chronic kidney disease( ckd) - msic
TRANSCRIPT
Chronic Kidney Disease( CKD)
Dr. Saad Mustafa


STAGING OF CKD


2018 ANNUAL DATA REPORT
VOLUME 1: CHRONIC KIDNEY DISEASE
2018 Annual Data Report Volume 1 CKD, Chapter 1
Chapter 1:CKD in the General Population

6
vol 1 Figure 1.1 Prevalence of CKD by stage among NHANES participants, 2001-2016
Data Source: National Health and Nutrition Examination Survey (NHANES), 2001-2004, 2005-2008, 2009-2012 & 2013–2016participants aged 20 & older. Whisker lines indicate 95% confidence intervals. Abbreviation: CKD, chronic kidney disease.

7
vol 1 Figure 3.1 Unadjusted and adjusted all-cause mortality rates per 1,000 patient-years at risk for Medicare patients aged 66 and older, by CKD
status and year, 2004-2016
(a) Unadjusted
Data source: Special analyses, Medicare 5% sample. January 1 of each reported year, point prevalent Medicare patients aged 66 and older. 1.b adjusted for age/sex/race and 1.c adjusted for age/sex/race/comorbidities. 1.e adjusted for age/sex and 1.f adjusted for age/sex/comorbidities. Standard population: Medicare 2011 patients. Abbreviation: CKD, chronic kidney disease.

CKD (And ESRD) are costly
• Cost of treating ESRD : almost $50B/year
• Cost of treating all CKD: $45.5B/year
• Cost of treating diabetic CKD: $24.6B/year
Reference: Adapted from USRDS Annual Data Report (NIDDK, 2013)

9
vol 1 Figure 7.6 Per person per year Medicare, Medicare advantage, and managed care spending for the CKD patients aged 65 and older, by
diabetes and heart failure, 2006-2016
Data Source: Medicare 5% sample and Optum Clinformatics™. Abbreviations: CKD, chronic kidney disease; DM, diabetes mellitus; ESRD, end-stage renal disease; HF, heart failure; PPPY, per person per year.

EVALUATION OF CKD
➢ Evaluation of chronicity
➢ In people with GFR <60 ml/min/1.73 m2 (GFR categories G3a-G5) or markers of kidney damage, review:
➢ past history and previous measurements to determine duration of kidney disease
-If duration is than3 months, CKD is confirmed. follow recommendations for CKD.
-If duration is not >3 months or unclear, CKD is not confirmed.( Patients may have CKD or acute kidneydiseases (including AKI) or both and tests should be repeated accordingly.)

Risk factors for CKD
▪ Diabetes
▪ Hypertension
▪ Family history of kidney disease
▪ Cardiovascular disease
▪ Recurrent urinary tract infections
▪ HIV infection
▪ Autoimmune diseases

PREDICTING PROGNOSIS OF CKD
• Identify the following variables:
✓ Cause of CKD✓ GFR category✓ albuminuria category✓ other risk factors and comorbid conditions

• Evaluation of cause• Evaluate the clinical context, including
-personal and family history, -social and environmental factors,-medications, -physical examination,- laboratory measures,- imaging, -pathologic diagnosis


Prognosis of CKD by GFR and albuminuria category
DEFINITION AND IDENTIFICATIONOF CKD PROGRESSION
• Define CKD progression based on one or more of the
following :➢ drop in GFR category accompanied by a 25% or
greater drop in eGFR from baseline
➢Rapid progression is defined as a sustained decline in
eGFR of more than 5 ml/min/1.73 m2/year
confidence in assessing progression is increased withincreasing number of serum creatinine measurementsand duration of follow-up.

PREDICTORS OF PROGRESSION
•Identify factors associated with CKD progression to inform
prognosis. These include:-• cause of CKD,
level of GFR,• level of albuminuria• Age, sex, race/ethnicity• Elevated BP, • Hyperglycemia, • Dyslipidemia,
Smoking, obesity,• History of cardiovascular disease,• Ongoing exposure to nephrotoxic agents, and others.

