1228.2.full.pdf - british journal of ophthalmology
TRANSCRIPT

Treatment of biopsy provedconjunctival intraepithelialneoplasia with topical interferonalfa-2bConjunctival intraepithelial neoplasia (CIN)is the most common conjunctival malignancyin the United States. It occurs in exposedareas of the bulbar conjunctiva with frequentinvolvement of the adjacent corneal epithe-lium. Recent studies1 have noted a recurrencerate of about 50% when there is pathologicalevidence of residual tumour in the surgicalmargin and a 5–33% recurrence rate withclear margins.2 We describe two cases ofprimary CIN successfully treated with topicalINFa-2b. This chart review was conductedwith a waiver from the Ochsner ClinicFoundation’s institutional review board, andconforms to HIPPA regulations.
Patient 1A 65 year old retired welder was referred forfurther treatment of a partially resected CIN1 month earlier. The patient had a longhistory of ultraviolet light exposure, multipleskin cancers of the face and hands, andtobacco use. He complained of redness andforeign body sensation in the right eye.Examination revealed a best corrected visualacuity of 20/25 in both eyes. The left eyeexamination was unremarkable. Slit lampexamination of the right eye showed anelevated white corneal and conjunctival plaqueextending 90 degrees along the limbus (fig 1A).The referring physician had performed a biopsyof the central portion of the lesion which, uponpathological examination, was consistent withseverely dysplastic conjunctival intraepithelial
neoplasia with chronic subconjunctival inflam-mation, suggestive but not diagnostic ofsquamous cell carcinoma. After punctual plugswere placed, treatment with INFa-2b (1millionunits/ml) four times a day was initiated. Thelesion regressed completely after 44 days oftreatment (fig 1B). The interferon drops werediscontinued after 70 days. No recurrenceshave been seen after 6 months of follow up.
Patient 2A 73 year old white male was referred for anasymptomatic left corneal/conjunctival mass.There was no history of skin cancer, but therewas a long history of sun exposure. The bestcorrected visual acuity was 20/50 in botheyes. Slit lamp examination showed anelevated, gelatinous conjunctival/corneallesion with feeder vessels extending 150degrees along the limbus (fig 2A). A biopsyrevealed moderate to severe dysplasia. Thepatient was treated with INFa-2b (1 millionunits/ml) four times a day after placement ofupper and lower lid punctal plugs. The lesionresolved after 84 days (fig 2B). No recurrencewas been observed after 3 months of treat-ment.Traditional therapy for CIN has involved
wide surgical excisions with adjunctivecryotherapy, b radiation, mitomycin C, and5-fluorouracil. All of these treatments maycause ocular surface inflammation, limbalstem cell deficiency, and epitheliopathy.Combination therapy of intralesional/subcon-junctival injections and topical application ofinterferon effectively treats CIN.3 However,perilesional interferon has systemic sideeffects that include transient fevers andmyalgias; therefore, topical therapy is pre-ferred.4 5 While presumptive treatment of CINwith topical IFNa-2b has demonstrated goodresults, to our knowledge there is only onecase series of regression of biopsy proved
primary and recurrent CIN with treatmentwith IFNa2b.4 5
Here we report treatment of CIN usingINFa-2b that was extremely well toleratedand had minimal side effects. At approxi-mately $US300 per treatment, INFa-2b coststhree and two times more than 5-fluorouraciland mitomycin C, respectively. However, theenhanced safety and reduced side effectsshould offset the additional expense. Inconclusion, topical INFa-2b offers an effec-tive alternative for the treatment of primaryCIN. Larger population studies with longerfollow up would better assess the risk of sideeffects or recurrence.
S Esquenazi, C L Fry, E HolleyDepartment of Ophthalmology, Louisiana State
University Health Sciences Center,New Orleans, LA, USA
S Esquenazi, C L Fry, E HolleyDepartment of Ophthalmology, Ochsner Clinic
Foundation, New Orleans, LA, USA
Correspondence to: Salomon Esquenazi, MD,Department of Ophthalmology, Louisiana State
University Health Sciences Center, 2020 GravierStreet, Suite B, New Orleans, LA 70112, USA;
doi: 10.1136/bjo.2004.063339
References
1 Tabin G, Levin S, Snibson G, et al. Laterecurrences and the necessity of long term follow-up in corneal and conjunctival intraepithelialneoplasia. Ophthalmology 1997;104:485–92.
2 Erie JC, Campbell RJ, Liesegang TJ. Conjunctivaland corneal intraepithelial and invasiveneoplasia. Ophthalmology 1986;93:176–83.
3 Vann RR, Karp CL. Perilesional and topicalinterferon alfa-2b for conjunctival and cornealneoplasia. Ophthalmology 1999;106:91–7.
4 Schecter BA, Schrier A, Nagler RS, et al.Regression of presumed primary conjunctival andcorneal intraepithelial neoplasia with topicalinterferon alpha-2b. Cornea 2002;21:6–11.
5 Karp CL, Moore JK, Rosa RH. Treatment ofconjunctival and corneal intraepithelial neoplasiawith topical interferon a-2b. Ophthalmology2001;108:1093–8.
Henoch-Schonlein purpura withkeratitis and granulomatousanterior uveitisHenoch-Schonlein purpura (HSP) is a vascu-litis with IgA dominant immune complexes.1
The small vessel vasculitis is characterised byinflammation and necrosis. We report a caseof granulomatous HSP nephritis (HSPN) inassociation with keratitis and bilateral ante-rior granulomatous uveitis.
Case reportA 42 year old man presented to the casualtydepartment with acute polyarthropathy, pur-pura, and nephritic syndrome. The urinalysisdemonstrated 3+ blood and protein, bloodpressure was 152/96, serum creatinine was130 mmol/l, complement C3 titre was 0.78 g/l(normal 0.88–1.82), and immunoglobulinIgA titre was 4.6 g/litre (normal 0.80–2.80).
Figure 1 Patient 1. (A) Clinical appearance ofconjunctival squamous cell carcinoma beforetreatment with INFa-2b. (B) Regression ofconjunctival squamous cell carcinoma 70 daysafter starting treatment with INFa-2b.
Figure 2 Patient 2. (A) Clinical appearance ofCIN before treatment. (B) Complete regressionof CIN with topical INFa-2b 84 days aftertreatment.
LETTERS
PostScript . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accepted for publication 12 February 2005
Br J Ophthalmol 2005;89:1221–1229 1221
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

He underwent a left native kidney needlebiopsy. Light microscopy demonstratedmesangial proliferative glomerulonephritiswith no signs of interstitial nephritis. Therewas prominent vasculitis with a granuloma-tous response and fibrinoid necrosis (fig 1),mainly affecting the glomerular arterioles.Immunofluorescence studies demonstrated apredominantly granular staining for IgA andC3. Electron microscopy of the glomerulusdemonstrated prominent endocapillary cellu-larity and neutrophil populations, with anumber of subepithelial immune complexes.The clinical and immunopathological find-
ings were consistent with HSPN. His condi-tion responded to oral prednisolone (1 mg/kg),and the laboratory parameters normalisedwithin a 5 month period. The steroid therapywas discontinued and the patient remainedsystemically well with normal renal function.One month after remission of the HSPN, he
attended the ophthalmic casualty departmentwith a painful right eye. He was treated for apunctate keratitis and corneal epithelial ero-sion with topical antibiotics and ocularlubricants. This developed into an epithelialdefect, but soon resolved. Corneal sensationwas intact. One month later, he representedwith blurred vision in the right eye.Examination of the left eye was normal.Vision was 6/24, with severe scleral hyper-aemia, corneal oedema, mutton-fat keraticprecipitates, fibrinous anterior chamber reac-tion, posterior synechiae, and 2+ anteriorvitreal cells. Intraocular pressure was32 mmHg and fundal examination wasunremarkable.Routine blood tests and a vasculitis screen,
including antinuclear antibodies, antineutro-phil cytoplasmic antibody (ANCA), rheuma-toid factor, viral serology, autoantibody titres,antistreptolysin O titre, VDRL, and serumangiotensin converting enzyme levels were allnormal. The erythrocyte sedimentation rate,C reactive protein, chest x ray, complementtitre, urinalysis, and renal function werenormal.The granulomatous anterior uveitis and
trabeculitis were treated with dexamethasone1% eye drops, cyclopentolate 1% eye drops,and oral acetozolamide. After 1 week, hedeveloped bilateral granulomatous anterioruveitis and was treated with topical steroids.After 2 months, the uveitis resolved comple-tely and the intraocular pressure normalised.He reported no recurrence of HSP symptomsduring this period.
CommentThe relation between idiopathic acute inter-stitial nephritis and uveitis is well establishedin the literature.2 There is only a single reportof ocular inflammatory disease associatedwith classic HSP.3 Our patient fulfilled theAmerican College of Rheumatology diagnos-tic criteria for HSP4; however, the histopatho-logical features demonstrated an unusualtype of HSPN.The differential diagnosis in this case
included sarcoidosis, tubulointerstitialnephritis syndrome, ANCA associated granu-lomatous nephritis, post-streptococcalnephritis, herpetic infections, syphilis, tuber-culosis, and Wegener’s granulomatosis. Theclinical and immunopathological findings inour patient were consistent with HSPN. Thelaboratory investigations excluded the otherpotential aetiologies.There are anatomic and haemodynamic
relations between uveal and renal vascula-ture, which are important determinants forthe site of immune complex deposition.Plasma passes through at high hydrostaticpressure and in large volumes through boththe capillaries in the renal glomerulus anduveal tissue, and both vessels containendothelial fenestrations.5
In classic HSP, there is alternative comple-ment pathway activation with elevated levelsof abnormally glycosylated serum IgA1. Thisis not sufficiently cleared by the liver andleads to increased levels of IgA1 containingcirculating immune complexes.6 The immunecomplexes may reach the eye in the circula-tion and then deposit in the uveal tissue. Thesites of immune complex deposition areocular resident cells—namely, vascularendothelial cells, pigmented epithelial cells,and corneal endothelial cells.7 There isexpression of adhesion molecules on theocular resident cells, which allows leucocytesto migrate to the uveal tissue and cornea andcause tissue injury—namely, uveitis andkeratitis.In our patient, the finding of a granulo-
matous vasculitis is highly unusual.Activation of MHC restricted autoreactiveCD4+ T cells in renal and uveal tissue maylead to strong macrophage responses, withthe formation of granulomas. However, over-lap syndromes with other forms of granulo-matous vasculitis may occur.8 This expressionof MHC class II markers on ocular residentcells has been observed in various experi-mental uveitides,9 10 and may explain thelater presentation of uveitis in this casefollowing remission of the HSPN.We report an unusual case of a granulo-
matous HSPN in association with bilateralgranulomatous anterior uveitis and keratitis.The inflammatory eye disease may be insi-dious in onset with an aggressive clinicalcourse.
AcknowledgementsWe thank Dr George Lindrop for help in interpret-ing the renal biopsy.
M M K Muqit, M J Gallagher, M GavinTennent Institute of Ophthalmology, Gartnavel
General Hospital, UK
F RobertsDepartment of Pathology, University of Glasgow,
Western Infirmary, UK
A G JardineRenal Unit, Western Infirmary, Glasgow, UK
Correspondence to: Mahiul M K Muqit, TennentInstitute of Ophthalmology, Gartnavel General
Hopsital, 1053 Great Western Road, Glasgow G120YN, UK; [email protected]
doi: 10.1136/bjo.2004.064519
References
1 Matteson E. Henoch-Schonlein purpura. In:A History of idiopathic vasculitis. Rochester: MayoFoundation for Medical Education and Research,1999:29.
2 Steinman TI, Silva P. Acute interstitial nephritisand iritis. Renal-ocular syndrome. Am J Med1984;77:189–91.
3 Yamabe H, Ozawa K, Fukushi, et al. IgAnephropathy and Henoch-Schonlein nephritis withanterior uveitis. Nephron 1988;50:368–70.
4 Mills JA, Michel BA, Bloch DA, et al. TheAmerican College of Rheumatology 1990 criteriafor the classification of Henoch-Schonlein purpuraArthritis Rheum 1990;33:1114–21.
5 Kaplan HJ. Immunologic insights into the eye anduveitis. Uveitis: pathophysiology and therapy.New York: Thieme Medical Publishers, 1986.
6 Saulsbury FT. Henoch-Schonlein purpura. CurrOpin Rheumatol 2001;13:35–40.
7 Chan C-C, Li Q. Immunopathology of uveitis.Br J Ophthalmol 1998;82:91–6.
8 Jones ND. Sarcoidosis and uveitis. OphthalmolClin North Am 2002;15:319–26.
9 Kim MK, Chan C-C, Nussenblatt RB, et al.Pharmacologic effects on the expression of class IIhistocompatibility antigen in experimentalendotoxin-induced uveitis. Clin ImmunolImmunopathol 1987;45:70–7.
10 Chan C-C, Hikita N, Dastgheib K, et al.Experimental melanin-protein induced uveitis inthe Lewis rat:immunopathological process.Ophthalmology 1994;101:1275–80.
Lymphoepithelioma-likecarcinoma of the eyelid: a reportof two casesLymphoepithelioma-like carcinoma (LELC)of the skin is a rare malignant epithelialneoplasm, which resembles histologically thenasopharyngeal neoplasm of the samename.1 2 Similar tumours have been reportedat a variety of sites including salivary gland,tonsil, thymus, stomach, and uterus. Thoseinvolving the skin usually present as apapulonodular lesion on the head or neck ofpatients above 50 years of age. Only one caseoriginating in the eyelid has been previouslydescribed.3 We describe a further two casesand discuss the differential diagnosis.
Case 1A 79 year old man presented with a fusiformswelling occupying the medial half of hisright lower lid (fig 1A). This had developed8 months previously and was graduallyincreasing in size. An ectropion repair hadbeen performed on this lid 7 years beforepresentation. The patient underwent excisionof the lesion with reconstruction of the lidusing a pedicle flap. The excised lesion wassubmitted for histopathological examination.The patient had a medical history of
carcinoma in situ of the right vocal cord,which was treated with laser excision in 2000with no recurrence on follow up.
Case 2A 67 year old man presented with a sub-cutaneous cystic lesion at the margin of thelower eyelid. This had been present for8 months and was gradually increasing insize. A clinical diagnosis of sebaceous cyst
Figure 1 Glomerular arteriole showing avasculitis with fibrinoid necrosis of the vesselwall (arrow) and swelling of the endothelialcells (E). Surrounding the vessel there isgranulomatous inflammation (G) (haematoxylinand eosin,6400).
Accepted for publication 2 March 2005
1222 PostScript
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

was considered. The lesion was excised andsubmitted for histopathological examination.
Histopathological examinationHistopathological examination of bothlesions showed a relatively well circum-scribed lesion situated within the dermiswith no connection with the overlyingepidermis (fig 1B). The lesions consisted ofclusters of malignant epithelial cells withvesicular nuclei and large nucleoli (fig 1C).Foci suggestive of hair follicle differentiationwere identified in case 2 (fig 1D). Theseclusters of malignant epithelial cells weresurrounded by a mixed reactive inflammatorycell infiltrate composed predominantly oflymphocytes and plasma cells. Eosinophilsand polymorphs were also identified in theinflammatory infiltrate from case 2.In both cases immunohistochemical stain-
ing showed strong positivity for cytokeratinsand epithelial membrane antigen in theislands of malignant epithelial cells.Immunohistochemical staining for Epstein-Barr virus was negative.
CommentLELC, first described in 1988 by Swanson etal,1 is a rare cutaneous neoplasm that usuallypresents as a cutaneous nodule of shortduration covered by an intact epidermis.The clinical diagnosis is often non-specificsuch as ‘‘lump’’ or ‘‘cyst.’’ In contrast, themicroscopic appearances, as described above,are distinctive.The histogenesis of LELC is uncertain.
Most authors support an adnexal origin.1 4
This is suggested by the tumour locationwithin the dermis and the absence of a
connection with the overlying epidermis.This is further supported by the identificationof areas of adnexal differentiation in sometumours, as in case 2.4 Conversely, casesdisplaying dysplasia in the overlying epider-mis have been reported and this is suggestiveof epidermal origin for LELC.5
Metastatic disease within the eyelid fromunderlying primary nasopharyngeal carci-noma (NPC) must be excluded before diag-nosing LELC of the skin. The first patient hada history of carcinoma in situ of the larynx.The histology of this was reviewed andconfirmed as squamous cell carcinoma insitu without evidence of invasion and therehas been no evidence of recurrence on regularfollow up. Furthermore, the surface epithelialcells of the laryngeal lesion were morpholo-gically unlike the clusters of malignantepithelial cells seen in the LELC of the eyelid.Both patients also underwent endoscopy ofthe nasopharynx and no tumour or otherabnormalities were identified.NPC has a strong association with Epstein-
Barr virus (EBV) infection. LELC at othersites has rarely been shown to have thisassociation. Similar to those previouslyreported in the skin, EBV was not identifiedin either of our cases.6 Other differentialdiagnoses include anaplastic lymphoma,poorly differentiated squamous cell carci-noma, sebaceous carcinoma, melanoma,Merkel cell tumour, and cutaneous lympha-denoma.7 These can usually be discriminatedfrom LELC with immunohistochemistry.In the small number of cases reported so
far, LELC appears to be of low malignantpotential with a tendency towards localrecurrence but a very low metastatic poten-tial.1 2 4 5 Both cases presented have shown no
sign of recurrence to date. LELC is a rare butdistinctive malignant neoplasm that shouldbe considered in the differential diagnosis ofcyst like or nodular lesions of the eyelid.
W Ho, A Taylor, E KempTennent Institute of Ophthalmology, Gartnavel
General Hospital, Glasgow, UK
F RobertsUniversity Department of Pathology, Western
Infirmary, Glasgow, UK
Correspondence to: Dr F Roberts, UniversityDepartment of Pathology, Western Infirmary,
Glasgow, UK;[email protected]
doi: 10.1136/bjo.2005.066589
References
1 Swanson SA, Cooper PH, Mills SE, et al.Lymphoepithelioma-like carcinoma of the skin.Mod Pathol 1988;1:359–65.
2 Carr KA, Bulengo S, Weiss LM, et al.Lymphoepithelioma-like carcinoma of the skin. Acase with immunophenotypic analysis and in situhybridization for Epstein-Barr viral genome.Am J Surg Pathol 1992;16:909–13.
3 Maruyama M, Miyauchi S, Ohtsuka H, et al.Lymphoepithelioma-like carcinoma originating onthe eyelid. J Dermatol 1995;22:218–22.
4 Wick MR, Swanson PE, LeBoit PE, et al.Lymphoepithelioma-like carcinoma of the skinwith adnexal differentiation. J Cut Pathol1990;18:93–102.
5 Shek WWH, Leung EYF, Luk ISC, et al.Lymphoepithelioma-like carcinoma of the skin.Am J Dermatopathol 1996;18:637–44.
6 Weiss LM, Movahed LA, Butler AE, et al. Analysisof lymphoepithelioma and lymphoepithelioma-like carcinomas for Epstein-Barr viral genomes byin situ hybridization. Am J Surg Pathol1989;13:625–31.
7 Requena L, Yus ES, Jimenez E, et al.Lymphoepithelioma-like carcinoma of the skin: alight-microscopic and immunohistochemicalstudy. J Cut Pathol 1994;21:541–8.
Nylon paper: an alternative tocellulose acetate paper for use inconjunctival impression cytologyConjunctival imprint cytology (CIC) offersvaluable clues to the diagnosis and study ofthe pathogenesis of conjunctival disorders.1–3
The technique involves the use of a mem-brane filter paper to pick up a layer of cellsfrom the conjunctival surface.This study was conducted to evaluate the
results of CIC using a nylon filter papercompared to routinely used cellulose acetatepaper. It involved 20 normal asymptomaticeyes of 10 participants. The participants hadno ocular complaints and they were evalu-ated to rule out any conjunctival disease.The procedure was explained to the parti-
cipants and their consent was given.CIC was done to assess the normal
conjunctival cytology using Ultipor (nylon6,6) and sartorius-type 111 (cellulose acetatepaper).The physical properties such as pore size
and thickness of the two papers werematched.
TechniqueCellulose acetate and nylon membrane filterswere cut into small triangles and squaresrespectively to make their identification easyafter staining. The conjunctiva was anaes-thetised by topical 4% xylocaine. The filter
Figure 1 (A) Clinical photograph of case 1 showing a smooth surfaced swelling at the medialaspect of the right lower eyelid. (B) Histological section from case 1 showing a relatively wellcircumscribed nodule of tumour situated within the superficial and deep dermis. There is cleardemarcation from the overlying epidermis (arrows) (haematoxylin and eosin,610). (C) Histologicalsection from case 1 showing a cluster of large epithelial cells (e), with an abnormal mitotic figure(arrow), surrounded by inflammatory cells (i) (haematoxylin and eosin,6200). (D) Histologicalsection from case 2 showing focal squamous eddies (arrows), reminiscent of an inverted follicularkeratosis, a tumour of the follicular infundibulum (haematoxylin and eosin,6100).
Accepted for publication 22 February 2005
PostScript 1223
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

