clinical decision support a population health approach farzad mostashari, md, msc nyc dohmh...
TRANSCRIPT
Clinical Decision SupportA Population Health Approach
Farzad Mostashari, MD, MScNYC DOHMH


THE INSTITUTEFOR URBAN
FAMILY HEALTH

Quality of Care With and Without EHR Use
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90 100
Percent Compliance without EHR
Wit
h E
HR
Preventive Counselling Chronic Disease Management Avoiding Hazardous Rx
EHR Better
"No EHR" Better
Tobacco cessation Statin Use
No Benzo in Depression

Government Role?
• Will HIT address priority public health issues?
• Will HIT adoption reach disadvantaged populations?

Primary Care Information Project
• Mission – Improve population health in medically
underserved areas through health information technology (HIT)
• Resources– NYS- $250 Million over 5 years for HIE– NYC- $27 million Community EHR Project– CDC- Center of Excellence PH Informatics

PCIP Roadmap1. Citywide EHR Network
• Procure “best of breed” Electronic Health Record • Add Public Health/Quality Improvement functionality• Prepare Network and Hardware Infrastructure• Extend to Correctional Health and community providers
2. Citywide Quality Improvement Network• Citywide automated quality measurement and reporting• Decision supports and other quality improvement• Extend to other ambulatory EHRs
3. Citywide Health Information Exchange Network• Interfaces to other systems (e.g., HHC)• Syndromic and Notifiable Disease Reporting• Citywide Immunization, Lead Registries, and School Health• Linkages to RHIOs• Medicaid medication history

HEAL-NY 1
• Impact– All NYC Community Health
Centers will have EHRs by 2009
• 648 providers• 500,000 patients• 50% Medicaid, 20%
uninsured
– Safety net providers “RHIO”

Other Providers
• Small doctors offices– Deliver 85% of primary care– Lowest EHR adoption rates– Greatest challenges in quality
and financing
• Convening and support– Medical Societies– QIO (IPRO)– Hospitals– Health Plans?

Eligibility and Public Purpose
• Care for underserved / vulnerable populations– Medicaid and uninsured– S Bronx, Harlem, Central Brooklyn
• Participate in public health goals – Mandatory indicator reporting (automated, confidential)– Quality improvement (inc. decision support tools)– Public health interfaces (school health, CIR)
• Financial Commitment– $4k per provider contribution to QI fund– Assume all ongoing costs after 2 yr testing phase

What do they get?
• Licenses to “NYC Build” eClinicalWorks• Common interfaces included • On-site training • Quality improvement technical assistance
• Predictable, low ongoing (M&S) costs– Less than $1,500 per FTE provider/ yr


10 Take New York Indicators1. Have a Regular Doctor or Other Health Care
Provider2. Be Tobacco-Free3. Keep Your Heart Healthy4. Know Your HIV Status5. Get Help for Depression6. Live Free of Dependence on Alcohol and Drugs7. Get Checked for Cancer8. Get the Immunizations You Need9. Make Your Home Safe and Healthy10. Have a Healthy Baby

Smart Web Form
• Facilitates n-level structured data collection • Built-in intelligence to make calculations based
on data entered – Initial Visit form– Tobacco Quit Readiness Assessment form – Fax-to-Quit form– Asthma Severity Assessment form– PHQ2 and PHQ9 for Depression Screening – AUDIT-C for Alcohol Misuse Screening – School Health New Admission Examination form– Sexual History form






