cancer immunology and immunotherapy center st. savas cancer hospital towards new approaches for...
TRANSCRIPT
Cancer Immunology and Immunotherapy CenterSt. Savas Cancer Hospital
Towards new approaches for cancer immunotherapyTowards new approaches for cancer immunotherapy
Constantin N. Baxevanis
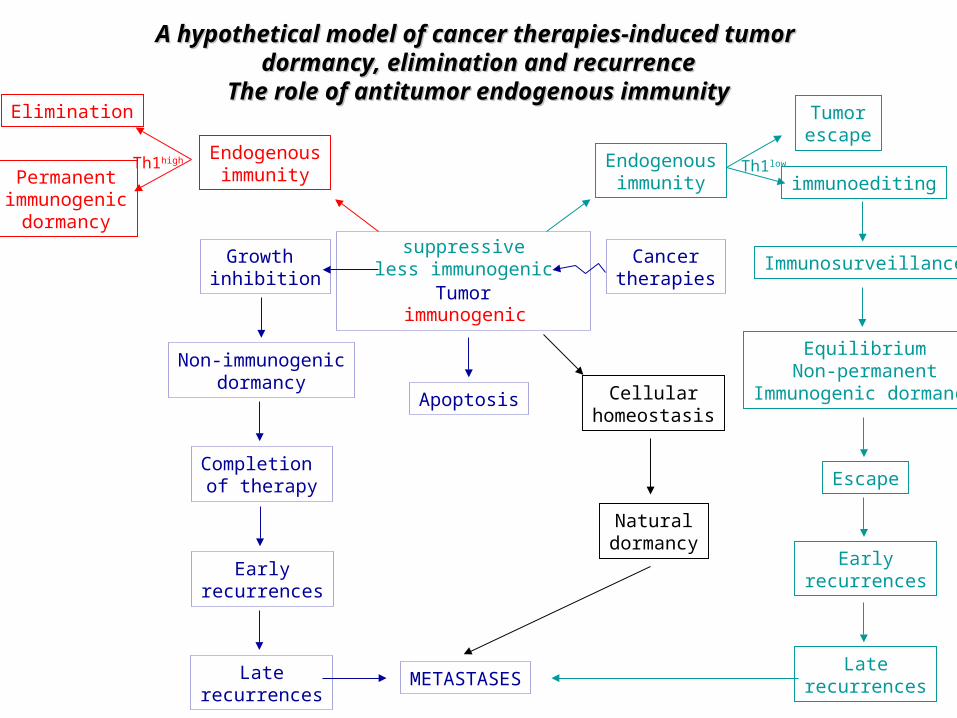
A hypothetical model of cancer therapies-induced tumor A hypothetical model of cancer therapies-induced tumor dormancy, elimination and recurrencedormancy, elimination and recurrence
The role of antitumor endogenous immunityThe role of antitumor endogenous immunity
Tumor
Growth inhibition
Non-immunogenicdormancy
Completion of therapy
Earlyrecurrences
Laterecurrences
METASTASES
Apoptosis
Cancertherapies
immunogenic
EndogenousimmunityPermanent
immunogenicdormancy
Th1high
Elimination
suppressiveless immunogenic
Endogenousimmunity immunoediting
Th1low
Immunosurveillance
EquilibriumNon-permanent
Immunogenic dormancy
Escape
Earlyrecurrences
Laterecurrences
Cellularhomeostasis
Naturaldormancy
Tumorescape
Epigenetic changes
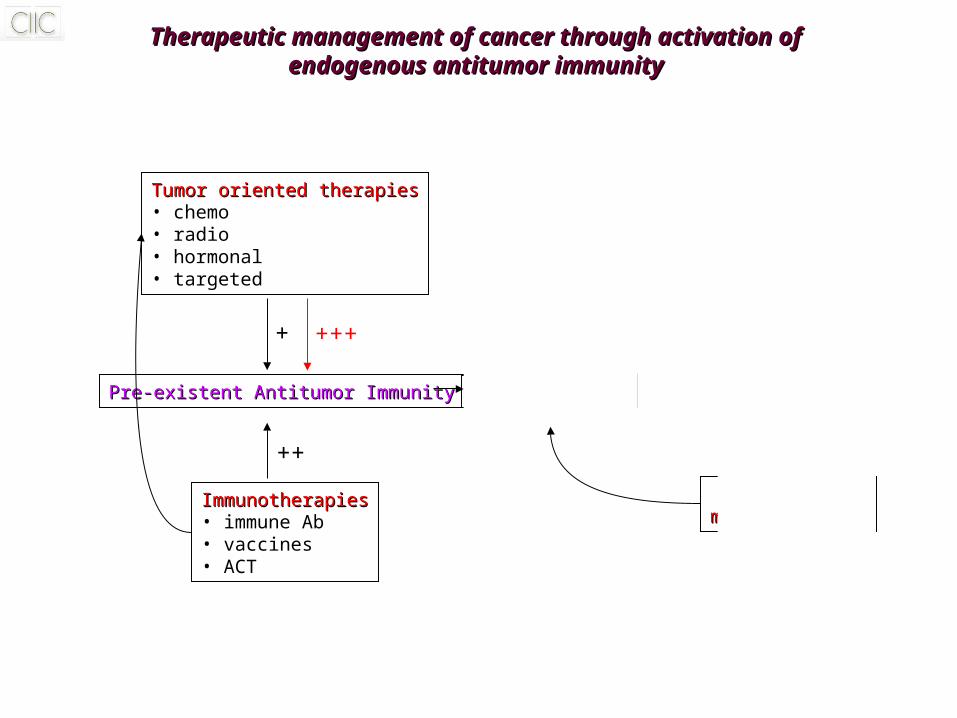
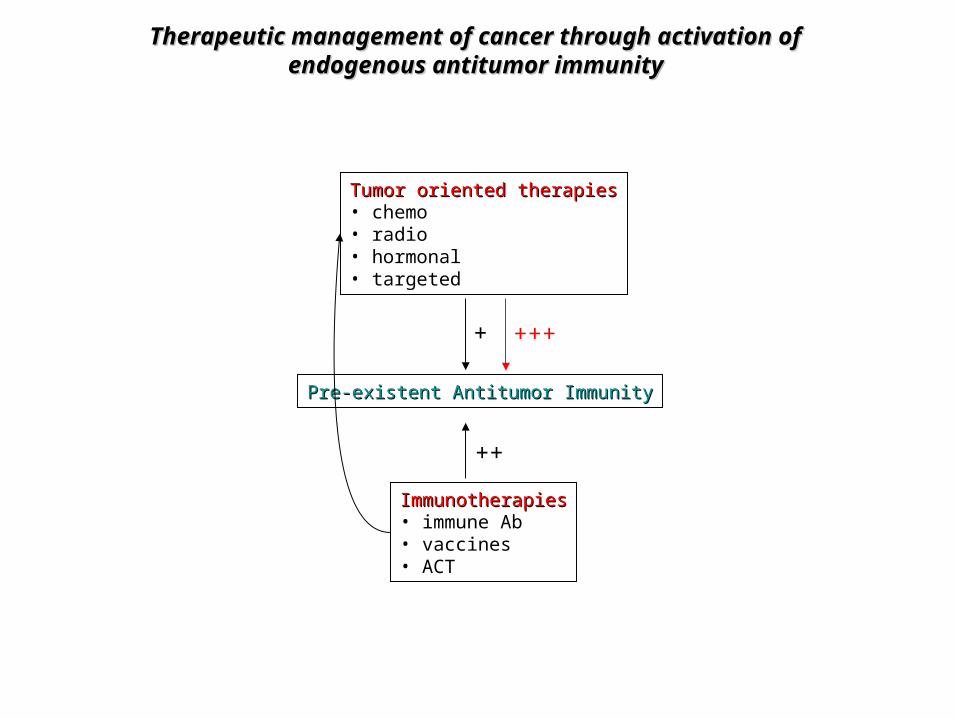
Therapeutic management of cancer through activation ofTherapeutic management of cancer through activation ofendogenous antitumor immunityendogenous antitumor immunity
Tumor oriented therapiesTumor oriented therapies• chemo• radio• hormonal• targeted
Pre-existent Antitumor ImmunityPre-existent Antitumor Immunity
ImmunotherapiesImmunotherapies• immune Ab• vaccines• ACT
+ +++
++
Tumor dormancyTumor dormancy escapeescape
ClinicalClinicalmanifestationsmanifestations
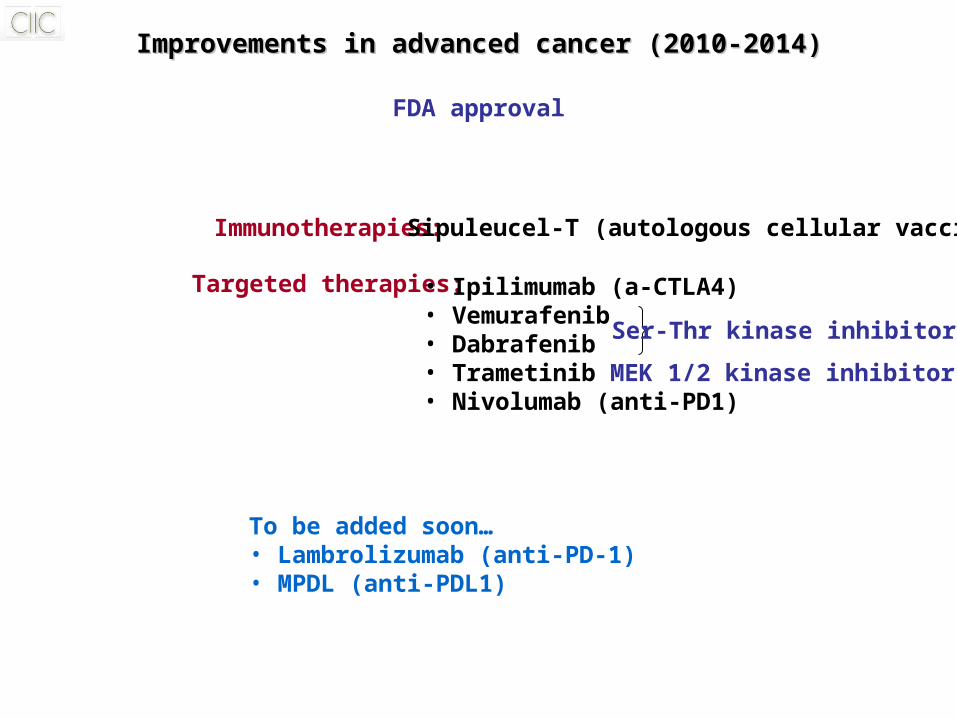
Improvements in advanced cancer (2010-2014)Improvements in advanced cancer (2010-2014)
Targeted therapies: • Ipilimumab (a-CTLA4)• Vemurafenib• Dabrafenib• Trametinib MEK 1/2 kinase inhibitor• Nivolumab (anti-PD1)
Ser-Thr kinase inhibitors
FDA approval
Immunotherapies: Sipuleucel-T (autologous cellular vaccine)
To be added soon…• Lambrolizumab (anti-PD-1)• MPDL (anti-PDL1)
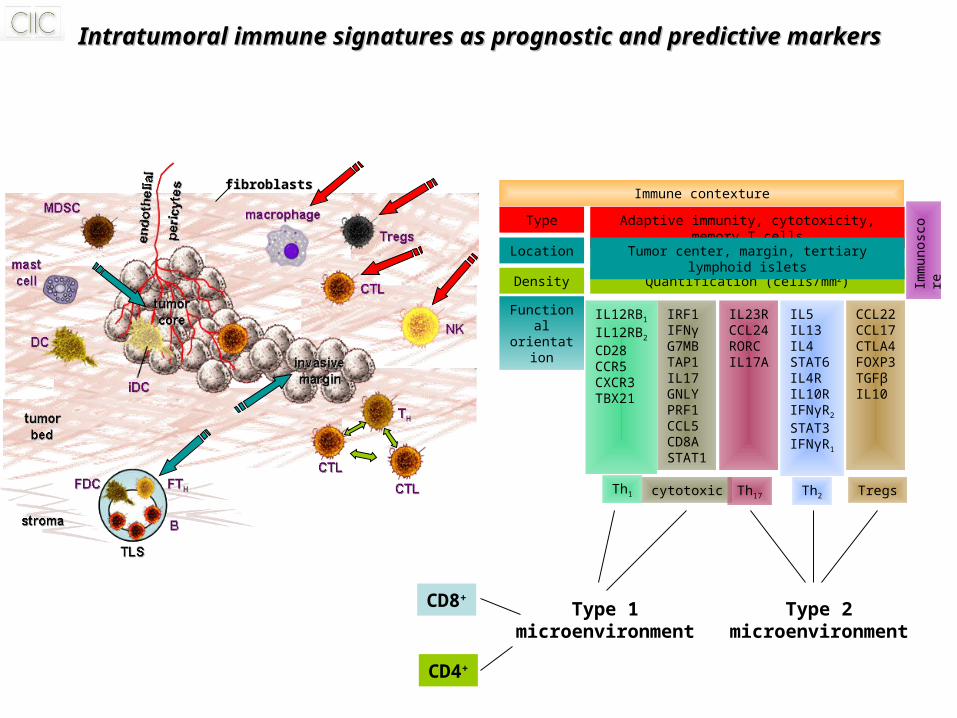
Intratumoral immune signatures as prognostic and predictive markersIntratumoral immune signatures as prognostic and predictive markers
Immune contexture
Location
Density
Type Adaptive immunity, cytotoxicity, memory T cells
Quantification (cells/mm2)
Tumor center, margin, tertiary lymphoid islets
Functionalorientation
