oncology fellows april 2012
DESCRIPTION
Publication for Oncology FellowsTRANSCRIPT
(Never) A Typical Day in the Life of a Pediatric
Hematologist/Oncologist
Using QOPI to Improve Quality Within Your
Fellowship Program
Providing Oncology Services in
Impoverished Countries
Volume 4 • Issue 1, April 2012
This edition is supported by
BIO0001014300
f e l l o w s
When Patients Refuse
Treatment for Their Cancer

FREE, personal websites for cancer patients, survivors, and their caregivers.
Get started with just a few clicks!
www.MyLifeLine.org
MyLifeLine has been an absolute blessing for me and my family. It’s a great way to keep so many people that want to know how I am in the process.
– Kimberly, 31 years old Infiltrating Ductal Carcinoma Grade 2
“
”
Thank you for providing this incredible resource. It has really helped us immensely!
– Benny, diagnosed age 52 Squamous cell carcinoma
“
”
Interested in contributing to Oncology Fellows? If you’d like to submit an article for consideration in an upcoming issue, please e-mail Donna Bonura at [email protected].
When Patients Refuse Treatment for Their CancerBy Aakanksha Prasad Asija, MD, MPHAn oncologist is trained to eradicate disease at almost any cost, but sometimes a patient feels otherwise. This physician describes one encounter with a woman who had made up her mind.
Table of Contents
2
8 (Never) A Typical Day in the Life of a Pediatric Hematologist/OncologistBy David Korones, MDIn his many years as a hematologist/oncologist and professor, one thing is constant in this doctor’s life: the unexpected. No 2 days are ever the same.
12 Using QOPI to Improve Quality Within Your Fellowship ProgramBy Christie J. Hilton, DO, and Alice Ulhoa-Cintra, MDIt is important for oncologists to monitor the quality of their care. This ASCO-maintained program can help fellows do just that within their institutions.
Volume 4 • Issue 1, April 2012
Features
A Word From Your Fellows 16 Providing Oncology Services in Impoverished CountriesBy Diana Osorio, MDIn the United States, the 5-year overall survival rate for childhood cancers is 80%; in developing countries such as Ethiopia, the 5-year survival rate is far worse. This article tells how you can help and includes a report from a physician who’s been working in Malawi for the past 2 years.
19 How Fellows Can Add Value to Their Internal Medicine Residency ProgramBy Cyrus Khan, MD, and Zachariah DeFilipp, MDOncology/hematology fellows can get the most out of their consultation and inpatient oncology services by teaming effectively with their internal medicine residents.
22 Cloud Computing for FellowsBy Jonathan Ticku, MDThere are several applications that can make your life as a fellow much easier. Here are 4 very helpful ones.
Transitions 24 Organizing a Fellows’ Career DayBy Aman Garsa, MDOncologists and hematologists have plenty of career choices, but most fellows have little experience with things like physician recruitment, contract negotiation, visa processing, and more. This article can help.
The Online Oncologist 26 Mobile MedicineApps for the health care professional
27 By the Numbers
28 Conference Center
Departments
Editorial & Production
Vice President, Clinical and Scientific AffairsJeff D. Prescott, PharmD, RPh Project DirectorDonna Bonura
Project Manager Jaclyn Pallotti
Assistant Editor Jeanne Linke Quality Assurance Editor David Allikas
Art DirectorRay Pelesko
Sales & Marketing
PresidentPeter [email protected]
Executive Vice President, SalesJack [email protected]
Vice President, Sales & MarketingLisa [email protected]
Vice President, Integrated Special Projects GroupDavid [email protected]
Directors of SalesScott [email protected]
Erik [email protected]
Senior National Accounts ManagerMike Hennessy, [email protected]
National Accounts ManagersRobert [email protected]
Corrie [email protected]
Sales & Marketing CoordinatorTeisia [email protected]
Digital Media
Vice President, Digital MediaJung Kim
Senior Director, Digital MediaCharlie Weiss
Operations & Finance
Director of CirculationJohn [email protected]
Director of OperationsThomas J. Kanzler
ControllerJonathan Fisher, CPA
Assistant ControllerLeah Babitz, CPA
Corporate
Chairman/Chief Executive Officer/PresidentMike Hennessy
Chief Operating OfficerTighe Blazier
Chief Financial OfficerNeil Glasser, CPA/CFE
Vice President, Executive Director of EducationJudy V. Lum, MPA
Vice President, Group Creative DirectorJeff Brown
Office Center at Princeton MeadowsBldg. 300 • Plainsboro, NJ 08536(609) 716-7777
www.onclive.comF E L L o W S
Q uoting statistics seemed to be a refuge to me. The objectivity of the numbers provided a hiding place and a shelter, and they helped me maintain
the emotional distance that my profession demanded. She repeated, “Can you cure me?” I responded, “Well, I
cannot guarantee a cure, but we can try.”
Her HistoryShe had received 3 cycles of neoadjuvant chemotherapy for her breast cancer and then decided that it was not for her. She did not follow up with her subsequent appointments. Then, she arrived one day in the emergency department, extremely short of breath. She had a pleural effusion that almost completely filled her right thorax. The pleural fluid was drained and she felt much better. Next was the question of treatment of the breast cancer. The medical team discussed the issue with her, but she insisted that she did not want any more treatment. That is when I first met her, as an oncology fellow on the consultation service.
I was briefed about her by an intern. There I was, a first-year oncology fellow in my not-so-crisp white coat, with a smile hiding my exhaustion as I walked into her room. She was a black woman in her early 50s (but looked much younger), with beautiful, carefully arranged dark hair, smiling and cheerful. She did not wear hospital clothes
April 2012 | 3
Cover Story
“Can you cure me?” she asked.
“Well,” I hesitated, “from what I know, you have stage III breast cancer and there is about a 50% chance you will be alive 5 years from now if we treat you.”
By Aakanksha Prasad Asija, MD, MPH
When Patients Refuse Treatment for Their Cancer
4 | April 2012
Cover Story
but rather a bright and colorful gown, matching nail polish, and somewhat large jewelry. She was bent forward in bed but was not uncomfortable.
After introducing myself, I asked her how she was doing and started my history and physical examination. As I examined her I realized she had a rock-hard right breast, with stretched skin that was warm and puckered where the lymphatics had presumably been invaded. The skin was so tight that I imagined it could break open any
moment and pour forth the tumor that lurked within. She had large rock-hard lymph nodes in her axilla and in the supraclavicular region. She could not lift her right arm beyond 30 to 40 degrees. Her entire right arm and forearm were swollen. She said this had occurred only within the last 2 weeks.
She denied feeling any pain and felt well except for the shortness of breath that had brought her to the hospital. She wanted the pleurodesis because it would prevent the fluid from reforming, and she would not have to get admitted to the hospital again. After that she wanted to go home. That’s all she wanted.
Refusing Further TreatmentI pressed for reasons why she had stopped her treatment. Was she having unmanageable side effects? We could switch her to alternate drugs. Treatment options for breast cancer are numerous, I explained. Was the treatment not shrinking the tumor? We could change the regimen or send her for radiation or surgery, possibly followed by chemo-therapy. Was it a long and difficult commute from home? We could arrange transportation. Did she understand her medical condition? I told her that she had triple-negative breast cancer, an aggressive form of cancer that without treatment could progress rapidly and take her life away.
“Yes, I know,” she said. “I thought about it several times, and I decided 3 months back I do not want any more treatment; the Lord wanted me to get 3 cycles and the Lord wanted me to stop.”
I said, “I realize this and am not trying to persuade you (even though I pretty much was), but I want to make sure that you understand the seriousness of your decision not to opt for any treatment. The choice is yours but I want you to carefully consider your options before deciding.”
“Yes,” she smiled, “I understand.” So I decided to change tactics. Did she have a family? “Yes,” and her face lit up in a wide smile, “4 children,
all grown up; 3 grandchildren, of all different ages.” They would all come to visit her that evening. They knew about her decision. Her daughter had objected initially, but had finally reconciled herself to her mother’s decision.
“Can we do anything to make your treatment experience better?” I pressed one last time.
“I want to make sure that you understand the seriousness of your decision not to opt for any treatment. The choice is yours but I want you to carefully consider your options before deciding.”

