business case for geraldton health campus
TRANSCRIPT
WA Country Health Service
BUSINESS CASE (2017)
FOR
GERALDTON HEALTH CAMPUS REDEVELOPMENT PROJECT
STAGE ONE and
COMMUNITY MENTAL HEALTH STEP UP/STEP DOWN SERVICE
WA COUNTRY HEALTH SERVICE
Capital Funding $79.206 million
Recurrent Funding $4.265 million
Version 7.0 17 January 2018
WA Country Health Service
Version Control Version Date Issued to Comment Issued By
V1.0 22 November 2017
J. Calver, WACHS Midwest A. Jalleh, DoH S. Matthews, WACHS Central R. Pulsford, WACHS Central
Draft for Review J. Thorley, CBRE
V2.0 01 December 2017
J. Calver, WACHS Midwest A. Jalleh, DoH S. Matthews, WACHS Central R. Pulsford, WACHS Central
Draft for Review J. Thorley, CBRE
V3.0 07 December 2017
J. Calver, WACHS Midwest A. Jalleh, DoH S. Matthews, WACHS Central R. Pulsford, WACHS Central
Draft for Review J. Thorley, CBRE
V4.0 13 December 2017
J. Calver, WACHS Midwest A. Jalleh, DoH S. Matthews, WACHS Central R. Pulsford, WACHS Central
Draft for Review J. Thorley, CBRE
V5.0 20 December 2017
J. Calver, WACHS Midwest A. Jalleh, DoH S. Matthews, WACHS Central R. Pulsford, WACHS Central
Final draft for Review
J. Thorley, CBRE
V6.0 22 December 2017
S. Matthews, WACHS Central R. Pulsford, WACHS Central
WACHS Amended Draft
J.Calver, WACHS Midwest
V6.1 3 January 2018
J Moffet, WACHS Central S Matthews, WACHS Central
WACHS Amended Draft
R Hosking, WACHS Central
V6.2 4 January 2018
S Matthews, WACHS Central WACHS Amended Draft
R Hosking, WACHS Central
V7.0 18 January 2018
J. Calver, WACHS Midwest A. Jalleh, DoH S. Matthews, WACHS Central R. Pulsford, WACHS Central
Amended final draft for Review
J. Thorley, CBRE
SIGNATORY PAGE
1. WA Gountry Health ServiceIn accordance with the conditions overleaf, this business case is:
ENDORSED
A/AREA DI RECTOR, INFRASTRUCTURE
APPROVED ON BEHALF OF AGENCY
,/-{
(*^-i-l/-+^'vl
SignedShane MatthewsA/CHIEF EXECUTIVE OFFICER
COMMENTS (or reference to attachments):
APPROVED ON BEHALF OF AGENCY
SignedTimothy MarneyMENTAL HEALTH COMMISSIONER
COMMENTS (or reference to attachments):
19 January 2018
1 9 January 201 8Date
2. Mental Health CommissionIn accordance with the conditions overleaf, this business case is:
WA Country Health Service
CONDITIONS RELATED TO BUSINESS CASE APPROVAL
1. By signing a business case on behalf of an Agency, the signatory is verifying to
Government that:
(a) The Agency supports the recommendation described in the business case (b) The business case has been prepared in accordance with the Strategic Asset
Management Framework (c) The need described in this business case is consistent with the priorities and strategies of
the Agency as described in its most recent corporate and strategic asset planning documents
(d) The specified benefits appear achievable, and are expected to be realised within the timeframe described
(e) The cost estimates for the ‘transition to operation’ and ongoing recurrent impacts are all-inclusive and realistic
(f) Land issues have been identified with strategies to resolve included in the business case (g) Key stakeholders are not opposed to the recommendation, except where otherwise noted
in the business case.
2. By signing a business case on behalf of the Department of Finance’s Building Management and Works (BMW), the signatory is verifying to Government that:
(a) The business case appropriately: • considers the range of business options available (long list) • shortlists options • includes the ‘do nothing’ option • describes the scope and evaluates the impacts of the shortlisted options,
to enable a comparative assessment in accordance with Building Management and Works guidelines and the Strategic Asset Management Framework;
(b) Land issues have been identified with strategies to resolve included in the business case (c) Non-residential buildings contemplated in the shortlisted options are of an appropriate
design quality consistent with relevant Government policies and standards (d) The time and cost estimates for the project definition, delivery and operations and
maintenance phases have been developed in accordance with relevant benchmarks, by suitably qualified and experienced persons, in accordance with Building Management and Works estimating processes and with an appropriate amount of contingency.
WA Country Health Service
Table of Contents 1 EXECUTIVE SUMMARY ...................................................................................................................... 1
1.1 KEY PROJECT DRIVERS ............................................................................................................... 1 1.2 PROJECT OBJECTIVES ................................................................................................................. 2
1.2.1 Geraldton Health Campus .................................................................................................. 2 1.2.2 Integrated Midwest Mental Health Services ....................................................................... 3
1.3 OPTIONS DEVELOPMENT ............................................................................................................. 3 1.3.1 Summary of Options ........................................................................................................... 6
1.4 PREFERRED OPTION ................................................................................................................. 12 1.4.1 Budget and Funding ......................................................................................................... 12
1.5 PROGRAM/KEY MILESTONES ..................................................................................................... 16 1.6 RECOMMENDATION .................................................................................................................... 17
2 PROJECT SCOPE AND EVALUATION ............................................................................................. 18 2.1 PROJECT PURPOSE ................................................................................................................... 18
2.1.1 Geraldton Health Campus ................................................................................................ 18 2.1.2 Integrated Midwest Mental Health Services ..................................................................... 21
2.2 WA STATE GOVERNMENT FUNDING AMOUNT ............................................................................. 26 2.3 PROJECT DESCRIPTION ............................................................................................................. 27
2.3.1 Geraldton Health Campus ................................................................................................ 27 2.3.2 Community Mental Health Step Up/Step Down Service................................................... 27 2.3.3 Gap Analysis ..................................................................................................................... 30
2.4 BACKGROUND ........................................................................................................................... 40 2.4.1 Approvals .......................................................................................................................... 44 2.4.2 Supporting Documenatation ............................................................................................. 46
2.5 POLICY AND STRATEGIC FRAMEWORK ........................................................................................ 46 2.5.1 Geraldton Health Campus ................................................................................................ 46 2.5.2 Community Mental Health Step Up/Step Down Services ................................................. 47 2.5.3 Policy Objectives............................................................................................................... 47 2.5.4 Alignment to Related Strategic Imperatives ..................................................................... 48
2.6 PROJECT DELIVERABLES ........................................................................................................... 52 2.7 STAKEHOLDER ENGAGEMENT .................................................................................................... 57 2.8 CRITICAL ASSUMPTIONS ............................................................................................................ 60 2.9 SOCIAL AND ECONOMIC ANALYSES ............................................................................................ 61 2.10 ASSESSMENT OF OPTIONS ......................................................................................................... 64
2.10.1 Information and Communication Technology ................................................................... 78 2.10.2 Evaluation of Options ........................................................................................................ 79
2.11 FUNDING STRATEGY .................................................................................................................. 79 2.11.1 Total Budget ...................................................................................................................... 79 2.11.2 Funding Amount................................................................................................................ 81 2.11.3 Sustainability and Ongoing Viability – Recurrent Costs ................................................... 82
2.12 PROJECT TIMEFRAME AND KEY MILESTONES .............................................................................. 90 2.13 RISK ANALYSIS .......................................................................................................................... 91 2.14 LOCAL CONTENT ....................................................................................................................... 94 2.15 ABORIGINAL PARTICIPATION ....................................................................................................... 95 2.16 STATE FUNDED INFRASTRUCTURE AND APPRENTICESHIP PARTICIPATION ..................................... 95
3 IMPLEMENTATION STRATEGY ....................................................................................................... 96 3.1 COMMUNICATION PLAN .............................................................................................................. 96
3.1.1 Summary Communications Plan ...................................................................................... 97 3.2 PROJECT MANAGEMENT ............................................................................................................ 99 3.3 PROJECT GOVERNANCE .......................................................................................................... 100
3.3.1 WACHS Governance Framework for Infrastructure Projects ......................................... 100 3.3.2 Mental Health Commission Governance Framework - Community Mental Health Step Up/Step Down Service ................................................................................................................. 101
3.4 PROCUREMENT STRATEGY ...................................................................................................... 103 3.4.1 WA Country Health Service ............................................................................................ 103 3.4.2 Community Mental Health Step Up/Step Down Services ............................................... 104

WA Country Health Service
3.5 SUPPORTING DOCUMENTS ....................................................................................................... 106 4 RECOMMENDATION ....................................................................................................................... 108 5 NEXT STEPS .................................................................................................................................... 109 APPENDIX A - GHC CONCEPT BRIEF APPENDIX B - GHC CONCEPT MASTER DEVELOPMENT PLAN
OPTION 2 – GROUND FLOOR PLAN OPTION 3 – GROUND FLOOR PLAN OPTION 4 - GROUND FLOOR PLAN OPTION 4 - FIRST FLOOR PLAN
APPENDIX C - COMMUNITY MENTAL HEALTH STEP UP/STEP DOWN SERVICE CONCEPT BRIEF APPENDIX D - COMMUNITY MENTAL HEALTH STEP UP/STEP DOWN SERVICE CONCEPT MASTER DEVELOPMENT PLAN
WA Country Health Service
Acronyms Abbreviation
ABF Activity Based Funding ACAT Aged Care Assessment Team ACCS Aged and Community Care Service AHFG Australasian Health Facility Guidelines AOD Alcohol Other Drugs APU Acute Psychiatric Unit BCA Building Condition Audit BMW Building Management and Works CADS Community Alcohol and Drug Service CAP Care Awaiting Placement CCTV Closed Circuit Television CMDP Concept Master Development Plans CMSAC Carnarvon Medical Service Aboriginal Corporation CPCG Capital Project Control Group CSF Clinical Services Framework CT Computed Tomography CTT Community Treatment Team DHAC District Health Advisory Council DoF Department of Finance DoH Department of Health DoCH Department of Communities, Housing DSU Day Surgery Unit EOI Expression of Interest ETS Emergency Telehealth Service FTE Full Time Equivalents GHC Geraldton Health Campus GRAMS Geraldton Regional Aboriginal Medical Service HACC Home and Community Care HITH Hospital in the Home ICT Information and Communication Technology IPU Inpatient Unit ISG Infrastructure Steering Group LDR Labour Delivery Room MH Mental Health MHC Mental Health Commission MHSSU Mental Health Short Stay Unit MMH Midwest Mental Health MOU Memorandum of Understanding MRI Magnetic Resonance Imaging MWDC Midwest Development Commission MWHI Midwest Health Initiative NCC National Construction Code NGO Non-Government Organisation OPG Orthopantomogram PDP Project Definition Plan PWG Project Working Group RFDS Royal Flying Doctor Service RLB Rider Levett Bucknall SCGH Sir Charles Gardiner Hospital step up/step down Community Mental Health step up/step down service WA Western Australia WACHS WA Country Health Service Definition: Aboriginal - The use of the word Aboriginal in this document refers to persons who are of Aboriginal and Torres Strait Islander descent.
WA Country Health Service
1 Executive Summary WA Country Health Service in partnership with the Mental Health Commission presents this Business Case to the WA State Government to seek a capital investment of $79.206 million for redevelopment of the Geraldton Health Campus and the development of an integrated Midwest Mental Health service. A recurrent investment of $4.265 million for a Community mental health step up/step down service is also sought from the WA State Government. This investment is requested to deliver a combination of new build and refurbishment infrastructure; to address the inability to meet current demand, increasing activity and accommodate the projected demand for services to 2025/26. In early 2017 the West Australian Labor Party committed to undertake a major staged redevelopment of the Geraldton Health Campus. The commitment included an upgrade to the Geraldton Hospital Emergency Service, an Acute Mental Health Facility, Mental Health Observation Area and subacute beds. The scope has been defined with stage one to include:
• An expanded Emergency/Critical Care aligning with projected service need to 2024;
• Acute Psychiatric Unit; • Mental Health Short Stay Unit; • Essential engineering service upgrades including the replacement of the chillers;
and • Community Mental Health step up/step down service located on another site.
In September 2017, WA Country Health Service confirmed the progression of this Business Case to secure funding for the Geraldton Health Campus site and the offsite Community mental health step up/step down service. This Business Case outlines the four options developed, for the Geraldton Health Campus, in response to the staged redevelopment. There is only one option for the Community mental health step up/step down service. WA Country Health Service is seeking funding on behalf of the Mental Health Commission. Granted funding would then be transferred to the Mental Health Commission.
1.1 Key Project Drivers
The key project drivers for this Business Case include:
• Alleviation of inadequate emergency and critical care infrastructure capacity for the Midwest. Delivery of infrastructure that is commensurate with demand, and reduces current clinical risks associated with infrastructure constraints, particularly acute patient transfers.
• The existing built infrastructure does not comply with relevant codes, safety related standards and the Australasian Health Facility Guidelines;
• Suboptimal service provision has resulted in reduced access and equity to healthcare compromising care closer to home;
• Current facilities are under unreasonable and increasing pressure, which compromises patient, visitor and staff safety;
• Site engineering services and infrastructure are currently at maximum capacity;
P a g e | 1
WA Country Health Service
• Improvement of key departmental functional relationships is required to facilitate efficient delivery of contemporary models of care;
• Provision of appropriate single rooms is required to meet growing demand for the care of patients with infectious diseases or those requiring single rooms for clinical reasons;
• Delivery of purpose built mental health inpatient beds in the Midwest, in the context of the future closure of Graylands Hospital significantly impacting on the available mental health beds for the Midwest;
• Existing community mental health treatment and alcohol and drug facilities are sub optimal, not purpose designed and are at capacity;
• Opportunity for master planning of the entire Geraldton Health Campus site as not to preclude any future collocation of other public services or private service operators; and
• The development of a purpose-built Community mental health step up/step down service to enable the delivery of services in accordance with contemporary models of care and allows consumers to be housed in an appropriate therapeutic environment.
Details of the service gap between current service delivery and projected demand and future service delivery is outlined in section 2.3.3.
1.2 Project Objectives
1.2.1 Geraldton Health Campus
The overarching vision for the Geraldton Health Campus is to provide safe and efficient health care to the residents of Geraldton and the Midwest region in line with contemporary models of care and as required from a Regional Resource Centre. It is acknowledged that the demand on services and the scope of work to redevelop the entire Geraldton Health Campus is significant and will require a staged approach. Stage Three identifies the potential for a private provider, to relocate relevant services onto the campus. The Stage One redevelopment will enable Geraldton Health Campus to safely manage health demand for emergency/critical care and mental health services that align with contemporary models of care by providing the following:
• A combination of level 4 and 5 emergency/critical care and mental health services onsite as per the role delineation in the WA Health Clinical Services Framework 2014 – 2024;
• Delivery of services in alignment with the Western Australian, Mental Health Alcohol and Other Drug Services Plan 2015 – 2025;
• Expansion of departments included in Stage One scope in response to updated role delineation in the WA Health Clinical Services Framework 2014 – 2024;
• Consumer centred health care services provided in a contemporary facility that enhances consumer recovery, safety and health outcomes;
• Co-located Midwest Mental Health and Community Alcohol and Drug Service; • Delivery of socially and culturally appropriate care; • Improved access to services; • Information and Communication Technology advancements for better care; in
particular Emergency Telehealth Services and Videoconferencing, Education and Communication; and
P a g e | 2
WA Country Health Service
• Essential engineering upgrades including the replacement of the chillers, to ensure continuation and safe provision of healthcare services.
1.2.2 Integrated Midwest Mental Health Services
In addition to the overarching vision for the Geraldton Health Campus, a region wide integrated mental health vision has been developed in response to the fact that there are no mental health inpatient beds, no Community mental health step-up/step-down beds, and minimal community treatment and support services for mental health and alcohol and other drugs. The integration will reduce the clinical risk to the individual by promoting best practice and contemporary models of care. In accordance with guiding principles and in alignment with the Western Australian, Mental Health Alcohol and Other Drug Services Plan 2015 – 2025 the following will be provided:
• Level 5 Adult Mental Health Inpatient services as per the role delineation in the WA Health Clinical Services Framework 2014 – 2024 and in accordance with The Chief Psychiatrist’s Standards for the Authorisation of Hospital Under the Mental Health Act 1996.
• Delivery of services upholding human rights and in accordance with the WA Mental Health Act 2014, including the WA Chief Psychiatrists Standards for Clinical Care and Charter of Mental Health Care Principles;
• The implementation of effective prevention, mental health promotion and early intervention activity;
• Recovery oriented practice, including supporting people to stay connected in their community;
• Holistic approach to all services; • Collaborative approach between consumers, families and carers with the
planning and delivery of appropriate services; • A balance between hospital based and community based services; • Evidence based service delivery models; • Expansion of services into the Midwest region; • Collaboration with appropriate Non-Government Organisations and primary care
service providers to deliver contemporary service delivery models; • Alcohol and other Drug services; • Culturally appropriate consumer focused care; • Integrated services for co-existing conditions; • An appropriate mix of services to meet individual requirements; • Service development across consumer lifespan; and • Services that assist individuals to avoid coming into contact with the criminal
justice system.
1.3 Options Development
The proposed combined redevelopment of the Geraldton Health Campus and the offsite Community mental health step up/step down service consists of three stages as summarised in the table below. The Community Mental Health step up/step down service is in Stage One. It should be noted that this Business Case is seeking funding for Stage One only and that the stages can be procured independent of each other.
P a g e | 3
WA Country Health Service
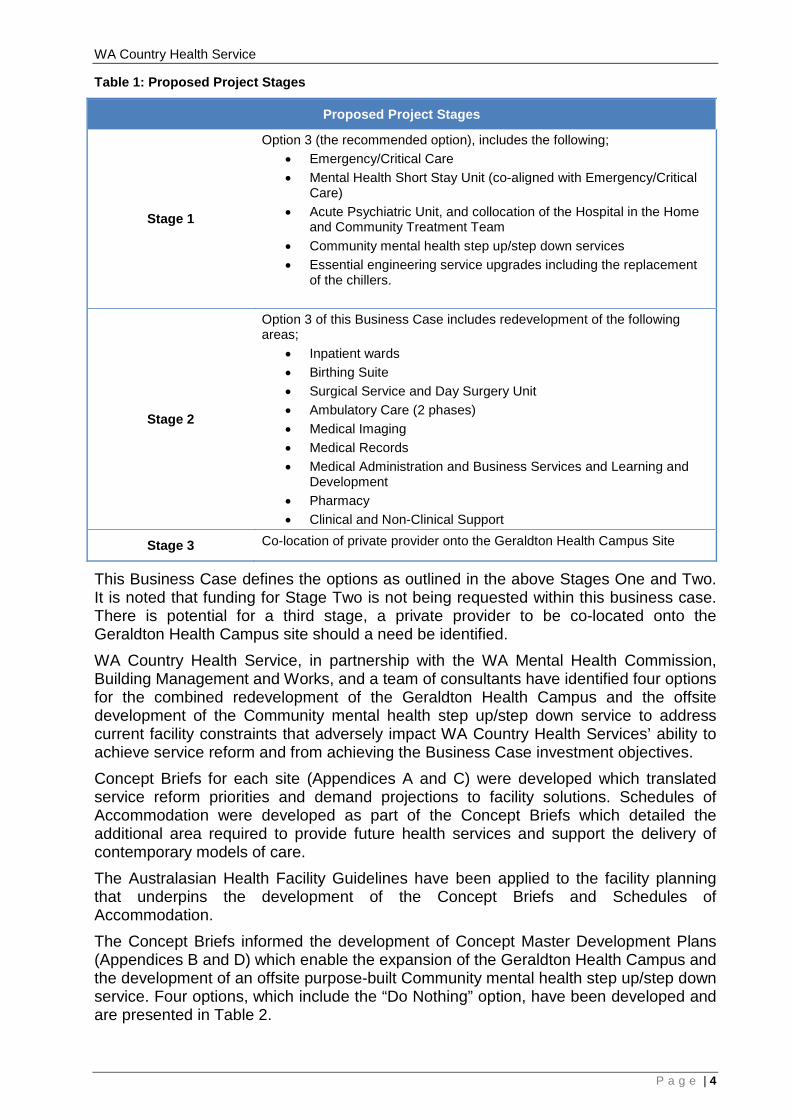
Table 1: Proposed Project Stages
Proposed Project Stages
Stage 1
Option 3 (the recommended option), includes the following; • Emergency/Critical Care • Mental Health Short Stay Unit (co-aligned with Emergency/Critical
Care) • Acute Psychiatric Unit, and collocation of the Hospital in the Home
and Community Treatment Team • Community mental health step up/step down services • Essential engineering service upgrades including the replacement
of the chillers.
Stage 2
Option 3 of this Business Case includes redevelopment of the following areas;
• Inpatient wards • Birthing Suite • Surgical Service and Day Surgery Unit • Ambulatory Care (2 phases) • Medical Imaging • Medical Records • Medical Administration and Business Services and Learning and
Development • Pharmacy • Clinical and Non-Clinical Support
Stage 3 Co-location of private provider onto the Geraldton Health Campus Site
This Business Case defines the options as outlined in the above Stages One and Two. It is noted that funding for Stage Two is not being requested within this business case. There is potential for a third stage, a private provider to be co-located onto the Geraldton Health Campus site should a need be identified. WA Country Health Service, in partnership with the WA Mental Health Commission, Building Management and Works, and a team of consultants have identified four options for the combined redevelopment of the Geraldton Health Campus and the offsite development of the Community mental health step up/step down service to address current facility constraints that adversely impact WA Country Health Services’ ability to achieve service reform and from achieving the Business Case investment objectives. Concept Briefs for each site (Appendices A and C) were developed which translated service reform priorities and demand projections to facility solutions. Schedules of Accommodation were developed as part of the Concept Briefs which detailed the additional area required to provide future health services and support the delivery of contemporary models of care. The Australasian Health Facility Guidelines have been applied to the facility planning that underpins the development of the Concept Briefs and Schedules of Accommodation. The Concept Briefs informed the development of Concept Master Development Plans (Appendices B and D) which enable the expansion of the Geraldton Health Campus and the development of an offsite purpose-built Community mental health step up/step down service. Four options, which include the “Do Nothing” option, have been developed and are presented in Table 2.
P a g e | 4

WA Country Health Service
The Geraldton Health Campus Concept Master Development Plan options have been assessed on the basis that planning includes capacity for other facilities (public and/or private) to be located on the site as part of potential future developments. Consideration has been given to collaboration with private sector provider/s with the potential for the provider to be located on the North West corner of the Geraldton Health Campus site. This option requires further investigation prior to inclusion in future stages.
P a g e | 5
WA Country Health Service
1.3.1 Summary of Options
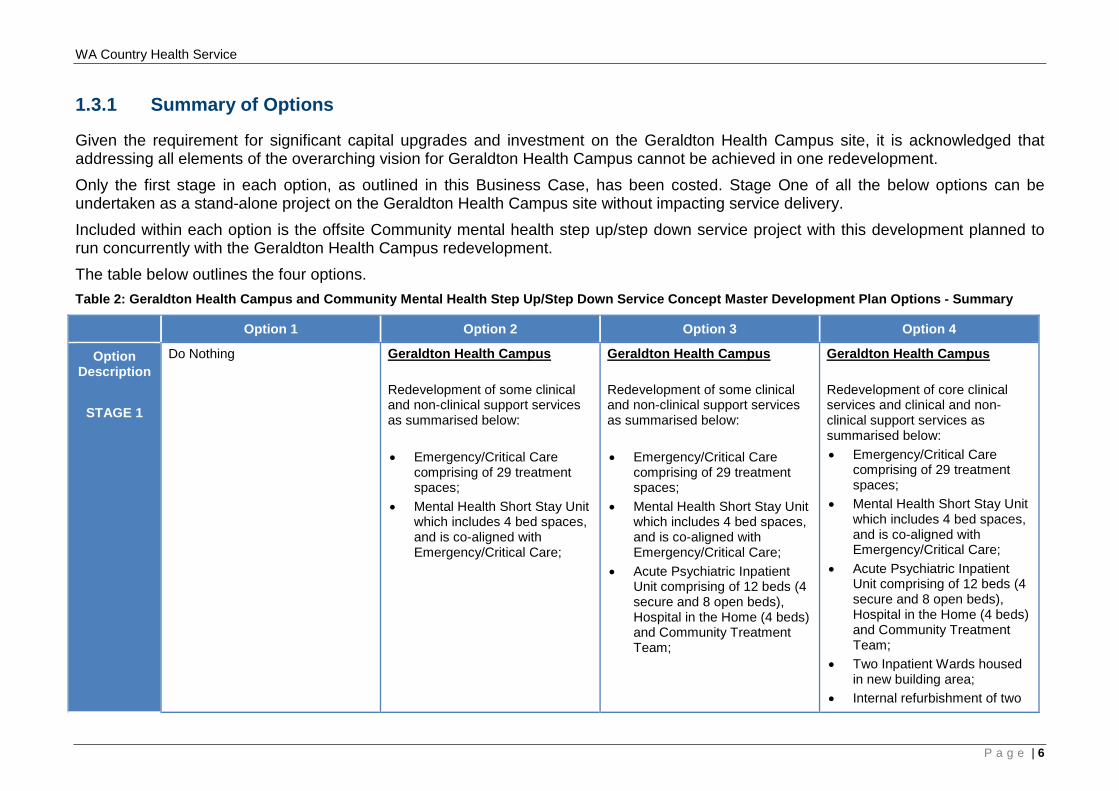
Given the requirement for significant capital upgrades and investment on the Geraldton Health Campus site, it is acknowledged that addressing all elements of the overarching vision for Geraldton Health Campus cannot be achieved in one redevelopment. Only the first stage in each option, as outlined in this Business Case, has been costed. Stage One of all the below options can be undertaken as a stand-alone project on the Geraldton Health Campus site without impacting service delivery. Included within each option is the offsite Community mental health step up/step down service project with this development planned to run concurrently with the Geraldton Health Campus redevelopment. The table below outlines the four options. Table 2: Geraldton Health Campus and Community Mental Health Step Up/Step Down Service Concept Master Development Plan Options - Summary
Option 1 Option 2 Option 3 Option 4
Option Description
STAGE 1
Do Nothing Geraldton Health Campus Redevelopment of some clinical and non-clinical support services as summarised below: • Emergency/Critical Care
comprising of 29 treatment spaces;
• Mental Health Short Stay Unit which includes 4 bed spaces, and is co-aligned with Emergency/Critical Care;
Geraldton Health Campus Redevelopment of some clinical and non-clinical support services as summarised below: • Emergency/Critical Care
comprising of 29 treatment spaces;
• Mental Health Short Stay Unit which includes 4 bed spaces, and is co-aligned with Emergency/Critical Care;
• Acute Psychiatric Inpatient Unit comprising of 12 beds (4 secure and 8 open beds), Hospital in the Home (4 beds) and Community Treatment Team;
Geraldton Health Campus Redevelopment of core clinical services and clinical and non-clinical support services as summarised below: • Emergency/Critical Care
comprising of 29 treatment spaces;
• Mental Health Short Stay Unit which includes 4 bed spaces, and is co-aligned with Emergency/Critical Care;
• Acute Psychiatric Inpatient Unit comprising of 12 beds (4 secure and 8 open beds), Hospital in the Home (4 beds) and Community Treatment Team;
• Two Inpatient Wards housed in new building area;
• Internal refurbishment of two
P a g e | 6
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 • Reconfiguration of Main Entry
due to new road and parking
• Reconfiguration of Main Entry
due to new road and parking
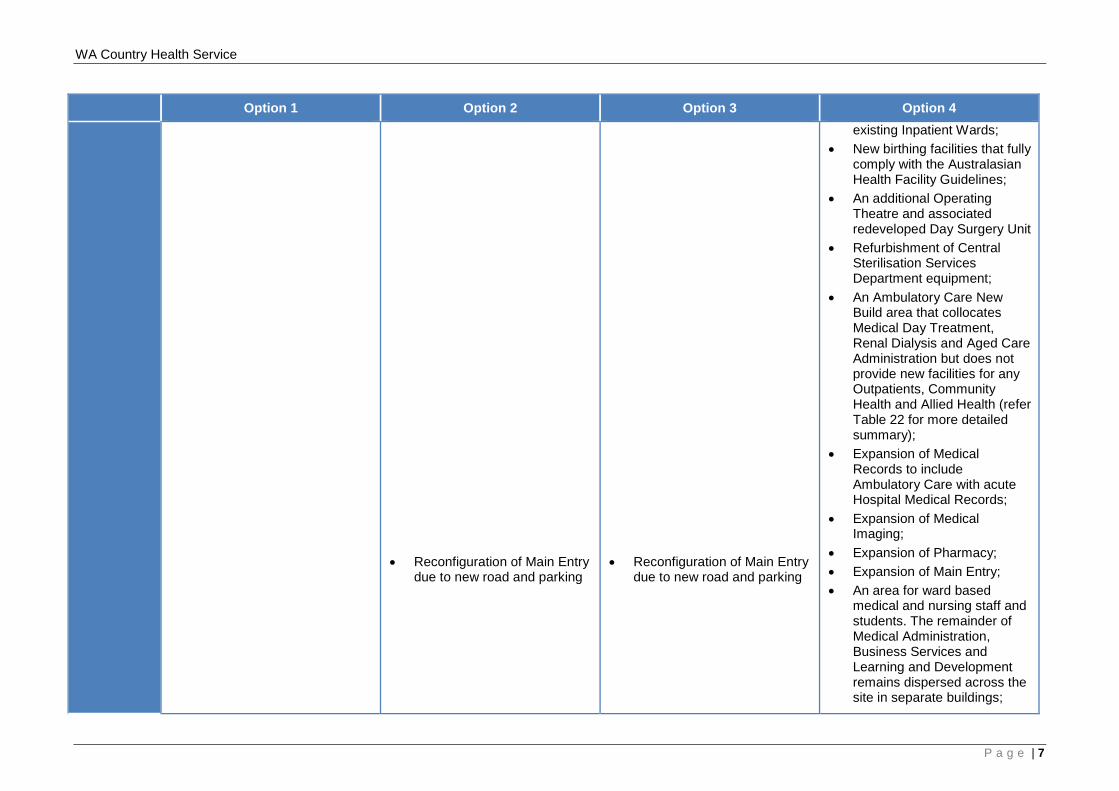
existing Inpatient Wards; • New birthing facilities that fully
comply with the Australasian Health Facility Guidelines;
• An additional Operating Theatre and associated redeveloped Day Surgery Unit
• Refurbishment of Central Sterilisation Services Department equipment;
• An Ambulatory Care New Build area that collocates Medical Day Treatment, Renal Dialysis and Aged Care Administration but does not provide new facilities for any Outpatients, Community Health and Allied Health (refer Table 22 for more detailed summary);
• Expansion of Medical Records to include Ambulatory Care with acute Hospital Medical Records;
• Expansion of Medical Imaging;
• Expansion of Pharmacy; • Expansion of Main Entry; • An area for ward based
medical and nursing staff and students. The remainder of Medical Administration, Business Services and Learning and Development remains dispersed across the site in separate buildings;
P a g e | 7
WA Country Health Service
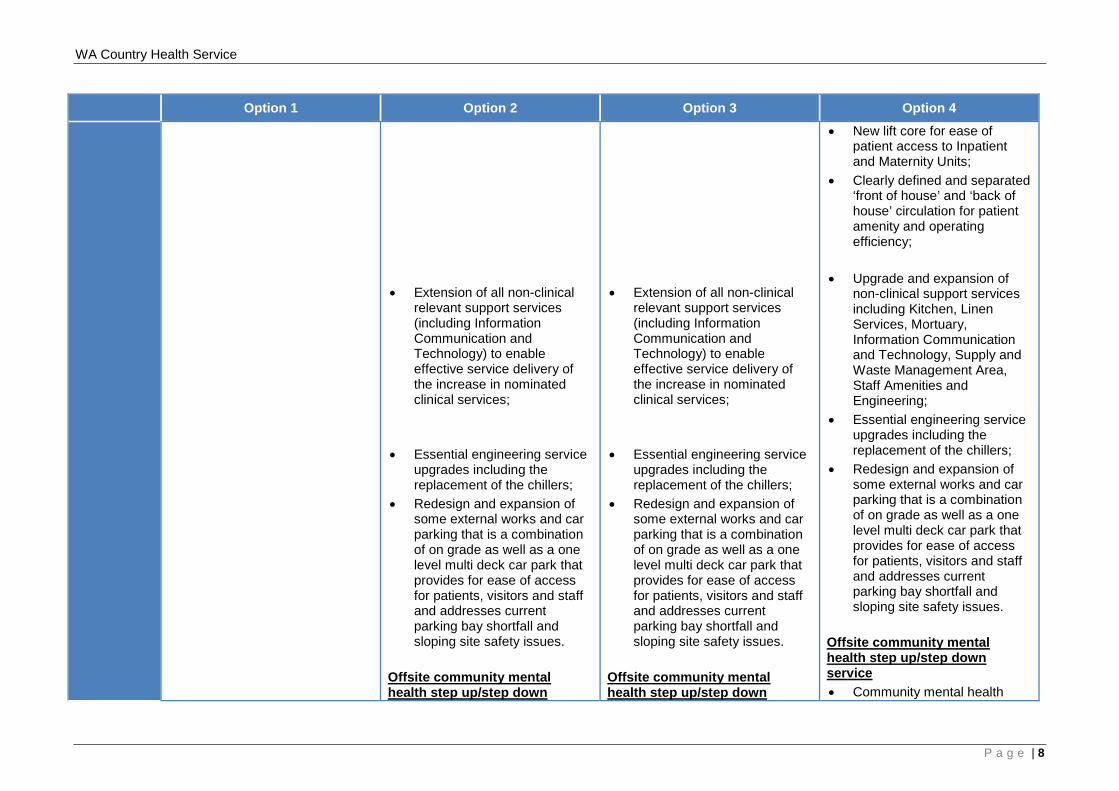
Option 1 Option 2 Option 3 Option 4 • Extension of all non-clinical
relevant support services (including Information Communication and Technology) to enable effective service delivery of the increase in nominated clinical services;
• Essential engineering service
upgrades including the replacement of the chillers;
• Redesign and expansion of some external works and car parking that is a combination of on grade as well as a one level multi deck car park that provides for ease of access for patients, visitors and staff and addresses current parking bay shortfall and sloping site safety issues.
Offsite community mental health step up/step down
• Extension of all non-clinical
relevant support services (including Information Communication and Technology) to enable effective service delivery of the increase in nominated clinical services;
• Essential engineering service
upgrades including the replacement of the chillers;
• Redesign and expansion of some external works and car parking that is a combination of on grade as well as a one level multi deck car park that provides for ease of access for patients, visitors and staff and addresses current parking bay shortfall and sloping site safety issues.
Offsite community mental health step up/step down
• New lift core for ease of patient access to Inpatient and Maternity Units;
• Clearly defined and separated ‘front of house’ and ‘back of house’ circulation for patient amenity and operating efficiency;
• Upgrade and expansion of
non-clinical support services including Kitchen, Linen Services, Mortuary, Information Communication and Technology, Supply and Waste Management Area, Staff Amenities and Engineering;
• Essential engineering service upgrades including the replacement of the chillers;
• Redesign and expansion of some external works and car parking that is a combination of on grade as well as a one level multi deck car park that provides for ease of access for patients, visitors and staff and addresses current parking bay shortfall and sloping site safety issues.
Offsite community mental health step up/step down service • Community mental health
P a g e | 8
WA Country Health Service
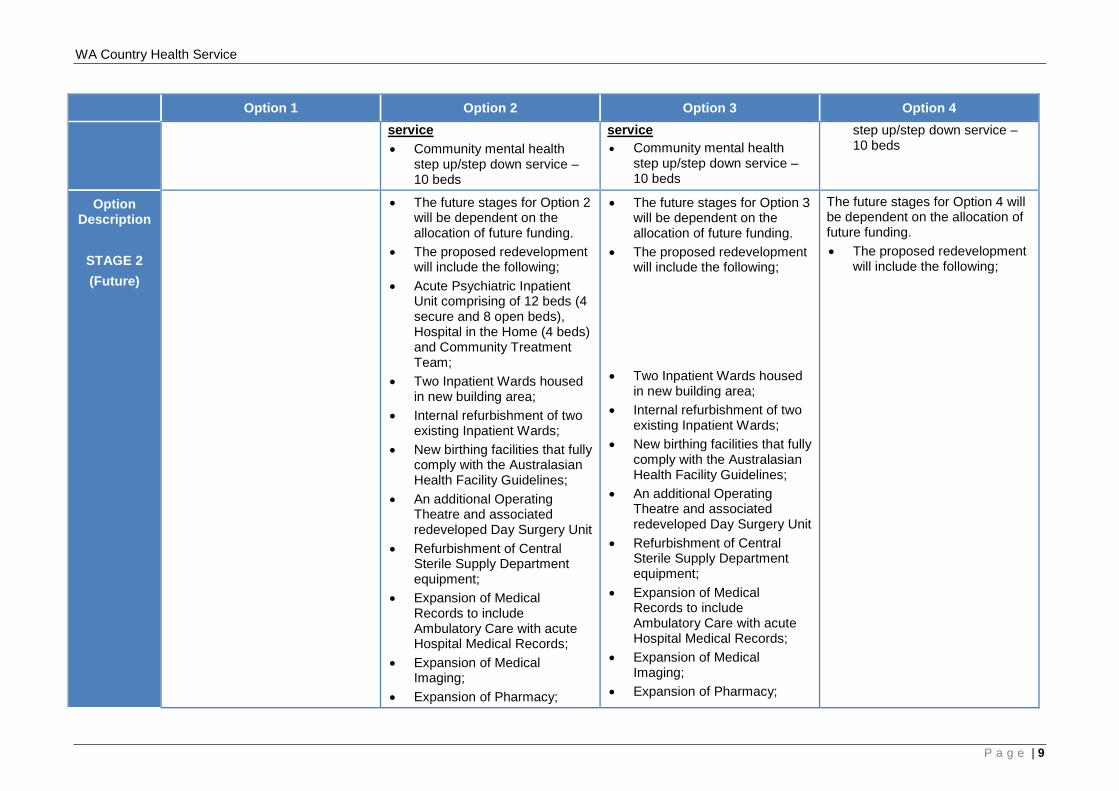
Option 1 Option 2 Option 3 Option 4 service • Community mental health
step up/step down service – 10 beds
service • Community mental health
step up/step down service – 10 beds
step up/step down service – 10 beds
Option Description
STAGE 2 (Future)
• The future stages for Option 2 will be dependent on the allocation of future funding.
• The proposed redevelopment will include the following;
• Acute Psychiatric Inpatient Unit comprising of 12 beds (4 secure and 8 open beds), Hospital in the Home (4 beds) and Community Treatment Team;
• Two Inpatient Wards housed in new building area;
• Internal refurbishment of two existing Inpatient Wards;
• New birthing facilities that fully comply with the Australasian Health Facility Guidelines;
• An additional Operating Theatre and associated redeveloped Day Surgery Unit
• Refurbishment of Central Sterile Supply Department equipment;
• Expansion of Medical Records to include Ambulatory Care with acute Hospital Medical Records;
• Expansion of Medical Imaging;
• Expansion of Pharmacy;
• The future stages for Option 3 will be dependent on the allocation of future funding.
• The proposed redevelopment will include the following;
• Two Inpatient Wards housed
in new building area; • Internal refurbishment of two
existing Inpatient Wards; • New birthing facilities that fully
comply with the Australasian Health Facility Guidelines;
• An additional Operating Theatre and associated redeveloped Day Surgery Unit
• Refurbishment of Central Sterile Supply Department equipment;
• Expansion of Medical Records to include Ambulatory Care with acute Hospital Medical Records;
• Expansion of Medical Imaging;
• Expansion of Pharmacy;
The future stages for Option 4 will be dependent on the allocation of future funding. • The proposed redevelopment
will include the following;
P a g e | 9
WA Country Health Service
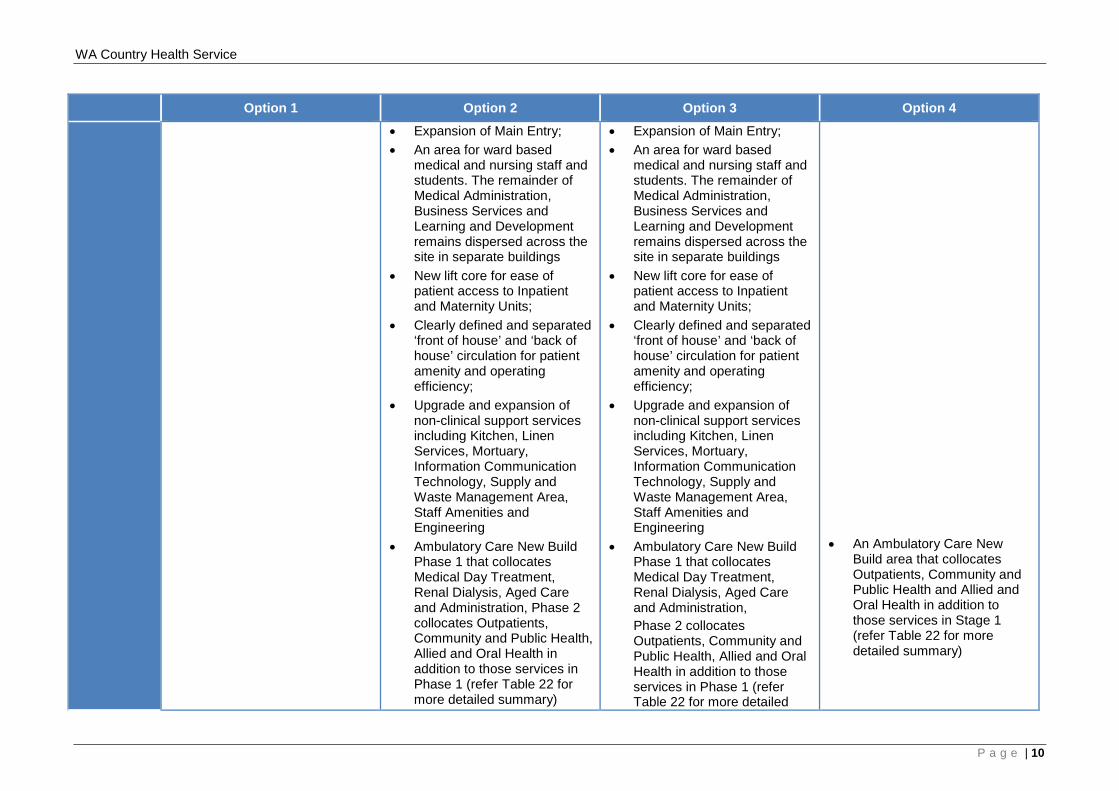
Option 1 Option 2 Option 3 Option 4 • Expansion of Main Entry; • An area for ward based
medical and nursing staff and students. The remainder of Medical Administration, Business Services and Learning and Development remains dispersed across the site in separate buildings
• New lift core for ease of patient access to Inpatient and Maternity Units;
• Clearly defined and separated ‘front of house’ and ‘back of house’ circulation for patient amenity and operating efficiency;
• Upgrade and expansion of non-clinical support services including Kitchen, Linen Services, Mortuary, Information Communication Technology, Supply and Waste Management Area, Staff Amenities and Engineering
• Ambulatory Care New Build Phase 1 that collocates Medical Day Treatment, Renal Dialysis, Aged Care and Administration, Phase 2 collocates Outpatients, Community and Public Health, Allied and Oral Health in addition to those services in Phase 1 (refer Table 22 for more detailed summary)
• Expansion of Main Entry; • An area for ward based
medical and nursing staff and students. The remainder of Medical Administration, Business Services and Learning and Development remains dispersed across the site in separate buildings
• New lift core for ease of patient access to Inpatient and Maternity Units;
• Clearly defined and separated ‘front of house’ and ‘back of house’ circulation for patient amenity and operating efficiency;
• Upgrade and expansion of non-clinical support services including Kitchen, Linen Services, Mortuary, Information Communication Technology, Supply and Waste Management Area, Staff Amenities and Engineering
• Ambulatory Care New Build Phase 1 that collocates Medical Day Treatment, Renal Dialysis, Aged Care and Administration, Phase 2 collocates Outpatients, Community and Public Health, Allied and Oral Health in addition to those services in Phase 1 (refer Table 22 for more detailed
• An Ambulatory Care New Build area that collocates Outpatients, Community and Public Health and Allied and Oral Health in addition to those services in Stage 1 (refer Table 22 for more detailed summary)
P a g e | 10
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 summary)
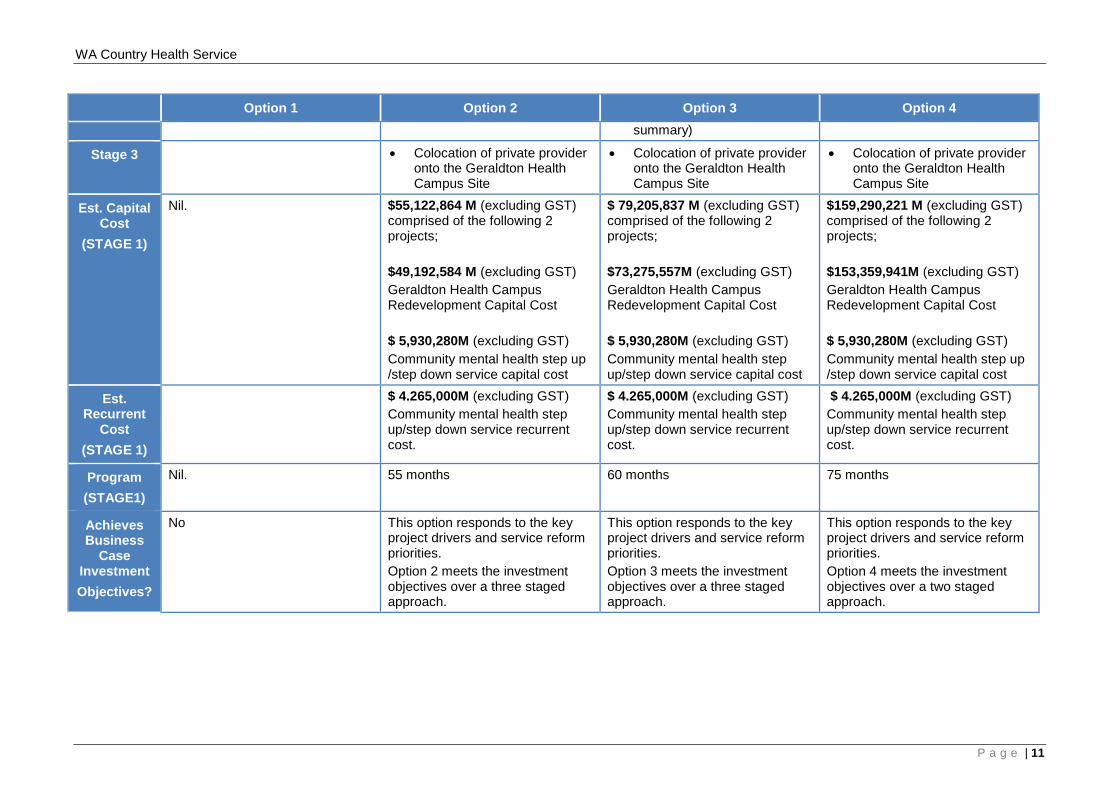
Stage 3 • Colocation of private provider onto the Geraldton Health Campus Site
• Colocation of private provider onto the Geraldton Health Campus Site
• Colocation of private provider onto the Geraldton Health Campus Site
Est. Capital Cost
(STAGE 1)
Nil. $55,122,864 M (excluding GST) comprised of the following 2 projects; $49,192,584 M (excluding GST) Geraldton Health Campus Redevelopment Capital Cost $ 5,930,280M (excluding GST) Community mental health step up /step down service capital cost
$ 79,205,837 M (excluding GST) comprised of the following 2 projects; $73,275,557M (excluding GST) Geraldton Health Campus Redevelopment Capital Cost $ 5,930,280M (excluding GST) Community mental health step up/step down service capital cost
$159,290,221 M (excluding GST) comprised of the following 2 projects; $153,359,941M (excluding GST) Geraldton Health Campus Redevelopment Capital Cost $ 5,930,280M (excluding GST) Community mental health step up /step down service capital cost
Est. Recurrent
Cost (STAGE 1)
$ 4.265,000M (excluding GST) Community mental health step up/step down service recurrent cost.
$ 4.265,000M (excluding GST) Community mental health step up/step down service recurrent cost.
$ 4.265,000M (excluding GST) Community mental health step up/step down service recurrent cost.
Program (STAGE1)
Nil. 55 months 60 months 75 months
Achieves Business
Case Investment Objectives?
No This option responds to the key project drivers and service reform priorities. Option 2 meets the investment objectives over a three staged approach.
This option responds to the key project drivers and service reform priorities. Option 3 meets the investment objectives over a three staged approach.
This option responds to the key project drivers and service reform priorities. Option 4 meets the investment objectives over a two staged approach.
P a g e | 11
WA Country Health Service
1.4 Preferred Option
Option 3 is the recommended option as it addresses current and future critical infrastructure and service pressures, fulfills the overarching vision for the Geraldton Health Campus redevelopment and the offsite Community mental health step up/step down service by meeting the investment objectives and service reform priorities as highlighted in the following:
• WA Health Clinical Services Framework 2014 – 2024;• Western Australian, Mental Health Alcohol and Other Drug Services Plan 2015 –
2025;• Geraldton Health Campus WACHS Midwest Service Plan 2010-2020; and• Midwest Regional Blueprint 2015.
Option 3 Stage One delivers nominated clinical services and essential associated clinical, non-clinical and Community mental health support services at a capital cost of $79.206 million. Recurrent funding of $4.265 million is required for the offsite Community mental health step up/step down service as this is a new stand-alone facility.
