a porcine model for endolaparoscopic abdominal aortic...
TRANSCRIPT

A Porcine Model for Endolaparoscopic AbdominalAortic Repair and Endoscopic Training
JSLS (2003)7129-136 129
ABSTRACT
Objectives The goals of this laboratory model were toevaluate the performance of the surgical team andendolaparoscopic techniques in the porcine model ofinfrarenal abdominal aortic repair
Methods Twenty-four pigs underwent full endolaparo-scopic aorto-aortic graft implantation with voice-activat-ed computerized robotics The first group of 10 pigs(acute) was sacrificed while under anesthesia at 05hours (5 animals) and 2 hours (5 animals) The secondgroup of 14 pigs (survival) were recovered from anes-thesia and maintained for 7 hours (5 pigs) and 7 days (9pigs) prior to sacrifice Survival animals were observedfor evidence of hind limb dysfunction All grafts werevisually inspected at autopsy
Results All animals survived the operation All graftswere successfully implanted and all were patent withintact anastomoses at autopsy Mean aortic clamp timefor each group was as follows acute 929plusmn2804 min-utes survival 596plusmn138 minutes P=00008 Total opera-tive time for each group was as follows acute 179plusmn396minutes survival 1646plusmn48 minutes P=044 ns Estimatedblood loss for each group was as follows acute214plusmn4378 mL survival 1692plusmn271 mL P=076 ns
The following outcomes were observed 1 animal died
INTRODUCTION
Minimally invasive abdominal aortic surgery has been asubject of great interest since Dionrsquos pioneering work in19931-5 The laboratory animal model has been the firststep of interaction between the endolaparoscopic surgi-cal team and this new technology prior to clinical appli-cation However except for the survival studies of Bryneet al6 and Audra et al7 the problem of spinal cord dys-function in an aortic endolaparoscopic model due to aor-tic cross clamping had not been systematically examined
Our objective was to study the feasibility of infrarenalgraft interposition involving 2 end-to-end anastomosesperformed with a transperitoneal approach with fullendolaparoscopic instrumentation In addition to thetechnical aspects of the protocol we focused particular-ly on the development of quantitative guidelines fortraining in the basic endolaparoscopic skills required Inaddition to the motor skills the learning process requiredadaptation to voice-operated computerized roboticequipment in this endolaparoscopic aortic laboratorymodel The end points of training instrumentation andtechnique are 3 (1) control of bleeding (2) long-term
Minimally Invasive Vascular Surgery Center St Vincent Mercy Medical CenterToledo Ohio USA (Drs Martinez Olsen)
Division of Vascular Surgery Stanford University School of Medicine StanfordCalifornia USA (Drs Fogarty Zarins)
Department of Comparative Medicine Stanford University Stanford California USA(Drs Coleman Daunt)
Ethicon Endo-Surgery University Branch for Education and Research CenterDepartment of Comparative Medicine Stanford University Stanford California USA(Dr Saenz)
Fogarty Research Stanford California USA (Mr Hermann)
Stanford Endoscopy Center for Training and Technology Stanford UniversitySchool of Medicine Stanford California USA (Dr Nezhat)
Address reprint requests to Bernardo D Martinez MD Director Minimally InvasiveVascular Surgery Center Suite 305 St Vincent Mercy Medical Center 2213 CherrySt Toledo OH 43608 USA Telephone 419 251 3512 Fax 419 251 2715
copy 2003 by JSLS Journal of the Society of Laparoendoscopic Surgeons Published bythe Society of Laparoendoscopic Surgeons Inc
Bernardo D Martinez MD Christopher K Zarins MD David A Daunt DVM PhDLeslie A Coleman DVM Yamil Saenz DVM Thomas J Fogarty MD
George D Hermann BSME Camran R Nezhat MD Eric K Olsen PhD
from respiratory arrest 1 animal suffered motor sensorydysfunction of the hind limbs (spinal cord ischemia) sig-nificant bleeding occurred in 6 of 24 pigs 8 of the 9seven-day survivors required minimal pain medicationand had normal hind limb function
Conclusions The reduction in aortic clamp time totaloperative time and blood loss as the study progressedindicate the feasibility of this surgical protocol and thematuration of the learning process which is paramountin prevention of 2 main sources of morbidity bleedingand spinal cord ischemia The reduction in aortic clamptime between the acute and survival groups was dramat-ic and statistically significant An intensive formal trainingprogram combining dry and live surgical laboratories isdeemed essential for the development of endoscopicskill sets necessary for this challenging procedure
Key Words Endolaparoscopy Abdominal aortic sur-gery Endoscopic surgical training Robotics
SCIENTIFIC PAPER
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
130 JSLS (2003)7129-136
graft patency and (3) elimination of spinal cord ischemia
METHODS
This study was conducted between April 1998 andJanuary 2000 under Protocol 6127-1 for care and use oflaboratory animals at Stanford University StanfordCalifornia USA Twenty-four female pigs with an averagebody weight of 55 kg (SDplusmn104 kg) were made to fastovernight premedicated for surgery with atropine (004mgkg IM) and sedated with tiletamine and zolazepam(Telazol Lederele Parenteral Inc Carolina Puerto Rico)at 6 mgkg IM Anesthesia was induced with 3halothane in oxygen delivered by facemask All animalswere orotracheally intubated and anesthesia was main-tained with 1 to 3 halothane in oxygen with mechan-ical ventilation (Hallowell model 2000 Hallowell EMCPittsfield MA USA) to maintain end-tidal carbon dioxidebetween 35 mm Hg and 55 mm Hg
Venous and arterial catheters were placed percutaneous-ly for drug and fluid administration and blood pressuremonitoring Electrocardiogram leads were placedFollowing instrumentation of the survival animals a 20-gauge 35-inch spinal needle (Monoject EmergencyMedical Products Waukesha WI USA) was placed in thelumbosacral joint and morphine sulfate was injectedepidurally at 01 mgkg for analgesia
Serial samples of hematocrit total serum protein andarterial blood gases were taken from the auricular arteri-al catheter Blood gas samples were analyzed immediate-ly on a calibrated blood gas analyzer (Ciba-Corningmodel 248 Global Medical Instrumentation Inc Albert-ville MN USA) Pulse oximetry (SpaceLabs model90651A Spacelabs Medical Issaquah WA USA) andcapnography (SpaceLabs model 1890-02 SpacelabsMedical Issaquah WA USA) were performed frequentlyduring anesthesia Lactated Ringerrsquos solution (AbbottLaboratories Abbott Park IL USA) was administeredintravenously at approximately 10 mLkghr throughoutanesthesia Fresh whole unmatched pig blood wasadministered to 2 pigs that had experienced intraopera-tive hemorrhaging Dobutamine was administered asneeded at 05 to 5 mcgkgmin to maintain systemic arte-rial blood pressure
The animals were placed in a full right lateral decubitusposition (left side up) in the Trendelenburg position(Figure 1) Preliminary measurements were made for
Figure 1 Position of pig and surgical team for endolaparoscop-ic aortic repair Pig in the right lateral decubitus position withTrendelenburg positioning Left to right scrub nurse surgeonassistant The labeled left costal margin is visible by the assistantrsquosleft hand The AESOP robotic arm is in the center of the fieldand the Hermes control system is to the right of the surgeonwho is wearing a voice-activation headset
Figure 2 Port placement for porcine endolaparoscopic aorticrepair model (1) Proximal aortic clamping (18 mm) (2) Distalaortic clamping (18 mm) (3) Endoscope (10 mm) (4) Left handinstrument (5 mm) (5) Right hand instrument (5 mm) (6) Assist(10 mm) Starting at costal margin 10 cm medially then 3 cmcaudally to (3) which is 5 cm from midline (6) is 3 cm from mid-line (4) and (5) are both 6 cm to 7 cm from the line between (3)and (6)
positioning the working and clamping ports as indicatedin Figure 2 The abdomen and groin were prepared withiodine-povidone solution and sterile drapes wereapplied Endolaparoscopic instrumentation included theUltraCision Harmonic scalpel and Ethicon Endoscissors(Ethicon Endo-Surgery Cincinnati OH USA) two 512-mm Ethicon Endopathreg trocars for the 0deg and 30deg 10-mmendoscopes (Stryker Endoscopy Mountain View CAUSA) and the Nezhat-Schroeder suction irrigation system(Davol Inc Cranston RI USA) two 355-mm EthiconEndopath trocars for the vascular instrumentation two18-mm GSI flexible ports (production rights currently heldby TycoUSSI Norwalk CT USA) for proximal and dis-tal clamping the Ethicon Ligaclip clip applier two 5-mmneedle holders and two 5-mm graspers (Ethicon Endo-Surgery Cincinnati OH USA) CO2 pneumoperitoneumwas created via a 511H Ethicon Endopath nonbladedOptiview trocar or a Veress needle introduced through asmall midline incision The endoscope was positionedwith a voice-activated AESOPreg 3000 robotic system(Computer Motion Inc Goleta CA USA) Video func-tions light source and insufflation were remotely con-trolled with the Hermes voice-activated system (StrykerEndoscopy Mountain View CA USA Computer MotionInc Goleta CA USA)
The surgical team consisted of the endolaparoscopic sur-geon 1 assistant and 1 scrub nurse The surgeon hadpreviously trained on a dry laboratory pelvic trainer Atthe beginning of the study the surgeon had accom-plished 65 hours of endolaparoscopic training increasingto 180 hours by the end of the study The endoscopictraining protocol used is divided into the following 3
JSLS (2003)7129-136 131
phases (Table 1) 10 hours are devoted to dry laborato-ry practice in endoscopic suturing cutting endo- andexoknot tying (Phase I) 20 hours are devoted to endo-scopic suture anastomosis of 8- 10- and 12-mm grafts invitro to develop technical precision (Phase II) and 50hours are devoted to increasing both quality and speedof anastomosis until they can be completed within 20minutes to 30 minutes (Phase III)