THE JOHN THEURER CANCER CENTER AT HACKENSACK UNIVERSITY MEDICAL CENTER
The most nationally acclaimed cancer doctors in New Jersey as recognized by:
•CastleConnollyAmerica’sBestDoctorsandBestCancerDoctors
•NewYorkandNewJerseyMagazinesBestDoctorsandBestCancerDoctors
•Who’sWhointheWorld•Who’sWhoinHealthCare
ThemostinnovativecancerdoctorsandnursesinNewJersey:
•Over100peerreviewedcontributionstoadvancingcancercare
•Featuredspeakersatinternationalconferences
•14specializeddivisionswithcancer-specificteamsofexperts
jtcancercenter.org/doctors
The greatest access to breakthrough technologies:
•MostdaVinci®surgicalrobotsinNewJersey,andoneof20trainingcenters
•MostexperiencedTomoTherapy®radiationcenterinNewJersey
•FirstcancercenterinNewJerseytoacquireTrueBeam™radiotherapysystem
•Tumorbankforpersonalizedcancertherapydevelopment
•Oneofthenation’slargestbloodandmarrowstemcelltransplantationprograms
jtcancercenter.org/research
The largest facility dedicated to delivering innovative, personalized care:
•New155,000squarefootfacilitysolelyforcancercare
-Inviting,dramaticatriumspace -Soothing“livingwall” -Abovegroundradiationfacility -Awalk-throughterracegarden•Personalizedcareprogramsasuniqueaseachpatient:
-ElizabethandDonlonHurtubise PatientResourceLibrary
-Cybercafé -Demonstrationkitchen -Yogaandexercisefacility
jtcancercenter.org/patientresources
201.996.5900 jtcancercenter.org
CANCER IS HARD ENOUGH. EVERY PATIENT DESERVES EXTRAORDINARY CARE, WE’RE COMMITTED TO DELIVERING IT.
WHY ONE CANCER CENTER CARES FOR MORE NEW JERSEY RESIDENTS THAN ANY OTHER
and is the Only New Jersey Cancer Center Ranked in the Top 50 by U.S. News & World Report
JTCC_Reg1_201mag_FELLOWS.indd 1 9/1/11 9:47 AM
6 | April 2012
Cover Story
“Well,” she sighed, “it is not about the treatment or the doctors or even the cancer.” This was about her. She had decided that she did not want to fight this thing anymore. No external factors had influenced her decision. She had decided 3 months ago that she did not want any more treatment. She had a few things to take care of, which she already had. She was at peace and ready to move on.
The conversation lasted about an hour. Just like all the other members of the medical team taking care of her, I had attempted to understand my patient’s reasons for refusing treatment. We had all tried, to different extents, either by questioning her repeatedly to ascertain her level of understanding or by talking about her family’s wishes or by subtly expressing our disapproval, to somehow persuade her to get more treatment. We had all failed.
That day, I came out of the room feeling disheartened, as if I had not done my duty. I did not understand her reasons; I had not been able to think of anything I could say that would make her change her mind.
On Her Own TermsMonths later I saw her daughter, who was visiting the hospital. She told me that her mother had died, at home, with her family at the bedside—probably a peaceful, quick, silent death. They had a big family dinner the night before. She had cooked for everybody and had been the ever-gracious hostess; there was music, love, and laughter in the household. And when the family woke up the next day, she was no more. That was how she had wanted it. She had died just as she had lived her life: on her own terms. As I reflect back, I think about the
Interested in contributing to Oncology Fellows? If you’d like to submit an article for consideration in an upcoming issue, please e-mail John Eichorn at [email protected].
I wondered: How long a discussion was long enough? When do we cross the thin line between attempting to understand our patients and imposing our opinion or conveying our disapproval of their decision?
day I saw her in the hospital. The sunlight streaming through the window of her 11th-floor room overlooking Center City Philadelphia, the certainty and determination written all over her face as she smiled at me, the tragic beauty of it all.
And I wondered: How long a discussion was long enough? When do we cross the thin line between attempting to understand our patients and imposing our opinion or conveying our disapproval of their decision? And when they do not agree with our opinions, how do we refrain from judging them for it? Or how do we leave the room not feeling annoyed and defeated? How do we, as physicians, not give up on our patients, even when they do not agree with what we think would be the right thing for them? How and when do I stop being a medical professional with firm, confident medical opinions, stop being a medical oncologist bent on eradicating disease at any cost, and become a fellow human being? Sometimes I wonder if it is then that we are closest to conquering cancer. ■
Aakanksha Prasad Asija, MD, MPH, is a second-year hematology/medical oncology fellow at Thomas Jefferson University Hospital in Philadelphia, Pennsylvania.

OncLive.com features full, exclusive online access to all the articles in each issue of Oncology Fellows. For the latest on the issues and concerns facing oncology and hematology Fellows, go to OncLive.com and click on “Publications” for free, unlimited access to Oncology Fellows.
Bringing the Oncology Community Together
OncLive(A)_12'11.indd 1 4/3/12 9:57 AM
8 | April 2012
Feature
(Never) A Typical Day in the Life of a Pediatric
Hematologist/OncologistBy David Korones, MD

April 2012 | 9
I go on to explain, however, that my inability to answer is part of the beauty of this remarkable field. For example, as I write this article, I am on an Ethiopian Airlines flight to Addis Ababa to participate in a multi-country initiative to bring pediatric oncology care to the children of Ethiopia. Just 10 years ago, I never in my wildest dreams would have imagined that such a mission would be part of my pediatric hematology/oncology duties. So, a typical day? I don’t believe that exists, because our days are punctuated by the unexpected and our field is so diverse that we often change what we do over the course of our careers. Time alters us and our field.
Expect the UnexpectedThere is no typical day because we live in an ever-morphing world. We counsel our patients to expect the unexpected, but we would be wise to tell ourselves the very same thing. Many is the day I have looked forward to quiet time in the office so that I can catch up and clear my head, but then my pager will sound and the emergency room will call. “Dave, we have a 4 year old down here with headaches and vomiting, and the head CT scan does not look good. Help!” Or a worried parent will call to talk about her 10-year-old daughter, who just finished treatment for acute lymphoblastic
leukemia and now has a little knot behind her left ear. Or there is a sad meeting with a bereaved parent who just needs to talk. Or, on a more cheerful note, a chance encounter with a bushy-haired, lanky teen—a 10-year survivor of Ewing sarcoma whom you would never in a million years recognize if he didn’t have his parents with him. So, seldom is the “quiet” day quiet.
A typical day does not exist because even when things go as planned, there is so much variety in the things we do. On Monday and Tuesday I might attend on the inpatient clinic service; Wednesday might find me devoted to administration and teaching; and on Thursday and Friday I may be focused on research. Even within each day there is further variability. One patient may be here for routine follow-up for sickle cell anemia, whereas the next is a 13-year-old boy with a white blood cell count of 100,000 and an enlarged spleen. A clinical research day may run the gamut from enrolling a child in a study to filling out endless Serious Adverse Event (SAE) Report forms to conference calls on how to conduct a particular clinical trial.
A typical day does not exist because as the years go by our careers flow in different, unexpected directions, and what was typical for us 10 years ago may bear little
I t seems the older I get, the more frequently high school students, undergraduates, medical students, or residents drop by my office to talk about career
choices, inquire about shadowing, or request an interview for a school project. “Tell me about your typical day,” they’ll ask. That is a challenging question to answer, because there is no such thing as a typical day. That response usually leaves my questioner a bit frustrated.

10 | April 2012
Feature
resemblance to what is typical for us now. In my own career, 20 years ago, my days were spent juggling test tubes in the lab with time in half-day clinics that morphed into 3/4-day clinics that morphed into full-day clinics—not to mention long stretches of wearying time in the inpatient trenches. Twenty years later, I am a very happy clinician who spends most of his clinical time caring for children with brain tumors, running a pediatric palliative care program, administering a fellowship, and delving into international pediatric hematology/oncology.
Then and NowA typical day does not exist because not only do we change as we grow older (or shall I say, more mature), but the times change as well. Twenty years ago, a desktop computer with Internet access was as far from standard issue as a landline is for a college student today. My typical day included very little time at the computer, because there just weren’t that many computers. Besides, there was not that much in the way of online medical information to click and scroll through, even when I had this novelty at my fingertips. So, a
typical day 20 years ago in the Web-less era included playing phone tag to reach referring physicians and experts in the field, calling labs for results, and reading through piles of hard-copy lab reports. Now that typical day includes many hours at the laptop, desperately trying to keep up with e-mails and trying to keep my cool in a vain attempt to decipher the bewildering electronic medical record system. Twenty years ago, a typical day might include an occasional tiff with an insurance company, whereas now our days are filled with skirmishes over prior authorizations and battles over covering the medications we know our patients need. Twenty years ago, we gave little thought to how much revenue our care and our notes would bring in. Now our typical days are filled with careful scrutiny
of what we write, not just for the purposes of medical care but for the need to bill commensurate with what we document.
