default template - children's memorial hermann hospital
TRANSCRIPT

Preterm Parturition in Twins An Evidence-Based Approach
George R. Saade, M.D. Professor, Departments of Ob-Gyn and Cell Biology
Jennie Sealy Smith Distinguished Chair in Obstetrics and Gynecology
Chief of Obstetrics and Maternal Fetal Medicine
Director, Perinatal Research Division
The University of Texas Medical Branch

Dr. George Saade has no conflict of
interest related to the content of this
presentation.

Prediction

fFN and Prediction of Delivery Meta-analysis of 27 Studies
Leitich et al. Am J Obstet Gynecol 1999;180:1169-76
81-918680-9789Patients with PTL96-97973-6022Symptom free
81-968857-9676All studies
95% CIValue95% CIValue
Specificity (%)Sensitivity (%)
Delivery within 7 days

Likelihood Ratio (LR)
LR for a positive test
Likelihood for positive test with disease
Likelihood for positive test without disease
LR for a negative test
Likelihood for negative test with disease
Likelihood for negative test without disease

Likelihood Ratio (LR) Positive result
Condition + Condition -
Test + a b
Test - c d
Likelihood of test positive with condition
Likelihood of test positive without condition
a/(a+c)
b/(b+d)
sensitivity / (1-specificity)
LR+ =
LR+ =
LR+ =

Likelihood Ratio (LR)
Condition + Condition -
Test + a b
Test - c d
sensitivity / (1-specificity) LR+ =
LR- = (1-sensitivity)/specificity

Bayes Nomogram

Bayes Nomogram

Bayes Nomogram

Bayes Nomogram

Significance of LR

Cervicovaginal fFN Systematic Review
Honest et al. BMJ 2002;325:301-4
Asymptomatic
<34 weeks
<37 weeks
Symptomatic
7-10 days
<34 weeks
<37 weeks
0.1 0.5 1 5 10
Likelihood Ratio Neg Pos

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Asymptomatic Multiples

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Asymptomatic Women

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Twins with Threatened Preterm Birth

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Pretest and Posttest Probabilities

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Pretest and Posttest Probabilities

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Pretest and Posttest Probabilities

fFN in Multiple Pregnancy Systematic Review
Conde-Agudelo. J Mat Fet Neo Med 2010;23:1365-76.
Pretest and Posttest Probabilities

What To Do With the Result?

Negative fFN and Probability of Delivery Plaut et al. Am J Obstet Gynecol 2003;188:1588-95
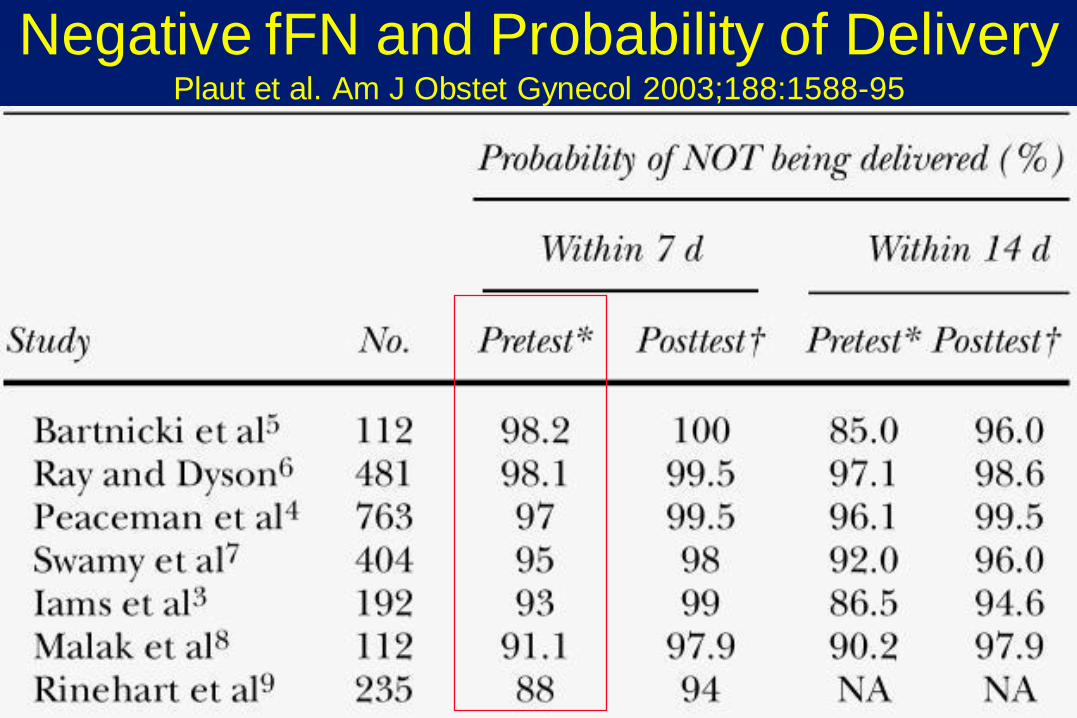
Negative fFN and Probability of Delivery Plaut et al. Am J Obstet Gynecol 2003;188:1588-95

Rapid Bedside fFN Prediction of Preterm Delivery
Coleman et al. Am J Obstet Gynecol 1998;179:1553-8
fFN and/or cervical dilatation > 1 cm for the predicting
delivery within 10 days in symptomatic women
fFN Cervix > 1 cm
fFN pos and/or
cervix > 1 cm
Sensitivity (%) 65 71 82Specificity (%) 85 87 76PPV (%) 41 46 36NPV (%) 94 95 96Likelihood Ratio
for positive testfor negative test
4.30.41
5.50.33
3.40.24

Rapid Bedside fFN Effect on Length of Hospital Stay
Plaut et al. Am J Obstet Gynecol 2003;188:1588-95

fFN and Physician Behavior RCT
Grobman et al. Am J Obstet Gynecol 2004;191: 235-40

