ce session #47 qapi required by cms 2013 session 47-12.pdf · will allow for the testing of...
TRANSCRIPT

FHCA 2012 Annual Conference
Hilton Hotel • Orlando, FL
Thursday, August 2, 2012 - 11:00 am - 12:00 pm
LEARNER OBJECTIVES
CE Session #47
QAPI Required by CMS 2013
Upon completion of this presentation, the learner will be able to:
Explain how the Affordable Care Act and Section 6102 requires CMS to establish Quality Assurance and Performance Improvement standards and provide technical assistance to nursing homes; and Describe the Florida demonstration program’s implementation in four nursing homes through the testing of a QAPI prototype for national implementation in 2014.
PRESENTER(S):
LuMarie Polivka West, MSP, is the Florida Health Care Association Senior Director of Policy, with responsibility for the planning and implementation of long term care related policies, programs, and training seminars. LuMarie is the past Florida Director of Licensure & Certification and Medicaid Program Development Chief, with over 20 years in state government and 18 with FHCA. She has a Master’s of Science Degree from FSU in Urban & Regional Planning, where she has been an adjunct faculty member for the past 28 years in health regulation. Diane Stone, RN, NHA, has been with the Catholic Health Services for 32 years and is currently the Executive Director of St. John’s Nursing Center. Diane began her career in health care as a Certified Nursing Assistant, and worked her way through the spectrum as an RN, an RN Supervisor, a Director of Health Services and as the Executive Director. Brad Graham has been the Executive Director of Oak Manor Senior Living Community in Largo, Florida since 2008. Prior to that, he served as the Nursing Home Administrator and as the Administrative Assistance in the same facility. During Brad’s tenure as Executive Director, Oak Manor was selected one of 17 SNFs nationwide to participate in CMS’s QAPI initiative. As Executive Director he has also endured a CMS backed Zone Program Integrity Contractor or ZPIC audit.

7/5/2012
1
QAPI – Quality Assurance and Performance Improvement
Brad Graham, NHADiane Stone, NHA, RN
LuMarie Polivka‐West, MSPAugust 2, 2012 11 a.m. ‐ noon
QAPI Intent
• Quality Assurance and Performance Improvement is a comprehensive program by which an organization identifies problems or issues early on, develops a plan to address the root causes of problems and prevent adverse events throughout the system, and involves the entire team in using data to understand quality and work to improve performance.
Demonstration Commitment
• Interdisciplinary quality team representing department leadership and administrative leadership and direct care staff
• Involve residents
• Dedicate staff and resources to establish, implement, and evaluate a Quality Assurance Performance Improvement program
• Be willing to share experiences and outcomes with others to promote a community‐wide culture of continuous improvement
7/5/2012
2
5 Elements of QAPI
• Appropriate Design and Scope developed
• Effective Governance and Leadership
• Feedback, Data Systems, and Monitoring systems implemented
• Conducting Performance Improvement Projects (PIPs
• Using Systematic Analysis and Systemic Action
QAPI Timeline
• March 2010: Affordable Care Act, Section 6102, (c) requires nursing homes to have a QAPI with CMS to provide standards and technical assistance.
• September 2010: CMS contracted with Univ. of Minn. and Stratis Health to conduct 2 year demonstration project, including 4 Florida NHs
• 2012: QAPI rule likely from CMS for comment• Late 2013 or early 2014: all nursing homes required to have a QAPI in place with a written plan.
2012 Activities
• QAPI Questionnaire sent June 29 to a representative sample of 4,200 randomly selected nursing homes. The findings will be used to (1) address identified challenges and barriers to implementing effective QAPI programs and (2) shape the direction and content of the QAPI tools and resources.
• Rollout of Prototype Tools on CMS’ QAPI Webpage in late summer. The tools will be posted in links below for easy downloading.
• Resources for Consumers: Resources and training materials that will empower consumers and advocates in their roles in nursing home QAPI.
• Tools and Education for Nursing Home Surveyors: CMS will continue to develop surveyor training materials and worksheets to enhance surveyors’ ability to identify QAPI concerns.
7/5/2012
3
CMS views
• “QAPI is about critical thinking. It involves figuring out what is causing certain problems and implementing interventions and solutions that address the root causes of the problems, rather than just the symptoms.”
‐‐Karen Schoeneman, Former Technical Director, CMS Division of Nursing Homes
…continued
• “Direct care workers and long term care leaders will drive performance improvement and learning through the QAPI process.”
‐‐‐Alice Bonner, Director, Division of Nursing Homes, CMS Survey and Certification Group
QAPI Questions
• Do all staff, residents, families feel free to speak up to identify areas that need improvement?
• How can you promote awareness of performance improvement and create the expectation that everyone in the nursing home must be involved?
• What are the challenges or barriers? What is successful?
• What is a potential project that will get you an early success?

