chapter 34 angioscopically assisted...
TRANSCRIPT

CHAPTER 34 Angioscopically Assisted Thromboembolectomy Thomas J Fogarty Christopher K Zarins Kenneth L Serra Christine E Newman and George D Hermann
lnrroduced In 19fi3 the balloon em bolectomy carhertr halgt proved to be ~ n im porranc contribution fO rhe deveJopmtnt of endovascular devices to assIst in the treatmen t of peripheral vascular ocdusi~e disease (l2) Ie has al~o provided a template for the deslgn of orher more speuabzed cltl(hner tools to address the remova l of the residual thrombus associmed with incom plcre throm boem bolectomy Before the adven r of balloon embolectomy Cllti)e(Cr technique gturgicaJ prncedures for removJIlg thrombus were tnwghr with complicashytions that resulted in high patient mortality md 1110(shy
hid it) USIng the embolectomy catheter to remove ac ute peripheral emboli has improed surgical outcome and conseq uently patiem survival Independent studies con shyducted by Tawes er a l (3) Ellior ct al (4 ) Abbott e( al L5) and Camhria an d Ahbott (6) have shown limb sa lshyvage ra tes of 85 to 95 with a ttendant l1 ortil lity cares reduced to 10 to 20ltgt1ltgt
Going beyond [he basic em boltcromy pro(edure new catbeter-based technologIes developed from a m()r~ lIl-depth knmvledge and understanding of (he niology of tht vacular occlusive disease process have em ergd to addrc)) the variou~ progressive 5laws of disease In so doing the less invasive endovascubr field has evolved to
indude man) n~w moda hties WhOil primary applicmion is not to physically remove th romboem bolic materia l but
to pr()ide assistance in 1) diagnosis 2 ) facil itation of the therapemie endovascu la r su rgical proa d ure and 3)
postoperative eva luation of rhe resultanf efficacy of [he surgical intervention These modalities include angllr scopy [hat allovs a 3600 endoscopic VIsualization of vesshysel lumen and th e more nccntlr introduced intral uminal Doppler ultrasonic imaging which provides an echo imlt1ge of rhe inrima and su rround ing li ~sue structures The followmg will describe applications suited to anglOscnpy and will specifically address the adva ntage~ and disadvantages associated with the llse of angioscopy tl thromboembol ectomy
Angioscopy Angioscopy may be defined simply as the end oscopic impccrioll of the lllrcrior of a blood vessel (7) Conshystra ined by the inappropriately sized instrumen ra tion ~a ilab le ar [he till1 and the diffic ulties with ligh t rmnsshymiss ion the ea rl iest attempt~ at endoscopic vlsualizashytiOll o f blood vessels had limited Sllccess Early ellcioshy~copes were large and infle xible and offered POOf
visualizmiddotuion in an opaque visual fi eld Ovcr the past 20 y~ars rhe development of ~maller tlexible and maneuvershyable endoscopcs videocamera technology ~nd improved
445
446 Part V Occlusive Arterial Diseases
irrigttion management has allowed surgeons to more accurately visualize the intraluminal field
Angioscopy experienced increased usage within the vascular surgery specialty after the benefits of using laparoscope~ within the general surgery field were documented (8) Currently angioscopic instrumentation not only offers valuable diagnostic capability but also may bc used adjunctivdy with other endovascular therashypeutic devices Angioscopy is used as a method of conshytrolled guidance to aid visualization within vessels when patients undergo procedures such as thromboembolecshytomy atherectomy artenovenom fistula graft revision in situ bypass venous valvulotomy and stent deployment
Potential diagnostic applications for angioscopy have been extensively described in the literature (9-11) They mclude but arc not limited to the following
1 intraluminal evaluation of traumatic arterial lllJury
2 in vessel occlusion defining the character and consistency of plaque whether it is thromboti( or atheromatous
3 direct correlation of angiographic findings 4 diagnosing pulmonary embolism 5 assessing the integrity of vascular reconstrucshy
nons 6 directly interrogating veins for bypass suitability 7 localizing discrete venous valves and branches
III vein preparation for 1Il situ bypass 8 evaluating coronary arteries 9 evaluation and location of l11ultifocal lesions
to choose a therapeutic modality 10 detection of potentially significant intimal flaps
and thrombi undetectable by Doppler ultrasolllc exammatlon
11 providing an alternat ive to angiographic assessshyment of reconstructions and detection of vessel abnormalities
As a monitorillg tool angloscopy is used in the treatshyment of vascular disease to provide dir~ct visualization during or afrer the following intcrvcnrional procedures
1 ll1fusion therapy (ie thrombolytic vasodilator treatment)
1 thromboembolectOmy 3 balloon dilatation or angioplasty 4 atherecromy 5 endarterectomy 6 valvulotomy 7 vein branch ligation
Proper angioscopic evaluation has been shown to affect the duration of a patients hospitahzation (12) and has been shown to be a safe SImple effective altershynative or adjunctive procedure to intraoperative angioshygraphy (13) To better appreciate the application of angioscopy assistance in thromboembolectomy the basic anglOscoplC system components and functionality should be understood
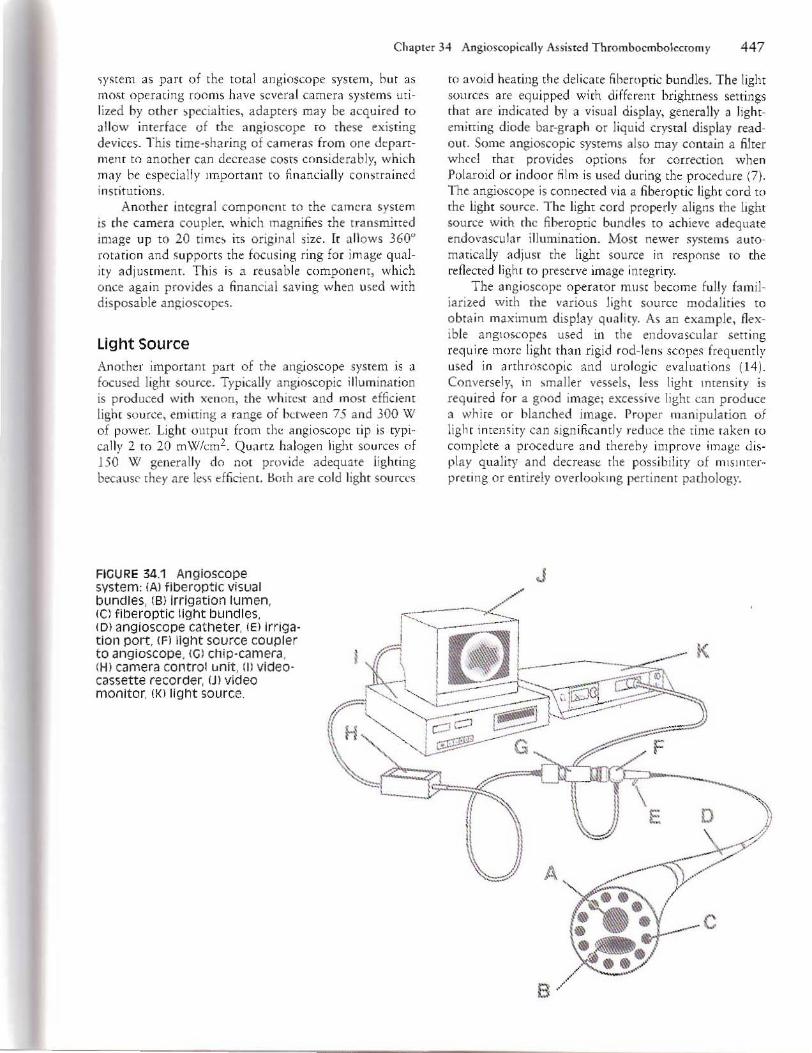
Angioscopic Instrumentation Angioscope The viewing tip of the angioscope is shown III Figure 341 It consists of a flexible catheter comprising one or two fiberoptic light bundles a fiberoptic image bundle and a working channel that is frequently used as an irrishygation port or to introduce guidewires or other intrashyvascular tools Currently anglOscopes come in lengths of 20 to lOa em with distal tips ranging III diameter from 06 to 7 mm The degree of variation 1Il angioscope components is directly related to the diameter of the catheter In smaller-diameter anglOscopes fewer fiberopshytic fibers can be accommodated necessitating exclusion of the working channel in many lllstances As stronger more inrense light sources become available it may be possible to decrease the light bundlts from tWO to one thus allowing room to accommodate the important working channel in all angioscopes
Fiberoptic bundlts can either be drum wound (leached hundles) consisting of individual fibers bound at the ends or three glas~ (fused bundles) which allows the scope size to be reduced by fUSIng individual fibers into one cohesive strand The drum wound angioscopes are nondisposable owning to their high cost while the fused bundle units are less expenSIve and disposable The angioscope is steered by passive guidance tracking with a guidewirc or activating tip deflection manually with a control button on the angioscope handl e More advanced deSIgns have incorporated an operatorshycontrolled deflecting tip allowing greater maneuver ability of the angioscope within the vessel This feature gIves the surgeon the ability to guide the anglOscope into the appropnate vessel conduit when encounrerlllg bifurcations or to more easily visualize branches or tributaries Two-way deflecting systems will allow 45deg deflection In one direction and up to 90 deflection in the oppo~ite direction for a more complete endolumishynal interrogation The flexibility of these soft deflecting tips reduces the potential for intimal damage
The proximal end of the catheter is attached directly to the angioscope The angioscope usually supshyports an Irngatiun port an attachment to the light source and an attachment to a miniature camera This camera acts a~ a small telescope outputting to an obsershyvation site which may be the viewers eye or through a standard videocassette recorder to a high-resolution monitor The video display provides real-time visual feedback during the p[(Judurc and a vid eo record of the Intervention for later use and procedure documentation
Camera System The camera system on an anglO~cope converts the image picked up at the proximal end of the ~cope proshyjected via the fiberoptic bundles mto a digital Image that is transmitted to the eyepiece or the display on the vJdeo monitor A fev manufacturns mdude a camera
Cllilplr 34 Aogiosoopically Assisled T hromboembolectomy 447
~y~tem as part of the total angioscope system hut as most operating woms have several camera systems utishylized by ath tr )pecia lties adapters may be acqu ired to allow imerface of the angioscope ro these existing devices This t ime-sha ring of eame ra~ from one departshyment to anmher can decreJse COStS considerably which may he especia ll y Important to fi nancially co nstrained institutions
Another integra l co mponCIH to the camera system is (he ca mera coupler which magnifies [he t ransmined image up to 20 ti me it s orig inal size It a llows 3600
rotation and suppons the focusi ng ring for image qualshyity adjustment This is a reusa ble component which once aga in provides a fina ncilt1l saving when mcd with d isposable angioscopcs
Light Source Another imponant part of thl angioscope system is a focused light so urce Typica ll y angimcopic illum ination is produced with xenon the whitest and mo~t efficient light source emitting a range of between 75 and 300 W of power Ligh( ompm from the angioscopc tip is tyPIshyca lly 2 to 20 mW(m2 Quartz halogen light so urces of 150 W genera lly do not pr~)V ide adequlte lighting because they are legt~ d ficient HOEll a re cold light sources
FIGURE 341 Angloscope System A) flberoptfc visual bundles (8) Irrigation lumen
t() avoid heating the del icate fi heroptic bundles The light sources are equipped with different brightness settings that are indicated by a visual display generally (l lightshyemirring d iode bar-graph or liqu id ctystal d isplay readshyout Some angioscopic systems also may conta in a filter wheel that provides options for correction w hen P()laroid or indoor film is used during the procedure (7) The mgioscope is connected via a fibero ptic light cord to
the light source The light cord properly aligns the light sou rce with (he fi heroptic bundlls to acll1(~v~ ad~quate tndovJscular illumination Most newer systems autoshymaricltltiy adjust the light source in re~p()nse to the reflected li ght to preserve image integrity
The angioscope operatOr mu st become fully famil shyiarized with the vario us light source modal ities to
obta in maxim um displa y qua lity As an exam ple flexshyib le anglOscopes used in the endovascular sen ing requ ire more light than rigid rod-lens scope~ freqllently used in arth r()~copic and uro logic evaluations (14 ) Conversel y in ~maller vessels less light lntensit ~middot is required for a good image Ixcessive light can produce n whi re o r blanc hed image Proper manipula tion of light intemity cln sign ificantly nduce the time take n m complete a procedure and therehy improve image disshyplay quality and decrease the possib ility of mlSl ntershyprecing or entirely overlookll1g pertinent pachology
J
(e) fiberoptic light bundles (0) angioscoOeuro catheter IE) Irrigashytion port (Fj 119ht source CO UPler to angioscope (G) chip -camera (HI camera controi llnit fIl videoshycassette recorder U) video monitor (Klll gh t source
F
E
A
c
8
448 Pari V Ocdusie Arlerial Disuses
Video Monitor A high-resolution color video monitor IS In indispcmshyaoll pan of an ilngioscope system This tcthnologr emerged from the gasr rointestin11 endoscopIc sysrem rhar dcmonMrared the suplriority o f di rect videoendosshycopy Early angioscope designs incorporated eyeplecc~ simi lar to l urologists cystOscope for di rec( visualizashy(ion o f the intralu minal splt1ce This viltualizuion techshynique pto ed cu mbersome for (he ascula r surgeon who is often required to move abou t within the sterile operating field or change position during an operat ion The video moniror alleviates these mobility mmtrainrs and provides the opportunity for rhe entire surgical team to monimr the proced ure In most modern opershyating rooms angioscopic mon itonng is iewed on a wlor video display
The video monitor display is cspecil il y useful as a tool to assist in traini ng d inicians in angioscopic techmiddot nique The l ngioscopic image is displayed as a small bright circle on rhe ideo monitor Newer systems allow digirizaTion of rh~ image to fill the entire screen for easier viewing A high-quality monitor caplble of displaying crisp dean color images wiU enable prec ise differentittion of endoluminal d isease characterinics As in the previous discusion of lighT source coupling proper connelt fion of elmlra clements to video display is crit ical to clear iSUll izniun
