december 2012 oncology fellows
DESCRIPTION
Oncology Fellows features articles writtenby practicing physicians, clinical instructors,researchers, and current fellows who sharetheir knowledge, advice, and insights on arange of issues.TRANSCRIPT

The ABCs of IRBs:A Brief Overview
Achieving Career Success in Academic Oncology
Volume 4 • Issue 4, December 2012
This edition is supported by
BIO0001466501
f e l l o w s
Canine CaringA therapy dog for cancer patients

FREE, personal websites for cancer patients, survivors, and their caregivers.
Get started with just a few clicks!
www.MyLifeLine.org
MyLifeLine has been an absolute blessing for me and my family. It’s a great way to keep so many people that want to know how I am in the process.
– Kimberly, 31 years old Infiltrating Ductal Carcinoma Grade 2
“
”
Thank you for providing this incredible resource. It has really helped us immensely!
– Benny, diagnosed age 52 Squamous cell carcinoma
“
”

Interested in contributing to Oncology Fellows? If you’d like to submit an article for consideration in an upcoming issue, please e-mail Donna Bonura at [email protected].
Canine Caring: A therapy dog for cancer patientsBy Brendan Curley, DO, MPHOncology fellow Brendan Curley, DO, MPH and his therapy dog Princess Danger Curley positively impact the lives of patients and their families, sometimes more than expected.
Table of Contents
2
8 The ABCs of IRBs: A Brief OverviewBy Nancy Fell Hill, MPHUnderstanding the Institutional Review Board (IRB) and its process for review and approval of research proposals.
Volume 4 • Issue 4, December 2012
Feature
A Word From Your Fellows 14 Bone Marrow Biopsy Simulation Training for FellowsBy Cyrus Khan, MD and Ghulam Rehman MohyuddinInstitutions are beginning to develop a model program that teaches fellows correct procedural techniques for performing a bone marrow aspirate and biopsy.
16 How do I keep up with the literature?By Amer M. ZeidanStrategies and resources to keep fellows current on the stream of published literature while balancing their clinical duties and research activities.
Transitions18 Achieving Career Success in Academic Oncology:What to know when deciding on a career in academiaBy Mohammed Almubarak, MD, and Jame Abraham, MD, FACPPractical advice for oncologists contemplating a career in academia.
The Online Oncologist 22 Mobile MedicineApps for the health care professional.
23 By the Numbers
24 Conference Center
Departments
President
Peter [email protected]
Editorial & Production
Senior Vice President, Clinical and Scientific AffairsJeff D. Prescott, PharmD, RPh Project DirectorDonna Bonura
Project Manager Jaclyn Pallotti
Editor Elizabeth McDonald
Assistant Editor Jeanne Linke Quality Assurance Editor David Allikas
Art DirectorRay Pelesko
Sales & Marketing
Vice President, Sales & MarketingLisa [email protected]
Director of SalesScott [email protected]
Digital Media
Vice President, Digital MediaJung Kim
Director,Digital ContentSean Johnson
Operations & Finance
Group Director, Circulation and ProductionJohn [email protected]
Director of OperationsThomas J. Kanzler
ControllerJonathan Fisher, CPA
Assistant ControllerLeah Babitz, CPA
Corporate
Chairman/Chief Executive Officer/PresidentMike Hennessy
Chief Operating OfficerTighe Blazier
Chief Financial OfficerNeil Glasser, CPA/CFE
Executive Vice President/Executive Director of EducationJudy V. Lum, MPA
Vice President, Group Creative DirectorJeff Brown
www.TargetedHC.com
f e l l o w s
Office Center at Princeton MeadowsBldg. 300 • Plainsboro, NJ 08536(609) 716-7777
HealthcareCommunications
Targeted
Canine CaringA therapy dog for cancer patients
By Brendan Curley, DO, MPH
Feature
2 | December 2012

December 2012 | 3
I wear 2 hats in the hospital. First, I am a hematology/oncology fellow. In this role, I am responsible for seeing consults,
primary patients, and patients in clinic. There are hundreds of other heme/onc fellows around the country, all doing the same things that I do. My second hat is my more unusual one; I am also a registered therapy dog handler.
During my residency, one of our rotations was in a community hospital away from the inner city university where I did most of my training. At this community hospital, I was first introduced to therapy dogs. At the time, I had no experience with therapy
dogs and really didn’t know anything about them. These dogs are normal house pets that do extraordinary things. To work as a therapy dog, the animals must be older than 1 year and have exceptional manners and behavior. Their job is simple: to provide joy and smiles. One day, a therapy dog may have an entire nursing unit doting over him; the next may be spent with a very sick patient and her family. Another day, a therapy dog and his handler provided answers to questions about “How is this dog here”…questions from me, a resident near the end of a 30-hour shift.
I have always had a dog in my life. While I was growing up, my family had
many different kinds of dogs in our home: Golden Retrievers, Irish Setters, Newfoundlands, and Chow Chows. Once I was in college, then medical school, I had little time to raise and care for a puppy. That didn’t stop me from dreaming, though. I knew that an English bulldog would soon be my pet. I also knew that I could not raise one alone. I was lucky that my future wife Anjaly fell in love with bulldogs as well. Our engagement consisted of her receiving a beautiful diamond, and her present to me was my first dog of my own, an English bulldog puppy we named Princess Danger Curley.
Princess Danger was never intended to be a therapy dog. She came into
Brendan Curley, DO, MPH, with Princess Danger Curley

