capacity building for adaptation of cpgs for the iv ig cpg working group
TRANSCRIPT

Intravenous Immunoglobulins
CPG Adaptation Proposal
Dr. Yasser S. AmerMBBCh, MS Ped, MS HCI, CPHQ, FISQua
Coordinator, KSUMC-Wide CPG Steering Committee
CPG Methodologist, CPGs Unit, Quality Management Dept.6/30/2016 1
Capacity Building for CPG Adaptation at KSUMC SeriesJune 2016/ Ramadan 1437

مبســـــم هللا الرحمـــــن الرحـــــي
In the name of Allah. Most Gracious, Most Merciful
6/30/2016 2

Statement of disclosure
6/30/2016 3
Dr. Yasser S. AmerMBBCh, MPedia, MHCI, CPHQ, FISQua
I have no actual or potential, commercial or
academic conflict of interest to declare in relation to
this presentation/ project

The EBM Triad
46/30/2016

Definition: (old)
“Systematically developed statements to assist
practitioner and patient decisions about appropriate
health care for specific clinical circumstances”
(IOM 1990)
Clinical Practice Guidelines (CPGs)
56/30/2016

CPGs Definition (New)
“Statements that include Recommendations
intended to optimize patient care that are
informed by a Systematic Review of evidence
and an assessment of the benefits and harms of
alternative care options”
Committee on Standards for Developing Trustworthy
CPGs (IOM-AHRQ 2011)
6/30/2016 6

Evidence Pyramid (Study design)
SR
RCT
Cohort
Case control
Case series
Case report
Expert opinion
I
II
III
IV
A
B
C
Leve
ls o
f E
vid
en
ce
Gra
des o
f Reco
mm
en
datio
ns
MA
6/30/2016 7

methods
6/30/2016 8
Benefits Risks/ Burden
QoE!

Level
Evidence
(LoE)
Grade
Recomm.
(GoR)
Strength
EVIDENCE PYRAMID6/30/2016 9

6/30/2016 10
What makes a trustworthy CPG?

Standards for high quality CPGsIOM 2011 – G-I-N 2012 – AGREE 2013
6/30/2016 11

Standards for trustworthy CPGsIOM 2011 G-I-N 2012
1- Establishing Transparency 1- Decision making process. 2- Methods
2- Management of COI 3- COI
3- (GDG) composition 4- GDG composition
4- (CPG – SR) intersection 5- Evidence reviews
5- Assign/ link to (LoE) & (GoR) 6- Rating of E & Rs
6- Articulation of (Rs) 7- CPG Rs (formulation/ wording)
7- External Review 8- Peer review & stakeholder consultation
8- Updating 9- Expiration & updating
10- Scope of CPG
11- Financial support/ sponsoring organization
6/30/2016 12

How to assess of the quality of any CPG ?
6/30/2016 13

CPG development methodologies
6/30/2016 14

CPGsWhat to do?
6/30/2016 15

Read
Adopt
AdaptDevelop
CPGs ?
6/30/2016 16

Different Options to deal with CPG
6/30/2016 17

CPGsDEVELOPMENT
(de novo)
vs.
ADAPTATION6/30/2016 18

Types of CPGs
1.Evidence-Based CPGs (evidence-based methodology)
2.Consensus/ expert-based CPGs
6/30/2016 19
Which type do you think is better?

The EBM Triad
206/30/2016

Process/ Methods
6/30/2016 21

6/30/2016 22

236/30/2016

Adaptation of CPGsIs the systematic approach to the endorsement and/or
modification of a guideline(s) produced in one cultural and organizational setting for application in a different context. Adaptation may be used as an alternative to de novo guideline development, e.g., for customizing (an) existing guideline(s) to suit the local context.
http://www.adapte.org/
http://www.g-i-n.net/
6/30/2016 24

Hospital-Wide Policy & Procedure for
Hospital CPGs Adaptation-SEPT 2013- in process for update WITH “NEW TOOLS”
6/30/2016 25

Formulation of a CPG Adaptation Working Group
6/30/2016 26
In collaboration with:
• Departmental CPG Committee
• Departmental Quality Team