Goals and Aims of the QAPI Demonstration in Nursing Homes The goal of the QAPI Demonstration is to test the feasibility and preliminary effectiveness of the new Quality Assurance and Performance Improvement (QAPI) approach to improving nursing home (NH) quality. A QAPI process is mandated as a new regulation under the Affordable Care Act. Within the year after CMS promulgates regulations, each facility will develop a QAPI plan, and implement a QAPI program that is consistent with the 5 elements of QAPI identified by CMS, namely: 1) Instituting a program with appropriate Design and Scope; 2) Developing effective Governance and Leadership; 3) Instituting Feedback, Data Systems, and Monitoring, which includes:
a. tracking and investigating Adverse Events, and b. monitoring quality using Performance Indicators;
4) Conducting Performance Improvement Projects (PIPs); 5) Using Systematic Analysis and Systemic Action. The Demonstration, which takes place between the first week of September 2011 and August 31, 2013, will allow for the testing of training materials, including QAPI curriculum modules, tools, resources, and best practices (which will also be incorporated in the Resource Library), and estimate their effectiveness. In turn, this allows us to generate improved materials and training processes for the CMS roll‐out of a national NH QAPI program. The implementation of QAPI will be consistent with compliance with all federal regulations at Part 483 F520 QAA. Specific aims for the QAPI Demonstration are: On completion of the Demonstration, participating NHs will have met the minimum expectations for a sustainable QAPI program as articulated under the new policy; On completion of the Demonstration, participating NHs will have gone beyond minimum regulatory compliance to have incorporated a culture of performance improvement and proactive efforts to identify and address a wide range of issues related to quality of care and quality of life in a proactive fashion; On completion of the Demonstration, tested technical assistance materials, training materials, instructional formats, and case examples of best practices will be available to assist CMS and all facilities in the national QAPI rollout.
II. Intervention Over a two year period, facilities in the Demonstration will be assisted to develop a QAPI program that reflects the 5 elements of QAPI articulated by CMS. They will: Develop a written plan for a comprehensive and continuous QAPI program with a design and scope consistent with the services delivered by the NH; Tab 4: Overview of QAPI Demonstration Project, Page 2 Establish a governance and leadership structure that supports QAPI, establishes expectations and a climate that supports safety in health care and resident choice, provides facility‐wide QAPI training, and allocates resources for QAPI activities; Develop a feedback and data system and monitoring for use in evaluating NH quality, including tracking and investigating adverse events, and applying performance indicators to overall quality. Feedback systems will rely on multiple sources of information including perceptions of residents and their families and staff input;

Conduct and respond to results of Performance Improvement Projects (PIPs); Apply a systematic approach to determining whether and how identified problems may be caused or exacerbated by the way care and services are organized or delivered and determining the root cause of these problems, and introducing systemic action when needed to bring about sustained change. The participating NHs will receive technical assistance to achieve these goals and to meet the more specific milestones of progress created for the Demonstration. Both to further assist the facilities but also to maximize lessons from the Demonstration to apply to the National Rollout, the participating NHs will take part in a learning collaborative of 16 NHs. Staff from the participating NHs will interact at four in‐person meetings (rotated among the four locations) and by telephone conference calls to share experiences and provide each other with support. Through the TA, participants will be introduced to practical tools to help them manage the elements of QAPI and particularize plans towards the challenges in their own facilities. Stratis Health, the Quality Improvement Organization (QIO) serving Minnesota, is leading in the creation and management of the learning collaborative.
III. Assumptions and Challenges A QAPI program can bring NHs more in line with other Federally regulated health providers, all of which are expected to conduct a QAPI program adhering to the same 5 elements that will be required of NHs; with reference to health care services delivered, NH QAPI promotes a culture of safety similar to that promoted for hospitals. A QAPI program in NHs will need to be particularized to the special challenges and differences between NHs and other health settings, particularly hospitals. All NH residents should be able to exercise autonomy over life circumstances and live according to their preferences (or those of family or legal agents when the resident lacks decisional capacity). Quality performance in a NH includes processes that individualize services and respect resident choice, and outcomes such as perceived good quality of life. Unlike most health settings, the NH is strictly regulated by an external group of state and federal inspectors. NHs will still need to comply with existing regulatory expectations at Part 483 F520 QAA, while attempting to develop a forward‐looking innovative QAPI program geared to particular challenges of achieving quality in NHs. The Demonstration is undertaken with recognition of the great heterogeneity of NHs, including in scope of programs, human resources available, and IT capability. Such heterogeneity affects the Design and Scope of the QAPI program and the ease with which a NH will be able to mount data‐driven feedback and monitoring systems. Demonstration is designed to maximize learning about practical approaches to developing and sustaining QAPI programs in NHs—this requires close attention to the challenges each participating NH experiences in its own environment with its own particular circumstances of organizational features, state policy, staff characteristics, reimbursement, resident mix, and events that may occur over the two years of implementation in the Demonstration.
IV. Specific Questions to be explored in the NH QAPI Demonstration How successful are NHs in the Demonstration in implementing an acceptable QAPI program? How successful are NHs in the Demonstration in implementing a QAPI program that goes beyond establishing a basic program to develop wide and deep activities relating to multiple areas of quality, involving large numbers of staff, and achieving better outcomes?
What level of effort, resources, and identifiable costs were associated with developing the QAPI program—and how many new resources did participating NHs need to use? What characteristics of technical assistance are helpful for QAPI implementation? What facilitates or impedes the development of a successful QAPI program? What characteristics of NHs predict greater or lesser success in QAPI implementation? Specifically, how do answers to the above questions vary based on NH size, complexity in range of programs, rural versus urban location, ownership status, chain membership, and stability of senior management and frontline staff? What is the relationship between a QAPI program and improved quality?
Do the NHs in the Demonstration achieve their targeted goals?
Do the NHs in the Demonstration achieve quality in non‐targeted areas? (i.e. does positive spin‐off occur and/or is no negative effect found in other areas because of concentration in targeted areas?) What has been learned from the Demonstration that will assist in national roll‐out, including:
Usefulness of tools and resources provided through the Demonstration;
Technical assistance, training, and resources that may be needed for leaders in some NHs;
Ways to engage front‐line staff, residents, and families;
Acceptability of QAPI approaches to stakeholders (provider, professional, and advocate groups) in the areas where the Demonstration takes place.

DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Office of Clinical Standards and Quality/Survey & Certification Group
Ref: S&C: 12-38-NH
DATE: June 29, 2012 TO: State Survey Agency Directors FROM: Director Survey and Certification Group SUBJECT: Quality Assurance and Performance Improvement (QAPI) in Nursing Homes-
Activities Related to QAPI Implementation Since the issuance of S&C Memo 11-22 on April 8, 2011, CMS has continued to engage in several activities related to QAPI implementation in nursing homes. QAPI Tools and Resources CMS, in collaboration with the University of Minnesota and Stratis Health, has been busy identifying and designing effective QAPI tools and resources specifically for nursing homes.
Memorandum Summary Quality Assurance and Performance Improvement (QAPI) Activities: Section 6102(c) of the Affordable Care Act mandates the Centers for Medicare & Medicaid Services (CMS) to establish standards and provide technical assistance to nursing homes on the development of best practices relating to QAPI. The CMS put forth several initiatives to implement these provisions that include: • Refinement of QAPI Tools and Resources: Ongoing development of QAPI tools and
resources that nursing homes may use to design and implement an effective QAPI program.
• Launch of a QAPI Demonstration: Demonstration project in 17 nursing homes in 4 States to test tools and resources and provide technical assistance to nursing homes in QAPI implementation.
• Rollout of QAPI materials: CMS will release materials later this calendar year that will support nursing homes in QAPI implementation.
• Draft of the QAPI Regulation: CMS is in the process of drafting a new QAPI regulation.
• Launch of the Nursing Home Quality Improvement Questionnaire: The CMS has launched a nursing home quality improvement questionnaire using an independent contractor. The data collection period is from June 25 through September 28, 2012.

