do the military’s frontline psychiatry/combat operational
TRANSCRIPT

Do the Military’s Frontline Psychiatry/Combat OperationalStress Control Programs Benefit Veterans? Part Two: SystematicReview of the Evidence
Mark C. Russell1 & Charles R. Figley2
Received: 24 September 2016 /Accepted: 19 December 2016 /Published online: 10 February 2017# Springer Science+Business Media New York 2017
Abstract The second of a three-part review provides the first-ever systematic investigation into the military’s claim that itscentury-old policy of preventing evacuation of psychiatric ca-sualties from war zones is beneficial to the health and well-being of individual service members and their families. Weconducted an extensive literature search for studies on themilitary’s frontline psychiatry doctrine, particularly researchcomparing the differential effects of deployed personnelreturned-to-duty (RTD) via frontline psychiatry or combatand operational stress control (COSC) and behavioral healthinterventions, as opposed to those evacuated out of war zonesas psychiatric casualties. In addition, we examined partial andindirect evidence in support of the military’s argument thatRTD and preventing psychiatric evacuations enhances post-traumatic growth and reduces adverse impact from mentalhealth stigma, shame, and guilt, as well as lowering the riskof developing PTSD or other war stress injury causing prema-ture military discharge. Results indicate support that frontlinepsychiatry benefits the war-fighting mission and goal of mil-itary medicine to prevent psychiatric attrition, with RTD ratesof 60 to 100% and severely limiting psychiatric evacuations.However, there is paucity of research on differential out-comes, with only three, small uncontrolled retrospectiveIsraeli studies from the 1982 Lebanon War reporting modestlong-term benefit, from frontline versus undefined rear hospi-tal treatment, such as lower PTSD rates. Overall, the reviewshowed insufficient and often contradictory evidence of
individual health benefits from frontline psychiatry, whichcalls for further research on military’s chief mental healthpolicy.
Keywords War stress . PTSD .Military . Veterans . Combatstress control . Forward psychiatry . Combat psychiatry .
Combat and operational stress control
The two overarching objectives of COSC (combat op-erational stress control) are to create and preserve aready force and to promote the long-term health andwell-being of individual Marines and Sailors and theirfamily members. The two objectives are interrelated andare recognized as of paramount strategic importancesince the mission of the Navy and Marine Corps is towin wars and to return good citizens to civilian life afterthose wars are fought. (Department of Navy & U.S.Marine Corps, 2010, pp. 1–2).
The second of a three-part review provides the first-eversystematic investigation into the military’s claims that its warzone mental health policies of preventing evacuation of psy-chiatric casualties are mutually beneficial to the military mis-sion as well as the health and well-being of individual servicemembers and their families. We collectively refer to the USmilitary’s combat operational stress control (COSC) and be-havioral health (BH) programs in war zones as frontline psy-chiatry (see Russell & Figley, 2016). Readers are referred toour first article for a historical and contemporary review of thedebate on frontline psychiatry that became military doctrineduring the First World War (WWI) to end mass psychiatricattrition and disability pensions threatening the military’s
* Charles R. [email protected]
1 Antioch University Seattle, Seattle, WA 98121, USA2 Tulane University, New Orleans, LA, USA
Psychol. Inj. and Law (2017) 10:24–71DOI 10.1007/s12207-016-9279-x

capacity to sustain the war effort as well as bankrupting soci-eties (Russell & Figley, 2016). Effectiveness of frontline psy-chiatry in achieving its explicit goal of conserving the fightingforce has traditionally been measured via return-to-duty(RTD) rates and restricting medical evacuations for psychiat-ric reasons (Russell & Figley, 2016). Over time, however, themilitary has increasingly justified its century-oldmental healthpolicy by messaging frontline psychiatry as mutually benefi-cial not only to the military mission through conserving thefighting force but also through enhancing the health and well-being of deployed personnel and their families (e.g.,Department of the Army, 2006; Russell & Figley, 2016). Forexample, the Pentagon’s top psychiatric advisor at the timewas quoted as stating, BIf people are treated on the front lineswith the expectation that they will go back to duty, they usu-ally recover^ (Rabasca, 2000, p. 50) and, conversely, Bif weevacuate them away from their unit, their psychiatric symp-toms tend to last^ (Rabasca, 2000, p. 50).
Periodically, the military’s claims are challenged on ethical(e.g., Camp, 2014), scientific (e.g., Jones & Wessely, 2003),and even legal grounds (McGeorge, Hughes, & Wessely, 2006;Russell, Zinn, & Figley, 2016). The most recent challenge camefrom a 2003 British High Court decision on a class action suitMultiple Claimants v. MoD (Ministry of Defense), wherebydischarged British soldiers suffering from chronic war stress in-jury, such as posttraumatic stress disorder (PTSD), allegedwrongdoing because of the MoD’s failure to ensure access topreventative frontline psychiatry services (e.g., McGeorge,Hughes, &Wessely, 2006). After extensive review of the empir-ical evidence on the efficacy of frontline psychiatry, the HighCourt dismissed the plaintiff’s claim by upholding the MoD’sargument that frontline psychiatry is generally ineffective inpreventing PTSD or other war stress injury (e.g., McGeorgeet al., 2006). The High Court even went so far as to questionthe ethics of the frontline psychiatry doctrine, echoing distantethical charges of harm from US Army psychiatrists during theVietnam War (e.g., Camp, 1994).
Purpose of the Study
The current study provides the first-ever comprehensive evi-dentiary review of the military’s claims that frontline psychi-atry is mutually beneficial to the military and its warfighters.After describing our methodology, we begin our analysis withan overview of military organizations responsible forconducting mental health-related research. This is followedby an in-depth analysis of investigations directly assessingresearch questions regarding the benefits of frontline psychi-atry to the military mission. Next, we examine studies directlyevaluating differential clinical outcomes between deployedpersonnel RTD via frontline psychiatry and those medicallyevacuated for treatment outside war zones. Lastly, we review
indirect evidence of the potential benefit of frontline psychia-try to deployed personnel and their families from multiplelines of research including related to (a) shame, guilt, andstigma caused by psychiatric evacuations and treatment as apsychiatric patient; (b) protective factors of war stress injury,like PTSD, such as unit morale, cohesion, leadership, andsocial support; (c) promoting resilience by reducing risk ofdeveloping chronic war stress injury (like PTSD); (d)preventing adverse personnel actions, including prematuremilitary discharge and loss of career; (e) posttraumatic growth(PTG); and (f) increasing positive family outcomes. Central toour analysis is the question: What is the evidence supportingthe military’s claims of improved short- and long-term out-comes for deployed individuals diagnosed and treated in thewar zones for combat stress reaction (CSR)/combat operation-al stress reaction (COSR) and/or a psychiatric condition(s) ascompared to those evacuated and treated outside of warzones?
Methodology
An extensive review of the literature was conducted on front-line psychiatry since WWI with emphasis on locating primarysources of research relating to assessing effectiveness, effica-cy, and clinical outcomes. In addition to multiple historicaltreatises on the subject (e.g., Dean, 1997; Holden, 1998;Jones, 1995a, b; Jones & Wessely, 2007; Lerner, 2003;Shepard, 2001), we reviewed current US military COSC-related publications (e.g., DOA, 2006; Department of Navy& U.S. Marine Corps, 2010; Department of Veterans Affairs& Department of Defense, 2010) and the US military’s docu-mented lessons learned for WWI (e.g., Salmon, 1917; Salmon& Fenton, 1929), Second World War (WWII; Glass, 1966),Korean War (e.g., Ritchie, 2002), Vietnam War (e.g., Camp,2014), and the Persian Gulf War (e.g., Martin & Cline, 1996),as well as independent government studies (e.g., Institute ofMedicine, 2014a; Government Accountability Office, 2016).
With regard to published scientific articles and militaryreports, an expansive key word search included relevant termsand phrases, such as forward psychiatry, war psychiatry, com-bat psychiatry, frontline psychiatry, combat stress, neuropsy-chiatry, combat stress control, combat and operational stresscontrol, acute psychiatric casualties, medical evacuation, andpreventative psychiatry, along with specific diagnostic terms(e.g., shell shock, war neuroses, battle fatigue, combat exhaus-tion, combat stress reaction, PTSD), as it pertains to treatment,prevention, resilience, and protective and risk factors.Specifically, we sought out sources cited by the US militaryas the evidentiary bases for positing the benefits of frontlinepsychiatry to service members, but also included researchfrom Australia, Canada, France, Israel, and the UK.
Psychol. Inj. and Law (2017) 10:24–71 25

Military Entities Investigating Mental Health Issues
The Department of Defense (DoD) employs multiple researchagencies whose mission involves investigating mental health-related issues including, but not limited to, the following:
In 2007, the USA dramatically increased funding for mil-itary mental health research by $1 billion for 2007 to 2013,including establishing the Psychological Health ResearchContinuum (PHRC) in 2013 to ensure that deployed personnelreceive the best evidence-based prevention, treatment, andcare possible (Castro, 2014). As depicted in Table 1, thePHRC represents just the latest in a host of military organiza-tions responsible for researching deployment issues since1893. Castro’s (2014) review of recent military mental healthresearch accomplishments includes prospective longitudinaloutcome studies after deployment, clinical trials, epidemiolog-ical studies, such as annual Mental Health Advisory Team(MHAT) surveys, as well as studies on etiology, prevention,screening, and follow-up care.
US Military Research Specific to Frontline PsychiatryOutcomes
Per the Pentagon’s top psychiatry advisor during Operation IraqiFreedom (OIF) and Operation Enduring Freedom (OEF) (Ritchie,2007), BThere is an obvious need for research regarding the effec-tiveness of our early interventions^ (p. 14). The senior advisor’sfrank admission of empirical uncertainty on the matter appears tocontradict previous assertive propositions that BIf people are treatedon the front lines with the expectation that they will go back toduty, they usually recover. But, if we evacuate them away fromtheir unit, their psychiatric symptoms tend to last^ (Rabasca, 2000,p. 50). After the past decade of protracted war, what can DoDresearchers now tell us about the present state-of-the-knowledgeof the health impact from its frontline policies?
Despite the multitude of research agencies whose shared mis-sion is to preserve or improve the mental health of military pop-ulations (see Table 1), our literature review failed to identify asingle study by the US military on the long-term clinical out-comes for deployed personnel receiving its frontline psychiatryservices, let alone any comparative analysis of war stress casual-ties evacuated out of war zones. Numerous military studies andinvestigative reports are available since WWI with regard toRTD, relapse, and evacuation rates, as well as surveys of riskand protective factors in the war zones of Iraq and Afghanistan(e.g., MHAT-I, 2003). However, overwhelmingly, those studiesaddress the benefit to the military in terms of preventing psychi-atric attrition via evacuations. In fact, the only US research ex-amining clinical outcomes from frontline psychiatry is from anonmilitary RAND group (Vaughan, Farmer, Breslau, &Burnette, 2015). Consequently, we expanded our literature re-view to any international investigations, such as by the BritishMoD and Israeli Defense Forces (IDF).
Direct Evidence That Frontline Psychiatry Benefitsthe Military Mission
Since WWI, hundreds of individual and multiple case studieshave been published with regard to the US military’s claimthat frontline psychiatry is beneficial to its mission to fight andwin wars by restricting psychiatric evacuations. Historically,the two pivotal outcome measures for directly assessing theefficacy of frontline psychiatry in reducing attrition have been(a) high RTD rate of deployed service members with warstress injury and/or behavioral health (BH) problems, coincid-ing with (b) low rate of psychiatric evacuations out of warzones.
Research on Preventing Psychiatric Attrition Priorto Current Afghanistan/Iraq Wars
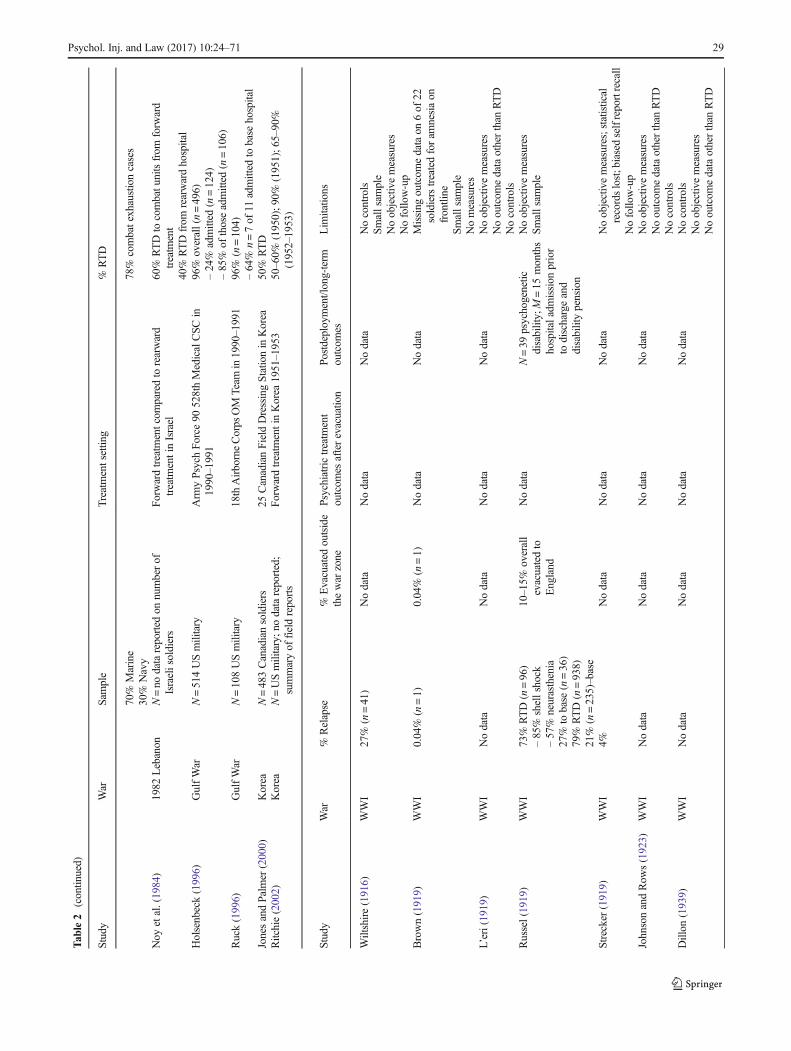
Table 2 provides a comprehensive analysis of frontline psy-chiatry from WWI (1914–1918) to the First Persian Gulf War(1990–1991), representing studies by the militaries ofAustralia, Canada, Israel, France, the UK, and the USA. Inthis research, the range of RTD is 10 to 100%, with lower ratesgenerally reported by base hospitals and general hospitals far-thest from war zones. It is apparent that the reporting of RTDrates is simply a measure of administrative disposition relatedto the military’s explicit bottom line of avoiding psychiatricattrition as opposed to any kind of an assessment of the pos-sible clinical benefits to service members. The net benefit tothe military in terms of preserving manpower is notable.
Table 2 also reveals the overall poor quality of empiricalsupport underlying the military’s frontline psychiatry doctrine.The historical record is replete with published accounts bymilitary clinicians from every war reporting high RTD ratesvia frontline interventions in comparison to soldiers treated inthe rear (e.g., Noy, Levy, & Solomon, 1984), but sometimeswithout any statistical data in terms of the number of person-nel RTD (e.g., Allerton, 1969), and regularly neglecting dura-bility of intervention effects in terms of relapse rates or clinicaloutcomes (e.g., Jones & Wessely, 2003).
Research on Frontline Psychiatry in CurrentAfghanistan/Iraq Wars
Table 3 contains published reports of the US military’s front-line psychiatry programs from the current wars in Afghanistanand Iraq. With the exception of Hoyt et al. (2015), the trend ofignoring the immediate and long-term BH impact from front-line psychiatry interventions has persisted in the twenty-firstcentury. It should be mentioned, however, that Hoyt et al.(2015) do not provide any analysis of clinical outcomes spe-cific to the 467 soldiers RTD or the 46 soldiers psychiatrically
26 Psychol. Inj. and Law (2017) 10:24–71

evacuated even though assigned to the same Army unit. Thisreflects a missed opportunity to evaluate the accuracy of themilitary’s narrative of the clinical benefit of frontline psychi-atry. Nevertheless, Tables 2 and 3 provide convincing proofthat frontline psychiatry is extremely effective in conservingthe fighting force via its RTD policy.
Current Research on Psychiatric Evacuationsout of War Zones
As evident in Tables 2 and 3, for the past 100 years, frontlinepsychiatry has proven to be highly effective in ensuring lowrates of psychiatric evacuations as compared to medical
Table 1 Sample of DoD entities responsible for mental health-related research
Agency Dateoforigin
Servicebranch
Mission Reference
Walter Reed Army Institute ofResearch
1893 Army To conduct biomedical research that is responsive to theDepartment of Defense and US Army requirements anddelivers life-saving products including knowledge,technology, and medical material that sustain the combateffectiveness of the warfighter
http://wrair-www.army.mil/
59th Medical Wing 1941 Air Force To meet the needs of the Air Force through the developmentand performance of medical readiness training forexpeditionary forces
http://www.59mdw.af.mil/
U.S. Army Medical ResearchMateriel Command/MilitaryOperational Medicine Research
1943 Army Psychological health and resilience research is focused on theprevention, treatment, and recovery of soldiers’ and families’behavioral health, which are critical to force health andreadiness. Research is necessary to guide policy and ensureoptimal delivery of behavioral health training and servicesacross the continuum of care and deployment cycle.
https://momrp.amedd.army.mil/
Naval Health Research Center 1959 Navy/MarineCorps
Optimizes the operational health and readiness of our armedforces by conducting research and development to informDoD policy and practice
http://www.med.navy.mil/sites/nhrc/Pages/default.aspx
Uniformed Services University ofHealth Sciences
1972 DoD To educate, train, and prepare uniformed services healthprofessionals, officers, and leaders to directly support theMilitary Health System, the National Security and NationalDefense Strategies of the United States, and the readiness ofour Armed Forces
https://www.usuhs.edu/centers
Center for Study of Traumatic Stress 1987 DoD Develops and carries out research programs to extend ourknowledge of the medical and psychiatric consequences ofwar, deployment, trauma, disaster, and terrorism, includingweapons of mass destruction
http://www.cstsonline.org/
Congressionally Directed MedicalResearch Programs
1992 DoD To transform healthcare for Service Members and theAmerican public through innovative andimpactful research
http://cdmrp.army.mil/
Deployment Health Clinical Center 1994 DoD To advance excellence in psychological healthcare across theMilitary Health System by enhancing care quality,effectiveness, and efficiencies; facilitating the translation ofresearch to practice; and providing leadership, advocacy, andimplementation support
http://www.pdhealth.mil/
Combat Casualty Care ResearchProgram
2001 Army To drive medical innovation through the development ofknowledge and materiel solutions for the acute and earlymanagement of combat-related trauma, includingpoint-of-injury, en route, and facility-based care
https://ccc.amedd.army.mil/Pages/default.aspx
Consortium for Health and MilitaryPerformance
2006 DoD To conduct and translate basic and clinical research in militaryhuman performance, so as to inform the development ofeducational products, clinical products, clinical carepathways, operational guidelines,and health policies
https://www.usuhs.edu/mem/champ
Psychological Health/TraumaticBrain Injury Research Program
2007 DoD Establish, fund, and integrate both individual and multi-agencyresearch efforts that will lead to improved prevention,detection, and treatment of PH/TBI
http://cdmrp.army.mil/phtbi/default.shtml
Center for Rehabilitation SciencesResearch
2011 DoD To advance the rehabilitative care for service members withcombat-related injuries
http://crsr.org/#/
Psychol. Inj. and Law (2017) 10:24–71 27

Tab
le2
Researchon
frontline
psychiatry/COSCeffectivenessin
preventin
gpsychiatricattrition
Study
War
Sample
Treatmentsettin
g%
RTD
Wiltshire(1916)
WWI
N=150UKsoldierswith
shellshock
GeneralhospitalinFrance
Nodata
Brown(1919)
WWI
N=22
UKsoldierstreatedwith
light
hypnosis
HospitalinFrancewar
zone
70–90%
overall;66%
oftreatm
entsam
plefor
amnesia(n=15)
L’eri(1919)
WWI
N=600French
soldierstreatedin
1916;N
=4000
treated1916–1919
2ndArm
yin
France
91%
100%
Russel(1919)
WWI
N=132Canadiansoldiersadmitted
tospecialty
hospitalinAugust1
917
N=1341
admitted
4monthsin
1917
CanadianStationary
hospitalinFrance
Nodata
Strecker
(1919)
WWI
N=400USmilitary
HospitalinFrancewith
inartillery
range.
4-dayaverage
65–75%
JohnsonandRow
s(1923)
WWI
N=5000
UKsoldiersadmitted
with
shellshock
NYDNCentre5thArm
yin
1917
55%
tocombatu
nits
Dillon
(1939)
WWI
N=4235
UKsoldiers
NYDNCentrefor3rdArm
yat6Statio
nary
Hospitalin1918
64%
CooperandSinclair(1942)
WWII
N=207Australiansoldiers
War
neuroses
clinicin
Tobruk
during
1941
80%
overall
–33%
(n=79)combat
–68%
(n=48)reassigned
GrinkerandSp
iegel(1943)
WWII
N=1720
USmilitary
95th
GeneralHospitalN
orth
Africain
1943
53%
overalln
=909
–Estim
ated
2%RTDcombatd
uty
Bartemeier,K
ubie,
Menninger,R
omano,
andWhitehorn
(1946)
WWII
USArm
yNodataon
samplesize
Battalio
nAideStatio
n-ClearingStatio
n-Sp
ecialty
hospitalo
utof
war
zone
-Generalpsychiatrichospital
50%
50-60%
80%
30%
Hunter(1946)
WWII
N=50
UKsoldiersin
1943
Forwardpsychiatriccenter
inItaly
<4days
30%
RTDto
combatu
nits;6
0%reassigned
Glass
(1947)
WWII
N=393USmilitary
Divisionneuropsychiatricunitduring
Apennines
Cam
paignin
1945
54%
overall
–30%
tocombatu
nits
LudwigandRanson(1947)
WWII
N=346USmilitary
random
lyselected
who
wereRTDto
combatu
nits
Forwardpsychiatriccenters
68%
returned
tocombat
HansonandRanson(1949)
WWII
N=18,255
USmilitary
admitted;
n=10,350
from
combatu
nitsand
n=7905
from
noncom
batu
nits
Mediterraneanhospitalin1945
72%
overall(n=13,175):
–81%
(n=8365)from
combat
–26%
(n=2698)combatd
uty
–55%
(n=5667)lim
itedservice
LudwigandRanson(1947)
WWII
N=no
dataon
numbersof
USmilitary
referred
from
divisions
Psychiatrictreatm
entcentersfor5thArm
yItalyand7thArm
yFrance
31%
5thArm
y;24%
7thArm
y
BrillandBeebe
(1952)
WWII
N=955USmilitary:M
=13
months
activ
eduty,M
=4.1monthscombat
Forw
ardpsychiatriccenters(preservice
personality
factorsassessed)
26%
of“normal”personality
;14%
with
neurotic
traits;1
3%suggestiv
eneuroses;1
0%overt
neuroses
Gordon(1967)
Vietnam
N=1000
USmilitary
1stInfantryDivisionforw
ardpsychiatry
unit
in1967
98%
(n=976):
–91%
(n=908)
tounits
–7%
(n=68)reassigned
Allerton
(1969)
Vietnam
USArm
yNostatsreported;sum
maryof
field
reports
Arm
ydivision
psychiatry,field,and
evacuatio
nhospitals
95%
1965–1966;
97–98%
1967–1968
Strange(1969)
Vietnam
N=USmilitary
nostatistic
reported;
NavyhospitalshipoffVietnam
in1966
62%
diagnosedwith
psychiatricdiagnosis
28 Psychol. Inj. and Law (2017) 10:24–71
Tab
le2
(contin
ued)
Study
War
Sample
Treatmentsettin
g%
RTD
70%
Marine
30%
Navy
78%
combatexhaustioncases
Noy
etal.(1984)
1982
Lebanon
N=no
datareported
onnumberof
Israelisoldiers
Forwardtreatm
entcom
paredto
rearward
treatm
entinIsrael
60%
RTDto
combatu
nitsfrom
forw
ard
treatm
ent
40%
RTDfrom
rearwardhospital
Holsenbeck(1996)
GulfWar
N=514USmilitary
Arm
yPsychForce
90528thMedicalCSC
in1990–1991
96%
overall(n=496)
–24%
admitted
(n=124)
–85%
ofthoseadmitted
(n=106)
Ruck(1996)
GulfWar
N=108USmilitary
18thAirborneCorps
OM
Team
in1990–1991
96%
(n=104)
–64%
n=7of
11admitted
tobase
hospital
JonesandPalm
er(2000)
Korea
N=483Canadiansoldiers
25CanadianFieldDressingStationin
Korea
50%
RTD
Ritchie(2002)
Korea
N=USmilitary;n
odatareported;
summaryof
fieldreports
Forw
ardtreatm
entinKorea
1951–1953
50–60%
(1950);9
0%(1951);6
5–90%
(1952–1953)
Study
War
%Relapse
%Evacuated
outside
thewar
zone
Psychiatrictreatm
ent
outcom
esafterevacuatio
nPo
stdeployment/long-term
outcom
esLim
itatio
ns
Wiltshire(1916)
WWI
27%
(n=41)
Nodata
Nodata
Nodata
Nocontrols
Smallsam
ple
Noobjectivemeasures
Nofollo
w-up
Brown(1919)
WWI
0.04%
(n=1)
0.04%
(n=1)
Nodata
Nodata
Missing
outcom
edataon
6of
22soldierstreatedforam
nesiaon
frontline
Smallsam
ple
Nomeasures
L’eri(1919)
WWI
Nodata
Nodata
Nodata
Nodata
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Nocontrols
Russel(1919)
WWI
73%
RTD(n=96)
–85%
shellshock
–57%
neurasthenia
27%
tobase
(n=36)
79%
RTD(n=938)
21%
(n=235)–base
10–15%
overall
evacuatedto
England
Nodata
N=39
psychogenetic
disability;M=15
months
hospitaladm
ission
prior
todischargeand
disabilitypension
Noobjectivemeasures
Smallsam
ple
Strecker
(1919)
WWI
4%Nodata
Nodata
Nodata
Noobjectivemeasures;statistical
recordslost;biasedselfreportrecall
Nofollo
w-up
JohnsonandRow
s(1923)
WWI
Nodata
Nodata
Nodata
Nodata
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Nocontrols
Dillon
(1939)
WWI
Nodata
Nodata
Nodata
Nodata
Nocontrols
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Psychol. Inj. and Law (2017) 10:24–71 29