So, in a nutshell, there is no typical day. And I for one would not have it any other way. I love the stimulation that the unexpected brings. I love the different sorts of gratification I get from a day spent teaching, in clinic, or on service. And I love the fact that nothing is static—that we change and the times change.
That said, there can and should be constants in our careers and in this field from day to day and from year to year. Overall, my passion for the field and the privilege of being a part of it is unwavering. I believe that is a thread that connects each day and represents what is typical in the world of pediatric hematology/oncology—not just from day to day and year to year, but from generation to generation. And perhaps the most important constant of all—at the core of all we do—is sitting at the bedside of the child with cancer and his/her family, stripped of time, technology, and the trappings of the modern era. May that relationship with child and family, and that perilous trip with them from diagnosis down whatever road it may take us, forever be a part of our typical or atypical day. ■
David Korones, MD, is a professor of pediatrics, oncology, and neurology at University of Rochester School of Medicine and Dentistry in Rochester, New York.
Perhaps the most important constant of all—at the core of all we do—is sitting at the bedside of the child with cancer and his/her family, stripped of time, technology, and the trappings of the modern era.

This space provided as a public service.©2010 Susan G. Komen for the Cure® The Running Ribbon is a registered trademark of Susan G. Komen for the Cure.
But scientifi c minds cannot solve breast cancer alone. Susan G.
Komen for the Cure®, the leader of the global breast cancer movement, is leading in science
again. We’ve just tapped 50 of the world’s top cancer experts to Komen’s new Scientifi c
Advisory Council, to drive innovation and breakthroughs in cancer research. We think of it as
the Ultimate Cancer Think Tank.
We’re also supplying the tools that will help global researchers unlock the secrets of breast
cancer. How it begins and grows. How we can stop it in its tracks. The answers may lie in the
Susan G. Komen for the Cure Tissue Bank at the Indiana University Melvin and Bren Simon
Cancer Center -- the largest source of healthy breast tissue in the world, soon to be available
digitally to researchers around the world over the Internet.
Make an impact and donate today. Visit komen.org/donations.
to fi nd the cures.
It takesIt takes
to fi nd the cures.NNOVATION
Komen Tissue Bank volunteer and Purdue University graduate student, Rebecca Fega, helps process breast tissue samples November 2009 in West Lafayette, Ind.
Using QOPI to Improve Quality Within Your Fellowship ProgramBy Christie J. Hilton, DO, and Alice Ulhoa-Cintra, MD
Quality Oncology Practice Initiative (QOPI) is an oncologist-created quality improvement program developed and maintained by ASCO. It is important to be able to objectively review the care that is given in your institution in order to improve the quality of care that is ultimately delivered. The QOPI program creates a
uniform measurement of the quality of care delivered by an oncologist; this affords self-examination and directed improvement of practices. QOPI enables self-assessment through twice-yearly retrospective medical chart reviews that are designed to be used in the outpatient hematology/oncology setting. The collection of data from medical records applies identified universal quality measures that have been defined and developed by practicing medical oncologists based on established consensus guidelines. QOPI is designed to objectively measure parameters reflective of quality care that are managed by the medical oncologist. The results of each chart audit allow participants to compare their findings against other participating groups, enabling them to direct their efforts of quality improvement by identifying areas of deficiency.
Feature
12 | April 2012

April 2012 | 13
Why should fellows be involved in QOPI? There are many benefits to QOPI. At its most basic level, QOPI places an emphasis on documentation. In medicine, we have all been told, “If it is not documented, it didn’t happen.” QOPI also focuses our attention on specifically what is important to include in an oncology patient’s medical record, which is paramount in a fellow’s education. For example, we may know that a particular chemotherapy in a certain case is for palliative intent and we may have discussed it with the patient, but it should be explicitly documented. QOPI also exposes us to continual practice-based quality improvement, which is one of the ACGME core competencies for fellowship. Participation in QOPI satisfies the practice-based improvement component of the ACGME requirements.
What type of information do you obtain from the charts? QOPI includes a variety of modules from which to choose. Some modules are universal (Core Measures, End-of-Life Care, and Symptom/Toxicity Management), and others are disease specific (Breast Cancer, Colorectal Cancer, and NHL). Our fellowship program plans to participate in the Core Measures and Symptom/Toxicity Management modules for the spring 2012 audit. (There are 2 audits each year, in the spring and fall.) These 2 modules contain 34 total data points (25 Core Measures and 9 Symptom/Toxicity Management measures) to be collected from patient charts. An example of the Core Measures data includes identifying chart documentation of pain assessment: Was the patient’s pain documented and quantified by the second visit? Was a plan documented for the treatment of moderate/severe pain? If narcotics were prescribed, was the effectiveness documented at the next visit, and
was constipation addressed? These questions address 5 of the 25 core measures.
How does the program work? One or several modules are chosen, and charts are sequestered for audit. It takes approximately 30 to 45 minutes to audit each chart. After the data are collected, they are entered into a Web-based program that is maintained by ASCO. The data (expressed as percent compliance for each measure) can then be reported in a variety of ways. Percent compliance for each measure can be reported by overall practice or broken down to report each individual physician/fellow. The results can then be compared with the overall database results. This allows each program to compare its compliance with results from previous audits in order to gauge its overall improvement, as well as to judge overall performance in comparison with other programs.
How does your program incorporate QOPI for the fellows? The Allegheny General Hospital has been using QOPI on the attending level since 2006, and it is being initiated on the fellow level in spring 2012. To prepare for the addition of the program, we have been asked to keep track of at least 10 patients from our continuity clinic to submit for the spring 2012 audit. We were asked to choose our patients based on the following criteria, which are established by ASCO QOPI guidelines: patients must be diagnosed with an invasive malignancy in the past 2 years and must have had 2 office visits in a 6-month-period. Additionally, we were asked to choose patients whom we were involved with directly in development of the treatment plan and its documentation. In spring 2012, we plan to submit our 10 patients for review by another fellow in the program. Charts will not be self-analyzed in an attempt
to prevent bias in regard to interpretation of the documentation.
In preparation of initiation of QOPI, the fellows were involved in auditing charts for the attending-level spring 2011 audit. At that time, each fellow was asked to review 2 charts that had been previously audited by a third party. We were instructed not to interpret the documentation and to record data based directly on what was documented. For quality control, our individual audits were compared with audits previously performed on the same charts by a third party to determine reproducibility of results. When compared, the results were within 2%, which indicated that we were auditing the charts appropriately.
How will we use the results of the audit? We plan to meet after the spring 2012 audit to review our results and formulate a plan for improvement based on our discovered deficiencies. We are excited to participate in the spring 2012 audit, and we are interested to see how our fellowship compares with the practice as a whole and to other fellowships regarding these measures of quality. We were left wondering, however, if QOPI truly measures quality of care, or if it simply measures the quality of documentation. Either way, we believe it is a good tool to utilize in fellowship to help prepare us for our careers in hematology oncology.
For more information on how your fellowship can get involved, go to www.asco.org/qopi.
Christie J. Hilton, DO, is a second-year hematology/oncology fellow at The West Penn Allegheny Health System in Pittsburgh, Pennsylvania.
Alice Ulhoa-Cintra, MD, is a third-year hematology/oncology fellow at The West Penn Allegheny Health System in Pittsburgh, Pennsylvania.
BIONP-42742A_M03_Asz_UPdt.indd3-30-2011 3:59 PM Dan Capobianco / John Gluth
Client CodeClient
LiveOverall TrimBleed
# of Colors
BIO0000330901GENENTECH
14.25” x 10”15.5” x 10.5”17” x 11.125”
4C
Job info
NoneNotes Fonts
Trade Gothic (Medium, Bold No. 2), TT Slug OTF (Regular)
ImagesBioOnc_Glider-Horz_HR.tif (CMYK; 532 ppi; 56.34%), Gene_Logo_KO_T.ai (70.15%), BioOnc_WM_R_4C.ai (60%)
Inks Cyan, Magenta,
Yellow, Black
Fonts & Images
Saved at
None
from dcapobianco3057 by
Printed At
Taking a broader view —charting a unique course in cancer care
At Genentech BioOncology, not only are we leading the fight against cancer with innovative science, but we’re also dedicated to supporting patients and others within the oncology community.
A commitment to patients — We created Genentech BioOncology™ Access Solutions®, a single source for all access and reimbursement issues, so healthcare providers can remain focused on patient care.
Reducing barriers to treatment — We help make treatment possible for patients in financial need through our BioOncology Co-pay Card Program and ongoing charitable donations to various independent, nonprofit organizations in support of co-pay assistance.
A commitment to care — Our first product was approved in 1985, and since then we have donated approximately $2.3 billion in medicine to uninsured patients through the Genentech® Access to Care Foundation and other donation programs.
