ca lâm sàng aidp - thuchanhthankinh.comthuchanhthankinh.com/userupload-thuchanhthankinh/files/ca...
TRANSCRIPT
Ca lâm sàng Guillain Barre
PGS. TS CAO PHI PHONG
2018

Họ và tên : Đoàn Văn C. Nam, sinh năm 1978
Dân tộc: Kinh
Nghề nghiệp: buôn bán
Địa chỉ : Cai Lậy- Tiền Giang
Ngày nhập viện: 05.12.2018
Ngày khám làm BA: 13.12.2018Thuận tay P
Lý do nhập viện: yếu 2 chi dưới

Bệnh sử:
Bệnh khởi phát cách nhập viện 3 ngày, ngày đầu bệnh nhân tê bì kiểu châm
chích bàn tay và bàn chân 2 bên, tê liên tục, cảm giác khó chịu, bệnh nhân tự
uống thuốc đông y nhưng không đỡ.
Ngày thứ 2, tê tay chân nhiều hơn lan dần lên đến giữa cẳng tay và cẳng chân 2
bên, bệnh nhân yếu 2 chân, loạng choạng đi lại khó khăn phải có người đỡ nên
vào viện.
Trong quá trình đó, bệnh nhân đổ mồ hôi lòng bàn tay và bàn chân nhiều,

Tình trạng lúc vào việnTỉnh táo
Huyết động ổn
Đi lại khó khăn
Cơ lực 2 chân 4/5 gốc = ngọn, 2 tay 5/5
Tê bì kiểu châm chích tay chân theo kiểu đi găng đi vớ(Bệnh nhân được thay huyết tương 4 lần, sau thay bệnh nhân đỡ tê bì, đi lại được nhưng còn loạng
choạng)
Tiền sử y khoa:
Trong vòng 2 tuần gần đây bệnh nhân không bị cảm cúm, viêm phổi ,hay rối loạn tiêu hóa
Không có tiêm vaccin gần đây
Không nghiện rượu,không hút thuốc lá
Tiền căn gia đình:
Bình thường
Tiền căn Xã hội :
Bình thường

Hệ vận động :
- Không teo cơ, rung giật bó cơ (+)
- Trương lực cơ tứ chi bình thường
- Cơ lực tứ chi : 5/5
Phan xa:Phản xạ tứ chi giảm, phản xạ da bụng bình thường
Dấu tháp:
Dấu tháp (-)
Khám thần kinh
Hệ cảm giác:
- Tê kiểu châm chích 2 bàn tay và 2 bàn chân
- Không giảm cảm giác nông
- Giảm nhẹ cảm giác rung âm thoa ở các đốt ngón chân và ngón tay
Các chức năng thần kinh khác chưa phát hiện bệnh lý
Tóm tắt bệnh án
Bệnh nhân nam, 40 tuổi, nhập viện vì tê tứ chi
Bệnh diễn tiến cấp tính , đã được thay huyết tương 4 lần, khám ngày 10 của
bệnh ghi nhận:
Tê tứ chi kiểu măng gang đi vớ
- giảm cảm giác rung âm thoa tứ chi
- Romberg cảm giác sâu (+)
- yếu 2 chân 4/5 gốc = ngọn (lúc vào viện)
- phản xạ gân xương giảm tứ chi
- tăng tiết mồ hôi tay chân

Bàn luận chẩn đoán
Vấn đề của bệnh nhân:
Hội chứng liệt mềm 4 chi kiểu ngoại biên(chân>tay)
Rối loạn cảm giác tứ chi kiểu mang găng vớ
Kế hoạch giải quyết vấn đề ?