P a g e | 12
WA Country Health Service
P a g e | 13
WA Country Health Service
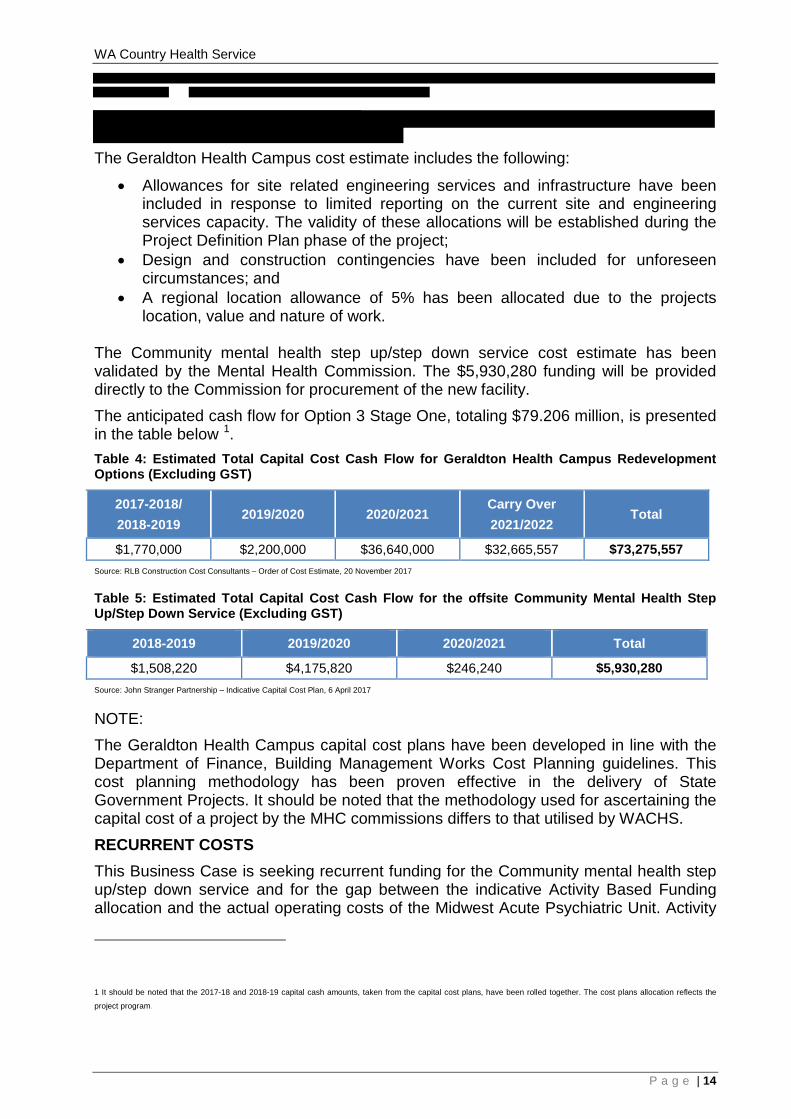
The Geraldton Health Campus cost estimate includes the following:
• Allowances for site related engineering services and infrastructure have been included in response to limited reporting on the current site and engineering services capacity. The validity of these allocations will be established during the Project Definition Plan phase of the project;
• Design and construction contingencies have been included for unforeseen circumstances; and
• A regional location allowance of 5% has been allocated due to the projects location, value and nature of work.
The Community mental health step up/step down service cost estimate has been validated by the Mental Health Commission. The $5,930,280 funding will be provided directly to the Commission for procurement of the new facility. The anticipated cash flow for Option 3 Stage One, totaling $79.206 million, is presented in the table below 1. Table 4: Estimated Total Capital Cost Cash Flow for Geraldton Health Campus Redevelopment Options (Excluding GST)
2017-2018/ 2018-2019
2019/2020 2020/2021 Carry Over 2021/2022
Total
$1,770,000 $2,200,000 $36,640,000 $32,665,557 $73,275,557 Source: RLB Construction Cost Consultants – Order of Cost Estimate, 20 November 2017
Table 5: Estimated Total Capital Cost Cash Flow for the offsite Community Mental Health Step Up/Step Down Service (Excluding GST)
2018-2019 2019/2020 2020/2021 Total
$1,508,220 $4,175,820 $246,240 $5,930,280 Source: John Stranger Partnership – Indicative Capital Cost Plan, 6 April 2017
NOTE: The Geraldton Health Campus capital cost plans have been developed in line with the Department of Finance, Building Management Works Cost Planning guidelines. This cost planning methodology has been proven effective in the delivery of State Government Projects. It should be noted that the methodology used for ascertaining the capital cost of a project by the MHC commissions differs to that utilised by WACHS. RECURRENT COSTS This Business Case is seeking recurrent funding for the Community mental health step up/step down service and for the gap between the indicative Activity Based Funding allocation and the actual operating costs of the Midwest Acute Psychiatric Unit. Activity
1 It should be noted that the 2017-18 and 2018-19 capital cash amounts, taken from the capital cost plans, have been rolled together. The cost plans allocation reflects the
project program.
P a g e | 14
WA Country Health Service
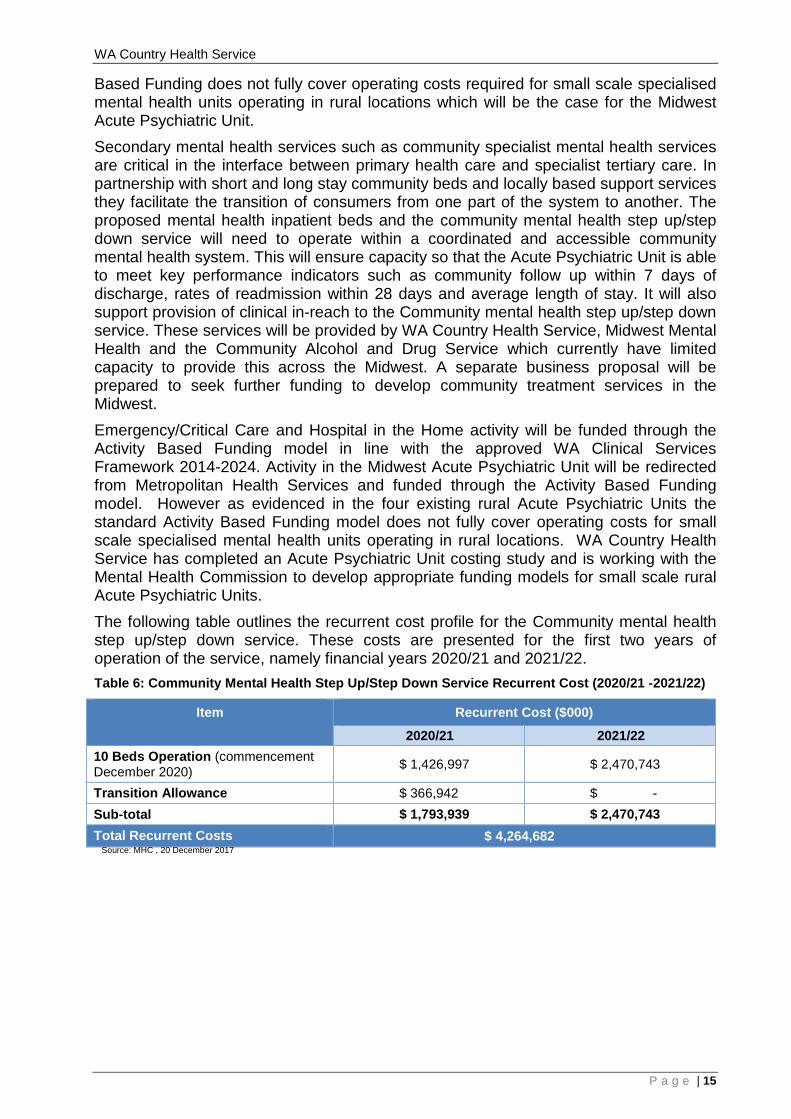
Based Funding does not fully cover operating costs required for small scale specialised mental health units operating in rural locations which will be the case for the Midwest Acute Psychiatric Unit. Secondary mental health services such as community specialist mental health services are critical in the interface between primary health care and specialist tertiary care. In partnership with short and long stay community beds and locally based support services they facilitate the transition of consumers from one part of the system to another. The proposed mental health inpatient beds and the community mental health step up/step down service will need to operate within a coordinated and accessible community mental health system. This will ensure capacity so that the Acute Psychiatric Unit is able to meet key performance indicators such as community follow up within 7 days of discharge, rates of readmission within 28 days and average length of stay. It will also support provision of clinical in-reach to the Community mental health step up/step down service. These services will be provided by WA Country Health Service, Midwest Mental Health and the Community Alcohol and Drug Service which currently have limited capacity to provide this across the Midwest. A separate business proposal will be prepared to seek further funding to develop community treatment services in the Midwest. Emergency/Critical Care and Hospital in the Home activity will be funded through the Activity Based Funding model in line with the approved WA Clinical Services Framework 2014-2024. Activity in the Midwest Acute Psychiatric Unit will be redirected from Metropolitan Health Services and funded through the Activity Based Funding model. However as evidenced in the four existing rural Acute Psychiatric Units the standard Activity Based Funding model does not fully cover operating costs for small scale specialised mental health units operating in rural locations. WA Country Health Service has completed an Acute Psychiatric Unit costing study and is working with the Mental Health Commission to develop appropriate funding models for small scale rural Acute Psychiatric Units. The following table outlines the recurrent cost profile for the Community mental health step up/step down service. These costs are presented for the first two years of operation of the service, namely financial years 2020/21 and 2021/22. Table 6: Community Mental Health Step Up/Step Down Service Recurrent Cost (2020/21 -2021/22)
Item Recurrent Cost ($000)
2020/21 2021/22 10 Beds Operation (commencement December 2020) $ 1,426,997 $ 2,470,743
Transition Allowance $ 366,942 $ - Sub-total $ 1,793,939 $ 2,470,743 Total Recurrent Costs $ 4,264,682 Source: MHC , 20 December 2017
P a g e | 15
WA Country Health Service
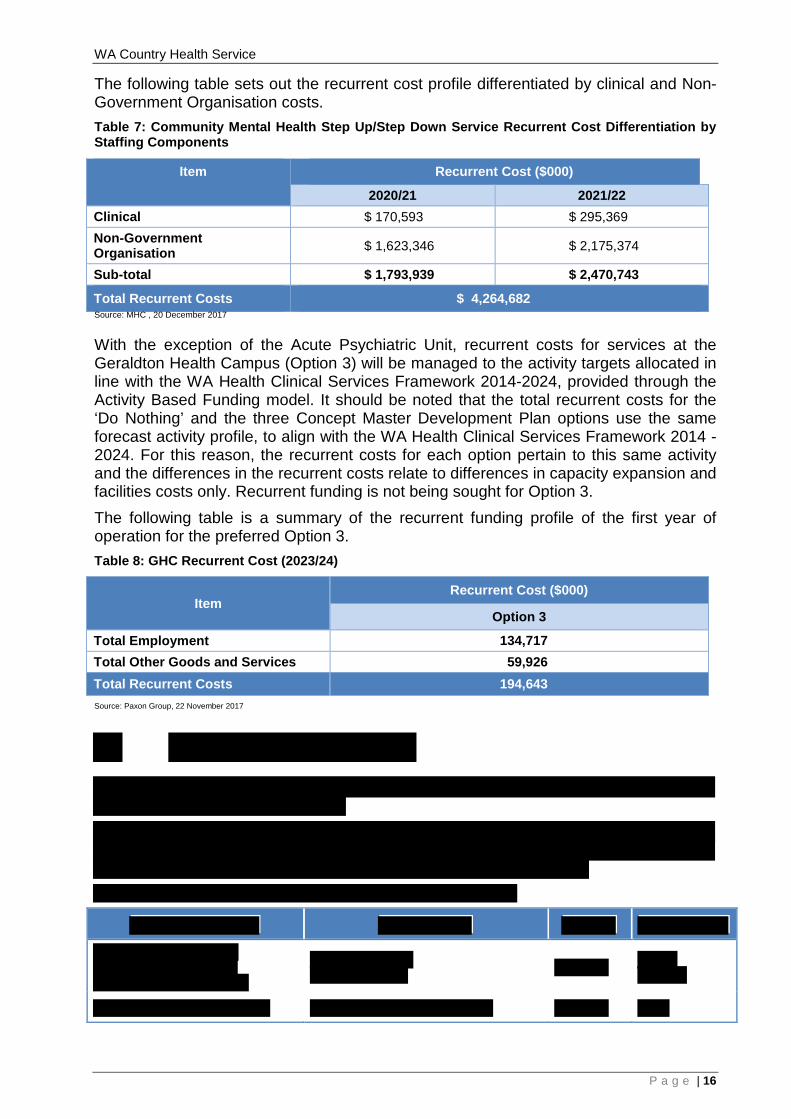
The following table sets out the recurrent cost profile differentiated by clinical and Non-Government Organisation costs. Table 7: Community Mental Health Step Up/Step Down Service Recurrent Cost Differentiation by Staffing Components
Item
Recurrent Cost ($000)
2020/21 2021/22 Clinical $ 170,593 $ 295,369 Non-Government Organisation $ 1,623,346 $ 2,175,374
Sub-total $ 1,793,939 $ 2,470,743
Total Recurrent Costs $ 4,264,682 Source: MHC , 20 December 2017
With the exception of the Acute Psychiatric Unit, recurrent costs for services at the Geraldton Health Campus (Option 3) will be managed to the activity targets allocated in line with the WA Health Clinical Services Framework 2014-2024, provided through the Activity Based Funding model. It should be noted that the total recurrent costs for the ‘Do Nothing’ and the three Concept Master Development Plan options use the same forecast activity profile, to align with the WA Health Clinical Services Framework 2014 - 2024. For this reason, the recurrent costs for each option pertain to this same activity and the differences in the recurrent costs relate to differences in capacity expansion and facilities costs only. Recurrent funding is not being sought for Option 3. The following table is a summary of the recurrent funding profile of the first year of operation for the preferred Option 3. Table 8: GHC Recurrent Cost (2023/24)
Item Recurrent Cost ($000)
Option 3
Total Employment 134,717 Total Other Goods and Services 59,926 Total Recurrent Costs 194,643 Source: Paxon Group, 22 November 2017
P a g e | 16
WA Country Health Service
1.6 Recommendation
In order to provide Stage One of the Geraldton Health Campus redevelopment and an integrated Midwest mental health service, $79.206 million of capital funding and $4.265 million recurrent investment for an offsite Community mental health step up/step down service is sought from the WA State Government. The $79.206 million amount includes the estimated construction cost of $43,850,657 million for Option 3 Stage One of the Geraldton Health Campus redevelopment and $2,560,000 million for development of the offsite Community mental health step up/step down service. This will provide a solution that will substantially meet the investment objectives of this Business Case.
P a g e | 17

WA Country Health Service
2 PROJECT SCOPE AND EVALUATION 2.1 Project Purpose
The purpose of this project is to respond to the increasing service demand in the Midwest region, in both the acute and subacute setting. The project seeks to address and remedy shortfalls in the provision of clinical services and future role delineation as outlined in the WA Health Clinical Services Framework (CSF) 2014-2024. The Geraldton Health Campus (GHC) delivers a combination of acute and subacute healthcare, with the proposed Community mental health step up/step down service (step up/step down) to provide subacute community based mental health care. The two facilities will be designed and developed simultaneously, however they will be constructed on two different sites. In early 2017 the West Australian Labor Party committed to undertake a major staged redevelopment of the GHC. The commitment included an upgrade to the Geraldton Hospital Emergency Service, an Acute Mental Health Facility, Mental Health Observation Area and subacute beds. The scope has been defined with stage one to include:
• an expanded Emergency/Critical Care aligning with projected service need to 2024
• Acute Psychiatric Unit • Mental Health Short Stay Unit • Essential engineering service upgrades including the replacement of the chillers;
and • Community mental health step up/step down located on another site.
In September 2017, WA Country Health Service (WACHS) confirmed the progression of this Business Case to secure funding for the GHC site and the offsite step up/step down. Recurrent funding is being sought for the operation of the step up/step down. This Business Case outlines four options in response to the staged redevelopment.
2.1.1 Geraldton Health Campus
GHC is the Regional Resource Centre for the Midwest region and provides healthcare services to residents of the City of Greater Geraldton, Gascoyne, Murchison and Midwest districts, and regional visitors. Because of the increase in demand on current services and the changes in contemporary health provision trends, the GHC no longer has the built capacity that enables service delivery to be able to respond to current and projected demand. Consequently, significant capital investment is required to upgrade GHC to be able to meet current demand, expand services, introduce new services and satisfy the health service obligations outlined in the WA Health CSF 2014-2024. Contributing factors to the increased demand on services include; an ageing population, increasing elective surgery, increasing need to isolate infectious patients, increasing need to provide mental health and drug and alcohol services and the need to be increasingly self-sufficient to provide care closer to home. The following are key reasons for the pressure on the existing built facility;
P a g e | 18
WA Country Health Service
• The population in the Midwest region has increased by 12% and in Geraldton district, the population has increased by 15% (Australian Bureau of Statistics Estimated Resident Population 2007 – 2015);
• The region has a high proportion of Aboriginal people (12%) compared to the state average of 3.2% who experience a high disease burden and this impacts the complexity and demand experienced at GHC;
• Between 2006/07 and 2014/15 Emergency presentations increased by 44%, same day stays increased by 74% and multi day stays increased by 40%;
• There have been significant increases in the number of Emergency services, as well as increasing levels of patient acuity presenting to the service. This has resulted in additional demand for inpatient services which in turn is placing pressure on the availability of beds and is leading to a bed block scenario with more patients waiting in the Emergency area for a bed to become available in the ward;
• Emergency presentations for patients with alcohol/drug and mental health disorders has increased 13.5% in the period 2012/13, (938 patients) to 2015/16 (1065 patients). This has placed considerable demand on the resources which are already at capacity. The Emergency presentations and hospital admission data does not include episodes of care for the major diagnostic category “alcohol/drug use or induced mental disorders” and anecdotally there is a high percentage of episodes coded as “injury poisoning toxic effects” that are related to alcohol/drug use that are also not captured in this data;
• The number of mental health-related hospital admissions from the various Midwest Emergency Departments has increased by 10% from 2011-12 to 2014-15
• The multi-day occupancy rate for GHC in 2015/16 was 93% increasing from 82% in 2011/12. The multi-day occupancy rates include the use of the Day Surgery Unit (DSU) ward for overnight stays. This has been a longstanding strategy to manage overflow and bed capacity issues however the environment is neither designed nor conducive to multi-day clinical care provision and has poor consumer satisfaction outcomes;
• GHC inpatient bed days for patients with alcohol/drug and mental disorders has increase by 7% and has grown from 860 bed days in 2013/14 to 923 bed days per year to date (May 2016);
• Increase in the Care Awaiting Placement (CAP) due to the ageing population and has increased from 2476 (2014-15) to 4301 (2015-16) bed days. This increase is due to longer waiting periods for people who are currently admitted to the inpatient ward to be transferred to appropriate residential care in the community; and
• Expanded or diversified Medical Specialist workforce enables higher level of care to be provided, however this is limited by bed capacity issues and suboptimal clinical areas e.g.: Emergency/Critical Care.
Currently the strategy to manage the bed capacity issue is to contract services to a private provider, St John of God Geraldton Hospital for a proportion of orthopaedic elective cases, all ophthalmology elective and emergency cases, palliative inpatient care and ad hoc bed purchasing: in 2012/13, 540 bed days were purchased (301 patients) increasing to 3551 bed days (782 patients) 2015/16 an increase in bed days of 557%. In addition to the clinical demand, the existing built infrastructure does not comply with relevant codes, safety related standards and the Australasian Health Facility Guidelines (AHFG). The original building fabric was not constructed to a standard that could
P a g e | 19
WA Country Health Service
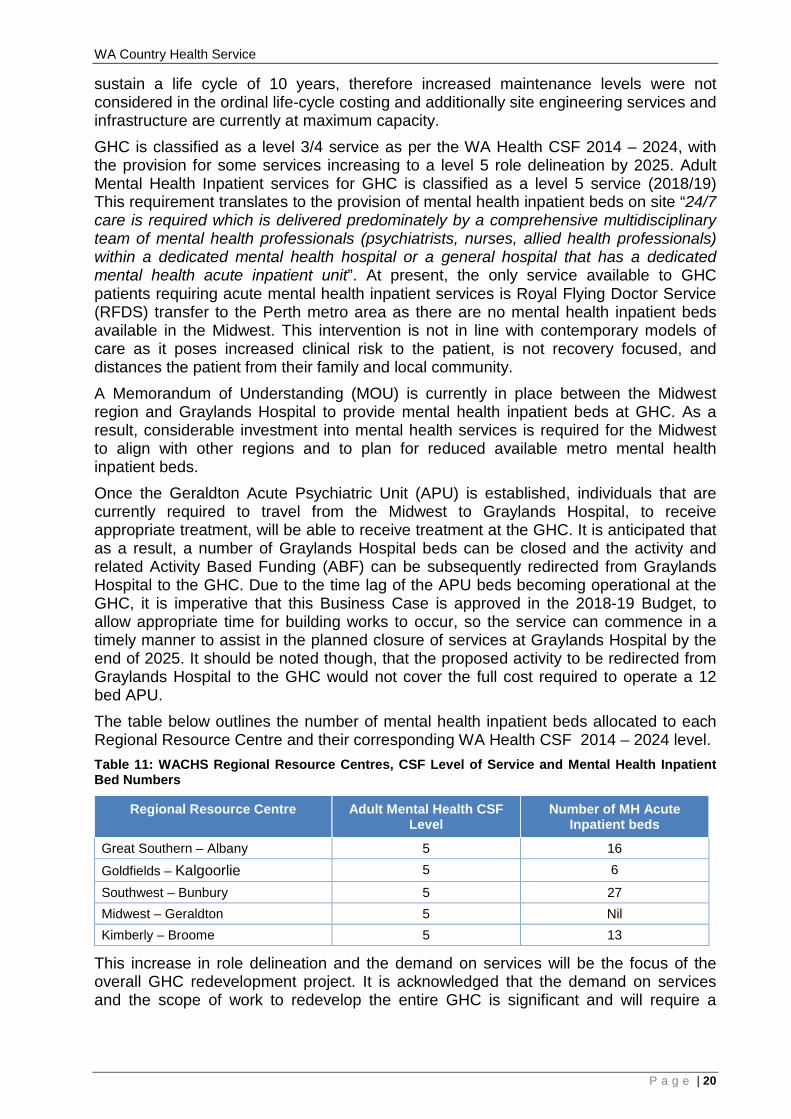
sustain a life cycle of 10 years, therefore increased maintenance levels were not considered in the ordinal life-cycle costing and additionally site engineering services and infrastructure are currently at maximum capacity. GHC is classified as a level 3/4 service as per the WA Health CSF 2014 – 2024, with the provision for some services increasing to a level 5 role delineation by 2025. Adult Mental Health Inpatient services for GHC is classified as a level 5 service (2018/19) This requirement translates to the provision of mental health inpatient beds on site “24/7 care is required which is delivered predominately by a comprehensive multidisciplinary team of mental health professionals (psychiatrists, nurses, allied health professionals) within a dedicated mental health hospital or a general hospital that has a dedicated mental health acute inpatient unit”. At present, the only service available to GHC patients requiring acute mental health inpatient services is Royal Flying Doctor Service (RFDS) transfer to the Perth metro area as there are no mental health inpatient beds available in the Midwest. This intervention is not in line with contemporary models of care as it poses increased clinical risk to the patient, is not recovery focused, and distances the patient from their family and local community. A Memorandum of Understanding (MOU) is currently in place between the Midwest region and Graylands Hospital to provide mental health inpatient beds at GHC. As a result, considerable investment into mental health services is required for the Midwest to align with other regions and to plan for reduced available metro mental health inpatient beds. Once the Geraldton Acute Psychiatric Unit (APU) is established, individuals that are currently required to travel from the Midwest to Graylands Hospital, to receive appropriate treatment, will be able to receive treatment at the GHC. It is anticipated that as a result, a number of Graylands Hospital beds can be closed and the activity and related Activity Based Funding (ABF) can be subsequently redirected from Graylands Hospital to the GHC. Due to the time lag of the APU beds becoming operational at the GHC, it is imperative that this Business Case is approved in the 2018-19 Budget, to allow appropriate time for building works to occur, so the service can commence in a timely manner to assist in the planned closure of services at Graylands Hospital by the end of 2025. It should be noted though, that the proposed activity to be redirected from Graylands Hospital to the GHC would not cover the full cost required to operate a 12 bed APU. The table below outlines the number of mental health inpatient beds allocated to each Regional Resource Centre and their corresponding WA Health CSF 2014 – 2024 level. Table 11: WACHS Regional Resource Centres, CSF Level of Service and Mental Health Inpatient Bed Numbers
Regional Resource Centre Adult Mental Health CSF Level
Number of MH Acute Inpatient beds
Great Southern – Albany 5 16
Goldfields – Kalgoorlie 5 6
Southwest – Bunbury 5 27 Midwest – Geraldton 5 Nil Kimberly – Broome 5 13
This increase in role delineation and the demand on services will be the focus of the overall GHC redevelopment project. It is acknowledged that the demand on services and the scope of work to redevelop the entire GHC is significant and will require a
P a g e | 20
WA Country Health Service
staged approach with significant capital investment. Stage One will focus on the following:
• an expanded Emergency/Critical Care area aligning with projected service need to 2024;
• Mental Health Short Stay Unit beds (MHSSU) x 4 (co-located with Emergency/ Critical Care);
• APU, mental health inpatient beds (4 secure and 8 open) Hospital in the Home (HITH) and Community Treatment Team (CTT); and
• Essential engineering service upgrades including the replacement of the chillers (to align with the capital expansion).
The overarching vision for the GHC is to provide safe and efficient health care to the residents of Geraldton and the Midwest region in line with contemporary models of care and as required from a Regional Resource Centre. The Stage One redevelopment will enable GHC to safely manage health demand for emergency/critical care and mental health services by providing:
• A combination of level 4 and 5 emergency/critical care and mental health services onsite as per the role delineation in the WA Health CSF 2014 – 2024;
• Expansion of departments included within the Stage One scope in response to updated role delineation in the WA Health CSF 2014 – 2024;
• Consumer centred health care provided in a contemporary facility that enhances consumer recovery, safety and health outcomes;
• Co-located Midwest Mental Health (MMH) and Community Alcohol and Drug Service (CADS);
• Delivery of socially and culturally appropriate care; • Improved access to services; • Information and Communication Technology (ICT) advancements for better care;
in particular Emergency Telehealth Services and Videoconferencing, Education and Communication; and
• Essential engineering service upgrades including the replacement of the chillers to ensure continuation and safe provision of healthcare services.
2.1.2 Integrated Midwest Mental Health Services
Currently there is no APU or authorised mental health inpatient beds, no step-up step-down and limited community treatment and support services for mental health and alcohol and drug problems in the Midwest region. The limitations of the current dedicated mental health and Alcohol Other Drugs (AOD) services in the Midwest region increases the level of risk to the individual, as treatment and management does not align with contemporary standards, required WA Health CSF 2014 – 2024 levels of service or best practice. This Business Case has been developed in accordance with the principles and aims detailed in the West Australian Mental Health Alcohol and Other Drug Services Plan 2015 – 2025 (The Plan), which outlines the optimal mix of mental health and AOD services required to meet the needs of Western Australians up to 2025. In particular, the development of this Business Case is driven by:
• Recovery-oriented practice, including supporting people to stay connected to their community, is central to the development of mental health services;
P a g e | 21
WA Country Health Service
• The development of all services to incorporate a holistic approach that acknowledges the impact of social determinants to health and wellbeing such as housing, education, and employment;
• Consumers, families, and carers will be supported to be fully involved in co-planning, co-designing, co-delivery and co-reviewing of policies and services;
• A primary focus on rebalancing services between hospital-based and community-based: moving services to the community where clinically appropriate;
• Services will expand in the regions and in locations where they are most required, and closer to where people live, wherever practical and feasible.
As outlined in the Plan, State-funded services are for individuals with severe mental health problems, and/or mild, moderate and severe alcohol and other drug problems. The Plan and the MHC also recognise the importance of an integrated and comprehensive service system from prevention through to acute care, to ensure the best outcomes for individuals and the community, and so individuals do not fall through the gaps. The proposed development of a fully integrated mental health and AOD model focuses on early intervention, community based care, acute inpatient care, and recovery focused case management which will enable consumer centred care based on individual requirements. Providing care closer to home facilitates the inclusion of families and carers in the development of the treatment and management plan. The Business Case is consistent with the aim of re-balancing the system and links to:
• Keeping people connected and close to home through community treatment services and community bed-based services; and
• Acute and specialised care of those who need it through the delivery of hospital based services.
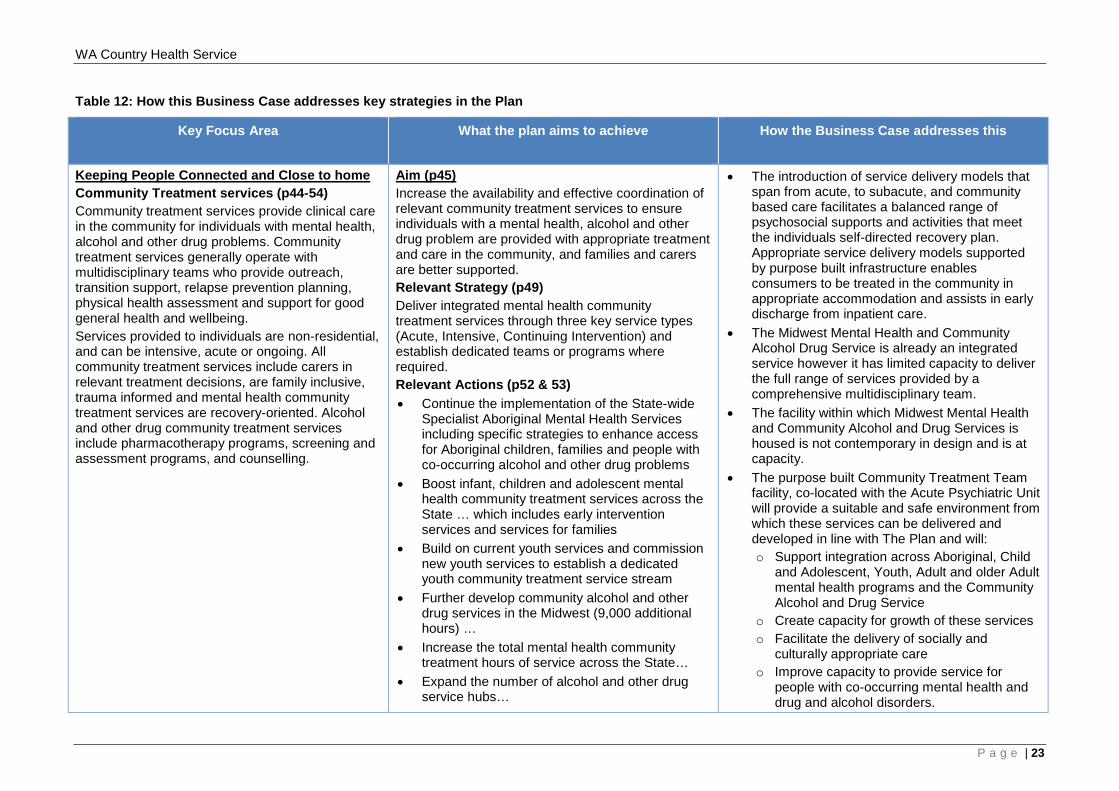
Table 12 demonstrates how this business case will deliver on the relevant strategies and actions in The Plan.
P a g e | 22
WA Country Health Service
Table 12: How this Business Case addresses key strategies in the Plan
Key Focus Area What the plan aims to achieve
How the Business Case addresses this
Keeping People Connected and Close to home Community Treatment services (p44-54) Community treatment services provide clinical care in the community for individuals with mental health, alcohol and other drug problems. Community treatment services generally operate with multidisciplinary teams who provide outreach, transition support, relapse prevention planning, physical health assessment and support for good general health and wellbeing. Services provided to individuals are non-residential, and can be intensive, acute or ongoing. All community treatment services include carers in relevant treatment decisions, are family inclusive, trauma informed and mental health community treatment services are recovery-oriented. Alcohol and other drug community treatment services include pharmacotherapy programs, screening and assessment programs, and counselling.
Aim (p45) Increase the availability and effective coordination of relevant community treatment services to ensure individuals with a mental health, alcohol and other drug problem are provided with appropriate treatment and care in the community, and families and carers are better supported. Relevant Strategy (p49) Deliver integrated mental health community treatment services through three key service types (Acute, Intensive, Continuing Intervention) and establish dedicated teams or programs where required. Relevant Actions (p52 & 53) • Continue the implementation of the State-wide
Specialist Aboriginal Mental Health Services including specific strategies to enhance access for Aboriginal children, families and people with co-occurring alcohol and other drug problems
• Boost infant, children and adolescent mental health community treatment services across the State … which includes early intervention services and services for families
• Build on current youth services and commission new youth services to establish a dedicated youth community treatment service stream
• Further develop community alcohol and other drug services in the Midwest (9,000 additional hours) …
• Increase the total mental health community treatment hours of service across the State…
• Expand the number of alcohol and other drug service hubs…
• The introduction of service delivery models that span from acute, to subacute, and community based care facilitates a balanced range of psychosocial supports and activities that meet the individuals self-directed recovery plan. Appropriate service delivery models supported by purpose built infrastructure enables consumers to be treated in the community in appropriate accommodation and assists in early discharge from inpatient care.
• The Midwest Mental Health and Community Alcohol Drug Service is already an integrated service however it has limited capacity to deliver the full range of services provided by a comprehensive multidisciplinary team.
• The facility within which Midwest Mental Health and Community Alcohol and Drug Services is housed is not contemporary in design and is at capacity.
• The purpose built Community Treatment Team facility, co-located with the Acute Psychiatric Unit will provide a suitable and safe environment from which these services can be delivered and developed in line with The Plan and will: o Support integration across Aboriginal, Child
and Adolescent, Youth, Adult and older Adult mental health programs and the Community Alcohol and Drug Service
o Create capacity for growth of these services o Facilitate the delivery of socially and
culturally appropriate care o Improve capacity to provide service for
people with co-occurring mental health and drug and alcohol disorders.
P a g e | 23
WA Country Health Service
Key Focus Area What the plan aims to achieve
How the Business Case addresses this
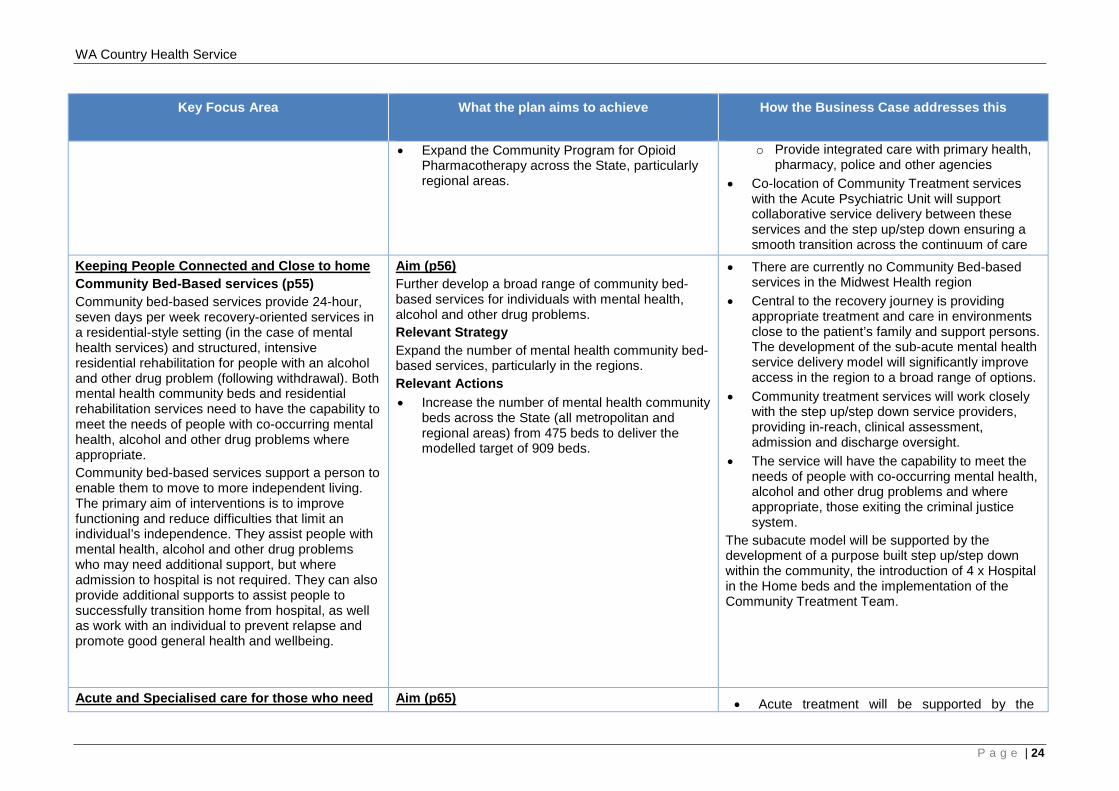
• Expand the Community Program for Opioid Pharmacotherapy across the State, particularly regional areas.
o Provide integrated care with primary health, pharmacy, police and other agencies
• Co-location of Community Treatment services with the Acute Psychiatric Unit will support collaborative service delivery between these services and the step up/step down ensuring a smooth transition across the continuum of care
Keeping People Connected and Close to home Community Bed-Based services (p55) Community bed-based services provide 24-hour, seven days per week recovery-oriented services in a residential-style setting (in the case of mental health services) and structured, intensive residential rehabilitation for people with an alcohol and other drug problem (following withdrawal). Both mental health community beds and residential rehabilitation services need to have the capability to meet the needs of people with co-occurring mental health, alcohol and other drug problems where appropriate. Community bed-based services support a person to enable them to move to more independent living. The primary aim of interventions is to improve functioning and reduce difficulties that limit an individual’s independence. They assist people with mental health, alcohol and other drug problems who may need additional support, but where admission to hospital is not required. They can also provide additional supports to assist people to successfully transition home from hospital, as well as work with an individual to prevent relapse and promote good general health and wellbeing.
Aim (p56) Further develop a broad range of community bed-based services for individuals with mental health, alcohol and other drug problems. Relevant Strategy Expand the number of mental health community bed-based services, particularly in the regions. Relevant Actions • Increase the number of mental health community
beds across the State (all metropolitan and regional areas) from 475 beds to deliver the modelled target of 909 beds.
• There are currently no Community Bed-based services in the Midwest Health region
• Central to the recovery journey is providing appropriate treatment and care in environments close to the patient’s family and support persons. The development of the sub-acute mental health service delivery model will significantly improve access in the region to a broad range of options.
• Community treatment services will work closely with the step up/step down service providers, providing in-reach, clinical assessment, admission and discharge oversight.
• The service will have the capability to meet the needs of people with co-occurring mental health, alcohol and other drug problems and where appropriate, those exiting the criminal justice system.
The subacute model will be supported by the development of a purpose built step up/step down within the community, the introduction of 4 x Hospital in the Home beds and the implementation of the Community Treatment Team.
Acute and Specialised care for those who need Aim (p65) • Acute treatment will be supported by the
P a g e | 24
WA Country Health Service
Key Focus Area What the plan aims to achieve
How the Business Case addresses this
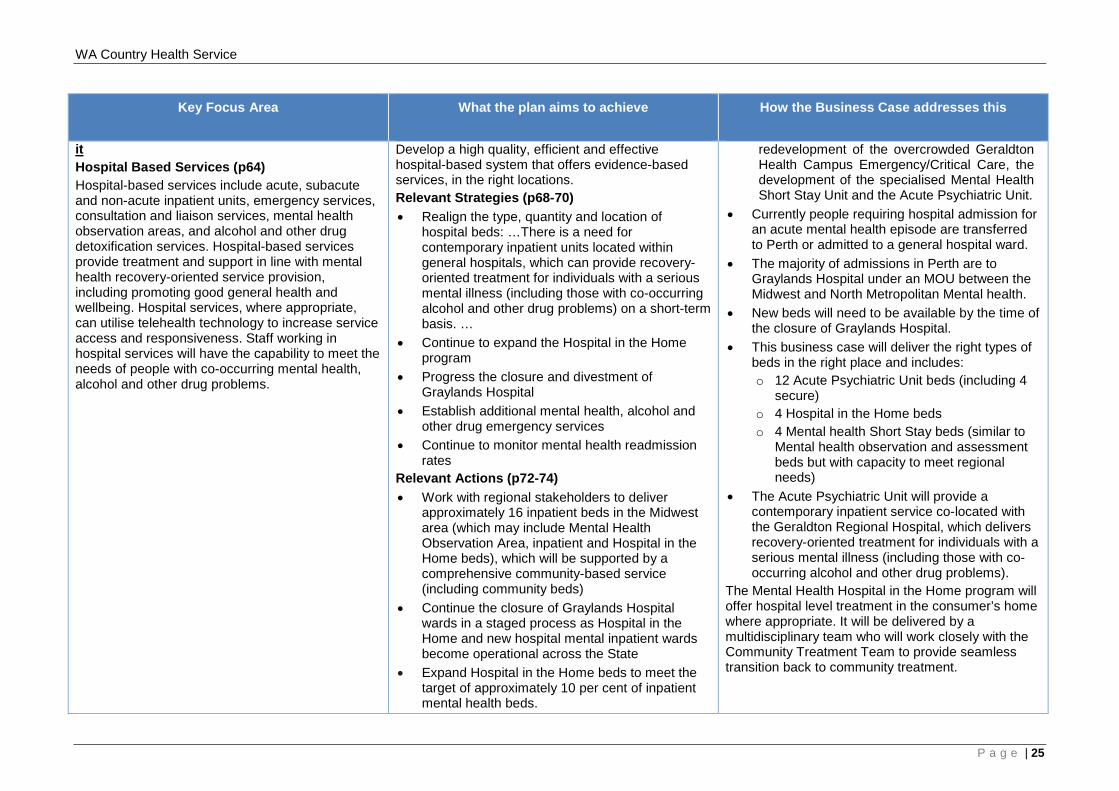
it Hospital Based Services (p64) Hospital-based services include acute, subacute and non-acute inpatient units, emergency services, consultation and liaison services, mental health observation areas, and alcohol and other drug detoxification services. Hospital-based services provide treatment and support in line with mental health recovery-oriented service provision, including promoting good general health and wellbeing. Hospital services, where appropriate, can utilise telehealth technology to increase service access and responsiveness. Staff working in hospital services will have the capability to meet the needs of people with co-occurring mental health, alcohol and other drug problems.
Develop a high quality, efficient and effective hospital-based system that offers evidence-based services, in the right locations. Relevant Strategies (p68-70) • Realign the type, quantity and location of
hospital beds: …There is a need for contemporary inpatient units located within general hospitals, which can provide recovery-oriented treatment for individuals with a serious mental illness (including those with co-occurring alcohol and other drug problems) on a short-term basis. …
• Continue to expand the Hospital in the Home program
• Progress the closure and divestment of Graylands Hospital
• Establish additional mental health, alcohol and other drug emergency services
• Continue to monitor mental health readmission rates
Relevant Actions (p72-74) • Work with regional stakeholders to deliver
approximately 16 inpatient beds in the Midwest area (which may include Mental Health Observation Area, inpatient and Hospital in the Home beds), which will be supported by a comprehensive community-based service (including community beds)
• Continue the closure of Graylands Hospital wards in a staged process as Hospital in the Home and new hospital mental inpatient wards become operational across the State
• Expand Hospital in the Home beds to meet the target of approximately 10 per cent of inpatient mental health beds.
redevelopment of the overcrowded Geraldton Health Campus Emergency/Critical Care, the development of the specialised Mental Health Short Stay Unit and the Acute Psychiatric Unit.
• Currently people requiring hospital admission for an acute mental health episode are transferred to Perth or admitted to a general hospital ward.
• The majority of admissions in Perth are to Graylands Hospital under an MOU between the Midwest and North Metropolitan Mental health.
• New beds will need to be available by the time of the closure of Graylands Hospital.
• This business case will deliver the right types of beds in the right place and includes: o 12 Acute Psychiatric Unit beds (including 4
secure) o 4 Hospital in the Home beds o 4 Mental health Short Stay beds (similar to
Mental health observation and assessment beds but with capacity to meet regional needs)
• The Acute Psychiatric Unit will provide a contemporary inpatient service co-located with the Geraldton Regional Hospital, which delivers recovery-oriented treatment for individuals with a serious mental illness (including those with co-occurring alcohol and other drug problems).
The Mental Health Hospital in the Home program will offer hospital level treatment in the consumer’s home where appropriate. It will be delivered by a multidisciplinary team who will work closely with the Community Treatment Team to provide seamless transition back to community treatment.
P a g e | 25
WA Country Health Service
In addition to the guiding principles detailed in the Plan, contributing factors to the increased demand on existing services are detailed as follows:
• Mental health consumers in emergency care often experience delays in obtaining transfers to a metropolitan facility and will at times, require sedation until transport and bed availability is confirmed. The practice of sedating agitated consumers for long periods is not consistent with best practice. Heavily sedated mental health consumers who require transport via the RFDS may be intubated and ventilated. This has the potential to physically compromise a consumer’s recovery;
• Consumers with co-existing mental health and AOD issues require observation and management in an appropriate short-stay environment, which is currently unavailable;
• High risk consumers or consumers experiencing high levels of distress with mental health conditions need one-on-one nursing and this currently occurs in an environment that is not designed for this purpose, either on the inpatient ward or within the Emergency area;
• Mental health consumers are given priority for single bedrooms in the inpatient wards; however, this impacts negatively on the operations of these wards. For example, consumers who are agitated can disturb others and require greater management. One-on-one nursing for mental health consumers significantly affects overall hospital nursing needs and staffing availability for general ward;
• The public, other patients and staff safety can be placed at risk from individuals with behavioural issues;
• In the absence of adequate community treatment services and step up step down services, mental health consumers are being managed in an acute care setting adding to acute activity, acute-care costs to the health care system and increasing the risk of bed block;
• The Midwest region does not have any purpose designed facilities to care for mental health consumers. Purpose built mental health facilities aid the treatment and recovery of the consumer by providing a “home like” environment with focus on promoting general consumer wellbeing and recovery;
• When consumers are transferred to metropolitan facilities, the quality of care and cultural safety is compromised because mental health illnesses are exacerbated by the lack of ready access to families, networks and carers;
• Community mental health workers have limited capacity to provide expert input to support generalist trained staff due to resource restrictions and workload demands/priorities; and
• Limited community treatment services available, making it difficult for individuals to lead meaningful and more contributing lives in the community.
2.2 WA State Government Funding Amount
Capital funding investment of $79,205,837 million is sought from the WA Government (Option 3). This amount is comprised of;
• $73,275,557 million, redevelopment of Geraldton Health Campus Stage One (including the Mental Health scope)
• $5,930,280 million, development of the community mental health step up/step down service.
A recurrent investment of $4.265 million is also sought for a community mental health step up/step down service
P a g e | 26
WA Country Health Service
2.3 Project Description
2.3.1 Geraldton Health Campus
The objective of the GHC Redevelopment Project will respond to the requirements of a Regional Resource Centre, the changes in role delineation as stated in the WA Health CSF 2014 – 2024 and The Plan. To do this, three stages of capital investment will be required. Stage One objectives include:
• Expanded Emergency/Critical Care in line with projected service need up to 2024;
• 4 MHSSU beds co-located with Emergency/Critical Care; • 12 APU beds in line with projected service need up to 2024, (4 are secure), HITH
(4 beds) and CTT; and • Essential engineering service upgrades including the replacement of the chillers.
The GHC redevelopment will take into consideration proposed future expansion, future planning for the redevelopment of services outside of the current scope, proposed and future co-location of services, access to the facility, relationships with existing and proposed buildings on the site, and any potential future co-location plans with a private provider onsite through the development of an approved GHC Concept Master Development Plan (CMDP). The submission of this Business Case is driven by the requirements outlined within the WA Health CSF 2014 – 2024; within the WACHS Geraldton Health Campus Services Plan 2010-2020; within The Plan and in line with contemporary models of care. In support of these documents a summary of all assumptions that underpin the modelling to arrive at key clinical bed, treatment and consultation spaces is documented in the Geraldton Health Campus Assumptions Paper 2016. The submission and subsequent approval of this Business Case will enable WACHS Midwest to deliver safe healthcare within a modern facility, improve patient outcomes, improve staff amenity and address social, economic and geographical issues. Importantly the role of GHC as the Regional Resource Centre for the Midwest region means that there is a region wide benefit by being able to deliver care closer to home.
2.3.2 Community Mental Health Step Up/Step Down Service
The Plan aims to achieve a more balanced mental health system through investment in community based treatment and support services. More community based services are a priority for the Midwest region as the demand for step up/step down beds is increasing. Without step up/step down in the community, more pressure is placed on acute services at GHC to fill the present need. The lack of dedicated mental health services in the Midwest region increases the level of risk to the individual, as treatment and management does not align with contemporary standards, required CSF levels of service or best practice. The WA Health CSF 2014 – 2024 level of service for Child and Adolescent, Adult and Older Adult Community Mental Health the Geraldton region is Level F. This requirement translates to the provision of community mental health services “for people who have the highest risk / complexity; extended hours are provided; Highly specialised multidisciplinary team of mental health clinicians (medical practitioners, psychiatrists,
P a g e | 27
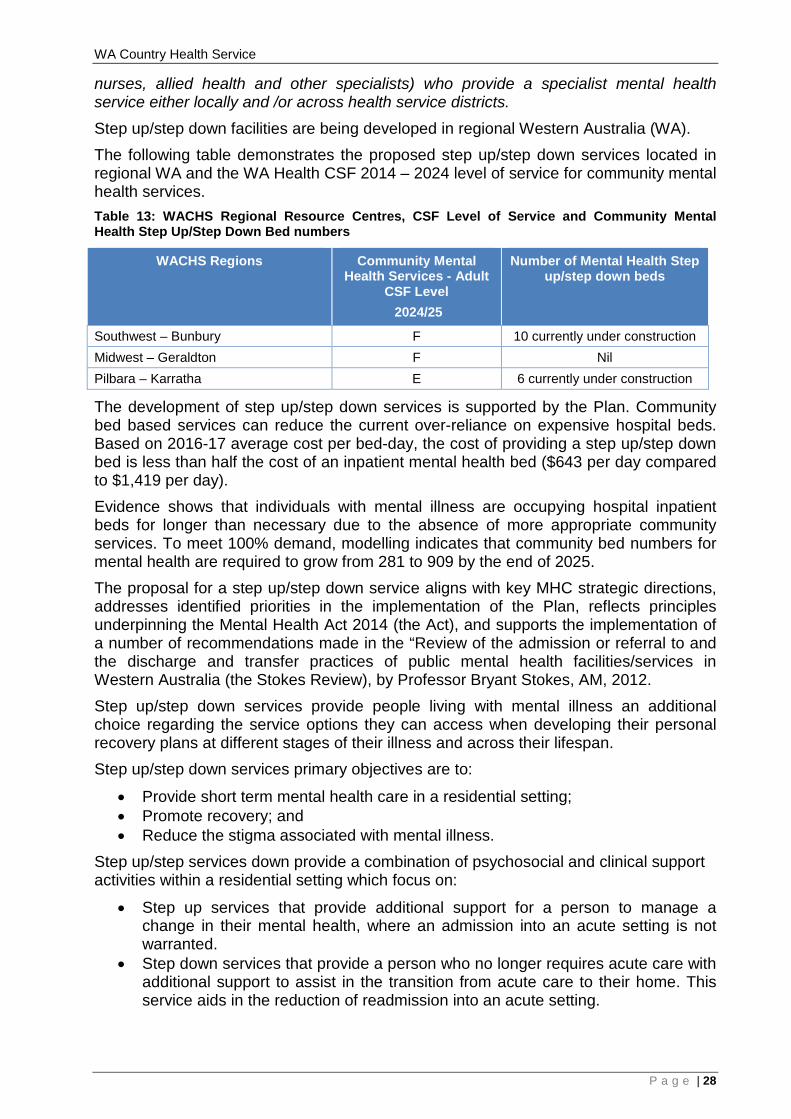
WA Country Health Service
nurses, allied health and other specialists) who provide a specialist mental health service either locally and /or across health service districts.