Our goal is to fundamentally change the way that cancer is treated by personalizing solutions to patient care.
www.BioOncology.com
© 2011 Genentech USA, Inc. All rights reserved. BIO0000330901 Printed in USA.
S:14.25”
S:10”
Trim: 15.5”
Trim: 10.5”
Bleed: 17”
Bleed: 11.125”
Page Trim: 7.75”
Safety: 7”
Page Trim: 7.75”
Grind Off: .125” Grind Off: .125”
Safety: 7”
BIONP-42742A_M03_Asz_UPdt.indd3-30-2011 3:59 PM Dan Capobianco / John Gluth
Client CodeClient
LiveOverall TrimBleed
# of Colors
BIO0000330901GENENTECH
14.25” x 10”15.5” x 10.5”17” x 11.125”
4C
Job info
NoneNotes Fonts
Trade Gothic (Medium, Bold No. 2), TT Slug OTF (Regular)
ImagesBioOnc_Glider-Horz_HR.tif (CMYK; 532 ppi; 56.34%), Gene_Logo_KO_T.ai (70.15%), BioOnc_WM_R_4C.ai (60%)
Inks Cyan, Magenta,
Yellow, Black
Fonts & Images
Saved at
None
from dcapobianco3057 by
Printed At
Taking a broader view —charting a unique course in cancer care
At Genentech BioOncology, not only are we leading the fight against cancer with innovative science, but we’re also dedicated to supporting patients and others within the oncology community.
A commitment to patients — We created Genentech BioOncology™ Access Solutions®, a single source for all access and reimbursement issues, so healthcare providers can remain focused on patient care.
Reducing barriers to treatment — We help make treatment possible for patients in financial need through our BioOncology Co-pay Card Program and ongoing charitable donations to various independent, nonprofit organizations in support of co-pay assistance.
A commitment to care — Our first product was approved in 1985, and since then we have donated approximately $2.3 billion in medicine to uninsured patients through the Genentech® Access to Care Foundation and other donation programs.
Our goal is to fundamentally change the way that cancer is treated by personalizing solutions to patient care.
www.BioOncology.com
© 2011 Genentech USA, Inc. All rights reserved. BIO0000330901 Printed in USA.
S:14.25”
S:10”
Trim: 15.5”
Trim: 10.5”
Bleed: 17”
Bleed: 11.125”
Page Trim: 7.75”
Safety: 7”
Page Trim: 7.75”
Grind Off: .125” Grind Off: .125”
Safety: 7”
BIONP-42742A_M03_Asz_UPdt.indd3-30-2011 3:59 PM Dan Capobianco / John Gluth
Client CodeClient
LiveOverall TrimBleed
# of Colors
BIO0000330901GENENTECH
14.25” x 10”15.5” x 10.5”17” x 11.125”
4C
Job info
NoneNotes Fonts
Trade Gothic (Medium, Bold No. 2), TT Slug OTF (Regular)
ImagesBioOnc_Glider-Horz_HR.tif (CMYK; 532 ppi; 56.34%), Gene_Logo_KO_T.ai (70.15%), BioOnc_WM_R_4C.ai (60%)
Inks Cyan, Magenta,
Yellow, Black
Fonts & Images
Saved at
None
from dcapobianco3057 by
Printed At
Taking a broader view —charting a unique course in cancer care
At Genentech BioOncology, not only are we leading the fight against cancer with innovative science, but we’re also dedicated to supporting patients and others within the oncology community.
A commitment to patients — We created Genentech BioOncology™ Access Solutions®, a single source for all access and reimbursement issues, so healthcare providers can remain focused on patient care.
Reducing barriers to treatment — We help make treatment possible for patients in financial need through our BioOncology Co-pay Card Program and ongoing charitable donations to various independent, nonprofit organizations in support of co-pay assistance.
A commitment to care — Our first product was approved in 1985, and since then we have donated approximately $2.3 billion in medicine to uninsured patients through the Genentech® Access to Care Foundation and other donation programs.
Our goal is to fundamentally change the way that cancer is treated by personalizing solutions to patient care.
www.BioOncology.com
© 2011 Genentech USA, Inc. All rights reserved. BIO0000330901 Printed in USA.
S:14.25”
S:10”
Trim: 15.5”
Trim: 10.5”
Bleed: 17”
Bleed: 11.125”
Page Trim: 7.75”
Safety: 7”
Page Trim: 7.75”
Grind Off: .125” Grind Off: .125”
Safety: 7”
BIONP-42742A_M03_Asz_UPdt.indd3-30-2011 3:59 PM Dan Capobianco / John Gluth
Client CodeClient
LiveOverall TrimBleed
# of Colors
BIO0000330901GENENTECH
14.25” x 10”15.5” x 10.5”17” x 11.125”
4C
Job info
NoneNotes Fonts
Trade Gothic (Medium, Bold No. 2), TT Slug OTF (Regular)
ImagesBioOnc_Glider-Horz_HR.tif (CMYK; 532 ppi; 56.34%), Gene_Logo_KO_T.ai (70.15%), BioOnc_WM_R_4C.ai (60%)
Inks Cyan, Magenta,
Yellow, Black
Fonts & Images
Saved at
None
from dcapobianco3057 by
Printed At
Taking a broader view —charting a unique course in cancer care
At Genentech BioOncology, not only are we leading the fight against cancer with innovative science, but we’re also dedicated to supporting patients and others within the oncology community.
A commitment to patients — We created Genentech BioOncology™ Access Solutions®, a single source for all access and reimbursement issues, so healthcare providers can remain focused on patient care.
Reducing barriers to treatment — We help make treatment possible for patients in financial need through our BioOncology Co-pay Card Program and ongoing charitable donations to various independent, nonprofit organizations in support of co-pay assistance.
A commitment to care — Our first product was approved in 1985, and since then we have donated approximately $2.3 billion in medicine to uninsured patients through the Genentech® Access to Care Foundation and other donation programs.
Our goal is to fundamentally change the way that cancer is treated by personalizing solutions to patient care.
www.BioOncology.com
© 2011 Genentech USA, Inc. All rights reserved. BIO0000330901 Printed in USA.
S:14.25”
S:10”Trim: 15.5”
Trim: 10.5”
Bleed: 17”
Bleed: 11.125”
Page Trim: 7.75”
Safety: 7”
Page Trim: 7.75”
Grind Off: .125” Grind Off: .125”
Safety: 7”
16 | April 2012
A Word from Your felloWs
Many of us training in the United States have encountered patients and their families from resource-limited regions of the world—families who have uprooted themselves for the chance
to save the lives of their children diagnosed with cancer. This will not come as a surprise when you review the cancer survival rates worldwide. The United States’ current 5-year overall survival rate for childhood cancers is 80%. Compare this with 30% for childhood cancers in Colombia, 20% for acute lymphoblastic leukemia (ALL) in Malawi, and close to 0% for most childhood cancers in Ethiopia. An estimated 100,000 children worldwide who die without treatment do so without access to palliative care.
It is estimated that 70% of the children with cancer in developing nations with cancer receive substandard
care, if any care at all. The incidence and mortality of cancer in the United States has declined dramatically over the past 50 years because of increased awareness, prevention, earlier detection, and increasingly effective treatment protocols. After reading numbers like these in developing countries, it behooves us as future pediatric hematologists/oncologists to help eliminate this disparity, especially since many childhood cancers are highly curable. So how can we make the biggest difference? Sharing our knowledge effectively with the rest of the world is a great start.
Bridging the GapTwinning programs, developed by the St. Jude’s Children Research Hospital, have become a successful model to
Providing Oncology Services in Impoverished CountriesBy Diana Osorio, MD
April 2012 | 17
help bridge this gap. Twinning partners high-income countries with resource-limited institutions to share information, organizational skills, and technology. One example is the Instituto Materno Infantil de Pernambuco, a St. Jude’s partner hospital in Recife, Brazil, which showed dramatic improvements after twinning with St. Jude’s by its markedly reduced rates of abandonment of treatment, relapse, and death due to toxic effects of treatment.
Another outstanding example of well-appointed funds exists in Egypt. Through a unique fund-raising strategy via the Association of Friends of (Egypt’s) National Cancer Institute, Egypt’s Children’s Cancer Hospital 57357 (http://beta.57357.com) opened in 2007 in El-Saida Zenab. This very modern facility has been able to change Egypt’s cancer survival rates from less than 40% to 75% to 80%.