Tab
le2
(contin
ued)
Study
War
%Relapse
%Evacuated
outside
thewar
zone
Psychiatrictreatm
ent
outcom
esafterevacuatio
nPo
stdeployment/long-term
outcom
esLim
itatio
ns
CooperandSinclair(1942)
WWII
Nodata
23%
(n=48)
evacuatedto
base
Nodata
Nodata
Noobjectivemeasures
Noclinicaloutcom
esNofollo
w-up
GrinkerandSp
iegel(1943)
WWII
Nodata
26%
(n=450)
Nodata
Nodata
Noobjectivemeasures
Nocontrol
Nofollo
w-up
Bartemeier,K
ubie,
Menninger,R
omano,
andWhitehorn
(1946)
WWII
Nodata
5%overall
Nodata
Nodata
Nostatisticalreporting;
noobjective
measures
Nooutcom
edataotherthan
RTD
Nofollo
wup
Hunter(1946)
WWII
Nodata
<10%
Nodata
Nodata
Noobjectivemeasures
Smallsam
ple
Nofollo
w-up
Glass
(1947)
WWII
2/3ofthoserelapsingviaother
routes
(e.g.,disease,injury
ormilitary
offense)
46%
Nodata
Nodata
Nocontrols
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
LudwigandRanson(1947)
WWII
24%
(n=51)relapsed
aspsychiatricpatients
9.7%
(n=21)
38.6%
ofRTDperformed
well
incombat;12%
legal
misconduct;2%
KIA
;9%
WIA
;11%
reassigned
indivision;.9%
self-inflicted
wound
Nodata
Reliedon
self-report
Noobjectivemeasures
Nofollo
w-up
HansonandRanson(1949)
WWII
Nodata
28%
overall
(n=5801):
–19%
(n=1986)
combatu
nits
–39%
(n=3095)
noncom
batu
nits
Nodata
Nodata
Noobjectivemeasures
Noclinicaloutcom
esNocontrolg
roup
Nofollo
w-up
LudwigandRanson(1947)
WWII
13%
5thArm
y;28%
7th
Arm
yNodata
Nodata
Nodata
Nostatisticalreporting
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
BrillandBeebe
(1952)
WWII
38.5%
“normal”admitted
afterbreakdow
n;57.5%
“neurotic”;51%
“suggestive”
neuroses;
69.6%
overtn
euroses
21%
of“normal”
personality
types
Nodata
5-year
follo
w-upafter
military
treatm
ent;7%
unem
ployment;38.5%
military
dischargeafter
firsth
ospitalization;
57.5%
“neurotic”;51%
“suggestiveneuroses”;
69.6%
overtn
euroses
Selectio
nbias
insample
Retrospectiv
eassessmento
fpreservice
personality
Noclinicaloutcom
es
Gordon(1967)
Vietnam
Nodata
2.4%
(n=24)
Nodata
Nodata
Noobjectivemeasures
Noclinicaloutcom
esNofollo
w-up
Allerton
(1969)
Vietnam
Nodata
5%1965–1966;
2–3%
1967–1968
Nodata
Nodata
Nostatisticalreporting
Noobjectivemeasures
30 Psychol. Inj. and Law (2017) 10:24–71

Tab
le2
(contin
ued)
Study
War
%Relapse
%Evacuated
outside
thewar
zone
Psychiatrictreatm
ent
outcom
esafterevacuatio
nPo
stdeployment/long-term
outcom
esLim
itatio
ns
Nooutcom
edataotherthan
RTD
Strange(1969)
Vietnam
Nodata
38%
outo
ftheater
hospital
Nodata
Nodata
Nostatisticalreporting
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Nonrandom
allocatio
nNoy
etal.(1984)
1982
Lebanon
Nodata
40%
evacuatedto
rearwardtreatm
ent
inIsrael
40%
tocombatu
nits
Nodata
Nostatisticalreporting
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Nonrandom
allocatio
nNofollo
w-upundertaken
toinvestigaterelapses;p
atientsnot
categorizedby
military
role
Holsenbeck(1996)
GulfWar
Nodata
3.5%
(n=18)of
soldiersadmitted
Nodata
Nodata
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Ruck(1996)
GulfWar
Nodata
3.7%
(n=4)
Nodata
Nodata
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
JonesandPalm
er(2000)
Korea
Nodata
30%
evacuatedto
Japan
Nodata
Nodata
Nocontrols
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Ritchie(2002)
Korea
5–10%
estim
ated
“repeaters”
1951–1953
n=1800
toJapanin
1950
before
frontline
psychiatry
Nodata
Nodata
Nostatisticalreporting
Noobjectivemeasures
Nooutcom
edataotherthan
RTD
Psychol. Inj. and Law (2017) 10:24–71 31

evacuations, thereby achieving the stated goal of avoidingevacuation syndromes. Table 4 summarizes contemporarystudies on psychiatric evacuations and shows that about only7–10% of all evacuations from war zones in Afghanistan andIraq are due to psychiatric reasons. The primary focus of themilitary’s evacuation research is extensively concerned withadministrative disposition, like categorical designation andRTD rates, as opposed to clinical outcomes.
For example, Rundell’s (2006) retrospective analysis of12,480 US military personnel medically evacuated toLandstuhl Germany out of Iraq and Afghanistan theaters, be-tween November 4, 2001, and July 30, 2004, revealed that1264 or 10% of evacuations were for psychiatric conditions.The most frequent psychiatric diagnostic categories were ad-justment disorders (34%), mood disorders (22%), personalitydisorders (16%), anxiety disorders (15%), no diagnosis(16%), and psychotic disorders (6%; Rundell, 2006). Afterpsychiatric hospitalization at Landstuhl, most patients (81%)were sent back to their home stations for outpatient mentalhealth treatment and 14% were transferred to other inpatientpsychiatric settings. The long-term clinical and administrative(i.e., military discharge or retention) rates are unreported(Rundell, 2006). The author emphasized that only 5% of psy-chiatric evacuees were RTD to frontline units after treatmentat Landstuhl (Rundell, 2006). No information on treatment orclinical outcomes is reported (Rundell, 2006). However,Rundell (2006) does offer possible explanations about why ameager 5% of war-stressed personnel were returned to the warzone. He noted that the assumption is that the service memberalready had Bsignificant mental health intervention^ (p. 355).He added that without providing data, evacuated service mem-bers start to Breconstitute^ in a manner preventing Bassimila-tion^ into the war theater (p. 355). In conclusion, Rundell(2006) opined, BAs in prior wars, it appears that rapid recon-stitution of psychiatric patients must be accomplished as nearto the area of operations as possible to facilitate a reasonablechance of return to combat or combat support duty^ (p. 355).The assumption is that RTD is an empirically informed mea-sure for favorable long-term clinical prognosis, while psychi-atric evacuation is generally therapeutically harmful.However, none of the studies in Table 4 describe long-termclinical outcomes of war zone psychiatric evacuees or offerany comparison with counterparts RTD via frontlinepsychiatry.
Likewise, Cohen et al. (2010) analyzed the medical reasonsand RTD rates of 34,006 US military personnel evacuated outof OIF/OEF war zones to Landsthul Germany from January2004 to December 2007. Most common categories for medi-cal evacuation were musculoskeletal and connective tissuedisorders (n = 8104 service members, 24% of total evacua-tions), combat injuries (n = 4713, 14%), neurological disor-ders (n = 3502, 10%), psychiatric diagnoses (n = 3108, 9%),and spinal pain (n = 2445, 7%; Cohen et al., 2010). The factors
most strongly associated with RTD were being a senior offi-cer, having a nonbattle-related injury or disease, and present-ing with chest or abdominal pain, a gastrointestinal disorder,or a genitourinary disorder (Cohen et al., 2010). Conversely,decreased probability of RTD was related to serving in theNavy, Coast Guard, or Marines and presenting with a combatinjury, a psychiatric disorder, musculoskeletal or connectivetissue disorder, spinal pain, or other medical wounds (Cohenet al., 2010). Nearly all (96%) of service members evacuatedfor a physical battle injury were not RTD (Cohen et al., 2010).According to Cohen et al. (2010), 9% of military personnelevacuated for psychiatric reasons were RTD to war zones,including 31 combatants previously diagnosed with TBI, 72with stress reactions, 13 with substance abuse, 67 with depres-sion or bipolar disorder, and 88 with another type of mentaldisorder. No treatment data, clinical outcomes, or long-termfollow-up were reported for either the 271 psychiatric evac-uees RTD or the 2837 service members transported to state-side treatment facilities.
Anecdotal Validation of Frontline PIE/BICEPSPrinciples
Historical overviews of managing war stress in the military’sofficial policy instructions (e.g., DOA, 2006) and medicaltextbooks (e.g., Jones, 1995a), universally refer to repeatedvalidation of frontline psychiatry principles through the unin-tended consequences of failure to learn from past war traumalessons by neglecting frontline psychiatry (e.g., Jones, 1995a;p. 16). Wartime mental health crises in the form of massivepsychiatric attrition via evacuation syndromes are regularlyattributed by the military to its initial failure in implementingfrontline psychiatry PIE (proximity, immediacy, and expec-tancy)/BICEP principles at the outset of WWI (e.g., Salmon& Fenton, 1929), WWII (e.g., Glass, 1966), Korean War(e.g., Jones, 1995a), and the 1973 Arab-Israeli Wars (e.g.,Belenky, Tyner, & Sodetz, 1983). In each periodic war, themilitary reports eventually rediscovering the validity of front-line psychiatry as confirmed by dramatic improvements inRTD rates and significant reduction in psychiatric evacuations(e.g., Belenky et al., 1983; Ritchie, 2002). For instance, duringthe Korean War, after initially evacuating 100% of war stresscasualties, frontline psychiatry was reinstituted to prevent fur-ther psychiatric attrition (Jones, 1995a, p. 16). Consequently,validation of the frontline psychiatry doctrine is reported interms of military-related versus individual clinical outcomesas in the following: BPsychiatric casualties accounted for onlyabout 5% of medical out-of-country evacuations, and some ofthese (treated in Japan) were returned to the combat zone^(Jones, 1995a, p. 16).
In sum, conclusions about the efficacy of frontline psychi-atry is in the research conducted to date mostly from the
32 Psychol. Inj. and Law (2017) 10:24–71

perspective of the logistical benefits to the military and itsdesired outcome of preserving the fighting force by avoidingpsychiatric attrition (i.e., RTD). To that end, there is sufficientevidence that the military profits from frontline psychiatry. Atthe same time, none of the studies reviewed thus far remotelyaddresses questions around the health and well-being of de-ployed service members experiencing war stress injury or oth-er behavioral health disorder, who are compelled by a RTDpolicy to endure repeated war stress exposure.
Does Frontline Psychiatry Enhance the Well-Beingof Deployed Personnel and Families?
Recent arguments used to justify the military’s frontline psy-chiatry policy center around the premise that preventing psy-chiatric attrition via RTD maintains protective factors (seeRussell & Figley, 2016). Conversely, the military posits thatresearch has allegedly shown poorer administrative and clin-ical outcomes for service members psychiatrically evacuatedand treated outside the war zone (Martin & Cline, 1996, p.164). However, is there empirical support for proof of themilitary’s assertions of the health-promoting benefits fromits frontline psychiatry policies?
Direct Empirical Evidence of Frontline Psychiatry’sHealth Benefit
Table 5 contains the results from an exhaustive search of acentury-old body of frontline psychiatry literature. Inclusioncriteria for the research were related to any investigation com-paring any immediate and/or long-term outcomes (other thanRTD) of deployed personnel RTD via frontline psychiatryversus those evacuated and treated outside the war zone.Results of our search yielded only three small retrospectivestudies by the IDF comparing clinical outcomes (PTSD rates)between groups of combat veterans RTD versus those evacu-ated to Israeli hospitals during the 1982 Lebanon War. Moreaccurately, the three IDF publications represent a single lon-gitudinal study starting with the initial report (Solomon &Benbenishty, 1986) and a follow-up analyses at 1 year(Solomon, Weisenberg, Schwarzwald, & Mikulincer, 1987)and at 20 years (Solomon, Shklar, & Mikulincer, 2005).
The IDF research provides the only direct assessment of themilitary’s health benefit claims, thereby constituting the onlyknown empirical foundation for the DoD’s frontline mentalhealth policies. However, that research was conducted in acountry with a military draft and with the vital role of themilitary in the culture of the country acknowledged. In thissense, generalizations from that research to the contemporaryAmerican context must be made with caution.
IDF Research on Longitudinal Effectsfrom Frontline Psychiatry
Solomon and Benbenishty’s (1986) paper reported the RTDand PTSD rates of an unspecified number of Israeli soldierstreated for CSR 1 year after the 1982 LebanonWar (the resultsincluded only relevant percentages). The sample was dividedinto three groups: (a) veterans treated within the war zone viafrontline PIE interventions, (b) veterans evacuated and treatedat general hospitals in Israel, and (c) veterans seeking mentalhealth treatment after the war. Results indicated that beingdiagnosed with CSR was significantly related to developingPTSD regardless of treatment group. In other words, there wasno overall significant difference in clinical outcomes betweenveterans treated by frontline PIE programs or the other condi-tions. However, veterans receiving frontline psychiatry werereported to have significantly lower PTSD rates than evacuees(Solomon & Benbenishty, 1986). This finding appears to lenddirect support for the military’s health benefit claims.
However, aside from the methodological issue of unreport-ed Ns, evacuated veterans with CSR were sent to generalcivilian hospitals and not to specialized military treatment fa-cilities, and no details of treatment are provided. Therefore, itis impossible to know if higher PTSD rates in evacuees rep-resent a by-product of inadequate hospital treatment or actualevidence of the psychiatric harm caused by evacuation.Moreover, as the authors rightly point out, major methodolog-ical flaws seriously limit the weight attributed to the researchfindings aside from the obvious limitations of relying upon 1-year retrospective self-reports and nonrandomized treatmentgroup assignment. For instance, the researchers were unable toassess CSR severity levels at the time of triage leading todecisions regarding evacuation (Solomon & Benbenishty,1986). Consequently, in this study, it is entirely possible thatevacuated veterans represented a more impaired group thanthose RTD.
Reported Dose-Response Benefit from FrontlinePsychiatry PIE Principles
In Solomon and Benbenishty (1986), an effort was made toempirical test the validity of core tenets of frontline psychia-try: veterans RTD via frontline psychiatry were asked to ret-rospectively report how many of the frontline PIE principlesthey received 1 year prior. The authors found no statisticallysignificant benefit in the number of PIE principles applied, butreported a modest cumulative trend whereby lower PTSDrates were associated with more PIE principles applied. Forexample, 71% of soldiers RTD who received no PIE-relatedintervention developed PTSD within 1 year after the war, incontrast to a 40% PTSD rate if veterans RTD received all threeprinciples (Solomon & Benbenishty, 1986).
Psychol. Inj. and Law (2017) 10:24–71 33

Tab
le3
Frontline
psychiatry
workloadandoutcom
edataduring
Afghanistan
andIraq
wars
Source
Deploym
ent
Totaln
umbers
receivingCOSC
/BH
Num
ber(%
)of
RTDin
war
zone
Num
ber(%
)of
relapsein
war
zone
Num
ber(%
)of
psychiatric
evacuatio
nsouto
fwar
zone
Num
ber(%
)receivingBH
treatm
entinwar
zone
Deploym
ent
outcom
esafterBH
treatm
entinwar
zone
Postdeployment
outcom
esof
personnel
RTDviafrontline
psychiatry
Postdeployment
outcom
esfor
personnelevacuated
forpsychiatric
condition
MHAT-I
(2003)
Iraq
2002–2003
3312
USmilitary
2643
(80–97%)
Nodata
n=669(20%
)n=440(13%
)excluding
Kuw
ait
Nodata
Nodata
Nodata
RTD36
of508(7%)
Nootheroutcom
edata
MHAT-II
(2005)
Iraq
Nodata
USmilitary
Nodata(80–100%
)Nodata
Nodata
Nodata
Nodata
Nodata
Nodata
Scott(2005)
Iraq
170UKsoldiers
receivingPIE
atFM
HTField
Hospital
N=123(72%
)–n=109adjustment
disorder
–n=8somatoform
disorder
–n=1generalized
anxiety
–n=1harm
ful
alcoholu
se–n=2delirium
–n=1phobia
–n=1PT
SD
N=3
N=47
(28%
)–n=23
major
depression
–n=7intentional
self-harm
–n=7adjustment
disorder
–n=4generalized
anxiety
–n=2harm
ful
alcoholu
se–n=1phobia
–n=1PT
SD–n=1dissociatio
n–n=1hypomania
Nodata
Nodata
Nodata
Nodata
Hung(2008)
Iraq
First6
months
of2008
N=49,770
Retrospectiv
ereview
ofdisposition
via
COSC
Workload
andActivity
Reportin
gSy
stem
(COSC
-WARS)
Overall,
99%
RTD
90.8%
(n=45,100)
RTDwithout
limitatio
ns;4
.4%
(n=2185)RTD
with
limitatio
ns;
3.4%
(n=1700)
“rest”(senttoa
nonm
edical
supportu
nit,
typically
farther
from
the
frontlines);0
.91%
(n=450)
“referred”
toa
higher
levelo
fmedicalcare
intheater
Nodata
n=335(0.67%
)n=5871
Psychiatric
diagnoses:
Depression
(n=1389)
Anxiety
(n=928)
Nicotineproblem
(n=1002)
ASD
/PTSD
(n=720)
Substance
abuse
(n=192)
Other
problem
(n=1640)
99.3%
Nodataon
relapseor
clinicaloutcom
es
Nodata
Nodata
Potter,Baker,
Sanders,
and
Peterson
(2009)
Iraq
War
N=57
USmilitary
personnelreferred
toa2-day
restorationcenter
inIraq
100%
RTDfor
(nodata)
treatm
ent
completers;67%
Nodata
Nodata
Nodata
Nodata
Nodata
Lackrandom
assignment;no
controls;selectio
nbias;h
igh
noncom
pleterrate
34 Psychol. Inj. and Law (2017) 10:24–71

Tab
le3
(contin
ued)
Source
Deploym
ent
Totaln
umbers
receivingCOSC
/BH
Num
ber(%
)of
RTDin
war
zone
Num
ber(%
)of
relapsein
war
zone
Num
ber(%
)of
psychiatric
evacuatio
nsouto
fwar
zone
Num
ber(%
)receivingBH
treatm
entinwar
zone
Deploym
ent
outcom
esafterBH
treatm
entinwar
zone
Postdeployment
outcom
esof
personnel
RTDviafrontline
psychiatry
Postdeployment
outcom
esfor
personnelevacuated
forpsychiatric
condition
N=38
(67%
)completed
the
2-dayprogram
N=19
didnot
completeeither
RTDearly,
medically
evacuated,or
required
extended
treatm
ent
RTDfortotal
sample
Nopostdeployment
outcom
edata
beyond
RTD
status
Nocomparisonof
RTDvs.
evacuationgroup
Ogle,Bradley,
Santiago,
and
Reynolds
(2012)
Afghanistan
12months
deploy
toRegional
Com
mand
East
16,000
USmilitary
individual
appointm
entsfor
COSC
and/or
BH
Nodata(99.2%
)Nodata
(0.8%)
About
9560
individual
appointm
ents
forBH
Nodata
Nodataforpersonnel
receivingCOSC
/BH
during
deployment
Nodata
Hoytetal.
(2015)
Afghanistan
9months
deploy
with
4000
mem
ber
Arm
yStryker
Brigade
Com
bat
Team
Nodata
467(97%
)—BH
only
Nodata
46(8%)
513(13%
)97%—RTD
Nodataforpersonnel
receivingCOSC
/BH
during
deployment
719of
3284
(21%
)brigademem
bers
screened
before
returninghomeas
moderatetohigh
risk
364sought
BHcare
ingarrison
and19
admitted
psychiatric
hospitalizations—no
outcom
edata
158referred
toBHafter
positivescreeningon
90–180-day
reassessment
Nodata
Psychol. Inj. and Law (2017) 10:24–71 35

However, caution is warranted in drawing conclusionsabout the efficacy of PIE principles in this research. Perhapsmost importantly, the reported trend, while generally lendingpositive support for frontline psychiatry, did not reach statis-tical significance. More than half (52%) of those RTD viafrontline psychiatry developed PTSD within a year as com-pared to 66% of soldiers evacuated to a general, nonmilitaryhospital (Solomon & Benbenishty, 1986). With regard to theprinciple of expectancy of RTD, there was no statisticallysignificant difference of PTSD rates, in that 55% to 62% ofsoldiers RTD were eventually diagnosed with PTSD(Solomon & Benbenishty, 1986). Moreover, the type andquality of hospitalized psychiatric treatment of evacuees wasnot reported, thereby limiting any conclusion about the com-parative benefit from frontline interventions and evacuees.Regardless of the study’s lack of rigor, the initial IDF findingsprovide at least tacit, provisional support for frontlinepsychiatry’s purported health benefits that would have benefit-ed had the US military conducted further research.
1987 IDF Research of Frontline Psychiatry’s HealthBenefits
The second IDF study compared outcomes from both front-line psychiatry and psychiatric evacuations and involved atotal of 470 Israeli veterans 1 year after the 1982 LebanonWar (Solomon, Weisenberg, Schwarzwald, et al., 1987). PerTable 5, 155 combat veterans who received frontline PIE treat-ment for CSR were compared to 315 veterans evacuated torear hospitals for treatment of CSR, matched to a controlgroup of 334 veterans without a diagnosed CSR (Solomon,Weisenberg, Schwarzwald, et al., 1987). Results indicated thatthere were no significant differences in clinical outcomes be-tween groups of veterans with CSR, whether treated at thefrontline or in rear hospitals. In other words, experiencingCSR significantly increased a veteran’s risk of subsequentPTSD diagnosis regardless of treatment setting. Specifically,59% (n = 255) of soldiers in the two CSR groups (frontlinepsychiatry and evacuees), as well as 16% (n = 53) of veteransin the control group, went on to develop PTSD within a yearafter the war. Identical scientific limitations exist in this studyas found in the previous IDF study, which prohibits any firmconclusions regarding frontline psychiatry efficacy.
2005 IDF 20-Year Follow-Up on Long-Term HealthBenefits from Frontline Psychiatry
The last published report on the purported health benefits fromfrontline psychiatry is a 20-year retrospective reanalysis of theprevious IDF studies (Solomon et al., 2005). Solomon et al.(2005) compared 79 veterans diagnosed with CSR who wereRTD after receiving frontline intervention with 156 veteranswith CSR who were evacuated and treated at rear hospitals,
matched to 196 veterans with no documented history of CSRin the war zone (Solomon et al., 2005). Veterans RTD viafrontline psychiatry were also asked to retrospectively recallwhether the frontline treatment they received included the PIEprinciples, replicating the authors’ 1986 study (Solomon &Benbenishty, 1986). In addition, veterans were asked to retro-spectively recall whether they felt recovered from their CSRprior to being RTD (Solomon et al., 2005). Results of theanalysis comparing veterans RTD after frontline psychiatryversus those evacuated revealed no significant differenceswith regard to PTSD diagnosis, that is, in the two targetgroups, 30% (frontline psychiatry) and 41% (evacuated) ofveterans were later diagnosed with PTSD, which are percent-ages that are significantly higher than the one for the controlgroup (Solomon et al., 2005). Interestingly, 14% of veterans inthe control group also developed PTSD (Solomon et al.,2005). Secondary analysis indicated that veterans in the front-line treatment group reported significantly more intrusion andhyperarousal symptoms than those who had been evacuated.However, there were no significant differences between front-line psychiatry and rear echelon treatment on a diverse rangeof outcomes, including avoidance symptoms, global symp-toms of distress, loneliness, perceived social support, interper-sonal functioning, and occupational functioning (Solomonet al., 2005). In their retrospective analysis of PIE principles,Solomon et al. (2005) concluded the presence of a nonsignif-icant, modest dose-response relationship between lower ratesof PTSD diagnosis and the number of PIE principles applied(Solomon & Benbenishty, 1986). For instance, a 25% PTSDrate was found when all three PIE principles were appliedcompared to 32.6% with two principles, 38.5% one principle,and 49.7% with no principles (Solomon et al., 2005). CSRcasualties who felt their RTD was premature reported 50%more PTSD symptoms than those RTD after feeling complete-ly recovered (Solomon et al., 2005). However, the researchersreiterated that the serious methodological flaws mentionedearlier prohibited any causal inferences associated with RTDand evacuation status. Furthermore, the cultural differences inthe Israeli and American military context limit generaliza-tions, as indicated.
Summary of Direct Empirical Testing of FrontlinePsychiatry Health Benefits
Despite the limitations of the IDF research for the contempo-rary American context, some implications can be consideredbecause, although methodologically flawed, the IDF researchoffers the only direct assessment of frontline psychiatry’s cen-tral tenets. In that research, a modest but nonsignificant trendwas replicated, whereby lower PTSD rates were linearly asso-ciated with the number of applied PIE principles, giving ten-tative support for frontline interventions (e.g., Solomon et al.,2005). However, two of three of the IDF’s head-to-head
36 Psychol. Inj. and Law (2017) 10:24–71