Chẩn đoán vị trí ?
Trả lời 5 câu hỏi ?
Sợi vđ, cg hay tự động?
Sợi lớn, sợi nhỏ, bệnh lý myelin, tổn thương sợi trục, thân nơron
(Myelinopathy, axonopathy, neuronopathy), Đau so với không đau Gần hay xa phụ thuộc chiều dài(prosximal or length dependant distal)
Kết luận:
Mono, multiple mononeuritis, polyneuropathies, plexopathy,
neuronopathy, radiculoplexopathy, myeloneuropathy,
cranial/truncal neuropathy ?
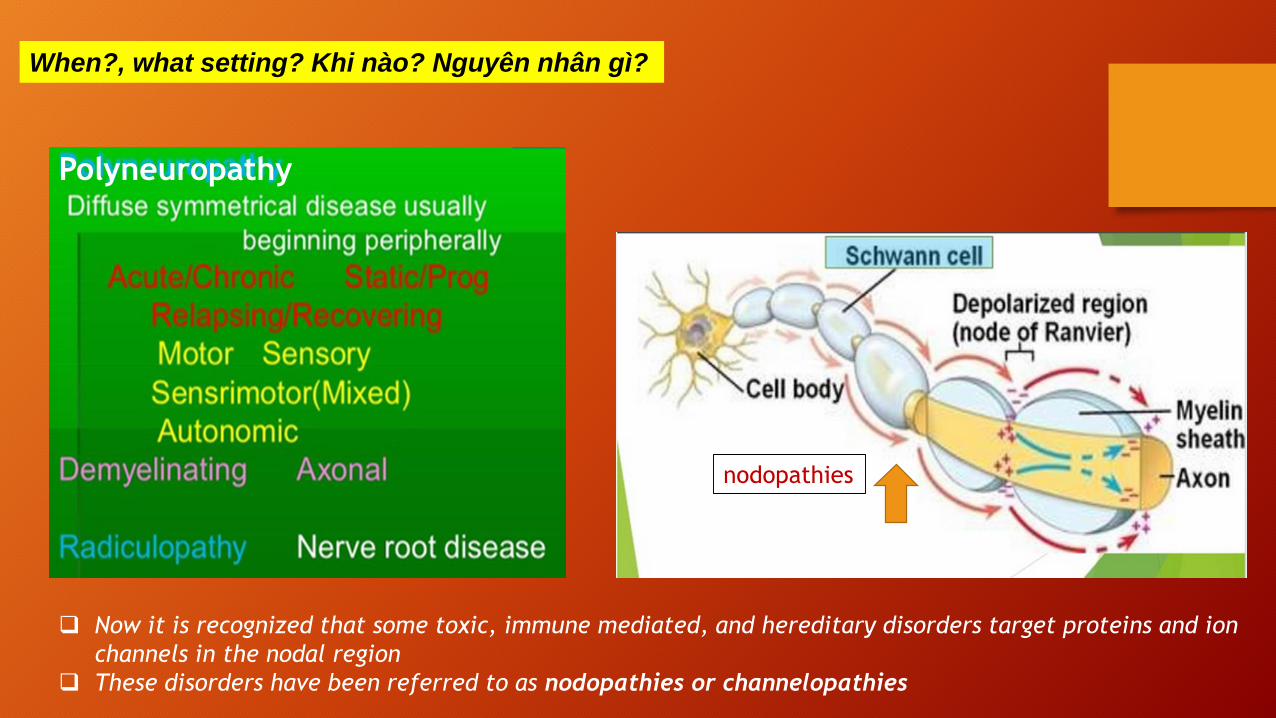
When?, what setting? Khi nào? Nguyên nhân gì?
Now it is recognized that some toxic, immune mediated, and hereditary disorders target proteins and ion
channels in the nodal region
These disorders have been referred to as nodopathies or channelopathies
nodopathies
Polyneuropathy

Chẩn đoán nguyên nhân ca lâm sàng?

(mất myelin: cho phép dòng điện thoát ra qua nơi bộc lộ sợi trục , có số ít kênh ion hiện diện, đe dọa sự lan truyền
điện thế động, qua trung gian miễn dịch tế bào và thể dịch, kháng nguyên khu trú cạnh và kề vùng liên nút)

Nguyên nhân


Chẩn đoán phân biệt ?
Chronic inflammatory demyelinating polyneuropathy
- AIDP là một bệnh bán cấp đơn pha, đạt đến ít nhất ba đến bốn tuần- CIDP tiếp tục tiến triển hoặc tái phát hơn tám tuần- Viêm đa dây thần kinh bán cấp tính (SIDP) được sử dụng bởi một số tác giả,
bệnh đạt đến ít nhất từ bốn đến tám tuần(tiền sử nhiễm trùng đường hô hấp, tiêu hóa xảy ra thường xuyên hơn với GBS (trong đó xảy ra
trong khoảng 70% trường hợp) so với CIDP (được tìm thấy trong ≤30 phần trăm các trường hợp)
Polyneuropathies khác- thiếu vitamin B1 (thiamine) nặng, cấp tính
- ngộ độc asenic cấp tính, viêm mạch, bệnh Lyme, bệnh bại liệt , sarcoidosis,
bệnh leptomeningeal, bệnh paraneoplastic và bệnh hiểm nghèo (critical illness).