The transperitoneal approach was deliberately selectedas potentially the most difficult procedure for maximumtraining benefit This approach was maintained through-out the study so that all procedures could be directlycompared as to time parameters and surgical outcomeTrocars and ports were positioned in the abdomeninstrumentation was introduced and bowel loops weremoved to the right side of the abdomen to expose theposterior peritoneum which was entered with theHarmonic scalpel Approximately 5 cm of infrarenal aortawas dissected with a combination of blunt and sharpintrumentation including the UltraCision Harmonicscalpel and Endoscissors The lumbar branches werevisualized and controlled with the Ligaclip endoscopicclip applier Systemic heparinization (3 mgkg IV) wasthen initiated and the proximal aorta was clamped witha conventional aortic or carotid clamp (Figure 3) Distalaortic occlusion was obtained with a 6 Fogarty venousballoon catheter (Edwards Lifesciences LLC Irvine CAUSA) introduced via the femoral artery in 7 of the 10acute animals or an iNtrack clamp (Novare SurgicalCupertino CA USA) in all remaining animals
Vertical transection of the aortic wall was performed with5- or 10-mm Endoscissors An 8- or 10-mm diameterpolytetrafluoroethylene graft (IMPRA Inc Tempe AZUSA) was implanted by continuous end-to-end sutureanastomosis with 4-0 and 3-0 Prolene with a TF or BBneedle (Ethicon Sommerville NJ USA) and 5-mm endo-scopic needle holders A 10- or 12-cm suture providedoptimal ergonomics for tying Endoknots Then the distalclamp was released and the anastomosis was examinedfor leaks Gelfoam (Upjohn Pharmaceuticals Chicago ILUSA) was used to control needle site holes Finally theproximal clamp was gradually released The posteriorperitoneum was closed with staples and in the survivalgroup the port sites were closed with absorbable suture
The animals were divided into the following 2 groupsacute (10 animals) and survival (14 animals) Five of theacute animals were maintained under anesthesia for 05
Table 1Endoscopic Motor Sensory Skill Acquisition
A Formal Training Program
Camps Time (hrs) Stage Goals
1 10 Basic Skills Suture-Cutting(Exercise)EndoknotsEqual Hands
2 Aesop and 30 Quality SutureHermes Anastomosis
3 Zeus 80 Quality and 20-30 MinutesSpeed Anastomosis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
132 JSLS (2003)7129-136
hour following surgery and 5 for 2 hours prior to beingsacrificed Five of the survival animals were recoveredfrom anesthesia and maintained for 7 hours and 9 weremaintained for 7 days prior to sacrifice and autopsyAnimals were scored for several behavioral criteria post-operatively Upon autopsy 1 cm of proximal and 1 cm ofdistal host aortic tissue including the graft end and anas-tomosis were harvested visually inspected under 35times magnification for suture line integrity and photo-graphic analysis Data groups were compared with 2-tailed Student t tests assuming unequal variance
RESULTS
Full endoscopic infrarenal aortic grafts involving 2 end-to-end anastomoses was successfully completed in all 24animals (Table 2) Mean aortic clamping time was
929plusmn2804 minutes in the acute group and 596plusmn138minutes in the survival group (Table 3) Mean total oper-ative time was 179plusmn396 minutes for the acute group and1646plusmn48 minutes in the survival group Mean blood losswas 214plusmn4378 mL for the acute group and 1692plusmn271 mLfor the survival group
One animal in the survival group died of respiratoryarrest due to airway obstruction 2 hours postoperativelyand the other 13 survived until the prescribed sacrificeOnly 1 animal suffered from hind limb dysfunction dueto a prolonged aortic clamping time of 92 minutes Thisresulted from a size mismatch between the preselectedgraft (10 mm) and the host aorta (7 mm) necessitatingadditional suturing to complete the anastomosis The ani-mal was able to stand up with assistance but could notambulate on its own due to severe proprioceptive anes-thesia Histology of the spinal cord showed medullarinfarctions mostly localized in the posterior sensoryhorns which is consistent with the clinical symptoms
Bleeding complications occurred in 6 animals from lum-bar branches and a vena cava branch tear during dissec-tion In 4 animals control was obtained endoscopicallyHowever in the case of the caval tear and aproximaldistal lumbar artery tear the bleeding wasmore difficult to control requiring conversion to a mini-laparotomy (5 cm) These animals required 1 unit ofpacked red cells (250 mL) each
No bleeding at the graft anastomoses was found onautopsy The 24 grafts were patent and all the sutureanastomoses were found intact Two grafts were foundto have an isolated 10 x 8-mm adherent blood clot at theanastomotic suture line All retroperitoneal spaces hadperigraft hematomas which were expectedly smallexcept for in 1 animal that had an estimated 100 mL clot
Figure 3 Suturing the distal aortic graft anatomosis with con-ventional clamps
Table 2Porcine Endoscopic Abdominal Aortic Resection Model
Type of Procedure Weight of Pig Aortic Clamp Time Total Operative Time Estimated Blood Loss
Acute (n = 10) 634 kg plusmn 6 kg 929 m plusmn 28 m 179 m plusmn 396 m 214 mL plusmn 4378 mL Survival (n = 14) 491 kg plusmn 86 kg 596 kg plusmn138 m 1646 m plusmn 48 m 1692 mL plusmn 271 mLSignificance (t test)dagger P = 000008 P = 00046 P = 043 ns P = 034 ns
Values are group means and standard deviationsdaggerThe surgical time and blood loss parameters for the early (acute) procedures are compared with the later (survival) proceduresns = not significant
JSLS (2003)7129-136 133
Tab
le 3
Par
amet
ers
of Exp
erim
enta
l Abdom
inal
Aortic
Endola
par
osc
opic
Rep
air
Model
s
Au
thor
An
imal
Pro
cedu
reSu
rgic
alN
oof
A
orti
c C
lam
pTo
tal O
per
ativ
eTo
tal B
lood
Mod
elA
pp
roac
h
An
asto
mos
es
Tim
e (m
in)
Tim
e (m
in)
Loss
(m
L)
Dio
n e
t al
199
52Porc
ine
acute
(n=26
)Aortobife
mora
lTP
1 Aortic
85ndash1
20dagger
lt24
0lt25
02
Fem
ora
l
Byr
ne
et a
l 19
956
Can
ine
surv
ival
(n=8Dagger
)Aortobife
mora
lTP =
15
1 Aortic
87 plusmn
206
19
3 plusmn
123
128
plusmn12
81
RP =
72
Fem
ora
l
Ahn e
t al
199
59Porc
ine
acute
(n=10
)Aorto-lef
t fe
mora
lTP =
71
Aortic
sectN
ot re
ported
147
(120
ndash240
)20
(5ndash
50)
RP =
31
Fem
ora
l
Chen
et al
199
610
Porc
ine
acute
(n=23
)Cust
om
tube
graf
tTP =
21
2 Aortic
Not re
ported
Not re
ported
Not re
ported
RP =
2
Dio
n e
t al
199
63Porc
ine
acute
(n=8)
Aortobife
mora
l||
Ant RP
1 Aortic
Not re
ported
270
ldquoNev
er gt
550rdquo
2
Fem
ora
l
Jones
et al
199
611
Porc
ine
acute
(n=10
)Aor
to-rig
ht fem
oral
paraTP =
51
Aortic
TP 27
plusmn5
TP 16
1 plusmn
22N
ot re
ported
RP =
51
Fem
ora
lRP 28
plusmn5
RP 19
2 plusmn
1
Bru
ns
et a
l 19
9812
Porc
ine
acute
(n=20
)Aortobife
mora
lTP =
10
1 Aortic
TP 60
(45
ndash75)
TP 24
0 (2
10ndash2
70)
Not re
ported
RP =
10
2 Fe
mora
lRP 75
(60
ndash90)
RP 27
0 (2
40ndash3
00)
Hill
et al
199
813
Can
ine
acute
(n=5)
Aorto-lef
t fe
mora
lRP
1 Aortic
95
286
400
(1)
1 Fe
mora
lldquoM
inim
alrdquo
(4)
Audra
et al
200
07Porc
ine
surv
ival
(n=11
)Thora
cic
Aorto-lef
t In
trap
leura
l1
Aortic
74
(53
ndash155
)31
0 (2
76ndash3
38)
611
(250
-130
0)fe
mora
l2
Fem
ora
l
Mar
tinez
et al
Porc
ine
acute
(n=10
)Aortic
tube
graf
tTP
2 Aortic
Acu
te 93
plusmn28
Acu
te 17
9 plusmn
396
Acu
te 21
4 plusmn
437
8(this s
tudy)
Porc
ine
surv
ival
(n=14
)Su
rviv
al 59
6 plusmn
14Su
rviv
al 16
46
plusmn48
Su
rviv
al 16
9 plusmn
271
RP re
troper
itonea
l TP tran
sper
itonea
ldaggerC
om
bin
es r
eported
cla
mp +
aortoto
my
and a
ortic
anas
tam
osi
s tim
es
Dagger8 o
f 24
anim
als
wer
e to
tal la
par
osc
opic
pro
cedure
ssect4
end-to-s
ide
tran
sper
itonea
l 1
retroper
itonea
l (s
utu
red) 2
end-to-e
nd tra
nper
itonea
l 2
retroper
itonea
l (tie
d to a
cuff)
||4
sim
ula
ted a
n A
AA r
esec
tion
paraA 4
-cm
open
inci
sion w
as m
ade
to c
om
ple
te the
end-to-s
ide
aortic
anas
tam
osi
sE
nd-to-s
ide
aortic
anas
tom
osis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
134 JSLS (2003)7129-136
in the retroperitoneal space and about 200 mL of freeserosanguinous intraperitoneal fluid The nine 7-day sur-vivors were evaluated postoperatively and scored forbehavioral criteria Animals required very little pain med-ication during the first 24 hours No wound complicationsoccurred The 12 survivors with normal hind limb func-tion became ambulatory between 3 and 20 hours post-operatively
DISCUSSION
Procedure
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imagi-nation of the surgeon coupled with the progressive devel-opment of endolaparoscopic instrumentation Theseincluded the possibilities of coronary bypass by endoscopeas had been performed in a porcine model8 Although wedemonstrated the feasibility of full endoscopic repair of theabdominal aorta with a tube graft one of our main goalswas the documentation of performance improvement ofthe surgical team as reflected by a reduction in surgicaltime parameters and bleeding as the study progressed Acomparison of the 10 early procedures with the 14 latersurgeries indicates a modest reduction in total operativetime and estimated blood loss that was not statistically sig-nificant More importantly a dramatic and highly signifi-cant reduction occurred in the aortic cross-clamp time forgraft anastomosis a parameter we deem most vital to sur-gical outcome and postoperative morbidity Althoughother animal models for endolaporoscopic aortic repairhave utilized a variety of protocols grafts and instrumen-tation (Table 3)23679-13 we observe that our aortic clamptimes and total operative times are less than or equal tothose of other studies to date even though they includetwo demanding intraabdominal anastomoses performedwith full endolaparoscopic technique with Endoknottying Of course rapid evolution of endoscopic tech-niques and instrumentation has occurred since the earli-est animal models were developed Most investigatorshave reported an observable reduction in surgical timeparameters that comes through training and experiencealthough the learning curve for this procedure may besteep3671013
Difficulties in retracting the small bowel have led some inves-tigators to prefer a retroperitoneal approach2312 al-thoughone study preferred the transperitoneal approach10 and twoothers found both approaches equally acceptable911
Robotics
The use of the voice-operated computerized roboticAESOP and Hermes systems greatly improved the levelof precision obtainable by the surgeon for visualizing theoperative field and recording the procedure for futureanalysis14 This technology reduces the surgeonrsquos depen-dence on assistants and the associated delays for com-munication and manual adjustments
Bleeding