Selecting a CPG Topic
Prevalence of the condition (high volume)
Patient safety concern (high risk)
Under-, over-, misuse of intervention(s)
Burden due to the condition
Practice variation
Costs of different practice options
Likelihood of effectiveness of CPG
Potential for improving quality of care and/or outcomes
Existence of relevant good quality CPGs
6/30/2016 27

Topic (concerns?)
6/30/2016 28
• Disease/ condition (Clinical Diagnosis) versus Healthcare Technology? CPG vs. HTA http://www.inahta.org/hta-tools-resources/
• Another CPG Dept. Committee may work on another CPG that includes IV IG as one option for management (conflict?)
• Decision according to priority Dx vs. HT?

HTA – IV IG in Sepsis (2012)
6/30/2016 29

KSUMC Protocol for New CPG
6/30/2016 30

Health/ Clinical/ Key Questions
Patient (& disease characteristics)
Intervention(s)
Professionals (Target users)
Outcomes (purpose of the CPGs)
Healthcare settings (& context)
6/30/2016 31
CPG Scope: PIPOH Model

Health Question Tool (modif.)
6/30/2016 32

6/30/2016 33

6/30/2016 34

6/30/2016 35

6/30/2016 36

Inclusion / Exclusion CPGs Selection Criteria (6)1. Methods of Development: Evidence-Based CPGs: (Detailed
Methodology not Consensus-based CPGs (Expert opinion)
2. Author(s): Organization and Specialized Society not single authors.
3. Country: International not national CPGs.
4. Date of Publication: range of year of publications: last 5 years or less(e.g. 2010 – 2014) – except if none!
5. Language: English CPGs only
6. Status: only Original source CPG (de novo developed) rather thanadapted CPGs
6/30/2016 37

CPG selection criteria Tool (new)
6/30/2016 38

Search and Screen for Source CPGs
6/30/2016 39

Producers Finders
6/30/2016 40

CPGs Finders
“Baseline Search List”
• National Guidelines Clearinghouse (NGC/ AHRQ)
• Guidelines International Network (G-I-N)
• EBSCO DynaMed
• PubMed/ MedLine
• Google Scholar
6/30/2016 41

> 408 CPGs
6/30/2016 42
AHRQ-NGC National Guideline Clearinghousewww.guidelines.gov

Shaikh Bahamdan’s Research Chair for Evidence-Based Health Care & Knowledge Translation
Member of G-I-N since Oct. 2009Free access to International CPG Library of G-I-N
http://c.ksu.edu.sa/ebhc
6/30/2016 43


6/30/2016 45

6/30/2016 46

6/30/2016 47


Some CPGs are only retrievable by “Googling” them!

6/30/2016 50

Specialized Scientific (Specialty) Societies
6/30/2016 51

Assessment of retrieved source CPGs
6/30/2016 52

Instructor
Dr. Yasser Sami AmerMS Pediatrics, MS Healthcare Informatics, CPHQ
Supervisor, EBPU, QMD, KSUMCCPGs Advisor , KSUHs, AUHs
Member, G-I-N Adaptation & Implementation Working Groups

The AGREE Research TeamPI: Melissa Brouwers, PhD
Head, HSR Oncology Dept., McMaster Univ.
https://youtu.be/z8nfqwvH4eM
Watch this video!
6/30/2016 54

Purpose
To guide on how to use and apply the AGREE II forassessing CPGS
Items
Domains
User’s Manual
Website

Outlines
• Overview of AGREE II including the items and domains.
• Present the scoring method of the CPG.
• How to use and apply the AGREE II for assessing CPG.
• Share the overall scoring.
• The AGREE Enterprise Website

What is the AGREE II Tool ?
• Quality (Methodological rigor & transparency; confident in resulting
Recommendations)
57 Using the AGREE II Instrument
Assess
Guide •CPGs Development •CPGs Reporting
History
1st AGREE was published in 2003,then refined in 2009 AGREE II (New scoring “7 point scale” – Items modifications – New user’s manual) – 11 YEARS !
Can be applied to any CPG in any Disease area !

