 Gy) were started.Antibody testing showed borderline thy-roglobulin and TPO antibody titres. Results ofTSH receptor antibody testing could not betraced.
As visual function was not restored within areasonable time another CT scan was per-formed which showed enlargement of all rectimuscles of right eye and in lesser extent of theleft eye with signs of compression of the rightoptic nerve. An orbital decompressionthrough a Caldwell-Luc approach was per-formed on the right side. Postoperatively,visual acuity of the right eye improved to20/30 and proptosis in the right eye wasreduced by 8 mm. A strabismus convergens ofthe right eye was the main side effect.
In April 2001 a bilateral medial recessionand a recession of the inferior rectus of theright eye were performed to treat the strabis-mus convergens. Binocular single vision wasachieved in the primary position with somediplopia at extremes of gaze.
CommentUnilateral proptosis as a result of Graves’ dis-ease cannot be rejected as a diagnosis, even 20or 30 years after the onset of thyroid disease.Only one retrospective study among 557patients mentioned intervals up to 25 yearswithout giving exact numbers and underlyingthyroid disease.3 For hypothyroidism and GOone study suggests intervals exceeding 15years.4
Thyroid hormone testing should be per-formed to rule out abnormalities in thyroidhormone levels although thyroid status doesnot seem important as the active phase ofophthalmopathy can occur during hyperthy-roidism, hypothyroidism, and euthyroidism.4
Thyroid antibody testing may be supportivefor the diagnosis. A CT scan can be essential infurther analysis showing enlargement ofextraocular muscles with sparing of thetendons.5 It is also known that a CT scan candemonstrate contralateral eye muscle involve-ment in 50–90% of patients with clinicallyunilateral eye involvement.6
Our two patients illustrate that the medicalhistory is important in evaluating proptosis.One should always think of Graves’ disease asa possible cause of unilateral exophthalmoseven though a patient may have had thyroiddisease more than 20 years earlier.
370 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from
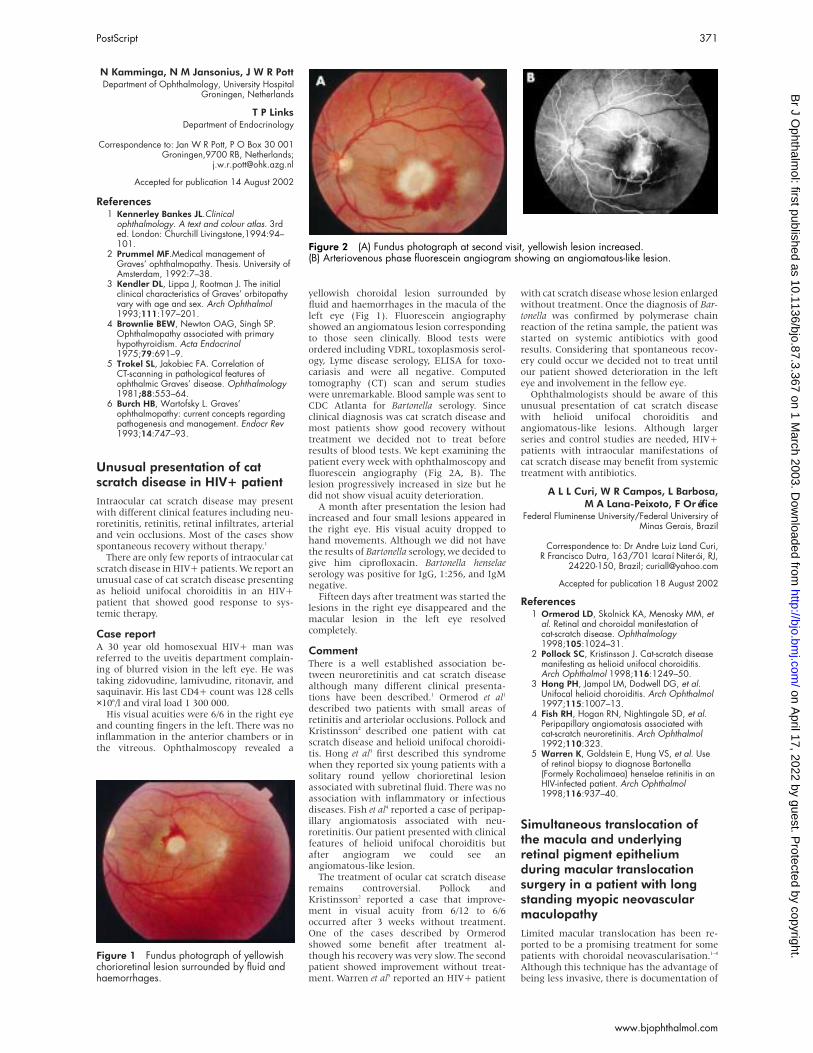
N Kamminga, N M Jansonius, J W R PottDepartment of Ophthalmology, University Hospital
Groningen, Netherlands
T P LinksDepartment of Endocrinology
Correspondence to: Jan W R Pott, P O Box 30 001Groningen,9700 RB, Netherlands;
Accepted for publication 14 August 2002
References1 Kennerley Bankes JL.Clinical
ophthalmology. A text and colour atlas. 3rded. London: Churchill Livingstone,1994:94–101.
2 Prummel MF.Medical management ofGraves’ ophthalmopathy. Thesis. University ofAmsterdam, 1992:7–38.
3 Kendler DL, Lippa J, Rootman J. The initialclinical characteristics of Graves’ orbitopathyvary with age and sex. Arch Ophthalmol1993;111:197–201.
4 Brownlie BEW, Newton OAG, Singh SP.Ophthalmopathy associated with primaryhypothyroidism. Acta Endocrinol1975;79:691–9.
5 Trokel SL, Jakobiec FA. Correlation ofCT-scanning in pathological features ofophthalmic Graves’ disease. Ophthalmology1981;88:553–64.
6 Burch HB, Wartofsky L. Graves’ophthalmopathy: current concepts regardingpathogenesis and management. Endocr Rev1993;14:747–93.
Unusual presentation of catscratch disease in HIV+ patientIntraocular cat scratch disease may presentwith different clinical features including neu-roretinitis, retinitis, retinal infiltrates, arterialand vein occlusions. Most of the cases showspontaneous recovery without therapy.1
There are only few reports of intraocular catscratch disease in HIV+ patients. We report anunusual case of cat scratch disease presentingas helioid unifocal choroiditis in an HIV+patient that showed good response to sys-temic therapy.
Case reportA 30 year old homosexual HIV+ man wasreferred to the uveitis department complain-ing of blurred vision in the left eye. He wastaking zidovudine, lamivudine, ritonavir, andsaquinavir. His last CD4+ count was 128 cells×106/l and viral load 1 300 000.
His visual acuities were 6/6 in the right eyeand counting fingers in the left. There was noinflammation in the anterior chambers or inthe vitreous. Ophthalmoscopy revealed a
yellowish choroidal lesion surrounded byfluid and haemorrhages in the macula of theleft eye (Fig 1). Fluorescein angiographyshowed an angiomatous lesion correspondingto those seen clinically. Blood tests wereordered including VDRL, toxoplasmosis serol-ogy, Lyme disease serology, ELISA for toxo-cariasis and were all negative. Computedtomography (CT) scan and serum studieswere unremarkable. Blood sample was sent toCDC Atlanta for Bartonella serology. Sinceclinical diagnosis was cat scratch disease andmost patients show good recovery withouttreatment we decided not to treat beforeresults of blood tests. We kept examining thepatient every week with ophthalmoscopy andfluorescein angiography (Fig 2A, B). Thelesion progressively increased in size but hedid not show visual acuity deterioration.