4 | December 2012
our home as a pet, a goofball who immediately stole our hearts. The funny thing is that she not only stole our hearts, but that of anyone who met her. She would roll on her back and kiss faces, and was a sweetheart to everyone she met. She left us no choice in the matter—she was clearly born to be a therapy dog! Waiting until she was a year old seemed like overkill, since she was ready at 8 months. Within a month of her first birthday, we scheduled her session to become certified. After 3 sessions, we had our own certified therapy dog.
We didn’t start small. We applied for her to be one of HUP’s Pups at the Hospital of the University of Pennsylvania (HUP). Her certification and vaccine reports were a start, but were not enough for HUP. She under- went a full veterinary examination and passed with flying colors. Her next test was with a veterinary behavioral psychologist, the final test prior to her entering the hospital. We were not surprised that she did not disappoint. She had her ID card picture taken the very next day. She was now a hospital therapy dog with patients to see.
The first day we took her to the hospital, my nerves were on edge. I was entering not as a doctor, not as a patient, but as a handler. My sole responsibility was to make sure
that my dog was well behaved and appropriate. Her first assignment was the Surgical Intensive Care Unit (SICU) where the head of the therapy dog program walked us through the unit. She gave her love to the nurses’ station and proceeded to see patients. She did this for months, approximately once a week. Her visits lasted between 90 minutes and 2 hours (which is standard for therapy dog visits). Patients laughed, cried, and told me about their dogs. Danger smiled, rolled around, and loved every moment of the scratching and attention she received. She was a rock star at HUP, but we were both leaving to a new city and job at West Virginia University (WVU).
I started my hematology/oncology fellowship at WVU and immediately loved what I was doing. Oncology was truly my calling, and each day that
passed showed me that I had made the right decision. Therapy dogs were conspicuously absent at WVU and Princess Danger was the perfect dog to fill that role. She started as a visitor, and soon turned herself into a regular at the cancer center. She first won over the nurses, followed by the staff and patients. She makes both outpatient and inpatient visits at the clinic and hospital, and some of her best work is with those receiving chemotherapy. Chemotherapy visits are typically outpatient (but can sometimes be inpatient) and can last many hours over months, even weeks. These patients love seeing her, as her visit is a bright spot during their time at the cancer center or in the hospital. She has made countless people laugh, smile, and some cry, but there is one experience that I will never forget.
Princess was making her rounds on the oncology floor as usual, when a nurse asked if she could come see a dying patient. He had a very aggressive form of leukemia that he had fought valiantly, but he had lost the battle. He was on comfort measures, being given only medications to make his last days of life as comfortable as possible. He was much younger than his sunken eyes showed, as I was able to tell by his young wife and high-school-aged daughter. They were obviously having such a tough time with his imminent death. I thought about how hard it must be for him and his wife. They had spent 18 years raising their daughter,
Feature
She left us no choice in the matter—she was clearly born to be a therapy dog!

Connect with PER on facebook
Don’t miss out on all the latest developments from our oncology conferences!
facebook.com/gotoPER
Friend us on facebook and recieve a discount to an upcoming meeting.
Feature
and now he was dying as she was about to become an adult, and her mom would be left alone.
Princess entered the room with her normal amount of energy. The patient could barely move, and each breath caused him pain. His daughter and wife were at his bedside, and the true therapy began. My 40-pound love bug hopped in their laps and cuddled up like she hadn’t done before. She knew they needed it, and they truly latched onto her. We stayed for almost 2 hours. They talked about their loved one, but were mainly distracted by Princess Danger. She showered them with love and affection, and moved them both to tears. I knew she truly made a difference, but I didn’t yet know how much she had done to change their lives.
I started taking care of the unfortunate gentlemen as a patient the next day, caring for him and his family. His wife never left his side. His
daughter was gone for the day, but I didn’t ask where she was. I can’t really imagine the level of emotion she was going through, losing her father at only 18. The next day I was in the physician workroom when a nurse asked me urgently to come to the unit. Usually this means that someone is gravely ill and needs immediate attention. That day, that was not why I was called. In the hallway, I found a bouncing, happy, 12-week-old English bulldog puppy, freshly picked out by the patient’s daughter the day she was not in the hospital. She was so happy to have her own little bundle of love, and that puppy picked up the staff’s morale that day. I spoke with the patient’s wife; she couldn’t say no to a puppy at that point. She told me that the dog was helping them get through the hardest days of their lives.
The patient died the day after the puppy joined their family. He passed
peacefully, surrounded by his family. I was at his bedside and let them know that he had died, and their emotions came pouring out. The family left that day broken, their husband and father taken from them prematurely and unfairly. Cancer is not a fair disease, especially when it relentlessly attacks the young and innocent. We did everything we could to save his life, and in the end we could not succeed. However, Princess Danger had changed their lives forever. I am sure that when they look in the eyes of their dog, they will not only see their lost loved one, but will always remember the day my therapy dog changed their lives. ■
Brendan Curley, DO, MPH, is a hematology/oncology fellow at the West Virginia University School of Medicine, Mary Babb Randolph Cancer Center, Morgantown, WV.
Natio
nal C
ance
r Ins
titut
e
Your source for information on clinical trials atNCI’s Center for Cancer Research (CCR) is
now smartphone friendly. Visit our easy-to-navigatemobile Web site for information on the more than150 cancer clinical trials now enrolling at the NationalInstitutes of Health in Bethesda,MD.
CCR is currently conducting trials for many typesof cancer including:
• Prostate Cancer • Lung Cancer•Thymoma • Pediatric Sarcoma• Kidney Cancer • Brain Cancer
To learn whether your patients may be eligible,visit
bethesdatrials.cancer.gov or call
1-888-NCI-1937 (1-888-624-1937)
41594-NIH CSSC Oncology Net Ad-v5 8/4/10 2:53 PM Page 1

This space provided as a public service.©2010 Susan G. Komen for the Cure® The Running Ribbon is a registered trademark of Susan G. Komen for the Cure.
But scientifi c minds cannot solve breast cancer alone. Susan G.
Komen for the Cure®, the leader of the global breast cancer movement, is leading in science
again. We’ve just tapped 50 of the world’s top cancer experts to Komen’s new Scientifi c
Advisory Council, to drive innovation and breakthroughs in cancer research. We think of it as
the Ultimate Cancer Think Tank.
We’re also supplying the tools that will help global researchers unlock the secrets of breast
cancer. How it begins and grows. How we can stop it in its tracks. The answers may lie in the
Susan G. Komen for the Cure Tissue Bank at the Indiana University Melvin and Bren Simon
Cancer Center -- the largest source of healthy breast tissue in the world, soon to be available
digitally to researchers around the world over the Internet.
Make an impact and donate today. Visit komen.org/donations.
to fi nd the cures.
It takesIt takes
to fi nd the cures.NNOVATION
Komen Tissue Bank volunteer and Purdue University graduate student, Rebecca Fega, helps process breast tissue samples November 2009 in West Lafayette, Ind.

Feature
8 | December 2012
The ABCs of IRBs:A Brief OverviewBy Nancy Fell Hill, MPH