Bệnh lý tủy sống
– bệnh lý tủy cấp tính do chèn ép tủy sống, viêm tủy ngang cấp tính có thể bị
nhầm lẫn với GBS
Bệnh lý nơron vận động: xơ cứng cột bên teo cơ và teo cơ tủy sống tiến triển
Rối loan tiếp hợp thần kinh cơ: botulism, myasthenia gravis, and Lambert-
Eaton myasthenic syndrome
Bệnh cơ: Acute polymyositis, critical illness myopathy, và critical illness
neuropathy có thể nhầm GBS.
(The myopathy and neuropathy of critical illness present as an acute paralysis. Corticosteroid tiêm tĩnh mạch liều cao, thuốc ức chế thần kinh cơ, nhiễm trùng huyết và suy đa cơ quan được cho
là có vai trò quan trọng, nhưng sinh lý bệnh học không được hiểu rõ?)

Hội chứng Miller Fisher (MFS) có thể bị nhầm lẫn với đột quỵ thân não.Tuy nhiên, sự khởi phát
dần dần của MFS đặc biệt phân biệt hội chứng này trên lâm sàng với đột quỵ thân não.
Chẩn đoán phân biệt của MFS bao gồm bệnh não Wernicke và viêm não mô cầu,
(tình trạng tâm thần thay đổi, ngoài ra bệnh não Wernicke thường có giật nhãn cầu, một đặc điểm
không liên quan đến MFS).
Chẩn đoán hình ảnh thần kinh có thể hữu ích để loại trừ đột quỵ và tổn thương cấp tính của
diencephalon, midbrain và các vùng quanh não thất tìm thấy ở bệnh não Wernicke.
Chẩn đoán phân biệt hội chứng Miller Fisher ?

Kết quả xét nghiệm ca lâm sàng
Bệnh đa dây thầnkinh cảm giác kiểutổn thương sợi trục ?
Chỉ có biên độ cảm giác thần kinh giữa và trụ giảm
Biên độ cảm giác thần kinh mác nông và bắp chân bình thường
Dẫn truyền chi trên và chi dưới bình thường
Sóng F bình thường
Điện cơ kim bình thường