Page 2 – State Survey Agency Directors A panel of national experts in nursing home quality has been assembled to provide feedback on the tools and resources being developed. Once fully tested and evaluated, these tools and resources will be made available to all nursing homes through a National Rollout. QAPI Demonstration The University of Minnesota and Stratis Health assisted CMS to develop a small demonstration project that launched in September of 2011. Seventeen nursing homes from four States (California, Florida, Massachusetts, and Minnesota) are currently using and testing the QAPI tools, resources, and systems that have been developed. Each nursing home is provided onsite technical assistance to get help as needed, in using the tools and resources. Feedback from the demonstration will be used to help us make any necessary modifications to the tools and resources for the National Rollout. National Rollout Later this summer, CMS will make some core materials available that may be helpful in getting ready for QAPI. This initial launch will occur through the CMS QAPI webpage found at: http://go.cms.gov/Nhqapi. QAPI Regulation The Affordable Care Act requires CMS to promulgate a new regulation and the new regulation is being drafted. Nursing homes will be expected to submit their QAPI plans to CMS one year after promulgation of the regulation. The Nursing Home Quality Improvement Questionnaire In another collaborative effort, CMS’ contractor, Abt Associates, Inc. and their subcontractor, the Colorado Foundation for Medical Care, designed a questionnaire to identify baseline information related to quality systems and processes in nursing homes. This questionnaire was sent to a representative sample of 4,200 randomly selected nursing homes on June 25, 2012. The data collection period is from June 25 through September 28, 2012. Abt Associates, Inc. will collect the completed questionnaires and responses will remain completely confidential. CMS will not have access to any identifying information from respondents. If you have any questions or comments about this questionnaire, please submit them to [email protected]. Check the Status of the National Rollout and Updates in Nursing Home QAPI Please visit the CMS QAPI webpage found at: http://go.cms.gov/Nhqapi for general information about nursing home QAPI. However, if you have specific questions, please email us at: [email protected].
Page 3 – State Survey Agency Directors Effective Date: Immediately. This information should be communicated with all survey and certification staff, their managers and the State/Regional Office training coordinators within 30 days of this memorandum.
/s/ Thomas E. Hamilton
Attachments:
A- The Nursing Home Quality Improvement Questionnaire information sheet B- The Nursing Home Quality Improvement Questionnaire
cc: Survey and Certification Regional Office Management

Nursing Home Providers Given Opportunity to Participate in CMS’ Landmark Quality Improvement Initiative
The Centers for Medicare & Medicaid Services (CMS) is giving nursing home providers the opportunity to
participate in a bold, new quality improvement initiative mandated through the Affordable Care Act. The Affordable
Care Act requires CMS to “establish standards relating to Quality Assurance and Performance Improvement”
(QAPI) and “provide technical assistance (TA) to facilities on the development of best practices” for QAPI.
CMS QAPI Initiatives:
Five Elements - CMS has identified the following key concepts that are found throughout effective quality
systems and are the framework for establishing a QAPI program: 1) Design and Scope; 2) Governance and
Leadership; 3) Feedback, Data Systems, and Monitoring; 4) Performance Improvement Projects; and
5) Systematic Analysis and Systemic Action.
QAPI Tools and Resources: CMS, in collaboration with their contractors, University of Minnesota (UM)
and subcontractor Stratis Health (SH), are continuing to identify and design effective QAPI tools and
resources specifically for nursing homes.
Technical Assistance (TA): CMS contractors are testing QAPI tools, resources, and approaches to
providing TA in a multi-year demonstration project with a small group of nursing homes. These materials
will be made available to all nursing homes following testing.
The Nursing Home Quality Improvement Questionnaire: In another collaborative effort, CMS’
contractor, Abt Associates, Inc., and their subcontractor, the Colorado Foundation for Medical Care,
designed a questionnaire to identify the quality systems and processes nursing homes currently have in
place, as well as assess the extent to which these systems and processes function to help nursing homes
recognize and address quality issues. This information will help CMS and our contractors refine the QAPI
components.
The Nursing Home Quality Improvement Questionnaire will be administered to a representative sample of 4,200
randomly selected nursing homes in two waves:
Summer
2012
First wave of data
collection Objective Establish a baseline of QAPI practices in nursing homes and gather
information on the challenges and barriers to implementing
effective QAPI programs
2013 -
2014
Second wave of
data collection Objective Assess the development of QAPI systems, determine what types of
TA to make available to nursing homes in the future, and
determine the potential impact of TA in advancing QAPI in
nursing homes

Nursing home providers participating in the data collection effort will be given the option of completing an electronic
questionnaire available via the internet or a hard copy questionnaire mailed directly to their facility. The questionnaire
will take approximately 20 minutes to complete. Nursing homes participating in the data collection will not be
identified by name or any other identifying information.
Your participation in this survey effort is crucial to the goals of CMS
in aligning QAPI Technical Assistance with provider needs.
Check your QIES mailbox for notification that you have been selected to participate
in this important information gathering!
CMS is being supported in this effort through partnership with the following organizations:

Nursing Home Quality Improvement Questionnaire
Your answers are being collected by Abt Associates, Inc., a contractor for CMS, who will maintain utmost confidentiality of individual responses. Only anonymous aggregate information will be sent to CMS. The questionnaire is typically completed within 20 minutes. Should you have any questions, please contact the principal investigator from Abt Associates at [email protected]. CMS and Abt Associates sincerely appreciate your participation. Instructions:
• Please read each question carefully and respond by marking an “X” in the box of the response that most closely represents your opinion.
• Please mark only one “X” for each question, unless it tells you to “Mark all that apply.” • While you can use a pen, please use a PENCIL in case you want to change your answer. • Please do NOT use felt tip pens. • Make solid heavy “X” marks in the box. • Please erase cleanly or white out any marks you wish to change. • Please do not make any stray marks on the form.
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this collection is 0938-1165. Public reporting burden for this collection of information is estimated to average 20 minutes, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
Form Approved OMB No. 0938-1165 Exp. Date: 06/30/2015
2
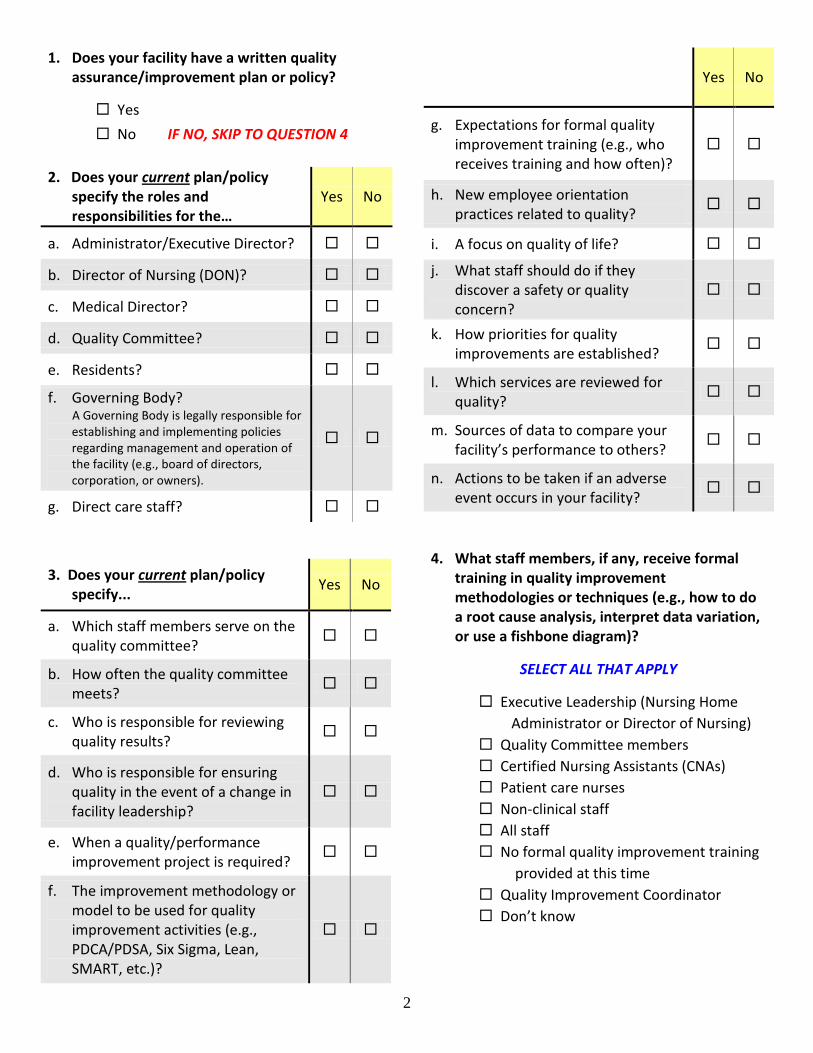
1. Does your facility have a written quality assurance/improvement plan or policy?
Yes No IF NO, SKIP TO QUESTION 4
2. Does your current plan/policy
specify the roles and responsibilities for the…
Yes No
a. Administrator/Executive Director?
b. Director of Nursing (DON)?
c. Medical Director?
d. Quality Committee?
e. Residents?
f. Governing Body? A Governing Body is legally responsible for
establishing and implementing policies regarding management and operation of the facility (e.g., board of directors, corporation, or owners).
g. Direct care staff? 3. Does your current plan/policy
specify... Yes No
a. Which staff members serve on the quality committee?
b. How often the quality committee meets?
c. Who is responsible for reviewing quality results?
d. Who is responsible for ensuring quality in the event of a change in facility leadership?
e. When a quality/performance improvement project is required?
f. The improvement methodology or model to be used for quality improvement activities (e.g., PDCA/PDSA, Six Sigma, Lean, SMART, etc.)?
Yes No
g. Expectations for formal quality improvement training (e.g., who receives training and how often)?
h. New employee orientation practices related to quality?
i. A focus on quality of life?
j. What staff should do if they discover a safety or quality concern?
k. How priorities for quality improvements are established?
l. Which services are reviewed for quality?
m. Sources of data to compare your facility’s performance to others?
n. Actions to be taken if an adverse event occurs in your facility?
4. What staff members, if any, receive formal
training in quality improvement methodologies or techniques (e.g., how to do a root cause analysis, interpret data variation, or use a fishbone diagram)?
SELECT ALL THAT APPLY
Executive Leadership (Nursing Home Administrator or Director of Nursing) Quality Committee members Certified Nursing Assistants (CNAs) Patient care nurses Non-clinical staff All staff No formal quality improvement training provided at this time
Quality Improvement Coordinator Don’t know