Certainly one of the most difficult tasks in endolaparo-scopic surgery is controlling bleeding Our model de-monstrated that secure proximal clamping is criticallyimportant in reducing blood loss The use of the 18-mmGSI flexible ports proved invaluable in permitting the useof conventional instruments for secure proximal and dis-tal clamping while maintaining the pneumoperitoneumOn the other hand the use of the endoluminal Fogartyballoon for distal aortic occlusion has certain benefits forcontrol in the relatively low-pressure distal aorta In theabsence of a second clamp more working space is avail-able for the surgeonrsquos instruments In case of excessivelumbar bleeding the balloon may be advanced and posi-tioned to help tamponade the site
Much of the bleeding encountered involved the lumbarvessels which in the pig are very delicate and subjectto tearing during aortic dissection Although this increas-es the surgical challenge only 6 of 24 animals (25) hadintraoperative bleeding problems and only 2 of these(8) required conversion to a minilaparotomy Westrongly advocate that the endoscopic surgeon always beready to make an abrupt conversion to open surgery forbleeding control
Spinal Cord Ischemia
Aortic clamping for graft anastomosis can produce hindlimb dysfunction if prolonged Excessive clamp time inturn is often a function of bleeding problems that mayobscure the surgical field and required additional sutur-ing time In other endolaparoscopic survival studiesBryne et al6 observed paraplegia in 3 of 8 dogs andAurdra et al7 recorded 1 case of paraplegia out of the 9pigs that survived the procedure Both studies had clamptimes in excess of 100 minutes for some cases The sin-gle case of hind limb sensory dysfunction in our studyresulted from a technical error that significantly delayedthe anastomosis All other surviving animals had good
ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study

A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
130 JSLS (2003)7129-136
graft patency and (3) elimination of spinal cord ischemia
METHODS
This study was conducted between April 1998 andJanuary 2000 under Protocol 6127-1 for care and use oflaboratory animals at Stanford University StanfordCalifornia USA Twenty-four female pigs with an averagebody weight of 55 kg (SDplusmn104 kg) were made to fastovernight premedicated for surgery with atropine (004mgkg IM) and sedated with tiletamine and zolazepam(Telazol Lederele Parenteral Inc Carolina Puerto Rico)at 6 mgkg IM Anesthesia was induced with 3halothane in oxygen delivered by facemask All animalswere orotracheally intubated and anesthesia was main-tained with 1 to 3 halothane in oxygen with mechan-ical ventilation (Hallowell model 2000 Hallowell EMCPittsfield MA USA) to maintain end-tidal carbon dioxidebetween 35 mm Hg and 55 mm Hg
Venous and arterial catheters were placed percutaneous-ly for drug and fluid administration and blood pressuremonitoring Electrocardiogram leads were placedFollowing instrumentation of the survival animals a 20-gauge 35-inch spinal needle (Monoject EmergencyMedical Products Waukesha WI USA) was placed in thelumbosacral joint and morphine sulfate was injectedepidurally at 01 mgkg for analgesia
Serial samples of hematocrit total serum protein andarterial blood gases were taken from the auricular arteri-al catheter Blood gas samples were analyzed immediate-ly on a calibrated blood gas analyzer (Ciba-Corningmodel 248 Global Medical Instrumentation Inc Albert-ville MN USA) Pulse oximetry (SpaceLabs model90651A Spacelabs Medical Issaquah WA USA) andcapnography (SpaceLabs model 1890-02 SpacelabsMedical Issaquah WA USA) were performed frequentlyduring anesthesia Lactated Ringerrsquos solution (AbbottLaboratories Abbott Park IL USA) was administeredintravenously at approximately 10 mLkghr throughoutanesthesia Fresh whole unmatched pig blood wasadministered to 2 pigs that had experienced intraopera-tive hemorrhaging Dobutamine was administered asneeded at 05 to 5 mcgkgmin to maintain systemic arte-rial blood pressure
The animals were placed in a full right lateral decubitusposition (left side up) in the Trendelenburg position(Figure 1) Preliminary measurements were made for
Figure 1 Position of pig and surgical team for endolaparoscop-ic aortic repair Pig in the right lateral decubitus position withTrendelenburg positioning Left to right scrub nurse surgeonassistant The labeled left costal margin is visible by the assistantrsquosleft hand The AESOP robotic arm is in the center of the fieldand the Hermes control system is to the right of the surgeonwho is wearing a voice-activation headset
Figure 2 Port placement for porcine endolaparoscopic aorticrepair model (1) Proximal aortic clamping (18 mm) (2) Distalaortic clamping (18 mm) (3) Endoscope (10 mm) (4) Left handinstrument (5 mm) (5) Right hand instrument (5 mm) (6) Assist(10 mm) Starting at costal margin 10 cm medially then 3 cmcaudally to (3) which is 5 cm from midline (6) is 3 cm from mid-line (4) and (5) are both 6 cm to 7 cm from the line between (3)and (6)
positioning the working and clamping ports as indicatedin Figure 2 The abdomen and groin were prepared withiodine-povidone solution and sterile drapes wereapplied Endolaparoscopic instrumentation included theUltraCision Harmonic scalpel and Ethicon Endoscissors(Ethicon Endo-Surgery Cincinnati OH USA) two 512-mm Ethicon Endopathreg trocars for the 0deg and 30deg 10-mmendoscopes (Stryker Endoscopy Mountain View CAUSA) and the Nezhat-Schroeder suction irrigation system(Davol Inc Cranston RI USA) two 355-mm EthiconEndopath trocars for the vascular instrumentation two18-mm GSI flexible ports (production rights currently heldby TycoUSSI Norwalk CT USA) for proximal and dis-tal clamping the Ethicon Ligaclip clip applier two 5-mmneedle holders and two 5-mm graspers (Ethicon Endo-Surgery Cincinnati OH USA) CO2 pneumoperitoneumwas created via a 511H Ethicon Endopath nonbladedOptiview trocar or a Veress needle introduced through asmall midline incision The endoscope was positionedwith a voice-activated AESOPreg 3000 robotic system(Computer Motion Inc Goleta CA USA) Video func-tions light source and insufflation were remotely con-trolled with the Hermes voice-activated system (StrykerEndoscopy Mountain View CA USA Computer MotionInc Goleta CA USA)
The surgical team consisted of the endolaparoscopic sur-geon 1 assistant and 1 scrub nurse The surgeon hadpreviously trained on a dry laboratory pelvic trainer Atthe beginning of the study the surgeon had accom-plished 65 hours of endolaparoscopic training increasingto 180 hours by the end of the study The endoscopictraining protocol used is divided into the following 3
JSLS (2003)7129-136 131
phases (Table 1) 10 hours are devoted to dry laborato-ry practice in endoscopic suturing cutting endo- andexoknot tying (Phase I) 20 hours are devoted to endo-scopic suture anastomosis of 8- 10- and 12-mm grafts invitro to develop technical precision (Phase II) and 50hours are devoted to increasing both quality and speedof anastomosis until they can be completed within 20minutes to 30 minutes (Phase III)
The transperitoneal approach was deliberately selectedas potentially the most difficult procedure for maximumtraining benefit This approach was maintained through-out the study so that all procedures could be directlycompared as to time parameters and surgical outcomeTrocars and ports were positioned in the abdomeninstrumentation was introduced and bowel loops weremoved to the right side of the abdomen to expose theposterior peritoneum which was entered with theHarmonic scalpel Approximately 5 cm of infrarenal aortawas dissected with a combination of blunt and sharpintrumentation including the UltraCision Harmonicscalpel and Endoscissors The lumbar branches werevisualized and controlled with the Ligaclip endoscopicclip applier Systemic heparinization (3 mgkg IV) wasthen initiated and the proximal aorta was clamped witha conventional aortic or carotid clamp (Figure 3) Distalaortic occlusion was obtained with a 6 Fogarty venousballoon catheter (Edwards Lifesciences LLC Irvine CAUSA) introduced via the femoral artery in 7 of the 10acute animals or an iNtrack clamp (Novare SurgicalCupertino CA USA) in all remaining animals
Vertical transection of the aortic wall was performed with5- or 10-mm Endoscissors An 8- or 10-mm diameterpolytetrafluoroethylene graft (IMPRA Inc Tempe AZUSA) was implanted by continuous end-to-end sutureanastomosis with 4-0 and 3-0 Prolene with a TF or BBneedle (Ethicon Sommerville NJ USA) and 5-mm endo-scopic needle holders A 10- or 12-cm suture providedoptimal ergonomics for tying Endoknots Then the distalclamp was released and the anastomosis was examinedfor leaks Gelfoam (Upjohn Pharmaceuticals Chicago ILUSA) was used to control needle site holes Finally theproximal clamp was gradually released The posteriorperitoneum was closed with staples and in the survivalgroup the port sites were closed with absorbable suture
The animals were divided into the following 2 groupsacute (10 animals) and survival (14 animals) Five of theacute animals were maintained under anesthesia for 05
Table 1Endoscopic Motor Sensory Skill Acquisition
A Formal Training Program
Camps Time (hrs) Stage Goals
1 10 Basic Skills Suture-Cutting(Exercise)EndoknotsEqual Hands
2 Aesop and 30 Quality SutureHermes Anastomosis
3 Zeus 80 Quality and 20-30 MinutesSpeed Anastomosis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
132 JSLS (2003)7129-136
hour following surgery and 5 for 2 hours prior to beingsacrificed Five of the survival animals were recoveredfrom anesthesia and maintained for 7 hours and 9 weremaintained for 7 days prior to sacrifice and autopsyAnimals were scored for several behavioral criteria post-operatively Upon autopsy 1 cm of proximal and 1 cm ofdistal host aortic tissue including the graft end and anas-tomosis were harvested visually inspected under 35times magnification for suture line integrity and photo-graphic analysis Data groups were compared with 2-tailed Student t tests assuming unequal variance
RESULTS
Full endoscopic infrarenal aortic grafts involving 2 end-to-end anastomoses was successfully completed in all 24animals (Table 2) Mean aortic clamping time was
929plusmn2804 minutes in the acute group and 596plusmn138minutes in the survival group (Table 3) Mean total oper-ative time was 179plusmn396 minutes for the acute group and1646plusmn48 minutes in the survival group Mean blood losswas 214plusmn4378 mL for the acute group and 1692plusmn271 mLfor the survival group