Other ResourcesThe Cure4Kids website is a tremendous resource for oncologists all over the world (www.cure4kids.org). Many other institutions have built international initiatives, including Baylor College of Medicine, Dana Farber Cancer Institute, Children’s Hospital Los Angeles, and Georgetown University, among others. A well-established international organization is the International Network for Cancer Treatment and Research (INCTR; www.inctr.org), which is headquartered in Brussels, Belgium, and has branches in Brazil, Canada, Egypt, France, Nepal, Cameroon, India, Tanzania, the United Kingdom, and the United States. Among its many tasks, INCTR has successfully devised lower-cost protocols for ALL and lymphoma; provided education and training for cancer treatments; and supplied supportive care, psychosocial support, and palliative care. The International Society of Paediatric Oncology (SIOP) holds annual conferences worldwide and is an excellent medium for sharing information. The International Confederation of Childhood Cancer Parent Organizations (ICCCPO) spans 5 continents and follows in this same vein, as does the World Child Cancer organization (www.worldchildcancer.org). Other outstanding organizations include the Asociación Hematología y Oncología Pediátrica Centro Americana (AHOPCA) and the Union for International Cancer Control (UICC).
In June 2011, Princess Dina Mired, director general of the King Hussein Cancer Foundation, delivered a keynote speech at the United Nations intended to bring awareness to noncommunicable diseases that include cancer, heart disease, diabetes, and chronic respiratory illnesses. These 4 categories of illness account for more deaths worldwide than all other causes combined. This is an example of how cancers, including pediatric cancer, are gaining recognition and how the geographic inequalities in treatment are beginning to be addressed.
http://beta.57357.com
www.cure4kids.org
www.inctr.org
www.worldchildcancer.org

A Word from Your felloWs
18 | April 2012
On the Ground in MalawiA close friend of mine, Nader Kim El-Mallawany, MD, is a recent pediatric hematology/oncology graduate who has been working for the past 2 years in Malawi, a country in southeast Africa that has been hit hard by the AIDS epidemic. His work there has primarily centered on patients who are HIV-positive and have Kaposi sarcoma (KS)—specifically, trying to improve the diagnostic and therapeutic approaches for these patients.
“We have about 20 to 25 children diagnosed with KS per year in our clinic, and this is probably an under-representation of the true numbers of children with KS in the surrounding areas, because very few clinicians are aware of the nuances of presentation of KS in children,” said El-Mallawany.
He also supports the pediatric oncology ward in the central hospital. “The most common diagnosis is Burkitt lymphoma, but certainly children present with a wide array of different diseases, including leukemia, solid tumors, Hodgkin disease, and other non-Hodgkin lymphomas,” he said.
“Because there is a paucity of subspecialists in this setting, teaching is one of the most important tools we can provide,” El-Mallawany noted. “We can significantly improve outcomes for common diagnoses by providing fundamental tools and carefully constructed protocols that are sensitive to the available resources and practical limitations that clinicians encounter.”
He finds his work in Malawi “rewarding, more so than any other work I have ever done.” He said, “Small and simple interventions can have very positive effects for
the patients and their families. Yet at the same time, the work can be frustrating when you consider the limitations imposed upon us by the severe shortage of resources. Therefore, with time, you come to figure out how to bridge the gap between these 2 extremes and try to provide the most effective therapeutic approach for the patients.”
El-Mallawany encourages international outreach because “there are very few subspecialists in the region bringing knowledge and teaching to local clinicians. Our colleagues throughout the world are trying their best to overcome the challenging situations that they struggle with on a daily basis, and empowering them with the sustainable tools to carry on treating pediatric cancers will be valuable for years to come.”
So how did he make this a reality? “Ultimately, it was simply a matter of deciding to make the move and finding the right opportunity,” he stated. He said that he made this decision “understanding that in a field like oncology, we cannot expect to go somewhere that is lacking so many resources and try to deliver the exact same approach as that which we are used to in the Western world.” El-Mallawany continued, “Yet nonetheless, we can try to effect systematic changes that aim to improve the outcomes and opportunities for individual children.”
Fellows who travel to other countries to help should not expect to work only in their field. El-Mallawany noted that they will need to “be aware of the context in which healthcare programs are trying to deal with diseases like cancer. When millions of children around the world still die of easily curable illnesses like malaria, diarrhea, pneumonia, measles, tuberculosis, malnutrition, etc, we must understand that our approach as pediatricians and as hematologist/oncologists should be driven by a goal to improve child health overall.”
Diana Osorio, MD, is a pediatric hematology/oncology fellow at Steven and Alexandra Cohen Children’s Medical Center in New Hyde Park, New York.
“Small and simple interventions can have very positive effects for the patients and their families. Yet at the same time, the work can be frustrating when you consider the limitations imposed upon us by the severe shortage of resources.”
As hematology/oncology fellows, we work with colleagues from multiple specialties. However, the majority of our interactions are with the internal medicine service, so here we will help you to
maximize the quality of your interactions with internal medicine residents. In the following paragraphs, you will find many ideas that if followed will not just help you to “do your time” during fellowship, but contribute to the internal medicine residency program. And who knows, you just might inspire a resident to pursue oncology as a career!
Generally, fellows work with internal medicine residents on the consultation service and on the inpatient oncology service. Thus, I will focus on these settings. At the end, there are also some general considerations that can be applied throughout your fellowship.
The Consultation ServiceThe consultation service is the bread and butter of the hematology/oncology fellowship. As a future consultant, you are expected to develop the skills nec- essary to become an effective and efficient team player. Remember, you have been consulted for clinical guid- ance in answering a question, no matter how simple it may seem to you. The following is a list of points to consider:
Do not belittle a consult. Residents are not born hema-tologists/oncologists—there is a reason why they are consulting you. Belittling a consult only creates tension between the consultant and primary team. Treat every consult as a learning and teaching opportunity.
How Fellows Can Add Value to Their Internal Medicine Residency ProgramBy Cyrus Khan, MD, and Zachariah DeFilipp, MD
April 2012 | 19

A Word from Your felloWs
20 | April 2012
Understand the questions being asked. It is imperative to know what questions the consulting team are asking. This is best clarified by speaking to the primary team directly. Oncology patients frequently have multiple problems. You do not want to write a detailed note regarding manage-ment of lung cancer when help is requested to evaluate thrombocytopenia.
Establish the urgency of the consult. Once again, this is best established by speaking directly to the consulting team. As fellows, we receive many consults of varying urgencies. Tri-age is of utmost importance. A 5 pm consult for thrombotic thrombocytopenic purpura is very different from a 5 pm consult for a mild chronic anemia.
Gather all patient-related information yourself. For an effective consult, every piece of clinically relevant data must be known. If this requires calling different offices and physicians, it is far more efficient to do it yourself than to delegate it to the primary team. We are often searching for specific information from a hematology/oncology perspective, which the primary resident may not yet be qualified to address. Not only is this a fel-low’s responsibility, but it also expedites the consult, preventing the patient and primary team from waiting in limbo.
Communicate recommendations. When you’re finished writing your note, it is best to call the resident on the con-sulting team and verbally communicate your recommenda-tions. Most training programs require that consultants not place orders on patients and instead allow the primary team to write all orders. This prevents multiple orders on the same patient and also serves as an opportunity for resident teach-ing. Speaking with the residents also results in quicker im-plementation of your recommendations. If you are unsure about the specifics of a recommendation, check with your attending before writing them down.
Do not offer unsolicited advice. It is important to under-stand your role as a consulting fellow. It may seem natural to comment on issues like electrolyte disturbances, hyper-tension, and diabetes with recommendations on how to correct them. This is especially true for first-year fellows who are just coming out of residency and are used to man-aging every aspect of patient care. These comments are of-ten not welcomed by the primary team or other consulting specialties. Thus, it is probably better to stick with making recommendations specific to your expertise, unless there is a glaring issue.
Provide educational material. Providing an article address-ing the consulting topic improves patient care and resident education. Not only will this give credence to your recom-
mendations, but it will serve as testament to your com-mitment to resident teaching. The extra effort to provide education today may even save you an extra consult on a busy day.
Provide appropriate follow-up. Your role as a consultant does not end with the initial consult. It is your professional responsibility to provide appropriate follow-up until the primary team is satisfied that their question has been an-swered. Consultation can conclude when the primary team feels comfortable managing the issue for which you were consulted.
The Inpatient ServiceMany programs have inpatient oncology, hematology, or bone marrow transplant services with resident and fellow coverage. The fellow serves as the junior attending and is encouraged to make decisions regarding patient care, as well as to take an active teaching role. It is important to make these services worthwhile for residents so that instead of considering the rotation a burden, they see it as an exceptional educational experience.
Treat residents as your colleagues. Do not consider resi-dents as simply “help.” They should be treated respect-fully, and it is your responsibility to look after their well-being. The service runs far smoother if the resi-dents feel they are part of the team and not just there to do grunt work.
