cefalea y embarazo
TRANSCRIPT

ACTUALIZACION TERAPEUTICA DE
CEFALEA EN LA EMBARAZADA
Interna Romina Verdugo
Interno Eduardo Neira
Internado neurología HFBC

INTRODUCCIÓN
• Más del 90% tienen un dolor de cabeza pre-existente
• menos del 10% desarrollan dolor de cabeza de nueva aparición
• La migraña mejora en 2 de cada 3 embarazadas, en el 30% se mantiene y 5% empeora.
(1)Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and Cheryl Bushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445(2)Migraña y gestación: una relación compleja, Hospital Universitario Marqués España, Rev Neurol 2010

FR migraña durante embarazo
• IMC pregestacional > 25
• < 5 hrs sueño por la noche
• Desempleo
• Depresión
• Asma
• HTA
• Suspensión ISRS
Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and CherylBushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445

CEFALEAS PRIMARIAS
• migraña y cefalea tensional
• Generalmente durante el 1° semestre
• mejora durante las últimas etapas del embarazo (aprox 50-80% migraña y 30% tensional)
Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and CherylBushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445

CEFALEAS SECUNDARIAS
• En cualquier momento durante el embarazo, más frecuentemente en el tercer trimestre.
• Causas: ACV, trombosis venosa central, malformaciones arterio venosas, TU cerebral , hipertension intracraneal benigna
Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and CherylBushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445

MANEJO NO FARMACOLÓGICO
• Dieta:▫ Evitar la hipoglicemia▫ Reconocer comidas que puedan desencadenar
cefalea▫ Adecuada hidratación
• Sueño adecuado (> 6 hrs)• Evitar situaciones estresantes• Ejercicio aeróbico moderado• No fumar• Acupuntura
1. Non-pharmacological management of migraine during pregnancy Gisella Airola Neurol Sci (2010) 31 (Suppl 1):S63–S652. Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and Cheryl Bushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445

MEDIDAS FARMACOLÓGICAS
• Manejar:
▫ cuadro agudo y prevención
• Evaluar su necesidad según:
▫ Frecuencia (>2 veces a la sem)
▫ intensidad de la migraña
▫ duración de los síntomas
▫ síntomas asociados
▫ grado de discapacidad
▫ interferencia con las actividades de la vida diaria.
Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and Cheryl Bushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445

OPCIONES DE TRATAMIENTO
• Métodos para determinar riesgo terapiafarmacológica
• Más utilizado: Sistema evaluación de riesgo de laFDA (1996).
• Otros: Servicio de información teratogénica(TERIS), que clasifica fármacos de acuerdo ariesgo teratogénico y no por escala deriesgo/beneficio
Migraine in Pregnancy Elizabeth Loder, M.D., M.P.H. Neurological Issues in Pregnancy; Guest Editor, Autumn M. Klein, M.D., Ph.D. DOI 10.1055/s-2007-991121. ISSN 0271-8235

FDA
Migraine in Pregnancy Elizabeth Loder, M.D., M.P.H. Neurological Issues in Pregnancy; Guest Editor, Autumn M. Klein, M.D., Ph.D. DOI 10.1055/s-2007-991121. ISSN 0271-8235

TERIS
Migraine in Pregnancy Elizabeth Loder, M.D., M.P.H. Neurological Issues in Pregnancy; Guest Editor, Autumn M. Klein, M.D., Ph.D. DOI 10.1055/s-2007-991121. ISSN 0271-8235

Tratamiento sintomáticos

TRIPTANES
• Clasificación C de acuerdo a FDA.
• Investigación más reciente: no existen casos deteratogenia secundarios a su uso.
• El mas indicado en los estudios es elSumatriptan
• Usado durante el segundo y tercer trimestre hapresentado casos de hemorragia postparto porútero atónico
Migraine in Pregnancy Elizabeth Loder, M.D., M.P.H. Neurological Issues in Pregnancy; Guest Editor, Autumn M. Klein, M.D.,Ph.D. DOI 10.1055/s-2007-991121. ISSN 0271-8235Loder E. Safety of sumatriptan in pregnancy: a review of the data so far. CNS Drugs 2003;17:1–7