One animal in the survival group died of respiratoryarrest due to airway obstruction 2 hours postoperativelyand the other 13 survived until the prescribed sacrificeOnly 1 animal suffered from hind limb dysfunction dueto a prolonged aortic clamping time of 92 minutes Thisresulted from a size mismatch between the preselectedgraft (10 mm) and the host aorta (7 mm) necessitatingadditional suturing to complete the anastomosis The ani-mal was able to stand up with assistance but could notambulate on its own due to severe proprioceptive anes-thesia Histology of the spinal cord showed medullarinfarctions mostly localized in the posterior sensoryhorns which is consistent with the clinical symptoms
Bleeding complications occurred in 6 animals from lum-bar branches and a vena cava branch tear during dissec-tion In 4 animals control was obtained endoscopicallyHowever in the case of the caval tear and aproximaldistal lumbar artery tear the bleeding wasmore difficult to control requiring conversion to a mini-laparotomy (5 cm) These animals required 1 unit ofpacked red cells (250 mL) each
No bleeding at the graft anastomoses was found onautopsy The 24 grafts were patent and all the sutureanastomoses were found intact Two grafts were foundto have an isolated 10 x 8-mm adherent blood clot at theanastomotic suture line All retroperitoneal spaces hadperigraft hematomas which were expectedly smallexcept for in 1 animal that had an estimated 100 mL clot
Figure 3 Suturing the distal aortic graft anatomosis with con-ventional clamps
Table 2Porcine Endoscopic Abdominal Aortic Resection Model
Type of Procedure Weight of Pig Aortic Clamp Time Total Operative Time Estimated Blood Loss
Acute (n = 10) 634 kg plusmn 6 kg 929 m plusmn 28 m 179 m plusmn 396 m 214 mL plusmn 4378 mL Survival (n = 14) 491 kg plusmn 86 kg 596 kg plusmn138 m 1646 m plusmn 48 m 1692 mL plusmn 271 mLSignificance (t test)dagger P = 000008 P = 00046 P = 043 ns P = 034 ns
Values are group means and standard deviationsdaggerThe surgical time and blood loss parameters for the early (acute) procedures are compared with the later (survival) proceduresns = not significant
JSLS (2003)7129-136 133
Tab
le 3
Par
amet
ers
of Exp
erim
enta
l Abdom
inal
Aortic
Endola
par
osc
opic
Rep
air
Model
s
Au
thor
An
imal
Pro
cedu
reSu
rgic
alN
oof
A
orti
c C
lam
pTo
tal O
per
ativ
eTo
tal B
lood
Mod
elA
pp
roac
h
An
asto
mos
es
Tim
e (m
in)
Tim
e (m
in)
Loss
(m
L)
Dio
n e
t al
199
52Porc
ine
acute
(n=26
)Aortobife
mora
lTP
1 Aortic
85ndash1
20dagger
lt24
0lt25
02
Fem
ora
l
Byr
ne
et a
l 19
956
Can
ine
surv
ival
(n=8Dagger
)Aortobife
mora
lTP =
15
1 Aortic
87 plusmn
206
19
3 plusmn
123
128
plusmn12
81
RP =
72
Fem
ora
l
Ahn e
t al
199
59Porc
ine
acute
(n=10
)Aorto-lef
t fe
mora
lTP =
71
Aortic
sectN
ot re
ported
147
(120
ndash240
)20
(5ndash
50)
RP =
31
Fem
ora
l
Chen
et al
199
610
Porc
ine
acute
(n=23
)Cust
om
tube
graf
tTP =
21
2 Aortic
Not re
ported
Not re
ported
Not re
ported
RP =
2
Dio
n e
t al
199
63Porc
ine
acute
(n=8)
Aortobife
mora
l||
Ant RP
1 Aortic
Not re
ported
270
ldquoNev
er gt
550rdquo
2
Fem
ora
l
Jones
et al
199
611
Porc
ine
acute
(n=10
)Aor
to-rig
ht fem
oral
paraTP =
51
Aortic
TP 27
plusmn5
TP 16
1 plusmn
22N
ot re
ported
RP =
51
Fem
ora
lRP 28
plusmn5
RP 19
2 plusmn
1
Bru
ns
et a
l 19
9812
Porc
ine
acute
(n=20
)Aortobife
mora
lTP =
10
1 Aortic
TP 60
(45
ndash75)
TP 24
0 (2
10ndash2
70)
Not re
ported
RP =
10
2 Fe
mora
lRP 75
(60
ndash90)
RP 27
0 (2
40ndash3
00)
Hill
et al
199
813
Can
ine
acute
(n=5)
Aorto-lef
t fe
mora
lRP
1 Aortic
95
286
400
(1)
1 Fe
mora
lldquoM
inim
alrdquo
(4)
Audra
et al
200
07Porc
ine
surv
ival
(n=11
)Thora
cic
Aorto-lef
t In
trap
leura
l1
Aortic
74
(53
ndash155
)31
0 (2
76ndash3
38)
611
(250
-130
0)fe
mora
l2
Fem
ora
l
Mar
tinez
et al
Porc
ine
acute
(n=10
)Aortic
tube
graf
tTP
2 Aortic
Acu
te 93
plusmn28
Acu
te 17
9 plusmn
396
Acu
te 21
4 plusmn
437
8(this s
tudy)
Porc
ine
surv
ival
(n=14
)Su
rviv
al 59
6 plusmn
14Su
rviv
al 16
46
plusmn48
Su
rviv
al 16
9 plusmn
271
RP re
troper
itonea
l TP tran
sper
itonea
ldaggerC
om
bin
es r
eported
cla
mp +
aortoto
my
and a
ortic
anas
tam
osi
s tim
es
Dagger8 o
f 24
anim
als
wer
e to
tal la
par
osc
opic
pro
cedure
ssect4
end-to-s
ide
tran
sper
itonea
l 1
retroper
itonea
l (s
utu
red) 2
end-to-e
nd tra
nper
itonea
l 2
retroper
itonea
l (tie
d to a
cuff)
||4
sim
ula
ted a
n A
AA r
esec
tion
paraA 4
-cm
open
inci
sion w
as m
ade
to c
om
ple
te the
end-to-s
ide
aortic
anas
tam
osi
sE
nd-to-s
ide
aortic
anas
tom
osis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
134 JSLS (2003)7129-136
in the retroperitoneal space and about 200 mL of freeserosanguinous intraperitoneal fluid The nine 7-day sur-vivors were evaluated postoperatively and scored forbehavioral criteria Animals required very little pain med-ication during the first 24 hours No wound complicationsoccurred The 12 survivors with normal hind limb func-tion became ambulatory between 3 and 20 hours post-operatively
DISCUSSION
Procedure
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imagi-nation of the surgeon coupled with the progressive devel-opment of endolaparoscopic instrumentation Theseincluded the possibilities of coronary bypass by endoscopeas had been performed in a porcine model8 Although wedemonstrated the feasibility of full endoscopic repair of theabdominal aorta with a tube graft one of our main goalswas the documentation of performance improvement ofthe surgical team as reflected by a reduction in surgicaltime parameters and bleeding as the study progressed Acomparison of the 10 early procedures with the 14 latersurgeries indicates a modest reduction in total operativetime and estimated blood loss that was not statistically sig-nificant More importantly a dramatic and highly signifi-cant reduction occurred in the aortic cross-clamp time forgraft anastomosis a parameter we deem most vital to sur-gical outcome and postoperative morbidity Althoughother animal models for endolaporoscopic aortic repairhave utilized a variety of protocols grafts and instrumen-tation (Table 3)23679-13 we observe that our aortic clamptimes and total operative times are less than or equal tothose of other studies to date even though they includetwo demanding intraabdominal anastomoses performedwith full endolaparoscopic technique with Endoknottying Of course rapid evolution of endoscopic tech-niques and instrumentation has occurred since the earli-est animal models were developed Most investigatorshave reported an observable reduction in surgical timeparameters that comes through training and experiencealthough the learning curve for this procedure may besteep3671013
Difficulties in retracting the small bowel have led some inves-tigators to prefer a retroperitoneal approach2312 al-thoughone study preferred the transperitoneal approach10 and twoothers found both approaches equally acceptable911
Robotics
The use of the voice-operated computerized roboticAESOP and Hermes systems greatly improved the levelof precision obtainable by the surgeon for visualizing theoperative field and recording the procedure for futureanalysis14 This technology reduces the surgeonrsquos depen-dence on assistants and the associated delays for com-munication and manual adjustments
Bleeding
Certainly one of the most difficult tasks in endolaparo-scopic surgery is controlling bleeding Our model de-monstrated that secure proximal clamping is criticallyimportant in reducing blood loss The use of the 18-mmGSI flexible ports proved invaluable in permitting the useof conventional instruments for secure proximal and dis-tal clamping while maintaining the pneumoperitoneumOn the other hand the use of the endoluminal Fogartyballoon for distal aortic occlusion has certain benefits forcontrol in the relatively low-pressure distal aorta In theabsence of a second clamp more working space is avail-able for the surgeonrsquos instruments In case of excessivelumbar bleeding the balloon may be advanced and posi-tioned to help tamponade the site
Much of the bleeding encountered involved the lumbarvessels which in the pig are very delicate and subjectto tearing during aortic dissection Although this increas-es the surgical challenge only 6 of 24 animals (25) hadintraoperative bleeding problems and only 2 of these(8) required conversion to a minilaparotomy Westrongly advocate that the endoscopic surgeon always beready to make an abrupt conversion to open surgery forbleeding control
Spinal Cord Ischemia
Aortic clamping for graft anastomosis can produce hindlimb dysfunction if prolonged Excessive clamp time inturn is often a function of bleeding problems that mayobscure the surgical field and required additional sutur-ing time In other endolaparoscopic survival studiesBryne et al6 observed paraplegia in 3 of 8 dogs andAurdra et al7 recorded 1 case of paraplegia out of the 9pigs that survived the procedure Both studies had clamptimes in excess of 100 minutes for some cases The sin-gle case of hind limb sensory dysfunction in our studyresulted from a technical error that significantly delayedthe anastomosis All other surviving animals had good
ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study

positioning the working and clamping ports as indicatedin Figure 2 The abdomen and groin were prepared withiodine-povidone solution and sterile drapes wereapplied Endolaparoscopic instrumentation included theUltraCision Harmonic scalpel and Ethicon Endoscissors(Ethicon Endo-Surgery Cincinnati OH USA) two 512-mm Ethicon Endopathreg trocars for the 0deg and 30deg 10-mmendoscopes (Stryker Endoscopy Mountain View CAUSA) and the Nezhat-Schroeder suction irrigation system(Davol Inc Cranston RI USA) two 355-mm EthiconEndopath trocars for the vascular instrumentation two18-mm GSI flexible ports (production rights currently heldby TycoUSSI Norwalk CT USA) for proximal and dis-tal clamping the Ethicon Ligaclip clip applier two 5-mmneedle holders and two 5-mm graspers (Ethicon Endo-Surgery Cincinnati OH USA) CO2 pneumoperitoneumwas created via a 511H Ethicon Endopath nonbladedOptiview trocar or a Veress needle introduced through asmall midline incision The endoscope was positionedwith a voice-activated AESOPreg 3000 robotic system(Computer Motion Inc Goleta CA USA) Video func-tions light source and insufflation were remotely con-trolled with the Hermes voice-activated system (StrykerEndoscopy Mountain View CA USA Computer MotionInc Goleta CA USA)