• Healthcare providers/ clinicians
• CPG developers/ adapters
• Policy makers
• Educators
Who can use the AGREE II ?

Considerations before a CPG Assessment
• increase the reliability of the assessment
2 – 4 Appraisers
• in full and obtain all related information and needed documents before undertaking the AGREE II assessment ( to make a well informed assessment)
Read CPG first

Rating Scale• All AGREE II Items are rated on the following 7-point scale
Score Meaning
7 (Strongly Agree)
= If the quality of reporting is exceptional and full criteria and considerations in User’s manual are met.
1 (Strongly Disagree)
= No information relevant to AGREE II item OR the concept is very poorly reported
2 – 6 = when the reporting of the item does not meet the full criteria or considerations, depending on the completeness & quality of reporting .

The AGREE II Includes….
•Core Items•(6 Domains)
23
•Overall Assessment Items
2

23 Items in 6 DomainsUSER’S MANUAL page 7
DOMAINS No. of Items
1 Scope & Purpose 3
2 Stakeholder Involvement 3
3 Rigour of Development 8
4 Clarity & Presentation 4
5 Applicability 3
6 Editorial Independence 2

Items and Domains: A Closer Look
AGREE II:USER’S MANUAL
Per each Domain (guidance for rating the 23 items) Pages 11 – 41
User’s Manual Description:Where to Look:How to Rate:Item content includes the following CRITERIA:Additional CONSIDERATIONS:

Domain 1

DOMAIN 1. SCOPE AND PURPOSE
1. Objective(s):
Health impact & benefits of a CPG on target population
Introduction, scope, purpose, rationale, background & objectives

DOMAIN 1 - Q1 - Objective(s)

2. Health Question(s):-Questions, Scope, Purpose, Rationale and
Background
3. Target population:-Pt. population, target population, relevant pt.s,
scope and purpose
DOMAIN 1. SCOPE AND PURPOSE

DOMAIN 1 – Q2 - Health Question(s)
6/30/2016 68

Health/ Clinical/ Key Questions
Patient (& disease characteristics)
Intervention(s)
Professionals (Target users)
Outcomes (purpose of the CPGs)
Healthcare settings (& context)
19th March 2013 EBCPGs: Dr. Yasser Sami Amer 69
CPG Scope: PIPOH Model

DOMAIN 1 – Q3 – Target population
6/30/2016 70

Domain 2

4. Guideline groupMethods, guideline panel list, acknowledgements, & appendices
DOMAIN 2. STAKEHOLDER INVOLVEMENT

5. Patient preference Scope, methods, guideline panel list, external review &target
population perspectives
DOMAIN 2. STAKEHOLDER INVOLVEMENT