paper was applied to the bulbar conjunctivawith blunt forceps. Gentle pressure wasapplied for 3–5 seconds and the paper wasremoved in a peeling motion. It was fixedthereafter in 95% ethanol and stained witheither haematoxylin and eosin (H&E) orperiodic acid Schiff (PAS) and haematoxylinstains.The filter papers after staining were cleared
in acetone and xylene, mounted in DPX andviewed under the light microscope. Themorphology of epithelial cells in H&E stainand number of goblet cells in PAS stain werenoted.
ResultsThe participants involved in this study werein age group 22–37 years. A few initialslides were discarded because of overstain-ing. The time required to stain the filterpapers compared to any other fixed tissue is
lessened, and staining time is reduced to halfwith nylon paper compared with celluloseacetate paper.Average time required for staining nylon
and cellulose acetate paper was 20 minutesand 35 minutes, respectively, for PAS stain-ing and with H&E stain it was 5 minutes and10 minutes, respectively.The specimens revealed sheets of small
round epithelial cells in H&E stained nylonpaper (fig 1A) and cellulose acetate paper(fig 1B).Additional plump, oval, deeply pink PAS
positive goblet cells amidst PAS negativecohesive sheet of epithelial cells were seenin schiff stained specimens on nylon paper.(fig 2).The cell layer varies from one to several
cells thick with occasional gaps where nocells adhere to the membrane filter. Celluloseacetate paper revealed a single layered sheetbut the Ultipor showed that there weremultiple layers in most places.Occasionally the cells were not picked up or
they were clumped so as to be visible aslayers. This was seen equally with both thefilter papers.Cells were collected on nylon paper even in
presence of lacrimation during the procedure.The cell morphology of specimens collectedon either of the filter papers was comparable.
CommentCIC has been in use, as diagnostic tool since1978, when Egbert first demonstrated itssuccessful use with absorbent filter paper.4
Before this Thatcher used a plastic device to
collect the epithelia.5 Since then membranefilters like cellulose acetate have been widelyused for this technique.6 7
The filtration membrane is a thin, poly-meric film made up of microscopic pores.They can be composed of variety of naturaland synthetic materials like cellulose acetateand cellulose nitrate in the former category,and PTFE, PVDF, glass fibres, and nylon inlatter.In this study nylon and cellulose acetate
were used for comparison of the results.The nylon paper is more compatible with
the organic solvents used in staining proce-dures. The adsorption is better with nylonthen the cellulose acetate paper. Also there isa cost difference between the two, withcellulose acetate paper costing three timesthat of nylon.The cytological features of epithelial as well
as goblet cells were studied. The goblet cellsare identified conclusively by the PAS posi-tive cytoplasm or by their eccentrically placednuclei and plump shape and large size. Theepithelial cells are small and round witheosinophilic cytoplasm. The nuclei are largeand basophilic.Added benefit of nylon over cellulose
acetate are:
(1) Cost effective
(2) Less staining time
(3) Ability to collect cell even if lacrimationwets the paper
(4) Comparable morphological results tocellulose acetate
(5) Compatible with variety of solventshence more stable
(6) Deeper layers also picked, hence detailedevaluation of biopsy.
AcknowledgementsThe authors acknowledge the assistance of DrKrishna Mohan, Birla Institute of Science andTechnology, for providing the filter papers.
M K B Meena, A KhutetaDepartment of Ophthalmology, SMS Hospital,
Jaipur, India
H SaxenaDepartment of Pathology, SMS Hospital, Jaipur, India
Correspondence to: Dr Monisha K Brijlal Meena,Department of Ophthalmology, SMS Hospital, Jaipur,
India, [email protected]
doi: 10.1136/bjo.2005.067991
References
1 Thygeson P. The cytology of conjunctivalexudates. Am J Ophthalmol 1946;29:1499.
2 Duszynski L. Cytology of the conjunctival sac.Amer J Ophthalmol 1954;37:576.
3 Norn MS. Cytology of the conjunctival fluid. ActaOphthalmol 1960;59(suppl):11.
4 Egbert PR, Lauber S, Maurice DM. A simpleconjunctival biopsy. Am J Ophthalmology1977;84:798–801.
5 Thatcher RW, Darougar S, Jones BR. Conjunctivalimpression cytology. Arch Ophthalmol1977;95:678–81.
6 Gadkari SS, Adrianwala SD, Prayag AS, et al.Conjunctival impression cytology—a study ofnormal conjunctiva. J Postgrad Med1992;38:21–3.
7 Nelson JD, Havener VR, Cameron JD. Celluloseacetate impressions of the ocular surface. Dry eyestates. Arch Ophthalmo1 1983;101:1869–72.
Figure 1 (A) Haematoxylin and eosin stainednylon paper at 406magnification showingsheets of epithelial cells. (B) Haematoxylin andeosin stained cellulose acetate paper at 406magnification revealing sheets of small roundepithelial cells.
Figure 2 Periodic acid Schiff (PAS) stainednylon paper at 106and 406magnificationshowing plump, oval, deeply pink PAS positivegoblet cells amidst PAS negative cohesive sheetof epithelial cells.
Accepted for publication 5 February 2005
1224 PostScript
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
‘‘C-scan’’ ultrasound imaging ofoptic nerve extension ofretinoblastomaThree dimensional ultrasound based coronal‘‘C-scan’’ imaging technique was used todemonstrate optic nerve extension of retino-blastoma. With a clinical diagnosis of retino-blastoma based on clinical evaluation,ultrasound, and computed radiographictomography, this patient was treated byprimary enucleation. Subsequent histopatho-logical evaluation of the enucleated globerevealed three risk factors for metastaticretinoblastoma (including optic nerve exten-sion).1 2 Both systemic chemotherapy andorbital radiation therapy were employed.3
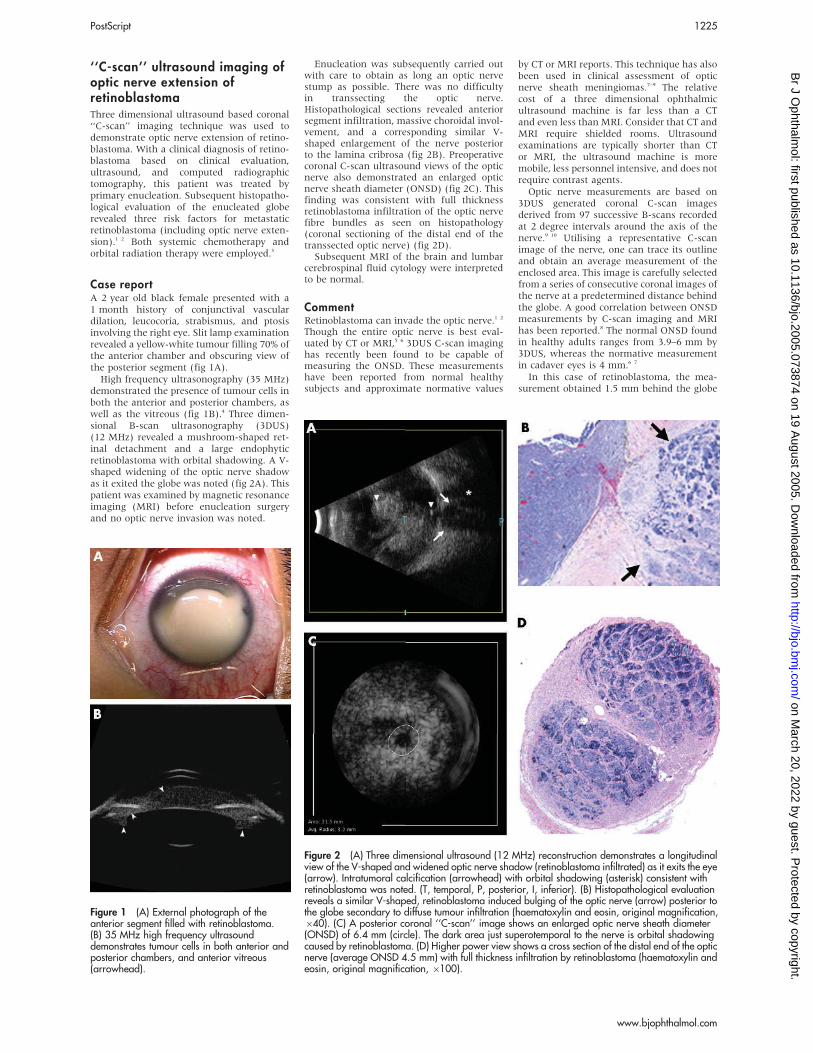
Case reportA 2 year old black female presented with a1 month history of conjunctival vasculardilation, leucocoria, strabismus, and ptosisinvolving the right eye. Slit lamp examinationrevealed a yellow-white tumour filling 70% ofthe anterior chamber and obscuring view ofthe posterior segment (fig 1A).High frequency ultrasonography (35 MHz)
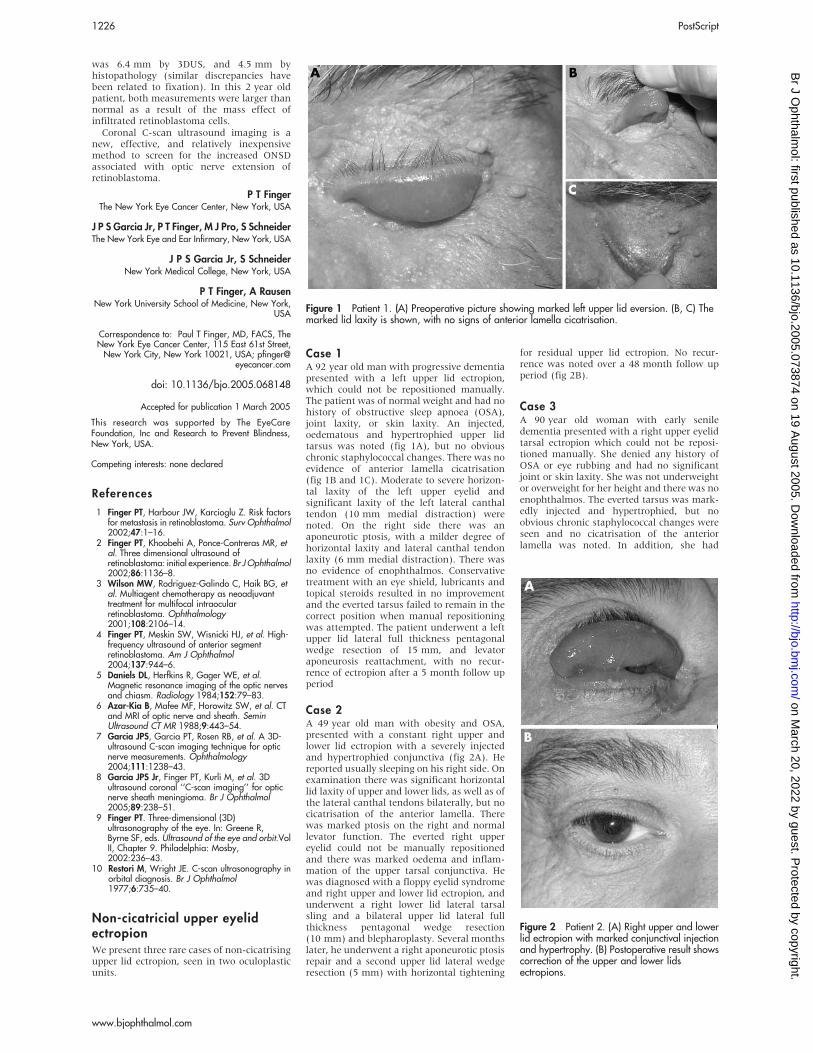
demonstrated the presence of tumour cells inboth the anterior and posterior chambers, aswell as the vitreous (fig 1B).4 Three dimen-sional B-scan ultrasonography (3DUS)(12 MHz) revealed a mushroom-shaped ret-inal detachment and a large endophyticretinoblastoma with orbital shadowing. A V-shaped widening of the optic nerve shadowas it exited the globe was noted (fig 2A). Thispatient was examined by magnetic resonanceimaging (MRI) before enucleation surgeryand no optic nerve invasion was noted.
Enucleation was subsequently carried outwith care to obtain as long an optic nervestump as possible. There was no difficultyin transsecting the optic nerve.Histopathological sections revealed anteriorsegment infiltration, massive choroidal invol-vement, and a corresponding similar V-shaped enlargement of the nerve posteriorto the lamina cribrosa (fig 2B). Preoperativecoronal C-scan ultrasound views of the opticnerve also demonstrated an enlarged opticnerve sheath diameter (ONSD) (fig 2C). Thisfinding was consistent with full thicknessretinoblastoma infiltration of the optic nervefibre bundles as seen on histopathology(coronal sectioning of the distal end of thetranssected optic nerve) (fig 2D).Subsequent MRI of the brain and lumbar
cerebrospinal fluid cytology were interpretedto be normal.
CommentRetinoblastoma can invade the optic nerve.1 2
Though the entire optic nerve is best eval-uated by CT or MRI,5 6 3DUS C-scan imaginghas recently been found to be capable ofmeasuring the ONSD. These measurementshave been reported from normal healthysubjects and approximate normative values
by CT or MRI reports. This technique has alsobeen used in clinical assessment of opticnerve sheath meningiomas.7–9 The relativecost of a three dimensional ophthalmicultrasound machine is far less than a CTand even less than MRI. Consider that CT andMRI require shielded rooms. Ultrasoundexaminations are typically shorter than CTor MRI, the ultrasound machine is moremobile, less personnel intensive, and does notrequire contrast agents.Optic nerve measurements are based on
3DUS generated coronal C-scan imagesderived from 97 successive B-scans recordedat 2 degree intervals around the axis of thenerve.9 10 Utilising a representative C-scanimage of the nerve, one can trace its outlineand obtain an average measurement of theenclosed area. This image is carefully selectedfrom a series of consecutive coronal images ofthe nerve at a predetermined distance behindthe globe. A good correlation between ONSDmeasurements by C-scan imaging and MRIhas been reported.8 The normal ONSD foundin healthy adults ranges from 3.9–6 mm by3DUS, whereas the normative measurementin cadaver eyes is 4 mm.6 7
In this case of retinoblastoma, the mea-surement obtained 1.5 mm behind the globe
Figure 1 (A) External photograph of theanterior segment filled with retinoblastoma.(B) 35 MHz high frequency ultrasounddemonstrates tumour cells in both anterior andposterior chambers, and anterior vitreous(arrowhead).
Figure 2 (A) Three dimensional ultrasound (12 MHz) reconstruction demonstrates a longitudinalview of the V-shaped and widened optic nerve shadow (retinoblastoma infiltrated) as it exits the eye(arrow). Intratumoral calcification (arrowhead) with orbital shadowing (asterisk) consistent withretinoblastoma was noted. (T, temporal, P, posterior, I, inferior). (B) Histopathological evaluationreveals a similar V-shaped, retinoblastoma induced bulging of the optic nerve (arrow) posterior tothe globe secondary to diffuse tumour infiltration (haematoxylin and eosin, original magnification,640). (C) A posterior coronal ‘‘C-scan’’ image shows an enlarged optic nerve sheath diameter(ONSD) of 6.4 mm (circle). The dark area just superotemporal to the nerve is orbital shadowingcaused by retinoblastoma. (D) Higher power view shows a cross section of the distal end of the opticnerve (average ONSD 4.5 mm) with full thickness infiltration by retinoblastoma (haematoxylin andeosin, original magnification, 6100).
PostScript 1225
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from
was 6.4 mm by 3DUS, and 4.5 mm byhistopathology (similar discrepancies havebeen related to fixation). In this 2 year oldpatient, both measurements were larger thannormal as a result of the mass effect ofinfiltrated retinoblastoma cells.Coronal C-scan ultrasound imaging is a
new, effective, and relatively inexpensivemethod to screen for the increased ONSDassociated with optic nerve extension ofretinoblastoma.
P T FingerThe New York Eye Cancer Center, New York, USA
J P S Garcia Jr, P T Finger, M J Pro, S SchneiderThe New York Eye and Ear Infirmary, New York, USA
J P S Garcia Jr, S SchneiderNew York Medical College, New York, USA
P T Finger, A RausenNew York University School of Medicine, New York,
USA
Correspondence to: Paul T Finger, MD, FACS, TheNew York Eye Cancer Center, 115 East 61st Street,New York City, New York 10021, USA; pfinger@
eyecancer.com
doi: 10.1136/bjo.2005.068148
References
1 Finger PT, Harbour JW, Karcioglu Z. Risk factorsfor metastasis in retinoblastoma. Surv Ophthalmol2002;47:1–16.
2 Finger PT, Khoobehi A, Ponce-Contreras MR, etal. Three dimensional ultrasound ofretinoblastoma: initial experience. Br JOphthalmol2002;86:1136–8.
3 Wilson MW, Rodriguez-Galindo C, Haik BG, etal. Multiagent chemotherapy as neoadjuvanttreatment for multifocal intraocularretinoblastoma. Ophthalmology2001;108:2106–14.
4 Finger PT, Meskin SW, Wisnicki HJ, et al. High-frequency ultrasound of anterior segmentretinoblastoma. Am J Ophthalmol2004;137:944–6.
5 Daniels DL, Herfkins R, Gager WE, et al.Magnetic resonance imaging of the optic nervesand chiasm. Radiology 1984;152:79–83.
6 Azar-Kia B, Mafee MF, Horowitz SW, et al. CTand MRI of optic nerve and sheath. SeminUltrasound CT MR 1988;9:443–54.
7 Garcia JPS, Garcia PT, Rosen RB, et al. A 3D-ultrasound C-scan imaging technique for opticnerve measurements. Ophthalmology2004;111:1238–43.
8 Garcia JPS Jr, Finger PT, Kurli M, et al. 3Dultrasound coronal ‘‘C-scan imaging’’ for opticnerve sheath meningioma. Br J Ophthalmol2005;89:238–51.
9 Finger PT. Three-dimensional (3D)ultrasonography of the eye. In: Greene R,Byrne SF, eds. Ultrasound of the eye and orbit.VolII, Chapter 9. Philadelphia: Mosby,2002:236–43.
10 Restori M, Wright JE. C-scan ultrasonography inorbital diagnosis. Br J Ophthalmol1977;6:735–40.
Non-cicatricial upper eyelidectropionWe present three rare cases of non-cicatrisingupper lid ectropion, seen in two oculoplasticunits.
Case 1A 92 year old man with progressive dementiapresented with a left upper lid ectropion,which could not be repositioned manually.The patient was of normal weight and had nohistory of obstructive sleep apnoea (OSA),joint laxity, or skin laxity. An injected,oedematous and hypertrophied upper lidtarsus was noted (fig 1A), but no obviouschronic staphylococcal changes. There was noevidence of anterior lamella cicatrisation(fig 1B and 1C). Moderate to severe horizon-tal laxity of the left upper eyelid andsignificant laxity of the left lateral canthaltendon (10 mm medial distraction) werenoted. On the right side there was anaponeurotic ptosis, with a milder degree ofhorizontal laxity and lateral canthal tendonlaxity (6 mm medial distraction). There wasno evidence of enophthalmos. Conservativetreatment with an eye shield, lubricants andtopical steroids resulted in no improvementand the everted tarsus failed to remain in thecorrect position when manual repositioningwas attempted. The patient underwent a leftupper lid lateral full thickness pentagonalwedge resection of 15 mm, and levatoraponeurosis reattachment, with no recur-rence of ectropion after a 5 month follow upperiod
Case 2A 49 year old man with obesity and OSA,presented with a constant right upper andlower lid ectropion with a severely injectedand hypertrophied conjunctiva (fig 2A). Hereported usually sleeping on his right side. Onexamination there was significant horizontallid laxity of upper and lower lids, as well as ofthe lateral canthal tendons bilaterally, but nocicatrisation of the anterior lamella. Therewas marked ptosis on the right and normallevator function. The everted right uppereyelid could not be manually repositionedand there was marked oedema and inflam-mation of the upper tarsal conjunctiva. Hewas diagnosed with a floppy eyelid syndromeand right upper and lower lid ectropion, andunderwent a right lower lid lateral tarsalsling and a bilateral upper lid lateral fullthickness pentagonal wedge resection(10 mm) and blepharoplasty. Several monthslater, he underwent a right aponeurotic ptosisrepair and a second upper lid lateral wedgeresection (5 mm) with horizontal tightening
for residual upper lid ectropion. No recur-rence was noted over a 48 month follow upperiod (fig 2B).
Case 3A 90 year old woman with early seniledementia presented with a right upper eyelidtarsal ectropion which could not be reposi-tioned manually. She denied any history ofOSA or eye rubbing and had no significantjoint or skin laxity. She was not underweightor overweight for her height and there was noenophthalmos. The everted tarsus was mark-edly injected and hypertrophied, but noobvious chronic staphylococcal changes wereseen and no cicatrisation of the anteriorlamella was noted. In addition, she had
Accepted for publication 1 March 2005
This research was supported by The EyeCareFoundation, Inc and Research to Prevent Blindness,New York, USA.
Competing interests: none declared
Figure 1 Patient 1. (A) Preoperative picture showing marked left upper lid eversion. (B, C) Themarked lid laxity is shown, with no signs of anterior lamella cicatrisation.
Figure 2 Patient 2. (A) Right upper and lowerlid ectropion with marked conjunctival injectionand hypertrophy. (B) Postoperative result showscorrection of the upper and lower lidsectropions.
1226 PostScript
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

bilateral medial lower lid ectropions withmoderate to severe horizontal lid laxity ofupper and lower lids, as well as the lateralcanthal tendons (10 mm medial distraction).The patient did not respond to conservativetreatment with lubricants and topical ster-oids, and she underwent right upper lidectropion repair with a lateral full thicknesspentagonal wedge excision (15 mm) andlevator aponeurosis reattachment. No recur-rence was noted after a 6 month follow upperiod.
CommentWe have described three patients with anunusual presentation of a non-cicatrisingconstant upper lid ectropion. Correcting theupper lid laxity with a full thickness penta-gonal wedge resection and horizontal tigh-tening1 resulted in a good outcome in allpatients.Upper lid ectropion is not common. In
newborns, it is usually temporary andresponds to conservative measures. Lesscommonly, it may results from shortage ofanterior lamella, as in blepharophimosissyndrome and congenital ichthyosis.2 Arecent report found mild degrees of upperlid eversion in a series of patients withmultiple endocrine neoplasia type 2B.3
Upper lid ectropion in adults usually resultsfrom pathologies affecting the anteriorlamella such as chronic sun damage, irradia-tion, chronic dermatitis, skin infections,ichthyosis, chemical burns, and previoussurgery.2 In patients with the floppy eyelidsyndrome the spontaneous upper lid eversionusually occurs during night sleep and is easilyrepositioned manually.4 5 In a recent report,Burkat and Lemke6 described 80 patientswith acquired lax eyelid syndrome who weretreated with the four eyelid tarsal stripperiosteal flap technique. Although allpatients had significant horizontal laxity,none of them had spontaneous upper lideversion. While spontaneous upper eyelideversion may occur in conditions such asfloppy eyelid syndrome or lax eyelid syn-drome which induce sufficient lid laxity,manual repositioning is generally possible.In all our patients the ectropion remainedconstant and could only be corrected surgi-cally. Only patient 2, who was the youngest,was diagnosed with the floppy eyelid syn-drome. The other two were older, had nosystemic signs of the floppy eyelid syndrome,and the eyelid changes appeared to be agerelated.We believe that the marked horizontal
laxity was the main causative factor causingupper lid ectropion in our cases, but poorlevator muscle function, dehiscence of theaponeurosis, and involutional tarsalchanges7 8 may further contribute to tarsalinstability and upper lid ectropion. Two of thepatients in our series had significant demen-tia, and frequent eye rubbing resulting inconjunctival forniceal oedema with tarsalconjunctival oedema and inflammation,may have been a factor in preventingrepositioning of the everted tarsus. In thecase of the patient with floppy eyelid syn-drome, traumatic irritation during sleep mayhave led to sufficient tarsal conjunctivaloedema and inflammation to prevent reposi-tioning of the eyelid.
I Leibovitch, G Davis, D SelvaOculoplastic and Orbital Unit, Department of
Ophthalmology, Royal Adelaide Hospital, Australia
J HsuanBristol Eye Hospital, Bristol, UK
D SelvaDepartments of Surgery and Medicine, University of
Adelaide, Australia
Correspondence to: Mr James Hsuan, Department ofOphthalmology, Walton Hospital, Rice Lane,
Liverpool, L9 1AE, UK; [email protected]
doi: 10.1136/bjo.2005.066720
References
1 Moore MB, Harrington J, McCulley JP. Floppyeyelid syndrome: management including surgery.Ophthalmology 1986;93:184–8.
2 Vallabhanath P, Carter SR. Ectropion andentropion. Curr Opin Ophthalmol2000;11:345–51.
3 Douglas G, Parker DG, Robinson BG, et al.External ophthalmic findings in multiple endocrineneoplasia type 2B. Clin Exp Ophthalmol2004;32:420–3.
4 Culbertson WW, Ostler HB. The floppy eyelidsyndrome. Am J Ophthalmol 1981;92:568–75.
5 McNab AA. Floppy eyelid syndrome andobstructive sleep apnea. Ophthal Plast ReconstrSurg 1997;13:98–114.
6 Burkat CN, Lemke BN. Acquired lax eyelidsyndrome: an unrecognized cause of thechronically irritated eye. Ophthal Plast ReconstSurg 2005;21:52–8.
7 Netland PA, Sugrue SP, Albert DM, et al.Histopathologic features of the floppy eyelidsyndrome. Involvement of tarsal elastin.Ophthalmology 1994;101:174–81.
8 Bashour M, Harvey J. Causes of involutionalectropion and entropion-age-related tarsalchanges are the key. Ophthal Plast Reconstr Surg2000;16:131–41.
Sub-Tenon’s block versus topicalanaesthesia for cataract surgeryWe read with great interest the article byRuschen et al comparing patient satisfactionduring cataract surgery with sub-Tenon’sblock (STB) versus topical anaesthesia(TOP).1 The authors concluded that in thesetting of day case cataract surgery, patientsreported significantly higher satisfactionscores with STB than TOP.We would like to raise two issues for
discussion. Firstly, the lower satisfactionscore in the TOP group may only reflect asuboptimal TOP that was given in the currentstudy and may not be generalisable to otherforms of TOP. In our experience, lignocainegel (lidocaine hydrochloride 2%, AstraZeneca,Sweden) produces significantly better anaes-thetic effects than local anaesthetic eye drops.Lignocaine gel has been previously shown tobe an effective2 3 and possibly a more super-ior4 5 anaesthetic agent in cataract surgery, aswell as giving better patient cooperation withless intraoperative supplement.5 To furtherevaluate the apparent lower satisfactionscores with TOP than STB, we would begrateful if the authors could provide thedetails of their TOP anaesthetic procedure—for example, how long before the actualsurgery were proxymetacaine and ametho-caine given and whether supplementaryanaesthetic eye drops were allowed duringthe surgery?Secondly, even though the median
satisfaction score in the TOP group was
significantly lower than that of the STBgroup, there was a much larger variation inthe TOP group (fig 1). This would imply somepatients were satisfied while some weredissatisfied. We certainly believe not allpatients can tolerate TOP and it would behighly desirable for cataract surgeons toidentify the latter group preoperatively.Were there any specific characteristics in thisgroup showing such dissatisfaction?Moreover, we noted that there were morefemales (12 out of 14 patients) in the TOPgroup, compared to the STB group (five out of14 patients). This difference was statisticallysignificant (p=0.018, Fisher’s exact test).We recognise that randomisation had beenimplemented in the present study and anysignificant differences in patients’ demo-graphics were beyond the control of theauthors. However, such difference mighthave impacted the satisfaction scores, as itis known that women have high rates ofphysical symptom reporting.6
None the less, we do commend the authors’work on this important topic. We agree withthe authors that sub-Tenon’s anaesthesia maybe a better choice in some patients undergoingcataract surgery. However, other forms oftopical anaesthesia may produce equally good,if not better, patient satisfaction especially inselected patients.
A C O Cheng, H K L Yuen, R F Lam, D S C LamDepartment of Ophthalmology and Visual Sciences,The Chinese University of Hong Kong, 3/F, HongKong Eye Hospital, 147K Argyle Street, Kowloon,
Hong Kong
Correspondence to: Dennis S C Lam, Department ofOphthalmology and Visual Sciences, The Chinese
University of Hong Kong, 3/F, Hong Kong EyeHospital, 147K Argyle Street, Kowloon, Hong Kong;
doi: 10.1136/bjo.2005.073858
References
1 Ruschen H, Celaschi D, Bunce C, et al.Randomised controlled trial of sub-Tenon’s blockversus topical anaesthesia for cataract surgery: acomparison of patient satisfaction. Br JOphthalmol2005;89:291–3.
2 Barequet IS, Soriano ES, Green WR, et al.Provision of anesthesia with single application oflidocaine 2% gel. J Cataract Refract Surg1999;25:626–31.
Accepted for publication 21 February 2005
MAILBOX
3
2
0
1
ISA
S sa
tisfa
ctio
n sc
ore
Sub-Tenon's block
0
Topical
0
Figure 1 Box and whisker plot of satisfactionscore with sub-Tenon’s block or topicalanaesthesia. (From Ruschen et al1)
Accepted for publication 25 April 2005
PostScript 1227
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

