colorectal cancer statistics risk assessment screening options luke crantock
TRANSCRIPT

COLORECTAL CANCER
STATISTICS
RISK ASSESSMENT
SCREENING OPTIONS
Luke Crantock


How Common is Bowel Cancer ?
14,410 new cases diagnosed in 2010
More common in Men 1 : 17 M, 1 : 26 F
7982 ( M), 6428 (F ) – 12.6% all new cancers

Rare before the age of 50 ( 7.6 % of all CRC’s )
Risk at 85 is 1 : 12
Incidence - increased in men from 66.7/10 000 in 1982 to 72/100 000 in 2009 , women stable at 50/100 000.


MORTALITY
Second most common cancer death : 14% ( Lung 20% )
2010 : 3982 deaths from CRC80 Australians dying from cancer /week – one
death every 2 hoursMortality rate has decreased from 31.5/100
000 in 1982 to 16.2 /100 000 in 2010Risk dying from cancer at age 85 is 1: 45
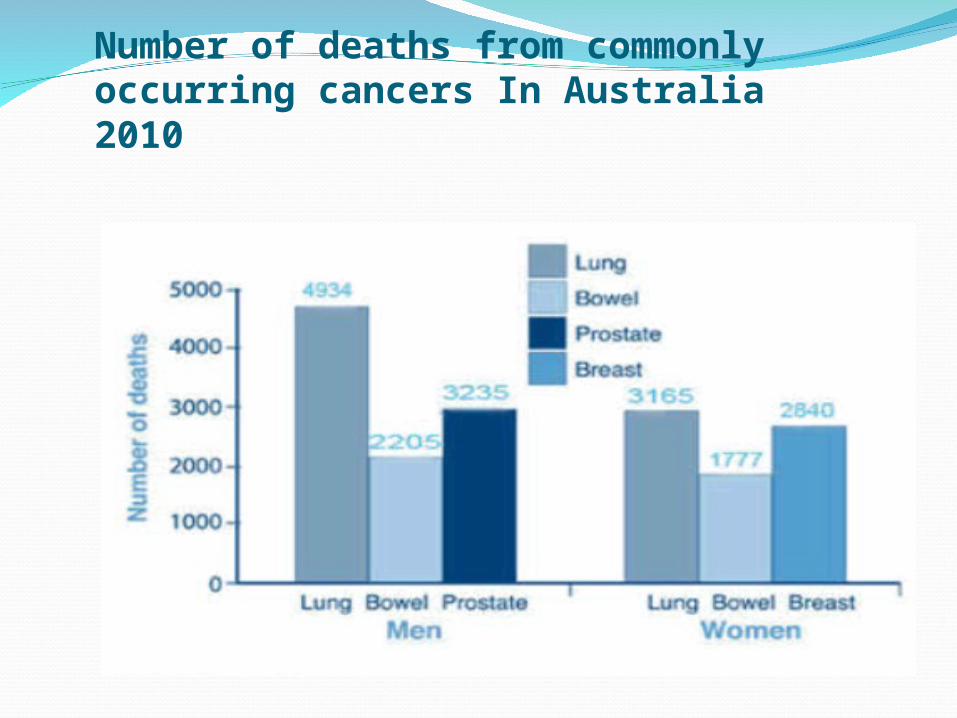
Number of deaths from commonly occurring cancers In Australia 2010
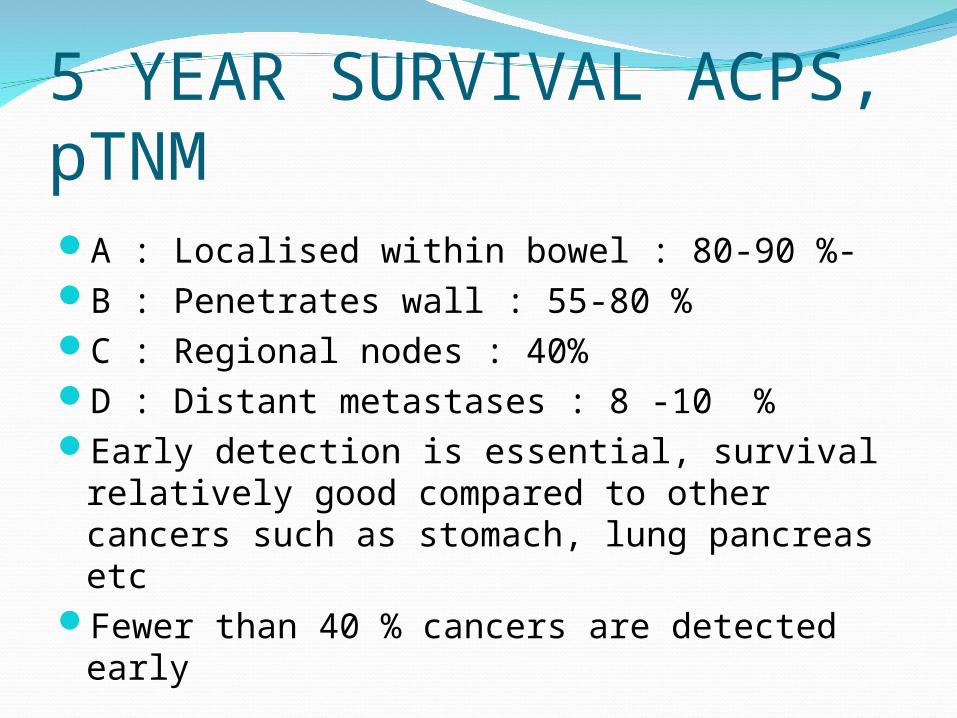
5 YEAR SURVIVAL ACPS, pTNMA : Localised within bowel : 80-90 %-B : Penetrates wall : 55-80 %C : Regional nodes : 40%D : Distant metastases : 8 -10 %Early detection is essential, survival
relatively good compared to other cancers such as stomach, lung pancreas etc
Fewer than 40 % cancers are detected early