The surgical team consisted of the endolaparoscopic sur-geon 1 assistant and 1 scrub nurse The surgeon hadpreviously trained on a dry laboratory pelvic trainer Atthe beginning of the study the surgeon had accom-plished 65 hours of endolaparoscopic training increasingto 180 hours by the end of the study The endoscopictraining protocol used is divided into the following 3
JSLS (2003)7129-136 131
phases (Table 1) 10 hours are devoted to dry laborato-ry practice in endoscopic suturing cutting endo- andexoknot tying (Phase I) 20 hours are devoted to endo-scopic suture anastomosis of 8- 10- and 12-mm grafts invitro to develop technical precision (Phase II) and 50hours are devoted to increasing both quality and speedof anastomosis until they can be completed within 20minutes to 30 minutes (Phase III)
The transperitoneal approach was deliberately selectedas potentially the most difficult procedure for maximumtraining benefit This approach was maintained through-out the study so that all procedures could be directlycompared as to time parameters and surgical outcomeTrocars and ports were positioned in the abdomeninstrumentation was introduced and bowel loops weremoved to the right side of the abdomen to expose theposterior peritoneum which was entered with theHarmonic scalpel Approximately 5 cm of infrarenal aortawas dissected with a combination of blunt and sharpintrumentation including the UltraCision Harmonicscalpel and Endoscissors The lumbar branches werevisualized and controlled with the Ligaclip endoscopicclip applier Systemic heparinization (3 mgkg IV) wasthen initiated and the proximal aorta was clamped witha conventional aortic or carotid clamp (Figure 3) Distalaortic occlusion was obtained with a 6 Fogarty venousballoon catheter (Edwards Lifesciences LLC Irvine CAUSA) introduced via the femoral artery in 7 of the 10acute animals or an iNtrack clamp (Novare SurgicalCupertino CA USA) in all remaining animals
Vertical transection of the aortic wall was performed with5- or 10-mm Endoscissors An 8- or 10-mm diameterpolytetrafluoroethylene graft (IMPRA Inc Tempe AZUSA) was implanted by continuous end-to-end sutureanastomosis with 4-0 and 3-0 Prolene with a TF or BBneedle (Ethicon Sommerville NJ USA) and 5-mm endo-scopic needle holders A 10- or 12-cm suture providedoptimal ergonomics for tying Endoknots Then the distalclamp was released and the anastomosis was examinedfor leaks Gelfoam (Upjohn Pharmaceuticals Chicago ILUSA) was used to control needle site holes Finally theproximal clamp was gradually released The posteriorperitoneum was closed with staples and in the survivalgroup the port sites were closed with absorbable suture
The animals were divided into the following 2 groupsacute (10 animals) and survival (14 animals) Five of theacute animals were maintained under anesthesia for 05
Table 1Endoscopic Motor Sensory Skill Acquisition
A Formal Training Program
Camps Time (hrs) Stage Goals
1 10 Basic Skills Suture-Cutting(Exercise)EndoknotsEqual Hands
2 Aesop and 30 Quality SutureHermes Anastomosis
3 Zeus 80 Quality and 20-30 MinutesSpeed Anastomosis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
132 JSLS (2003)7129-136
hour following surgery and 5 for 2 hours prior to beingsacrificed Five of the survival animals were recoveredfrom anesthesia and maintained for 7 hours and 9 weremaintained for 7 days prior to sacrifice and autopsyAnimals were scored for several behavioral criteria post-operatively Upon autopsy 1 cm of proximal and 1 cm ofdistal host aortic tissue including the graft end and anas-tomosis were harvested visually inspected under 35times magnification for suture line integrity and photo-graphic analysis Data groups were compared with 2-tailed Student t tests assuming unequal variance
RESULTS
Full endoscopic infrarenal aortic grafts involving 2 end-to-end anastomoses was successfully completed in all 24animals (Table 2) Mean aortic clamping time was
929plusmn2804 minutes in the acute group and 596plusmn138minutes in the survival group (Table 3) Mean total oper-ative time was 179plusmn396 minutes for the acute group and1646plusmn48 minutes in the survival group Mean blood losswas 214plusmn4378 mL for the acute group and 1692plusmn271 mLfor the survival group
One animal in the survival group died of respiratoryarrest due to airway obstruction 2 hours postoperativelyand the other 13 survived until the prescribed sacrificeOnly 1 animal suffered from hind limb dysfunction dueto a prolonged aortic clamping time of 92 minutes Thisresulted from a size mismatch between the preselectedgraft (10 mm) and the host aorta (7 mm) necessitatingadditional suturing to complete the anastomosis The ani-mal was able to stand up with assistance but could notambulate on its own due to severe proprioceptive anes-thesia Histology of the spinal cord showed medullarinfarctions mostly localized in the posterior sensoryhorns which is consistent with the clinical symptoms
Bleeding complications occurred in 6 animals from lum-bar branches and a vena cava branch tear during dissec-tion In 4 animals control was obtained endoscopicallyHowever in the case of the caval tear and aproximaldistal lumbar artery tear the bleeding wasmore difficult to control requiring conversion to a mini-laparotomy (5 cm) These animals required 1 unit ofpacked red cells (250 mL) each
No bleeding at the graft anastomoses was found onautopsy The 24 grafts were patent and all the sutureanastomoses were found intact Two grafts were foundto have an isolated 10 x 8-mm adherent blood clot at theanastomotic suture line All retroperitoneal spaces hadperigraft hematomas which were expectedly smallexcept for in 1 animal that had an estimated 100 mL clot
Figure 3 Suturing the distal aortic graft anatomosis with con-ventional clamps
Table 2Porcine Endoscopic Abdominal Aortic Resection Model
Type of Procedure Weight of Pig Aortic Clamp Time Total Operative Time Estimated Blood Loss
Acute (n = 10) 634 kg plusmn 6 kg 929 m plusmn 28 m 179 m plusmn 396 m 214 mL plusmn 4378 mL Survival (n = 14) 491 kg plusmn 86 kg 596 kg plusmn138 m 1646 m plusmn 48 m 1692 mL plusmn 271 mLSignificance (t test)dagger P = 000008 P = 00046 P = 043 ns P = 034 ns
Values are group means and standard deviationsdaggerThe surgical time and blood loss parameters for the early (acute) procedures are compared with the later (survival) proceduresns = not significant
JSLS (2003)7129-136 133
Tab
le 3
Par
amet
ers
of Exp
erim
enta
l Abdom
inal
Aortic
Endola
par
osc
opic
Rep
air
Model
s
Au
thor
An
imal
Pro
cedu
reSu
rgic
alN
oof
A
orti
c C
lam
pTo
tal O
per
ativ
eTo
tal B
lood
Mod
elA
pp
roac
h
An
asto
mos
es
Tim
e (m
in)
Tim
e (m
in)
Loss
(m
L)
Dio
n e
t al
199
52Porc
ine
acute
(n=26
)Aortobife
mora
lTP
1 Aortic
85ndash1
20dagger
lt24
0lt25
02
Fem
ora
l
Byr
ne
et a
l 19
956
Can
ine
surv
ival
(n=8Dagger
)Aortobife
mora
lTP =
15
1 Aortic
87 plusmn
206
19
3 plusmn
123
128
plusmn12
81
RP =
72
Fem
ora
l
Ahn e
t al
199
59Porc
ine
acute
(n=10
)Aorto-lef
t fe
mora
lTP =
71
Aortic
sectN
ot re
ported
147
(120
ndash240
)20
(5ndash
50)
RP =
31
Fem
ora
l
Chen
et al
199
610
Porc
ine
acute
(n=23
)Cust
om
tube
graf
tTP =
21
2 Aortic
Not re
ported
Not re
ported
Not re
ported
RP =
2
Dio
n e
t al
199
63Porc
ine
acute
(n=8)
Aortobife
mora
l||
Ant RP
1 Aortic
Not re
ported
270
ldquoNev
er gt
550rdquo
2
Fem
ora
l
Jones
et al
199
611
Porc
ine
acute
(n=10
)Aor
to-rig
ht fem
oral
paraTP =
51
Aortic
TP 27
plusmn5
TP 16
1 plusmn
22N
ot re
ported
RP =
51
Fem
ora
lRP 28
plusmn5
RP 19
2 plusmn
1
Bru
ns
et a
l 19
9812
Porc
ine
acute
(n=20
)Aortobife
mora
lTP =
10
1 Aortic
TP 60
(45
ndash75)
TP 24
0 (2
10ndash2
70)
Not re
ported
RP =
10
2 Fe
mora
lRP 75
(60
ndash90)
RP 27
0 (2
40ndash3
00)
Hill
et al
199
813
Can
ine
acute
(n=5)
Aorto-lef
t fe
mora
lRP
1 Aortic
95
286
400
(1)
1 Fe
mora
lldquoM
inim
alrdquo
(4)
Audra
et al
200
07Porc
ine
surv
ival
(n=11
)Thora
cic
Aorto-lef
t In
trap
leura
l1
Aortic
74
(53
ndash155
)31
0 (2
76ndash3
38)
611
(250
-130
0)fe
mora
l2
Fem
ora
l
Mar
tinez
et al
Porc
ine
acute
(n=10
)Aortic
tube
graf
tTP
2 Aortic
Acu
te 93
plusmn28
Acu
te 17
9 plusmn
396
Acu
te 21
4 plusmn
437
8(this s
tudy)
Porc
ine
surv
ival
(n=14
)Su
rviv
al 59
6 plusmn
14Su
rviv
al 16
46
plusmn48
Su
rviv
al 16
9 plusmn
271
RP re
troper
itonea
l TP tran
sper
itonea
ldaggerC
om
bin
es r
eported
cla
mp +
aortoto
my
and a
ortic
anas
tam
osi
s tim
es
Dagger8 o
f 24
anim
als
wer
e to
tal la
par
osc
opic
pro
cedure
ssect4
end-to-s
ide
tran
sper
itonea
l 1
retroper
itonea
l (s
utu
red) 2
end-to-e
nd tra
nper
itonea
l 2
retroper
itonea
l (tie
d to a
cuff)
||4
sim
ula
ted a
n A
AA r
esec
tion
paraA 4
-cm
open
inci
sion w
as m
ade
to c
om
ple
te the
end-to-s
ide
aortic
anas
tam
osi
sE
nd-to-s
ide
aortic
anas
tom
osis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
134 JSLS (2003)7129-136
in the retroperitoneal space and about 200 mL of freeserosanguinous intraperitoneal fluid The nine 7-day sur-vivors were evaluated postoperatively and scored forbehavioral criteria Animals required very little pain med-ication during the first 24 hours No wound complicationsoccurred The 12 survivors with normal hind limb func-tion became ambulatory between 3 and 20 hours post-operatively
DISCUSSION
Procedure
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imagi-nation of the surgeon coupled with the progressive devel-opment of endolaparoscopic instrumentation Theseincluded the possibilities of coronary bypass by endoscopeas had been performed in a porcine model8 Although wedemonstrated the feasibility of full endoscopic repair of theabdominal aorta with a tube graft one of our main goalswas the documentation of performance improvement ofthe surgical team as reflected by a reduction in surgicaltime parameters and bleeding as the study progressed Acomparison of the 10 early procedures with the 14 latersurgeries indicates a modest reduction in total operativetime and estimated blood loss that was not statistically sig-nificant More importantly a dramatic and highly signifi-cant reduction occurred in the aortic cross-clamp time forgraft anastomosis a parameter we deem most vital to sur-gical outcome and postoperative morbidity Althoughother animal models for endolaporoscopic aortic repairhave utilized a variety of protocols grafts and instrumen-tation (Table 3)23679-13 we observe that our aortic clamptimes and total operative times are less than or equal tothose of other studies to date even though they includetwo demanding intraabdominal anastomoses performedwith full endolaparoscopic technique with Endoknottying Of course rapid evolution of endoscopic tech-niques and instrumentation has occurred since the earli-est animal models were developed Most investigatorshave reported an observable reduction in surgical timeparameters that comes through training and experiencealthough the learning curve for this procedure may besteep3671013