6. Target usersTarget user & intended user
DOMAIN 2. STAKEHOLDER INVOLVEMENT
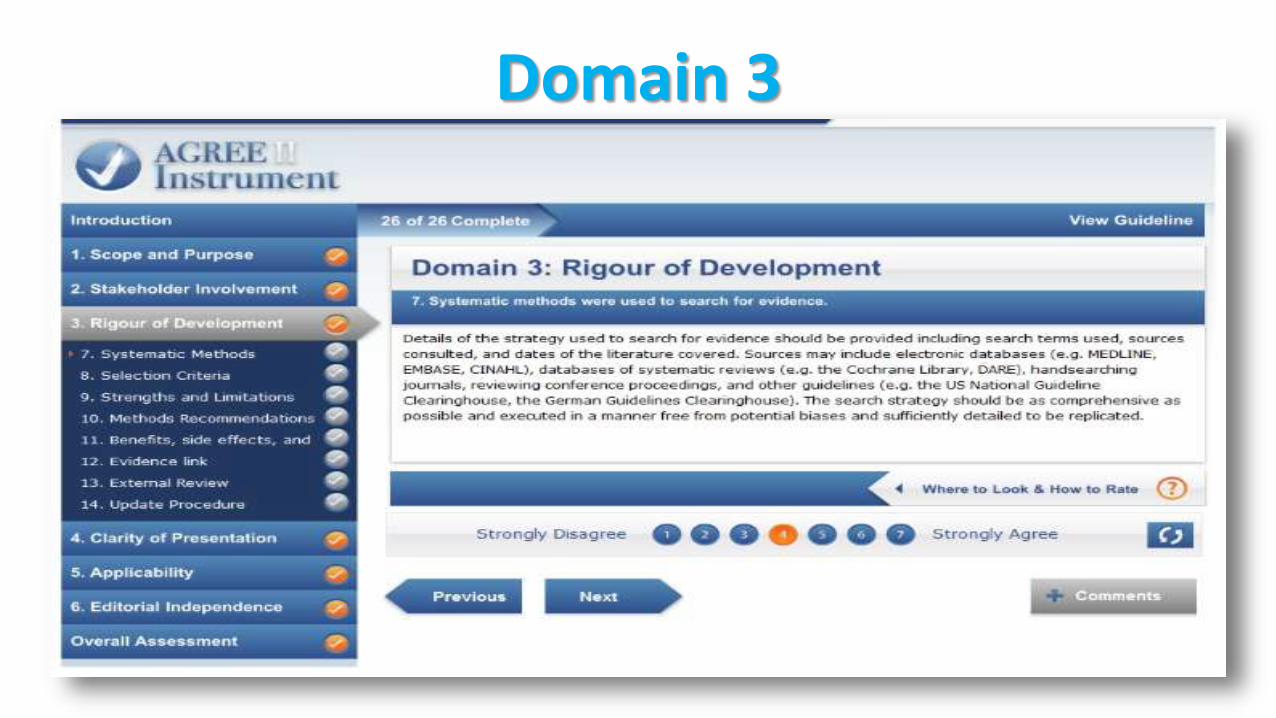
Domain 3

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E
10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process same sections+ Rs, Key Evidence+ acknowledgements+ CPG update, date of CPG

Level
Evidence
(LoE)
Grade
Recomm.
(GoR)
Strength
EVIDENCE PYRAMID6/30/2016 77

Methodology of development
• In same CPG document (in brief or detailed)
• In a separate document or supplement (usu. Detailed)
• Not documented

Within CPG document (ENT IDSA ABRS CPG)

Mentioned but not documented

KSUMC CPGs: Adaptation Process Methodology

Separate Methodology document (SIGN 50: A guideline developer’s handbook -2011)

NICE: The guideline manual (2012)

7. Systematic methods for E search
8. Selection Criteria of E9. Strengths & Limitations of E
10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices
+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process same sections+ Rs, Key Evidence+ acknowledgements+ CPG update, date of CPG

Selection Criteria of E
6/30/2016 85

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria
+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process same sections+ Rs, Key Evidence+ acknowledgements+ CPG update, date of CPG

Strengths/ Limitations of E
6/30/2016 87

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E
10. Methods of Rs 11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)
Methods, CPG Development process same sections+ Rs, Key Evidence+ acknowledgements+ CPG update, date of CPG

Methods of Rs
6/30/2016 89

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E
10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process
same sections+ Rs, Key Evidence+ acknowledgements+ CPG update, date of CPG

Benefits, SE’s, Risks in Rs
6/30/2016 91

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E
10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process same sections
+ Rs, Key Evidence+ acknowledgements+ CPG update, date of CPG

Evidence Links (Rs-LoE)
6/30/2016 93

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E
10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review 14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process same sections+ Rs, Key Evidence
+ acknowledgements+ CPG update, date of CPG

External Review
6/30/2016 95

7. Systematic methods for E search
8. Selection Criteria of E
9. Strengths & Limitations of E
10. Methods of Rs
11. Benefits , side effect and risks in Rs
12. Evidence Links (Gs of Rs – LoE)
13. External Review
14. Update Procedure
DOMAIN 3. RIGOUR OF DEVELOPMENT
Methods, literature search strategy & appendices+ inclusion/ exclusion criteria+ Evidence tables, clinical evidence, evidence description (results), evidence interpretation (discussion)Methods, CPG Development process same sections+ Rs, Key Evidence+ acknowledgements
+ CPG update, date of CPG