LR for CL <25 mm in Predicting Delivery <34 wks Honest et al. Ultrasound Obstet Gynecol 2003;22:305-22
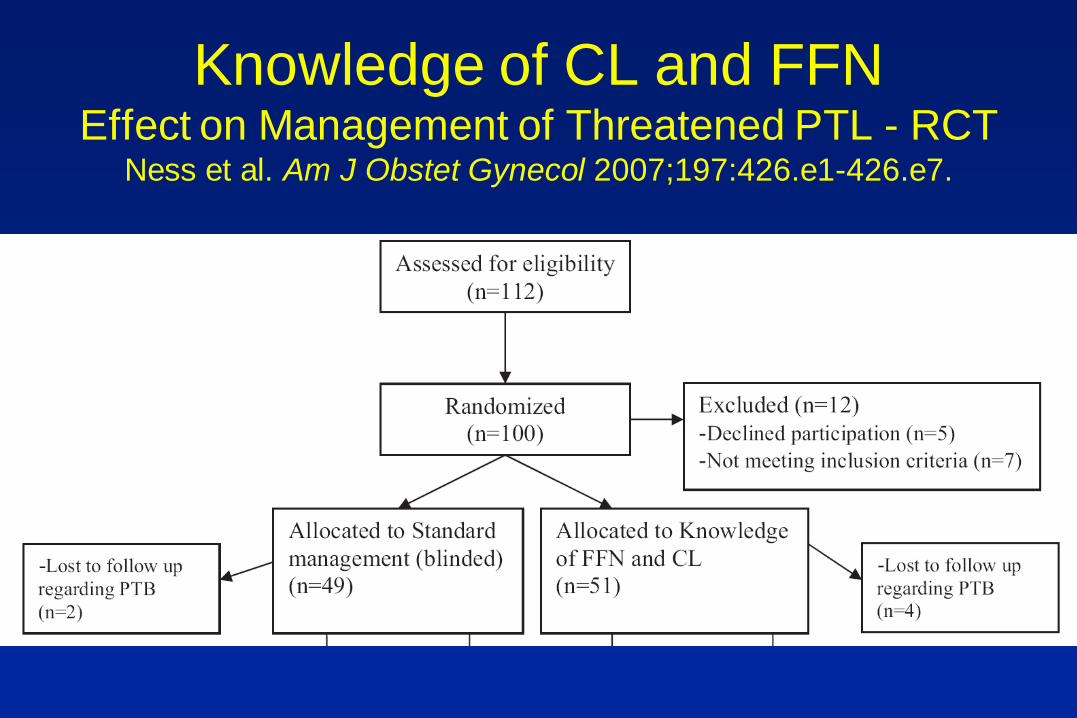
Knowledge of CL and FFN Effect on Management of Threatened PTL - RCT
Ness et al. Am J Obstet Gynecol 2007;197:426.e1-426.e7.
Knowledge of CL and FFN Effect on Management of Threatened PTL - RCT
Ness et al. Am J Obstet Gynecol 2007;197:426.e1-426.e7.

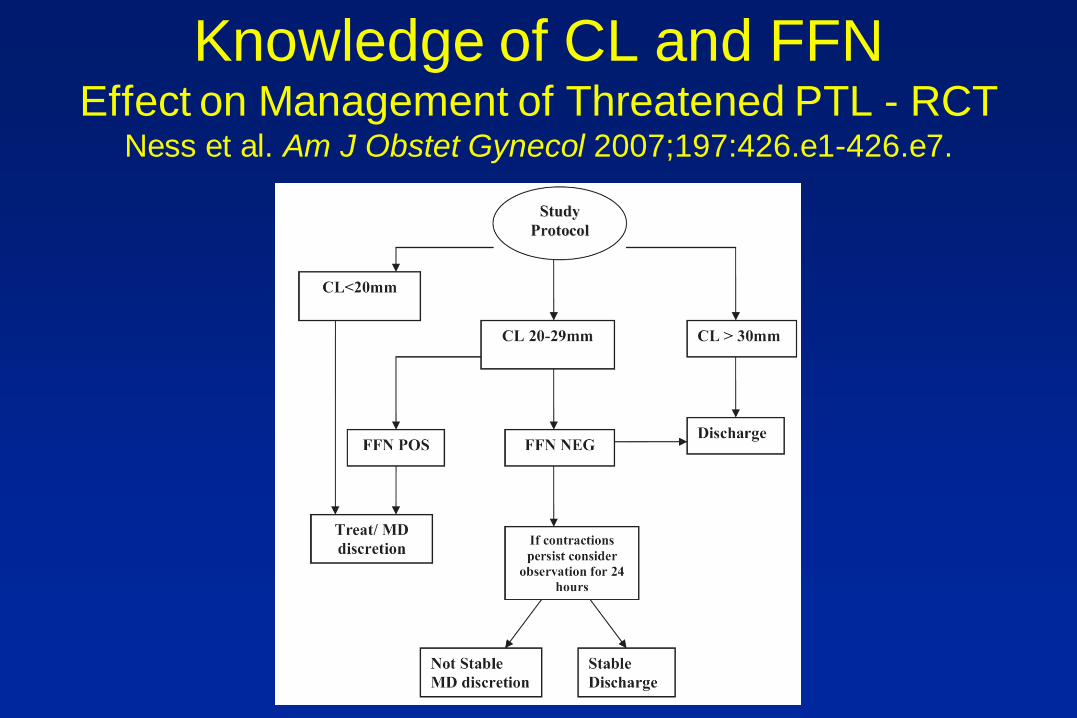
Knowledge of CL and FFN Effect on Management of Threatened PTL - RCT
Ness et al. Am J Obstet Gynecol 2007;197:426.e1-426.e7.

CL Assessment in Twins Systematic Review of Randomized Trials
Berghella et al. Cochrane Review 2013
PTB < 36 weeks

CL Assessment in Twins Systematic Review of Randomized Trials
Berghella et al. Cochrane Review 2013