IL12RB1
IL12RB2
CD28CCR5CXCR3TBX21
IRF1IFNγG7MBTAP1IL17GNLYPRF1CCL5CD8ASTAT1
IL23RCCL24RORCIL17A
IL5IL13IL4STAT6IL4RIL10RIFNγR2
STAT3IFNγR1
CCL22CCL17CTLA4FOXP3TGFβIL10
Th1 cytotoxic Th17 Th2 Tregs
Imm
unos
core
fibroblastsfibroblasts
Type 1microenvironment
CD8+
CD4+
Type 2microenvironment
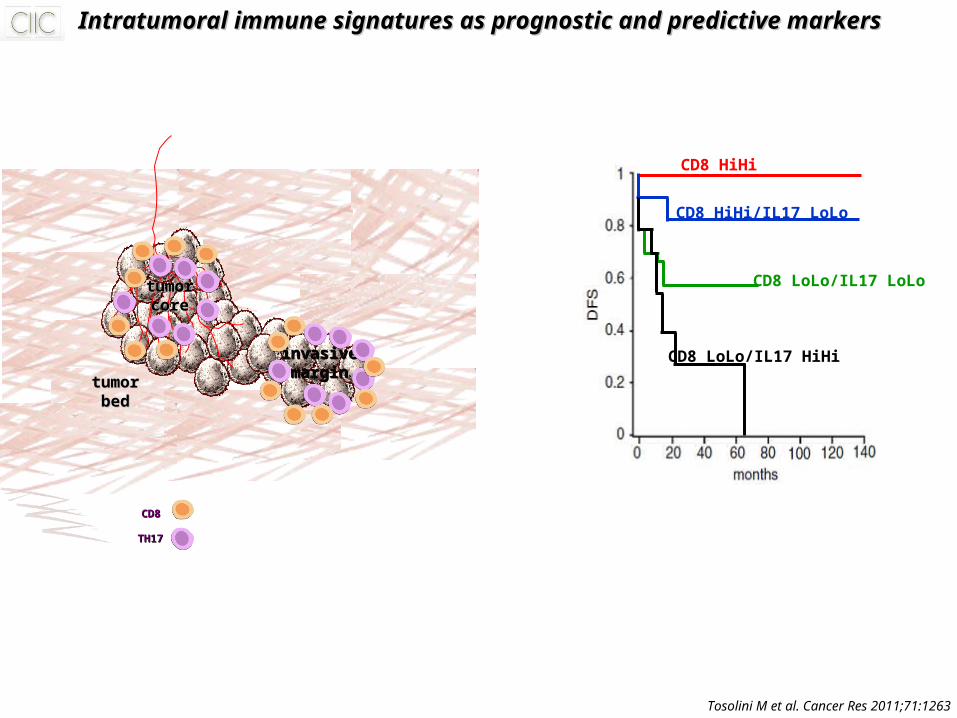
Intratumoral immune signatures as prognostic and predictive markersIntratumoral immune signatures as prognostic and predictive markers
tumortumorcorecore
invasiveinvasivemarginmargin
tumortumorbedbed
CD8CD8
TH17TH17
CD8 HiHi
CD8 HiHi/IL17 LoLo
CD8 LoLo/IL17 HiHi
CD8 LoLo/IL17 LoLo
Tosolini M et al. Cancer Res 2011;71:1263
Therapeutic management of cancer through activation ofTherapeutic management of cancer through activation ofendogenous antitumor immunityendogenous antitumor immunity
Tumor oriented therapiesTumor oriented therapies• chemo• radio• hormonal• targeted
Pre-existent Antitumor ImmunityPre-existent Antitumor Immunity
ImmunotherapiesImmunotherapies• immune Ab• vaccines• ACT
+ +++
++
Targeted therapies to potentiate the Targeted therapies to potentiate the endogenous antitumor immunityendogenous antitumor immunity
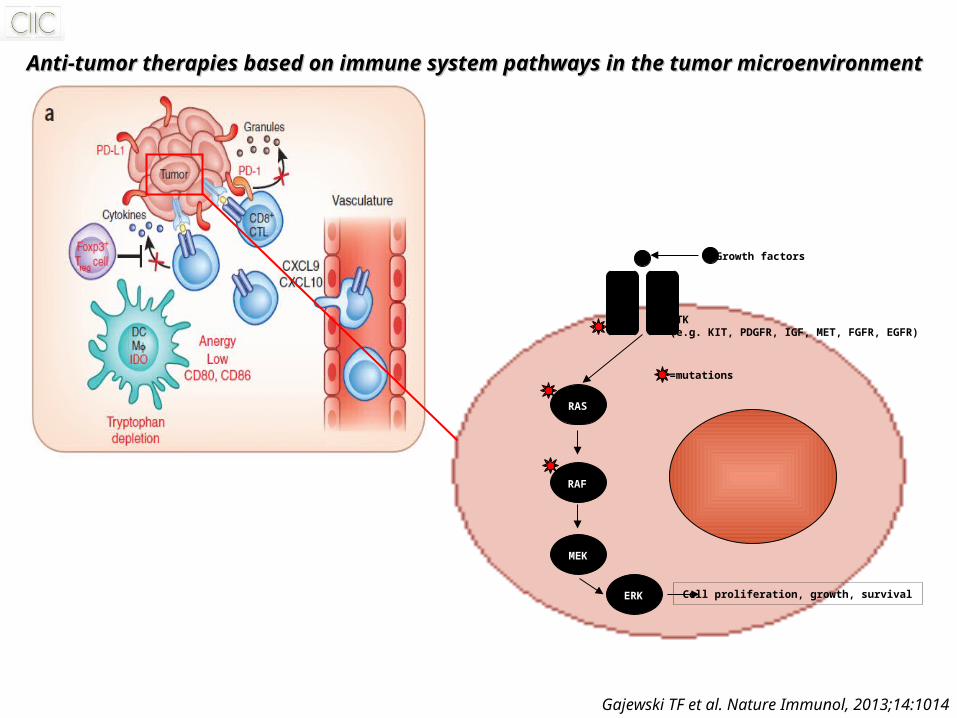
Growth factors
RTK(e.g. KIT, PDGFR, IGF, MET, FGFR, EGFR)
RAS
RAF
MEK
ERK Cell proliferation, growth, survival
=mutations
Gajewski TF et al. Nature Immunol, 2013;14:1014
Anti-tumor therapies based on immune system pathways in the tumor microenvironmentAnti-tumor therapies based on immune system pathways in the tumor microenvironment
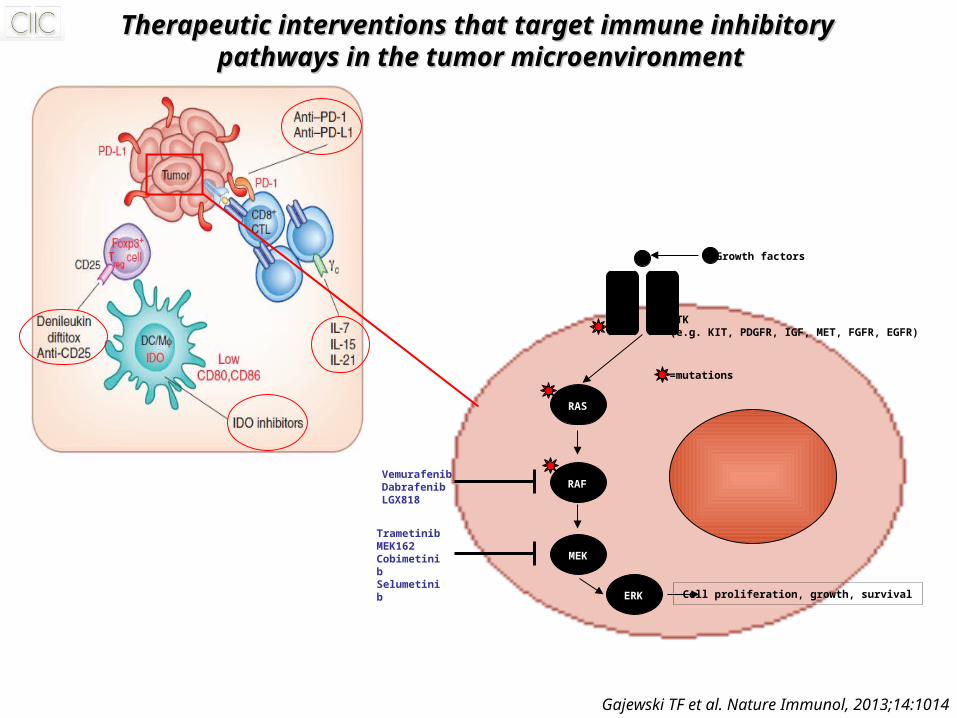
Therapeutic interventions that target immune inhibitory Therapeutic interventions that target immune inhibitory pathways in the tumor microenvironmentpathways in the tumor microenvironment
Gajewski TF et al. Nature Immunol, 2013;14:1014
Growth factors
RTK(e.g. KIT, PDGFR, IGF, MET, FGFR, EGFR)
RAS
RAF
MEK
ERK Cell proliferation, growth, survival
=mutations
VemurafenibDabrafenibLGX818
TrametinibMEK162CobimetinibSelumetinib
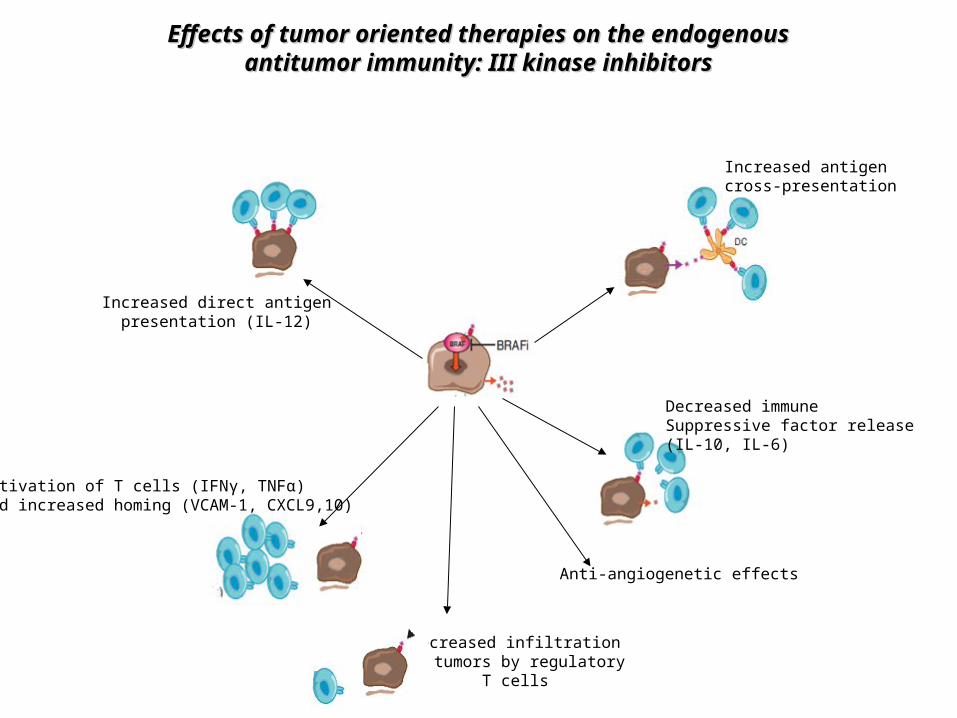
Effects of tumor oriented therapies on the endogenousEffects of tumor oriented therapies on the endogenousantitumor immunity: III kinase inhibitorsantitumor immunity: III kinase inhibitors
Increased direct antigenpresentation (IL-12)
Decreased immuneSuppressive factor release(IL-10, IL-6)
Anti-angiogenetic effects