3
5. Do you have a dedicated position, such as a Quality Improvement Coordinator, that has been established specifically to manage, coordinate, or oversee quality assurance/improvement activities in your facility (e.g., train staff in quality methods, how to use quality tools, or to lead quality improvement projects)?
Yes No IF NO, SKIP TO QUESTION 8
Please answer the following questions for the
staff member that fills the position described above.
a. Please indicate the percentage of this person’s time that is dedicated specifically to quality improvement coordination.
______%
b. What other role(s), if any, does this person have in your facility?
SELECT ALL THAT APPLY
No other roles / 100% of time is dedicated to quality improvement coordination
----------OR----------
Staff Development Coordinator ADON DON NHA Infection Control Dietary Other (Specify):
_______________
c. Does this person have any formal certification or degree related to quality improvement or organizational development?
Yes No Don’t Know
6. Is this position shared with a second person?
Yes No IF NO, SKIP TO QUESTION 7
Please answer the following questions for this
additional staff member.
a. Please indicate the percentage of this person’s time that is dedicated specifically to quality improvement coordination.
______%
b. What other role(s), if any, does this person have in your facility?
SELECT ALL THAT APPLY
No other roles / 100% of time is dedicated to quality improvement coordination
----------OR----------
Staff Development Coordinator ADON DON NHA Infection Control Dietary Other (Specify):
_______________
c. Does this person have any formal certification or degree related to quality improvement or organizational development?
Yes No Don’t Know
7. If the questions on this page do not adequately capture the nature of quality improvement coordination at your facility, please describe:
_______________________________________
_______________________________________
_______________________________________
_______________________________________

4
8. Select the frequency that most closely matches how often performance data are routinely reviewed by the Nursing Home Administrator (during QA meetings or otherwise) for each of the topics listed below.
FREQUENCY OF REVIEW
SELECT ONE ANSWER FOR EACH TOPIC
As n
eede
d bu
t n
ot ro
utin
ely
Dai
ly
Wee
kly
Mon
thly
Qua
rter
ly
Ann
ually
Not
Rev
iew
ed
Not
App
licab
le
SATISFACTION DATA
a. Resident satisfaction
b. Family satisfaction
c. Staff satisfaction
d. Consistent assignment of CNAs or other caregivers (monitoring whether consistent assignments actually occur as scheduled)
e. Call light response times
f. Quality of food services
g. Other (Specify): ___________________
________________________________
CLINICAL DATA
h. Quality Measures from MDS (QMs)
i. Adverse events (e.g., medication error, falls with injury)
j. Near misses (could have caused harm, e.g., medication filled incorrectly but not given)
k. Data related to rehabilitative therapy outcomes (e.g., return to community/previous residence)
l. Healthcare-Associated Infections (including multi-drug resistant organisms)
m. Antipsychotic use
n. Hospital admissions/readmissions
o. Other (Specify): ___________________
________________________________

5
Item 8 (Continued) FREQUENCY OF REVIEW
SELECT ONE ANSWER FOR EACH TOPIC
As n
eede
d bu
t n
ot ro
utin
ely
Dai
ly
Wee
kly
Mon
thly
Qua
rter
ly
Ann
ually
Not
Rev
iew
ed
Not
App
licab
le
STAFFING and OPERATIONAL DATA
p. Staff turnover
q. Staff absenteeism
r. Financial
s. Quality Improvement Project A Quality Improvement Project is a set of related activities designed to achieve measurable improvement in processes and outcomes.
t. QA Committee meeting minutes
u. Direct care nursing hours per resident day
v. Use of agency/temp staff
w. Resident census
x. Other (Specify): ___________________
________________________________
STATE SURVEY & PUBLIC DATA
y. State survey deficiencies
z. Complaints
aa. Occurrences or incidents reportable to survey agency
bb. Advancing Excellence Campaign
cc. Five Star Rating
dd. Other (Specify): ___________________
________________________________
6
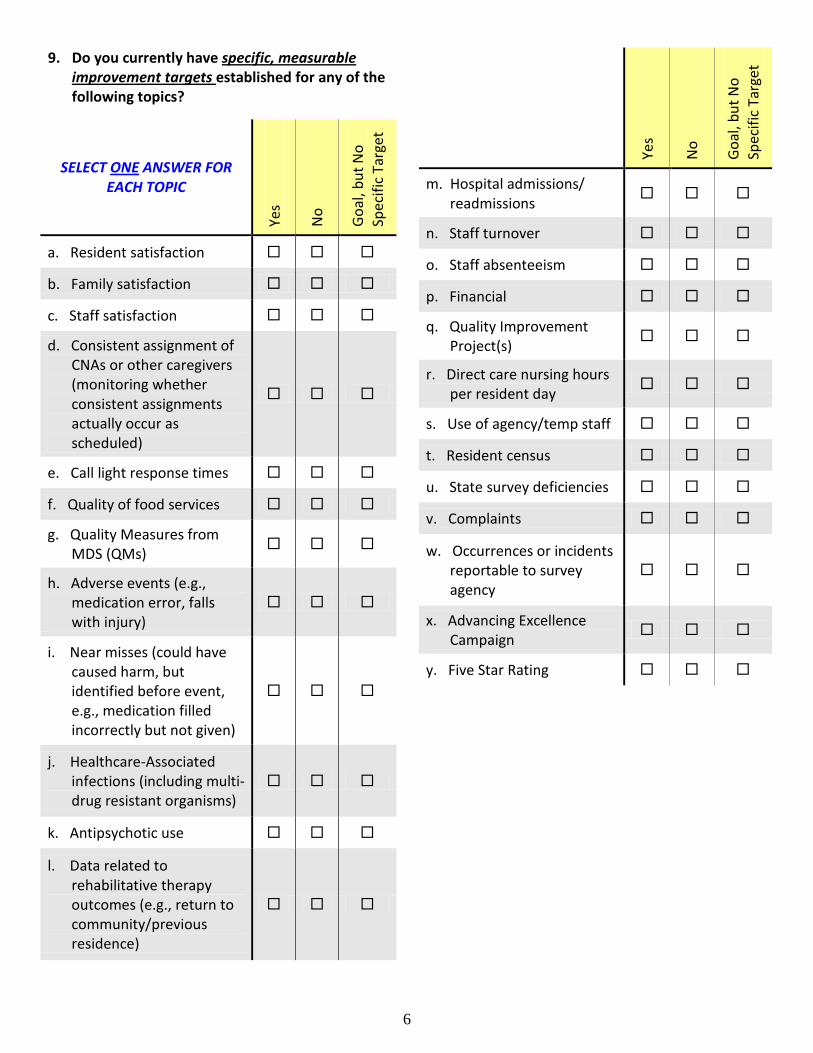
9. Do you currently have specific, measurable improvement targets established for any of the following topics?
SELECT ONE ANSWER FOR EACH TOPIC
Yes
No
Goal
, but
No
Spec
ific
Targ
et
a. Resident satisfaction
b. Family satisfaction
c. Staff satisfaction
d. Consistent assignment of CNAs or other caregivers (monitoring whether consistent assignments actually occur as scheduled)
e. Call light response times
f. Quality of food services
g. Quality Measures from MDS (QMs)
h. Adverse events (e.g., medication error, falls with injury)
i. Near misses (could have caused harm, but identified before event, e.g., medication filled incorrectly but not given)
j. Healthcare-Associated infections (including multi-drug resistant organisms)
k. Antipsychotic use
l. Data related to rehabilitative therapy outcomes (e.g., return to community/previous residence)
Yes
No
Goal
, but
No
Spec
ific
Targ
et
m. Hospital admissions/ readmissions
n. Staff turnover
o. Staff absenteeism
p. Financial
q. Quality Improvement Project(s)
r. Direct care nursing hours per resident day
s. Use of agency/temp staff
t. Resident census
u. State survey deficiencies
v. Complaints
w. Occurrences or incidents reportable to survey agency
x. Advancing Excellence Campaign
y. Five Star Rating