Prevention
Prior to Labor

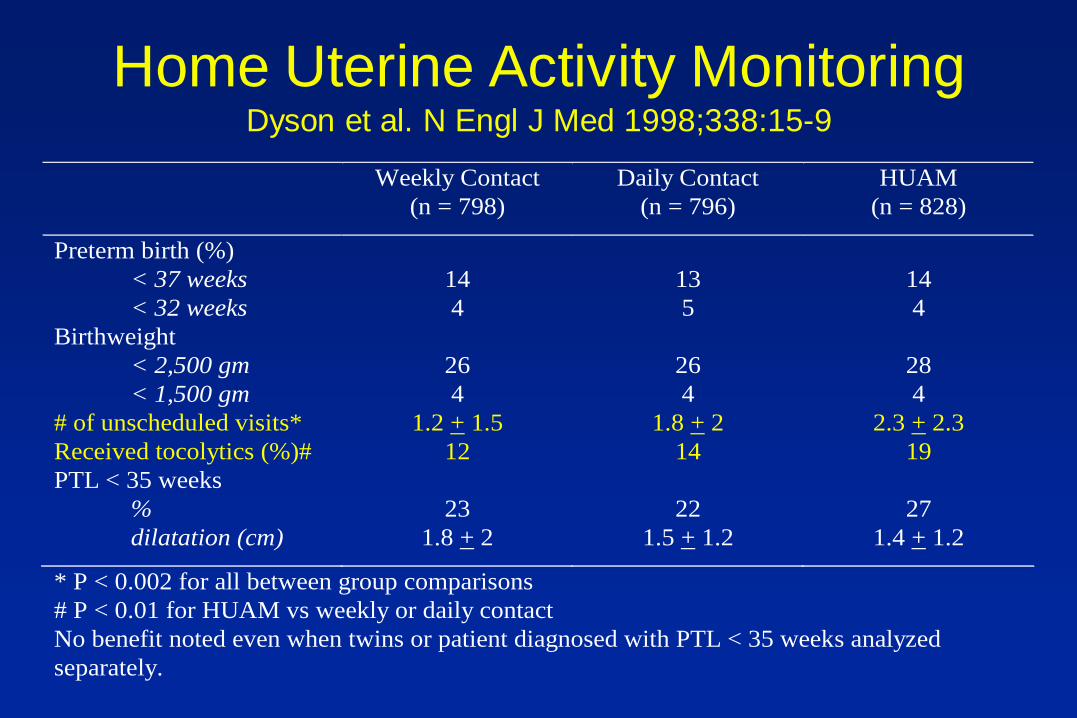
Home Uterine Activity Monitoring Dyson et al. N Engl J Med 1998;338:15-9
Weekly Contact
(n = 798)
Daily Contact
(n = 796)
HUAM
(n = 828)
Preterm birth (%)
< 37 weeks
< 32 weeks
14
4
13
5
14
4
Birthweight
< 2,500 gm
< 1,500 gm
26
4
26
4
28
4
# of unscheduled visits* 1.2 + 1.5 1.8 + 2 2.3 + 2.3
Received tocolytics (%)# 12 14 19
PTL < 35 weeks
%
dilatation (cm)
23
1.8 + 2
22
1.5 + 1.2
27
1.4 + 1.2
* P < 0.002 for all between group comparisons
# P < 0.01 for HUAM vs weekly or daily contact
No benefit noted even when twins or patient diagnosed with PTL < 35 weeks analyzed
separately.
Home Uterine Activity Monitoring Dyson et al. N Engl J Med 1998;338:15-9
Weekly Contact
(n = 798)
Daily Contact
(n = 796)
HUAM
(n = 828)
Preterm birth (%)
< 37 weeks
< 32 weeks
14
4
13
5
14
4
Birthweight
< 2,500 gm
< 1,500 gm
26
4
26
4
28
4
# of unscheduled visits* 1.2 + 1.5 1.8 + 2 2.3 + 2.3
Received tocolytics (%)# 12 14 19
PTL < 35 weeks
%
dilatation (cm)
23
1.8 + 2
22
1.5 + 1.2
27
1.4 + 1.2
* P < 0.002 for all between group comparisons
# P < 0.01 for HUAM vs weekly or daily contact
No benefit noted even when twins or patient diagnosed with PTL < 35 weeks analyzed
separately.

Hospitalization and Bed Rest for Multiples Systematic Review
Crowther. Cochrane Review 2010
Birth weight

Hospitalization and Bed Rest for Multiples Systematic Review
Crowther. Cochrane Review 2010
Delivery < 34 weeks

Hospitalization and Bed Rest for Multiples Systematic Review
Crowther. Cochrane Review 2010
Birth weigth < 2500 g

Hospitalization and Bed Rest for Multiples Systematic Review
Crowther. Cochrane Review 2010
No effect on other outcomes
No benefit in twins or triplets only
No benefit in asymptomatic women with
cervical dilatation

Oral Beta-mimetics for Twins Systematic Review
Yamasmit. Cochrane Review 2012
Delivery < 37 weeks

Cerclage for Short Cervix Berghella et al. Obstet Gynecol 2005;106:181-9

17P for Prevention of Recurrent PTB ACOG Committee Opinion. Nov 2003
Further studies needed for other high
risk factors
When used, restrict to documented
history of previous spontaneous birth
less than 37 weeks
Multiple gestation was an exclusion in
original trial

Progesterone for PTB Prevention in
Twins Systematic Review
Norman et al. Lancet 2009; 373: 2034–40

Higher Dose of Vaginal Progesterone RCT Serra et al. BJOG 2013;120:50-7.


Eligibility
Singleton or twin gestation
Gestational age between 20 and 25
weeks
Transvaginal sonographic cervical
length <15 mm
Asymptomatic (without signs or
symptoms of preterm labor or ROM)

Treatment
Daily vaginal capsules containing 200
mg micronized progesterone versus
placebo
From 24 to 33 6/7 weeks

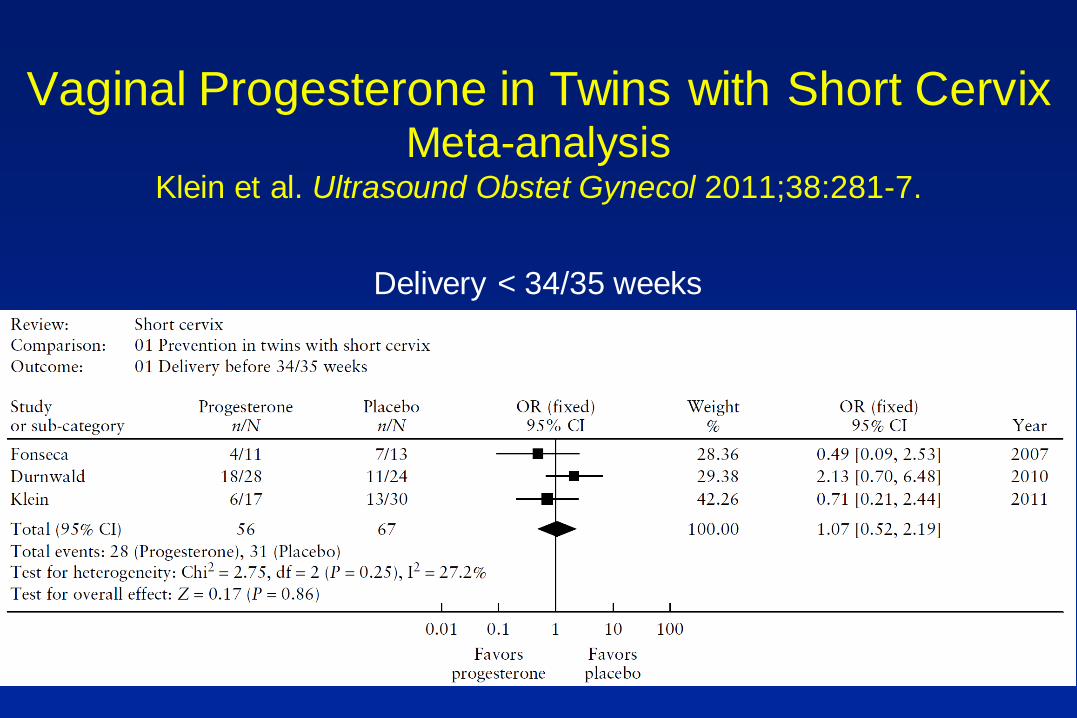
Vaginal Progesterone in Twins with Short Cervix Meta-analysis
Klein et al. Ultrasound Obstet Gynecol 2011;38:281-7.
Delivery < 34/35 weeks

IPD Meta-analysis of Vaginal Progesterone for
Asymptomatic Short Cervix Romero et al. Am J Obstet Gynecol 2012;206:124.e1-19
Singleton vs Twins

IPD Meta-analysis of Vaginal Progesterone for
Asymptomatic Short Cervix Romero et al. Am J Obstet Gynecol 2012;206:124.e1-19
Twins

17P (500 mg 2x/wk) in Twins with Short Cervix RCT
Senat et al. Am J Obstet Gynecol 2013;208:194.