Chẩn đoán xác định và điều trị
Bệnh viêm đa dây rễ dây thần kinh cấp tính ưu thế cảm giác
(Pure sensory GBS)
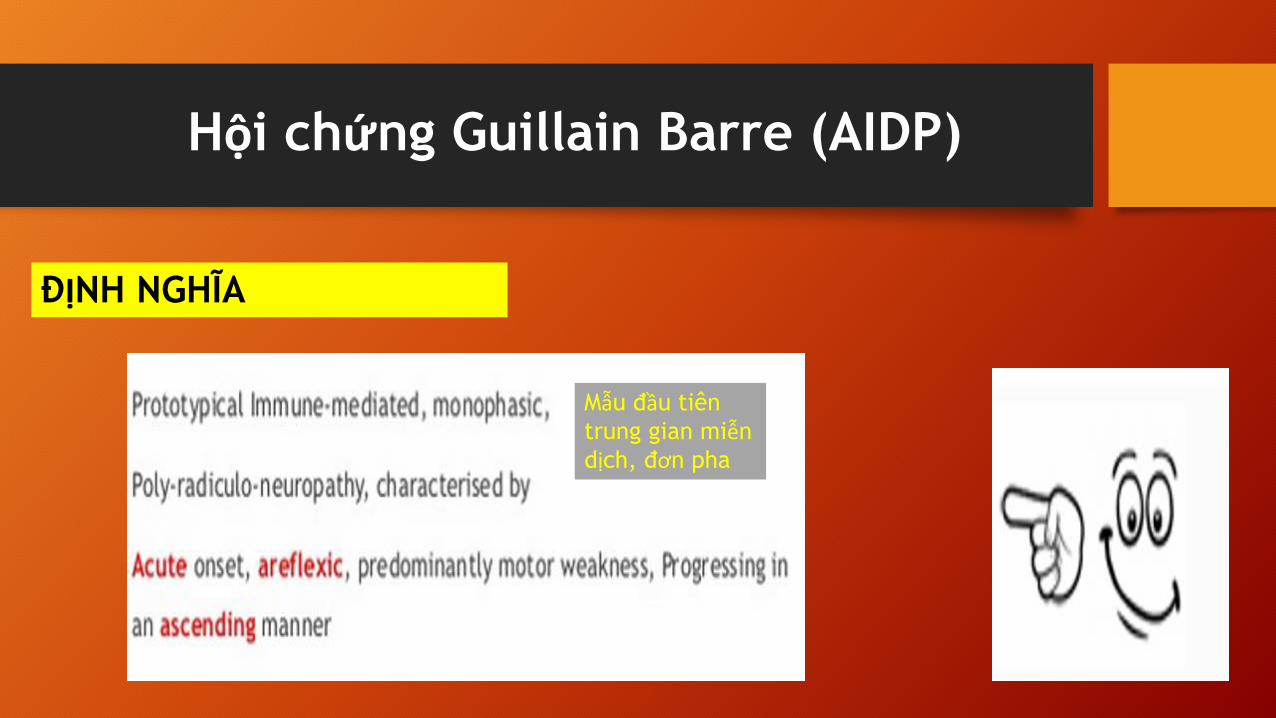
Hội chứng Guillain Barre (AIDP)
ĐỊNH NGHĨA
Mẫu đầu tiên
trung gian miễndịch, đơn pha
Polyneuropathies qua trung gian miễn dịch, cấp tính, hội chứng
Guillain-Barré (GBS),
GBS không đồng nhất với nhiều biến thể.
Thông thường, GBS biểu hiện liệt cấp tính, đơn pha, được kích thích
bởi nhiễm trùng trước đó.
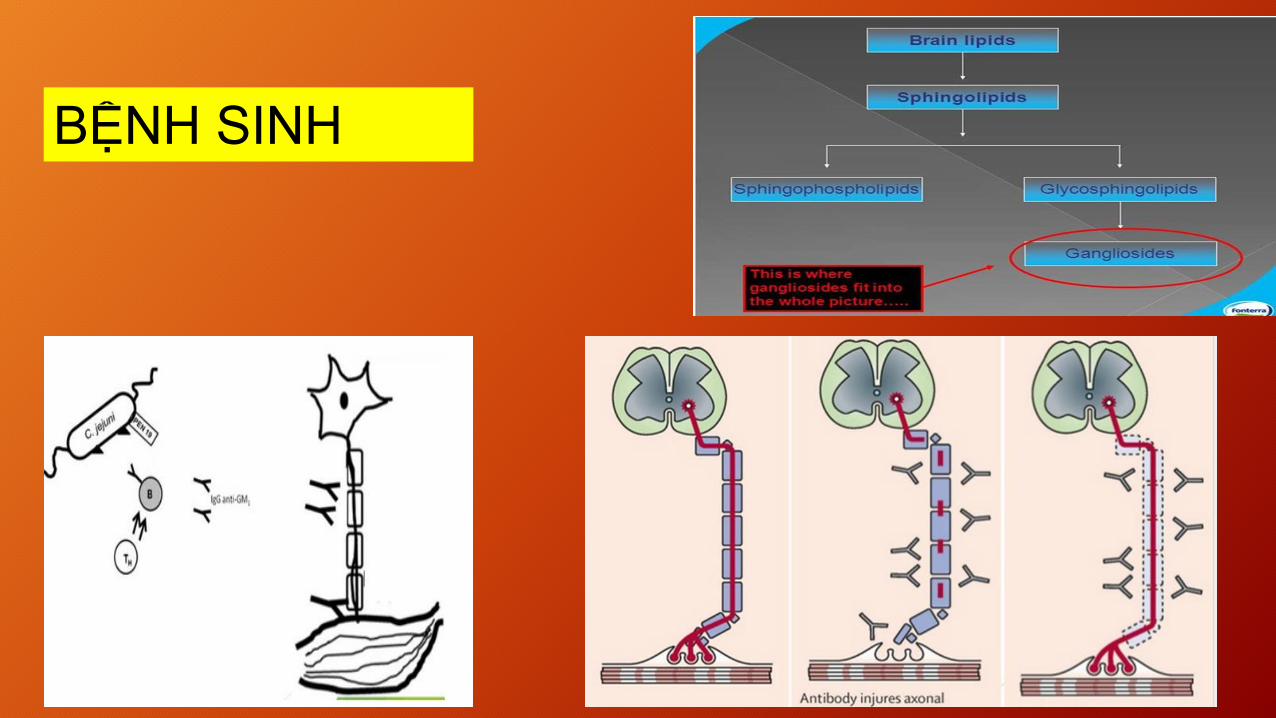
BỆNH SINH

No specific myelin antigen(s)- Schwann cell surface membrane or myelin
- Multifocal inflammatory demyelination starting at the level of
the nerve roots.