Respect the residents’ time. Learn to run an efficient ser-vice from the get-go. As the liaison between the attending and the residents, you will be in the best position to coor-dinate a smooth service. This ensures that the resident’s time is not wasted waiting for rounds to finish, etc.
Teaching. Teach residents on a daily basis. Be it a 5-min- ute talk on common hematology/oncology topics or re-viewing board questions, residents will appreciate your commitment to education. With education incorporated into resident interactions, the internal medicine program will see the value and continue to staff the inpatient oncol-ogy service with residents. Minimize scut work. Try to help out the residents from time to time in areas where there is no educational value, such as appointment scheduling and gathering outside records. This goes a long way in establishing rapport with your residents.
General ConsiderationsOutside of the 2 major settings described, there are many other opportunities to contribute to the internal medicine program.

Natio
nal C
ance
r Ins
titut
e
Your source for information on clinical trials atNCI’s Center for Cancer Research (CCR) is
now smartphone friendly. Visit our easy-to-navigatemobile Web site for information on the more than150 cancer clinical trials now enrolling at the NationalInstitutes of Health in Bethesda,MD.
CCR is currently conducting trials for many typesof cancer including:
• Prostate Cancer • Lung Cancer•Thymoma • Pediatric Sarcoma• Kidney Cancer • Brain Cancer
To learn whether your patients may be eligible,visit
bethesdatrials.cancer.gov or call
1-888-NCI-1937 (1-888-624-1937)
41594-NIH CSSC Oncology Net Ad-v5 8/4/10 2:53 PM Page 1
Attend morning reports as a subject expert. Hematology/oncology patients are invariably presented at morning re-port. Since it is hard to be well versed in our specialty at a resident’s level, it is of great benefit to the program to attend these sessions. This develops a healthy relationship between yourself and the program and establishes your commitment to resident education.
Help with board reviews. Another area where you can pitch in is at board review sessions. Many internal medicine programs will arrange these sessions for their third-year residents. You can provide guidance in how to approach he-matology/oncology questions and identify the key issues. This is an easy way to enhance the quality of the internal medicine program and cement resident-appropriate teach-ing points.
Help with research. In every program, there are residents aspiring to be fellows like yourself. They will invariably want to get involved in research projects. Attendings are often hard to get a hold of, so you can serve as a great re-source. Include residents in your research or develop ideas with them that they can pursue on their own. This act of goodwill will help them advance their careers.
Following the above advice will not only help you train as an effective teacher and team player, but will add immense value to the internal medicine residency program. As future hospitalists and internists, today’s residents will look to your teachings in their care of patients with hematological or oncological problems. In the end, remember this twist on the famous quote by John F. Kennedy: “Ask not what your residency program can do for you, ask what you can do for your residency program.” ■
Cyrus Khan, MD, is chief fellow in the hematology/oncology fellowship program at the West Penn Allegheny Health System in Pittsburgh, Pennsylvania. He is planning a career in hematopoietic stem cell transplantation.
Zachariah DeFilipp, MD, is a second-year internal medicine resident at the West Penn Allegheny Health System in Pittsburgh, Pennsylvania. He is planning to apply for a hematology/oncology fellowship in the upcoming year.

22 | April 2012
A Word from Your felloWs
Cloud computing refers to Web-based programs that allow the user to store information in a central location, typically not the device being used to access the information (such as your
laptop, desktop PC, or iPad). In this article I will describe 4 valuable programs that I have discovered during my fellowship: Evernote, Dropbox, GoodReader, and EndNote.
EvernoteUpon reflection, most senior fellows realize that they entered their fellowship with just a small fraction of the specialty knowledge that they have today. During the course of our training we acquire little gems of knowledge from our peers and attendings, and many times we write these down on little pieces of paper, on the back of patient lists, and on small steno notepads. The problem with this method is that there is no way to arrange, rearrange, or efficiently search the accumulated information.
Fortunately, I discovered the free program Evernote (www.evernote.com), a cloud-based note-taking program
that is available for Mac OS X, Windows, BlackBerry, Apple iOS, and Android. The iOS program comes with an iPhone/iPod Touch version as well as a version scaled natively for the iPad. Regardless of on which device a note is made or edited, it is automatically synchronized to the cloud.
Evernote has a Web-browser interface, so you can access and update without having to download the program to each computer. When an update is made with Evernote through any of your devices, the changes are synchronized when logging onto another device. Everything is updated all the time. Evernote can be a repository of information from books, but also more practical information learned in clinic and on wards. These small bits of information can be arranged however you like. But the icing on the cake is being able to search through your notes. Don’t remember the TKI resistance mutations? Search your Evernotes and they will come back to you.
Sharing is another nice feature of Evernote. If you feel your notes would be helpful to the incoming class of fellows, it is simple to designate a folder or folders to
Cloud Computing for Fellows By Jonathan Ticku, MD

April 2012 | 23
be shared with other Evernote users. This can be simple information, such as frequently called telephone numbers, or more complex material, like the initial workup of a particular disease. The sharing feature is helpful for rotating residents on the hematology or oncology service.
The word processor–like interface of Evernote is basic, with only simple formatting available, so it is not nearly as encompassing as a stand-alone word processor. This may be a limitation for some users. Another drawback for some may be the data limit. Each user has an upload limit of 60 MB per month with unlimited storage. There is also a cap on data transfers per month, but additional storage and data transfer can be purchased. (I’ve never even come close to the monthly data limit.)
DropboxAnother issue that you undoubtedly deal with is the accumulation of journal articles that are printed and then end up in a huge stack on your desk. Why not use a cloud-based program for this as well? I found that Dropbox (www.dropbox.com) is a very useful program to store those PDF articles—and many other things, too. The articles can be saved to the Dropbox folder and accessed through the Dropbox app (on iPhone, iPod Touch, iPad, Android, and BlackBerry devices) or they can be downloaded to your Windows, Mac, or Linux computer. Dropbox is basically just a shared folder that is synchronized in the cloud.
GoodReaderAn even more powerful, robust app to use for articles is GoodReader (http://www.goodiware.com/goodreader.html), especially if you have an iPad. There is also GoodReader for iPhone and iPod Touch, but these are different apps than the iPad version. It is not free, but for $4.99 GoodReader is still a great deal as it allows you to annotate PDF articles directly on any of these devices. The articles are managed locally on the device rather than in a folder in the cloud, but the Dropbox folder can be integrated into GoodReader.
EndNoteYou will probably also need to write research papers or protocols during training. Although it is neither free nor inexpensive (the full Windows and Mac versions are $249.95 for a download, and upgrades are $99.95 for a download), the EndNote (www.endnote.com) program, which makes your research and citation tasks much simpler, is used by many fellows. EndNote has also begun to utilize the cloud as well. Instead of having to carry a USB thumb drive with all the EndNote data files, you can access the EndNote website’s cloud system for online storage. This online library allows you to synchronize citations later, especially when you are working with multiple computers.
As we move forward in our oncology/hematology careers, there will be an ever-increasing amount of information to handle. The use of programs like Evernote, Dropbox, GoodReader, and EndNote can help us become efficient at managing and consolidating this information. As a note of caution, these programs should never be used for HIPAA-protected information such as sign-outs or patient notes.
Jonathan Ticku, MD, is a second-year hematology/oncology fellow with Orlando Health/MD Anderson Cancer Center Orlando in Florida.
www.evernote.com
www.dropbox.com
www.endnote.com
http://www.goodiware.com/goodreader.html
24 | December 2011
Everybody is aware that career choices in oncology abound these days. But when you ask fellows what job they are interested in once they complete their fellowship, many just don’t know—even
in their third year. This isn’t surprising, because we’re so busy with patient care and learning more about oncology and hematology that little time is left to contemplate our careers after fellowship. Instead, our time is spent adapting to our new fellowship training programs in our first year and then consolidating our knowledge in our second year. Then before we know it, it is time to apply for a job. Although we have waited for this opportunity for many years, now that it’s arrived most of us feel ill-equipped to make a decision. For this reason, organizing an oncology/hematology fellows’ career day is very important.
A fellows’ career day is best held in an informal setting—and ideally with the involvement of a few local hospitals’ fellowship programs. You should invite a diverse group of fellows so as to ensure that everyone is exposed to a number of career choices. In my opinion, the career day is best held between September and December, as the first-year fellows have by then adapted to their respective programs, second-year fellows have not started looking for a job, and third-year fellows are gearing up to sign their employment contracts. There are a few key elements that should be covered in the career day, which I will discuss here.