Decreased infiltrationof tumors by regulatory
T cells
Activation of T cells (IFNγ, TNFα)and increased homing (VCAM-1, CXCL9,10)
Increased antigencross-presentation
Conventional therapies to potentiate the Conventional therapies to potentiate the endogenous antitumor immunityendogenous antitumor immunity
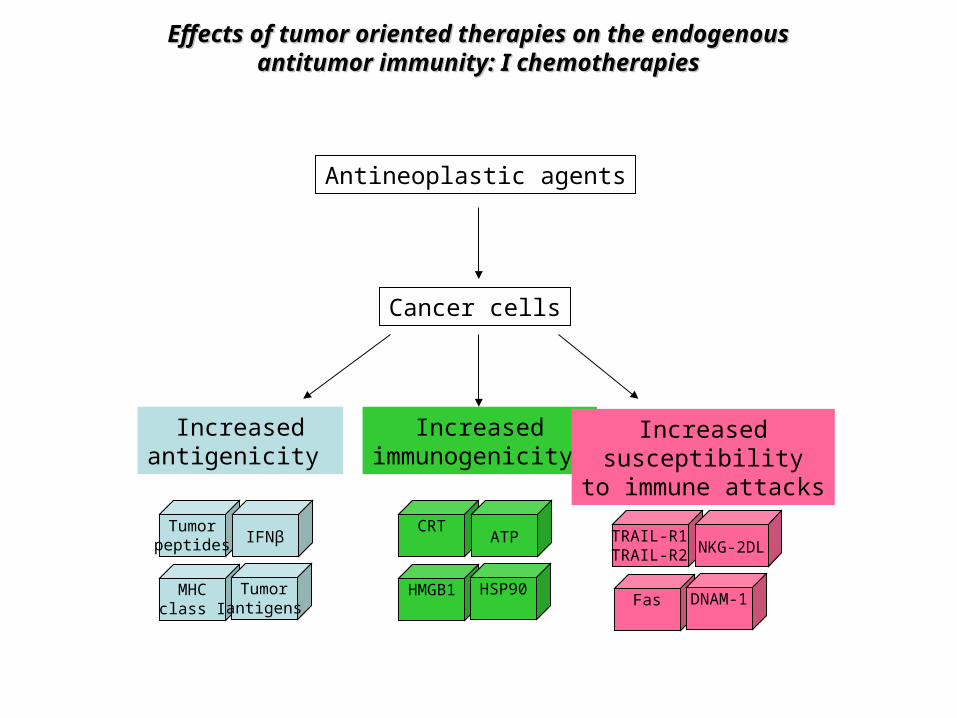
Effects of tumor oriented therapies on the endogenousEffects of tumor oriented therapies on the endogenousantitumor immunity: I chemotherapiesantitumor immunity: I chemotherapies
Antineoplastic agents
Cancer cells
Increasedantigenicity
Tumorpeptides IFNβ
MHCclass I
Tumorantigens
Increasedimmunogenicity
CRTATP
HMGB1 HSP90
Increasedsusceptibility
to immune attacks
TRAIL-R1TRAIL-R2 NKG-2DL
Fas DNAM-1
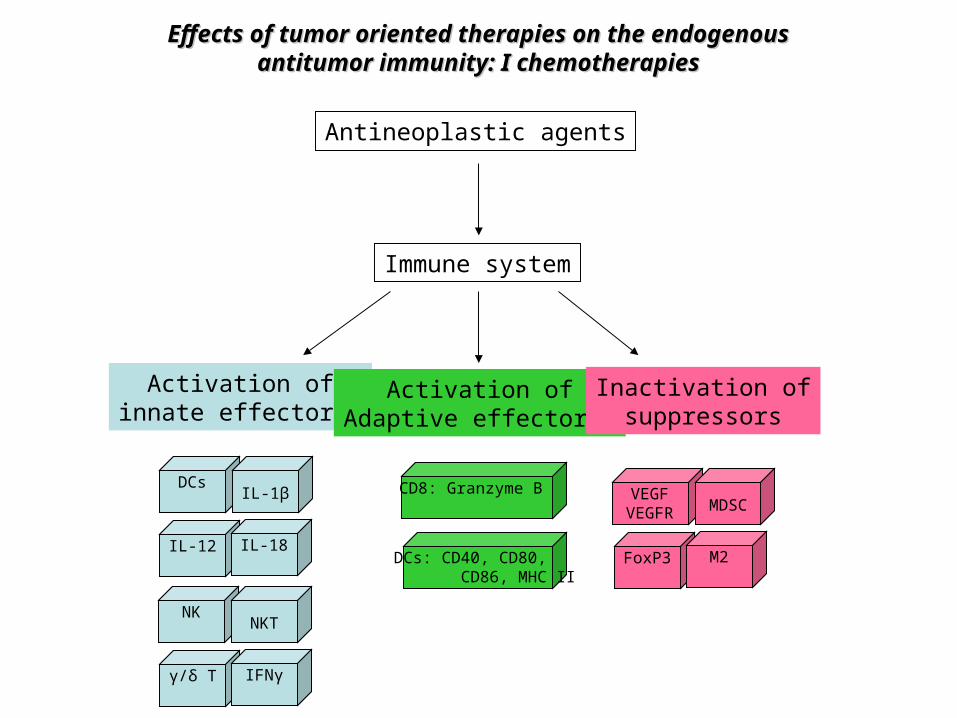
Effects of tumor oriented therapies on the endogenousEffects of tumor oriented therapies on the endogenousantitumor immunity: I chemotherapiesantitumor immunity: I chemotherapies
Antineoplastic agents
Immune system
Activation ofinnate effectors
DCsIL-1β
IL-12 IL-18
Activation ofAdaptive effectors
CD8: Granzyme B
DCs: CD40, CD80, CD86, MHC II
Inactivation ofsuppressors
VEGFVEGFR MDSC
FoxP3 M2
NKNKT
γ/δ T IFNγ
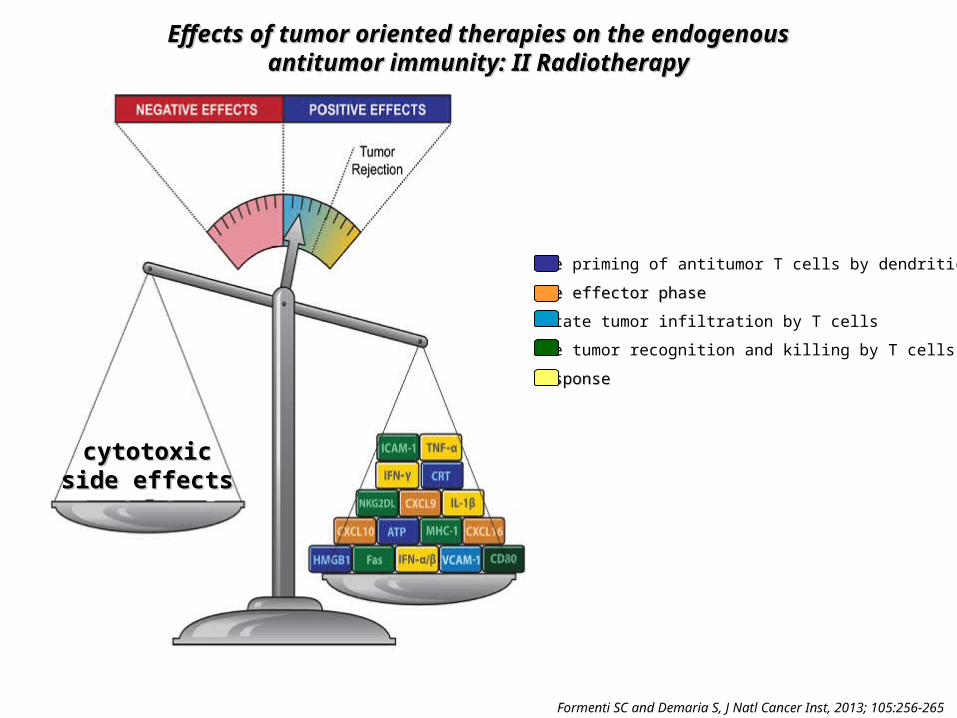
Effects of tumor oriented therapies on the endogenousEffects of tumor oriented therapies on the endogenousantitumor immunity: II Radiotherapyantitumor immunity: II Radiotherapy
Formenti SC and Demaria S, J Natl Cancer Inst, 2013; 105:256-265
Promote priming of antitumor T cells by dendritic cells
PromotPromotee effector phase effector phase
Facilitate tumor infiltration by T cells
Improve tumor recognition and killing by T cells
Th1 responseTh1 response
cytotoxiccytotoxicside effectsside effects
Immunotherapies to potentiate the Immunotherapies to potentiate the endogenous antitumor immunityendogenous antitumor immunity
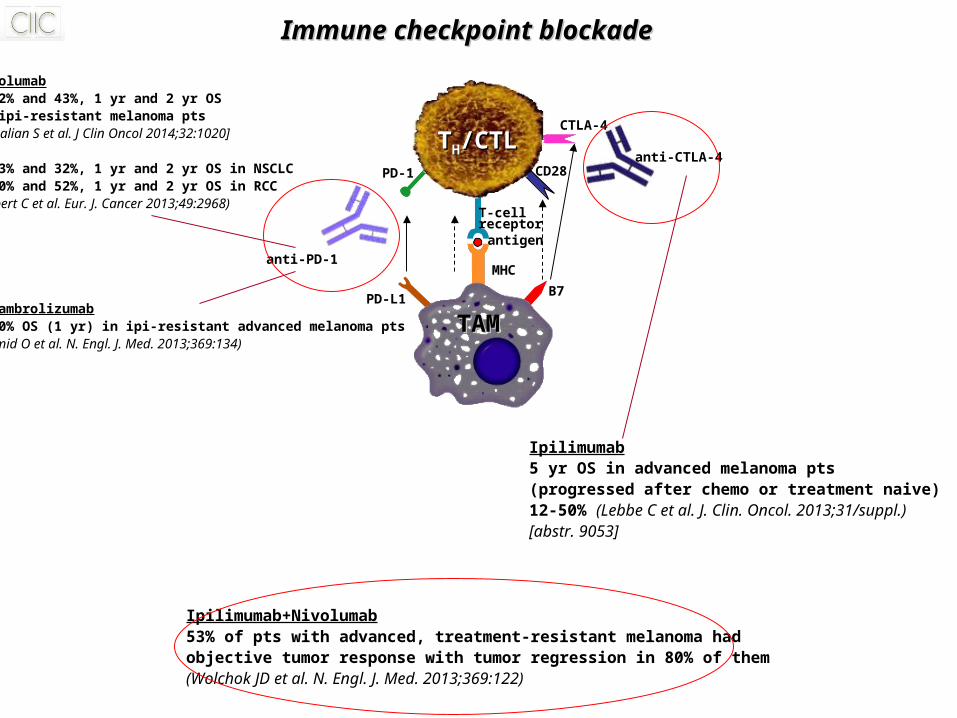
T-cellreceptor
antigen
MHC
CTLA-4
CD28
TAMTAM
B7PD-L1
PD-1anti-CTLA-4
anti-PD-1
Ipilimumab5 yr OS in advanced melanoma pts(progressed after chemo or treatment naive)12-50% (Lebbe C et al. J. Clin. Oncol. 2013;31/suppl.)[abstr. 9053]
Nivolumab• 62% and 43%, 1 yr and 2 yr OSin ipi-resistant melanoma pts(Topalian S et al. J Clin Oncol 2014;32:1020]
• 43% and 32%, 1 yr and 2 yr OS in NSCLC 70% and 52%, 1 yr and 2 yr OS in RCC(Robert C et al. Eur. J. Cancer 2013;49:2968)
