changing behaviours & the human factors approach jenny ingram head of service improvement nhs...
TRANSCRIPT

Changing Behaviours & The Human Factors Approach
Jenny IngramHead of Service Improvement
NHS Grampian

Appreciation of a System• Complex system of interaction between people, procedures and
equipment• Success depends on integration, not performance of individual
parts
Understanding Variation• Variation is to be expected – everything we measure
varies• We make decisions based on interpretation• Data over time – data story of what has been happening
Theory of Knowledge
• Change is prediction of improvement
based on knowledge of the system• Learning from theory,
experience• Operational definitions are the
basis for improvement with PDSA cycles for learning
Psychology• Interaction of people with
systems• Motivation & will of individuals &
teams• Situation awareness/decision
making• Managing stress and fatigue• Helps planning for change
management
Improvement
Aims
&
Values
✔
✔
✔

Human Factors
• Critical incident studies reveal that around 80% of underlying issues relate to human factors.
• Systems should be designed with ‘defenses in depth’
Organisational, management, equipment design, workspace layout
Should provide the human in the systems with the necessary knowledge and skills to deal with threats in their environment to act as hero
Technical skills are not enough!
(Reason 1997))

Human Factors Approach
Focus on behaviours that contribute to safe & effective performance
• Situation Awareness• “mindfulness”• Detection and recognition of threats• “Chronic Unease” / Attention to weak signals
• Decision Making• Balancing competing pressures• Ability to make “sacrificial decisions”
• Communication• Handover• Between Professions• Organisationally

Human Factors Approach
• Teamwork• Recognise the contribution of individuals to the success of the team.• Work to peoples strengths as well as supporting developments.
• Leadership• Required at all levels but needs organisational direction if it is to make
a difference.
• Managing Stress• High stress is recognised but low levels of ongoing stress are equally
important.
• Managing Fatigue• Prolonged work has shown the same deterioration in performance as making it illegal to drive.

Lessons from other industries
• Human factors & safety integrated to the core curriculum• Compulsory incident reporting, investigation and learning • Briefing and debriefing part of the culture• Expect things to go wrong and plan for it
• 15/01/2009• Flight 1549• Routine flight from New York to
Charlottesville• Landed safely in the Hudson River• All passengers and crew alive & well• Lessons shared across the world

Relevance To Healthcare?

COMPONENTS OFNON-TECHNICAL
SKILLS
Situation Awareness
Decision Making
Communication
Teamwork
Leadership
Managing Stress
Coping with Fatigue
RELEVANCE TO HEALTHCARE
A study by McCulloch et al (2007) showed that implementing non-technical skills training in the operating theatre improved the situational awareness of the team and led to improved outcomes of 30-50% less technical errors.
A study by Wilson (1999) showed that 27% of claims within a healthcare organisation resulted from diagnostic and cognitive decision making errors.
A study by Gawande, Zinner, Studdert & Brennan (2003) showed that 43% of adverse events in surgery were due to communication breakdowns.Joint Commission root cause analysis of over 4,000 adverse events identified communication breakdown as the most common factor (2008).Lingard, Espin & Whyte (2004) classified 25% of communication failures as they were made too early or too late.
Haig, Sutton and Whittington (2006) concluded that in order to improve patient safety a shared mental model between medical and nursing staff with a focus on the patient’s condition needs to exist.Risser, Rice & Salisbury (1999) identified key team behaviours needed to prevent medical error following review of adverse event cases.
Flin & Yule (2004) found that supervisors who communicate effectively with employees about safety gain a greater commitment to improvement.McKee et al (2010) state that NHS organisations who are high performers in terms of patient safety are able to assess and prioritise the internal processes and structure changes needed to balance the external threats and pressures.Changing practice in patient safety requires a change in organisational culture and attitudes and this requires commitment from the Board Leadership. (Carthey & Clarke, 2009).
28% of EU employees have suffered from stress-related illness and it is the second most common work-related problem in UK (HSE, 2007).40% Consultant Surgeons were ‘burned out’ and 30% depressed (Shanafelt et al., 2010).
Junior Doctors attributed most serious error to fatigue (Volpp & Grande, 2003).61% Anaesthetists acknowledged an error related to fatigue (Weinger, & Ancoli-Israel, 2002).