Career OptionsClearly, career options will be the primary theme of your career-day program. Almost all careers in oncology can be categorized into 3 areas: academic practice, community-based practice, and practice in industry or government. According to FREIDA Online, almost as many oncology fellows go into academia as community practice.1 So, it is important that both fields be equally represented. While the goal of academic practice is patient care, research, and teaching, community oncology is more focused on patient care. Most fellows already know about academic-based practice because most fellowship programs are based in academic institutions (of course), but it is still useful to get a faculty member’s perspective on the pros and cons of academia. Also, for the appropriate audience, discussing career choices in basic lab research will be helpful. On the whole, however, most fellows are less familiar with community oncology practice. It will be very helpful to have an open
conversation among practitioners from these 2 disciplines to discuss the various aspects of these career tracks.
Whereas the majority of fellows go into either community or academic practice, careers in industry or pharmaceuticals are less common. And to be frank, oncology fellows rarely go into the pharmaceutical industry or the FDA; however, given the current scenario of a rapidly growing drug armamentarium, this is becoming a more attractive option. Having people from industry interact with the fellows will open your eyes to career options beyond the traditional choices.
Physician Recruitment ProcessIt’s not enough to merely learn about the nitty-gritty details of various career options; it is also important that fellows learn the basics of launching a career search. It is helpful to discuss the appropriate time to start a job search, resources to use during your search, tips on writing your CV, the qualities or accomplishments that each career choice requires, how to prepare for the interview day, and what questions to ask during the interview.
Physician recruitment agencies are a great resource, so try to have at least 1 such representative at your career day. As you’re undoubtedly aware, most fellows receive job offers from the time they start their fellowships. But it is important to match your needs with the appropriate job description. The physician recruitment agencies can get basic information from you, determine what you’re looking for, and match it to the appropriate jobs. There’s no sense in going through hundreds of job advertisements when you have a certain job description in mind. If you have visa restrictions, for example, it is no use seeking a job at an employer that does not sponsor your particular visa.
Contract NegotiationContract negotiation is an important aspect of starting a job, yet no fellow is ever trained in it. Although most fellows hire a lawyer, that won’t help them learn about the various contract terms. Ultimately, it is you who will be up all night taking extra calls, even when you were told in the contract that calls would be “equitable.” (Yes, I learned that equitable doesn’t mean “equal”!) Also, many lawyers are not that familiar with contract negotiation in the health care fields, so you should retain a lawyer experienced in these matters who can highlight the important points in the contract.
Organizing a Fellows’ Career DayBy Aman Garsa, MD
transitions
24 | April 2012

April 2012 | 25
Visa ProcessingWith nearly half of all fellows being international medical graduates, it goes without saying that visa concerns should not be ignored.1 With particular job restrictions and J-1 waiver/H1-B visa processing methods in the United States, most fellows are in the dark about how to go about finding the right job with their particular visa. A great addition to your career day, if it can be arranged, would be an immigration expert and/or lawyer or an agency that deals with visa applicants. Because this might be relatively useless for fellows who are not in the United States on a visa, it might be a good idea to present this information at the conclusion of the career day or at an after-hours meeting for interested people only.
Board CertificationFellowship is all about learning and expanding your knowledge, but the ultimate test of your efforts will be the medical examining boards. Given that preparation for these boards and finding a job go hand in hand, it will be a good idea to teach attendees the best methods of preparation for their boards. Also appreciated will be advice on how to obtain state licensures and CME requirements.
Role of New PhysiciansLife after fellowship is another important area to cover at your career day. This is most important for third-year fellows, because once you sign on the dotted line of your contract you’ll be on your way to your new career. It will be crucial for you to learn how to contribute profitably to your practice, how to make contacts, how to approach difficult cases, and whom to ask for help.
Oncology is a difficult field emotionally; most of us already have experienced this downside of our field. And it doesn’t make it easier when you become an attending physician to learn that you are the person who is solely responsible for making potentially life-altering decisions for your patients. For example, maybe you chose a particular chemotherapy
regimen that your patient did not tolerate well, and she ended up having an adverse event or even dying. How do you deal with this situation? Or when do you decide you’ve tried enough and it’s time to let your patient go? As a new attending physician, how will you continue to maintain your inner peace and empathy? This would be a great philosophical discussion to have at the career day.
Its drawbacks aside, oncology is an exciting field to be in. Most fellows (>99%) will be employed at the end of their training program.1 And with the anticipated shortage of 3800 oncologists by 2020, the demand far exceeds the supply.2 A fellows’ career day is an ideal opportunity for you to learn and explore your career possibilities. Its goal is to ensure that each fellow gets something out of it. By the end of the day, the first-year fellows should know their career options and best resources for boards preparation, the second-years should know how to embark on the process of job hunting, and the third-years should learn about contract negotiation and how to prepare for their roles as new independent physicians. With a bit of planning, your fellows’ career day will be a great learning experience for all attendees. ■
Aman Garsa, MD, is a second-year hematology/oncology fellow at the Western Pennsylvania and Allegheny General Hospital in Pittsburgh.
RefeRences1. American Medical Association. FREIDA Online. http://www.ama-assn.org/ama/pub/education-careers/graduate-medical-education/freida-online.page. Accessed February 2, 2012.2. Hortobagyi GN. A shortage of oncologists? The American Society of Clinical Oncology workforce study [published online ahead of print March 14, 2007]. J Clin Oncol. 2007;25(12):1468-1469. doi:10.1200/JCO.2007.10.9397.
26 | April 2012