Irrigation System Irriga tion systems are critical to an angioscopy system ye t arc one of th e mtl~t overlooked component~ Tht vascular SYlum nnli ke the gas roimes tin ai uro logic or arthroscopic fields po~es a unique challenge in that its visual field is obscured by pllJsltltile ~w i rling opaque blood As nooILiminal angioscopic fechnology hai been borrow~d from th~se other endoscopic modalities the irrigalio n ystcms successfull y used in genera l surgery ha e pro ed to b~ inappropria te for endmasshycular applications Oercoming this obsracle hy fi nding bem r ways to cl iminHe baekflow and displace blood from the visual fidd is still an uea of devc1upment Recogniz ing th e s t rcngth~ and limitations of cu rrent irrigation systcms will impro e the video image and minimize complicat ions associated with nUld ovcrload Currentl three types o f irrig1tion system are availahle (0 tht vascula r surgeon (Fig 3421
The bltlsic irrigalion s)s(em consists of a sali ne bag with a line directly artached to (he irrigation port on the angioscopc (Fig 342A) The irrigating ~J lu tion bag when suspended on 1 pole used fo r intra~nous drip provide~ a source of co nstant pa~s i e pr(ssure tha t clears the visual intraluminal field Alternatively )1 asmant mar sq ueeze the bag either h~ hand or with a blood pressure cuff placed around th l bag while pinching off the direct li ne TO pro ide arying amounts of pressure as deemed appropriare to clear the
o
A
B
o
c
Pinch Valve
FIGURE 342 VariOUS angloscope irrlga iOn systems fA simple saline bag irrigation system f81peristaltic foot middotactivated pump fe) foot -activated pressure vessel pump
field The disadvantages of this somewha t cumbetsome tnhnique are tw()fold monitori ng the amount of fl uid infused into the e~sel often can he unreliable and il is difficu h to ~ ccunltely regu late the Auid pres~ure This initial approach has been la rgely abandoned
A moce advanced infusion irrigaion systtm is the roller pu mp IFig 342B) This sySTem is more sophi~tj cated than the passive pressure sa line bag setup in that a roller pump activated by a foot switch crcate~ a pe rlmiddot staltic infusion of sa line eliminating rhe need tn coorshydinate sa li ne infusion willl an assistant Furthermore rhe flow rafe ca n be preset co a desired level emin ing from 10 TO 400 Ill i per minure from the angioscopt rip and rhe volume of infused fl uid can be continuallv monitored aurom3tiClt1Ily A fairly high pressure level i~ required ro rransmit Il uid down the sma ll-diameter angioscopic work ins clulOnel over I distance of up to 100 em The period of high-pressure infusion is temposhyrary and gener311y not of great concern but should be considered when operat ing within a dosed s~rs re m
The ollcr pump although t provides ~~veral au tomiddot mared fcatu res i~ nOt without drawbacks When the foot SWitch is initially 3ni 1ted sali ne is infused at a
Chapter 34 Angioscopically Assisted Thromboembolectomy 449
low pressure unt il the roller pump build s up to rh e de ired set speed This shorr period o f low-pressure infusion is insufficienr to displalte blood and dea r the visual held yet some volume of saline h~l S been ltldded to the patients vascu lar system rncreasing fl uid load whil e fading to maxllm ze the rime spent visu ally intershyrogating the vessel Also becau~e the pump IS not responsive to flu id bui ldup an d pre~sure feedback vesshysels infused wirh in a closed system (ie disnl Jlr cla mped vessels wi th occluded side branches) lIlay undergo a dramatic increase in intra-arterial pressure that has the potential to damage the ve~sel waJl among othel vascu lar complicatimls Curre ntly rherc is no effective mea n~ to com pensate fo the potential pre~s ure buildup u~ ing the roller pumps because (h ey are not pressurl $ensitive Conseq uendy care should be taken to monitor fluid ind ucrion with rhis system
The rhird irriga rion system combines the -d va nshyt1ges of the two previously dc~cribed systems (Fig 342C) The release of irrigatio n fluid (contai ned in a ali ne-filled bag housed within a press ure vessel) is conshytrolled by pressure changes initiated when an onJo ff foot )witch is activitcd A bolus of fluid in rhe range of 250 to 350 ml per minUTe may be infused to quickly clear the visual field when baddlow is encou ntered wh ile 10w~llo infusion at 60 ro 80 ml per minute is us ually adequate to maintai n a constant unobstructed field of view In addition to having an external pressure regul ator this irrigation system is pressure ciependenr thathy OVerC0l11111g the problems assoClated wi th inrrashyarten1 pressure buildu p and minlllllzmg the ri sk of fluid oved oad Usually 21 to 30 psi IS sufficient (Q proshycure a d ear visual field in the ileofemoral system and below (14) A pinch vahe ensures that the ini tial infushyStOll () f saline will he ma imined at the preset pressu re thereby providing rapid clearing of the visual fi eld and saving procedure time and 1Il1IleCessary fluid ad tn imstrashynon Tot al infused volume ~h o uld be carefully monishy(Ored co preent patient fl uid oerload O fte n newer Ifrigation systems have heen designed with an autoshymatic shut-off fea ture as a ~afety mechanism in tracki ng tluid infus ion to alen [he dinician to fl uid admi niHra~ [I on volumes before reac ht ng a lOOO-ml mfusion level
operative setup Optimal utilization of rhe angioscopc in surgery requ ires omplete familiarity with the equ ipmenr and its approshypriate loca tion relative to the sterile ~ lIfgica l fi eld The ltlstrumenratlOl1 includ ing the chip-videocamera ca mshyera coup ler light source videocassette recorder video d l ~p lay mOllitOr and irrigation pump shou ld be mounted on a mobile cart (lpposite the surgeon Duplishycate display monitors may he mounted at OIher st ra tegic locations for easy visualiza tiOIl of rhe procedu re hy the other members of the su rgical ream as appropriate
The ste rile angioscope is placed on a separate table so that prepa ration for angioscopy can be made withshy
out distllrbitlg the surgical p reparation of the operati ve site PIeopenaive preparations should include connecshyt ion of the camera to the light source focusi ng the angioscope and white-balancing the light for proper co lor before using the mstrumentation in the case The angioscope its co nnecting cable lnd irrigation tubing are brought around th e angl0~c(1p i s t and secured to the drapes over the chest of rhe patient (15)
Operative Considerations for AngioscopyshyAssisted Thromboembolectomy A sttndard method of angioscopic exam mati on shou ld be developed for each angioscopic apphc3tioll and ~hould be varied according to the operative procedure and th e nature of the region of inte rest Mill er describes Llcil procedures in his recent work Angioshyscopy Itl rroducrion and Bltlsic Techniq ues wh icn tne intervenriona list may find useful as a template for ind ishyvidualizing operative prOTOcols ( 16) When using angioscopy w assist during throm boembolectomy choosing the proper size ltl T1 gioscope IS of paramount importanlte The diamete r of the angioscope shou ld be the largest that can be easily introd uced into the vem1 giving due considera rion to lumi nal tapering as rhe cathete r is advanced Carefu l angioscope selection will min imize visualization difficulties such as dark or hlanc hed images and reduce tle danger of ind ucing spasm in a native artery
New Thrombectomy Devices A grea ter understandmg of the pathology of peripheral vascular disease was brought about in parr by improved vis ualiza tion modali ties This in rurn ha~ prompted the development of new thrombeCTOmy devices designed to address the various stages of ath eroshy~lerotic disease Two ~uch rools ha ve recently been added to the surgeons endovascular instrumentation arnU mentllrium Both the corkscrew-shaped adherenr clot catheter and the open~V i re graft thromhectomy catheter (Baxter Healthcare Corp Vascular Division Irvine C lli) are deSigned to more complete ly remove adherent throm botic material after embol ectomy and their benefi cial dfects cnn be easily docum ented when th~y He used in conj unoioll with angioscopy
Adherent Clot Catheter Figure 343 is a drawing showing rhe longitudinally colshyl ap~ed insertion position of the adherent clot catheter ti p The device comim of a tlexible catheter with a disshytallarex-covered coiled cable at its tip A rhu11 b-ilctishyvated lever on the instrument hnndle allows the surgeon to adjust rhe pi tch of the co rkscrew membrJne from a fully collapsed sman~dia meter position to a tightly spiraled retracted con ligu ration with a diameter of up to 10 mm (14) By advancing the catheter in the
450 Part V Occlusive Amrial Diseasegt
low-profi le collapsed position then expanding it to its wider-diameter con figurat ion adherenr thrombus is grasped by the closing spi r1l loops of the corkscrew membrane (Fig 344 ) In the sa me fam iliar manner an em bolectom ) procedure is perfo rmed the adheren t clot catheter is withd rawn in its expanded posi tion toward the aneriotomy and the clot is removed manually The pitch of the rerr iev3 1 element may be adjusted b) the thumb lever if resistance is encounter ld during the withdrawa l process (0 ad iu~t the gripping force during withdrawa l
Graft Thrombectomy catheter The distal working eilmem of th l graft thrombectomy ca th ecer is designed much rhe same as the adherem dot catheter (Fig 34 5) Both use the principle of a hand shyoperated expandab le variable-pitch coil to grasp and remove adherent thrombus However two features difshyferentia te the devices Unlike the adherent dOt catheter whic h is composed of one membrane-covered wire the grafr thrombectomy ca theter is constructed using twO helically arranged exposed wire~ These tWO wires are d iscally mounted on a central retractable wire in an opposi ng ldt-handed and right-handed helical arrangeshymemo In both ca rherer designs rhumb-activated retracshydon of rhis centra l wire causes the respective coils (Q
expand in dia meter The lack o f a latex membrane covshy
ering over rhe helica Jl r arra nged wires makes the graft rhrnmhecromy c-u heter parricularly well suiled for removal of adhe rent throm bus oc d isrupted neoinrima commonly asgtociattd with symher ic grafts
Surgical Technique Removal of Adherent Thrombus in Native Vessel The follow ing is it de~crip[ion of an angiolt(opy-ascisted [hrom~omy of the superficial fe moral artery and poplitea l arrer) containing fresh throm hus with undershylying adherent cloT
Afttr the angioscop) system is white-balanced and prepared fo r use a ttrmdud cutdown is madt OVtr the femoral triangle Va~cular clamps are applied to the proximal superficial lOd the deep femoral arteries An 3T1eriotomy is made JUSt proximal to the br1nch of the deep femoral artery in the superficial femora l artery A sta ndard 3 or 4 Fr balloon embolectomy catheter is used to remove soft thrombus in the major vessds of the femoropopliteal srstem
It is usdul in fact imptrativC to reconStruct the d ot with removed clot segments on a towel to provide in shysight imo the anatomic location structure dimensions and charlcter of rhe d ot Otten a meniscus is formed at the distal end of th e thrombus at the flow boundary of th e dista l pa rent brmch Reconstruction of the clot with
A
B
f
c
FIGURE 343 Adherent ClOt catheter (A) catheter tip In Its COllapsed lowest-profile setting (8) cathmiddot eter tip In medlummiddotprofile setting showing partiall y retracted thumb lever (el fully retracted and expanded catheter tip
FIGURE 344 Adherent clot cathetEr retrieving adherent thrombus
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993

446 Part V Occlusive Arterial Diseases
irrigttion management has allowed surgeons to more accurately visualize the intraluminal field