Tab
le4
Current
research
ofmedicalevacuatio
nsfrom
Afghanistan
andIraq
war
zones
Study
Sampleof
medicalevacuatio
nsNum
berof
(%)
psychiatric
evacuatio
ns
Primary
psychiatric
diagnosis
Num
ber
(%)
receiving
frontline
COSC/BH
Num
ber
(%)of
relapse
after
initial
RTD
Num
ber(%
)with
know
npsychiatric
diagnosisbefore
deployment
Num
ber
(%)on
>1
deployment
Num
ber(%
)receiving
definitiv
eMH
treatm
entafter
evacuatio
n
Adm
inistrative
disposition
(e.g.,
RTD,retentio
nin
military,ormilitary
discharge)
Harman,
Hooper,and
Gackstetter
(2005)
N=11,183
USmilitary
evacuated
outo
fIraq
in2003
n=769(7%)
Nodata
Nodata
Nodata
Nodata
Nodata
Nodata
Stetz, McD
onald,
Lukey,and
Gifford
(2005)
N=12,480
USmilitary
evacuatedfrom
Iraq
andAfghanistan
n=386(7%)
73(19%
)with
psychotic
disorders
and242(63%
)with
nonpsychoticdisorders
Sixty
N=60
patients(15%
)had
DSM
-IVV-codes
orhadadeferred
diagnosispending
furtherevaluatio
n;suicidalideatio
nsand
self-injurious
behaviorsaccounted
forabout3
%of
the
cases
Nodata
Nodata
Nodata
Nodata
Nodata
Nodata
Turneretal.
(2005)
N=2009
UKmilitary
evacuatedto
UKfrom
Iraq
in2003
n=178(9%)
n=117admitted
toUKhospital
91(78%
)depression
14(12%
)anxiety
4(3%)somatic
2(2%)delusion
Nodata
48% (n
=8-
5)
37%
prior
contactw
ithmentalh
ealth
Nodata
Nodata
M=1.4days
stay
inhospital
34%
RTDn=61
Noclinical
outcom
es
Rundell(2006)
N=12,480
USmilitary
evacuated
toLandstuhl
Arm
yMedical
Centerin
Germanyfrom
OIF/OEFbetweenNovem
ber4,
2001,toJuly
30,2004
n=1264
(10%
)49%
evacuatedduring
thefirst3
months
ofdeployment,
33%
during
the
second
3months
Adjustm
entd
isorders
(34%
)Mooddisorders(22%
)Personalitydisorders
(16%
)Anxiety
disorders(15%
)ASD
(36%
)PTSD
(29%
)Psychotic
(6%)
Bipolar
disorder
(4%)or
substanceabuse
disorder
(5%)
Nodata
Nodata
Nodata
Nodata
81%
evacuated
back
tothe
USAfor
outpatient
follo
w-up
14%
evacuated
toinpatient
5%RTDto
frontline
units
Noclinical
outcom
esor
long-term
data
Peterson,B
aker,
and
McC
arthy
(2008)
Nodata
Contin
gencyAerom
edicalStaging
Facility(CASF
)atBalad
Air
Base,Iraq
Deploym
ent
N=262
52%
depressive
disorders;23%
anxiety
disorders;5%
personality
disorders;
20%
other
Nodata
Nodata
Nodata
Nodata
Nodata
Nodata
Psychol. Inj. and Law (2017) 10:24–71 37

Tab
le4
(contin
ued)
Study
Sampleof
medicalevacuatio
nsNum
berof
(%)
psychiatric
evacuatio
ns
Prim
ary
psychiatric
diagnosis
Num
ber
(%)
receiving
frontline
COSC/BH
Num
ber
(%)of
relapse
after
initial
RTD
Num
ber(%
)with
know
npsychiatric
diagnosisbefore
deployment
Num
ber
(%)on
>1
deployment
Num
ber(%
)receiving
definitiv
eMH
treatm
entafter
evacuatio
n
Adm
inistrative
disposition
(e.g.,
RTD,retentio
nin
military,ormilitary
discharge)
2004
and2006
In2004,only7%
classified
asmoderatelyto
severely
ill(cat.1B);88%
categorizedas
moderately
ill(category1C
)In
2006,50%
classified
asmoderatelyto
severely
illpatients(1B);39%
asmoderatelyill
(1C)
Cohen
etal.
(2010)
N=34,046
USmilitary
medically
evacuatedouto
fOEF/OIF
January2004–D
ecem
ber2007
n=3108
(9%)
Traum
aticbraininjury
(TBI;n=218)
Substanceabuse(SA;
n=98)
Stress
reactio
ns(n=803)
Depressionor
bipolar
disorder
(n=1045)
Other
(n=814)
Nodata
Nodata
Nodata
Nodata
Nodata
RTDN=271
TBIn=31
(14%
)SAn=13
(13%
)Stress
reactio
nn=72
(9%)
Depressionor
bipolarn=67
(6%)
Other
n=88
(11%
)Noclinical
outcom
esor
long-term
data
Hauret,Taylor,
Clemmons,
Block,and
Jones(2010)
N=31,728
USmilitary
evacuated
outo
fIraq
andAfghanistan
2001–2006
(7%)
n=6 8
TBI
Nootherpsychiatric
diagnosesreported
Nodata
Nodata
Nodata
Nodata
Nodata
Nodata
38 Psychol. Inj. and Law (2017) 10:24–71

comparisons between personnel RTD versus evacuationfound no significant differences in the primary clinical out-come measured (PTSD rates; Solomon, Weisenberg,Schwarzwald, et al., 1987; Solomon et al., 2005). In fact, thedominant statistical finding is that experiencing CSR by itselfis a far greater predictor of subsequent harm irrespective oftreatment setting (e.g., Solomon, Weisenberg, Schwarzwald,et al., 1987; Solomon et al., 2005).
Nevertheless, caution in interpreting the IDF’s findings iswarranted especially with regard to comparing outcomes ofevacuated veterans. For example, the military’s stated purposeof psychiatric triage is to determine whether combatants cansafely be retained in war zones with an expectancy of eventualRTD (e.g., DOA, 2006). If combatants are exhibiting signs ofsevere CSR and impairment, they will most likely be evacu-ated per military policy (e.g., DOA, 2006). Logically speak-ing, it is most likely that the groups of evacuated veterans inthe three IDF studies generally represent more severe casesthan those RTD. Although the relationship of CSR severityand PTSD was not evaluated in the aforementioned IDF stud-ies, subsequent investigations report significant association(e.g., Solomon, Benbenishti, & Mikulincer, 1988).Moreover, the nature and quality of hospitalized psychiatrictreatment IDF evacuees received is highly questionable sincesome hospitals were general or civilian in nature and not spe-cialized in treating war stress injury (e.g., Solomon &Benbenishty, 1986). Considering these factors alone, IDF re-ports of essentially equivalent treatment outcomes for evacueeand RTD groups (e.g., Solomon, Weisenberg, Schwarzwald,et al., 1987; Solomon et al., 2005) remain essentially unsup-ported and not indicative of the claimed value of frontlinepsychiatry’s health benefits.
Needed Replication of the IDF Studies in the Twenty-FirstCentury
The PIE/BICEPS principles of modern-day frontline psychia-try are relatively unchanged from WWI or WWII (e.g.,Russell & Figley, 2016). Today, the US military expects95% RTD from its frontline psychiatric policies (see Russell& Figley, 2016). Therefore, we should reasonably not expectsignificant differences in positive clinical outcomes for vet-erans RTD, consistent with the research on the IDF (e.g.,Solomon et al., 2005). However, if twenty-first century vet-erans will be evacuated to specialized centers delivering high-quality, evidence-based treatments (e.g., Department ofVeterans Affairs & Department of Defense, 2010) as opposedto the intervention technology of 1982, we should reasonablyexpect to see notable improvements from the IDF’s baselineoutcome data on evacuees, which may even eclipse that offrontline psychiatry. Better controlled research is direly need-ed on these types of questions.
Partial Evidence of Frontline Psychiatry’s HealthBenefits
The past century of frontline psychiatry has produced a highvolume of case studies, retrospective record reviews, fieldreports, and medical bulletins that offer a partial, albeit incom-plete assessment of its central tenets. Usually, the focus in thematerial is on one aspect or another (e.g., measuring outcomesof personnel RTD, but not evacuees, and vice versa). Thesefractional studies can be divided into five general lines ofinquiry: (a) outcomes of deployed personnel with CSR receiv-ing frontline intervention versus veterans without CSR (seeTable 6); (b) outcomes of deployed personnel receiving front-line psychiatry only (see Table 7); (c) outcomes of deployedpersonnel receiving a supplemental component of frontlinepsychiatry, such as resilience training (see Table 8); (d) out-comes of deployed personnel receiving BH treatment for psy-chiatric conditions in addition to PIE/BICEP interventions(see Table 8); and (d) outcomes of only deployed personnelevacuated and treated outside war zones (see Table 9). Thetables provide only a sampling of a vast literature. Importantly,all the studies reviewed, whether included or not included inthe tables, share major methodological limitations that prohib-it their utility in answering basic questions: BDo deployedpersonnel RTD via frontline psychiatry enjoy better long-term outcomes than those evacuated?^ In short, they criticallyomit necessary comparison groups and rarely provide long-term outcomes. Nevertheless, if the military’s claims of indi-vidual health benefit are generally accurate, we would expectpositive trends across most if not all five lines of investigation.In the following, we review the source material for all fiveareas to ascertain how effective is contemporary frontline psy-chiatry in the war zone with respect to outcome.
1. Outcome Research on CSR and Frontline Psychiatry
The IDF has taken the clear lead among world militarypowers in investigating the effects of CSR and frontline psy-chiatry. The clear majority of IDF studies depicted in Table 6compare a wide array of long-term outcomes of veterans treat-ed for CSR via frontline psychiatry matched with a controlgroup of veterans not diagnosed with CSR and thus not treatedby frontline psychiatry. It bears mentioning that several stud-ies in Table 6 provide unclear descriptions as to whether vet-erans referred to frontline interventions after CSR diagnosesmeans they received frontline psychiatry (e.g., Solomon &Mikulincer, 1992). Other IDF studies clearly specify that re-ferred CSR groups received frontline psychiatry services (e.g.,Solomon et al., 2005). Given the continuity in IDF researchersand methodology, it is reasonable to assume that referral andreceipt of frontline psychiatry are one in the same. Per Table 6,outcomes measured by the IDF include risk of immediate anddelayed onset of PTSD (e.g., Horesh, Solomon, Zerach, &
Psychol. Inj. and Law (2017) 10:24–71 39

Tab
le5
Researchdirectly
comparing
outcom
esfordeployed
IDFpersonnelR
TDversus
evacuatio
n
Study
War
Sam
ple
Treatmentsetting
Assessm
ent
Deploym
ent
outcom
esPo
stdeployment/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
Solomon
and
Benbenishty
(1986)
1982
IsraeliL
ebanon
War
N=“severalhundred”
Israeli
soldiersdiagnosedand
treatedforCSR
.Sam
ple
size
unspecified,only
percentagesreported:
dividedinto
four
groups:
(1)Treated
atfrontline;(2)
treatedwith
inborder
ofwar
zone;(3)
evacuated
togeneralh
ospitalin
Israel;(4)
sought
psychiatrichelp
after
deploymentw
hileon
leave
FrontlinePIE
treatm
ent
Bygroups:
(1)=
43%
atfront
(2)=
59%
border
(3)=
21%
evacuated
(4)=
28%
onleave
151%
totalu
nexplained
ifincludingrelapses
Retrospective1year
afterwar
assessed
forPIE,R
TD,
andPTSD
Proximity:R
TDrate;frontline
treatm
entv
s.evacuatedto
rear
hospitalinIsrael
Immediacy:q
ueried
iftreatm
entreceivedwith
inhours,days,w
eek,or
after
thewar
Expectancy:
1year
after
ceasefirequeriedabout
perceptio
nsof
PIE
treatm
entg
oals
(e.g.,RTD)
93%
Nodata
Overall,
34%
ofRTDdiagnosedwith
PTSD
1year
afterthewar
vs.74%
ofthoseevacuatedto
rear
orsought
treatm
entafter
deployment
–Proxim
itydidnotsignificantly
reduce
PTSD
:52%
ofRTDafterfrontline
treatm
entd
eveloped
PTSD
vs.66%
evacuatedto
rear
–59%
ofRTDafterPIE
treatm
entat
border
developedPTSD
vs.66%
evacuatedto
rear
–Im
mediatetreatm
entsignificantly
reducedPT
SD:5
4%of
44%
soldierstreatedim
mediately
developedPTSD;7
3%of
26%
soldierstreatedwithin
1day;
56%
of29%
treatedwith
in2or
moredays;
and74%
of24%
afterthewar
Expectancydidnotsignificantly
reduce
PTSD
,but
lowered
rates:55%
of53%
soldiersRTDatallcost
developedPTSD;6
2%of
40%
RTDifcapable;and67%
of23%
not-RTD
–Trend
ofcumulativebenefito
fPIE
reported,but
notstatistically
significant:
Num
berof
PIEprinciples
/RTD%
/PTSD
%0/2
2/7
11/2
3/6
42/4
8/5
93/6
0/4
0
Nostatisticaldataexcept
%Sm
allsam
plesize
Lackrandom
izationand
controlg
roup
Severity
ofCSR
notm
easured
Samplingbias
ofpossiblemore
severe
CSR
inevacuatedgroup
Retrospectiv
estudywith
self-report
andrecallbias
Inform
al,unsystematicassessment
ofPIEprinciples
Nodataon
relapse
Measurementerror
(e.g.,all
reported%
total>
100)
Noinform
ationon
treatm
entb
yageneral,nonm
ilitary
hospital
Solomon,W
eisenberg,
Schw
arzw
ald,
etal.(1987)
1982
Lebanon
War
N=470Israelisoldierswith
CSR
:n=155received
frontline
treatm
entfor
CSR
;n=315soldiers
evacuatedto
rear
hospital
treatm
entfor
CSR
,comparedto
controlo
fn=334matched
soldiers
withoutC
SR
Frontlineuseof
PIE
principles;u
nspecified
treatm
entatrearh
ospitals
Retrospectiveassessment
1year
afterthewar
ofCSR
andPT
SD
Nodata
Nodata
Overall,
59%
(n=255)
ofsoldiers
experiencing
CSRdevelopedPT
SD1year
afterthewar
statistically
significantcom
paredto
control
N=53
(16%
)of
thecontrolg
roup
developedPTSD,but
none
sought
treatm
ent
Older
veterans
hadhigher
PTSD
ratesandmarital
status
was
notsignificant
Noreportof
significant
difference
betweenCSR
grouptreatedatfrontline
vs.evacuated
torearhospital
Retrospectiv
estudy
Self-reportand
recallbias
Nodataon
hospitaltreatment
Severity
ofCSR
orim
pairment
notassessed
Solomon
etal.(2005)
1982
Israeli
Lebanon
War
N=79
Israelisoldierswho
received
frontline
treatm
ent
FrontlinePIE
treatm
ent
andunspecifiedrear
hospitaltreatment
20-yearpostwar
assessment
ofmental,physical,
andsocialfunctio
ning
Nodata
Nodata
After
20years,soldiers
diagnosedwith
CSRand
received
frontline
treatm
ent
20-yearretrospectiveself-
reportandrecallbias
40 Psychol. Inj. and Law (2017) 10:24–71

Tab
le5
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ent
outcom
esPo
stdeployment/long-term
outcom
esLim
itations
%RTD
%Relapse
forCSR
;n=156soldiers
with
CSR
evacuatedfor
treatm
entinrear
hospitals;
matched
with
n=194
soldiersnotd
iagnosed
with
CSR
IES
SCL-90R
ULS
PTSD
-IProblemsin
Social
Functioning
Score
SubjectsaskedwhatP
IEprinciples
they
received
and
levelofrecoverybeforeRTD
hadlower
ratesof
PTSD,
psychiatricsymptom
s,and
postwar
socialfunctioning
problems,butn
otstatistically
significant
Cum
ulativetrendof
PIEtreatm
ent
andPT
SDratereported,but
was
notstatistically
significant,
revealing25%
PTSD
ratewhen
allthree
PIE
principles
applied;
32.6%
with
twoprinciples;
38.5%
oneprinciple;and
49.7%
noprinciples
Nosignificantg
roup
difference
inPTSDrate,occupational
functioning
forCSRcasualties
treatedon
frontlinesor
evacuatedto
hospitals
Nostatistically
significant
outcom
esbetweenCSR
casualtiesRTD,and
those
notR
TD
50%
morePT
SDsymptom
sin
CSR
casualtieswho
felt
RTDwas
prem
aturevs.
thoseRTDwho
felt
completelyrecovered
Unableto
substantiatePIE
principles
applied
Nomeasuresof
CSR
severity
Quasi-experim
entald
esign,
lack
random
assignment;
samplingbias.S
mall
samplesize
intheanalysis
oflong-term
effectsof
frontline
treatm
entinthe
comparisongroup(n
=27),
CSR
groupreceiving
frontline
treatm
ent(n=24)
ascomparedto
theCSR
groupreceivingrear
echelontreatm
ent(n=64)
Unspecified
hospitaltreatment
Psychol. Inj. and Law (2017) 10:24–71 41

Ein-Dor, 2011), multiple somatic complaints (e.g., Ginzburg& Solomon, 2011), harmful drinking (e.g., Solomon &Mikulincer, 1992), global psychiatric distress (e.g., Solomon&Mikulincer, 1988), poor physical health (e.g., Benyamini &Solomon, 2005), as well as postdeployment effects on marital(e.g., Solomon & Mikulincer, 1992), family (e.g., Zerach,Solomon, Horesh, & Ein-Dor, 2013), parenting (e.g.,Solomon, Debby-Aharonl, Zerach, & Horesh, 2011), and oc-cupational (e.g., Solomon, Mikulincer, & Kotler, 1987) func-tioning, along with secondary traumatization of militaryspouses (Solomon et al., 1992).
The research designs of studies in Table 6 permit a partialassessment of frontline psychiatry’s efficacy in preventing ad-verse health effects. Results from this line of research reveal auniversal pattern whereby CSR alone is significantly associatedwith negative impact on nearly every individual and family-related outcome measure regardless if veterans received frontlinepsychiatry or not (see Table 6). Furthermore, the cumulativeeffects of repeated CSR are reported to coincide with progres-sively poorer clinical outcomes (e.g., Solomon, Mikulincer, &Jakob, 1987; Solomon, Oppenheimer, Elizur, & Waysman,1990), which has negative implications for the military’s mentalhealth policies of repeated RTD until individuals are deemed tooimpaired or dangerous to remain inwar zones (e.g., DOA, 2006).
Solomon et al. (2005) offered the following conclusion fromtheir 20-year longitudinal study on CSR and frontline psychiatry:BAlthough persons with combat stress reactions may recover,combat stress reaction often crystallizes into chronic PTSD andplaces casualties at risk for chronic PTSD^ (p. 2312) adding that,BAs the disease evolves over time, pathological changes anddebilitating co-morbidity may become fixed and irreversible^(p. 2312). Importantly, the IDF studies reflect only the outcomesof veterans who remained in war zones after experiencing CSRwho may still do better after deployments than their evacuatedcounterparts. However, it is equally, if not more, likely that theopposite may be the case—especially if the IDF’s findings provereplicated that suffering CSR by itself may be sufficient to causenegative health outcomes.
Methodological limitations, such as the absence of ran-domization, lack of adequate control groups (e.g., no compar-ison of evacuated veterans with CSR), and inherent potentialbias from retrospective reporting (see Table 6), prevent anycausal inferences about possible benefits or adverse healtheffects from frontline psychiatry. It remains possible, however,that a control group of evacuated veterans with CSRmay haveworse outcomes than those receiving frontline psychiatry(e.g., Martin & Cline, 1996), but this remains conjecture.
2. Outcome Research on Personnel Receiving OnlyFrontline Psychiatry
Table 7 contains several uncontrolled outcome studies narrowlyfocusing on war-stressed veterans receiving only frontline
intervention. For example, a UK study (Jones, Fear, Jones,Wessely, & Greenberg, 2010) followed 825 British soldiers whoreceived frontline psychiatry/COSC during an Iraq War deploy-ment. Results indicated that 73% of soldiers RTD after frontlineintervention remained in the military 2 years following their de-ployment, but the researchers offered no comparative analysis forsoldiers evacuated outside the war zone or those not receivingfrontline psychiatry (Jones et al., 2010). Despite the inherent meth-odological limitations in this study, one can reasonably concludethat most British veterans RTD after breaking down in war zonesare not readily discharged by the MoD. It is unclear, however,whether the 73%career retention reflects the effectiveness of front-line psychiatry, per se, or the MoD’s mental health policies, orboth. For example, fundamental differences between MoD andDoD mental health policies have been reported with regard todeployment length, regulating the amount of war stress exposure,and access to definitive treatment of war stress injury (e.g., Fearet al., 2010). Therefore, it is problematic to generalize UK researchon frontline psychiatry to the US military.
US military researchers recently published a single casestudy on career retention in a deployed soldier diagnosed withacute combat-related PTSD who was RTD after successfullycompleting a 2-week COSC program in Iraq (e.g., Mattila,Crandall, & Goldman, 2011). The soldier was eventually pro-moted in rank after returning home from deployment and waspending a second deployment (e.g., Mattila et al., 2011).Therefore, there is emerging evidence that frontline psychiatrydoes not harm career standing. The absence of an evacueecomparison precludes any further interpretation. In addition,Hoyt et al. (2015) reported that 97% of 513 US soldiers de-ployed to Afghanistan were RTD after receiving frontline psy-chiatry with the remainder evacuated. The US researchers alsoreported postdeployment outcomes for the 4000-member unit,including 365 soldiers seeking mental healthcare shortly afterreturning home, 19 admitted as psychiatric inpatients, and 158members referred for BH treatment after screening positive formental health problems several months later (Hoyt et al.,2015). It is unclear, however, how many soldiers receivingpostdeployment BH treatment were of the 513 RTD via front-line psychiatry (Hoyt et al., 2015). No data were provided onthe 46 soldiers psychiatrically evacuated out of the war zone,and there was no long-term outcome data reported on thosewho received frontline psychiatry and BH services (Hoytet al., 2015). That said, the research constitutes the first USmilitary study that examines frontline psychiatry andpostdeployment adjustment.
3. Outcomes of Deployed Personnel Receiving SupplementalFrontline Psychiatry Interventions
Table 8 contains various studies on deployed personnel re-ceiving either some type of supplemental or additive frontlinepsychiatry/COSC intervention (e.g., resilience training). The
42 Psychol. Inj. and Law (2017) 10:24–71

nonmilitary RAND research agency investigated the MarineCorps’ version of frontline psychiatry/COSC, calledOperational Stress Control and Readiness (OSCAR) program(Vaughan et al., 2015). In that study, the health benefits fromextensive predeployment OSCAR prevention or resilience train-ing and peer support were examined in a sample of 2523 USMarines deployed to Iraq or Afghanistan who either received thesupplemental frontline psychiatry services, or did not. A widearray of psychiatric, social, physical health, behavioral, andwork-related outcomes were assessed before and after deploy-ment (Vaughan et al., 2015). The researchers found that the onlysignificant benefit that OSCAR provided was an increase in per-sonal help-seeking (Vaughan et al., 2015). More importantly, theresearchers expressed surprise that many clinical outcomes fromthe OSCAR group were generally worse than for Marines whodid not receive the extra prevention intervention, including show-ing higher rates of PTSD, depression, and poor physical health(Vaughan et al., 2015).
In contrast, UK researchers compared the outcomes of 180British soldiers from deployed units receiving frontline peersupport training and implementation via a peer-mentored trau-ma risk management (TRiM) program and units that did notreceive TRiM training (Frappell-Cooke, Gulina, Green,Hacker Hughes, & Greenberg, 2010). Results indicated sig-nificantly reduced scores of psychological distress and anxietyreported after deployment from units receiving TRiM, butlong-term outcomes were not assessed (Frappell-Cookeet al., 2010). The major limitations of this line of researchare the absence of suitable controls or comparison groups, aswell as a lack of long-term outcomes. Thus, the mixed natureof the findings strongly raises the need for a better evidence-base underlying frontline psychiatry’s claims of individualhealth benefits (e.g., Vaughan et al., 2015).
4. Outcome Research on Behavioral Health Treatment inWar Zones
Provision of BH in war zones falls within the frontlinepsychiatry/COSC mission, with the identical expectation ofmaximizing RTD and reducing evacuation (see Russell &Figley, 2016). Referrals for BH treatment include treatmentfor both severe CSR/COSR conditions evolving into psychi-atric diagnosis like PTSD, as well as noncombat-related psy-chiatric disorders (e.g., adjustment disorder due to maritalstrain). Table 8 contains BH treatment outcome studies be-yond mere application of PIE/BICEPS frontline principlesprovided within war zones and to psychiatric evacuees receiv-ing BH treatment outside of war zones. Such an analysis iscritical in evaluating the accuracy of military claims that re-search has demonstrated that RTD is clinically beneficial forservice members versus evacuation. As reflected in Table 8,research on BH treatments in war zones consists primarily ofcase studies or retrospective record reviews. For instance,
three deployed US Marines diagnosed with acute PTSD inIraq were successfully treated with brief exposure therapy,resulting in 100% RTD and 53% PTSD symptom reduction(Cigrang, Peterson, & Schobitz, 2005). The authors reportedthat the Marines returned home with their units, but they pro-vided no postdeployment or long-term outcomes (Cigranget al., 2005). In another US study, 10 deployed personnel wereevacuated to a combat stress clinic within Iraq, at which 6received virtual reality therapy and 4 exposure therapy (e.g.,McLay, McBrien, Wiederhold, & Wiederhold, 2010). APTSD symptom reduction of 67% across both treatmentgroups was reported, along with no significant outcome dif-ferences between treatment groups, resulting in a 100% RTDrate (McLay et al., 2010). No data on relapse orpostdeployment adjustment was provided. Similarly, Mooreand Krakow (2007) reported a 100%RTD rate of 11 deployedUS personnel after receiving frontline psychiatry and BHtreatment (imagery rehearsal) for traumatic nightmares thatresulted in 64% symptom reduction. Additional treatmentstudies include Stoller, Greul, Cimini, Fowler, and Koomar(2012), who randomly assigned 80 US soldiers deployed toIraq to yoga or control groups. They reported significantlylower scores of anxiety and other symptom measures 1 weekafter training, as well as Parrish (2008) reporting that 99% of5000 US personnel deployed to Iraq were RTD after receivingboth PIE/BICEPS and BH treatment, as well as the finding ofonly 5 personnel evacuated for psychiatric treatment outsidethe war zone.
Other war zone clinical research consists of large retrospec-tive record reviews (see Table 8). For instance, Hung (2008)conducted a retrospective analysis of medical records for49,670US personnel who received frontline psychiatry duringtheir Iraq deployment, including 8262 who also received BHtreatment for a psychiatric condition. Hung (2008) reportedthat 99% of psychiatric casualties were RTD and only 355, or0.67%, evacuated outside the war zone. In addition, Schmitzet al. (2012) reported that 99% of 1167 deployed US person-nel were RTD after BH treatment for a psychiatric disorderand only 4% were evacuated outside war zones. Unlike theabove case studies, the analysis of medical records does notinclude clinical outcome data, such as symptom improvement.However, it is certainly implied that RTD coincides withsymptom resolution, with evacuation reserved for treatment-resistant cases. Therefore, on the face of it, the BH treatmentfindings appear quite impressive when significant symptomreduction is paired with reports of 99 to 100%RTD. However,none of the studies reviewed include relapse data. Also, crit-ical questions about the long-term health effects of repeatedexposure to war stress after CSR/COSR and/or having a psy-chiatric condition are ignored. Consequently, the only firmconclusion that can be reached in this line of inquiry is thatthe overwhelming majority (i.e., 97% to 100%) of servicemembers diagnosed and treated for psychiatric conditions
Psychol. Inj. and Law (2017) 10:24–71 43