ERGOTAMINA
• Contraindicación basada en estudios quedemuestran disminución importante del flujouterino hipoxia fetal y RCIU(1).
• Existen reportes de casos de malformacionesespecificas relacionadas a uso de ergotamina (2)
(1)Acs N, Banhidy F, Puho E, Czeizel AE. A possible dosedependent teratogenic effect of ergotamine. Reprod Toxicol 2006;22:551–552(2) Raymond GV. Teratogen update: ergot and ergotamine. Teratology 1995;51:344–347

AINEs
• En general, se evita uso en embarazo,particularmente durante 3er trimestre (cierreprecoz ducto arterioso)
• FDA: C en el 1° y 2° trimestre y la categoría D en el tercer trimestre
• Paracetamol (clase A) eficacia es <10% en migraña
• Fármacos que se deben evitar: Inhibidores desíntesis de PGs (AAS, Indometacina)
- AAS en bajas dosis y ocasionalmente puede serusada.
• AINEs menos potentes: Ibuprofeno, se puedeadministrar con seguridad en primer trimestre.
(2)Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and Cheryl Bushnellb, Current Opinion in Obstetrics and Gynecology USA 2010, 22:437–445
(1) Migraña y gestación: una relación compleja, Hospital Universitario Marqués España, Rev Neurol 2010
BARBITÚRICOS Y BENZODIAZEPINAS
• Limitación a su uso mejor avalada.
• Frecuentemente asociadas a abuso.
• BZD: Sd. Abstinencia neonatal
• Barbitúricos: Efectos en desarrollo neurológico.
Reinisch JM, Sanders SA, Mortensen EL, Rubin DB. In utero exposure to phenobarbital and intelligence deficits in adult men.JAMA 1995;274:1518–1525Holmes LB, Coull BA, Dorfman J, Rosenberger PB. The correlation of deficits in IQ with midface and digit hypoplasia inchildren exposed in utero to anticonvulsant drugs. J Pediatr 2005;146:118–122

OTROS
• Productos naturales poco estudiados.
• Hierba de Santa María: posible teratogenia(1)
• Metoclopramida, domperidona, proclorperacina,clorpromacina: Exposición sin asociación riesgosignificativo de malformaciones congénitasmayores (2)
• Náuseas tratadas con Vit B6: sin evidencia deteratogenia.
- Terapia combinada más efectiva.
(1) Yao M, Ritchie HE, Brown-Woodman PD. A reproductive screening test of feverfew: is a full reproductive studywarranted? Reprod Toxicol 2006;22:688–693.(2) Ilan Matok, M.Sc.Pharm., Rafael Gorodischer, M.D., Gideon Koren, M.D., Eyal Sheiner, M.D., Ph.D., Arnon Wiznitzer,M.D., and Amalia Levy, M.P.H., Ph.D. The Safety of Metoclopramide Use in the First Trimester of Pregnancy . N Engl J Med2009; 360

OTROS
• Opiaceos: categoria C, eficacia limitada, riesgode dependencia materna y fetal
• Corticoides: en ocasiones son útiles para losataques prolongados de migraña.
- Prednisona v/s Dexametasona porque la últimaatraviesa placenta más fácilmente.
- Evidencia: 1er trimestre, no hay riesgo teratogénicoimportante.
(1)Gur C, Diav-Citrin O, Shechtman S, Arnon J, Ornoy A. Pregnancy outcome after first trimester exposure to corticosteroids: a prospective controlled study. Reprod Toxicol 2004;18:93–101(2)Leung TN, Lam PM, Ng PC, Lau TK. Repeated courses of antenatal corticosteroids: is it justified? Acta Obstet Gynecol Scand2003;82:589–596(3)Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and Cheryl Bushnellb, CurrentOpinion in Obstetrics and Gynecology USA 2010, 22:437–445
TRATAMIENTO PREVENTIVO
• Beta-bloqueadores (Propanolol*, timolol)preferido como terapia preventiva de la cefaleaen embarazadas.
• FDA: Clase C
• Se han reportado eventos adversos,principalmente retardo del crecimientointrauterino
Buchanan TM, Ramadan NM. Prophylactic pharmacotherapy for migraine headaches. Semin Neurol 2006;26:188–198Pfaffenrath V, Rehm M. Migraine in pregnancy: what are the safest treatment options? Drug Saf 1998;19:383–388