Step up/step down facilities are being developed in regional Western Australia (WA). The following table demonstrates the proposed step up/step down services located in regional WA and the WA Health CSF 2014 – 2024 level of service for community mental health services. Table 13: WACHS Regional Resource Centres, CSF Level of Service and Community Mental Health Step Up/Step Down Bed numbers
WACHS Regions Community Mental Health Services - Adult
CSF Level 2024/25
Number of Mental Health Step up/step down beds
Southwest – Bunbury F 10 currently under construction Midwest – Geraldton F Nil Pilbara – Karratha E 6 currently under construction
The development of step up/step down services is supported by the Plan. Community bed based services can reduce the current over-reliance on expensive hospital beds. Based on 2016-17 average cost per bed-day, the cost of providing a step up/step down bed is less than half the cost of an inpatient mental health bed ($643 per day compared to $1,419 per day). Evidence shows that individuals with mental illness are occupying hospital inpatient beds for longer than necessary due to the absence of more appropriate community services. To meet 100% demand, modelling indicates that community bed numbers for mental health are required to grow from 281 to 909 by the end of 2025. The proposal for a step up/step down service aligns with key MHC strategic directions, addresses identified priorities in the implementation of the Plan, reflects principles underpinning the Mental Health Act 2014 (the Act), and supports the implementation of a number of recommendations made in the “Review of the admission or referral to and the discharge and transfer practices of public mental health facilities/services in Western Australia (the Stokes Review), by Professor Bryant Stokes, AM, 2012. Step up/step down services provide people living with mental illness an additional choice regarding the service options they can access when developing their personal recovery plans at different stages of their illness and across their lifespan. Step up/step down services primary objectives are to:
• Provide short term mental health care in a residential setting; • Promote recovery; and • Reduce the stigma associated with mental illness.
Step up/step services down provide a combination of psychosocial and clinical support activities within a residential setting which focus on:
• Step up services that provide additional support for a person to manage a change in their mental health, where an admission into an acute setting is not warranted.
• Step down services that provide a person who no longer requires acute care with additional support to assist in the transition from acute care to their home. This service aids in the reduction of readmission into an acute setting.
P a g e | 28
WA Country Health Service
The step up/step down services are centred around a framework of recovery, focusing on rehabilitation activities delivered by a comprehensive suite of psychosocial programs and clinical interventions, tailored to meet the individual requirements. The framework aims to improve the individual’s symptom control, encourages personal abilities and assists in the return to their daily living environment. The objective of the redevelopment will be to construct a 10 bed step up/step down (off site from GHC). The facility will consist of:
• 10 x single occupancy units; • Main entry and staff zone; • Day area zone, including activity rooms, communal kitchen and dining, shared
recovery spaces; • Communal courtyard with recovery focused areas; and • Back of house facility support zone.
The submission and subsequent approval of this Business Case in regard to community mental health will:
• Improve recovery outcomes for consumers with a mental illness; • Provide care and support closer to home; • Reduce avoidable admissions and re-admissions to hospital for consumers living
with a mental illness; • Provide consumer centred services in a contemporary facility that enhances
consumer recovery, safety and health outcomes; • Facilitate appropriate and earlier discharge from inpatient care; • Offer a balanced range of psychosocial support and activities that meet the
individual’s self-directed recovery plan; • Assist consumers in developing prevention and crisis resolution strategies; • Contribute to reducing the burden of care experienced by carers in supporting
consumers who are unwell but do not require inpatient care; • Reduce over reliance on crisis and emergency services for the provision of
services more appropriately delivered in the community; • Ensure that the day to day management of services provides a safe and secure
environment for service users, staff, visitors and the community; • Facilitate the delivery of socially and culturally appropriate care; • Improve access to services; • Promote consumer self-sufficiency and care closer to home; and • Promote the expansion of recovery focused mental health community support
services. *Developed in collaboration with the MHC
P a g e | 29
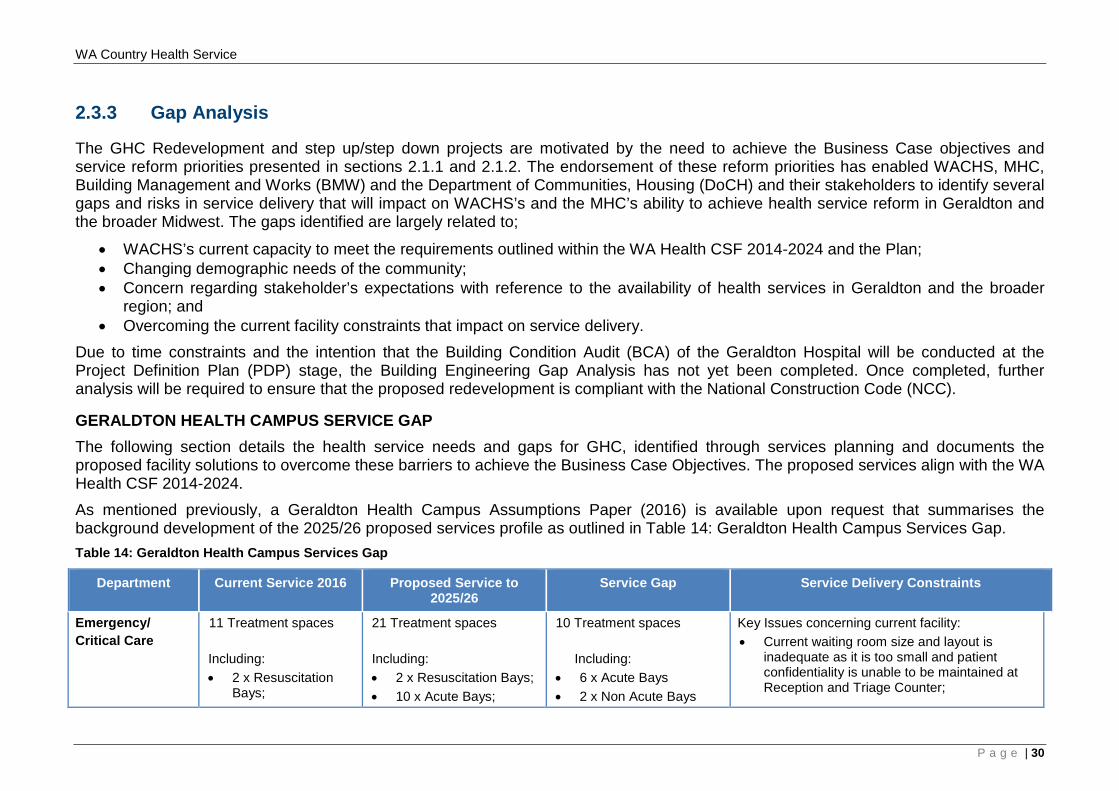
WA Country Health Service
2.3.3 Gap Analysis
The GHC Redevelopment and step up/step down projects are motivated by the need to achieve the Business Case objectives and service reform priorities presented in sections 2.1.1 and 2.1.2. The endorsement of these reform priorities has enabled WACHS, MHC, Building Management and Works (BMW) and the Department of Communities, Housing (DoCH) and their stakeholders to identify several gaps and risks in service delivery that will impact on WACHS’s and the MHC’s ability to achieve health service reform in Geraldton and the broader Midwest. The gaps identified are largely related to;
• WACHS’s current capacity to meet the requirements outlined within the WA Health CSF 2014-2024 and the Plan; • Changing demographic needs of the community; • Concern regarding stakeholder’s expectations with reference to the availability of health services in Geraldton and the broader
region; and • Overcoming the current facility constraints that impact on service delivery.
Due to time constraints and the intention that the Building Condition Audit (BCA) of the Geraldton Hospital will be conducted at the Project Definition Plan (PDP) stage, the Building Engineering Gap Analysis has not yet been completed. Once completed, further analysis will be required to ensure that the proposed redevelopment is compliant with the National Construction Code (NCC).
GERALDTON HEALTH CAMPUS SERVICE GAP The following section details the health service needs and gaps for GHC, identified through services planning and documents the proposed facility solutions to overcome these barriers to achieve the Business Case Objectives. The proposed services align with the WA Health CSF 2014-2024. As mentioned previously, a Geraldton Health Campus Assumptions Paper (2016) is available upon request that summarises the background development of the 2025/26 proposed services profile as outlined in Table 14: Geraldton Health Campus Services Gap. Table 14: Geraldton Health Campus Services Gap
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
Emergency/ Critical Care
11 Treatment spaces Including: • 2 x Resuscitation
Bays;
21 Treatment spaces
Including: • 2 x Resuscitation Bays; • 10 x Acute Bays;
10 Treatment spaces Including:
• 6 x Acute Bays • 2 x Non Acute Bays
Key Issues concerning current facility: • Current waiting room size and layout is
inadequate as it is too small and patient confidentiality is unable to be maintained at Reception and Triage Counter;
P a g e | 30
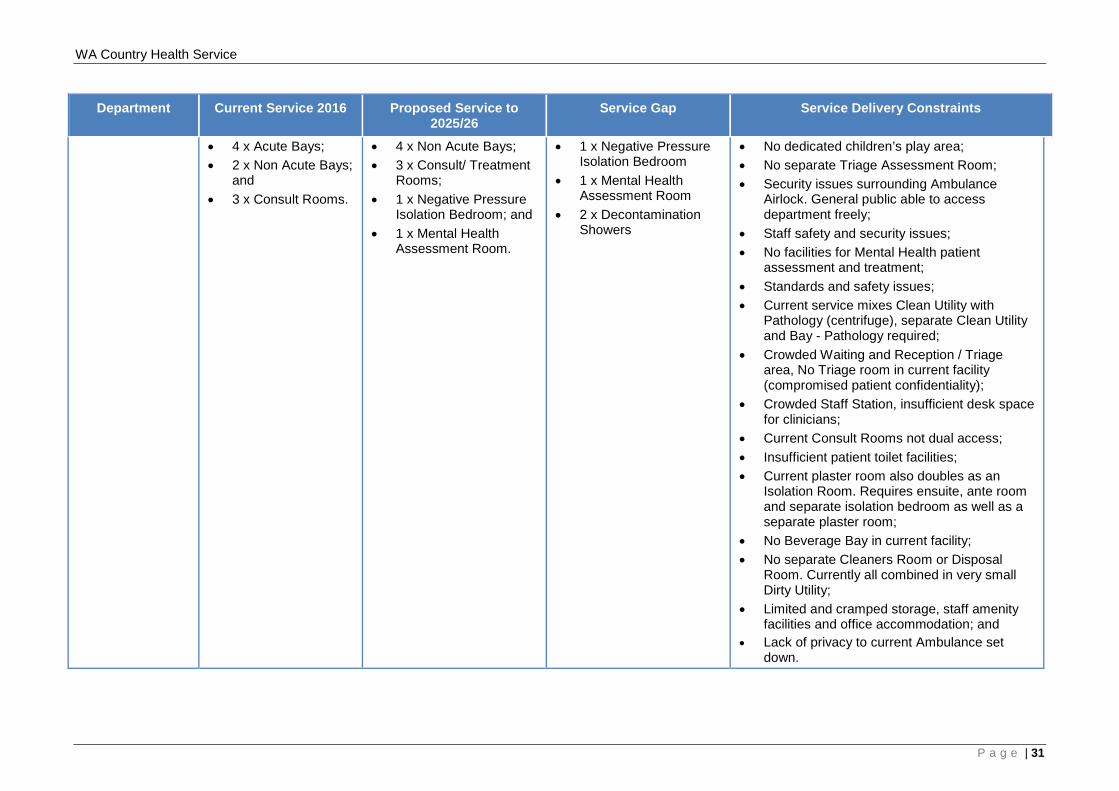
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
• 4 x Acute Bays; • 2 x Non Acute Bays;
and • 3 x Consult Rooms.
• 4 x Non Acute Bays; • 3 x Consult/ Treatment
Rooms; • 1 x Negative Pressure
Isolation Bedroom; and • 1 x Mental Health
Assessment Room.
• 1 x Negative Pressure Isolation Bedroom
• 1 x Mental Health Assessment Room
• 2 x Decontamination Showers
• No dedicated children’s play area; • No separate Triage Assessment Room; • Security issues surrounding Ambulance
Airlock. General public able to access department freely;
• Staff safety and security issues; • No facilities for Mental Health patient
assessment and treatment; • Standards and safety issues; • Current service mixes Clean Utility with
Pathology (centrifuge), separate Clean Utility and Bay - Pathology required;
• Crowded Waiting and Reception / Triage area, No Triage room in current facility (compromised patient confidentiality);
• Crowded Staff Station, insufficient desk space for clinicians;
• Current Consult Rooms not dual access; • Insufficient patient toilet facilities; • Current plaster room also doubles as an
Isolation Room. Requires ensuite, ante room and separate isolation bedroom as well as a separate plaster room;
• No Beverage Bay in current facility; • No separate Cleaners Room or Disposal
Room. Currently all combined in very small Dirty Utility;
• Limited and cramped storage, staff amenity facilities and office accommodation; and
• Lack of privacy to current Ambulance set down.
P a g e | 31
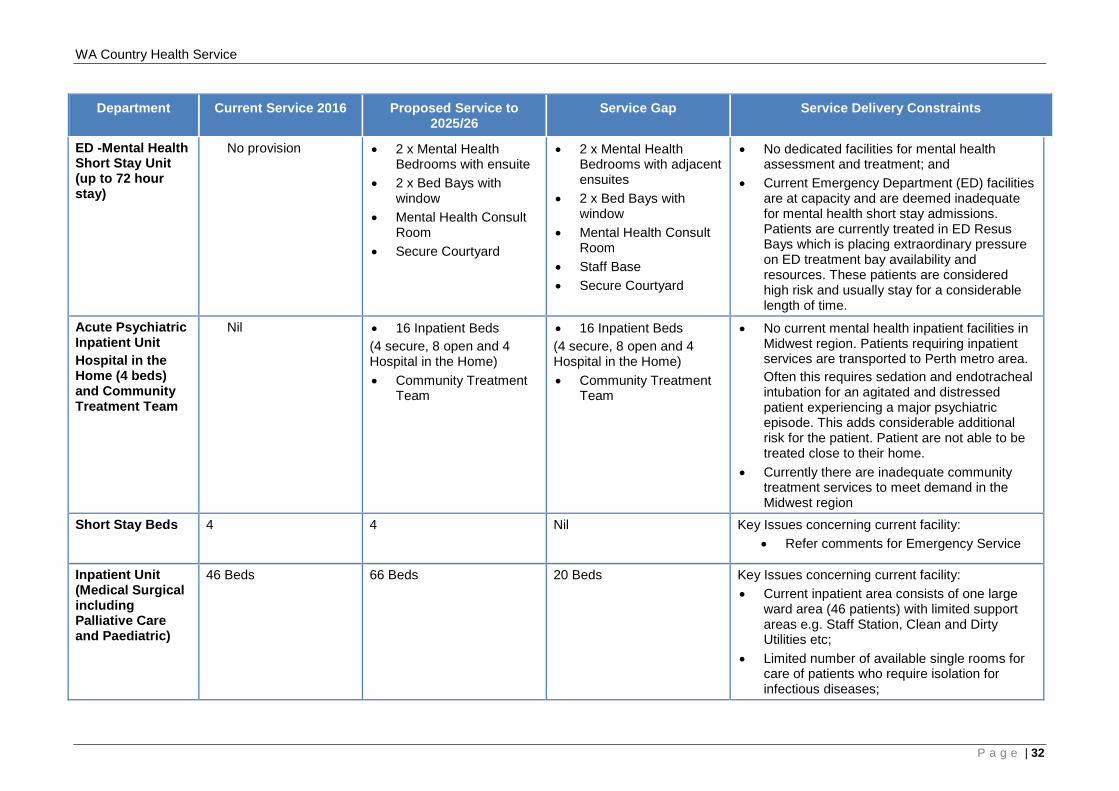
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
ED -Mental Health Short Stay Unit (up to 72 hour stay)
No provision • 2 x Mental Health Bedrooms with ensuite
• 2 x Bed Bays with window
• Mental Health Consult Room
• Secure Courtyard
• 2 x Mental Health Bedrooms with adjacent ensuites
• 2 x Bed Bays with window
• Mental Health Consult Room
• Staff Base • Secure Courtyard
• No dedicated facilities for mental health assessment and treatment; and
• Current Emergency Department (ED) facilities are at capacity and are deemed inadequate for mental health short stay admissions. Patients are currently treated in ED Resus Bays which is placing extraordinary pressure on ED treatment bay availability and resources. These patients are considered high risk and usually stay for a considerable length of time.
Acute Psychiatric Inpatient Unit Hospital in the Home (4 beds) and Community Treatment Team
Nil • 16 Inpatient Beds (4 secure, 8 open and 4 Hospital in the Home) • Community Treatment
Team
• 16 Inpatient Beds (4 secure, 8 open and 4 Hospital in the Home) • Community Treatment
Team
• No current mental health inpatient facilities in Midwest region. Patients requiring inpatient services are transported to Perth metro area. Often this requires sedation and endotracheal intubation for an agitated and distressed patient experiencing a major psychiatric episode. This adds considerable additional risk for the patient. Patient are not able to be treated close to their home.
• Currently there are inadequate community treatment services to meet demand in the Midwest region
Short Stay Beds 4 4 Nil Key Issues concerning current facility: • Refer comments for Emergency Service
Inpatient Unit (Medical Surgical including Palliative Care and Paediatric)
46 Beds
66 Beds 20 Beds
Key Issues concerning current facility: • Current inpatient area consists of one large
ward area (46 patients) with limited support areas e.g. Staff Station, Clean and Dirty Utilities etc;
• Limited number of available single rooms for care of patients who require isolation for infectious diseases;
P a g e | 32
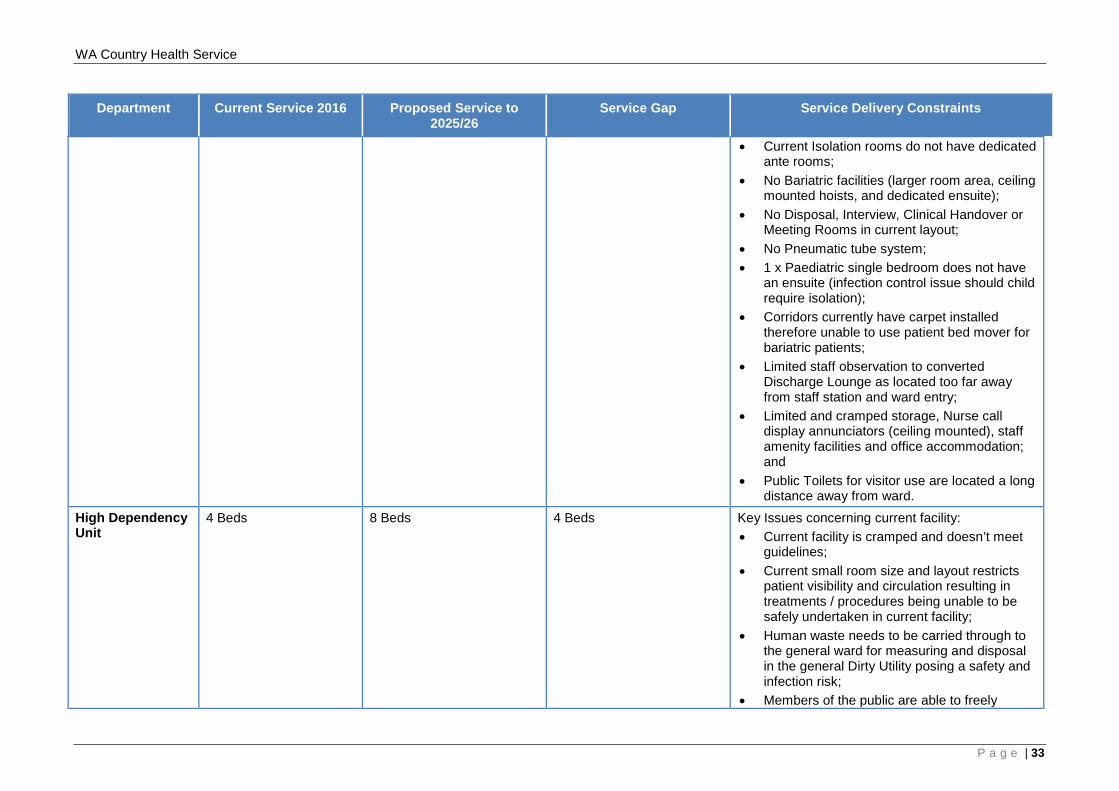
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
• Current Isolation rooms do not have dedicated ante rooms;
• No Bariatric facilities (larger room area, ceiling mounted hoists, and dedicated ensuite);
• No Disposal, Interview, Clinical Handover or Meeting Rooms in current layout;
• No Pneumatic tube system; • 1 x Paediatric single bedroom does not have
an ensuite (infection control issue should child require isolation);
• Corridors currently have carpet installed therefore unable to use patient bed mover for bariatric patients;
• Limited staff observation to converted Discharge Lounge as located too far away from staff station and ward entry;
• Limited and cramped storage, Nurse call display annunciators (ceiling mounted), staff amenity facilities and office accommodation; and
• Public Toilets for visitor use are located a long distance away from ward.
High Dependency Unit
4 Beds 8 Beds 4 Beds
Key Issues concerning current facility: • Current facility is cramped and doesn’t meet
guidelines; • Current small room size and layout restricts
patient visibility and circulation resulting in treatments / procedures being unable to be safely undertaken in current facility;
• Human waste needs to be carried through to the general ward for measuring and disposal in the general Dirty Utility posing a safety and infection risk;
• Members of the public are able to freely
P a g e | 33
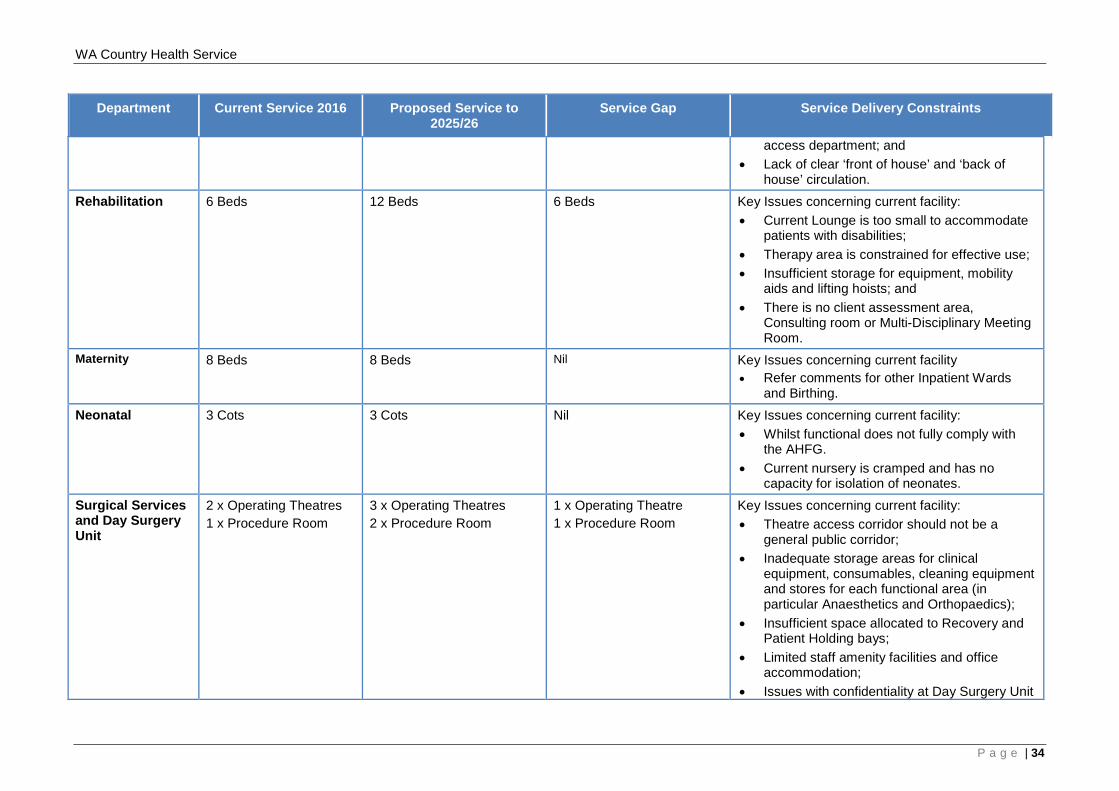
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
access department; and • Lack of clear ‘front of house’ and ‘back of
house’ circulation. Rehabilitation 6 Beds 12 Beds 6 Beds
Key Issues concerning current facility: • Current Lounge is too small to accommodate
patients with disabilities; • Therapy area is constrained for effective use; • Insufficient storage for equipment, mobility
aids and lifting hoists; and • There is no client assessment area,
Consulting room or Multi-Disciplinary Meeting Room.
Maternity 8 Beds 8 Beds Nil Key Issues concerning current facility • Refer comments for other Inpatient Wards
and Birthing. Neonatal 3 Cots 3 Cots Nil Key Issues concerning current facility:
• Whilst functional does not fully comply with the AHFG.
• Current nursery is cramped and has no capacity for isolation of neonates.
Surgical Services and Day Surgery Unit
2 x Operating Theatres 1 x Procedure Room
3 x Operating Theatres 2 x Procedure Room
1 x Operating Theatre 1 x Procedure Room
Key Issues concerning current facility: • Theatre access corridor should not be a
general public corridor; • Inadequate storage areas for clinical
equipment, consumables, cleaning equipment and stores for each functional area (in particular Anaesthetics and Orthopaedics);
• Insufficient space allocated to Recovery and Patient Holding bays;
• Limited staff amenity facilities and office accommodation;
• Issues with confidentiality at Day Surgery Unit
P a g e | 34
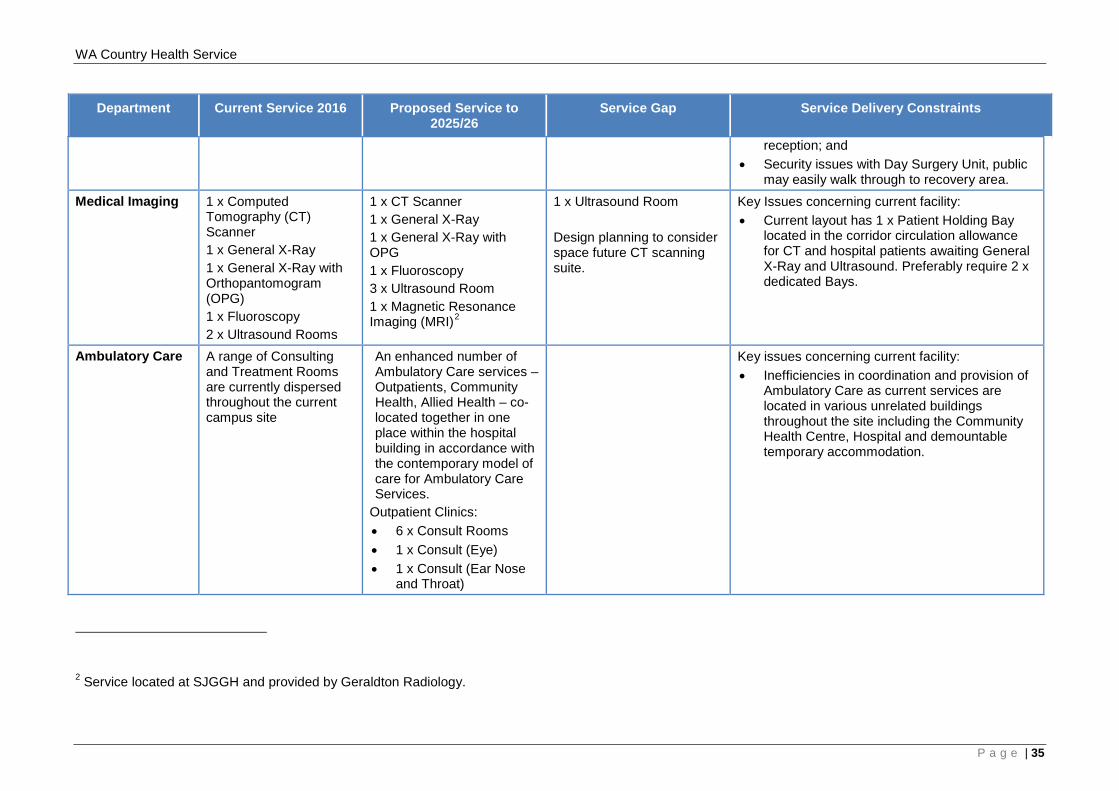
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
reception; and • Security issues with Day Surgery Unit, public
may easily walk through to recovery area. Medical Imaging 1 x Computed
Tomography (CT) Scanner 1 x General X-Ray 1 x General X-Ray with Orthopantomogram (OPG) 1 x Fluoroscopy 2 x Ultrasound Rooms
1 x CT Scanner 1 x General X-Ray 1 x General X-Ray with OPG 1 x Fluoroscopy 3 x Ultrasound Room 1 x Magnetic Resonance Imaging (MRI)2
1 x Ultrasound Room Design planning to consider space future CT scanning suite.
Key Issues concerning current facility: • Current layout has 1 x Patient Holding Bay
located in the corridor circulation allowance for CT and hospital patients awaiting General X-Ray and Ultrasound. Preferably require 2 x dedicated Bays.
Ambulatory Care A range of Consulting and Treatment Rooms are currently dispersed throughout the current campus site
An enhanced number of Ambulatory Care services – Outpatients, Community Health, Allied Health – co-located together in one place within the hospital building in accordance with the contemporary model of care for Ambulatory Care Services.
Outpatient Clinics: • 6 x Consult Rooms • 1 x Consult (Eye) • 1 x Consult (Ear Nose
and Throat)
Key issues concerning current facility: • Inefficiencies in coordination and provision of
Ambulatory Care as current services are located in various unrelated buildings throughout the site including the Community Health Centre, Hospital and demountable temporary accommodation.
2 Service located at SJGGH and provided by Geraldton Radiology.
P a g e | 35
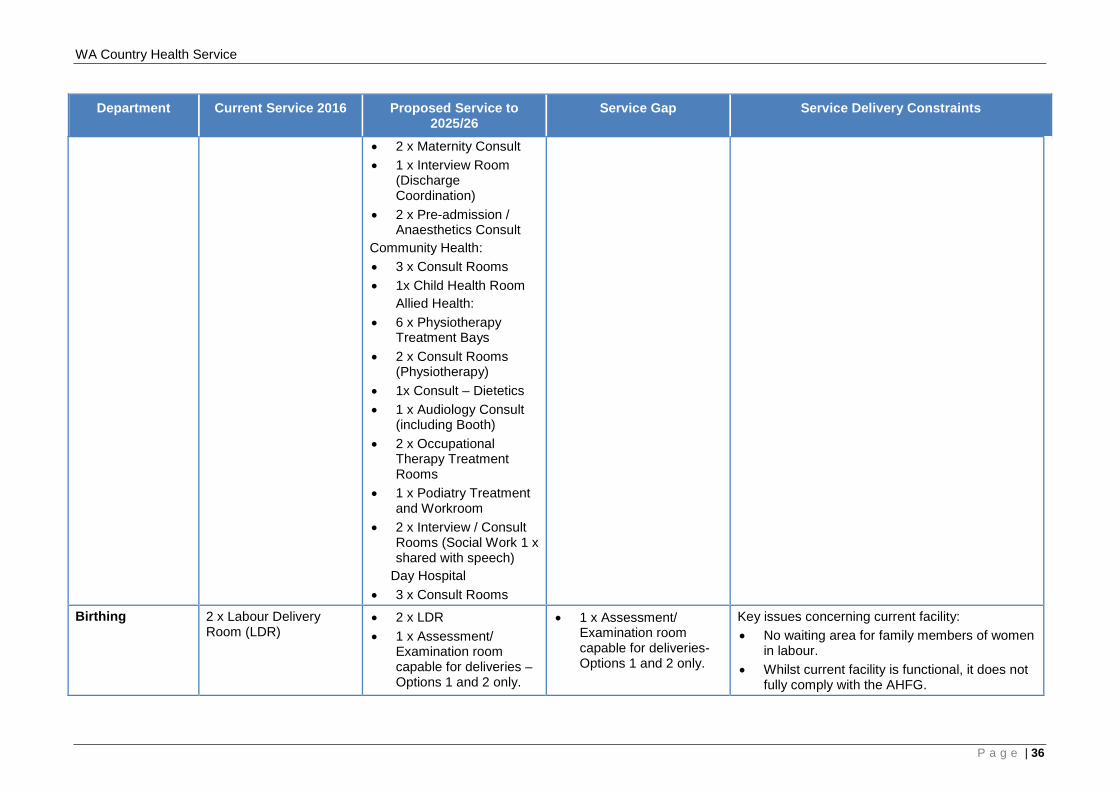
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
• 2 x Maternity Consult • 1 x Interview Room
(Discharge Coordination)
• 2 x Pre-admission / Anaesthetics Consult
Community Health: • 3 x Consult Rooms • 1x Child Health Room
Allied Health: • 6 x Physiotherapy
Treatment Bays • 2 x Consult Rooms
(Physiotherapy) • 1x Consult – Dietetics • 1 x Audiology Consult
(including Booth) • 2 x Occupational
Therapy Treatment Rooms
• 1 x Podiatry Treatment and Workroom
• 2 x Interview / Consult Rooms (Social Work 1 x shared with speech)
Day Hospital • 3 x Consult Rooms
Birthing 2 x Labour Delivery Room (LDR)
• 2 x LDR • 1 x Assessment/
Examination room capable for deliveries – Options 1 and 2 only.
• 1 x Assessment/ Examination room capable for deliveries- Options 1 and 2 only.
Key issues concerning current facility: • No waiting area for family members of women
in labour. • Whilst current facility is functional, it does not
fully comply with the AHFG.
P a g e | 36
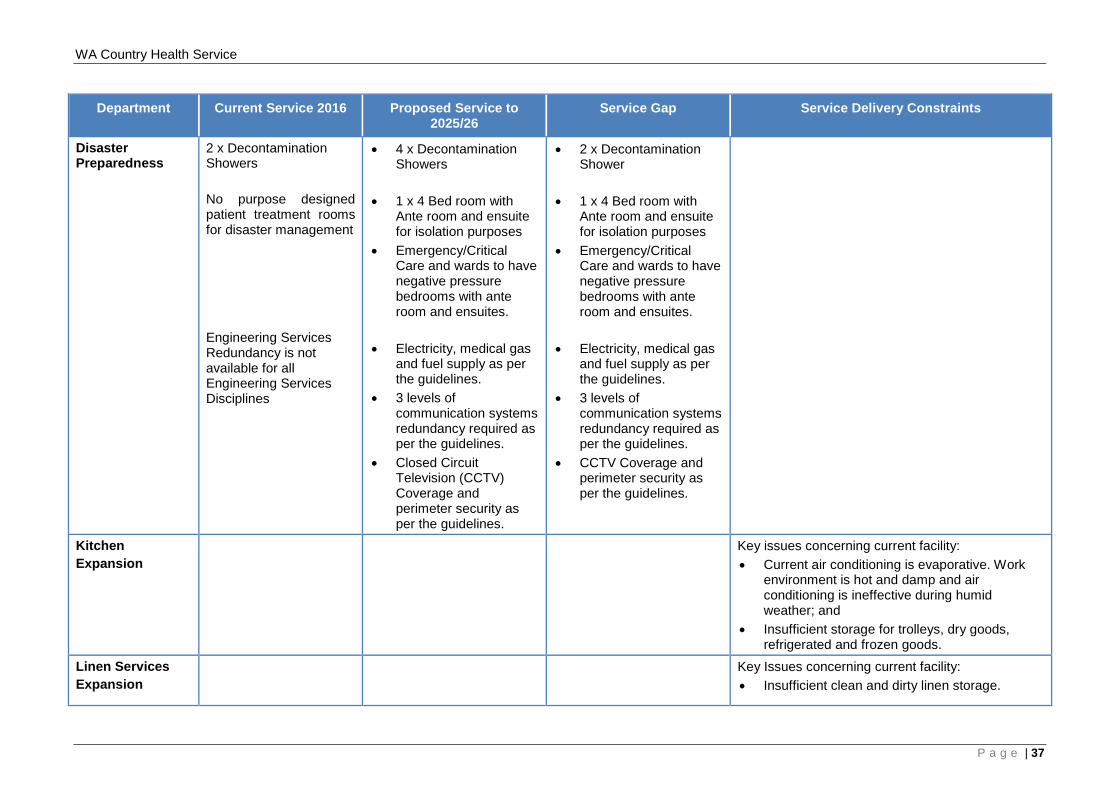
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
Disaster Preparedness
2 x Decontamination Showers No purpose designed patient treatment rooms for disaster management Engineering Services Redundancy is not available for all Engineering Services Disciplines
• 4 x Decontamination Showers
• 1 x 4 Bed room with Ante room and ensuite for isolation purposes
• Emergency/Critical Care and wards to have negative pressure bedrooms with ante room and ensuites.
• Electricity, medical gas and fuel supply as per the guidelines.
• 3 levels of communication systems redundancy required as per the guidelines.
• Closed Circuit Television (CCTV) Coverage and perimeter security as per the guidelines.
• 2 x Decontamination Shower
• 1 x 4 Bed room with Ante room and ensuite for isolation purposes
• Emergency/Critical Care and wards to have negative pressure bedrooms with ante room and ensuites.
• Electricity, medical gas and fuel supply as per the guidelines.
• 3 levels of communication systems redundancy required as per the guidelines.
• CCTV Coverage and perimeter security as per the guidelines.
Kitchen Expansion
Key issues concerning current facility: • Current air conditioning is evaporative. Work
environment is hot and damp and air conditioning is ineffective during humid weather; and
• Insufficient storage for trolleys, dry goods, refrigerated and frozen goods.
Linen Services Expansion
Key Issues concerning current facility: • Insufficient clean and dirty linen storage.
P a g e | 37
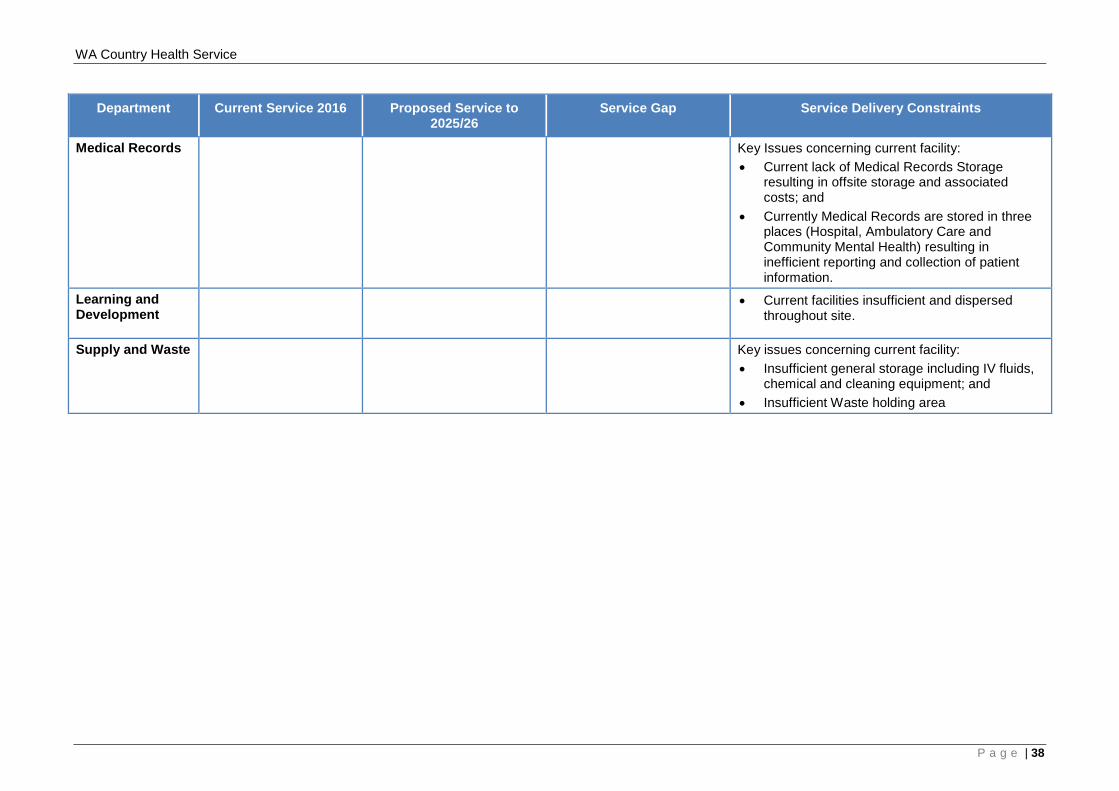
WA Country Health Service
Department Current Service 2016 Proposed Service to 2025/26
Service Gap Service Delivery Constraints
Medical Records Key Issues concerning current facility: • Current lack of Medical Records Storage
resulting in offsite storage and associated costs; and
• Currently Medical Records are stored in three places (Hospital, Ambulatory Care and Community Mental Health) resulting in inefficient reporting and collection of patient information.
Learning and Development
• Current facilities insufficient and dispersed throughout site.
Supply and Waste Key issues concerning current facility: • Insufficient general storage including IV fluids,
chemical and cleaning equipment; and • Insufficient Waste holding area
P a g e | 38
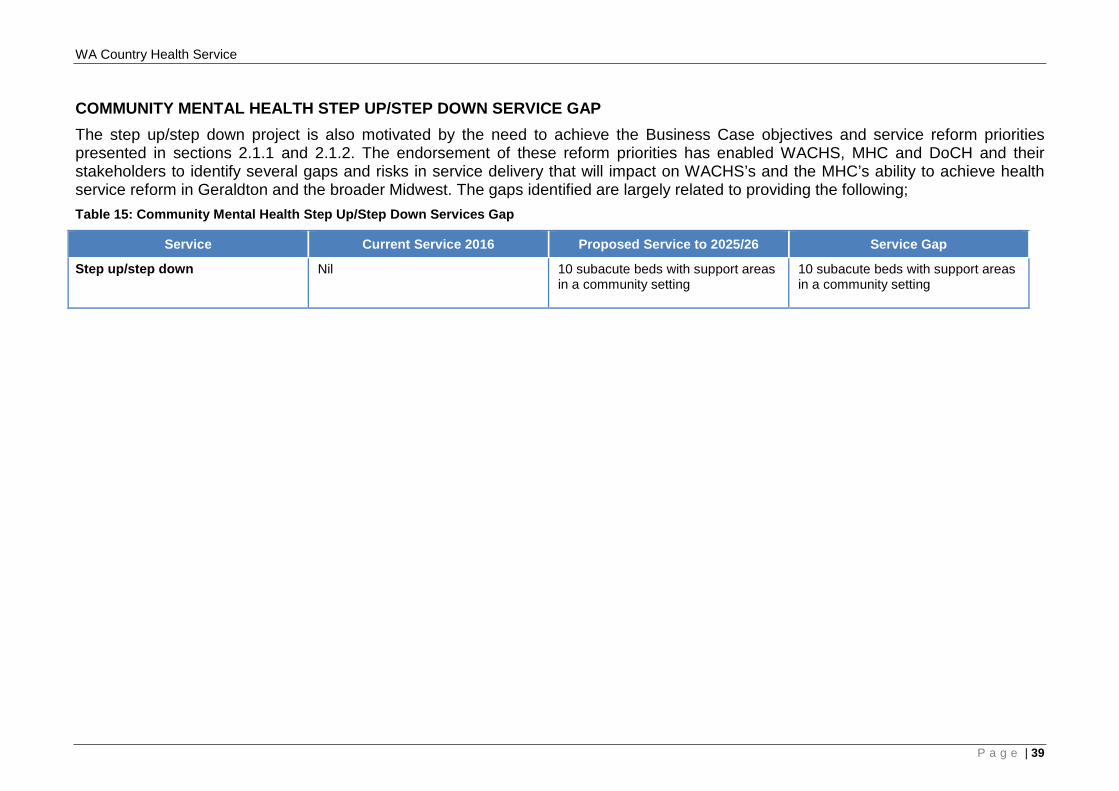
WA Country Health Service
COMMUNITY MENTAL HEALTH STEP UP/STEP DOWN SERVICE GAP The step up/step down project is also motivated by the need to achieve the Business Case objectives and service reform priorities presented in sections 2.1.1 and 2.1.2. The endorsement of these reform priorities has enabled WACHS, MHC and DoCH and their stakeholders to identify several gaps and risks in service delivery that will impact on WACHS’s and the MHC’s ability to achieve health service reform in Geraldton and the broader Midwest. The gaps identified are largely related to providing the following; Table 15: Community Mental Health Step Up/Step Down Services Gap
Service Current Service 2016 Proposed Service to 2025/26 Service Gap
Step up/step down service Nil 10 subacute beds with support areas in a community setting
10 subacute beds with support areas in a community setting
P a g e | 39
WA Country Health Service
2.4 Background
Geraldton Health Campus In 2015, the Midwest Development Commission (MWDC) developed the Midwest Regional Blueprint as a high level strategy for the short, medium and long term objectives for the Midwest region. The regional health and wellbeing goal as stated in the blueprint was for “sophisticated health services and infrastructure provision to support improved health quality of life within communities”. This overarching goal was then translated into high level strategies to:
• Enable health infrastructure that enables the highest standard of healthcare; • Attract and retain high quality healthcare workers in all communities; • Prioritise healthy communities and preventative healthcare; • Enable innovative healthcare provision throughout the region through technology; • Provide best practice mental health and alcohol and drug services and support
throughout the region; • Ensure Aboriginal health indicators match the regions non-Aboriginal population;
and • Ensure aged care services enable Midwest residents to age in place.
Building upon the recommendations and high level health and wellbeing strategies of the blueprint, the WACHS Geraldton Health Campus Services Plan 2010-2020, and the WACHS Strategic Directions 2015 – 2018: Healthier Country Communities through Partnerships and Innovation, identify a strategic direction for service delivery at GHC to 2024. The following overarching priorities were developed:
• Provide services to the level outlined in the WA Health CSF 2014 – 2024; • Provide mental health services in accordance with The Plan; • Optimise time and cost efficiencies in delivering health care services across the
continuum of care; • Provide safe high quality consumer centered care; • Collaborate with health and community partners to increase awareness of health
issues; • Collaborate with health and community partners to broaden the range of service
options available to the community; • Introduce service delivery models that improve access to services; • Enhance Aboriginal health initiatives consistent with our existing programs,
Regional Aboriginal Health Plan and other local priorities; • Build the capacity of Aboriginal health initiatives by attracting and retaining
positions and leadership roles for Aboriginal people; • Improve the health outcomes of the community by providing services closer to
home for the catchment population; • Attract and retain a skilled workforce and visiting specialists; • Increase the use of telehealth and technology solutions in the provision of clinical
and non – clinical services; and • Enhance and strengthen health networks to improve coordination and timeliness
in access to high quality care. In response to the strategic directions for service delivery, the GHC Concept Brief was developed to translate the overarching service and facility requirements for the GHC site.
P a g e | 40
WA Country Health Service
Given the requirement for significant capital upgrades and investment on the GHC site, it has been acknowledged that addressing all elements of the overarching vision for GHC cannot be achieved in the one redevelopment. A staged approach is recommended. Stage One, which this Business Case seeks funding for, includes:
• Emergency/Critical Care expansion in line with projected service need up to 2024 and providing high dependency capability;
• MHSSU beds x 4 (co-located with Emergency/Critical Care); • APU (4 secure and 8 open beds) HITH and CTT; and • Essential engineering service upgrades including the replacement of the chillers.
It is proposed that the future Stage Two and Three redevelopments would address the remaining site objectives with potential for colocation with a private provider. CMDP options and high level site architectural drawings have been developed, costed and approved by the WACHS Midwest region demonstrating that the Stage One scope can be located on the GHC site. Integrated Midwest Mental Health Services The Midwest Health region covers an area of 601,894 square kilometers and is the second largest WACHS region, (Its population is widely dispersed and includes some areas of significant disadvantage, high numbers of low income and single income families, and high levels of developmentally vulnerable children. These are all predictors of greater than average demand for mental health and drug and alcohol services. In 2011, the former Minister for Mental Health requested a review into public mental health services in WA. The resultant report, the Stokes Review, provided clear guidance for reform. The Government response to the Stokes Review was noted by Cabinet who endorsed 115 of the 117 recommendations. The GHC and step up/step down projects will contribute to the implementation of the following relevant Stokes Review recommendations:
• 5.1 – The current acute bed configuration can only be adjusted when there is appropriate step-down rehabilitation and supported accommodation beds established. Any attempt to close acute beds before these systems are in place will be further detrimental to the system.
• 5.3 – Rural child, adolescent and youth beds should be considered a priority in forward planning and attended to immediately. (Whilst not necessarily delivering dedicated youth beds, the Midwest facility will provide acute inpatient beds locally which can be accessed by young people where clinically appropriate).
• 5.4 - Close working between the Department of Health as the provider and the Mental Health Commission as the funder, need to occur so that a robust Clinical Services Plan is developed that provides step-down facilities as an early and pressing need.
• 5.5 – The full range of beds needs to be provided in each geographical area. This is crucial to ensure continuity of care across the spectrum of accommodation.
• 7.9 – Develop respite services and increase rehabilitation services. • 7.10.12 – There is a very real need for day hospital facilities/transition
units/wellbeing centres – whatever one chooses to call them as outlined by Professor Silburn in more locations throughout the metropolitan region and the rest of the State. Such centres will accommodate the difficult transition from
P a g e | 41
WA Country Health Service
admission to the community following discharge and as a community support for those dealing with mental health issues.
• 7.10.13 – There needs to be relevant facilities out of the metropolitan area for short-term care of patients in crisis to avoid dislocation as an added stress.
• 8.2 – After hours’ services are established for children and adolescent services in rural and remote communities where possible. (Enhanced CTT involvement will include child and adolescent mental health services)
Building upon the recommendations of the Stokes Review, this redevelopment will also respond to the requirements detailed in the Plan. This Business Case aims to support the implementation of service reform to establish a fully integrated mental health service by establishing new facilities that support contemporary models of care. This Business Case seeks capital funding to build:
• A new 12 bed APU inpatient facility (8 open and 4 secure beds) on the GHC, inclusive of facilities for staff to operate the 4 bed HITH service, and all elements of the existing CTT, and planned new services
• A new four bed MHSSU, co-located with the GHC Emergency/Critical Care; • A new 10-bed step up/step down service; and • Tele-mental health services.