December 2012 | 9
An Abbreviated HistoryThe mandate for IRBs in the United States is a result of notorious human experiments performed over the last century. The horrific Nazi experiments during World War II involved physi-cians overseeing research on: the effects of drinking sea water; human experiments with spreading diseases such as hepatitis, typhus, and malaria; cold immersion studies; and, human sterilization experiments. Sadly, irre- sponsible studies were carried out in the United States as well, including the Willowbrook Hepatitis Studies, Milgram Studies of Obedience, and the Tuskegee Syphilis Study.
In short, these types of research prompted the current US system of protection in human subject research. The ethical standards for the conduct of human subject research are codified in several federal regulations, includ-ing 45CFR46 and 21 CFR Parts 50 & 56. The IRB serves an integral part in the system of protection by upholding these standards.
The Role of the IRBThe IRB has the authority to approve, require modifications to, or disapprove a research activity. Each IRB is com-posed of at least 5 members from vari-ous disciplines, at least one of whom is a non-scientist. Some institutions have multiple IRBs, depending on the number of research proposals to be reviewed.
According to 45CFR46.111, in order to approve a research proposal the IRB must determine that each of the follow-ing requirements is satisfied:
• Risks to subjects are minimized: o By using procedures that are
consistent with sound research design and do not unnecessarily expose subjects to risk.
o Whenever appropriate, by using procedures already being per-formed on subjects for diagnostic or treatment purposes.
• Risks to subjects are reasonable in relation to anticipated benefits, if any, to subjects and the importance of the knowledge that may reason-ably be expected to result. In evalu-ating risks and benefits, the IRB considers only those risks and ben-efits that may result from the re-search (as distinguished from risks and benefits of therapies subjects would receive even if not participat-ing in the research).
• Selection of subjects is equitable. In making this assessment the IRB takes into account the purposes of the research and the setting in which the research will be conducted.
• Informed consent will be sought from each prospective subject or the subject’s legally authorized repre-sentative.
At some point in their careers, most oncologists will need to submit a research proposal to their hospital’s Institutional Review Board (IRB). Too many physicians view the IRB process as an additional bureaucratic burden in their already overloaded daily schedules. In reality, these boards serve an extremely important purpose: protecting human subjects who choose to participate in research.
Since most medical schools do not provide information regarding IRBs in their curriculum, many oncology fellows may not have a basic understanding of IRBs or what they do. This article provides a brief overview of IRBs and outlines pertinent resources for fellows who conduct or may contribute to human research studies.
• Informed consent will be appropri-ately documented, typically with a signed consent form.
• When appropriate, the research plan makes adequate provision for moni-toring the data collected to ensure the safety of subjects.
• When appropriate, there are ade- quate provisions to protect the pri-vacy of subjects and to maintain the confidentiality of data.
• When some or all of the subjects are likely to be vulnerable to coercion or undue influence, additional safe-guards are included in the study.
Is This Project Human Research?This is a question often asked by clini-cians and investigators. At times there is an affirmative and straightforward answer, such as in the case of drug trials designed to determine the effec-tiveness of a new pharmaceutical for-mulation in treating a certain illness. But at other times, the answer is not as immediately apparent.
The federal regulations define research as “a systematic investiga-tion, including research development, testing and evaluation, designed to develop or contribute to generalizable knowledge.”[45CFR46.102(d)] A hu-man subject is defined as “a living in-dividual about whom an investigator (whether professional or student) con-ducting research obtains data through intervention or interaction with the individual, or identifiable private in-formation.” [45CFR46.102(f)]
There are a lot of grey areas here. If you have any questions regarding whether a project you are planning to implement is considered human re-search, you should address them to your local IRB office. They will likely require some written documentation from you to consider the question. The details vary by site, but you may be asked to submit a written protocol and/or an application; this varies by site.
Types of IRB ReviewThere are 3 types of IRB review cat-egories:
• Full Board Review This type of review is conducted for studies that entail greater than minimal risk to subjects. It is car-ried out by a fully convened IRB committee. According to federal regulation, minimal risk means that “The probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests.” [45CFR26.102(f)]
• Expedited Review This type of review is for studies that involve minimal risk to sub-jects. The review is performed by the IRB chair or an experienced designee. One example is a project that collects biological specimens for research purposes via noninvasive means (such as hair and nail clip-pings in a non-disfiguring manner). The Department of Health and Hu-man Services (DHHS) Office for Hu-man Research Protections (OHRP) has a list of activities that fall under the category of minimal risk. Please note that use of the term “expedited” does not necessarily translate into a speedier review by the IRB.
• Exempt Review Regulations specify several research activities that are considered exempt from review (45CFR46.101b). An example would be a minimal risk survey that cannot be linked to sub-jects through any form of identifiers. Due to the potential for conflict of interest, it is important to note that someone other than the investiga-tor must make the determination of whether or not a study meets the criteria for exemption. Typically, this determination should be made by an IRB member. Contact your IRB office
to determine the local procedures for exemption in your institution.
In assessing the type of review your research project may require, a useful tool to have on hand is a group of deci-sion charts published by the DHHS. This will guide you through a list of questions to determine which review category is appropriate for your particular study (see sidebar for resources). Also, communi-cating with the IRB office to confirm that you are completing the correct forms for submission can save you time later.
Documents Needed for IRB ReviewTypically, IRBs include a list of docu-ments required for review submissions on their website. The documents may vary according to the type of research involved. The website will also have a template consent form containing stan-dard language.
Examples of documents that may be required to be submitted with each new full-board review submission include an IRB application, detailed study protocol, subject consent form, data collection tools, grant/contract application, Investigator Brochure, recruitment advertisements, subject questionnaires, and Financial Interest Disclosure forms.
In addition, funding and accredita-tion agencies have adopted policies that mandate human research protec-tion education for all study personnel. Many institutions utilize the Collabora-tive Institutional Training Initiative (CITI) course for this purpose. This contains various training modules and a certificate is issued upon suc-cessful completion of the course. Most IRBs will not issue final approval of a project until they have verified that all study personnel have completed this training.
The Full Board IRB Review ProcessFor full IRB review, the board will need all of the required documenta-tion to assess that the study meets
Feature
10 | December 2012

the federal criteria for approval. Many IRBs operate on a primary reviewer system whereby 1 or more IRB mem-bers are assigned a protocol based on the member’s education, background, and expertise. If no member has the appropriate expertise, an outside con-sultant is usually called upon. Some IRBs invite the investigator to the con-vened meeting to present their new protocols and answer any questions that might arise.
Much of the committee’s discussion is typically focused on weighing the risks involved with the study versus the potential for benefit to subjects. Risks include not only physical risks but also psychological and social risks. Recommended changes to the consent form are also discussed. If significant concerns are raised by the IRB, the protocol may be tabled or disapproved.
During the meeting, the IRB will de-termine the length of approval. This is based on the risks associated with the study and cannot exceed 1 year. The IRB may shorten the approval period for higher-risk protocols.
At the conclusion of the discussion, an IRB member makes a motion, it is seconded by another member, and then all members vote for or against approval or may abstain from voting. Members with a conflict of interest are required to leave the meeting room during the discussion and cannot par-ticipate in the vote.
IRB Approval TimelineOncology fellows need to be aware that once an application is submitted to the IRB it may take up to a month to be reviewed, although the time frame depends on the particular institution. Ask your local IRB for its average turn around time. This may vary according to review category and deadlines for submission. Since projects cannot be initiated until IRB approval is received, it is imperative to take this interval into consideration when developing a timeline for the implementation of any given research project.
Another issue to consider in sched-uling planning is that project approval will likely not be granted outright.
Upon review, the IRB may determine that certain changes are required in order to obtain approval. These could include recommended changes to the protocol, consent document, data col-lection sheet, etc. The investigator will need to respond to the IRB’s suggested revisions in writing and resubmit the materials for review by the IRB.
ConclusionIt is the responsibility of the investi- gator to maintain IRB approval at all times. This means that continuing reviews must be submitted in a timely manner to avoid a lapse in approval. All study amendments must be sub-mitted for approval prior to their implementation. Protocol deviations or violations and adverse reactions must be reported.
It is important for oncology fel-lows to communicate with their local IRB office. The IRB staff can review materials (such as study protocols, consent forms, etc) prior to the formal submission to the full IRB commit-tee and can provide answers to many questions. This can save investigators valuable time and avoid aggravation in the long run.
Breaches in compliance can lead not only to bad headlines in newspapers, but also a suspension of all federally funded research at the institution. The ultimate responsibility for the protec-tion of human subjects in research rests with the investigator and is con-gruent with the declaration in the Hip-pocratic Oath to “Do no harm.”
The primary mission of the IRB is to protect human subjects. But it is important to note that in so doing, they can serve as a resource and can also protect investigators who are conduct-ing the studies.
Nancy Fell Hill, MPH, is a New Jersey– based research administrator and free-lance author. She has more than 10 years of experience working with IRBs in both a hospital setting and a large university.
December 2012 | 11
US Department of Health and Human Services: Human Subject Regulations Decision Charts http://tinyurl.com/8rren7b
Online Resources for Human Research Studies
US Department of Health and Human Services: Office for Human Research Protections www.hhs.gov/ohrp/
US Food and Drug Administration: Science & Research: Running Clinical Trials http://tinyurl.com/y995a4r
National Institutes of Health: Bioethics Resources on the Web http://tinyurl.com/8jjxljf