Tab
le6
Outcomeresearch
onCSR
andfrontline
psychiatry
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
Solomon,
Mikulincer,
andHobfoll
(1986)
1982
Israeli
Lebanon
War
N=382Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=334
soldiersmatched
from
thesameunit
notd
iagnosed
with
CSR
Frontline
PIE
treatm
ent
1-year
postwar
assessmento
fCSR
andperceptio
nof
socialsupportand
lonelin
ess
MCEI
Perceptio
nof
lonelin
ess
Battle
intensity
Nodata
Nodata
Lackof
socialsupportfrom
officersrelatedto
greater
feelings
oflonelin
essand
greaterlik
elihoodof
CSRin
soldiers
Lackof
socialsupportfrom
buddiesassociated
with
greaterlonelin
ess
Intensity
ofbattlewas
also
relatedto
greaterfeelings
oflonelin
essandincreased
likelihoodof
CSR
Retrospectiv
e;self-reportand
recallbias
Nodataon
frontline
treatm
entfor
CSR
Unclear
iftheCSR
groupwas
RTD
afterPIE
vs.
evacuatedor
discharged
Severity
ofCSR
not
assessed
Solomon,
Oppenhei-
mer,and
Noy
(1986)
1973
Yom
Kippur
War
and
1982
Lebanon
War
Severalh
undredsof
Israelisoldiers
diagnosedwith
CSR
during
1973
war;m
atched
with
thesamenumberof
soldiersafterthe
1973
war
Raw
datanotprovided
Noinform
ationifthe
CSR
group
received
frontline
orothertreatm
ent
9-year
postwar
assessmento
fmilitaryretentionand
relapse
Reviewof
military
health
record
profile
ratin
gs
Nodata
1%94%
ofYom
Kippurveterans
diagnosedwith
CSRwere
ratedas
combatready
before
the1973
war,but
only
42%
wereratedcombatready
before
the1982
war
−6%
oftheseveterans
were
discharged
from
military;47%
reassigned
tononcom
batroles
1%relapserateforCSR
during
the1982
war
Retrospectiv
estudy
Exclusive
relianceon
percentagesand
proportio
nsSeverity
ofCSR
not
assessed
Notreatm
entd
ata
Lackof
objective
measures
Solom
onand
Mikulincer
(1988)
1982
Israeli
Lebanon
War
N=382Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=334
matched
soldiers
from
thesameunit
notd
iagnosed
with
CSR;control
ofn=88
soldierswho
didnotd
eploy
Frontline
PIE
treatm
ent
1-year
postwar
assessmento
fPT
SDandsocial
adjustment
PTSD-I
Problemssocial
functio
ning
scale
Prem
ilitary
social
adjustment
Battle
intensity
Nodata
Nodata
Com
batexposureby
itselfdid
notaccount
forpoor
social
functio
ning
1-year
afterthe
war
Being
diagnosedwith
both
CSR
andPTSD
andPT
SDaloneis
significantly
relatedto
poor
postwar
socialfunctio
ning
CSRaloneisnotsignificantly
relatedto
postwar
social
problems
Retrospectiv
estudy;
self-reportand
recallbias
Intensity
ofCSR
not
assessed
Noprecom
bat
assessmentofsocial
adjustment
Solomon,
Mikulincer,
andJakob
(1987)
1982
Israeli
Lebanon
War
N=382Israelisoldiers
diagnosedwith
CSR
atfrontline;
n=384matched
soldiersfrom
the
sameunitnot
diagnosedwith
CSR
CSR
groupwas
referred
for
psychiatric
interventio
nbut
noinform
ationif
treatedand
treatm
entsettin
g(frontlin
evs.
evacuated)
1-year
postwar
assessmento
fCSR
andbattleintensity
Self-report
questio
nnaire.E
ach
Israelisoldier
was
askedifhe
(1)
participated
in
Nodata
Nodata
Soldierswith
previous
CSR
episodeweresignificantly
morelik
elyto
have
another
CSR
episoderegardless
ofperceivedbattleintensity
Under
high
battleintensity,
soldierswith
outp
rior
CSR
episodeweresignificantly
less
1-year
retrospective
study
Noassessmento
flong-term
outcom
eof
repeated
CSR
episodes
Unclear
iftheCSR
groupwas
RTD
afterPIE
vs.
44 Psychol. Inj. and Law (2017) 10:24–71

Tab
le6
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
combatand
(2)had
diagnosisof
CSR
Battle
intensity
ratin
g
likelyto
have
CSR
episodein
thecurrentb
attle
Highbattleintensity
was
significantly
relatedtoCSRin
both
groups
evacuatedor
discharged
Self-reportand
recall
bias
Solomon,
Mikulincer
andKotler
(1987)
1982 Lebanon
War
N=483Israeli
soldiers:n
=285
diagnosedwith
CSR
atfrontline
and
referred
for
psychiatric
treatm
ent;n=198
soldiersfrom
the
sameunitnot
diagnosedwith
CSR
CSR
groupreferred
fortreatm
ent,but
noinform
ationif
received
frontline
PIE
orevacuated
2-year
postwar
assessmento
fCSR
andsomatic
symptom
sHealth
status
PTSD
-I
Nodata
Nodata
CSR
groupreported
significantly
moreworkabsences,alcohol
use,cigarette
use,new
medications,new
onsetchest
pain,and
digestiveproblems
CSR
groupreported
significantly
greaternumberof
somatic
complaintsvs.control
CSR
andPT
SDindependently
andcombinedpredicated
greatersomaticcomplaints
Retrospectiv
estudy
Self-reportand
recall
bias
Unclear
iftheCSR
groupreceived
frontline
treatm
ent
Noprecom
bat
measure
ofsomatic
complaints
Mikulincer,
Solomon,
and
Benbenisht-
y(1988)
1982 Lebanon
War
N=104Israeli
soldiers:d
iagnosed
with
CSRat
frontline
and
referred
for
psychiatric
treatm
ent;all
subjectswere
discharged
from
activ
eduty
afterthe
war
andnowin
reserves
Frontlin
ePIE
treatm
ent
1-year
postwar
assessmento
fCSR
symptom
sandbattle
(CE)events
Interviewscoded
PTSD
-ISC
L-90R
SEP
100%
Nodata
17psychologicaland
somatic
symptom
sof
CSR
reported
by10%
ofsample
TotalPTSD
symptom
scorrelated
with
anxietyduring
combat
CSR
notsignificantly
relatedto
problemsinsocialfunctio
ning
CSRsignificantly
associated
with
PTSD
andpsychiatric
symptom
s1-year
postwar
Veteranswith
CSRareoften
preoccupiedwith
their
breakdow
nscontributeto
postwar
adjustmentp
roblem
s
Retrospectiv
estudy
Self-reportand
recall
bias
Noprecom
bat
assessmento
foutcom
emeasures
Severity
ofCSRnot
assessed
Solomon,
Benbenisht-
i,etal.
(1988)
1982
Israeli
Lebanon
War
N=104Israelisoldiers
diagnosedwith
CSR
atthefrontline
andreferred
for
psychiatric
treatm
ent
Noinform
ationon
CSRgroup
receivingfrontline
treatm
ento
revacuated
1-year
postwar
assessmento
fPT
SD
Premilitary
and
postmilitary
adjustment,combat
experiences,andthe
extent
oftheCSR
episode
Nodata
Nodata
Extento
fCSRepisodeand
specificcombatexperiences
predictsPTSD
Psychologicalsymptom
swere
predictedmainlyby
combat
experiences,andpostwar
functio
ning
was
predicted
mainlyby
prew
arfactors
Implicationof
combat
experiencesandsoldiers’
immediatereactio
nsduring
combatinthegenesisof
subsequent
PTSD
Retrospectiv
estudy
Self-reportand
recall
bias
Smallsam
plesize
Psychol. Inj. and Law (2017) 10:24–71 45

Tab
le6
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
Solomon
and
Flum
(1988)
1982
Israeli
Lebanon
War
N=716Israeli
soldiers:C
SRgroup
(n=382)
diagnosed
andtreatedforCSR
atfrontline;
comparedton=334
non-CSR
group
Frontlin
ePIE
treatm
ent
1-year
postwar
assessmentofprew
arlifeeventsandCSR
PTSD
-IPre-war
LifeEvents
Survey
Nodata
Nodata
Nosignificantrelationbetween
CSR
andpositiv
eandnegativ
elifeeventsbefore
thewar
CSRsignificantly
relatedto
PTSD
diagnosis
PTSDseverity
correlated
with
numberof
negativ
elifeevents
PTSDsignificantly
relatedto
impaired
socialties
Retrospectiv
estudy
Self-reportand
recall
bias
Noprecom
bat
measure
ofPTSD
Severity
ofCSRnot
measured
Solomon
and
Mikulincer
(1988)
1982
Israeli
Lebanon
War
N=483Israeli
soldiers:C
SRgroup
(n=285)
diagnosed
andtreatedforCSR
atfrontline;
comparedton=198
non-CSRgroup
CSR
groupreferred
forpsychiatric
interventio
nat
frontline,but
noinform
ationif
treatm
entw
asreceived
1-and2-year
postwar
assessmento
fCSR
andPTSD
IES
PTSD
-I
Nodata
Nodata
CSRwas
significantly
relatedto
intrusive,avoidance,andother
PTSDsymptom
satboth1and
2years
Totald
istresshigherfortheCSR
groupacross
each
timeperiod
Bothgroups
reported
significantly
lower
avoidant
andintrusivesymptom
satthe
2ndyear
Retrospectiv
estudy
Self-reportand
recall
bias
Unclear
iftheCSR
groupreceived
frontline
treatm
ent
Noprecom
bat
measure
ofPTSD
Nodatatreatm
entfor
theCSRgroup
Solomon
and
Mikulincer
(1988)
1982 Lebanon
Wa r
N=382Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=334
matched
soldiers
from
combatu
nit
notd
iagnosed
with
CSR
Frontlin
ePIE
treatm
ent
1-and2-year
postwar
assessmento
fPT
SD
symptom
sIES
PTSD
-I
Nodata
Nodata
After
1year:
59%
oftheCSR
group
diagnosedwith
PTSD
;15%
controld
iagnosed
with
PTSD
After
2years:
56%
CSR
groupand14%
controld
iagnosed
with
PTSD
CSRassociated
with
intrusion
andavoidancesymptom
sIntrusionsymptom
sdecline
morethan
avoidance
symptom
sovertim
e
Retrospectiv
estudy
Self-reportand
recall
bias
Noprecom
bat
measure
ofPTSD
Severity
ofCSRnot
assessed
Solomon,
Mikulincer,
andBleich
(1988)
1982
Israeli
Lebanon
War
N=382)
Israeli
soldiersdiagnosed
with
CSRatthe
frontlines;n=334
matched
control
frontline
soldiers
notd
iagnosed
with
CSR
Diagnosed
atfrontline
butn
oreportiftreatedat
frontline
orevacuated
1-year
postwar
assessmentv
iaPT
SD-I
SCL-90
Nodata
Nodata
CSR
groupsignificantly
more
likelyto
developPTSD
(n=228)
oftheCSRgroup
diagnosedwith
PTSD
;comparedto
n=50
ofthe
non-CSR
group
CSR
groupsignificantly
higher
clinicalseverity
onallthree
globalsymptom
measures
PTSD
diagnosissignificantly
associated
with
anxiety,
depression,hostility,and
Notreatm
entd
ata
Retrospectiv
estudy
Self-reportand
recall
bias
Severity
ofCSRnot
assessed
46 Psychol. Inj. and Law (2017) 10:24–71

Tab
le6
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
obsessive-compulsive
symptom
sSo
lomon
etal.
(1990)
1973
Yom
Kippur
War
and
1982
Lebanon
War
N=24
Israelisoldiers
who
received
frontline
treatm
ent
forCSR
inboth
1973
and1982
wars;n=39
matched
soldiers
from
thesameunit
with
firsttim
eCSR
in1982
war
only
Frontlin
ePIE
treatm
ent
3-year
post-Lebanon
War
assessed
effects
ofrepeatCSR
PTSD
-IIES
SCL-90-R
SFP
Health
status
interview
PSE
Nodata
Nodata
The
repeatCSRgroupreported
significantly
moresevere
pathologyandalowerlevelof
socialfunctio
ning
than
the
firsttim
eCSR
group
CSR
groupadjustmentand
symptom
atologywere
significantly
worse
follo
wing
thesecond
war
than
afterthe
first
Successfuladjustm
entafter
the
1stC
SRepisodedidnot
inoculateagainstsubsequent
CSR
episodes
Retrospectiv
estudy
Self-reportand
recall
bias
Smallsam
plesize
Noprecom
batd
ataon
outcom
emeasures
Solomon,
Benbenisht-
i,and
Mikulincer
(1991)
1982
Israeli
Lebanon
War
N=65
Israelisoldiers
diagnosedwith
CSR
atfrontline
and
referred
for
psychiatric
interventio
nbut
remainedin
the
military;com
pared
tomatched
control
groupof
unknow
nnumberof
veterans
with
outC
SR
Noinform
ationon
CSRgroup
receivingfrontline
treatm
ento
revacuated
1-,2-,and3-year
postwar
assessment
ofself-efficacy
Com
bat-related
perceived
self-efficacyratin
gPT
SD-I
SCL-90R
Military
record
ofprem
ilitary
adjustment
Nodata
Nodata
Self-efficacyof
theCSR
group
significantly
lower
than
the
non-CSR
controlg
roup
Psychicnumbing
andloss
ofcontrold
uringcombatw
ascorrelated
with
lower
combat-relatedself-efficacy1
and2yearsafterthewar,but
notaty
ear3
CSR
andPT
SDseverity
associated
with
lower
self-efficacy
Higherprem
ilitary
adjustment
ratin
gresultedin
higher
self-efficacyscores
across
time
Retrospectiv
estudy
Self-reportand
recall
bias
Smallsam
plesize
Noreportof
treatm
ent
fortheCSR
group
Noinform
ationon
controlg
roup
Noprecom
bat
measure
ofself-efficacy
S olomon,
Mikulincer,
etal.(1991)
1982
Israeli
Lebanon
War
N=71
Israelisoldiers
identifiedwith
delayedPT
SDgroup2yearsafter
thewar
ended,
with
outp
rior
CSR
during
thewar;
comparedto
n=73
soldiersdiagnosed
with
CSRand
immediateonset
Frontlin
ePIE
treatm
entlikely
butn
otcertainfor
immediateonset
PTSD
group
20-yearpostwar
assessmento
fsocial
supportand
coping
resourceson
PTSD
onset
MCEI
WCC
PSQ
CAQ
Nodata
Nodata
Findings
indicatedthatboth
immediateanddelayedPTSD
casualtiesreported
higher
levelsof
battlestress
than
controlsubjects
Delayed
PTSDcasualties
evincedless
personal
resourcesthan
thecontrol
groupandim
mediatePT
SDcasualtiesevincedstill
less
Retrospectiv
estudy
Self-reportand
recall
bias
Unclear
iftheCSR
groupreceived
frontline
treatm
ent
Noprecom
bat
measure
ofcoping
resourcesand
attributionalstyle
Psychol. Inj. and Law (2017) 10:24–71 47

Tab
le6
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
PTSD;m
atched
with
n=73
control
groupof
veterans
with
outC
SRor
PTSD
diagnosis
2yearsafterthe
war
personalresourcesthan
delayedPTSD
casualties
Delayed
onsetu
sedmore
problem-focused
coping
than
immediateonset
Bothim
mediateanddelayed
onsetP
TSD
reported
lower
officersupport
PTSDcasesattributed
causes
tomorestableandunpredictable
factorsthan
non-PT
SDSolom
onand
Mikulincer
(1992)
1982 Lebanon
War
N=213Israelisoldiers
diagnosedwith
CSR
andreferred
forpsychiatric
treatm
ent;n=116
matched
soldiers
from
combatu
nit
notd
iagnosed
with
CSR
CSR
groupreferred
fortreatm
ent,but
noinform
ationif
received
frontline
PIEor
evacuated
1-,2-,and3-year
postwar
assessment
ofCSR
PTSD
-IIES
SCL-90R
SFP
Health
status
Perceivedself-efficacy
Nodata
Nodata
CSRgroupreported
significantly
greaterPTSD
andpsychiatric
symptom
atologyacross
time
than
controls
Psychiatricsymptom
atologywas
stableacross
timein
theCSR
group,butn
otPT
SDsymptom
sCSR
groupreported
greaterw
ork
absences,smoking,drinking,
newonsetchest,and
back
pain,aswellasdigestive
problems
CSRissignificantly
relatedto
PTSD
CSRgroupreported
significantly
moreproblemsin
social,
marital,work,sexual,and
family
functio
ning
Retrospectiv
estudy
Self-reportand
recall
bias
Noprecom
bat
assessmento
foutcom
emeasures
Severity
ofCSR
not
assessed
Solomon,
Waysm
an,
Levy,etal.
(1992)
1982
Israeli
Lebanon
War
N=120wives
ofIsraelisoldiers
diagnosedwith
CSR;n
=85
wives
ofsoldiersnot
diagnosedwith
CSR
UncertainiftheCSR
groupreceived
frontline
orother
treatm
ent
Secondarytrauma
was
assessed
Wife’sperceptio
nsof
husband’sP T
SDWife’s
SCL-90-R
FES
SCQ
DAS
ULS
SSQ
Nodata
Nodata
CSR
andPT
SDwereboth
independently
and
cumulativelyassociated
with
significantincreasein
wife’s
psychiatricsymptom
sCSRsignificantly
relatedto
PTSD
Current
husbandPT
SDsignificantly
contributesto
wife’sim
paired
social
functio
ning,feelin
gsof
lonelin
ess,adversemaritaland
family
functio
n
Retrospectiv
estudy
Self-reportand
recall
bias
Noprecom
batd
ataon
outcom
emeasures
Severity
ofCSR
not
measured
48 Psychol. Inj. and Law (2017) 10:24–71
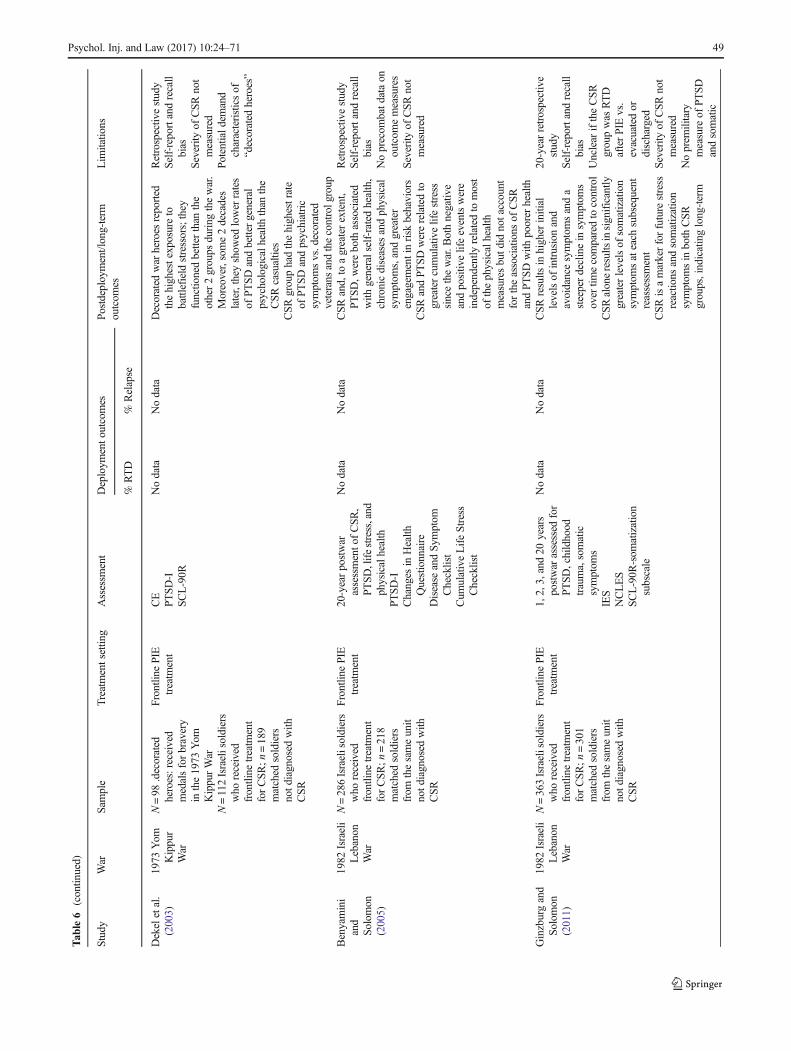
Tab
le6
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
Dekeletal.
(2003)
1973
Yom
Kippur
War
N=98
.decorated
heroes:received
medalsforbravery
inthe1973
Yom
KippurWar
N=112Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=189
matched
soldiers
notd
iagnosed
with
CSR
Frontline
PIE
treatm
ent
CE
PTSD-I
SCL-90R
Nodata
Nodata
Decorated
war
heroes
reported
thehighestexposureto
battlefield
stressors;they
functio
nedbetterthan
the
other2groups
during
thewar.
Moreover,some2decades
later,they
show
edlower
rates
ofPTSDandbettergeneral
psychologicalh
ealth
than
the
CSRcasualties
CSR
grouphadthehighestrate
ofPTSDandpsychiatric
symptom
svs.decorated
veterans
andthecontrolgroup
Retrospectiv
estudy
Self-reportand
recall
bias
Severity
ofCSR
not
measured
Potentiald
emand
characteristicsof
“decorated
heroes”
Benyamini
and
Solom
on(2005)
1982
Israeli
Lebanon
War
N=286Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=218
matched
soldiers
from
thesameunit
notd
iagnosed
with
CSR
Frontline
PIE
treatm
ent
20-yearpostwar
assessmento
fCSR
,PT
SD,lifestress,and
physicalhealth
PTSD-I
Changes
inHealth
Questionnaire
Disease
andSym
ptom
Checklist
Cum
ulativeLifeStress
Checklist
Nodata
Nodata
CSR
and,to
agreaterextent,
PTSD
,wereboth
associated
with
generalself-ratedhealth,
chronicdiseases
andphysical
symptom
s,andgreater
engagementinrisk
behaviors
CSRandPT
SDwererelatedto
greatercumulativelifestress
sincethewar.B
othnegativ
eandpositiv
elifeeventswere
independently
relatedto
most
ofthephysicalhealth
measuresbutd
idnotaccount
fortheassociations
ofCSR
andPTSD
with
poorer
health
Retrospectiv
estudy
Self-reportand
recall
bias
Noprecom
batd
ataon
outcom
emeasures
Severity
ofCSR
not
measured
Ginzburgand
Solom
on(2011)
1982
Israeli
Lebanon
War
N=363Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=301
matched
soldiers
from
thesameunit
notd
iagnosed
with
CSR
Frontline
PIE
treatm
ent
1,2,3,and20
years
postwar
assessed
for
PTSD
,childhood
trauma,somatic
symptom
sIES
NCLES
SCL-90R
-som
atization
subscale
Nodata
Nodata
CSRresults
inhigher
initial
levelsof
intrusionand
avoidancesymptom
sanda
steeperdeclinein
symptom
sovertim
ecomparedto
control
CSRaloneresults
insignificantly
greaterlevelsof
somatization
symptom
sateach
subsequent
reassessment
CSRisamarkerforfuture
stress
reactio
nsandsomatization
symptom
sin
both
CSR
groups,indicatinglong-term
20-yearretrospective
study
Self-reportand
recall
bias
Unclear
iftheCSR
groupwas
RTD
afterPIE
vs.
evacuatedor
discharged
Severity
ofCSR
not
measured
Noprem
ilitary
measure
ofPT
SDandsomatic
Psychol. Inj. and Law (2017) 10:24–71 49

Tab
le6
(contin
ued)
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
impacton
psychological
well-being
Num
berof
adversechild
hood
eventsdidnotp
redictPTSD
andsomaticsymptom
sHoreshetal.
(2011)
1982
Israeli
Lebanon
War
N=369Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=306
matched
soldiers
from
thesameunit
notd
iagnosed
with
CSR
Veteransweredivided
into
4groups,
accordingto
the
timeof
PTSDonset
(e.g.,1983,1984,
2002,and
noPTSD)
Frontline
PIE
treatm
ent
20-yearpostwar
assessmento
fim
mediateand
delayedonseto
fPT
SD;com
bat
exposure
(CE),
PTSD
,childhood
andpostwar
life
events
PTSD-I
IES
LEQ
NCLES
CEratin
g
Nodata
Nodata
ImmediateonsetP
TSD
significantly
relatedtoseverity
ofsubjectiv
eandobjective
levelo
fCE
CSRandCEmostp
redictive
across
alln
egativeoutcom
esfollo
wed
bysocialsupport,
homecom
ingexclusion,
family
conflictand
expressiveness
CSR
was
foundto
bethemost
powerfulp
redictor
ofPT
SDonset
Recency
effectwas
foundwith
morerecent
lifeevents
provingto
bestronger
predictorsof
PTSD
onsetthan
child
hood
events
Delayed-onsetPT
SDwas
found
amongasubstantialnum
berof
non-CSRgroup(16.5%
)
Retrospectiv
estudy
Self-reportand
recall
bias
Unclear
iftheCSR
groupwas
RTD
afterPIE
vs.
evacuatedor
discharged
Severity
ofCSR
not
assessed
Noprecom
bat
measure
ofPT
SDandsocial
adjustment
Solom
onetal.
(2011)
1982
Israeli
Lebanon
War
N=264Israelisoldiers
who
received
frontline
treatm
ent
forCSR;n
=209
matched
soldiers
from
thesameunit
notd
iagnosed
with
CSR
Frontline
PIE
treatm
ent
20-yearpostwar
assessmento
fPTSD
,maritaland
parenting
problems
PTSD-I
DAS
Parentalfunctio
ning
Lifeevents
questio
nnaire
Nodata
Nodata
60%
oftheCSR
groupand10%
controlssoughtpsychotherapy
afterthewar
CSRsignificantly
relatedto
PTSD
CSR
andPT
SDgroups
independently
and
cumulativelyreported
significantly
lower
marital
satisfactionandincreased
parentingproblemsthan
non-CSRandnon-PT
SDgroups
Emotionalsharing
moderated
PTSDseverity
andparenting
functio
ning,but
notm
arital
adjustment
Retrospectiv
eSelf-reportand
recall
bias
Noprecom
bat
measure
ofmarital
andparenting
functio
ning
Severity
ofCSR
not
assessed
50 Psychol. Inj. and Law (2017) 10:24–71