A CMDP for the step up/step down has been developed using a potential site in Geraldton. A final decision regarding the location and procurement is yet to be confirmed, costed and approved by WACHS and the MHC. The following sections detail the service delivery model relating to the capital infrastructure: Acute Psychiatric Unit The APU will provide comprehensive inpatient assessment and treatment services for consumers from the Midwest region experiencing serious episodes of mental illness who cannot be adequately and safely supported in a less restrictive environment. All 12 beds will be authorised allowing treatment to be provided on an involuntary basis where required. The average length of stay in this service will be 14 days 3. The key functions of the APU are to:
• Provide acute care and crisis interventions to consumers suffering from an acute mental illness;
• Provide multidisciplinary specialist comprehensive assessment and evidence based clinical interventions in a safe, therapeutic and consumer friendly environment;
• Provide physical health screening, assessment, treatment and referral for all consumers admitted into the APU;
• Support consumers to return to live in their community and maintain community living through comprehensive and effective discharge planning in partnership with consumer and their carer/family; and
3 Better Choices. Better Lives. Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015-2015
P a g e | 42
WA Country Health Service
• Facilitate community reintegration through linkages with support agencies and timely onward referral to appropriate internal and external services including community mental health treatment services, community based recovery oriented services (e.g. step up/step down, community living program, community supported residential units, general practitioners and primary health).
Within a recovery focused, trauma informed and culturally appropriate model of care, the APU will:
• Provide evidence-based clinical assessment and treatment services and manage psychiatric emergencies and drug induced psychosis safely and effectively;
• Provide the appropriate levels of physical and visual observation and individual support to maintain a place of safety within a therapeutic and consumer friendly setting;
• Provide education, information and support to consumers, families and carers; and;
• Engage a broad range of community based clinical and non-clinical supports and services to meet individual consumer and family/carer needs.
MMH&CADS will be co-located in the APU to align operational efficiencies and promote a cohesive, integrated approach to mental health services. Co-locating the afore mentioned services within the APU will additionally open up much needed clinical space in the Geraldton Hospital that is currently being utilised by this service. Mental Health Short Stay Unit The proposed MHSSU is an emergency observation area for short-stay consumers with acute mental health disorders and/or AOD issues. The MHSSU will provide mental health assessment and treatment to individuals who may not require admission into a mental health inpatient unit, but do require close observation and intervention for up to 72 hours. The inclusion of four MHSSU beds for GHC is modelled on the mental health observation beds operated at Sir Charles Gardiner Hospital (SCGH) in the metropolitan area. It is acknowledged that the Plan states that this type of facility is usually required in hospitals that have over 500 inpatient beds (National Mental Health Service Planning Framework), however it is also noted in the Plan that careful consideration is required when applying this rationale in the Western Australian context where it is acknowledged that certain hospitals have a high level of mental health emergency presentations. GHC ED presentations for patients with AOD and mental health disorders have increased 13.5% in the period 2012/13, (938 patients) to 2015/16 (1065 patients). It is recognised that complex care is required to properly assess and treat these patients and that not having the dedicated treatment spaces or staff to provide this specialised short term care results in poor consumer outcomes and considerable strain on the current GHC ED. Redevelopment of the GHC Emergency/Critical Care with the provision of a co-located MHSSU which is in close proximity to the APU will:
• Provide a low stimulus environment for psychiatric assessment and brief treatment (72 hours) in a safe environment;
• Consist of 4 beds and an observation nurse station; • Work closely with the APU, CTT and HITH ensuring a seamless referral pathway; • Provide support to other regional sites via Tele-mental Health Services; and • Be managed as part of the MMH&CADS service.
P a g e | 43
WA Country Health Service
Hospital in the Home Assessment and treatment under a HITH service is provided by a multidisciplinary team based at the GHC, in collaboration with consumers, carers and families. This proposal includes the establishment of 4 HITH beds, and will provide short-term intensive management for up to 14 to 21 days, where consumers remain in their own homes (or alternative accommodation), and the multidisciplinary teams travel to the consumers’ home/accommodation to provide the treatment, care and support required. HITH beds provide an alternative to hospital admission and reduce the duration of inpatient admissions providing an increased range of treatment and intervention options for consumers. Proximity to the GHC will form a part of the eligibility for this service in order to ensure responsive and timely face to face interventions as required. Consumers who access these services require a period of additional support because they are becoming unwell, or are in the early stages of recovery from an acute illness and need a short period of additional support to successfully transition back to their homes. Community Mental Health Step Up/Step Down Service Step up/step down provide active recovery oriented treatment and support to minimise the impact of mental illness. Services are recovery-focused, family inclusive, are often delivered in home-like, cluster-style residential facilities; and are staffed 24 hours per day, seven days per week. They provide a mix of clinical interventions and psychosocial support. Step up/step down are expected (where appropriate), to have the capability of meeting the needs of people with co-existing mental health and AOD conditions. Tele-mental Health support Consumers presenting to outlying Midwest hospitals and requiring admission to hospital and/or awaiting transfer to the GHC will have virtual access to specialist services from the CTT via Tele-mental health and Ruralink. This will include:
• Psychiatric assessment; • Support for treatment and discharge planning from Mental Health specialist staff; • Carer support; and • Facilitation and support of transfer where required.
2.4.1 Approvals
PROJECT APPROVALS The GHC redevelopment project has completed the initial planning process required for the submission of the Business Case. The completed planning is supported by the WACHS Geraldton Health Campus Services Plan 2010-2020, and the WACHS Strategic Directions 2015 – 2018: Healthier Country Communities through Partnerships and Innovation in the GHC Concept Brief and CMDP options. The GHC Concept Brief and CMDP options have been endorsed by WACHS Midwest region. Business Case Planning for the step up/step down, is also underway and is supported by The Plan. The Geraldton step up/step down Concept Brief and CMDP option has been endorsed by the MHC and WACHS Midwest region.
LAND Geraldton Health Campus The existing Crown Land Title issued in 2004 for use of the land for the purpose of hospital and allied purposes is still relevant to this project. This Business Case does not
P a g e | 44

WA Country Health Service
seek approval for the purchase of additional land. No land issues have been identified in the site investigations.
P a g e | 45
WA Country Health Service
Community Mental Health Step Up/Step Down Service DoCH has previously investigated land options in Geraldton, and identified a potential site next to one the Department of Health (DoH) have a management order over. DoCH requested DoH to relinquish Lot 2470 to Housing so that the Lots could be combined for the sole purpose of constructing and operating a step up/step down facility. DoH had provided formal in principle support for this to occur. DoCH has not yet preceded with a management order over Lot 2469 Quarry Street (Unallocated Crown land) Greater Geraldton, which would require a land management process undertaken by the Department of Lands, Land Asset Management Unit. The latest advice from DoCH indicates that there are multiple native title claims over Lot 2469 and finding a larger suitable site may be difficult given the terrain in Geraldton. Further investigations in Geraldton have confirmed that a typical step up/step down facility would easily be located on State Government owned land within the Geraldton town site boundaries. If the project receives funding, available land will have to be reviewed and purchased in a timely manner. This project program indicates that ideally the piece of land that the step up/step down will be located upon will already be owned by WA Government.
HERITAGE No items have been placed on the heritage register for the GHC site.
2.4.2 Supporting Documentation
In order to fulfil the vision of WACHS Midwest region, this Business Case will build upon the recommendations as outlined in the Midwest Health Initiative (MWHI) Concept Brief 2014. This document has not been included within the appendix, however is available on request.
2.5 Policy and Strategic Framework
2.5.1 Geraldton Health Campus
The GHC redevelopment project will enable alignment with the following policies and strategic frameworks:
• WA Health Clinical Services Framework 2014-2024 • Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015 –
2025: Better Choices. Better Lives, 2015; • WA Country Health Service - Service Plan 2010 – 2020 Geraldton Health
Campus, WACHS Midwest, Version 6 (May 2012); • WA Country Health Service - Midwest Health Initiative (MWHI) Concept Brief
(October 2014) • WA Country Health Service - Strategic Directions 2015 – 2018: Healthier County
Communities through Partnerships and Innovation (2015); • Council of Australian Governments (COAG) National Health Reform Agreement
(2011); • WA Health WA Health Strategic Intent (2015 – 2020); • WA Health Model of Care, Over view and Guidelines – WA Health Networks • Geraldton Regional Aboriginal Medical Services (GRAMS) Strategic Plan (2015 –
2018);
P a g e | 46
WA Country Health Service
• WA Health – Health Information and Communication Technology (ICT) Strategy (2015 – 2018);
• WACHS Renal Dialysis Plan (2010 – 2021); • WA Mental Health Commission Strategic Plan (2020); • Mental Health Act (2014); • The Drug and Alcohol Interagency Strategic Framework for WA (2011 – 2015); • Review of the admission or referral to and the discharge and transfer practices of
public mental health facilities/services in Western Australia (The Stokes Review), (2012);
• WA Health Redundancy and Disaster Planning in Health’s Capital Works Programs 2nd Edition (January 2012);
• WA Country Health Service WACHS Public and Primary Health Strategy (2015-2018) Healthier Country Communities Through Partnerships and Innovation;
• WA Country Health Service WACHS Healthy Country Kids: An Integrated Child Health and Development Service Strategy 2016-2019 (May 2016);
• WA Country Health Service WACHS Chronic Conditions Prevention and Management Strategy (2015-2020) Healthier Country Communities Through Partnerships and Innovation; and
• Midwest Regional Blueprint (August 2015)
2.5.2 Community Mental Health Step Up/Step Down Services
The step up/step down will enable alignment with the following policies and strategic frameworks:
• Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015 – 2025: Better Choices. Better Lives, 2015;
• Mental Health Commission, Western Australian community mental health step up/step down Model of Service;
• Mental Health Act (2014); • The Drug and Alcohol Interagency Strategic Framework for WA (2011 – 2015); • Mental Health 2020: Making it personal and everybody’s business; and • Review of the admission or referral to and the discharge and transfer practices of
public mental health facilities/services in Western Australia (The Stokes Review), (2012).
2.5.3 Policy Objectives
The redevelopment of GHC and the development of the step up/step down will positively impact the following objectives for regional communities: Building capacity in regional communities The proposed expansion and redevelopment of the Emergency/Critical Care, the development and co-location of the MHSSU with Emergency/Critical Care, a purpose built APU and step up/step down will attract and retain specialist staff in the Midwest region. Specialist staff will bring their expertise and allow for continuing education, training and development. Given the strong relationships GHC has with the Midwest region, the opportunities for specialists to travel and work within other Midwest health facilities will be encouraged for the benefit of both the community and staff.
P a g e | 47
WA Country Health Service
Retaining benefits in regional communities The redeveloped GHC, purpose built APU and step up/step down will provide modern working facilities that align with contemporary models of care. New (or redeveloped) facilities assist in the attraction and retention of staff of all disciplines leading to improved patient and consumer outcomes. The retention of staff, particularly specialist staff will enable patients and consumers to remain in the region for treatment. Improving services to regional communities The GHC redevelopment and step up/step down will respond to the changes in role delineation as stated in the WA Health CSF 2014 – 2024 and the recommendations detailed in The Stokes Review 2012. The increase in service delivery and mental health recommendations will be supported by the infrastructure project and will enable a combination of new and expanded services to be delivered at the GHC and the Midwest region. The step up/step down will respond to the recommendations detailed by the MHC in the Western Australian community mental health step up/step down Model of Service document.
2.5.4 Alignment to Related Strategic Imperatives
GERALDTON HEALTH CAMPUS In addition to the strategic objectives as stated in the WACHS Geraldton Health Campus Services Plan 2010-2020, and the WACHS Strategic Directions 2015 – 2018: Healthier Country Communities through Partnerships and Innovation, the Geraldton Business Case will align with the following Western Australian Regional Development Trust themes. Investment in regional strategic corridors Investment in regional strategic corridors will align with the high level strategy “enable health infrastructure that enables the highest standard of healthcare” as stated in the Midwest Regional Blueprint. The proposed scope of capital works at GHC aligns with contemporary models of health care planning with reference to the AHFG and the NCC. The redeveloped modern facility will attract new specialist staff and provide high level healthcare to patients within Geraldton and the Midwest region. Regional and rural human capacity building: further investment in job-creating activities, particularly investment targeted at Aboriginal workforce participation The GHC redevelopment will aim to attract and retain staff as per the Midwest Regional Blueprint high level strategy “attract and retain high quality healthcare workers in all communities” through new and expanded services on the GHC site. In line with the Geraldton Regional Aboriginal Medicals Service (GRAMS) Strategic Plan 2015 – 2018 and the WA Country Health Service Aboriginal Employment Strategy 2014–2018 the GHC redevelopment will build upon the integrated and coordinated approach to Aboriginal Healthcare through the targeted recruitment of Aboriginal personnel. Retaining aged populations in the country Retaining aged populations in the country is also one of the key strategies of the Midwest Regional Blueprint “ensure aged care services enable Midwest residents to age in place”. The capital element of the GHC Redevelopment Project will ensure all environments will be specifically designed to enable delivery of contemporary specialist
P a g e | 48
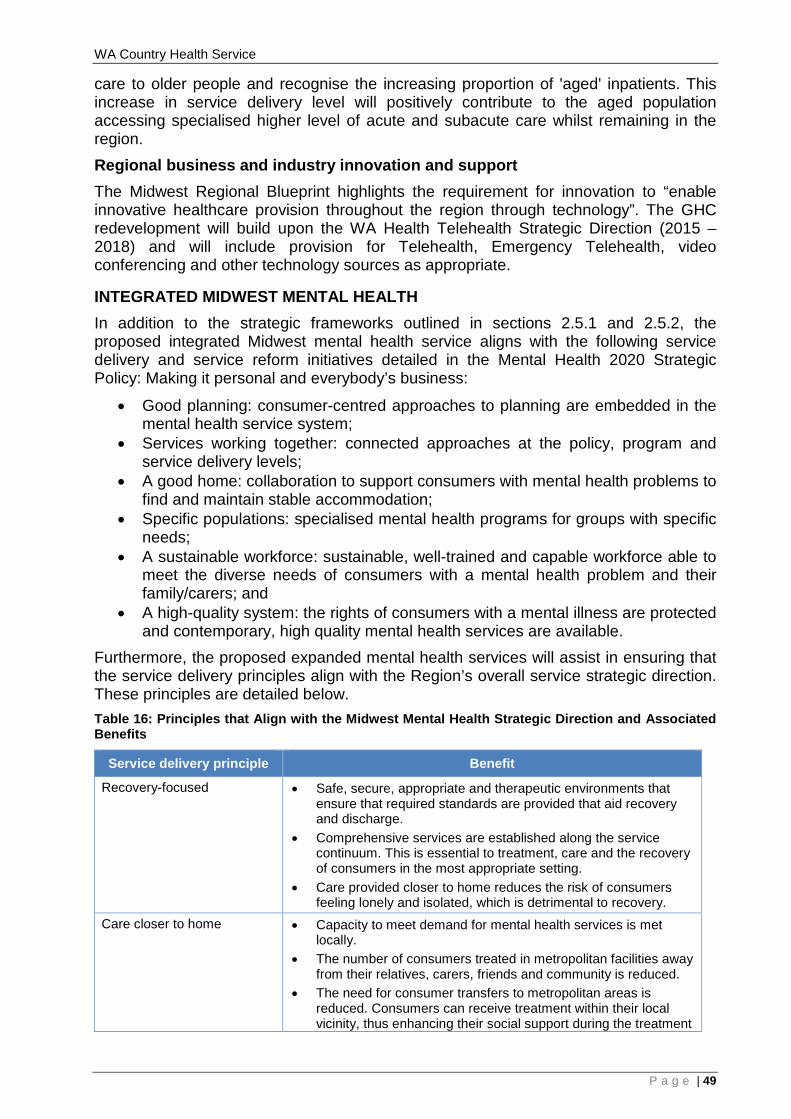
WA Country Health Service
care to older people and recognise the increasing proportion of 'aged' inpatients. This increase in service delivery level will positively contribute to the aged population accessing specialised higher level of acute and subacute care whilst remaining in the region. Regional business and industry innovation and support The Midwest Regional Blueprint highlights the requirement for innovation to “enable innovative healthcare provision throughout the region through technology”. The GHC redevelopment will build upon the WA Health Telehealth Strategic Direction (2015 – 2018) and will include provision for Telehealth, Emergency Telehealth, video conferencing and other technology sources as appropriate.
INTEGRATED MIDWEST MENTAL HEALTH In addition to the strategic frameworks outlined in sections 2.5.1 and 2.5.2, the proposed integrated Midwest mental health service aligns with the following service delivery and service reform initiatives detailed in the Mental Health 2020 Strategic Policy: Making it personal and everybody’s business:
• Good planning: consumer-centred approaches to planning are embedded in the mental health service system;
• Services working together: connected approaches at the policy, program and service delivery levels;
• A good home: collaboration to support consumers with mental health problems to find and maintain stable accommodation;
• Specific populations: specialised mental health programs for groups with specific needs;
• A sustainable workforce: sustainable, well-trained and capable workforce able to meet the diverse needs of consumers with a mental health problem and their family/carers; and
• A high-quality system: the rights of consumers with a mental illness are protected and contemporary, high quality mental health services are available.
Furthermore, the proposed expanded mental health services will assist in ensuring that the service delivery principles align with the Region’s overall service strategic direction. These principles are detailed below. Table 16: Principles that Align with the Midwest Mental Health Strategic Direction and Associated Benefits
Service delivery principle Benefit
Recovery-focused • Safe, secure, appropriate and therapeutic environments that ensure that required standards are provided that aid recovery and discharge.
• Comprehensive services are established along the service continuum. This is essential to treatment, care and the recovery of consumers in the most appropriate setting.
• Care provided closer to home reduces the risk of consumers feeling lonely and isolated, which is detrimental to recovery.
Care closer to home • Capacity to meet demand for mental health services is met locally.
• The number of consumers treated in metropolitan facilities away from their relatives, carers, friends and community is reduced.
• The need for consumer transfers to metropolitan areas is reduced. Consumers can receive treatment within their local vicinity, thus enhancing their social support during the treatment
P a g e | 49
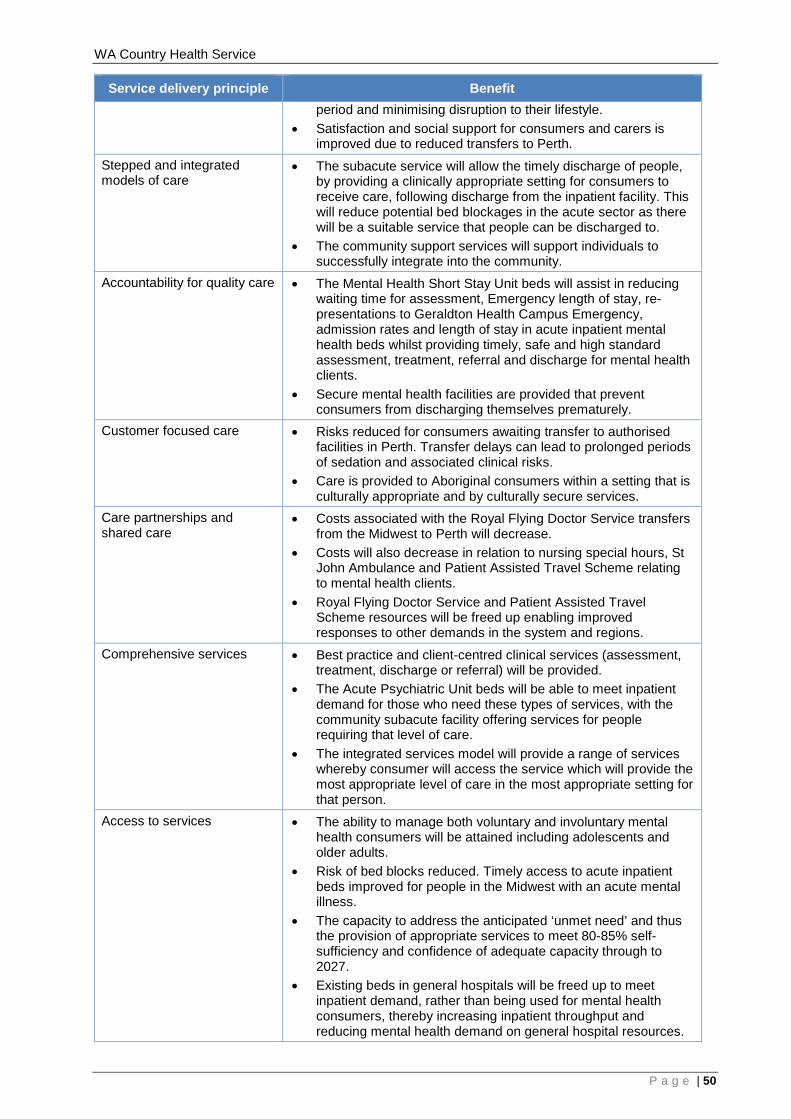
WA Country Health Service
Service delivery principle Benefit period and minimising disruption to their lifestyle.
• Satisfaction and social support for consumers and carers is improved due to reduced transfers to Perth.
Stepped and integrated models of care
• The subacute service will allow the timely discharge of people, by providing a clinically appropriate setting for consumers to receive care, following discharge from the inpatient facility. This will reduce potential bed blockages in the acute sector as there will be a suitable service that people can be discharged to.
• The community support services will support individuals to successfully integrate into the community.
Accountability for quality care • The Mental Health Short Stay Unit beds will assist in reducing waiting time for assessment, Emergency length of stay, re-presentations to Geraldton Health Campus Emergency, admission rates and length of stay in acute inpatient mental health beds whilst providing timely, safe and high standard assessment, treatment, referral and discharge for mental health clients.
• Secure mental health facilities are provided that prevent consumers from discharging themselves prematurely.
Customer focused care • Risks reduced for consumers awaiting transfer to authorised facilities in Perth. Transfer delays can lead to prolonged periods of sedation and associated clinical risks.
• Care is provided to Aboriginal consumers within a setting that is culturally appropriate and by culturally secure services.
Care partnerships and shared care
• Costs associated with the Royal Flying Doctor Service transfers from the Midwest to Perth will decrease.
• Costs will also decrease in relation to nursing special hours, St John Ambulance and Patient Assisted Travel Scheme relating to mental health clients.
• Royal Flying Doctor Service and Patient Assisted Travel Scheme resources will be freed up enabling improved responses to other demands in the system and regions.
Comprehensive services • Best practice and client-centred clinical services (assessment, treatment, discharge or referral) will be provided.
• The Acute Psychiatric Unit beds will be able to meet inpatient demand for those who need these types of services, with the community subacute facility offering services for people requiring that level of care.
• The integrated services model will provide a range of services whereby consumer will access the service which will provide the most appropriate level of care in the most appropriate setting for that person.
Access to services • The ability to manage both voluntary and involuntary mental health consumers will be attained including adolescents and older adults.
• Risk of bed blocks reduced. Timely access to acute inpatient beds improved for people in the Midwest with an acute mental illness.
• The capacity to address the anticipated ‘unmet need’ and thus the provision of appropriate services to meet 80-85% self-sufficiency and confidence of adequate capacity through to 2027.
• Existing beds in general hospitals will be freed up to meet inpatient demand, rather than being used for mental health consumers, thereby increasing inpatient throughput and reducing mental health demand on general hospital resources.
P a g e | 50
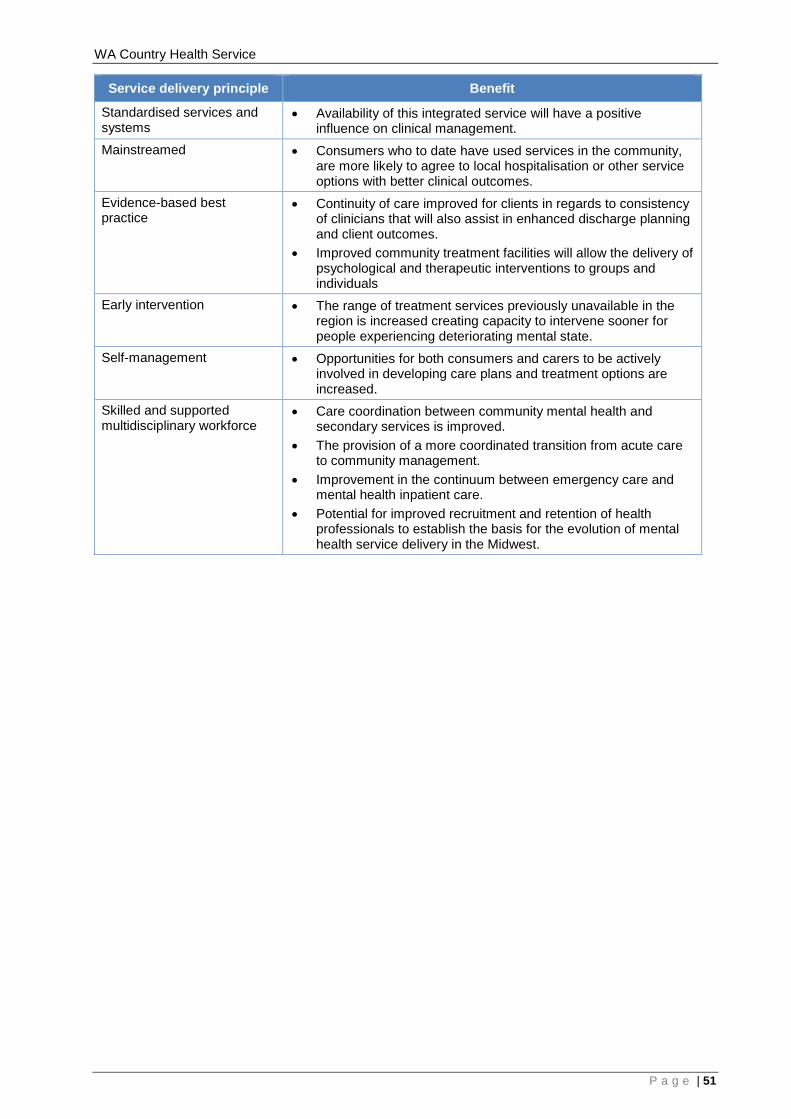
WA Country Health Service
Service delivery principle Benefit
Standardised services and systems
• Availability of this integrated service will have a positive influence on clinical management.
Mainstreamed • Consumers who to date have used services in the community, are more likely to agree to local hospitalisation or other service options with better clinical outcomes.
Evidence-based best practice
• Continuity of care improved for clients in regards to consistency of clinicians that will also assist in enhanced discharge planning and client outcomes.
• Improved community treatment facilities will allow the delivery of psychological and therapeutic interventions to groups and individuals
Early intervention • The range of treatment services previously unavailable in the region is increased creating capacity to intervene sooner for people experiencing deteriorating mental state.
Self-management • Opportunities for both consumers and carers to be actively involved in developing care plans and treatment options are increased.
Skilled and supported multidisciplinary workforce
• Care coordination between community mental health and secondary services is improved.
• The provision of a more coordinated transition from acute care to community management.
• Improvement in the continuum between emergency care and mental health inpatient care.
• Potential for improved recruitment and retention of health professionals to establish the basis for the evolution of mental health service delivery in the Midwest.
P a g e | 51
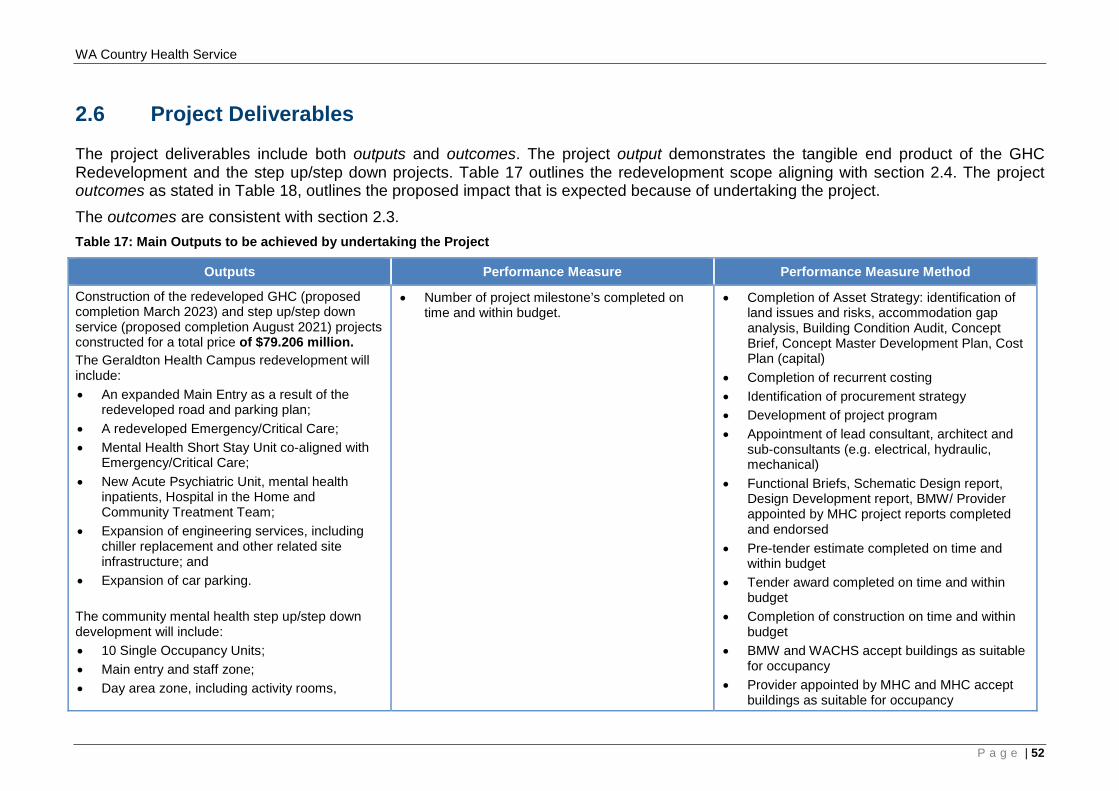
WA Country Health Service
2.6 Project Deliverables
The project deliverables include both outputs and outcomes. The project output demonstrates the tangible end product of the GHC Redevelopment and the step up/step down projects. Table 17 outlines the redevelopment scope aligning with section 2.4. The project outcomes as stated in Table 18, outlines the proposed impact that is expected because of undertaking the project. The outcomes are consistent with section 2.3. Table 17: Main Outputs to be achieved by undertaking the Project
Outputs Performance Measure Performance Measure Method
Construction of the redeveloped GHC (proposed completion March 2023) and step up/step down service (proposed completion August 2021) projects constructed for a total price of $79.206 million. The Geraldton Health Campus redevelopment will include: • An expanded Main Entry as a result of the
redeveloped road and parking plan; • A redeveloped Emergency/Critical Care; • Mental Health Short Stay Unit co-aligned with
Emergency/Critical Care; • New Acute Psychiatric Unit, mental health
inpatients, Hospital in the Home and Community Treatment Team;
• Expansion of engineering services, including chiller replacement and other related site infrastructure; and
• Expansion of car parking. The community mental health step up/step down development will include: • 10 Single Occupancy Units; • Main entry and staff zone; • Day area zone, including activity rooms,
• Number of project milestone’s completed on time and within budget.
• Completion of Asset Strategy: identification of land issues and risks, accommodation gap analysis, Building Condition Audit, Concept Brief, Concept Master Development Plan, Cost Plan (capital)
• Completion of recurrent costing • Identification of procurement strategy • Development of project program • Appointment of lead consultant, architect and
sub-consultants (e.g. electrical, hydraulic, mechanical)
• Functional Briefs, Schematic Design report, Design Development report, BMW/ Provider appointed by MHC project reports completed and endorsed
• Pre-tender estimate completed on time and within budget
• Tender award completed on time and within budget
• Completion of construction on time and within budget
• BMW and WACHS accept buildings as suitable for occupancy
• Provider appointed by MHC and MHC accept buildings as suitable for occupancy
P a g e | 52
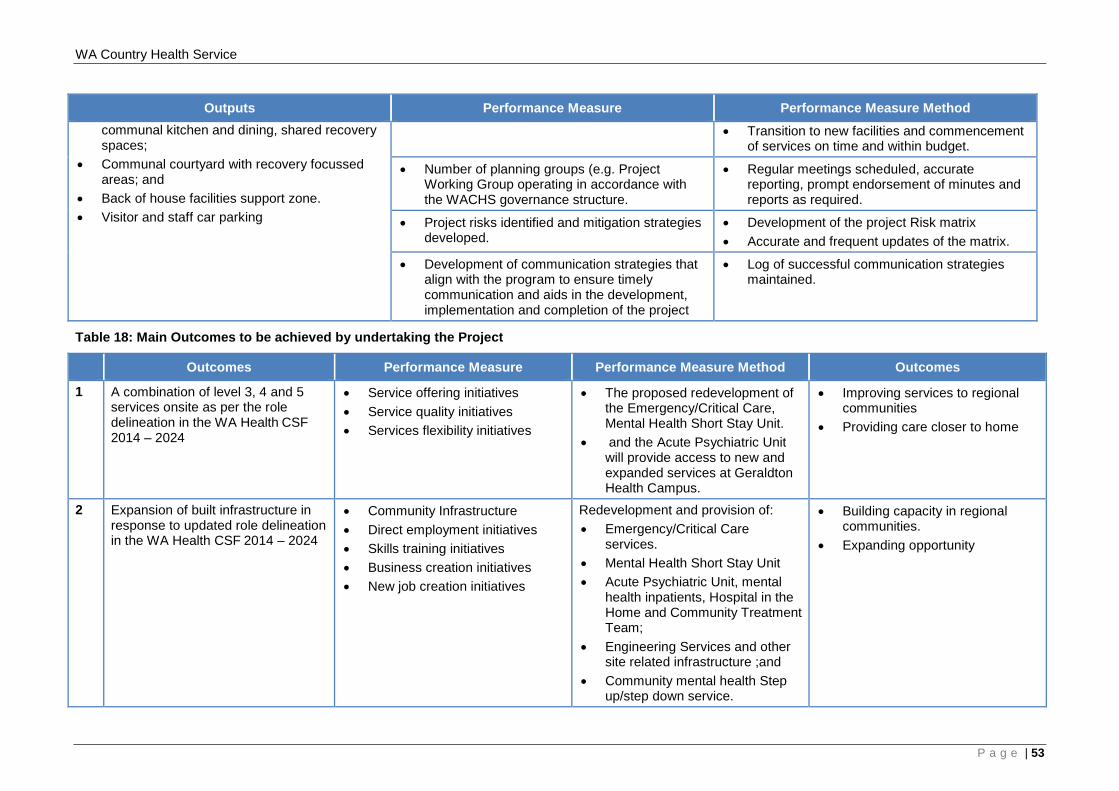
WA Country Health Service
Outputs Performance Measure Performance Measure Method communal kitchen and dining, shared recovery spaces;
• Communal courtyard with recovery focussed areas; and
• Back of house facilities support zone. • Visitor and staff car parking
• Transition to new facilities and commencement of services on time and within budget.
• Number of planning groups (e.g. Project Working Group operating in accordance with the WACHS governance structure.
• Regular meetings scheduled, accurate reporting, prompt endorsement of minutes and reports as required.
• Project risks identified and mitigation strategies developed.
• Development of the project Risk matrix • Accurate and frequent updates of the matrix.
• Development of communication strategies that align with the program to ensure timely communication and aids in the development, implementation and completion of the project
• Log of successful communication strategies maintained.
Table 18: Main Outcomes to be achieved by undertaking the Project
Outcomes Performance Measure Performance Measure Method Outcomes
1 A combination of level 3, 4 and 5 services onsite as per the role delineation in the WA Health CSF 2014 – 2024
• Service offering initiatives • Service quality initiatives • Services flexibility initiatives
• The proposed redevelopment of the Emergency/Critical Care, Mental Health Short Stay Unit.
• and the Acute Psychiatric Unit will provide access to new and expanded services at Geraldton Health Campus.
• Improving services to regional communities
• Providing care closer to home
2 Expansion of built infrastructure in response to updated role delineation in the WA Health CSF 2014 – 2024
• Community Infrastructure • Direct employment initiatives • Skills training initiatives • Business creation initiatives • New job creation initiatives
Redevelopment and provision of: • Emergency/Critical Care
services. • Mental Health Short Stay Unit • Acute Psychiatric Unit, mental
health inpatients, Hospital in the Home and Community Treatment Team;
• Engineering Services and other site related infrastructure ;and
• Community mental health Step up/step down service.
• Building capacity in regional communities.
• Expanding opportunity
P a g e | 53
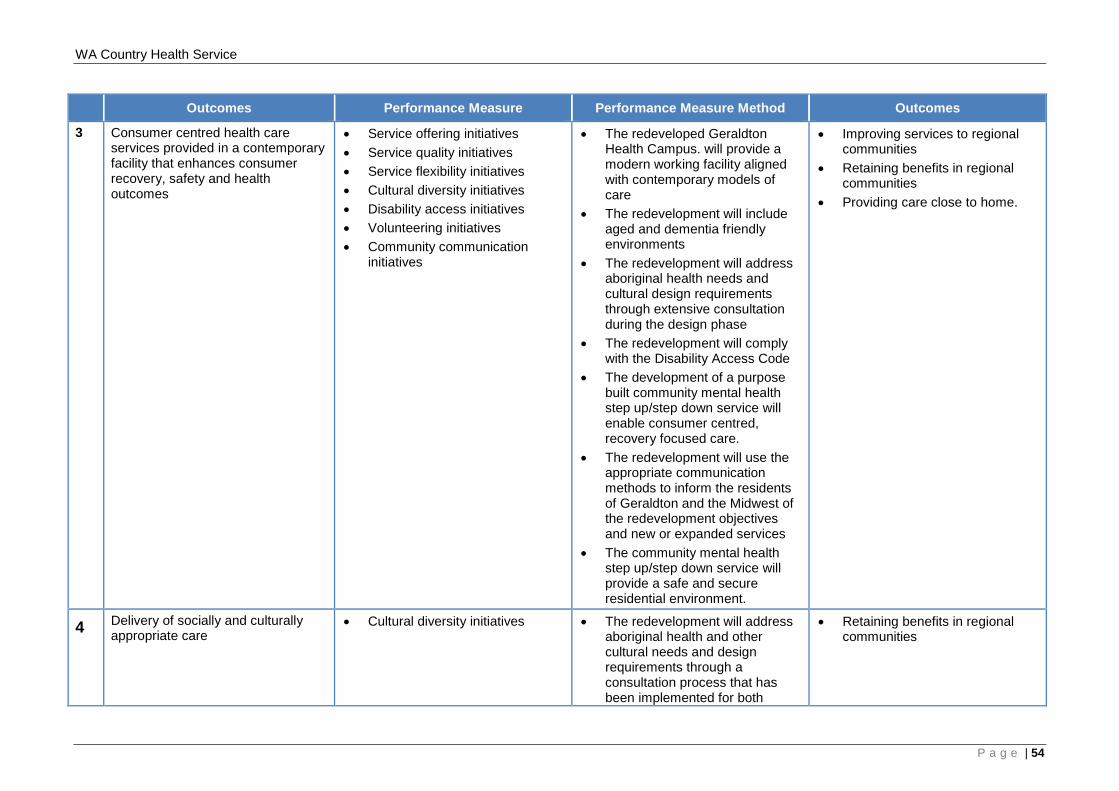
WA Country Health Service
Outcomes Performance Measure Performance Measure Method Outcomes
3 Consumer centred health care services provided in a contemporary facility that enhances consumer recovery, safety and health outcomes
• Service offering initiatives • Service quality initiatives • Service flexibility initiatives • Cultural diversity initiatives • Disability access initiatives • Volunteering initiatives • Community communication
initiatives
• The redeveloped Geraldton Health Campus. will provide a modern working facility aligned with contemporary models of care
• The redevelopment will include aged and dementia friendly environments
• The redevelopment will address aboriginal health needs and cultural design requirements through extensive consultation during the design phase
• The redevelopment will comply with the Disability Access Code
• The development of a purpose built community mental health step up/step down service will enable consumer centred, recovery focused care.
• The redevelopment will use the appropriate communication methods to inform the residents of Geraldton and the Midwest of the redevelopment objectives and new or expanded services
• The community mental health step up/step down service will provide a safe and secure residential environment.
• Improving services to regional communities
• Retaining benefits in regional communities
• Providing care close to home.
4 Delivery of socially and culturally appropriate care
• Cultural diversity initiatives • The redevelopment will address aboriginal health and other cultural needs and design requirements through a consultation process that has been implemented for both
• Retaining benefits in regional communities
P a g e | 54
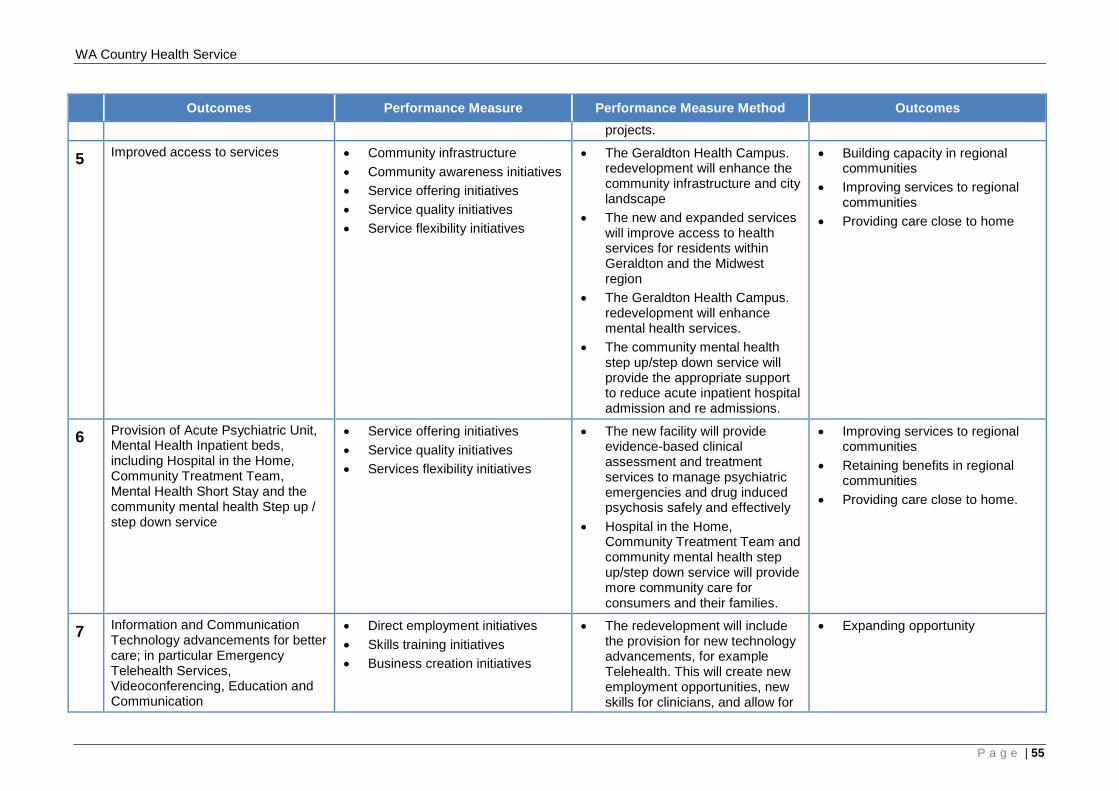
WA Country Health Service
Outcomes Performance Measure Performance Measure Method Outcomes projects.
5 Improved access to services • Community infrastructure • Community awareness initiatives • Service offering initiatives • Service quality initiatives • Service flexibility initiatives
• The Geraldton Health Campus. redevelopment will enhance the community infrastructure and city landscape
• The new and expanded services will improve access to health services for residents within Geraldton and the Midwest region
• The Geraldton Health Campus. redevelopment will enhance mental health services.
• The community mental health step up/step down service will provide the appropriate support to reduce acute inpatient hospital admission and re admissions.
• Building capacity in regional communities
• Improving services to regional communities
• Providing care close to home
6 Provision of Acute Psychiatric Unit, Mental Health Inpatient beds, including Hospital in the Home, Community Treatment Team, Mental Health Short Stay and the community mental health Step up / step down service
• Service offering initiatives • Service quality initiatives • Services flexibility initiatives
• The new facility will provide evidence-based clinical assessment and treatment services to manage psychiatric emergencies and drug induced psychosis safely and effectively
• Hospital in the Home, Community Treatment Team and community mental health step up/step down service will provide more community care for consumers and their families.
• Improving services to regional communities
• Retaining benefits in regional communities
• Providing care close to home.
7 Information and Communication Technology advancements for better care; in particular Emergency Telehealth Services, Videoconferencing, Education and Communication
• Direct employment initiatives • Skills training initiatives • Business creation initiatives
• The redevelopment will include the provision for new technology advancements, for example Telehealth. This will create new employment opportunities, new skills for clinicians, and allow for
• Expanding opportunity
P a g e | 55
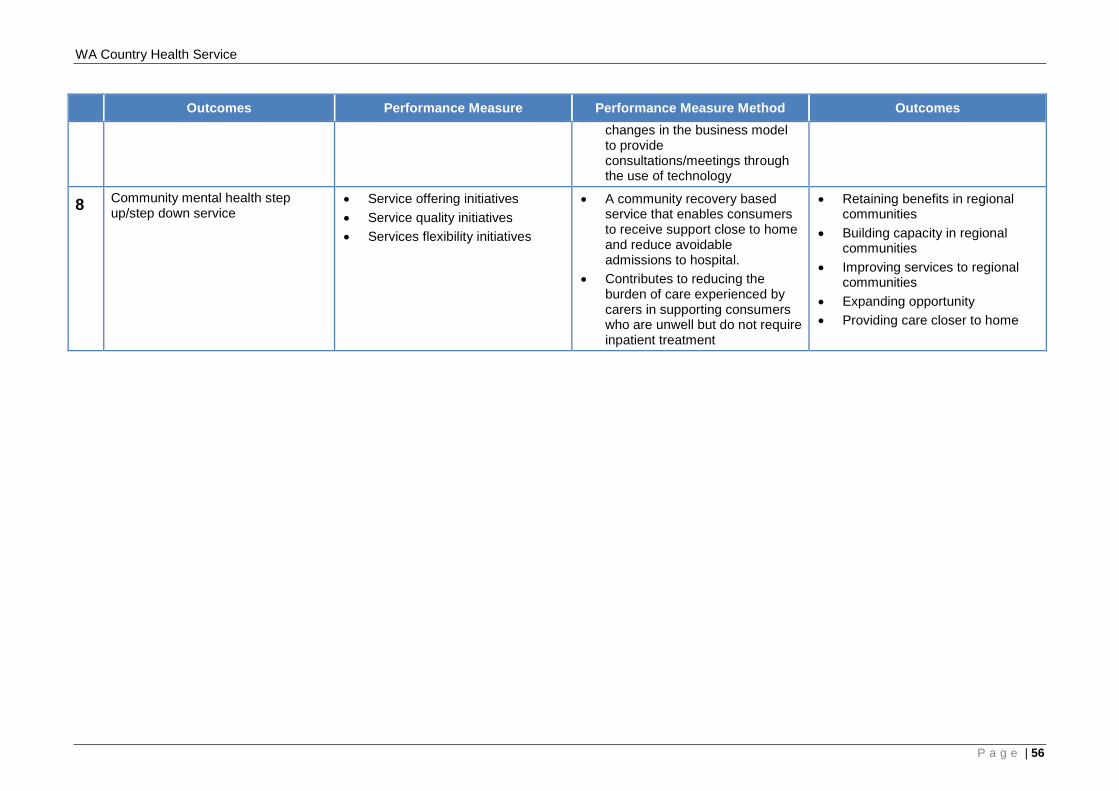
WA Country Health Service
Outcomes Performance Measure Performance Measure Method Outcomes changes in the business model to provide consultations/meetings through the use of technology
8 Community mental health step up/step down service
• Service offering initiatives • Service quality initiatives • Services flexibility initiatives
• A community recovery based service that enables consumers to receive support close to home and reduce avoidable admissions to hospital.
• Contributes to reducing the burden of care experienced by carers in supporting consumers who are unwell but do not require inpatient treatment
• Retaining benefits in regional communities
• Building capacity in regional communities
• Improving services to regional communities
• Expanding opportunity • Providing care closer to home
P a g e | 56
WA Country Health Service
2.7 Stakeholder Engagement
To understand the full extent of the requirements for the GHC Redevelopment and step up/step down projects and to ensure a successful outcome for both, it is recognised that it is essential to fully engage with all stakeholders. The consultation to date has largely occurred with internal stakeholders although key external stakeholders have been identified and the process for future engagement is outlined as part of the ongoing communications plan (refer section 3.1). Internal stakeholders include key staff recognised for their expertise and understanding in what are the particular and essential redevelopment requirements for these projects. The Project Working Group (PWG) has been the key mechanism for stakeholder engagement. The membership and structure is described in detail in the Governance section (refer section 3.3). The following course of action outlines the process of engagement with internal stakeholders to progress and establish the various GHC and step up/step down CMDP options for both sites:
• Site visit and review of existing facilities to develop the GHC Concept Brief (including robust Schedules of Accommodation – refer Appendix A). Future service delivery requirements for the GHC could be determined following internal consultation with the GHC staff providing direct services, in combination with consultation with the WACHS Clinical Planning Unit and reference to the WA Health CSF 2014 – 2024;
• Consultation and liaison with the MHC, a site visit to the Rockingham step up/step down facility (extensive consultation with staff) and a desk top review of current literature and associated similar current facilities, informed the development of the Concept Brief and associated Schedules of Accommodation (refer Appendix C).
• The GHC and step up/step down Concept Briefs were presented to the PWG and MHC for review, update and endorsement;
• The GHC and step up/step down Concept Briefs have informed the development of the CMDP options and associated programming and cost planning for both sites;
• A PWG workshop meeting with the architect and cost planner was held to explore and evaluate the first CMDP option against key criteria selected from both Concept Briefs. Once accepted and costed, two more CMDP options were then developed and costed for GHC. One CMDP was developed for the step up /step down; and
• The approvals process to date has constituted the review of key documentation in alignment with the well-established WACHS and MHC governance structures.
The detailed assessment of four CMDP options for GHC and the CMDP for step up/step down is featured in Section 2.10 of this document. The following two tables includes internal and external stakeholders that are relevant to the development of the Business Case and future planning processes for the redevelopment of the GHC and the design and construction of step up/step down.