The Online Oncologist™
Mobile Medicine: Apps for the heAlth cAre professionAl
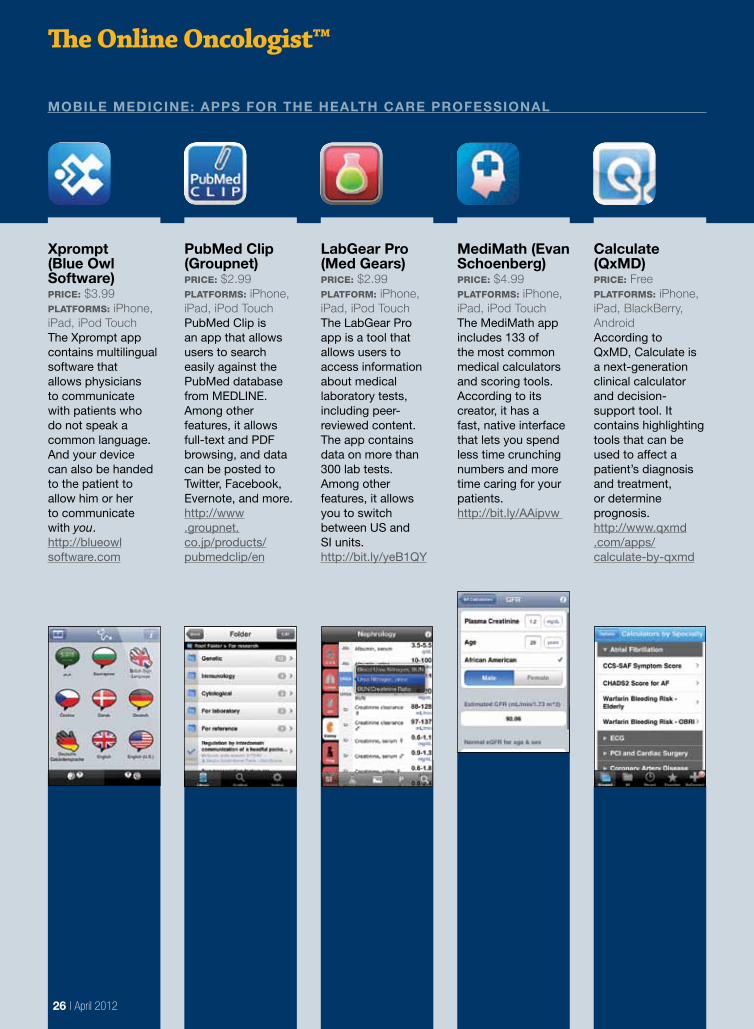
Xprompt (blue owl software)Price: $3.99Platforms: iPhone, iPad, iPod TouchThe Xprompt app contains multilingual software that allows physicians to communicate with patients who do not speak a common language. And your device can also be handed to the patient to allow him or her to communicate with you.http://blueowl software.com
pubMed clip (Groupnet)Price: $2.99Platforms: iPhone, iPad, iPod TouchPubMed Clip is an app that allows users to search easily against the PubMed database from MEDLINE. Among other features, it allows full-text and PDF browsing, and data can be posted to Twitter, Facebook, Evernote, and more. http://www .groupnet.co.jp/products/pubmedclip/en
labGear pro (Med Gears)Price: $2.99Platform: iPhone, iPad, iPod TouchThe LabGear Pro app is a tool that allows users to access information about medical laboratory tests, including peer-reviewed content. The app contains data on more than 300 lab tests. Among other features, it allows you to switch between US and SI units.http://bit.ly/yeB1QY
MediMath (evan schoenberg)Price: $4.99Platforms: iPhone, iPad, iPod TouchThe MediMath app includes 133 of the most common medical calculators and scoring tools. According to its creator, it has a fast, native interface that lets you spend less time crunching numbers and more time caring for your patients.http://bit.ly/AAipvw
calculate (QxMd)Price: FreePlatforms: iPhone, iPad, BlackBerry, AndroidAccording to QxMD, Calculate is a next-generation clinical calculator and decision-support tool. It contains highlighting tools that can be used to affect a patient’s diagnosis and treatment, or determine prognosis. http://www.qxmd .com/apps/calculate-by-qxmd
By the Numbers
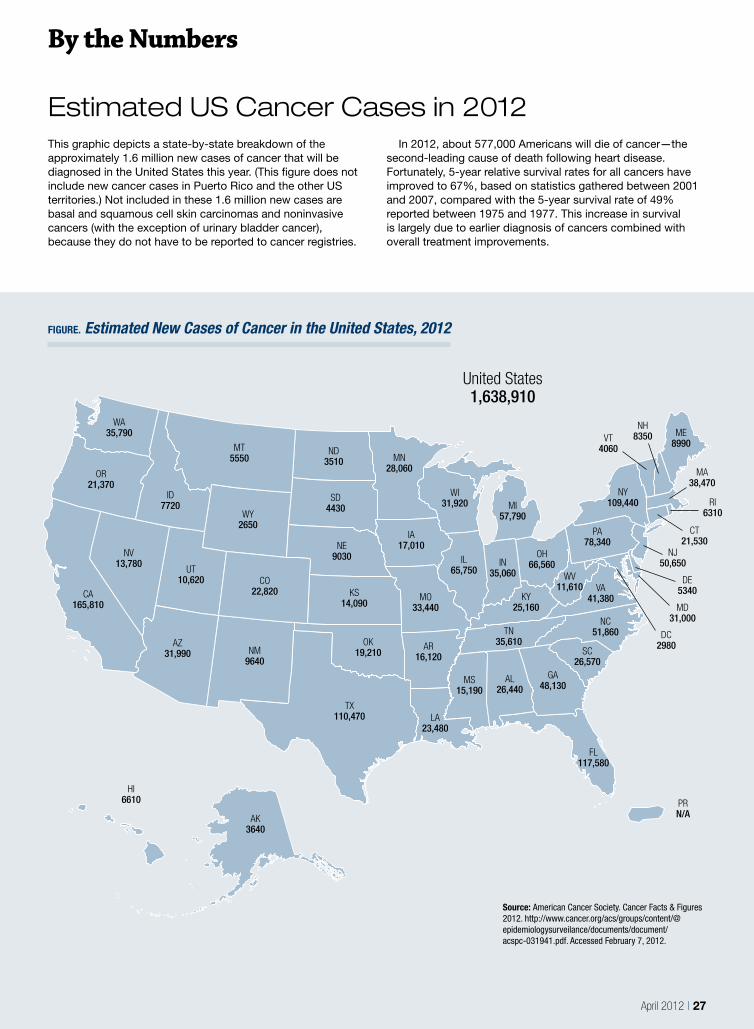
Estimated US Cancer Cases in 2012This graphic depicts a state-by-state breakdown of the approximately 1.6 million new cases of cancer that will be diagnosed in the United States this year. (This figure does not include new cancer cases in Puerto Rico and the other US territories.) Not included in these 1.6 million new cases are basal and squamous cell skin carcinomas and noninvasive cancers (with the exception of urinary bladder cancer), because they do not have to be reported to cancer registries.
In 2012, about 577,000 Americans will die of cancer—the second-leading cause of death following heart disease. Fortunately, 5-year relative survival rates for all cancers have improved to 67%, based on statistics gathered between 2001 and 2007, compared with the 5-year survival rate of 49% reported between 1975 and 1977. This increase in survival is largely due to earlier diagnosis of cancers combined with overall treatment improvements.
April 2012 | 27
FIGURE. Estimated New Cases of Cancer in the United States, 2012
Source: American Cancer Society. Cancer Facts & Figures 2012. http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdf. Accessed February 7, 2012.
WA35,790
OR21,370
CA165,810
NV13,780
ID7720
MT5550
WY2650
UT10,620
AZ31,990 NM
9640
CO22,820
ND3510
SD4430
NE9030
KS14,090
OK19,210
TX110,470 LA
23,480
AR16,120
MO33,440
IA17,010
MN28,060
WI31,920
IL65,750
MS15,190
AL26,440
TN35,610
SC26,570
NC51,860
VA41,380KY
25,160
IN35,060
MI57,790
OH66,560
WV11,610
PA78,340
NY109,440
VT4060
NH8350 ME
8990
MA38,470
RI6310
CT21,530
NJ50,650
DE5340
MD31,000
DC2980
PRN/A
United States1,638,910
AK3640
HI6610
GA48,130
FL117,580

28 | April 2012
Conference Center
2012 Oncology & Hematology Meetings
March 14-1729th Annual Miami Breast Cancer ConferenceMiami, FLhttp://bit.ly/nkDSmS
March 21-24SSO 65th Annual Cancer SymposiumOrlando, FLhttp://www.surgonc.org/meetings--events/annual-cancer-symposium.aspx
March 25-282012 Annual Meeting on Women’s CancerAustin, TXhttp://www.sgo.org
March 30-319th International Symposium on Ovarian Cancer and Other Gynecologic MalignanciesNew York, NYhttp://bit.ly/tHCyBP
March 315th Annual Interdisciplinary Prostate Cancer CongressNew York, NY http://bit.ly/yU8G5b
May 3-637th Annual ONS CongressNew Orleans, LAhttp://www.ons.org/CNECentral/Conferences/Congress
July 27-29Gynecologic Oncology Group Semiannual MeetingBoston, MAhttp://www.gog.org/meetinginformation.html
August 10-1210th International Congress on Targeted Therapies in CancerWashington, DChttp://bit.ly/wJ2t32
May 9-12ASPHO 25th Annual MeetingNew Orleans, LAhttp://bit.ly/yZ0fWC
June 1-548th Annual ASCO MeetingChicago, ILhttp://chicago2012.asco.org/
June 14-17Radiation Therapy Oncology Group MeetingPhiladelphia, PAwww.rtog.org
July 19-2213th International Lung Cancer CongressHuntington Beach, CAhttp://bit.ly/yb4SbB
July 26-2811th International Congress on the Future of Breast CancerCoronado, CAhttp://bit.ly/zpo6AO
Hote
l del
Cor
onad
o ph
oto
by J
ohn
Mar
cini
ak
Call for PaPersWe welcome submissions to Oncology Fellows, a publication that speaks directly to the issues that matter most to hematology/oncology fellows at all stages of training. Oncology Fellows aims to provide timely and practical information that is geared toward fellows from a professional and lifestyle standpoint—from opportunities that await them after the conclusion of their fellowship training, to information on what their colleagues and peers are doing and thinking right now.
Oncology Fellows features articles written by practicing physicians, clinical instructors, researchers, and current fellows who share their knowledge, advice, and insights on a range of issues.
We invite current fellows and oncology professionals to submit articles on a variety of topics, including, but not limited to:
• Lifestyle and general interest articles pertaining to fellows at all stages of training.
• A Word From Your Fellows: articles written by current fellows describing their thoughts and opinions on various topics.
• Transitions: articles written by oncology professionals that provide career-related insight and advice to fellows on life post-training.
• A Day in the Life: articles describing a typical workday for a fellow or an oncology professional post-training.
The list above is not comprehensive, and suggestions for future topics are welcome. Please note that we have the ability to edit and proofread submitted articles, and all manuscripts will be sent to the author for final approval prior to publication.
If you are interested in contributing an article to Oncology Fellows, or would like more information, please e-mail Donna Bonura at [email protected].
With CancerCare, the difference comes from: • Professional oncology social workers• Free counseling • Education and practical help• Up-to-date information • CancerCare for Kids®
For needs that go beyond medical care, refer your patients and their loved ones to CancerCare.
CancerCare’s free services help people cope with the emotional and practical concerns arising from a cancer diagnosis and are integral to the standard of care for all cancer patients, as recommended by the Institute of Medicine.
makes all the difference
®
1-800-813-HOPE (4673)
www.cancercare.org
Help and Hope
41960ALT_Queen_v1 1 5/13/08 10:03:26 AM