Tab
le6
(contin
ued)
Study
War
Sample
Treatmentsettin
gAssessm
ent
Deploym
ento
utcomes
Postdeployment/long-term
outcom
esLim
itatio
ns
%RTD
%Relapse
Zerachetal.
(2013)
1982
Israeli
Lebanon
War
N=208Israeli
soldiers:C
SRgroup
(n=128)
diagnosed
andtreatedforCSR
atfrontline;
comparedto
n=80
non-CSR
group
Frontline
PIE
treatm
ent
1-,3-,and20-year
postwar
assessment
ofCSRandfamily
cohesion
IES
FES
Nodata
Nodata
CSRgrouphadsignificantly
greateravoidancesymptom
svs.control
Intrusiveandavoidance
symptom
sgradually
decreasedover
timein
both
groups
CSRgroupreported
significantly
lower
family
cohesion
ateach
assessmentp
eriod
CSRgroupreported
significantly
greaterPTSD
symptom
sSeverity
ofPTSD
symptom
snegativ
elyim
pacted
family
cohesion,and
lowfamily
cohesion
increasedPTSD
symptom
s
Retrospectiv
estudy
Self-reportand
recall
bias
Unclear
iftheCSR
groupreceived
frontline
treatm
ent
Noprecom
bat
measure
offamily
cohesion
andPTSD
AUDIT-C
Alcohol
Use
DisordersIdentificationTest-Consumption,CAQCausalA
ttributionQuestionnaire,D
ASDyadicAdjustm
entS
cale,F
ESFamily
EnvironmentS
cale,D
RRID
eploym
entR
iskand
Resiliency
Inventory,HPQHealth
Performance
Questionnaire,IESIm
pactof
EventsScale,LE
QLifeEventsQuestionnaire,M
CEIMilitary
Com
pany
EnvironmentInventory(socialsupport),N
CLE
SNegativeChildhood
LifeEventScale,O
Q-45OutcomeQuestionnaire-45,PBQ-SRPeritraumaticBehaviorQuestionnaire-Self-Rating,PCL-M
PTSDChecklist-Military
Version,P
HQ-2/8PatientHealth
Questionnaire2or
8items,PIS
PTSD
InventoryScale,P
SEPerceived
Self-EfficacyScale,P
SQPerceivedStressQuestionnaire,U
LSUCLALonelinessScale,SCL-90-R
Symptom
Checklist-90-Revised,
SCQSo
maticCom
plaintsQuestionnaire,SF-12Sh
ortF
orm
Health
Survey,SF
PProblemsin
SocialFunctioning
Scale,SSQSo
cialSu
pportQ
uestionnaire,W
CCWaysof
CopingChecklist
Psychol. Inj. and Law (2017) 10:24–71 51

Tab
le7
Outcomeresearch
onfrontline
psychiatry
only
Study
War
Sam
ple
Treatmentsettin
gAssessm
ent
Deploym
ent
outcom
esPo
stdeployment/long-term
outcom
esLim
itatio
ns
% RTD
% Relapse
Jones
etal.
(2007)
WWI
N=3580
UKsoldiersadmitted
toinpatient
NYDNCentrein
France
M=25
days
inpatient
war
zone
4Stationary
Hospital
NYDNCentre
M=11.2monthsin
war
zone
before
admission
40.3%
brokedown
after6monthsCE
9%2-year
CEold
sergeants
35% reassigned
in convales-
cent
17%
RTD
n=606
20% evacuated
tobase
Ofthe
606RTD,15(2.5%)w
erereadmitted
to4Stationary
Hospitalshortly
afterdischarge
n=93
(2.6%)of
thetotalsam
pleof
3580
soldiershadtwohospitaladm
issions
Lackrandom
assignment
Onlyoutcom
emeasure
isRTD
Nocomparisonof
RTDvs.
evacuatio
ngroup
Jones
etal.
(2010)
Iraq
War
N=825Britishmilitary
personnel
deployed
toIraq
diagnosedwith
COSR
,who
received
frontline
treatm
ent(Field
MentalH
ealth
Team
s-FM
HTs)
Frontline
FMHTtreatm
entin
Iraq
usingBICEPS
FMHTrecordsreview
indicatin
gshort-term
outcom
eof
RTDor
evacuatio
nduring
deployment
Military
record
review
oflong-term
outcom
eifretained
vs.dischargedfrom
military
71.6%
RTD
with
adocument-
ed short-term
military
work
outcom
e
73.5%
ofthoseRTDhadadocumented
long-termmilitary
workoutcom
eevidentby
retentionforgreaterthan
2years
postdeployment
Adjustin
gforpotentialconfounders,a
shorter
servicelength
andremovalfrom
the
operationaltheater
wereboth
strongly
associated
with
prem
aturedischarge;
however,itw
asnotpossibletodeterm
inethe
severity
ofthepresentin
gmentalh
ealth
problem
andassess
whether
thisim
pacted
outcom
e
Retrospectiv
erecord
review
Severity
ofCOSR
notassessed
Nocomparisonof
evacuee
treatm
ento
rsoldierswith
CSRnottreated
byFM
HT
Mattila
etal.
(2011)
Iraq
N=1;
singlecase
study,
24-year-oldArm
yCorporal
with
COSRaftercombat
involvingkilling
ofinsurgents
2-weekCOSCfitness
program,consultatio
nwith
unitleaders;sleep
medication;
coping
skills;
individualsupportiv
ecounselin
g
Nodata
RTD;
completed
deployment
with
unit
1½yearsfollo
w-up,subjectw
asprom
oted
inrank,re-enlistedandpending2nd
deployment
Singlecase
study
Nopsychometrics
Nolong-term
follo
w-updata
on2nd
deployment
Hoyt
etal.
(2015)
Afghanistan
9monthsdeploymentw
ith4000
mem
berArm
yStryker
Brigade
Com
batT
eam
N=513(13%
)
COSC/BHem
bedded
with
StrykerBrigade
combat
team
Nodata
97%—RTD
467(97%
)—BHonly
46(8%)
evacuated
719of
3284
(21%
)brigademem
bersscreened
before
returninghomeas
moderateto
high
risk
364soughtBHcareingarrison
and19
admitted
psychiatrichospitalizations—no
outcom
edata
158referred
toBHafterpositiv
escreeningon
90–180-day
reassessment
Nodatafor
personnel
receiving
COSC/BH
during
deployment
Noclinical
outcom
edata
52 Psychol. Inj. and Law (2017) 10:24–71
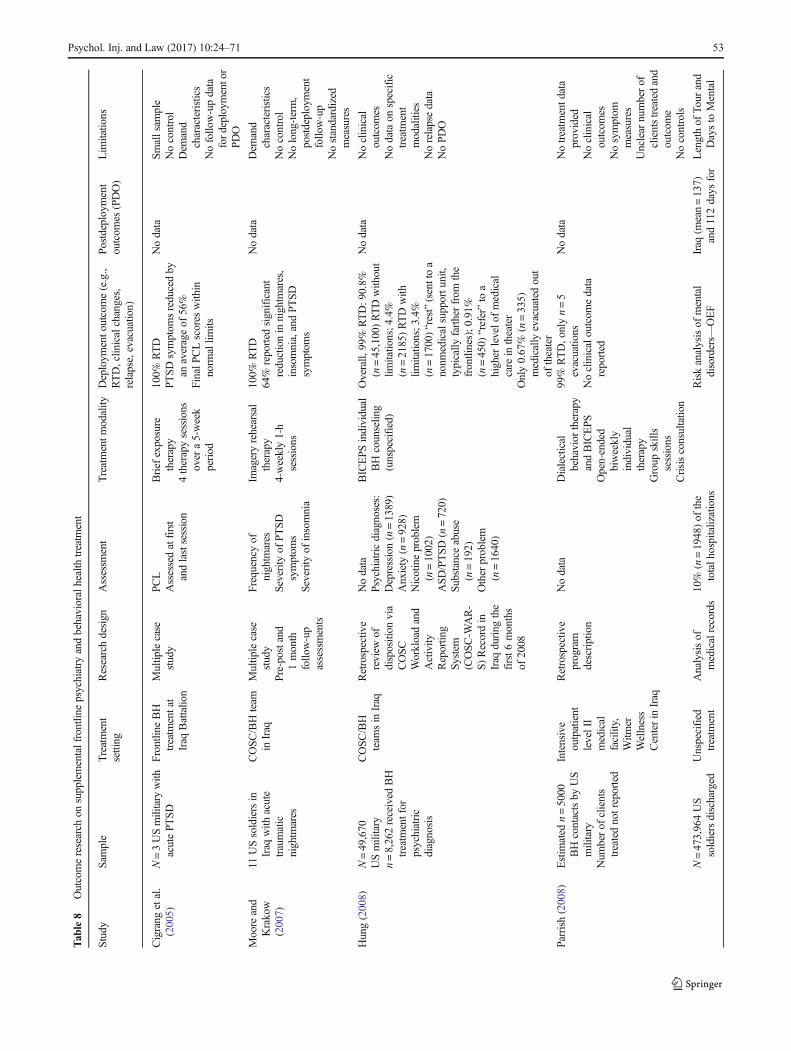
Tab
le8
Outcomeresearch
onsupplementalfrontlin
epsychiatry
andbehavioralhealth
treatm
ent
Study
Sam
ple
Treatment
setting
Researchdesign
Assessm
ent
Treatmentm
odality
Deploym
ento
utcome(e.g.,
RTD,clin
icalchanges,
relapse,evacuatio
n)
Postdeployment
outcom
es(PDO)
Lim
itatio
ns
Cigrang
etal.
(2005)
N=3USmilitary
with
acutePT
SD
Frontline
BH
treatm
entat
Iraq
Battalio
n
Multip
lecase
study
PCL
Assessedatfirst
andlastsession
Brief
exposure
therapy
4therapysessions
over
a5-week
period
100%
RTD
PTSD
symptom
sreducedby
anaverageof
56%
FinalPCLscores
with
innorm
allim
its
Nodata
Smallsam
ple
Nocontrol
Dem
and
characteristics
Nofollo
w-updata
fordeploymentor
PDO
Moore
and
Krakow
(2007)
11USsoldiersin
Iraq
with
acute
traumatic
nightm
ares
COSC/BHteam
inIraq
Multip
lecase
study
Pre-postand
1month
follo
w-up
assessments
Frequencyof
nightm
ares
Severity
ofPT
SDsymptom
sSeverity
ofinsomnia
Imageryrehearsal
therapy
4-weekly1-h
sessions
100%
RTD
64%
reported
significant
reductionin
nightm
ares,
insomnia,andPTSD
symptom
s
Nodata
Dem
and
characteristics
Nocontrol
Nolong-term,
postdeployment
follo
w-up
Nostandardized
measures
Hung(2008)
N=49,670
USmilitary
n=8,262received
BH
treatm
entfor
psychiatric
diagnosis
COSC/BH
team
sin
Iraq
Retrospectiv
ereview
ofdisposition
via
COSC
Workloadand
Activity
Reportin
gSystem
(COSC-W
AR-
S)Recordin
Iraq
during
the
first6
months
of2008
Nodata
Psychiatricdiagnoses:
Depression(n=1389)
Anxiety
(n=928)
Nicotineproblem
(n=1002)
ASD/PTSD
(n=720)
Substanceabuse
(n=192)
Other
problem
(n=1640)
BICEPS
individual
BHcounselin
g(unspecified)
Overall,
99%
RTD:9
0.8%
(n=45,100)RTDwith
out
limitatio
ns;4
.4%
(n=2185)RTDwith
limitatio
ns;3
.4%
(n=1700)“rest”(senttoa
nonm
edicalsupportu
nit,
typically
fartherfrom
the
frontlines);0
.91%
(n=450)
“refer”to
ahigher
levelo
fmedical
care
intheater
Only0.67%
(n=335)
medically
evacuatedout
oftheater
Nodata
Noclinical
outcom
esNodataon
specific
treatm
ent
modalities
Norelapsedata
NoPDO
Parrish
(2008)
Estim
ated
n=5000
BHcontactsby
US
military
Num
berof
clients
treatednotreported
Intensive
outpatient
levelII
medical
facility,
Witm
erWellness
Centerin
Iraq
Retrospectiv
eprogram
description
Nodata
Dialectical
behavior
therapy
andBICEPS
Open-ended
biweekly
individual
therapy
Group
skills
sessions
Crisisconsultatio
n
99%
RTD,onlyn=5
evacuatio
nsNoclinicaloutcom
edata
reported
Nodata
Notreatm
entd
ata
provided
Noclinical
outcom
esNosymptom
measures
Unclear
numberof
clientstreatedand
outcom
eNocontrols
N=473,964US
soldiersdischarged
Unspecified
treatm
ent
Analysisof
medicalrecords
10%
(n=1948)of
the
totalh
ospitalizations
Riskanalysisof
mental
disorders—
OEF
Iraq
(mean=137)
and112days
for
Lengthof
Tour
and
Daysto
Mental
Psychol. Inj. and Law (2017) 10:24–71 53
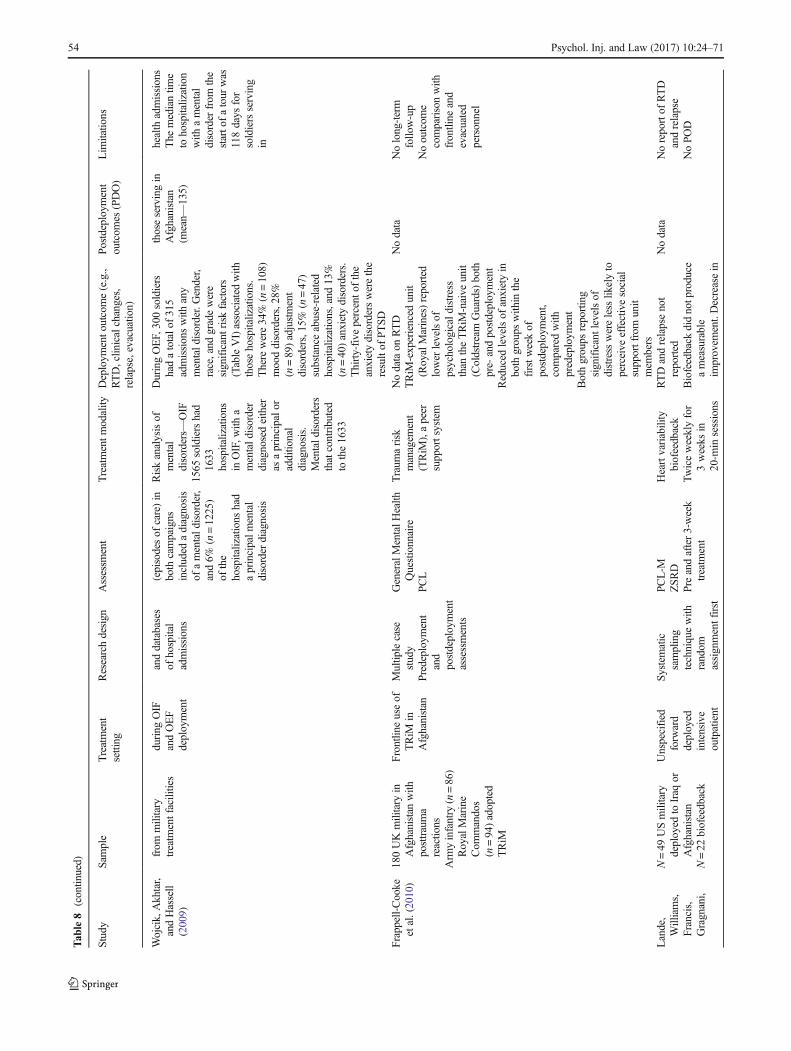
Tab
le8
(contin
ued)
Study
Sam
ple
Treatment
setting
Researchdesign
Assessm
ent
Treatmentm
odality
Deploym
ento
utcome(e.g.,
RTD,clin
icalchanges,
relapse,evacuatio
n)
Postdeployment
outcom
es(PDO)
Lim
itatio
ns
Wojcik,Akhtar,
andHassell
(2009)
from
military
treatm
entfacilities
during
OIF
andOEF
deployment
anddatabases
ofhospital
admissions
(episodesof
care)in
both
campaigns
included
adiagnosis
ofamentald
isorder,
and6%
(n=1225)
ofthe
hospitalizations
had
aprincipalm
ental
disorder
diagnosis
Riskanalysisof
mental
disorders—
OIF
1565
soldiershad
1633
hospitalizations
inOIF,w
itha
mentald
isorder
diagnosedeither
asaprincipalo
radditio
nal
diagnosis.
Mentald
isorders
thatcontributed
tothe1633
DuringOEF,300soldiers
hadatotalo
f315
admissionswith
any
mentald
isorder.Gender,
race,and
gradewere
significantriskfactors
(TableVI)associated
with
thosehospitalizations.
Therewere34%
(n=108)
mooddisorders,28%
(n=89)adjustment
disorders,15%
(n=47)
substanceabuse-related
hospitalizations,and
13%
(n=40)anxietydisorders.
Thirty-five
percento
fthe
anxietydisorderswerethe
resultof
PTSD
thoseservingin
Afghanistan
(mean—
135)
health
admissions
The
mediantim
eto
hospitalization
with
amental
disorder
from
the
starto
fatour
was
118days
for
soldiersserving
in
Frappell-Cooke
etal.(2010)
180UKmilitary
inAfghanistan
with
posttrauma
reactio
nsArm
yinfantry
(n=86)
RoyalMarine
Com
mandos
(n=94)adopted
TRiM
Frontline
useof
TRiM
inAfghanistan
Multip
lecase
study
Predeployment
and
postdeployment
a ssessments
GeneralMentalH
ealth
Questionnaire
PCL
Traum
arisk
managem
ent
(TRiM
),apeer
supportsystem
Nodataon
RTD
TRiM
-experienced
unit
(RoyalMarines)reported
lower
levelsof
psychologicald
istress
than
theTRiM
-naive
unit
(Coldstream
Guards)both
pre-
andpostdeployment
Reduced
levelsof
anxietyin
both
groups
with
inthe
firstw
eekof
postdeployment,
comparedwith
predeploym
ent
Bothgroups
reporting
significantlevelsof
distress
wereless
likelyto
perceive
effectivesocial
supportfrom
unit
mem
bers
Nodata
Nolong-term
follo
w-up
Nooutcom
ecomparisonwith
frontline
and
evacuated
personnel
Lande,
Williams,
Francis,
Gragnani,
N=49
USmilitary
deployed
toIraq
orAfghanistan
N=22
biofeedback
Unspecified
forw
ard
deployed
intensive
outpatient
Systematic
sampling
techniquewith
random
assignmentfirst
PCL-M
ZSRD
Preandafter3-week
treatm
ent
Heartvariability
biofeedback
Twiceweeklyfor
3weeks
in20-m
insessions
RTDandrelapsenot
reported
Biofeedback
didnotproduce
ameasurable
improvem
ent.Decreasein
Nodata
Noreportof
RTD
andrelapse
NoPOD
54 Psychol. Inj. and Law (2017) 10:24–71

Tab
le8
(contin
ued)
Study
Sam
ple
Treatment
setting
Researchdesign
Assessm
ent
Treatmentm
odality
Deploym
ento
utcome(e.g.,
RTD,clin
icalchanges,
relapse,evacuatio
n)
Postdeployment
outcom
es(PDO)
Lim
itatio
ns
andMorin
(2010)
N=17
control
treatm
entasusual
(TAU)
trauma
recovery
program
subjectand
alternating
assignmentto
TAUor
biofeedback
PTSDanddepression
symptom
sfrom
baselin
eto
3weeks
forboth
the
controland
treatm
ent
group
Nosignificantd
ifferencein
treatm
entand
control
McL
ayetal.
(2010)
10USmilitary
personneld
eployed
inIraq
diagnosed
with
acutecombat
PTSD
Com
batS
tress
Clin
ic,C
amp
FallujahIraq
Multip
lecase
study
Inform
edconsent
ledto
assignmentto
either
virtual
reality
therapy
(VRT;n
=6)
ortraditional
exposure
therapy(TET;
n=4)
PCL-M
Patient
Health
Questionnaire-9
BeckAnxiety
Inventory
VRT(m
ean6.5
sessions)
TET(m
ean9
sessions)
Treatmentd
uration
10days–13-
weeks
100%
RTD
Onaverage,patientsin
VR
therapyexperienceda
67%
decrease
inPTSD
symptom
sas
measuredon
thePC
L-M
.In5outo
f6
patientswho
nolonger
metcriteria,themean
change
was
74%,w
hereas
theoneremaining
individualexperienced
only
a32%
drop.
Statistically,there
was
asignificanteffectb
etween
pretreatmentand
posttreatm
ent(p<0.001)
butn
ostatistically
significanteffecto
ftreatm
entg
roup
(VRvs.
traditionalET)
Nodata
Norandom
assignment
Nocontrol
Nofollo
w-updata
Nodeploymento
rpostdeployment
outcom
edata
Schmitz
etal.
(2012)
N=1136
USmilitary
seekingBH
treatm
entinIraq
Datacollected
by19
Navy
BHproviders
servingin
Iraq
Archivald
ata
analysis
Nomeasuresreported
Psychiatricdiagnoses
includeanxiety
disorder
(n=184;
31%)PT
SD(n=152;
11%),
adjustmentd
isorder
(n=360;
27%),
mooddisorders
(n=340;
25%).8%
ASD(n=111)
Medication
Psychotherapyor
counselin
g—unspecified
Behavioral
modification
(practicecoping
skills,exercise,
sleephygiene)
96%
RTD;4
%evacuatio
n(n=54)
65%
on1std
eploym
ent
Medicationmostcom
monly
prescribed
treatm
ent
Totaln
umberBHvisitsfor
each
person
ranged
1–16,
50%
only
1visit
41%
received
treatm
entp
lan
includingmedication
35%
givenaplan
including
psychotherapyor
counselin
g(nospecifics)
34%
received
behavioral
modification
recommendatio
ns
Nodata
Nodataon
treatm
ent
effectivenessin
war
zone
Nofollo
w-updata
afterdeployment
Nooutcom
ecomparisonof
RTDand
evacuees
Psychol. Inj. and Law (2017) 10:24–71 55

Tab
le8
(contin
ued)
Study
Sam
ple
Treatment
setting
Researchdesign
Assessm
ent
Treatmentm
odality
Deploym
ento
utcome(e.g.,
RTD,clin
icalchanges,
relapse,evacuatio
n)
Postdeployment
outcom
es(PDO)
Lim
itatio
ns
(practicecoping
skills,
exercise,sleep
hygiene)
21%
(n=245)
containedno
treatm
entp
lan
Medsonly:PTSD
26%
meds
alone;ASD
9%,anxiety
32%;d
epression(30%
)Stolleretal.
(2012)
N=70
USmilitary
Iraq:n
=35
received
3-week
yoga
treatm
ent;
n=35
control
groupno
treatm
ent
Forw
ard
Operatin
gBaseWarrior,
Kirkuk,Iraq
Randomized
controlledtrial
(RCT)to
evaluatethe
effectof
sensory--
enhanced
hatha
yoga
oncombat
stress,our
prim
arystudy
objective
Pretreatm
entand
1-week
posttreatm
ent
assessment
Adolescent/A
dult
SensoryProfile
STAI
Qualityof
LifeSu
rvey
Sensory-enhanced
hathayoga
classes—
treatm
entg
roup
attended
aminim
umof
2sessions/week
andaminim
umof
9sessions
for
a3-weekperiod.
Eachclasswas
75min
long
and
taught
bythe
principal
investigator
Sensory-enhanced
hatha
yoga
was
effectivein
reducing
stateandtrait
anxiety,despite
norm
alpretestscores
Treatmentp
articipants
show
edsignificantly
greaterim
provem
entthan
controlp
articipantson
16of
18mentalh
ealth
and
quality
-of-lifefactors
Sensoryseekingwas
negativ
elycorrelated
with
allm
easuresexcept
low
registratio
n,which
was
insignificant
Nodata
Dem
and
characteristics
Nodeployment
outcom
esNolong-term,
postdeployment
follo
w-up
Noindependent
raters
Jarrett(2013)
N=3456
USmilitary
completed
training
feedback
survey
98th
Com
bat
StressControl
Detachm
ent
serving
Baghdad
5-questio
nLikert
scaleon
training
satisfaction
survey
Predeploym
entW
arrior
Resiliency
Training
(WRT)combined
with
in-theater
RationalE
motive
Behavioral
Therapy
(REBT)
classes
Participantsreported
high
meanaveragein
satisfactionoverall,
includingbeingbetterable
toidentifyPTGand
PTSD;abilityto
enhance
resilienceandPTGduring
andafterdeployment
Nodata
Nodeploymento
rPD
Ooutcom
esotherthan
posttraining
satisfaction
Externalv
alidity
Nocontrol
Nomeasuresother
than
satisfaction
Vaughan
etal.
(2015)
N=2523
USMarines
deployed
toIraq
orAfghanistan:
n=1631
Marines
from
battalio
nsreceived
OSC
AR/COSC
training
toprom
ote
resilience,
comparedto
n=892Marines
Battalio
nresilience
training
before
deployment
Nonrandom
ized
design
with
matched
control
ofunitnot
receiving
OSC
AR
Assessedpre-
and
postdeployment
afterreturning
homeon
LifeEventsChecklist
Com
batE
xperience
subscaleof
DRRI
PBQ-SR
Socialsupport
Help-seeking
Unitsupport
PCL-C
PHQ-2/8
AUDIT-C
SF-12
OSCARresilience
training
andpeer
support
Nodata
Nosignificant
groupdifference
onperceptio
nof
stress
response,
unitsocial
support;unit
cohesion,
perceptio
nof
leadership
Onlysignificant
benefitfrom
Noinform
ationon
deployment
outcom
essuch
asutilizatio
nof
frontline
psychiatry,R
TD,
evacuatio
nNolong-term
clinicaloutcom
esSamplingbias
56 Psychol. Inj. and Law (2017) 10:24–71