3 Assia EI, Pras E, Yehezkel M, et al. Topicalanesthesia using lidocaine gel for cataractsurgery. J Cataract Refract Surg 1999;25:635–9.
4 Bardocci A, Lofoco G, Perdicaro S, et al.Lidocaine 2% gel versus lidocaine 4% unpreserveddrops for topical anesthesia in cataract surgery: arandomized controlled trial. Ophthalmology2003;110:144–9.
5 Soliman MM, Macky TA, Samir MK. Comparativeclinical trial of topical anesthetic agents in cataractsurgery: lidocaine 2% gel, bupivacaine 0.5%drops, and benoxinate 0.4% drops. J CataractRefract Surg 2004;30:1716–20.
6 Van Wijk CM, Kolk AM. Sex differences inphysical symptoms: the contribution of symptomperception theory. Soc Sci Med1997;45:231–46.
Patient satisfaction withanaesthesia comparing sub-Tenon’s block and topicalanaesthesiaWe read with great interest the results of thepilot study comparing patient satisfactionbetween topical and sub-Tenon’s anaesthe-sia.1 In conclusion, the authors state that sub-Tenon’s block produces higher satisfactionscores than topical anaesthesia.1
The scores used were obtained using theIowa Satisfaction with Anesthesia Scale(ISAS), which has been used many timesduring other forms of surgery.2
However, the ISAS has not been used inthe setting of unmonitored anaesthetic careand has not as yet been fully validated in apurely local anaesthetic environment. Dexter,who was part of the team that developed theISAS, has said that the ISAS is still to bevalidated in this setting. Therefore, we wouldsuggest that the conclusions that sub-Tenon’sanaesthesia gives better satisfaction thantopical anaesthesia, purely based on thisscale, is slightly premature.The ISAS is due to be validated soon using
local anaesthesia and sedation3; however, it isstill used specifically during monitoredanaesthetic care and is as yet not tested onunmonitored anaesthetic care, which is oftenfound during topical cataract lists.
Correspondence to: Dr Wendy E Adams, SunderlandEye Infirmary, Queen Alexandra Road, Sunderland
SR2 9HP, UK; [email protected]
doi: 10.1136/bjo.2005.075895
References
1 Ruschen H, Celaschi D, Bunce C, et al.Randomised controlled trial of sub-Tenon’s blockversus topical anaesthesia for cataract surgery: acomparison of patient satisfaction. Br JOphthalmol2005;89:291–3.
2 Dexter F, Aker J, Wright WA. Development of ameasure of patient satisfaction with monitoredanesthesia care: the Iowa Satisfaction withAnesthesia Scale. Anesthesiology1997;87:865–73.
3 Fung D, Cohen M, Stewart S, et al. Can the IowaSatisfaction with Anesthesia Scale be used tomeasure patient satisfaction with cataract careunder topical local anesthesia and monitoredsedation at a community hospital? AnesthesiaAnalgesia 2005;100(6).
Cataract surgery and IOPWe would like to congratulate Issa et al1 ontheir excellent and, we believe, importantpaper regarding cataract surgery and intra-ocular pressure drop.
It has become increasingly obvious to us, inour practice, that many patients do indeedget a significant drop in intraocular pressure(IOP) after phacoemulsification. We nowhave a substantial number of patients withboth acute and chronic angle closure who,following cataract surgery, have been able tocome off all antihypertensive medications.We would now goes as far as to say that inthese patients it is now the operation ofchoice (when medical therapy has deemed tohave failed) and this is supported by anumber of studies.2–5 There is also the addedbenefit of a reduction in the incidence ofaqueous misdirection.It is interesting that Issa et al used
‘‘normal’’ patients in their study and stillfound a significant reduction in IOP. We havethought for sometime that a number ofglaucoma patients who, on gonioscopy, areseen to have ‘‘open angles’’ but on closerinspection have some (usually central) ante-rior chamber shallowing, often seem to haveprofound drops in their IOP following catar-act surgery. Although many of these patientshave degrees of hypermetropia, this is notalways the case. Indeed with increasingnuclear sclerosis some may be myopic atpresentation.The authors rightly state that their study
needs to be repeated by others to confirmtheir results. We think that lens thickness hasmore of a role than this study suggests. Thereis an important flaw—acknowledged by theauthors—regarding the lack of data oncorneal thickness. Any future studies needto correct for this, not only to allow a moreaccurate assessment of the IOP, but becausethe cornea itself is part of the anteriorstructure of the eye and may not necessarilybe an independent variable.Finally we speculate that there is likely to
be a measurable relation between IOP,volume of the anterior segment, lens size,and possibly corneal thickness. Once we havequantified this it may then allow us not onlyto be able to assess the likely magnitude ofIOP drop after phacoemulsification, but willgive an essential insight into some of theunderlying mechanisms of raised IOP.
S Fraser, P S PhelanSunderland Eye Infirmary, Queen Alexandra Road,
Sunderland SR4 9HP, UK
Correspondence to: Mr Scott Fraser, Sunderland EyeInfirmary, Queen Alexandra Road, Sunderland SR4
9HP, UK; [email protected]
doi: 10.1136/bjo.2005.073874
References
1 Issa SA, Pacheco J, Mahmood U, et al. A novelindex for predicting intraocular pressurereduction following cataract surgery.Br J Ophthalmol 2005;89:543–6.
2 Gunning FP, Greve EL. Lens extraction foruncontrolled angle- closure glaucoma: long-termfollow-up. J Cataract Refract Surg1998;24:1347–56.
3 Acton J, Salmon JF, Scholtz R. Extracapsularcataract extraction with posterior chamber lensimplantation in primary angle-closure glaucoma.J Cataract Refract Surg 1997;23:930–4.
4 Jacobi PC, Dietlein TS, Luke C, et al. Primaryphacoemulsification and intraocular lensimplantation for acute angle-closure glaucoma.Ophthalmology 2002;109:1597–603.
5 Teekhasaenee C, Ritch R. Combinedphacoemulsification and goniosynechialysis foruncontrolled chronic angle-closure glaucoma
after acute angle-closure glaucoma.Ophthalmology 1999;106:669–74.
Normal tension glaucomaI enjoyed the recent study by Ogata et al, inwhich they attempted to assess the interrela-tion between intracranial vascular compres-sion of the optic nerves and normal tensionglaucoma.1 Coronal magnetic resonanceimages of the optic nerves were used toassess the degree of compression of theintracranial optic nerves and the supraclinoidinternal carotid arteries. Compression of anoptic nerve by a normal internal carotidartery was found in 51 of 103 eyes (49.5%)of patients with normal tension glaucomaand in 36 of 104 (34.6%) eyes of controlpatients. The degree of compression wasnoted to be greater in patients with normaltension glaucoma. These findings led theauthors to conclude that one cause of normaltension glaucoma may be compression of theoptic nerve by the internal carotid artery.As noted in the discussion, Jacobson et al
found compression of the intracranial opticnerve by the internal carotid artery to becommon in asymptomatic patients (bilateralcontact in 70%, bilateral compression in 12%,unilateral contact or compression in 5%).2 Insymptomatic patients, Jacobson noted glau-comatous visual field defects and ‘‘saucer-like temporal excavation’’ of the optic disc onthe side of the compression.3 Symptomaticpatients also had temporal neuroretinal rimpallor and other signs of compressive opticneuropathy such as decreased visual acuityand decreased colour vision, thereby distin-guishing them from patients with normaltension glaucoma.4
In the Ogata study, inclusion of threeadditional outcome measures would be use-ful in defining any association that may existbetween intracranial optic nerve compressionand pseudoglaucomatous cupping. Firstly,did patients with normal tension glaucomaand intracranial optic nerve compressionhave decreased visual acuity, decreased col-our vision, or associated pallor of the tem-poral neuroretinal rim on the side of thecompressed optic nerve? Secondly, was theobserved cupping in eyes with normal ten-sion glaucoma and optic nerve compressionvertical in orientation (that is, pseudoglauco-matous) or horizontal or round (that is, non-glaucomatous), and did this configurationdiffer in eyes without optic nerve compres-sion? Finally, was the diagnosis of normaltension glaucoma confined to the involvedside in the nine patients with unilateral opticnerve compression, as the study hypothesiswould predict?
Correspondence to: Professor M C Brodsky,Department of Ophthalmology Arkansas Children’s
Hospital, 800 Marshall Street, Little Rock, AR 72202,USA; [email protected]
doi: 10.1136/bjo.2005.073866
References
1 Ogata N, Imaizumi M, Arichi M, et al. Opticnerve compression by normal carotid artery.Br J Ophthalmol 2005;90:174–9.
2 Jacobson DM, Warner JJ, Broste ST. Optic nervecompression by the internal carotid artery inasymptomatic patients. Am J Ophthalmol1997;123:677–83.
3 Jacobson DM. Symptomatic compression of opticnerve compression by the internal carotid artery.
Accepted for publication 31 May 2005
Accepted 25 April 2005
Accepted for publication 25 April 2005
1228 PostScript
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

Clinical profile of 18 patients with 24 affectedeyes identified by magnetic resonance imaging.Ophthalmology 1999;106:1994–2004.
4 Trobe JD, Glaser JS, Cassady J, et al. Non-glaucomatous excavation of the optic disc. ArchOphthalmol 1980;98:1046–50.
Vision restoration therapyA recent paper1 and accompanying editor-ials2 3 in the BJO have raised the question ofwhether vision restoration therapy is effectivein the rehabilitation of visual field defects. Asmembers of the scientific medical advisoryboard of NovaVision, we believe these editor-ials require comment and refer the interestedreader to an opposing editorial in a recentissue of the BJO by Sabel and colleagues4 andto an article in press in Restorative Neurologyand Neuroscience.5 Although we acknowledgethat statements by members of an advisoryboard are always complicated by potentialconflicts of interest, we hope that ourcolleagues will recognise our commitment toscientific debate.We believe the current evidence does not
support Horton’s contention that ‘‘no ther-apeutic intervention…can correct effectivelythe underlying visual field deficit’’ after post-chiasmatic injury. On the contrary, a com-prehensive and critical review of the litera-ture reveals that there is a sound scientificbasis for recommending vision restorationtherapy for some patients with hemianopia.Studies of the practical effectiveness andscientific basis of vision restoration therapyare now ongoing, and patients are beingtreated at nine US centres. We urge physi-cians and scientists to review the currentliterature and the results of future studies asthey become available. Although there areclearly important questions regarding thisintervention that need to be elucidated, it isevident that the main goal, that of visualrehabilitation, is attained for some of thosetreated with vision restoration therapy. In ouropinion, the preponderance of the datasupports the notion that this intervention isvaluable and results in visual improvementfor certain patients with visual field defects.
L R CaplanDepartment of Neurology, Beth Israel Deaconess
Medical Center, Boston, MA, USA
A FirlikNew York University School of Medicine, NY, USA
N J NewmanEmory University School of Medicine, Atlanta, GA,
USA
M PlessNeurology and Neuro-Ophthalmology, Northeast
Health System, USA
J G RomanoCerebrovascular Division, University of Miami, FL,
USA
N SchatzBascom Palmer Eye Institute, Miami, FL, USA
Correspondence to: Jose G Romano, MD,Cerebrovascular Division, University of Miami, FL,
USA; [email protected]
References
1 Reinhard J, Schreiber A, Schiefer U, et al. Doesvisual restitution training change absolutehomonymous visual field defect? A fundus-controlled study. Br J Ophthalmol 2005;89:30–5.
2 Horton JC. Disappointing results from NovaVision’s visual restoration therapy. Br JOphthalmol2005;89:1–2.
3 Plant GT. A workout for hemianopia.Br J Ophthalmol 2005;89:2.
4 Sabel BA, S Kenkel S, Kasten E. Vision restorationtherapy. Br J Ophthalmol 2005;89:522–4.
5 Sabel BA, Kenkel S, Kasten E. Vision restorationtherapy (VRT) efficacy as assessed bycomparative perimetric analysis and subjectivequestionnaires. Restor Neurol Neurosci2004;22:399–420.
Disclosure: The authors are members of the Scientificand Medical Advisory Board of NovaVision, thecompany that has developed vision restoration
therapy.
doi: 10.1136/bjo.2005.069773
Accepted for publication 1 March 2005
NOTICES
Thoughts on Ophthalmology andDevelopmentThe Matuis Eye Foundation is a small,privately-financed organisation, established17 years ago by a former international bankerwho began his medical studies at age 40with the specific intention of working inthird world surgical ophthalmology. TheFoundation’s experiences and lessons learnedare presented in a 26 page bound summaryentitled Thoughts on Poor World OphthalmologyDevelopment, an often critical look at eyesurgery programs in Latin America, Africa,and Haiti. To obtain this report without cost,please contact. [email protected].
EVER 2005 meetingThis will take place on 5-8 October 2005 inVilamoura, Portugal. For further detailsplease contact: Christy Lacroix, EVERSecretary, Kapucijnenover 33, B-3000Leuven, Belgium (tel: +32 (0)16 233 849;fax +32 (0)16 234 097; email:[email protected]).
World Ophthalmology Congress2006 – BrazilThe World Ophthalmology Congress (whichis replacing the International Congress ofOphthalmology) is meeting in February 2006in Brazil.For further information on the congress
and committees, scientific program andcoordinators of different areas are availableat the congress website www.ophthalmolo-gy2006.com.br
Red eyeThe latest issue of Community Eye Health (No53) discusses the role of primary care in thetreatment of red eye. For further information
yplease contact: Journal of Community EyeHealth, International Resource Centre,International Centre for Eye Health,Department of Infectious and TropicalDiseases, London School of Hygiene andTropical Medicine, Keppel Street, LondonWC1E 7HT, UK (tel: +44 (0)20 7612 7964;email: [email protected]; online edi-tion: www.jceh.co.uk). Annual subscription(4 issues) UK £28/US$45. Free to developingcountry applicants.
ORBIS introduces surgical simulatorto train ophthalmologists acrossdeveloping worldInternational development agency, ORBIS, isusing a high-tech ophthalmic surgical simu-lator for the first time this month, as part ofits Flying Eye Hospital training programme inVarna, Bulgaria (8-24 June). The ‘Eyes-1’training system will be used by ORBIS to helptrain eye specialists in developing countries inthe latest surgical techniques to prevent andtreat avoidable blindness.Through its work as an international
development agency ORBIS has completedover 500 training programmes in 76 countriesand has established permanent countryprogramme offices in five nations –Bangladesh, China, Ethiopia, India, andVietnam. Since 1982 ORBIS volunteers havetreated more than 25000 patients and trainedover 70000 medical professionals.The Eyes-1 surgical simulator was created
by VRmagic Technology Group in 2002, aGerman company specialising in image pro-cessing and display technology.For further information or contributions of
any kind please call +44 (0)20 7608 7260 orvisit www.ukorbis.org
4th International Conference onOcular InfectionsThis will take place on 1–4 October 2005 inHokkaido, Japan. For further informationplease contact the Management Secretariat,[email protected].
PostScript 1229
www.bjophthalmol.com
on March 20, 2022 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.2005.073874 on 19 A
ugust 2005. Dow
nloaded from

Bilateral naevus of Ota withchoroidal melanoma and diffuseretinal pigmentation in a darkskinned personNaevus of Ota (naevus fusculocoeruleusophthalmomaxillaris) was described by theJapanese dermatologist, Ota, in 1939 as adermal melanocytic hamartoma that presentsas bluish hyperpigmentation along theophthalmic, maxillary, and mandibularbranches of the trigeminal nerve. It isbilateral in less than 5% cases, occurringfrequently in Orientals (0.2%–1%) and darkerraces and rarely in white people (0.04%).Open angle glaucomas and choroidal mela-noma are the rare ocular involvements. Ota’snaevus is more common in Asians than whitepeople but uveal melanoma occurs predomi-nantly in white populations.1 2 Dark skinnedpatients represent only 1% of all cases oforbital melanomas.3 The risk of developinguveal melanoma in a patient with naevus ofOta is one in 400 patients in their lifetime.1 2
We report a rare case of bilateral naevus ofOta with a right (RE) choroidal melanomaand left (LE) diffuse pigmentation of retina.
Case reportA 73 year old Anglo-Indian woman wasreferred with complaints of photopsia. Shehad black hair and light brown skin.Examination revealed a brownish-black pig-mentation of the conjunctiva, episclera, andperiocular skin bilaterally (fig 1). Visualacuity for distance and near was 6/6 andN5, respectively, in each eye. Heterochromiawas present, the right iris being a darkerbrown than the left, which had a sector oflight brown colour. Gonioscopy and intra-ocular pressure were normal. The rightfundus revealed a pigmented, large, elevatedchoroidal mass 10 disc diameter (DD) in size,4 DD superonasal to the disc. Drusen wereoverlying it. No subretinal fluid was seen. Theleft eye showed a patchy dark pigmentation3 DD in size, at the temporal edge of themacula. A ridge-like pigmented elevation,3 DD long, was also seen along the super-onasal vessels. Both optic discs and maculaswere normal. Ultrasound in the right eyeshowed a 10 mm tumour, 4.2 mm high.Fluorescein angiography confirmed its inde-pendent circulation. A systemic examinationfound no signs of metastasis. A diagnosis of a
bilateral naevus of Ota with low grade,choroidal melanoma in the right eye (fig 2)and retinal pigmentation in the left eye wasmade. The patient was reluctant to accept theoption of enucleation in view of the rightvision. A 125I radioactive plaque was applied(COMS study). A follow up examination3 years postoperatively showed a flatter,yellow 4 DD61.5 DD scarred tumour withmottled pigmentation. The left melanosisremained unchanged. The vision was 6/6 inboth eyes 6 years after 125I treatment andcataract surgery.
CommentOta’s naevus is commonly seen unilaterally(90%). Bilateral involvement is rare. Itrepresents melanocytes that have notmigrated completely from the neural crestto the epidermis during the embryonic stage.Orientals and pigmented races have a highprevalence with a predilection for women (1:4.8). Variable prevalence among differentpopulations suggests genetic influences,although familial cases are rare. Two peakages of onset in early infancy (50%) and inearly adolescence suggest hormonal influ-ence.1 In addition to the skin, pigmentationmay involve oral mucosa, tympanic mem-brane, intranasal mucosa, leptomeninges andocular structures such as the sclera, retro-bulbar fat, cornea, lens, trabeculum, disc, andretina. Associated malignant melanomas ofthe uvea, orbit, skin, and CNS have beendescribed.2 Choroidal melanomas are knownto occur in less than 4% of cases andglaucoma has been noticed in less than 10%of cases.4
Our case reports a rare occurrence ofbilateral naevus of Ota with choroidal malig-nant melanoma in the right eye and retinalpigmentation in the left eye in a pigmentedperson. She was born to Anglo-Indian par-ents but did not know how far back in timethe intermarriage had occurred.Ophthalmological follow up care is necessaryfor patients with increased melanosis. This
case illustrates the need for regular ophthal-mic review of all pigmented lesions and therecognition that patients with naevus of Otamay also have the additional complication ofmelanoma. There is need for close observa-tion of all pigmented lesions of the eye.Regardless of the patient’s race, there is agreater than normal chance that a patientwith the naevus of Ota might have amalignant melanoma develop within one ofthe affected tissues.
S Sharan, J R Grigg, F A BillsonSave Sight Institute, University of Sydney, Departmentof Ophthalmology, Sydney Eye Hospital, 8 Macquarie
Street, Sydney 2000, Australia
Correspondence to: Sapna Sharan, Save SightInstitute, University of Sydney, Department of
Ophthalmology, Sydney Eye Hospital, 8 MacquarieStreet, Sydney 2000, Australia;
doi: 10.1136/bjo.2005.070839
References
1 Hidano A, Kajima H, Ikeda S, et al. Naturalhistory of nevus of Ota. Arch Dermatol1967;95:187–95.
2 Gonder JR, Shields JA, Albert DM, et al. Uvealmalignant melanoma associated with ocular andoculodermal melanocytosis. Ophthalmology1982;89:953–60.
3 Margo CE, McLean IW. Malignant melanoma ofthe choroid and ciliary body in black patients.Arch Ophthalmol 1984;102:77–9.
4 Roy PE, Schaeffer EM. Nevus of Ota andchoroidal melanoma. Surv Ophthalmol1967;12:130–40.
Treatment of neurotrophickeratopathy with nasal dilatorstripsNeurotrophic keratopathy, characterised bypoorly healing corneal epithelium, occurs ineyes with decreased corneal sensory innerva-tion. Clinical findings include chronic epithe-lial defects and corneal ulceration. Numerousconditions predispose to neurotrophic kerato-pathy including diabetes mellitus, accidentaland surgical trauma, herpes simplex andherpes zoster keratitis, leprosy, and topicalanaesthetic abuse.Management of neurotrophic keratopathy
includes ocular lubrication, pressure patch-ing, autologous serum eye drops,1 fitting of abandage contact lens,2 amniotic membranegrafting,3 4 and surgical tarsorrhaphy.Surgical tarsorrhaphy can be very successfulin resolving neurotrophic corneal ulceration,5
but many patients find this option cosmeti-cally unacceptable.We describe a novel method of non-
surgical tarsorrhaphy using over the counteradhesive, non-medicated, nasal dilator strips(NDS) (Breathe Right Nasal Strips,Whippany, NJ, USA) applied vertically acrossthe eyelids (fig 1). The adhesive strip consistsof parallel bands of plastic imbedded in apad, and is available in different sizes.The nasal strips were originally developed
to treat patients with snoring problems,6
or to improve nasal congestion.7 In rhino-logical applications, the strip is typically usedFigure 1 Oculodermal pigmentation.
Figure 2 Choroidal melanoma.
LETTERS
PostScript . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accepted for publication 1 May 2005
Br J Ophthalmol 2005;89:1529–1545 1529
www.bjophthalmol.com