Goya et al. Lancet 2012;379:1800-6

Pessary in Multiple Gestation RCT - Overall Result
Liem et al. Am J Obstet Gynecol 2013

Pessary in Multiple Gestation RCT – Subgroup CL < 25th%ile (38 mm)
Liem et al. Am J Obstet Gynecol 2013
PTB <32 wk
RR 0.43 (0.21-0.89)
NN morbidity
RR 0.41 (0.19-0.90)

MFMU Trial Study Design
Standard three-arm trial of women with twin
gestations and cervical shortening identified at
16-24 wk randomized to either:
1. Vaginal progesterone
2. Arabin pessary
3. Vaginal placebo
Twin Management in MFMU Sites (N=21)
Routine CL screening
– 11 sites assess CL in most twins
Definition of short CL
– Varies from 15 – 30 mm; 25 mm
Progesterone
– 5 sites offer vaginal progesterone for short CL; others individualize
Pessary
– Used only at 2 sites

Prevention Prior to Labor Recommendations
Testing and treatment for asymptomatic
bacteriuria
Testing and oral treatment (5 – 7 days)
for abnormal vaginal flora in
asymptomatic at-risk women
No CL screening
Vaginal progesterone if find cervix <20
mm before 24 weeks


Prevention
Symptomatic

Hydration for PTL Effect on Delivery <37 wks
Boulvain et al. The Cochrane Library 2003

Hydration for PTL Effect on Use of Tocolytics
Boulvain et al. The Cochrane Library 2003
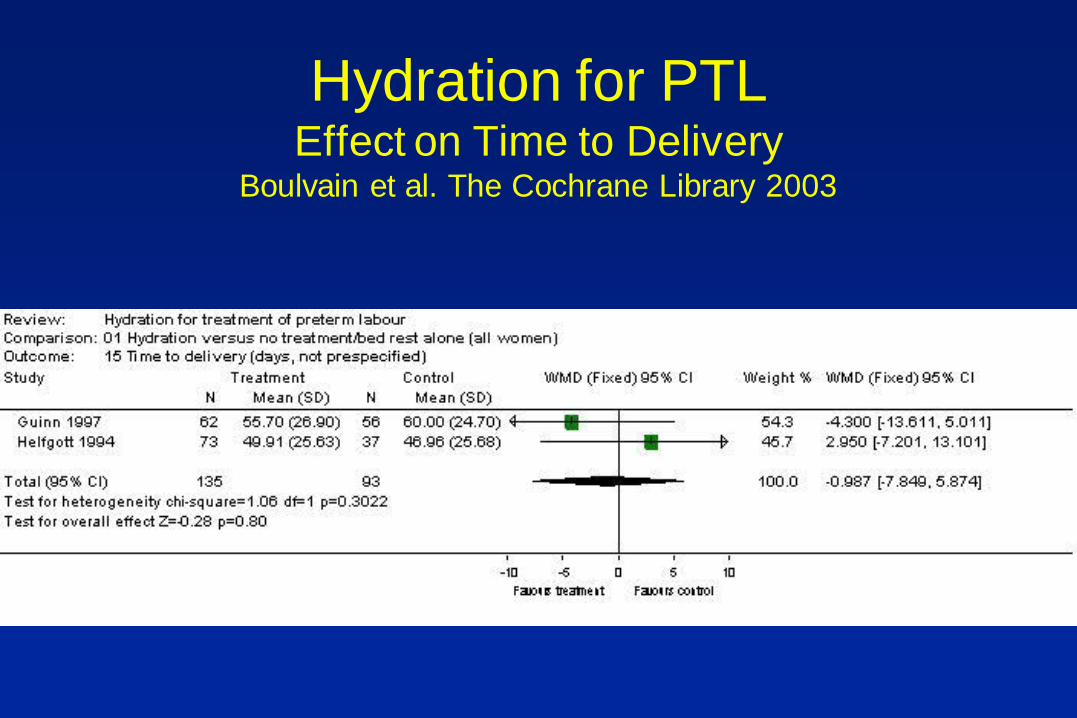
Hydration for PTL Effect on Time to Delivery
Boulvain et al. The Cochrane Library 2003
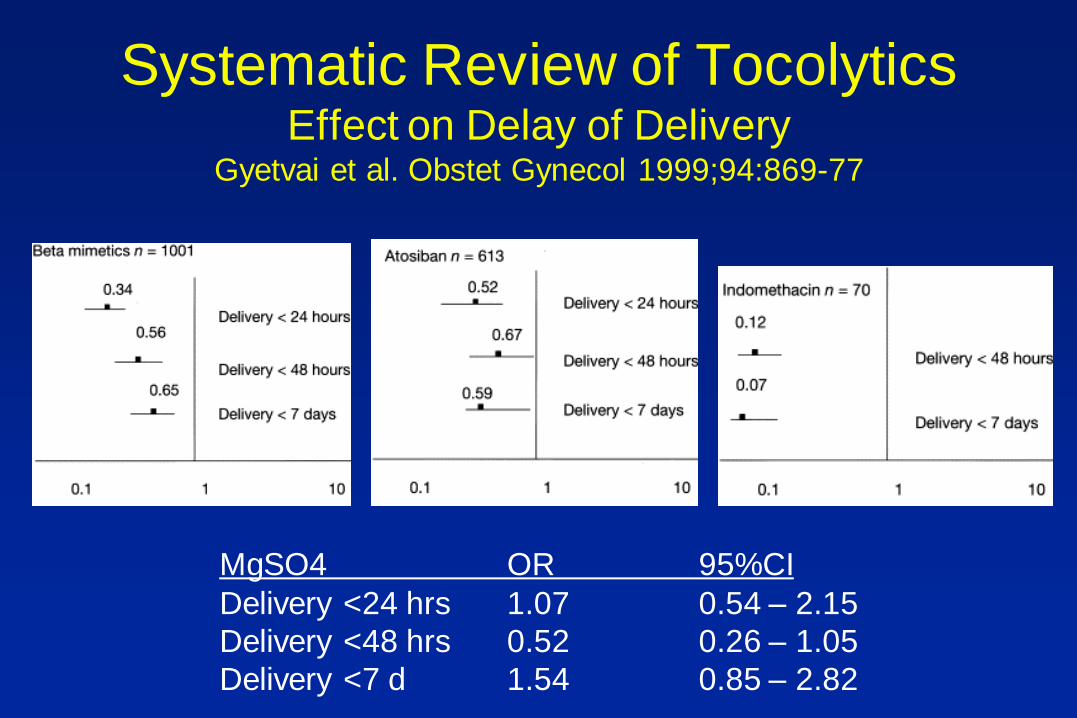
Systematic Review of Tocolytics Effect on Delay of Delivery
Gyetvai et al. Obstet Gynecol 1999;94:869-77
MgSO4 OR 95%CI
Delivery <24 hrs 1.07 0.54 – 2.15
Delivery <48 hrs 0.52 0.26 – 1.05
Delivery <7 d 1.54 0.85 – 2.82