• Lambrolizumab 50% OS (1 yr) in ipi-resistant advanced melanoma pts(Hamid O et al. N. Engl. J. Med. 2013;369:134)
Ipilimumab+Nivolumab53% of pts with advanced, treatment-resistant melanoma had objective tumor response with tumor regression in 80% of them(Wolchok JD et al. N. Engl. J. Med. 2013;369:122)
Immune checkpoint blockadeImmune checkpoint blockade
TTHH/CTL/CTL
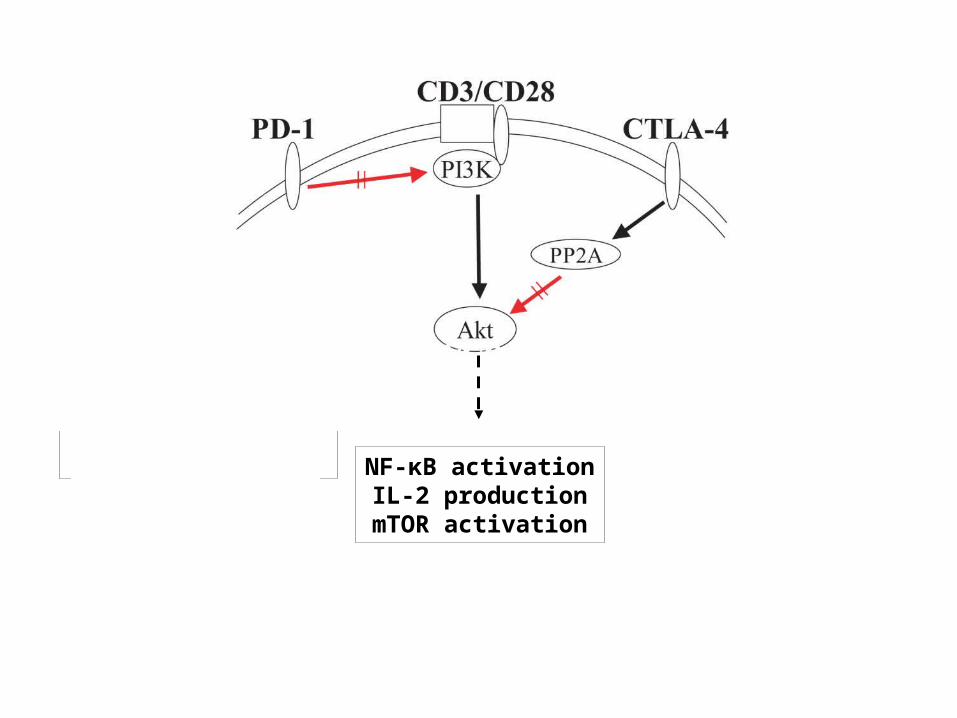
cell proliferationgrowthsurvival NF-κB activation
IL-2 productionmTOR activation
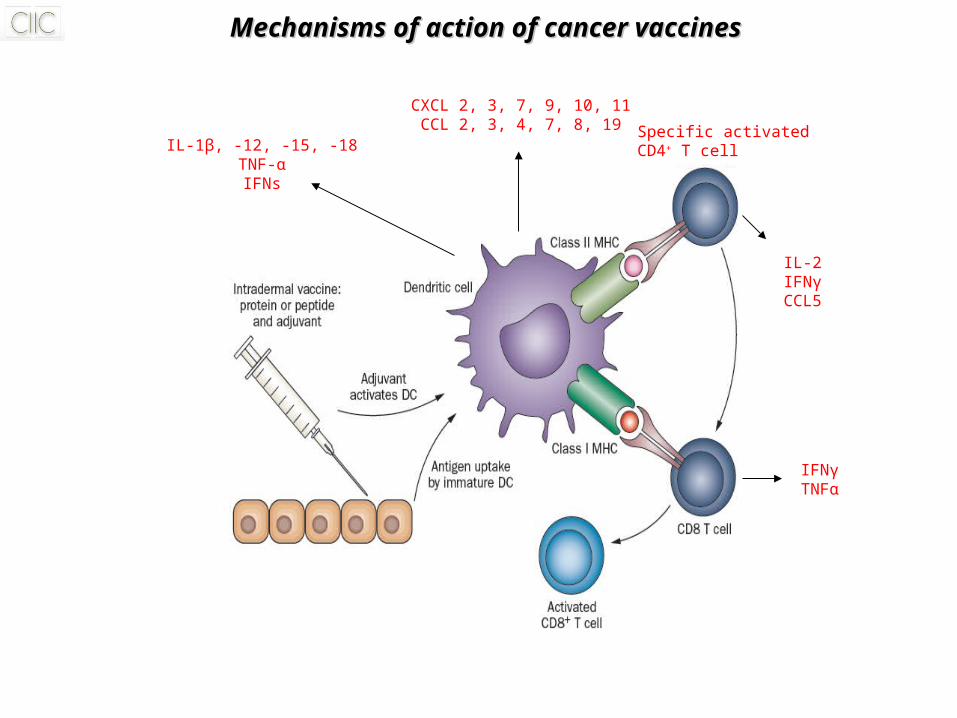
Mechanisms of action of cancer vaccinesMechanisms of action of cancer vaccines
IL-1β, -12, -15, -18TNF-αIFNs
CXCL 2, 3, 7, 9, 10, 11CCL 2, 3, 4, 7, 8, 19 Specific activated
CD4+ T cell
IL-2IFNγCCL5
IFNγTNFα
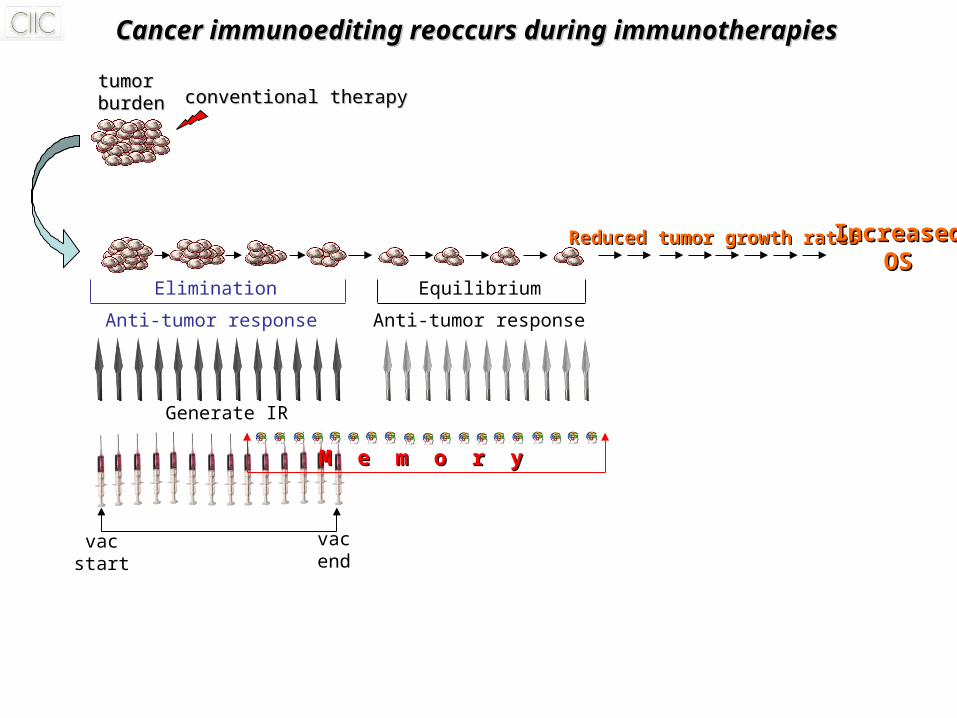
Cancer immunoediting reoccurs during immunotherapiesCancer immunoediting reoccurs during immunotherapies
vacstart
vacend
Generate IR
Equilibrium
Anti-tumor response
Reduced tumor growth ratesReduced tumor growth rates IncreasedIncreasedOSOS
M e m o r yM e m o r y
Anti-tumor response
Elimination
tumortumorburdenburden conventional therapyconventional therapy
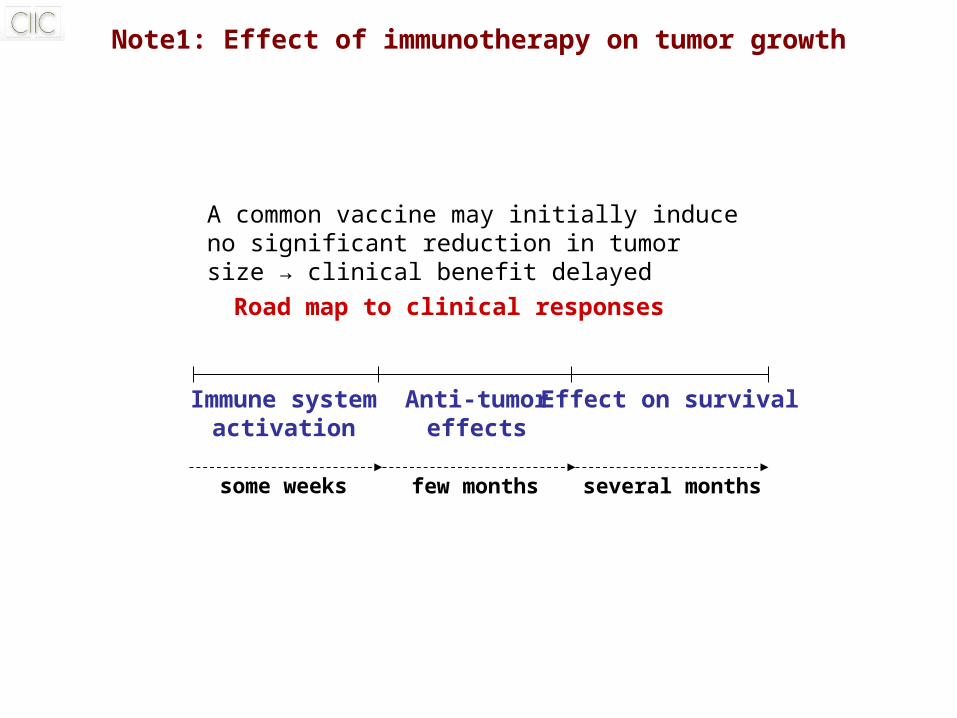
Note1: Effect of immunotherapy on tumor growth
A common vaccine may initially induce no significant reduction in tumor size → clinical benefit delayed
Road map to clinical responses
Immune systemactivation
Anti-tumoreffects
Effect on survival
some weeks few months several months
Note2: Patient selection in immunotherapy trials
Phase III trials have shown that immunotherapies are
less effective in patients with heavy disease burden
providing a biologic rationale for using
therapeutic vaccines earlier in disease process
Patients with progressive cancers may not have time to
develop a significant immune response and derive
benefit from treatment
Note3: Identifying intermediate endpoints in immunotherapy
Biomarkers to evaluate biologic response in the
absence of clinical response are needed• Cellular immune responses• Humoral immune responses
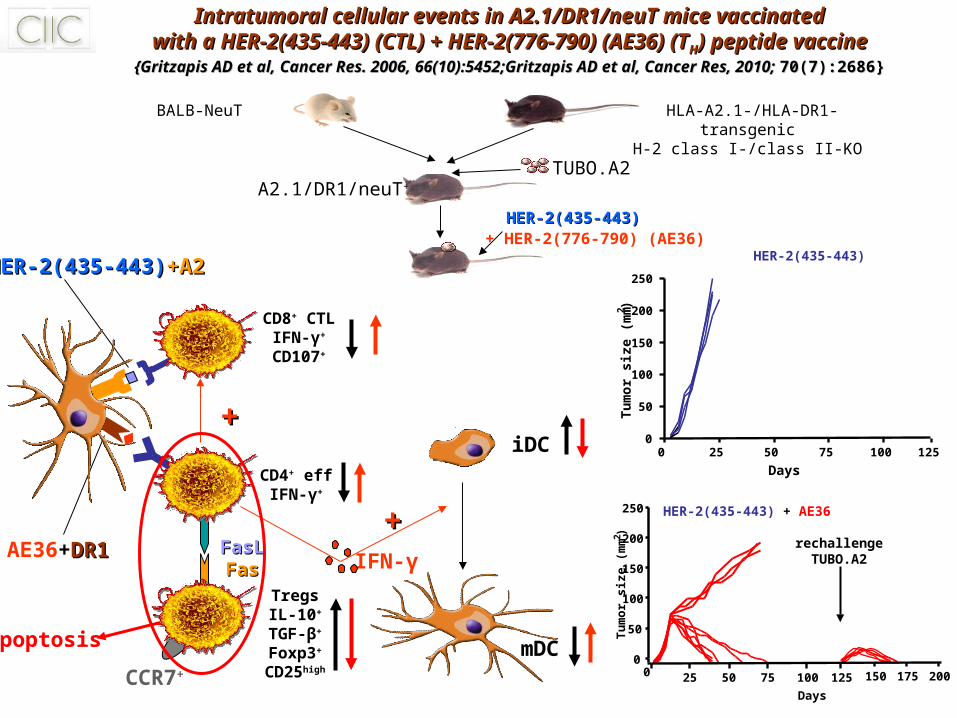
Intratumoral cellular events in A2.1/DR1/neuT mice vaccinatedIntratumoral cellular events in A2.1/DR1/neuT mice vaccinatedwith a HER-2(435-443) (CTL) + HER-2(776-790) (AE36) (Twith a HER-2(435-443) (CTL) + HER-2(776-790) (AE36) (THH) peptide vaccine) peptide vaccine