7
10. Select the extent to which you Agree or Disagree with each of the following statements about your facility’s practices related to ADVERSE EVENTS and follow up ACTION PLANS.
NOTE: An Adverse Event is an untoward, undesirable, and usually unanticipated event that actually or potentially causes serious harm, affecting a resident’s quality of life or quality of care. St
rong
ly D
isagr
ee
Disa
gree
Agre
e
Stro
ngly
Agr
ee
Don’
t Kno
w
UNDERSTANDING ADVERSE EVENTS a. Our facility has defined
what we consider to be an adverse event.
b. Our facility has a specified methodology to evaluate adverse events.
c. Our facility does a root cause analysis when an adverse event occurs.
d. Our facility tracks data related to adverse events.
e. Our facility provides training to key staff on how to investigate an adverse event.
f. Our facility has a policy that protects staff who report adverse events from retaliation.
RESPONDING TO AN ADVERSE EVENT g. Our facility develops an
improvement action plan or project after an adverse event occurs.
h. Our facility’s improvement action plans routinely include measureable goals or targets for desired improvements.
Stro
ngly
Disa
gree
Disa
gree
Agre
e
Stro
ngly
Agr
ee
Don’
t Kno
w
i. Our facility monitors the progress of improvement action plans to determine if desired results are being obtained.
j. Our facility monitors improvement project results after completion to determine if desired results are sustained over time.
k. We almost always make changes to systems or processes when adverse events occur.
l. We almost always make changes to policies and protocols when adverse events occur.
m. Disciplinary action is not taken when adverse events are reported by staff, unless the outcome was the result of deliberate intent to harm.
n. Staff members are encouraged to report an adverse event.
o. Staff feel safe when reporting an adverse event (do not feel they will be disciplined or fear losing their jobs).
p. Our Governing Body reviews all adverse event findings.
q. We have set clear expectations of staff to ensure resident safety.
r. It is easy to make changes to improve resident safety in this nursing home.

8
11. Who would perform a root cause analysis (RCA) and action plan following an adverse event in your facility?
SELECT THE ONE ANSWER THAT MOST CLOSELY MATCHES THE PRACTICE THAT OCCURS IN YOUR FACILITY.
We would not perform a RCA An individual (e.g., QA/QI Coordinator, NHA, DON) performs the RCA A team performs the RCA A team performs the RCA and the team
includes those involved in the event
12. Select the source(s) of data that your facility uses to evaluate your facility’s performance.
SELECT ALL THAT APPLY Advancing Excellence Campaign Corporate data MDS QM reports National averages Nursing Home Compare Results achieved in other industries Satisfaction survey vendor reports Software vendor reports (e.g., quality tracking programs or products) State averages Compare to our own previous data or trend Other (Specify): ____________________
_________________________________ None
13. Select the extent to which you Agree or Disagree with the following statements about your facility’s INITIATION of quality improvement projects or action plans.
NOTE: A Quality Improvement Project is a set of related activities designed to achieve measurable improvement in processes and outcomes.
Stro
ngly
Disa
gree
Disa
gree
Agre
e
Stro
ngly
Agr
ee
Don’
t Kno
w
a. Quality improvement projects are initiated only when something goes wrong.
b. Our Governing Body mandates what improvement projects will be undertaken in our facility.
c. Our facility maintains a calendar that provides a schedule to evaluate the performance of important care and service areas on a regular basis.
d. The Quality Committee decides when an improvement project needs to occur.
e. When several residents complain about the same issue, the need for initiating a performance improvement project is evaluated.
f. Staff members in our facility identify areas in need of improvement.
g. Residents in our facility identify areas in need of improvement.