Nifedipine vs -mimetics Meta-Analysis
Tsatsaris et al. Obstet Gynecol 2001;97:840-7
Effect on # of patients OR 95% CI
Delay >48 hrs
Interruption of Rx
RDS
Admission to NICU
Neonatal death
520
590
497
493
651
1.52
0.12
0.57
0.65
1.51
1.03 – 2.24
0.05 – 0.29
0.37 – 0.89
0.43 – 0.97
0.63 – 3.65

Systematic Review of Tocolytics Maternal Harm
Berkman et al. Am J Obstet Gynecol 2003;188:1648-59
-mimetics Ca-channel
blockers
Magnesium Atosiban Placebo

Systematic Review of Tocolytics Effect on Perinatal and Neonatal Outcome
Gyetvai et al. Obstet Gynecol 1999;94:869-77
Berkman et al. Am J Obstet Gynecol 2003;188:1648-59
None shown to improve perinatal or
neonatal outcome

Maintenance Tocolysis Meta-Analysis
Sanchez-Ramos et al. Am J Obstet Gynecol 1999;181:484-90
Effect on # of patients OR 95% CI
Preterm Delivery
Recurrent PTL
RDS
IVH
NEC
Admission to NICU
Perinatal death
1498
1491
1273
1119
1001
861
1393
0.95
0.81
1.06
1.36
1.90
1.03
1.73
0.77 – 1.17
0.64 – 1.03
0.72 – 1.55
0.70 – 2.64
0.64 – 5.61
0.75 – 1.42
0.80 – 3.72

Maintenance with Beta-mimetics Effect on SPTB <37 weeks
Honest H et al. Health Technol Assess 2009;13(43)
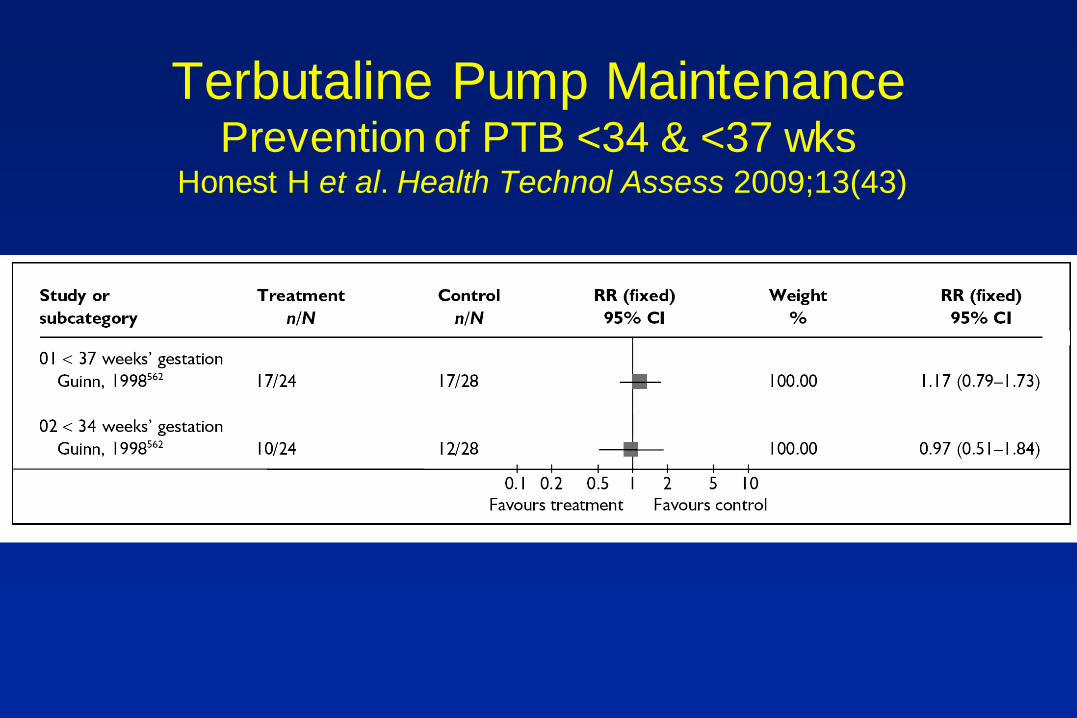
Terbutaline Pump Maintenance Prevention of PTB <34 & <37 wks
Honest H et al. Health Technol Assess 2009;13(43)

Maintenance Ca Channel Blockers Effect on PTB <37 wks
Honest H et al. Health Technol Assess 2009;13(43)

RCOG Clinical Guideline Grade A Recommendations
No. 1(B), October 2002
It is reasonable not to use tocolysis
Tocolysis should be used if few days
gained would be put to good use
Ritodrine no longer best choice
Atosiban or nifedipine preferable
Maintenance tocolysis not
recommended for routine practice

Indomethacin vs Nifedipine Author Agent N Percent undelivered
48 hours 7 days
Gyetvai12- 3 studies Indomethacin 49 88 83
Morales4 Indomethacin 49 90
Besinger34 Indomethacin 22 83 67
King29- 1-2 studies Indomethacin 34 88.2 67.6
Total 88.0 (N= 154) 74.6 (N=105)
Lyell3 Nifedipine 100 92
Cararach42 Nifedipine 39 76.9 66.7
Weerakul43 Nifedipine 45 68.8
Tsatsaris44- 9 studies Nifedipine 268 75.3
King20- 4-9 studies Ca Channel blocker 383 80.7 69.0
Total 79.5 (N=835) 68.8 (N=422)