Tab
le8
(contin
ued)
Study
Sam
ple
Treatment
setting
Researchdesign
Assessm
ent
Treatmentm
odality
Deploym
ento
utcome(e.g.,
RTD,clin
icalchanges,
relapse,evacuatio
n)
Postdeployment
outcom
es(PDO)
Lim
itatio
ns
from
battalio
nsthat
didnotreceive
OSC
AR/COSC
resiliencetraining
averageof
92days
HPQ
OSC
ARwas
increased
individual
help-seeking
OSC
ARgroup
reported
worse
clinicaloutcom
esincludinghigher
levelsof
current
stress,P
TSD,
depression,and
somatic
complaints—
although
nolevel
ofsignificance
Nosignificant
difference
betweengroups
onhigh-risk
drinking
oroccupatio
nal
impairment
Baselineand
deployment
differences
whereby
mosto
ftheOSCAR
groupwas
infantry
and
controlg
roup
prim
arily
support
personnel
AUDIT-C
Alcohol
Use
DisordersIdentificationTest-Consumption,CAQCausalA
ttributionQuestionnaire,D
ASDyadicAdjustm
entS
cale,F
ESFamily
EnvironmentS
cale,D
RRID
eploym
entR
iskand
Resiliency
Inventory,HPQHealth
Performance
Questionnaire,IESIm
pactof
EventsScale,L
EQLifeEventsQuestionnaire,M
CEIMilitary
Com
pany
EnvironmentInventory(socialsupport),N
CLE
SNegativeChildhood
LifeEventScale,OQ-45OutcomeQuestionnaire-45,PBQ-SRPeritraumaticBehaviorQuestionnaire-Self-Rating,PCL-M
PTSD
Checklist-Military
Version,P
HQ-2/8PatientHealth
Questionnaire2or
8items,PIS
PTSDInventoryScale,PSE
PerceivedSelf-EfficacyScale,PSQ
PerceivedStressQuestionnaire,U
LSUCLALonelinessScale,SCL-90-R
Symptom
Checklist-90-Revised,
SCQSo
maticCom
plaintsQuestionnaire,SF-12Sh
ortF
ormHealth
Survey,SFPProblemsinSocialF
unctioning
Scale,SSQSo
cialSu
pportQ
uestionnaire,W
CCWaysof
CopingChecklist,ZS
RDSZung
Self-RatingDepressionScale
Psychol. Inj. and Law (2017) 10:24–71 57

Tab
le9
Outcomeresearch
only
ondeployed
personnelevacuated
andtreatedoutsidewar
zones
Study
War
Sam
ple
Treatmentsetting
Treatment
Treatmento
utcomes
Postdeploym
ent/long-term
outcom
esLim
itations
Yealland
(1918)
Reportedin
Linden
etal.(2013)
WWI
N=196UKsoldierstreated
during
WWI1915–1919
Queen
Square
Hospitalin
London
M=71
days
Electricshock(n
=108)
Isolation(n
=12)
Physicaltreatm
ent(massage,
baths,heatetc.):n=59
Exercises
(n=35)
Persuasion
(n=2)
12%
RTDn=23
N=88
“cured”
N=84
“improved”
N=24
noim
provem
ent
Hom
eservice:n=22
Garrisonservice:n=1
Discharge,“no
furtheruse”:n
=32
Already
discharged
from
military
service:
n=21
Nodata
Nolong-term
outcom
edata
beyond
status
inthe
military
Wild
e(1942)
WWII
50UKsoldierstreatedforwar
neuroses
atbase
hospital
Basehospital
Narco-analysis
N=33
RTD
Improvem
entinsomatic,sleep,headinjury,
anxietysymptom
s
Nodata
Nofollow-updata
Nocomparisonof
frontline
RTD
Smallsam
ple
Brooke(1946)
WWII
500UKsoldiersevacuatedfor
battleexhaustion
53%
had4–6yearsmilitary
service
Specialty
inpatient
neuroses
center
inEngland
Nodataon
treatm
enttype
2weeks
to3months.Median
53days
Cum
ulativeeffectsof
stress
45%
(27/60)relapsed
from
CSC
18%
(11/60)previously
treatedin
neuroses
centers
5 .6%
military
discharge
17.6%
RTD
76.8%
reassignment
Nodata
Dem
andcharacteristics
Nocontrol
Nolong-term,
postdeployment
follo
w-up
Nostandardized
measures
Levav
etal.(1979)
1973
Yom
Kippur
War
N=35
Israelisoldierswith
CSR
evacuatedto
rear
echelon
hospital
Authorsreportcontrolg
roup
ofn=55
soldiersevacuatedand
treatedforphysicalinjuries,
notC
SR
Note.Num
bersreported
are
estim
ates
basedon
data
presentedby
theauthors
Rearecheloninpatient
hospitalo
utside
war
zone
Military
psychiatricgrading
(e.g.,diagnosis,disability
level)
Sociopsych.grading
(e.g.,level
ofeducation,intelligence,
personality
style)
Assessm
entato
nsetof
CSR
,afterhospitaltreatment
during
war,and
18months
afterwar
ended
RTDandrelapserates—
nodata
Lengthof
treatm
entcorrelatednegativ
elywith
lowerpsychiatricgrading
Upto
1weekof
treatm
ent:
35%
oftheCSRgrouphadlower
psychiatric
grading(pooroutcom
e)65%
oftheCSRgrouphad“nochange”in
grading
Nodatareported
onim
proved
grading
After“m
ore”
than
1week(unspecified
length):
70%
hadlower
grading
30%
hadno
change
Atw
ar’send,17%
oftheCSRgroup
categorizedas
temporary
orperm
anently
unfitfor
military
service.Mostlikely
received
military
discharge
Byendof
thewar:5
5%of
the
CSR
grouphadlower
psychiatricgradingthan
atthe
onseto
fhostilities
45%
“nochange”
At1
8month
follow-up:
60%
oftheCSRgrouphadlower
psychiatricgrading
40%
“nochange”
Nodataon
controlg
roup
Nocomparisonof
soldiers
with
CSR
who
werenot
evacuatedandtreatedat
rearechelon
Assessm
entand
outcom
esreported
areunclear
Nospecificreporton
RTDor
long-term
adjustment
Russell(2006)
Iraq
4USmilitary
with
combatA
SDNavyfieldhospitalin
communication
zone
during
Iraq
invasion
Eye
movem
entd
esensitization
andreprocessing
(EMDR)
NoneRTD,allstabilizedevacuatedtostateside
hospital
All4reported
significantp
re-postreductionin
PTSD
anddepression
symptom
s
Nodata
Nofollow-updata
Nocomparisonof
frontline
RTD
Smallsam
ple
Joneset
al.(2007)
WWI
N=3580
UKsoldiersadmitted
toinpatient
NYDNCentrein
France
M=25
days
inpatient
war
zone
4Stationary
Hospital
NYDNCentre
Nodataon
type
oftreatm
ent
M=11.2
monthsin
war
zone
before
admission
40.3%
brokedownafter
6-month
CE
9%2-yearCEoldsergeants
35%
reassigned
inconvalescent
17%
RTDn=606
20%
evacuatedto
base
Ofthe606RTD,15(2.5%)werereadmitted
to4Stationary
Hospitalshortlyafterd
ischarge
n=93
(2.6%)of
thetotalsam
pleof
3580
soldiershadtwohospitaladm
issions
Nodata
Lackrandom
assignment
Onlyoutcom
emeasure
isRTD
Nocomparisonof
RTDvs.
evacuatio
ngroup
58 Psychol. Inj. and Law (2017) 10:24–71

during deployment are RTD, with less than 5% evacuated. Inshort, the predominant emphasis of clinically oriented studiescoming out of war zones serves to confirm the benefit to themilitary mission by conserving the fighting force, but failsentirely to address the consequential long-term health impli-cations for deployed personnel and their families.
5. Outcome Research on Personnel Evacuated from WarZones
Table 9 reviews outcomes of deployed personnel evacuatedand treated outside of war zones (e.g., Levav, Greenfeld, &Baruch, 1979), but none of the material includes comparisonwith personnel RTD via frontline psychiatry. For instance,Yealland (1918) reported that 172 of 196 (88%) shell-shocked soldiers were favorably treated with electrical shocktherapy after being evacuated to a London hospital, including12% RTD to frontline units and 142, or 72%, of soldiersretained on military service (Linden, Jones, & Lees, 2013).During WWII, Wilde (1942) reported the clinical outcomesof 50US soldiers evacuated and admitted to a base hospital forbattle exhaustion. After receiving narco-analysis, 33 (66%) ofsoldiers were RTD (Wilde, 1942). Brooke (1946) examinedthe records of 500 UK soldiers evacuated to London-basedspecialized hospitals for battle exhaustion during WWII andreported that 18% were RTD and 77% remained on activeduty (33% discharged from the military). Levav et al. (1979)reviewed medical records for 35 Israeli soldiers during the1973 Yom Kippur War evacuated to inpatient hospitals out-side the war zone for CSR, matched to 55 veterans evacuatedfor medical reasons. An 18-month follow-up record reviewwas also conducted. The CSR group had significantly poorerhealth ratings than their medical counterparts, as well as
longer duration of stay correlating with poorer outcomes(Levav et al., 1979). Specifically, 35% of veterans with CSRhad lower psychiatric grading at the time of medical dischargeand 65% were rated as unchanged (Levav et al., 1979). Thenature and type of psychiatric treatment was not specified andoutcome measures consisted only of physician grading. Atwar’s end, 17% of the CSR group were classified as unfitfor military service and likely discharged, suggesting that83% were determined to be fit for duty (Levav et al., 1979).
Table 4 contains contemporary military studies on psy-chiatric evacuations, and treatment admissions from theUK (e.g., Turner et al., 2005) and the USA (e.g., Cohenet al., 2010) all report RTD as outcome. Historically,since WWI, poor RTD rates following evacuations andhospital admission (see Tables 2, 3, and 4) have routine-ly been interpreted by the military as evidence of indi-v i d u a l h a rm ( s e e Ru s s e l l & F i g l e y, 2 0 1 6 ) .Methodologically, all studies reviewed on evacuees haveserious methodological limitations, such as the lack ofstandardized symptom measures, inadequate or lack oftreatment details, the absence of control groups, and thelack of long-term outcomes (see Table 9). In sum, theliterature on long-term outcomes of psychiatric evacueesis sparse and methodologically flawed, thus prohibitingany meaningful conclusions. That said, the available out-come data on psychiatric evacuees is mixed with somefindings supportive of the military claims (e.g., Levavet al., 1979), with others less so (e.g., Brooke, 1946).Unfortunately, what isn’t known in the twenty-first cen-tury is how might contemporary psychiatric evacueesfare if they receive high-quality evidence-based therapies(e.g., Department of Veterans Affairs & Department ofDefense, 2010) via specialized centers.
Table 10 Protective factors for US Army personnel deployed to Iraq or Afghanistan (adapted from J-MHAT, 2013)
Survey question 2005 2007 2009 2010 2012
Unit cohesion
Unit cohesion rated as medium, high, or very high 52.6 61.0 64.1 71.5 74.1
Morale
Individual morale rated as medium, high, or very high 68.4 52.5 57.5 49.9 47.0
Unit morale rated as medium, high, or very high 60.5 48.7 44.3 45.3 34.5
Leadership
Officer leadership rated as medium, high, or very high 41.9 48.8 50.2 54.5 43.9
Enlisted leadership rated as medium, high, or very high 41.9 48.4 46.1 51.5 47.1
Resilience
The training in managing the stress of deployment and/or combat was adequate No data No data No data 56.4 49.9
Posttraumatic growth
I feel pride in my accomplishments during this deployment 68.0 52.3 57.0 57.6 52.1
Deployment made me more self-confident 63.3 50.1 41.7 39.7 33.3
I deal with stress better because of this deployment 31.4 22.8 25.7 24.3 25.8
Psychol. Inj. and Law (2017) 10:24–71 59

Tab
le11
Meta-analyses
andsystem
aticreview
ofrisk
factorsforcombat-relatedPTSD
Study
Design
Sample
Major
findings
Lim
itatio
ns
Kulka
etal.
(1990)
NationalV
ietnam
VeteransReadjustm
ent
Study—
natio
nalp
robabilitysampling
andinterviewresearch:p
relim
inary
valid
ation,clinicalinterviews,
andfamily
interviews
N=3016
totalinterview
s:n=344Vietnam
theatervets;
n=474spouse
interviews;n=96
Vietnam
eravets
Exposureto
war
stress
significantly
relatedto
combatP
TSD
independent
ofprecom
batp
redisposingfactors
PTSDsignificantly
higher
inVietnam
theatervs.era
vets
Prem
ilitary
child
hood
adversity
;depression,substance
abusehigher
inVietnam
theatervets
Dosageeffectof
levelo
fcombatexposureand
severity
ofpostwar
readjustmentp
roblem
sReadjustm
entp
roblem
ssignificantly
relatedto
war
stress
exposure,P
TSD
,substance
abuse,
andserviceconnecteddisability
Nonrandom
ization
Retrospectiv
eanalysis
Verificationof
reported
combat
exposure
oftheatervets
Brewin
etal.
(2000)
Meta-analysisof
risk
factors
forPT
SD
77studieson
military
(n=28)and
nonm
ilitary
populatio
nsTraum
aseverity
was
strongestriskfactor
during
andaftertraumafollo
wed
by:
Lackof
socialsupport
Posttraumalifestress
Weakeffectsforpretraum
afactors
Heterogeneity
ofstudieswith
regard
tosampling,design,
measurement,statistical
analysis,and
resulting
effects
Ozeretal.
(2003)
Meta-analysisof
studieson
predictors
ofadultP
TSD
68studiesmetinclusioncriteria,
17involvingmilitary
veterans:7
predictors:p
rior
trauma,priorpsychological
adjustment,
family
mentalh
ealth
history,
perceivedlifethreat,posttraumasocial
support,peritraumaticem
otional
response,and
peritraumatic
dissociatio
n
Allpredictorsyieldedsignificanteffectsizes
Peritraumaticdissociatio
nstrongestp
redictor
Socialsupporth
adsm
alltomedium
effect
Weakestpredictorswerefamily
history,prior
trauma,andprioradjustment
Overrelianceon
retrospective
self-report
Self-reportand
recallbias
Lackof
prospectivestudies
Variabilityin
defining
and
measuring
variables
Levelof
exposure
(com
bat)
was
notanalyzed
Zohar
etal.
(2009)
Semiprospectiv
estudyof
demographic,
prem
ilitary,precombatfactors,and
military
risk
factorsassessed
2years
priorto
military
serviceandafter
deployment
2362
Israeliw
arveterans
diagnosedwith
combatP
TSD
,matched
with
2323
veterans
notd
iagnosed
with
PTSD
Socialfunctio
ning,m
otivation,training,
pre-military/pre-traum
arisk
factorsall
foundto
beinsignificantinpredictin
gPT
SD
Ceilin
geffectfrom
stigma,Ex.
“Hidden-PT
SD”in
control
groupwhere16%
eventually
diagnosedwith
PTSD
;Com
batexposuretype,
intensity,and
duratio
nnot
assessed
Pietrzaketal.
(2009)
Retrospectiv
e,nonrandomized
mailin
gof
surveysto
1000
veterans
28.5%
response
(N=272)
from
US
OEF/OIF
veterans
1–4yearsafter
military
discharge
Resilience
scores
correlated
negativ
elytoPTSD,
depression,and
psychosocialproblems
CEcorrelated
negativ
elywith
postdeployment
socialsupportand
positiv
elyforPTSD
,depression,socialp
roblem
sResilience-m
ediatedunitsupportand
PTSD
and
depression
Unitsupportpredictedincrease
postdeployment
socialsupport
Samplingbias
Reportand
recallbias
from
retrospectiveself-report
Lim
itedgeneralizability
dueto
lowresponse
rate
Lim
itedassessmento
fspectrum
ofwarstressinjury
(e.g.,substanceabuse)
10.8%
diagnosedwith
newonsetP
TSD
60 Psychol. Inj. and Law (2017) 10:24–71

Tab
le11
(contin
ued)
Study
Design
Sample
Major
findings
Lim
itatio
ns
Phillips
etal.
(2010)
Prospectivestudyof
demographic,pretrauma
risk
factors,anddeploymentriskfactors
before
andafterdeployment
706USMarinerecruitsevaluated
before
andafterdeploymentand
combatstressexposure
Com
batexposuretype
(e.g.,threatof
death,
exposure
toviolence)was
thestrongest
predictorof
PTSD
than
otherdeployment,
postdeployment,andpretraum
arisk
factors
Levelof
postdeploymentsocialsupport
reducesrisk
ofPT
SD
Samplingbias
ofself-selected
volunteers
Use
ofnonanonymoussurveys
Low
response
rate(13%
)Ceilin
geffectsfrom
stigmaand
fearsof
career
reprisal
PTSDsymptom
snotassessed
priorto
deployment
Elbogen
etal.
(2012)
Cross-sectio
nal,random
samplingfor
natio
nalsurveyby
theDepartm
ento
fVeterans’Affairs
N=1388
(56%
)of
3000
OEF/OIF
USveterans
completed
mailed
surveys
20%
metPTSD
criteriaand27%
alcohol
abuse;33%
reportviolentactin
community
;11%
severe
violence
Increase
risk
ofviolence
linkedto
CE,
youngerage,PTSD
,alcohol,criminalarrest
Decreased
risk
ofviolence
linkedto
olderage,
levelo
fsocialsupportand
resilience
Generalizability
limitedby
design
Lacking
longitu
dinal
assessmento
fprotectiv
efactors
Targetof
violence
notassessed
Noreportinglevelo
fviolence
experiencedduring
deployment
Ram
chandetal.
(2015)
Reviewof
literature2009
to2014
onrisk
factorsfor
combat-relatedPTSDandothermentalh
ealth
(MH)
diagnosesin
military
personneld
eployedto
Iraq
and
Afghanistan.A
lsoanalyzed
treatm
entseeking
vs.
nontreatmentseeking
48USstudieson
military
personnel;56
studieson
USveterans
10non-USstudieson
military
personnel;4studieson
non-USveterans
0–48%
PTSD
ratesin
nontreatmentseeking
samples;2
–68%
intreatm
entseeking
4–45%
depression
ratesin
deployed
samples
4–60%
alcoholabuse
indeployed
samples
Com
batexposurestrongestp
redictor
ofallM
Hproblems
Multip
ledeploymentsincrease
PTSD
Low
ersocialsupportd
uringandafter
deploymentincreaserisk
inMHproblems
<50%
who
reported
they
need
treatm
ent,receive
itCom
bat-PT
SDsignificantly
relatedto
poor
physicalhealth,suicidalideation,dyingby
suicide,depression,substance
abuse,
aggression,and
crim
inaloutcom
es
Manystudiesdo
notcontrol
forcombatexposure
Significantv
ariatio
nin
methodologicalrigor
and
measurement
Inadequatelongitu
dinald
ata
Xue
etal.(2015)
Meta-analysisof
combatP
TSD
risk
factors
32studiesaccepted
outo
f2657
screened;2
7risk
factorsevaluated
Levelof
combatexposuregreatestrisk
factor
forcombatP
TSD
Psychiatrichistory,lifestress,pretraumahistory
notsignificant
predictors
Inconsistent,but
strong
findingof
postdeploymentsocialsupportandlower
PTSDrisk
Heterogeneity
ofstudieswith
regard
tosampling,design,
measurement,statistical
analysis,and
resulting
effects
Inclusionof
observational
studiesonly
relyingon
self-report
Psychol. Inj. and Law (2017) 10:24–71 61

Summary of Partial Evidence of FrontlinePsychiatry’s Health Benefits
Of the partial studies reviewed on frontline psychiatry’s healthbenefits, we found mixed empirical support for the military’sclaims of mutual benefits. The most positive line of inquiriessupportive of frontline psychiatry involves military studiesfocusing exclusively on reporting deployment-related out-comes (i.e., symptom reduction; RTD) of veterans receivingeither frontline psychiatry alone (Table 7) or in conjunctionwith BH treatment (Table 8). Overwhelmingly, these researchlines emphasize RTD as a primary outcome measure and findhigh RTD rates (96–100%) and low evacuation rates (1–8%).Similarly, it is also routine for military researchers to focuspredominantly on immediate short-term clinical (i.e., symp-tom reduction) and dispositional (e.g., RTD) gains at the al-most universal exclusion of long-term outcomes of war zonefrontline psychiatry (Tables 2, 3, and 4; Tables 5, 6, 7, 8, and9). This trend is consistent with the only other review of front-line psychiatry (Jones &Wessely, 2003). Consequently, Jonesand Wessely (2003) openly questioned the objectivity andveracity of military research on its frontline programs.Moreover, several classified investigations by UK and USauthorities during WWII cited major discrepancies betweenthe reported effectiveness of frontline psychiatry and undis-closed high relapse rates (e.g., Jones & Wessely, 2003).
To the lay public, reports of 95–100% RTD imply that de-ployed personnel have access to highly effective mentalhealthcare. However, many of the results from our review sug-gest the contrary. For example, the only nonmilitary investigationinto frontline psychiatry (Vaughan et al., 2015) reported poorerpostdeployment outcomes for unitmembers after receiving front-line psychiatry services (OSCAR) compared to those who didnot participate. Although methodological limitations do not per-mit causal inferences, that independent RAND researchers foundadverse outcomes from frontline psychiatry is worrisome.Moreover, extensive research on CSR and frontline psychiatryby the world’s leading experts, the IDF (see Table 6), indicatesthat CSR alone represents a significant risk factor for a host ofnegative individual and family outcomes regardless if veteransreceive frontline psychiatry or not, and repeated CSR results inpoorer outcomes (see Table 6). With regard to family outcomes,the only research we could find that examines potential healthbenefits for family members from frontline psychiatry was con-ducted by the IDF (e.g., Solomon, Waysman, Levy, et al., 1992;see Table 6). Those studies reveal that CSR in deployed familymembers is significantly related to developing PTSD and otherproblematic health conditions (e.g., drinking) that, in turn, issignificantly associatedwithmultiple adverse outcomes for spou-sal health, including secondary traumatization (e.g., Solomonet al., 1992), as well as impaired couple and family functioningirrespective if deployed members were treated via frontline psy-chiatry or not (e.g., Solomon, Waysman, Levy, et al., 1992).T
able12
Percentagree
orstrongly
agreeon
war
zone
stigmaandbarriersin
Afghanistan
(adapted
from
J-MHAT,
2013)
Survey
questio
n2003
Arm
y(M
HAT-I).
Screenedpositiv
efora
MHdisorder—Iraq
(%)
2003
Arm
y(M
HAT-I).
Not
screened
positiv
eforMHdisorder—Iraq
(%)
2013
Arm
y(J-M
HAT,
2013).Screened
positiv
eforaMH
disorder—Afghanistan
(%)
2013
Arm
y(J-M
HAT,
2013).Not
screened
positiv
eforMH
disorder—Afghanistan
(%)
2004
Arm
yPost-Deploym
ent
Survey(H
ogeetal.,2006).Married
Soldiersscreened
positiv
efora
MH
disorder—USA
Soldiers(%
)Spouses
(%)
Iwould
beseen
asweak
5929
4723
7722
Itwould
harm
mycareer
(orspouses’career)
Not
asked
Not
asked
4017
5621
Myunitleadership
might
treatm
edifferently
5829
3922
63(H
ogeetal.,
2004)
N/A
Myleaderswould
blam
emefortheproblem
4614
3614
51(H
ogeetal.,
2004)
N/A
Myleadersdiscourage
theuseof
mentalh
ealth
services
Not
asked
Not
asked
204
8(H
ogeetal.,2004)
N/A
There
would
bedifficulty
getting
timeoffworkfor
treatm
ent
4616
4617
6143
62 Psychol. Inj. and Law (2017) 10:24–71