Learn about our commitment to patients at BioOncologyAccessSolutions.com/support
Taking a broader view —charting a unique course in cancer care
© 2012 Genentech USA, Inc. All rights reserved. BIO0001046900 Printed in USA.
At Genentech BioOncology, not only are we leading the � ght against cancer with innovative science, but we’re also dedicated to supporting patients and others within the oncology community.
A commitment to patients — We created Genentech BioOncology™ Access Solutions®, a single source for all access and reimbursement issues, so healthcare providers can remain focused on patient care.
Reducing barriers to treatment — We help make treatment possible for patients in � nancial need through our BioOncology Co-pay Card and ongoing charitable donations to various co-pay assistance foundations.
A commitment to care — Since 1985, when our � rst product was approved, we have donated $2.85* billion in free medicine through the Genentech® Access to Care Foundation (GATCF) and other product donation programs.
Our goal is to fundamentally change the way that cancer is treated by personalizing solutions to patient care.
*GATCF donation value is based on the most current forecast.
74472ha_a.indd 1 8/27/12 8:30 PM

Learn about our commitment to patients at BioOncologyAccessSolutions.com/support
Taking a broader view —charting a unique course in cancer care
© 2012 Genentech USA, Inc. All rights reserved. BIO0001046900 Printed in USA.
At Genentech BioOncology, not only are we leading the � ght against cancer with innovative science, but we’re also dedicated to supporting patients and others within the oncology community.
A commitment to patients — We created Genentech BioOncology™ Access Solutions®, a single source for all access and reimbursement issues, so healthcare providers can remain focused on patient care.
Reducing barriers to treatment — We help make treatment possible for patients in � nancial need through our BioOncology Co-pay Card and ongoing charitable donations to various co-pay assistance foundations.
A commitment to care — Since 1985, when our � rst product was approved, we have donated $2.85* billion in free medicine through the Genentech® Access to Care Foundation (GATCF) and other product donation programs.
Our goal is to fundamentally change the way that cancer is treated by personalizing solutions to patient care.
*GATCF donation value is based on the most current forecast.
74472ha_a.indd 1 8/27/12 8:30 PM
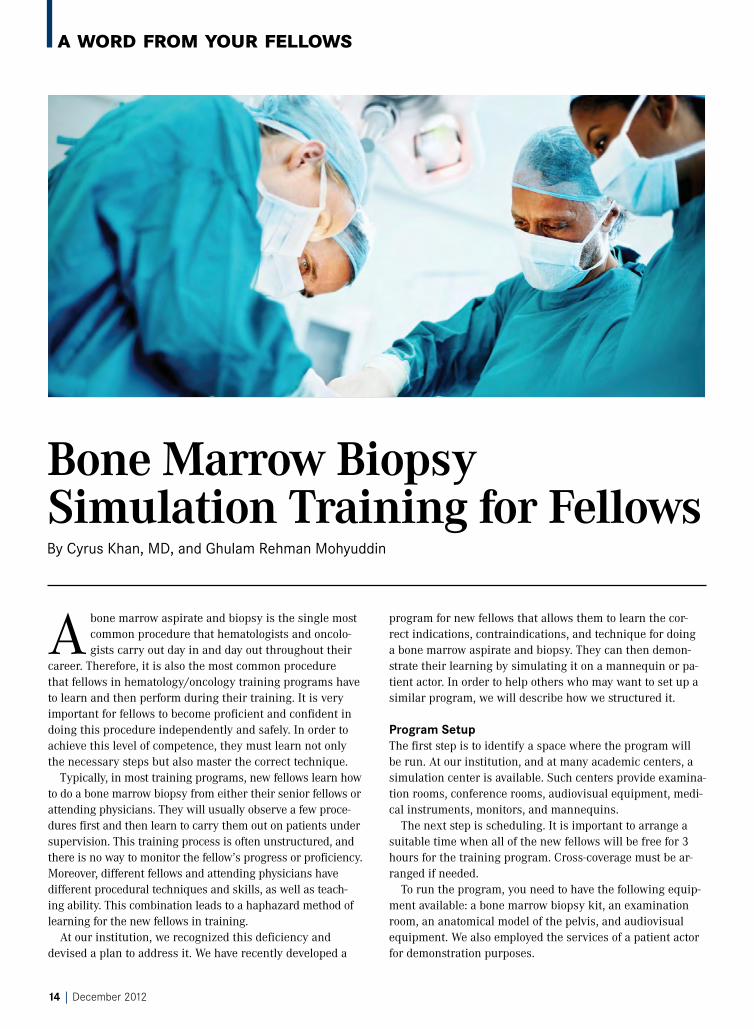
Bone Marrow Biopsy Simulation Training for FellowsBy Cyrus Khan, MD, and Ghulam Rehman Mohyuddin
A bone marrow aspirate and biopsy is the single most common procedure that hematologists and oncolo-gists carry out day in and day out throughout their
career. Therefore, it is also the most common procedure that fellows in hematology/oncology training programs have to learn and then perform during their training. It is very important for fellows to become proficient and confident in doing this procedure independently and safely. In order to achieve this level of competence, they must learn not only the necessary steps but also master the correct technique.
Typically, in most training programs, new fellows learn how to do a bone marrow biopsy from either their senior fellows or attending physicians. They will usually observe a few proce-dures first and then learn to carry them out on patients under supervision. This training process is often unstructured, and there is no way to monitor the fellow’s progress or proficiency. Moreover, different fellows and attending physicians have different procedural techniques and skills, as well as teach-ing ability. This combination leads to a haphazard method of learning for the new fellows in training.
At our institution, we recognized this deficiency and devised a plan to address it. We have recently developed a
A Word from Your felloWs
program for new fellows that allows them to learn the cor-rect indications, contraindications, and technique for doing a bone marrow aspirate and biopsy. They can then demon-strate their learning by simulating it on a mannequin or pa-tient actor. In order to help others who may want to set up a similar program, we will describe how we structured it.
Program SetupThe first step is to identify a space where the program will be run. At our institution, and at many academic centers, a simulation center is available. Such centers provide examina-tion rooms, conference rooms, audiovisual equipment, medi-cal instruments, monitors, and mannequins.
The next step is scheduling. It is important to arrange a suitable time when all of the new fellows will be free for 3 hours for the training program. Cross-coverage must be ar-ranged if needed.
To run the program, you need to have the following equip-ment available: a bone marrow biopsy kit, an examination room, an anatomical model of the pelvis, and audiovisual equipment. We also employed the services of a patient actor for demonstration purposes.
14 | December 2012