AetiologyInteraction between inherited susceptibility
and environmental factors leading to accumulation of mutations in DNA resulting in uncontrolled cell growth
Benign precursor lesion – Adenoma Sequential multistep process involving
damage to genes leads to invasive malignancy


How Common are Polyps ?50 Yrs : 30%60 yrs : 40-50 %70 Yrs : 50-65 %
Risk family history Adenoma similar to CRCSerrated adenoma ( Methylation )

All in the GenesGene changes may be acquired ( diet, age etc
) or inherited.Tumours suppressor genes ( protective )
- acquired or inherited
DNA repair genes - acquired or inherited
Oncogenes – activation of ( K-ras ) - acquired

1990 Fearon & Vogelstein proposed multistep hypothesis for tumorigenesis particularly p53 and APC genes involved



RISKS - CRC
Age ( low before 50yrs -7.6 %) Family History Medical History ( polyps , IBD ) Environmental Factors
Up to 75 % of CRC could be prevented by
improvements in diet , activity and screening
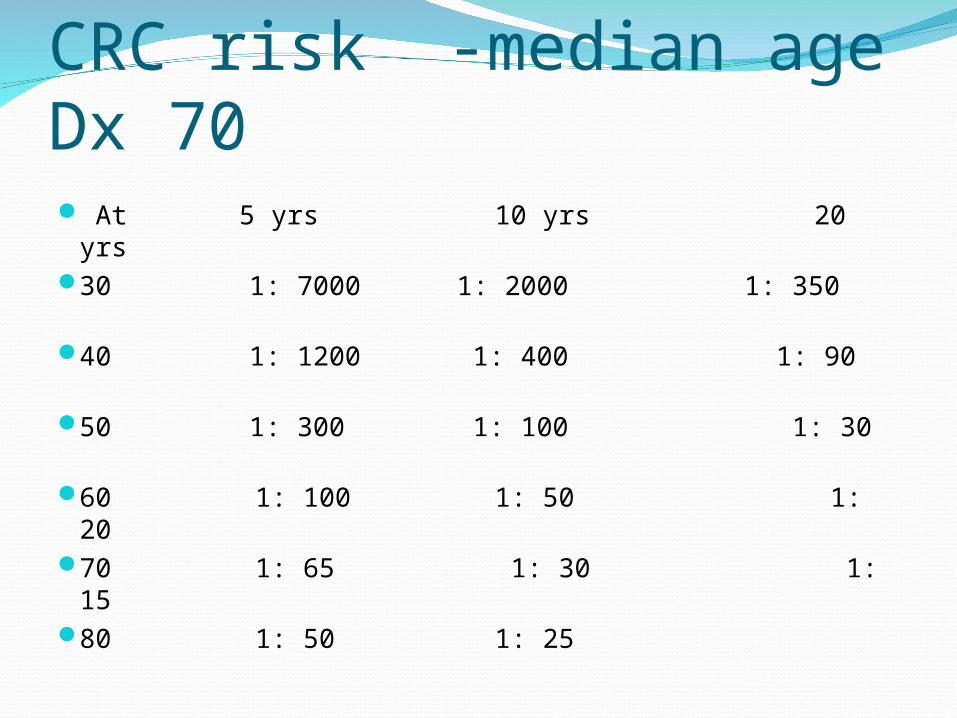
CRC risk -median age Dx 70 At 5 yrs 10 yrs 20 yrs
30 1: 7000 1: 2000 1: 350 40 1: 1200 1: 400 1: 90
50 1: 300 1: 100 1: 30
60 1: 100 1: 50 1: 20 70 1: 65 1: 30 1: 15
80 1: 50 1: 25