TRATAMIENTO PREVENTIVO
• Antiepilepticos:
▫ Topiramato (clase C) DE 2° LINEA, Evitar en 1°tri.
▫ Ac. Valproico (clase D) NO RECOMENDADO
▫ Menor riesgo en monoterapia y bajas dosis
• Antidepresivos
▫ De 2° linea, amitriptilina y fluoxetina solo recomendado en el 2° trimestre, clase C
▫ Riesgo de HT pulmonar primaria en el RN
Contemporary management of migrainous disorders in pregnancy Stephen A. Contaga and Cheryl Bushnellb, CurrentOpinion in Obstetrics and Gynecology USA 2010, 22:437–445

FCOS DURANTE EL EMBARAZO
Medication Use in the Treatment of Migraine During Pregnancy and Lactation Current Pain & Headache Reports 2009, 13:392–398 Current Medicine Group LLC ISSN 1531-3433

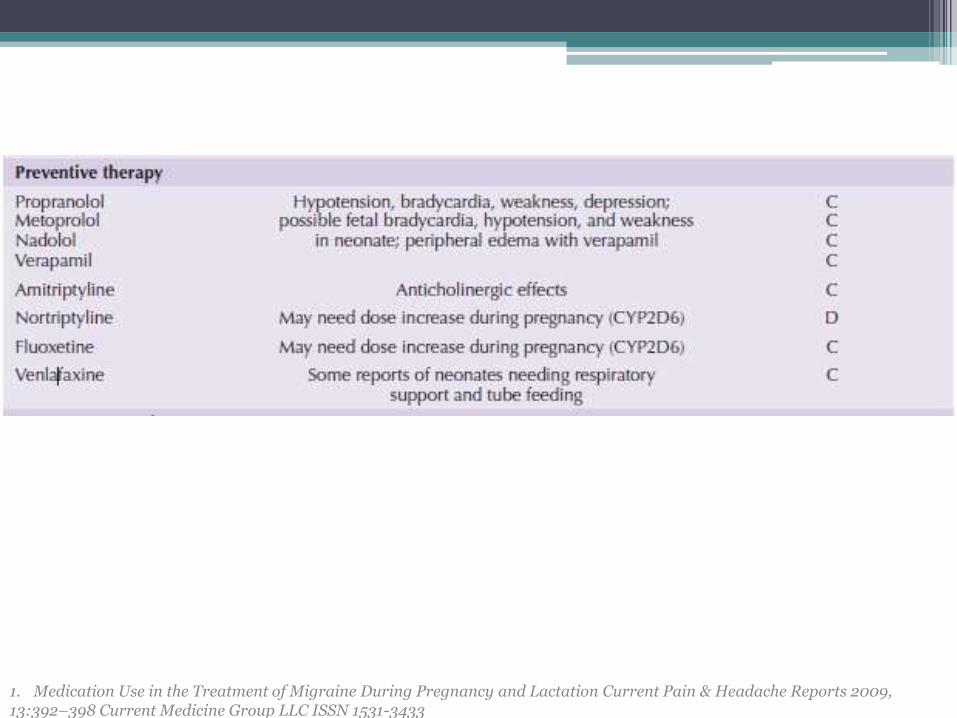
FCOS DURANTE EL EMBARAZO
1. Medication Use in the Treatment of Migraine During Pregnancy and Lactation Current Pain & Headache Reports 2009, 13:392–398 Current Medicine Group LLC ISSN 1531-3433
FCOS DURANTE EL EMBARAZO
1. Medication Use in the Treatment of Migraine During Pregnancy and Lactation Current Pain & Headache Reports 2009, 13:392–398 Current Medicine Group LLC ISSN 1531-3433