Angioscopy experienced increased usage within the vascular surgery specialty after the benefits of using laparoscope~ within the general surgery field were documented (8) Currently angioscopic instrumentation not only offers valuable diagnostic capability but also may bc used adjunctivdy with other endovascular therashypeutic devices Angioscopy is used as a method of conshytrolled guidance to aid visualization within vessels when patients undergo procedures such as thromboembolecshytomy atherectomy artenovenom fistula graft revision in situ bypass venous valvulotomy and stent deployment
Potential diagnostic applications for angioscopy have been extensively described in the literature (9-11) They mclude but arc not limited to the following
1 intraluminal evaluation of traumatic arterial lllJury
2 in vessel occlusion defining the character and consistency of plaque whether it is thromboti( or atheromatous
3 direct correlation of angiographic findings 4 diagnosing pulmonary embolism 5 assessing the integrity of vascular reconstrucshy
nons 6 directly interrogating veins for bypass suitability 7 localizing discrete venous valves and branches
III vein preparation for 1Il situ bypass 8 evaluating coronary arteries 9 evaluation and location of l11ultifocal lesions
to choose a therapeutic modality 10 detection of potentially significant intimal flaps
and thrombi undetectable by Doppler ultrasolllc exammatlon
11 providing an alternat ive to angiographic assessshyment of reconstructions and detection of vessel abnormalities
As a monitorillg tool angloscopy is used in the treatshyment of vascular disease to provide dir~ct visualization during or afrer the following intcrvcnrional procedures
1 ll1fusion therapy (ie thrombolytic vasodilator treatment)
1 thromboembolectOmy 3 balloon dilatation or angioplasty 4 atherecromy 5 endarterectomy 6 valvulotomy 7 vein branch ligation
Proper angioscopic evaluation has been shown to affect the duration of a patients hospitahzation (12) and has been shown to be a safe SImple effective altershynative or adjunctive procedure to intraoperative angioshygraphy (13) To better appreciate the application of angioscopy assistance in thromboembolectomy the basic anglOscoplC system components and functionality should be understood
Angioscopic Instrumentation Angioscope The viewing tip of the angioscope is shown III Figure 341 It consists of a flexible catheter comprising one or two fiberoptic light bundles a fiberoptic image bundle and a working channel that is frequently used as an irrishygation port or to introduce guidewires or other intrashyvascular tools Currently anglOscopes come in lengths of 20 to lOa em with distal tips ranging III diameter from 06 to 7 mm The degree of variation 1Il angioscope components is directly related to the diameter of the catheter In smaller-diameter anglOscopes fewer fiberopshytic fibers can be accommodated necessitating exclusion of the working channel in many lllstances As stronger more inrense light sources become available it may be possible to decrease the light bundlts from tWO to one thus allowing room to accommodate the important working channel in all angioscopes
Fiberoptic bundlts can either be drum wound (leached hundles) consisting of individual fibers bound at the ends or three glas~ (fused bundles) which allows the scope size to be reduced by fUSIng individual fibers into one cohesive strand The drum wound angioscopes are nondisposable owning to their high cost while the fused bundle units are less expenSIve and disposable The angioscope is steered by passive guidance tracking with a guidewirc or activating tip deflection manually with a control button on the angioscope handl e More advanced deSIgns have incorporated an operatorshycontrolled deflecting tip allowing greater maneuver ability of the angioscope within the vessel This feature gIves the surgeon the ability to guide the anglOscope into the appropnate vessel conduit when encounrerlllg bifurcations or to more easily visualize branches or tributaries Two-way deflecting systems will allow 45deg deflection In one direction and up to 90 deflection in the oppo~ite direction for a more complete endolumishynal interrogation The flexibility of these soft deflecting tips reduces the potential for intimal damage
The proximal end of the catheter is attached directly to the angioscope The angioscope usually supshyports an Irngatiun port an attachment to the light source and an attachment to a miniature camera This camera acts a~ a small telescope outputting to an obsershyvation site which may be the viewers eye or through a standard videocassette recorder to a high-resolution monitor The video display provides real-time visual feedback during the p[(Judurc and a vid eo record of the Intervention for later use and procedure documentation
Camera System The camera system on an anglO~cope converts the image picked up at the proximal end of the ~cope proshyjected via the fiberoptic bundles mto a digital Image that is transmitted to the eyepiece or the display on the vJdeo monitor A fev manufacturns mdude a camera
Cllilplr 34 Aogiosoopically Assisled T hromboembolectomy 447
~y~tem as part of the total angioscope system hut as most operating woms have several camera systems utishylized by ath tr )pecia lties adapters may be acqu ired to allow imerface of the angioscope ro these existing devices This t ime-sha ring of eame ra~ from one departshyment to anmher can decreJse COStS considerably which may he especia ll y Important to fi nancially co nstrained institutions
Another integra l co mponCIH to the camera system is (he ca mera coupler which magnifies [he t ransmined image up to 20 ti me it s orig inal size It a llows 3600
rotation and suppons the focusi ng ring for image qualshyity adjustment This is a reusa ble component which once aga in provides a fina ncilt1l saving when mcd with d isposable angioscopcs
Light Source Another imponant part of thl angioscope system is a focused light so urce Typica ll y angimcopic illum ination is produced with xenon the whitest and mo~t efficient light source emitting a range of between 75 and 300 W of power Ligh( ompm from the angioscopc tip is tyPIshyca lly 2 to 20 mW(m2 Quartz halogen light so urces of 150 W genera lly do not pr~)V ide adequlte lighting because they are legt~ d ficient HOEll a re cold light sources
FIGURE 341 Angloscope System A) flberoptfc visual bundles (8) Irrigation lumen
t() avoid heating the del icate fi heroptic bundles The light sources are equipped with different brightness settings that are indicated by a visual display generally (l lightshyemirring d iode bar-graph or liqu id ctystal d isplay readshyout Some angioscopic systems also may conta in a filter wheel that provides options for correction w hen P()laroid or indoor film is used during the procedure (7) The mgioscope is connected via a fibero ptic light cord to
the light source The light cord properly aligns the light sou rce with (he fi heroptic bundlls to acll1(~v~ ad~quate tndovJscular illumination Most newer systems autoshymaricltltiy adjust the light source in re~p()nse to the reflected li ght to preserve image integrity
The angioscope operatOr mu st become fully famil shyiarized with the vario us light source modal ities to
obta in maxim um displa y qua lity As an exam ple flexshyib le anglOscopes used in the endovascular sen ing requ ire more light than rigid rod-lens scope~ freqllently used in arth r()~copic and uro logic evaluations (14 ) Conversel y in ~maller vessels less light lntensit ~middot is required for a good image Ixcessive light can produce n whi re o r blanc hed image Proper manipula tion of light intemity cln sign ificantly nduce the time take n m complete a procedure and therehy improve image disshyplay quality and decrease the possib ility of mlSl ntershyprecing or entirely overlookll1g pertinent pachology
J
(e) fiberoptic light bundles (0) angioscoOeuro catheter IE) Irrigashytion port (Fj 119ht source CO UPler to angioscope (G) chip -camera (HI camera controi llnit fIl videoshycassette recorder U) video monitor (Klll gh t source
F
E
A
c
8
448 Pari V Ocdusie Arlerial Disuses
Video Monitor A high-resolution color video monitor IS In indispcmshyaoll pan of an ilngioscope system This tcthnologr emerged from the gasr rointestin11 endoscopIc sysrem rhar dcmonMrared the suplriority o f di rect videoendosshycopy Early angioscope designs incorporated eyeplecc~ simi lar to l urologists cystOscope for di rec( visualizashy(ion o f the intralu minal splt1ce This viltualizuion techshynique pto ed cu mbersome for (he ascula r surgeon who is often required to move abou t within the sterile operating field or change position during an operat ion The video moniror alleviates these mobility mmtrainrs and provides the opportunity for rhe entire surgical team to monimr the proced ure In most modern opershyating rooms angioscopic mon itonng is iewed on a wlor video display
The video monitor display is cspecil il y useful as a tool to assist in traini ng d inicians in angioscopic techmiddot nique The l ngioscopic image is displayed as a small bright circle on rhe ideo monitor Newer systems allow digirizaTion of rh~ image to fill the entire screen for easier viewing A high-quality monitor caplble of displaying crisp dean color images wiU enable prec ise differentittion of endoluminal d isease characterinics As in the previous discusion of lighT source coupling proper connelt fion of elmlra clements to video display is crit ical to clear iSUll izniun
Irrigation System Irriga tion systems are critical to an angioscopy system ye t arc one of th e mtl~t overlooked component~ Tht vascular SYlum nnli ke the gas roimes tin ai uro logic or arthroscopic fields po~es a unique challenge in that its visual field is obscured by pllJsltltile ~w i rling opaque blood As nooILiminal angioscopic fechnology hai been borrow~d from th~se other endoscopic modalities the irrigalio n ystcms successfull y used in genera l surgery ha e pro ed to b~ inappropria te for endmasshycular applications Oercoming this obsracle hy fi nding bem r ways to cl iminHe baekflow and displace blood from the visual fidd is still an uea of devc1upment Recogniz ing th e s t rcngth~ and limitations of cu rrent irrigation systcms will impro e the video image and minimize complicat ions associated with nUld ovcrload Currentl three types o f irrig1tion system are availahle (0 tht vascula r surgeon (Fig 3421
The bltlsic irrigalion s)s(em consists of a sali ne bag with a line directly artached to (he irrigation port on the angioscopc (Fig 342A) The irrigating ~J lu tion bag when suspended on 1 pole used fo r intra~nous drip provide~ a source of co nstant pa~s i e pr(ssure tha t clears the visual intraluminal field Alternatively )1 asmant mar sq ueeze the bag either h~ hand or with a blood pressure cuff placed around th l bag while pinching off the direct li ne TO pro ide arying amounts of pressure as deemed appropriare to clear the
o
A
B
o
c
Pinch Valve
FIGURE 342 VariOUS angloscope irrlga iOn systems fA simple saline bag irrigation system f81peristaltic foot middotactivated pump fe) foot -activated pressure vessel pump
field The disadvantages of this somewha t cumbetsome tnhnique are tw()fold monitori ng the amount of fl uid infused into the e~sel often can he unreliable and il is difficu h to ~ ccunltely regu late the Auid pres~ure This initial approach has been la rgely abandoned
A moce advanced infusion irrigaion systtm is the roller pu mp IFig 342B) This sySTem is more sophi~tj cated than the passive pressure sa line bag setup in that a roller pump activated by a foot switch crcate~ a pe rlmiddot staltic infusion of sa line eliminating rhe need tn coorshydinate sa li ne infusion willl an assistant Furthermore rhe flow rafe ca n be preset co a desired level emin ing from 10 TO 400 Ill i per minure from the angioscopt rip and rhe volume of infused fl uid can be continuallv monitored aurom3tiClt1Ily A fairly high pressure level i~ required ro rransmit Il uid down the sma ll-diameter angioscopic work ins clulOnel over I distance of up to 100 em The period of high-pressure infusion is temposhyrary and gener311y not of great concern but should be considered when operat ing within a dosed s~rs re m
The ollcr pump although t provides ~~veral au tomiddot mared fcatu res i~ nOt without drawbacks When the foot SWitch is initially 3ni 1ted sali ne is infused at a