horizontally across the nose in order to openthe nasal airway. In the current study, weapplied the strip vertically over the closedeyelid as shown in figure 1. The adhesive stripcreates a firm and effective eyelid closure,and patients can control the application andremoval of the strip. The strips have theadvantage of being relatively inexpensive,reusable, and reversible, and their use hasreplaced standard eye patching in our clinicalpractice. We have noted success with the useof these strips for the management ofneurotrophic ulceration and describe tworepresentative cases.
Case reportsA 60 year old woman developed a neuro-trophic corneal ulcer following a complicatedretinal detachment repair. After a year ofstandard medical therapies, including lubri-cation and frequent conventional patching,she continued to have a 4 mm64 mmchronic non-healing epithelial defect.Treatment with reversible NDS tarsorrhaphywas initiated with instructions to apply thestrips at bedtime and as much as possibleduring the day. Nine weeks later the cornealepithelial defect had healed completely. Overthe next year she gradually decreased thewearing time of the strips and is currentlystable without their use.A 48 year old woman with a 6 mm62 mm
neurotrophic corneal ulcer was referred formanagement after failing numerous medicaland surgical therapies including lubrication,autologous serum eye drops, patching, andan amniotic membrane graft. The patient wasinstructed to use NDS tarsorrhaphy accordingto the schedule described in the previouscase. Within 2 weeks the corneal epithelialdefect healed completely. The patient con-tinues to apply the tarsorrhaphy but withdecreasing frequency.The novel use of nasal dilator strips to
perform a temporary tarsorrhaphy has aidedus greatly in our management of neuro-trophic corneal ulceration. We believe it is anattractive, cost effective, efficient alternativeto patching for any ocular condition. Inaddition, nasal strip tarsorrhaphy allows forimmediate reversibility that facilitates patientacceptance.
M T Magone, G D Seitzman, S Nehls,T P Margolis
Francis I Proctor Foundation, University of CaliforniaSan Francisco, 95 Kirkham Street, San Francisco, CA
94143, USA
Correspondence to: T P Margolis, MD, PhD, Francis IProcter Foundation, 95 Kirkham Street, San Francisco,
CA 94143, USA; [email protected]
doi: 10.1136/bjo.2005.073114
References
1 Matsumoto Y, Dogru M, Goto E, et al. Autologousserum application in the treatment of neurotrophickeratopathy. Ophthalmology2004;111:1115–20.
2 Montero J, Sparholt J, Mely R, et al. Retrospectivecase series of therapeutic applications oflotrafilcon a silicone hydrogel soft contact lenses.Eye Contact Lens 2003;29:72–5.
3 Solomon A, Meller D, Prabhasawat P, et al.Amniotic membrane grafts for nontraumaticcorneal perforations, descemetoceles, and deepulcers. Ophthalmology 2002;109:694–703.
4 Prabhasawat P, Tesavibul N. Preserved amnioticmembrane transplantation for conjunctivalsurface reconstruction. Cell Tissue Bank2001;2:31–9.
5 Cosar CB, Cohen EJ, Rapuano CJ, et al.Tarsorrhaphy: clinical experience from a corneapractice. Cornea 2001;20:787–91.
6 Ufberg J. Fenton G. Effect of breathe right nasalstrip on decrease snoring. Rhinology1997;35:50–2.
7 Ochi K, Mitsui M, Kaneko T, et al. The applicationof Breathe Right for otorhinolaryngologicdisorders. Otorhinology 1997;90:597–601.
Confocal microscopy of thecornea in nephropathic cystinosisCystinosis is an autosomal recessive inheriteddisorder of amino acid metabolism charac-terised by the deposition of cystine crystals inthe eye, kidney, reticuloendothelial system,and various other tissues.1 Childhood ornephropathic cystinosis can present as aninfantile or a juvenile variant.1 The infantilevariant tends to have a more devastatingcourse and is associated with growth retarda-tion, rickets, and eventual renal failure whichrequires transplantation within the firstdecade.1 The juvenile variant has later onsetand milder nephropathy.1
In nephropathic cystinosis, crystal depositsusually appear in the peripheral, anteriorcornea within the first year of life andprogress centrally and posteriorly until theentire cornea is involved.2–7 The diagnosis canbe confirmed histopathologically by demon-stration of characteristic crystals by electronmicroscopy in a conjunctival biopsy.8 9
Stromal deposition of crystal deposits hasbeen demonstrated by confocal microscopy.9
We provide the first demonstration, to thebest of our knowledge, of cystine crystals inthe corneal epithelium using in vivo confocalmicroscopy.
Case reportA 9 year old boy presented to the KingKhaled Eye Specialist Hospital in Riyadh,Saudi Arabia, with a complaint of recurrentforeign body sensation, associated withsevere photophobia and blepharospasm. Hehad been diagnosed with infantile nephro-pathic cystinosis at age of 9 months and hadbeen treated with systemic cysteamine. Onexamination, the visual acuity was 20/20 inthe right eye and 20/25 in the left eye. The
intraocular pressure was 12 mmHg in botheyes. Slit lamp examination showed crystaldeposits of 2.5 in Gahl density score7 in bothcorneas, predominantly involving the ante-rior stroma and with limbus to limbusdistribution (fig 1). Dilated fundus examina-tion was normal with no maculopathy orperipheral retinal pigment abnormalities.Topical treatment with cysteamine 0.5%drops resulted in symptomatic relief.Confocal microscopy (Confoscan 3, Nidek
Technologies, Vigonza, Italy) demonstratedcrystalline deposits in the corneal epithelium(fig 2A, B) and stroma (fig 2C, D). Crystaldeposits in the corneal epithelium wereneedle shaped and fusiform shaped andoriented parallel to the plane of the epithelialcells (fig 2A, B). In the basal cell layer, thecrystals were associated with dendritic cells(fig 2B). The highest crystal density was inthe mid-stroma, where fusiform shapedcrystals were more predominant than needleshaped crystals (fig 2C). The lowest crystaldensity was in the posterior stroma, wheremost of the deposits were needle shaped(fig 2E). Within the stroma the crystals wereoriented parallel to the plane of the stromallamella. The needle shaped crystals werehighly variable in length with some as longas 100 mm. The endothelial cell layer wasnormal.
CommentThe current case clearly documents thatcrystalline deposits may be found in theepithelium of patients with nephropathiccystinosis, unlike previous electron micro-scopic8 and confocal microscopic9 studies thatsuggest these deposits are localised to thestroma. In addition, we found maximumcrystal density in the mid-stroma and mini-mum density in the posterior stroma, incontrast with a previous report in whichmaximum crystal density was just anterior toDescemet’s membrane.9
We hypothesise the presence of theseabnormal deposits in the corneal epitheliummay contribute, in part, to the foreign bodysensation and photophobia that is invariablyassociated with this disorder, as well as thepredisposition to recurrent epithelial ero-sions. Chronic low grade inflammation ofthe epithelium and epithelial basementmembrane zone associated with recurrentepithelial erosions is the probable explana-tion for the presence of dendritic cells in thebasal epithelium of the central cornea.10
Successful reduction in the density of cornealcrystals and symptomatic relief was obtainedwith the use of topical cysteamine 0.5%drops, as in previous reports.5–7
Figure 1 Applying a nasal dilator stripvertically over the eyelid creates an easilyreversible tarsorrhaphy. It also provides aneffective and, for patients, cosmeticallyacceptable way to treat chronic cornealneurotrophic disorders.
Accepted for publication 10 May 2005
Figure 1 Crystal deposits in the right eyepredominantly involving the anterior and mid-stroma, with limbus to limbus distribution.
1530 PostScript
www.bjophthalmol.com

A H Alsuhaibani, M D WagonerAnterior Segment Division, Department of
Ophthalmology, King Khaled Eye Specialist Hospital,Riyadh, Kingdom of Saudi Arabia
A O KhanPediatric Ophthalmology and Strabismus Division,Department of Ophthalmology, King Khaled Eye
Specialist Hospital, Riyadh, Kingdom of Saudi Arabia
Correspondence to: Michael D Wagoner, MD, KingKhaled Eye Specialist Hospital, PO Box 7191, Riyadh
11462, Kingdom of Saudi Arabia;[email protected]
doi: 10.1136/bjo.2005.074468
References
1 Theone JG. Cystinosis. J Inherit Metab Dis1995;18:380–6.
2 Wong VG, Schulman JD, Seegmiller JE.Conjunctival biopsy for the biochemical diagnosisof cystinosis. Am J Ophthalmol 1970;70:278–81.
3 Kaiser-Kupfer MI, Chan CC, Rodriques M, et al.Nephropathic cystinosis: immunohistochemicaland histopathologic studies of cornea,conjunctiva, and iris. Curr Eye Res1987;66:17–22.
4 Cotran PR, Bajart AM. Congenital cornealopacities. Int Ophthalmol Clin 1992;32:93–105.
5 Iwata F, Kuehl EM, Reed GF, et al. A randomizedclinical trial of topical cysteamine disulfide(cystamine) versus free thiol (cysteamine) in thetreatment of corneal cystine crystals in cystinosis.Mol Genet Metab 1998;64:237–42.
6 Gahl WA, Kuehl EM, Iwata F, et al. Cornealcrystals in nephropathic cystinosis: natural historyand treatment with cysteamine eyedrops. MolGenet Metab 2000;71:100–20.
7 Khan AO, Latimer B. Successful use of topicalcysteamine formulated from the oral preparationin a child with keratopathy secondary tocystinosis. Am J Ophthalmol 2004;138:674–5.
8 Kenyon KR, Sensenbrenner JA. Electronmicroscopy of cornea and conjunctiva inchildhood cystinosis. Am J Ophthalmol1974;78:68–76.
9 Grupcheva CN, Ormonde SE, McGhee C. In vivoconfocal microscopy of the cornea innephropathic cystinosis. Arch Ophthalmol2002;120:1742–5.
10 Gillette TE, Chandler JW, Greiner JV. Langerhanscells of the ocular surface. Ophthalmology1982;89:700–11.
Total parenteral nutrition,vitamin E, and reversible maculardysfunction morphologicallymimicking age related maculardegenerationA variety of nutrient deficiencies may predis-pose to the development of age relatedmacular degeneration (AMD).1 Patients
receiving parenteral nutrition (TPN) may beat particular risk of early onset AMD, becauseof inadequate or excess nutritional supple-mentation.1 Studies including the EyeDisease Case-Control Study and Beaver DamEye Study have evaluated the relationbetween antioxidant and micronutrientlevels, and the risk of AMD.2–4 A protectiveeffect of high plasma vitamin E levels wasconvincingly demonstrated.5
We describe a patient treated with parent-eral fluid support who developed visualsymptoms and signs of AMD, in conjunctionwith longstanding vitamin E deficiency.Isolated cases of visual disturbance inpatients undergoing TPN have been reportedin the literature6 7; however, to our knowl-edge, no case of visual disturbance attributedto vitamin E deficiency has been reported inthis context.
Case reportA 57 year old man received parenteral fluidfive times a week at home because of shortbowel syndrome secondary to Crohn’s dis-ease. It was thought he had undergone boweladaptation to meet macronutrient and micro-nutrient needs in the 13 years since hissurgery. He presented with subacute visualdisturbance. He described altered colourperception in situations analogous to macularstress testing (moving from dark adaptedsituations to bright lights) and enlargingcentral scotomata. Visual acuity was 6/6 inthe right eye, 6/12 in the left. Visual fields,intraocular pressures, and neurologicalexamination were normal. Funduscopyrevealed macular soft drusen, and extensivesubretinal basal laminar deposits in themacular region, more marked in the rightthan left eye (fig 1). Electroretinogram wasnormal.The patient was receiving electrolyte sup-
port 6 days a week at time of presentation.Measured haematological parameters and
urea and electrolyte levels revealed a lowhaemoglobin level (11.0 g/dl), and a milddegree of macrocytosis (102.3 fl). Becausehypervitaminosis and/or deficiency in traceminerals were suspected, serum values ofvitamins A, E, B1, B2, B6, plasma zinc,copper, selenium, manganese, caeruloplas-min, and red cell GSH activity were mea-sured. Results revealed vitamin E deficiency(12 mmol/l, normal range: 14–39 mmol/l). Aretrospective survey of previous serum vita-min E levels suggested longstanding defi-ciency, with levels of 10 mmol/l, and 13 mmol/l, 6 months and 1 year respectively, beforeonset of symptoms. Treatment with vitaminsupplementation lead to complete resolutionof symptoms in 3 weeks. Vitamin E levelsreturned to normal; however, fundal appear-ances remained unchanged.
CommentThe presence of bilateral hard and soft drusenand pigmentary abnormalities in the maculaare the clinical hallmarks of AMD.8 The earlyonset of morphological changes at Bruch’smembrane/retinal pigment epithelium (RPE)interface may relate to vitamin or micronu-trient deficiency, associated with parenteralnutrition.7
Cumulative oxidative damage may have animportant role in the pathogenesis of AMD,since accumulation of lipofuscin pigmentsmay arise as a consequence of antioxidantdeficiency, or under pro-oxidant conditions.5
Evidence exists for an association betweenatrophic AMD and excessive lipofuscin accu-mulation.8 9 Compromised RPE in this con-text is believed to be due to the amphiphilicstructure and photoreactivity of the di-retinalconjugate A2E, the major constituent oflipofuscin.5 9 Antioxidant vitamins have beenshown to aid in the defence against AMD.5
Vitamins E and C suppress A2E epoxidation,suggesting one mechanism by which thesevitamins may protect the ageing macula.9
Vitamin E deficiency was present consis-tently over the 12 month period precedingsymptom onset, reinforcing the likelihoodthat the clinical presentation had beencaused by vitamin E deficiency. Vitamin Edeficiency results in retinal degeneration,excessive RPE lipofuscin, and decrease inthe polyunsaturated fatty acid content of rodouter segments and the RPE.5 Furthermore,vitamin E deficiency may cause mild macro-cytic anaemia and accumulation of ceroidlipofuscin in nerves, affecting function ofcentral and peripheral nervous systems.6
Patients with sufficient gut length for proteincalorie nutrition receiving parenteral fluidsmay run the risk of micronutrient deficiencydespite a normal diet, and may present to theophthalmology department. We recommendformal micronutrient screening in patientswith extensive small bowel resection.
Figure 2 Crystal deposits in the corneal epithelium and stroma. A mixture of needle shaped and fusiform shaped crystals are present in (A) thesuperficial epithelial cell layer and (B) the wing cell layer. (C) Dendritic cells are present in the basal cell layer. (D) The greatest density of crystals is inthe mid-stroma, where fusiform shaped crystals are the predominant morphology. (E) The least density of crystals is in the posterior stroma, whereneedle shaped crystals are the predominant morphology.
Accepted for publication 10 May 2005
Competing interests: none declared
Figure 1 Macular soft drusenosis,characterised by subretinal basal laminardeposits in the macular region.
PostScript 1531
www.bjophthalmol.com
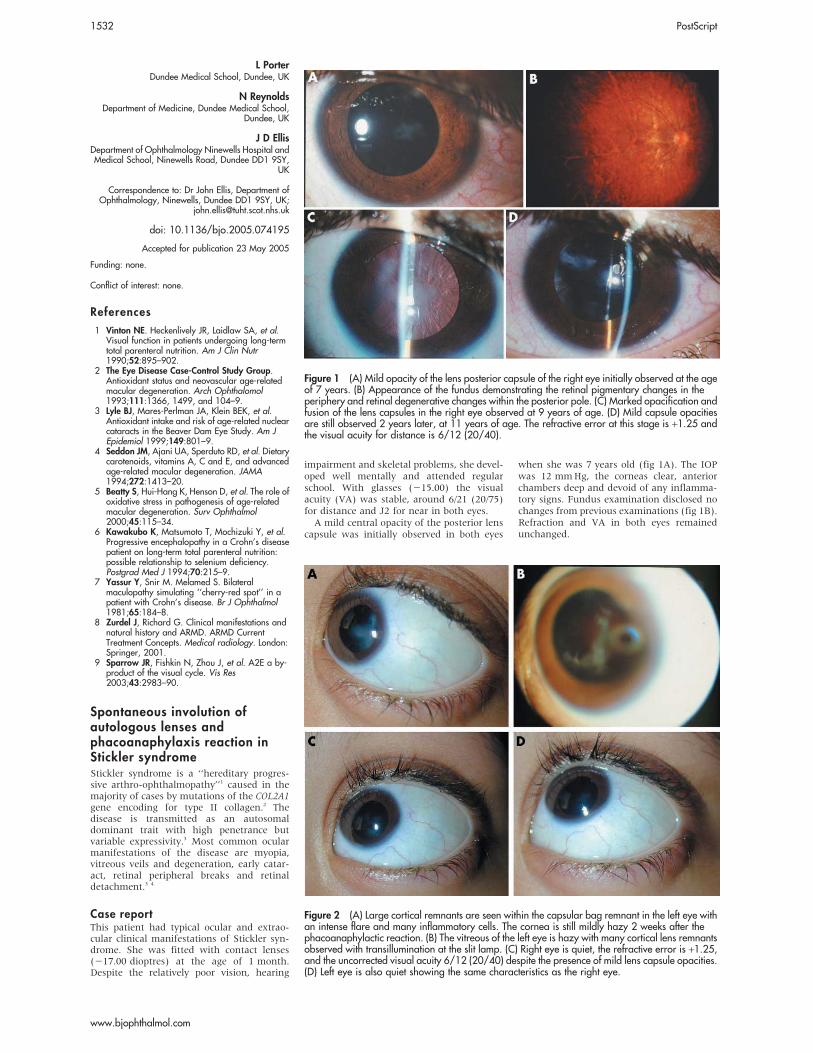
L PorterDundee Medical School, Dundee, UK
N ReynoldsDepartment of Medicine, Dundee Medical School,
Dundee, UK
J D EllisDepartment of Ophthalmology Ninewells Hospital andMedical School, Ninewells Road, Dundee DD1 9SY,
UK
Correspondence to: Dr John Ellis, Department ofOphthalmology, Ninewells, Dundee DD1 9SY, UK;
doi: 10.1136/bjo.2005.074195
References
1 Vinton NE. Heckenlively JR, Laidlaw SA, et al.Visual function in patients undergoing long-termtotal parenteral nutrition. Am J Clin Nutr1990;52:895–902.
2 The Eye Disease Case-Control Study Group.Antioxidant status and neovascular age-relatedmacular degeneration. Arch Ophthalomol1993;111:1366, 1499, and 104–9.
3 Lyle BJ, Mares-Perlman JA, Klein BEK, et al.Antioxidant intake and risk of age-related nuclearcataracts in the Beaver Dam Eye Study. Am JEpidemiol 1999;149:801–9.
4 Seddon JM, Ajani UA, Sperduto RD, et al. Dietarycarotenoids, vitamins A, C and E, and advancedage-related macular degeneration. JAMA1994;272:1413–20.
5 Beatty S, Hui-Hang K, Henson D, et al. The role ofoxidative stress in pathogenesis of age-relatedmacular degeneration. Surv Ophthalmol2000;45:115–34.
6 Kawakubo K, Matsumoto T, Mochizuki Y, et al.Progressive encephalopathy in a Crohn’s diseasepatient on long-term total parenteral nutrition:possible relationship to selenium deficiency.Postgrad Med J 1994;70:215–9.
7 Yassur Y, Snir M. Melamed S. Bilateralmaculopathy simulating ‘‘cherry-red spot’’ in apatient with Crohn’s disease. Br J Ophthalmol1981;65:184–8.
8 Zurdel J, Richard G. Clinical manifestations andnatural history and ARMD. ARMD CurrentTreatment Concepts. Medical radiology. London:Springer, 2001.
9 Sparrow JR, Fishkin N, Zhou J, et al. A2E a by-product of the visual cycle. Vis Res2003;43:2983–90.
Spontaneous involution ofautologous lenses andphacoanaphylaxis reaction inStickler syndromeStickler syndrome is a ‘‘hereditary progres-sive arthro-ophthalmopathy’’1 caused in themajority of cases by mutations of the COL2A1gene encoding for type II collagen.2 Thedisease is transmitted as an autosomaldominant trait with high penetrance butvariable expressivity.3 Most common ocularmanifestations of the disease are myopia,vitreous veils and degeneration, early catar-act, retinal peripheral breaks and retinaldetachment.3 4
Case reportThis patient had typical ocular and extrao-cular clinical manifestations of Stickler syn-drome. She was fitted with contact lenses(217.00 dioptres) at the age of 1 month.Despite the relatively poor vision, hearing
impairment and skeletal problems, she devel-oped well mentally and attended regularschool. With glasses (215.00) the visualacuity (VA) was stable, around 6/21 (20/75)for distance and J2 for near in both eyes.A mild central opacity of the posterior lens
capsule was initially observed in both eyes
when she was 7 years old (fig 1A). The IOPwas 12 mmHg, the corneas clear, anteriorchambers deep and devoid of any inflamma-tory signs. Fundus examination disclosed nochanges from previous examinations (fig 1B).Refraction and VA in both eyes remainedunchanged.
Accepted for publication 23 May 2005
Funding: none.
Conflict of interest: none.
Figure 1 (A) Mild opacity of the lens posterior capsule of the right eye initially observed at the ageof 7 years. (B) Appearance of the fundus demonstrating the retinal pigmentary changes in theperiphery and retinal degenerative changes within the posterior pole. (C) Marked opacification andfusion of the lens capsules in the right eye observed at 9 years of age. (D) Mild capsule opacitiesare still observed 2 years later, at 11 years of age. The refractive error at this stage is +1.25 andthe visual acuity for distance is 6/12 (20/40).
Figure 2 (A) Large cortical remnants are seen within the capsular bag remnant in the left eye withan intense flare and many inflammatory cells. The cornea is still mildly hazy 2 weeks after thephacoanaphylactic reaction. (B) The vitreous of the left eye is hazy with many cortical lens remnantsobserved with transillumination at the slit lamp. (C) Right eye is quiet, the refractive error is +1.25,and the uncorrected visual acuity 6/12 (20/40) despite the presence of mild lens capsule opacities.(D) Left eye is also quiet showing the same characteristics as the right eye.
1532 PostScript
www.bjophthalmol.com