P a g e | 57
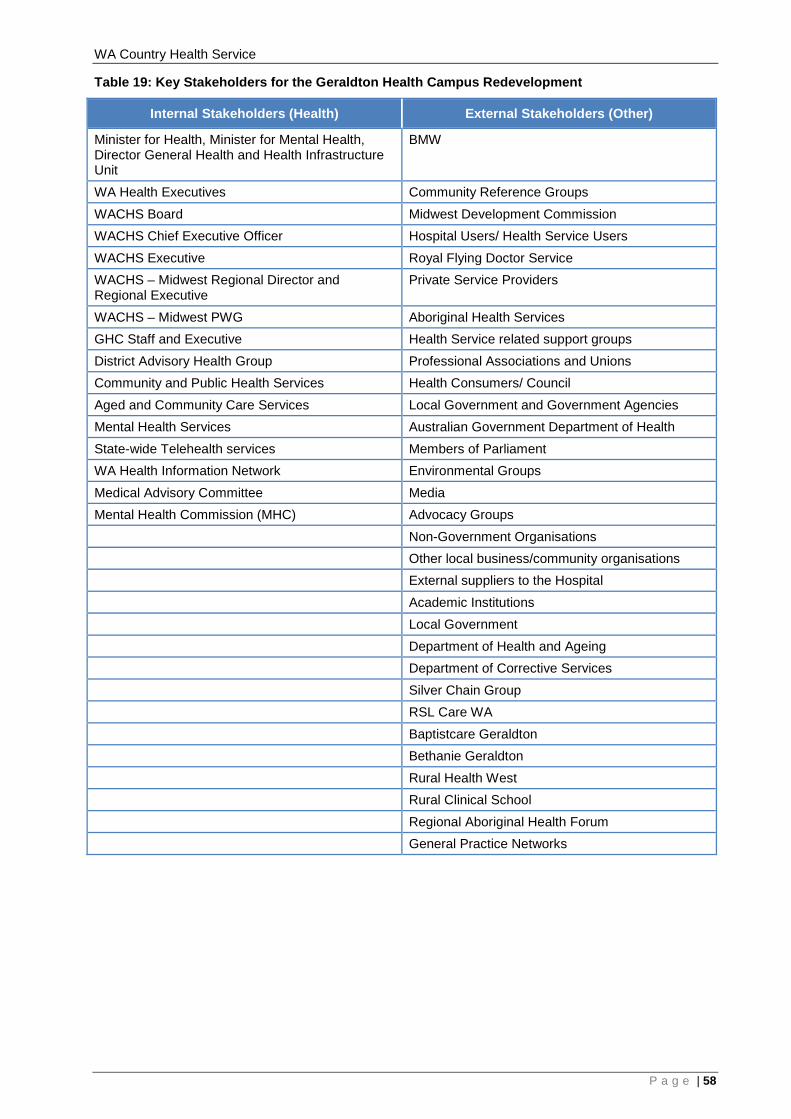
WA Country Health Service
Table 19: Key Stakeholders for the Geraldton Health Campus Redevelopment
Internal Stakeholders (Health) External Stakeholders (Other)
Minister for Health, Minister for Mental Health, Director General Health and Health Infrastructure Unit
BMW
WA Health Executives Community Reference Groups WACHS Board Midwest Development Commission WACHS Chief Executive Officer Hospital Users/ Health Service Users WACHS Executive Royal Flying Doctor Service WACHS – Midwest Regional Director and Regional Executive
Private Service Providers
WACHS – Midwest PWG Aboriginal Health Services GHC Staff and Executive Health Service related support groups District Advisory Health Group Professional Associations and Unions Community and Public Health Services Health Consumers/ Council Aged and Community Care Services Local Government and Government Agencies Mental Health Services Australian Government Department of Health State-wide Telehealth services Members of Parliament WA Health Information Network Environmental Groups Medical Advisory Committee Media Mental Health Commission (MHC) Advocacy Groups Non-Government Organisations Other local business/community organisations External suppliers to the Hospital Academic Institutions Local Government Department of Health and Ageing Department of Corrective Services Silver Chain Group RSL Care WA Baptistcare Geraldton Bethanie Geraldton Rural Health West Rural Clinical School Regional Aboriginal Health Forum General Practice Networks
P a g e | 58
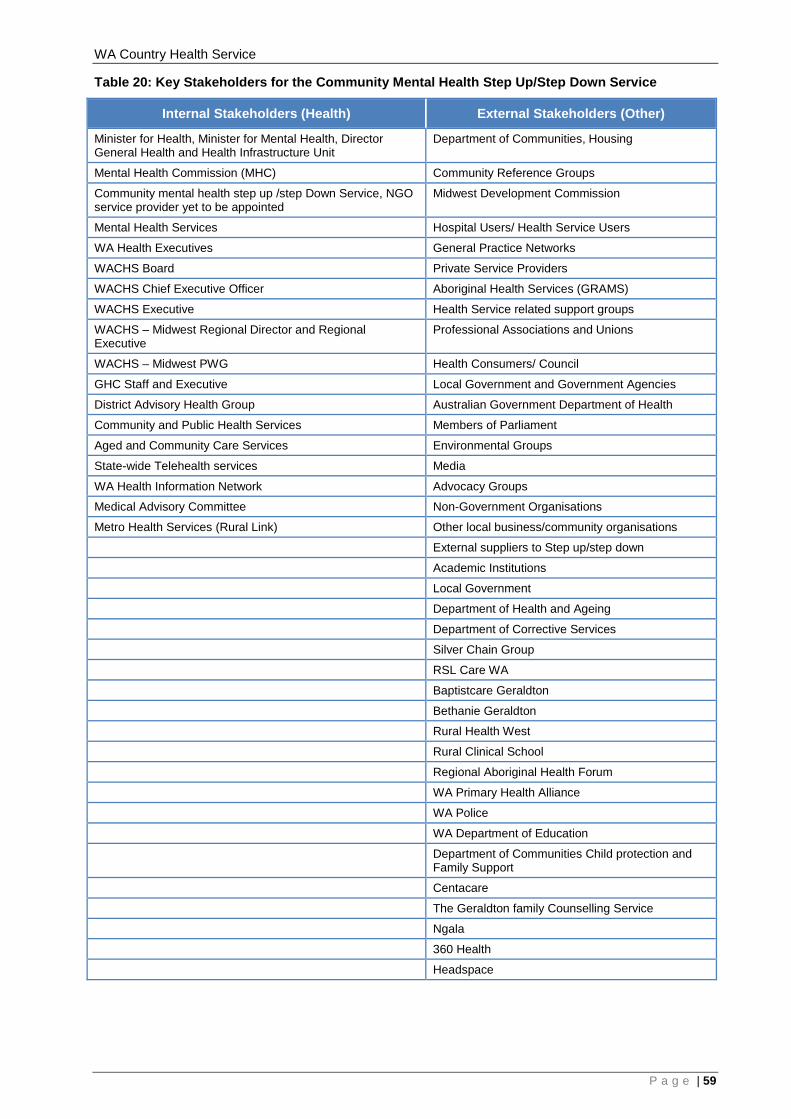
WA Country Health Service
Table 20: Key Stakeholders for the Community Mental Health Step Up/Step Down Service
Internal Stakeholders (Health) External Stakeholders (Other)
Minister for Health, Minister for Mental Health, Director General Health and Health Infrastructure Unit
Department of Communities, Housing
Mental Health Commission (MHC) Community Reference Groups
Community mental health step up /step Down Service, NGO service provider yet to be appointed
Midwest Development Commission
Mental Health Services Hospital Users/ Health Service Users
WA Health Executives General Practice Networks
WACHS Board Private Service Providers
WACHS Chief Executive Officer Aboriginal Health Services (GRAMS)
WACHS Executive Health Service related support groups
WACHS – Midwest Regional Director and Regional Executive
Professional Associations and Unions
WACHS – Midwest PWG Health Consumers/ Council
GHC Staff and Executive Local Government and Government Agencies
District Advisory Health Group Australian Government Department of Health
Community and Public Health Services Members of Parliament
Aged and Community Care Services Environmental Groups
State-wide Telehealth services Media
WA Health Information Network Advocacy Groups
Medical Advisory Committee Non-Government Organisations
Metro Health Services (Rural Link) Other local business/community organisations
External suppliers to Step up/step down
Academic Institutions
Local Government
Department of Health and Ageing
Department of Corrective Services
Silver Chain Group
RSL Care WA
Baptistcare Geraldton
Bethanie Geraldton
Rural Health West
Rural Clinical School
Regional Aboriginal Health Forum
WA Primary Health Alliance
WA Police
WA Department of Education
Department of Communities Child protection and Family Support
Centacare
The Geraldton family Counselling Service
Ngala
360 Health
Headspace
P a g e | 59
WA Country Health Service
2.8 Critical Assumptions
The following assumptions have been made in determining the outcomes of the GHC redevelopment and the step up/step down projects: Geraldton Health Campus Redevelopment
• The redevelopment will address the deficits identified within the existing Hospital, meet contemporary health design standards and provide optimal functional relationships;
• The redevelopment will create an environment that is safe for patients, staff and visitors;
• The redevelopment will provide sufficient health service capacity to support future demands of the catchment area by Growing the “Hub and Spoke” Health Service Delivery model with the GHC supporting multipurpose centers and regional health providers in smaller communities;
• The redevelopment will improve the effectiveness and safety of patient care in the Emergency/Critical Care so 24-hour medical cover is provided and it is closely aligned with acute services facilities such as Emergency/Critical Care, Operating Theatres, Pathology and Medical Imaging;
• Enhancing health services in high Aboriginal population settlements through further expansion of the GRAMS model and working with Carnarvon Medical Service Aboriginal Corporation (CMSAC);
• Telemedicine systems will become more commonly used; • More health care consultations for services not available locally are being
delivered through video conferencing and supported by digital diagnostic data; • Increasing numbers of non-rural based health care providers (including medical
specialists) are developing skills at remote, on line, consultation, diagnosis and support;
• WACHS is committed to investing in advancing technology to improve health delivery;
• Staffing resources will be available to operate proposed services; • Staffing levels will reflect the relevant activity profile; • Offices and housing accommodation is available to staff; • Whilst a high level car parking analysis has been conducted for the CMDP
options, it will be further interrogated during Stage One of the redevelopment to reduce costs caused by abortive work; and
• The redevelopment will improve staff attraction, recruitment and retention. Community Mental Health Step Up/Step Down Service
• The service will support individuals and their families in the community to improve their quality of life and reduce the need for admission to an inpatient setting;
• The focus of the service is to be related to individual recovery and promotion of independence;
• The service will be domestic in setting and will integrate well within the local neighborhood and community;
• The service will create an environment that is safe for individuals, staff and visitors;
• Synergies between the APU, CTT and this service will be fostered; • Staffing resources will be available to operate proposed services; • Staffing levels will reflect the relevant activity profile;
P a g e | 60
WA Country Health Service
• Offices and housing accommodation is available in the community for staff; and • The facility will attract staff and assist with staff retention.
2.9 Social and Economic Analyses
The GHC redevelopment and the step up/step down projects will result in a range of social and economic benefits for the local and surrounding communities. The investment will address the recognised gaps in service provision, address rising level of current and projected demand and provide new opportunities for synergy. Building upon the benefits outlined in sections 2.5.3 and 2.5.4 of this Business case, key benefits for Geraldton and the broader Midwest region are further identified but not limited to the following. Improved access to necessary services for the Midwest community to meet rising demand A core element of a regional health system is the role of the GHC as a Regional Resource Centre. If Geraldton Hospital does not have the capability to eventually provide the full range of identified services, as outlined in this Business Case, elements of the region’s population will find it necessary to seek care in Perth. This puts undue financial and social pressure on local individuals, families and the health service as a result of having to travel to Perth and being disconnected from support networks. It also places pressure on metropolitan services for both general and mental health services. It should be noted that with the enhancement of the Emergency service to deliver Emergency/Critical Care services there will be the ability to treat patients in Geraldton and not have to transfer critically compromised patients to Perth for treatment. GHC processes a large number of these types of patients which is a compromised and ineffective model of care preventing patients being provided care closer to home. Integrated mental health services for the Midwest region WACHS currently manages a community mental health service which also provides in-reach services to hospitals in the region. The service is based in Geraldton with satellite teams in Carnarvon, Meekatharra and Exmouth. There are no dedicated mental health or drug and alcohol inpatient beds in the Midwest. Patients are frequently admitted into a general ward in Geraldton Hospital, to other hospitals in the Midwest or transferred out of the region to Perth for clinical care resulting in financial pressure to deliver the expected services from the respective sites. The cost of transferring patients to the metropolitan area comes at a significant cost to Government. There are often delays in transferring mentally unwell patients; this presents an elevated level of clinical risk to the patient as well as raising concerns for the safety of staff and, at times, other patients. Addressing these will improve outcomes for people with mental health and drug and alcohol problems. The current lack of an APU facility within the Midwest region restricts the ability to provide care close to home for Midwest residents and reduces continuity of care. In particular, this is a distinct issue for involuntary mental health patients, as a significant number of these patients admitted in the region have experienced a delay in transfer due to unavailability of beds at Graylands Hospital and other metropolitan facilities. The delay in transfer not only reduces the continuity of care, it poses significant clinical and security risks for the mental health patient, other hospital patients and staff, in both the Emergency and Inpatient areas. If APU and Mental Health Short Stay beds are not developed at GHC this situation is likely to get worse in the future, as Graylands
P a g e | 61
WA Country Health Service
Hospital continues to downsize, in preparation of the final closure by 2025, as per the Plan. To enable the existing services at Graylands Hospital to be decommissioned and the site divested, it is necessary for new community-based services and other inpatient units to be established, to enable consumers to be transferred effectively and safely from Graylands Hospital. Due to the lack of this current service there are individuals suffering from not receiving adequate treatment in a timely manner that results in a loss of employment adding burden to their own circumstances and that of the community. The provision of APU beds will facilitate community reintegration through linkages with support agencies and timely onward referral to appropriate internal and external services including community mental health treatment services, community based recovery oriented services (e.g. step up/step down, community living program, community supported residential units, general practitioners and primary health) thereby relieving the pressures that arise from utilising existing general inpatient beds. Similarly, the promotion of HITH beds provides an alternative to hospital admission and reduces the duration of inpatient admissions providing an increased range of treatment and intervention options for consumers. Consumers who access these services require a period of additional support because they are becoming unwell, or are in the early stages of recovery from an acute illness and need a short period of additional support to successfully transition back to their homes. Increased general health and well-being In 2011, the ABS, Socio-economic Indexes for Areas (20033.0.55.011), recorded the Shires of Meekatharra, Mount Magnet, Murchison and Wiluna as ranked in the top 10% of the most socio‑economically disadvantaged areas within WA and Geraldton was ranked within the top 20%. Given that a community's socio‑economic characteristics have a significant impact on health behaviours and outcomes, there is an important need to promote healthy communities and encourage preventative health care. As hospitals and community services are an essential part of the community, the provision of service delivery driven outcome facilities solutions will enable increased communication, participation and economic growth for the overall community. Job creation, workforce benefits and economic development. Investment in the health facilities and consequently the services will enhance the ability of the Midwest region to recruit and retain highly skilled health professionals. This is essential for the ongoing sustainability and growing prosperity of the catchment area. The recurrent analysis that has been undertaken for the Business Case anticipates an increase in Full Time Equivalent (FTE) staff numbers relative to the increased activity as a result of redirection of patients that are currently receiving services in a metropolitan tertiary facility who will now be cared for closer to home. The increase in FTE will be funded through a redirection of Activity Based Funding as a result. In turn this will have a positive local economic impact by enhancing the ability of families to be provided for and education opportunities realised. Increased mental health services through the APU, Mental Health Short Stay unit and Step Up Step Down facility will result in economic development with over 100 jobs being created within WA Country Health Service and the NGO sector funded through re-directed and increased activity based funding. This in turn can be linked to more activity in the community in general for services such as schools and other government departments, housing, retail etc and therefore stimulating economic growth for the Region.
P a g e | 62

WA Country Health Service
P a g e | 63
WA Country Health Service
Local economy impact from jobs arising from the impact of the construction of the project BMW has advised that based on an approximate $78 million budget an estimate of a total workforce of some 600 persons during the construction phase would be expected. BMW based this on extrapolating actual data realised on the Southern Inland Health Initiative program of works where all main projects are currently in construction. The local area of Geraldton is home to a substantially capable sub-contractor market which will enable involvement of local suppliers. Facilities upgrades to achieve building compliance and increase safety The proposed upgrade of the relevant existing facilities and the provision of new facilities will achieve compliance with current NCC and AHFG. This will enhance the delivery of safe and efficient services. Prolonged consideration of a ‘Do Nothing’ option would incur risk and result in:
• Demand continuing to exceed capacity and services being delivered in suboptimal facilities, potentially compromising patient care and staff safety;
• Further increased reliance on patient transport; • Increasing maintenance costs due to high patient turnover/traffic/throughput; and • Escalating financial and social cost of operating inefficient facilities, based on out
dated models of care.
2.10 Assessment of Options
Four Options have been developed for evaluation in this Business Case. These include redevelopment on the GHC site as well as the design and construction of the step up/step down in a community setting in Geraldton. The four options, as outlined in Table 18, have been developed recognising the requirement for a staged GHC development. Furthermore, the site planning includes capacity for other facilities and colocation opportunities (e.g. private providers) on the GHC site in the future. Additionally, future expansion of services has also been considered. Due to the timeframes associated with development and completion of this Business Case, the detailed engineering and GHC site services reports usually undertaken to inform the options definitions and costings have been limited. It is therefore the intent that detailed investigation of services and site will take place during the PDP stage of the project. In order to mitigate the risk of unknown site constraints/issues, BMW has provided the following comments;
• Appropriate contingencies have been included in this project to cover potential extra site constraints/issues, and planning and design not sufficiently investigated due to time limitations in developing this Business Case;
• Necessity for a detailed PDP to test and validate project budget for the proposed site before proceeding to construction; and
• This applies to all options presented in this Business Case. It should be noted that due to time constraints and the urgent requirement to develop the CMDP’s, a long list of options has not been developed.
P a g e | 64
WA Country Health Service
One CMDP option has been developed for the step up/step down. This service is included within each option for this Business Case.
P a g e | 65
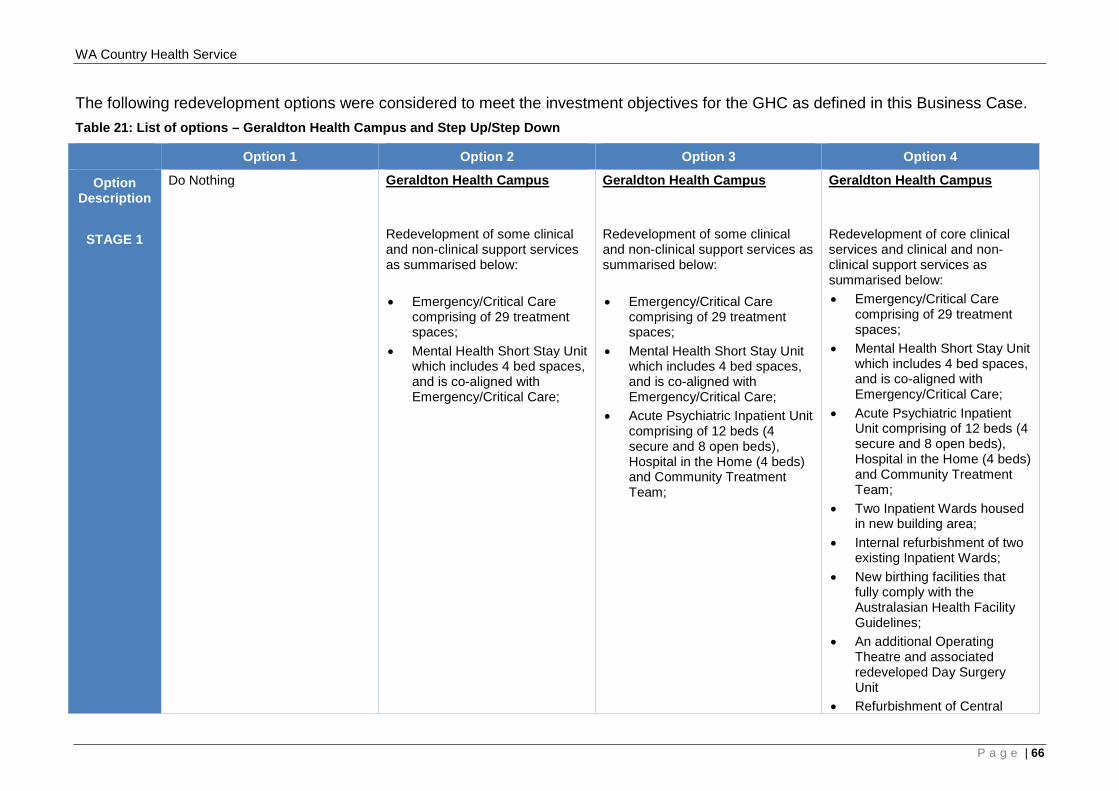
WA Country Health Service
The following redevelopment options were considered to meet the investment objectives for the GHC as defined in this Business Case. Table 21: List of options – Geraldton Health Campus and Step Up/Step Down
Option 1 Option 2 Option 3 Option 4
Option Description
STAGE 1
Do Nothing Geraldton Health Campus Redevelopment of some clinical and non-clinical support services as summarised below: • Emergency/Critical Care
comprising of 29 treatment spaces;
• Mental Health Short Stay Unit which includes 4 bed spaces, and is co-aligned with Emergency/Critical Care;
Geraldton Health Campus Redevelopment of some clinical and non-clinical support services as summarised below: • Emergency/Critical Care
comprising of 29 treatment spaces;
• Mental Health Short Stay Unit which includes 4 bed spaces, and is co-aligned with Emergency/Critical Care;
• Acute Psychiatric Inpatient Unit comprising of 12 beds (4 secure and 8 open beds), Hospital in the Home (4 beds) and Community Treatment Team;
Geraldton Health Campus Redevelopment of core clinical services and clinical and non-clinical support services as summarised below: • Emergency/Critical Care
comprising of 29 treatment spaces;
• Mental Health Short Stay Unit which includes 4 bed spaces, and is co-aligned with Emergency/Critical Care;
• Acute Psychiatric Inpatient Unit comprising of 12 beds (4 secure and 8 open beds), Hospital in the Home (4 beds) and Community Treatment Team;
• Two Inpatient Wards housed in new building area;
• Internal refurbishment of two existing Inpatient Wards;
• New birthing facilities that fully comply with the Australasian Health Facility Guidelines;
• An additional Operating Theatre and associated redeveloped Day Surgery Unit
• Refurbishment of Central
P a g e | 66
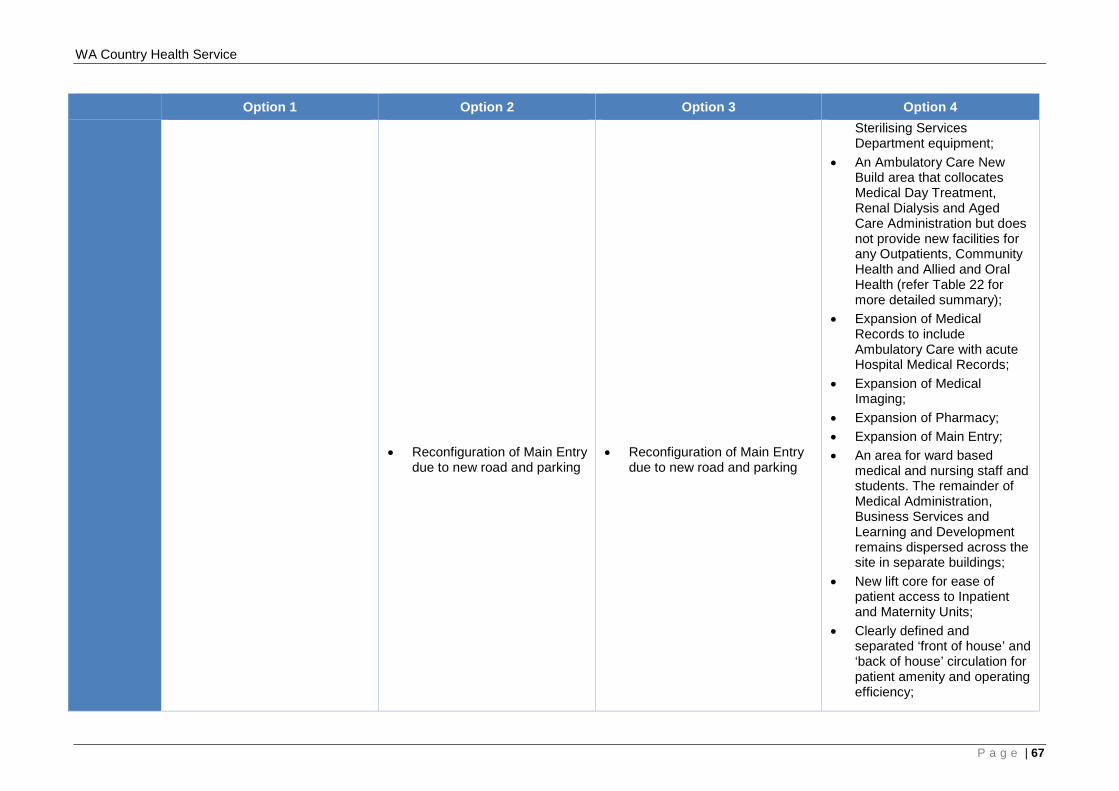
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 • Reconfiguration of Main Entry
due to new road and parking
• Reconfiguration of Main Entry
due to new road and parking
Sterilising Services Department equipment;
• An Ambulatory Care New Build area that collocates Medical Day Treatment, Renal Dialysis and Aged Care Administration but does not provide new facilities for any Outpatients, Community Health and Allied and Oral Health (refer Table 22 for more detailed summary);
• Expansion of Medical Records to include Ambulatory Care with acute Hospital Medical Records;
• Expansion of Medical Imaging;
• Expansion of Pharmacy; • Expansion of Main Entry; • An area for ward based
medical and nursing staff and students. The remainder of Medical Administration, Business Services and Learning and Development remains dispersed across the site in separate buildings;
• New lift core for ease of patient access to Inpatient and Maternity Units;
• Clearly defined and separated ‘front of house’ and ‘back of house’ circulation for patient amenity and operating efficiency;
P a g e | 67
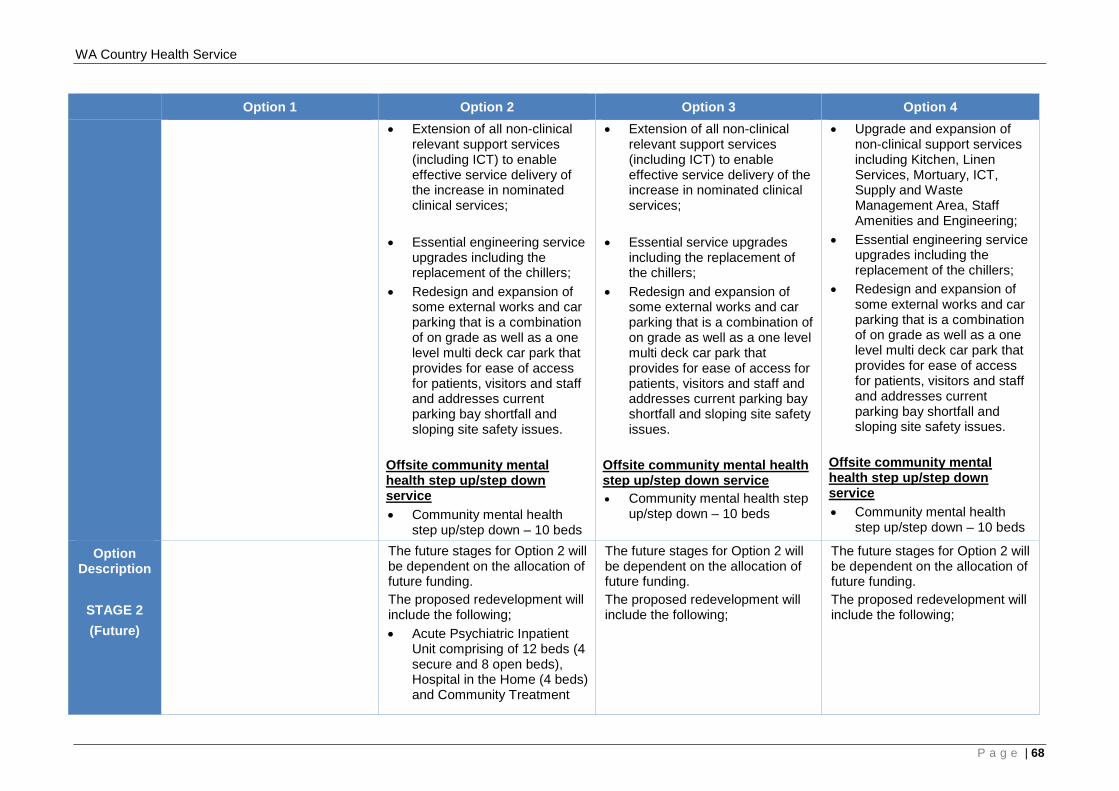
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 • Extension of all non-clinical
relevant support services (including ICT) to enable effective service delivery of the increase in nominated clinical services;
• Essential engineering service
upgrades including the replacement of the chillers;
• Redesign and expansion of some external works and car parking that is a combination of on grade as well as a one level multi deck car park that provides for ease of access for patients, visitors and staff and addresses current parking bay shortfall and sloping site safety issues.
Offsite community mental health step up/step down service • Community mental health
step up/step down – 10 beds
• Extension of all non-clinical relevant support services (including ICT) to enable effective service delivery of the increase in nominated clinical services;
• Essential service upgrades
including the replacement of the chillers;
• Redesign and expansion of some external works and car parking that is a combination of on grade as well as a one level multi deck car park that provides for ease of access for patients, visitors and staff and addresses current parking bay shortfall and sloping site safety issues.
Offsite community mental health step up/step down service • Community mental health step
up/step down – 10 beds
• Upgrade and expansion of non-clinical support services including Kitchen, Linen Services, Mortuary, ICT, Supply and Waste Management Area, Staff Amenities and Engineering;
• Essential engineering service upgrades including the replacement of the chillers;
• Redesign and expansion of some external works and car parking that is a combination of on grade as well as a one level multi deck car park that provides for ease of access for patients, visitors and staff and addresses current parking bay shortfall and sloping site safety issues.
Offsite community mental health step up/step down service • Community mental health
step up/step down – 10 beds
Option Description
STAGE 2 (Future)
The future stages for Option 2 will be dependent on the allocation of future funding. The proposed redevelopment will include the following; • Acute Psychiatric Inpatient
Unit comprising of 12 beds (4 secure and 8 open beds), Hospital in the Home (4 beds) and Community Treatment
The future stages for Option 2 will be dependent on the allocation of future funding. The proposed redevelopment will include the following;
The future stages for Option 2 will be dependent on the allocation of future funding. The proposed redevelopment will include the following;
P a g e | 68
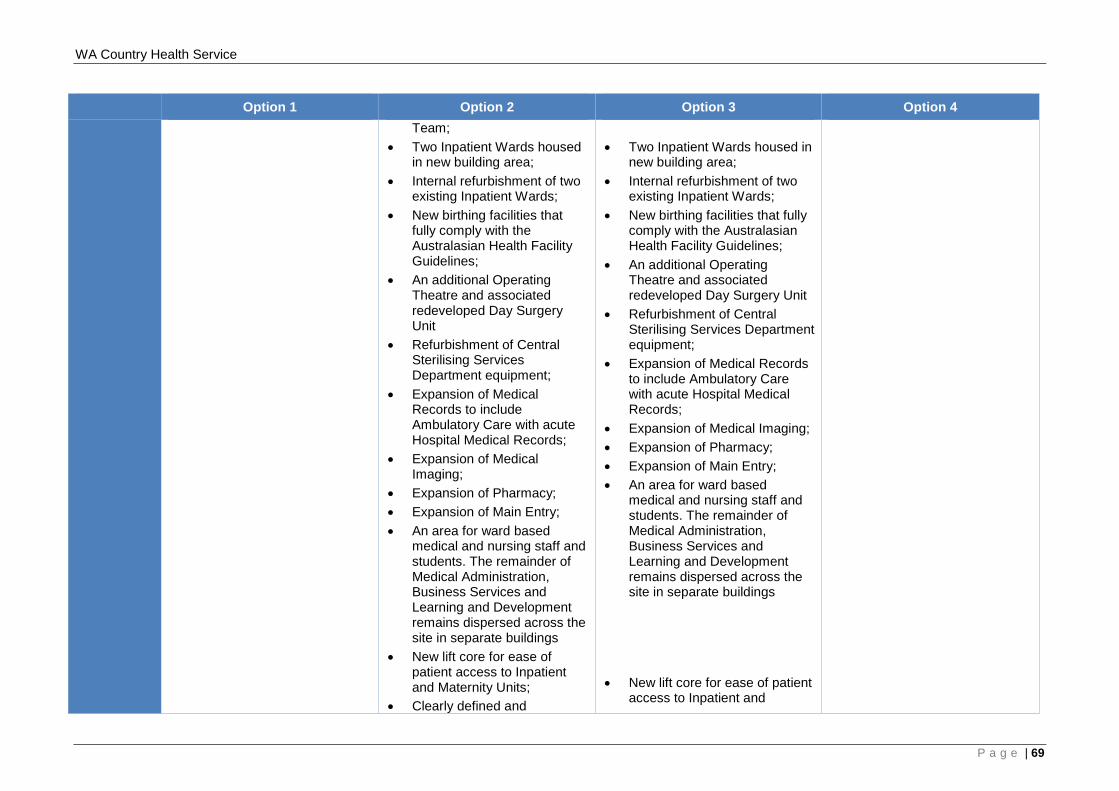
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 Team;
• Two Inpatient Wards housed in new building area;
• Internal refurbishment of two existing Inpatient Wards;
• New birthing facilities that fully comply with the Australasian Health Facility Guidelines;
• An additional Operating Theatre and associated redeveloped Day Surgery Unit
• Refurbishment of Central Sterilising Services Department equipment;
• Expansion of Medical Records to include Ambulatory Care with acute Hospital Medical Records;
• Expansion of Medical Imaging;
• Expansion of Pharmacy; • Expansion of Main Entry; • An area for ward based
medical and nursing staff and students. The remainder of Medical Administration, Business Services and Learning and Development remains dispersed across the site in separate buildings
• New lift core for ease of patient access to Inpatient and Maternity Units;
• Clearly defined and
• Two Inpatient Wards housed in
new building area; • Internal refurbishment of two
existing Inpatient Wards; • New birthing facilities that fully
comply with the Australasian Health Facility Guidelines;
• An additional Operating Theatre and associated redeveloped Day Surgery Unit
• Refurbishment of Central Sterilising Services Department equipment;
• Expansion of Medical Records to include Ambulatory Care with acute Hospital Medical Records;
• Expansion of Medical Imaging; • Expansion of Pharmacy; • Expansion of Main Entry; • An area for ward based
medical and nursing staff and students. The remainder of Medical Administration, Business Services and Learning and Development remains dispersed across the site in separate buildings
• New lift core for ease of patient
access to Inpatient and
P a g e | 69
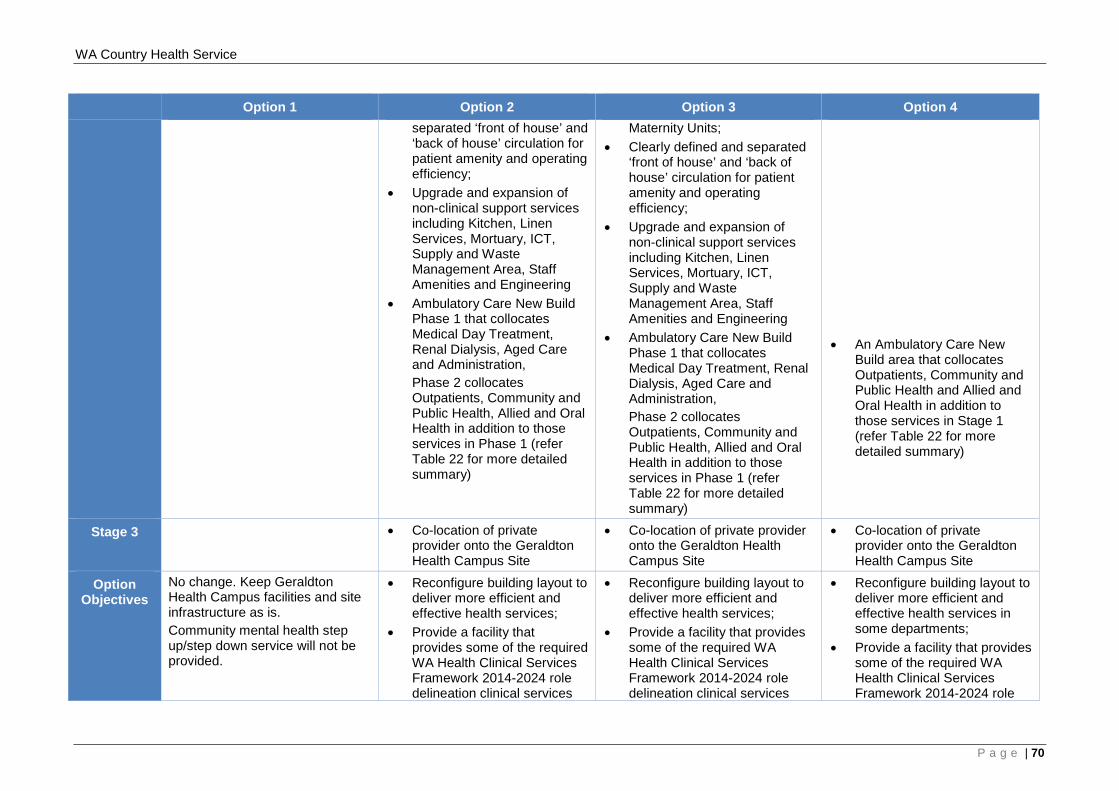
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 separated ‘front of house’ and ‘back of house’ circulation for patient amenity and operating efficiency;
• Upgrade and expansion of non-clinical support services including Kitchen, Linen Services, Mortuary, ICT, Supply and Waste Management Area, Staff Amenities and Engineering
• Ambulatory Care New Build Phase 1 that collocates Medical Day Treatment, Renal Dialysis, Aged Care and Administration, Phase 2 collocates Outpatients, Community and Public Health, Allied and Oral Health in addition to those services in Phase 1 (refer Table 22 for more detailed summary)
Maternity Units; • Clearly defined and separated
‘front of house’ and ‘back of house’ circulation for patient amenity and operating efficiency;
• Upgrade and expansion of non-clinical support services including Kitchen, Linen Services, Mortuary, ICT, Supply and Waste Management Area, Staff Amenities and Engineering
• Ambulatory Care New Build Phase 1 that collocates Medical Day Treatment, Renal Dialysis, Aged Care and Administration, Phase 2 collocates Outpatients, Community and Public Health, Allied and Oral Health in addition to those services in Phase 1 (refer Table 22 for more detailed summary)
• An Ambulatory Care New
Build area that collocates Outpatients, Community and Public Health and Allied and Oral Health in addition to those services in Stage 1 (refer Table 22 for more detailed summary)
Stage 3 • Co-location of private provider onto the Geraldton Health Campus Site
• Co-location of private provider onto the Geraldton Health Campus Site
• Co-location of private provider onto the Geraldton Health Campus Site
Option Objectives
No change. Keep Geraldton Health Campus facilities and site infrastructure as is. Community mental health step up/step down service will not be provided.
• Reconfigure building layout to deliver more efficient and effective health services;
• Provide a facility that provides some of the required WA Health Clinical Services Framework 2014-2024 role delineation clinical services
• Reconfigure building layout to deliver more efficient and effective health services;
• Provide a facility that provides some of the required WA Health Clinical Services Framework 2014-2024 role delineation clinical services
• Reconfigure building layout to deliver more efficient and effective health services in some departments;
• Provide a facility that provides some of the required WA Health Clinical Services Framework 2014-2024 role
P a g e | 70
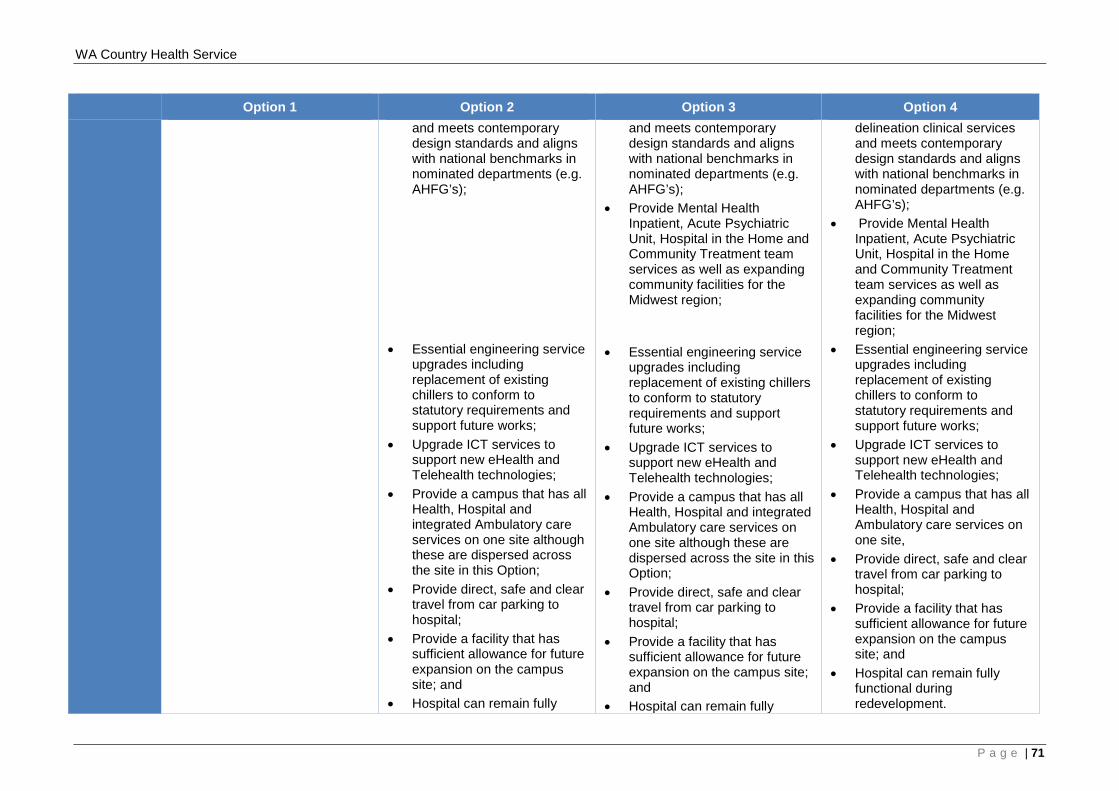
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 and meets contemporary design standards and aligns with national benchmarks in nominated departments (e.g. AHFG’s);
• Essential engineering service
upgrades including replacement of existing chillers to conform to statutory requirements and support future works;
• Upgrade ICT services to support new eHealth and Telehealth technologies;
• Provide a campus that has all Health, Hospital and integrated Ambulatory care services on one site although these are dispersed across the site in this Option;
• Provide direct, safe and clear travel from car parking to hospital;
• Provide a facility that has sufficient allowance for future expansion on the campus site; and
• Hospital can remain fully
and meets contemporary design standards and aligns with national benchmarks in nominated departments (e.g. AHFG’s);
• Provide Mental Health Inpatient, Acute Psychiatric Unit, Hospital in the Home and Community Treatment team services as well as expanding community facilities for the Midwest region;
• Essential engineering service upgrades including replacement of existing chillers to conform to statutory requirements and support future works;
• Upgrade ICT services to support new eHealth and Telehealth technologies;
• Provide a campus that has all Health, Hospital and integrated Ambulatory care services on one site although these are dispersed across the site in this Option;
• Provide direct, safe and clear travel from car parking to hospital;
• Provide a facility that has sufficient allowance for future expansion on the campus site; and
• Hospital can remain fully
delineation clinical services and meets contemporary design standards and aligns with national benchmarks in nominated departments (e.g. AHFG’s);
• Provide Mental Health Inpatient, Acute Psychiatric Unit, Hospital in the Home and Community Treatment team services as well as expanding community facilities for the Midwest region;
• Essential engineering service upgrades including replacement of existing chillers to conform to statutory requirements and support future works;
• Upgrade ICT services to support new eHealth and Telehealth technologies;
• Provide a campus that has all Health, Hospital and Ambulatory care services on one site,
• Provide direct, safe and clear travel from car parking to hospital;
• Provide a facility that has sufficient allowance for future expansion on the campus site; and
• Hospital can remain fully functional during redevelopment.
P a g e | 71
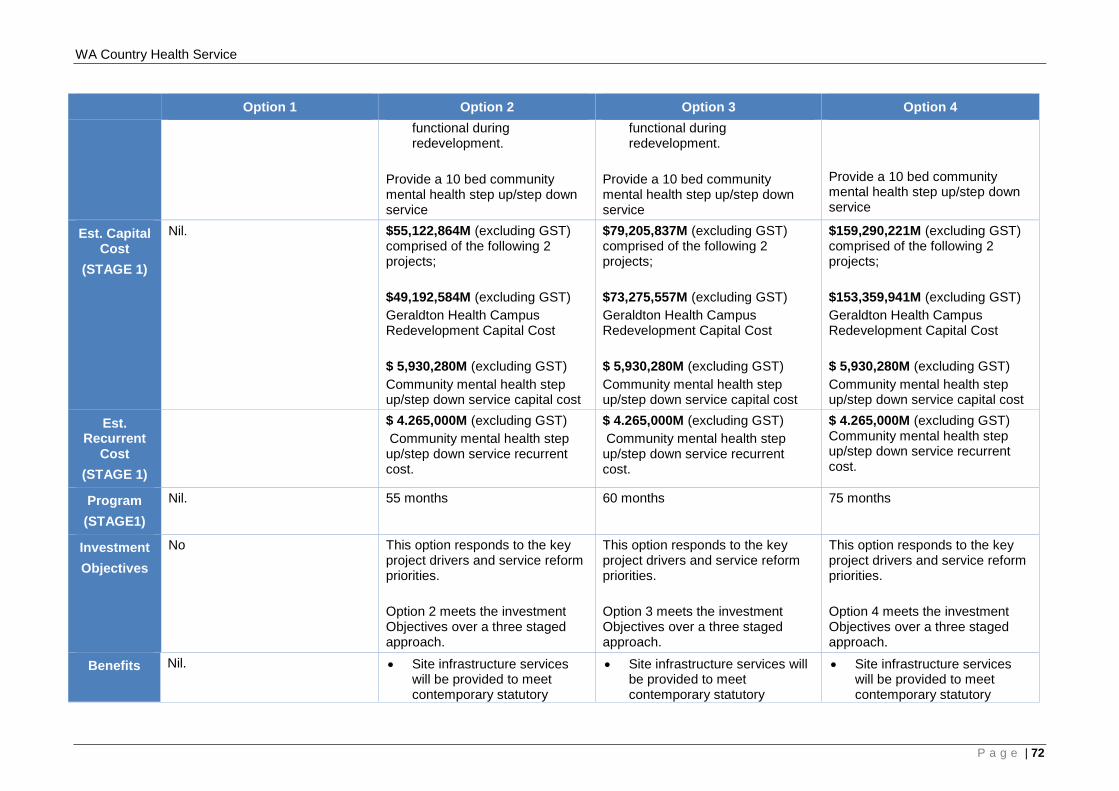
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 functional during redevelopment.
Provide a 10 bed community mental health step up/step down service
functional during redevelopment.
Provide a 10 bed community mental health step up/step down service
Provide a 10 bed community mental health step up/step down service
Est. Capital Cost
(STAGE 1)
Nil. $55,122,864M (excluding GST) comprised of the following 2 projects; $49,192,584M (excluding GST) Geraldton Health Campus Redevelopment Capital Cost $ 5,930,280M (excluding GST) Community mental health step up/step down service capital cost
$79,205,837M (excluding GST) comprised of the following 2 projects; $73,275,557M (excluding GST) Geraldton Health Campus Redevelopment Capital Cost $ 5,930,280M (excluding GST) Community mental health step up/step down service capital cost
$159,290,221M (excluding GST) comprised of the following 2 projects; $153,359,941M (excluding GST) Geraldton Health Campus Redevelopment Capital Cost $ 5,930,280M (excluding GST) Community mental health step up/step down service capital cost
Est. Recurrent
Cost (STAGE 1)
$ 4.265,000M (excluding GST) Community mental health step up/step down service recurrent cost.
$ 4.265,000M (excluding GST) Community mental health step up/step down service recurrent cost.
$ 4.265,000M (excluding GST) Community mental health step up/step down service recurrent cost.
Program (STAGE1)
Nil. 55 months 60 months 75 months
Investment Objectives
No This option responds to the key project drivers and service reform priorities. Option 2 meets the investment Objectives over a three staged approach.
This option responds to the key project drivers and service reform priorities. Option 3 meets the investment Objectives over a three staged approach.
This option responds to the key project drivers and service reform priorities. Option 4 meets the investment Objectives over a three staged approach.
Benefits Nil. • Site infrastructure services will be provided to meet contemporary statutory
• Site infrastructure services will be provided to meet contemporary statutory
• Site infrastructure services will be provided to meet contemporary statutory
P a g e | 72
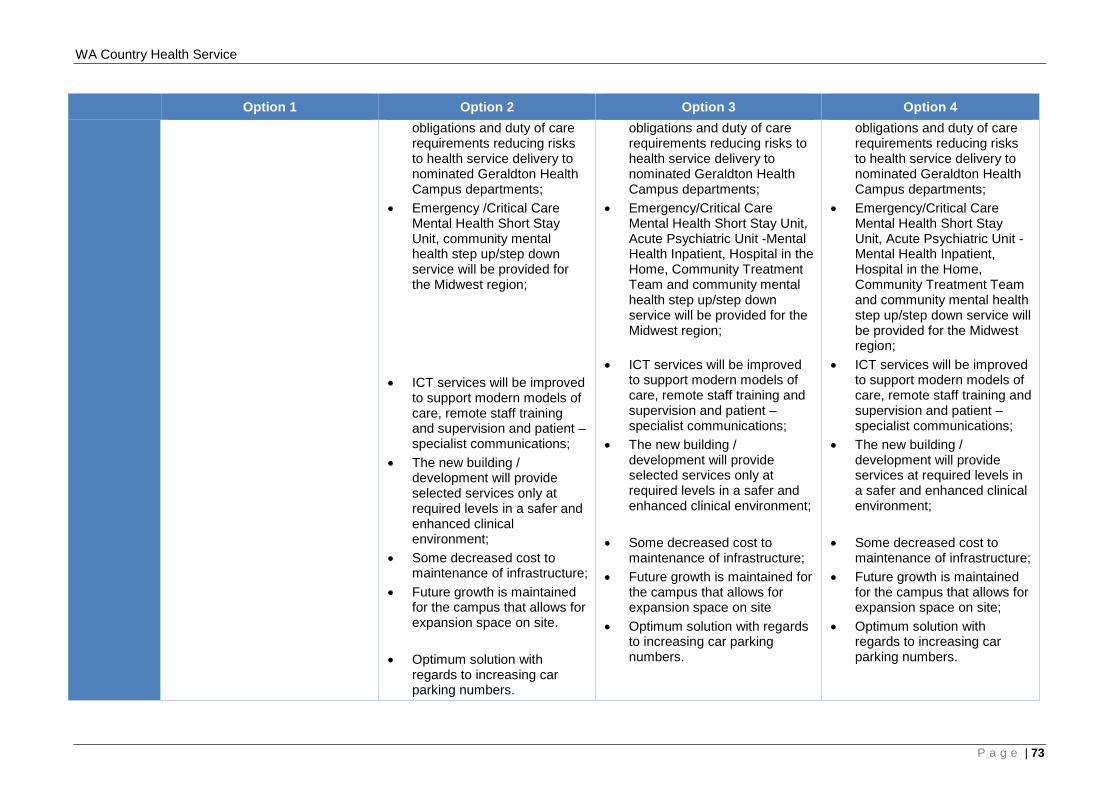
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 obligations and duty of care requirements reducing risks to health service delivery to nominated Geraldton Health Campus departments;
• Emergency /Critical Care Mental Health Short Stay Unit, community mental health step up/step down service will be provided for the Midwest region;
• ICT services will be improved to support modern models of care, remote staff training and supervision and patient – specialist communications;
• The new building / development will provide selected services only at required levels in a safer and enhanced clinical environment;
• Some decreased cost to maintenance of infrastructure;
• Future growth is maintained for the campus that allows for expansion space on site.