9
14. Select the extent to which you Agree or Disagree with the following statements about ACTIONS TAKEN and RESULTS from your facility’s quality improvement projects.
NOTE: A Quality Improvement Project is a set of related activities designed to achieve measurable improvement in processes and outcomes.
Stro
ngly
Disa
gree
Disa
gree
Agre
e
Stro
ngly
Agr
ee
Don’
t Kno
w/N
A
a. Staff re-education is mainly all that is needed to prevent reoccurrence of a quality problem.
b. Quality improvement projects are typically carried out by our DON.
c. Quality improvement projects are carried out by improvement teams that are multidisciplinary.
d. The focus of our quality improvement projects is primarily to meet regulatory compliance.
e. During a quality improvement initiative, we use data to inform our actions or decisions.
f. Revising policies or procedures is mainly all that is needed to prevent reoccurrence of a quality problem.
g. Our quality improvement project action plans almost always include changes to a system or process related to the problem.
Stro
ngly
Disa
gree
Disa
gree
Agre
e
Stro
ngly
Agr
ee
Don’
t Kno
w/N
A
h. Our organization continues to advance the quality of our services by maintaining improvements over long periods of time.
i. An evaluation of any needed change to the environment, equipment or physical plant is generally part of our improvement plan process.
j. Our Medical Director actively participates in quality improvement teams.
k. Physicians working in our nursing home (other than our Medical Director) actively participate in our quality improvement teams.
l. Nurse Practitioners and/or Physician Assistants working in our nursing home actively participate in our quality improvement teams.
10
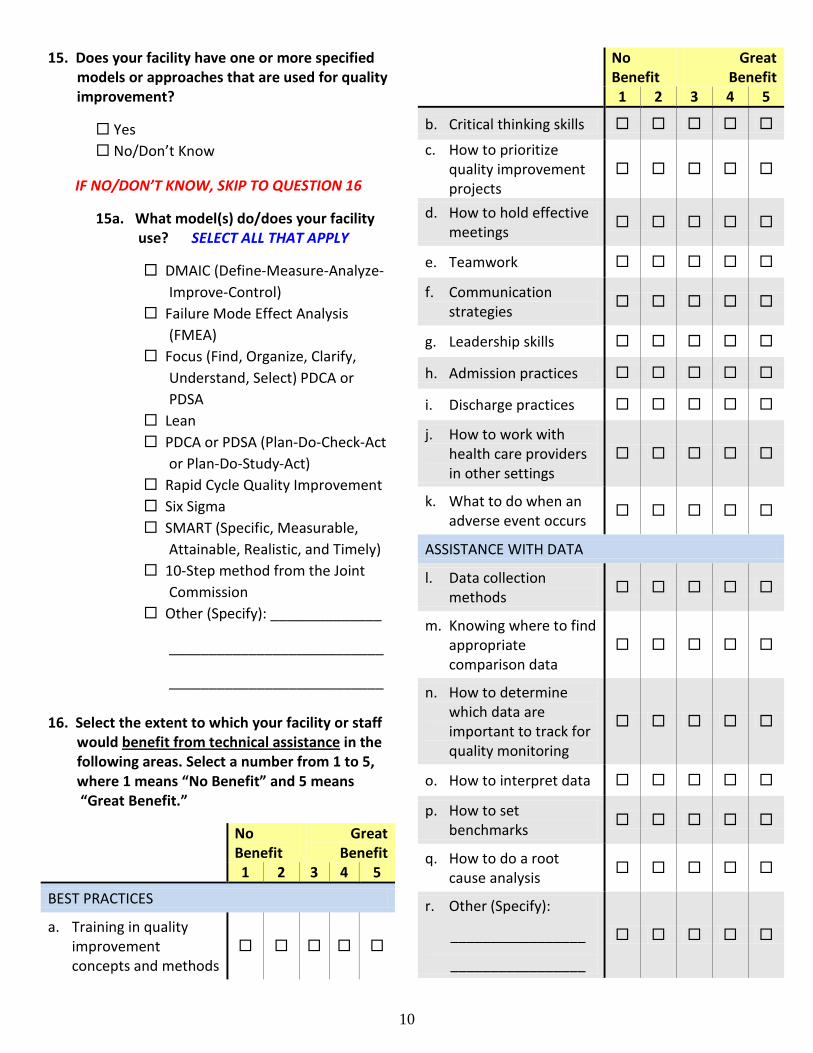
15. Does your facility have one or more specified models or approaches that are used for quality improvement? Yes No/Don’t Know
IF NO/DON’T KNOW, SKIP TO QUESTION 16
15a. What model(s) do/does your facility use? SELECT ALL THAT APPLY
DMAIC (Define-Measure-Analyze- Improve-Control) Failure Mode Effect Analysis (FMEA) Focus (Find, Organize, Clarify, Understand, Select) PDCA or PDSA Lean PDCA or PDSA (Plan-Do-Check-Act or Plan-Do-Study-Act) Rapid Cycle Quality Improvement Six Sigma SMART (Specific, Measurable, Attainable, Realistic, and Timely) 10-Step method from the Joint Commission Other (Specify): ______________
___________________________
___________________________
16. Select the extent to which your facility or staff would benefit from technical assistance in the following areas. Select a number from 1 to 5, where 1 means “No Benefit” and 5 means “Great Benefit.”
No Benefit
Great Benefit
1 2 3 4 5
BEST PRACTICES
a. Training in quality improvement concepts and methods
No Benefit
Great Benefit
1 2 3 4 5
b. Critical thinking skills
c. How to prioritize quality improvement projects
d. How to hold effective meetings
e. Teamwork
f. Communication strategies
g. Leadership skills
h. Admission practices
i. Discharge practices
j. How to work with health care providers in other settings
k. What to do when an adverse event occurs
ASSISTANCE WITH DATA
l. Data collection methods
m. Knowing where to find appropriate comparison data
n. How to determine which data are important to track for quality monitoring
o. How to interpret data
p. How to set benchmarks
q. How to do a root cause analysis
r. Other (Specify):
_________________
_________________
11
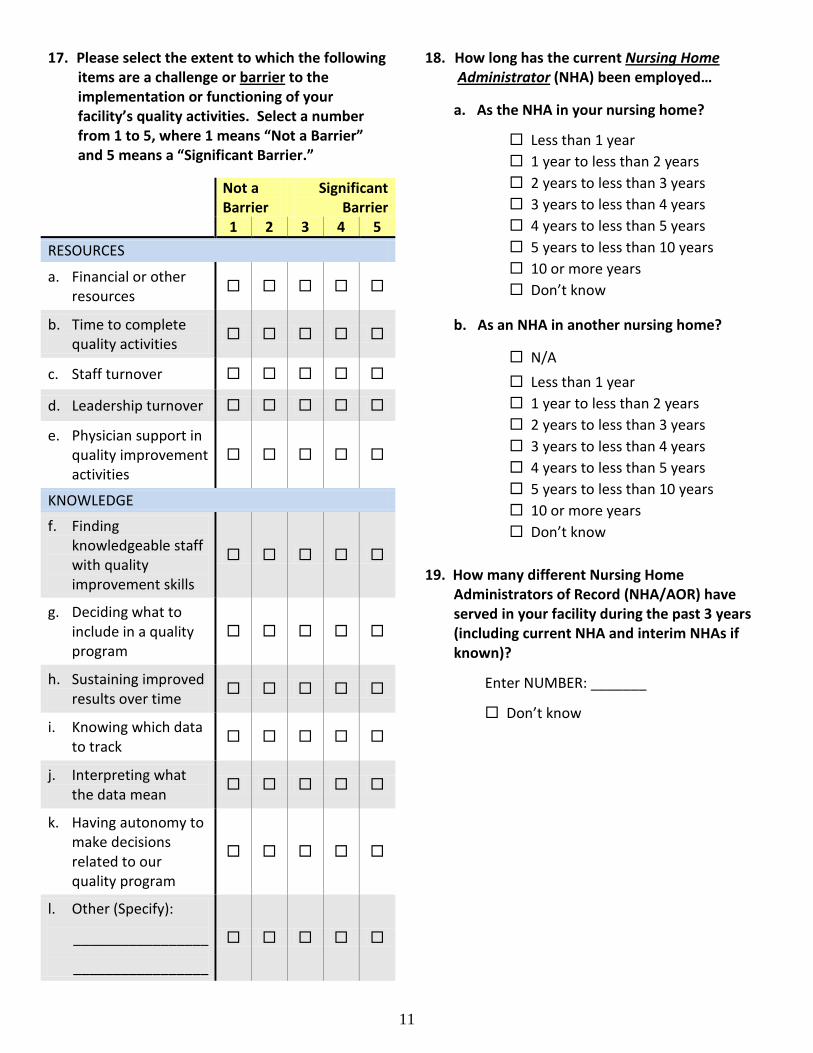
17. Please select the extent to which the following items are a challenge or barrier to the implementation or functioning of your facility’s quality activities. Select a number from 1 to 5, where 1 means “Not a Barrier” and 5 means a “Significant Barrier.”
Not a Barrier
Significant Barrier
1 2 3 4 5 RESOURCES
a. Financial or other resources
b. Time to complete quality activities
c. Staff turnover
d. Leadership turnover
e. Physician support in quality improvement activities
KNOWLEDGE
f. Finding knowledgeable staff with quality improvement skills
g. Deciding what to include in a quality program
h. Sustaining improved results over time
i. Knowing which data to track
j. Interpreting what the data mean
k. Having autonomy to make decisions related to our quality program
l. Other (Specify):
_________________
_________________
18. How long has the current Nursing Home Administrator (NHA) been employed… a. As the NHA in your nursing home?
Less than 1 year 1 year to less than 2 years 2 years to less than 3 years 3 years to less than 4 years 4 years to less than 5 years 5 years to less than 10 years 10 or more years Don’t know
b. As an NHA in another nursing home?
N/A Less than 1 year 1 year to less than 2 years 2 years to less than 3 years 3 years to less than 4 years 4 years to less than 5 years 5 years to less than 10 years 10 or more years Don’t know
19. How many different Nursing Home Administrators of Record (NHA/AOR) have served in your facility during the past 3 years (including current NHA and interim NHAs if known)?
Enter NUMBER: _______ Don’t know