A month after presentation the lesion hadincreased and four small lesions appeared inthe right eye. His visual acuity dropped tohand movements. Although we did not havethe results of Bartonella serology, we decided togive him ciprofloxacin. Bartonella henselaeserology was positive for IgG, 1:256, and IgMnegative.
Fifteen days after treatment was started thelesions in the right eye disappeared and themacular lesion in the left eye resolvedcompletely.
CommentThere is a well established association be-tween neuroretinitis and cat scratch diseasealthough many different clinical presenta-tions have been described.1 Ormerod et al1
described two patients with small areas ofretinitis and arteriolar occlusions. Pollock andKristinsson2 described one patient with catscratch disease and helioid unifocal choroidi-tis. Hong et al3 first described this syndromewhen they reported six young patients with asolitary round yellow chorioretinal lesionassociated with subretinal fluid. There was noassociation with inflammatory or infectiousdiseases. Fish et al4 reported a case of peripap-illary angiomatosis associated with neu-roretinitis. Our patient presented with clinicalfeatures of helioid unifocal choroiditis butafter angiogram we could see anangiomatous-like lesion.
The treatment of ocular cat scratch diseaseremains controversial. Pollock andKristinsson2 reported a case that improve-ment in visual acuity from 6/12 to 6/6occurred after 3 weeks without treatment.One of the cases described by Ormerodshowed some benefit after treatment al-though his recovery was very slow. The secondpatient showed improvement without treat-ment. Warren et al5 reported an HIV+ patient
with cat scratch disease whose lesion enlargedwithout treatment. Once the diagnosis of Bar-tonella was confirmed by polymerase chainreaction of the retina sample, the patient wasstarted on systemic antibiotics with goodresults. Considering that spontaneous recov-ery could occur we decided not to treat untilour patient showed deterioration in the lefteye and involvement in the fellow eye.
Ophthalmologists should be aware of thisunusual presentation of cat scratch diseasewith helioid unifocal choroiditis andangiomatous-like lesions. Although largerseries and control studies are needed, HIV+patients with intraocular manifestations ofcat scratch disease may benefit from systemictreatment with antibiotics.
A L L Curi, W R Campos, L Barbosa,M A Lana-Peixoto, F Oréfice
Federal Fluminense University/Federal Universiry ofMinas Gerais, Brazil
Correspondence to: Dr Andre Luiz Land Curi,R Francisco Dutra, 163/701 Icaraí Niterói, RJ,
24220-150, Brazil; [email protected]
Accepted for publication 18 August 2002
References1 Ormerod LD, Skolnick KA, Menosky MM, et
al. Retinal and choroidal manifestation ofcat-scratch disease. Ophthalmology1998;105:1024–31.
2 Pollock SC, Kristinsson J. Cat-scratch diseasemanifesting as helioid unifocal choroiditis.Arch Ophthalmol 1998;116:1249–50.
3 Hong PH, Jampol LM, Dodwell DG, et al.Unifocal helioid choroiditis. Arch Ophthalmol1997;115:1007–13.
4 Fish RH, Hogan RN, Nightingale SD, et al.Peripapillary angiomatosis associated withcat-scratch neuroretinitis. Arch Ophthalmol1992;110:323.
5 Warren K, Goldstein E, Hung VS, et al. Useof retinal biopsy to diagnose Bartonella(Formely Rochalimaea) henselae retinitis in anHIV-infected patient. Arch Ophthalmol1998;116:937–40.
Simultaneous translocation ofthe macula and underlyingretinal pigment epitheliumduring macular translocationsurgery in a patient with longstanding myopic neovascularmaculopathyLimited macular translocation has been re-ported to be a promising treatment for somepatients with choroidal neovascularisation.1–4
Although this technique has the advantage ofbeing less invasive, there is documentation of
Figure 1 Fundus photograph of yellowishchorioretinal lesion surrounded by fluid andhaemorrhages.
Figure 2 (A) Fundus photograph at second visit, yellowish lesion increased.(B) Arteriovenous phase fluorescein angiogram showing an angiomatous-like lesion.
PostScript 371
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

various complications that have been experi-enced with its use.5–8 In this report, wedescribe an unusual complication associatedwith limited macular translocation in apatient with long standing choroidal neovas-cularisation.
Case reportA 35 year old woman was referred to ourdepartment because of a gradual decrease invisual acuity in her right eye. At the first visit,her best corrected visual acuity was right eye,20/40, with a refractive error of −17.5 dioptresin the spherical equivalent. Clinical andangiographic examinations showed a juxta-foveal choroidal neovascularisation. Duringthe subsequent follow up period, choroidalneovascularisation and surrounding retinalpigment epithelial atrophy gradually ex-panded and involved the subfoveal region (Fig1A). We gave the patient detailed informationon the available therapeutic options, includ-ing macular translocation, but she chose con-servative follow up rather than surgical inter-vention. Three years after her first visit, thevisual acuity in her right eye worsened to20/100. At that time, the patient decided tohave surgical treatment. With her consent,limited macular translocation was performedon her right eye, as described previously.4
Postoperatively, fluorescein angiography
showed an extrafoveal neovascular mem-
brane with a foveal shift of 0.7 disc diameter
(Fig 1B). Sharply demarcated hypofluores-
cence in the macular area was also demon-
strated. Biomicroscopic examination revealed
a slightly hyperpigmented lesion underneath
the translocated macula, which corresponded
to the area of hypofluorescence. A horizontal
optical coherence tomography (Humphrey
Systems, San Leandro, CA, USA) section
taken through the translocated macula dis-
played highly reflective double layers (Fig 2A).
These findings may indicate that the abnor-
mal subfoveal retinal pigment epithelium,
which adhered tightly to the overlying neuro-
sensory retina, probably because of the long
history of neovascular maculopathy, was
translocated with the macula during surgery.
Two reflective bands observed on an optical
coherence tomography image may have corre-
sponded to the native retinal pigment epithe-
lium and abnormal retinal pigment epithe-
lium translocated with the macula.
Indocyanine green angiography findings sup-
ported this speculation (Fig 2B).
Despite sufficient foveal displacement, the
patient’s visual acuity has not improved. Dur-
ing a follow up period of 15 months, it has
remained at the same level as her preoperative
vision.
CommentIn many eyes with choroidal neovascularisa-tion, the macula can easily be separated fromthe subjacent fibrovascular tissue. In someeyes with long standing choroidal neovascu-larisation, however, the outer portion ofneurosensory retina may adhere firmly to thesubjacent tissue. In such cases, an innerportion of fibrovascular tissue may be torn offand translocated with overlying neurosensoryretina during macular translocation. Theunderlying healthy retinal pigment epithe-lium covered with the translocated abnormaltissue may not be able to fulfil its physiologi-cal roles on the overlying neurosensory retina,and good functional recovery of the translo-cated macula is unlikely to be achieved. Asdocumented here, simultaneous translocationof the underlying abnormal retinal pigmentepithelium associated with long standingchoroidal neovascularisation can occur duringlimited macular translocation and result in anunsatisfactory visual outcome. When patientsare deciding whether to consent to surgicalintervention with limited macular transloca-tion in such cases, they should be informed ofthe benefits and risks of the treatment, withdue consideration of this complication.