December 2012 | 15
Training ProcessAbout 2 weeks prior to the session, all of the fellows were sent a link to an online video that is available on the website of the New England Journal of Medicine1 that demonstrates how to do a bone marrow biopsy. They were also sent a copy of the article “How to do the perfect bone marrow biopsy.”2 On the day of the training session, they were given a PowerPoint presentation on the didactics of a bone marrow biopsy to rein-force specific relevant points, including indications, contrain-dications, possible complications, etc. They were also shown the anatomical landmarks on a pelvic model. They were then guided through a review of all of the requisition forms they would need to fill out when doing an actual biopsy and how to correctly complete them.
After this review, all the fellows were taken to an exami-nation room to observe the entire process of a bone mar-row biopsy demonstrated on the patient actor. The actual procedure was not performed on the actor, but the process was simulated from taking consent all the way through to making slides and sending off the specimens in the cor-rect containers.
Alternatively, if an anatomy lab is available, the procedure can be performed on a cadaver. Each fellow then demon-strated how he/she would carry out the procedure. Teaching faculty and senior fellows observed these demonstrations and provided critiques. They also demonstrated their ability in making slides, using fake blood. Specific attention was paid to the communication aspects of the demonstration, es-pecially ensuring that correct consent was obtained, the indi-cations and complications of the procedure were explained, and that adequate anesthetic and pain control was offered.
This simulation lesson must be followed up with reinforce-ment of the procedures taught in this program during live-patient encounters. We have developed an evaluation form that is used by an attending physician or a senior fellow to evaluate the junior fellows on their performance when they perform a bone marrow biopsy on their first 5 patients. This is an invaluable tool in helping to streamline the process of feedback and helps the fellows hone their skills further. The specific areas on which each fellow is graded are shown in the Table. In these areas, each fellow is graded on a 5-point scale from “superior performance,” “good,” “fair,” “sub-stan-dard,” to “unable to grade because of lack of observation.”
ConclusionFeedback from the participating fellows and attending phy-sicians has been very encouraging. The fellows now have greater self-confidence when carrying out their first bone marrow biopsy and their learning curve is much steeper. We plan to offer this program to incoming fellows every year. We strongly believe that this program will streamline the pro-cess of fellows learning this essential procedure. The more detailed training offered in this program helps fellows be-come skilled at performing a bone marrow biopsy, and these abilities are practiced and reinforced further during their live-patient encounters.
When this article was written, Cyrus Khan, MD, was chief fellow in the hematology/oncology fellowship program at the West Penn Allegheny Health System in Pittsburgh, Pennsylvania. He is now a member of the faculty in the Division of Stem Cell Trans-plantation and Cellular Therapy at the same institution. Ghulam Rehman Mohyuddin is a final-year medical student at the Aga Khan University, Karachi, Pakistan, who has completed a clini-cal elective in hematology/oncology at the same institution.
References
1. Malempati S, Joshi S, Lai S, et al. Videos in clinical medicine: bone marrow aspiration and biopsy. N Engl J Med. 2009;361(15): e28.
2. Khan C, Moffa C. How to do the perfect bone marrow biopsy. Onc Fellows. 2011;3(3):12-16.
Table. The evaluation criteria for observation of new fellows performing bone marrow biopsy procedures
Patient Care
‘Time Out’ performed
Anatomic landmarks identified
Aseptic technique maintained
Adequate local anesthesia used
Appropriate technique
Medical Knowledge
Understands indications
Understands what specimens are needed, ie, cytogenetics, flocytometry
Communication/Interpersonal skills
Explains the indication for the procedure
Explains what the patient will experience
Explains the potential risks; consent properly obtained
Uses clear, understandable terms
Professionalism
Accepts instruction and suggestions
Respects patient privacy and dignity
Uses respectful language
Courteous to nursing and allied health staff
Practice-Based Learning
Reviews final results of the test
Systems-Based Practice
Understands logistics of setting up a bone marrow biopsy
Understands logistics of specimen handling, transportation to lab

How do I keep up with the literature?By Amer M. Zeidan
A s an oncology fellow pursuing an academic career, one of the major challenges I face is the arduous process of multi-tasking and time management to
balance my clinical duties and my research activities. In ad-dition to taking care of my clinic patients and conducting several clinical research studies, I have had to find an effi-cient way to keep up with the developments reported in the literature.
Through current literature, I learn about many practice-changing clinical trials, novel insights into the pathogenesis and molecular mechanisms underlying various malignancies including newly identified potential therapeutic targets, and many newly approved drugs and therapeutic approaches to different types of malignancies and hematologic disorders. The sheer volume of clinical studies, case reports, and re-view articles available in print journals and online creates a daunting mountain to face.
One of the most successful senior investigators at my institution always told fellows that we should follow the “hour-glass” model of knowledge and skill acquisition in
order to succeed in the academic world. According to this model, at the beginning of your fellowship you should focus on understanding general principles and acquiring a wealth of actionable knowledge in general oncology and hematol-ogy. This knowledge is needed for safe and efficient care of patients. Then, in the latter parts of fellowship and during the junior faculty years, the focus should shift to becoming the “world expert” in a particular area of research interest through detailed and comprehensive reading and learning. In the later phases of an academic career, after becoming an established investigator in a specific area of interest, the focus can be broadened again to encompass other possible areas of interest.
I have tried to follow this model during my fellowship training. As a result, during my second and third years of fel-lowship (the narrow neck of the “sand-glass”), I have devoted the vast majority of my time to expanding my knowledge in the micro-details in my area of expertise and the focus of my future academic career: pathogenesis and management of myelodysplastic syndromes (MDS) and acute myeloid leuke-
A Word from Your felloWs
16 | December 2012