On 23 June 2002, at the age of 9 years, shecomplained of blurred vision in the right eye.Without glasses, VA for distance was 6/60(20/200) and for near less than J16.Involution of the lens material with markedopacity of the fused capsules was detected(fig 1C). Accurate retinoscopy was notpossible. No intraocular inflammatory signswere observed.On 23 May 2004, the right eye lens
opacities reabsorbed. Mild posterior capsuleopacity remains (fig 1D). VA without correc-tion was 6/12 (20/40) and J10. Refractiondisclosed +1.25 D. The left eye VA andmyopia remained unchanged.Six weeks later sudden pain, redness, and
loss of vision in the left eye occurred. A highIOP of 60 mmHg, hazy cornea, mutton fatkeratic precipitates with flare 3+ and cells 4+were observed in the left eye anteriorchamber. She was treated with corticoster-oids and antiglaucoma drops. Two weekslater, a central tear of the posterior capsulewith large cortical remnants within thecapsular bag (fig 2A) and a multitude offloating lens remnants with a granulomatousinflammatory reaction were observed in thevitreous (fig 2B). Following complete arrestof the inflammatory processes and a return tonormal of the IOP, medical treatment wasdiscontinued 5 weeks after its initiation.At her last visit on 21 November 2004, both
eyes were quiet. Only mild scattered lenscapsule opacities were detected in both eyes(figs 2C and 2D). The VA without correctionwas 6/12 (20/40) and J10 in both eyes. Withcorrection (+1.25) for distance and nearaddition (+3.00), the VA in both eyes was 6/9 (20/30) and J1 respectively. Multifocalglasses were prescribed.
CommentA quiet and uneventful involution of theautologous lens occurred in the right eyewhen the child was 9 years old. The mechan-ism of this phenomenon is unclear and maybe associated with abnormalities of the lenscollagen and/or crystallines. The lens involu-tion in the right eye was not associated withany noticeable symptom but for a drop invision. Progressive clearing of the lens opacitywas followed by emmetropisation of theinitial refractive error and visual improve-ment in the left eye. Two years later,spontaneous involution of the lens in theother eye was associated with a markedintraocular granulomatous inflammatoryreaction (‘‘granulomatous uveitis’’) reminis-cent of a phacoanaphylaxis reaction. Thisacute reaction was, most probably, associatedwith the ‘‘escape’’ of immune tolerancetowards the autologous lens antigens.We are not aware of previous reports in the
literature describing similar ocular phenomena.
I Habil, E Cohen, I Karshai, D BenEzraPediatric Ophthalmology Unit, Hadassah Hebrew
University, Jerusalem, Israel
F Behar-CohenRothschild Ophthalmic Foundation, Paris, France
D BenEzra, F Behar-CohenU598, INSERM, Paris, France
Correspondence to: David BenEzra, MD, PhD,Hadassah Hebrew University Hospital, POB 12000
Jerusalem, Israel; [email protected]
doi: 10.1136/bjo.2005.076935
References
1 Stickler GB, Belau PG, Farrell FJ, et al. Hereditaryprogressive arthro-ophthalmopathy. Mayo ClinProc 1965;40:433–55.
2 Francomano CA, Liberfarb RM, Hirose T, et al.The Stickler syndrome is closely linked toCOL2A1, the structural gene for type II collagen.Pathol Immunopathol Res 1988;7:104–6.
3 Donoso LA, Edwards AO, Frost AT, et al.Identification of a stop codon mutation in exon 2of the collagen 2A1 gene in large sticklersyndrome family. Am J Ophthalmol2002;134:720–7.
4 Spallone A. Stickler’s syndrome: a study of 12families. Br J Ophthalmol 1987;71:504–9.
Temporal pterygium: benign ornot?A true pterygium is a degenerative andhyperplastic process in which the cornea isinvaded by a triangular fold of bulbarconjunctiva. Duke-Elder states that the pter-ygium when single is almost invariably foundon the nasal side.1 The literature on pter-ygium is abundant and almost from thebeginning the emphasis has been placed onits location on the nasal side.Squamous cell neoplasia of the conjunctiva
is relatively uncommon and can masqueradeas common, but less significant, ocular sur-face conditions including pterygium orchronic blepharoconjunctivitis. We present acase of intraepithelial neoplasia, initiallydiagnosed as inflamed pterygium.
Case reportA 77 year old man, who had worked on therailways, presented with a 3 week history ofredness on the outer aspect of the left eye. Nohistory of associated pain, discharge, orwatering was elicited.His medical history included hypertension
and hypercholesterolaemia under treatment.Best corrected visual acuity in each eye was
6/5. On inspection of the anterior segment,the left temporal conjunctiva showed a fleshytissue encroaching on the temporal periph-eral cornea (fig 1). The peripheral corneashowed an elevated ridge with punctatestaining. The overlying conjunctiva wasinjected. The rest of the ocular examinationwas within normal limits.A provisional diagnosis of inflamed pter-
ygium of left eye was made and the patientwas commenced on prednisolone 0.5% eyedrops at this stage with advice to review in2 weeks’ time.On follow up no significant change was
noticed in the lesion. On further inquiry thepatient gave a history of injury to left eyewith hot ashes many years earlier. In view of
the atypical location and the appearance ofthe lesion, we did an excision biopsy ofthe conjunctival and corneal lesion.Histopathology revealed an irregular epithe-lial thickening associated with dyskeratosisand full thickness dysplasia. Numerous mito-tic figures, some atypical, were presentthroughout the epithelium (fig 2). A diag-nosis of conjunctival intraepithelial neoplasiawas made. Although no unequivocal evidenceof invasion was seen in the multiple sectionsexamined, fragmentation of the tissue duringprocessing precluded confirmation of com-plete excision.The patient was referred for further treat-
ment to an ocular oncologist and underwentruthenium plaque therapy followed by topical5-fluorouracil treatment.
CommentTemporal pterygium is reported, althoughDolezalova found only one case of unilateraltemporal pterygium out of 1388 Arab patientswith pterygia.2 We would therefore considerthis case to be atypical.The role of pterygium in the development
of ocular surface squamous neoplasia isunclear.3 Both conditions have a strongassociation with exposure to ultraviolet-Bradiation. Sevel and Sealy’s study of 12squamous cell carcinoma and 17 carcinomain situ arising in 100 pterygia found that itcan be difficult to distinguish a ‘‘reactivepterygium’’ from carcinoma in situ andmalignant change should be considered in apterygium if there is unusual evidence ofinvasion, extension, or if the lesion becomesparticularly vascular.4
To our knowledge, the last reported case oftemporal pterygium was in the 1970s.2 5 Wepresent this case to refresh the memory andto highlight the importance of keeping anindex of suspicion for squamous cell neopla-sia in any atypical presentation of the moreAccepted for publication 20 June 2005
Figure 1 Left eye showing presence of a softtissue lesion on the temporal conjunctivaencroaching on the limbus before local excisionand radiotherapy.
Figure 2 Section through the conjunctivastained with haematoxylin and eosin. The mainfigure demonstrates grossly and irregularlythickened, dysplastic epithelium (Ep; scale bar,100 mm). The inserts show an atypical mitosis(above, arrow) and dyskeratosis (below,arrowhead) within the epithelium.
PostScript 1533
www.bjophthalmol.com
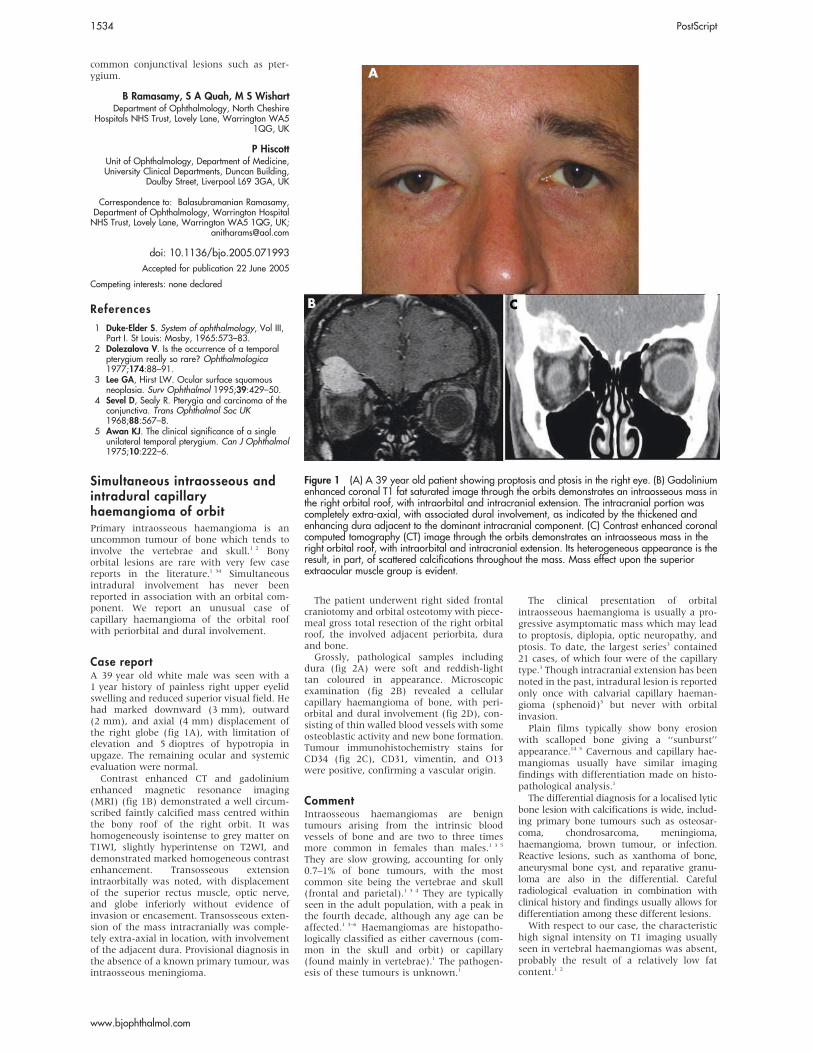
common conjunctival lesions such as pter-ygium.
B Ramasamy, S A Quah, M S WishartDepartment of Ophthalmology, North Cheshire
Hospitals NHS Trust, Lovely Lane, Warrington WA51QG, UK
P HiscottUnit of Ophthalmology, Department of Medicine,University Clinical Departments, Duncan Building,
Daulby Street, Liverpool L69 3GA, UK
Correspondence to: Balasubramanian Ramasamy,Department of Ophthalmology, Warrington HospitalNHS Trust, Lovely Lane, Warrington WA5 1QG, UK;
doi: 10.1136/bjo.2005.071993
References
1 Duke-Elder S. System of ophthalmology, Vol III,Part I. St Louis: Mosby, 1965:573–83.
2 Dolezalova V. Is the occurrence of a temporalpterygium really so rare? Ophthalmologica1977;174:88–91.
3 Lee GA, Hirst LW. Ocular surface squamousneoplasia. Surv Ophthalmol 1995;39:429–50.
4 Sevel D, Sealy R. Pterygia and carcinoma of theconjunctiva. Trans Ophthalmol Soc UK1968;88:567–8.
5 Awan KJ. The clinical significance of a singleunilateral temporal pterygium. Can J Ophthalmol1975;10:222–6.
Simultaneous intraosseous andintradural capillaryhaemangioma of orbitPrimary intraosseous haemangioma is anuncommon tumour of bone which tends toinvolve the vertebrae and skull.1 2 Bonyorbital lesions are rare with very few casereports in the literature.1 34 Simultaneousintradural involvement has never beenreported in association with an orbital com-ponent. We report an unusual case ofcapillary haemangioma of the orbital roofwith periorbital and dural involvement.
Case reportA 39 year old white male was seen with a1 year history of painless right upper eyelidswelling and reduced superior visual field. Hehad marked downward (3 mm), outward(2 mm), and axial (4 mm) displacement ofthe right globe (fig 1A), with limitation ofelevation and 5 dioptres of hypotropia inupgaze. The remaining ocular and systemicevaluation were normal.Contrast enhanced CT and gadolinium
enhanced magnetic resonance imaging(MRI) (fig 1B) demonstrated a well circum-scribed faintly calcified mass centred withinthe bony roof of the right orbit. It washomogeneously isointense to grey matter onT1WI, slightly hyperintense on T2WI, anddemonstrated marked homogeneous contrastenhancement. Transosseous extensionintraorbitally was noted, with displacementof the superior rectus muscle, optic nerve,and globe inferiorly without evidence ofinvasion or encasement. Transosseous exten-sion of the mass intracranially was comple-tely extra-axial in location, with involvementof the adjacent dura. Provisional diagnosis inthe absence of a known primary tumour, wasintraosseous meningioma.
The patient underwent right sided frontalcraniotomy and orbital osteotomy with piece-meal gross total resection of the right orbitalroof, the involved adjacent periorbita, duraand bone.Grossly, pathological samples including
dura (fig 2A) were soft and reddish-lighttan coloured in appearance. Microscopicexamination (fig 2B) revealed a cellularcapillary haemangioma of bone, with peri-orbital and dural involvement (fig 2D), con-sisting of thin walled blood vessels with someosteoblastic activity and new bone formation.Tumour immunohistochemistry stains forCD34 (fig 2C), CD31, vimentin, and O13were positive, confirming a vascular origin.
CommentIntraosseous haemangiomas are benigntumours arising from the intrinsic bloodvessels of bone and are two to three timesmore common in females than males.1 3 5
They are slow growing, accounting for only0.7–1% of bone tumours, with the mostcommon site being the vertebrae and skull(frontal and parietal).1 3 4 They are typicallyseen in the adult population, with a peak inthe fourth decade, although any age can beaffected.1 3–6 Haemangiomas are histopatho-logically classified as either cavernous (com-mon in the skull and orbit) or capillary(found mainly in vertebrae).1 The pathogen-esis of these tumours is unknown.1
The clinical presentation of orbitalintraosseous haemangioma is usually a pro-gressive asymptomatic mass which may leadto proptosis, diplopia, optic neuropathy, andptosis. To date, the largest series3 contained21 cases, of which four were of the capillarytype.3 Though intracranial extension has beennoted in the past, intradural lesion is reportedonly once with calvarial capillary haeman-gioma (sphenoid)5 but never with orbitalinvasion.Plain films typically show bony erosion
with scalloped bone giving a ‘‘sunburst’’appearance.14 5 Cavernous and capillary hae-mangiomas usually have similar imagingfindings with differentiation made on histo-pathological analysis.1
The differential diagnosis for a localised lyticbone lesion with calcifications is wide, includ-ing primary bone tumours such as osteosar-coma, chondrosarcoma, meningioma,haemangioma, brown tumour, or infection.Reactive lesions, such as xanthoma of bone,aneurysmal bone cyst, and reparative granu-loma are also in the differential. Carefulradiological evaluation in combination withclinical history and findings usually allows fordifferentiation among these different lesions.With respect to our case, the characteristic
high signal intensity on T1 imaging usuallyseen in vertebral haemangiomas was absent,probably the result of a relatively low fatcontent.1 2
Accepted for publication 22 June 2005
Competing interests: none declared
Figure 1 (A) A 39 year old patient showing proptosis and ptosis in the right eye. (B) Gadoliniumenhanced coronal T1 fat saturated image through the orbits demonstrates an intraosseous mass inthe right orbital roof, with intraorbital and intracranial extension. The intracranial portion wascompletely extra-axial, with associated dural involvement, as indicated by the thickened andenhancing dura adjacent to the dominant intracranial component. (C) Contrast enhanced coronalcomputed tomography (CT) image through the orbits demonstrates an intraosseous mass in theright orbital roof, with intraorbital and intracranial extension. Its heterogeneous appearance is theresult, in part, of scattered calcifications throughout the mass. Mass effect upon the superiorextraocular muscle group is evident.
1534 PostScript
www.bjophthalmol.com
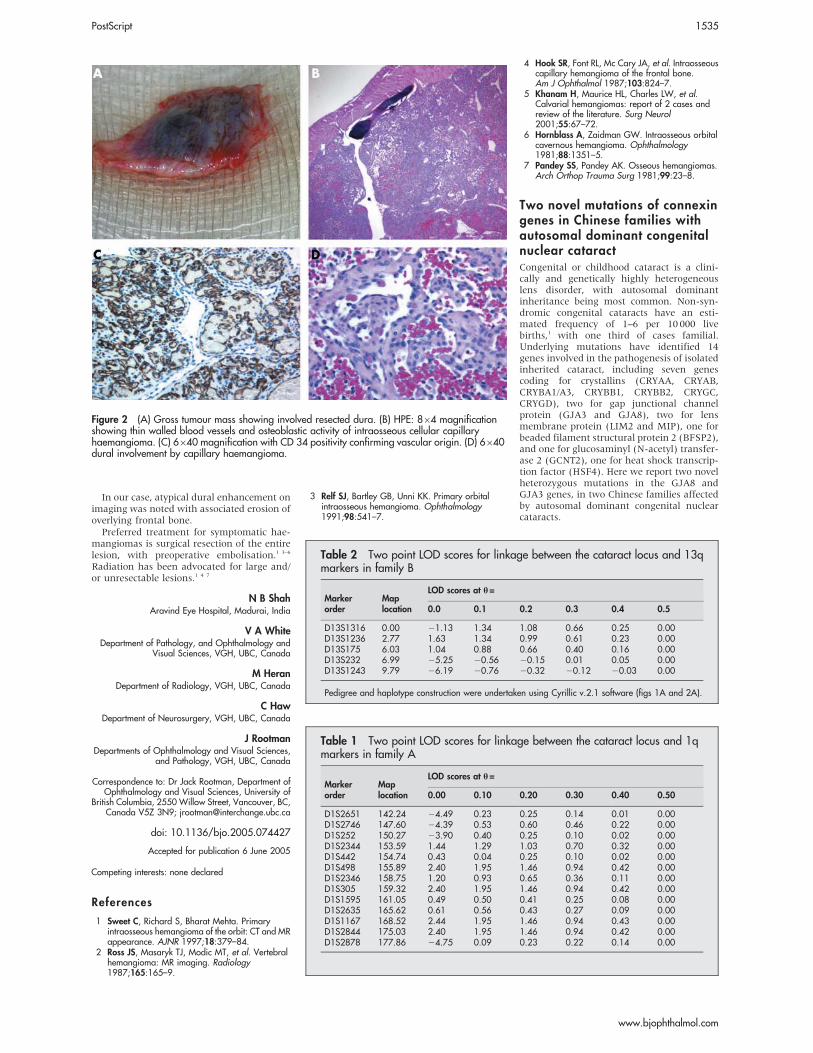
In our case, atypical dural enhancement onimaging was noted with associated erosion ofoverlying frontal bone.Preferred treatment for symptomatic hae-
mangiomas is surgical resection of the entirelesion, with preoperative embolisation.1 3–6
Radiation has been advocated for large and/or unresectable lesions.1 4 7
N B ShahAravind Eye Hospital, Madurai, India
V A WhiteDepartment of Pathology, and Ophthalmology and
Visual Sciences, VGH, UBC, Canada
M HeranDepartment of Radiology, VGH, UBC, Canada
C HawDepartment of Neurosurgery, VGH, UBC, Canada
J RootmanDepartments of Ophthalmology and Visual Sciences,
and Pathology, VGH, UBC, Canada
Correspondence to: Dr Jack Rootman, Department ofOphthalmology and Visual Sciences, University of
British Columbia, 2550 Willow Street, Vancouver, BC,Canada V5Z 3N9; [email protected]
doi: 10.1136/bjo.2005.074427
References
1 Sweet C, Richard S, Bharat Mehta. Primaryintraosseous hemangioma of the orbit: CT and MRappearance. AJNR 1997;18:379–84.
2 Ross JS, Masaryk TJ, Modic MT, et al. Vertebralhemangioma: MR imaging. Radiology1987;165:165–9.
3 Relf SJ, Bartley GB, Unni KK. Primary orbitalintraosseous hemangioma. Ophthalmology1991;98:541–7.
4 Hook SR, Font RL, Mc Cary JA, et al. Intraosseouscapillary hemangioma of the frontal bone.Am J Ophthalmol 1987;103:824–7.
5 Khanam H, Maurice HL, Charles LW, et al.Calvarial hemangiomas: report of 2 cases andreview of the literature. Surg Neurol2001;55:67–72.
6 Hornblass A, Zaidman GW. Intraosseous orbitalcavernous hemangioma. Ophthalmology1981;88:1351–5.
7 Pandey SS, Pandey AK. Osseous hemangiomas.Arch Orthop Trauma Surg 1981;99:23–8.
Two novel mutations of connexingenes in Chinese families withautosomal dominant congenitalnuclear cataractCongenital or childhood cataract is a clini-cally and genetically highly heterogeneouslens disorder, with autosomal dominantinheritance being most common. Non-syn-dromic congenital cataracts have an esti-mated frequency of 1–6 per 10 000 livebirths,1 with one third of cases familial.Underlying mutations have identified 14genes involved in the pathogenesis of isolatedinherited cataract, including seven genescoding for crystallins (CRYAA, CRYAB,CRYBA1/A3, CRYBB1, CRYBB2, CRYGC,CRYGD), two for gap junctional channelprotein (GJA3 and GJA8), two for lensmembrane protein (LIM2 and MIP), one forbeaded filament structural protein 2 (BFSP2),and one for glucosaminyl (N-acetyl) transfer-ase 2 (GCNT2), one for heat shock transcrip-tion factor (HSF4). Here we report two novelheterozygous mutations in the GJA8 andGJA3 genes, in two Chinese families affectedby autosomal dominant congenital nuclearcataracts.
Figure 2 (A) Gross tumour mass showing involved resected dura. (B) HPE: 864 magnificationshowing thin walled blood vessels and osteoblastic activity of intraosseous cellular capillaryhaemangioma. (C) 6640 magnification with CD 34 positivity confirming vascular origin. (D) 6640dural involvement by capillary haemangioma.
Accepted for publication 6 June 2005
Competing interests: none declared
Table 1 Two point LOD scores for linkage between the cataract locus and 1qmarkers in family A
Markerorder
Maplocation
LOD scores at h=
0.00 0.10 0.20 0.30 0.40 0.50
D1S2651 142.24 24.49 0.23 0.25 0.14 0.01 0.00D1S2746 147.60 24.39 0.53 0.60 0.46 0.22 0.00D1S252 150.27 23.90 0.40 0.25 0.10 0.02 0.00D1S2344 153.59 1.44 1.29 1.03 0.70 0.32 0.00D1S442 154.74 0.43 0.04 0.25 0.10 0.02 0.00D1S498 155.89 2.40 1.95 1.46 0.94 0.42 0.00D1S2346 158.75 1.20 0.93 0.65 0.36 0.11 0.00D1S305 159.32 2.40 1.95 1.46 0.94 0.42 0.00D1S1595 161.05 0.49 0.50 0.41 0.25 0.08 0.00D1S2635 165.62 0.61 0.56 0.43 0.27 0.09 0.00D1S1167 168.52 2.44 1.95 1.46 0.94 0.43 0.00D1S2844 175.03 2.40 1.95 1.46 0.94 0.42 0.00D1S2878 177.86 24.75 0.09 0.23 0.22 0.14 0.00
Table 2 Two point LOD scores for linkage between the cataract locus and 13qmarkers in family B
Markerorder
Maplocation
LOD scores at h=
0.0 0.1 0.2 0.3 0.4 0.5
D13S1316 0.00 21.13 1.34 1.08 0.66 0.25 0.00D13S1236 2.77 1.63 1.34 0.99 0.61 0.23 0.00D13S175 6.03 1.04 0.88 0.66 0.40 0.16 0.00D13S232 6.99 25.25 20.56 20.15 0.01 0.05 0.00D13S1243 9.79 26.19 20.76 20.32 20.12 20.03 0.00
Pedigree and haplotype construction were undertaken using Cyrillic v.2.1 software (figs 1A and 2A).
PostScript 1535
www.bjophthalmol.com
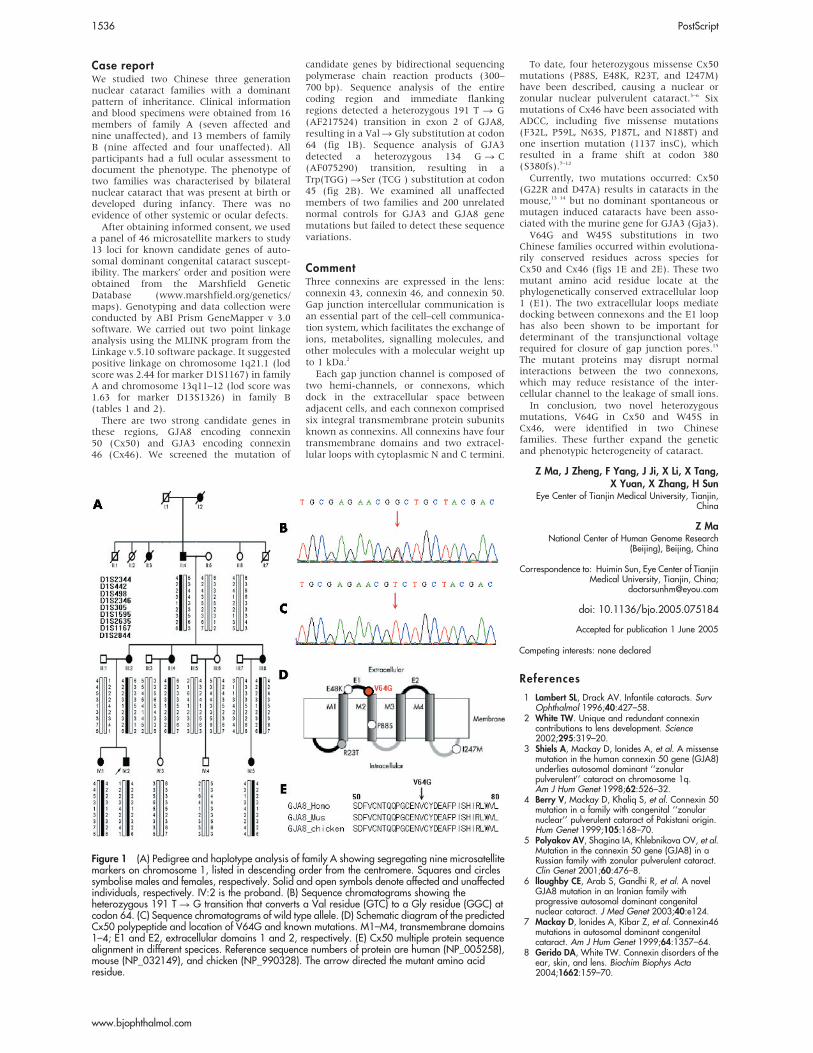
Case reportWe studied two Chinese three generationnuclear cataract families with a dominantpattern of inheritance. Clinical informationand blood specimens were obtained from 16members of family A (seven affected andnine unaffected), and 13 members of familyB (nine affected and four unaffected). Allparticipants had a full ocular assessment todocument the phenotype. The phenotype oftwo families was characterised by bilateralnuclear cataract that was present at birth ordeveloped during infancy. There was noevidence of other systemic or ocular defects.After obtaining informed consent, we used
a panel of 46 microsatellite markers to study13 loci for known candidate genes of auto-somal dominant congenital cataract suscept-ibility. The markers’ order and position wereobtained from the Marshfield GeneticDatabase (www.marshfield.org/genetics/maps). Genotyping and data collection wereconducted by ABI Prism GeneMapper v 3.0software. We carried out two point linkageanalysis using the MLINK program from theLinkage v.5.10 software package. It suggestedpositive linkage on chromosome 1q21.1 (lodscore was 2.44 for marker D1S1167) in familyA and chromosome 13q11–12 (lod score was1.63 for marker D13S1326) in family B(tables 1 and 2).There are two strong candidate genes in
these regions, GJA8 encoding connexin50 (Cx50) and GJA3 encoding connexin46 (Cx46). We screened the mutation of
candidate genes by bidirectional sequencingpolymerase chain reaction products (300–700 bp). Sequence analysis of the entirecoding region and immediate flankingregions detected a heterozygous 191 T R G(AF217524) transition in exon 2 of GJA8,resulting in a ValR Gly substitution at codon64 (fig 1B). Sequence analysis of GJA3detected a heterozygous 134 G R C(AF075290) transition, resulting in aTrp(TGG) RSer (TCG ) substitution at codon45 (fig 2B). We examined all unaffectedmembers of two families and 200 unrelatednormal controls for GJA3 and GJA8 genemutations but failed to detect these sequencevariations.
CommentThree connexins are expressed in the lens:connexin 43, connexin 46, and connexin 50.Gap junction intercellular communication isan essential part of the cell–cell communica-tion system, which facilitates the exchange ofions, metabolites, signalling molecules, andother molecules with a molecular weight upto 1 kDa.2
Each gap junction channel is composed oftwo hemi-channels, or connexons, whichdock in the extracellular space betweenadjacent cells, and each connexon comprisedsix integral transmembrane protein subunitsknown as connexins. All connexins have fourtransmembrane domains and two extracel-lular loops with cytoplasmic N and C termini.
To date, four heterozygous missense Cx50mutations (P88S, E48K, R23T, and I247M)have been described, causing a nuclear orzonular nuclear pulverulent cataract.3–6 Sixmutations of Cx46 have been associated withADCC, including five missense mutations(F32L, P59L, N63S, P187L, and N188T) andone insertion mutation (1137 insC), whichresulted in a frame shift at codon 380(S380fs).7–12
Currently, two mutations occurred: Cx50(G22R and D47A) results in cataracts in themouse,13 14 but no dominant spontaneous ormutagen induced cataracts have been asso-ciated with the murine gene for GJA3 (Gja3).V64G and W45S substitutions in two
Chinese families occurred within evolutiona-rily conserved residues across species forCx50 and Cx46 (figs 1E and 2E). These twomutant amino acid residue locate at thephylogenetically conserved extracellular loop1 (E1). The two extracellular loops mediatedocking between connexons and the E1 loophas also been shown to be important fordeterminant of the transjunctional voltagerequired for closure of gap junction pores.15
The mutant proteins may disrupt normalinteractions between the two connexons,which may reduce resistance of the inter-cellular channel to the leakage of small ions.In conclusion, two novel heterozygous
mutations, V64G in Cx50 and W45S inCx46, were identified in two Chinesefamilies. These further expand the geneticand phenotypic heterogeneity of cataract.
Z Ma, J Zheng, F Yang, J Ji, X Li, X Tang,X Yuan, X Zhang, H Sun
Eye Center of Tianjin Medical University, Tianjin,China
Z MaNational Center of Human Genome Research
(Beijing), Beijing, China
Correspondence to: Huimin Sun, Eye Center of TianjinMedical University, Tianjin, China;
doi: 10.1136/bjo.2005.075184
References
1 Lambert SL, Drack AV. Infantile cataracts. SurvOphthalmol 1996;40:427–58.
2 White TW. Unique and redundant connexincontributions to lens development. Science2002;295:319–20.
3 Shiels A, Mackay D, Ionides A, et al. A missensemutation in the human connexin 50 gene (GJA8)underlies autosomal dominant ‘‘zonularpulverulent’’ cataract on chromosome 1q.Am J Hum Genet 1998;62:526–32.
4 Berry V, Mackay D, Khaliq S, et al. Connexin 50mutation in a family with congenital ‘‘zonularnuclear’’ pulverulent cataract of Pakistani origin.Hum Genet 1999;105:168–70.
5 Polyakov AV, Shagina IA, Khlebnikova OV, et al.Mutation in the connexin 50 gene (GJA8) in aRussian family with zonular pulverulent cataract.Clin Genet 2001;60:476–8.
6 lloughby CE, Arab S, Gandhi R, et al. A novelGJA8 mutation in an Iranian family withprogressive autosomal dominant congenitalnuclear cataract. J Med Genet 2003;40:e124.
7 Mackay D, Ionides A, Kibar Z, et al. Connexin46mutations in autosomal dominant congenitalcataract. Am J Hum Genet 1999;64:1357–64.
8 Gerido DA, White TW. Connexin disorders of theear, skin, and lens. Biochim Biophys Acta2004;1662:159–70.
Figure 1 (A) Pedigree and haplotype analysis of family A showing segregating nine microsatellitemarkers on chromosome 1, listed in descending order from the centromere. Squares and circlessymbolise males and females, respectively. Solid and open symbols denote affected and unaffectedindividuals, respectively. IV:2 is the proband. (B) Sequence chromatograms showing theheterozygous 191 T R G transition that converts a Val residue (GTC) to a Gly residue (GGC) atcodon 64. (C) Sequence chromatograms of wild type allele. (D) Schematic diagram of the predictedCx50 polypeptide and location of V64G and known mutations. M1–M4, transmembrane domains1–4; E1 and E2, extracellular domains 1 and 2, respectively. (E) Cx50 multiple protein sequencealignment in different specices. Reference sequence numbers of protein are human (NP_005258),mouse (NP_032149), and chicken (NP_990328). The arrow directed the mutant amino acidresidue.
Accepted for publication 1 June 2005
Competing interests: none declared
1536 PostScript
www.bjophthalmol.com
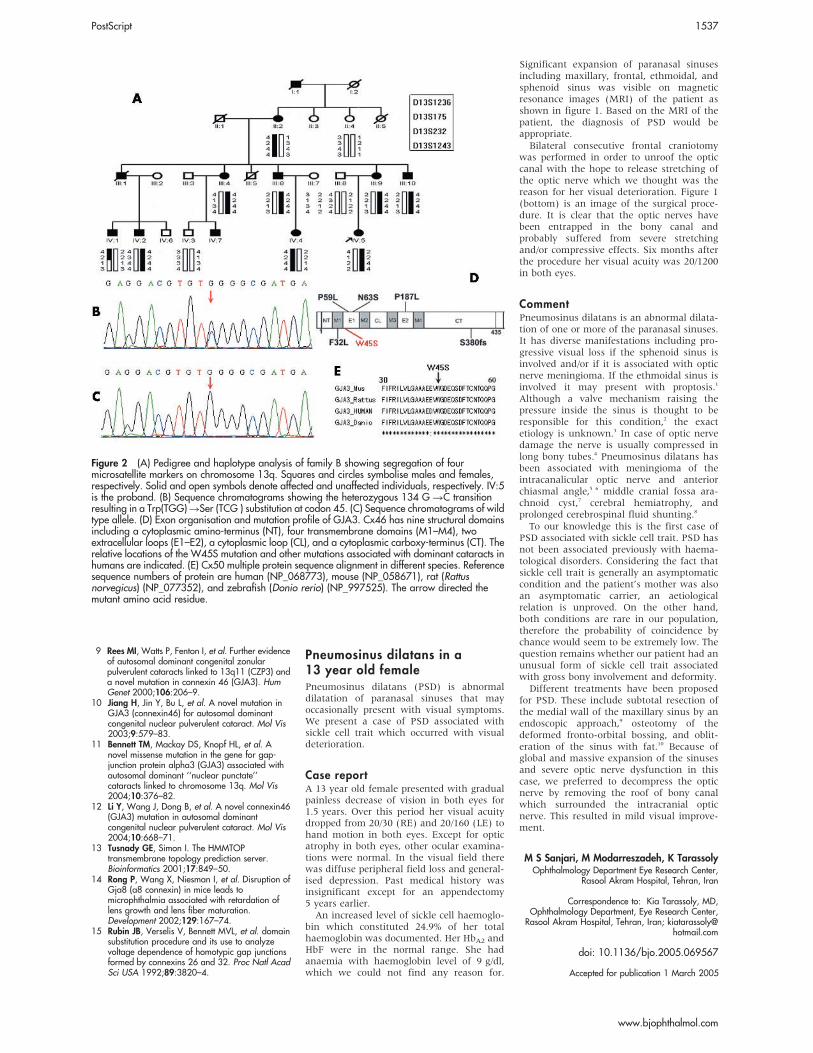
9 Rees MI, Watts P, Fenton I, et al. Further evidenceof autosomal dominant congenital zonularpulverulent cataracts linked to 13q11 (CZP3) anda novel mutation in connexin 46 (GJA3). HumGenet 2000;106:206–9.
10 Jiang H, Jin Y, Bu L, et al. A novel mutation inGJA3 (connexin46) for autosomal dominantcongenital nuclear pulverulent cataract. Mol Vis2003;9:579–83.
11 Bennett TM, Mackay DS, Knopf HL, et al. Anovel missense mutation in the gene for gap-junction protein alpha3 (GJA3) associated withautosomal dominant ‘‘nuclear punctate’’cataracts linked to chromosome 13q. Mol Vis2004;10:376–82.
12 Li Y, Wang J, Dong B, et al. A novel connexin46(GJA3) mutation in autosomal dominantcongenital nuclear pulverulent cataract. Mol Vis2004;10:668–71.
13 Tusnady GE, Simon I. The HMMTOPtransmembrane topology prediction server.Bioinformatics 2001;17:849–50.
14 Rong P, Wang X, Niesman I, et al. Disruption ofGja8 (a8 connexin) in mice leads tomicrophthalmia associated with retardation oflens growth and lens fiber maturation.Development 2002;129:167–74.
15 Rubin JB, Verselis V, Bennett MVL, et al. domainsubstitution procedure and its use to analyzevoltage dependence of homotypic gap junctionsformed by connexins 26 and 32. Proc Natl AcadSci USA 1992;89:3820–4.
Pneumosinus dilatans in a13 year old femalePneumosinus dilatans (PSD) is abnormaldilatation of paranasal sinuses that mayoccasionally present with visual symptoms.We present a case of PSD associated withsickle cell trait which occurred with visualdeterioration.
Case reportA 13 year old female presented with gradualpainless decrease of vision in both eyes for1.5 years. Over this period her visual acuitydropped from 20/30 (RE) and 20/160 (LE) tohand motion in both eyes. Except for opticatrophy in both eyes, other ocular examina-tions were normal. In the visual field therewas diffuse peripheral field loss and general-ised depression. Past medical history wasinsignificant except for an appendectomy5 years earlier.An increased level of sickle cell haemoglo-
bin which constituted 24.9% of her totalhaemoglobin was documented. Her HbA2 andHbF were in the normal range. She hadanaemia with haemoglobin level of 9 g/dl,which we could not find any reason for.
Significant expansion of paranasal sinusesincluding maxillary, frontal, ethmoidal, andsphenoid sinus was visible on magneticresonance images (MRI) of the patient asshown in figure 1. Based on the MRI of thepatient, the diagnosis of PSD would beappropriate.Bilateral consecutive frontal craniotomy
was performed in order to unroof the opticcanal with the hope to release stretching ofthe optic nerve which we thought was thereason for her visual deterioration. Figure 1(bottom) is an image of the surgical proce-dure. It is clear that the optic nerves havebeen entrapped in the bony canal andprobably suffered from severe stretchingand/or compressive effects. Six months afterthe procedure her visual acuity was 20/1200in both eyes.
CommentPneumosinus dilatans is an abnormal dilata-tion of one or more of the paranasal sinuses.It has diverse manifestations including pro-gressive visual loss if the sphenoid sinus isinvolved and/or if it is associated with opticnerve meningioma. If the ethmoidal sinus isinvolved it may present with proptosis.1
Although a valve mechanism raising thepressure inside the sinus is thought to beresponsible for this condition,2 the exactetiology is unknown.3 In case of optic nervedamage the nerve is usually compressed inlong bony tubes.4 Pneumosinus dilatans hasbeen associated with meningioma of theintracanalicular optic nerve and anteriorchiasmal angle,5 6 middle cranial fossa ara-chnoid cyst,7 cerebral hemiatrophy, andprolonged cerebrospinal fluid shunting.8
To our knowledge this is the first case ofPSD associated with sickle cell trait. PSD hasnot been associated previously with haema-tological disorders. Considering the fact thatsickle cell trait is generally an asymptomaticcondition and the patient’s mother was alsoan asymptomatic carrier, an aetiologicalrelation is unproved. On the other hand,both conditions are rare in our population,therefore the probability of coincidence bychance would seem to be extremely low. Thequestion remains whether our patient had anunusual form of sickle cell trait associatedwith gross bony involvement and deformity.Different treatments have been proposed
for PSD. These include subtotal resection ofthe medial wall of the maxillary sinus by anendoscopic approach,9 osteotomy of thedeformed fronto-orbital bossing, and oblit-eration of the sinus with fat.10 Because ofglobal and massive expansion of the sinusesand severe optic nerve dysfunction in thiscase, we preferred to decompress the opticnerve by removing the roof of bony canalwhich surrounded the intracranial opticnerve. This resulted in mild visual improve-ment.
M S Sanjari, M Modarreszadeh, K TarassolyOphthalmology Department Eye Research Center,
Rasool Akram Hospital, Tehran, Iran
Correspondence to: Kia Tarassoly, MD,Ophthalmology Department, Eye Research Center,
Rasool Akram Hospital, Tehran, Iran; [email protected]
doi: 10.1136/bjo.2005.069567
Figure 2 (A) Pedigree and haplotype analysis of family B showing segregation of fourmicrosatellite markers on chromosome 13q. Squares and circles symbolise males and females,respectively. Solid and open symbols denote affected and unaffected individuals, respectively. IV:5is the proband. (B) Sequence chromatograms showing the heterozygous 134 G RC transitionresulting in a Trp(TGG)RSer (TCG ) substitution at codon 45. (C) Sequence chromatograms of wildtype allele. (D) Exon organisation and mutation profile of GJA3. Cx46 has nine structural domainsincluding a cytoplasmic amino-terminus (NT), four transmembrane domains (M1–M4), twoextracellular loops (E1–E2), a cytoplasmic loop (CL), and a cytoplasmic carboxy-terminus (CT). Therelative locations of the W45S mutation and other mutations associated with dominant cataracts inhumans are indicated. (E) Cx50 multiple protein sequence alignment in different species. Referencesequence numbers of protein are human (NP_068773), mouse (NP_058671), rat (Rattusnorvegicus) (NP_077352), and zebrafish (Donio rerio) (NP_997525). The arrow directed themutant amino acid residue.
Accepted for publication 1 March 2005
PostScript 1537
www.bjophthalmol.com
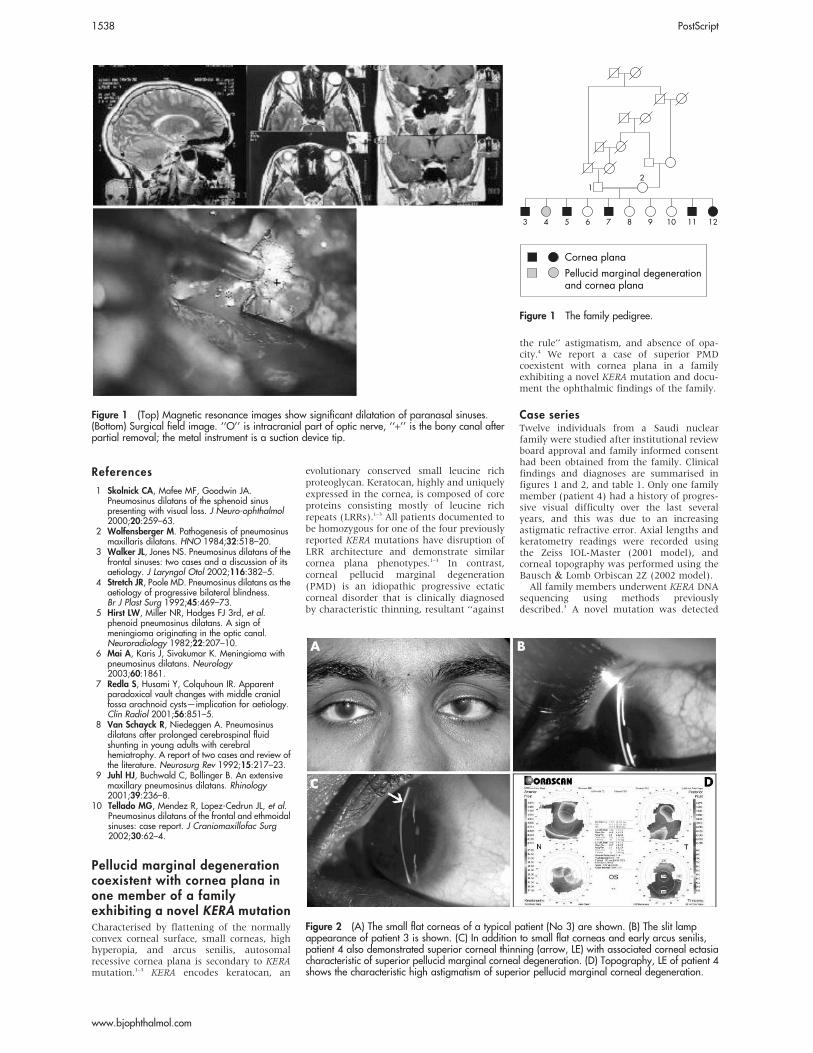
References
1 Skolnick CA, Mafee MF, Goodwin JA.Pneumosinus dilatans of the sphenoid sinuspresenting with visual loss. J Neuro-ophthalmol2000;20:259–63.
2 Wolfensberger M. Pathogenesis of pneumosinusmaxillaris dilatans. HNO 1984;32:518–20.
3 Walker JL, Jones NS. Pneumosinus dilatans of thefrontal sinuses: two cases and a discussion of itsaetiology. J Laryngol Otol 2002;116:382–5.
4 Stretch JR, Poole MD. Pneumosinus dilatans as theaetiology of progressive bilateral blindness.Br J Plast Surg 1992;45:469–73.
5 Hirst LW, Miller NR, Hodges FJ 3rd, et al.phenoid pneumosinus dilatans. A sign ofmeningioma originating in the optic canal.Neuroradiology 1982;22:207–10.
6 Mai A, Karis J, Sivakumar K. Meningioma withpneumosinus dilatans. Neurology2003;60:1861.
7 Redla S, Husami Y, Colquhoun IR. Apparentparadoxical vault changes with middle cranialfossa arachnoid cysts—implication for aetiology.Clin Radiol 2001;56:851–5.
8 Van Schayck R, Niedeggen A. Pneumosinusdilatans after prolonged cerebrospinal fluidshunting in young adults with cerebralhemiatrophy. A report of two cases and review ofthe literature. Neurosurg Rev 1992;15:217–23.
9 Juhl HJ, Buchwald C, Bollinger B. An extensivemaxillary pneumosinus dilatans. Rhinology2001;39:236–8.
10 Tellado MG, Mendez R, Lopez-Cedrun JL, et al.Pneumosinus dilatans of the frontal and ethmoidalsinuses: case report. J Craniomaxillofac Surg2002;30:62–4.
Pellucid marginal degenerationcoexistent with cornea plana inone member of a familyexhibiting a novel KERA mutationCharacterised by flattening of the normallyconvex corneal surface, small corneas, highhyperopia, and arcus senilis, autosomalrecessive cornea plana is secondary to KERAmutation.1–3 KERA encodes keratocan, an
evolutionary conserved small leucine richproteoglycan. Keratocan, highly and uniquelyexpressed in the cornea, is composed of coreproteins consisting mostly of leucine richrepeats (LRRs).1–3 All patients documented tobe homozygous for one of the four previouslyreported KERA mutations have disruption ofLRR architecture and demonstrate similarcornea plana phenotypes.1–3 In contrast,corneal pellucid marginal degeneration(PMD) is an idiopathic progressive ectaticcorneal disorder that is clinically diagnosedby characteristic thinning, resultant ‘‘against
the rule’’ astigmatism, and absence of opa-city.4 We report a case of superior PMDcoexistent with cornea plana in a familyexhibiting a novel KERA mutation and docu-ment the ophthalmic findings of the family.
Case seriesTwelve individuals from a Saudi nuclearfamily were studied after institutional reviewboard approval and family informed consenthad been obtained from the family. Clinicalfindings and diagnoses are summarised infigures 1 and 2, and table 1. Only one familymember (patient 4) had a history of progres-sive visual difficulty over the last severalyears, and this was due to an increasingastigmatic refractive error. Axial lengths andkeratometry readings were recorded usingthe Zeiss IOL-Master (2001 model), andcorneal topography was performed using theBausch & Lomb Orbiscan 2Z (2002 model).All family members underwent KERA DNA
sequencing using methods previouslydescribed.3 A novel mutation was detected
Figure 1 (Top) Magnetic resonance images show significant dilatation of paranasal sinuses.(Bottom) Surgical field image. ‘‘O’’ is intracranial part of optic nerve, ‘‘+’’ is the bony canal afterpartial removal; the metal instrument is a suction device tip.
Cornea planaPellucid marginal degenerationand cornea plana
11
21
753 12109864
Figure 1 The family pedigree.
Figure 2 (A) The small flat corneas of a typical patient (No 3) are shown. (B) The slit lampappearance of patient 3 is shown. (C) In addition to small flat corneas and early arcus senilis,patient 4 also demonstrated superior corneal thinning (arrow, LE) with associated corneal ectasiacharacteristic of superior pellucid marginal corneal degeneration. (D) Topography, LE of patient 4shows the characteristic high astigmatism of superior pellucid marginal corneal degeneration.
1538 PostScript
www.bjophthalmol.com
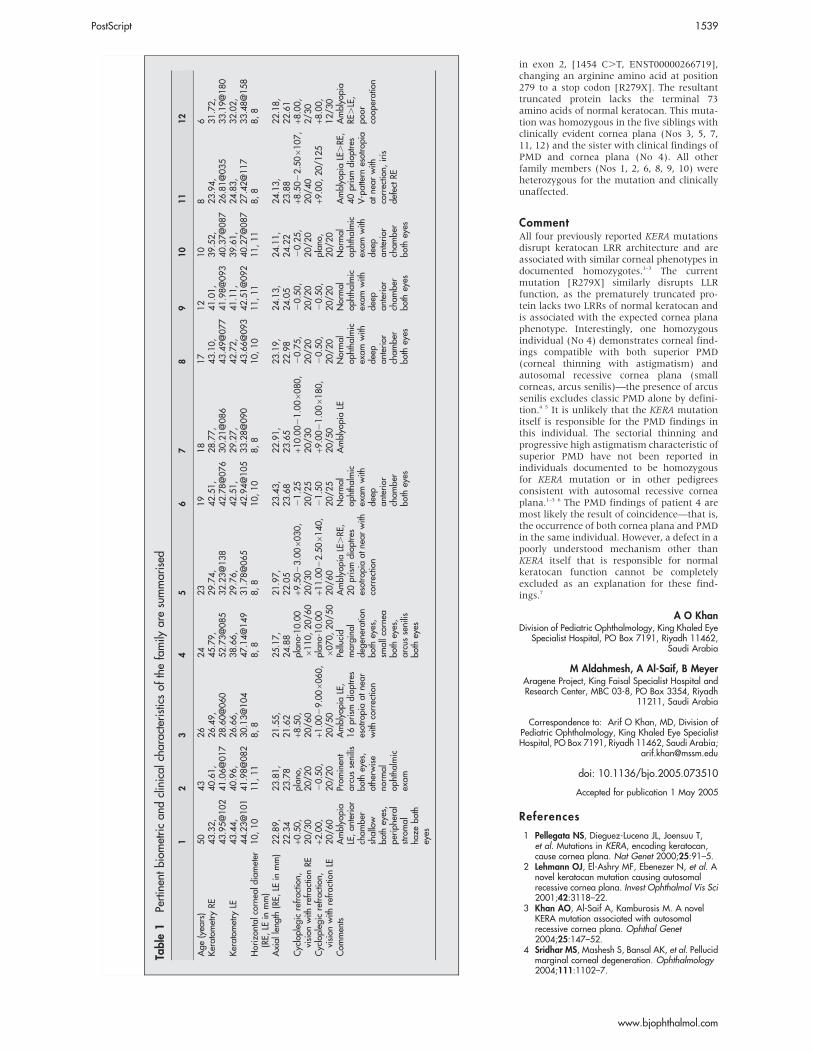
in exon 2, [1454 C.T, ENST00000266719],changing an arginine amino acid at position279 to a stop codon [R279X]. The resultanttruncated protein lacks the terminal 73amino acids of normal keratocan. This muta-tion was homozygous in the five siblings withclinically evident cornea plana (Nos 3, 5, 7,11, 12) and the sister with clinical findings ofPMD and cornea plana (No 4). All otherfamily members (Nos 1, 2, 6, 8, 9, 10) wereheterozygous for the mutation and clinicallyunaffected.
CommentAll four previously reported KERA mutationsdisrupt keratocan LRR architecture and areassociated with similar corneal phenotypes indocumented homozygotes.1–3 The currentmutation [R279X] similarly disrupts LLRfunction, as the prematurely truncated pro-tein lacks two LRRs of normal keratocan andis associated with the expected cornea planaphenotype. Interestingly, one homozygousindividual (No 4) demonstrates corneal find-ings compatible with both superior PMD(corneal thinning with astigmatism) andautosomal recessive cornea plana (smallcorneas, arcus senilis)—the presence of arcussenilis excludes classic PMD alone by defini-tion.4 5 It is unlikely that the KERA mutationitself is responsible for the PMD findings inthis individual. The sectorial thinning andprogressive high astigmatism characteristic ofsuperior PMD have not been reported inindividuals documented to be homozygousfor KERA mutation or in other pedigreesconsistent with autosomal recessive corneaplana.1–3 6 The PMD findings of patient 4 aremost likely the result of coincidence—that is,the occurrence of both cornea plana and PMDin the same individual. However, a defect in apoorly understood mechanism other thanKERA itself that is responsible for normalkeratocan function cannot be completelyexcluded as an explanation for these find-ings.7
A O KhanDivision of Pediatric Ophthalmology, King Khaled Eye
Specialist Hospital, PO Box 7191, Riyadh 11462,Saudi Arabia
M Aldahmesh, A Al-Saif, B MeyerAragene Project, King Faisal Specialist Hospital andResearch Center, MBC 03-8, PO Box 3354, Riyadh
11211, Saudi Arabia
Correspondence to: Arif O Khan, MD, Division ofPediatric Ophthalmology, King Khaled Eye SpecialistHospital, PO Box 7191, Riyadh 11462, Saudi Arabia;
doi: 10.1136/bjo.2005.073510
References
1 Pellegata NS, Dieguez-Lucena JL, Joensuu T,et al. Mutations in KERA, encoding keratocan,cause cornea plana. Nat Genet 2000;25:91–5.
2 Lehmann OJ, El-Ashry MF, Ebenezer N, et al. Anovel keratocan mutation causing autosomalrecessive cornea plana. Invest Ophthalmol Vis Sci2001;42:3118–22.
3 Khan AO, Al-Saif A, Kamburosis M. A novelKERA mutation associated with autosomalrecessive cornea plana. Ophthal Genet2004;25:147–52.
4 Sridhar MS, Mashesh S, Bansal AK, et al. Pellucidmarginal corneal degeneration. Ophthalmology2004;111:1102–7.
Table
1Pertinen
tbiom
etrican
dclinical
characteristicsof
thefamily
aresummarised
12
34
56
78
910
11
12
Age
(yea
rs)
50
43
26
24
23
19
18
17
12
10
86
Keratom
etry
RE43.32,
43.95@102
40.61,
41.06@017
26.49,
28.60@060
45.79,
52.73@085
29.74,
32.23@138
42.51,
42.78@076
28.77,
30.21@086
43.10,
43.49@077
41.01,
41.98@093
39.52,
40.37@087
23.94,
26.81@035
31.72,
33.19@180
Keratom
etry
LE43.44,
44.23@101
40.96,
41.98@082
26.66,
30.13@104
38.66,
47.14@149
29.76,
31.78@065
42.51,
42.94@105
29.27,
33.28@090
42.72,
43.66@093
41.11,
42.51@092
39.61,
40.27@087
24.83,
27.42@117
32.02,
33.48@158
Horizon
talcorne
aldiam
eter
(RE,
LEin
mm)
10,10
11,11
8,8
8,8
8,8
10,10
8,8
10,10
11,11
11,11
8,8
8,8
Axial
leng
th(RE,
LEin
mm)
22.89,
22.34
23.81,
23.78
21.55,
21.62
25.17,
24.88
21.97,
22.05
23.43,
23.68
22.91,
23.65
23.19,
22.98
24.13,
24.05
24.11,
24.22
24.13,
23.88
22.18,
22.61
Cyclopleg
icrefractio
n,vision
with
refractio
nRE
+0.50,
20/3
0plan
o,20/2
0+8
.50,
20/6
0plan
o-10.00
6110,20/6
0+9
.5023.006
030,
20/3
021.25
20/2
5+1
0.0021.006
080,
20/3
020.75,
20/2
020.50,
20/2
020.25,
20/2
0+8
.5022.506
107,
20/4
0+8
.00,
2/3
0Cyclopleg
icrefractio
n,vision
with
refractio
nLE
+2.00,
20/6
020.50,
20/2
0+1
.0029.006
060,
20/5
0plan
o-10.00
6070,20/5
0+1
1.0022.506
140,
20/6
021.50
20/2
5+9
.0021.006
180,
20/5
020.50,
20/2
020.50,
20/2
0plan
o,20/2
0+9
.00,20/1
25
+8.00,
12/3
0Com
men
tsAmblyo
pia
LE,an
terior
cham
ber
shallow
both
eyes,
periph
eral
stromal
haze
both
eyes
Prom
inen
tarcussenilis
both
eyes,
othe
rwise
norm
alop
htha
lmic
exam
Amblyo
piaLE,
16prism
diop
tres
esotropiaat
near
with
correctio
n
Pellucid
margina
lde
gene
ratio
nbo
theyes,
smallcorne
abo
theyes,
arcussenilis
both
eyes
Amblyo
piaLE.RE
,20prism
diop
tres
esotropiaat
near
with
correctio
n
Normal
ophtha
lmic
exam
with
deep
anterior
cham
ber
both
eyes
Amblyo
piaLE
Normal
ophtha
lmic
exam
with
deep
anterior
cham
ber
both
eyes
Normal
ophtha
lmic
exam
with
deep
anterior
cham
ber
both
eyes
Normal
ophtha
lmic
exam
with
deep
anterior
cham
ber
both
eyes
Amblyo
piaLE.RE
,40prism
diop
tres
V-pattern
esotropia
atne
arwith
correctio
n,iris
defect
RE
Amblyo
pia
RE.LE,
poor
coop
eration
Accepted for publication 1 May 2005
PostScript 1539
www.bjophthalmol.com