RELATIVE RISKAverage risk ( 75% have no family history )
Slight increased risk – 2nd degree relative – 1.3 times
Low Risk – 1st degree relative ( eg parent ) with CRC older than 55 - 2 times risk
Moderate Risk- One relative less than 55 yrs or Father and grandfather , (one younger than 50 risk) 3-6 times
High Risk – FAP, HNPCC syndromes, “3,2,1 “ rule – 3 relatives ( one first degree ), 2 generations , one less than 50yrs. 80% risk of CRC, 40-60% endometrial or ovarian cancer



Medical History
Past Hx PolypsPast Hx CRCHx IBD

Lifestyle factors-Prevention
Healthy Lifestyle – Physical activity – Healthy BMI
– Limit alcohol – Quit smoking




Lifestyle & Diet, Regular activity 30-60min/dayNHMRC attributes dietary factors to 50%
CRCReduce daily energy intake < 2000
calories/day for men, < 2000 calories /day for women.
Increased risk Type 2 DiabetesReduces fats - Exception is omega-3 fatty
acids inverse correlate –reduce epithelial proliferation
Limit alcohol <2 std drinks/day

Lifestyle & Diet 5 or more serves vegetables/day2 serves fruit/dayEncourage cerealsLean meats, avoid charring & processed
meats Stop smoking ( 50% increased risk )Folate, SeleniumAspirin, NSAIDSHMG-Co A reductase inhibitors1000-1200mg calcium/day
Patient AssessmentAny family members with CRC ? ( 75 %
do not ) Any family members with polyps ?Any previous polyps ?Any rectal bleeding ?Any recent change in bowel habit ?Any new abdominal pain or weight loss ?A history of colitis ?Iron deficiency ? – up to 15 % have CRC

One third of CRC cases could be prevented by screening !
Survival depends on early detection !

SCREENING -Screening involves asymptomatic patients !
Faecal Occult Blood TestingFlexible SigmoidoscopyColonoscopyBarium EnemaVirtual ColonoscopyDetection of DNA mutations & stool
tumour markers
ScreeningOne step – Colonoscopy , select on age.
Many individuals will have –ve test ( 4-7 % develop CRC in life
time ) Expense and morbidity . Are risks matched by benefit ?
Two Step – Screen with cheap test such as FOBT follow by colonoscopy if
+ve - evidence based - colonoscopic resources managed - overcomes initial patient
reluctance for invasive test

NBCSPPilot from 2002About 45% participation rateNow testing 50, 55, 60 and 65 yr oldsBy 2015 include 70 yr olds2012-2015 4.8 million Australians eligibleBy 2017/18 biennial screening phased in
between 50-74 yrsExpect detect 12 000 new cases /yr and save
300-500 lives