• Optimum solution with
regards to increasing car parking numbers.
obligations and duty of care requirements reducing risks to health service delivery to nominated Geraldton Health Campus departments;
• Emergency/Critical Care Mental Health Short Stay Unit, Acute Psychiatric Unit -Mental Health Inpatient, Hospital in the Home, Community Treatment Team and community mental health step up/step down service will be provided for the Midwest region;
• ICT services will be improved to support modern models of care, remote staff training and supervision and patient – specialist communications;
• The new building / development will provide selected services only at required levels in a safer and enhanced clinical environment;
• Some decreased cost to
maintenance of infrastructure; • Future growth is maintained for
the campus that allows for expansion space on site
• Optimum solution with regards to increasing car parking numbers.
obligations and duty of care requirements reducing risks to health service delivery to nominated Geraldton Health Campus departments;
• Emergency/Critical Care Mental Health Short Stay Unit, Acute Psychiatric Unit -Mental Health Inpatient, Hospital in the Home, Community Treatment Team and community mental health step up/step down service will be provided for the Midwest region;
• ICT services will be improved to support modern models of care, remote staff training and supervision and patient – specialist communications;
• The new building / development will provide services at required levels in a safer and enhanced clinical environment;
• Some decreased cost to maintenance of infrastructure;
• Future growth is maintained for the campus that allows for expansion space on site;
• Optimum solution with regards to increasing car parking numbers.
P a g e | 73
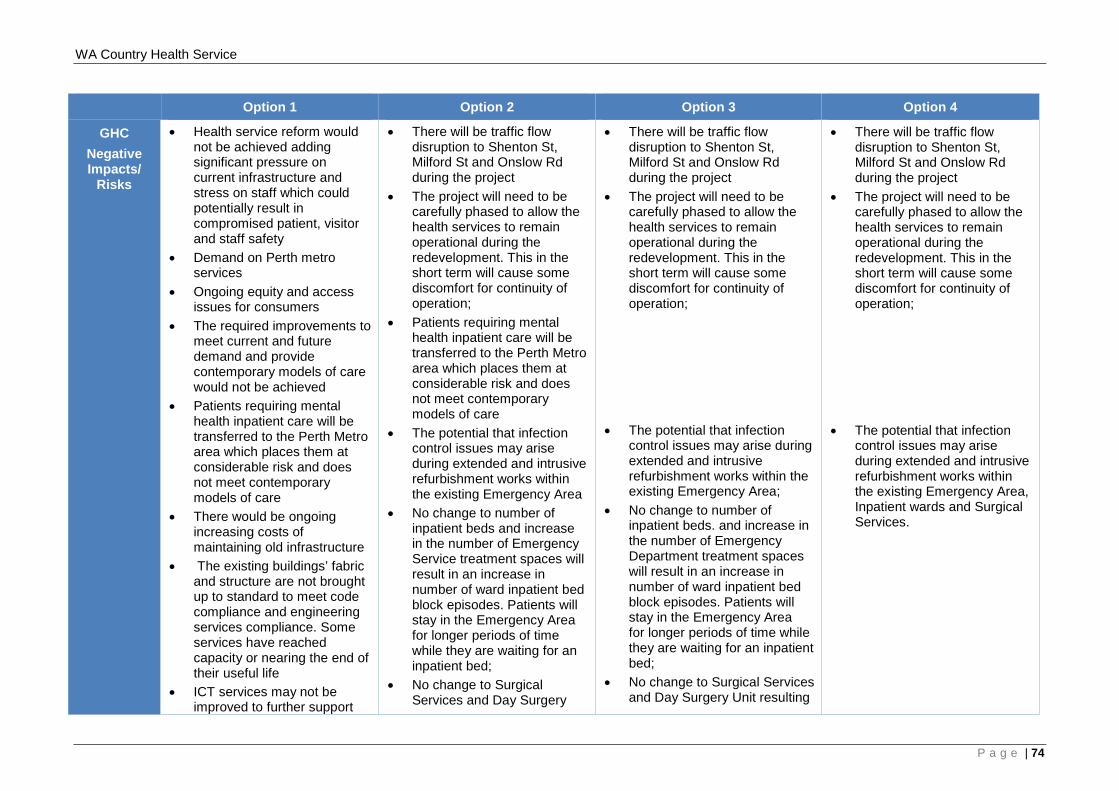
WA Country Health Service
Option 1 Option 2 Option 3 Option 4
GHC Negative Impacts/
Risks
• Health service reform would not be achieved adding significant pressure on current infrastructure and stress on staff which could potentially result in compromised patient, visitor and staff safety
• Demand on Perth metro services
• Ongoing equity and access issues for consumers
• The required improvements to meet current and future demand and provide contemporary models of care would not be achieved
• Patients requiring mental health inpatient care will be transferred to the Perth Metro area which places them at considerable risk and does not meet contemporary models of care
• There would be ongoing increasing costs of maintaining old infrastructure
• The existing buildings’ fabric and structure are not brought up to standard to meet code compliance and engineering services compliance. Some services have reached capacity or nearing the end of their useful life
• ICT services may not be improved to further support
• There will be traffic flow disruption to Shenton St, Milford St and Onslow Rd during the project
• The project will need to be carefully phased to allow the health services to remain operational during the redevelopment. This in the short term will cause some discomfort for continuity of operation;
• Patients requiring mental health inpatient care will be transferred to the Perth Metro area which places them at considerable risk and does not meet contemporary models of care
• The potential that infection control issues may arise during extended and intrusive refurbishment works within the existing Emergency Area
• No change to number of inpatient beds and increase in the number of Emergency Service treatment spaces will result in an increase in number of ward inpatient bed block episodes. Patients will stay in the Emergency Area for longer periods of time while they are waiting for an inpatient bed;
• No change to Surgical Services and Day Surgery
• There will be traffic flow disruption to Shenton St, Milford St and Onslow Rd during the project
• The project will need to be carefully phased to allow the health services to remain operational during the redevelopment. This in the short term will cause some discomfort for continuity of operation;
• The potential that infection
control issues may arise during extended and intrusive refurbishment works within the existing Emergency Area;
• No change to number of inpatient beds. and increase in the number of Emergency Department treatment spaces will result in an increase in number of ward inpatient bed block episodes. Patients will stay in the Emergency Area for longer periods of time while they are waiting for an inpatient bed;
• No change to Surgical Services and Day Surgery Unit resulting
• There will be traffic flow disruption to Shenton St, Milford St and Onslow Rd during the project
• The project will need to be carefully phased to allow the health services to remain operational during the redevelopment. This in the short term will cause some discomfort for continuity of operation;
• The potential that infection
control issues may arise during extended and intrusive refurbishment works within the existing Emergency Area, Inpatient wards and Surgical Services.
P a g e | 74
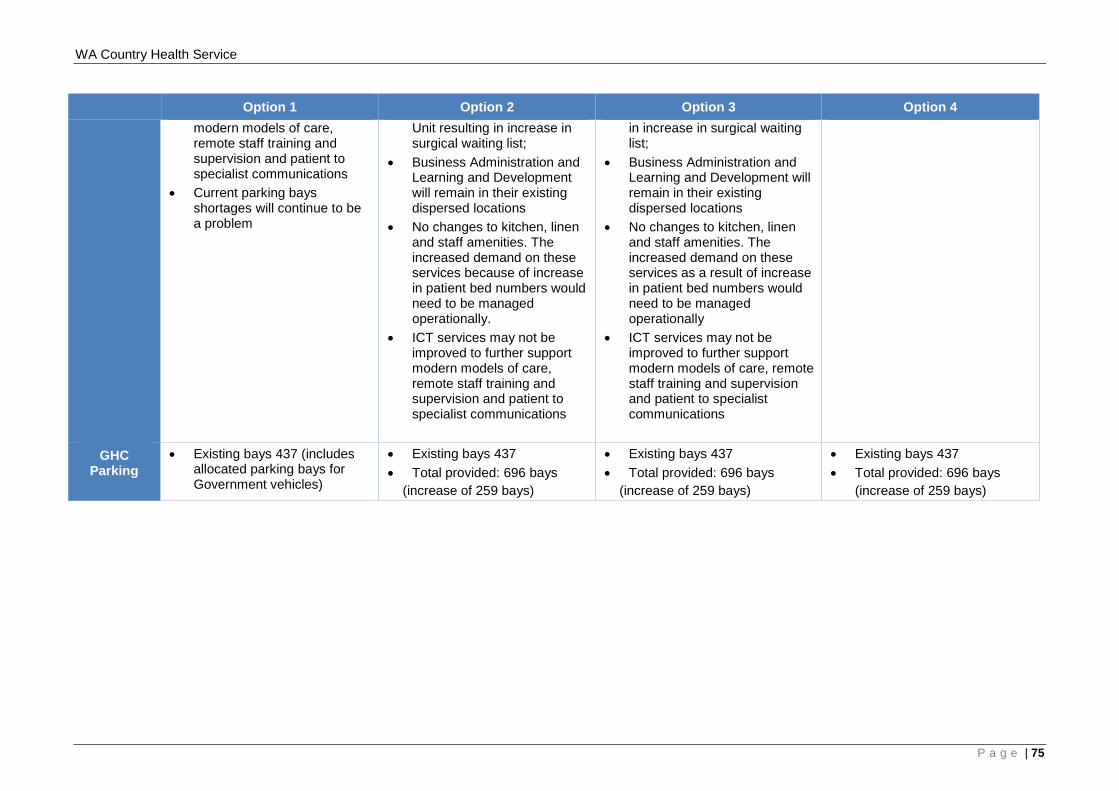
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 modern models of care, remote staff training and supervision and patient to specialist communications
• Current parking bays shortages will continue to be a problem
Unit resulting in increase in surgical waiting list;
• Business Administration and Learning and Development will remain in their existing dispersed locations
• No changes to kitchen, linen and staff amenities. The increased demand on these services because of increase in patient bed numbers would need to be managed operationally.
• ICT services may not be improved to further support modern models of care, remote staff training and supervision and patient to specialist communications
in increase in surgical waiting list;
• Business Administration and Learning and Development will remain in their existing dispersed locations
• No changes to kitchen, linen and staff amenities. The increased demand on these services as a result of increase in patient bed numbers would need to be managed operationally
• ICT services may not be improved to further support modern models of care, remote staff training and supervision and patient to specialist communications
GHC Parking
• Existing bays 437 (includes allocated parking bays for Government vehicles)
• Existing bays 437 • Total provided: 696 bays
(increase of 259 bays)
• Existing bays 437 • Total provided: 696 bays
(increase of 259 bays)
• Existing bays 437 • Total provided: 696 bays
(increase of 259 bays)
P a g e | 75
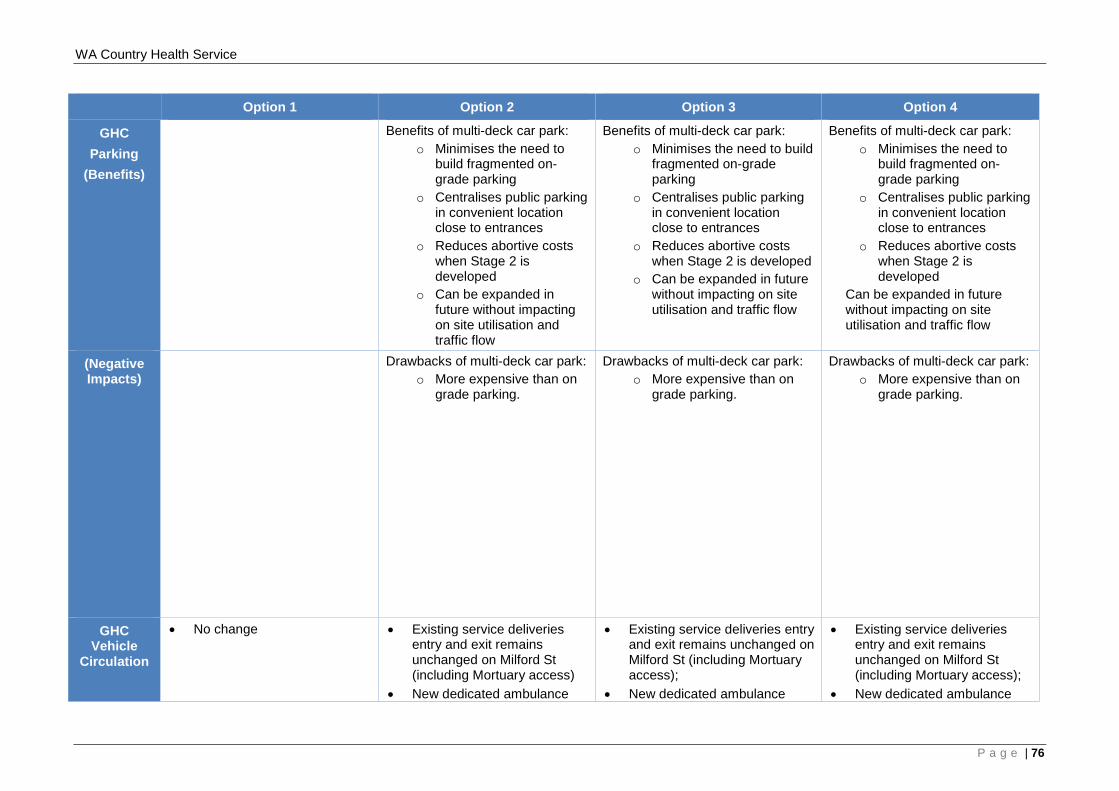
WA Country Health Service
Option 1 Option 2 Option 3 Option 4
GHC Parking
(Benefits)
Benefits of multi-deck car park: o Minimises the need to
build fragmented on-grade parking
o Centralises public parking in convenient location close to entrances
o Reduces abortive costs when Stage 2 is developed
o Can be expanded in future without impacting on site utilisation and traffic flow
Benefits of multi-deck car park: o Minimises the need to build
fragmented on-grade parking
o Centralises public parking in convenient location close to entrances
o Reduces abortive costs when Stage 2 is developed
o Can be expanded in future without impacting on site utilisation and traffic flow
Benefits of multi-deck car park: o Minimises the need to
build fragmented on-grade parking
o Centralises public parking in convenient location close to entrances
o Reduces abortive costs when Stage 2 is developed
Can be expanded in future without impacting on site utilisation and traffic flow
(Negative Impacts)
Drawbacks of multi-deck car park: o More expensive than on
grade parking.
Drawbacks of multi-deck car park: o More expensive than on
grade parking.
Drawbacks of multi-deck car park: o More expensive than on
grade parking.
GHC Vehicle
Circulation
• No change • Existing service deliveries entry and exit remains unchanged on Milford St (including Mortuary access)
• New dedicated ambulance
• Existing service deliveries entry and exit remains unchanged on Milford St (including Mortuary access);
• New dedicated ambulance
• Existing service deliveries entry and exit remains unchanged on Milford St (including Mortuary access);
• New dedicated ambulance
P a g e | 76
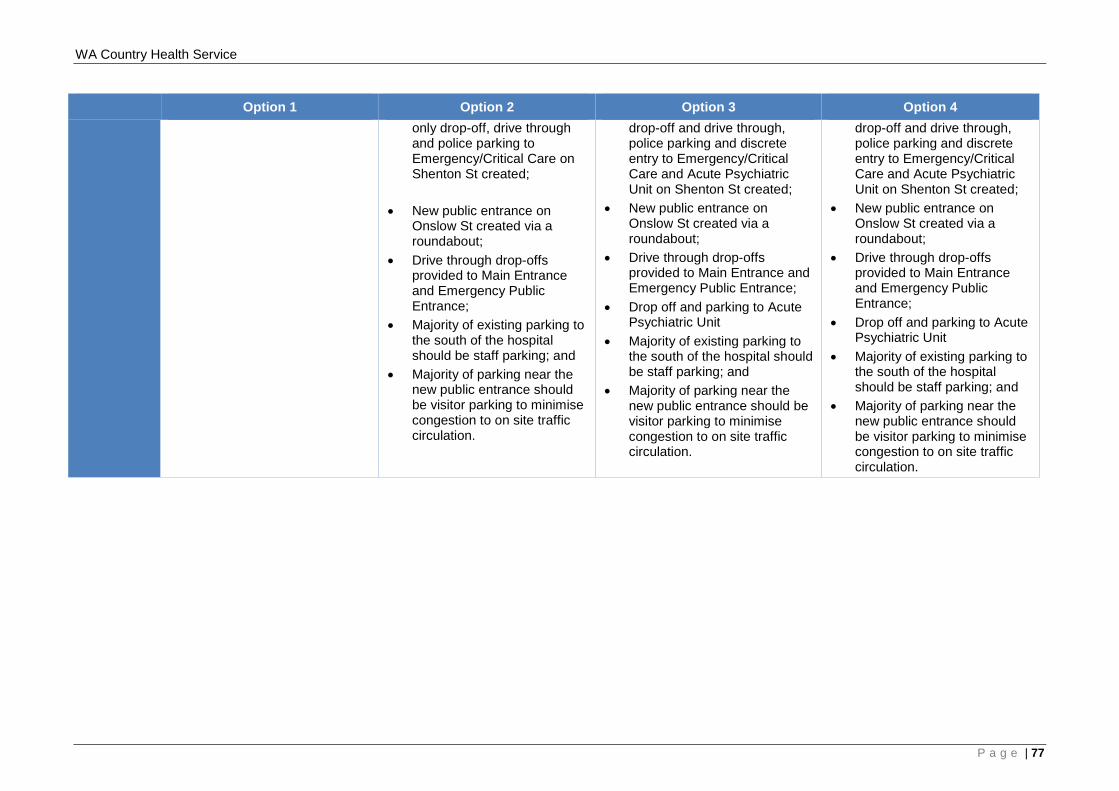
WA Country Health Service
Option 1 Option 2 Option 3 Option 4 only drop-off, drive through and police parking to Emergency/Critical Care on Shenton St created;
• New public entrance on Onslow St created via a roundabout;
• Drive through drop-offs provided to Main Entrance and Emergency Public Entrance;
• Majority of existing parking to the south of the hospital should be staff parking; and
• Majority of parking near the new public entrance should be visitor parking to minimise congestion to on site traffic circulation.
drop-off and drive through, police parking and discrete entry to Emergency/Critical Care and Acute Psychiatric Unit on Shenton St created;
• New public entrance on Onslow St created via a roundabout;
• Drive through drop-offs provided to Main Entrance and Emergency Public Entrance;
• Drop off and parking to Acute Psychiatric Unit
• Majority of existing parking to the south of the hospital should be staff parking; and
• Majority of parking near the new public entrance should be visitor parking to minimise congestion to on site traffic circulation.
drop-off and drive through, police parking and discrete entry to Emergency/Critical Care and Acute Psychiatric Unit on Shenton St created;
• New public entrance on Onslow St created via a roundabout;
• Drive through drop-offs provided to Main Entrance and Emergency Public Entrance;
• Drop off and parking to Acute Psychiatric Unit
• Majority of existing parking to the south of the hospital should be staff parking; and
• Majority of parking near the new public entrance should be visitor parking to minimise congestion to on site traffic circulation.
P a g e | 77
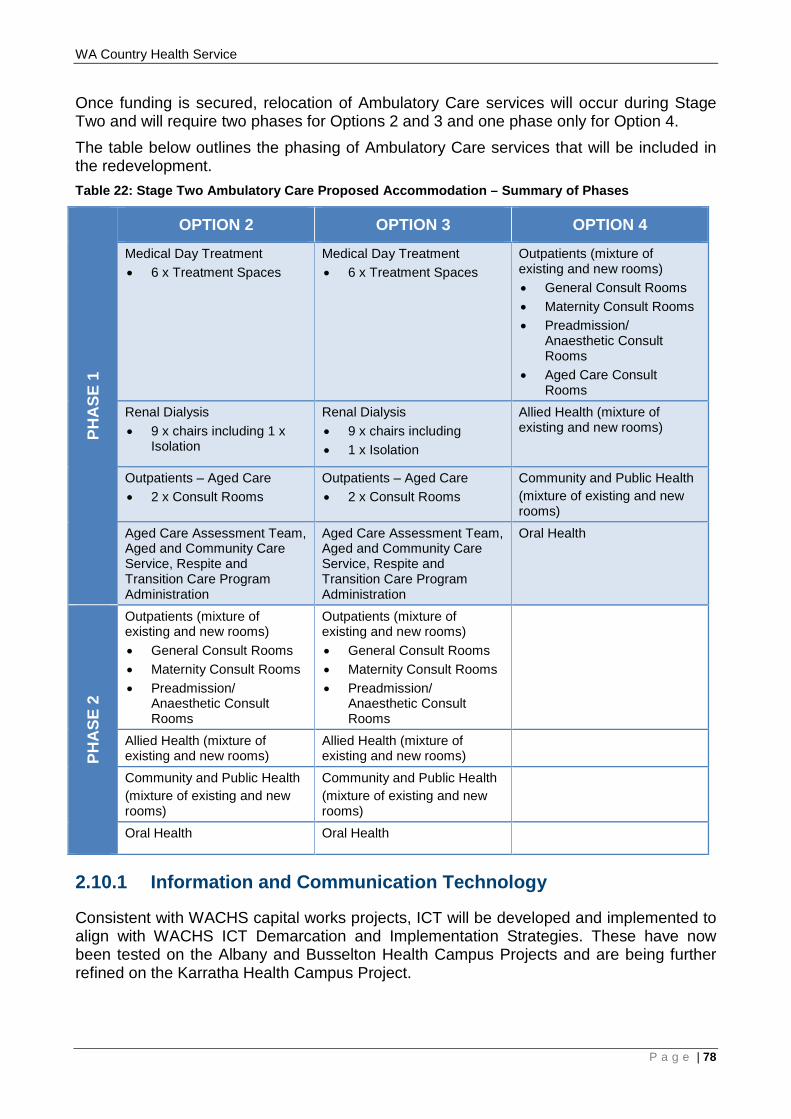
WA Country Health Service
Once funding is secured, relocation of Ambulatory Care services will occur during Stage Two and will require two phases for Options 2 and 3 and one phase only for Option 4. The table below outlines the phasing of Ambulatory Care services that will be included in the redevelopment. Table 22: Stage Two Ambulatory Care Proposed Accommodation – Summary of Phases
PHA
SE 1
OPTION 2 OPTION 3 OPTION 4
Medical Day Treatment • 6 x Treatment Spaces
Medical Day Treatment • 6 x Treatment Spaces
Outpatients (mixture of existing and new rooms) • General Consult Rooms • Maternity Consult Rooms • Preadmission/
Anaesthetic Consult Rooms
• Aged Care Consult Rooms
Renal Dialysis • 9 x chairs including 1 x
Isolation
Renal Dialysis • 9 x chairs including • 1 x Isolation
Allied Health (mixture of existing and new rooms)
Outpatients – Aged Care • 2 x Consult Rooms
Outpatients – Aged Care • 2 x Consult Rooms
Community and Public Health (mixture of existing and new rooms)
Aged Care Assessment Team, Aged and Community Care Service, Respite and Transition Care Program Administration
Aged Care Assessment Team, Aged and Community Care Service, Respite and Transition Care Program Administration
Oral Health
PHA
SE 2
Outpatients (mixture of existing and new rooms) • General Consult Rooms • Maternity Consult Rooms • Preadmission/
Anaesthetic Consult Rooms
Outpatients (mixture of existing and new rooms) • General Consult Rooms • Maternity Consult Rooms • Preadmission/
Anaesthetic Consult Rooms
Allied Health (mixture of existing and new rooms)
Allied Health (mixture of existing and new rooms)
Community and Public Health (mixture of existing and new rooms)
Community and Public Health (mixture of existing and new rooms)
Oral Health Oral Health
2.10.1 Information and Communication Technology
Consistent with WACHS capital works projects, ICT will be developed and implemented to align with WACHS ICT Demarcation and Implementation Strategies. These have now been tested on the Albany and Busselton Health Campus Projects and are being further refined on the Karratha Health Campus Project.
P a g e | 78
WA Country Health Service
2.10.2 Evaluation of Options
Option 3 is the recommended option as it fulfills the overarching vision for the GHC redevelopment through a staged approach meeting the investment objectives and service reform priorities as highlighted in the WA Health Clinical Services Framework 2014 – 2024, Western Australian, Mental Health Alcohol and Other Drug Services Plan 2015 – 2025, Geraldton Health Campus WACHS Midwest Service Plan 2010-2020, Midwest Regional Blueprint 2015 and the Midwest Integrated Mental Health Service, - Service Model 2015 and it delivers core GHC clinical services and essential associated clinical and non-clinical support services and step up/step down for $79,205,837 million. The main differences between Option 3 Stage One and the other two options is that it delivers all mental health services and focuses on delivering acute emergency/critical care as well as providing step up/step down services. It is considered that these differences do not:
• prevent health services delivery, for the Geraldton and Midwest region communities, from a contemporary health facility;
• prevent reduction of the risks to service delivery; • prevent improvement to operational efficiency at Geraldton Health Campus; • hamper improvement of patient and staff amenity; and • prevent the hospital remaining fully functional during project delivery.
As demonstrated in Table 21 the option objectives are achieved for all three options. Option 3 presents value for money, noting that this option has been master-planned so that it can accommodate growth in the future.
2.11 Funding Strategy
2.11.1 Total Budget
The capital cost estimate for Option 3 Stage 1 is $79,205,837 million (excluding GST). The table below outlines the project budget details.
P a g e | 79
WA Country Health Service
Item / Deliverable Option 2 Stage 1 Option 3 Stage 1 Option 4 Stage 1
The cost estimates include the following:
• Appropriate cost allowances for site related engineering services and infrastructure in response to limited reporting on the current site and engineering services capacity;
• Suitable design and construction contingencies for unforeseen circumstances; • Regional location allowance of 5% due to the location, value and nature of work.
P a g e | 80
WA Country Health Service
2.11.2 Funding Amount
In order to provide Stage One of the GHC redevelopment and the step up/step down service, $79.206 million worth of funding is sought from the WA State Government. The anticipated cash flow for each option is presented in the table below.
P a g e | 81
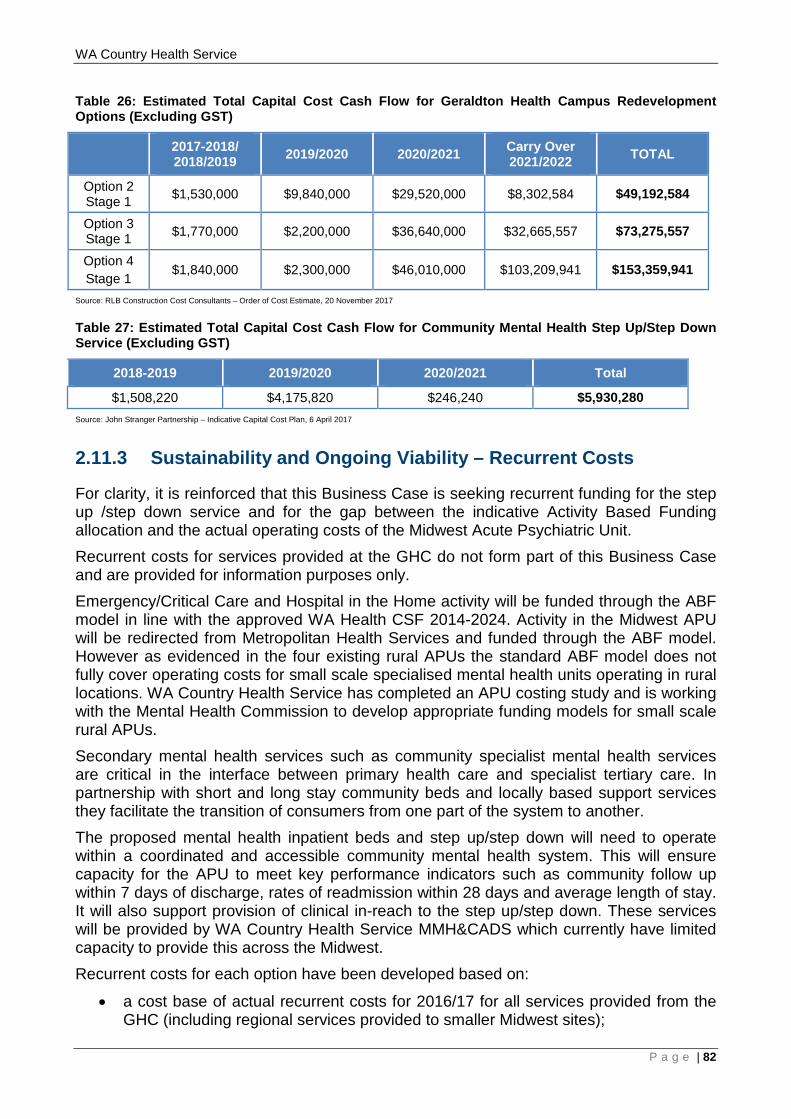
WA Country Health Service
Table 26: Estimated Total Capital Cost Cash Flow for Geraldton Health Campus Redevelopment Options (Excluding GST)
2017-2018/ 2018/2019 2019/2020 2020/2021 Carry Over
2021/2022 TOTAL
Option 2 Stage 1 $1,530,000 $9,840,000 $29,520,000 $8,302,584 $49,192,584
Option 3 Stage 1 $1,770,000 $2,200,000 $36,640,000 $32,665,557 $73,275,557
Option 4 Stage 1
$1,840,000 $2,300,000 $46,010,000 $103,209,941 $153,359,941
Source: RLB Construction Cost Consultants – Order of Cost Estimate, 20 November 2017
Table 27: Estimated Total Capital Cost Cash Flow for Community Mental Health Step Up/Step Down Service (Excluding GST)
2018-2019 2019/2020 2020/2021 Total
$1,508,220 $4,175,820 $246,240 $5,930,280 Source: John Stranger Partnership – Indicative Capital Cost Plan, 6 April 2017
2.11.3 Sustainability and Ongoing Viability – Recurrent Costs
For clarity, it is reinforced that this Business Case is seeking recurrent funding for the step up /step down service and for the gap between the indicative Activity Based Funding allocation and the actual operating costs of the Midwest Acute Psychiatric Unit. Recurrent costs for services provided at the GHC do not form part of this Business Case and are provided for information purposes only. Emergency/Critical Care and Hospital in the Home activity will be funded through the ABF model in line with the approved WA Health CSF 2014-2024. Activity in the Midwest APU will be redirected from Metropolitan Health Services and funded through the ABF model. However as evidenced in the four existing rural APUs the standard ABF model does not fully cover operating costs for small scale specialised mental health units operating in rural locations. WA Country Health Service has completed an APU costing study and is working with the Mental Health Commission to develop appropriate funding models for small scale rural APUs. Secondary mental health services such as community specialist mental health services are critical in the interface between primary health care and specialist tertiary care. In partnership with short and long stay community beds and locally based support services they facilitate the transition of consumers from one part of the system to another. The proposed mental health inpatient beds and step up/step down will need to operate within a coordinated and accessible community mental health system. This will ensure capacity for the APU to meet key performance indicators such as community follow up within 7 days of discharge, rates of readmission within 28 days and average length of stay. It will also support provision of clinical in-reach to the step up/step down. These services will be provided by WA Country Health Service MMH&CADS which currently have limited capacity to provide this across the Midwest. Recurrent costs for each option have been developed based on:
• a cost base of actual recurrent costs for 2016/17 for all services provided from the GHC (including regional services provided to smaller Midwest sites);
P a g e | 82
WA Country Health Service
• the latest clinical activity modelling, aligned with the WA Health CSF 2014-2024; • activity growth caps consistent with the quantity of bed and treatment places under
each option; • adjustment of the cost base to account for differences in facilities costs
(maintenance, utilities etc) relating to the size and nature of the facility under each option;
• cost escalation consistent with the latest cost escalators produced by Health Finance, consistent with the Whole of Health Cost Model; and
• offsite services are assumed to be available and accessible to manage activity volumes beyond current and forecast capacity at the GHC.
It is important to note that the recurrent cost projections developed do not only include the Inpatient, Emergency/Critical Care and Outpatient services performed at the GHC, but include other services based out of the Health Campus including:
1. Aged Care; 2. Community Mental Health; 3. Population Health; and 4. Regional Services.
Details of the recurrent cost profile of the CMDP options proposed for the GHC site are as follows:
• Option 1 (‘do nothing’) has been included in the analysis as a baseline comparator and utilises unreformed 2016/17 GHC recurrent costs as a cost base;
• Option 2 (‘WACHS-Midwest’) utilises the same cost base as the ‘Do Nothing’ option, driven by activity growth applied to expanded Emergency/Critical Care and Mental Health capacity. Facilities cost adjustments were based on the increased floor space of the partial new build and facilities upgrade, with allowance for efficiency from economies of scale and modern design/technology;
• Option 3 (‘Election Commitment’) utilises the same cost base as the ‘Do Nothing’ option, driven by activity growth applied to expanded Emergency/Critical Care and Mental Health capacity. Facilities cost adjustments were based on the increased floor space of the partial new build and facilities upgrade, with allowance for efficiency from economies of scale and modern design/technology;
• Option 4 (‘Previous Business Case’) utilises the same cost base as the ‘Do Nothing’ option, driven by activity growth applied to expanded Inpatient, Emergency/Critical Care, Outpatient and Mental Health capacity. Facilities cost adjustments were based on the increased floor space of the partial new build and facilities upgrade, with allowance for efficiency from economies of scale and modern design/technology.
2.11.3.1 Recurrent Costs - Geraldton Health Campus The following table compares the recurrent costs for each of the GHC CMDP options for the first year in which the above comparative recurrent cost impacts are anticipated to occur across all shortlisted options for the entire financial period (2023/24). The table highlights that the greatest recurrent costs are expected in the option with the greatest expansion of service capacity, as this option is able to service the growth in activity expected for the catchment. Although there is an expected increase in recurrent costs consistent with capacity expansion, this is confined to GHC, and excess demand is serviced by offsite providers or left unmet, which may result in poorer cost and service outcomes overall.
P a g e | 83

WA Country Health Service
P a g e | 84
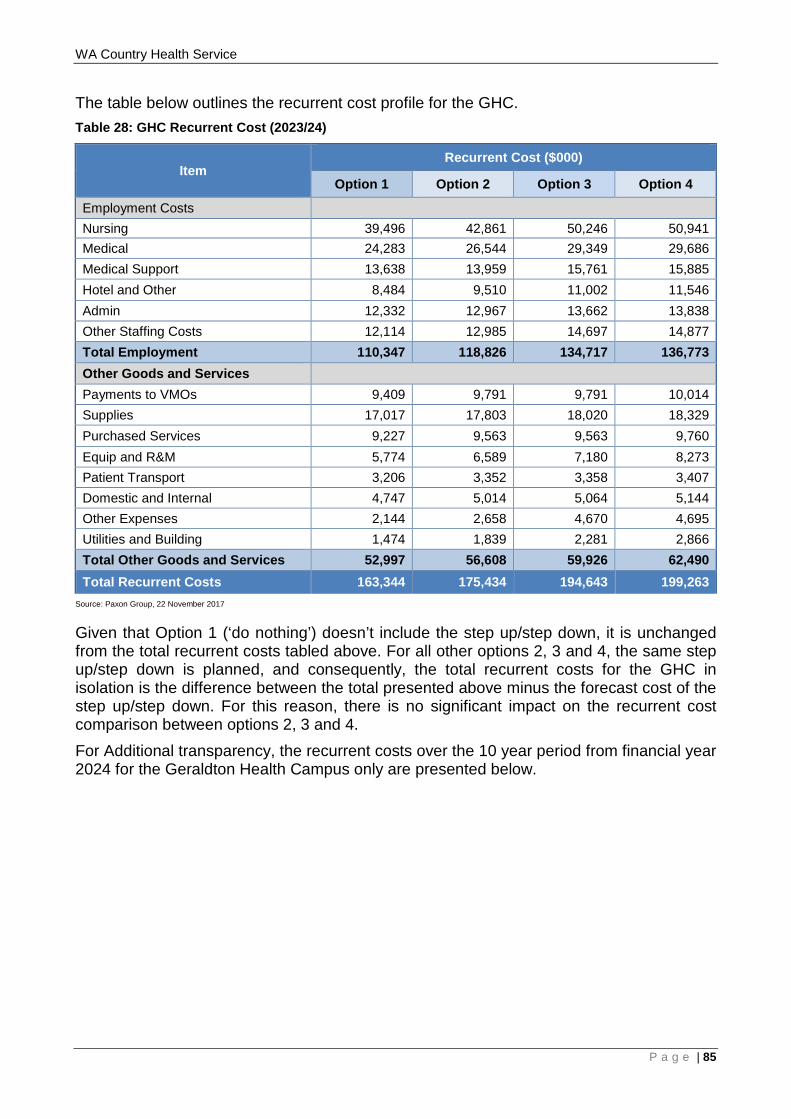
WA Country Health Service
The table below outlines the recurrent cost profile for the GHC. Table 28: GHC Recurrent Cost (2023/24)
Item Recurrent Cost ($000)
Option 1 Option 2 Option 3 Option 4
Employment Costs Nursing 39,496 42,861 50,246 50,941 Medical 24,283 26,544 29,349 29,686 Medical Support 13,638 13,959 15,761 15,885 Hotel and Other 8,484 9,510 11,002 11,546 Admin 12,332 12,967 13,662 13,838 Other Staffing Costs 12,114 12,985 14,697 14,877 Total Employment 110,347 118,826 134,717 136,773 Other Goods and Services Payments to VMOs 9,409 9,791 9,791 10,014 Supplies 17,017 17,803 18,020 18,329 Purchased Services 9,227 9,563 9,563 9,760 Equip and R&M 5,774 6,589 7,180 8,273 Patient Transport 3,206 3,352 3,358 3,407 Domestic and Internal 4,747 5,014 5,064 5,144 Other Expenses 2,144 2,658 4,670 4,695 Utilities and Building 1,474 1,839 2,281 2,866 Total Other Goods and Services 52,997 56,608 59,926 62,490 Total Recurrent Costs 163,344 175,434 194,643 199,263
Source: Paxon Group, 22 November 2017
Given that Option 1 (‘do nothing’) doesn’t include the step up/step down, it is unchanged from the total recurrent costs tabled above. For all other options 2, 3 and 4, the same step up/step down is planned, and consequently, the total recurrent costs for the GHC in isolation is the difference between the total presented above minus the forecast cost of the step up/step down. For this reason, there is no significant impact on the recurrent cost comparison between options 2, 3 and 4. For Additional transparency, the recurrent costs over the 10 year period from financial year 2024 for the Geraldton Health Campus only are presented below.
P a g e | 85
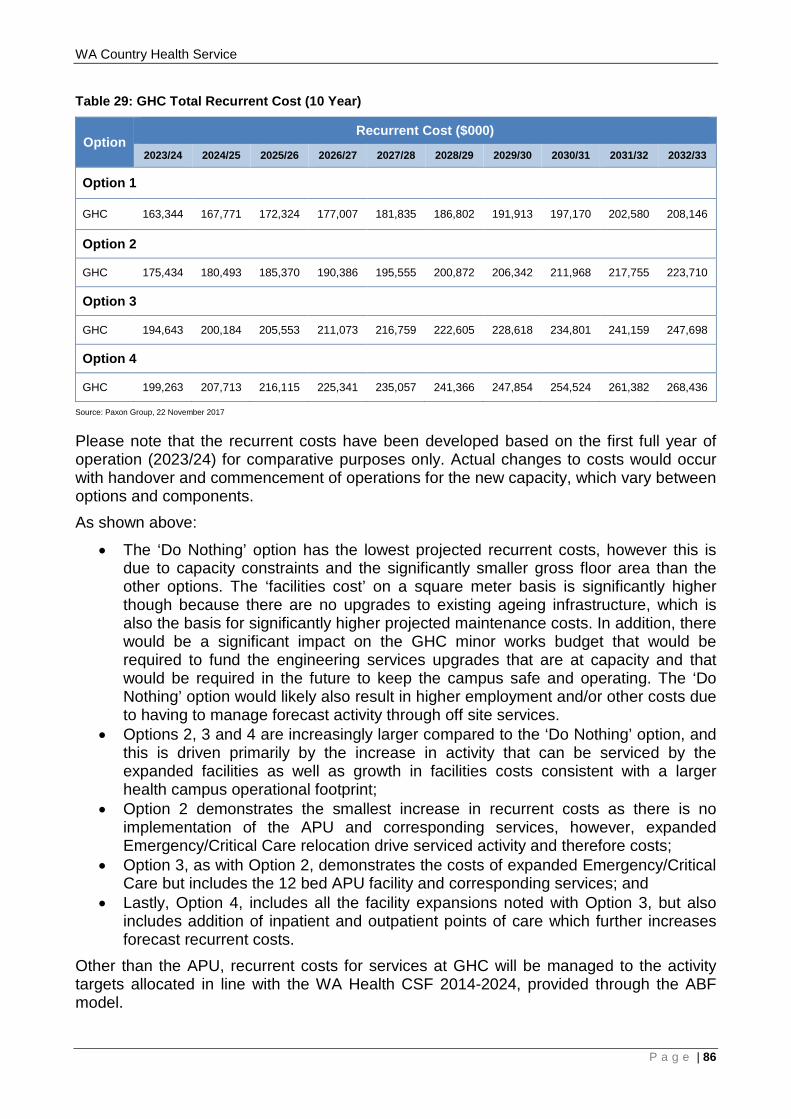
WA Country Health Service
Table 29: GHC Total Recurrent Cost (10 Year)
Option Recurrent Cost ($000)
2023/24 2024/25 2025/26 2026/27 2027/28 2028/29 2029/30 2030/31 2031/32 2032/33
Option 1
GHC 163,344 167,771 172,324 177,007 181,835 186,802 191,913 197,170 202,580 208,146
Option 2
GHC 175,434 180,493 185,370 190,386 195,555 200,872 206,342 211,968 217,755 223,710
Option 3
GHC 194,643 200,184 205,553 211,073 216,759 222,605 228,618 234,801 241,159 247,698
Option 4
GHC 199,263 207,713 216,115 225,341 235,057 241,366 247,854 254,524 261,382 268,436
Source: Paxon Group, 22 November 2017
Please note that the recurrent costs have been developed based on the first full year of operation (2023/24) for comparative purposes only. Actual changes to costs would occur with handover and commencement of operations for the new capacity, which vary between options and components. As shown above:
• The ‘Do Nothing’ option has the lowest projected recurrent costs, however this is due to capacity constraints and the significantly smaller gross floor area than the other options. The ‘facilities cost’ on a square meter basis is significantly higher though because there are no upgrades to existing ageing infrastructure, which is also the basis for significantly higher projected maintenance costs. In addition, there would be a significant impact on the GHC minor works budget that would be required to fund the engineering services upgrades that are at capacity and that would be required in the future to keep the campus safe and operating. The ‘Do Nothing’ option would likely also result in higher employment and/or other costs due to having to manage forecast activity through off site services.
• Options 2, 3 and 4 are increasingly larger compared to the ‘Do Nothing’ option, and this is driven primarily by the increase in activity that can be serviced by the expanded facilities as well as growth in facilities costs consistent with a larger health campus operational footprint;
• Option 2 demonstrates the smallest increase in recurrent costs as there is no implementation of the APU and corresponding services, however, expanded Emergency/Critical Care relocation drive serviced activity and therefore costs;
• Option 3, as with Option 2, demonstrates the costs of expanded Emergency/Critical Care but includes the 12 bed APU facility and corresponding services; and
• Lastly, Option 4, includes all the facility expansions noted with Option 3, but also includes addition of inpatient and outpatient points of care which further increases forecast recurrent costs.
Other than the APU, recurrent costs for services at GHC will be managed to the activity targets allocated in line with the WA Health CSF 2014-2024, provided through the ABF model.
P a g e | 86
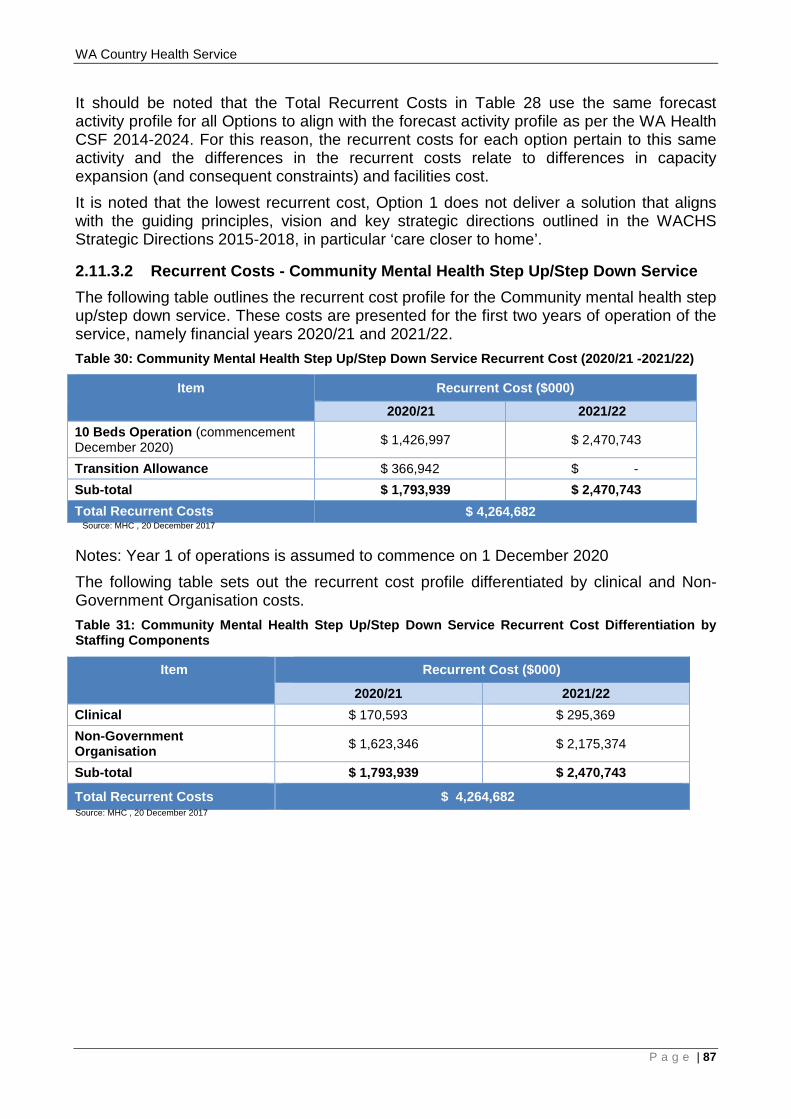
WA Country Health Service
It should be noted that the Total Recurrent Costs in Table 28 use the same forecast activity profile for all Options to align with the forecast activity profile as per the WA Health CSF 2014-2024. For this reason, the recurrent costs for each option pertain to this same activity and the differences in the recurrent costs relate to differences in capacity expansion (and consequent constraints) and facilities cost. It is noted that the lowest recurrent cost, Option 1 does not deliver a solution that aligns with the guiding principles, vision and key strategic directions outlined in the WACHS Strategic Directions 2015-2018, in particular ‘care closer to home’.
2.11.3.2 Recurrent Costs - Community Mental Health Step Up/Step Down Service The following table outlines the recurrent cost profile for the Community mental health step up/step down service. These costs are presented for the first two years of operation of the service, namely financial years 2020/21 and 2021/22. Table 30: Community Mental Health Step Up/Step Down Service Recurrent Cost (2020/21 -2021/22)
Item Recurrent Cost ($000)
2020/21 2021/22 10 Beds Operation (commencement December 2020) $ 1,426,997 $ 2,470,743
Transition Allowance $ 366,942 $ - Sub-total $ 1,793,939 $ 2,470,743 Total Recurrent Costs $ 4,264,682 Source: MHC , 20 December 2017
Notes: Year 1 of operations is assumed to commence on 1 December 2020
The following table sets out the recurrent cost profile differentiated by clinical and Non-Government Organisation costs. Table 31: Community Mental Health Step Up/Step Down Service Recurrent Cost Differentiation by Staffing Components
Item
Recurrent Cost ($000)
2020/21 2021/22 Clinical $ 170,593 $ 295,369 Non-Government Organisation $ 1,623,346 $ 2,175,374
Sub-total $ 1,793,939 $ 2,470,743
Total Recurrent Costs $ 4,264,682 Source: MHC , 20 December 2017
P a g e | 87
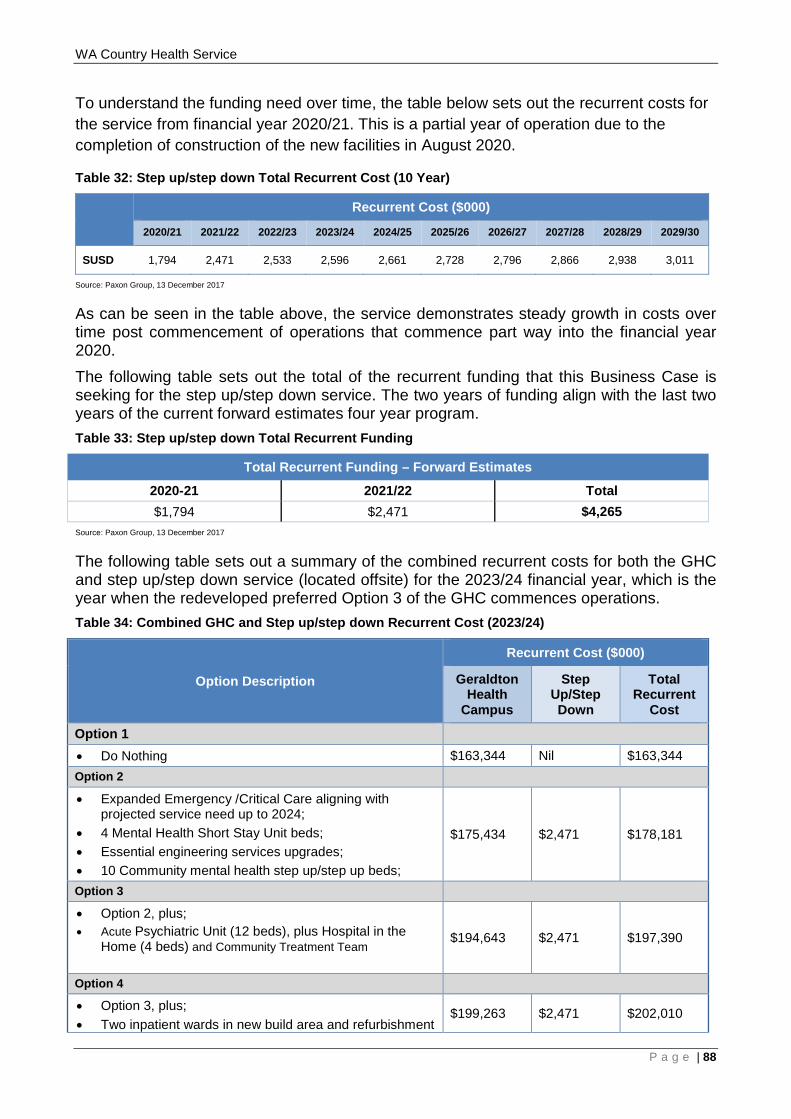
WA Country Health Service
To understand the funding need over time, the table below sets out the recurrent costs for the service from financial year 2020/21. This is a partial year of operation due to the completion of construction of the new facilities in August 2020.