{Gritzapis AD et al, {Gritzapis AD et al, Cancer Res. 2006Cancer Res. 2006, , 66(10):545266(10):5452;Gritzapis AD et al, Cancer Res, 2010; ;Gritzapis AD et al, Cancer Res, 2010; 70(7):268670(7):2686}}
APC
AE36+DR1DR1
HER-2(435-443)HER-2(435-443)+A2+A2
iDC
CD8+ CTLIFN-γ+
CD107+
CD4+ effIFN-γ+
++
FasLFasLFasFas
TregsIL-10+
TGF-β+
Foxp3+
CD25high
mDC
IFN-γ
++
CCR7+
A2.1/DR1/neuT+
TUBO.A2
BALB-NeuT HLA-A2.1-/HLA-DR1-transgenic H-2 class I-/class II-KO
HER-2(435-443)HER-2(435-443)+ HER-2(776-790) (AE36)
apoptosis
HER-2(435-443)
0 25 50 75 1251000
50
100
150
200
250
Days
Tu
mo
r si
ze (
mm
2)
2
HER-2(435-443) + AE36
00
50
100
150
200
250
Days
Tu
mo
r si
ze (
mm
)
25 50 75 125100 150 175 200
rechallengeTUBO.A2
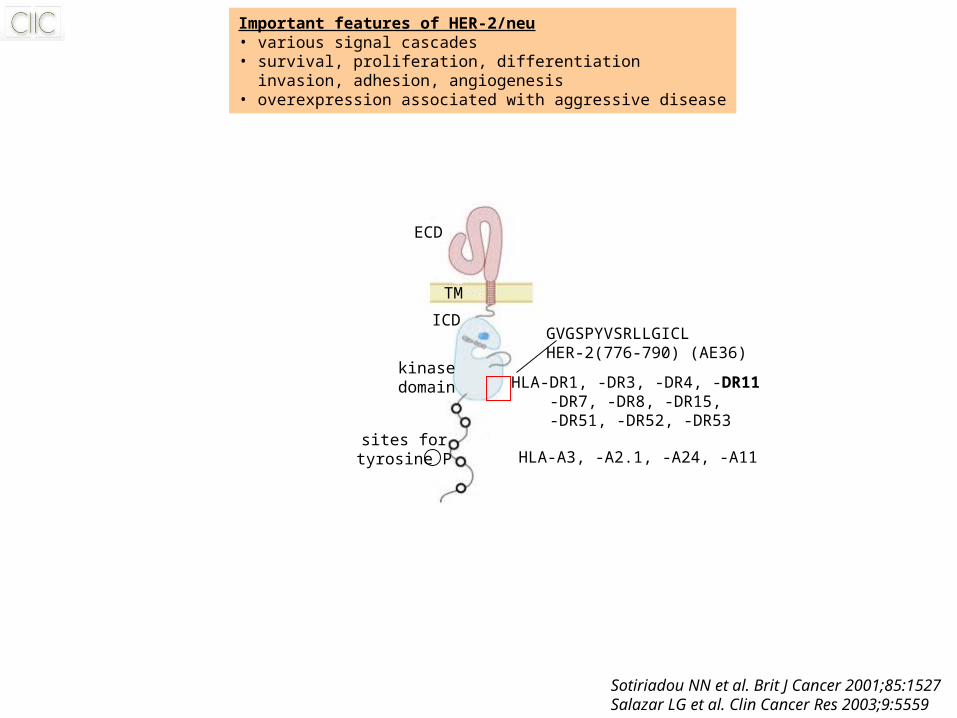
Important features of HER-2/neu• various signal cascades• survival, proliferation, differentiation invasion, adhesion, angiogenesis• overexpression associated with aggressive disease
ECD
TM
ICD
kinasedomain
sites fortyrosine P
GVGSPYVSRLLGICLHER-2(776-790) (AE36)
HLA-A3, -A2.1, -A24, -A11
HLA-DR1, -DR3, -DR4, -DR11 -DR7, -DR8, -DR15,
-DR51, -DR52, -DR53
Sotiriadou NN et al. Brit J Cancer 2001;85:1527Salazar LG et al. Clin Cancer Res 2003;9:5559
CD4+
CD8+
IL-2IL-2
IFN-IFN-γγ
+
perforinperforin
GZGZ
XX
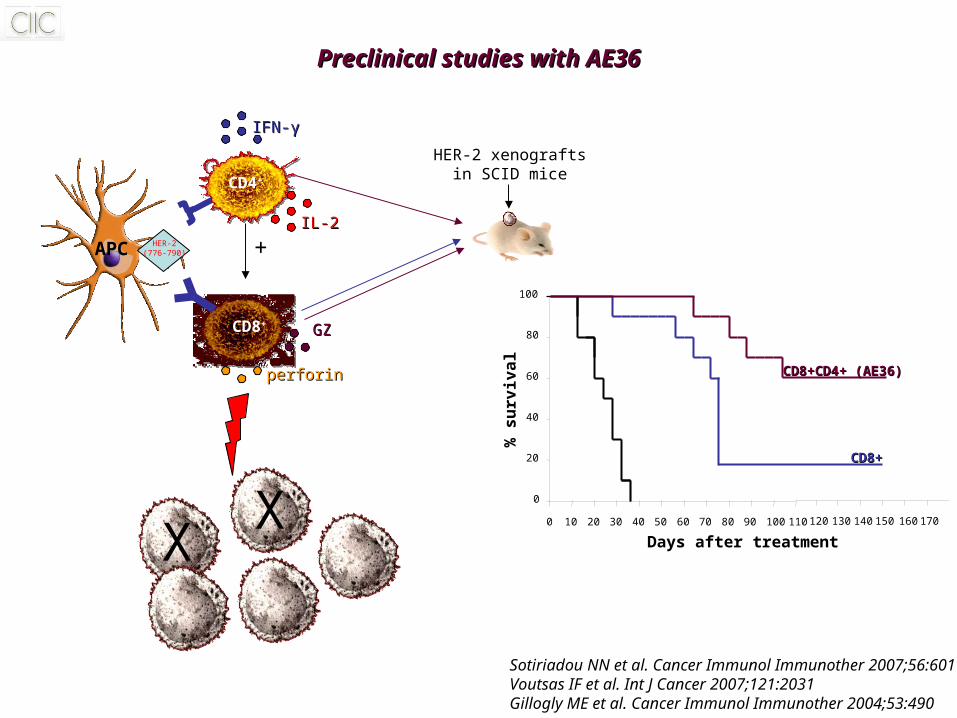
HER-2 xenograftsin SCID mice
% s
urv
ival
0
Days after treatment
0
20
40
60
80
100
10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170
APC HER-2(776-790)
Preclinical studies with AE36Preclinical studies with AE36
CD8+CD4+ (AE36)CD8+CD4+ (AE36)
CD8+CD8+
Sotiriadou NN et al. Cancer Immunol Immunother 2007;56:601Voutsas IF et al. Int J Cancer 2007;121:2031Gillogly ME et al. Cancer Immunol Immunother 2004;53:490
Vaccinating prostate cancer patients with AE37Vaccinating prostate cancer patients with AE37
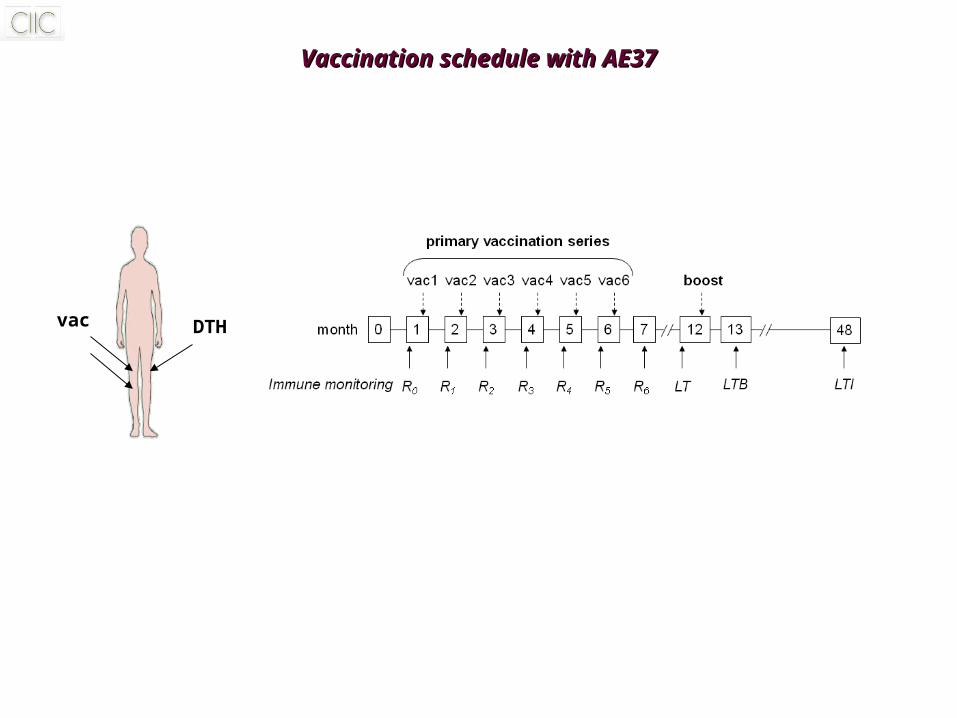
vac DTH
Vaccination schedule with AE37Vaccination schedule with AE37
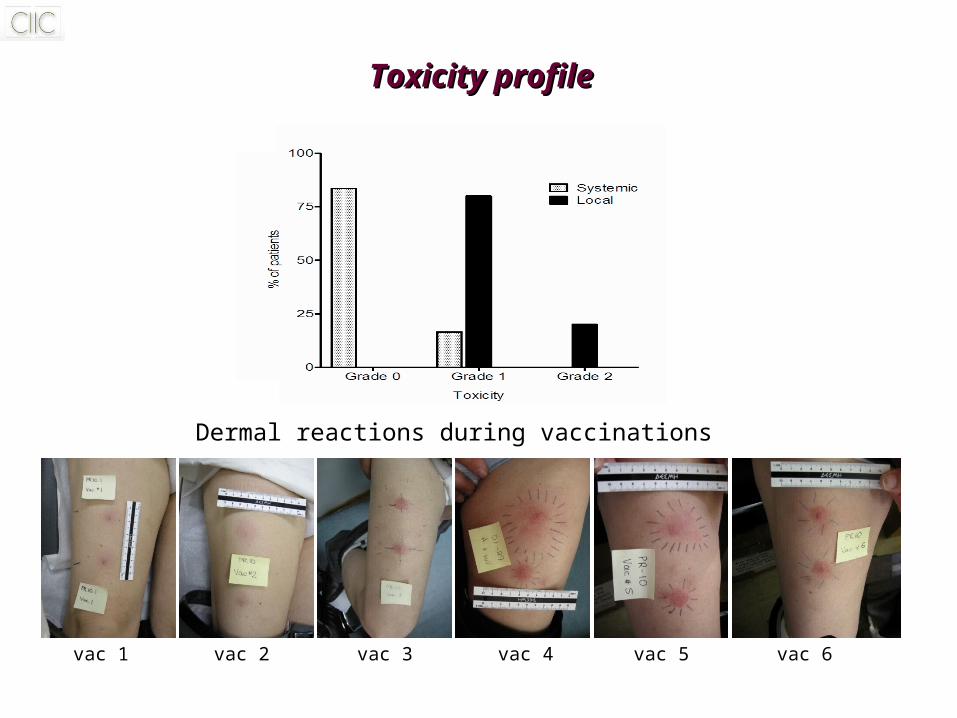
Toxicity profileToxicity profile
Dermal reactions during vaccinations
vac 1 vac 2 vac 3 vac 4 vac 5 vac 6
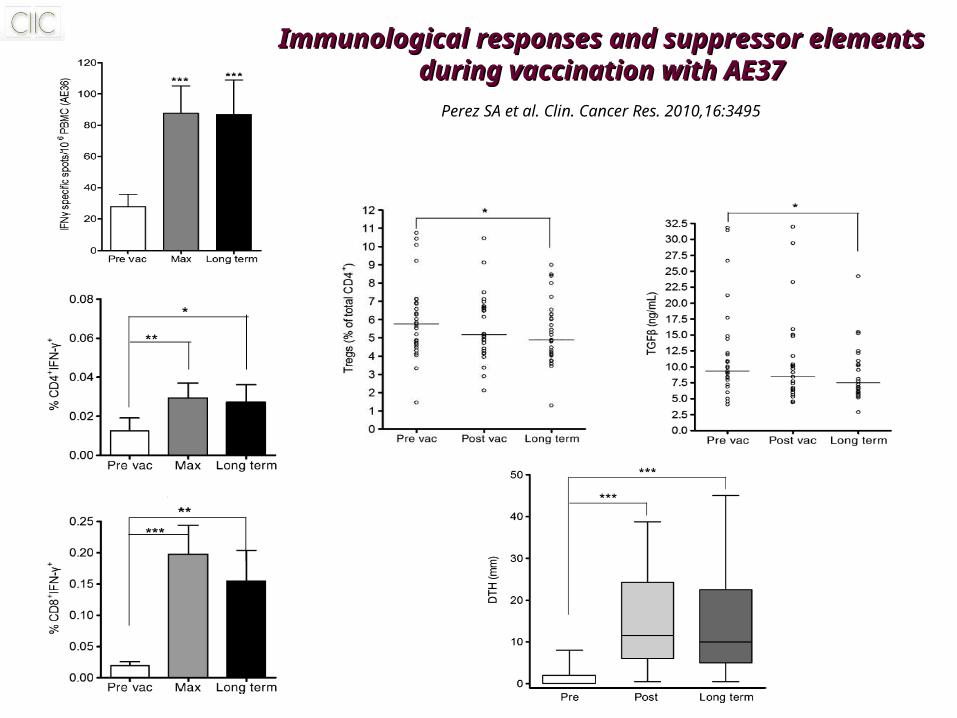
Immunological responses and suppressor elementsImmunological responses and suppressor elementsduring vaccination with AE37during vaccination with AE37
Perez SA et al. Clin. Cancer Res. 2010,16:3495
THE AE37 CANCER VACCINETHE AE37 CANCER VACCINE
Retrospective analyses from the prostate Ca trialRetrospective analyses from the prostate Ca trial