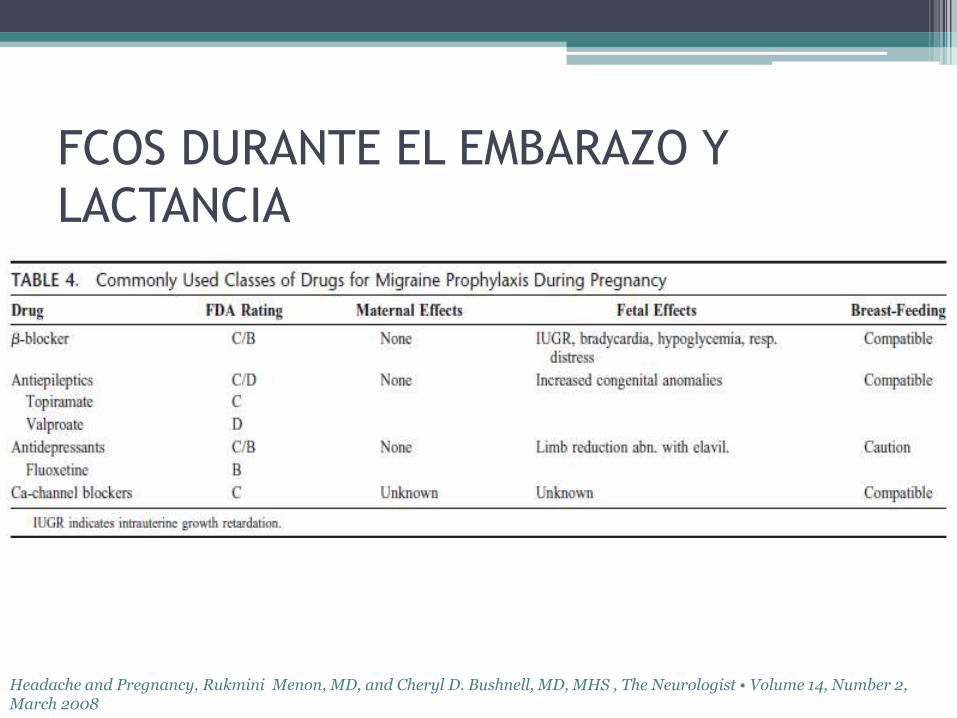
FCOS DURANTE EL EMBARAZO Y
LACTANCIA
Headache and Pregnancy, Rukmini Menon, MD, and Cheryl D. Bushnell, MD, MHS , The Neurologist • Volume 14, Number 2, March 2008
FCOS DURANTE EL EMBARAZO Y
LACTANCIA
Headache and Pregnancy, Rukmini Menon, MD, and Cheryl D. Bushnell, MD, MHS , The Neurologist • Volume 14, Number 2, March 2008

CEFALEA POST PARTO
• PRIMARIA: migraña y tensional• SECUNDARIA: Cefalea post punción dural,
trombosis de seno venoso, ACV
• incidencia global es difícil de determinar (cefalea leves no se reportan)
• 39% reportaron cefalea en la 1° semana post parto, la mayoría es tensional, 4,7% post puncion, 8,1% causa indeterminada(Canada, cohortes)
• 34% migrañas recurrentes en la primera semana posparto y el 55% en el primer mes(Estudio prospectivo italiano)
Postpartum headache, A.M. Klein, E. Loder, Department of Neurology, Harvard Medical School, Boston, MA, USA, 2010

BANDERAS ROJAS
Postpartum headache, A.M. Klein, E. Loder, Department of Neurology, Harvard Medical School, Boston, MA, USA, 2010

DIAG. DIFERENCIAL
Postpartum headache, A.M. Klein, E. Loder, Department of Neurology, Harvard Medical School, Boston, MA, USA, 2010