Table 32: Step up/step down Total Recurrent Cost (10 Year)
Recurrent Cost ($000)
2020/21 2021/22 2022/23 2023/24 2024/25 2025/26 2026/27 2027/28 2028/29 2029/30
SUSD 1,794 2,471 2,533 2,596 2,661 2,728 2,796 2,866 2,938 3,011
Source: Paxon Group, 13 December 2017
As can be seen in the table above, the service demonstrates steady growth in costs over time post commencement of operations that commence part way into the financial year 2020. The following table sets out the total of the recurrent funding that this Business Case is seeking for the step up/step down service. The two years of funding align with the last two years of the current forward estimates four year program. Table 33: Step up/step down Total Recurrent Funding
Total Recurrent Funding – Forward Estimates
2020-21 2021/22 Total $1,794 $2,471 $4,265
Source: Paxon Group, 13 December 2017
The following table sets out a summary of the combined recurrent costs for both the GHC and step up/step down service (located offsite) for the 2023/24 financial year, which is the year when the redeveloped preferred Option 3 of the GHC commences operations. Table 34: Combined GHC and Step up/step down Recurrent Cost (2023/24)
Option Description
Recurrent Cost ($000)
Geraldton Health
Campus
Step Up/Step Down
Total Recurrent
Cost
Option 1 • Do Nothing $163,344 Nil $163,344 Option 2
• Expanded Emergency /Critical Care aligning with projected service need up to 2024;
• 4 Mental Health Short Stay Unit beds; • Essential engineering services upgrades; • 10 Community mental health step up/step up beds;
$175,434 $2,471 $178,181
Option 3
• Option 2, plus; • Acute Psychiatric Unit (12 beds), plus Hospital in the
Home (4 beds) and Community Treatment Team
$194,643 $2,471 $197,390
Option 4
• Option 3, plus; • Two inpatient wards in new build area and refurbishment
$199,263 $2,471 $202,010
P a g e | 88
WA Country Health Service
Option Description
Recurrent Cost ($000)
Geraldton Health
Campus
Step Up/Step Down
Total Recurrent
Cost of existing inpatient wards;
• New birthing facilities; • Additional operating theatre and Day Surgery Unit
redevelopment; • Refurbishment of Central Sterilisation Services
Department • Ambulatory care new build area; • Expansion of Medical Records, Medical Imaging,
Pharmacy and Main Entry; • Development of administration and Learning and
Development area; • New lift core and clearly defined front of house and back
of house circulation for patient amenity and operating efficiency;
• Upgrade and expansion to non-clinical support services.
2.11.3.3 APU recurrent funding gap WACHS and the MHC have been working to develop appropriate funding models for small scale rural APUs. To do this WACHS has completed an APU costing study. This study has shown a shortfall of $2.3 million between the indicative ABF allocation (that will be redirected from Metropolitan Health Services) and the actual operating costs required for the Midwest APU. It is intended that this shortfall will be presented to the Expenditure Review Committee as part of the 2018-19 Mid Year Review. The study was conducted across the 2016/17 and 2017/18 years, to date, for the four APUs located in Albany, Bunbury, Broome and Kalgoorlie. The employment, overheads and goods and services costs were analysed to arrive at a weighted cost per bed. These were then extrapolated to the 12 bed profile for the GHC APU resulting in the $2.3 million operating costs shortfall. The following inputs and assumptions should be noted:
• cost profile has been calculated based on 2016/17 actual average cost per bed at Albany & Kalgoorlie +1.5% escalation;
• cost may be higher depending on the costing of the utility costing practice at the differing WACHS regions (some regions don’t separate out the cost between wards);
• estimated costs include overhead charges; • the weighted activity unit profile has been calculated based on 2016/17 actual
weighted activity unit per bed delivered in Albany & Kalgoorlie +1.5% escalation; • the teaching, training and research component has been based on 2016/17 actual
teaching, training and research received per bed for Albany & Kalgoorlie + 1.5% escalation; and
• revenue is based on $4988 price per weighted activity unit.
P a g e | 89
WA Country Health Service
2.12 Project Timeframe and Key Milestones
The following tables outlines the proposed program and durations for key project phases for all the GHC redevelopment options and the step up/step down service.
a g e | 90
WA Country Health Service
2.13 Risk Analysis
The following table presents the main risks associated with the preferred Option 3 in this Business Case. The risks have been assessed as to the level of risk it presents and mitigation strategies have been outlined for each identified risk for both sites.
P a g e | 91
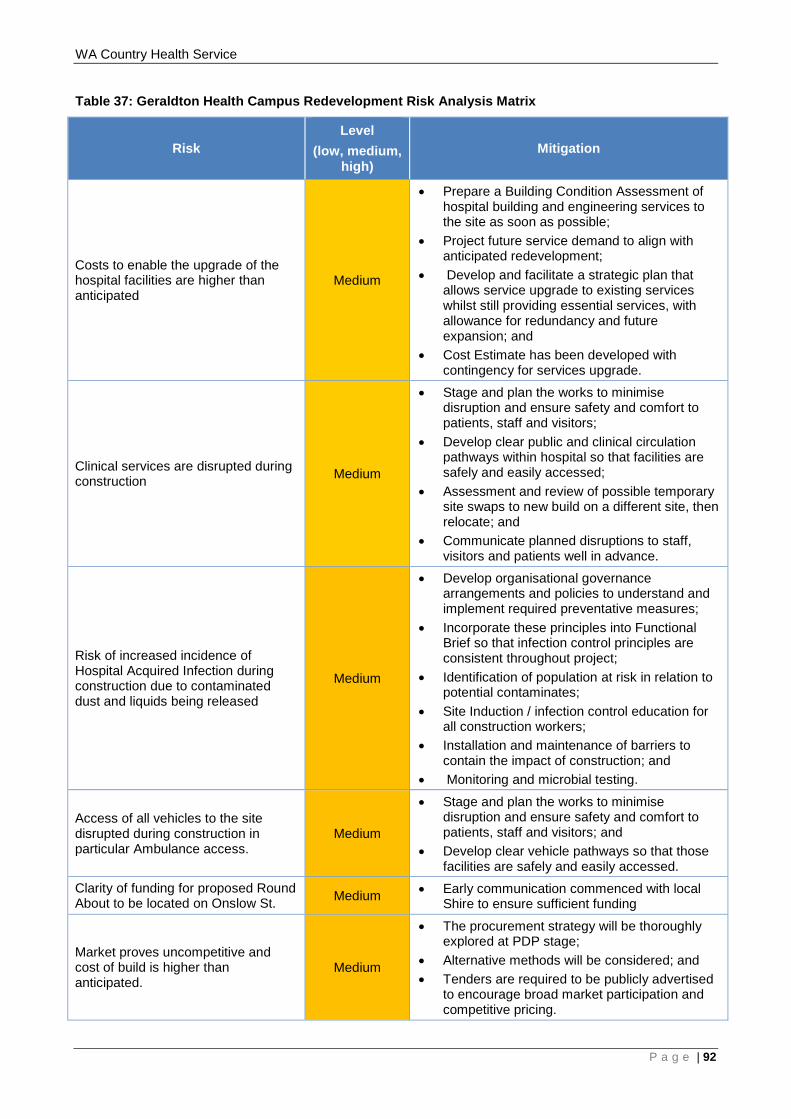
WA Country Health Service
Table 37: Geraldton Health Campus Redevelopment Risk Analysis Matrix
Risk Level
(low, medium, high)
Mitigation
Costs to enable the upgrade of the hospital facilities are higher than anticipated
Medium
• Prepare a Building Condition Assessment of hospital building and engineering services to the site as soon as possible;
• Project future service demand to align with anticipated redevelopment;
• Develop and facilitate a strategic plan that allows service upgrade to existing services whilst still providing essential services, with allowance for redundancy and future expansion; and
• Cost Estimate has been developed with contingency for services upgrade.
Clinical services are disrupted during construction Medium
• Stage and plan the works to minimise disruption and ensure safety and comfort to patients, staff and visitors;
• Develop clear public and clinical circulation pathways within hospital so that facilities are safely and easily accessed;
• Assessment and review of possible temporary site swaps to new build on a different site, then relocate; and
• Communicate planned disruptions to staff, visitors and patients well in advance.
Risk of increased incidence of Hospital Acquired Infection during construction due to contaminated dust and liquids being released
Medium
• Develop organisational governance arrangements and policies to understand and implement required preventative measures;
• Incorporate these principles into Functional Brief so that infection control principles are consistent throughout project;
• Identification of population at risk in relation to potential contaminates;
• Site Induction / infection control education for all construction workers;
• Installation and maintenance of barriers to contain the impact of construction; and
• Monitoring and microbial testing.
Access of all vehicles to the site disrupted during construction in particular Ambulance access.
Medium
• Stage and plan the works to minimise disruption and ensure safety and comfort to patients, staff and visitors; and
• Develop clear vehicle pathways so that those facilities are safely and easily accessed.
Clarity of funding for proposed Round About to be located on Onslow St. Medium • Early communication commenced with local
Shire to ensure sufficient funding
Market proves uncompetitive and cost of build is higher than anticipated.
Medium
• The procurement strategy will be thoroughly explored at PDP stage;
• Alternative methods will be considered; and • Tenders are required to be publicly advertised
to encourage broad market participation and competitive pricing.
P a g e | 92
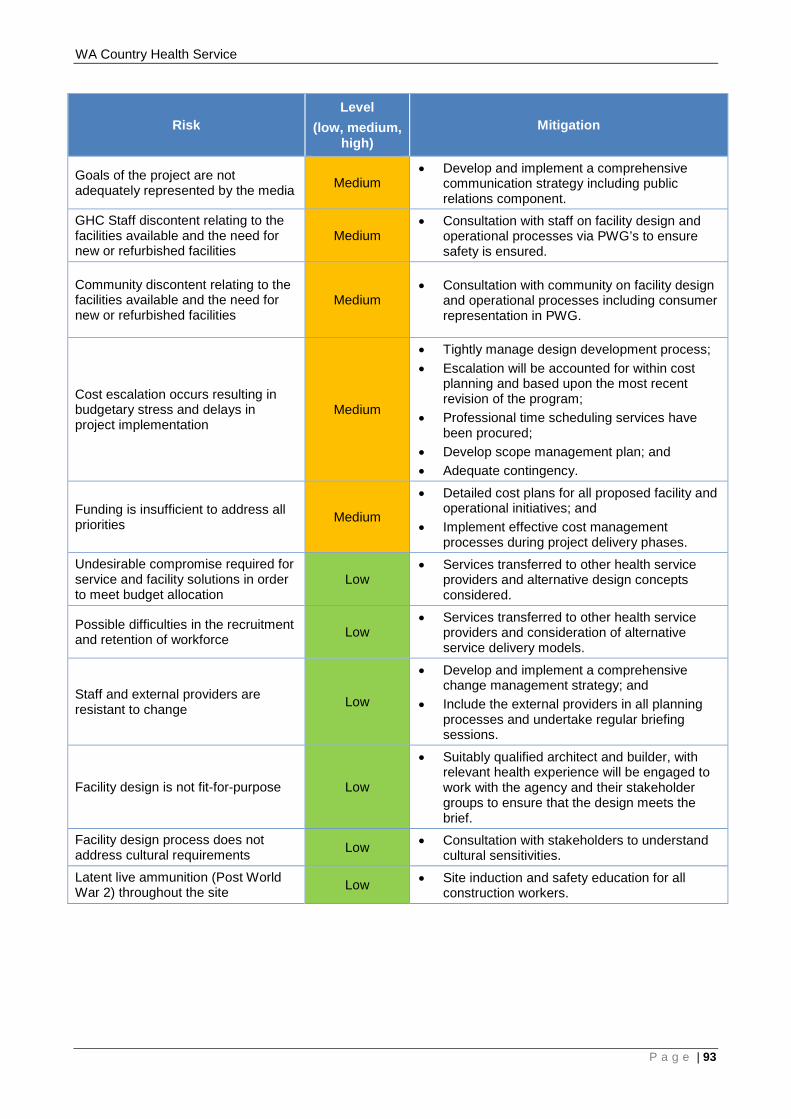
WA Country Health Service
Risk Level
(low, medium, high)
Mitigation
Goals of the project are not adequately represented by the media Medium
• Develop and implement a comprehensive communication strategy including public relations component.
GHC Staff discontent relating to the facilities available and the need for new or refurbished facilities
Medium • Consultation with staff on facility design and
operational processes via PWG’s to ensure safety is ensured.
Community discontent relating to the facilities available and the need for new or refurbished facilities
Medium • Consultation with community on facility design
and operational processes including consumer representation in PWG.
Cost escalation occurs resulting in budgetary stress and delays in project implementation
Medium
• Tightly manage design development process; • Escalation will be accounted for within cost
planning and based upon the most recent revision of the program;
• Professional time scheduling services have been procured;
• Develop scope management plan; and • Adequate contingency.
Funding is insufficient to address all priorities Medium
• Detailed cost plans for all proposed facility and operational initiatives; and
• Implement effective cost management processes during project delivery phases.
Undesirable compromise required for service and facility solutions in order to meet budget allocation
Low • Services transferred to other health service
providers and alternative design concepts considered.
Possible difficulties in the recruitment and retention of workforce Low
• Services transferred to other health service providers and consideration of alternative service delivery models.
Staff and external providers are resistant to change Low
• Develop and implement a comprehensive change management strategy; and
• Include the external providers in all planning processes and undertake regular briefing sessions.
Facility design is not fit-for-purpose Low
• Suitably qualified architect and builder, with relevant health experience will be engaged to work with the agency and their stakeholder groups to ensure that the design meets the brief.
Facility design process does not address cultural requirements Low • Consultation with stakeholders to understand
cultural sensitivities. Latent live ammunition (Post World War 2) throughout the site Low • Site induction and safety education for all
construction workers.
P a g e | 93
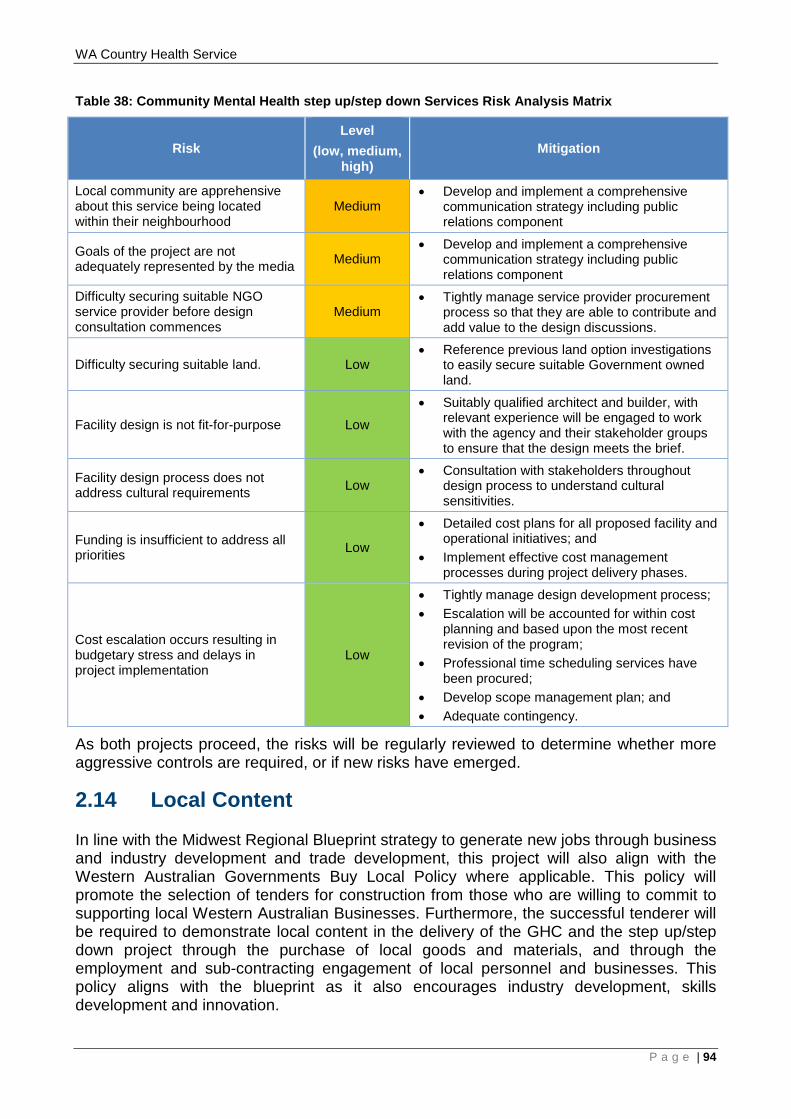
WA Country Health Service
Table 38: Community Mental Health step up/step down Services Risk Analysis Matrix
Risk Level
(low, medium, high)
Mitigation
Local community are apprehensive about this service being located within their neighbourhood
Medium • Develop and implement a comprehensive
communication strategy including public relations component
Goals of the project are not adequately represented by the media Medium
• Develop and implement a comprehensive communication strategy including public relations component
Difficulty securing suitable NGO service provider before design consultation commences
Medium • Tightly manage service provider procurement
process so that they are able to contribute and add value to the design discussions.
Difficulty securing suitable land. Low • Reference previous land option investigations
to easily secure suitable Government owned land.
Facility design is not fit-for-purpose Low
• Suitably qualified architect and builder, with relevant experience will be engaged to work with the agency and their stakeholder groups to ensure that the design meets the brief.
Facility design process does not address cultural requirements Low
• Consultation with stakeholders throughout design process to understand cultural sensitivities.
Funding is insufficient to address all priorities Low
• Detailed cost plans for all proposed facility and operational initiatives; and
• Implement effective cost management processes during project delivery phases.
Cost escalation occurs resulting in budgetary stress and delays in project implementation
Low
• Tightly manage design development process; • Escalation will be accounted for within cost
planning and based upon the most recent revision of the program;
• Professional time scheduling services have been procured;
• Develop scope management plan; and • Adequate contingency.
As both projects proceed, the risks will be regularly reviewed to determine whether more aggressive controls are required, or if new risks have emerged.
2.14 Local Content
In line with the Midwest Regional Blueprint strategy to generate new jobs through business and industry development and trade development, this project will also align with the Western Australian Governments Buy Local Policy where applicable. This policy will promote the selection of tenders for construction from those who are willing to commit to supporting local Western Australian Businesses. Furthermore, the successful tenderer will be required to demonstrate local content in the delivery of the GHC and the step up/step down project through the purchase of local goods and materials, and through the employment and sub-contracting engagement of local personnel and businesses. This policy aligns with the blueprint as it also encourages industry development, skills development and innovation.
P a g e | 94
WA Country Health Service
It is noted that the WA Jobs Bill 2017 has been passed as an act of parliament. This Bill, in its implementation, will support small and medium businesses to participate in the supply of goods and services to the Government, creating more local jobs for local workers.
2.15 Aboriginal Participation
The Midwest Regional Blueprint states approximately 12% of the Midwest population identifies as being Aboriginal (compared to the state average of 3.2%) and comparatively they experience a high disease burden. When looking at the sub regional distribution of Aboriginal people, 67% live within the Greater Geraldton region and this impacts the complexity and demand experienced at GHC. Currently there are a number of Aboriginal Medical Services that provide a service to the Aboriginal population of the Midwest. This project will build upon the existing relationships between Aboriginal Medical Services and WACHS to deliver culturally appropriate healthcare. It is imperative that the Aboriginal Medical Services and other local Aboriginal people are consulted throughout the planning and design process to ensure that the redeveloped facility reflects their health needs and specific design requirements. The Midwest Regional Blueprint also states that approximately 17% of Aboriginal people in the Midwest are employed full time, compared with 42% non-Aboriginal people. In line with the proposed economic development strategies as per the blueprint, this redevelopment project will look at employment opportunities to improve social and economic outcomes for Aboriginal people.
2.16 State Funded Infrastructure and Apprenticeship Participation
As per the Government Building Training Policy the State Government is aiming to increase the overall numbers of apprentices and trainees in the building and construction industry. This will be achieved by requiring Government building, construction and maintenance head contractors to commit to meet or exceed a target training rate through the employment of construction apprentices and trainees by their company and the subcontractors they are using for the contract, as determined by the Department of Training and Workforce Development. The Government Building Training Policy applies to:
• All State Government building and construction contracts with an estimated labour value of $2 million and over for the construction component of the contract;
• All State Government maintenance contracts with an estimated labour value of $2 million and over for the total contract; and
• Where the duration is three months or more.
P a g e | 95
WA Country Health Service
3 IMPLEMENTATION STRATEGY 3.1 Communication Plan
A comprehensive Communications Plan for the GHC component of the project will be developed by WACHS Midwest. A comprehensive plan for the step up step down service will be developed by the MHC. These plans will communicate updates and achievements of the redevelopment project to a variety of stakeholders (refer section 2.7 of this document). The aim of the communication plan will be to define the:
• Objectives, key deliverables and rationale for service reform and the redevelopment of the sites;
• Key messages that will be consistently promoted to all stakeholders; • Strategies to communicate to stakeholder groups to mitigate risks to project
performance; and • Type and frequency of communication methods.
The Communication plan will align with the project timeframe and key milestones to ensure communication is timely and aids the development, implementation and completion of the projects.
P a g e | 96
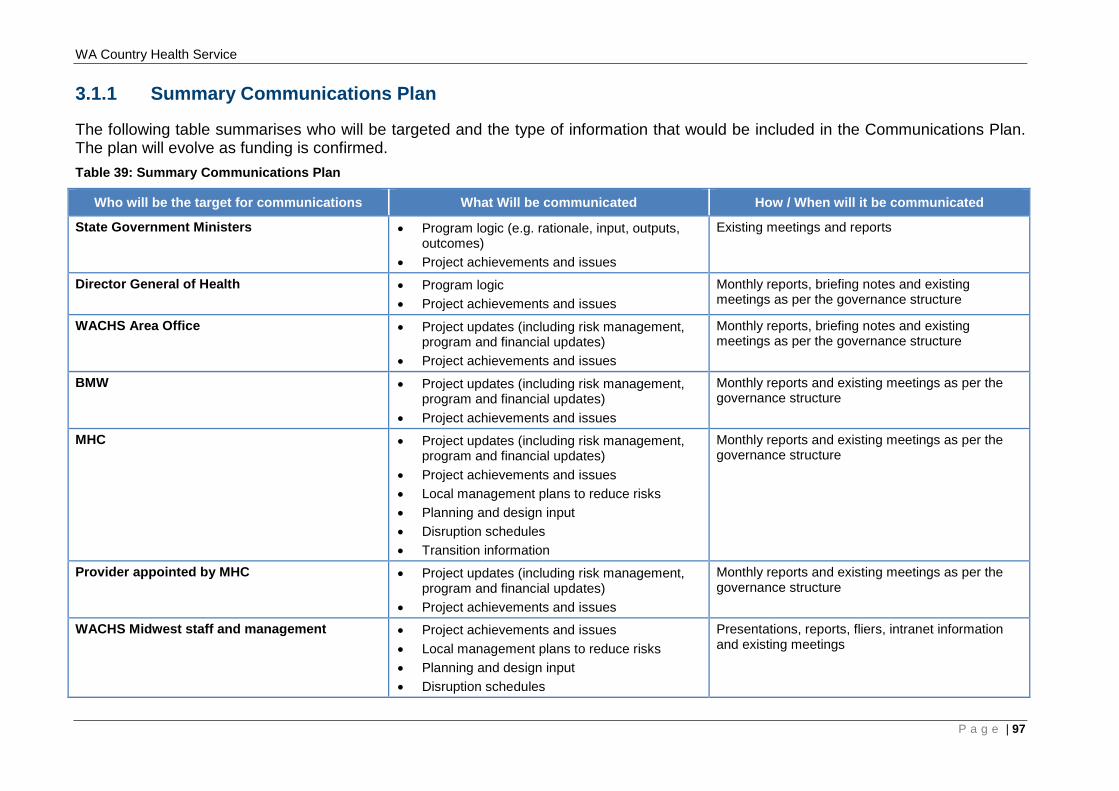
WA Country Health Service
3.1.1 Summary Communications Plan
The following table summarises who will be targeted and the type of information that would be included in the Communications Plan. The plan will evolve as funding is confirmed. Table 39: Summary Communications Plan
Who will be the target for communications What Will be communicated How / When will it be communicated
State Government Ministers • Program logic (e.g. rationale, input, outputs, outcomes)
• Project achievements and issues
Existing meetings and reports
Director General of Health • Program logic • Project achievements and issues
Monthly reports, briefing notes and existing meetings as per the governance structure
WACHS Area Office • Project updates (including risk management, program and financial updates)
• Project achievements and issues
Monthly reports, briefing notes and existing meetings as per the governance structure
BMW • Project updates (including risk management, program and financial updates)
• Project achievements and issues
Monthly reports and existing meetings as per the governance structure
MHC • Project updates (including risk management, program and financial updates)
• Project achievements and issues • Local management plans to reduce risks • Planning and design input • Disruption schedules • Transition information
Monthly reports and existing meetings as per the governance structure
Provider appointed by MHC • Project updates (including risk management, program and financial updates)
• Project achievements and issues
Monthly reports and existing meetings as per the governance structure
WACHS Midwest staff and management • Project achievements and issues • Local management plans to reduce risks • Planning and design input • Disruption schedules
Presentations, reports, fliers, intranet information and existing meetings
P a g e | 97
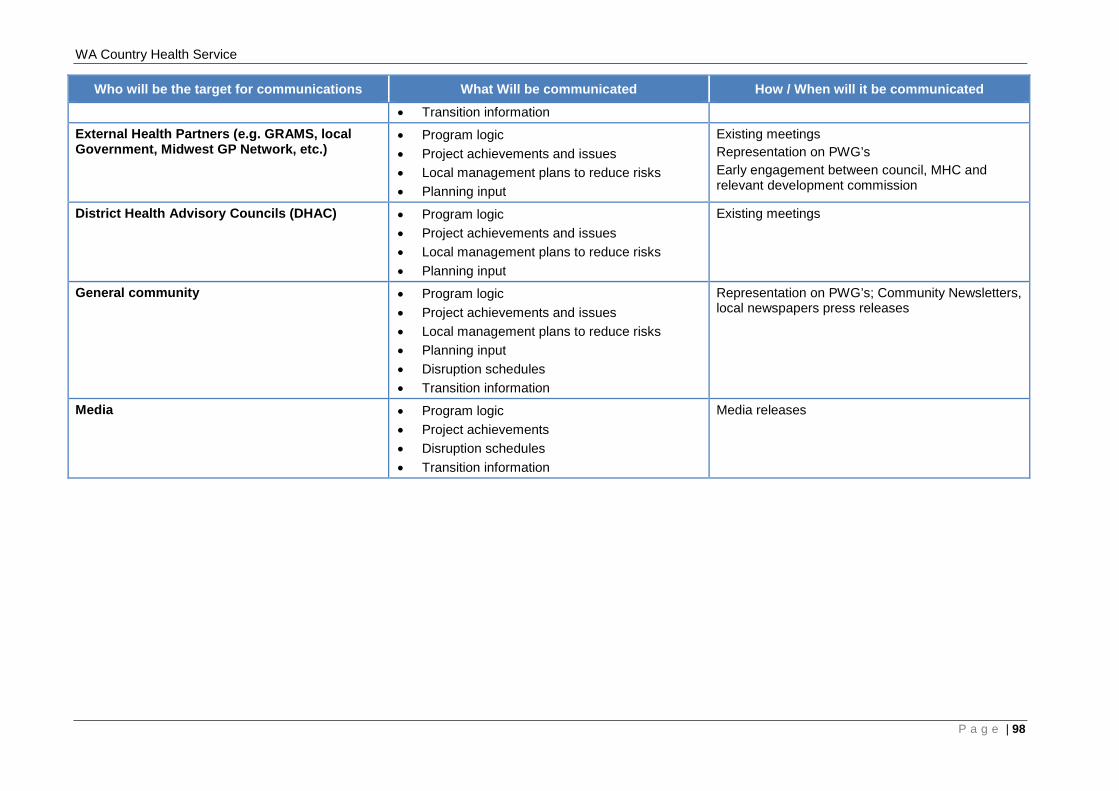
WA Country Health Service
Who will be the target for communications What Will be communicated How / When will it be communicated • Transition information
External Health Partners (e.g. GRAMS, local Government, Midwest GP Network, etc.)
• Program logic • Project achievements and issues • Local management plans to reduce risks • Planning input
Existing meetings Representation on PWG’s Early engagement between council, MHC and relevant development commission
District Health Advisory Councils (DHAC) • Program logic • Project achievements and issues • Local management plans to reduce risks • Planning input
Existing meetings
General community • Program logic • Project achievements and issues • Local management plans to reduce risks • Planning input • Disruption schedules • Transition information
Representation on PWG’s; Community Newsletters, local newspapers press releases
Media • Program logic • Project achievements • Disruption schedules • Transition information
Media releases
P a g e | 98
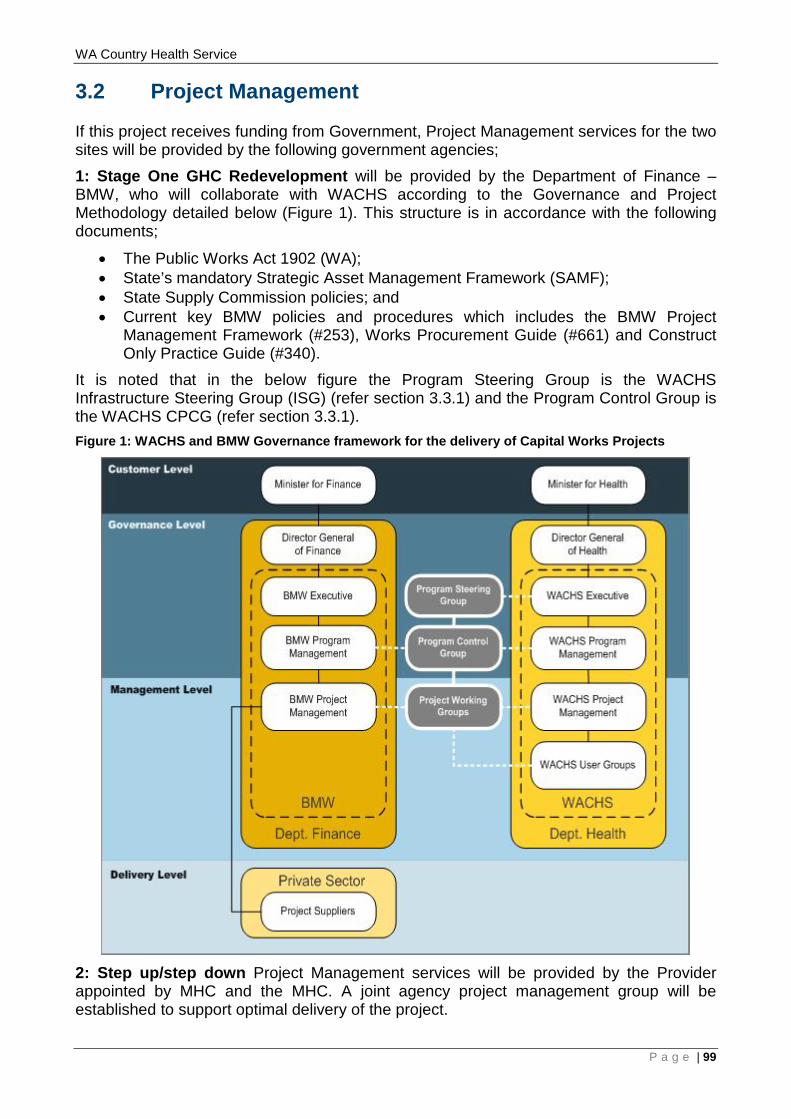
WA Country Health Service
3.2 Project Management
If this project receives funding from Government, Project Management services for the two sites will be provided by the following government agencies; 1: Stage One GHC Redevelopment will be provided by the Department of Finance – BMW, who will collaborate with WACHS according to the Governance and Project Methodology detailed below (Figure 1). This structure is in accordance with the following documents;
• The Public Works Act 1902 (WA); • State’s mandatory Strategic Asset Management Framework (SAMF); • State Supply Commission policies; and • Current key BMW policies and procedures which includes the BMW Project
Management Framework (#253), Works Procurement Guide (#661) and Construct Only Practice Guide (#340).
It is noted that in the below figure the Program Steering Group is the WACHS Infrastructure Steering Group (ISG) (refer section 3.3.1) and the Program Control Group is the WACHS CPCG (refer section 3.3.1). Figure 1: WACHS and BMW Governance framework for the delivery of Capital Works Projects
2: Step up/step down Project Management services will be provided by the Provider appointed by MHC and the MHC. A joint agency project management group will be established to support optimal delivery of the project.
P a g e | 99
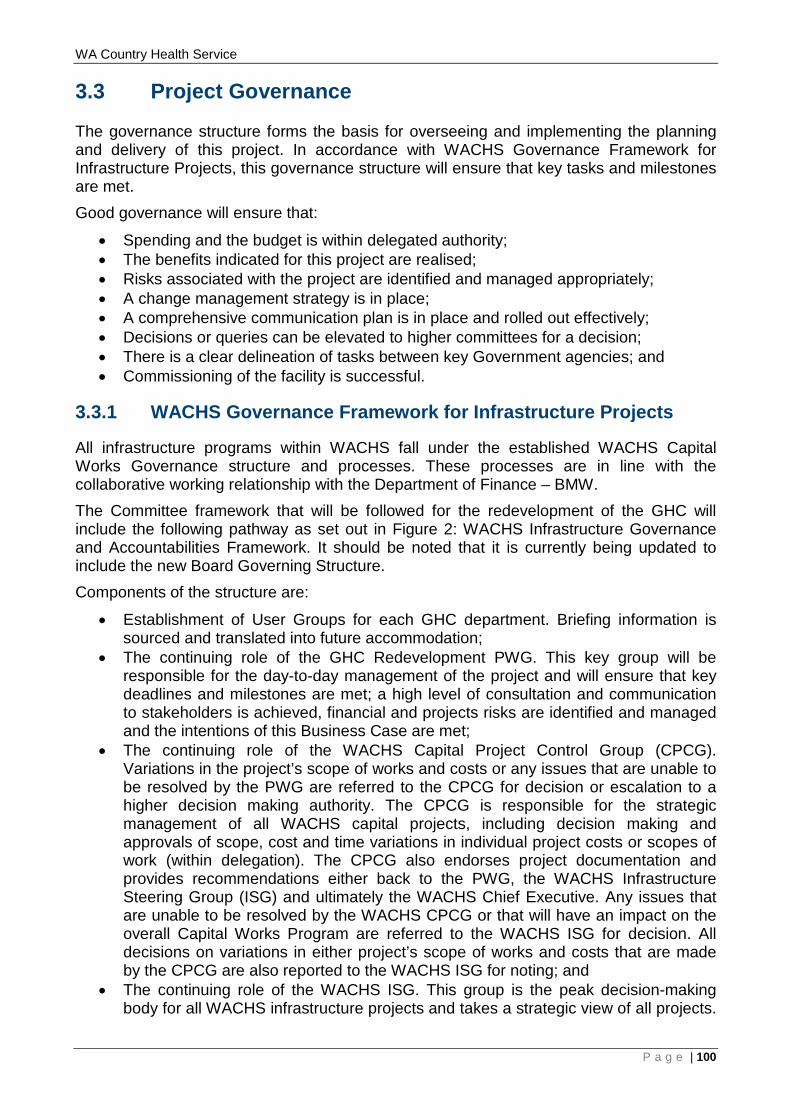
WA Country Health Service
3.3 Project Governance
The governance structure forms the basis for overseeing and implementing the planning and delivery of this project. In accordance with WACHS Governance Framework for Infrastructure Projects, this governance structure will ensure that key tasks and milestones are met. Good governance will ensure that:
• Spending and the budget is within delegated authority; • The benefits indicated for this project are realised; • Risks associated with the project are identified and managed appropriately; • A change management strategy is in place; • A comprehensive communication plan is in place and rolled out effectively; • Decisions or queries can be elevated to higher committees for a decision; • There is a clear delineation of tasks between key Government agencies; and • Commissioning of the facility is successful.
3.3.1 WACHS Governance Framework for Infrastructure Projects
All infrastructure programs within WACHS fall under the established WACHS Capital Works Governance structure and processes. These processes are in line with the collaborative working relationship with the Department of Finance – BMW. The Committee framework that will be followed for the redevelopment of the GHC will include the following pathway as set out in Figure 2: WACHS Infrastructure Governance and Accountabilities Framework. It should be noted that it is currently being updated to include the new Board Governing Structure. Components of the structure are:
• Establishment of User Groups for each GHC department. Briefing information is sourced and translated into future accommodation;
• The continuing role of the GHC Redevelopment PWG. This key group will be responsible for the day-to-day management of the project and will ensure that key deadlines and milestones are met; a high level of consultation and communication to stakeholders is achieved, financial and projects risks are identified and managed and the intentions of this Business Case are met;
• The continuing role of the WACHS Capital Project Control Group (CPCG). Variations in the project’s scope of works and costs or any issues that are unable to be resolved by the PWG are referred to the CPCG for decision or escalation to a higher decision making authority. The CPCG is responsible for the strategic management of all WACHS capital projects, including decision making and approvals of scope, cost and time variations in individual project costs or scopes of work (within delegation). The CPCG also endorses project documentation and provides recommendations either back to the PWG, the WACHS Infrastructure Steering Group (ISG) and ultimately the WACHS Chief Executive. Any issues that are unable to be resolved by the WACHS CPCG or that will have an impact on the overall Capital Works Program are referred to the WACHS ISG for decision. All decisions on variations in either project’s scope of works and costs that are made by the CPCG are also reported to the WACHS ISG for noting; and
• The continuing role of the WACHS ISG. This group is the peak decision-making body for all WACHS infrastructure projects and takes a strategic view of all projects.
P a g e | 100
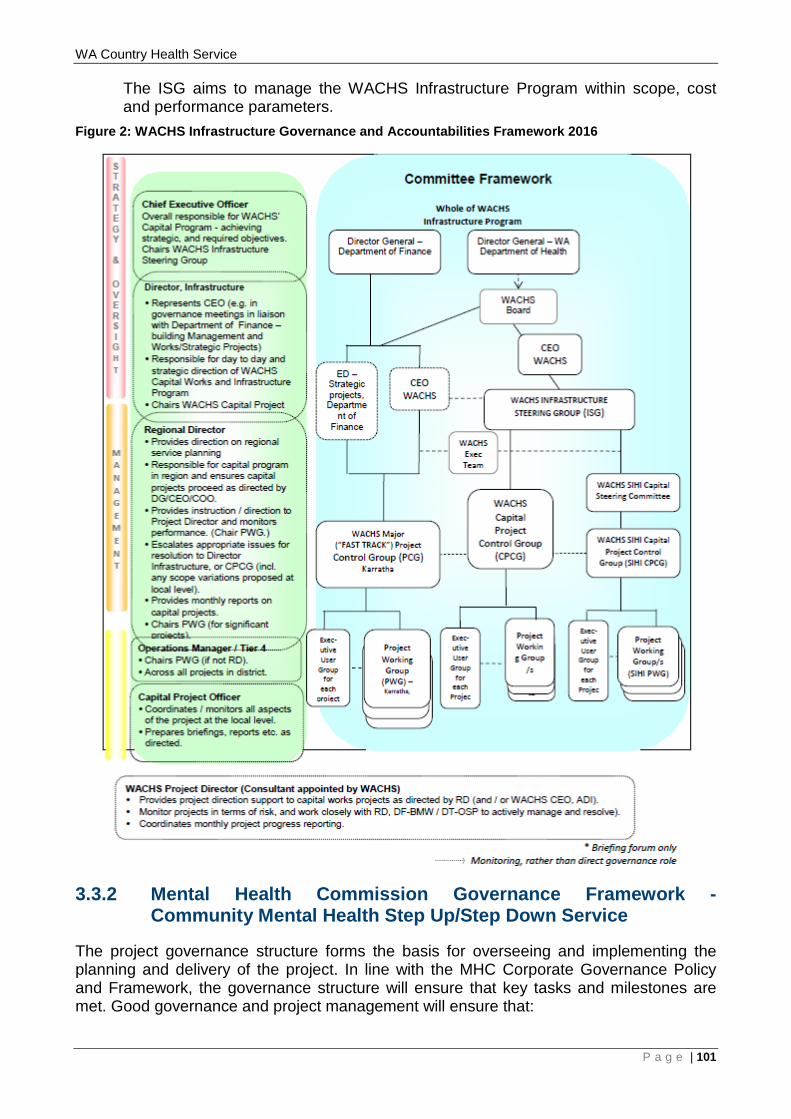
WA Country Health Service
The ISG aims to manage the WACHS Infrastructure Program within scope, cost and performance parameters.
Figure 2: WACHS Infrastructure Governance and Accountabilities Framework 2016
3.3.2 Mental Health Commission Governance Framework - Community Mental Health Step Up/Step Down Service
The project governance structure forms the basis for overseeing and implementing the planning and delivery of the project. In line with the MHC Corporate Governance Policy and Framework, the governance structure will ensure that key tasks and milestones are met. Good governance and project management will ensure that:
P a g e | 101
WA Country Health Service
• Spending and the budget is within delegated authority; • The benefits indicated for this project are realised; • Risks associated with the project are identified and managed appropriately; • A change management strategy is in place; • A comprehensive communication plan is in place and rolled out effectively; • Decisions or queries can be elevated to higher committees for a decision; • There is a clear delineation of tasks between key government agencies; and • Commissioning of the facility is successful.
To achieve this, the following deliverables will be developed by the MHC:
• A detailed project plan, timeline and agreed budget to enable the MHC to plan, monitor and control project performance;
• Meaningful and ongoing engagement with local stakeholders including community, Health Service Providers, non-government service providers, consumers and carers;
• A communication strategy supporting this process – including tools such as a briefing to industry and supporting printed materials promoting the approach proposed by the MHC to interested providers;
• A procurement strategy including: o Market research whereby the feasibility of the proposal and service provider
capacity are adequately tested and understood; o Determining the scope of procurement – whether an approach is made for all
regional sites in one package or requests are made in a staged manner; and o Design of the service delivery request and contracting documentation; and o Service agreements awarded for the full breadth of work involved in
development of a nominated site, enabling transition to operation of the particular step up/step down in a timely manner;
• Licenses and approvals obtained through relevant approving bodies (including local councils, Western Australian Planning Commission et al);
• Development and fit-out and licensing (if required) of the nominated site to a state that is fit-for-purpose to deliver step up/step down services; and
• Ongoing progress reporting. These deliverables will assist in establishing an operational service providing clinical and psychosocial supports by 1 July 2020.
P a g e | 102
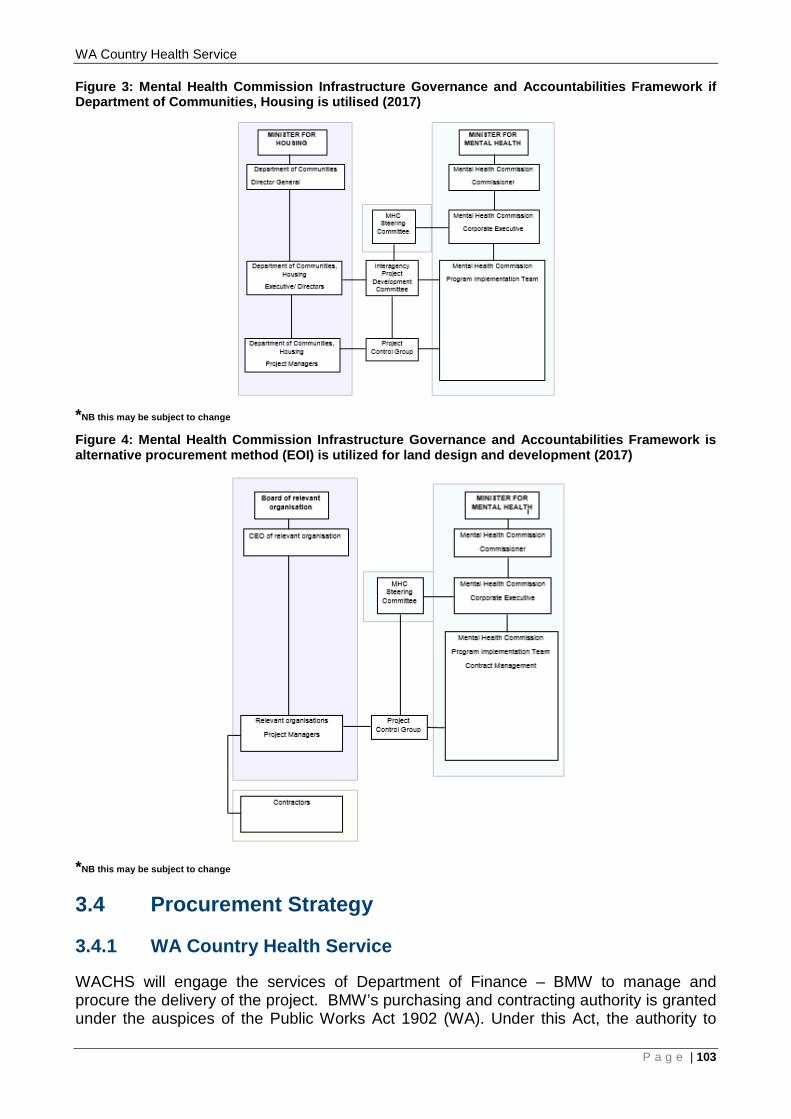
WA Country Health Service Figure 3: Mental Health Commission Infrastructure Governance and Accountabilities Framework if Department of Communities, Housing is utilised (2017)
*NB this may be subject to change
Figure 4: Mental Health Commission Infrastructure Governance and Accountabilities Framework is alternative procurement method (EOI) is utilized for land design and development (2017)
*NB this may be subject to change
3.4 Procurement Strategy
3.4.1 WA Country Health Service
WACHS will engage the services of Department of Finance – BMW to manage and procure the delivery of the project. BMW’s purchasing and contracting authority is granted under the auspices of the Public Works Act 1902 (WA). Under this Act, the authority to
P a g e | 103
WA Country Health Service enter into works contracts rests with the Minister for Works. In order to assist the Minister to carry out the works, procurement officers within BMW have been empowered to exercise certain powers on behalf of the Minister through issuance of formal delegations and/or authorisations. BMW applies the requirements of the Act and other applicable legislation, regulations, standards, codes and policies in delivering non-residential construction projects for State Government Agencies. The tendering method to be used will be determined via a Procurement Workshop held at the PDP stage. BMW have been engaged in the development of this Business Case to provide technical advice and have regularly consulted, including participation at the PWG meetings. BMW’s Cost Plan Guidelines have been applied to the development of the cost plans that form part of this Business Case.
3.4.2 Community Mental Health Step Up/Step Down Services
The MHC will lead the process and project governance, with the procurement process yet to be determined. This may include a partnership with DoCH, or alternatively an Expression of Interest process for another provider. The MHC procurement process is bound by the applicable State Supply Commission policies, the Delivering Community Services in Partnership policy and MHC's internal processes and will be conducted in consultation with the DoF. Existing relationships with the DoF will be capitalised upon meaning, that they will provide support to progress the timely procurement of a non-Government service provider to operate the facility.
DESIGN AND CONSTRUCTION Procurement processes for the management of the design and construction are yet to be determined, however the functional brief and model of service will be provided by the MHC to the relevant provider.
P a g e | 104
WA Country Health Service
P a g e | 105
WA Country Health Service
3.5 Supporting Documents
The documentation referred to in this Business Case that is attached is:
• Appendix A - Geraldton Health Campus Concept Brief V5.0 (9 November 2017) • Appendix B – Concept Master Development Plan Geraldton Health Campus
Redevelopment Options 2, 3 and 4 • Appendix C - Community Mental Health (Geraldton) Step up/step down service
Concept Brief V3.0 (6 November 2017) • Appendix D – Concept Master Development Plan Community Mental Health Step
up/step down Service The following documents relevant to the development of this Business Case are not provided as attachments but are available on request.
• Midwest Regional Blueprint (August 2015); • WA Country Health Service - Service Plan 2010 – 2020 Geraldton Health Campus,
WACHS Midwest, Version 6 (May 2012); • WA Country Health Service - Midwest Health Initiative (MWHI) Concept Brief
(October 2014); • WA Health Clinical Services Framework 2014 – 2024; • Geraldton Health Campus Assumptions Paper V1.0 (9 September 2016); • WA Country Health Service – Strategic Directions 2015 – 2018; • Healthier County Communities through Partnerships and Innovation (2015); • Council of Australian Governments (COAG) National Health Reform Agreement
(2011); • WA Health WA Health Strategic Intent (2015 – 2020); • WA Health Model of Care, Over view and Guidelines – WA Health Networks; • Geraldton Regional Aboriginal Medical Services (GRAMS) Strategic Plan (2015 –
2018); • WA Health – Health Information and Communication Technology (ICT) Strategy
(2015 – 2018); • WACHS Renal Dialysis Plan (2010 – 2021); • WA Mental Health Commission Strategic Plan (2020); • Integrated Midwest Mental Health Services: Business Case (2016-17); • MHC Western Australian Community Mental Health Step Up/Step down Services;
Model of Service (June 2017); • Integrated Midwest Mental Health Service Concept Brief (V:18, 26 November
2015); • Midwest Integrated Mental Health Service, Service Model (V:2.5, 2 December
2015); • Review of the Admission or Referral to and the Discharge and Transfer Practices of
Public Mental Health Facilities/services in Western Australia, by Professor Bryant Stokes, AM, 2012 (the Stokes Review);
• WA Health Redundancy and Disaster Planning in Health’s Capital Works Programs 2nd Edition (January 2012);
• WA Country Health Service WACHS Public and Primary Health Strategy (2015-2018) Healthier Country Communities Through Partnerships and Innovation;
• WA Country Health Service WACHS Healthy Country Kids: An Integrated Child Health and Development Service Strategy 2016-2019 (May 2016);
P a g e | 106

WA Country Health Service
• WA Country Health Service WACHS Chronic Conditions Prevention and Management Strategy (2015-2020) Healthier Country Communities Through Partnerships and Innovation; and
• WA Country Health Service Aboriginal Employment Strategy 2014–2018.