Identification of immunologic biomarkers to predict treatmentactivity and overall survival
Perez SA et al. Cancer Immunol. Immunother. 2013, 62:1599Perez SA et al. Cancer Immunol. Immunother. 2014, in press
R0 R6 LTLTB
LTI0
10
20
30
4040
80
TG
Fβ
(n
g/m
l)
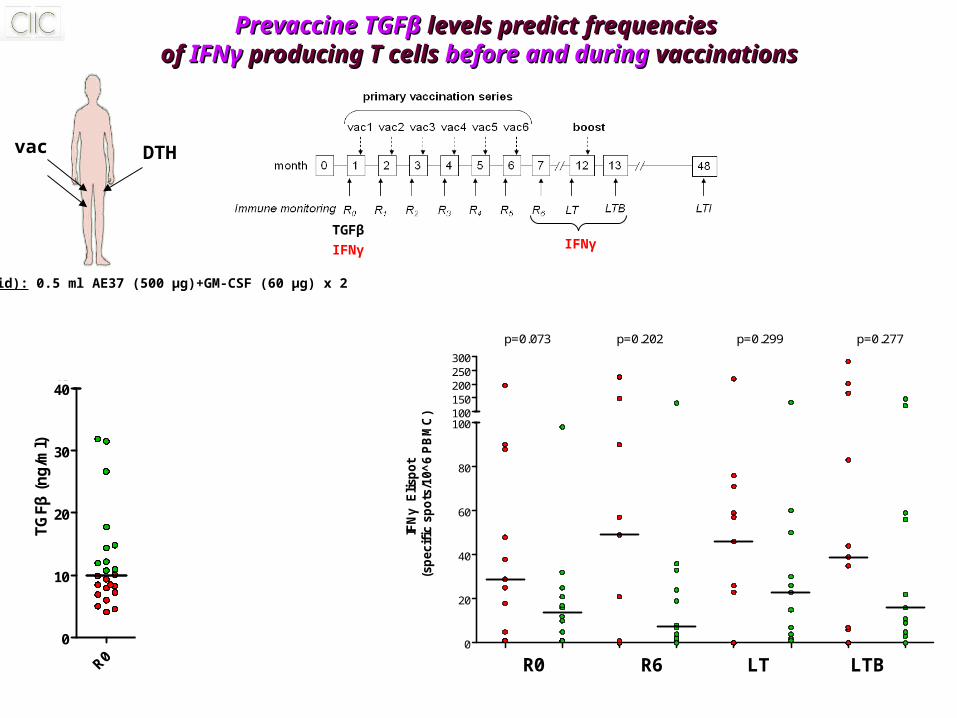
Vac(id): 0.5 ml AE37 (500 μg)+GM-CSF (60 μg) x 2
vac DTH
R0 R6 LT LTB
TGF IFN specific spots
0
20
40
60
80
100100150200250300
p=0.073 p=0.202 p=0.299 p=0.277
IFN
γ E
lisp
ot
(sp
ecif
ic s
po
ts/1
0^
6 P
BM
C)
PrevaccinePrevaccine TGFTGFββ levels predict frequencies levels predict frequencies of of IFNIFNγγ producing T cells producing T cells before and duringbefore and during vaccinations vaccinations
IFNγTGFβ
IFNγ
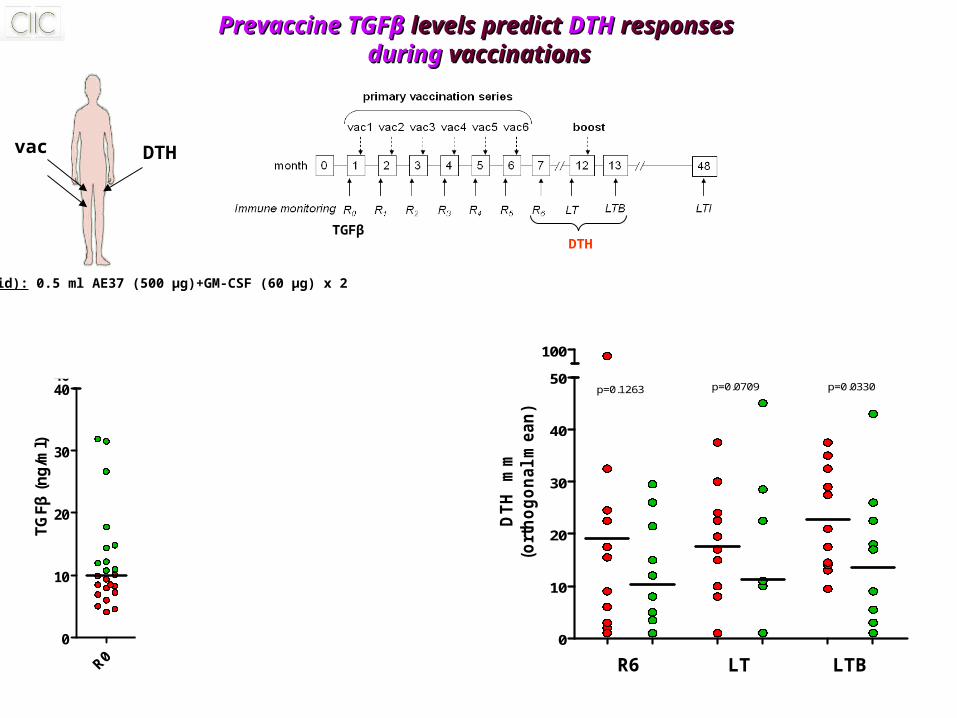
Vac(id): 0.5 ml AE37 (500 μg)+GM-CSF (60 μg) x 2
vac DTH
R0 R6 LTLTB
LTI0
10
20
30
4040
80
TG
Fβ
(n
g/m
l)
0
10
20
30
40
50
100
p=0.1263 p=0.0709 p=0.0330
DT
H
mm
(ort
ho
go
nal
mean
)
R6 LT LTB
PrevaccinePrevaccine TGFTGFββ levels predict levels predict DTHDTH responses responses duringduring vaccinations vaccinations
TGFβDTH
1.1. Inverse correlation between Inverse correlation between pre-existingpre-existing TGF- TGF-ββ and IFN and IFNγγ levels levels
2. Patients with 2. Patients with low TGFlow TGFββ levels levels beforebefore vaccinations vaccinations
develop develop positivepositive AE37-induced immunityAE37-induced immunity both in vitro and in vivo both in vitro and in vivo
ConclusionsConclusions
0
50
100
150
200
IFN
-γ s
pots
/10
6 P
BM
Cs
0
10
20
30
40
50
DT
H
mm
(o
rth
og
on
al m
ean
)
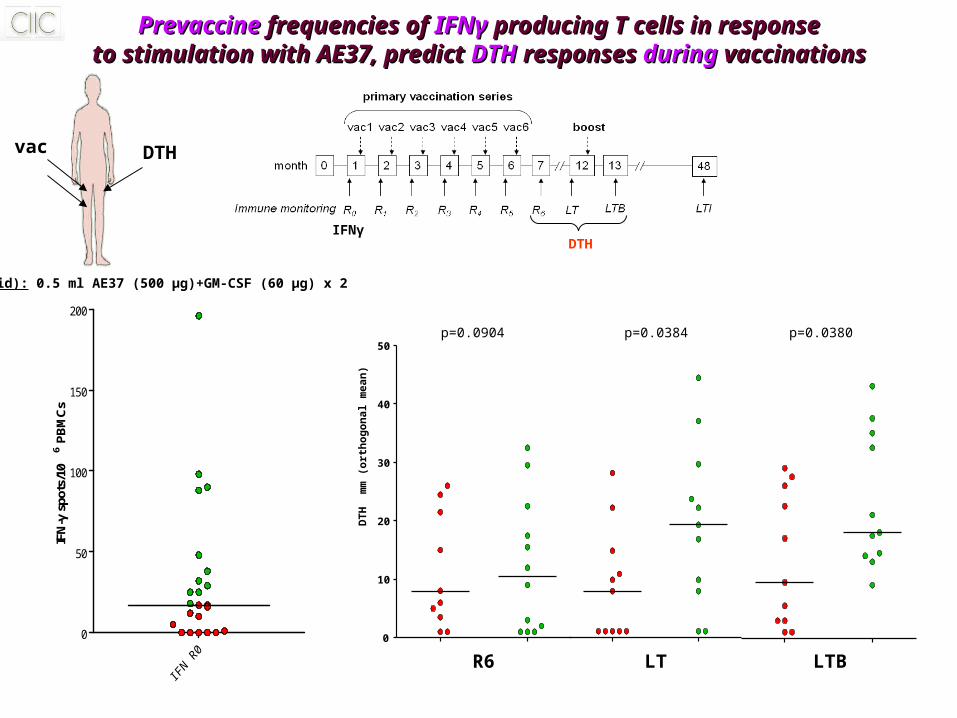
Vac(id): 0.5 ml AE37 (500 μg)+GM-CSF (60 μg) x 2
vac DTH
R6 LT LTB
p=0.0384 p=0.0380
PrevaccinePrevaccine frequencies of frequencies of IFN IFNγγ producing T cells in responseproducing T cells in responseto stimulation with AE37, predict to stimulation with AE37, predict DTHDTH responses responses duringduring vaccinations vaccinations
IFNγDTH
p=0.0904
Patients with higher frequencies of Patients with higher frequencies of AE37-specific IFNAE37-specific IFNγγ producing T cells producing T cells
beforebefore vaccinations develop vaccinations develop positive AE37-induced DTH positive AE37-induced DTH reactions reactions
ConclusionsConclusions
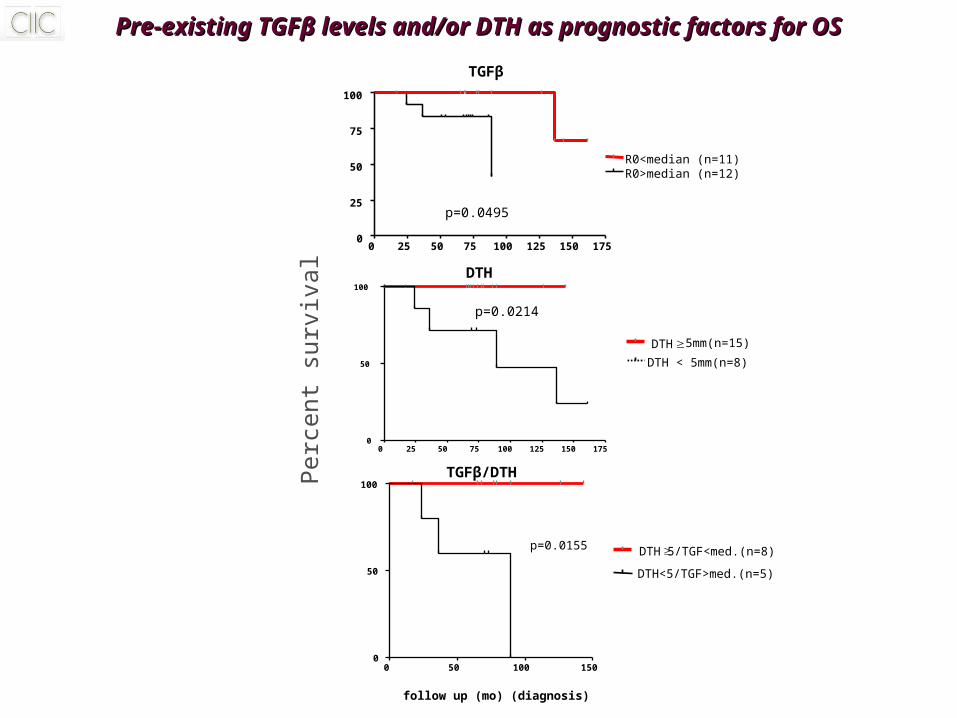
Pre-existing TGFPre-existing TGFββ levels and/or DTH as prognostic factors for OS levels and/or DTH as prognostic factors for OS