Update procedure
6/30/2016 97

Domain 4

DOMAIN 4. CLARITY OF PRESENTATION
15. Rs are specific Rs & executive summary
16. Options for management + discussion, Treatment (options/alternatives)
17. Recommendation identifiableKey Rs; separate (e.g. QRG)

Rs are specific
6/30/2016 100

Options for management ((? IV IG))
6/30/2016 101

Rs are identifiable
6/30/2016 102

Domain 5

DOMAIN 5. APPLICABILITY
18. Facilitators & barriers CPG dissemination/ implementation, barriers, CPG utilization &
Quality indicators
19. Tools+ tools, resources, appendices
20. Resource implicationsMethod, cost utility, cost effectiveness, acquisition costs &
implications for budgets
21. Monitoring /audit criteria Rs, Quality indicators & audit criteria

Facilitators & Barriers
6/30/2016 105

Implementation Tools
6/30/2016 106

Resource implications
6/30/2016 107

Monitoring/ audit criteria
6/30/2016 108

Domain 6

DOMAIN 6. EDITORIAL INDEPENDENCE
22. Funding bodyDisclaimer & funding source
23. Competing interestsMethods, Conflicts of interest (COI), CPG panel &
appendices

Funding body
6/30/2016 111

DCOI
6/30/2016 112

Overall Assessment

OVERALL CPG ASSESSMENT1. Rate the overall quality of this CPG
2. I would recommend this CPG for use
3. Notes
YES
Yes ,with modification
No

6/30/2016 115


Selected CPG DomainsOverall
Is CPG
Recommended for
use ?1 2 3 4 5 6
CPG 1
CPG 2
CPG 3
CPG 4
CPG 5
Finally AGREE II Domain Scores Color Coding (Prof. Lubna Al-Ansary)
< 40 % Red >41-70 Yellow >71 Green

AGREE Domains Scores Table
CPG 1: SIGN CPG 2: EPR3 CPG 3: GINA CPG 4: ICSI CPG 5: Singapore MOH
Domain 1 60 % 74 % 45 % 61 % 42 %Domain 2 55 % 56 % 60 % 58 % 63 %
Domain 3 92 % 83 % 79 % 38 % 43 %
Domain 4 95 % 90 % 92 % 75 % 87 %Domain 5 70 % 82 % 80 % 33 % 58 %Domain 6 80 % 60 % 22 % 50 % 10 %Overall assessment 7 6 5 3 4Recommended for use Yes Yes (w M) Yes (w M) No No

Graphical Representation

AGREE II DOMAINS
(ENT-ABRS CPG)
IDSA CPG 2012 Canadian CPG 2011
D1: Scope & Purpose 86 % 80 %D2: Stakeholder Involvement 86 % 69 %D3: Rigour of Development 90 % 85 %D4: Clarity & Presentation 92 % 90 %D5: Applicability 67 % 64 %D6: Editorial Independence 96 % 76 %Overall assessment 7 5Recommended for use Yes No
This table uses the AGREE II Domain Score Colour Coding proposed by Dr. Lubna Alansary
(< 40% red - > 41 – 70% yellow - > 71 % green)

AGREE II DOMAINS CPG1 (Singapore) CPG2 (WFSBP) CPG3 (Canada)
D1: Scope & Purpose 90.7% 90.7% 96.3 %D2: Stakeholder Involvement 72.2% 65 % 81.5 %D3: Rigour of Development 39. 5% 84.5 % 90.3 %D4: Clarity & Presentation 98.1% 88.9 % 87.03 %D5: Applicability 34.7% 23.6% 40.3 %D6: Editorial Independence ZERO % 86.1% 55.6 %Overall assessment 4 5 6Recommended for use NO NO YES
This table uses the AGREE II Domain score colour coding proposed by Dr Lubna Al-Ansary
(< 40% Red - >41-70% Yellow - >71% Green)

The paper tool (handout!)