Chapter 34 Angioscopically Assisted Thromboembolectomy 449
low pressure unt il the roller pump build s up to rh e de ired set speed This shorr period o f low-pressure infusion is insufficienr to displalte blood and dea r the visual held yet some volume of saline h~l S been ltldded to the patients vascu lar system rncreasing fl uid load whil e fading to maxllm ze the rime spent visu ally intershyrogating the vessel Also becau~e the pump IS not responsive to flu id bui ldup an d pre~sure feedback vesshysels infused wirh in a closed system (ie disnl Jlr cla mped vessels wi th occluded side branches) lIlay undergo a dramatic increase in intra-arterial pressure that has the potential to damage the ve~sel waJl among othel vascu lar complicatimls Curre ntly rherc is no effective mea n~ to com pensate fo the potential pre~s ure buildup u~ ing the roller pumps because (h ey are not pressurl $ensitive Conseq uendy care should be taken to monitor fluid ind ucrion with rhis system
The rhird irriga rion system combines the -d va nshyt1ges of the two previously dc~cribed systems (Fig 342C) The release of irrigatio n fluid (contai ned in a ali ne-filled bag housed within a press ure vessel) is conshytrolled by pressure changes initiated when an onJo ff foot )witch is activitcd A bolus of fluid in rhe range of 250 to 350 ml per minUTe may be infused to quickly clear the visual field when baddlow is encou ntered wh ile 10w~llo infusion at 60 ro 80 ml per minute is us ually adequate to maintai n a constant unobstructed field of view In addition to having an external pressure regul ator this irrigation system is pressure ciependenr thathy OVerC0l11111g the problems assoClated wi th inrrashyarten1 pressure buildu p and minlllllzmg the ri sk of fluid oved oad Usually 21 to 30 psi IS sufficient (Q proshycure a d ear visual field in the ileofemoral system and below (14) A pinch vahe ensures that the ini tial infushyStOll () f saline will he ma imined at the preset pressu re thereby providing rapid clearing of the visual fi eld and saving procedure time and 1Il1IleCessary fluid ad tn imstrashynon Tot al infused volume ~h o uld be carefully monishy(Ored co preent patient fl uid oerload O fte n newer Ifrigation systems have heen designed with an autoshymatic shut-off fea ture as a ~afety mechanism in tracki ng tluid infus ion to alen [he dinician to fl uid admi niHra~ [I on volumes before reac ht ng a lOOO-ml mfusion level
operative setup Optimal utilization of rhe angioscopc in surgery requ ires omplete familiarity with the equ ipmenr and its approshypriate loca tion relative to the sterile ~ lIfgica l fi eld The ltlstrumenratlOl1 includ ing the chip-videocamera ca mshyera coup ler light source videocassette recorder video d l ~p lay mOllitOr and irrigation pump shou ld be mounted on a mobile cart (lpposite the surgeon Duplishycate display monitors may he mounted at OIher st ra tegic locations for easy visualiza tiOIl of rhe procedu re hy the other members of the su rgical ream as appropriate
The ste rile angioscope is placed on a separate table so that prepa ration for angioscopy can be made withshy
out distllrbitlg the surgical p reparation of the operati ve site PIeopenaive preparations should include connecshyt ion of the camera to the light source focusi ng the angioscope and white-balancing the light for proper co lor before using the mstrumentation in the case The angioscope its co nnecting cable lnd irrigation tubing are brought around th e angl0~c(1p i s t and secured to the drapes over the chest of rhe patient (15)
Operative Considerations for AngioscopyshyAssisted Thromboembolectomy A sttndard method of angioscopic exam mati on shou ld be developed for each angioscopic apphc3tioll and ~hould be varied according to the operative procedure and th e nature of the region of inte rest Mill er describes Llcil procedures in his recent work Angioshyscopy Itl rroducrion and Bltlsic Techniq ues wh icn tne intervenriona list may find useful as a template for ind ishyvidualizing operative prOTOcols ( 16) When using angioscopy w assist during throm boembolectomy choosing the proper size ltl T1 gioscope IS of paramount importanlte The diamete r of the angioscope shou ld be the largest that can be easily introd uced into the vem1 giving due considera rion to lumi nal tapering as rhe cathete r is advanced Carefu l angioscope selection will min imize visualization difficulties such as dark or hlanc hed images and reduce tle danger of ind ucing spasm in a native artery
New Thrombectomy Devices A grea ter understandmg of the pathology of peripheral vascular disease was brought about in parr by improved vis ualiza tion modali ties This in rurn ha~ prompted the development of new thrombeCTOmy devices designed to address the various stages of ath eroshy~lerotic disease Two ~uch rools ha ve recently been added to the surgeons endovascular instrumentation arnU mentllrium Both the corkscrew-shaped adherenr clot catheter and the open~V i re graft thromhectomy catheter (Baxter Healthcare Corp Vascular Division Irvine C lli) are deSigned to more complete ly remove adherent throm botic material after embol ectomy and their benefi cial dfects cnn be easily docum ented when th~y He used in conj unoioll with angioscopy
Adherent Clot Catheter Figure 343 is a drawing showing rhe longitudinally colshyl ap~ed insertion position of the adherent clot catheter ti p The device comim of a tlexible catheter with a disshytallarex-covered coiled cable at its tip A rhu11 b-ilctishyvated lever on the instrument hnndle allows the surgeon to adjust rhe pi tch of the co rkscrew membrJne from a fully collapsed sman~dia meter position to a tightly spiraled retracted con ligu ration with a diameter of up to 10 mm (14) By advancing the catheter in the
450 Part V Occlusive Amrial Diseasegt
low-profi le collapsed position then expanding it to its wider-diameter con figurat ion adherenr thrombus is grasped by the closing spi r1l loops of the corkscrew membrane (Fig 344 ) In the sa me fam iliar manner an em bolectom ) procedure is perfo rmed the adheren t clot catheter is withd rawn in its expanded posi tion toward the aneriotomy and the clot is removed manually The pitch of the rerr iev3 1 element may be adjusted b) the thumb lever if resistance is encounter ld during the withdrawa l process (0 ad iu~t the gripping force during withdrawa l
Graft Thrombectomy catheter The distal working eilmem of th l graft thrombectomy ca th ecer is designed much rhe same as the adherem dot catheter (Fig 34 5) Both use the principle of a hand shyoperated expandab le variable-pitch coil to grasp and remove adherent thrombus However two features difshyferentia te the devices Unlike the adherent dOt catheter whic h is composed of one membrane-covered wire the grafr thrombectomy ca theter is constructed using twO helically arranged exposed wire~ These tWO wires are d iscally mounted on a central retractable wire in an opposi ng ldt-handed and right-handed helical arrangeshymemo In both ca rherer designs rhumb-activated retracshydon of rhis centra l wire causes the respective coils (Q
expand in dia meter The lack o f a latex membrane covshy
ering over rhe helica Jl r arra nged wires makes the graft rhrnmhecromy c-u heter parricularly well suiled for removal of adhe rent throm bus oc d isrupted neoinrima commonly asgtociattd with symher ic grafts
Surgical Technique Removal of Adherent Thrombus in Native Vessel The follow ing is it de~crip[ion of an angiolt(opy-ascisted [hrom~omy of the superficial fe moral artery and poplitea l arrer) containing fresh throm hus with undershylying adherent cloT
Afttr the angioscop) system is white-balanced and prepared fo r use a ttrmdud cutdown is madt OVtr the femoral triangle Va~cular clamps are applied to the proximal superficial lOd the deep femoral arteries An 3T1eriotomy is made JUSt proximal to the br1nch of the deep femoral artery in the superficial femora l artery A sta ndard 3 or 4 Fr balloon embolectomy catheter is used to remove soft thrombus in the major vessds of the femoropopliteal srstem
It is usdul in fact imptrativC to reconStruct the d ot with removed clot segments on a towel to provide in shysight imo the anatomic location structure dimensions and charlcter of rhe d ot Otten a meniscus is formed at the distal end of th e thrombus at the flow boundary of th e dista l pa rent brmch Reconstruction of the clot with
A
B
f
c
FIGURE 343 Adherent ClOt catheter (A) catheter tip In Its COllapsed lowest-profile setting (8) cathmiddot eter tip In medlummiddotprofile setting showing partiall y retracted thumb lever (el fully retracted and expanded catheter tip
FIGURE 344 Adherent clot cathetEr retrieving adherent thrombus
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993
Cllilplr 34 Aogiosoopically Assisled T hromboembolectomy 447
~y~tem as part of the total angioscope system hut as most operating woms have several camera systems utishylized by ath tr )pecia lties adapters may be acqu ired to allow imerface of the angioscope ro these existing devices This t ime-sha ring of eame ra~ from one departshyment to anmher can decreJse COStS considerably which may he especia ll y Important to fi nancially co nstrained institutions
Another integra l co mponCIH to the camera system is (he ca mera coupler which magnifies [he t ransmined image up to 20 ti me it s orig inal size It a llows 3600
rotation and suppons the focusi ng ring for image qualshyity adjustment This is a reusa ble component which once aga in provides a fina ncilt1l saving when mcd with d isposable angioscopcs
Light Source Another imponant part of thl angioscope system is a focused light so urce Typica ll y angimcopic illum ination is produced with xenon the whitest and mo~t efficient light source emitting a range of between 75 and 300 W of power Ligh( ompm from the angioscopc tip is tyPIshyca lly 2 to 20 mW(m2 Quartz halogen light so urces of 150 W genera lly do not pr~)V ide adequlte lighting because they are legt~ d ficient HOEll a re cold light sources
FIGURE 341 Angloscope System A) flberoptfc visual bundles (8) Irrigation lumen
t() avoid heating the del icate fi heroptic bundles The light sources are equipped with different brightness settings that are indicated by a visual display generally (l lightshyemirring d iode bar-graph or liqu id ctystal d isplay readshyout Some angioscopic systems also may conta in a filter wheel that provides options for correction w hen P()laroid or indoor film is used during the procedure (7) The mgioscope is connected via a fibero ptic light cord to
the light source The light cord properly aligns the light sou rce with (he fi heroptic bundlls to acll1(~v~ ad~quate tndovJscular illumination Most newer systems autoshymaricltltiy adjust the light source in re~p()nse to the reflected li ght to preserve image integrity
The angioscope operatOr mu st become fully famil shyiarized with the vario us light source modal ities to
obta in maxim um displa y qua lity As an exam ple flexshyib le anglOscopes used in the endovascular sen ing requ ire more light than rigid rod-lens scope~ freqllently used in arth r()~copic and uro logic evaluations (14 ) Conversel y in ~maller vessels less light lntensit ~middot is required for a good image Ixcessive light can produce n whi re o r blanc hed image Proper manipula tion of light intemity cln sign ificantly nduce the time take n m complete a procedure and therehy improve image disshyplay quality and decrease the possib ility of mlSl ntershyprecing or entirely overlookll1g pertinent pachology
J
(e) fiberoptic light bundles (0) angioscoOeuro catheter IE) Irrigashytion port (Fj 119ht source CO UPler to angioscope (G) chip -camera (HI camera controi llnit fIl videoshycassette recorder U) video monitor (Klll gh t source
F
E
A
c
8
448 Pari V Ocdusie Arlerial Disuses
Video Monitor A high-resolution color video monitor IS In indispcmshyaoll pan of an ilngioscope system This tcthnologr emerged from the gasr rointestin11 endoscopIc sysrem rhar dcmonMrared the suplriority o f di rect videoendosshycopy Early angioscope designs incorporated eyeplecc~ simi lar to l urologists cystOscope for di rec( visualizashy(ion o f the intralu minal splt1ce This viltualizuion techshynique pto ed cu mbersome for (he ascula r surgeon who is often required to move abou t within the sterile operating field or change position during an operat ion The video moniror alleviates these mobility mmtrainrs and provides the opportunity for rhe entire surgical team to monimr the proced ure In most modern opershyating rooms angioscopic mon itonng is iewed on a wlor video display