5 Sridhar MS, Mahesh S, Bansak AK, et al.Superior pellucid marginal corneal degeneration.Eye 2004;18:393–9.
6 Forsius H, Damsten M, Eriksson AW, et al.Autosmal recessive cornea plana. A clinical andgenetic study of 78 cases in Finland. ActaOphthalmol Scand 1998;76:196–203.
7 Dipple KM, McCabe ERB. Phenotypes of patientswith ‘‘simple’’ Mendelian disorders are complextraits: thresholds, modifiers, and systemsdynamics. Am J Hum Genet 2000;66:1729–35.
Alteration of cyclic frequency bybotulinum toxin injection in adultonset cyclic esotropiaCyclic strabismus is an uncommon disorderin which strabismus comes and goes alter-nately, consistently, and repetitively over aperiod of time. In a 48 hour cycle, a 24 hourperiod of orthotropia would be followed by a24 hour period of constant strabismus. Cyclesof 24 hour1 to 96 hour2 patterns have beenreported. Most cases have been described inchildren, and the aetiology of cyclic strabis-mus is still speculative.
Case reportA 57 year old woman was referred toKaohsiung Medical University Hospital withthe complaint of a periodic visual fluctuationof a ‘‘good day‘‘ and a ‘‘bad day’’ alternatelyfor about 6 months. She had diplopia on baddays. She did not have diabetes or hyperten-sion. There was no history of strabismus,amblyopia, patching therapy, ocular trauma,or oculomotor palsy. She had received trialsof Mestinon treatment by two neurologists.Except for pterygium excision 4 years earlier,other ocular and medical history were unre-markable. There was no family history ofstrabismus.Her visual acuity was 20/25 with +1.25 lens
RE and 20/20 LE plano. Cycloplegic refractionwas +1.25 RE and +0.50 LE. The anteriorsegments were normal except for recurrentpterygia on the nasal limbus in both eyes.
Ophthalmoscopic examination, ocular align-ment (fig 1A), and ocular motility werenormal. Since the initial examination wason her ‘‘good day,’’ she was asked to comeback the next day—that is, on the ‘‘bad day.’’The next day, there was a 25 prism dioptre,
commitant right esotropia (fig 1B) with fullocular motility. The visual acuity wasunchanged. Brain and orbit magnetic reso-nance imaging studies were unremarkableexcept for a suspected small arachnoid cyston the right side of the falx.She received 2.5 U botulinum toxin
(Botox) injection in her right medial rectusmuscle (MR). The alignment was orthotropia1 week after the injection. She was asympto-matic for about 2 months, but the cyclicpattern returned with a 96 hour cycle bypatient history. A repeated 2.5 U Botoxinjection in right MR, which was given3 months after the first, produced anotherasymptomatic period of 2 months. Twomonths after the second injection, sheexperienced constant strabismus withoutcyclic pattern, which persisted for about1 year. She received right MR recession by4 mm and right lateral rectus muscle resec-tion by 5 mm for constant esotropia of25 prism dioptres. After the surgery, thealignment was orthotropic and no recurrentof the cyclic pattern during 1 month of followup. The stereopsis was 200 seconds of arc byTitmus test.
CommentAdult onset cyclic strabismus is rare,2–8 and,to the best of our knowledge, only 10 patientshave been reported. The reported cases ofadult onset cyclic strabismus are summarisedin table 1. The patients had various ages ofonset between 21 and 67 years. Mostreported cases demonstrated 48 hour cyclicpatterns. The persistence of the cycles, if notinterrupted by surgery, was as long as7 years.8 It is interesting that adult onsetcyclic strabismus occurs predominantly infemales and is frequently related to ocular ororbital diseases, trauma, or surgery.4–8
Botox injection has been used as treatmentof cyclic strabismus.7 However, no change ofthe cyclic pattern was mentioned. We notedthat the cyclic pattern in our patient changed3 months after the first Botox injection, andthe cycles were eliminated 2 months after thesecond injection.The characteristics of cyclic strabismus in
children are an average age of onset between3 and 4 years, moderate hyperopia, andmoderate angle.3 However, a female prepon-derance was not noted in childhood onsetcyclic esotropia. No pertinent explanation forcyclic strabismus has been reported.Although Botox only has a temporary effect,both Botox injection7 and eye muscle surgery3
produce good ocular alignment results. Moreevidence and further investigation arerequired to elucidate the mystery.
AcknowledgementsThe authors thank Professor William F Hoyt andProfessor Creig S Hoyt for their review and criticismof this letter.
Y-H LaiDepartment of Ophthalmology, Kaohsiung MedicalUniversity Hsiao-Kang Hospital, Kaohsiung Medical
University, Kaohsiung, Taiwan
D R FredrickDepartment of Ophthalmology, University of
California, San Francisco, San Francisco, CA, USA
Figure 1 (A) ‘‘Good day’’—orthotropia; (B)‘‘Bad day’’—esotropia.
Table 1 Summary of the adult onset cyclic strabismus
CaseNo
Age ofonset(years) Sex
Cyclicpattern
Durationofcycles Angle (D)
Related diseasesor coexistent conditions Outcome References
1 34 Male 4 days 3 years ET 35Optic atrophy both eyes, alcoholabuse
No treatment Frenkel2
2 32 Female* 2 days NA ET 35 NA No treatment, CPP? Helveston3
3 53 Female 2 days NAXT 15,RHT 30
Graves’ disease OT after muscle surgery Knapp4
4 55 Female 2 days NA RHT 25 Graves’ disease OT after muscle surgery Knapp4
5 67 Female 2 days 5 yearsET 25,RHT 8
RD RE, 360˚ encircling scleralbuckling procedure RE, cyclicmydriasis and ptosis
No treatment, CPP Troost5
6 34 Female 2 days 9 weeksLHT 20,XT 10
Craniofacial surgery for fronto-orbital fibrous dysplasia, left side
OT after muscle surgery Metz6
7 46 Female 2 days 1 yearET 12 to45
ECCE RE, high myopia REBotulinum toxin injection, ET2D with cycle eliminated aftermuscle surgery
Riordan-Eva7
8 21 Female 5 days? 2 years ET 25RD RE, vitreolensectomy andsilicone oil exchange RE
Botulinum toxin injection, CPP Riordan-Eva7
9 49 Female 2 days 7 yearsRHT 15,ET 25
ECCE RE, RD and PVR RE, PVTand scleral buckling RE, ECCE LE,prophylactic encircling bandsurgery LE
OT after muscle surgery Bagheri8
10 57 Female 2 days 1year ET 30 Recurrent pterygia in both eyes,Botulinum toxin injection,cyclic pattern changed,OT after muscle surgery
Present report
*Information provided by Dr Eugene Helveston (personal communication). NA, not available; CPP, cyclic pattern persisted; D, prism dioptre; ET, esotropia; XT,exotropia; RHT, right hypertropia; LHT, left hypertropia; OT, orthotropia; RD, retinal detachment; PVR, proliferative vitreoretinopathy; ECCE, extracapsularcataract extraction; PVT, posterior vitrectomy.
1540 PostScript
www.bjophthalmol.com