Using the AGREE II Instrument 123

AGREE II rater concordance calculator (EXCEL)

AGREE II rater concordance calculator(McMaster University)





The online tool “My AGREE PLUS”

My AGREE PLUS(OR Our AGREE!)

My AGREE II Report PDF


A tool for evaluation of clinical validity/ credibility of CPGs (in progress)

AGREE-REX: Recommendation EXcellence:Innovations to enhance the capacity of practice guidelines to
improve health and health care systems
Develop a useful, reliable, and valid knowledge resource tocomplement the AGREE II, which will guide the development,reporting, and evaluation of the clinical credibility of CPGrecommendations.
Volunteers Needed for AGREE-REX Testing
April 2016

Other AGREE Resources
• AGREE Reporting Checklist (PDF, Word)Brouwers MC, Kerkvliet K, Spithoff K, on behalf of the AGREE Next Steps Consortium. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ 2016;352:i1152. doi: 10.1136/bmj.i1152.
A checklist based on the domains and items of the AGREE II intended to assist in the completeness of reporting in practice guidelines.
• AGREE II-GRS InstrumentA short item tool to evaluate the quality and reporting of practice guidelines. Get the AGREE II-GRS here.
6/30/2016 136

CPG Implementation
“The concrete activities and interventions undertaken to turn policies into desired results“
Guidelines for clinical practice: from development to use. IOM, 1992
CPGs Practice
6/30/2016 137

CPG Implementability
Set of characteristics that PREDICT the relative ease of implementation of CPG recommendations.
Implementability…….BEFORE implementation
6/30/2016 138

CPG implementation Strategies (SIGN)
Dissemination Process (print/ e-/website).
Local Clinical Champions.
Awareness raising/ training activities.
Regular M & E (Auditing) (The ‘living’ CPG concept!).
Networking and linking with existing projects (e.g. Dept. Clinical Rounds, CPD/CME activities, Accreditation, etc..).
Patients as champions for change.
1396/30/2016

CPG implementation Toolsavailable at the point of care (* MR)
Examples
1.Clinical Algorithm
2. Integrated Care/ Clinical Pathways
3.Protocol and/ or Policy & Procedure
4.Chart Documentation/ forms (e.g. Physician Order Sets: eSIHI
CPOE PowerPlans)
5.Quick Reference Guides/ Physician Guides & Pocket
Guide/Reference Cards (at-a-glance summary of key
recommendations 5 or 1-2 pages).
1406/30/2016

1.Clinical audit criteria (tool)
2.Quality (outcome/performance) measures
3.Slide Presentation.
4.Wall Poster.
5.Patient Resources/ Information (health education guides).
6.Foreign language Translation (Non-English, Non-Arabic).
7.Implementation Tool Kits (collections of tools and/or strategies).
8.Staff Training/ Competency Material.
CPG implementation tools (cont’d)
6/30/2016 141

Mobile Apps
6/30/2016 142

Individual Positive attitude Learning through small
group interaction
Environmental• Professional
association/society support• Inter-organizational
collaboration networks
Facilitators
Organizational• Leadership support• Champions• Team work
collaboration
6/30/2016 143

CPG Implementation Failure….WHY?
Extrinsic to CPG:
provider & care system-related
Intrinsic to CPG:
ambiguity – inconsistency - incompleteness
6/30/2016 144

6/30/2016 145

6/30/2016 146
The concept of
the ‘LIVING’ CPG

CPG Adaptation ProgramCurrent status 2016 - 1437
6/30/2016 147

Clinical Practice Guidelines (CPGs) Adaptation
Program at King Saud University Medical City
KSUMC CPG Program Partners:-
KSUMC-Wide CPGs Steering Committee
Clinical Department(s); CPGs Dept. Committees)
Research Chair for Evidence-Based Health Care &Knowledge Translation
Quality Management Department; DQTs
Top Management of KSUMC; Medical Director(s), Dept. Chairperson(s), Unit Head(s)
IMPLEMENTQIP
ADAPTMethods
6/30/2016 148