Difficulties in retracting the small bowel have led some inves-tigators to prefer a retroperitoneal approach2312 al-thoughone study preferred the transperitoneal approach10 and twoothers found both approaches equally acceptable911
Robotics
The use of the voice-operated computerized roboticAESOP and Hermes systems greatly improved the levelof precision obtainable by the surgeon for visualizing theoperative field and recording the procedure for futureanalysis14 This technology reduces the surgeonrsquos depen-dence on assistants and the associated delays for com-munication and manual adjustments
Bleeding
Certainly one of the most difficult tasks in endolaparo-scopic surgery is controlling bleeding Our model de-monstrated that secure proximal clamping is criticallyimportant in reducing blood loss The use of the 18-mmGSI flexible ports proved invaluable in permitting the useof conventional instruments for secure proximal and dis-tal clamping while maintaining the pneumoperitoneumOn the other hand the use of the endoluminal Fogartyballoon for distal aortic occlusion has certain benefits forcontrol in the relatively low-pressure distal aorta In theabsence of a second clamp more working space is avail-able for the surgeonrsquos instruments In case of excessivelumbar bleeding the balloon may be advanced and posi-tioned to help tamponade the site
Much of the bleeding encountered involved the lumbarvessels which in the pig are very delicate and subjectto tearing during aortic dissection Although this increas-es the surgical challenge only 6 of 24 animals (25) hadintraoperative bleeding problems and only 2 of these(8) required conversion to a minilaparotomy Westrongly advocate that the endoscopic surgeon always beready to make an abrupt conversion to open surgery forbleeding control
Spinal Cord Ischemia
Aortic clamping for graft anastomosis can produce hindlimb dysfunction if prolonged Excessive clamp time inturn is often a function of bleeding problems that mayobscure the surgical field and required additional sutur-ing time In other endolaparoscopic survival studiesBryne et al6 observed paraplegia in 3 of 8 dogs andAurdra et al7 recorded 1 case of paraplegia out of the 9pigs that survived the procedure Both studies had clamptimes in excess of 100 minutes for some cases The sin-gle case of hind limb sensory dysfunction in our studyresulted from a technical error that significantly delayedthe anastomosis All other surviving animals had good
ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study

A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
132 JSLS (2003)7129-136
hour following surgery and 5 for 2 hours prior to beingsacrificed Five of the survival animals were recoveredfrom anesthesia and maintained for 7 hours and 9 weremaintained for 7 days prior to sacrifice and autopsyAnimals were scored for several behavioral criteria post-operatively Upon autopsy 1 cm of proximal and 1 cm ofdistal host aortic tissue including the graft end and anas-tomosis were harvested visually inspected under 35times magnification for suture line integrity and photo-graphic analysis Data groups were compared with 2-tailed Student t tests assuming unequal variance
RESULTS
Full endoscopic infrarenal aortic grafts involving 2 end-to-end anastomoses was successfully completed in all 24animals (Table 2) Mean aortic clamping time was
929plusmn2804 minutes in the acute group and 596plusmn138minutes in the survival group (Table 3) Mean total oper-ative time was 179plusmn396 minutes for the acute group and1646plusmn48 minutes in the survival group Mean blood losswas 214plusmn4378 mL for the acute group and 1692plusmn271 mLfor the survival group
One animal in the survival group died of respiratoryarrest due to airway obstruction 2 hours postoperativelyand the other 13 survived until the prescribed sacrificeOnly 1 animal suffered from hind limb dysfunction dueto a prolonged aortic clamping time of 92 minutes Thisresulted from a size mismatch between the preselectedgraft (10 mm) and the host aorta (7 mm) necessitatingadditional suturing to complete the anastomosis The ani-mal was able to stand up with assistance but could notambulate on its own due to severe proprioceptive anes-thesia Histology of the spinal cord showed medullarinfarctions mostly localized in the posterior sensoryhorns which is consistent with the clinical symptoms
Bleeding complications occurred in 6 animals from lum-bar branches and a vena cava branch tear during dissec-tion In 4 animals control was obtained endoscopicallyHowever in the case of the caval tear and aproximaldistal lumbar artery tear the bleeding wasmore difficult to control requiring conversion to a mini-laparotomy (5 cm) These animals required 1 unit ofpacked red cells (250 mL) each
No bleeding at the graft anastomoses was found onautopsy The 24 grafts were patent and all the sutureanastomoses were found intact Two grafts were foundto have an isolated 10 x 8-mm adherent blood clot at theanastomotic suture line All retroperitoneal spaces hadperigraft hematomas which were expectedly smallexcept for in 1 animal that had an estimated 100 mL clot
Figure 3 Suturing the distal aortic graft anatomosis with con-ventional clamps
Table 2Porcine Endoscopic Abdominal Aortic Resection Model
Type of Procedure Weight of Pig Aortic Clamp Time Total Operative Time Estimated Blood Loss
Acute (n = 10) 634 kg plusmn 6 kg 929 m plusmn 28 m 179 m plusmn 396 m 214 mL plusmn 4378 mL Survival (n = 14) 491 kg plusmn 86 kg 596 kg plusmn138 m 1646 m plusmn 48 m 1692 mL plusmn 271 mLSignificance (t test)dagger P = 000008 P = 00046 P = 043 ns P = 034 ns
Values are group means and standard deviationsdaggerThe surgical time and blood loss parameters for the early (acute) procedures are compared with the later (survival) proceduresns = not significant
JSLS (2003)7129-136 133
Tab
le 3
Par
amet
ers
of Exp
erim
enta
l Abdom
inal
Aortic
Endola
par
osc
opic
Rep
air
Model
s
Au
thor
An
imal
Pro
cedu
reSu
rgic
alN
oof
A
orti
c C
lam
pTo
tal O
per
ativ
eTo
tal B
lood
Mod
elA
pp
roac
h
An
asto
mos
es
Tim
e (m
in)
Tim
e (m
in)
Loss
(m
L)
Dio
n e
t al
199
52Porc
ine
acute
(n=26
)Aortobife
mora
lTP
1 Aortic
85ndash1
20dagger
lt24
0lt25
02
Fem
ora
l
Byr
ne
et a
l 19
956
Can
ine
surv
ival
(n=8Dagger
)Aortobife
mora
lTP =
15
1 Aortic
87 plusmn
206
19
3 plusmn
123
128
plusmn12
81
RP =
72
Fem
ora
l
Ahn e
t al
199
59Porc
ine
acute
(n=10
)Aorto-lef
t fe
mora
lTP =
71
Aortic
sectN
ot re
ported
147
(120
ndash240
)20
(5ndash
50)
RP =
31
Fem
ora
l
Chen
et al
199
610
Porc
ine
acute
(n=23
)Cust
om
tube
graf
tTP =
21
2 Aortic
Not re
ported
Not re
ported
Not re
ported
RP =
2
Dio
n e
t al
199
63Porc
ine
acute
(n=8)
Aortobife
mora
l||
Ant RP
1 Aortic
Not re
ported
270
ldquoNev
er gt
550rdquo
2
Fem
ora
l
Jones
et al
199
611
Porc
ine
acute
(n=10
)Aor
to-rig
ht fem
oral
paraTP =
51
Aortic
TP 27
plusmn5
TP 16
1 plusmn
22N
ot re
ported
RP =
51
Fem
ora
lRP 28
plusmn5
RP 19
2 plusmn
1
Bru
ns
et a
l 19
9812
Porc
ine
acute
(n=20
)Aortobife
mora
lTP =
10
1 Aortic
TP 60
(45
ndash75)
TP 24
0 (2
10ndash2
70)
Not re
ported
RP =
10
2 Fe
mora
lRP 75
(60
ndash90)
RP 27
0 (2
40ndash3
00)
Hill
et al
199
813
Can
ine
acute
(n=5)
Aorto-lef
t fe
mora
lRP
1 Aortic
95
286
400
(1)
1 Fe
mora
lldquoM
inim
alrdquo
(4)
Audra
et al
200
07Porc
ine
surv
ival
(n=11
)Thora
cic
Aorto-lef
t In
trap
leura
l1
Aortic
74
(53
ndash155
)31
0 (2
76ndash3
38)
611
(250
-130
0)fe
mora
l2
Fem
ora
l
Mar
tinez
et al
Porc
ine
acute
(n=10
)Aortic
tube
graf
tTP
2 Aortic
Acu
te 93
plusmn28
Acu
te 17
9 plusmn
396
Acu
te 21
4 plusmn
437
8(this s
tudy)
Porc
ine
surv
ival
(n=14
)Su
rviv
al 59
6 plusmn
14Su
rviv
al 16
46
plusmn48
Su
rviv
al 16
9 plusmn
271
RP re
troper
itonea
l TP tran
sper
itonea
ldaggerC
om
bin
es r
eported
cla
mp +
aortoto
my
and a
ortic
anas
tam
osi
s tim
es
Dagger8 o
f 24
anim
als
wer
e to
tal la
par
osc
opic
pro
cedure
ssect4
end-to-s
ide
tran
sper
itonea
l 1
retroper
itonea
l (s
utu
red) 2
end-to-e
nd tra
nper
itonea
l 2
retroper
itonea
l (tie
d to a
cuff)
||4
sim
ula
ted a
n A
AA r
esec
tion
paraA 4
-cm
open
inci
sion w
as m
ade
to c
om
ple
te the
end-to-s
ide
aortic
anas
tam
osi
sE
nd-to-s
ide
aortic
anas
tom
osis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
134 JSLS (2003)7129-136
in the retroperitoneal space and about 200 mL of freeserosanguinous intraperitoneal fluid The nine 7-day sur-vivors were evaluated postoperatively and scored forbehavioral criteria Animals required very little pain med-ication during the first 24 hours No wound complicationsoccurred The 12 survivors with normal hind limb func-tion became ambulatory between 3 and 20 hours post-operatively
DISCUSSION
Procedure
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imagi-nation of the surgeon coupled with the progressive devel-opment of endolaparoscopic instrumentation Theseincluded the possibilities of coronary bypass by endoscopeas had been performed in a porcine model8 Although wedemonstrated the feasibility of full endoscopic repair of theabdominal aorta with a tube graft one of our main goalswas the documentation of performance improvement ofthe surgical team as reflected by a reduction in surgicaltime parameters and bleeding as the study progressed Acomparison of the 10 early procedures with the 14 latersurgeries indicates a modest reduction in total operativetime and estimated blood loss that was not statistically sig-nificant More importantly a dramatic and highly signifi-cant reduction occurred in the aortic cross-clamp time forgraft anastomosis a parameter we deem most vital to sur-gical outcome and postoperative morbidity Althoughother animal models for endolaporoscopic aortic repairhave utilized a variety of protocols grafts and instrumen-tation (Table 3)23679-13 we observe that our aortic clamptimes and total operative times are less than or equal tothose of other studies to date even though they includetwo demanding intraabdominal anastomoses performedwith full endolaparoscopic technique with Endoknottying Of course rapid evolution of endoscopic tech-niques and instrumentation has occurred since the earli-est animal models were developed Most investigatorshave reported an observable reduction in surgical timeparameters that comes through training and experiencealthough the learning curve for this procedure may besteep3671013