Correspondence to: Yu-Hung Lai, Department ofOphthalmology, Kaohsiung Medical University Hsiao-
Kang Hospital, Kaohsiung Medical University, 100Zihyou 1st Road, Kaohsiung, 807, Taiwan; yuhung.
doi: 10.1136/bjo.2005.069021
References
1 Windsor CE, Berg EF. Circadian heterotropia.Am J Ophthalmol 1969;67:565–71.
2 Frenkel RE, Brodsky MC, Spoor TC. Adult-onsetcyclic esotropia and optic atrophy. J Clin Neuro-ophthalmol 1986;6:27–30.
3 Helveston EM. Cyclic strabismus. Am Orthopt J1973;23:48–51.
4 Knapp P. Special types of muscle anomaliesassociated with Graves’ disease. Ophthalmology1979;86:2081–4.
5 Troost BT, Abel L, Noreika J, et al. Acquired cyclicesotropia in an adult. Am J Ophthalmol1981;91:8–13.
6 Metz HS, Searl SS. Cyclic vertical deviation. TransAm Ophthalmol Soc 1984;82:158–65.
7 Riordan-Eva P, Vickers SF, McCarry B, et al.Cyclic strabismus without binocular function.J Pediatr Ophthalmol Strabismus1993;30:106–8.
8 Bagheri A, Ahmadieh H, Repka MX. Acquiredcyclic strabismus in an adult. J Pediatr OphthalmolStrabismus 2002;39:310–12.
Hand hygiene in routineglaucoma clinicsNosocomial infection occurs via the hands ofhealthcare workers (HCWs).1 Hand hygienereduces hospital infection rates; however,HCWs seldom comply with this.2
We determined how often ophthalmolo-gists and allied professionals cleaned theirhands and whether intervention was effec-tive.
Participants, methods, and resultsWe conducted the study in the daily glau-coma clinics of Moorfields Eye Hospitalwhere policy states that all HCWs must cleantheir hands between patients.For 1 week, hand hygiene practice was
monitored covertly by two observers.Potential hand cleaning opportunities werebefore or during patient contact, before or
after manipulative procedures, and afterglove removal. Manipulative procedures weredefined as 5-fluorouracil subconjunctivalinjection, taking an eye swab, suture, orsupramid removal, and bleb needling ormassage.Without revealing how the study was
conducted, preliminary results were pre-sented and also distributed by memo. Twoweeks after this intervention, hand hygienewas re-monitored for 1 week.Baseline hand hygiene episodes were 18%
but increased significantly to 28% (p=0.005)following intervention (table 1). Before inter-vention two out of seven people performingprocedures cleaned their hands, but not forthe single episode that 5-fluorouracil wasused. However, after intervention six out ofseven HCWs cleaned their hands (p=0.04),including all three episodes in which 5-fluorouracil was handled.Before intervention, female HCWs cleaned
their hands significantly more than males(30% v 9%, p,0.001). After interventionhand hygiene increased further for females(54%, p,0.001) with no change for males(11%, p=0.57).Nurses had the highest frequency of hand
cleaning but with no change after interven-tion (69% v 58%, p=0.36). Increased handhygiene was significant for doctors followingintervention (11% v 20%, p=0.01).
CommentRecently, nosocomial infection has attractedconsiderable media interest. While proble-matic worldwide, the United Kingdom hasone of the highest rates of methicillinresistant Staphylococcus aureus (MRSA).3 Thehands of HCWs are a major route oftransmission. Hand hygiene frequenciesrange from 3%,2 increasing to more than60% when HCWs are aware of beingobserved.4
In our study, hand hygiene was low (18%).Although significant improvement followedintervention (28%) this was far from thehospital standard. Our new level of handcleaning is likely to be transient as all but onestudy has demonstrated sustained improve-ment.5
Previous studies, including our own, haveshown that female HCWs clean their handsmore often than males.6 In general, sexdifferences in hand washing are explainedby the social role theory—that is, females arecommunal whereas men are agentic.7 Hence,women are more likely than men to partici-pate in socially acceptable behaviour such ashand washing.8 In our study, interventionproduced a significant improvement in handhygiene for females with no effect on males.Behaviourally, men are less easily influencedthan women,7 which may explain why inter-vention had no effect on male HCWs.As with previous studies5 9 our nurses had
the highest frequency of hand hygiene (69%).This could be because most nurses are femaleor because of an emphasis on hand washingin their undergraduate training. However,with our nurses hand hygiene did notincrease following intervention. Possibly fewnurses were present at the lecture, hence,they only received written information con-cerning initial study results.As observed by others,5 6 9 we found hand
hygiene among doctors was low (11%).However, intervention had its greatest effecton the doctors (p=0.01). Although numbersare small, intervention had a positive effecton manipulative procedures, especially whenusing 5-fluorouracil.Our study demonstrates that hospital
policy is not being practised. Getting HCWsto clean their hands has been an ongoingstruggle since Semmelweis. It has beensuggested that patients should ask theirhealthcare professional to hand wash.10
Although controversial, this may help in theeradication of hospital acquired infection.
E Mensah, I E Murdoch, K Binstead,C Rotheram, W Franks
Moorfields Eye Hospital NHS Foundation Trust, CityRoad, London EC1V 2PD, UK
Correspondence to: E Mensah, Moorfields EyeHospital NHS Foundation Trust, City Road, London
EC1V 2PD, UK; [email protected]
Accepted for publication 3 May 2005
Table 1 Effect of intervention on hand hygiene compliance
Hand hygiene before interventionHand hygiene afterintervention
p ValueNo (%) No (%)
Hand hygiene opportunities 249 291Hand hygiene episodes before patient contact 36 (14) 73 (25) 0.002Hand hygiene episodes during patient contact 8 (3) 8 (3) 1.00Total hand hygiene episodes 44 (18) 81 (28) 0.005Hand hygiene episodes for procedures 2/7 (0/1 for 5-FU) 6/7 (3/3 for 5-FU) 0.04Sex of healthcare workerFemale 32/107 (30)* 62/115 (54** ,0.001Male 12/133 (9)* 20/182 (11)** 0.57
Profession of healthcare workerDoctor 21/191 (11) 44/220 (20) 0.01Nurse 18/26 (69) 25/43 (58) 0.36Optometrist 3/19 (16) 8/26 (31) 0.25Other 2/8 (25) 1/7 (14) 0.62
Only three out of nine examination bays were observed for 1 hour at a time, in random order, during morning (from 09:30 to 12:30) and afternoon (from 14:00to 17:00) clinics.Data were analysed using x2 contingency tests.5-FU = 5-fluorouracil.*p,0.001; **p,0.001.
Local ethics approval was obtained for this study.
doi: 10.1136/bjo.2005.072538
Accepted for publication 21 May 2005
PostScript 1541
www.bjophthalmol.com