12
20. How long has the current Director of Nursing been employed…
a. As the DON in your nursing home?
Less than 1 year 1 year to less than 2 years 2 years to less than 3 years 3 years to less than 4 years 4 years to less than 5 years 5 years to less than 10 years 10 or more years Don’t know
b. In any other prior position in your nursing home?
N/A Less than 1 year 1 year to less than 5 years 5 years to less than 10 years 10 or more years Don’t know
21. How many different Directors of Nursing have served in your facility during the past 3 years (include current DON and interim DONs if known)?
Enter NUMBER: _________ Don’t know
22. Does your nursing home follow any culture change/person-centered care practices?
Yes No IF NO, SKIP TO QUESTION 23
22a. If “Yes,” select all that apply:
Small Houses Households/Neighborhoods Consistent Assignment Use of Artifacts of Culture Change for self-assessment Other (Specify): ______________
___________________________
23. What is your facility’s affiliation?
Independent, free-standing Hospital system, attached Hospital system, free-standing Multi-facility nursing home organization (chain or corporation)
24. If your nursing home is part of a multi-facility
organization, approximately how many nursing homes are affiliated with the parent corporation?
N/A 1 - 2 3 - 5 6 - 10 11 - 25 26 - 100 More than 100
25. What is your title?
Administrator Director of Nursing Other (Specify): ___________________
________________________________
Thank you very much for your time to respond to this questionnaire. Your participation
will help support all nursing homes.

QAPI (Quality Assurance and Performance Improvement) Participating Facilities will: 1. Create an interdisciplinary quality team, including members representing department leadership and administrative leadership, unit manager(s), floor nurses, nurse aide(s), therapist(s), social worker(s), nutrition staff, and others interested and committed to quality improvement; 2. Involve residents in the QAPI program. Participate in conference calls/ webinar sessions, and other virtual forms of communication on focus topics; 3. Dedicate staff and resources to establish, implement, and evaluate a Quality Assurance Performance Improvement program. In addition to the in‐person trainings, team members will need to devote ongoing time to this effort at the nursing facility; 4. Send at least two team members to group educational workshops for participating nursing facilities that will be offered. Fulfill the expectations for pre‐work and completion of self‐study modules; 5. Designate one person to serve as the primary facility contact, who, in a leadership capacity, can drive and support the facility’s improvement efforts, serve as the project contact, and serve as an external spokesperson as appropriate. Designate one person to serve as the secondary facility contact; 6. Be willing to share experiences and outcomes with others to promote a community‐wide culture of continuous improvement, and to be identified publicly with the initiative for future nursing facility and surveyor training; 7. Conduct at least one PIP (Performance Improvement Program) project in Demo Year 1 and begin at least one other PIP project in Demo Year