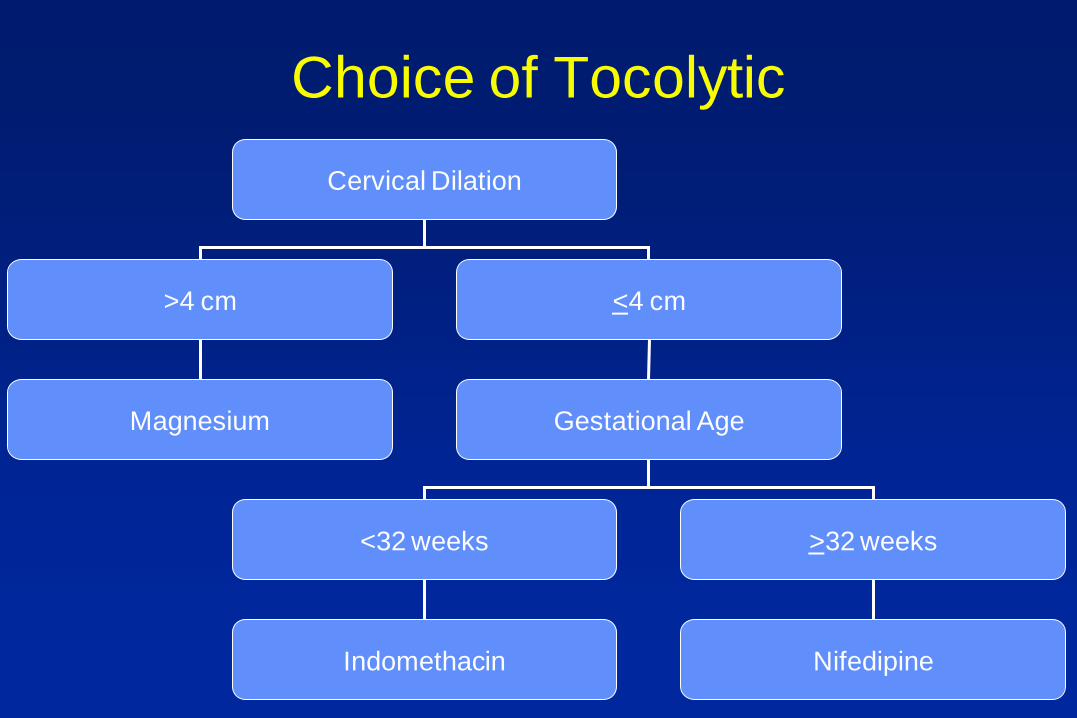
Choice of Tocolytic
Cervical Dilation
>4 cm <4 cm
Magnesium Gestational Age
<32 weeks >32 weeks
Indomethacin Nifedipine

Choice of Tocolytic
Cervical Dilation
>4 cm <4 cm
Magnesium Gestational Age
<32 weeks >32 weeks
Indomethacin Nifedipine

Choice of Tocolytic
Cervical Dilation
>4 cm <4 cm
Magnesium Gestational Age
<32 weeks >32 weeks
Indomethacin Nifedipine

Choice of Tocolytic
Cervical Dilation
>4 cm <4 cm
Magnesium Gestational Age
<32 weeks >32 weeks
Indomethacin Nifedipine
Choice of Tocolytic
Cervical Dilation
>4 cm <4 cm
Magnesium Gestational Age
<32 weeks >32 weeks
Indomethacin Nifedipine
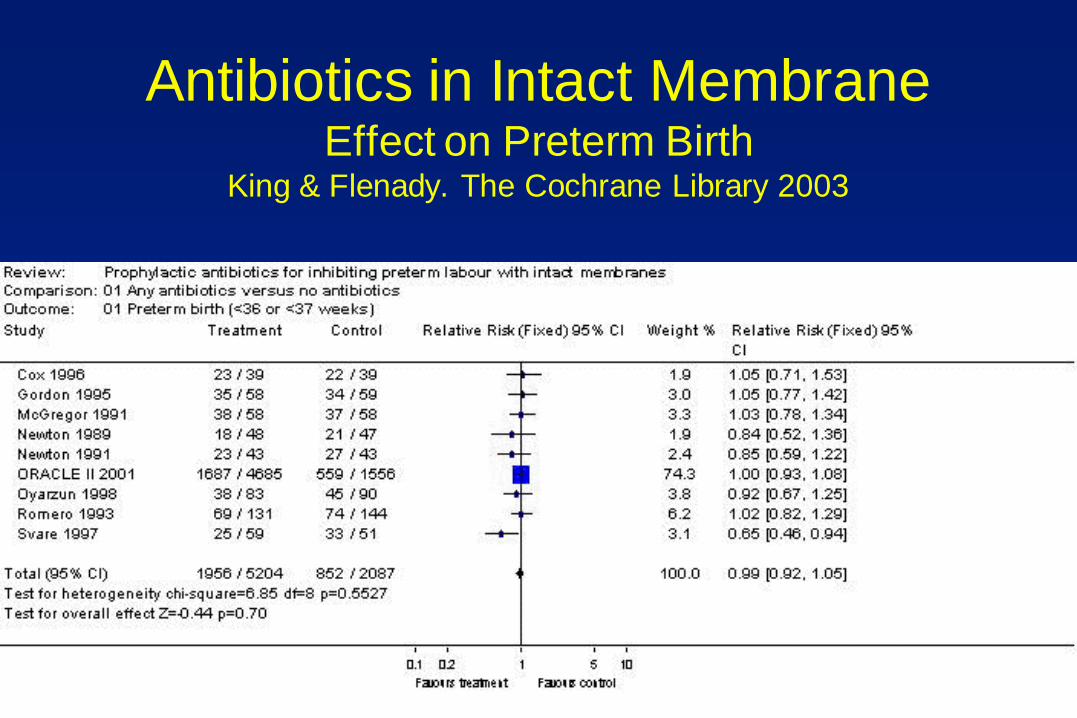
Antibiotics in Intact Membrane Effect on Preterm Birth
King & Flenady. The Cochrane Library 2003

Antibiotics in Intact Membrane Effect on Delivery <48 hrs or <7 d King & Flenady. The Cochrane Library 2003