Difficulties in retracting the small bowel have led some inves-tigators to prefer a retroperitoneal approach2312 al-thoughone study preferred the transperitoneal approach10 and twoothers found both approaches equally acceptable911
Robotics
The use of the voice-operated computerized roboticAESOP and Hermes systems greatly improved the levelof precision obtainable by the surgeon for visualizing theoperative field and recording the procedure for futureanalysis14 This technology reduces the surgeonrsquos depen-dence on assistants and the associated delays for com-munication and manual adjustments
Bleeding
Certainly one of the most difficult tasks in endolaparo-scopic surgery is controlling bleeding Our model de-monstrated that secure proximal clamping is criticallyimportant in reducing blood loss The use of the 18-mmGSI flexible ports proved invaluable in permitting the useof conventional instruments for secure proximal and dis-tal clamping while maintaining the pneumoperitoneumOn the other hand the use of the endoluminal Fogartyballoon for distal aortic occlusion has certain benefits forcontrol in the relatively low-pressure distal aorta In theabsence of a second clamp more working space is avail-able for the surgeonrsquos instruments In case of excessivelumbar bleeding the balloon may be advanced and posi-tioned to help tamponade the site
Much of the bleeding encountered involved the lumbarvessels which in the pig are very delicate and subjectto tearing during aortic dissection Although this increas-es the surgical challenge only 6 of 24 animals (25) hadintraoperative bleeding problems and only 2 of these(8) required conversion to a minilaparotomy Westrongly advocate that the endoscopic surgeon always beready to make an abrupt conversion to open surgery forbleeding control
Spinal Cord Ischemia
Aortic clamping for graft anastomosis can produce hindlimb dysfunction if prolonged Excessive clamp time inturn is often a function of bleeding problems that mayobscure the surgical field and required additional sutur-ing time In other endolaparoscopic survival studiesBryne et al6 observed paraplegia in 3 of 8 dogs andAurdra et al7 recorded 1 case of paraplegia out of the 9pigs that survived the procedure Both studies had clamptimes in excess of 100 minutes for some cases The sin-gle case of hind limb sensory dysfunction in our studyresulted from a technical error that significantly delayedthe anastomosis All other surviving animals had good
ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study
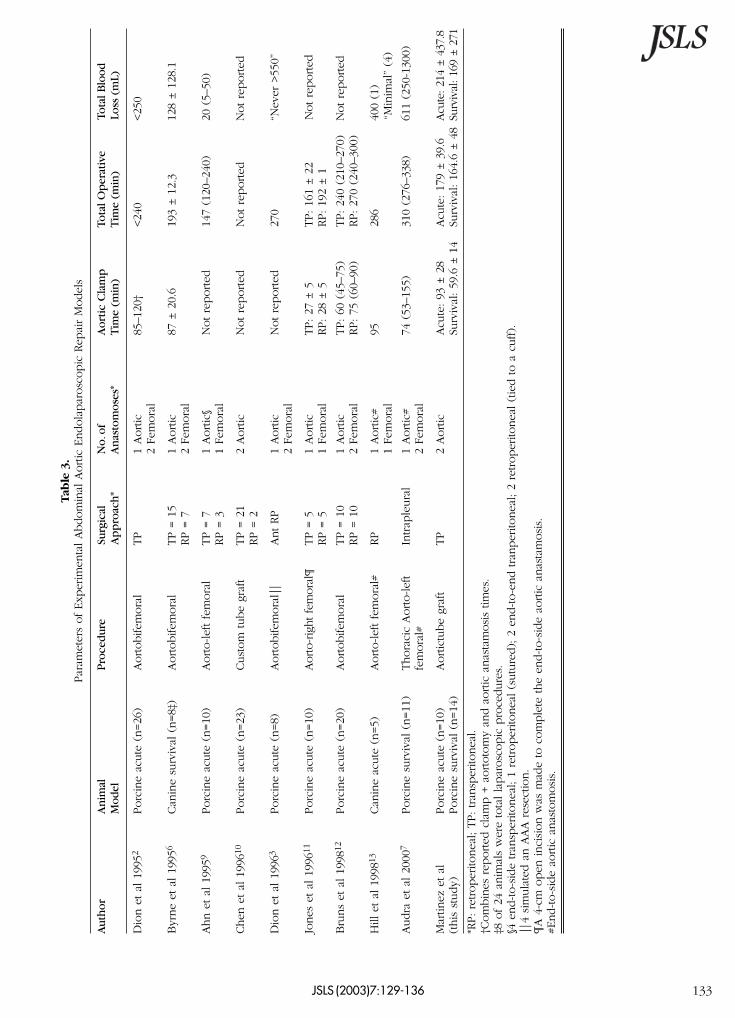
JSLS (2003)7129-136 133
Tab
le 3
Par
amet
ers
of Exp
erim
enta
l Abdom
inal
Aortic
Endola
par
osc
opic
Rep
air
Model
s
Au
thor
An
imal
Pro
cedu
reSu
rgic
alN
oof
A
orti
c C
lam
pTo
tal O
per
ativ
eTo
tal B
lood
Mod
elA
pp
roac
h
An
asto
mos
es
Tim
e (m
in)
Tim
e (m
in)
Loss
(m
L)
Dio
n e
t al
199
52Porc
ine
acute
(n=26
)Aortobife
mora
lTP
1 Aortic
85ndash1
20dagger
lt24
0lt25
02
Fem
ora
l
Byr
ne
et a
l 19
956
Can
ine
surv
ival
(n=8Dagger
)Aortobife
mora
lTP =
15
1 Aortic
87 plusmn
206
19
3 plusmn
123
128
plusmn12
81
RP =
72
Fem
ora
l
Ahn e
t al
199
59Porc
ine
acute
(n=10
)Aorto-lef
t fe
mora
lTP =
71
Aortic
sectN
ot re
ported
147
(120
ndash240
)20
(5ndash
50)
RP =
31
Fem
ora
l
Chen
et al
199
610
Porc
ine
acute
(n=23
)Cust
om
tube
graf
tTP =
21
2 Aortic
Not re
ported
Not re
ported
Not re
ported
RP =
2
Dio
n e
t al
199
63Porc
ine
acute
(n=8)
Aortobife
mora
l||
Ant RP
1 Aortic
Not re
ported
270
ldquoNev
er gt
550rdquo
2
Fem
ora
l
Jones
et al
199
611
Porc
ine
acute
(n=10
)Aor
to-rig
ht fem
oral
paraTP =
51
Aortic
TP 27
plusmn5
TP 16
1 plusmn
22N
ot re
ported
RP =
51
Fem
ora
lRP 28
plusmn5
RP 19
2 plusmn
1
Bru
ns
et a
l 19
9812
Porc
ine
acute
(n=20
)Aortobife
mora
lTP =
10
1 Aortic
TP 60
(45
ndash75)
TP 24
0 (2
10ndash2
70)
Not re
ported
RP =
10
2 Fe
mora
lRP 75
(60
ndash90)
RP 27
0 (2
40ndash3
00)
Hill
et al
199
813
Can
ine
acute
(n=5)
Aorto-lef
t fe
mora
lRP
1 Aortic
95
286
400
(1)
1 Fe
mora
lldquoM
inim
alrdquo
(4)
Audra
et al
200
07Porc
ine
surv
ival
(n=11
)Thora
cic
Aorto-lef
t In
trap
leura
l1
Aortic
74
(53
ndash155
)31
0 (2
76ndash3
38)
611
(250
-130
0)fe
mora
l2
Fem
ora
l
Mar
tinez
et al
Porc
ine
acute
(n=10
)Aortic
tube
graf
tTP
2 Aortic
Acu
te 93
plusmn28
Acu
te 17
9 plusmn
396
Acu
te 21
4 plusmn
437
8(this s
tudy)
Porc
ine
surv
ival
(n=14
)Su
rviv
al 59
6 plusmn
14Su
rviv
al 16
46
plusmn48
Su
rviv
al 16
9 plusmn
271
RP re
troper
itonea
l TP tran
sper
itonea
ldaggerC
om
bin
es r
eported
cla
mp +
aortoto
my
and a
ortic
anas
tam
osi
s tim
es
Dagger8 o
f 24
anim
als
wer
e to
tal la
par
osc
opic
pro
cedure
ssect4
end-to-s
ide
tran
sper
itonea
l 1
retroper
itonea
l (s
utu
red) 2
end-to-e
nd tra
nper
itonea
l 2
retroper
itonea
l (tie
d to a
cuff)
||4
sim
ula
ted a
n A
AA r
esec
tion
paraA 4
-cm
open
inci
sion w
as m
ade
to c
om
ple
te the
end-to-s
ide
aortic
anas
tam
osi
sE
nd-to-s
ide
aortic
anas
tom
osis
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
134 JSLS (2003)7129-136
in the retroperitoneal space and about 200 mL of freeserosanguinous intraperitoneal fluid The nine 7-day sur-vivors were evaluated postoperatively and scored forbehavioral criteria Animals required very little pain med-ication during the first 24 hours No wound complicationsoccurred The 12 survivors with normal hind limb func-tion became ambulatory between 3 and 20 hours post-operatively
DISCUSSION
Procedure
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imagi-nation of the surgeon coupled with the progressive devel-opment of endolaparoscopic instrumentation Theseincluded the possibilities of coronary bypass by endoscopeas had been performed in a porcine model8 Although wedemonstrated the feasibility of full endoscopic repair of theabdominal aorta with a tube graft one of our main goalswas the documentation of performance improvement ofthe surgical team as reflected by a reduction in surgicaltime parameters and bleeding as the study progressed Acomparison of the 10 early procedures with the 14 latersurgeries indicates a modest reduction in total operativetime and estimated blood loss that was not statistically sig-nificant More importantly a dramatic and highly signifi-cant reduction occurred in the aortic cross-clamp time forgraft anastomosis a parameter we deem most vital to sur-gical outcome and postoperative morbidity Althoughother animal models for endolaporoscopic aortic repairhave utilized a variety of protocols grafts and instrumen-tation (Table 3)23679-13 we observe that our aortic clamptimes and total operative times are less than or equal tothose of other studies to date even though they includetwo demanding intraabdominal anastomoses performedwith full endolaparoscopic technique with Endoknottying Of course rapid evolution of endoscopic tech-niques and instrumentation has occurred since the earli-est animal models were developed Most investigatorshave reported an observable reduction in surgical timeparameters that comes through training and experiencealthough the learning curve for this procedure may besteep3671013
Difficulties in retracting the small bowel have led some inves-tigators to prefer a retroperitoneal approach2312 al-thoughone study preferred the transperitoneal approach10 and twoothers found both approaches equally acceptable911
Robotics
The use of the voice-operated computerized roboticAESOP and Hermes systems greatly improved the levelof precision obtainable by the surgeon for visualizing theoperative field and recording the procedure for futureanalysis14 This technology reduces the surgeonrsquos depen-dence on assistants and the associated delays for com-munication and manual adjustments
Bleeding
Certainly one of the most difficult tasks in endolaparo-scopic surgery is controlling bleeding Our model de-monstrated that secure proximal clamping is criticallyimportant in reducing blood loss The use of the 18-mmGSI flexible ports proved invaluable in permitting the useof conventional instruments for secure proximal and dis-tal clamping while maintaining the pneumoperitoneumOn the other hand the use of the endoluminal Fogartyballoon for distal aortic occlusion has certain benefits forcontrol in the relatively low-pressure distal aorta In theabsence of a second clamp more working space is avail-able for the surgeonrsquos instruments In case of excessivelumbar bleeding the balloon may be advanced and posi-tioned to help tamponade the site
Much of the bleeding encountered involved the lumbarvessels which in the pig are very delicate and subjectto tearing during aortic dissection Although this increas-es the surgical challenge only 6 of 24 animals (25) hadintraoperative bleeding problems and only 2 of these(8) required conversion to a minilaparotomy Westrongly advocate that the endoscopic surgeon always beready to make an abrupt conversion to open surgery forbleeding control
Spinal Cord Ischemia
Aortic clamping for graft anastomosis can produce hindlimb dysfunction if prolonged Excessive clamp time inturn is often a function of bleeding problems that mayobscure the surgical field and required additional sutur-ing time In other endolaparoscopic survival studiesBryne et al6 observed paraplegia in 3 of 8 dogs andAurdra et al7 recorded 1 case of paraplegia out of the 9pigs that survived the procedure Both studies had clamptimes in excess of 100 minutes for some cases The sin-gle case of hind limb sensory dysfunction in our studyresulted from a technical error that significantly delayedthe anastomosis All other surviving animals had good
ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study

A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
134 JSLS (2003)7129-136
in the retroperitoneal space and about 200 mL of freeserosanguinous intraperitoneal fluid The nine 7-day sur-vivors were evaluated postoperatively and scored forbehavioral criteria Animals required very little pain med-ication during the first 24 hours No wound complicationsoccurred The 12 survivors with normal hind limb func-tion became ambulatory between 3 and 20 hours post-operatively