FOBTFive randomised controlled trials of serial
FOBT’s ( more than 250 000 subjects ) - Reduction in CRC mortality of 33 % with annual screening
21% reduction with biennial screening

FOBT - Types AvailableGuaiac – HemoccultHaem-derived porphyrin – HemoQuantFaecal Immunochemical tests – Inform ,
HemeSelect

Guaiac TestsDependent on peroxidase activity of heme
molecule which is stable during digestion and therefore not selective for colorectal bleeding
Restriction of heme rich or peroxidase rich foods and some medications . Vit C gives false negatives
Requires testing on three separate occasions
Not suitable for automated testing

Immunochemical Tests - FITDetection is based on antibodies specific for human
Hb Not subject to interference by diet or drugsFIT’s are selective for colorectal bleeding as Hb is
degraded by digestion ( do not detect gastric bleeding )
More sensitive than Guaiac FOBT ‘s with similar specificity : 0.1mg Hb per gram faeces . FIT’s have better performance than guaiac tests
Sampling of toilet bowl water around immersed stool – improved participation
Mass processing by automated readingFIT tests can be quantified. Sensitivity for cancer
may be as high as 68-85 %
Most positive FOBT’s will not be anything serious !
Do improve detection of asymptomatic CRC
65 – 90 % Dukes A/B compared to 33-35 % control
FOBT PERFORMANCE 4 % +ve3-5 % CRC30 - 45 % Adenomas 30-40 % CRC missed.Over 13 yrs – Annual screening : 33%
reduction in mortality -Biennial : 20 % reduction

Flexible SigmoidoscopyVisualisation of distal bowel where 70 % of
cancers occur ( rectum 40% and sigmoid )No sedationRetrospective case controlled studies
support reduction in mortality for distal cancers ( 70 % ) but not for proximal lesions
A distal adenoma indicates 2-5 % chance of advanced proximal adenoma
If sigmoidoscopy negative – repeat in 5 yrs
COLONOSCOPYNo RCTs but National Cooperative Polyp Study
cohort-1418 pts, 1 or more adenomas removed , followed progressively, CRC incidence 76-90 % lower than expected. Other estimates at least 50 % reduction in risk.
Missed polyps 6-25 %, 6-10 min withdrawal time, good prep
Cost benefit analysis suggests value for colonoscopy at 10 yearly intervals – US guidelines
1 : 500 post polypectomy haemorrhage1 : 1500 chance of bowel perforation
Double Contrast Barium EnemaNo randomised trials showing reduction in
mortalityInferior sensitivity to colonoscopy by 5 - 10 %
with no prospect for polyp removal nor biopsy
Virtual ColonoscopyCT or MRI imaging used to develop 2 and 3
dimensional images of colonColonic preparation and bowel insufflation with CO2No sedationMinimal risk of bowel perforation , infection or
bleedingSensitivity good for polyps > 10 mmNo chance of biopsy or polyp removal No texture or colour detailHigh colonoscopy follow up rates – 15 – 25 %Radiation exposureNo randomised trials showing benefit

Radiation ExposureMillisieverts2-3 mSv/yrCT – 5- 15mSvCXR - 0.02mSv> 100mSv may increase cancer risk>1000 mSv cumulative increase cancer risk
in later years 5/100 develop cancer
Detection of DNA mutations and tumour markers in stool
Mutations of genes are associated with malignancy and adenomas
Oncogenes ( RAS ) , tumour suppressor genes ( p53 & APC ) , microsatellite instability sequences are known and can be assessed
Cells from tumours with the above mutations are shed into the gut and can be detected in stool
Screening for a panel of markers is suggested combined with FOBT – promise for future
Key Points
Lifestyle MeasuresIdentify riskScreening for asymptomatic patients33% reduction in mortality with early
detection
Practical approach to screening – see NHMRC clinical guidelines
Thorough history and physical examDiscussion of diet and lifestyle – boost fruit
and vegetable intake ,allow lean meat (not charred ), no real benefit from antioxidants or vitamin supplements ( folate )
Average risk - FOBT second yearly +/- endoscopy 5 yearly
Above average risk ( 5 -8 % ) – 5 yearly colonoscopy with interval FOBT
High Risk – special consideration and referral

Hang in there