R0>median (n=12)R0<median (n=11)
TGFβ
0 25 50 75 100 125 150 1750
25
50
75
100
Per
cent
sur
viva
l
p=0.0495
0 50 100 1500
50
100
p=0.0155 DTH5/TGF<med.(n=8)
DTH<5/TGF>med.(n=5)
follow up (mo) (diagnosis)
p=0.0214
DTH5mm(n=15)
DTH < 5mm(n=8)
0 25 50 75 100 125 150 1750
50
100
DTH
TGFβ/DTH
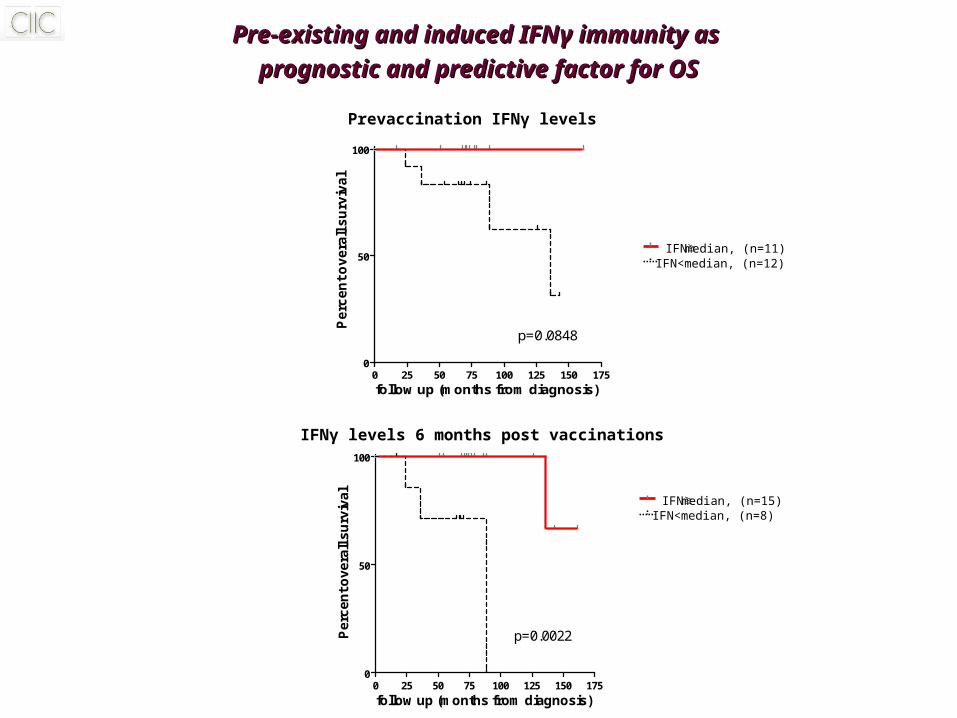
Pre-existing and induced IFNPre-existing and induced IFNγγ immunity as immunity as
prognostic and predictive factor for OSprognostic and predictive factor for OS
IFNmedian, (n=15)IFN<median, (n=8)
IFNmedian, (n=11)IFN<median, (n=12)
IFNγ levels 6 months post vaccinations
Prevaccination IFNγ levels
0 25 50 75 100 125 150 1750
50
100
follow up (months from diagnosis)
Pe
rce
nt
ov
era
ll s
urv
iva
lp=0.0848
0 25 50 75 100 125 150 1750
50
100
follow up (months from diagnosis)
Pe
rce
nt o
ve
rall
su
rviv
al
p=0.0022
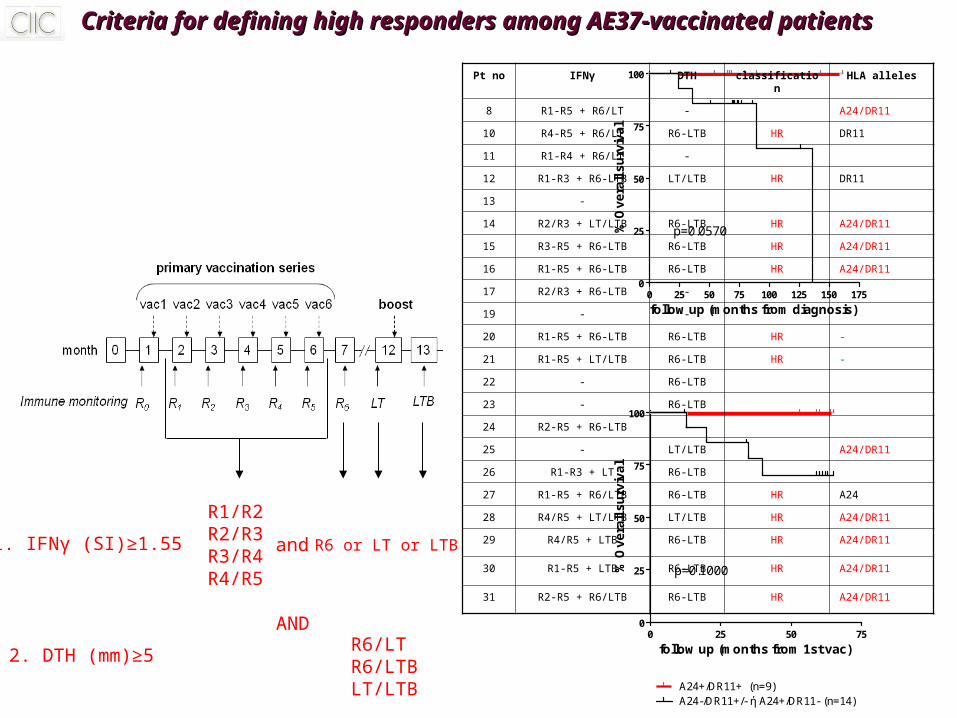
HLA-A24/HLA-DR11
0 25 50 75 100 125 150 1750
25
50
75
100
p=0.0570
follow up (months from diagnosis)
% O
ve
rall
su
rviv
al
0 25 50 750
25
50
75
100
A24+/DR11+ (n=9)A24-/DR11+/- ή A24+/DR11- (n=14)
p=0.1000
follow up (months from 1st vac)
% O
ve
rall
su
rviv
al
Criteria for defining high responders among AE37-vaccinated patientsCriteria for defining high responders among AE37-vaccinated patients
1. IFNγ (SI)≥1.55
R1/R2R2/R3R3/R4R4/R5
and R6 or LT or LTB
2. DTH (mm)≥5R6/LTR6/LTBLT/LTB
AND
Pt no IFNγ DTH classification HLA alleles
8 R1-R5 + R6/LT - A24/DR11
10 R4-R5 + R6/LT R6-LTB HR DR11
11 R1-R4 + R6/LT -
12 R1-R3 + R6-LTB LT/LTB HR DR11
13 -
14 R2/R3 + LT/LTB R6-LTB HR A24/DR11
15 R3-R5 + R6-LTB R6-LTB HR A24/DR11
16 R1-R5 + R6-LTB R6-LTB HR A24/DR11
17 R2/R3 + R6-LTB -
19 - -
20 R1-R5 + R6-LTB R6-LTB HR -
21 R1-R5 + LT/LTB R6-LTB HR -
22 - R6-LTB
23 - R6-LTB
24 R2-R5 + R6-LTB -
25 - LT/LTB A24/DR11
26 R1-R3 + LT R6-LTB
27 R1-R5 + R6/LTB R6-LTB HR A24
28 R4/R5 + LT/LTB LT/LTB HR A24/DR11
29 R4/R5 + LTB R6-LTB HR A24/DR11
30 R1-R5 + LTB R6-LTB HR A24/DR11
31 R2-R5 + R6/LTB R6-LTB HR A24/DR11
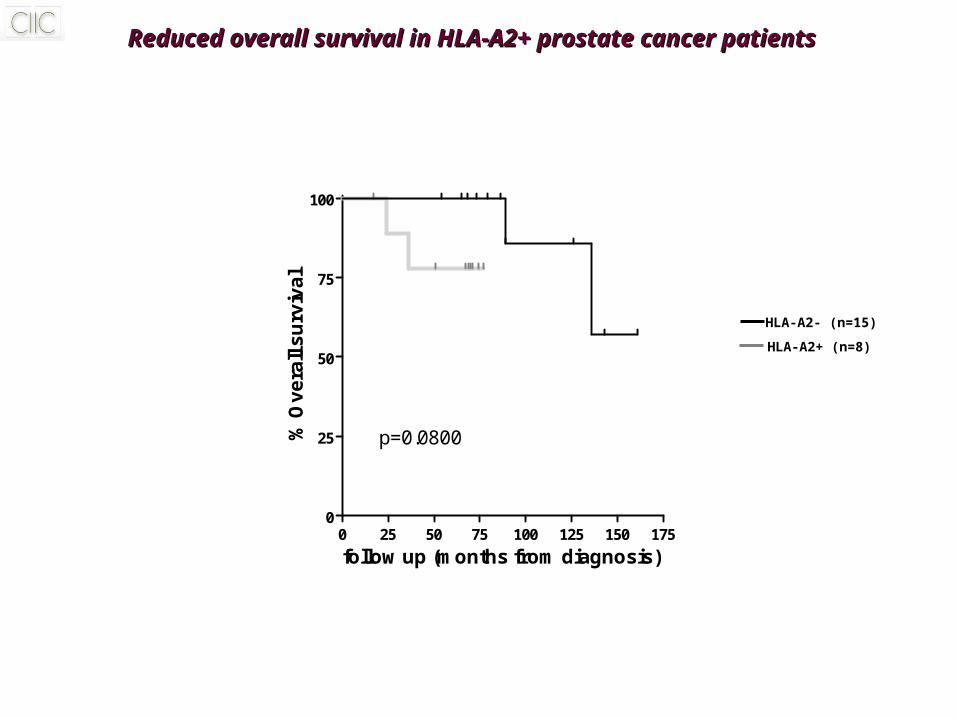
HLA-A2
0 25 50 75 100 125 150 1750
25
50
75
100
p=0.0800
follow up (months from diagnosis)
% O
ve
rall
su
rviv
al
HLA-A2- (n=15)
HLA-A2+ (n=8)
Reduced overall survival in HLA-A2+ prostate cancer patients Reduced overall survival in HLA-A2+ prostate cancer patients