The video monitor display is cspecil il y useful as a tool to assist in traini ng d inicians in angioscopic techmiddot nique The l ngioscopic image is displayed as a small bright circle on rhe ideo monitor Newer systems allow digirizaTion of rh~ image to fill the entire screen for easier viewing A high-quality monitor caplble of displaying crisp dean color images wiU enable prec ise differentittion of endoluminal d isease characterinics As in the previous discusion of lighT source coupling proper connelt fion of elmlra clements to video display is crit ical to clear iSUll izniun
Irrigation System Irriga tion systems are critical to an angioscopy system ye t arc one of th e mtl~t overlooked component~ Tht vascular SYlum nnli ke the gas roimes tin ai uro logic or arthroscopic fields po~es a unique challenge in that its visual field is obscured by pllJsltltile ~w i rling opaque blood As nooILiminal angioscopic fechnology hai been borrow~d from th~se other endoscopic modalities the irrigalio n ystcms successfull y used in genera l surgery ha e pro ed to b~ inappropria te for endmasshycular applications Oercoming this obsracle hy fi nding bem r ways to cl iminHe baekflow and displace blood from the visual fidd is still an uea of devc1upment Recogniz ing th e s t rcngth~ and limitations of cu rrent irrigation systcms will impro e the video image and minimize complicat ions associated with nUld ovcrload Currentl three types o f irrig1tion system are availahle (0 tht vascula r surgeon (Fig 3421
The bltlsic irrigalion s)s(em consists of a sali ne bag with a line directly artached to (he irrigation port on the angioscopc (Fig 342A) The irrigating ~J lu tion bag when suspended on 1 pole used fo r intra~nous drip provide~ a source of co nstant pa~s i e pr(ssure tha t clears the visual intraluminal field Alternatively )1 asmant mar sq ueeze the bag either h~ hand or with a blood pressure cuff placed around th l bag while pinching off the direct li ne TO pro ide arying amounts of pressure as deemed appropriare to clear the
o
A
B
o
c
Pinch Valve
FIGURE 342 VariOUS angloscope irrlga iOn systems fA simple saline bag irrigation system f81peristaltic foot middotactivated pump fe) foot -activated pressure vessel pump
field The disadvantages of this somewha t cumbetsome tnhnique are tw()fold monitori ng the amount of fl uid infused into the e~sel often can he unreliable and il is difficu h to ~ ccunltely regu late the Auid pres~ure This initial approach has been la rgely abandoned
A moce advanced infusion irrigaion systtm is the roller pu mp IFig 342B) This sySTem is more sophi~tj cated than the passive pressure sa line bag setup in that a roller pump activated by a foot switch crcate~ a pe rlmiddot staltic infusion of sa line eliminating rhe need tn coorshydinate sa li ne infusion willl an assistant Furthermore rhe flow rafe ca n be preset co a desired level emin ing from 10 TO 400 Ill i per minure from the angioscopt rip and rhe volume of infused fl uid can be continuallv monitored aurom3tiClt1Ily A fairly high pressure level i~ required ro rransmit Il uid down the sma ll-diameter angioscopic work ins clulOnel over I distance of up to 100 em The period of high-pressure infusion is temposhyrary and gener311y not of great concern but should be considered when operat ing within a dosed s~rs re m
The ollcr pump although t provides ~~veral au tomiddot mared fcatu res i~ nOt without drawbacks When the foot SWitch is initially 3ni 1ted sali ne is infused at a
Chapter 34 Angioscopically Assisted Thromboembolectomy 449
low pressure unt il the roller pump build s up to rh e de ired set speed This shorr period o f low-pressure infusion is insufficienr to displalte blood and dea r the visual held yet some volume of saline h~l S been ltldded to the patients vascu lar system rncreasing fl uid load whil e fading to maxllm ze the rime spent visu ally intershyrogating the vessel Also becau~e the pump IS not responsive to flu id bui ldup an d pre~sure feedback vesshysels infused wirh in a closed system (ie disnl Jlr cla mped vessels wi th occluded side branches) lIlay undergo a dramatic increase in intra-arterial pressure that has the potential to damage the ve~sel waJl among othel vascu lar complicatimls Curre ntly rherc is no effective mea n~ to com pensate fo the potential pre~s ure buildup u~ ing the roller pumps because (h ey are not pressurl $ensitive Conseq uendy care should be taken to monitor fluid ind ucrion with rhis system
The rhird irriga rion system combines the -d va nshyt1ges of the two previously dc~cribed systems (Fig 342C) The release of irrigatio n fluid (contai ned in a ali ne-filled bag housed within a press ure vessel) is conshytrolled by pressure changes initiated when an onJo ff foot )witch is activitcd A bolus of fluid in rhe range of 250 to 350 ml per minUTe may be infused to quickly clear the visual field when baddlow is encou ntered wh ile 10w~llo infusion at 60 ro 80 ml per minute is us ually adequate to maintai n a constant unobstructed field of view In addition to having an external pressure regul ator this irrigation system is pressure ciependenr thathy OVerC0l11111g the problems assoClated wi th inrrashyarten1 pressure buildu p and minlllllzmg the ri sk of fluid oved oad Usually 21 to 30 psi IS sufficient (Q proshycure a d ear visual field in the ileofemoral system and below (14) A pinch vahe ensures that the ini tial infushyStOll () f saline will he ma imined at the preset pressu re thereby providing rapid clearing of the visual fi eld and saving procedure time and 1Il1IleCessary fluid ad tn imstrashynon Tot al infused volume ~h o uld be carefully monishy(Ored co preent patient fl uid oerload O fte n newer Ifrigation systems have heen designed with an autoshymatic shut-off fea ture as a ~afety mechanism in tracki ng tluid infus ion to alen [he dinician to fl uid admi niHra~ [I on volumes before reac ht ng a lOOO-ml mfusion level
operative setup Optimal utilization of rhe angioscopc in surgery requ ires omplete familiarity with the equ ipmenr and its approshypriate loca tion relative to the sterile ~ lIfgica l fi eld The ltlstrumenratlOl1 includ ing the chip-videocamera ca mshyera coup ler light source videocassette recorder video d l ~p lay mOllitOr and irrigation pump shou ld be mounted on a mobile cart (lpposite the surgeon Duplishycate display monitors may he mounted at OIher st ra tegic locations for easy visualiza tiOIl of rhe procedu re hy the other members of the su rgical ream as appropriate
The ste rile angioscope is placed on a separate table so that prepa ration for angioscopy can be made withshy
out distllrbitlg the surgical p reparation of the operati ve site PIeopenaive preparations should include connecshyt ion of the camera to the light source focusi ng the angioscope and white-balancing the light for proper co lor before using the mstrumentation in the case The angioscope its co nnecting cable lnd irrigation tubing are brought around th e angl0~c(1p i s t and secured to the drapes over the chest of rhe patient (15)
Operative Considerations for AngioscopyshyAssisted Thromboembolectomy A sttndard method of angioscopic exam mati on shou ld be developed for each angioscopic apphc3tioll and ~hould be varied according to the operative procedure and th e nature of the region of inte rest Mill er describes Llcil procedures in his recent work Angioshyscopy Itl rroducrion and Bltlsic Techniq ues wh icn tne intervenriona list may find useful as a template for ind ishyvidualizing operative prOTOcols ( 16) When using angioscopy w assist during throm boembolectomy choosing the proper size ltl T1 gioscope IS of paramount importanlte The diamete r of the angioscope shou ld be the largest that can be easily introd uced into the vem1 giving due considera rion to lumi nal tapering as rhe cathete r is advanced Carefu l angioscope selection will min imize visualization difficulties such as dark or hlanc hed images and reduce tle danger of ind ucing spasm in a native artery
New Thrombectomy Devices A grea ter understandmg of the pathology of peripheral vascular disease was brought about in parr by improved vis ualiza tion modali ties This in rurn ha~ prompted the development of new thrombeCTOmy devices designed to address the various stages of ath eroshy~lerotic disease Two ~uch rools ha ve recently been added to the surgeons endovascular instrumentation arnU mentllrium Both the corkscrew-shaped adherenr clot catheter and the open~V i re graft thromhectomy catheter (Baxter Healthcare Corp Vascular Division Irvine C lli) are deSigned to more complete ly remove adherent throm botic material after embol ectomy and their benefi cial dfects cnn be easily docum ented when th~y He used in conj unoioll with angioscopy
Adherent Clot Catheter Figure 343 is a drawing showing rhe longitudinally colshyl ap~ed insertion position of the adherent clot catheter ti p The device comim of a tlexible catheter with a disshytallarex-covered coiled cable at its tip A rhu11 b-ilctishyvated lever on the instrument hnndle allows the surgeon to adjust rhe pi tch of the co rkscrew membrJne from a fully collapsed sman~dia meter position to a tightly spiraled retracted con ligu ration with a diameter of up to 10 mm (14) By advancing the catheter in the
450 Part V Occlusive Amrial Diseasegt
low-profi le collapsed position then expanding it to its wider-diameter con figurat ion adherenr thrombus is grasped by the closing spi r1l loops of the corkscrew membrane (Fig 344 ) In the sa me fam iliar manner an em bolectom ) procedure is perfo rmed the adheren t clot catheter is withd rawn in its expanded posi tion toward the aneriotomy and the clot is removed manually The pitch of the rerr iev3 1 element may be adjusted b) the thumb lever if resistance is encounter ld during the withdrawa l process (0 ad iu~t the gripping force during withdrawa l
Graft Thrombectomy catheter The distal working eilmem of th l graft thrombectomy ca th ecer is designed much rhe same as the adherem dot catheter (Fig 34 5) Both use the principle of a hand shyoperated expandab le variable-pitch coil to grasp and remove adherent thrombus However two features difshyferentia te the devices Unlike the adherent dOt catheter whic h is composed of one membrane-covered wire the grafr thrombectomy ca theter is constructed using twO helically arranged exposed wire~ These tWO wires are d iscally mounted on a central retractable wire in an opposi ng ldt-handed and right-handed helical arrangeshymemo In both ca rherer designs rhumb-activated retracshydon of rhis centra l wire causes the respective coils (Q
expand in dia meter The lack o f a latex membrane covshy
ering over rhe helica Jl r arra nged wires makes the graft rhrnmhecromy c-u heter parricularly well suiled for removal of adhe rent throm bus oc d isrupted neoinrima commonly asgtociattd with symher ic grafts
Surgical Technique Removal of Adherent Thrombus in Native Vessel The follow ing is it de~crip[ion of an angiolt(opy-ascisted [hrom~omy of the superficial fe moral artery and poplitea l arrer) containing fresh throm hus with undershylying adherent cloT
Afttr the angioscop) system is white-balanced and prepared fo r use a ttrmdud cutdown is madt OVtr the femoral triangle Va~cular clamps are applied to the proximal superficial lOd the deep femoral arteries An 3T1eriotomy is made JUSt proximal to the br1nch of the deep femoral artery in the superficial femora l artery A sta ndard 3 or 4 Fr balloon embolectomy catheter is used to remove soft thrombus in the major vessds of the femoropopliteal srstem
It is usdul in fact imptrativC to reconStruct the d ot with removed clot segments on a towel to provide in shysight imo the anatomic location structure dimensions and charlcter of rhe d ot Otten a meniscus is formed at the distal end of th e thrombus at the flow boundary of th e dista l pa rent brmch Reconstruction of the clot with
A
B
f
c