December 2012 | 17
mia (AML). Achieving this goal successfully required that I dedicate a lot of time to keep up with the countless new re-search papers in these areas while conducting my own clini-cal research. The natural result of this shift to a narrow focus during the latter parts of my fellowship was that I have had little time to keep up with the rapidly expanding literature in other areas of oncology and hematology disciplines.
It is important to me to keep updated on general hematol-ogy and oncology developments for a number of reasons. First, this information helps me to appropriately treat my clinic patients, who present with a variety of malignancies and hematologic diseases. Also, since I have pursued dual certification in both hematology and oncology, I need to be prepared to take the boards. Last but not least, I have a relentless desire to be aware of all the new exciting devel-opments in the fields of oncology and hematology. Senior fellows interested in academic careers share this challenge: How to tackle the never-ending stream of published litera-ture. In attempting to maintain a balance, I have found sev-eral strategies and resources to be quite useful.
First, since it is virtually impossible to read every medical journal on regular basis to keep up with new oncology and hematology research, a reasonable alternative for me was to focus on the leading MDS and AML journals. I also read at least one of the clinical journals that regularly tracks and summarizes the major papers and developments in the field. One such resource is the “Oncology and Hematology Journal Watch,” which summarizes key hematology and oncology research papers from more than 250 medical journals and offers clinical commentary from experts in the field. The American Society of Clinical Oncology (ASCO) produces “ASCO News,” which also presents many updates in oncology research. In addition, I always try to read two of the leading journals in the field, Blood and Journal of Clinical Oncology (JCO), as well as the oncology/hematology articles in the New England Journal of Medicine (NEJM). Recent review articles can also be very helpful in keeping updated in a particular area without devoting as much time as it takes to read every new clinical research article. Each of the major journals in oncology and hematology publishes serial reviews of current hot topics in the field. For example, for benign and malignant hematology, I find the “How I treat” review articles in Blood to be good reviews of the current status of the literature on that particular subject.
Second, in addition to reading journals, another helpful re-source that I frequently use are the audio updates that can be downloaded in mp3 format and so I can listen to them on my iPod while working out or while driving back and forth to work. For example, the oncologic educational activities produced by Research To Practice are distributed by mail to subscribers or can be downloaded from the website. These educational mate-rials include audio interviews with experts in the field, case-based panel discussions, studies of patterns of care, and other programs that are delivered in an easy to follow format.
Third, in addition to attending some of the major national and international meetings in AML and MDS that are impor-tant for my research interest, I also try to attend one of the smaller regional meetings that summarizes the most impor-tant presentations in the international meetings of oncology and hematology. For example, both ASCO and the American Society of Hematology (ASH) organizes several condensed regional “highlights” meetings in different cities throughout the year to print the information to a wider audience of on-cologists and hematologists who might not have the chance to attend the main meetings. Some of these highlights of ASH and ASCO meetings are being conducted internation-ally as well. Many institutions, societies, and agencies also conduct their own “board-review” courses or conferences in specific areas of oncology, hematology, clinical pharmacol-ogy, targeted therapies, immunologic mechanisms, and other disciplines.
These approaches have been most useful to me in keeping current in the oncology and hematology disciplines that are out of the scope of my focused research interest. But I’m sure other fellows have developed other useful strategies. I wel-come any suggestions of other approaches to this important challenge that faces most senior fellows in oncology or hema-tology preparing for academic careers.
Amer M. Zeidan, MD is a clinical hematology/oncology fellow at the Sidney Kimmel Comprehensive Cancer Center, The Johns Hopkins Hospital in Baltimore, MD. Email: [email protected].
Online Resources •American Society of Clinical Oncology (ASCO) Meetings
http://tinyurl.com/963mnwm
•ASCO News http://tinyurl.com/9hxz8yx
•American Society of Hematology (ASH) Meetings http://tinyurl.com/9oq9s7e
•Blood http://tinyurl.com/2tvpmv
•Journal of Clinical Oncology http://jco.ascopubs.org
•The New England Journal of Medicine www.nejm.org
•Oncology and Hematology Journal Watch http://tinyurl.com/9bg9tet
•OncLive www.OncLive.com
•Research To Practice www.researchtopractice.com

transitions
Achieving Career Success in
Academic OncologyWhat to know when deciding on a career in academia
By Mohammed almubarak, MD, and Jame abraham, MD, FaCP
18 | December 2012
December 2012 | 19
applying for an academic jobIf you are planning to pursue an academic career, make sure you have a mentor who can guide you through the application, interview, and selection processes. Generally speaking, there are usually many academic oncology practices in universities and cancer centers that actively search for young talent to build their department or join their established staff. A fellow should start looking for an academic job opportunity before the end of the second year of fellowship or during the early part of third year. A good place to start is with advertisements in major oncology journals or postings at national meetings such as the American Society of Clinical Oncology or the American Society of Hematology Symposium.
Preparing an adequate curriculum vitae (CV) is probably the most important step in the job application process. The CV should include the following information in a clear and organized manner: contact information, academic background and training history, research experience, grants and publications, awards, and voluntary work experience. Emphasizing teaching or mentoring experience and research skills (while avoiding falsifying information) will make a candidate more desirable for an academic job. A candidate should also identify mentors who know him or her well, and who are willing to write letters of recommendation or serve as references if needed.
the job interview processInstitutions that have great interest in a candidate will send an invitation for a job interview. This is an opportunity for the candidate to make a lasting impression and also take a closer look at the work environment. To prepare for the interview, the candidate should inquire about interviewees—including other cancer specialists such as radiation oncologists and surgical oncologists—and their clinical interests. This information can be used to emphasize potential areas of collaboration in the future. In general, the candidate is expected to give a presentation related to his or her work and research interest. It’s vital to tailor the depth of the presentation based on the audience’s clinical interest and background. For example, if your audience is predominantly clinicians, try to focus on the translational or clinical aspects of your research as opposed to basic science. The interview is also an opportunity to highlight individual strengths such as involvement with investigator-initiated clinical trials and prior publication.
tenure versus non-tenure tracksIt is important to understand the different aspects of a tenure vs non-tenure academic oncology track, including the academic ranks and specific requirements for each. A proper understanding of the responsibilities associated with a specific academic position, as well as the culture and expectations of the cancer center and department, is crucial for the candidate’s success in that environment.
Usually, a candidate who has recently completed fellowship is accepted as an assistant professor or, in some cases, as a tutor or clinical instructor. In general, the candidate is offered a position in either tenure track or non-tenure track. In the past, tenure track meant guaranteed, permanent job appointment and benefits. The definition, however, varies from one institution to another. It is very important to find out if you are interviewing for a position in the tenure or non-tenure track and what the specific requirements are for each track. The type of appointment and the requirements needed to achieve tenure status should be made clear in the offer letter.
A key factor to advancing the academic ladder is identifying a mentor who shares common clinical and research interests. On average, an assistant professor is usually eligible to be promoted to an associate professor rank after 5 to 7 years. Each institution will have its own criteria for promotion, and new faculty should familiarize themselves with them. The promotion process involves a thorough review of performance in various aspects of the particular track you are in. It is important to maintain a high level of academic, research, and clinical productivity.
types of academic appointmentsIn general, there are 3 types of academic appointments in oncology: clinical track, scientist track, and clinician scientist track.
Clinical track: Academic oncologists in a clinical track spend most of their working hours (up to 90%) in direct patient care–related activities. This can involve an assigned number of outpatient clinics per week (sometimes up to 4 days of clinic), along with hospital setting or inpatient coverage. The remainder of the time is dedicated to teaching and some research. Since this is a primarily patient care–focused track, the research expectation is limited. However, the faculty member is strongly encouraged to enroll patients in clinical trials and participate
The field of oncology has undergone a significant transformation in the last few years. In this era of individualized medicine, we are learning new ways to tailor treatment based on the molecular pathways of the tumor. There has never been a more exciting time to be in the field of oncology, especially in academic oncology. In addition to the ability to develop a disease-focused clinical career, an academic oncologist can build a research, educational, or administrative career (as, for example, a cancer center medical director or a department section chief). Academic oncologists have a critical role as opinion leaders and shape the future of cancer care by research and training future oncologists, residents, and medical students.