FOLLOW UP
• Assess GFR and albuminuria at least
annually in people with CKD.
• Assess GFR and albuminuria more often
for individuals at higher risk of progression
• The AER is one of the best indicators of
diabetic nephropathy risk in both type 1and type 2 diabetes

FOLLOW UP

Pathogenesis of the manifestations of CKD
▪ We have a large physiologic reserve of renal functional mass
▪ Slow, progressive loss of functioning nephrons may not be
noticeable.
▪ The slow, progressive loss of function triggers a numberof maladaptive compensatory mechanisms
▪ Either the loss of renal function or the adaptations to
reduced renal function lead to the manifestations ofuremia
▪ The person with CKD may not feel different (silent killer).

• Chronic kidney disease (CKD) progresses through three phases:
• 1) An initial injury stimulates :
• 2) repair mechanisms that may be misdirected, impairing nephron function.
• 3) the remaining nephrons respond, compensating for decreased function with further changes in activity that may be deleterious for nephronsurvival.

Nephron loss in the pathogenesis of uremia
• During initial nephron loss,hypertrophy of remaining nephrons maintains GFR.
• the limit of this adjustment is reached, and as more nephrons are lost GFR decreases.
• when nephrons are lost plasma phosphate rises andcalcium falls.
• A series of events mediate an increase in parathyroid hormone (PTH) and fibroblast growth factor (FGF)-23 secretion, which stimulates phosphate excretion to normalize plasma phosphate and calcium.
• With continued nephron loss, phosphate increases, calciumdecreases and PTH and FGF23 rise steadily in a vain attempt to compensate.

Structural events in nephron loss
• Glomerular hypertrophy and podocyte loss lead to theformation of synechiae
• Increased filtration of protein , (2 shaded area) leads to its extrusion directly into the tubulointerstitium through the synechiaor through its delivery to the renal tubules (3), where it may activate cells or be transported into the tissues.
• Biologically active lipids (L, 4) or cytokines (C, 5) are present as a result of reabsorption, local production by tubular and other resident cells or generation by inflammatory cells (6) that are recruited to the tubulointerstitium.
• A number of mediators of injury contribute to tissue loss and mediators of scarring alter the balance between extracellular matrix synthesis and degradation, leading to fibrosis

Mechanisms of Progression ofChronic Kidney Disease
Structural events in nephron loss Nephron loss as a self-fulfilling prophecy

Sodium Retention in CKD
• The Input Solution
– Dietary Na Restriction in proportion to the decrement
in GFR
• The output solution
Decreased Na Reabsorption
Increased Fractional Na Excretion
Adaptive Natriuresis

Not all solutes are regulated to thesame extent
A) Little regulation: Plasma concentrations
increase as nephrons are lost.
Creatinine
Urea
B)Partial regulation: Plasma
concentrations maintained until 50% lost.
HCO3-
Ca++
Pi
C)Near complete regulation: Plasma
concentration can be maintained until
approximately 90% nephron loss.
Water
Na+
K+

Regulation of solutes with progressivenephron loss: Plasma concentration and
urine concentrating ability by GFR
100 % 65 % 33 % 20 % 10 %
Cr 1 1.3 3.1 5 10.4
BUN 14 18 29 46 82
[Pi] 4 4.2 4.3 5.2 5.8
[HCO3] 24 24 22 16 13
[Na+] 140 140 140 138 136
[K+] 4 4 4 4.5 5.5
pH 7.4 7.4 7.37 7.3 7.26
Max Uosm 1200 1000 500 350 310
Min Uosm 50 50 70 200 310

CKD-MBD

what is CKD-MBD?
• It's a systemic disorder of mineral and bone etabolism due to CKD, manifested by either one or a combination of the following.
1) Abnormalities of calcium, phosphorus, PTH, or vitamin D metabolism. So, essentially, abnormal blood tests.
2) Abnormalities of bone turnover, mineralization, volume, linear growth, and strength. So, bone abnormalities
3) Vascular or other soft tissue calcification. So either abnormal blood tests, abnormal bone health, orvascular calcification. Either one of the these, or in anycombination, is what CKD-MBD is.