Immune reactions against epitopes contained in the
axonal membrane cause the acute axonal forms of GBSAMAN, AMSAN
Một cơ chế được đề xuất cho GBS: Molecular mimicry
Nhiễm trùng tiền đề gợi lên phản ứng miễn dịch,
Từ đó phản ứng chéo với các thành phần thần kinh ngoại biên (bắt chước phân tử).
Kết quả bệnh đa dây thần kinh cấp tính.
(Phản ứng miễn dịch này có thể được hướng vào myelin hoặc sợi trục của dây thần kinh ngoại biên).


Tiền sử nhiễm trùng
Campylobacter jejuni
(Other studies have found that about 60 to 70 percent of AMAN and AMSAN cases and up to 30
percent of AIDP cases are preceded by C. jejuni infection)
HIV, Zika virus, Cytomegalovirus, virus Epstein-Barr
Influenza vaccination
Meningococcal vaccination
Các yếu tố khác: surgery, trauma, and bone-marrow transplantation

Lâm sàng
NHIỄM TRÙNG
7-10 ngày trước khởi phát yếu chi
Hồi phục 2-3 tuầnsau ngưng tiến triển

Kháng thể

Đặc điểm yếu cơ tiến triển, khá đối xứng kèm theo phản xạ gân cơ giảmhay mất .
Thường xuất hiện vài ngày đến một tuần sau khi khởi phát.
Yếu có thể từ khó khăn nhẹ với đi bộ đến tê liệt gần như hoàn toàn tất cả
các chi, cơ mặt, hô hấp và cơ bắp.

Thường bắt đầu ở chân, (cánh tay hoặc cơ mặt 10%).
Liệt cơ hô hấp cần hỗ trợ thở máy (10 đến 30 %).
Liệt thần kinh mặt xảy ra ở hơn 50% và yếu cơ vòm họng 50%).
Liệt dây III khoảng 15%.
Phản xạ giảm hoặc mất khoảng 90% khi bệnh tiến triển
Dị cảm ở tay và chân liệt hơn 80% , nhưng bất thường về cảm giác khi khám
thường nhẹ.
Đau do viêm rễ thần kinh, thường ở lưng và tứ chi, trong giai đoạn cấp chiếm hai
phần ba bệnh nhân với tất cả các thể GBS

Loạn thần kinh tự động (Dysautonomia) xảy ra ở khoảng 70 % bệnh nhân.
Rối loạn chức năng TKTĐ phổ biến hơn ở bệnh nhân GBS bao gồm: tiêu chảy /
táo bón, hạ natri máu, nhịp tim chậm, bí tiểu, nhịp tim nhanh, bệnh cơ tim và hội
chứng Horner.
Rối loạn chức năng tự động nặng đôi khi liên quan đến cái chết đột ngột
Hội chứng bài tiết hormone chống bài niệu không phù hợp (SIADH),
Ít gặp: papilledema, facial myokymia, hearing loss, meningeal signs, vocal cord
paralysis, and mental status changes . Thêm vào, posterior reversible
encephalopathy syndrome, còn biết như reversible posterior leukoencephalopathy
syndrome

Biến thể GBS
Guillain-Barré syndrome (GBS) = heterogeneous syndrome with
several variant forms.
Each form of GBS has distinguishing clinical, pathophysiologic,
and pathologic features.

