congenital toxoplasmosis dr.omar h.amer prof.of parasitology
TRANSCRIPT

CONGENITAL TOXOPLASMOSIS
Dr.Omar H.Amer
Prof.of Parasitology
Objectives
State the ways of transmission of the disease to the fetus
Describe the pathogenesis pathway for congenital toxoplasmosis
Discuss the clinical significance of the infection Define significance of detection of IgM and IgG Discuss different methods for management the disease
in mother and infant Describe the main aspects of prevention and control . Mode transmission of congenital toxoplasmosis Pathogenesis of congenital toxoplasmosis Significance of congenital toxoplasmosis Treatment and management of congenital toxoplasmosis

What causes Toxoplasmosis?The protozoan Toxoplasma gondii, is a coccidian, obligate, intracellular parasite responsible for zoonotic infections in man and other mammals

Congenital Toxoplasmosis
Congenital transmission happens when the mother is exposed to infection by Toxoplasma gondii for first time while she is pregnant.
The effect on the foetus depends on the time of infection during pregnancy.

Host
Definitive host (final host):-Only Cat
Accidental host (Non specific host) :-All mammals including Man, Farm animals,Rat,Mice and Avian (harbor asexual stages).

What causes Toxoplasmosis?

Site of infection
In definitive host:- Intra-cytoplasmic epithelial cells of small intestine.
In accidental host ( Man):-Reticuloendothelial system , brain and retinal cells.

Primary Transmission of Toxoplasmosis
Ingesting cysts Raw or undercooked meat
Especially pork, mutton Ingesting oocysts
Accidental ingestion of feline feces Contaminated dirt at playgrounds or
sandboxes Hands contaminated when changing
litter boxes

Ways of Infection
Oral intake of raw or rare ("under-cooked") meat or of contamination with cats feces or consumption of contaminated vegetables, fruits, and salad, ...
A fresh maternal infection during pregnancy can lead to an infection of the placenta.
Congenital Toxoplasmosis results from transplacental infection of the fetus during pregnancy.

Transmission Cycle
DEFINITIVE HOST (cat)
Cysts ingestedby cat
Unsporulated oocyst passed in feces
Sporulatedoocyst
Intermediate host ingests oocysts in
feed, water, or soil
Cysts containing bradyzoitesin tissues of intermediate hosts
INTERMEDIATE HOSTS
Contamination offood and water
Ingests cystsin infected meat
Infection of fetus
Tachyzoitestransmittedthrough placenta

life-cycle for Toxoplasma gondii
The asexual stages of T. gondii can cause disease
in humans and most animals . There are two asexual forms. The first form, called tachyzoite,( fast replicating form) can invade all
types of cells and divides rapidly, leading to cell death .
The second form, called the bradyzoite, divides slowly and forms cysts, most prominently in muscle and brain. Tissue cysts can be ingested
by a cat where they undergo sexual reproduction and oocyst formation.

Toxoplasma gondii – Life cycle
Oocyst
Tachyzoite
Bradyzoite

Transplacental Transmissionof Toxoplasmosis
Occurs when primary infection occursduring pregnancy Risk and severity vary depending on
the trimester in which infection occurs 1st trimester: 15% of fetuses infected 2nd trimester: 30% of fetuses infected 3rd trimester: 60% of fetuses infected But the earlier in pregnancy the
infection occurs, the more severe the fetal infection

Congenital Toxoplasmosis
A)Frist trimester…… Abortion B)Second trimester…
StillbirthC)Third trimester…
Infection may be present as:-Hydrocephaly,
Neonatal jaundice . Mental retardation.

Congenital Toxoplasmosis
The consequences of the infection of the fetus can be very different: between subclinical and very serious.
Abortion Overt disease. The symptoms vary widely, the classical triad of Congenital Toxoplasmosis is Hydrocephalus
Intracranial calcification
Chorioretinitis

Complications of toxoplasmosis
Complications list for Toxoplasmosis: The list of complications that have been mentioned in
various sources for Toxoplasmosis includes: Complications of a pregnant women becoming newly
infected with toxoplasmosis: Spontaneous abortion - in affected pregnant women Stillbirth - in affected pregnant women
Fetal or newborn complications of a pregnant woman with toxoplasmosis: Congenital toxoplasmosis - passed to newborn by
infected mother by cross-placental contagion. Neonatal jaundice Newborn brain disorders Newborn eye disorders

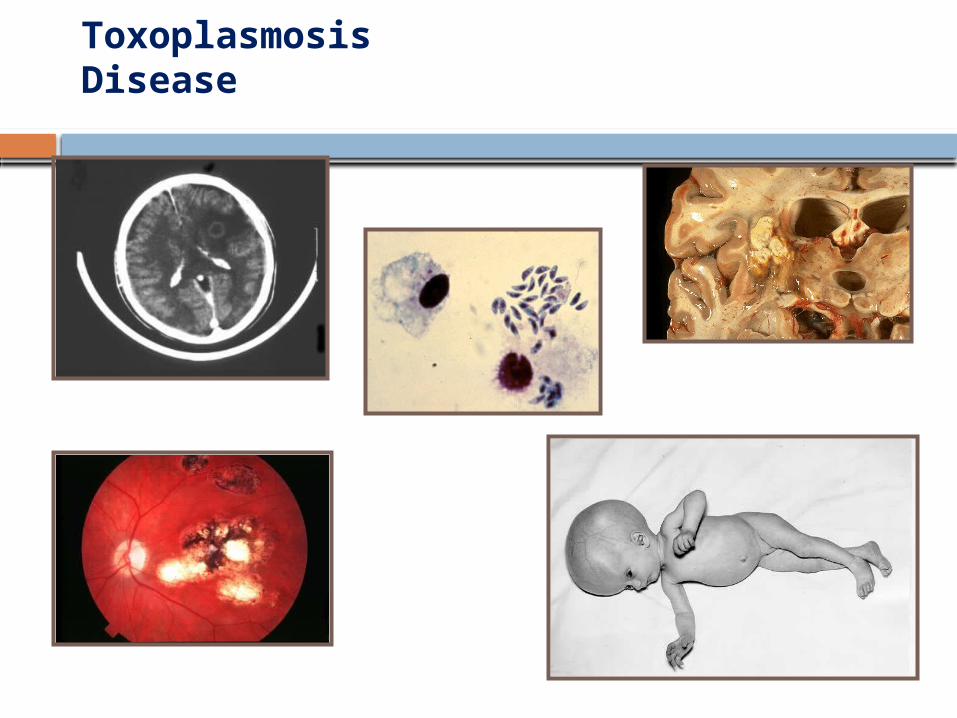
Some pictures of symptoms of Congenital Toxoplasmosis:
Hydrocephalus