DISCUSSION
Procedure
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imagi-nation of the surgeon coupled with the progressive devel-opment of endolaparoscopic instrumentation Theseincluded the possibilities of coronary bypass by endoscopeas had been performed in a porcine model8 Although wedemonstrated the feasibility of full endoscopic repair of theabdominal aorta with a tube graft one of our main goalswas the documentation of performance improvement ofthe surgical team as reflected by a reduction in surgicaltime parameters and bleeding as the study progressed Acomparison of the 10 early procedures with the 14 latersurgeries indicates a modest reduction in total operativetime and estimated blood loss that was not statistically sig-nificant More importantly a dramatic and highly signifi-cant reduction occurred in the aortic cross-clamp time forgraft anastomosis a parameter we deem most vital to sur-gical outcome and postoperative morbidity Althoughother animal models for endolaporoscopic aortic repairhave utilized a variety of protocols grafts and instrumen-tation (Table 3)23679-13 we observe that our aortic clamptimes and total operative times are less than or equal tothose of other studies to date even though they includetwo demanding intraabdominal anastomoses performedwith full endolaparoscopic technique with Endoknottying Of course rapid evolution of endoscopic tech-niques and instrumentation has occurred since the earli-est animal models were developed Most investigatorshave reported an observable reduction in surgical timeparameters that comes through training and experiencealthough the learning curve for this procedure may besteep3671013
Difficulties in retracting the small bowel have led some inves-tigators to prefer a retroperitoneal approach2312 al-thoughone study preferred the transperitoneal approach10 and twoothers found both approaches equally acceptable911
Robotics
The use of the voice-operated computerized roboticAESOP and Hermes systems greatly improved the levelof precision obtainable by the surgeon for visualizing theoperative field and recording the procedure for futureanalysis14 This technology reduces the surgeonrsquos depen-dence on assistants and the associated delays for com-munication and manual adjustments
Bleeding
Certainly one of the most difficult tasks in endolaparo-scopic surgery is controlling bleeding Our model de-monstrated that secure proximal clamping is criticallyimportant in reducing blood loss The use of the 18-mmGSI flexible ports proved invaluable in permitting the useof conventional instruments for secure proximal and dis-tal clamping while maintaining the pneumoperitoneumOn the other hand the use of the endoluminal Fogartyballoon for distal aortic occlusion has certain benefits forcontrol in the relatively low-pressure distal aorta In theabsence of a second clamp more working space is avail-able for the surgeonrsquos instruments In case of excessivelumbar bleeding the balloon may be advanced and posi-tioned to help tamponade the site
Much of the bleeding encountered involved the lumbarvessels which in the pig are very delicate and subjectto tearing during aortic dissection Although this increas-es the surgical challenge only 6 of 24 animals (25) hadintraoperative bleeding problems and only 2 of these(8) required conversion to a minilaparotomy Westrongly advocate that the endoscopic surgeon always beready to make an abrupt conversion to open surgery forbleeding control
Spinal Cord Ischemia
Aortic clamping for graft anastomosis can produce hindlimb dysfunction if prolonged Excessive clamp time inturn is often a function of bleeding problems that mayobscure the surgical field and required additional sutur-ing time In other endolaparoscopic survival studiesBryne et al6 observed paraplegia in 3 of 8 dogs andAurdra et al7 recorded 1 case of paraplegia out of the 9pigs that survived the procedure Both studies had clamptimes in excess of 100 minutes for some cases The sin-gle case of hind limb sensory dysfunction in our studyresulted from a technical error that significantly delayedthe anastomosis All other surviving animals had good
ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study

ambulation in one case within only 3 hours after sur-gery after clamp times of less than 90 minutes We alsofeel that by taking extra care to minimize aortic dissec-tion and preserve the lumbar vessels we were able tomaintain a better blood supply to the spinal cord
Training
Other studies have not emphasized the importance oftraining although the majority of investigators havetaken aortic clamp time and total operative time asbenchmarks for performance The majority of investiga-tors observed a reduction in surgical time as the studiesprogressed3671013 Aortic clamp time measures the per-formance of the entire surgical team particularly the skillof the surgeon and assistant in completing the anasto-moses The integration of the team with the instrumenta-tion and equipment is critical in minimizing this timewhile preserving the quality of the anastomoses In ourmodel the surgeon was committed to a rigorous trainingprotocol as indicated in Table 1 The most importantaspect of technical proficiency is the brain-eye-handcoordination that must be developed in the motor sen-sory cortical and subcortical portions of our brain Thesimulation in vitro of the type of anastomosis used wasvery important in this skill development process
Finally voice training in the integration of voice-activat-ed AESOP and Hermes robotics ie using your voicerather than your hands to direct an instrument or devicemade a critical improvement in clamp time as shown inTable 2 Voice training is a new experience for the sur-geon and requires an integration of the visual and themotor speech areas of the occipital and parietal lobesnever before required by the surgeon in the learning andmemory process
CONCLUSION
Nezhat et al8 aptly characterized the frontiers of laparo-scopic surgery in 1992 as being limited only by the imag-ination of the surgeon coupled with the progressivedevelopment of endolaparoscopic instrumentation Totalendolaparoscopic abdominal aortic replacement with atransperitoneal approach through a pneumoperitoneumis technically feasible and can be completed within atime frame as good as or better than that of retroperi-toneal approaches and alternative graft options in otheranimal models reported in the published literature todate Although the surgical time may be greater than that
JSLS (2003)7129-136 135
for open procedures postoperative outcome was of avery good quality in our survival animals Requirementfor pain medication was minimal Full control of hindlimbs and ambulation was obtained as early as 3 hourspostoperatively
A disciplined and intensive training regimen is essentialfor achieving the necessary skill set for this challengingprocedure but we believe it will become a regularoption to reduce postoperative pain morbidity and hos-pital stay in select patients We strongly advocate a com-prehensive formal training program combining dry andlive surgical laboratory models for surgeons to acquiremotor-sensory skills and anatomical familiarity beforeattempting clinical application
References
1 Dion YM Katkhouda N Roleau C Aucom A Laparoscopy-assisted aortobifemoral bypass Surg Laparosc Endosc 19933425-429
2 Dion YM Chin AK Thompson TA Experimental laparo-scopic aortobifemoral bypass Surg Endosc 19959894-897
3 Dion YM Gracia CR Experimental laparoscopic aorticaneurysm resection and aortobifemoral bypass Surg LaparoscEndosc 19966184-190
4 Dion YM Gracia CR A new technique for laparoscopic aor-tobifemoral grafting in occlusive aortoiliac disease J Vasc Surg199726685-692
5 Dion YM Gracia CR Estakhri M Demalsy JC Douville YPiccinini E Stancanelli V Totally laparoscopic aortobifemoralbypass a review of 10 patients Surg Laporosc Endosc19988165-170
6 Byrne J Hallett JW Kollmorgen CF Gayari MM Davies WTotally laparoscopic aortobifemoral bypass grafting in an exper-imental model description of technique with initial surgicalresults Ann Vasc Surg 199610156-165
7 Audra AN Gloviczki P Young MM Karnicki K DeschampsC Moir C Videoendoscopic thoracic aorta-to-femoral arterybypass in the pig J Surg Res 20009370-74
8 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) state of the art J Gyn Surg 19928111-139
9 Ahn SS Clem FF Braithwaite MA Concepcion B Petrik PVMoore WS Laparoscopic aortofemoral bypass initial experiencein an animal model Ann Surg 1995222677-683
10 Chen MH Murphy EA Levison J Cohen JR Laparoscopicaortic replacement in the porcine model a feasibility study inpreparation for laparoscopically assisted abdominal aortic
A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study

A Porcine Model for Endolaparoscopic Abdominal Aortic Repair and Endoscopic Training Martinez BD et al
136 JSLS (2003)7129-136
aneurysm repair in humans J Am Coll Surg 1996183126-132
11 Jones DB Thompson RW Soper NJ Olin JM Rubin BGDevelopment and comparison of transperitoneal and retroperi-toneal approaches to laparoscopic-assisted aortofemoral bypassin a porcine model J Vasc Surg 199623466-471
12 Bruns CJ Wolfgarte B Kasper M Zenner D Walter MManich B Gasless videoendoscopic implantation of aortob-ifemoral vascular prothesis via transperitoneal versus extraperi-toneal approach in an animal model Surg Endosc 199812137-141
13 Hill AB MacKenzie KS Steinmetz OK Fried GMVideoendoscopic thoracic aorta-to-femoral artery bypass J VascSurg 199827948-954
14 Kavic MS Robotics technology and the future of surgeryJSLS 20004277-279
Acknowledgments Partial financial support for this study hasbeen provided by the following companies Fogarty ResearchEthicon Endo-Surgery Computer Motion IMPRA Inc StrykerEndoscopy and TycoUSSI We would also like to thank ourscrub nurses Elisa Marles RN and Carol Worden RN StanfordHealth Services Stanford CA USA for their invaluable assistanceduring the study
Disclosure Thomas J Fogarty MD and George D HermannBSME are affiliated with Fogarty Research which developedseveral instruments used in this study Yamil Saenz DVM ispresently employed by Ethicon Endo-Surgery which producesmany of the instruments used in the study