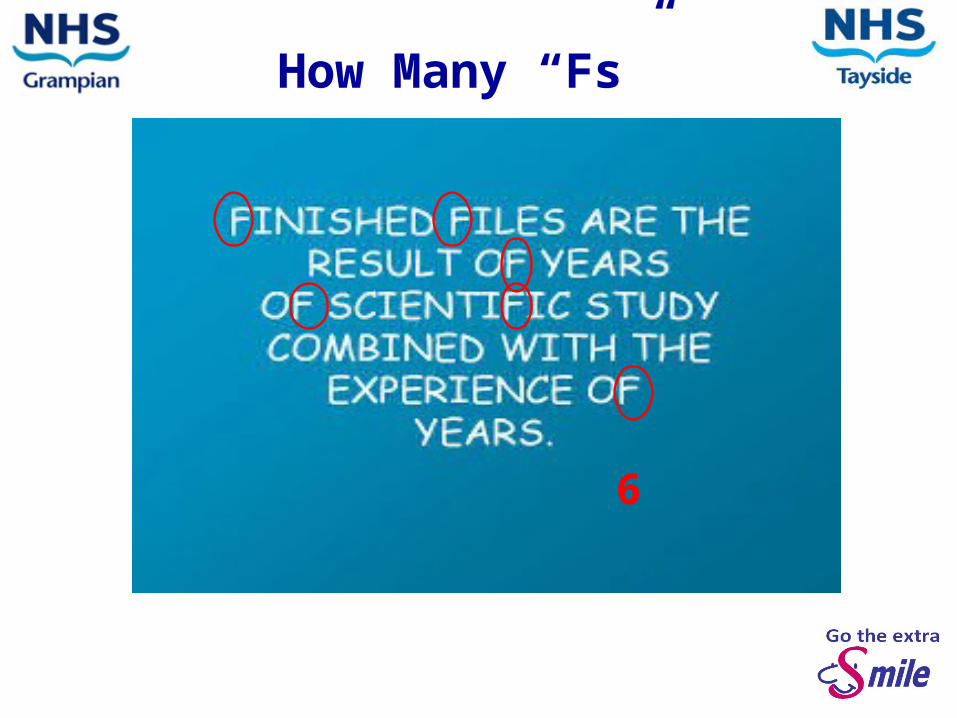
How Many “Fs”
6

Human FactorsA common language
“Not only knowing but doing.” (HF SLWG 2012)
“Making it easy to do the right thing.”
“Enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organisation on human behaviour and abilities and application of that knowledge in clinical settings.”
(Bromiley 2010)
(Catchpole 2010)
OrganisationalManagement
- Safety Culture- Managers’ Leadership- Organisation communication
Work - Environment- Hazards- Ergonomics
Work Group- Teamwork- Structures & processes- Team Leadership- Communication
Individual- Cognitive skills- Situation awareness- Decision making- Personal resources- Management of stress- Management of fatigue
(Flin & Patey 2011)

Can We Assess Non-Technical Skills?


Are You Convinced That You Need To Consider Human Factors?....
Let Me Try More!!!!
• I am taking you to a strange planet with a very strange atmosphere.
• In this atmosphere they cannot speak, as sound does not travel.
• The planet also has a very weird gravity system. Only four people can stand up at once. It is also impossible to stand for more than ten seconds.
• The challenge for survival on this planet is for the group to keep four
people standing up all of the time, for not more than ten seconds each.
Solutions
• Use human factors to plan work and minimise “surprises”
• Avoid reliance on memory
• Make things more visible
• Review and simplify processes
• Standardise common processes and procedures
• Routinely use checklists
• Decrease reliance on vigilance
www.lmq.co.uk

So What’s In It For You And Your Patients?
• Reduced hospitalisation and costs• Increased effectiveness and innovation• Increased well-being of team members• Multi-disciplinary teams deliver high quality patient care
and implement more innovations• Lower patient mortality• Reduced error rates• Reduced turnover• Lower and sickness absence• Increased organisational commitment and engagement
Lyubovnikova, J., & West, M.A. (2013)

Berwick, D.M. (2008). The Science of Improvement. JAMMA. Vol. 299, 10: 1182-1184
In Summary
“ Where is the randomised trial?” is, for many purposes, theright question for many others it is the wrong question, a myopic
one. A better one is broader: “What is everyone learning?” Asking the question in that way will help clinicians and
researchers in navigating towards improvement. Berwick (2008)
Berwick, D.M. (2008). The Science of Improvement. JAMMA. Vol. 299, 10: 1182-1184

And Finally………..