cardinal manifestations of disease: alterations in body temp. dr. meg-angela christi amores
TRANSCRIPT

Cardinal Manifestations of Disease: ALTERATIONS IN BODY TEMP.
Dr. Meg-angela Christi Amores
Fever and Hyperthermia
• hypothalamic thermoregulatory center – regulates body temperature (core BT 37 C)
• A.M. temperature of >37.2°C (>98.9°F) or a P.M. temperature of >37.7°C (>99.9°F) would define a fever
• Rectal temperatures are generally 0.4°C (0.7°F) higher than oral readings

Fever
• Elevation of body temperature that exceeds the normal daily variation
• occurs in conjunction with an increase in the hypothalamic set point
• Vasoconstriction in hands and feet, feeling cold, shivers = heat conversion and production
• until the temperature of the blood bathing the hypothalamic neurons matches the new thermostat setting
Fever
• Pathogenesis– Pyrogens – substances that cause fever• Exogenous (microbial products, microbial toxins, or
whole microorganisms)• Endogenous a.k.a Cytogenic Pyrogens (IL-1, IL-6, tumor
necrosis factor (TNF), ciliary neurotropic factor (CNTF), and interferon (IFN) )
– Elevation of Hypothalamic Set point• levels of prostaglandin E2 (PGE2) are elevated in
hypothalamic tissue and the third cerebral ventricle


Hyperthermia
• uncontrolled increase in body temperature that exceeds the body's ability to lose heat
• setting of the hypothalamic thermoregulatory center is unchanged
• does not involve pyrogenic molecules• Exogenous heat exposure and endogenous
heat production


Fever and Rash
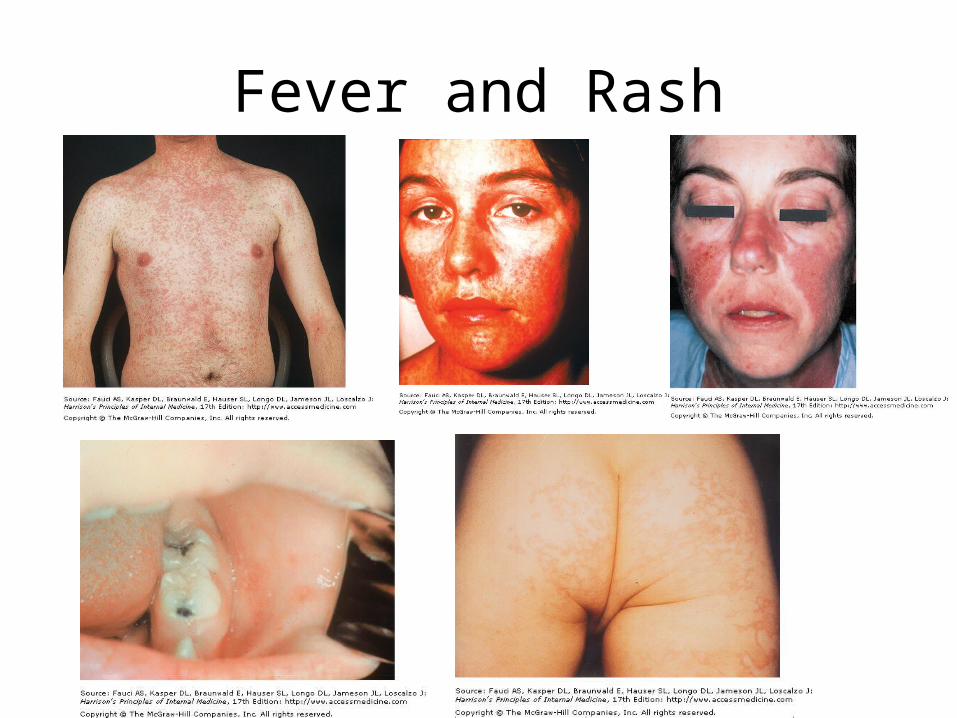
• presents a diagnostic challengeMeasles – Rubeola, rash starts at the hairline 2–3
days into the illness and moves down the body, sparing the palms and solesKoplik's spots - seen during the first 2 days
Rubella – German measles, also spreads from the hairline downward, but tend to clear from originally affected areas as it migrates, and it may be pruritic