Which biomarker is most predictive of outcome?
• 13 studies with over 92,000 patients. And, virtually, every study that has looked at this has demonstrated that the higher the level of serum phosphorus, the greater is the risk for death or death from cardiovascular causes.
• There is most consistent evidence
• There is evidence also for association of blood levels of calcium and parathyroid hormone with outcomes, but the evidence is either much less strong or much less consistent.
• Alkaline phosphatase. The association of alkaline phosphatasewith the risk for death is linear.
• FGF-23 the higher the level of FGF-23,the greater the risk for death.

Kidney Function Ability to maintain P
Klotho Deficiency FGF-23 PTH
1,25 vit D
Urinary excretion of P
Why do these abnormalities occur
Inhibits
Inhibits
P maintained in normal range

• PTH and FGF23 reduce proximal tubular phosphate reabsorption by promoting removal of sodium-phosphate co-transporters from the brush border membrane ,and both hormones increase calcium reabsorption in the distal convoluted tubule

Pathogenesis of Metabolic Bone Disease in CKD
• High-Turnover Metabolic Bone Disease in CKDresult of the development of secondary hyperparathyroidism.
Role of Phosphate Retention. (tradeoff)Decrease in GFR causes transient decreases in the levels of ionized calcium, which would, in turn, trigger an increase in PTH secretion. restoration of normal calcium and phosphate levels
The “tradeoff” for the maintenance of normal concentrations of calcium and phosphorus is the development of hyperparathyroidismN.B Because studies in experimental animals have shown that phosphate seems to affect parathyroid function independent of calcium or calcitriol, it is likely that phosphate mediates these effects directly.It has been shown, however, that the effects of high phosphorus concentrations to increase PTH secretion is a posttranscriptional effect (the stability of PTH mRNA )

• Role of Decreased Synthesis of Calcitriol.• The decreased production of calcitriol contributes to the development of secondary
hyperparathyroidism (!! increased levels of PTH would be expected to increase the activity of the 1—α hydroxylase in the kidney in an effort to maintain these concentrations close to normal.
• These observations indicate that other factors are involved in limiting the ability of the diseased kidney to increase calcitriol production
• these factors are :• phosphate retention,• FGF 23• 25-VIT D (, the principle storage form of vitamin D,) circulates bound to vitamin D–
binding protein (Decreased GFR results in decreased delivery of substrate to the 1-α hydroxylase, which will limit the ability of the kidney to produce the active sterol)
• Skeletal Resistance to the Actions of PTH
•

• Low-Turnover Metabolic Bone Disease in CKD (Adynamic)
• characterized by an extremely slow rate of bone formation. -osteomalacia (defective bone mineralization)
Number of factors might be involved ;
Administration of high calcium loads from calcium-containing phosphate binders
- the use of potent vitamin D sterols-use of aluminum-based phosphorus binders- Age
-

Anemia

Disorders of erythropoiesis in CKD
• EPO is produced by the kidneyperitubular interstitial fibroblasts• Renal EPO Producing Cells
• In CKD, REPC undergotransdifferentiation tomyofibroblasts losing the abilityto produce EPO (erythropoietin)
• In CKD kidneys, the number ofREPC is reduced, which results ininadequate EPO production inresponse to hypoxic stimuli andleads to the development ofanemia
Blood Rev. 2013 Jan; 27(1): 41–53.