M Ichibe, K Imai, M Ohta,Y Oya,T Yoshizawa, H Abe
Department of Ophthalmology, Niigata UniversitySchool of Medicine, Niigata, Japan
Correspondence to: Dr Ichibe, Department ofOphthalmology, Niigata University School of
Medicine, 1-757 Asahimachi, Niigata 951-8510,Japan; [email protected]
Accepted for publication 22 August 2002
References1 De Juan E Jr, Loewenstein A, Bressler NM, et
al. Translocation of the retina for managementof subfoveal choroidal neovascularization.II: apreliminary report in humans. Am JOphthalmol 1998;125:635–46.
2 Fujikado T, Ohji M, Saito Y, et al. Visualfunction after foveal translocation with scleralshortening in patients with myopicneovascular maculopathy. Am J Ophthalmol1998;125:647–56.
3 Fujii GY, Humayun MS, Pieramici DJ, et al.Initial experience of inferior limited maculartranslocation for subfoveal choroidalneovascularization resulting from causes otherthan age-related macular degeneration. Am JOphthalmol 2001;131:90–100.
4 Ichibe M, Imai K, Ohta M, et al. Fovealtranslocation with scleral imbrication inpatients with myopic neovascularmaculopathy. Am J Ophthalmol2001;132:164–71.
5 American Academy of Ophthalmology.Macular translocation. Ophthalmology2000;107:1015–18.
6 Fujii GY, Pieramici DJ, Humayun MS, et al.Complications associated with limited maculartranslocation. Am J Ophthalmol2000;130:751–62.
7 Fujii GY, De Juan E Jr, Zarbin MA, et al.Unintentional transplantation of autologousretinal pigment epithelium during limitedmacular translocation. Retina2001;21:380–2.
8 Ohji M, Fujikado T, Kusaka S, et al.Comparison of three techniques of fovealtranslocation in patients with subfovealchoroidal neovascularization resulting fromage-related macular degeneration. Am JOphthalmol 2001;132:888–96.
Fungal and bacterial chronicendophthalmitis followingcataract surgeryEndophthalmitis, although rare, is one of themost vision threatening complication of cata-ract surgery. The majority of these infections
Figure 1 (A) A preoperative fluorescein angiogram shows myopic choroidalneovascularisation with marked atrophy of the surrounding retinal pigment epithelium. Anarea of relatively healthy retinal pigment epithelium is shown inferonasal to the fovea. (B) Afluorescein angiogram taken 3 months after the surgery demonstrates a sharply delineatedblockage of choroidal fluorescence in the translocated macular area (white arrow). Theoriginal macular area shows hypofluorescence with larger choroidal vessels well visualised(black arrow). This finding may indicate that the retinal pigment epithelium of the originalmacular region has been torn away and subsequent atrophy of the underlying choriocapillarishas occurred.
Figure 2 (A) A horizontal optical coherence tomography section taken through thetranslocated macula displays highly reflective double layers underneath the fovea thatprobably correspond to the native retinal pigment epithelium and simultaneously translocatedretinal pigment epithelium. (B) A postoperative indocyanine green angiogram shows wellvisualised larger choroidal vessels in the original macular area probably caused by theabsence of the retinal pigment epithelium-choriocapillaris complex (black arrow). The relativehypofluorescence in the translocated macular area may represent blockage of choroidalfluorescence by the translocated retinal pigment epithelium (white arrow).
372 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

are bacterial in the Western world. The occur-rence of fungal endophthalmitis after cataractsurgery is rare as well as polymicrobialinfections.1
We report a case of chronic postoperativeendophthalmitis caused by bacterial and fun-gal pathogenic agents.
Case reportA 73 year old woman was referred for painand redness in the left eye. Her past historywas remarkable for an extracapsular cataractextraction in the left eye with a posteriorchamber intraocular lens implant that hadbeen performed in Turkey in 1998. The patienthad recurrent episodes of decreased visionand ocular pain in the postoperative courseand was treated with peribulbar injections ofcorticosteroids over 2 years. On presentation,visual acuity was hand movements in the lefteye. Slit lamp examination of the left eyeshowed a white corneal infiltrates involvingthe superior and nasal quadrant (Fig 1). Therewas a moderate anterior chamber reactionand a 1 mm hypopyon. The implant was ingood position and no residual cortical mate-rial was seen. The vitreous showed 2+ cells.Intraocular pressure was normal. Examina-tion of the right eye was normal except for amild nuclear cataract. The diagnosis ofchronic infectious endophthalmitis was sus-pected.
The aqueous cultures were sterile for bacte-ria and fungi. Intravitreal injections of vanco-mycin and amikacin were performed. Postop-eratively, the patient was given intravenousciprofloxacin, piperillin, and topical fortifiedticarcillin, gentamicin, and vancomycin drops.The eye showed no improvement during thenext 3 weeks and the patient subsequentlyunderwent removal of the implant and capsu-lar bag which grew Candida parapsilosis, Coryne-bacterium striatum, and Staphylococcus epider-midis.
Intravitreal injection of amphotericin B (5µg, weekly), topical amphotericin B (7 mg/mleye drops every 2 hours), and oral fluconazole(400 mg a day) were then added to thepatient’s regimen. A decrease in intraocularinflammation and corneal infiltrates wasnoted after 1 month of treatment that wasstopped by the patient. Six months later,visual acuity of the left eye was no lightperception and biomicroscopic examinationshowed panophthalmitis. The patient refusedmedical treatment and enucleation was per-formed.
CommentSpecies of candida, other than Candida albi-cans, are normal flora of cutaneous and muco-cutaneous surfaces and are only rarely in-criminated as agents of clinical disease inimmunocompetent hosts. Candida parapsilosisis in fact one of the most common fungi cul-tured from the normal human external eye.2
However, it can cause infectious crystallinekeratopathy or, more typically, suppurativestromal keratitis. Candida parapsilosis has alsobeen reported as a cause of small epidemics ofpostoperative endophthalmitis.3 In thepresent case, Candida parapsilosis could be con-sidered as a true pathogenic organism be-cause of its localisation, in the capsular bag,and also because antifungal therapy waseffective.
On the other hand, Staphylococcus andCorynebacterium species are frequently identi-fied in postoperative endophthalmitis.1
This case is, to our knowledge, the firstdocumented report of bacterial and fungalendophthalmitis following cataract surgery.The use of broad spectrum antibiotics, theadministration of steroids, and the increasednumber of patients with local or systemicimmunosuppression could explain the devel-opment of such infections which are frequentin post-traumatic endophthalmitis but ex-tremely rare after cataract surgery.1 4 However,cross contamination by hospital personnelmay also account for increase in yeastinfections in certain environments. A recentsurvey of hospital personnel revealed that70% of nurses and non-nursing hospitalpersonnel carried yeasts on their hands,particularly subungual spaces, with Candidaparapsilosis being those most frequentlyrecovered.5
This case demonstrates the atypical presen-tation and the poor prognosis of polymicrobialendophthalmitis. Identification of all theorganisms is essential before the onset oftherapy, emphasising the need for completemicrobiological evaluation of any postopera-tive endophthalmitis.
T Bourcier, S Scheer, C Chaumeil,C Morel, V Borderie, L Laroche
Quinze-Vingts National Center of Ophthalmology,Paris, France
Correspondence to: Tristan Bourcier;[email protected]
Accepted for publication 28 August 2002
References1 Kunimoto DY, Das T, Sharma S, et al, and
the Endophthalmitis Reseach Group.
Microbiologic spectrum and susceptibility ofisolates: Part I. Postoperative endophthalmitis.Am J Ophthalmol 1999;128:240–2.
2 Weems JJ Jr. Candida parapsilosis:epidemiology, pathogenicity, clinicalmanifestations, and antimicrobialsusceptibility. Clin Infect Dis1992;14:756–66.