Registry



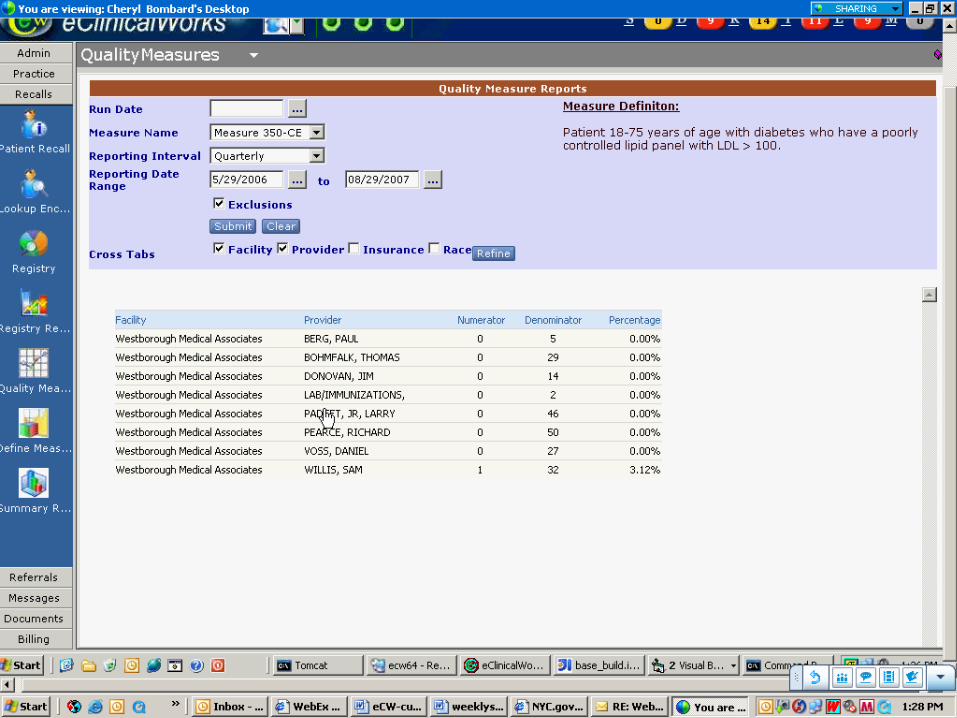
Measure Reporting
• User Interface to run measure report
• Can view with/ without exclusions
• Cross tab: facility, provider, insurance & race
• Drill-down capability

Decision Support Tools
• Based on TCNY measures• Passive alerts and reminders
– Wary of “alert fatigue”– Minimal set– Actionable (Order, Historical Order or Suppress)– Consonant with workflows, not disruptive
• Not just alerts– Order sets, templates, clinical knowledge, data
presentation, process reengineering

Desired Attributes
• Acceptable to small independent providers
• Priority health issues (premature deaths) comprehensively addressed
• Could be implemented in multiple EHR systems
• Mechanism for updating as evidence base changes

Identify last recorded quit date and date of last status
update
FORMER SMOKER BPA PATHWAY
Was last quit date within past 2 years
(or null)?
Was last status update < 90 days ago?
Was last update > 12 months ago?
No BPA activated
NO
YES
NO
BPA #4b: "Update Smoking Status"
YES
BPA #4a: "Update Smoking Status"
NO
Clinician clicks status radio button and clicks verify
button
Was current status updated and verified?
NO. BPA not satisfied.
NO
Store status update
verification date.
YES
BPA satisfied
Clinician clicks status radio button and clicks verify
button
Was current status updated and verified?
BPA #4a not satisfied.
NO
BPA #4a satisfied
Relapse prevention counseling in past 90 days OR quit date > 12 months
ago?
STOP YES
YES
BPA #5: "Review relapse prevention
interventions" NO
Congratulation, you've been tobacco-free for ___ days!
Offer relapse prevention literature.Review current treatment plan
Clinical Decision Support – Tobacco Best Practice Alert