Feature
20 | December 2012
in national cooperative oncology group– or industry-sponsored studies. A clinician track oncologist is rarely expected to write an investigator-initiated trial due to their limited time.
Scientist track: In this track, the emphasis is primarily on research (bench or translational). These oncologists can have up to 90% protected time for research, with less emphasis on patient care and teaching responsibilities. In general, academic oncologists in this setting are guaranteed lab space and initial funding to buy supplies and cover other overhead costs for the first 1 to 2 years. In addition, other ancillary services (eg, animal facilities and tissue banking) and access to other collaborative facilities (eg, clinical trial research units and statisticians) is provided. Academic oncologists are expected to eventually bring extramural support for research and mentor fellows with research interest. The patient care responsibility is usually minimal, consisting of 1 or 2 half-day clinics per week.
Clinician scientist track: Clinician scientists are usually translational investigators. They are the bridge between clinicians and basic scientists or oncologist in the scientist track. Clinician scientists are expected to write investigator-initiated trials and be principal investigator for national cooperative oncology group or industry-sponsored trials. Clinician scientists are also expected to acquire financial support through clinical trials or extramural funding. Usually, clinician scientists are in the clinic 2 or 3 days per week, with the rest of their time dedicated to research and clinical trial activities.
Financial compensation in academia The financial compensation for an academic oncologist is significantly less than for an oncologist in a private practice. The starting salary for an academic oncologist is $160,000 to $200,000, compared with $175,000 to $300,000 for an oncologist in private practice. However, the financial risk in academia is less since academic oncologists work within the structure of university hospitals where the costs and profits are spread over multiple departments. Academic oncologists can choose to supplement their salary through research grants or by giving lectures at pharmaceutical-sponsored conferences.
Academic oncologists are not isolated from real-world medical-financial concerns; they will need to learn about the “ins and outs” of medical billing including, for example, assigning the correct Current Procedural Terminology code for Medicare patients. Familiarity with reimbursement measures such as Relative Value Units (RVUs) is essential since they are also used as a productivity indicator (ie, many practices set RVU goals based on the number of years in practice and assigned academic track).
All in all, finding your niche in academia and tailoring your career to suit your personal strengths and interests is instrumental. As Confucius said, “If you enjoy what you do, you will never work another day in your life.” ■
Mohammed Almubarak, MD, is assistant professor of medicine in the hematology/oncology section of Mary Babb Randolph Cancer Center in Morgantown, West Virginia.
Jame Abraham, MD, FACP, is Bonnie Wells Wilson Distinguished Professor and Eminent Scholar; co-leader of the Breast Cancer Program; chief of the hematology/oncology section; and medical director of the Mary Babb Randolph Cancer Center at West Virginia University in Morgantown.
Keys to success in academic oncology • Thoroughly understand the expectations and
goals of your track.
• Identify a mentor who is familiar with your career goals and who is willing to help you.
• Focus is essential for academic success; concentrate on your strengths and focus on your goals.
• Always try to be a good team player and treat others with respect.
• Take care of your patients, yourself, your family.
• Remember to keep a positive outlook and have fun!
“ On average, an assistant professor is usually eligible to be promoted to an associate professor rank after 5 to 7 years. Each institution will have its own criteria for promotion, and new faculty should familiarize themselves with them.”

About HealthAdviser Why should I join HealthAdviser?
HealthAdviser is a growing community of healthcare experts who share insights and earn honoraria through participation in focus groups, one-on-one interviews, and online surveys.
HealthAdviser is the healthcare professional community of HRA – Healthcare Research & Analytics, a leading market research firm serving the pharmaceutical, biotechnology, and medical device industries. Along with Oncology Fellows, HRA is part of the MJH & Associates family of companies.
As a registered HealthAdviser member, you...
• Become part of a community of healthcare experts.
• Engage with the leading pharmaceutical, biomedical, and medical device companies.
• Lend your insights to help shape the future of healthcare.
• Earn honoraria for your contributions.
Visit Health-Adviser.comto join today!
Heard about HealthAdviser,a new forum for healthcare experts?
Use your smartphone to scan this code or visithttp://bit.ly/VR8Spqfor more information.
Earn honoraria for your contributions!
HealthAdviser_Ad_Asize.indd 4 11/19/12 10:19 AM