Manegment of complications

Calcium and Phosphorus Balance:
National Kidney Foundation Recommendations
(KDOQI)
◼ it has become clear that CKD patients have a nutritional deficiency of 25-
OH Vitamin D which itself leads to an increase in PTH secretion
◼ Levels of 25-OH D should be measured when PTH-Intact >70pg/ml and
supplementation instituted if necessary, a level of <30ng/ml is abnormal
and <15ng/ml, moderate to severe
◼ Treatment
◼ <5ng/ml 50,000U Ergocalciferol/wk x12, then q mo x6
◼ 5-15ng/ml 50,000/wk x 4, then q mo x 6
◼ 16-30ng/ml 50,000/month x 6
◼ Measure 25(OH)-D at 6months
◼ Maintenance 800-1200 IU qd
(AJKD, 39, 2002, pS214)

Calcium and Phosphorus Balance
KDOQI Recommendations
• Stage 3 CKD, GFR 30-59
• ◼ Measure Ca, Phosand PTH-I every 12months
• ◼ Target levels
• ◼ Calcium WNL for lab
• ◼ Phos > 2.7- 4.6 mg/dL
• ◼ Ca X Phos < 55
• ◼ PTH-I 30-70 pg/ml
• ◼Stage 4 CKD, GFR 15-29
• ◼ Measure Ca, Phos andPTH-I every 3 months
• ◼ Target levels
• ◼ Ca preferably WNL for lab
• ◼ Phos > 2.7-</= 4.6mg/dL
• ◼ Ca X Phos < 55
• ◼ PTH-I 70-110 pg/ml

Kdigo Guidelines CKD-MBD
• We recommend monitoring serum levels of calcium, phosphate, PTH, and alkaline phosphatase activity beginning in CKD G3a .
• In children, we suggest such monitoring beginning in CKD G2 .
In CKD G4: for serum calcium and phosphate, every 3–6 months; and for PTH, every 6–12 months.
➢ In CKD G5, including G5D: for serum calcium and phosphate, every 1–3 months; and for PTH, every 3–6 months.In CKD G4–G5D: for alkaline phosphatase activity, every 12 months, or more frequently in the presence of elevated PTH
➢ In patients with CKD G3a–G5D, we suggest that 25(OH)D (calcidiol) levels might be measured, and repeated testing determined by baseline values and therapeutic interventions
➢ We suggest that vitamin D deficiency and insufficiency be corrected using treatment strategies recommended for the general population
➢ In patients with CKD G3a–G5D, we suggest that individual values of serum calcium and phosphate, evaluated together, be used to guide clinical practice rather than the mathematical construct of calcium-phosphate product (CaXP)

KDIGO Guidelines
CKD-MBD/SHPT Anemia
1.
2.
3.
4.
5.
Assess calcium, phosphorus, PTHand vitamin D
Correct these abnormalitiesbefore treating elevated PTH
Dietary intervention andphosphate binders forhyperphosphatemia
If PTH > UNL in CKD 3-5 usevitamin D analogs or calcitriol
In ESRD, use vitamin D analogs,calcitriol, calcimimetics orcombination
1. Investigate anemia usingHb, red cell indices, WBC &PLTs, absolute retic count,ferritin, TSAT, B12, folate
2. Address iron deficiency(TSAT< 30%, ferritin < 500ng/ml) before using ESA
3. ESAs are started whenhemoglobin < 10 g/dl
4. Do not use to maintain Hb>11.5 g/dl

Calcium and Phosphorus Balance
KDOQI Recommendations
• How are these goals achieved ?
• ◼ Control of dietary phosphorus intake to 0.8-1g/d
• ◼ May need initiation of “Phosphate binders” with
meals
• ◼ When 25(OH)-D >30pg/ml and PTH-I > target,
initiate treatment with exogenous “Active Vitamin D”
• ◼ A few patients with very elevated PTH-I values may
benefit from Calcimimetics