3 Fox GM, Joondeph BC, Flynn HW Jr, et al.Delayed-onset pseudophakic endophthalmitis.Am J Ophthalmol 1991;111:163–73.
4 Kunimoto DY, Das T, Sharma S, et al, andthe Endophthalmitis Reseach Group.Microbiologic spectrum and susceptibility ofisolates: Part II. Posttraumatic endophthalmitis.Am J Ophthalmol 1999;128:242–4.
5 Strausbaugh LJ, Sewell DL, Ward TT, et al.High frequency of yeast carriage on hands ofhospital personnel. J Clin Microbiol1994;32:2299–300.
MAILBOX
Surgical performance forspecialties undertaking temporalartery biopsies: who shouldperform them?We read with interest the paper by Gallowayand colleagues which suggests that ophthal-mologists are best suited to perform temporalartery biopsies.1 We recently completed aretrospective study of all the temporal arterybiopsies performed at four teaching hospitals(Hammersmith Hospital, Charing Cross Hos-pital, St Mary’s Hospital and The Western EyeHospital) in north London between January1998 and January 2002. Ninety one patientsunderwent 92 biopsies. Of these, 15 werepositive for temporal arteritis implying a 16%positive biopsy rate which is compatible withGalloway et al’s results. Ophthalmologists per-formed 54 biopsies (59%) while general andvascular surgeons (GVS) performed 38 biop-sies (31%). Both groups had similar positivebiopsy rates—ophthalmologists 10/54 (19%)and GVS 5/28 (13%). In an analysis of theability to perform biopsies, the ophthalmolo-gists had two failed biopsies (onespecimen—no artery identified and onespecimen—crushed artery) while the GVSgroup had one failed biopsy (no artery identi-fied). The average artery length was 13.0 mm(range 5–21 mm) for the ophthalmologistsand 14.0 mm (range 7–22 mm) for the GVSgroup.
We disagree with Galloway and colleagues’assertions that ophthalmologists are bestsuited to performing temporal artery biopsiesas our study found that both groups of
Figure 1 Anterior segment photograph ofthe left eye showing an hypopyon and acrystalline keratopathy.
Figure 2 Higher magnification showingcrystalline keratopathy.
If you have a burning desire to respond toa paper published in the BJO, why notmake use of our “rapid response” option?
Log on to our website(www.bjophthalmol.com), find the paperthat interests you, and send your responsevia email by clicking on the “eLetters”option in the box at the top right handcorner.
Providing it isn’t libellous or obscene, itwill be posted within seven days. You canretrieve it by clicking on “read eLetters”on our homepage.
The editors will decide as beforewhether to also publish it in a futurepaper issue.
PostScript 373
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

surgeons obtained similar lengths of arteryand had similar positive biopsy rates. We notethat in their study, while the vascular sur-geons only performed two of the 41 biopsies,the average length of specimen obtained was22.5 mm, thus suggesting that the vascularsurgeons may well be the best group toperform these biopsies. In Charing Cross Hos-pital, the vascular surgeons routinely use aDoppler ultrasound probe to help detect anddemarcate the superficial temporal arterybefore biopsy and this practice has been advo-cated by other studies to help improve theyield of the biopsy.2 3 In our study, all the biop-sies performed by ophthalmologists weredone as extra cases in theatre and seven caseshad to be performed outside normal workinghours as emergencies because of lack of thea-tre time. The fact that ophthalmologistsperformed 59% of biopsies may be due to thefact that all four hospitals had large neuro-logical and rheumatological units attached tothem. We feel that both ophthalmologists andgeneral and vascular surgeons are equallycapable of performing temporal artery biop-sies and that guidelines should be designedlocally to decide who should perform thebiopsies. More importantly, the follow up ofthese patients should be clearly stated and beideally under the care of the rheumatologists.
K Fong, V FergusonThe Western Eye Hospital, Marylebone Road,
London NW1 5YE
Correspondence to: Dr Kenneth Fong;[email protected]
References1 Galloway GD, Klebe B, Riordan-Eva P.
Surgical performance for specialtiesundertaking temporal artery biopsies: whoshould perform them? Br J Ophthalmol2002;86:250.
2 Brosig J, Holtkamp A, Clemens S. Possibilitiesand limits in the imaging of extracranialvessels with conventional ultrasonography.Klin Monatsbl Augenheilkd 1997;211:301–5.
3 Hunder GG, Weyand CM. Sonography ingiant-cell arteritis. N Engl J Med1997;337:1385–6.
Major complications ofendoscopic sinus surgery: acommentWe were pleased to read the informative arti-cle by Rene et al.1 The authors refer to “Odonicells” as, “aerated posterior ethmoid air cellsalong the optic canal.” Could it be that theymeant to refer to the cells as “Onodi cells”?Onodi described a number of variations ofposterior ethmoid anatomy.2 Endoscopic sinussurgeons refer to the pattern of extramuralpneumatisation of the ethmoid lateral orsuperolateral to the sphenoid, where the pos-terior ethmoid is indented by the optic canal,as an Onodi cell.3 More recently it has beensuggested that this cell is better characterisedas a “sphenoethmoidal” cell.4
The main significance of the Onodi or sphe-noethmoid cell is that while sinus surgeonsexpect to find the optic nerve in the sphenoidsinus, they are not routinely looking for it inthe posterior ethmoid. Consequently, thechance of iatrogenic injury is likely to behigher in patients with Onodi cells and evenhigher in patients with extensively pneuma-tised Onodi cells.5 The exact incidence ofOnodi cells is unclear. Endoscopic dissectionstudies suggest an incidence as high as 39%5
or 42%.3 CT imaging studies suggest a lowerincidence of 7%.5 Driben et al5 feel that the
likelihood of a sphenoethmoid cell increaseswith increasing obliquity of the anteriorsphenoid wall. Racial factors may also have arole as Onodi cells appear to be more commonin Asian patients.6
Every effort should be made to identifysphenoethmoid cells preoperatively and to beaware of intraoperative clues such as anteriorsphenoid wall alignment, which may point tothe presence of an Onodi cell. Attention tothese important details will increase the like-lihood of uncomplicated endoscopic sinussurgery at the sphenoethmoidal junction.
S M GrahamDepartment of Otolaryngology-Head and Neck
Surgery
K D CarterOculoplastic and Orbital Service, Department of
Ophthalmology and Visual Sciences, University ofIowa, Iowa City, IA, USA.
Correspondence to: Scott M Graham, MD,University of Iowa Hospitals and Clinics,
Department of Otolaryngology-Head and NeckSurgery, 200 Hawkins Drive, 21201 PFP, Iowa
City, IA 52242–1093, USA;[email protected]
References1 Rene C, Rose GE, Lenthall R, et al. Major
orbital complications of endoscopic sinussurgery. Br J Ophthalmol 2001;85:598–603.
2 Onodi A. The optic nerve and the accessorysinuses of the nose: a contribution ofcanalicular neuritis and atrophy of the opticnerve of nasal origin. Ann Otol RhinolLaryngol 1908;17:1–116.
3 Kainz J, Stammberger H. Danger areas of theposterior rhinobasis: an endoscopic andanatomical surgical study. Acta Otolaryngol1992;112:852–61.
4 Kennedy DW. International conference onsinus disease: terminology, staging, therapy.Ann Otol Rhinol Laryngol 1995;104(suppl167):7–16.
5 Driben JS, Bolger WE, Robles HA, et al. Thereliability of computerized tomographicdetection of the Onodi (sphenoethmoid) cell.Am J Rhinol 1998;12:105–11.