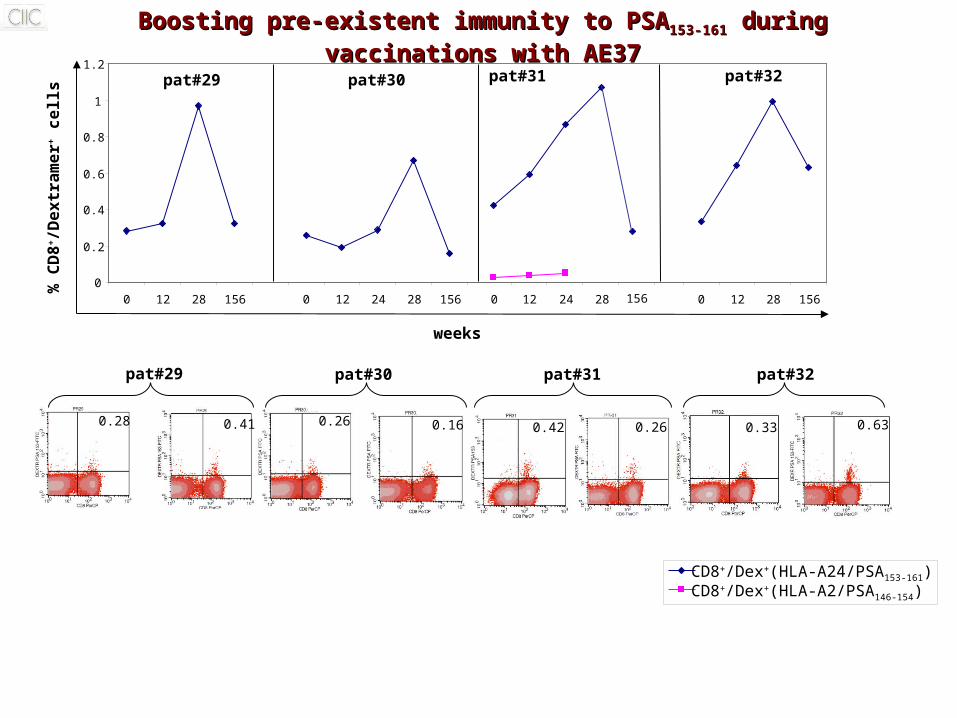
0
0.2
0.4
0.6
0.8
1
1.2
0 12 28 156 0 12 24 28 156 0 12 24 28 0 12 28 156
% C
D8+
/De
xtr
am
er+
ce
lls
Boosting pre-existent immunity to PSABoosting pre-existent immunity to PSA153-161153-161 during vaccinations with AE37 during vaccinations with AE37
pat#29 pat#30 pat#32pat#31
CD8+/Dex+(HLA-A24/PSA153-161)CD8+/Dex+(HLA-A2/PSA146-154)
0.41 0.16 0.26 0.63
weeks
0.28 0.26 0.42 0.33
pat#29 pat#30 pat#31 pat#32
156
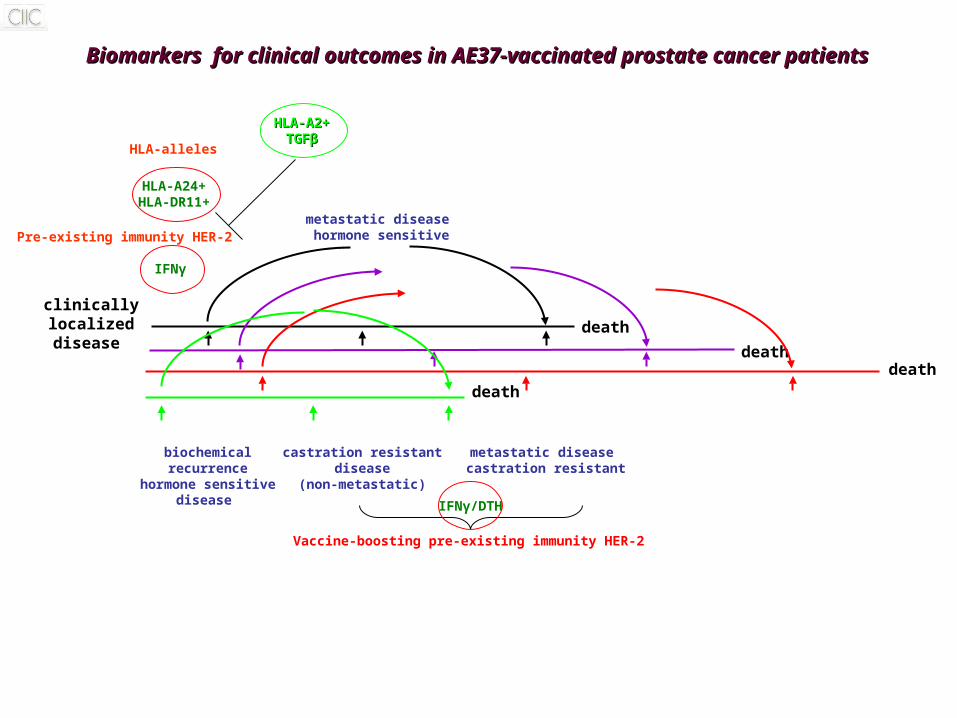
Biomarkers for clinical outcomes in AE37-vaccinated prostate cancer patientsBiomarkers for clinical outcomes in AE37-vaccinated prostate cancer patients
clinicallylocalizeddisease
biochemicalrecurrence
hormone sensitivedisease
castration resistantdisease
(non-metastatic)
metastatic disease castration resistant
metastatic disease hormone sensitive
death
death
Vaccine-boosting pre-existing immunity HER-2
death
IFNγ
IFNγ/DTH
HLA-A24+HLA-DR11+
HLA-A2+HLA-A2+TGFTGFββ
death
Pre-existing immunity HER-2
HLA-alleles
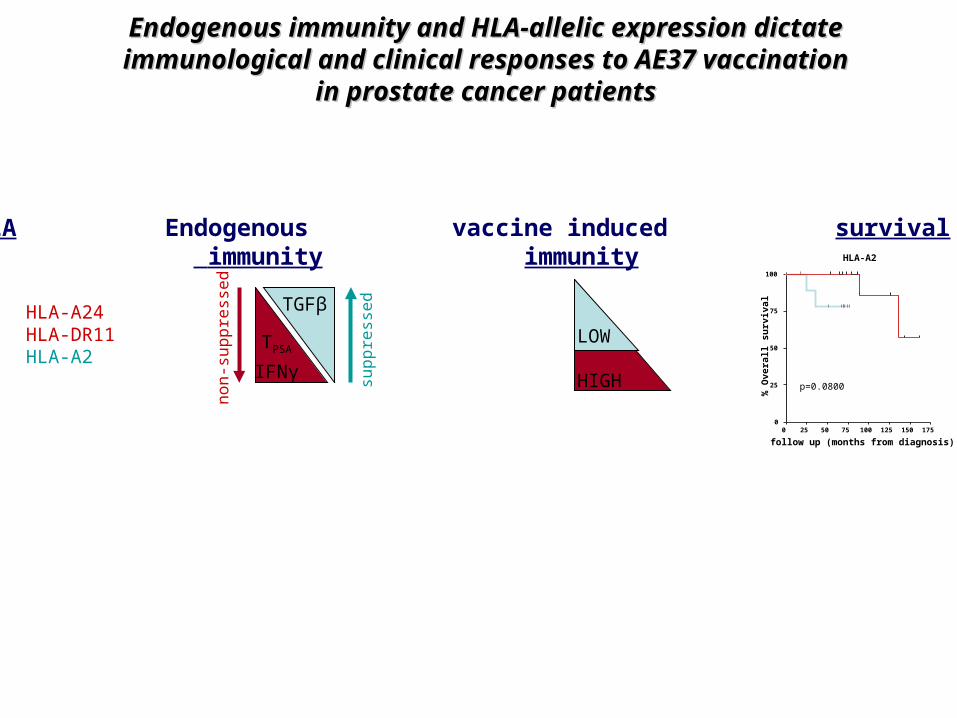
Endogenous immunity and HLA-allelic expression dictateEndogenous immunity and HLA-allelic expression dictateimmunological and clinical responses to AE37 vaccinationimmunological and clinical responses to AE37 vaccination
in prostate cancer patientsin prostate cancer patients
HLA Endogenous vaccine induced survival immunity immunity
HLA-A24HLA-DR11HLA-A2
TGFβ
TPSA
IFNγ
LOW
HIGHsup
pre
sse
d
no
n-s
up
pre
sse
d
HLA-A2
0 25 50 75 100 125 150 1750
25
50
75
100
p=0.0800
follow up (months from diagnosis)
% O
vera
ll su
rviv
al
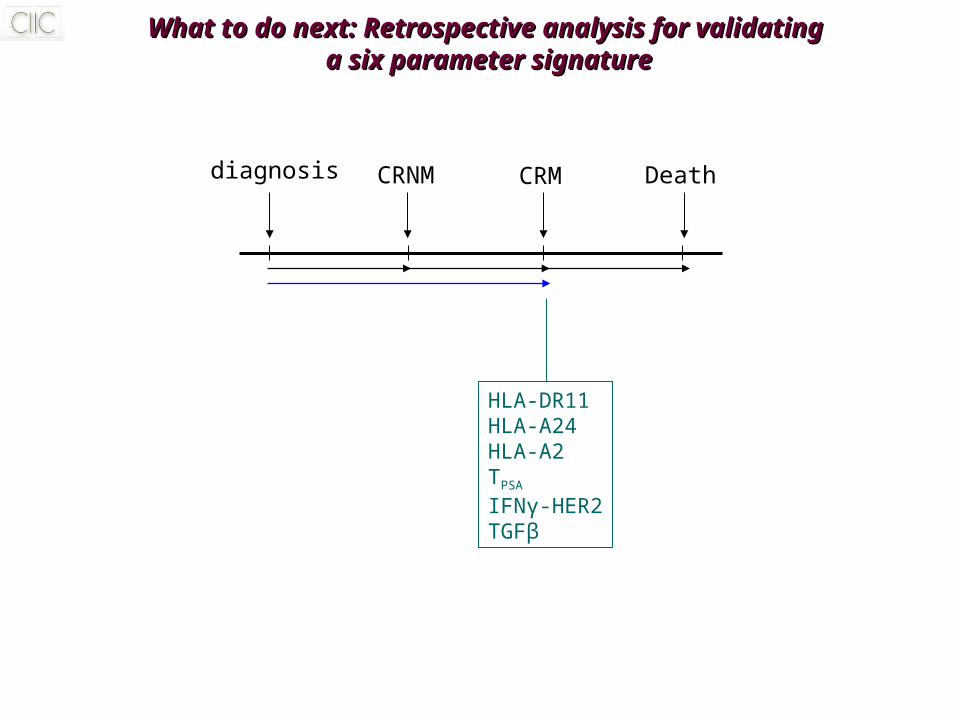
What to do next: Retrospective analysis for validating What to do next: Retrospective analysis for validating a six parameter signaturea six parameter signature
diagnosis CRNM CRM Death
HLA-DR11HLA-A24HLA-A2TPSA
IFNγ-HER2TGFβ
AcknowledgementsAcknowledgements
Dr. S.A. Perez, PhD, Research coordinator at CIICDr. A. Thanos, MD, Director of the Urology Clinic at St Savas HospitalDr. M. Papamichail, PhD, MD, Honorary Director at CIICDr. E. von Hofe, PhD, President of Antigen Express Inc.Dr. I.F. Voutsas, PhDDr. L. Mahaira, PhDDr. O. Katsara, PhDDr. E. Iliopoulou, PhDP. Tzonis, MDE. Anastasopoulou, MScI. Kalogeropoulou, BScE. Pappou, BScT. Keramitsoglou, PhD, Immunobiology dept. Helena Venizelou HospitalM. Varla-Eleftherioti, MD, PhD, Immunobiology dept. Helena Venizelou Hospital