Lastly, the partial line of research on evacuee outcomes (Table 9)indicates that military claims of significant harm caused by evac-uation and psychiatric treatment are empirically supported pri-marily whenRTD is the desired outcome (see Tables 2, 3, and 4).Otherwise, long-term outcome data on psychiatric evacuees arenearly nonexistent. When examined, the overall empirical sup-port for frontline psychiatry along the partial lines of inquiryreviewed is tenuous.
We next examine the indirect evidence that underlies themilitary’s health benefit claims. Specifically, we briefly re-view the research on protective social factors, stigma, andprevention of war stress injury, like PTSD, that reportedlyjustifies sustaining the frontline psychiatric doctrine.
Indirect Evidence of Frontline Psychiatryand Protective Factors
Since its WWI inception, frontline psychiatry’s emphasis onpreventing psychiatric evacuations has been heralded as thecenterpiece for military’s humane approach in managing warstress casualties by avoiding harm caused by social disrup-tions that undermine resilience and mental health (e.g.,Martin & Cline, 1996). Yet, no study has ever examined thedifferential impact of protective factors, such as social sup-port, unit cohesion, leadership, and morale, on military per-sonnel RTD via frontline psychiatry compared to those evac-uated for treatment outside war zones (see Tables 2, 3, 4, 5,and 6). As reviewed earlier (Russell & Figley, 2016), the USmilitary’s frontline psychiatry/COSC programs involve train-ing leaders and unit members on ways to prevent war stresscasualties (e.g., Jones et al., 2012). Table 10 provides a de-scriptive snapshot of the kinds of protective and resilient fac-tors surveyed in the war zones of Afghanistan and Iraq by theUS Army’s MHAT survey teams. Although this constitutesvaluable information for senior leaders in monitoring troopwell-being and the capacity to fight and win wars, it doesnot represent applicable data for justification of RTD of psy-chiatric casualties to promote the health and well-being ofindividual service members.
Research on Unit Cohesion, Morale, and Leadershipin Reducing War Stress Casualties
The US military regularly cites research from WWII demon-strating the significant impact of unit cohesion, morale, andleadership in reducing incidence of CSR/COSR casualties andPTSD, as well as enhancing military performance (e.g., Jones,1995a; Solomon et al., 2005). A retrospective IDF study afterthe 1973 Yom Kippur War reported that veterans diagnosedwith CSR at the frontlines had lower morale than veteranswithout CSR (Steiner & Neuman, 1978), and meta-analyses
of military research indicate that cohesion is positively corre-lated with job satisfaction, retention, sense of well-being, andless disciplinary problems (Oliver, Harman, Hoover, Hayes, &Pandhi, 1999), as well as lower levels of psychological dis-tress (Ahronson & Cameron, 2007). The importance of unitcohesion and social support is illustrated by Stouffer et al.(1949), who described that BThe men in my squad were myspecial friends^ (p. 99).
Protective Factors of Cohesion, Leadership, and Moralein Elite Forces
The military regularly avows that the Special Forces havehistorically produced the highest levels of cohesion, morale,and leadership, coinciding with the lowest rates of psychiatriccasualties among military groups (e.g., Jones, 1995b). Suchclaims add credence to the health-promoting value frompreventing psychiatric evacuations. In addition, IDF re-searchers reported similarly low PTSD rates in decorated vet-erans (Dekel, Solomon, Ginzburg, & Neria, 2003), implyingthat membership to elite status may be a protective variable.However, caution is warranted in overinterpreting the protec-tive benefits of cohesion and the like, especially consideringheightened stigma active-duty elite personnel experience inself-disclosing stress symptoms (e.g., Hing, Cabrera,Barstow, & Forsten, 2012). For instance, a recent anonymoussurvey of US Army Special Operations Forces personnel re-veals PTSD rates of 16–20%, nearly doubling the prevalencerate reported by regular Army soldiers and contradicting as-sertions of Bhyper-resilience^ (Hing et al., 2012). Similarly,the US Army’s summary of the 1982 Lebanon War,BDespite high morale and a good deal of attention given bycommand to morale and the factors maintaining it, the IDFstill suffered relatively high rates of psychiatric casualties dur-ing the war in Lebanon^ (Belenky et al., 1983, p. 22).
Everything said, there is no dispute that factors such ascohesion, morale, and leadership can be beneficial insupporting the mental health of deployed service members.However, this does not automatically translate to better long-term health outcomes for personnel RTD after experiencingwar stress injury and/or diagnosed with psychological disor-der in war zones. Researchers often make the distinction be-tween delayed presentation and delayed onset with regard toPTSD, with the former often involving the toleration versusabsence of symptoms (e.g., Solomon, Mikulincer, &Waysman, 1991). For instance, IDF researchers found theso-called delayed onset of PTSD in 16.5% of combat veteransafter leaving military service who were never diagnosed withCSR on active duty (Horesh et al., 2011). Another IDF studyused the term hidden-PTSD to account for 16% of combatveterans who refused to self-disclose symptoms largely outof fear of stigma and career reprisal (e.g., Zohar et al.,2009). Several authors attribute significant escalation in
Psychol. Inj. and Law (2017) 10:24–71 63

veterans diagnosed with mental health problems after militaryservice to phenomena such as diminished levels of protectivesocial support and decreased fear of career reprisal (e.g.,Camp, 2014; Kulka et al., 1990). Therefore, it is reasonableto assume that, at least in some if not many cases, the imme-diate protective benefit from unit support, cohesion, and lead-ership even in the military’s elite forces may erode afterreturning deployed personnel relocate to other units, retire,or separate from the military.
Research on Risk and Protective Factorsfor Combat-Related PTSD
Table 11 contains etiologic research on risk and protectivevariables for combat-related PTSD, revealing that the levelof perceived social support is reliably the best predictor forresilience and the second strongest risk factor for combat-related PTSD after cumulative exposure to war stress.Importantly, the PTSD protection/risk factor of perceived lev-el of social support typically measures postdeployment socialsupport from spouses, family, friends, and community, as op-posed to social support during deployment (e.g., Brewin,Andrews, & Valentine, 2000; Kulka et al., 1990; Ozer, Best,Lipsey, & Weiss, 2003). Unfortunately, no studies have com-pared the purported social protective variables betweengroups of veterans RTD via frontline psychiatry versus thoseevacuated.
Contemporary Research on Unit Cohesionand Social Support
Research on the protective benefits from unit cohesionand deployment-related social support appears to bemixed. Most empirical findings of predictors for combatPTSD, as reflected in Table 11, report that the level ofsocial support in the postdeployment environment (e.g.,family, friends, and community) constitutes the most reli-able indicator of resilience (e.g., Brewin et al., 2000; Ozeret al., 2003; Phillips, LeardMann, Gumbs, & Smith,2010). However, recent military studies from the UK(e.g., Du Preez, Sundin, Wessely, & Fear, 2012) and theUSA (e.g., Armistead-Jehle, Johnston, Wade, & Ecklund,2011; Pietrzak et al., 2009) indicate that high levels ofunit cohesion are associated with lower probability ofpostdeployment mental health diagnoses, includingPTSD, with the exception of one US finding that onlythe deployment variable of high morale was a significantbuffer against combat PTSD, not unit cohesion or patriot-ism (Whitesell & Owens, 2012). Additionally, Han et al.(2014) concluded that postdeployment social support wasa stronger buffer against combat PTSD than unit social
support during deployment. Others observed how lowlevels of perceived social support both during and afterdeployment are significantly related to mental healthproblems (e.g., Ramchand, Rudavsky, Grant, Tanielian,& Jayconx, 2015). The relative protective benefit fromunit cohesion, morale, leadership, social support, etc. isnot in question. The critical matter at hand is the fact thatnone of the studies in Table 11 compare outcomes ofdeployed personnel RTD via frontline psychiatry to thoseevacuated out of war zones. We are left with overgener-alization and inferences that service members RTD farebetter in the long term than evacuees because of the pro-tective influence of unit cohesion, morale, and leadership.
Logical Inconsistencies of Beneficial Claims of RTDand Social Protective Factors
Several logical contradictions exist regarding the military’s asser-tion about the iatrogenic effects of disrupted social ties frompsychiatric evacuations, such as (a) the fact that unit membership(social ties) is constantly disrupted via the mobility of militarylifestyle, requiring frequent changes in duty stations every 3 to4 years, thus undercutting the resilience narrative; (b) extensivereliance on individual augmentees (IA) during the current wars inAfghanistan and Iraq, whereby individuals routinely deploy fromdifferent organizations and return home separately from theircombat buddies without significant differences in mental healthoutcomes as reported by the MoD (e.g., Sundin et al., 2012) andDoD (e.g., Granado et al. (2012); (c) evacuated personnel arerestoring social ties with family, friends, undeployed coworkers,and support staff (e.g., mental health professionals, chaplain,etc.), of which research has demonstrated is the single best pre-dictor of resilience (e.g., Brewin et al., 2000; Phillips et al., 2010);and (d) the overwhelming majority (90 to 95%) of military per-sonnel evacuated out of war zones are due to medical reasons(e.g., Cohen et al., 2010), and they must similarly endure disrup-tions in hypothesized war zone protective factors, yet there is nocomparison in the intensity by which the military restricts med-ical evacuations.
Evidence That RTD Prevents Harmful Effectsof Stigma, Shame, and Guilt from Evacuation
BEvacuees had to deal with the stigma and shame of evacua-tion out of the theater. However, if psychological casualtieswere treated at forward locations with brief supportive therapyand the expectation of return to duty, between 60% and 80%could continue as soldiers^ (Ritchie, 2007, p. 12). This is along-standing and central argument used by the military sinceWWI to justify its frontline psychiatry policies of RTD andpreventing evacuation syndromes (e.g., DOA, 2006).
64 Psychol. Inj. and Law (2017) 10:24–71

However, the claim appears to be factually baseless. Evidencesupportive of the military’s assertion is entirely dependentupon broad generalizations from research related to work per-formance and PTSD protective factors, like unit cohesion,morale, leadership, and social support reviewed earlier. Noresearch has ever compared the differential experience ofmental health stigma, shame, and guilt of deployed personnelRTD and return home with their units versus those evacuatedand treated at psychiatric facilities outside war zones. Asdepicted in Table 4, the clear majority (e.g., 90 to 95%) ofpersonnel evacuated out of war zones are for medical and notpsychiatric reasons. Many of those service members may like-wise experience stigma, shame, and guilt over being wound-ed, injured, or sick and leaving their combat buddies behind(e.g., Stouffer et al., 1949). Therefore, stigma, shame, andguilt are not unique to psychiatric evacuees, yet evacuationpolicies are nowhere as restrictive for nonpsychiatricevacuees, thus reflecting a certain bias. Moreover, attitudestoward combat exposure and stress injury may differ per theperspective of warfighters and nonwar fighters. For example,during WWII, Stouffer et al. (1949) conducted a series ofsocial psychological studies on veterans, including the onlystudy we could find that speaks about the issue of possibleshame, guilt, and stigma in psychiatric evacuees. Per Stoufferet al. (1949), BPresumptive evidence of this lies in the indica-tions of guilt feelings among men who were out of combatwhile their comrades were still fighting^ (p. 136). There is awide array of circumstances responsible for separating vet-erans from their frontline units, and the experience of shameor guilt is not at all unique to evacuated psychiatric casualties.If, however, psychiatric evacuation invokes some exceptionaltype or intensity of shame, guilt, and stigma above and beyondthat experienced by personnel evacuated for other reasons, thephenomena should be researched.
With regard to stigma associated with psychiatricbreakdown and possible evacuation, again we refer toWWII research. In an attitude survey, 1766 infantry sol-diers in Italy after 5 months of combat exposure wereasked BWhat do you think should be done to a man whocracks up mentally at the front?^ (Stouffer et al., 1949). Inresponse, 86% of combat veterans answered, Bhe shouldbe given medical treatment,^ whereas only 3% endorsedeither Bhe should be court martialed^ or Bhe should bemade to go right back to combat^ (Stouffer et al., 1949).Similarly, Momen, Strychacz, and Virre (2012) recentlysurveyed 553 US Marines about CSR and found that70.5% believe CSRs are treatable, 68.2% normal reac-tions, and 57.4% thought they can be individually man-aged; however, 46.7% personally feared career repercus-sion if diagnosed with CSR. Whether such seemingly pro-gressive nonstigmatizing attitudes are conveyed to, or per-ceived by their peers as such in those who might be psy-chiatrically evacuated is another matter, but it does raise
questions over the legitimacy of military concerns overharmful stigma caused by violating its RTD policy.
Contemporary Research on Prevalence of Stigmaand Barriers to Care
Table 12 illustrates the prevalence of mental health stigmaand barriers to care in the war zones of Iraq andAfghanistan as well in the USA. The general trend is fora slight lessening of stigma and barriers to seeking care inthe war zones (e.g., MHAT, 2003; J-MHAT, 2013) andincreased stigma back home (e.g., Hoge, Castro, &Eaton, 2006). The US Army credits frontline psychiatry,including embedded mental health specialists in opera-tional units (e.g., Army division, Navy aircraft carriers,Marine OSCAR), as being a main contributor in reducingwar zone stigma (e.g., J-MHAT, 2013). The evidencewould seem to partially support that position. However,per the Department of the Army (2006), modern-dayCOSC programs are active throughout the entire deploy-ment cycle and the military has permanently embeddedmental health specialists in air wings, army divisions,and air craft carriers for decades (e.g., Russell & Figley,2016). Reducing stigma and barriers to care is a designat-ed function of today’s COSC program (e.g., Departmentof Navy & U.S. Marine Corps, 2010). Therefore, otherfactors than the presence of forward deployed mentalhealth services may be responsible for incremental reduc-tions in war zone stigma. Regardless, caution is warrantedin overinterpreting the military’s frontline psychiatry suc-cess in reducing war zone stigma. For example, in 2013,47% of deployed personnel who screened positive for amental health disorder, such as PTSD, depression, or anx-iety, reported reluctance to seek mental health treatmentfor fear of being weak (J-MHAT, 2013). Similarly, 40%feared career reprisal, 39% believed their unit leadershipwould blame them for their mental health condition, 46%reported difficulty getting time off to see a specialist and,perhaps most alarmingly, 20% reported unit leadershipactively discouraged seeking mental healthcare (e.g., J-MHAT, 2013).
Per Table 12, oppressive levels of stigma both within andoutside of war zones appear to negate the military’s claim thatfrontline psychiatry avoids harmful stigma by preventing psy-chia t r ic evacuat ion. Moreover, the GovernmentAccountability Office (2016) recently reported that significantstigma and organizational barriers to seeking mentalhealthcare widely persists in the DoD, despite repeated rec-ommendations from six independent investigations. In otherwords, whenever military personnel develop a war stress in-jury or mental health problem, they face potential harm fromstigma and organizational bias, regardless if RTD or evacuated
Psychol. Inj. and Law (2017) 10:24–71 65

from war zones or never deployed. On the other hand,Table 12 also suggests that stigma is slightly greater at homethan abroad, so one may technically cite greater stigmata ef-fects for personnel evacuated back home. However, without acomparison of the stigmata effects experienced by nonpsychi-atric evacuees and/or deployed personnel RTD who subse-quently develop war stress injury (e.g., PTSD), any assertionthat frontline psychiatry helps individuals avoid harmful stig-ma by preventing evacuation is not yet substantiated. Thehypothesis is worthy of investigation, and the health benefitsfor service members require that this happens.
Evidence That Frontline Psychiatry Prevents Harmfrom Career Loss
Since WWI, psychiatric evacuation to hospitals outside the warzone has been associated with increased risk of military dis-charge, which in large part led to the military’s adoption of front-line psychiatry in the first place (see Russell & Figley, 2016). Forexample, after scouting the British Army’s management of warstress casualties before the USA entered WWI, Salmon (1917)reported that 79% of British soldiers were discharged from themilitary after being evacuated and admitted to UK general hos-pitals and insane asylums for conditions like Bshell shock.^Military personnel discharged early from the military for anyreason (physical or mental health) were reported to have higherlevels of mental health problems than personnel transitioning atthe end of their service contracts (Buckman et al., 2012).Therefore, concerns over potential harm from premature militarydischarge appear justified.
Contemporary Research on Military Hospitalizationsand Discharge
In contemporary US military settings, psychiatric disorder isconsistently the leading category of discharge diagnoses formilitary separation. For example, Hoge et al. (2002) reportedthat nearly 50% of nondeployed service members hospital-ized for a psychiatric disorder received a military dischargewithin 6 months, compared to only 12% of personnel hos-pitalized for any of 15 other major illness categories (regard-less of age, gender, or length of service). Similarly, a 2005study reported that 45% of US military personnel whosedeployment status was unreported were separated from themilitary for any reason within 6 months of their psychiatricadmission, as compared to 11% of discharges followingmedical justification (Hoge et al., 2005). In other words, amental health diagnosis, irrespective if deployment related ornot, places service members at risk for early military dis-charge. Possible explanations for the vastly disproportionaterate of psychiatric and medical discharges include mentalhealth stigma, personality disorder, pre-existing mental
health condition, and/or related behaviors incompatible withmilitary service, such as misconduct, substance abuse, andsuicide gestures (e.g., Hoge et al., 2005). Importantly, noneof these studies specifically examined the role of psychiatricevacuations and hospital admission from war zones. In fact,there is no research comparing postdeployment military sep-aration rates between service personnel RTD via frontlinepsychiatry and those evacuated and treated in mental healthfacilities (see Table 9).
For instance, Hoge, Auchterlonie, and Milliken (2006) foundthat 20.8% of OEF veterans and 21.4% of OIF veterans weredischarged from the military within 1 year after endorsing psy-chiatric symptoms on a postdeployment health assessment(PDHA) suggestive of conditions like PTSD. It bears mention-ing, however, that the subjects in the study all returned homewiththeir deployed units as opposed to obtaining psychiatric evacua-tion. It is unknown what percentage of discharged OEF/OIFveterans were RTD via frontline psychiatry and what percentageof those who screened negative on PDHAwere later diagnosedwith a war stress injury or the comparative military separationrates for successful treatment completers. The latter is particularlyrelevant given reports by the architect of the US military’s WWIfrontline psychiatry doctrine, who reported that 60% of Britishsoldiers were eventually RTD to their units after receiving properspecialized treatment outside the war zone (Salmon, 1917).
Fur thermore , a contemporary US analys i s ofpostdeployment hospitalizations for both medical and mentalhealth reasons found that deployed service members overallhad a lower risk of hospitalization when compared withnondeployers (Smith, LeardMann, Smith, Jacobson, &Ryan, 2009). Thus, personnel evacuated out of war zonesfor psychiatric reasons may engender less risk for hospitaliza-tion and possible military discharge than those never de-ployed. In addition, UK researchers reported that individualsprematurely discharged from the military for psychiatric rea-sons were significantly less likely to have been deployed(Buckman et al., 2012).
Taken together, there appears to be considerable evidenceagainst the automatic assumption that psychiatric evacuees areinherently at greater risk of harm from losing their militarycareers than those RTD. The bottom line is that we simply donot know the true state of affairs because the issue has yet to beinvestigated. In sum, the most accurate conclusion that can bereached is that deployed US personnel with a diagnosable warstress injury are at high risk of military discharge whether theyare RTD or evacuated for psychiatric treatment. The reasonsbehind this apparent outcome might relate to mental healthstigma and bias, as well as inadequate access to quality mentalhealth treatment (e.g., Institute of Medicine, 2014a).Therefore, until head-to-head comparisons of deployed per-sonnel RTD and evacuated are conducted, any claim thatfrontline psychiatry benefits military members and their fam-ilies by preventing career loss is unsubstantiated.
66 Psychol. Inj. and Law (2017) 10:24–71

Evidence That Frontline Psychiatry and RTDPrevents War Stress Injury like PTSD
One of the military’s most frequently cited individual healthbenefits from frontline psychiatry is that RTD prevents orreduces the risk of long-term harm from developing condi-tions like PTSD. As mentioned earlier, the direct empiricalbasis of such claims is essentially comprised of a single lon-gitudinal IDF study from the 1982 Lebanon War, in whichlower PTSD rates were reported in Israeli veterans RTD afterreceiving frontline treatment as compared to veterans evacu-ated to rear hospitals (e.g., Solomon & Benbenishty, 1986;Solomon et al., 2005). Missing, however, is any informationon the nature, quality, and effectiveness of the psychiatrictreatment the hospitalized evacuees had received.Furthermore, the IDF findings often did not reach statisticalsignificance, as more than half (52%) of those RTD via front-line psychiatry developed PTSD within a year as compared to66% of soldiers evacuated to a general, nonmilitary hospital(e.g., Solomon & Benbenishty, 1986; Solomon, Weisenberg,Schwarzwald, et al., 1987). Furthermore, as evident inTable 6, the IDF’s extensive outcome research on CSR andfrontline psychiatry reveals that CSR is robustly associatedwith a host of chronic adverse health effects, includingPTSD, irrespective of whether combatants receive frontlineor hospitalized interventions. For example, Solomon andBenbenishty (1986) reported that 52% of Israeli soldiers diag-nosed and treated for CSR via frontline psychiatry developedPTSD.
More recently, two independent reviews of the USmilitary’s PTSD prevention programs were conducted by theInstitute of Medicine (IOM, 2014b) and RAND (Weinicket al., 2011). They examined frontline psychiatry/COSCBattlemind resilience training, and Comprehensive SoldierFitness resilience and posttraumatic growth training programs,respectively. Both agencies found little empirical support forthe military’s prevention programs (IOM, 2014b; Weinicket al., 2011). According to the IOM (2014b), BAssessmentsof DOD programs conducted by this committee and othersshow that a majority of DOD resilience, prevention, and rein-tegration programs are not consistently based on evidence andthat programs are evaluated infrequently or inadequately^ (p.166). They concluded that BFinally, the committee found lim-ited ongoing evaluation to inform program areas lacking evi-dence, and a clear need for longitudinal follow-up assessmentto determine the impact of resilience, prevention, and earlyintervention efforts^ (p. 166). Similarly, RAND researchersreported BPrograms are evaluated infrequently-fewer thanone-third of programs in any branch of service reported hav-ing had an outcome evaluation in the past 12 months^(Weinick et al., 2011, p. xvii). The general absence of outcomeresearch and data as reported by the agencies seriously under-mines the veracity of military claims that frontline psychiatry
is evidence-informed in terms of reducing risk of PTSD orother war stress injury.
Evidence That RTD via Frontline PsychiatryEnhances Posttraumatic Growth
Lastly, contemporary frontline psychiatry/COSC policy adver-tises that the benefits to service members include enhancingPTG (DOA, 2006; see Russell & Figley, 2016). Tedeschi(2011) cited evidence of PTG in various studies of combat vet-erans from the Vietnam, Yom Kippur, and Persian Gulf Wars.The veterans reported positive life outcomes following traumaticamputation, TBI, severe PTSD, and being a prisoner of war. ThatPTG is one possible pathway for war veterans is not disputed.The issue, however, is whether frontline psychiatry enhancesPTG, as the military purports. To that end, commissioned studiesof the military’s prevention programs by RAND (Weinick et al.,2011) and IOM (2014b) concluded that there is no evidence ofefficacy in prevention programs like the US Army’sComprehensive Soldier Fitness training in facilitating PTG.Moreover, no research has ever been conducted on PTG andRTD via frontline psychiatry (see Tables 2, 3, 4, 5, 6, 7, 8, and9). Similarly, there has been no research on PTG in psychiatricwar zone evacuees. Therefore, any claim that frontline psychiatrypromotes PTG is unsubstantiated.
Conclusions on the Health Benefits to MilitaryPersonnel and Their Families
In sum, the first-ever systematic review of the military’s 100-year-old mental health doctrine provides evidence that the soleempirically tested benefit of frontline psychiatry involvespreventing psychiatric attrition fromwar zones and thus conserv-ing the fighting force. This research outcome is conducive to theprimary mission of the military, i.e., to fight and win wars. Withregard to the military’s claim that frontline psychiatry is mutuallybeneficial to deployed personnel and their families, we could findno credible evidence to reliably support any of the advertisedhealth-promoting benefits. In fact, trends were identified thatappear to neutralize or even contradict most of the military’sclaims. There has been no effort to properly investigate thelong-term health impact from the military’s frontline mentalhealth policies. Instead, the vast bulk of military outcome re-search has narrowly focused on maximizing RTD and restrictingevacuations. Instead of any direct testing of the long-term healthconsequence from its frontline doctrine, the US military has re-lied extensively on anecdotal reports and on unsubstantiated nar-rative. We will examine other trends that filter out of the researchin our final evidentiary review of potential harm arising out of themilitary’s frontline psychiatry doctrine.
Psychol. Inj. and Law (2017) 10:24–71 67

Acknowledgements We thank David Gellman for his assistance withthe literature review. This study was unfunded.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflicts ofinterest.
References
Ahronson, A., & Cameron, J. E. (2007). The nature and consequences ofgroup cohesion in the military sample.Military Psychology, 19, 9–25.
Allerton, W. S. (1969). Army psychiatry in Viet Nam. In P. G. Bourne(Ed.), The psychology and physiology of stress: With reference tospecial studies of the Viet Nam War (pp. 1–17). New York:Academic Press.
Armistead-Jehle, P., Johnston, S. L., Wade, N. G., & Ecklund, C. J.(2011). Posttraumatic stress in U.S. marines: The role of unit cohe-sion and combat exposure. Journal of Counseling & Development,89, 81–88.
Bartemeier, L. H., Kubie, L. S., Menninger, K. A., Romano, J., &Whitehorn, J. C. (1946). Combat exhaustion. Journal of Nervousand Mental Disease, 104, 358–389.
Belenky, G. L., Tyner, C. F., & Sodetz, F. J. (1983). Israeli battle shockcasualties: 1973 and 1982. Washington, DC: Walter Reed ArmyInstitute of Research.
Benyamini, Y., & Solomon, Z. (2005). Combat stress reactions, posttrau-matic stress disorder, cumulative life stress, and physical healthamong Israeli veterans twenty years after exposure to combat.Social Science & Medicine, 61, 1267–1277.
Brewin, C. R., Andrews, B., & Valentine, J. D. (2000). Meta-analysis of riskfactors for posttraumatic stress disorder in trauma-exposed adults.Journal of Consulting and Clinical Psychology, 68, 748–766.
Brill, N. Q., & Beebe, G. W. (1952). Psychoneurosis: Military applica-tions of a follow-up study. U.S Armed Services Medical Journal, 3,15–33.
Brooke, E. M. (1946). Battle exhaustion review of 500 cases fromWestern Europe. British Medical Journal, 2, 491–493.
Brown, W. (1919). War neurosis: A comparison of cases seen in the fieldwith those seen at a base. Lancet, 1, 833–836.
Buckman, J. E. J., Forbes, H. J., Clayton, T., Jones, M., Jones, N.,Greenberg, N.,… Fear, N. T. (2012). Early service leavers: A studyof the factors associated with premature separation from the U.K.armed forces and the mental health of those that leave early.European Journal of Public Health, 23, 410–415.
Camp, N. M. (1994). Ethical challenges for the psychiatrist during theVietnam conflict. In F. D. Jones, L. R. Sparacino, V. L. Wilcox, & J.M. Rothberg (Eds.), Textbook of military medicine, military psychi-atry: Preparing in peace for war (pp. 133–150). Washington, DC:Office of the Surgeon General, U. S. Army, Borden Institute.
Camp, N. M. (2014). U.S. army psychiatry in the Vietnam War: Newchallenges in extended counterinsurgency warfare. Fort SamHuston: Borden Institute, U.S. Army Medical Department Centerand School.
Castro, A. C. (2014). The US framework for understanding, preventing,and caring for the mental health needs of service members whoserved in combat in Afghanistan and Iraq: A brief review of theissues and the research. European Journal of Psychotraumatology,5, 1–12.
Cigrang, J. A., Peterson, A. L., & Schobitz, R. P. (2005). Three Americantroops in Iraq: Evaluation of a brief exposure therapy treatment for
the secondary prevention of combat-related PTSD. Pragmatic CaseStudies in Psychotherapy, 1, 1–25.
Cohen, S. P., Brown, C., Kurihara, C., Plunkett, A., Nguyen, C., &Strassels, S. A. (2010). Diagnoses and factors associated with med-ical evacuation and return to duty for service members participatingin Operation Iraqi Freedom or Operation Enduring Freedom: Aprospective cohort study. Lancet, 375, 301–309.
Cooper, E. L., & Sinclair, A. J. M. (1942). War neuroses in Tobruk: Areport on 207 patients from the Australian Imperial force units inTobruk. The Medical Journal of Australia, 2, 73–81.
Dean, E. T. (1997). Shook over hell: Post-traumatic stress Vietnam andthe Civil war. Cambridge, MA: Harvard University Press.
Dekel, R., Solomon, Z., Ginzburg, K., & Neria, Y. (2003). Combat ex-posure, wartime performance, and long-term adjustment amongcombatants. Military Psychology, 15(2), 117–131.
Department of Navy, & U.S. Marine Corps. (2010). Combat and opera-tional stress control. Washington, DC: U.S. Navy, NTTP 1-15M;U.S. Marine Corps, MCRP 6-11C. December 2010.
Department of the Army. (2006). Combat and operational stress control:Field manual 4-02.51 (FM 8-51). Washington, DC: Headquarters,Department of the Army.
Department of Veterans Affairs, & Department of Defense. (2010). VA/DoD clinical practice guideline for the management of post-t raumat ic s t ress . Washington , DC: Veterans Heal thAdministration, Department of Veterans Affairs and HealthAffairs, Department of Defense, Office of Quality andPerformance publication 10Q-CPG/PTSD-10.
Dillon, F. (1939). Neuroses among combatant troops in the Great War.British Medical Journal, 2, 66.
Du Preez, J., Sundin, J., Wessely, S., & Fear, N. T. (2012). Unit cohesionand mental health in the UK armed forces. Occupational Medicine,62, 47–53.
Elbogen, E. B., Johnson, S. C., Wagner, H. R., Newton, V.M., Timko, C.,Vasterling, J. J., & Beckham, J. C. (2012). Protective factors and riskmodification of violence in Iraq and Afghanistan. Journal ofClinical Psychiatry, 73, 767–773.
Fear, N. T., Jones, M., Murphy, D., Hull, L., Iversen, A. C., Coker, B.,…Wessely, S. (2010). What are the consequences of deployment toIraq and Afghanistan on the mental health of the UK armed forces?A cohort study. Lancet, 375, 1783–1797.
Frappell-Cooke, W., Gulina, M., Green, K., Hacker Hughes, J., &Greenberg, N. (2010). Does trauma risk management reduce psy-chological distress in deployed troops? Occupational Medicine, 60,645–650.
Ginzburg, K., & Solomon, Z. (2011). Trajectories of stress reactions andsomatization symptoms amongwar veterans: A 20-year longitudinalstudy. Psychological Medicine, 41, 353–362.
Glass, A. J. (1947). Effectiveness of forward neuropsychiatric treatment.Bulletin of the U.S Army Medical Department, 7, 1034–1041.
Glass, A. J. (1966). Army psychiatry before World War II. In A. J. Glass& R. J. Bernucci (Eds.), Medical Department United States Army.Neuropsychiatry in World War II, Vol. I: Zone of interior (pp. 3–23).Washington, DC: Office of the Surgeon General, Department of theArmy.
Gordon, E. L. (1967). Division psychiatry: Documents of a tour.US ArmyVietnam Medical Bulletin, November/December, 62–69.
Government Accountability Office. (2016). Human capital: Additionalactions needed to enhance DoD’s efforts to address mental healthcare stigma: GAO-16-404. Washington, DC: GovernmentAccountability Office.
Granado, N. S., Zimmermann, L., Smith, B., Jones, K. A., Wells, T. S.,Ryan, M. A., … Smith, T.C. (2012). Individual augmentee deploy-ment and newly reported mental health morbidity. Journal ofOccupational Environmental Medicine, 54, 615–620.
Grinker, R. R., & Spiegel, J. P. (1943).War neuroses in North Africa: TheTunisian campaign (January-May 1943). Restricted report prepared
68 Psychol. Inj. and Law (2017) 10:24–71