6 Yeoh KH, Tan KK. The optic nerve in theposterior ethmoid in Asians. Acta Otolaryngol(Stockh) 1994;114:329–36.
Trabeculectomy augmented withantimetabolites with aviscocanalostomy technique forthe management of open angleglaucomaIn a small randomised, prospective study,O’Brart and co-workers1 attempted to provethat trabeculectomy (n=25) provided betterintraocular pressure (IOP) control than visco-canalostomy (n=23). However, we have seri-ous concerns about the methodology of thisstudy that need to be addressed.
Viscocanalostomy is characterised by theinjection of viscoelastic into Schlemm’scanal.2 However, this was not performed inhalf of the patients randomised to this group.This would be as inappropriate as using anantimetabolite in only half the patients in thetrabeculectomy group, and then comparingthis entire group to the viscocanalostomygroup. Although the authors do state that thesubgroup of patients with intracanalicularviscoelastic injection was inferior to trab-eculectomy, this cohort consisted only of 12patients and it is not known how many hadcompleted follow up after 18 months. Surely,these small numbers are insufficient to drawsuch conclusions.
We are also concerned that the use of intra-operative antimetabolites in the trabeculec-tomy group added a major confounding vari-able in this study. This is particularlyperplexing as the authors’ viscocanalostomytechnique primarily relied on subconjunctivalfiltration, as evidenced by their triangularscleral flap design and looser suturing tech-nique in which only three 10/0 nylon sutureswere used. Furthermore, their excellent earlysuccess rate of viscocanalostomy (95% at 6months), the presence of filtering blebs intheir successful viscocanalostomy procedures,the lack of one in their failures, and the needfor postoperative bleb needling and5-fluorouracil injections all indicate this. Theuse of mitomycin-C and 5-fluorouracil im-proves the success rate of glaucoma filteringsurgery by reducing episcleral fibrosis,3 andprobably explains the difference in successrates in this study. We wonder what theresults would have been had the use of intra-operative antimetabolites been used in allgroups, or if none was used at all.
In contrast with the authors’ technique, weemploy Stegmann’s approach to viscocanalos-tomy in using a parabolic superficial flapsecured tightly with five sutures in a relativelywater tight fashion.2 Although low lying blebsmay develop, most patients achieve IOPlowering through multiple alternate path-ways including uveoscleral, through Sch-lemm’s canal, and subconjunctival.4 Certainlyin higher risk cases, we feel that there is a rolefor antimetabolites in non-penetrating sur-gery, and have found it to be safer than whenused with trabeculectomy.
It should be mentioned that quite often wedo rely on subconjunctival filtration in non-penetrating procedures (that is, deep sclerec-tomy) but advocate the use of a collagenwick5 or hyaluronic acid6 implant with anintraoperative antimetabolite in higher riskcases to obtain optimal IOP control.
Fibrosis and loss of permeability of thetrabeculo-Descemet’s window (TDW) is a welldescribed cause of postoperative elevation inIOP after non-penetrating glaucoma surgery.Postoperative Nd:YAG goniopuncture of theTDW in these cases is a relatively easy adjunc-tive procedure and may be needed in up to41% of non-penetrating procedures.7 It hasbeen reported to successfully lower postopera-tive IOP in over 80% of cases.7 Yet, we are dis-mayed that the authors decided not toattempt laser goniopuncture in those viscoca-nalostomy cases with postoperative IOP eleva-tions because “such interventions clearly con-vert a ‘non-penetrating’ technique into apenetrating, full thickness procedure.” Wevehemently disagree with this line of reason-ing as we feel goniopuncture is an extremelyuseful adjunctive procedure and converting toa penetrating (not “full thickness”) procedurein the safety of the controlled postoperativeperiod is completely reasonable. This is akin tosuture lysis in trabeculectomy. Would theauthors feel that performing suture lysis con-stitutes conversion of a guarded trabeculec-tomy into a full thickness unguarded trab-eculectomy and thus cannot be fairlycompared? Although goniopuncture was per-formed in only three eyes at 18 months, wewonder what results would have be obtainedif this was done in all cases with uncontrolledIOPs at any point in the postoperative period.
Although we are critical of this study, weapplaud O’Brart and colleagues for attempt-ing to investigate this evolving area ofglaucoma surgery. Although they may haveshown that trabeculectomy with the use of anantimetabolite is superior to a modified form
374 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

of viscocanalostomy dependent on subcon-junctival filtration without the use of anantimetabolite, this study unfortunately doesnot fairly compare the efficacy of Stegmann’sviscocanalostomy technique versus trab-eculectomy. Non-penetrating glaucoma sur-gery certainly has an improved safety profileand surely as future well designed controlledstudies become available, the efficacy of theseprocedures compared to trabeculectomy willbecome clearer.
I I K Ahmed, C KranemannUniversity of Toronto, Toronto, Ontario, Canada
Correspondence to: I I K Ahmed, 43 Bywood Drive,Toronto, Ontario M9A 1M1;
References1 O’Brart DPS, Rowlands E, Islam N, et al. A
randomised, prospective study comparingtrabeculectomy augmented withantimetabolites with a viscocanalostomytechnique for the management of open angleglaucoma uncontrolled by medical therapy. BrJ Ophthalmol 2002;86:748–54.
2 Stegmann R, Pienaar A, Miller D.Viscocanalostomy for open-angle glaucoma inblack African patients. J Cataract Refract Surg1999;25:316–22.
3 Skuta GL, Beeson CC, Higginbotham EJ, etal. Intraoperative mitomycin-C versuspostoperative 5-fluorouracil in high-riskglaucoma filtering surgery. Ophthalmology1992;99:438–44.
4 Chiou A, Mermoud A, Underdahl JP, et al.An ultrasound biomicroscope study of eyesafter deep sclerectomy with collagen implant.Ophthalmology 1998;105:746–50.
5 Mermoud A, Schnyder CC, Sickenberg M, etal. Comparison of deep sclerectomy withcollagen implant and trabeculectomy inopen-angle glaucoma. J Cataract Refract Surg1999;25:323–31.
6 Sourdille P, Santiago P-Y, Villain F, et al.Reticulated hyaluronic acid implant innonperforating trabecular surgery. J CataractRefract Surg 1999;25:332–9.
7 Mermoud A, Karlen ME, Schnyder CC, et al.Nd:YAG goniopuncture after deepsclerectomy with collagen implant.Ophthalmic Surg Lasers 1999;30:120–5.
Argon laser and trichiasisWe were interested to read the approach takenby Sahni and Clark1 to facilitate the effectiveargon laser treatment of trichiasis. They haveably reviewed the complications of trichiasis,the different forms of management of trichi-asis, the advantages of argon laser treatmentin the management of trichiasis, the tech-nique of argon laser trichiasis therapy, and thelimitations of lash laser therapy.
We take issue with the authors in two areas.Firstly, the almost certain consequence ofusing a duration of laser treatment of 0.1 sec-ond is that if the laser “takes,” the lash willdisappear within the space of a few lasershots, effectively precluding the destruction ofthat particular lash follicle. We have particu-larly made it a point that when teachingtrainees the technique of lash laser, we ensurethat the energy burst lasts long enough tocommence visible lash destruction as well asdestruction of the subcutaneous lash, as theburn is directed towards the lash follicle. Thuswe always use a duration of several seconds,or even continuous energy, and aim to achieveinitiation of effective lash destruction abovethe lid level after the first shot, or certainlywithin three shots. Thus, 1–3 second durationbursts may be required, depending on theindividual lash. Just a few more shots willeffectively and completely destroy the sub-cutaneous lash and its follicle.