Congenital Toxoplasmosis:
Intracranial calcification Chorioretinitis
ToxoplasmosisDisease

Diagnosis of Toxoplasmosis Diagnosis of Toxoplasmosis:
pregnant women Serological diagnosis in case of
maternal (swollen lymphatic glands, fever) or
fetal symptoms (detected in ultrasound) : Serological screening: to detect
asymptomatic infections

Diagnosis
A)Clinical diagnosis:- Depends on history and clinical picture.
B)Laboratory diagnosis:- 1- Direct methods :-Biobsy 2-Indirect methods :- a)Toxoplasmin skin test b )Serological tests (Sabin Feldman
Methylene Blue Dye Test ,IHAT ,ELISA, IFAT).

Immunonological diagnosis When an infection happens, IgG and
IgM get "positive". IgM are "positive" during acute infection and stay positive for a limited time (depending the methods of test You use). (Maybe 6 months to a year) IgG-titers rise during an acute infection, sink slowly again, but stay positive, and protect against another parasitaemia (and protects so the unborn baby).

DIAGNOSIS
IgG appear within 2 weeks of infection, peak in 6-8 wks, then decline over next 2 years, but detectable for life
IgM within first week and decline within a few months, however can persist for years after initial infection (therefore can not be used to confirm recent or acute infection)
Acute infection can be confirmed by culture, documented seroconversion, or 2-fold rise in antibody level

Toxoplasmosis – DiagnosisSignificance of detection of IgM and IgG
Antibody testing

Fetal diagnosis in case of maternal infection during pregnancy
When a pregnant woman has got an infection, there is the possibility, that she passes the infection on to her baby. To know, if the fetus (unborn baby) is infected helps to
find adequate treatment (for mother and fetus)
start treatment of the baby immediately after birth

Fetal diagnosis in case of maternal infection during pregnancy if the infection occurred during
pregnancy: anti-parasitic drugs should be taken until birth to reduce the risk of a fetal infection and the fetus (unborn baby) should be tested

Pediatric diagnosis
Serological tests of a blood sample of the newborn baby (or of an umbilical cord blood sample taken by the midwife) can help to find the diagnosis of Congenital Toxoplasmosis. IgG are passed from the mother to the baby through the placenta and could be of maternal origin. IgM cannot pass the placenta. If they are found infection of the baby is proofed. But: not all infected babies produce IgM, that mean, that the absence of IgM does not exclude Congenital Toxoplasmosis! In these cases the serological diagnosis of Toxoplasmosis can be performed by a follow-up. IgG-titers of maternal origin sink (half-life period about a month). Persisting (or rising) IgG proof congenital infection of the baby! Therefore serological testing should be repeated until IgG turns negative, exclusion of Congenital Toxoplasmosis cannot be done before that!

Treatment of pregnant women
Before 16th weeks' gestation 4 weeks Spiramycine [Rovamycine©]
After 16th weeks' gestation , if fetus is infected:
alternating to birth 4 weeks combination of:Pyrimethamin [Daraprim©], Sulfadiazin, Folinic Acid 4 weeks Spiramycine [Rovamycine©]
After 16th weeks' gestation, if fetus is not infected: Spiramycine [Rovamycine©] to birth
The combination of:Pyrimethamin [Daraprim©], Sulfadiazin, can pass through placenta and treat the fetus. But it is not allowed to give before about 16th weeks' gestation.

Treatment of prenataly infected children
Treatment of prenataly infected children with (symptomatic) disease
6 months: Combination of: Pyrimethamin [Daraprim©) Sulfadiazin Folinic Acid
6 months: alternating to the first birthday 4 weeks Spiramycine [Rovamycine©] 4 weeks Pyrimethamin [Daraprim©],
Sulfadiazin, Folinic Acid .

Treatment of prenataly infected children with subclinical infection (no symptoms)
6 weeks: A) Combination of: Pyrimethamin [Daraprim©] Sulfadiazin Folinic Acid 6 weeks: B) Spiramycine [Rovamycine©] alternating A and B to the first birthday 4 weeks Pyrimethamin [Daraprim©], Sulfadiazin, Folinic Acid 6 weeks Spiramycine [Rovamycine©]

Toxoplasmosis prevention of Congenital.
Primary prevention is an information about the ways of infection (cats, raw meet) to avoid ingestion or inhalation. This is important for all pregnant women who are "seronegative"
Secondary prevention is the detection of infected women during pregnancy to start treatment before the fetus gets infected.
Tertiary Prevention is the treatment of infected children to reduce or avoid symptoms.

Textbook