High Phosphorus Foods◼ Dairy products (Cheese, ice cream, milk), nuts,
peanut butter, biscuits, processed meats-hotdogs,
chocolate, dark sodas (Coke, Pepsi), beans
Calcium and Phosphorus Balance:
Limit Phosphorus intake to 0.8-1.0 g/d

Given with meals, timing essential
◼ Aluminum based medicines;
◼ Calcium Based
◼ Calcium Carbonate/Magnesium Carbonate
◼ Calcium Carbonate
◼ CalciumAcetate
Use of Phosphate binders

Vitamin D supplementation and bisphosphonates in people with CKD
•3.3.5: We suggest not to routinely prescribe vitamin D supplements or vitamin D analogs, in the absence of suspected or documented deficiency, to suppress elevated PTH concentrations in people with CKD not on dialysis. (2B)3.3.6: We suggest not to prescribe bisphosphonatetreatment in people with GFR o30 ml/min/1.73 m2 (GFR categories G4-G5) without a strong clinical rationale. (2B

Anemia-Treatment Guidelines
• Goal Hgb 11-12
• ◼ Recombinant erythropoeitin
• ◼ Epogen/Procrit 50-150 U/kg/wk SQ
• ◼ Darbopoetin alfa (ARANESP) Start 0.45mcg/kg SQ once every 2weeks, usually dosed every three to four weeks when patient is stable inthe therapeutic range
• ◼ Recent concerns are increased risk of cardiovascular eventsassociated with an elevated Hgb in association with use of high doses ofthese products
• ◼ Iron
• ◼ Goal Ferritin >200, TSAT >20%
• ◼ Oral agents
• ◼ Chromagen: 33% iron
• ◼ Ferrous sulfate: 20% iron
• ◼ Niferex (Polysaccharide with Vit C): 150mg elemental iron
• ◼ Ferrous fumurate: 33% iron
• ◼ Ferrous gluconate (Fergon): 12% iron
• ◼ Oral agents do not work well, primarily b/o ill tolerated GI side effects

Cardiovascular Risk
• Individuals with CKD are at increased risk for CVD, they
should be considered in the “highest risk group for evaluation
and management” according to NKF recommendations.• If we consider the patients at Stages 3 and 4, they have a
higher risk of death than progressing to need for dialysis !!!!


PLAN OF CARE AND ACTION PLAN FOR CHRONIC KIDNEY DISEASE STAGES 1–4

Management of CKD (General)