Secondly, the article by Bartley and Lowryquoted by the authors, describes using a “dropof ink from a fountain pen” to facilitate lashlaser.2 Presumable in the interests of sterility,Sahni and Clark have used the ink from a“blue skin marker pen” to allow improvedabsorption of argon laser energy. While use ofa fresh marker pen for each patient may berelatively efficient, it could not be regarded ascost effective. By contrast, in a proceduredescribed by us in 1994,3 we found that trans-ferring a tiny drop of the patient’s own blood,whether still liquid or already coagulated, tothe lash base on the lid margin is a simple,rapid, cheap, safe, and highly effective methodof getting the laser reaction started when thelashes are pale. We have found that therequired amount of blood is invariably presenton the patient’s own lid skin at the site of localanaesthetic infiltration. We usually transfer itby picking it up with a sterile drawing up nee-dle. This is achieved remarkably easily on thelaser slit lamp, which allows adequate magni-fication for the accurate siting of the trans-ferred blood.
G A Wilcsek, I C FrancisThe Ocular Plastics Unit, Prince of Wales Hospital,
and the University of New South Wales, Randwick,Sydney, Australia
Correspondence to: Ian C Francis;[email protected]
References1 Sahni J, Clark D. Argon laser and trichiasis:
a helpful tip. Br J Ophthalmol 2001;85:761.2 Bartley GB, Lowry JC. Argon laser treatment
of trichiasis. Am J Ophthalmol1992;113:71–4.
3 Ghabrial R, Francis IC, Kappagoda MB.Autologous blood facilitation of lid lasertreatment. Aust NZ J Ophthalmol1994;22:218.
Management of age relatedmacular degeneration: still roomfor improvementThe aim of Mitchell et al’s study1 in collabora-tion with the Macular Disease Society (MDS)was to assess the perceived quality of healthcare of people with macular disease in theUnited Kingdom. The study was performed in1999 and took the form of a retrospectiveaudit by postal survey of 2000 members of theMDS. I performed a similar but smaller studyin collaboration with the MDS 7 yearsearlier.2 This also took the form of a retrospec-tive audit by postal survey of 200 members ofthe MDS. The aim was to assess the clinicalmanagement of patients with age relatedmacular degeneration (ARMD) in the UnitedKingdom from the patients’ perspective. Thefinal response rate was 79% (similar to 77% ofMitchell et al) and patients had attended over105 ophthalmic units throughout the UnitedKingdom. Mitchell et al omitted this earlierstudy from their discussion but comparison ofthe two studies raises some noteworthypoints.
The prevention3 and treatment4 of ARMDremains far from ideal both for the majority ofpatients and their ophthalmologists. Mem-bers of the MDS are likely to be a highly moti-vated study group and it is not clear how theirviews will reflect the views of patients as awhole with ARMD. However, both studieshighlighted the fact that lack of informationand advice on ARMD is a significant cause ofdissatisfaction for these patients. Mitchell et alasked if the diagnostic consultation with theeye specialist was satisfactory: 59% responded
“yes” and 41% “no.” The two most commonreasons given for a negative answer were theattitude of the specialist and lack of infor-mation and advice (43.5% and 43.4% respec-tively of those answering this question). Theearlier study specifically asked whether pa-tients were given written information onARMD, were informed about support groupsor informed about relevant radio programmesby the eye department.2 Only 6% receivedwritten information, 14% were given detailsof support groups, and 3% details of relevantprogrammes. By definition 100% of the studygroup would have liked to have been in-formed of the existence of the MacularDisease Society by the eye unit. However, ninedifferent sources were cited for discoveringthe MDS; over 80% from radio and magazineswith only 12% from the ophthalmic unit.Unfortunately, despite that fact that the twostudies are separated by 7 years, any temporalcomparison has to be undertaken withcaution. The protocol of both surveys includedquestionnaires being sent to members of theMDS chosen at random from the MDSmailing list. It is therefore conceivable that aproportion of the original study group alsoformed part of the second, larger study group.What is clear though, is that despite the factthat patients want information on ARMD andthe fact that there are readily available sources(for example, free information booklets onARMD from the Royal College of Ophthal-mologists or Royal National Institute for theBlind), ophthalmic units throughout theUnited Kingdom are still failing routinely toprovide such information to their patients.
L J HoweMoorfields Eye Hospital, City Road, London
EC1V 2PD, UK; [email protected]
References1 Mitchell J, Bradley P, ffytche T, et al.
Perceived quality of health care in maculardisease: a survey of members of the MacularDisease Society. Br J Ophthalmol2002;86:777–81.
2 Howe LJ. Clinical management of age-relatedmacular degeneration: room for improvement.Eye 1995;9 (suppl.):42–6.
3 Hall NF, Gale CR. Prevention of age relatedmacular degeneration. BMJ 2002;325:1–2.
4 Wormald R, Evans J, Smeeth L, et al.Photodynamic therapy for neovascular agerelated macular degeneration. CochraneDatabase of Systemic Reviews(3):CD002030, 2001.
Standardised clinicalphotography in ophthalmicplastic surgeryWe read with keen interest the path breakingarticle by Calista et al regarding the successfultreatment of an eyelid squamous cell carci-noma with intralesional cidofovir.1 The dra-matic response of this highly malignant lesionto such a non-invasive form of therapy isremarkable and certainly worth further clini-cal evaluation. However, we would like to raisea few crucial issues pertaining to the docu-mentation of this case.
The authors have presented an extremeclose up of the affected eye in Figure 1, whichhighlights the pretreatment appearance of thelesion quite adequately. However, the post-treatment photograph (Fig 2) is almost halfthe magnification of Figure 1. Therefore,although there is an indisputable reduction inthe size of the tumour, the two clinical photo-graphs are not strictly comparable since adecrease in magnification results in visualclues that lead to the lesion being perceived assmaller in size.
PostScript 375
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

Secondly, the pretreatment view (Fig 1) hasbeen taken in primary gaze and reveals a rightlower lid retraction as well as the semblance ofa mild lid notch. In contrast, the post-treatment view (Fig 2) has been photo-graphed on the left and slight downgaze anddoes not show either of the above findings.Now, it is difficult to discern whether there isan actual disappearance of these pretreatmentfindings or it is due to the inherent lack ofcomparability of these pictures because oftheir being in totally different positions ofgaze, which is compounded by the magnifica-tion factor mentioned earlier. It would be ofimmense benefit to the readers if the authorscould kindly clarify these points of discrep-ancy, which have arisen due to dissimilarphotographs.
It is imperative that extremely high stand-ards of clinical photography be maintained inplastic surgery/oncology and photographs betaken with similar parameters to ensure validpretreatment and post-treatment compari-sons that accurately reflect the results.2 3 Thestandards and recommendations for clinicalphotography have been widely documentedand should be universally practised.4 Theseinclude using the same camera lens, settings,lighting, film, magnification, and patientposition to ensure reproducibility andcomparisons.2 Even small variations in thepictures may cause drastic changes in theclinical and research value of photographyand, unless stringent criteria are met, thephotographs may lose their relevance andoverall impact.5
M S Bajaj, N Pushker, A Mahindrakar,R Balasubramanya
Correspondence to: Mandeep S Bajaj, RP Centre,All India Institute of Medical Sciences, Ansari
Nagar, New Delhi 110029, India;[email protected]
References1 Calista D, Riccioni L, Coccia L. Successful
treatment of squamous cell carcinoma of thelower eyelid with intralesional cidofovir. Br JOphthalmol 2002;86:932–33.
2 DiBernardo BE, Adams RL, Krause J, et al.Photographic standards in plastic surgery.Plast Reconstr Surg 1998;102:559–68.