FIGURE 343 Adherent ClOt catheter (A) catheter tip In Its COllapsed lowest-profile setting (8) cathmiddot eter tip In medlummiddotprofile setting showing partiall y retracted thumb lever (el fully retracted and expanded catheter tip
FIGURE 344 Adherent clot cathetEr retrieving adherent thrombus
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993

448 Pari V Ocdusie Arlerial Disuses
Video Monitor A high-resolution color video monitor IS In indispcmshyaoll pan of an ilngioscope system This tcthnologr emerged from the gasr rointestin11 endoscopIc sysrem rhar dcmonMrared the suplriority o f di rect videoendosshycopy Early angioscope designs incorporated eyeplecc~ simi lar to l urologists cystOscope for di rec( visualizashy(ion o f the intralu minal splt1ce This viltualizuion techshynique pto ed cu mbersome for (he ascula r surgeon who is often required to move abou t within the sterile operating field or change position during an operat ion The video moniror alleviates these mobility mmtrainrs and provides the opportunity for rhe entire surgical team to monimr the proced ure In most modern opershyating rooms angioscopic mon itonng is iewed on a wlor video display
The video monitor display is cspecil il y useful as a tool to assist in traini ng d inicians in angioscopic techmiddot nique The l ngioscopic image is displayed as a small bright circle on rhe ideo monitor Newer systems allow digirizaTion of rh~ image to fill the entire screen for easier viewing A high-quality monitor caplble of displaying crisp dean color images wiU enable prec ise differentittion of endoluminal d isease characterinics As in the previous discusion of lighT source coupling proper connelt fion of elmlra clements to video display is crit ical to clear iSUll izniun
Irrigation System Irriga tion systems are critical to an angioscopy system ye t arc one of th e mtl~t overlooked component~ Tht vascular SYlum nnli ke the gas roimes tin ai uro logic or arthroscopic fields po~es a unique challenge in that its visual field is obscured by pllJsltltile ~w i rling opaque blood As nooILiminal angioscopic fechnology hai been borrow~d from th~se other endoscopic modalities the irrigalio n ystcms successfull y used in genera l surgery ha e pro ed to b~ inappropria te for endmasshycular applications Oercoming this obsracle hy fi nding bem r ways to cl iminHe baekflow and displace blood from the visual fidd is still an uea of devc1upment Recogniz ing th e s t rcngth~ and limitations of cu rrent irrigation systcms will impro e the video image and minimize complicat ions associated with nUld ovcrload Currentl three types o f irrig1tion system are availahle (0 tht vascula r surgeon (Fig 3421
The bltlsic irrigalion s)s(em consists of a sali ne bag with a line directly artached to (he irrigation port on the angioscopc (Fig 342A) The irrigating ~J lu tion bag when suspended on 1 pole used fo r intra~nous drip provide~ a source of co nstant pa~s i e pr(ssure tha t clears the visual intraluminal field Alternatively )1 asmant mar sq ueeze the bag either h~ hand or with a blood pressure cuff placed around th l bag while pinching off the direct li ne TO pro ide arying amounts of pressure as deemed appropriare to clear the
o
A
B
o
c
Pinch Valve
FIGURE 342 VariOUS angloscope irrlga iOn systems fA simple saline bag irrigation system f81peristaltic foot middotactivated pump fe) foot -activated pressure vessel pump
field The disadvantages of this somewha t cumbetsome tnhnique are tw()fold monitori ng the amount of fl uid infused into the e~sel often can he unreliable and il is difficu h to ~ ccunltely regu late the Auid pres~ure This initial approach has been la rgely abandoned
A moce advanced infusion irrigaion systtm is the roller pu mp IFig 342B) This sySTem is more sophi~tj cated than the passive pressure sa line bag setup in that a roller pump activated by a foot switch crcate~ a pe rlmiddot staltic infusion of sa line eliminating rhe need tn coorshydinate sa li ne infusion willl an assistant Furthermore rhe flow rafe ca n be preset co a desired level emin ing from 10 TO 400 Ill i per minure from the angioscopt rip and rhe volume of infused fl uid can be continuallv monitored aurom3tiClt1Ily A fairly high pressure level i~ required ro rransmit Il uid down the sma ll-diameter angioscopic work ins clulOnel over I distance of up to 100 em The period of high-pressure infusion is temposhyrary and gener311y not of great concern but should be considered when operat ing within a dosed s~rs re m
The ollcr pump although t provides ~~veral au tomiddot mared fcatu res i~ nOt without drawbacks When the foot SWitch is initially 3ni 1ted sali ne is infused at a
Chapter 34 Angioscopically Assisted Thromboembolectomy 449
low pressure unt il the roller pump build s up to rh e de ired set speed This shorr period o f low-pressure infusion is insufficienr to displalte blood and dea r the visual held yet some volume of saline h~l S been ltldded to the patients vascu lar system rncreasing fl uid load whil e fading to maxllm ze the rime spent visu ally intershyrogating the vessel Also becau~e the pump IS not responsive to flu id bui ldup an d pre~sure feedback vesshysels infused wirh in a closed system (ie disnl Jlr cla mped vessels wi th occluded side branches) lIlay undergo a dramatic increase in intra-arterial pressure that has the potential to damage the ve~sel waJl among othel vascu lar complicatimls Curre ntly rherc is no effective mea n~ to com pensate fo the potential pre~s ure buildup u~ ing the roller pumps because (h ey are not pressurl $ensitive Conseq uendy care should be taken to monitor fluid ind ucrion with rhis system
The rhird irriga rion system combines the -d va nshyt1ges of the two previously dc~cribed systems (Fig 342C) The release of irrigatio n fluid (contai ned in a ali ne-filled bag housed within a press ure vessel) is conshytrolled by pressure changes initiated when an onJo ff foot )witch is activitcd A bolus of fluid in rhe range of 250 to 350 ml per minUTe may be infused to quickly clear the visual field when baddlow is encou ntered wh ile 10w~llo infusion at 60 ro 80 ml per minute is us ually adequate to maintai n a constant unobstructed field of view In addition to having an external pressure regul ator this irrigation system is pressure ciependenr thathy OVerC0l11111g the problems assoClated wi th inrrashyarten1 pressure buildu p and minlllllzmg the ri sk of fluid oved oad Usually 21 to 30 psi IS sufficient (Q proshycure a d ear visual field in the ileofemoral system and below (14) A pinch vahe ensures that the ini tial infushyStOll () f saline will he ma imined at the preset pressu re thereby providing rapid clearing of the visual fi eld and saving procedure time and 1Il1IleCessary fluid ad tn imstrashynon Tot al infused volume ~h o uld be carefully monishy(Ored co preent patient fl uid oerload O fte n newer Ifrigation systems have heen designed with an autoshymatic shut-off fea ture as a ~afety mechanism in tracki ng tluid infus ion to alen [he dinician to fl uid admi niHra~ [I on volumes before reac ht ng a lOOO-ml mfusion level
operative setup Optimal utilization of rhe angioscopc in surgery requ ires omplete familiarity with the equ ipmenr and its approshypriate loca tion relative to the sterile ~ lIfgica l fi eld The ltlstrumenratlOl1 includ ing the chip-videocamera ca mshyera coup ler light source videocassette recorder video d l ~p lay mOllitOr and irrigation pump shou ld be mounted on a mobile cart (lpposite the surgeon Duplishycate display monitors may he mounted at OIher st ra tegic locations for easy visualiza tiOIl of rhe procedu re hy the other members of the su rgical ream as appropriate
The ste rile angioscope is placed on a separate table so that prepa ration for angioscopy can be made withshy
out distllrbitlg the surgical p reparation of the operati ve site PIeopenaive preparations should include connecshyt ion of the camera to the light source focusi ng the angioscope and white-balancing the light for proper co lor before using the mstrumentation in the case The angioscope its co nnecting cable lnd irrigation tubing are brought around th e angl0~c(1p i s t and secured to the drapes over the chest of rhe patient (15)
Operative Considerations for AngioscopyshyAssisted Thromboembolectomy A sttndard method of angioscopic exam mati on shou ld be developed for each angioscopic apphc3tioll and ~hould be varied according to the operative procedure and th e nature of the region of inte rest Mill er describes Llcil procedures in his recent work Angioshyscopy Itl rroducrion and Bltlsic Techniq ues wh icn tne intervenriona list may find useful as a template for ind ishyvidualizing operative prOTOcols ( 16) When using angioscopy w assist during throm boembolectomy choosing the proper size ltl T1 gioscope IS of paramount importanlte The diamete r of the angioscope shou ld be the largest that can be easily introd uced into the vem1 giving due considera rion to lumi nal tapering as rhe cathete r is advanced Carefu l angioscope selection will min imize visualization difficulties such as dark or hlanc hed images and reduce tle danger of ind ucing spasm in a native artery
New Thrombectomy Devices A grea ter understandmg of the pathology of peripheral vascular disease was brought about in parr by improved vis ualiza tion modali ties This in rurn ha~ prompted the development of new thrombeCTOmy devices designed to address the various stages of ath eroshy~lerotic disease Two ~uch rools ha ve recently been added to the surgeons endovascular instrumentation arnU mentllrium Both the corkscrew-shaped adherenr clot catheter and the open~V i re graft thromhectomy catheter (Baxter Healthcare Corp Vascular Division Irvine C lli) are deSigned to more complete ly remove adherent throm botic material after embol ectomy and their benefi cial dfects cnn be easily docum ented when th~y He used in conj unoioll with angioscopy
Adherent Clot Catheter Figure 343 is a drawing showing rhe longitudinally colshyl ap~ed insertion position of the adherent clot catheter ti p The device comim of a tlexible catheter with a disshytallarex-covered coiled cable at its tip A rhu11 b-ilctishyvated lever on the instrument hnndle allows the surgeon to adjust rhe pi tch of the co rkscrew membrJne from a fully collapsed sman~dia meter position to a tightly spiraled retracted con ligu ration with a diameter of up to 10 mm (14) By advancing the catheter in the
450 Part V Occlusive Amrial Diseasegt
low-profi le collapsed position then expanding it to its wider-diameter con figurat ion adherenr thrombus is grasped by the closing spi r1l loops of the corkscrew membrane (Fig 344 ) In the sa me fam iliar manner an em bolectom ) procedure is perfo rmed the adheren t clot catheter is withd rawn in its expanded posi tion toward the aneriotomy and the clot is removed manually The pitch of the rerr iev3 1 element may be adjusted b) the thumb lever if resistance is encounter ld during the withdrawa l process (0 ad iu~t the gripping force during withdrawa l
Graft Thrombectomy catheter The distal working eilmem of th l graft thrombectomy ca th ecer is designed much rhe same as the adherem dot catheter (Fig 34 5) Both use the principle of a hand shyoperated expandab le variable-pitch coil to grasp and remove adherent thrombus However two features difshyferentia te the devices Unlike the adherent dOt catheter whic h is composed of one membrane-covered wire the grafr thrombectomy ca theter is constructed using twO helically arranged exposed wire~ These tWO wires are d iscally mounted on a central retractable wire in an opposi ng ldt-handed and right-handed helical arrangeshymemo In both ca rherer designs rhumb-activated retracshydon of rhis centra l wire causes the respective coils (Q
expand in dia meter The lack o f a latex membrane covshy
ering over rhe helica Jl r arra nged wires makes the graft rhrnmhecromy c-u heter parricularly well suiled for removal of adhe rent throm bus oc d isrupted neoinrima commonly asgtociattd with symher ic grafts
Surgical Technique Removal of Adherent Thrombus in Native Vessel The follow ing is it de~crip[ion of an angiolt(opy-ascisted [hrom~omy of the superficial fe moral artery and poplitea l arrer) containing fresh throm hus with undershylying adherent cloT