Fever and Rash
• erythema infectiosum (fifth disease) - human parvovirus B19, primarily affects children 3–12 years old; develops after fever has resolved as a bright blanchable erythema on the cheeks – more diffuse rash (often pruritic) appears the next
day on the trunk and extremities and then rapidly develops into a lacy reticular eruption that may wax and wane

Fever and Rash
• systemic lupus erythematosus - typically develop a sharply defined, erythematous eruption in a butterfly distribution on the cheeks (malar rash)
• Still's disease - manifests as an evanescent salmon-colored rash on the trunk and proximal extremities that coincides with fever spikes
Types of lesions
• Macules - flat lesions defined by an area of changed color • Papules - raised, solid lesions <5 mm in diameter• plaques ->5 mm in diameter with a flat, plateau-like surface• nodules ->5 mm in diameter with a rounded configuration• Wheals (urticaria, hives) - papules or plaques that are pale pink
and may appear annular (ringlike) as they enlarge• Vesicles (<5 mm) and bullae (>5 mm) are circumscribed,
elevated lesions containing fluid• Pustules are raised lesions containing purulent exudate
Fever and Rash

Fever of Unknown Origin (FUO)
Classic Definition• 1) temperatures of >38.3°C (>101°F) on
several occasions• (2) a duration of fever of >3 weeks• (3) failure to reach a diagnosis despite 1 week
of inpatient investigation

Fever of Unknown Origin
New Classification• (1) classic FUO• (2) nosocomial FUO• (3) neutropenic FUO• (4) FUO associated with HIV infection

Classic FUO• temperatures of >38.3°C on several occasions• a duration of fever of >3 weeks• outpatient visits or 3 days in the hospital without
elucidation of a cause or 1 week of "intelligent and invasive" ambulatory investigation
• CAUSES: – Undiagnosed – 30%– Infections (e.g. Tuberculosis) – 26%– Non-infectious Inflammatory (e.g.PR, SLE)– 24%– Neoplasms – 12.5%

FUO
• Nosocomial FUO – more than 50% are infected– Intravascular lines, septic phlebitis, and prostheses
are all suspect– Multiple blood, wound, and fluid cultures are
mandatory– Threshold for CT scans, ultrasonography, 111In WBC
scans, noninvasive venous studies is low
FUO
• Neutropenic FUO – Neutropenic patients are susceptible to focal
bacterial and fungal infections, to bacteremic infections, to infections involving catheters (including septic thrombophlebitis), and to perianal infections
– Candida and Aspergillus infections are common– 50–60% of febrile neutropenic patients are
infected, and 20% are bacteremic
FUO
• HIV- associate FUO– Due to HIV alone– due to Mycobacterium avium or Mycobacterium
intracellulare, tuberculosis, toxoplasmosis, CMV infection, Pneumocystis infection, salmonellosis, cryptococcosis, histoplasmosis, non-Hodgkin's lymphoma, and (of particular importance) drug fever

Hypothermia and Frostbite
• Accidental hypothermia - unintentional drop in the body's core temperature below 35°C
• Primary accidental hypothermia is a result of the direct exposure of a previously healthy individual to the cold


Hypothermia
• Heat loss occurs through five mechanisms: – radiation (55–65% of heat loss)– conduction (10–15% of heat loss, but much
greater in cold water)– convection (increased in the wind)– Respiration– evaporation (which are affected by the ambient
temperature and the relative humidity)

Hypothermia
• Hypothermia is confirmed by measuring the core temperature, preferably at two sites.
• cardiac monitoring should be instituted, along with attempts to limit further heat loss
• Supplemental oxygenation is always warranted
• NGT, FBC

• For the next meeting, read on Cardinal Manifestations of Disease : DYSPNEA
• Harrison’s Principles of Internal Medicine 17th edition