3 Talamas I, Pando L. Specific requirements forpreoperative and postoperative photos used inpublication. Aesthetic Plast Surg2001;25:307–10.
4 Yavuzer R, Smirnes S, Jackson IT. Guidelinesfor standard photography in plastic surgery.Ann Plast Surg 2001;46:293–300.
5 Jemec BI, Jemec GB. Photographic surgery:standards in clinical photography. AestheticPlast Surg 1986;10:177–80.
Entonox as an analgesic agentWe read with great interest the paper onEntonox as an analgesic agent by Cook et al.1
We congratulate the authors for their work.However, we would like to clarify certainaspects of the study.
We recently performed a randomised, pla-cebo controlled, double blind study with 100patients on the analgesic effect of Entonox forpain relief during local anaesthetic injectionsin minor eyelid procedures (accepted for pub-lication). We administered Entonox for 30seconds in our study and found no statisti-cally significant difference in the pain scoresbetween the control and the study groups. Noside effects were reported but in our pilotstudy, where the patients were given Entonoxfor 60 seconds, all the Entonox group patientsreported light headedness and required pro-longed observation before being discharged.
We attributed our results of lack of statisti-cally significant pain relief with Entonox toless than 50 seconds’ administration ofEntonox. Waud et al2 have shown that optimaladministration of Entonox should cover 50seconds, based on theoretical calculations foreffective pain relief. Based on the aboveexperience, we would like to know if theauthors administered Entonox throughoutthe laser treatment and, if so, did it not inter-fere with the laser delivery since the inhala-tion process is likely to be associated withhead movements? If the Entonox was givenfor a shorter duration, we need to know theduration of administration since that wouldbe of practical benefit to the readers.
The authors have concluded that Entonox isuseful in young patients, those undergoingre-treatments, and in patients who havepreviously not been able to tolerate the fulltreatment. We would like to know how theauthors came to this conclusion, as there is nomention of the type of patients selected fortheir study.
S Sandramouli, M KurliWolverhampton and Midland Counties EyeInfirmary, Compton Road, Wolverhampton
WV3 9QR, UK
Correspondence to: Mr S Sandramouli;[email protected]
References1 Cook HL, Newsom RSB, Mensah E, et al.
Entonox as an analgesic agent duringpanretinal photocoagulation. Br J Ophthalmol2002;86:1107–8.
2 Waud BE, Waud DR. Calculated kinetics ofdistribution of nitrous oxide and methoxyflurane during intermittent administration inobstetrics. Anaesthesiology 1970;32:306–16.
Mechanism of ophthalmic arteryocclusion following pars planavitrectomySaito et al present a patient with Terson’s syn-drome and dense vitreous haemorrhage whounderwent pars plana vitrectomy and wasnoted postoperatively to have developed anophthalmic artery occlusion.1 They proposethat the ophthalmic artery was occluded bythe spontaneous release of an embolus froman atheromatous plaque in the internalcarotid artery. This seems unlikely in a 39 yearold man without a previous history ofsymptomatic atherosclerotic disease. Al-though the authors identified plaques in thepatient’s carotid artery by ultrasound, thesecan be seen in 11% of asymptomatic malesunder age 40 and may therefore be anincidental finding in this case.2
An alternate explanation for the patient’socular findings is trauma from the retrobulbarinjection. Intravascular injection into theophthalmic artery has been reported as acomplication of retrobulbar anaesthesia.3 It ispossible that either an intravascular injectionor simply needle tip trauma resulted inthrombus formation with obstruction of flowin the ophthalmic artery. It should also benoted that although acute ophthalmic arteryocclusion is the presumed diagnosis, the samefindings could result from simultaneous ob-structions of the retinal and choroidal circula-tions4, also a potential consequence of errantretrobulbar injection. The possibility that thepatient’s chorioretinal disturbance could havebeen iatrogenic highlights the importance of athorough preoperative discussion with pa-tients about the risks and benefits of different
methods of delivering anaesthesia for oph-thalmic surgery.
J M StewartOphthalmology, University of California, San
Francisco, CA, USA; [email protected]
References1 Saito W, Yamamoto S, Takeuchi S, et al.
Ophthalmic artery occlusion following parsplana vitrectomy in a patient with Terson’ssyndrome. Br J Ophthalmol2002;86:1063–4.
2 Sun Y, Lin CH, Lu CJ, et al. Carotidatherosclerosis, intima media thickness andrisk factors—an analysis of 1781asymptomatic subjects in Taiwan.Atherosclerosis 2002;164:89–94.
3 Morgan CM, Schatz H, Vine AK, et al.Ocular complications associated withretrobulbar injections. Ophthalmology1988;95:660–5.
4 Brown GC, Magargal LE, Sergott R. Acuteobstruction of the retinal and choroidalcirculations. Ophthalmology1986;93:1373–82.
Dynamics of corneal endothelialcell death in organ cultureWe read with interest the remarks of Crow-ston et al1 on our article.2 We showed that theTUNEL technique revealed a far higherpercentage of endothelial cells (ECs) irrevers-ibly engaged in a cell death process than thatobtained by trypan blue staining.
The two techniques were performed se-quentially: after observation of trypan bluestaining, corneas were immediately fixed informaldehyde for TUNEL. Crowston et al sug-gest that the trypan blue itself and/or the timespent outside the organ culture mediumbefore fixing in formaldehyde may havecaused an artefactual increase in the percent-age of TUNEL positive ECs. Two argumentscounter this remark.
(1) The trypan blue staining procedure isidentical to that used, during endothelialexamination(s) of grafts, in all European cor-nea banks that use organ culture duringendothelial examination(s) of grafts. Neitherthe low concentration of trypan blue (0.4%)nor the short exposure time (about 1 minute)nor the short incubation in the presence of0.9% NaCl has ever been incriminated in theover-mortality of ECs in routine practice.3
Moreover, the innocuity of injections oftrypan blue into the anterior chamber, a com-mon feature during cataract surgery, has beenwell demonstrated.4
(2) The time spent outside the organculture medium before fixing in formalde-hyde, a period required for vital staining andmicroscopic examination of the endothelium,lasts only a few minutes. The cornea remainsunder the microscope for about 1 minute only,the time needed for image acquisition. Suchrapidity is possible by using a prototype auto-matic analyser of the endothelium, which wedeveloped and have recently published.5 Thisis very probably insufficient time for DNAfragmentation to occur at the level weobserved. Moreover, the fixing of the endothe-lial layer in 10% formaldehyde is immediate,and prevents any continuation of fragmenta-tion phenomena. On balance, it is highlyunlikely that the succession of markings isresponsible for the discrepancy between thepositivity percentages of the two techniques.In addition, we chose not to perform the twotechniques simultaneously on paired corneasor on the halves of one cornea because wewanted to superimpose the two stains on thesame cornea and thus obtain a double cellstaining.
376 PostScript
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from

The second remark by Crowston et al is par-ticularly interesting. We too were surprised bythe high percentage of TUNEL positive ECs(mean 12.7%, SD 16.4). This may imply thatall the cells died within 8 days, which was evi-dently not the case. We believe this apparentcontradiction can be explained by the follow-ing theory. The TUNEL staining is positiveduring a relatively long window (24–48hours6). The TUNEL index, measured at agiven moment, provides a global view of allthe cells with fragmented DNA. However, theDNA fragmentation may be at differentstages, and the cells very likely spread accord-ing to a Gaussian distribution. Therefore thecells, which are TUNEL positive at a givenmoment, will not all die instantaneously andsimultaneously. Only the cells furthest to theright on the curve will die in the very shortterm, and it is probably these that are liable tobe revealed by trypan blue. If it were possibleto perform TUNEL on two consecutive days,the percentage of positive cells revealed wouldprobably be very similar, but a large majorityof the positive cells recorded on the secondday would have already been counted on dayone. It is, however, undeniable that the cellsthat are TUNEL positive at a given momentwill all die eventually. In other words, webelieve that, at the end of storage, corneascontain a number of ECs engaged in anirreversible cell death process far more exten-sive than the highly unreliable trypan bluestaining technique suggests.