Recommendations for Controlling
HTN
• • Use of ARB or ACE-I in both diabetic and non-diabetic adults with CKD and urine albuminexcretion >300 mg/24 hours
If diabetic, albuminuria 30-300mg /24 hrsis indicated for ACE/ARBI
•Pay a close attention in CKD to preventadverse effects of antihypertensive therapy.(electrolyte disorders, acute deteriorationin kidney function, orthostatic hypotensionand drug side effects )
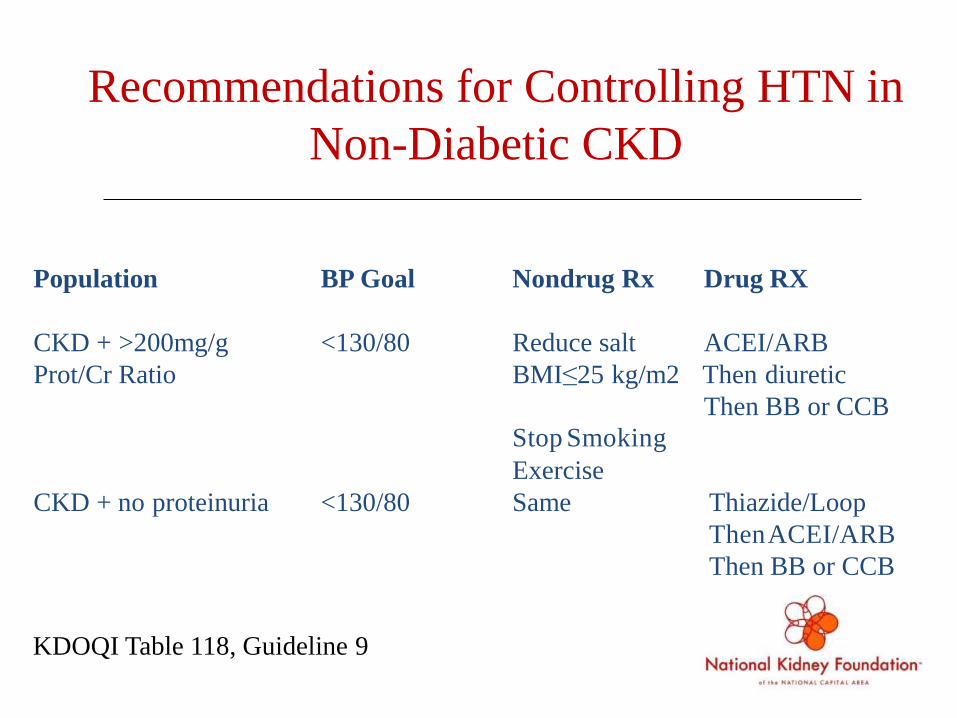
Recommendations for Controlling HTN in
Non-Diabetic CKD
Population BP Goal Nondrug Rx Drug RX
CKD + >200mg/g <130/80 Reduce salt ACEI/ARB
Prot/Cr Ratio BMI≤25 kg/m2 Then diuretic
Then BB or CCB
Stop Smoking
Exercise
CKD + no proteinuria <130/80 Same Thiazide/Loop
ThenACEI/ARB
Then BB or CCB
KDOQI Table 118, Guideline 9

Interventions that delay progression
of CKD: Strict Glycemic Control
80% Type I DM with microalbuminuria
develop DN in 10-15years, 50% to ESRD– DCCT, benefit of tight control in reducing
occurrence subclinical and overt DN(40-60%)
• 20-40% Type II DM with microalbuminuria
develop DN, 20% to ESRD– UKPDS 33, 25% reduction in microvascular
Events

Modification of Comorbidity:
Cardiovascular Disease
• CVD is the cause of death in 40-50% ESRD
patients• ESRD CVD mortality rates 15x higher than
general population.• CVD is leading cause of death in patients with
CKD, regardless of stage.
– British Regional Heart Study, 50% deaths CV in
patients in upper decile of baseline Cr

GUIDELINE 15. ASSOCIATION OF CHRONIC KIDNEY DISEASE WITH
CARDIOVASCULAR DISEASE
Patients with CKD, irrespective of diagnosis, are at increased risk of
cardiovascular disease (CVD), including coronary heart disease,
cerebrovascular disease, peripheral vascular disease, and heart failure.
Both “traditional” and “chronic kidney disease related (nontraditional)” CVD
risk factors may contribute to this increased risk.
-All patients with CKD should be considered in the “highest risk” group
for CVD, irrespective of levels of traditional CVD risk factors.
-All patients with CKD should undergo assessment of CVD risk factors,
including:Measurement of “traditional” CVD risk factors in all patients;
Individual decision-making regarding measurement of selected
“CKD-related” CVD risk factors in some patients.
-Recommendations for CVD risk factor reduction should take into
account the “highest-risk” status of patients with chronic kidney disease.

Prevention of Uremic Complications:
Just a Word About Immunizations
• Don’t forget to continue routine immunizations, e.g.– Tetanus
– Pneumococcus
– Influenza
• Hepatitis B– Check for immunity first--ie, hepatitis B sAb, sAg, cAb– Those who are immune or have chronic infection do not
need the vaccine.– All others should receive the vaccine. Don’t wait for dialysis!
Patients with advanced chronic kidney disease are lesslikely to gain immunity from the vaccine. Consider for allStage 3 or greater CKD patients!

THANKS