Mobile Medicine: Apps for the heAlth cAre professionAl
DrawMDPrice: FreePlatforms: iPadThe DrawMD app was originally developed by surgical oncologists and is now available for a number of specialties. The app provides detailed anatomic drawings to help doctors explain conditions and procedures to their patients. Users can add freehand drawings or stamps to illustrate patients’ specific findings or planned surgical procedures. Developed by Visible Health, the app also offers the ability to import backgrounds and to e-mail or save sketches for later reference.www.drawmd.com
MedSpeakPrice: Lite versions are Free; full versions $9.99Platforms: iPhone, iPod, and iPadThe MedSpeak app is available in both Mandarin and Cantonese versions. Designed to increase patient communication, the apps provide written and audio translations of more than 3300 common medical phrases. These phrases are designed to help obtain patient history and perform a complete physical examination. The free Lite versions offer sample content to help users determine if the full version would be useful. www.qxmd.com/apps/medspeak
MedscapePrice: FreePlatforms: iPod Touch, iPhone, iPad, Android, BlackBerry, and Kindle Fire From WebMD, the Medscape app offers a variety of resources for physicians. Medscape medical news can be filtered by specialty and can be e-mailed or posted to Facebook for sharing. Medical reference resources include prescribing and safety information on more than 8000 prescription and over-the-counter medications, as well as supplements. The Diseases & Conditions resources include more than 4000 articles by medical experts and more than 600 videos demonstrating medical procedures, step by step. The iPhone version also includes medical calculators. www.medscape.com/public/mobileapp
Electronic Preventive Services Selector (ePSS)Price: FreePlatforms: iPod Touch, iPhone, iPad, An-droid, BlackBerry, Palm, and Windows mobile The Agency for Healthcare Research and Quality, part of the US Department of Health and Human Services, has entered the mobile app market. The ePSS app offers searchable access to US Preventive Services Task Force (USPSTF) recommendations for clinical preventative services for your patients. Users can save searches for frequently needed information and can e-mail or print pertinent articles or patient-specific recommendations.epss.ahrq.gov
CellAtlasPrice: FreePlatforms: iPhone, iPod Touch, AndroidCellAtlas is the mobile access point to the CellaVision Blood Cell Morphology Guide. Expert faculty present lectures and relevant images in the following areas: Hematopoiesis, Normal Findings in Peripheral Blood, Other Findings in Peripheral Blood, and Erythrocytes. Several images of each cell type are included for visual reference. In addition, the app includes a CellQuiz of image matching quiz to select the correct images for each cell type as well as links to relevant videos.www.cellavision.com/cellatlas
22 | December 2012
ONLINEONCOLOGIST®

By the Numbers
The graph below illustrates the 2012 estimates of new cases of cancer, by cancer type and sex. The total number of new cases of cancer in males is projected to be 848,170, and 790,740 in females. These data do not include cases of basal or squamous cell skin cancer and in situ carcinoma except urinary bladder. The largest combined cause of new cases of cancer for both genders is cancer of the lung and bronchus, accounting for a total of 226,160 (13.7%) new cases of cancer.
Leading New Cancer Cases, 2012 estimates
Source: American Cancer Society. Cancer Facts & Figures 2012. Atlanta, GA: 2012; 10. Available online at the American Cancer Society website http://tinyurl.com/8kylgc7.
December 2012 | 23
1,638,910
116,470
73,420
55,600
44,250
40,250
38,160
28,540
26,830
22,090
109,690
70,040
47,130
43,210
32,000
31,970
24,520
22,280
21,830
O 50,000
Prostate
Lung & bronchus
Colon & rectum
Urinary bladder
Melanoma of the skin
Kidney & renal pelvis
Non-Hodgkin lymphoma
Oral cavity & pharynx
Leukemia
Pancreas
100,000 150,000 200,000 250,000
O 50,000
Breast
Lung & bronchus
Colon & rectum
Uterine corpus
Thyroid
Melanoma of the skin
Non-Hodgkin lymphoma
Kidney & renal pelvis
Ovary
Pancreas
100,000 150,000 200,000 250,000
Male -- All sites 848,170
Female -- All sites 790,740
241,740
226,870

Conference Center
2012-2013 Oncology & Hematology Meetings
November 15–18Society for Neuro-Oncology 17th Annual Scientific Meeting & Education Day of the Society for Neuro-Oncology Washington, DChttp://tinyurl.com/932gw6h
November 15–16Thoracic Oncology for the OncologistScottsdale, AZhttp://mayocl.in/PcDDSB
November 18–2017th Annual Perspectives in Thoracic OncologyNew York, NYhttp://bit.ly/Qhl9n7
November 30–December 1Hematologic Issues in Cancer CareDallas, TXhttp://tinyurl.com/8rt5oox
December 4–835th Annual San Antonio Breast Cancer SymposiumSan Antonio, TXhttp://www.sabcs.org/
December 8–1154th American Society of Hematology Annual Meeting and ExpositionAtlanta, GAhttp://tinyurl.com/d447zr8
January 16–18Pediatric Oncology Centers of ExcellencePhiladelphia, PAhttp://tinyurl.com/8sspmu8
January 18–19Advances in Thyroid Cancer Diagnosis and TherapyPhoenix, AZhttp://tinyurl.com/9dohhmf
January 199th Annual Clinical Breakthroughs & Challenges in Hematologic MalignanciesLake Buena Vista, FLhttp://tinyurl.com/9caeqb3
February 15-17International Congress on Hematologic MalignanciesNew York, NYhttp://tinyurl.com/awpyrpl
March 7-10Miami Breast Cancer ConferenceMiami, FLhttp://tinyurl.com/amnukaq
November 28–December 2Global Conference on Perioperative Medicine: Care of the Elderly & the Cancer PatientHouston, TXhttp://bit.ly/MUAZxm
November 30–December 1American Society of Clinical Oncology Quality Care SymposiumSan Diego, CAhttp://tinyurl.com/9togz7e
24 | December 2012

Call for PaPers
We welcome submissions to Oncology Fellows, a publication that speaks directly to the issues that matter most to hematology/oncology fellows at all stages of training. Oncology Fellows aims to provide timely and practical information that is geared toward fellows from a professional and lifestyle standpoint—from opportunities that await them after the conclusion of their fellowship training, to information on what their colleagues and peers are doing and thinking right now.
Oncology Fellows features articles written by practicing physicians, clinical instructors, researchers, and current fellows who share their knowledge, advice, and insights on a range of issues.
We invite current fellows and oncology professionals to submit articles on a variety of topics, including, but not limited to:
• Lifestyle and general interest articles pertaining to fellows at all stages of training.
• A Word From Your Fellows: articles written by current fellows describing their thoughts and opinions on various topics.
• Transitions: articles written by oncology professionals that provide career-related insight and advice to fellows on life post-training.
• A Day in the Life: articles describing a typical workday for a fellow or an oncology professional post-training.
The list above is not comprehensive, and suggestions for future topics are welcome. Please note that we have the ability to edit and proofread submitted articles, and all manuscripts will be sent to the author for final approval prior to publication.
If you are interested in contributing an article to Oncology Fellows, or would like more information, please e-mail Donna Bonura at [email protected].

With CancerCare, the difference comes from: • Professional oncology social workers• Free counseling • Education and practical help• Up-to-date information • CancerCare for Kids®
For needs that go beyond medical care, refer your patients and their loved ones to CancerCare.
CancerCare’s free services help people cope with the emotional and practical concerns arising from a cancer diagnosis and are integral to the standard of care for all cancer patients, as recommended by the Institute of Medicine.
makes all the difference
®
1-800-813-HOPE (4673)
www.cancercare.org
Help and Hope
41960ALT_Queen_v1 1 5/13/08 10:03:26 AM