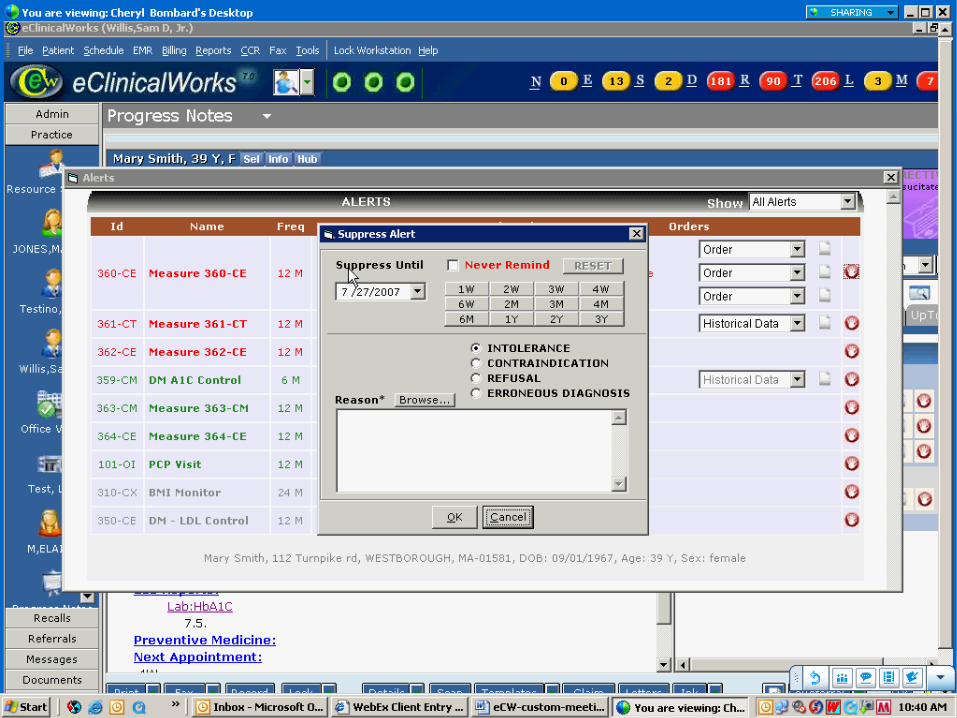

Actionable, non-intrusive alert will show on the right-pane.

Measure Defn as CDSS Logic?
• Potential solution to portability of CDSS• Consistent message of “what’s good care”• Providers “clean” measures as they go• But can’t afford lots of “false positives”
– Need CDSS Numerator inclusions• “snooze” on order• Incorporates epidemiologic info (never smoker > 26 yo)
– Denominator exclusions • Patient refusal, medical contraindication, system reasons

Order Set
• Triggered by TCNY quality indicator• Full order set vs. Quick order
– Quick - lab• A1C testing in patients with diabetes (6 months)• LDL testing in high risk patients (IVD, DM)
– Full - medication, referral, education (provider/patient)
• A1C control in patients with diabetes (good control)• BP control in high risk (130/80) patients (IVD, DM)• LDL control in high risk patients (IVD, DM)



Other Decision Supports
• Order Sets
• Templates
• Adverse drug event alerts
• Data display and visualization
• Pricing and formulary information

eMedNY
Allows treating physicians to access to their respective Medicaid patients’ Medication history at the point of care, at the time of treatment
Eliminates steps from the practice workflow by linking Medicaid Eligibility checking directly into eClinicalWorks’ practice management




“Not Just Alerts”
• Practice workflow reorganization– Structured data collection – Registries and panel management– Alternative visit types– Team-based care– Case management– Patient education and self-management

Key Features
• Framework for comprehensive, but limited, set of evidence-based interventions
• Measure definition= CDSS trigger logic
• Incorporation of epidemiologic information
• Underpins a distributed query architecture

Future Directions
• Human-Computer interface optimization
• Extension of concepts to other EHRs
• Establish architecture for distributing new measures and order sets
• Extension to Public Health alerts and reporting
• Evaluation– AHRQ, NORC

Provider Patient
Cough!
Step 1: EHR institution to public health agency – clinical encounters
IUFH
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
7/8/03 8/8/03 9/8/03 10/8/03 11/8/03 12/8/03 1/8/04 2/8/04 3/8/04 4/8/04 5/8/04 6/8/040.00
0.01
0.02
0.03
0.04
0.05
0.06
Step 2: Public health agency to EHR institution - epidemiologic awareness
NYCDOH
1
2
Practice Alert in EHR for age 18-45, relevant Sx/Dx, requests provider to do nasopharyngeal wash and call DOH for immediate pick-up and viral ID by DOH lab
DOH receives signal of outbreak of respiratory illness in young adults
Cough