Antibiotics in Intact Membrane Effect on Neonatal Sepsis
King & Flenady. The Cochrane Library 2003
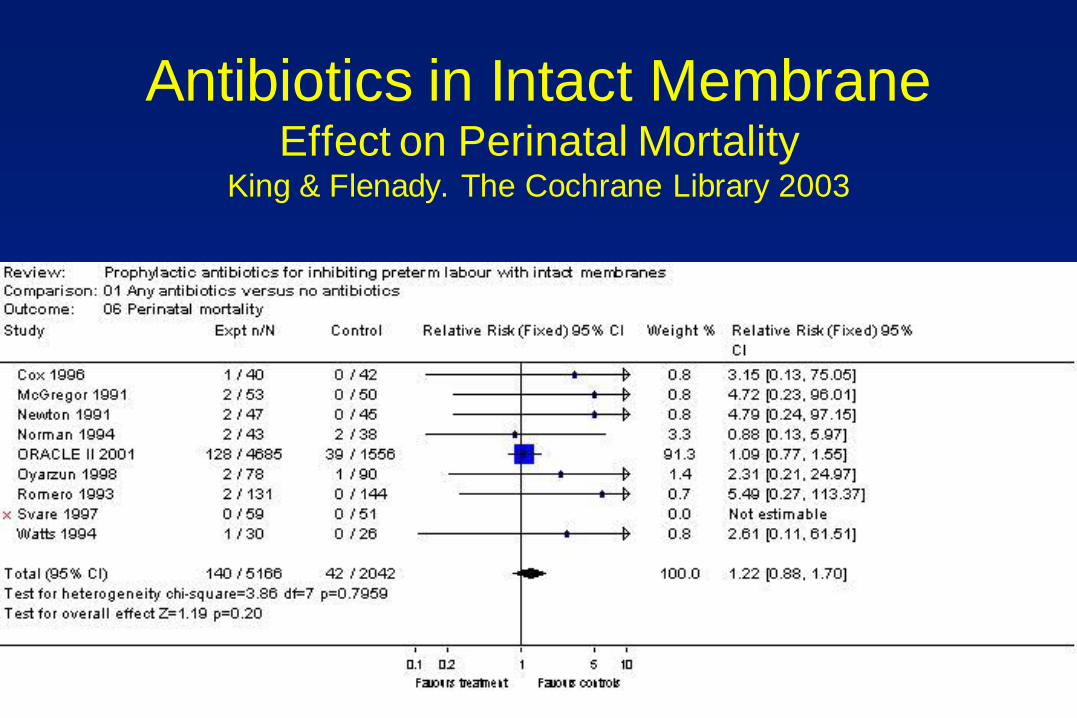
Antibiotics in Intact Membrane Effect on Perinatal Mortality
King & Flenady. The Cochrane Library 2003

7 Year Follow up
of ORACLE II Kenyon et al. Lancet 2008;372:1319–27

Antibiotics in pPROM Effect on Major Cerebral Abnormality
Kenyon et al. The Cochrane Library 2003

Co-amoxiclav in pPROM Effect on Incidence of NEC
Kenyon et al. The Cochrane Library 2003
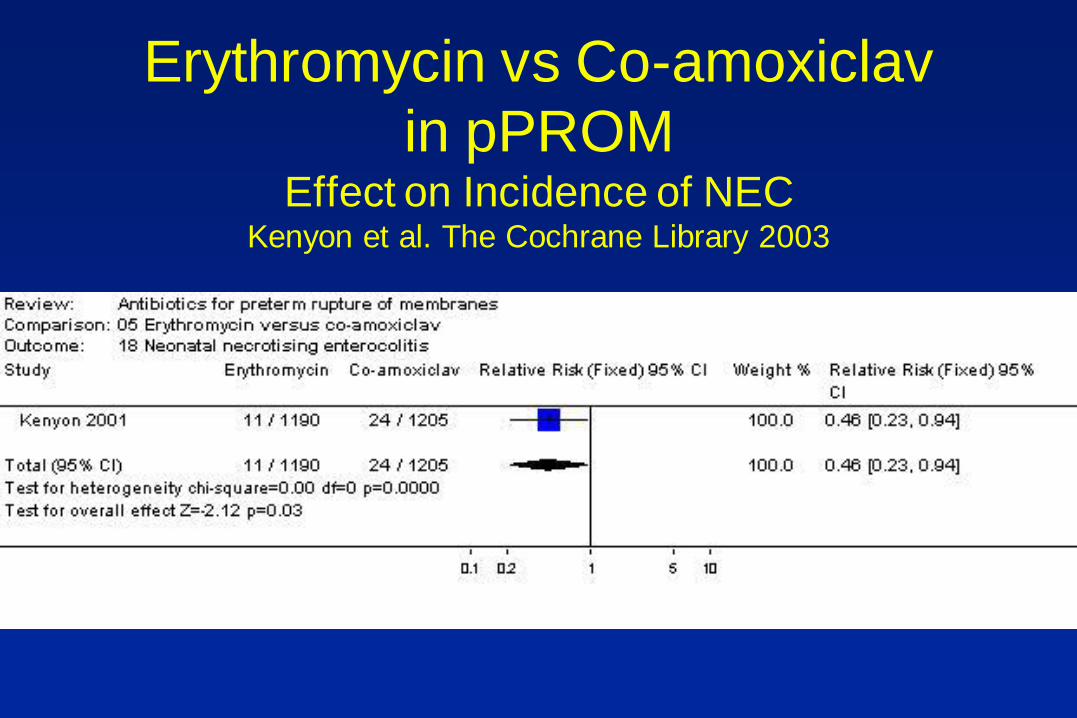
Erythromycin vs Co-amoxiclav
in pPROM Effect on Incidence of NEC
Kenyon et al. The Cochrane Library 2003
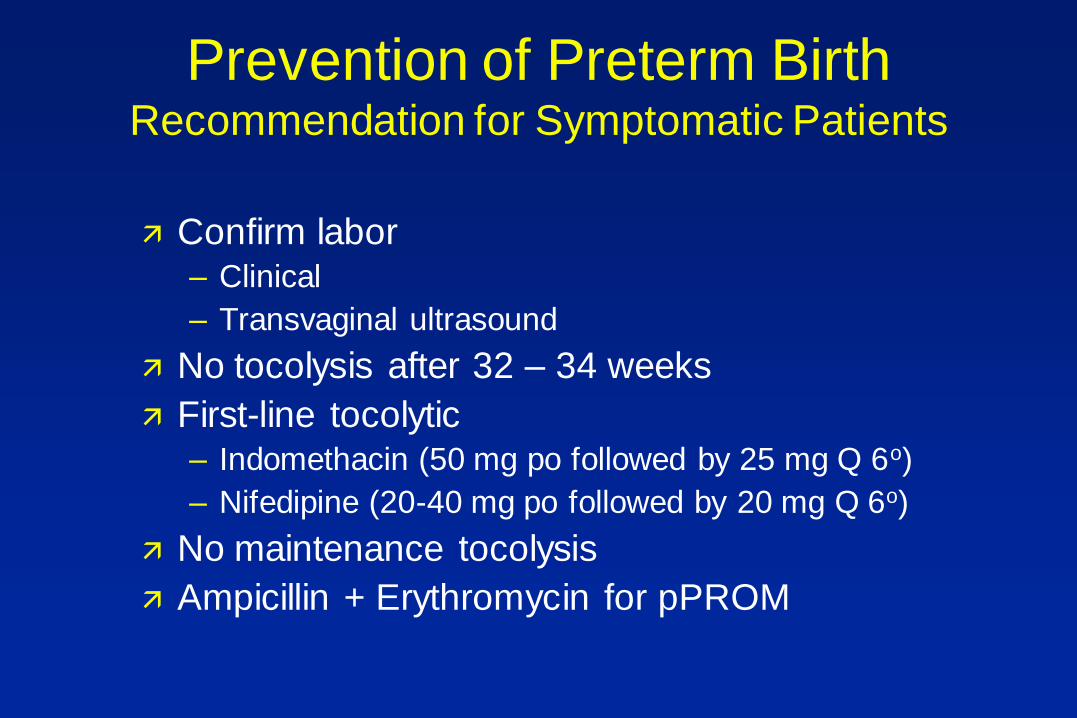
Prevention of Preterm Birth Recommendation for Symptomatic Patients
Confirm labor – Clinical
– Transvaginal ultrasound
No tocolysis after 32 – 34 weeks
First-line tocolytic – Indomethacin (50 mg po followed by 25 mg Q 6o)
– Nifedipine (20-40 mg po followed by 20 mg Q 6o)
No maintenance tocolysis
Ampicillin + Erythromycin for pPROM