References
1 Bauer TM, Ofner E, Just HM, et al. Anepidemiological study assessing the relativeimportance of airborne and direct contacttransmission of microorganisms in a medicalintensive care unit. J Hosp Infect 1990;15:301–9.
2 Bischoff WE, Reynolds TM, Sessler CN, et al.Handwashing compliance by health care workers.The impact of introducing an accessible, alcohol-based hand antiseptic. Arch Intern Med2000;160:1017–21.
3 Tiemersma EW, Bronzwaer SLAM, Lyytikainen O,et al. Methicillin-resistant Staphylococcus aureusin Europe, 1999–2002. Emerg Infect Dis2004;10:1627–34.
4 Pittet D, Simon A, Hugonnet S, et al. Handhygiene among physicians: performance, beliefs,and perceptions. Ann Intern Med 2004;141:1–8.
5 Hugonnet S, Perneger TV, Pittet D. Alcohol-basedhandrub improves compliance with hand hygienein intensive care units. Arch Intern Med2002;162:1037–43.
6 van de Mortel T, Bourke R, McLoughlin J, et al.Gender influences handwashing rates in thecritical care unit. Am J Infect Control2001;29:395–9.
7 Eagly AH. Sex differences and socialbehaviour: a social role interpretation. Hillsdale,NJ: Erlbaum, 1987.
8 Johnson HD, Sholcosky D, Gabello K, et al. Sexdifferences in public restroom handwashingbehaviour associated with visual behaviourprompts. Percept Mot Skills 2003;97(3Pt1):805–10.
9 Pittet D, Hugonnet S, Harbarth S, et al.Effectiveness of a hospital-wide programme toimprove compliance with hand hygiene. Infectioncontrol programme. Lancet 2000;356:1307–12.
10 Jarvis WR. Handwashing—the Semmelweislesson forgotten? Lancet 1994;344:1311–12.
Successful treatment ofWegener’s granulomatosisassociated scleritis withrituximabRituximab (Rituxan, Genentech, Inc, SouthSan Francisco, CA, USA) is a new anti-CD20B cell monoclonal antibody that has beenused successfully to treat refractory cases ofWegener’s granulomatosis (WG).1–3 There hasbeen no published report of its effect inWegener’s associated eye disease. Wedescribe the successful treatment ofWegener’s associated scleritis with rituximab.
Case reportA 21 year old man with WG, proved on renalbiopsy and by anti-neutrophil cytoplasmantibody (ANCA) positivity 6 years earlier,presented with bilateral, painful, red eyes. Onexamination his visual acuities were 6/4 righteye and 6/5 left eye. Anterior segmentexamination showed subconjunctival hae-morrhage, congested scleral vessels, scleraloedema, peripheral corneal infiltrates, andmild anterior chamber inflammation in eacheye. Funduscopy revealed bilateral swollenoptic discs with scattered retinal haemor-rhages in the right eye. A diagnosis of scleritiswas made. Oral prednisolone was increasedfrom 5–40 mg daily and maintenance oralmycophenolate mofetil 2 g daily was contin-ued. Topical prednisolone acetate 1% hourlywas commenced to both eyes.Over the next month the scleritis had not
improved and his systemic vasculitis hadbecome more active, causing arthralgia,haemoptysis, and new vasculitic skin lesions.His white cell count (WCC) had risen to13.96109 compared to 9.66109 the previousmonth. His ANCA had become positive byindirect immunofluorescence (titre of 1 in
25), and by proteinase 3 specific ELISA (titre22 units, normal range,10). A new infiltratewas present in the lower lobe of his right lungon chest x ray.Owing to concern over the total cumulative
dose of cyclophosphamide he had previouslyreceived (.25 g), he was given an intrave-nous infusion of rituximab 1 g. Intravenouscyclophosphamide (12.5 mg/kg, adjusted forrenal function) was also given with therituximab infusion. These infusions wererepeated after 2 weeks.This led to an immediate significant systemic
improvement accompanied by reduction ofWCC to 9.66109 and ANCA became undetect-able. The pulmonary infiltrate resolved. Thescleritis also resolved promptly, evident fromcompletely white eyes, resolution of activescleral vessels, corneal infiltrates, optic discswelling, and subjective resolution of ocularpain. At 7 months after the infusion, thepatient remained in remission. His systemictreatment was slowly reduced to prednisolone15 mg daily and mycophenolate mofetil750 mg twice daily.
CommentRituximab is a humanised monoclonal anti-body against the CD20 antigen that isexpressed on the cell surface during earlypre-B cell development and persists throughall stages of B cell differentiation.4 It resultsin rapid depletion of CD20 positive B lym-phocytes from the circulating blood and iswell tolerated. The precise role of B cells inthe pathogenesis of WG remains elusive atpresent, but several possibilities exist. B cellscan act as antigen presenting cells to T cells orprovide additional co-stimulatory signals forthem. Another possibility is that self reactiveB cells, derived from unusual B cell subsets,5
may follow an alternative maturation pro-cess, including the continued expression ofCD20 during antibody production.There has been no report on its effect on
WG associated scleritis. Our patient wasgiven rituximab primarily for his generalisedvasculitis, but his refractory scleritis alsoresponded promptly. Although he alsoreceived cyclophosphamide at the same time,the dose and course were limited to avoidtoxicity. Therefore, in this case the promptimprovement was attributed to rituximab,rather than cyclophosphamide.This is the first case reporting rituximab as
an effective treatment for refractory WGassociated scleritis.
C M G Cheung, P I MurrayOphthalmology, Division of Immunity and Infection,
University of Birmingham, Birmingham, UK
C O S SavageNephrology, Division of Immunity and Infection,
University of Birmingham, Birmingham, UK
Correspondence to: Professor P I Murray, AcademicUnit of Ophthalmology, Birmingham and Midland EyeCentre, City Hospital, Dudley Road, Birmingham B18
7QU, UK; [email protected]
doi: 10.1136/bjo.2005.075689
References
1 Specks U, Fervenza FC, McDonald TJ, et al.Response of Wegener’s granulomatosis to anti-CD20 chimeric monoclonal antibody therapy.Arthritis Rheum 2001;44:2836–40.
2 Keogh KA, Wylan ME, Stone JH, et al. Inductionof remission by B lymphocyte depletion in eleven
patients with refractory antineutrophil cytoplasmicantibody-associated vasculitis. Arthritis Rheum2005;52:262–8.
3 Ferraro AJ, Day CJ, Drayson MT, et al. Effectivetherapeutic use of rituximab in refractoryWegener’s granulomatosis. Nephrol DialTransplant 2005;20:622–5.
4 Stashenko P, Nadler LM, Hardy R, et al.Characterization of a human B lymphocyte-specific antigen. J Immunol 1980;125:1678–85.
5 Chumley MJ, Dal Porto JM, Cambier JC. Theunique Ag receptor signaling phenotype of B-1cells is influenced by locale but induced byantigen. J Immunol 2002;169:1735–43.
Retinopathy is not the only ocularsymptom: myasthenia gravis inassociation with interferontherapyInterferons (IFNs) have antiviral and anti-mitogenic effects and are often used in thetreatment of viral hepatitis or some neo-plasms. However, they have various sideeffects including fever, nausea, depression,retinopathy, and autoimmune diseases.Although myasthenia gravis (MG) is rarelyassociated with IFN therapy, some casesdeveloping MG after IFN or IFN/ribavirincombined therapy for chronic active hepatitisC have been reported.1–5 We report such a caseby reviewing the clinical data.
Case reportA 69 year old man with chronic hepatitis Cfor 11 years had been treated with IFN-amonotherapy (IFN 66106 IU three times aweek after 2 weeks of daily injections). Thefirst treatment started in April 2002. Therewas no complication noted in that treatment.After the therapy hepatitis C virus activitysettled for a while, but during the observationhis clinical data showed a rise in hepatitis Cvirus RNA and aminotransferases. He under-went IFN-a therapy conjugated with ribavirin(IFN 66106 IU three times a week after2 weeks of daily injections, ribavirin 800 mgtwice a day) again on 6 December 2002.During the course his condition was checkedperiodically, mainly in terms of retinopathy.He had finished 7 months of treatmentwithout significant side effects.Around December 2003 he began to notice
fluctuating diplopia. Examination revealed hisreduced right adduction, exotropia and left/right hypertropia. Since his condition driftedand there was no significant disorder onmagnetic resonance imaging, MG was sus-pected and edrophonium chloride was tested.With the medication, his diplopia prominentlyimproved and MG was diagnosed; however,there was no elevation in his anti-acetylcholinereceptor antibody titre or other auto-antibo-dies, and thymoma was not detected.
CommentIt is well known that IFN therapy inducesautoimmunity. Thyroid auto-antibodies arethe most frequent findings; autoimmunehepatitis, rheumatoid symptoms, inductionof insulin dependent diabetes, etc, are alsoseen. In relation to this autoimmune effect,several cases concerning MG associated withIFN therapy have been reported. Some casesdeveloped myasthenia newly or others exa-cerbated pre-existing symptoms.1–5 It isreported that cases with pre-existing MGhave a tendency to present more severesymptoms including myasthenic crisis.4 Thepathogenesis is not completely understood
Accepted for publication 19 June 2005
1542 PostScript
www.bjophthalmol.com
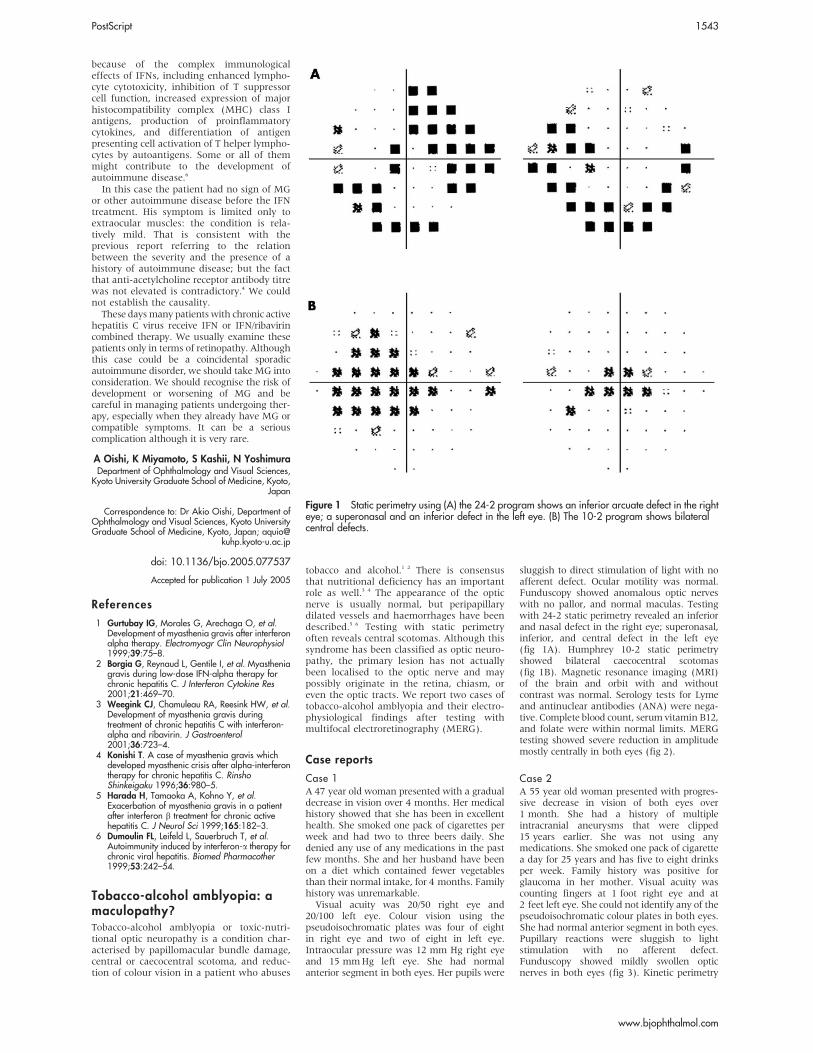
because of the complex immunologicaleffects of IFNs, including enhanced lympho-cyte cytotoxicity, inhibition of T suppressorcell function, increased expression of majorhistocompatibility complex (MHC) class Iantigens, production of proinflammatorycytokines, and differentiation of antigenpresenting cell activation of T helper lympho-cytes by autoantigens. Some or all of themmight contribute to the development ofautoimmune disease.6
In this case the patient had no sign of MGor other autoimmune disease before the IFNtreatment. His symptom is limited only toextraocular muscles: the condition is rela-tively mild. That is consistent with theprevious report referring to the relationbetween the severity and the presence of ahistory of autoimmune disease; but the factthat anti-acetylcholine receptor antibody titrewas not elevated is contradictory.4 We couldnot establish the causality.These daysmany patients with chronic active
hepatitis C virus receive IFN or IFN/ribavirincombined therapy. We usually examine thesepatients only in terms of retinopathy. Althoughthis case could be a coincidental sporadicautoimmune disorder, we should take MG intoconsideration. We should recognise the risk ofdevelopment or worsening of MG and becareful in managing patients undergoing ther-apy, especially when they already have MG orcompatible symptoms. It can be a seriouscomplication although it is very rare.
A Oishi, K Miyamoto, S Kashii, N YoshimuraDepartment of Ophthalmology and Visual Sciences,
Kyoto University Graduate School of Medicine, Kyoto,Japan
Correspondence to: Dr Akio Oishi, Department ofOphthalmology and Visual Sciences, Kyoto UniversityGraduate School of Medicine, Kyoto, Japan; aquio@
kuhp.kyoto-u.ac.jp
doi: 10.1136/bjo.2005.077537
References
1 Gurtubay IG, Morales G, Arechaga O, et al.Development of myasthenia gravis after interferonalpha therapy. Electromyogr Clin Neurophysiol1999;39:75–8.
2 Borgia G, Reynaud L, Gentile I, et al. Myastheniagravis during low-dose IFN-alpha therapy forchronic hepatitis C. J Interferon Cytokine Res2001;21:469–70.
3 Weegink CJ, Chamuleau RA, Reesink HW, et al.Development of myasthenia gravis duringtreatment of chronic hepatitis C with interferon-alpha and ribavirin. J Gastroenterol2001;36:723–4.
4 Konishi T. A case of myasthenia gravis whichdeveloped myasthenic crisis after alpha-interferontherapy for chronic hepatitis C. RinshoShinkeigaku 1996;36:980–5.
5 Harada H, Tamaoka A, Kohno Y, et al.Exacerbation of myasthenia gravis in a patientafter interferon b treatment for chronic activehepatitis C. J Neurol Sci 1999;165:182–3.
6 Dumoulin FL, Leifeld L, Sauerbruch T, et al.Autoimmunity induced by interferon-a therapy forchronic viral hepatitis. Biomed Pharmacother1999;53:242–54.
Tobacco-alcohol amblyopia: amaculopathy?Tobacco-alcohol amblyopia or toxic-nutri-tional optic neuropathy is a condition char-acterised by papillomacular bundle damage,central or caecocentral scotoma, and reduc-tion of colour vision in a patient who abuses
tobacco and alcohol.1 2 There is consensusthat nutritional deficiency has an importantrole as well.3 4 The appearance of the opticnerve is usually normal, but peripapillarydilated vessels and haemorrhages have beendescribed.5 6 Testing with static perimetryoften reveals central scotomas. Although thissyndrome has been classified as optic neuro-pathy, the primary lesion has not actuallybeen localised to the optic nerve and maypossibly originate in the retina, chiasm, oreven the optic tracts. We report two cases oftobacco-alcohol amblyopia and their electro-physiological findings after testing withmultifocal electroretinography (MERG).
Case reports
Case 1A 47 year old woman presented with a gradualdecrease in vision over 4 months. Her medicalhistory showed that she has been in excellenthealth. She smoked one pack of cigarettes perweek and had two to three beers daily. Shedenied any use of any medications in the pastfew months. She and her husband have beenon a diet which contained fewer vegetablesthan their normal intake, for 4 months. Familyhistory was unremarkable.Visual acuity was 20/50 right eye and
20/100 left eye. Colour vision using thepseudoisochromatic plates was four of eightin right eye and two of eight in left eye.Intraocular pressure was 12 mm Hg right eyeand 15 mmHg left eye. She had normalanterior segment in both eyes. Her pupils were
sluggish to direct stimulation of light with noafferent defect. Ocular motility was normal.Funduscopy showed anomalous optic nerveswith no pallor, and normal maculas. Testingwith 24-2 static perimetry revealed an inferiorand nasal defect in the right eye; superonasal,inferior, and central defect in the left eye(fig 1A). Humphrey 10-2 static perimetryshowed bilateral caecocentral scotomas(fig 1B). Magnetic resonance imaging (MRI)of the brain and orbit with and withoutcontrast was normal. Serology tests for Lymeand antinuclear antibodies (ANA) were nega-tive. Complete blood count, serum vitamin B12,and folate were within normal limits. MERGtesting showed severe reduction in amplitudemostly centrally in both eyes (fig 2).
Case 2A 55 year old woman presented with progres-sive decrease in vision of both eyes over1 month. She had a history of multipleintracranial aneurysms that were clipped15 years earlier. She was not using anymedications. She smoked one pack of cigarettea day for 25 years and has five to eight drinksper week. Family history was positive forglaucoma in her mother. Visual acuity wascounting fingers at 1 foot right eye and at2 feet left eye. She could not identify any of thepseudoisochromatic colour plates in both eyes.She had normal anterior segment in both eyes.Pupillary reactions were sluggish to lightstimulation with no afferent defect.Funduscopy showed mildly swollen opticnerves in both eyes (fig 3). Kinetic perimetry
Accepted for publication 1 July 2005
Figure 1 Static perimetry using (A) the 24-2 program shows an inferior arcuate defect in the righteye; a superonasal and an inferior defect in the left eye. (B) The 10-2 program shows bilateralcentral defects.
PostScript 1543
www.bjophthalmol.com
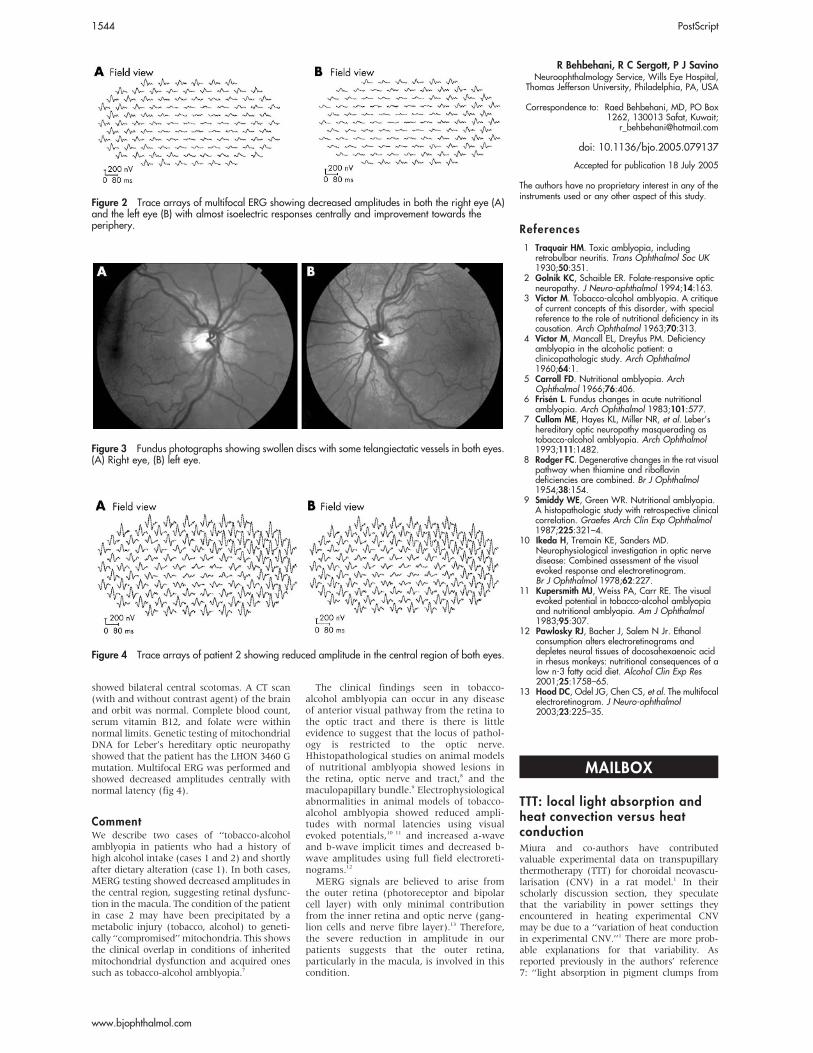
showed bilateral central scotomas. A CT scan(with and without contrast agent) of the brainand orbit was normal. Complete blood count,serum vitamin B12, and folate were withinnormal limits. Genetic testing of mitochondrialDNA for Leber’s hereditary optic neuropathyshowed that the patient has the LHON 3460 Gmutation. Multifocal ERG was performed andshowed decreased amplitudes centrally withnormal latency (fig 4).
CommentWe describe two cases of ‘‘tobacco-alcoholamblyopia in patients who had a history ofhigh alcohol intake (cases 1 and 2) and shortlyafter dietary alteration (case 1). In both cases,MERG testing showed decreased amplitudes inthe central region, suggesting retinal dysfunc-tion in the macula. The condition of the patientin case 2 may have been precipitated by ametabolic injury (tobacco, alcohol) to geneti-cally ‘‘compromised’’ mitochondria. This showsthe clinical overlap in conditions of inheritedmitochondrial dysfunction and acquired onessuch as tobacco-alcohol amblyopia.7
The clinical findings seen in tobacco-alcohol amblyopia can occur in any diseaseof anterior visual pathway from the retina tothe optic tract and there is there is littleevidence to suggest that the locus of pathol-ogy is restricted to the optic nerve.Hhistopathological studies on animal modelsof nutritional amblyopia showed lesions inthe retina, optic nerve and tract,8 and themaculopapillary bundle.9 Electrophysiologicalabnormalities in animal models of tobacco-alcohol amblyopia showed reduced ampli-tudes with normal latencies using visualevoked potentials,10 11 and increased a-waveand b-wave implicit times and decreased b-wave amplitudes using full field electroreti-nograms.12
MERG signals are believed to arise fromthe outer retina (photoreceptor and bipolarcell layer) with only minimal contributionfrom the inner retina and optic nerve (gang-lion cells and nerve fibre layer).13 Therefore,the severe reduction in amplitude in ourpatients suggests that the outer retina,particularly in the macula, is involved in thiscondition.
R Behbehani, R C Sergott, P J SavinoNeuroophthalmology Service, Wills Eye Hospital,
Thomas Jefferson University, Philadelphia, PA, USA
Correspondence to: Raed Behbehani, MD, PO Box1262, 130013 Safat, Kuwait;
doi: 10.1136/bjo.2005.079137
References
1 Traquair HM. Toxic amblyopia, includingretrobulbar neuritis. Trans Ophthalmol Soc UK1930;50:351.
2 Golnik KC, Schaible ER. Folate-responsive opticneuropathy. J Neuro-ophthalmol 1994;14:163.
3 Victor M. Tobacco-alcohol amblyopia. A critiqueof current concepts of this disorder, with specialreference to the role of nutritional deficiency in itscausation. Arch Ophthalmol 1963;70:313.
4 Victor M, Mancall EL, Dreyfus PM. Deficiencyamblyopia in the alcoholic patient: aclinicopathologic study. Arch Ophthalmol1960;64:1.
5 Carroll FD. Nutritional amblyopia. ArchOphthalmol 1966;76:406.
6 Frisen L. Fundus changes in acute nutritionalamblyopia. Arch Ophthalmol 1983;101:577.
7 Cullom ME, Hayes KL, Miller NR, et al. Leber’shereditary optic neuropathy masquerading astobacco-alcohol amblyopia. Arch Ophthalmol1993;111:1482.
8 Rodger FC. Degenerative changes in the rat visualpathway when thiamine and riboflavindeficiencies are combined. Br J Ophthalmol1954;38:154.
9 Smiddy WE, Green WR. Nutritional amblyopia.A histopathologic study with retrospective clinicalcorrelation. Graefes Arch Clin Exp Ophthalmol1987;225:321–4.
10 Ikeda H, Tremain KE, Sanders MD.Neurophysiological investigation in optic nervedisease: Combined assessment of the visualevoked response and electroretinogram.Br J Ophthalmol 1978;62:227.
11 Kupersmith MJ, Weiss PA, Carr RE. The visualevoked potential in tobacco-alcohol amblyopiaand nutritional amblyopia. Am J Ophthalmol1983;95:307.
12 Pawlosky RJ, Bacher J, Salem N Jr. Ethanolconsumption alters electroretinograms anddepletes neural tissues of docosahexaenoic acidin rhesus monkeys: nutritional consequences of alow n-3 fatty acid diet. Alcohol Clin Exp Res2001;25:1758–65.
13 Hood DC, Odel JG, Chen CS, et al. The multifocalelectroretinogram. J Neuro-ophthalmol2003;23:225–35.
TTT: local light absorption andheat convection versus heatconductionMiura and co-authors have contributedvaluable experimental data on transpupillarythermotherapy (TTT) for choroidal neovascu-larisation (CNV) in a rat model.1 In theirscholarly discussion section, they speculatethat the variability in power settings theyencountered in heating experimental CNVmay be due to a ‘‘variation of heat conductionin experimental CNV.’’1 There are more prob-able explanations for that variability. Asreported previously in the authors’ reference7: ‘‘light absorption in pigment clumps from
Figure 2 Trace arrays of multifocal ERG showing decreased amplitudes in both the right eye (A)and the left eye (B) with almost isoelectric responses centrally and improvement towards theperiphery.
Figure 3 Fundus photographs showing swollen discs with some telangiectatic vessels in both eyes.(A) Right eye, (B) left eye.
Accepted for publication 18 July 2005
The authors have no proprietary interest in any of theinstruments used or any other aspect of this study.
Figure 4 Trace arrays of patient 2 showing reduced amplitude in the central region of both eyes.
MAILBOX
1544 PostScript
www.bjophthalmol.com

prior focal photocoagulation can cause local hotspots in large TTT treatment fields.’’2
Additionally, local choroidal blood flow2 mayhave been altered by vascular remodelling thatoccurred in the 14 days between the intensefocal laser photocoagulation that the authorsused to produce CNV and their subsequentliposomal monitored TTT at the site.Chorioretinal temperature rise from a
lengthy 60 seconds TTT exposure is affected:(1) by pigmentation at the treatment site,which determines how effectively laser radiantenergy is converted locally into thermal energy,and (2) to a lesser extent by choroidal bloodflow,3 which transfers thermal energy by heatconvection away from the exposure site. It isunlikely that local heat conduction is alteredsignificantly by the initial photocoagulation orsubsequent tissue remodelling because heatconduction in most normal biological tissues isessentially the same as that of water.4–6
M A MainsterDepartment of Ophthalmology, University of KansasMedical School, 3901 Rainbow Boulevard, Kansas
City, KS 66160-7379, USA
D H SilneyLaser/Optical Radiation Program, US Army
Environmental Hygiene Agency, Aberdeen ProvingGround, MD 21010, USA
Correspondence to: Professor Martin A Mainster,Department of Ophthalmology, M53009, University
of Kansas Medical School, 3901 Rainbow Boulevard,Kansas City, KS 66160-7379, USA;
doi: 10.1136/bjo.2005.082453
References
1 Miura S, Nishiwaki H, Ieki Y, et al. Chorioretinaltemperature monitoring during transpupillarythermotherapy for choroidal neovascularisation.Br J Ophthalmol 2005;89:475–9.
2 Mainster MA, Reichel E. Transpupillarythermotherapy for age- related maculardegeneration: long-pulse photocoagulation,
apoptosis, and heat shock proteins. OphthalmicSurg Lasers 2000;31:359–73.
3 Welch AJ, Wissler EH, Priebe LA. Significance ofblood flow in calculations of temperature in laserirradiated tissue. IEEE Trans Biomed Eng1980;27:164–6.
4 Mainster MA, White TJ, Tips JH, et al. Retinal-temperature increases produced by intense lightsources. J Opt Soc Am 1970;60:264–70.
5 Welch AJ, van Gemert MJC. Optical-thermalresponse of laser-irradiated tissue. New York:Plenum Press, 1995.
6 Mainster MA. Decreasing retinalphotocoagulation damage: principles andtechniques. Sem Ophthalmol 1999;14:200–9.
Accepted for publication 6 September 2005
NOTICES
19th International Society forGeographical & EpidemiologicalOphthalmology CongressThe 19th ISGEO congress will be held in SaoPaulo, Brazil on 18-19 February, 2006, justprior to the ICO. Abstract submission andregistration forms can be obtained by email-ing Dr Paul Courtright ([email protected], url: ) or by accessing the ISGEO websiteat www.kcco.net/isgeo.
Medical Contact Lens & Ocularsurface Association WinterSymposiumThe MCLOSAWinter Symposium will be heldat the Western Eye Hospital, MaryleboneRoad, London NW1 on Friday 18 November2005. For further information please visitthe MCLOSA website at www.mclosa.org.uk/annualmtg.html.
World Ophthalmology Congress2006 – BrazilThe World Ophthalmology Congress (whichis replacing the International Congress ofOphthalmology) is meeting in February 2006in Brazil.For further information on the congress and
committees, scientific program and coordina-tors of different areas are available at thecongress website www.ophthalmology2006.com.br
Vision 2020The latest issue of Community Eye Health (No54) assesses the progress of Vision 2020 atthe district level. For further informationplease contact: Journal of Community EyeHealth, International Resource Centre,International Centre for Eye Health,Department of Infectious and TropicalDiseases, London School of Hygiene andTropical Medicine, Keppel Street, LondonWC1E 7HT, UK (tel: +44 (0)20 7612 7964;email: [email protected]; online edi-tion: www.jceh.co.uk). Annual subscription(4 issues) UK £28/US$45. Free to developingcountry applicants.
CORRECTIONS
doi: 10.1136/bjo.2005.75895corr1
In the letter titled, Patient satisfaction withanaesthesia comparing sun-Tenon’s blockand topical anaesthesia (Br J Ophthalmol2005;89:1228) the second author wasomitted. The second author for this letterwas R W D Bell, Sunderland Eye Infirmary,Queen Alexandra Road, Sunderland SR29HP, UK. The author apologises for thisomission.
doi: 10.1136/bjo.2004.58941corr1
In the paper titled, En-face optical coherencetomography (OCT): A new method to analysestructural changes of the optic nerve headin rat glaucoma (Br J Ophthalmol 2005;89:1210–6) one of the author’s name has beenspelt incorrectly. The author Podolean AG,should be spelt Podoleanu AG. The journalapologises for this error.
PostScript 1545
www.bjophthalmol.com