Afttr the angioscop) system is white-balanced and prepared fo r use a ttrmdud cutdown is madt OVtr the femoral triangle Va~cular clamps are applied to the proximal superficial lOd the deep femoral arteries An 3T1eriotomy is made JUSt proximal to the br1nch of the deep femoral artery in the superficial femora l artery A sta ndard 3 or 4 Fr balloon embolectomy catheter is used to remove soft thrombus in the major vessds of the femoropopliteal srstem
It is usdul in fact imptrativC to reconStruct the d ot with removed clot segments on a towel to provide in shysight imo the anatomic location structure dimensions and charlcter of rhe d ot Otten a meniscus is formed at the distal end of th e thrombus at the flow boundary of th e dista l pa rent brmch Reconstruction of the clot with
A
B
f
c
FIGURE 343 Adherent ClOt catheter (A) catheter tip In Its COllapsed lowest-profile setting (8) cathmiddot eter tip In medlummiddotprofile setting showing partiall y retracted thumb lever (el fully retracted and expanded catheter tip
FIGURE 344 Adherent clot cathetEr retrieving adherent thrombus
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993

Chapter 34 Angioscopically Assisted Thromboembolectomy 449
low pressure unt il the roller pump build s up to rh e de ired set speed This shorr period o f low-pressure infusion is insufficienr to displalte blood and dea r the visual held yet some volume of saline h~l S been ltldded to the patients vascu lar system rncreasing fl uid load whil e fading to maxllm ze the rime spent visu ally intershyrogating the vessel Also becau~e the pump IS not responsive to flu id bui ldup an d pre~sure feedback vesshysels infused wirh in a closed system (ie disnl Jlr cla mped vessels wi th occluded side branches) lIlay undergo a dramatic increase in intra-arterial pressure that has the potential to damage the ve~sel waJl among othel vascu lar complicatimls Curre ntly rherc is no effective mea n~ to com pensate fo the potential pre~s ure buildup u~ ing the roller pumps because (h ey are not pressurl $ensitive Conseq uendy care should be taken to monitor fluid ind ucrion with rhis system
The rhird irriga rion system combines the -d va nshyt1ges of the two previously dc~cribed systems (Fig 342C) The release of irrigatio n fluid (contai ned in a ali ne-filled bag housed within a press ure vessel) is conshytrolled by pressure changes initiated when an onJo ff foot )witch is activitcd A bolus of fluid in rhe range of 250 to 350 ml per minUTe may be infused to quickly clear the visual field when baddlow is encou ntered wh ile 10w~llo infusion at 60 ro 80 ml per minute is us ually adequate to maintai n a constant unobstructed field of view In addition to having an external pressure regul ator this irrigation system is pressure ciependenr thathy OVerC0l11111g the problems assoClated wi th inrrashyarten1 pressure buildu p and minlllllzmg the ri sk of fluid oved oad Usually 21 to 30 psi IS sufficient (Q proshycure a d ear visual field in the ileofemoral system and below (14) A pinch vahe ensures that the ini tial infushyStOll () f saline will he ma imined at the preset pressu re thereby providing rapid clearing of the visual fi eld and saving procedure time and 1Il1IleCessary fluid ad tn imstrashynon Tot al infused volume ~h o uld be carefully monishy(Ored co preent patient fl uid oerload O fte n newer Ifrigation systems have heen designed with an autoshymatic shut-off fea ture as a ~afety mechanism in tracki ng tluid infus ion to alen [he dinician to fl uid admi niHra~ [I on volumes before reac ht ng a lOOO-ml mfusion level
operative setup Optimal utilization of rhe angioscopc in surgery requ ires omplete familiarity with the equ ipmenr and its approshypriate loca tion relative to the sterile ~ lIfgica l fi eld The ltlstrumenratlOl1 includ ing the chip-videocamera ca mshyera coup ler light source videocassette recorder video d l ~p lay mOllitOr and irrigation pump shou ld be mounted on a mobile cart (lpposite the surgeon Duplishycate display monitors may he mounted at OIher st ra tegic locations for easy visualiza tiOIl of rhe procedu re hy the other members of the su rgical ream as appropriate
The ste rile angioscope is placed on a separate table so that prepa ration for angioscopy can be made withshy
out distllrbitlg the surgical p reparation of the operati ve site PIeopenaive preparations should include connecshyt ion of the camera to the light source focusi ng the angioscope and white-balancing the light for proper co lor before using the mstrumentation in the case The angioscope its co nnecting cable lnd irrigation tubing are brought around th e angl0~c(1p i s t and secured to the drapes over the chest of rhe patient (15)
Operative Considerations for AngioscopyshyAssisted Thromboembolectomy A sttndard method of angioscopic exam mati on shou ld be developed for each angioscopic apphc3tioll and ~hould be varied according to the operative procedure and th e nature of the region of inte rest Mill er describes Llcil procedures in his recent work Angioshyscopy Itl rroducrion and Bltlsic Techniq ues wh icn tne intervenriona list may find useful as a template for ind ishyvidualizing operative prOTOcols ( 16) When using angioscopy w assist during throm boembolectomy choosing the proper size ltl T1 gioscope IS of paramount importanlte The diamete r of the angioscope shou ld be the largest that can be easily introd uced into the vem1 giving due considera rion to lumi nal tapering as rhe cathete r is advanced Carefu l angioscope selection will min imize visualization difficulties such as dark or hlanc hed images and reduce tle danger of ind ucing spasm in a native artery
New Thrombectomy Devices A grea ter understandmg of the pathology of peripheral vascular disease was brought about in parr by improved vis ualiza tion modali ties This in rurn ha~ prompted the development of new thrombeCTOmy devices designed to address the various stages of ath eroshy~lerotic disease Two ~uch rools ha ve recently been added to the surgeons endovascular instrumentation arnU mentllrium Both the corkscrew-shaped adherenr clot catheter and the open~V i re graft thromhectomy catheter (Baxter Healthcare Corp Vascular Division Irvine C lli) are deSigned to more complete ly remove adherent throm botic material after embol ectomy and their benefi cial dfects cnn be easily docum ented when th~y He used in conj unoioll with angioscopy
Adherent Clot Catheter Figure 343 is a drawing showing rhe longitudinally colshyl ap~ed insertion position of the adherent clot catheter ti p The device comim of a tlexible catheter with a disshytallarex-covered coiled cable at its tip A rhu11 b-ilctishyvated lever on the instrument hnndle allows the surgeon to adjust rhe pi tch of the co rkscrew membrJne from a fully collapsed sman~dia meter position to a tightly spiraled retracted con ligu ration with a diameter of up to 10 mm (14) By advancing the catheter in the
450 Part V Occlusive Amrial Diseasegt
low-profi le collapsed position then expanding it to its wider-diameter con figurat ion adherenr thrombus is grasped by the closing spi r1l loops of the corkscrew membrane (Fig 344 ) In the sa me fam iliar manner an em bolectom ) procedure is perfo rmed the adheren t clot catheter is withd rawn in its expanded posi tion toward the aneriotomy and the clot is removed manually The pitch of the rerr iev3 1 element may be adjusted b) the thumb lever if resistance is encounter ld during the withdrawa l process (0 ad iu~t the gripping force during withdrawa l
Graft Thrombectomy catheter The distal working eilmem of th l graft thrombectomy ca th ecer is designed much rhe same as the adherem dot catheter (Fig 34 5) Both use the principle of a hand shyoperated expandab le variable-pitch coil to grasp and remove adherent thrombus However two features difshyferentia te the devices Unlike the adherent dOt catheter whic h is composed of one membrane-covered wire the grafr thrombectomy ca theter is constructed using twO helically arranged exposed wire~ These tWO wires are d iscally mounted on a central retractable wire in an opposi ng ldt-handed and right-handed helical arrangeshymemo In both ca rherer designs rhumb-activated retracshydon of rhis centra l wire causes the respective coils (Q
expand in dia meter The lack o f a latex membrane covshy
ering over rhe helica Jl r arra nged wires makes the graft rhrnmhecromy c-u heter parricularly well suiled for removal of adhe rent throm bus oc d isrupted neoinrima commonly asgtociattd with symher ic grafts
Surgical Technique Removal of Adherent Thrombus in Native Vessel The follow ing is it de~crip[ion of an angiolt(opy-ascisted [hrom~omy of the superficial fe moral artery and poplitea l arrer) containing fresh throm hus with undershylying adherent cloT
Afttr the angioscop) system is white-balanced and prepared fo r use a ttrmdud cutdown is madt OVtr the femoral triangle Va~cular clamps are applied to the proximal superficial lOd the deep femoral arteries An 3T1eriotomy is made JUSt proximal to the br1nch of the deep femoral artery in the superficial femora l artery A sta ndard 3 or 4 Fr balloon embolectomy catheter is used to remove soft thrombus in the major vessds of the femoropopliteal srstem
It is usdul in fact imptrativC to reconStruct the d ot with removed clot segments on a towel to provide in shysight imo the anatomic location structure dimensions and charlcter of rhe d ot Otten a meniscus is formed at the distal end of th e thrombus at the flow boundary of th e dista l pa rent brmch Reconstruction of the clot with
A
B
f
c
FIGURE 343 Adherent ClOt catheter (A) catheter tip In Its COllapsed lowest-profile setting (8) cathmiddot eter tip In medlummiddotprofile setting showing partiall y retracted thumb lever (el fully retracted and expanded catheter tip
FIGURE 344 Adherent clot cathetEr retrieving adherent thrombus
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993
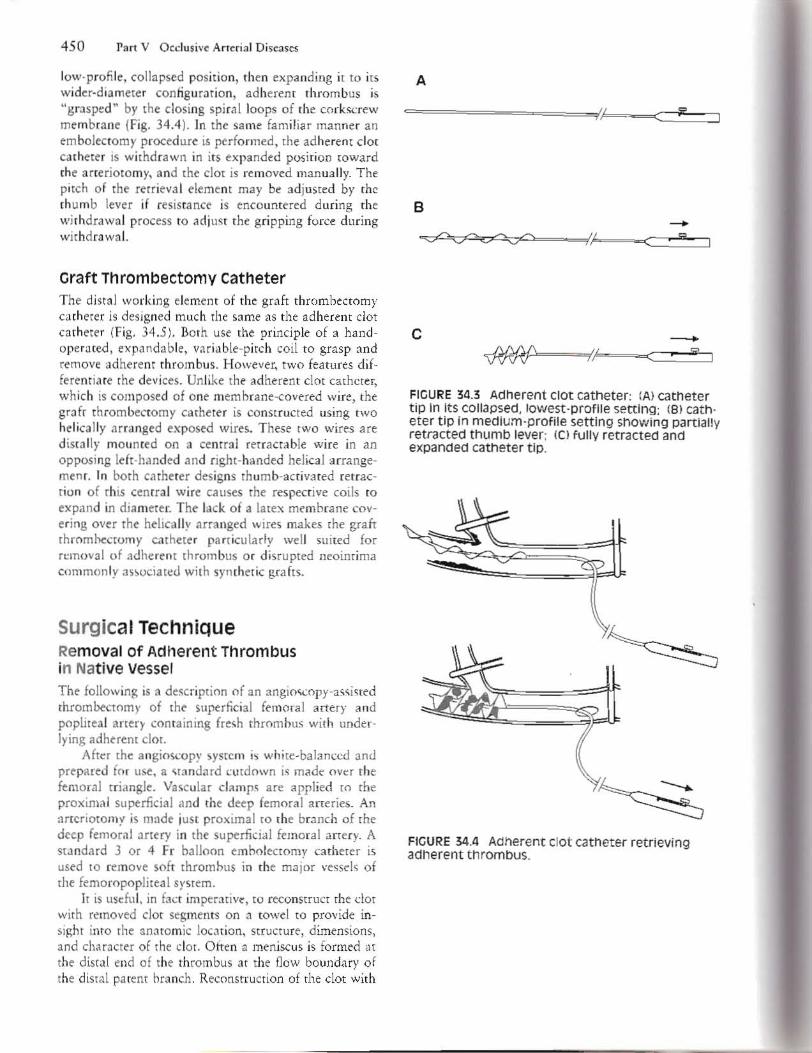
450 Part V Occlusive Amrial Diseasegt
low-profi le collapsed position then expanding it to its wider-diameter con figurat ion adherenr thrombus is grasped by the closing spi r1l loops of the corkscrew membrane (Fig 344 ) In the sa me fam iliar manner an em bolectom ) procedure is perfo rmed the adheren t clot catheter is withd rawn in its expanded posi tion toward the aneriotomy and the clot is removed manually The pitch of the rerr iev3 1 element may be adjusted b) the thumb lever if resistance is encounter ld during the withdrawa l process (0 ad iu~t the gripping force during withdrawa l
Graft Thrombectomy catheter The distal working eilmem of th l graft thrombectomy ca th ecer is designed much rhe same as the adherem dot catheter (Fig 34 5) Both use the principle of a hand shyoperated expandab le variable-pitch coil to grasp and remove adherent thrombus However two features difshyferentia te the devices Unlike the adherent dOt catheter whic h is composed of one membrane-covered wire the grafr thrombectomy ca theter is constructed using twO helically arranged exposed wire~ These tWO wires are d iscally mounted on a central retractable wire in an opposi ng ldt-handed and right-handed helical arrangeshymemo In both ca rherer designs rhumb-activated retracshydon of rhis centra l wire causes the respective coils (Q
expand in dia meter The lack o f a latex membrane covshy
ering over rhe helica Jl r arra nged wires makes the graft rhrnmhecromy c-u heter parricularly well suiled for removal of adhe rent throm bus oc d isrupted neoinrima commonly asgtociattd with symher ic grafts
Surgical Technique Removal of Adherent Thrombus in Native Vessel The follow ing is it de~crip[ion of an angiolt(opy-ascisted [hrom~omy of the superficial fe moral artery and poplitea l arrer) containing fresh throm hus with undershylying adherent cloT
Afttr the angioscop) system is white-balanced and prepared fo r use a ttrmdud cutdown is madt OVtr the femoral triangle Va~cular clamps are applied to the proximal superficial lOd the deep femoral arteries An 3T1eriotomy is made JUSt proximal to the br1nch of the deep femoral artery in the superficial femora l artery A sta ndard 3 or 4 Fr balloon embolectomy catheter is used to remove soft thrombus in the major vessds of the femoropopliteal srstem