Interventions to Improve Neonatal
Outcome

Magnesium for Fetal
Neuroprotection

Observational Studies Nelson & Grether. Pediatrics 1995;95:263-269

Randomized Controlled Trials
Intent for neuroprotection
– MagNET Mittendorf et al. Lancet 1997;350:1517-8.
– ACTOMgSO4 Crowther et al. JAMA 2003;290:2669-76.
– PreMag Marret et al. Br J Obstet Gynecol 2007;114:310-8.
– BEAM Rouse et al. 2008.
Other Intent
– MAGPIE Br J Obstet Gynecol 2007;114:289-99.

Meta-analysis of all RCT CP or Death
Costantine et al. Obstet Gynecol 2009;114:354–64

Meta-analysis of all RCT Any CP
Costantine et al. Obstet Gynecol 2009;114:354–64

Meta-analysis of all RCT Death or Moderate-Severe CP
Costantine et al. Obstet Gynecol 2009;114:354–64
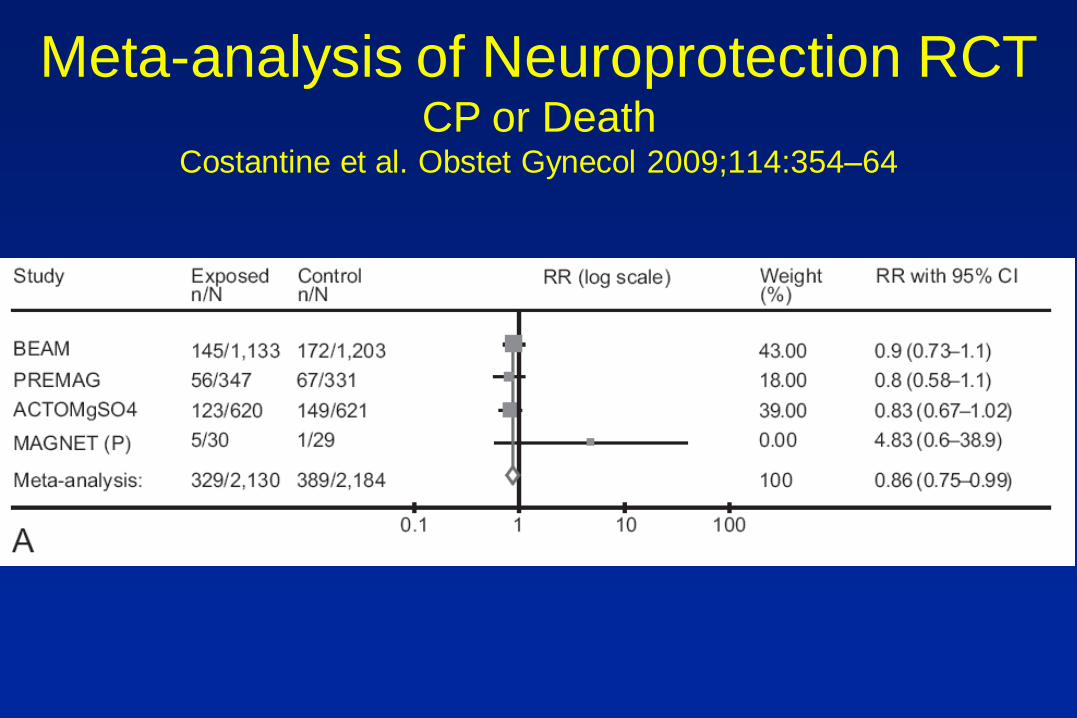
Meta-analysis of Neuroprotection RCT CP or Death
Costantine et al. Obstet Gynecol 2009;114:354–64

Considerations
To prevent one case of cerebral palsy
– Treat 56 (overall)
– Treat 46 (<30 weeks)
To prevent one eclamptic convulsion
– Treat 71 with severe disease
– Treat 400 with mild disease

Conclusions
Not a tocolytic
Use for imminent delivery (within 24 hrs)
or pPROM
Limit to less than 32 weeks (best less
than 28 weeks)
Caution

UTMB Protocol Indications
Likely delivery within 2- 24 hours at 23-32 weeks with patient not candidate for tocolysis. Examples of such cases
– PPROM at 23 to 32 weeks
– Preterm labor at 24-32 weeks with cervix between 4 and 8 cm dilatation
– Severe IUGR (with abnormal Doppler) requiring delivery
– Abnormal Testing (Late, REDF, etc) requiring delivery within 24 hours
– Chorioamnionitis requiring delivery

UTMB Protocol Exclusions
– Imminent delivery within < 2 hours
– Cervix > 8 cm
– PPROM < 23 weeks or > 32 weeks gestation
– Preeclampsia / Eclampsia on Mag
– Prior magnesium sulfate therapy within 12 hours
– Major fetal anomalies
– Delay delivery deemed detrimental to mom
• Severe preeclampsia with unstable HELLP
• Maternal respiratory compromise
• Cardiac arrest or heart Block
• Severe bleeding requiring immediate delivery

UTMB Protocol Exclusions
– Expedited delivery is required or delayed delivery
deemed detrimental to fetus
• Unstable abruption- bleeding
• Fetal distress- Category III
• Unstable previa
• Prolapsed umbilical cord
– Maternal contraindication to magnesium sulfate
• Myasthenia gravis
• Pulmonary hypertension
• Cardiac diseases (Class II-IV)
• Severe acute pulmonary dz- pneumonia, acute
asthma, ARDS, edema
• Serum creatinine > 1 mg/dL

UTMB Protocol Administration
• Dose- 6 gm loading then 2 gm/hour (40 gm of magnesium
sulfate in 500 cc of NS)
• Duration of treatment- until delivery or 12 hours whichever
comes first then discontinued.
• Resume treatment if still less than 32 weeks and delivery
deemed likely
– If < 6 hours since discontinuation of magnesium sulfate, restart
infusion at 2 gm/hour
– If > 6 hours since discontinuation of magnesium sulfate, load with 6
gm then 2 gm/hour
– Do not retreat if it will delay delivery that is detrimental to mom or
fetus
• Once on magnesium for neuroprotection, do not use any
tocolytic agents. These patients are not candidate for
tocolysis

Thank you