Acute inflammatory demyelinating polyradiculoneuropathy (AIDP): thể thường
gặp nhất ở Hoa kỳ và châu Âu 80-90%
Lâm sàng Miller Fisher syndrome (MFS), đặc điểm ophthalmoplegia, ataxia,
areflexia, 5% ca ở Hoa kỳ và 25% ở Nhật.
Acute motor axonal neuropathy (AMAN) và acute sensorimotor axonal neuropathy(AMSAN)thể sợi trục nguyên phát của GBS. Thường gặp China,
Japan, Mexico, 5 - 10 % ca GBS ở Hoa kỳ

AMSAN nặng hơn thể AMAN, cả vận động và cảm giác, tổn thương sợi trục,
hồi phục không hoàn toàn. Lâm sàng giống AMAN, triệu chứng cảm giác
nhiều hơn. Bệnh lý ưu thế tổn thương sợi trục
(In AMSAN, motor and sensory responses are frequently severely reduced or absent on
electrodiagnostic studies. Axonal degeneration in these patients is demonstrated by
extensive denervation on follow-up electromyography studies).
Acute motor and sensory axonal neuropathy

Ophthalmoplegia, ataxia, areflexia. (1/4 MFS sẽ có yếu chi, thể không hoàn toàn: acute
ophthalmoplegia without ataxia, and acute ataxic neuropathy without ophthalmoplegia. Một
vài bn MFS có dãn đồng tử .
Antibodies against GQ1b (a ganglioside component of nerve) 85 đến 90 % . GQ1b antibody liên
hệ mạnh dây III, và tìm thấy hầu hết ưu thế liệt dây III và GBS.
(Electrodiagnostic studies in patients with MFS reveal reduced or absent sensory responses
without slowing of sensory conduction velocities. When there is associated weakness, the motor
nerve conduction abnormalities of AIDP may be present).
Miller Fisher syndrome
Miller Fisher syndrome is classified as an acute or subacute
demyelinating polyradiculoneuropathy, but its clinical
presentation differs markedly from typical GBS

Bickerstaff encephalitis: Bickerstaff encephalitis: brainstem encephalitis, đặc điểm:
encephalopathy + hyperreflexia với Miller Fisher syndrome (MFS) như ophthalmoplegia và ataxia.
Pharyngeal-cervical-brachial weakness — biến thể pharyngeal-cervical-brachial của GBS:
liệt hầu họng cấp, cổ, cơ vai với rối loạn chức năng nuốt
Paraparesis — biến thể paraparetic liên hệ thể nhẹ GBS: yếu giới hạn 2 chi dưới. Tuy nhiên hầu
hết giảm hay mất px chi trên 90% có bất thường điện cơ
Biến thể khác
• Acute pandysautonomia, có thể đáp ứng intravenous immune globulin.
Bao gồm: diarrhea, vomiting, dizziness, abdominal pain, ileus, orthostatic hypotension, urinary
retention, pupillary abnormalities, an invariant heart rate, and decreased sweating, salivation, and
lacrimation. Reflexes are absent or diminished and sensory symptoms may be present.

• Pure sensory GBS, liên quan large sensory fibers: sensory ataxia. Phản xạ mất và có thểliên quan nhẹ vận động. Ghi nhận antibodies to GD1b
• Facial diplegia and distal limb paresthesia, biến thể của acute inflammatory
demyelinating polyneuropathy.
• Acute bulbar palsy with areflexia, ophthalmoplegia, ataxia, and facial palsy,
neck and limb weakness are absent, thể trùng lấp cả Miller Fisher syndrome và
pharyngeal-cervical-brachial biến thể GBS.
• Sixth nerve palsy and distal paresthesia


multifocal motor neuropathy with conduction block (MMNCB) after Campylobacter jejuni enteritis.

Cận lâm sàng
Cerebrospinal fluid analysis
In patients with GBS, lumbar puncture often reveals an elevated CSF protein with a normal CSF
white blood cell count.
Albuminocytologic dissociation, is present in 50 to 66 percent of patients with GBS in the first
week after the onset of symptoms and ≥75 percent of patients in the third week
Elevated protein may be due to increased permeability of the blood-nerve-barrier at the level
of the proximal nerve roots.
A normal CSF protein is found in one-third to one-half of patients when tested earlier than one
week after symptom onset and therefore does not exclude the diagnosis of GBS

Electrodiagnostic studies
Nerve conduction studies (NCS) and needle electromyography (EMG)
• Demyelinating forms of GBS: decreased motor nerve conduction velocity, prolonged distal
motor latency, increased F wave latency, conduction blocks, and temporal dispersion.
• Axonal forms of GBS: by decreased distal motor and/or sensory amplitudes. Transient motor
nerve conduction block (ie, reversible conduction failure) can be present
• Since the nerve conduction abnormalities progress over time, serial electrodiagnostic studies are
frequently helpful. Findings can be normal early in the course of GBS, and are typically most
pronounced approximately two weeks after the onset of weaknes

Antibodies
Testing for serum IgG antibodies to
GQ1b is useful for the diagnosis of
Miller Fisher syndrome, having a
sensitivity of 85 to 90 percent.
Antibodies to GQ1b may also be
present in GBS with
ophthalmoparesis, Bickerstaff
encephalitis, and the pharyngeal-
cervical brachial GBS variant, but
not in disorders other than GBS.