G Thuret, C Chiquet, L Campos, P GainCell Death and Neoplasia Laboratory EA 3063,
University Hospital, St Etienne, France
Correspondence to: Gilles Thuret;[email protected]
References1 Crowston JG, Healey PR, Maloof A, et al.
Quantifying corneal endothelial cell death. BrJ Ophthalmol 2002;86:1068.
2 Gain P, Thuret G, Chiquet C, et al. Value oftwo mortality assessment techniques for organcultured corneal endothelium: trypan blueversus TUNEL technique. Br J Ophthalmol2002;86:306–10.
3 Sperling S. Evaluation of the endothelium ofhuman donor corneas by induced dilation ofintercellular spaces and trypan blue. GraefesArch Clin Exp Ophthalmol 1986;224:428–34.
4 Norn MS. Per operative trypan blue vitalstaining of corneal endothelium. Eight years’follow up. Acta Ophthalmol 1980;58:550–5.
5 Gain P, Thuret G, Kodjikian L, et al.Automated tri-image analysis of stored cornealendothelium. Br J Ophthalmol2002;86:801–8.
6 Mesner PW, Epting CL, Hegarty JL, et al. Atimetable of events during programmed celldeath induced by trophic factor withdrawalfrom neuronal PC12 cells. J Neurosci1995;15:7357–66.
NOTICES
Role of optometry in Vision 2000The latest issue of Community Eye Health (No43) discusses the mobilisation of optometry todeal with uncorrected refractive error, whichis now a major cause of functional blindness.
For further information please contact: Jour-nal of Community Eye Health, InternationalCentre for Eye Health, Institute of Ophthal-mology, 11–43 Bath Street, London EC1V 9EL,UK (tel: +44 (0)20 7608 6910; fax: +44 (0)207250 3207; email: [email protected];web site: www.jceh.co.uk). Annual subscrip-tion (4 issues) UK£25/US$40. Free to workersin developing countries.
International Centre for EyeHealthThe International Centre for Eye Health haspublished a new edition of the Standard List ofMedicines, Equipment, Instruments and OpticalSupplies (2001) for eye care services indeveloping countries. It is compiled by theTask Force of the International Agency for thePrevention of Blindness. Further details: SueStevens, International Centre for Eye Health,11–43 Bath Street, London EC1V 9EL, UK (tel:+44 (0)20 7608 6910; email:[email protected]).
Second SightSecond Sight, a UK based charity whose aimsare to eliminate the backlog of cataract blindin India by the year 2020 and to establishstrong links between Indian and British oph-thalmologists, is regularly sending volunteersurgeons to India. Details can be found at thecharity web site (www.secondsight.org.uk) orby contacting Dr Lucy Mathen([email protected]).
SPecific Eye ConditionS (SPECS)SPecific Eye ConditionS (SPECS) is a not forprofit organisation which acts as an umbrellaorganisation for support groups of any condi-tions or syndrome with an integral eye disor-der. SPECS represents over fifty differentorganisations related to eye disorders rangingfrom conditions that are relatively common tovery rare syndromes. We also include groupswho offer support of a more general nature tovisually impaired and blind people. Supportgroups meet regularly in the Boardroom atMoorfields Eye Hospital to offer support toeach other, share experiences and explore newways of working together. The web sitewww.eyeconditions.org.uk acts as a portalgiving direct access to support groups ownsites. The SPECS web page is a valuableresource for professionals and may also be ofinterest to people with a visual impairment orwho are blind. For further details aboutSPECS contact: Kay Parkinson, SPECS Devel-opment Officer (tel: +44 (0)1803 524238;email: [email protected];web site: ww-w.eyeconditions.org.uk).
16th Annual Meeting of GermanOphthalmic SurgeonsThe 16th Annual Meeting of German Oph-thalmic Surgeons will be held 8–11 May 2003in Nürnberg, Germany, Messezentrum. Or-ganised by the Professional Association ofGerman Ophthalmologists Ophthalmic Sur-gery Group the conference will cover cataractsurgery, refractive surgery, glaucoma surgery,vitreoretinal surgery, corneal surgery, eye sur-gery in developing countries, and orbita,
lacrimal and lid surgery. Further details: MCNMedisinische Congress organisation Nürn-berg AG, Zerzabelshofstr 29, 90478 Nürnberg,Germany (tel:+49 911 3931621; fax: +49 9113931620; email: [email protected]; web site:www.doc-nuernberg.de).
3rd British Oculoplastic SurgerySociety MeetingThe 3rd British Oculoplastic Surgery SocietyMeeting will be held 18–19 May 2003 inBirmingham, UK. For further details pleasecontact the Secretary of the British Oculoplas-tic Surgery Society Jane Olver (tel: +44(0)121 424 5464; fax: +44 (0)121 424 4464;email: [email protected]; website: www.bopss.org).
13th Meeting of the EASD EyeComplication Study GroupThe 13th Meeting of the EASD Eye Complica-tion Study Group will be held on the 23–25May 2003, in Prague, Czech Republic. The sci-entific programme includes keynote lecturesfrom Professor John H Fuller (UK) on Theepidemiology of diabetic retinopathy; Dr PMartin van Hagen (The Netherlands) onGrowth factors and diabetic retinopathy; Pro-fessor Terezie Pelikanova (Czech Republic) onPathophysiology of diabetic microvascularcomplications; Dr Tomas Sosna (Czech Re-public) on Risk and protective factors ofdiabetic retinopathy.
Three travel grants of €1000 each, spon-sored by GlaxoSmithKline for young scien-tists (under 35 years at the time of the meet-ing). Applications should be made with thesubmission of abstracts. The deadline forabstracts is 14 February 2003.
Further details: Ortopedicke Centrum,s.r.o., Strekovské nabrezi 51, 400 03 Usti nadLabem, Czech Republic (tel: +420 47 5216588; fax: +420 47 533 40 77; email:[email protected]; web site:www.ortopedicke-centrum.cz).
Detachment Course withinternational faculty on: Retinaland Vitreous Surgery with CasePresentations preceding theAnnual Meeting of IranianSociety of OphthalmologyThe detachment course with internationalfaculty on: Retinal and Vitreous Surgery withCase Presentations preceding Annual Meetingof Iranian Society of Ophthalmology will beheld on 29–30 November 2003 and 1–4December 2003 respectively, at the RaziConference Center, Hemmat Hyw, Tehran,Iran. Further details: Scientific programme:Prof Ingrid Kreissig, University of Tuebingen,Schleichstr. 12, Breuningerbau, 72076 Tuebin-gen, Germany (tel: +49 7071 295209;email:[email protected]). Local organisation: Dr ArmanMasheyekhi, Dr Siamak Moradian, Dept ofOphthalmology, Labbanfinejad MedicalCenter, Pasdaran Ave, Boostan 9, Tehran,16666, Iran (fax: +98 21 254 9039; email:[email protected]).
PostScript 377
www.bjophthalmol.com
on April 17, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.87.3.367 on 1 M
arch 2003. Dow
nloaded from