Guidelines International Network (G-I-N)www.g-i-n.net
EBHC-KT Chair, King Saud University: Org. Member
since 2009
(1st Member from Gulf & 3rd Member from MENA
Countries)
Founded in Nov.
2002
6/30/2016 149

23 KSUMC CPGs Subcommittees1. Department of Pediatrics
2. Department of Critical Care
3. Department of Psychiatry
4. Primary Care/ Family Medicine Clinics
5. Department of Pharmacy
6. Department of Emergency Medicine
7. Department of Medicine
8. Department of Orthopedic Surgery
9. Department of Otorhinolaryngology
10. Department of Ophthalmology
11. Department of Cardiac Sciences/ KFCC
12. Department of Surgery
13. Department of Obstetrics & Gynecology
14. Department of Dermatology
15. Department of Anesthesiology
16. Department of Laboratory Medicine &
Pathology
17. Department of Nursing
18. Department of Radiology
19. Health Education Center
20. Department of Rehabilitation Medicine
21. Department of Infection Control
22. Department of Occupational Health & Safety
23. Department of Clinical Nutrition
1506/30/2016

How to access the KSUMC CPGs?
• PAPER1. CPG Binder (full document)
2. Forms (Implementation tools)
3. Algorithm Booklet
• ELECTRONICOnline:1. ICity website (KSU email)
2. G-I-N website (EBHCKT)
Offline: (intranet)Desktop Icon (IP Address?)
PARADIGMSHIFT: eSiHi
6/30/2016 151

How to access CPGs on Intranet City (ICity)
6/30/2016 152

Desktop Icon
6/30/2016 153

6/30/2016 154

Type: MED
6/30/2016 155

6/30/2016 156
Currently, 18 out of the 29 adapted CPGs are already built on eSiHi as ‘CPOE with Order Sets’ (i.e. Cerner POWERPLANS). The rest are in progress!

5 PowerPlans from Medicine CPGs
1. MED Diabetic Ketoacidosis CPG (adults)
2. MED Gout CPG
3. MED Hypertensive emergencies/urgencies CPG
4. MED oncology premedication
5. PULM Asthma CPG (adults)
6/30/2016 157

1 from DEM/ ICU CPGsED septic shock (adults)
1 from Cardiology (KFCC) CPGsCARD Heart Failure CPG
6/30/2016 158

6/30/2016 159
29
KSUMC CPG PROGRAM IN NUMBERS

Who is the contact person for EBCPGs in each clinical department?
Chairperson, CPG Departmental Committee
Members, CPG Departmental Committee
Department Quality Team (former Accreditation teams)
Department Chairman & Units’ Heads
General Coordinator, CPG Steering Committee
Medical Secretary, CPG Steering Committee
6/30/2016 160

6/30/2016 161

Medicine (6 +5)
6/30/2016 162
1. Asthma (Adult)
2. Diabetic ketoacidosis (Adult)
3. Hypertensive emergencies & urgencies
4. Gout (acute gouty arthritis/ hyperuricemia)
5. Lung Cancer
6. Antiemetics for Chemotherapy-induces nausea & vomiting
7. Venous Thromboembolism Prophylaxis
8. Dyslipidemia
9. Vancomycin dosing and monitoring (Adult)
10. Surgical Antibiotic prophylaxis (Adult)
11. Heart Failure (Adult)

Pharmacy Services (3)
6/30/2016 163
• Vancomycin dosing and monitoring (Adult)
• Pediatric and neonatal parenteral nutrition (TPN)
• Antiemetics for Chemotherapy-induces nausea & vomiting

How to read the KSUMC CPGs full documents?
Table of contents
• Preface by authors
• Acknowledgments
• Abbreviations
• Overview material
• Introduction
• Disclaimer/
Statement of intent
• Scope & Purpose (PIPOH)
• Recommendations (Key & details)
• External review & consensus
• Plan for scheduled review & update
• List of funding sources
• Adaptation process methodology
• Implementation considerations & Tools
• References
1646/30/2016

Role as a Physician in CPGs
1) CPG implementers/users:
“Your continuous feedback!”
2) CPG developers/adapters.
3) Improvement research projects.
6/30/2016 165