MRI
Spinal MRI may reveal thickening and enhancement of the intrathecal spinal
nerve roots and cauda equina.
The anterior spinal nerve roots only may be involved, or both the anterior
and posterior spinal nerve roots can be involved.
In exceptional cases of Miller Fisher syndrome, abnormalities of the spinal
cord posterior columns have been described .
In the brain, enhancement of the oculomotor, abducens, and facial nerves.

(A) Coronal brain T1 MRI with Gd images showing bilateral facial nerve enhancement (arrows).
(B) Sagittal lumbar spine T1 MRI with Gd showing enhancement in the medullary cone (arrow).
(C) Axial lumbar-spine T2 MRI showing increased signal intensity in the spinal ganglia bilaterally (arrowheads).
(D) Axial lumbar-spine T1 MRI (fast scanning) with Gd showing enhancement of the spinal ganglia (arrowheads)
and cauda equina roots (dashed arrows)

Tiêu chuẩn Brighton trong chẩn đoán Guillain-Barre
Level 1 of Diagnostic Certainty
Bilateral AND flaccid weakness of the limbs
AND
Decreased or absent deep tendon reflexes in weak limbs
AND
Monophasic illness pattern AND interval between onset and nadir of weakness between 12 hours
and 28 days AND subsequent clinical plateau
AND
Electrophysiologic findings consistent with Guillain-Barre syndrome (GBS)
AND
Albuminocytologic dissociation (ie, elevation of CSF protein level above laboratory normal value
and CSF total white blood cell count less than 50 cells/2L)
AND
Absence of an identified alternative diagnosis for weakness


Điều trị
GBS- Chẩn đoán lâm sàng- đối xứng
Can thiệp sớm cần thiết ngăn chận tiến triểnImmunotherapy là điều trị chuẩn mực
Thêm vào điều trị hổ trợ

Ích lợi của immunotherapy
Thay huyết tương (PE) có lợi trong vòng bốn tuần đầu tiên kể từ khi khởi phát,
nhưng hiệu quả lớn nhất khi bắt đầu sớm (trong vòng hai tuần đầu tiên).
Phác đồ thông thường năm lần PE trong hai tuần,
RCT đầu tiên về việc sử dụng IVIg (0,4 gram IVIg / kg trọng lượng / ngày trong
năm ngày liên tiếp) từ năm 1992, IVIg có hiệu quả như PE.
IVIg đã thay thế PE, phương pháp điều trị đầu tiên ở nhiều trung tâm, chủ yếu vì
sự tiện lợi và sẵn có của nó.

Đánh giá của Cochrane về việc sử dụng IVIg trong GBS cho thấy rằng không
có sự khác biệt giữa IVIg và PE liên quan đến sự cải thiện mức độ khuyết
tật sau 4 tuần, thời gian thở máy, tử vong, hoặc di chứng tàn tật.
Sự kết hợp của PE theo sau IVIg không tốt hơn đáng kể so với PE hoặc IVIg
một mình.
Steroid đường uống, hoặc methylprednisolone tiêm tĩnh mạch 500 mg /
ngày trong 5 ngày liên tiếp) một mình không có lợi trong GBS.
Sự kết hợp của IVIg và methylprednisolone tiêm tĩnh mạch không hiệu quả hơn IVIg một mình, nhưng có thể có một số tác dụng ngắn hạn.