It is usdul in fact imptrativC to reconStruct the d ot with removed clot segments on a towel to provide in shysight imo the anatomic location structure dimensions and charlcter of rhe d ot Otten a meniscus is formed at the distal end of th e thrombus at the flow boundary of th e dista l pa rent brmch Reconstruction of the clot with
A
B
f
c
FIGURE 343 Adherent ClOt catheter (A) catheter tip In Its COllapsed lowest-profile setting (8) cathmiddot eter tip In medlummiddotprofile setting showing partiall y retracted thumb lever (el fully retracted and expanded catheter tip
FIGURE 344 Adherent clot cathetEr retrieving adherent thrombus
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993
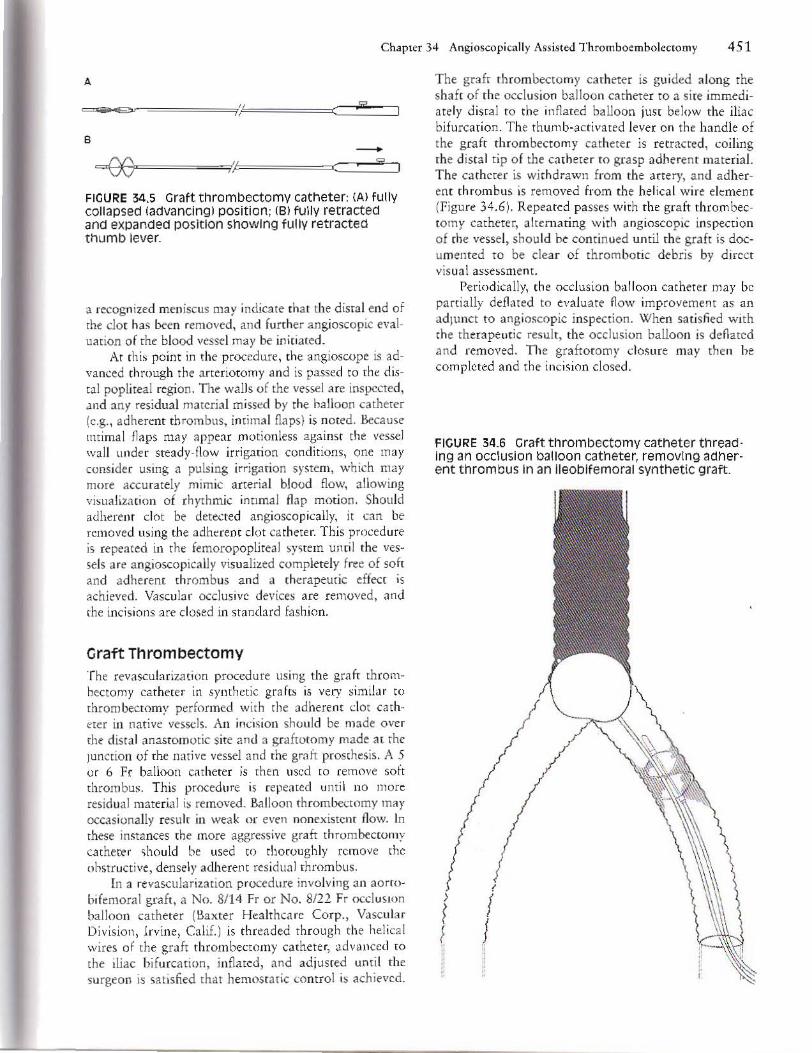
Chapter 34 Angioscopi ca1y Aisis ted Thromboembolectomy 451
A
B --Cf~~=lF-C7v- 1 ~~lt===JJr
FIGURE 345 Graft thrombectomy catheter (Al fully collapsed (adVancing I position (BI fully retracted and expanded positiOn showing fully retracted thumb lever
a recognized meniscus may indicate that the dista l end of the d O( has been removed and further angioscopic evalshyuation of rhe blood vessel may be iniciated
At chis point in the procedure the angioscope is adshyvamed through the arteriotomy and is passed to the disshytal popliteal region TIle walls o f the Vessel are inspected 1Ild any residual material missed bl the balloon catheter (eg adherent thrombus intima l flaps) is noted Because ll1 timal flaps ma~ appear motionless against the vessel vaU unde r steadymiddot flow irri gation conditions one may consider usmg a pulsing irngati on sstem which may more accu ra tely mim ic aneri1 blood flow allowing ViSll( iz1 tion of rhyth mic intHnal fl ap motion Should aclherem clot be detected angioscoPlcally it can be removed using the adherent cl ot ca th ete r This procedure is repened in the femoropoplitea )jt em umil the vesshysels are ans ioscopica lJ y visualized completely free of soft and adherent thrombus and a therapeUTic effect is achieved Vascubr occlUS ive devices are removed and the incisions are cl o~ed in standard fashion
Graft Thrombectomy The revasculariza ti on procedu re using the graft thromshybectomy catheter in synthetic grafts is very similar to
thrombectomy performed with he adheren t dot ca thmiddot erer in native vessels An jmision should be made over the distal anastomotic site amI 3 graftotomy made 3l rhe Junction of the native vessel and the graft prosthesis A 5 or 6 FI balloon catheter is then used to rem()Ve soft thrombu~ This procedure is repeated until no more residual material is removed amp11l001l thrombectomy may occasiona lly resu lt in weak Of even nonexistcll( flow In these in~tances (he more aggressive graft thrombectomy cathete r ~hould be used to thoroughly remove the ohstructive densely adheren t residua l thrombus
In a re vascularizuion procedure involving an aortoshybifemoral graft a No 814 Fr or No 8121 Fr occl USion balloon catheter (Baxter Htahhca re Corp Vascular Division Irvine Calif ) is threaded through the helical wires of the graft thrombectomy cathete r advltlllced to
(he iliac bifurcation inflated and ad jusced until the su rgeon is satisfied that hemostatic cont rol is achieved
The grafr thrombectomy catheter is guided along the shah of the occlusion balloon catheter to a si te immedishyately disral to the inflated balloon just below the iliac bifurcation The thumb-activated lever on the handle of the graft thrombectomy catheter is retracted coiling the d ista l tip o f the catheter to grasp adherent material The ca theter is withdrawn from the artery and adhershyent thrombus IS removed from the hel ica l wire elcment (Figure 346) Repeat~d passes with the graft thrombecmiddot tomy cathete r alternating with ang ioscopic inspection of (he vessel shou ld be comi nued until the graft is docshyumented to be clear of throm botic debris by d irect vis ual assessment
PeriodICally the occlusion ba lloon catheter may be partially deflated to evaluat e flow improveme nt as an adlunct to angioscopic inspection When sa tisfi ed with the therapeutic result the occlusion balloon is deflated and removed TIl e graftorom closure may then he completed and th e i llci~ion closed
FICURE 346 Graft thrombectomy catheter threadmiddot Ing an occlusion ba lloon cathete r removing adhermiddot ent thrombus In an ileobifemora l synthetiC graft
4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993

4 52 Pan V Occlusive Arteria l Diseases
Conclusion Despite the many benefi t afforded vascular surgeons from dirC(t viualizaton with angio$copr harriers exist that prevnt widesp read adoption o f rh e lll odality (3) Some of the disadvantages associJted with usc of angioscopy are cost of l1lstru1l1entJtion fragility uf eq uipmem espeC ia lly opt ica l fi bers inability to US~ ~n angioseope concu rrently with therapeutlc modahtles ow ing 10 small vessel sIze re lat ive to tht size of the devices inability lO quantit] poundtgt flow d ifficu lty na vigatshying tonuous vessels a steep learni ng ~u rvc and possishyhie d in ic1 disadvantages such as mismttrprctanon of da ta system fl uid overload traurnatk intimal injur and potential emboli znion or thromb(J)I~
To expa nd upon ome of these drawbacks to uti shyli zation one pnmary ohsrade IS the cost of angioscopic equi pm(Cnt Thc Initial monetary investment to procure a dedicated angw5COj)IC system incl uding the ligh t source camera video monitor pu mp and irrigation components can be SIgnificant (lpproximarely $60000 to $65000) RepaI r of ex pcn~ie reusable mgioscopes cln easily a l1lount fO half as much as the original pur middot chase COSt and mily run approximareler $2500 to $3000 pel repai r Choosing to milize Jess expensive disshyposable angioscopes Inte rfaced to exisring camera and monitor endoscopy or laporo5coPY systems wdl allow a facil ity to et up an angio~copic ~ervlce fo r a fr action of the cost of purchaSing a dedicated system (approximate $SOOO cm t wou ld Incl ude purcbase of an irrigation pump twO angioscopes and a came ra cOllpler unit) bur the COSt of replacing single-use angloscopes IS also nor insignificant
A secondary dererrent to adopting this technology has been the learning curve associated with system opec shyarion which reqUIres an understanding not onl y of device function and application bLlt also of its mainteshynance However as angioscop~ instrumenta tion usage increases and the full potentia l of the device is recog shyIlIzcd the technical learning curve should decrease as experienced operators include angioscopic assessment III thelT surgllI repertoire and surgical tra in in) programs includt thl~ ntw modality in their course curricula
In the past ready Jtceptance of the device was thwarted bv tht somewhat limited aVlibbility at tec hshynical supp~rt fhis situation is changing as the two nin suppliers of the devices ser lling the vascular COl1 shymUllity have expanded their clinical person nel to ofter physicia ns more opponU l1ities to gai n 11a ndson experience eval uating angioscopy sysre ms m climcal settings Thl rwo L(Jns istent man uiclcrurers providing angioscopic eq uipment are Intrlrned (SIO Diego Ca lil dis r ibu t~middotd b~ Baxter Hea lthca re Corp Vascula r Divishysion Irv ine Calif) and Ol~mpus (Lake ~uccess NYl O lympm manufactures a broad range of rcusa~1c ang i l)SCOpe~ fm vascular and other med ical speclaltlcI while In tramcd markets primarily to the vascu lar com shymunity ks~-expensive disposa ble ang ioscopes or the
new ly int rod uced respo~ablt (li mited reusahi li ty) angioscopes It is likely that other eq uipment manufacshyrurers will enter the field in the fueure as the endovasshycula r surgical communit) recognigtes the value of using this technique vhich will Significantly improve th e acshycelbility to the ll1strumeIHatio n and the technical sup shypon serViCes
Despite some of the ohstacles to rea dy acceptance of this moda lity the posit ive fi nancial Impact angiosshycopy may have on the net COSt of surgica l II1rervent ions should be considered h is becoming mcreasmgly Jpparent fhar cost savings may he realized in several uelS such as decreases in proced ure time operating room rime anes thesia time often pmtopcrat ive hospishy[ltll i1ation time an d th e dIrect cosr savings aSSOCiated wirh eliminating th e completion angiogram
Trad itionally thrombectomy was performed as a semiclosed blind techni que The ahility to cl early and complete ly VIsualize the intraluminal fi eld with fl exible mllleuverlble lngjoscopes has shed new light on duomboembolectomr and in situ and synthetic bypass grafts procedures as well a prov iding the abili t to evaluate hemodialsis access shums
The growlIlg trend in vuscIIL1c surgery is toward lllltlimally invasive surgica l inrervenrion Angimcopy provides opportunities to perform these procedures With greater efficacy and safery Despite some of the currene barriers to us ing angioscop) this method of Visuali za tion has real ut ili ty in the thromhoemho lectomy process Angioscopy allows for a thorough intralum ina l IIl specshytlOIl o f blood vessels in three-di mensional f(al- time color images that are a fam il ia r visua l modality for urgCOI1S Pathology o ften missed by Doppler ultrasound or angiography such as intimal flaps can be ascssed with greater accuracy and acuirr (12 )
Tec hnological advances in Image quality and reso shylu t ion along with an increlsed ability to lllterrogare sma ll er vcs~el~ should sign ificantly improve curren t a l1 g i mC(~py ~ptems and cn hll1 ce their acceptance hy the surgical community The use 01 angioscopy to gu ide c ndova~cular surgical intervenriolls will become rout ine in the futu re The information dire([ middotisualization proshyIdes IS Vi tal to adunclIlg the development of new endoascular therapeutic tllodliit ies
References 1 foga rty T( Cr~nlcy JC et (d A mer hoJ for exnmiddotacri(ll1
of arter ial emboli and thrombi ~llmiddot (ynecol O bsrc 1963Fcb241- 244
2 Thomp~on JL Vascular surgicll l lthmques a hi5IO rie1 pcrwenive In Bergan JJ and Yao JT ed~ Technique~
in lrtlrI1 wrglry Phihldelphia WS SlImders t9903- U
J Tawes KL Jr Harm lJ el al Arterial hromboembolism a 20 year pcrspltXive Af(h Surg 1981 12U595- 599
4 Elliott WfT H agenun jJ-t ~t al Arrena l emhohatlon problem of sou rce multiplicity recurrence and dday~d rrCorl1ClH Surgery 19808lJJ- H45
Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993

Chapler 34 Angioscopically Assisted Thromboemboleclomy 453
5 Abbott WM Ma loney RD et a1 Arterial embolism J
44 )e~ r perspective Am J Su rg 19112143460-464 6 CambtIJ RI) Abbon WM Acure arterial fhromho~ls of
the lowe r exrremity irS nalural hi)wry eonlrasreU with merial embolism Ar(h 5urg 19841 19784-7IP
7 Whit~ GH Whicc RA Introduction and o cr--iew In Angioscopy a~(u[lr and cor)narr Jpplilt3 tinns Chicago Ynr Book Medical Publisncrs 1989 1
R Stone-bridge PA Muric IA Angioscopy 3 new light on
penpheral VR)(UiU disease Eur Vase Surg 19926(41 346-353
9 White GH WhHe RA er 1 Im rapcnmve video Rngioscop) eompil red with Ileriography dur in~
ptr iphera v ll ~cu lil r oXrations Vase Surg 19876 4Hl-495
10 Whit( G H Ansio~ j)py SUIS Cl in North Am 1991 72(4 )791-82 1
J I Glgub kis AG ( jairzsch A Vasc ular cnJ oscopyshylnglOSCOl) (llrrenC indkarioll A tn iew of the iteramiddot nu e Vasa 199 120(3) 199-2U6
12 Maini 85 Andrew L rT al A modified lI ngioscorkally ltlsslSIcd technique fo r m-Sltu saphenous vein bypass impact on patenCy complications li nd k nglh of sTay J Vase Surg 19931 7 1041-1 049
13 Mille r A Srom bndge PA er al Continutd t(perience with iOlraoperatlVf angloscopy for monitoring mframiddot inguinal bypau grJ ft Surgery 1991 109Z86- 2lJ
14 FClgJr)middot TJ Hcrmann CD Angioscopymiddotassis(cd Thromboembolectomy In Vao JT Pearce (H eJ~ Tech rlo losic~ in va~cular surgery Ph iladelphia WB Saundrr 992143U6- 3 16
15 Miller A j tpsol1 5j Technique of intraoperative angioseopy In lower c)(trcmirv revltlscuia rizaTioll I ll Bergan TJ Vao j T cd TcchmqulS In arceril SUf-ery PhiladelphIa (11 Sau ndcr~ 1990409-416
J6 M iller A Angio$copy Introduction and basit t hmiddot niq ues Presented at r ropess III Angiosopy Intt rvenshyt ional and Monitoring Ttchniques in V1 Mu b r Surgery lloston Decemher 6-8 1993