for The Air Surgeon, Army Air Forces. New York: Josiah Macy, Jr.Foundation.
Han, S. C., Castro, F., Lee, L. O., Charney, M. E., Marx, B. P., Brailey,…Vasterling, J. J. (2014). Military unit support, post deployment socialsupport, and PTSD symptoms among active duty and NationalGuard soldiers deployed to Iraq. Journal of Anxiety Disorders, 28,446–453.
Hanson, F. R., & Ranson, S. W. (1949). Statistical studies. In F. R.Hanson (Ed.), Combat psychiatry: Experiences in the NorthAfrican and Mediterranean theaters of operation American groundforces, World War II. Honolulu: U.S. Army Medical Department,University Press of Pacific.
Harman, D. R., Hooper, T. I., & Gackstetter, G. D. (2005). Aeromedicalevacuations from Operation Iraqi freedom: A descriptive study.Military Medicine, 170, 521–527.
Hauret, K. G., Taylor, B. J., Clemmons, N. S., Block, S. R., & Jones, B.H. (2010). Frequency and causes of non-battle injuries air evacuatedfrom operations Iraqi freedom and enduring freedom, U.S. army,2001–2006. American Journal of Preventive Medicine, 38, 94–107.
Hing, M., Cabrera, J., Barstow, C., & Forsten, R. (2012). Special opera-tions forces and incidence of post-traumatic stress disorder symp-toms. Journal of Special Operations Medicine, 12, 23–35.
Hoge, C. W., Auchterlonie, J. L., & Milliken, C. S. (2006). Mental healthproblems, use of mental health services and attrition from militaryservice after returning from deployment to Iraq or Afghanistan.Journal of the American Medical Association, 295, 1023–1032.
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., &Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, men-tal health problems, and barriers to care. New England Journal ofMedicine, 351, 13–22.
Hoge, C. W., Castro, C. A., & Eaton, K. M. (2006). Impact of combatduty in Iraq and Afghanistan on family functioning: Findings fromthe Walter Reed Army Institute of research land combat study. In:Human dimensions in military operations—military leaders’ strate-gies for addressing stress and psychological support (pp. 5-1–5-6).Meeting Proceedings RTO-MP-HFM-134, Paper 5. Neuilly-sur-Seine, France: RTO. Available from: http://www.rto.nato.int/abstracts.asp
Hoge, C. W., Lesikar, S. E., Guevara, R., Lange, J., Brundage, J. F.,Engel, C. C., … & Orman, D. T. (2002). Mental disorders amongUS military personnel in the 1990’s: Association with high levels ofhealth care utilization and early military attrition. American Journalof Psychiatry, 159, 1576–1583.
Hoge, C. W., Toboni, H. E., Messer, S. C., Bell, N., Amoroso, P., &Orman, D. T. (2005). The occupational burden of mental disordersin the US military: Psychiatric hospitalizations, involuntary separa-tions, and disability. American Journal of Psychiatry, 162, 585–591.
Holden, W. (1998). Shell shock: The psychological impact of war.London: Macmillan.
Holsenbeck, L. S. (1996). Psych force 90. In J. A. Martin, L. R.Sparacino, & G. Belenky (Eds.), The gulf war and mental health(pp. 39–58). Westport: Praeger.
Horesh, D., Solomon, Z., Zerach, G., & Ein-Dor, T. (2011). Delayed-onset PTSD among war veterans: The role of life events throughoutthe life cycle. Social Psychiatry and Psychiatric Epidemiology, 46,863–870.
Hoyt, T., Garnica, G., Marsh, D., Clark, K., Desadier, J., & Brodniak, S.(2015). Behavioral health trends throughout a 9-month brigade com-bat team deployment to Afghanistan. Psychological Services, 12,59–65.
Hung, B. (2008). Behavioral health activity and workload in the Iraq theaterof operations. US Army Medical Department Journal, 39, 42.
Hunter, D. (1946). The work of a corps psychiatrist in the Italian cam-paign. Journal of the Royal Army Medical Corps, 86, 127–130.
Institute of Medicine. (2014a). Preventing psychological disorders inservice members and their families: An assessment of programs.Washington, DC: The National Academies Press.
Institute of Medicine. (2014b). Treatment for posttraumatic stress disor-der in military and veteran populations: Final assessment.Washington, DC: The National Academies Press.
Jarrett, T. A. (2013). Warrior resilience and thriving (WRT): Rationalemotive behavior therapy (REBT) as a resiliency and thriving foun-dation to prepare warriors and their families for combat deploymentand posttraumatic growth in operation Iraqi freedom, 2005–2009.Journal of Rational-Emotive & Cognitive-Behavioral Therapy, 31,93–107.
Johnson, W., & Rows, R. G. (1923). Neurasthenia and war neuroses. InW. G. Macpherson, W. P. Herringham, T. R. Elliott, & A. Balfour(Eds.), History of the Great War based on official documents, med-ical services, diseases of the war (Vol. 2, pp. 2–61). London:HMSO.
Joint Mental Health Advisory Team-8. (2013) Operation enduring free-dom 2013 Afghanistan (12 August 2013). Office of the SurgeonGeneral United States Army Medical Command and Office of theCommand Surgeon HQ, USCENTCOM and Office of theCommand Surgeon U.S. Forces Afghanistan (USFOR-A).Retrieved from http://armymedicine.mil/Documents/J_MHAT_8_OEF_Report.pdf
Jones, F. D. (1995a). Psychiatric lessons of war. In R. Zatchuk & R. F.Bellamy (Eds.), Textbook of military medicine: War psychiatry (pp.1–34). Washington, DC: Office of the SurgeonGeneral, U. S. Army,Borden Institute.
Jones, F. D. (1995b). Traditional warfare combat stress casualties. In R.Zatchuk & R. F. Bellamy (Eds.), Textbook of military medicine: Warpsychiatry (pp. 35–61). Washington, DC: Office of the SurgeonGeneral, U. S. Army, Borden Institute.
Jones, N., Fear, N. T., Jones, M., Wessely, S., & Greenberg, N. (2010).Long-term military work outcomes in soldiers who become mentalhealth casualties when deployed on operations. Psychiatry:Interpersonal and Biological Processes, 73, 352–364.
Jones, E., & Palmer, I. P. (2000). Army psychiatry in the KoreanWar: Theexperience of 1 Commonwealth Division. Military Medicine, 165,256–260.
Jones, N., Seddon, R., Fear, N. T., McAllister, P., Wessely, S., &Greenberg, N. (2012). Leadership, cohesion, morale, and the mentalhealth of UK Armed Forces in Afghanistan. Psychiatry, 75(1), 49–59.
Jones, E., Thomas, A., & Ironside, S. (2007). Shell shock: an outcome studyof a first world war ‘PIE’ unit. Psychology Medicine, 37, 215–223.
Jones, E., & Wessely, S. (2003). Forward psychiatry in the military: Itsorigin and effectiveness. Journal of Traumatic Stress, 16, 411–419.
Jones, E., &Wessely, S. (2007). A paradigm shift in the conceptualizationof psychological trauma in the 20th century. Journal of AnxietyDisorders, 21, 164–175.
Kulka, R. A., Schlenger, W. E., Fairbank, J. A., Hough, R. L., Jordan, B.K., Marmar, C. R., & Weiss, D. S. (1990). Trauma and the VietnamWar generation: Report of findings from the National VietnamVeterans readjustment study. New York: Brunner/Mazel.
L’eri, A. (1919). Shell shock, commotional and emotional aspects.London: University of London Press.
Lande, R. G., Williams, L. B., Francis, J. L., Gragnani, C., & Morin, M.L. (2010). Efficacy of biofeedback for post-traumatic stress disorder.Complimentary Therapies in Medicine, 18, 256–259.
Lerner, P. (2003). Hysterical men: War, psychiatry, and the politics oftrauma in Germany, 1890–1930. London: Cornell University Press.
Levav, I., Greenfeld, H., & Baruch, E. (1979). Psychiatric combat reac-tions during the Yom Kippur War. American Journal of Psychiatry,136, 637–641.
Linden, S. C., Jones, E., & Lees, A. J. (2013). Shell shock at QueenSquare: Lewis Yealland 100 years on. Brain, 136, 1976–1988.
Psychol. Inj. and Law (2017) 10:24–71 69

Ludwig, A., & Ranson, S. (1947). A statistical follow-up of effectivenessof treatment of combat-induced psychiatric casualties: Returns tofull combat duty. Military Surgeon, 100, 51–62.
Martin, J. A., & Cline, W. R. (1996). Mental health lessons from thePersian Gulf War. In J. A. Martin, L. R. Sparacino, & G. Belenky(Eds.), The Gulf War and mental health: A comprehensive guide (pp.161–178). Westport: Praeger.
Mattila, A. M., Crandall, B. D., & Goldman, S. B. (2011). U.S. Armycombat operational stress control throughout the deployment cycle:A case study. Cancer Biomarkers, 38, 13–18.
McGeorge, T., Hughes, J. H., & Wessely, S. (2006). The MoD PTSDdecision: A psychiatric perspective. Occupational Health Review,122, 21–28.
McLay, R. N., McBrien, C., Wiederhold, M. D., & Wiederhold, B. K.(2010). Exposure therapy with and without virtual reality to treatPTSD while in the combat theater: A parallel case series.Cyberpsychology, Behavior and Social Networking, 13, 37–43.
Mental Health Advisory Team-I. (2003). MHAT Operation Iraqi freedom 16December 2003. U.S. Army Surgeon General. Retrieved fromhttp://www-tc.pbs.org/wgbh/pages/frontline/shows/heart/readings/mhat.pdf
Mental Health Advisory Team-II. (2005). Operation Iraqi freedom-II,Mental Health Advisory Team (MHAT-II), 20 January 2005. U.S.Army Surgeon General. Retrieved from http://armymedicine.mil/Documents/MHAT-Team-II-OIF-II-REPORT.pdf.
Mikulincer, M., Solomon, Z., & Benbenishty, R. (1988). Battle events,acute combat stress reaction and long term psychological sequelaeof war. Journal of Anxiety Disorders, 2, 121–133.
Momen, N., Strychacz, C. P., & Virre, E. (2012). Perceived stigma andbarriers to mental health care in Marines attending the combat oper-ational stress control program. Military Medicine, 177, 1143–1148.
Moore, B. A., & Krakow, B. (2007). Imagery rehearsal therapy for acuteposttraumatic nightmares among combat soldiers in Iraq. TheAmerican Journal of Psychiatry, 164, 683.
Noy, S., Levy, R., & Solomon, Z. (1984). Mental health care in theLebanon War 1982. Israel Journal of Medical Sciences, 20, 360–363.
Ogle, A. D., Bradley, D., Santiago, P., & Reynolds, D. (2012).Description of combat and operational stress control in regionalcommand east, Afghanistan. Military Medicine, 177, 1279–1286.
Oliver, L. W., Harman, J., Hoover, E., Hayes, S. M., & Pandhi, N. A.(1999). A quantitative integration of the military cohesion literature.Military Psychology, 11, 57–83.
Ozer, E. J., Best, S. R., Lipsey, T. L., &Weiss, D. S. (2003). Predictors ofposttraumatic stress disorder and symptoms in adults: A meta-anal-ysis. Psychology Bulletin, 129, 52–73.
Parrish, B. D. (2008). Dialectical behavior therapy deployed: An aggres-sive alternative to traditional mental health on the noncontiguousbattlefield. U.S. Army Medical Department Journal, 24–31.
Peterson, A. L., Baker, M. T., & McCarthy, K. R. (2008). Combat stresscasualties in Iraq. Part 2: Psychiatric screening prior to aeromedicalevacuation. Perspectives in Psychiatric Care, 44, 159–168.
Phillips, C. J., LeardMann, C. A., Gumbs, G. R., & Smith, B. (2010).Risk factors for posttraumatic stress disorder among deployed USmale marines. BMC Psychiatry, 10, 52.
Pietrzak, R. H., Johnson, D. C., Goldstein,M. B.,Malley, J. C., Rivers, A.J., Morgan, C. A., & Southwick, S. M. (2009). Psychosocial buffersof traumatic stress, depressive symptoms, and psychosocial difficul-ties in veterans of operations enduring freedom and Iraqi freedom:The role of resilience, unit support, and post-deployment social sup-port. Journal of Special Operations Medicine, 9, 74–78.
Potter, A. R., Baker, M. T., Sanders, C. S., & Peterson, A. L. (2009).Combat stress reactions during military deployments: Evaluationof the effectiveness of combat stress control treatment. Journal ofMental Health Counseling, 31, 137–148.
Rabasca, L. (2000). More psychologists in the trenches: Under a newmilitary directive, mental health professionals’ work gains promi-nence. APA monitor, 31, 50.
Ramchand, R., Rudavsky, R., Grant, S., Tanielian, T., & Jayconx, L.(2015). Prevalence of, risk factors for, and consequences of post-traumatic stress disorder and other mental health problems in mili-tary populations deployed to Iraq and Afghanistan. CurrentPsychiatry Reports, 17, 1–11.
Ritchie, E. C. (2002). Psychiatry in the Korean War: Perils, PIES, andprisoners of war. Military Medicine, 167, 898–903.
Ritchie, E. C. (2007). Update on combat psychiatry: From the battle frontto the home front and back again. Military Medicine, 172, 11–14.
Ruck, D. C. (1996). 18th airborne corps OM team. In J. A. Martin, L. R.Sparacino, & G. Belenky (Eds.), The gulf war and mental health: Acomprehensive guide (pp. 59–72). Westport: Praeger.
Rundell, J. R. (2006). Demographics of and diagnoses in operation en-during freedom and operation Iraqi freedom personnel who werepsychiatrically evacuated from the theater of operations. GeneralHospital Psychiatry, 28, 352–356.
Russel, C. (1919). The management of psychoneuroses in the Canadianarmy. Journal of Abnormal Psychology, 14, 29–30.
Russell, M. (2006). Treating combat-related stress disorders: A multiplecase study utilizing eye movement desensitization and reprocessing(EMDR) with battlefield casualties from the Iraqi War. MilitaryPsychology, 18(1), 1–18.
Russell, M. C., & Figley, C. R. (2016). Does the military’s frontlinepsychiatry/combat and operational stress control doctrine harm vet-erans?—Part one: Framing the issue. Manuscript submitted forpublication.
Russell, M. C., Zinn, B., & Figley, C. R. (2016). Exploring options in-cluding class action to transformmilitarymental healthcare and endsthe generational cycle of preventable wartime behavioral health cri-ses. Psychological Injury and Law, 9, 166–197.
Salmon, T. W. (1917). The care and treatment of mental diseases and warneuroses (‘shell shock’) in the British Army. Mental Hygiene, 1,509–547.
Salmon, T. W., & Fenton, N. (1929). In the American expeditionaryforces (section 2). Neuropsychiatry. Vol. 10. In the MedicalDepartment of the United States Army in the World War.Washington, DC: Office of the Surgeon General, U.S. Army.
Schmitz, K. J., Schmied, E. A., Webb-Murphy, J. A., Hammer, P. S.,Larson, G. E., Conway, T. L., Galameau, M. R., Boucher, W. C.,Edwards, N. K., & Johnson, D. C. (2012). Psychiatric diagnoses andtreatment of U.S. military personnel while deployed to Iraq.MilitaryMedicine, 177, 380–389.
Scott, J. N. (2005). Diagnosis and outcome of psychiatric referrals to thefield mental health team, 202 field hospital, Op Telic I. Journal ofthe Royal Army Medical Corps, 151, 95–100.
Shepard, B. (2001). A war of nerves: Soldiers and psychiatrists in thetwentieth century. Cambridge: Harvard University Press.
Smith, T. C., LeardMann, C. A., Smith, B., Jacobson, I. G., & Ryan, M.A. K. (2009). Postdeployment hospitalizations among service mem-bers deployed in support of the operations in Iraq and Afghanistan.Annals of Epidemiology, 19, 603–612.
Solomon, Z., Benbenishti, R., & Mikulincer, M. (1988). A follow-up ofIsraeli casualties of combat stress reaction (‘battle shock’) in the1982 Lebanon War. British Journal of Clinical Psychology, 27,125–135.
Solomon, Z., Benbenishti, R., &Mikulincer, M. (1991). The contributionof wartime, pre-war, and post-war factors to self-efficacy: A longi-tudinal study of combat stress reactions. Journal of TraumaticStress, 4, 345–362.
Solomon, Z., & Benbenishty, R. (1986). The role of proximity, immedi-acy, and expectancy in frontline treatment of combat stress reactionamong Israelis in the LebanonWar. American Journal of Psychiatry,143, 613–617.
70 Psychol. Inj. and Law (2017) 10:24–71

Solomon, Z., Debby-Aharonl, S., Zerach, G., & Horesh, D. (2011).Marital adjustment, parental functioning, and emotional sharing inwar veterans. Journal of Family Issues, 32, 127.
Solomon, Z.,&Flum,H. (1988). Life events, combat stress reaction and post-traumatic stress disorder. Social Science & Medicine, 26, 319–325.
Solomon, Z., &Mikulincer, M. (1988). Psychological sequelae of war: A2-year follow-up study of Israeli combat stress reaction casualties.The Journal of Nervous and Mental Disease, 176, 264–269.
Solomon, Z., & Mikulincer, M. (1992). Aftermaths of combat stressreactions: A three-year study. British Journal of ClinicalPsychology, 31, 21–32.
Solomon, Z.,Mikulincer,M., &Bleich, A. (1988). Characteristic expressionsof combat-related posttraumatic stress disorder among Israeli soldiers inthe 1982 Lebanon War. Behavioral Medicine, 14, 171–178.
Solomon, Z., Mikulincer, M., & Hobfoll, S. E. (1986). Effects of socialsupport and battle intensity on loneliness and breakdown duringcombat. Journal of Personality and Social Psychology, 51, 1269–1276.
Solomon, Z., Mikulincer, M., & Jakob, B. R. (1987). Exposure to recur-rent combat stress: Combat stress reactions in Israeli soldiers in theLebanon war. Psychological Medicine, 17, 423–433.
Solomon, Z., Mikulincer, M., & Kotler, M. (1987). A two year follow-upof somatic complaints among Israeli combat stress reaction casual-ties. Journal of Psychosomatic Research, 31, 463–469.
Solomon, Z., Mikulincer, M., & Waysman, M. (1991). Delayed and im-mediate onset posttraumatic stress disorder: II. The role of battleexperiences and personal resources. Social Psychiatry andPsychiatric Epidemiology, 26, 8–13.
Solomon, Z., Oppenheimer, B., Elizur, Y., & Waysman, M. (1990).Trauma deepens trauma: Consequences of recurrent combat stressreaction. Israeli Journal of Psychiatry Relationship Science, 27,233–241.
Solomon, Z., Oppenheimer, B., & Noy, S. (1986). Subsequent militaryadjustment of combat stress reaction casualties—A nine yearfollow-up study. Military Medicine, 151, 8–11.
Solomon, Z., Shklar, R., & Mikulincer, M. (2005). Frontline treatment ofcombat stress reaction: A 20-year longitudinal study. The AmericanJournal of Psychiatry, 162, 2309–2314.
Solomon, Z., Waysman, M., Fried, B., Mikulincer, M., Benbenishty, R.,Florian, V., & Blieich, A. (1992). From frontline to home front: Astudy of secondary traumatization. Family Process, 31, 289–302.
Solomon, Z., Waysman, M., Levy, G., Fried, B., Mikulincer, M.,Benbenishty, R., … & Bleich, A. (1992). From front line to homefront: A study of secondary traumatization. Family Process, 31,289–302.
Solomon, Z., Weisenberg, M., Schwarzwald, J., & Mikulincer, M.(1987). Posttraumatic stress disorder among frontline soldiers withcombat stress reaction: The 1982 Israeli experience. The AmericanJournal of Psychiatry, 144, 448–454.
Steiner, M., & Neuman, M. (1978). Traumatic neurosis and social sup-port in the YomKippur war returnees. Paper presented at the SecondInternational Conference on Psychological Stress and Adjustment inTime of War and Peace, Jerusalem, Israel, 19–23 June 1978.
Stetz, M. C., McDonald, J. J., Lukey, B. J., & Gifford, R. K. (2005).Psychiatric diagnoses as a cause of medical evacuation. AviationSpace, and Environmental Medicine, 76, 15–20.
Stoller, C. C., Greul, J. H., Cimini, L. S., Fowler, M. S., & Koomar, J. A.(2012). Effects of sensory-enhanced yoga on symptoms of combatstress in deployed military personnel. American Journal ofOccupational Therapy, 66(1), 59–68.
Stouffer, S. A., Lumsdaine, A. A., Lumsdaine, M. H., Williams, R. M.,Smith, M. B., Janis, I. L., … Cottrell, L. S. (1949). The Americansoldier: Combat and its aftermath. Volume 2. New Jersey: PrincetonUniversity Press.
Strange, R. E. (1969). Effects of combat stress on hospital ship psychiatricevacuees. In P. G. Bourne (Ed.), The psychology and physiology ofstress: With reference to special studies of the Viet NamWar (pp. 75–93). New York: Academic Press.
Strecker, E. A. (1919). Experiences in the immediate treatment of warneuroses. The American Journal of Psychiatry, 76, 45–69.
Sundin, J., Mulligan, K., Henry, S., Hull, L., Jones, N., Greenberg, N.,…Fear, N. T. (2012). Impact on mental health of deploying as anindividual augmentee in the U.K. Armed Forces. MilitaryMedicine, 177, 511–516.
Tedeschi, R. G. (2011). Posttraumatic growth in combat veterans. Journalof Clinical Psychology in Medical Settings, 18, 137–144.
Turner, M. A., Kiernan, M. D., McKechanie, A. G., Finch, P. J. C.,McManus, F. B., & Neal, L. A. (2005). Acute military psychiatriccasualties from the war in Iraq. British Journal of Psychiatry, 186,476–479.
Vaughan, C. A., Farmer, C. M., Breslau, J., & Burnette, C. (2015).Evaluation of the operational stress control and readiness(OSCAR) program. Santa Monica: RAND Corporation.
Weinick, R. M., Beckjord, E. B., Farmer, C. M., Martin, L. T., Gillen, E.M., Acosta, J. D., … Scharf, D. M. (2011). Programs addressingpsychological health and traumatic brain injury among U.S. mili-tary service members and their families. Prepared for the Office ofthe Secretary of Defense Center forMilitary Health Policy Research.Santa Monica: RAND.
Whitesell, A. A., & Owens, G. P. (2012). The impact of patriotism, mo-rale, and unit cohesion on mental health in veterans of Iraq andAfghanistan. Traumatology, 18, 1–7.
Wilde, J. F. (1942). Narco-analysis in the treatment of war neuroses.British Medical Journal, 2(4252), 4–7.
Wiltshire, H. (1916). A contribution to the etiology of shell shock. Lancet,1, 1207–1212.
Wojcik, B. E., Akhtar, F. Z., & Hassell, L. H. (2009). Hospital admissionsrelated to mental disorders in U.S. Army soldiers in Iraq andAfghanistan. Military Medicine, 174, 1010–1018.
Xue, C., Ge, Y., Tang, B., Liu, Y., Yang, P., Wang, M., & Zhang, L.(2015). A meta-analysis of risk factors for combat-related PTSDamong military personnel and veterans. PLoS One, 10, 1–11.
Yealland, L. R. (1918).Hysterical disorders of warfare. London:MacMillan.Zerach, G., Solomon, Z., Horesh, D., & Ein-Dor, T. (2013). Family co-
hesion and posttraumatic intrusion and avoidance among war vet-erans: A 20-year longitudinal study. Social Psychiatry andPsychiatric Epidemiology, 48, 205–214.
Zohar, J., Fostick, L., Cohen, A., Bleich, A., Dolfin, D., Weissman, Z.,…Shalev, A. Y. (2009). Risk factors for the development of posttrau-matic stress disorder following combat trauma: A semiprospectivestudy. Journal of Clinical Psychiatry, 70, 1629–1634.
Psychol. Inj. and Law (2017) 10:24–71 71