Có rất nhiều bằng chứng chủ yếu từ phòng thí nghiệm, kích hoạt bổ thể đóng
một vai trò quan trọng trong GBS.
Tác dụng của Eculizumab (complement C5 inhibitor) được thí nghiệm đầu tiên
ở Scotland .
Nhật Bản gần đây đã nghiên cứu tác dụng của Eculizumab (JET-GBS), RCT
nhỏ này không cho thấy sự khác biệt đáng kể
Eculizumab có thể là một phương pháp điều trị hiệu quả cho GBS, nhưng cầnnghiên cứu bổ sung

Indication to start IVIg or PE
Severely affected patients (inability to walk unaided = GBS disability scale ≥3).
Start preferable within first 2 weeks from onset IVIg: 0.4g/kg for 5 days
(unknown whether 1.0g/kg for 2 days is superior)
PE: standard 5x PE with total exchange of five plasma volumes
Xem xét điều trị đặc hiệu IVIg hay PE
Unknown whether IVIg is effective Mildly affected patients (GBS disability
scale ≤2) or MFS patients
Indication for re-treatment with IVIg ?
Secondary deterioration after initial improvement or stabilization (treatment related
fluctuation): treat with 0.4g/kg for 5 days
No proven effect of re-treatment with IVIg in patients who continue to worsen
Theo dõi và điều trị nâng đỡ
During the initial phase of GBS, all patients require close monitoring of motor,
autonomic (ie, blood pressure, heart rate and sphincter function), and
respiratory function
Patients should be electively intubated if clinical evaluation or pulmonary
function tests suggest impending respiratory failure. Vigilance is essential since
respiratory deterioration can occur rapidly
Mortality is often due to complications such as nosocomial infection, acute
respiratory arrest, deep venous thrombosis with pulmonary embolism, and
pneumothorax

Rapidly progressive severe weakness often with impaired respiration
(vital capacity < 20 ml/kg), and or direct need for artificial ventilation
Insufficient swallowing with high chance for pulmonary infection
Severe autonomic dysfunction
Chỉ định điều trị tích cực

Sự thận trong là cần thiết khi chăm sóc bn GBS, sự tổn thương do liệt cơ xảy ra
nhanh chóng
Respiratory failure in GBS is common, and 15 to 30 percent of patients need ventilatory support.
Thus, close respiratory monitoring with frequent measurement (eg, every four hours) of vital
capacity and negative inspiratory force (NIF) should be instituted initially in all patients.
Bulbar dysfunction with swallowing problems and inability to clear secretions may add to the need
for ventilatory support.
Succinylcholine should be avoided when invasive airway management becomes necessary.
Respiratory failure

The following parameters warn of impending respiratory arrest and are an indication for
intubation:
Forced vital capacity < 20 mL/kg
Maximum inspiratory pressure <30 cmH2O
Maximum expiratory pressure <40 cmH2O
Specific clinical findings and measurements on admission predict a high risk for respiratory failure. In
a French prospective study of 722 patients with GBS not ventilated at admission, mechanical
ventilation was needed in 313 (43 percent). The following factors were identified as predictors of
respiratory failure:
●Time of onset to admission less than seven days
●Inability to cough
●Inability to stand
●Inability to lift the elbows
●Inability to lift the head
●Liver enzyme increases
In patients with at least four of these six predictors, mechanical ventilation was required in >85%

Another report of 397 patients with GBS found that independent predictors of the
need for mechanical ventilation on admission were as follows:
●Fewer days between onset of weakness and admission
●Presence of facial or bulbar weakness
●Severe muscle weakness
Weaning from mechanical ventilation should be guided by improvement in strength and serial
pulmonary function tests (PFTs).
Tracheostomy should be performed after two weeks if PFTs do not show any significant
improvement from baseline, but can be deferred for another week if PFTs do show improvement

Autonomic dysfunction is a well-recognized feature of GBS and is a
significant source of mortality.
Consequently, close monitoring of blood pressure, fluid status, and cardiac
rhythm are essential to the management of these patients.
Care must also be taken when vasoactive or sedative drugs are used, because
GBS-related dysautonomia may exaggerate the hypotensive responses to
these drugs
Rối loạn thần kinh tự động

Dysautonomia occurs in 70 percent of patients and manifests as symptoms that
include: Tachycardia (the most common), urinary retention, hypertension
alternating with hypotension, orthostatic hypotension, bradycardia, other
arrhythmias, ileus, and loss of sweating.
Severe autonomic disturbances occur in about 20 percent of patients, mostly (but
not always) in patients who develop severe weakness and respiratory failure.

Cardiovascular complications of GBS are an important cause of morbidity.
Common manifestations include paroxysmal fluctuations in blood pressure, and
tachy and bradyarrhythmias, while less frequent manifestations include
myocardial involvement ranging from myocarditis to heart failure
Therefore, cardiac rhythm and blood pressure monitoring for patients in the
progressive phase of GBS.
Điều trị tim mạch









Dự hậu
Dự hậu xấu