P a g e | 107
WA Country Health Service
4 RECOMMENDATION It is recommended that:
1. The WA State Government endorses Option 3 Stage One for the GHC and the offsite step up/step down service as the preferred option because it:
• responds through a three staged approach to the investment objectives and service reform priorities as highlighted in the WA Health Clinical Services Framework 2014 – 2024, Geraldton Health Campus WACHS Midwest Service Plan 2010-2020 and Midwest Regional Blueprint (2015);
• delivers services in alignment with the Western Australian, Mental Health Alcohol and Other Drug Services Plan 2015 – 2025 (The Plan);
• enables health services delivery, for the Geraldton and Midwest region communities, from a contemporary health facility;
• reduces many of the current risks to service delivery at Geraldton Health Campus, increases consumer access and improves operational efficiency;
• significantly improves patient and staff amenity; and • can be delivered without significant disruption to the existing service, staff and
patients whilst still meeting business objectives. 2. The WA State Government approves the preferred option of the Geraldton Health
Campus Redevelopment Option 3 Stage One, that includes the offsite step up/step down service, costed at $79.206 million.
3. The WA State Government approves capital funding of $73.276 million, for expenditure across five years, to be provided to WACHS to complete the capital works on the GHC.
4. The WA State Government approves capital funding of $5.930 million for expenditure across three years for the step up/step down service, to be provided to the MHC to complete the step up/step down capital works.
5. The WA State Government approves operational funding of $4.265 million for expenditure across two years for the step up/step down service, to be provided to the MHC, and to form part of the MHC base funding.
6. The WA State Government notes that a further business case detailing the recurrent costing required, to operate the APU, HITH, Mental Health Short Stay Unit, and CTT services, will be jointly developed by WACHS and the MHC and be submitted for Government consideration as part of the 2018-19 Budget process.
P a g e | 108
WA Country Health Service
5 NEXT STEPS Should the request to provide capital funding for $79.206 million and recurrent funding of $4.265 million be successful, the next step would be to implement the project and mitigate associated risks by establishing the following:
• Confirm that the existing WACHS and MHC Project Governance Structure is appropriate for the projects;
• Confirm that the established project meetings and reporting structure reflects the intended Governance structure for the next stage of the projects;
• Develop Project Communications Plans; • Develop Project Implementation and Delivery Management Plans; • Undertake a GHC Building Condition Audit and detailed Site Investigations as a
matter of priority to properly determine the building facility and engineering services gaps in order to confirm that the allowances in the cost estimate are robust;
• Identify and procure suitable land for the step up/step down; • Review the CMDP’s to establish that they remain deliverable following the outcome
of the BCA and detailed Site Investigations; • Commence development of the Functional Briefs; • Commence development of the PDP, ensuring the following are done as priority
items to input into the Plan. This involves the following steps: 1. Develop a detailed GHC staging construction and engineering services
diversion plan; 2. Undertake a GHC detailed traffic and car parking audit and plan; 3. Develop both Risk Analysis Matrices into detailed Risk Management Plans via
Risk Management Workshops; and 4. Identify the preferred procurement option via a procurement options workshop.
P a g e | 109

WA Country Health Service
Appendix A - GHC Concept Brief
P a g e | 110
WA Country Health Service
Appendix B - GHC Concept Master Development Plan
P a g e | 111
WA Country Health Service
Option 2 – Ground Floor Plan
P a g e | 112
WA Country Health Service
Option 3 – Ground Floor Plan
P a g e | 113
WA Country Health Service
Option 4 - Ground Floor Plan
P a g e | 114
WA Country Health Service
Option 4 - First Floor Plan
P a g e | 115
WA Country Health Service
Appendix C - Community Mental Health Step Up/Step Down Service Concept Brief Geraldton Step up/step down Service
P a g e | 116
WA Country Health Service
Appendix D - Community Mental Health Step Up/Step Down Service Concept Master Development Plan
P a g e | 117
Prepared for
WACHS - MIDWEST
09 November 2017
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
Version Control
1.0
2.0
3.0
4.0
5.0
! 1 Jeff Calver I I Michele Young
11 October 2017 Rob Pulsford
Jeff Calver 16 October 2017 j Michele Young
! Rob Pulsford i Jeff Calver
23 October 2017 ; Michele Young
06 November 2017
09 November 2017
! Rob Pulsford ; Jeff Calver ! Michele Young i Rob Pulsford I Jeff Calver j Michele Young · Rob Pulsford
For review and feedback Asha Harrison
Final
Final - updated as per WACHS feedback.
Final.
Final.
Jeanette Cooke
Jeanette Cooke
Jeanette Cooke
Jeanette Cooke
\\ap.cbre.net\DFS\AU-SDC-AUR\Jobs\J 282 WACHS\282.4 Midwest\282.4.12 GHC Stage One\(_Planning\Concept Brief\GHC\Version 4 Final\171109 GHC Concept Brief VS.0.docx
Corporate Details
Project Leader
Principal Author
CBRE
Jo Thorley
Asha Harrison
Concept Brief I 2017 CBRE I
CBRE / Project Management / Health & Higher Education / Geraldton Health Campus
TABLE OF CONTENTS Introduction .. ... ... ........ ........ .... ........... .... .... ........... .... .. ... ....... ..... ..... ..... ... ...... .... l
1.1 Background .................................................................................................................................... 1
1.2 Proposed Directions for Service Delivery ............................................................................ 2
2 Vision .................................... .. ........... .. ........ ..... ... .................. ... .......... .......... ... 3
2.1 Campus Design Objectives ....................................................................................................... 3
3 General Planning Parameters .. .... .... ....... .. ........ ..... .......... .............. .......... .... ... .. .. 3
4 Zoning for Expansion .......................... ........... ..... .. ............................................ 5
5 Future Facility Requirements ............ ............................... .. .......... ...... ................ 6
6 Key Functional Relationships ......................... .... .. ............... ................. ....... ..... .. 9
7 Summary of Schedules of Accommodation .... .. ............. ....... ... .......... ........ ....... l 0
CBRE Concept Brief / 2017 CBRE I
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
1 INTRODUCTION This Concept Brief summarises the overarching vision for the Geraldton Health Campus (GHC) project; outlines the general planning principles and key functional models of care that will enable the delivery of health services in accordance with the WA Country Health Services' (WACHS) Geraldton Health Campus Service Plan 2010 - 2020 and the WA Mental Health,
Alcohol and Other Drug Services Plan 2015 - 2025.
It builds on the key recommendations and service delivery strategies as described in the Service Plan and the WACHS Strategic Directions 2015 - 2018: Healthier Country Communities through
Partnerships and Innovation.
This Concept Brief will inform the Concept Master Development Plan for the Geraldton Health Campus Stage One Business Case.
1.1 Background The Geraldton Health Campus is the regional resource centre for the Midwest Health Region and provides the following services to residents of the City of Greater Geraldton, the residents within the Gascoyne, Murchison and Midwest districts, and regional visitors:
Emergency Services; Acute and Sub acute Medical and Surgical Services; A range of Ambulatory Care Services; Primary and Population Health Services; Mental Health Services, Community Alcohol and Drug Services; Obstetric, neonate and paediatric services; Oral Health Care Services; Cancer and Palliative Care Services; Community Aged Care Services; and Rehabilitation Services.
The demand for services on the GHC site has outgrown its original design and as a result minor works have been undertaken to try and accommodate the demand. Some of the contributing factors on service demand include: an ageing population, increased elective surgery, increased need to isolate infectious patients and an increase in mental health and drug and alcohol presentations. In addition to the clinical demand, site services and infrastructure are also at capacity and require a detailed investigation prior to the commencement of any future capital works.
Geraldton Health Campus is classified as a level 3/4 service as per the WA Health Clinical Services Framework 2014 - 2024, with the provision for some services increasing to a level 5 role delineation by 2025.
This increase in role delineation and the demand on services will be the focus of the overall GHC redevelopment project. It is acknowledged that the demand on services and the scope of
CBRE Concept Brief J 2017 CBRE Jl
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
work to redevelop the entire GHC is significant and will require a three staged approach with significant capital investment. Subject to affordability, Stage One will focus on the following:
• Emergency Department (ED) expansion in line with projected service need up to 2024 and providing high dependency capability;
• Mental Health Short Stay Unit (MHSSU) beds x 4 (collocated with the ED); • 12 bed Acute Psychiatric Unit (APU) featuring a Hospital in the Home (HITH)
service (4 beds), and a Community Treatment Team (CTT); and • Essential service upgrades including chil ler replacement.
l .2 Proposed Directions for Service Delivery
The WACHS Geraldton Health Campus Services Plan 2010-2020, overlaid with the WACHS Strategic Directions 2015 - 2018: Healthier Country Communities through Partnerships and Innovation suggests a strategic direction for service delivery at Geraldton Health Campus to 2024. The WA Mental Health, Alcohol and Other Drug Services Plan 2015 - 2025 enhances the overarching strategic directions and the combined overarching priorities applicable to the services for the Stage One scope of works are as follows:
•
•
•
•
Provide services to the level outlined in the WA Health Clinical Services Framework 2014 - 2024 (CSF);
Optimise time and cost efficiencies in delivering health care services across the continuum of care;
Provide safe high quality consumer centred care; Collaborate with health and community partners to increase awareness of health issues;
Collaborate with health and community partners to broaden the range of service options available to the community;
Introduce service delivery models that improve access to services; Enhance Aboriginal health initiatives consistent with our existing programs, Regional Aboriginal Health Plan and other local priorities; Build the capacity of Aboriginal health initiatives by attracting and retaining positions and leadership roles for Aboriginal people; Improve the health outcomes of the community by providing services closer to home for the catchment population;
Attract and retain a skilled workforce and visiting specialists; Increase the use of telehealth in the provision of clinical and non - clinical services;
Enhance and strengthen health networks to improve timeliness in access to high quality care.
The ultimate goal for the future service development across the entire GHC site is to provide optimal services and facilities that support and enable the future model of care for health services as described in the Service planning documentation.
CBRE Concept Brief I 2017 CBRE 12
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
2 VISION In response to the Geraldton Health Campus Service Plan 2010 - 2020, the WA Health Clinical
Services Framework 2014 - 2024, and the WA Mental Health, Alcohol and Other Drug Services Plan 2015 - 2025, the Stage One redevelopment w ill enable GHC to safely manage health demand for emergency/high dependency and mental health services that aligns w ith contemporary models of care by providing the following:
• A combination of level 4 and 5 emergency/high dependency and mental health services onsite as per the role delineation in the WA Health Clinical Services Framework (CSF) 2014 - 2024;
• Expansion of departments included within the Stage One scope in response to updated role delineation in the CSF 2014 - 2024;
• Consumer- centred health care services provided in a contemporary facility that enhances consumer recovery, safety and health outcomes;
• Collocated Integrated Mental Health and Drug and Alcohol Services; • Delivery of socially and culturally appropriate care; • Improved access to services; and
Information & Communication Technology (ICT) advancements for better care; in particular Emergency Telehealth Services and Videoconferencing, Education
and Communication.
2. l Cam pus Design Objectives
The Stage One design objectives are to provide a facility that:
Provides contemporary functional models of care; Provides patient focussed health care services; Meets contemporary design standards and aligns with national benchmarks (e.g. Australasian Health Facility Guidelines); Continues to provide safe existing hospital services during the redevelopment; Supports sustainable principles - environmental, socia l and economic; Will assist in the attraction, recruitment and retention of staff and specialists; Allows for the provision of role delineation changes as per the CSF 2014 -2024;
Incorporates future expansion opportunities; Provides ED HDU synergies to create staffing efficiencies and 24hour care; Collocates the ED with the MHSSU; Complies with the WACHS Office Accommodation Policy; Minimises traffic congestion by separating public traffic access from back of
house/ambulance access.
3 GENERAL PLANNING PARAMETERS The following planning parameters underpin the overarching operational model for the
redeveloped health service;
• Facilitate a Service Delivery driven so lution;
CBRE Concept Brief I 2017 CBRE 13

CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
• Ensure facility design allows for flexibility in service delivery; • Ensure zoning allows for collocation of complementary services including
potential private sector;
• Both site and internal planning of the facilities is to provide clearly defined areas for public and staff only/back of house access including separate circulation pathways for efficiency of travel time and patient amenity;
• Provide secure and safe work environments by minimising public access points ensuring areas can be safely shut down afterhours, at times of low staff numbers and during emergencies;
• Provide adequate and safe parking for staff, patients and visitors; • The ED triage will have a clear view over the public and ambulance entrances; • A clear security presence to be evident at the front of the health facilities; • Ensure that the environment caters for visiting staff; • Allow engineering design to support state of the art Telehealth and other ICT; • Comply with the WA Health Redundancy and Disaster Planning Guidelines (2012)
for health facilities;
• Facility design must support contemporary standards of infection control. In particular isolation rooms with separate negative and positive pressure are to be provided as appropriate and hand basins must be located at the entrance of rooms; and
• Ambulance set down and pick up bays must be under cover, and drive through.
CBRE Concept Brief I 2017 CBRE 14
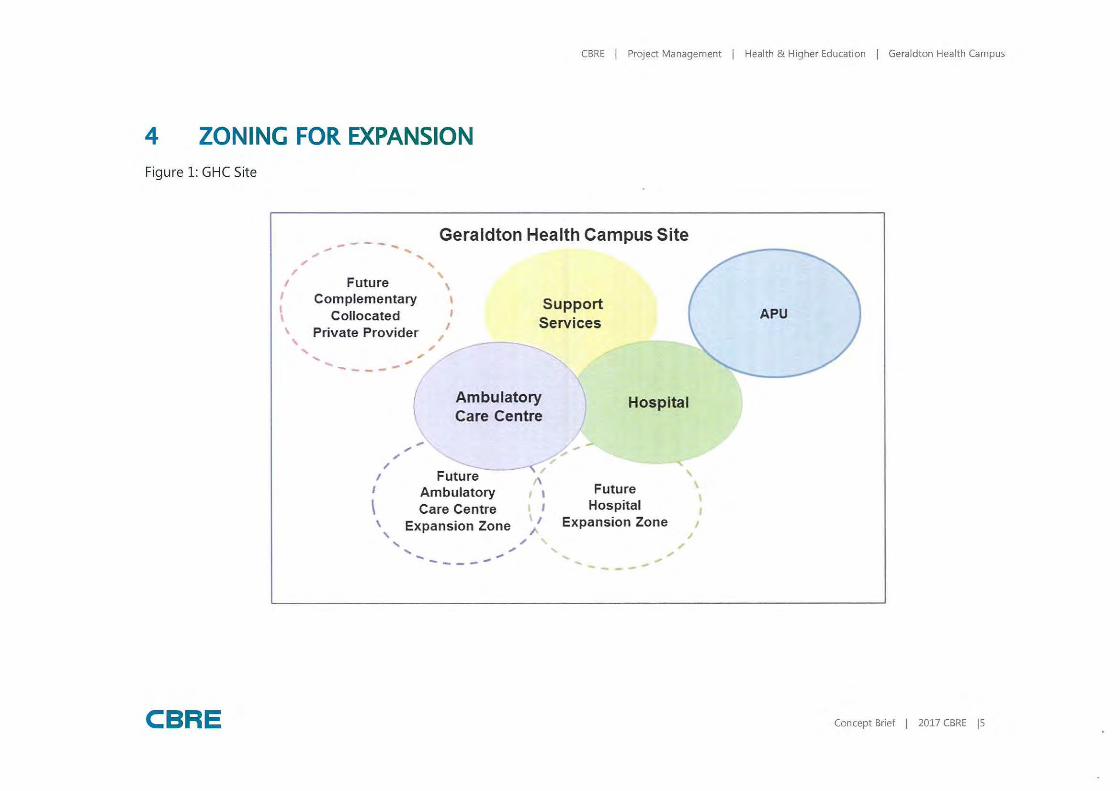
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
4 ZONING FOR EXPANSION Figure 1: GHC Site
CBRE
.,,--- - ... Geraldton Health Campus Site ., .... ..... .,. ' , '
, Future , 1 Complementary 1
\ Collocated
' Private Provider I
Support Services ,
..... ., - ., -- ---
I I
\ '
, ., .,.
Ambulatory Care Centre
....... ---< Future ,
Ambulatory Care Centre
I Expansion Zone ' .,. ' .,
/
..... ., .... ____ __
Hospital
._.. --
Future Hospital
Expansion Zone
....-· '
..... ., ... ., ------
APU
\ \
I
Concept Brief I 2017 CBRE IS
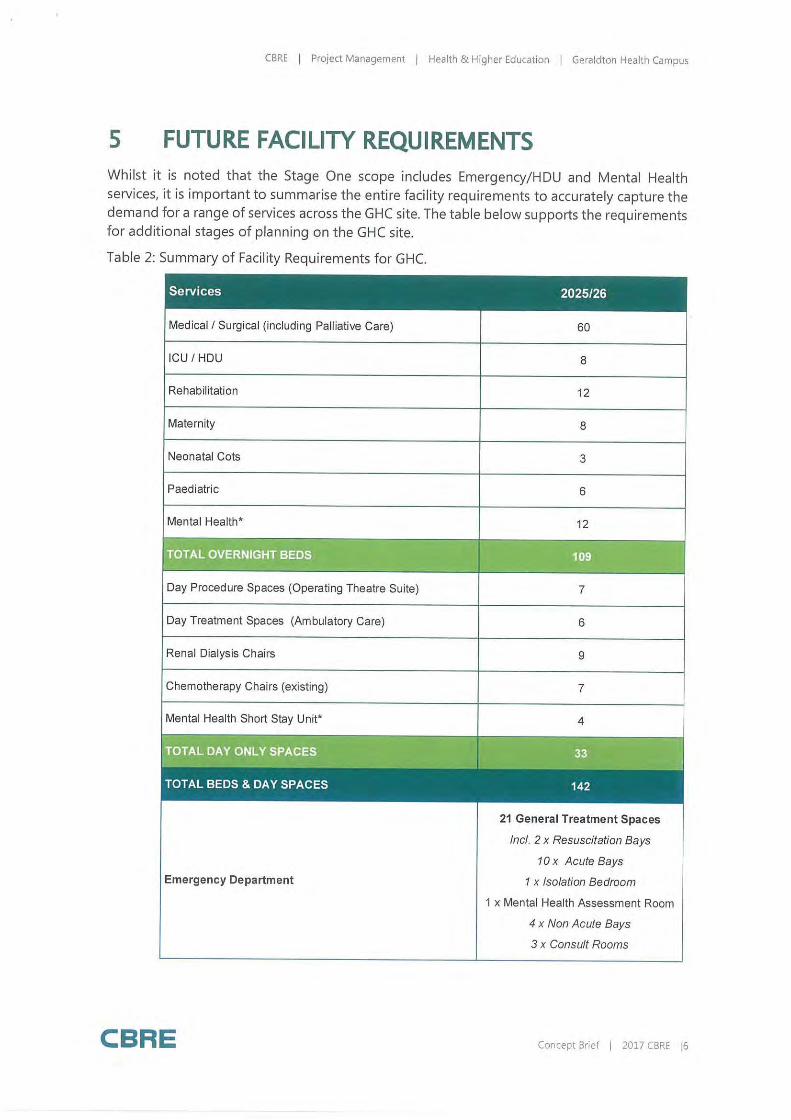
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
5 FUTURE FACILITY REQUIREMENTS Whilst it is noted that the Stage One scope includes Emergency/HOU and Mental Health services, it is important to summarise the entire facility requirements to accurately capture the demand for a range of services across the GHC site. The table below supports the requirements for additional stages of planning on the GHC site.
Table 2: Summary of Facility Requirements for GHC.
Services 2025/26
Medical I Surgical (including Palliative Care)
ICU I HOU
Rehabilitation
Maternity
Neonatal Cots
Paediatric
Mental Health*
Day Procedure Spaces (Operating Theatre Suite)
Day Treatment Spaces (Ambulatory Care)
Renal Dialysis Chairs
Chemotherapy Chairs (existing)
Mental Health Short Stay Unit*
Emergency Department
CBRE
60
8
12
8
3
6
12
, .
7
6
9
7
4
21 General Treatment Spaces
Incl. 2 x Resuscitation Bays
10 x Acute Bays
1 x Isolation Bedroom
1 x Mental Health Assessment Room
4 x Non Acute Bays
3 x Consult Rooms
Concept Brief I 2017 CBRE 16
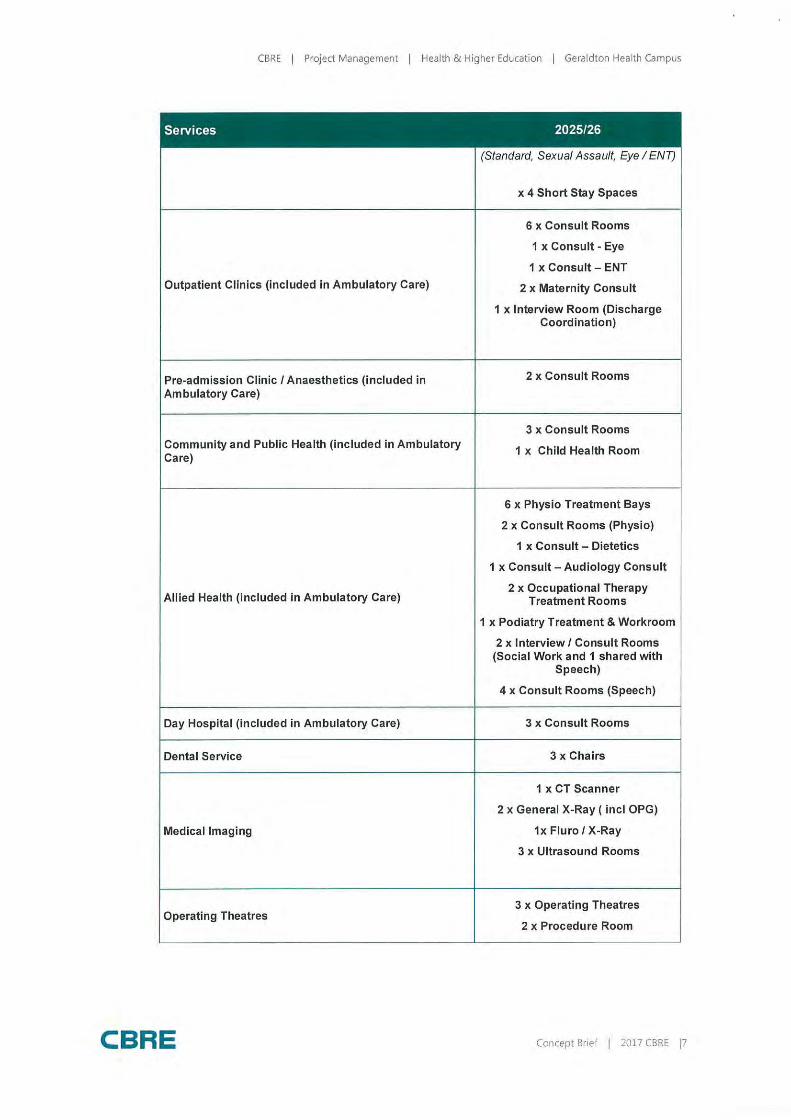
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
Services 2025/26
(Standard, Sexual Assault, Eye I ENT)
x 4 Short Stay Spaces
6 x Consult Rooms
1 x Consult - Eye
1 x Consult - ENT
Outpatient Clinics (included in Ambulatory Care) 2 x Maternity Consult
1 x Interview Room (Discharge Coordination)
Pre-admission Clinic I Anaesthetics (included in 2 x Consult Rooms
Ambulatory Care)
3 x Consult Rooms Community and Public Health (included in Ambulatory 1 x Child Health Room Care)
6 x Physio Treatment Bays
2 x Consult Rooms (Physio)
1 x Consult - Dietetics
1 x Consult - Audiology Consult
Allied Health (included in Ambulatory Care) 2 x Occupational Therapy
Treatment Rooms
1 x Podiatry Treatment & Workroom
2 x Interview I Consult Rooms (Social Work and 1 shared with
Speech)
4 x Consult Rooms (Speech)
Day Hospital (included in Ambulatory Care) 3 x Consult Rooms
Dental Service 3 x Chairs
1 x CT Scanner
2 x General X-Ray ( incl OPG)
Medical Imaging 1x Fluro IX-Ray
3 x Ultrasound Rooms
Operating Theatres 3 x Operating Theatres
2 x Procedure Room
CBRE Concept Brief I 2017 CBRE 17
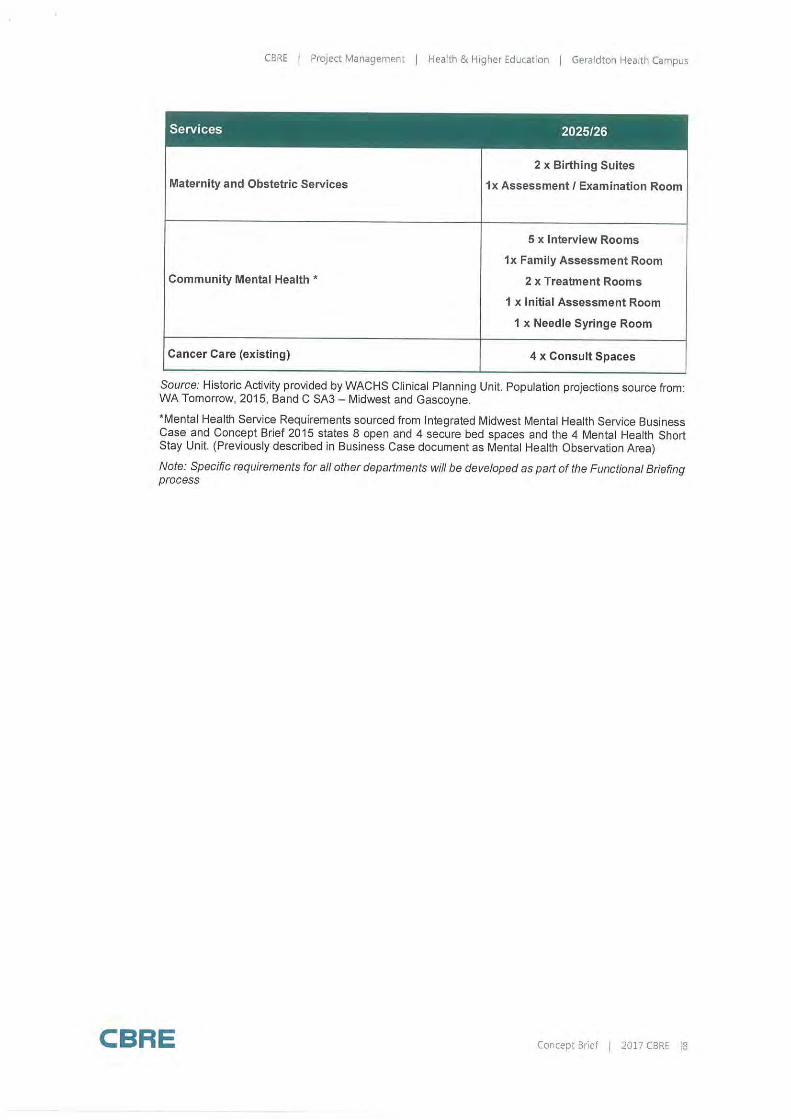
CBRE / Project Management / Health & Higher Education / Geraldton Health Campus
Services 2025/26
2 x Birthing Suites
Maternity and Obstetric Services 1x Assessment/ Examination Room
5 x Interview Rooms
1x Family Assessment Room
Community Mental Health * 2 x Treatment Rooms
1 x Initial Assessment Room
1 x Needle Syringe Room
Cancer Care (existing) 4 x Consult Spaces
Source: Historic Activity provided by WACHS Clinical Planning Unit. Population projections source from: WA Tomorrow, 2015, Band C SA3 - Midwest and Gascoyne.
*Mental Health Service Requirements sourced from Integrated Midwest Mental Health Service Business Case and Concept Brief 2015 states 8 open and 4 secure bed spaces and the 4 Mental Health Short Stay Unit. (Previously described in Business Case document as Mental Health Observation Area)
Note: Specific requirements for all other departments will be developed as part of the Functional Briefing process
CBRE Concept Brief I 2017 CBRE 18
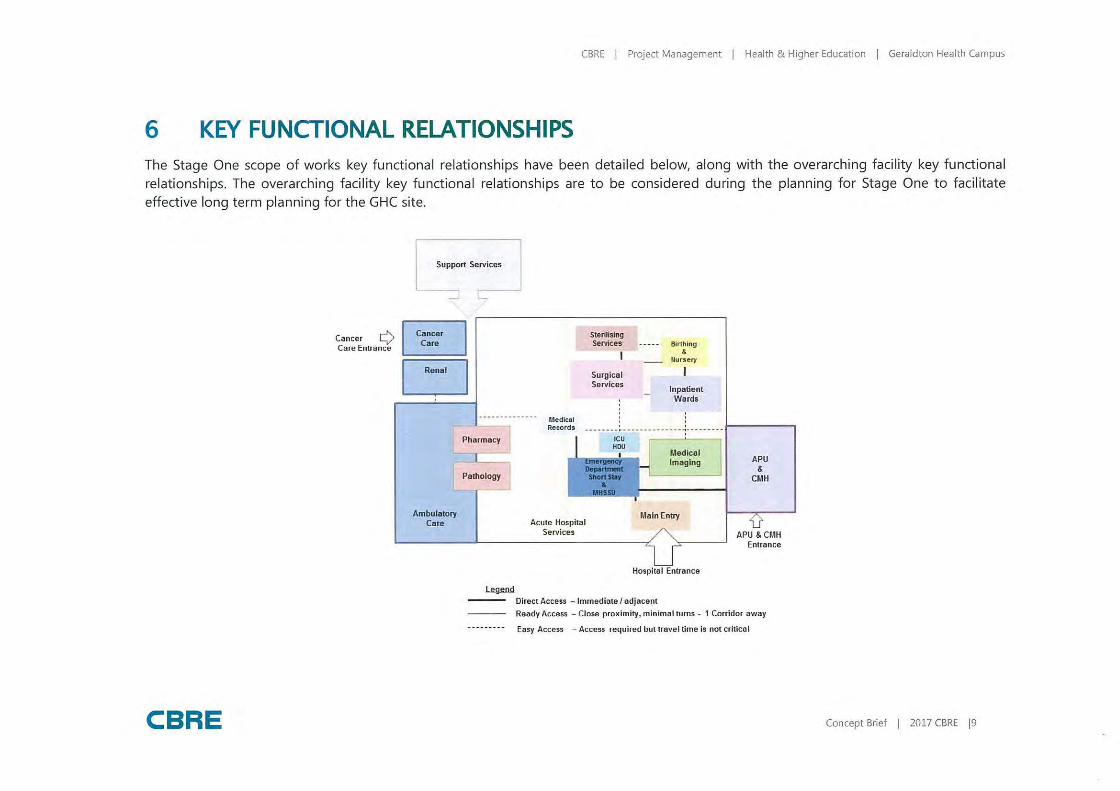
CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
6 KEY FUNCTIONAL RELATIONSHIPS The Stage One scope of works key functional relationships have been detailed below, along with the overarching facility key functional relationships. The overarching facility key functional relationships are to be considered during the planning for Stage One to facilitate effective long term planning for the GHC site.
CBRE
Cancer Q Care Entrance
Support Services
Cancer Care
[::]
Ambula10ry Care
l&9fill.l!
SteriHslng Services
Surgical Services
Birthing &
uursery
Inpatient Wards
. ' Medical Records -- ---- - - ,. __ -------------.---------
Acute Hospital Services
Medical Imaging
Main Entry
Hospital Entrance
Direct Access - Immediate / adjacent
APU &
CMH
APU & CMH Entrance
Ready Access - Close proximity, minimal turns - 1 Corridor away
Easy Access - Access required but travel time is not critical
Concept Brief I 2017 CBRE 19

CBRE I Project Management I Health & Higher Education I Geraldton Health Campus
7 SUMMARY OF SCHEDULES OF ACCOMMODATION
CBRE Concept Brief I 2017 CBRE 110
©=l®••ii•)~1:1:M•i:1-i:ja!J(etffldf11:1l@Jl~1:a-1#)(1J$l::11et•l~teJ::t~!l!Ut~nUe) GROUND FLOOR P.LAN • OP.TION 3: ED/APU/HDU/NEW ENTRY DRIVEWAt
M=!$1!1•)l•l~1:l:f!1!:ii:l§l:j;V4~t,m1j§fj~jij."h"VR!lit1)~[1]:j:iij1:j111.,~1~n~te1 GROUND FLOOR P.LAN • OP.TION 4: LARGE SCALE REDEVELOPMENT
~YiB•)~ll3111'r■@=IWfilTWl•(f;l:Jllffl~iJ•~1fflUMcJ
1ntm111.~~~IB1
,
JI /
/
, '
'
' '
'
' '
\
' \
'
' ,, '
CBRE I Proiect Management I Healfh & Higher Education I Geraldton Step up/ step down Service
Date
l.O 11 October 2017
19 October 201 7
3 .0 6 November 2017
File Location
Issued To
Natasa Spasic (MHC) Rob Pulsford (WACHS) Jeff Calver (WACHS) Michele Young (WACHS)
Natasa Spasic (MHC) Rob Pulsford (WACHS) Jeff Calver (WACHS) Michele Young (WACHS)
Natasa Spasic (MHC) Rob Pulsford (WACHS) Jeff Calver (WACHS) Michele Young (WACHS)
Remarks
I Fo, Re,iew
I Fiool
Final - in collaboration with the Mental Health Commission
I Jeonette Cooke
I Jeonette Cooke
Asha Harrison
N:\AU-SDC-AUR\Jobs\J 282 WACHS\282.4 Midwest\282.4.12 GHC Stage One\C_planning\Concept Brief\Step up Step Down\ 171106 Geraldton SUSD Service Concept Brief V3.0.docx
Corporate Details
Projed Leader
Principal Author
CBRE
Jo Thorley
Jeanette Cooke
Concept Brief I 201 7 CBRE I
CBRE I Project Management I Heolth & Higher Education I Geraldton Step up/ step down Service
TABLE OF CONTENTS Definitions
1 Introductio n ................. ....... .. .................................. ................................................ 1
1 .1 Background .................................................................. .. ......................... .... 1
l .2 Scope of Service * .................... .................................. ............................ ...... 2
1 .3 Mental Health Services System* ................................... ..... ..... ................... ..... 2
1 .4 Personal Recovery ........................................................... .. ........................... 3
1.5 Program Aim ... ..... ........... ......... ................................................................... 3
2 Vision .... .................. ... ... .. . ..................................... .. ...... .. ...... ...... ........... . .......... ..... 4
2. 1 Design Objectives ........................................................................................ 5
3 Facility Planning Requirements ........... .. ..... ........... .. .. .... ... . .... .............. .................. ... 6
4 Key Functional Relationships .... ............................................................................... 7
5 Summary Schedules of Accommodation ................... ............ .. . ......... . ...................... 8
CBRE Concept Brief I 20 l 7 CBRE I

CBRE I Pro iect Management I Health & Higher Education I Geraldton Step up/ step down Service
DEFINITIONS
WORD DEFINITION
Step up Services *
Step down Services*
Facility
I
I Services, which allow people to step up from the community, 1 and provide additional support for a person to manage a deterioration in their mental health, but where an admission to an inpatient facility is not warranted
Services , which allow people to step-down from a stay in an inpatient facility, and provide additional support to a person who no longer requires acute inpatient care but does require assistance in re-establishing themselves in the community.
For the purposes of this document and to avoid any confusion regarding the word "service", the word facility is used to describe the actual buildings that are to be designed.
It is understood that the current philosophy for Community Mental Health is moving away from a facility to a service focused model, where the emphasis is placed on consumer recovery.
*Definition sourced from Western Australian Community Mental Health Step up / step down Services. Model of Service June 2017 Document
CBRE Concept Brief I 201 7 CBRE I
CBRE I Project Management I Health & Higher Education I Geraldton Step up/ step down Service
1 INTRODUCTION
This Concept Brief summarises the overarching vision for the Geraldton step up / step down Service. It outlines the background of the project, general planning principles for facility development and proposes notional space allocations as well as key functional Models of Care that will enable the delivery of a mental health service aligned with the Mental Health Commissions step up/step down Model of Care.
The following documents have also informed the content of this Concept Brief;
•
• •
West Australian Mental Health, Alcohol and Other Drug Services Plan 2015-2025: Better Choices. Better Lives, 2015 (The Plan); The Mental Health Commission, Western Austral ian Community Mental Health Step Up/ Step down Services, Model of Service, June 2017; The Mental Health Commission, Western Australian Community Mental Health Step Up / Step down Services, Functional Brief, 2017; Midwest Integrated Mental Health Service, Service Model, November 2015; and Australasian Health Facility Guidelines, Part B - Health Facility Briefing and Planning.
This Concept Brief wi ll inform the development of the Concept Plan for this service.
1.1 Background
Central to current mental health, alcohol and other drug (AOD) reforms is the delivery of better care options for people with mental illness and alcohol and other drug problems, closer to where they live, while also reducing the pressure on hospital inpatient beds. This is consistent with the Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015-2025: Better Choices. Better lives, (the Plan) that aims to achieve a more balanced mental health system through investment in community based treatment and support services.
The Midwest Region currently does not have any purpose designed facilities to care for mental health consumers. Purpose built mental health facilities aid the treatment and recovery of the consumer by providing a "home -like" environment with particular focus on promoting general consumer wellbeing and recovery.
More community-based services are a priority for the Midwest Region as the demand for community mental health step up/step down beds in Geraldton (Midwest Region) to support and relieve the pressure on the Geraldton Health Campus is increasing. Without step up/step down beds in the community more pressure is placed on acute services with consumers presenting at hospitals as this currently is the only option available.
The Mental Health Commission (MHC) is responsible for planning, commissioning and delivering mental health and AOD services in Western Austral ia. The delivery of the Geraldton step up/step down service will involve the contracting of a clinical services provider, and a provider to deliver the psychosocial support for the 10 - bed step up/step down service proposed for Geraldton.
Step up/step down services provide people living with a mental illness an additional choice regarding the service options they can access when developing their personal recovery plans at different stages of their illness and across their lifespan. Community step up/step down services primary objectives are to:
• Provide short term mental health care in a residential setting;
CBRE Concept Brief I 201 7 CBRE I 1
CBRE I Proiect Management I Health & Higher Education I Geraldton Step up/ step down Service
• Promote recovery; and • Reduce the disability associated with mental illness.
Community step up/step down services provide a combination of psychosocial and clinical support activities that are provided within a residential domestic style setting, which are directed at delivering:
• Step up services that provide additional support for a person to manage a change in their mental health, but where admission to an inpatient facility is not warranted. In many cases this may avoid the requirement for an inpatient stay, which unfortunately due to lack of local Mental Health inpatient beds at present, involves travel to Perth or other regional areas which already have this facility in place; and
• Step down services that provide a person, who no longer requires acute inpatient care (i .e. Acute Psychiatric Unit, Hospital in the Home or the Mental Health Observation Area located in the GHC Emergency Department), with additional supports to help transition from acute care to their home, and in many cases, avoid acute readmissions and allow people to live meaningful lives in the community.
This is achieved within a framework of recovery focused rehabilitation activities that are delivered through the provision of a comprehensive suite of psychosocial programs and clinical interventions that are centred on delivering the individualised supports to improve a person's symptom control, encourage the use of personal abilities and assist their return to their usual social environment.
1 .2 Scope of Service *
The State Government has, through its Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015-2025: Better Choices. Better Lives (the Plan), made significant commitments to develop a more balanced mental health system. Central to this reform is the delivery of better care options for people with mental illness and AOD problems, closer to where they live, whi le also reducing the pressure on hospital inpatient beds.
The MHC has recognised that to meet these aims a range of services are required including providing individuals experiencing mental health problems with the support to effectively transition from in-patient settings to the community, as well as providing alternative community based options when individuals require additional support to maintain their usual way of life and reduce their need for admission in an in-patient setting.
1 .3 Mental Health Services System*
The mental health service system includes the services and supports required by the whole population to prevent mental illness, promote mental wellbeing and to provide treatment and support for individuals and their families living with a mental illness to assist in their recovery. In support of this the Plan has identified five key service streams. These are:
Prevention
Initiatives that reduce stigma, enhance mental health literacy, foster healthy community attitudes and to promoting good menta l health and wellbeing across, and at all levels of, the community.
CBRE Concept Brief I 201 7 CBRE I 2
CBRE I Project Management I Health & Higher Education [ Geraldton Step up/ sfep down Service
Community Support
Activities that support recovery for individuals, which aim to improve the quality of life and psychosocial functioning of people using mental health services, through the provision of individual and/or group-based social, recreational or prevocational activities. They are generally delivered by community managed organisations, including peer led organisations.
Community Treatment
Activities involved in the identification, assessment, treatment and ongoing management of people exhibiting mental health disorders. Treatment is largely in the form of specialist counselling, the provision of support pharmacotherapy and occupational and social support services. Services may be provided in the primary healthcare sector (GPs), through specialist community based mental health service or specialist working in the private sector (psychologist and psychiatrist).
Community Bed-Based
Provides a range of service that take into consideration the particular needs of people with a mental illness who require access to similar structured psychosocial activities, clinical support and rehabilitation programs within a residential setting. Services are primarily focused on addressing the disability dimension of mental illness and promoting personal recovery. These services are characterised by an expectation that they can offer a range of interventions, over the short, medium or long term, that assist the person to live successfully in the community of their choice. They are generally delivered by community managed organisations often in collaboration with public mental health services.
Hospital-Based
Inpatient mental health treatment, which includes emergency departments, represents the most intensive level of care where multidisciplinary assessments and multimodal interventions are provided in a secure and protected treatment environment. Individuals using these services may have length of stays that range from days to weeks. However, there are some specialist services that offer long term treatment and rehabilitation for people with persistent and severe symptoms of mental illness and may have complex presentations.
Within this context, step up/step down services are part of the Community Bed-Based Stream.
1 .4 Personal Recovery
The term recovery used in this document relates to the unique and personal process of supporting a person living with a mental illness to achieve a life that is satisfying, hopeful and contributing, and which is meaningful to them.
It is important to note that recovery is not synonymous with cure, as it refers to the internal conditions experienced by the individua l that include hope, healing, empowerment and connection.
In this context, the Community Step up / step down facility exists to support the provision of services that enable that personal Recovery journey.
1.5 Program Aim
Community Step-Up, Step-Down services provide people living with a mental illness an additional choice regarding the service options they can access when developing their personal recovery plans at different stages of their illness and across their lifespan.
CBRE Concept Brief I 2017 CBRE I 3
CBRE I Pro ject Management I Health & Higher Education I Geraldton Step up/ step down Service
Community Step-Up, Step-Down services primary ob jectives are to:
• Provide short-term mental health care, in a residential setting. • Promote recovery. • Reduce the disability associated with mental illness.
Community Step-Up, Step-Down services provide a combination of psychosocial and clinical support activities that are provided within a residential domestic style setting, w hich are directed at delivering:
Step-Up services that provide additional support for a person to manage a change in their mental health, but where an admission to an inpatient facility is not warranted ; and
Step-Down services that provide a person, who no longer requires acute inpatient care, with additional supports that assist them to re-establish themselves in the community.
This is achieved w ithin a framework of Recovery focussed rehabilitation activities that are delivered through the provision of a comprehensive suite of psychosocial programs and clinical interventions that are centred on delivering the individualised supports to improve a person's symptom control, encourage the use of personal abilities and assist their return to their usual social environment.
*Source Mental Health Commission - Functional Brief - Community Step up / step down, Planning Policy and Strategy Directorate document.
2 VISION
The future Geraldton step up / step down service w ill efficiently and safely manage the community health demand of the Midwest community enabled by service delivery that aligns with contemporary models of care.
The future Geraldton step up/ step down service aims to:
•
•
CBRE
Improve recovery outcomes for people with a mental illness; Provide care and support closer to home; Reduce avoidable admissions and re-adm issions to hospital for people living w ith
a mental illness; Provide person-centred services provided in a contemporary facility that enhances consumer recovery, safety and health outcomes Facilitate appropriate and earl ier discharge from inpatient care; Offer a balanced range of psychosocial supports and other activities that meet the individual's self-directed recovery plan; Assist individuals in developing prevention and crisis resolution strategies; Contribute to reducing the burden of care experienced by carers in supporting consumers who are unwell but do not require inpatient care; Reduce over reliance on crisis and emergency services for the provision of services more appropriately delivered in the community Ensure that the day-to-day management of services provides a safe and secure environment for service users, staff, visitors and the community; Facilitate the delivery of socially and culturally appropriate care; Improve access to services; Promote consumer self-sufficiency and care close to home Promote the expansion of recovery-focused mental health community support services; and
Concept Brief I 201 7 CBRE I 4
CBRE I Project Management I Health & Higher Education I Geraldton Step up/ step down Service
Provide updated role delineation for Community and Integrated Mental Health Services in the WA Clinical Services Framework 2014 - 2024 (community services only) .
2 . 1 Design Objectives
The design objectives are to provide a facility that:
• •
•
•
CBRE
Provides contemporary functional models of care; Provides person - centred recovery focused health care services and support; Allows Day Therapy opportunities for residents currently residing at or have recently left the service, thus providing support and opportunities for the seamless provision of continued community care; Meets contemporary design standards and aligns with national benchmarks (e.g . Australasian Health Facility Guidelines (AHFG); Supports sustainable principles - environmental, social and economic;
Wi ll assist in the attraction, recruitment and retention of clinical and non -cl inical staff and visiting specia lists; and Supports the implementation of Tel eh ea Ith initiatives and other ICT requirements
Concept Brief I 201 7 CBRE I 5
CBRE I Project Management I Health & Higher Education I Geraldton Step up/ step down Service
3 FACILITY PLANNING REQUIREMENTS
The following facility planning requirements are applicable for the Geraldton Step up / step down Service;
• Facilitate a Service Delivery driven solution; 10 Single Occupancy Units are required . These are to be designed to meet Universal Design Standards - Adaptable Housing (AS:4299) with one unit to meet Accessible Design Standards - Design for Access and Mobility (AS: 1428); The facilities are to be single storey;
• The facilities are to be designed to maximise a homely, calm and residential ambience;
• The facilities are to be built to allow for robust use whilst achieving a practical residential and de -institutionalised design;
• The Administration / Day Therapy Zone / Staff Area / Support Zones are to be incorporated together, to promote consumer focused care.
• Visual access and connection from inside facility to natural light and garden areas is required;
• Good line of sight from the communal courtyard area to all Single Occupancy Units is required;
• Facility design and landscaping must be culturally appropriate; • Access to heating and cooling equipment is required (consideration to be given
to renewable energy options); • Consider the cultural and traditional needs of people using the facility; • Both site and internal planning of the facilities is to provide clearly defined areas
for public and back of house access; A safe and secure environment is required for residents and staff with one main building entrance;
• Secure and safe work environments must be provided by minimising public access points ensuring areas can be safely shut down afterhours and at times of low staff numbers;
• Adequate and safe parking for staff, patients and visitors must be provided; • The environment must cater for visiting staff; • Low maintenance landscaping is required; • Engineering design is to support state of the art !CT;
Facility design must support contemporary standards of infection control; • Have outdoor areas that allow for social and recreational activities to take p lace;
Consider the specific needs of a wide range of people with or without physical/sensory disabilities to al low for maximum usage; Provide boundary barriers to the facility that are in keeping with the immediate surrounds but that provide safety and security for service users and staff of the service; and Have a clear and obvious point of entry to the facility either through the use of site layout, signage or pathways (or via a combination).
CBRE Concept Brief I 2017 CBRE I 6
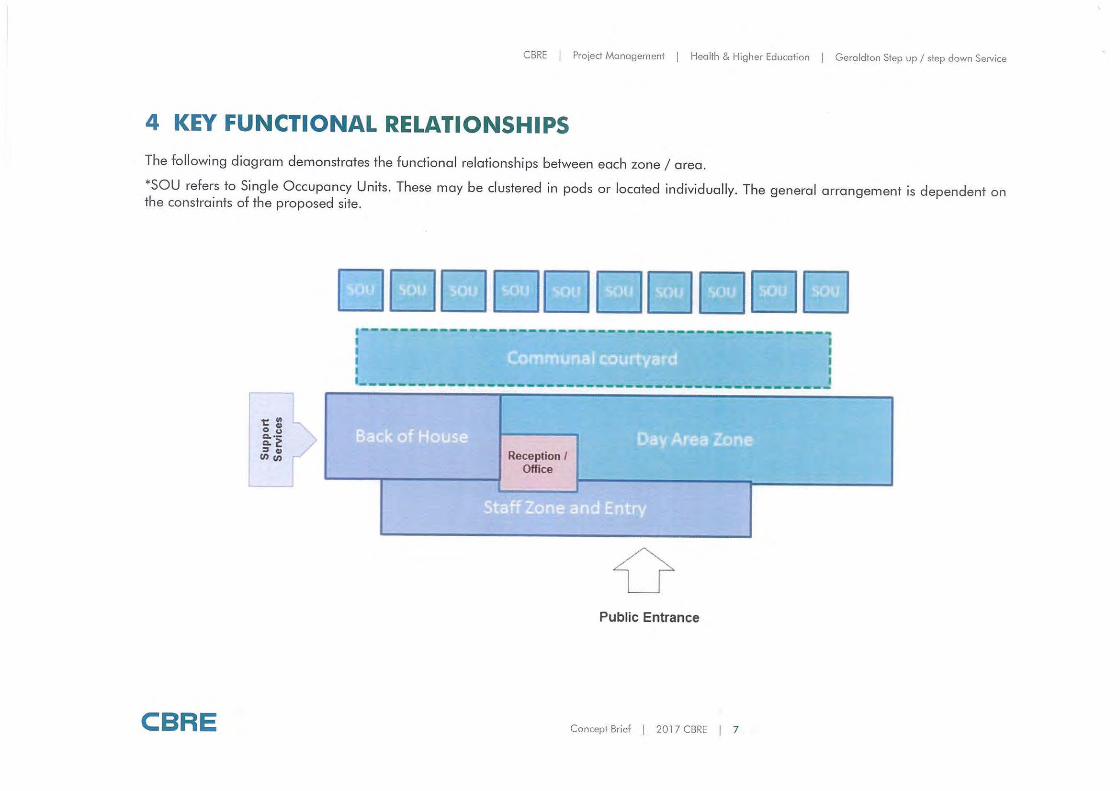
CBRE I Project Management I Health & Higher Education I Geraldton Step up/ step down Service
4 KEY FUNCTIONAL RELATIONSHIPS
The following diagram demonstrates the functional relationships between each zone/ area.
*SOU refers to Single Occupancy Units. These may be clustered in pods or located individually. The general arrangement is dependent on the constraints of the proposed site.
CBRE
~ = ... > g:·~ :::, Cl>
UJ en ,...
~,II , ·'7" II ~~ 11 ,, .. ,,,, II ~GI, ··~· II .,,,-,, I I_,,_, II ),~_,,, I ........................................... ----.-. .. -..... -.......... ._ ..... ______ ......... ._..... ................. _ ..... ~ r I I ~ ·~ . J , &'!J.illfil!] ~ ~fe]:]@ r I I --~•"Mwwwwwwwwwwww.-wwwwww..,~ .. ...,_.-wwww:iaarmwmrww _,_ _ _,.-.www ... wwwwwwwww-
Reception / Office
0 Public Entrance
Concept Brief I 2017 CBRE I 7

CBRE I Projed Management I Health & Higher Education I Gero ldton Step up/ step down Service
5 SUMMARY SCHEDULES OF ACCOMMODATION
CBRE Concept Brief I 20 l 7 CBRE I 8
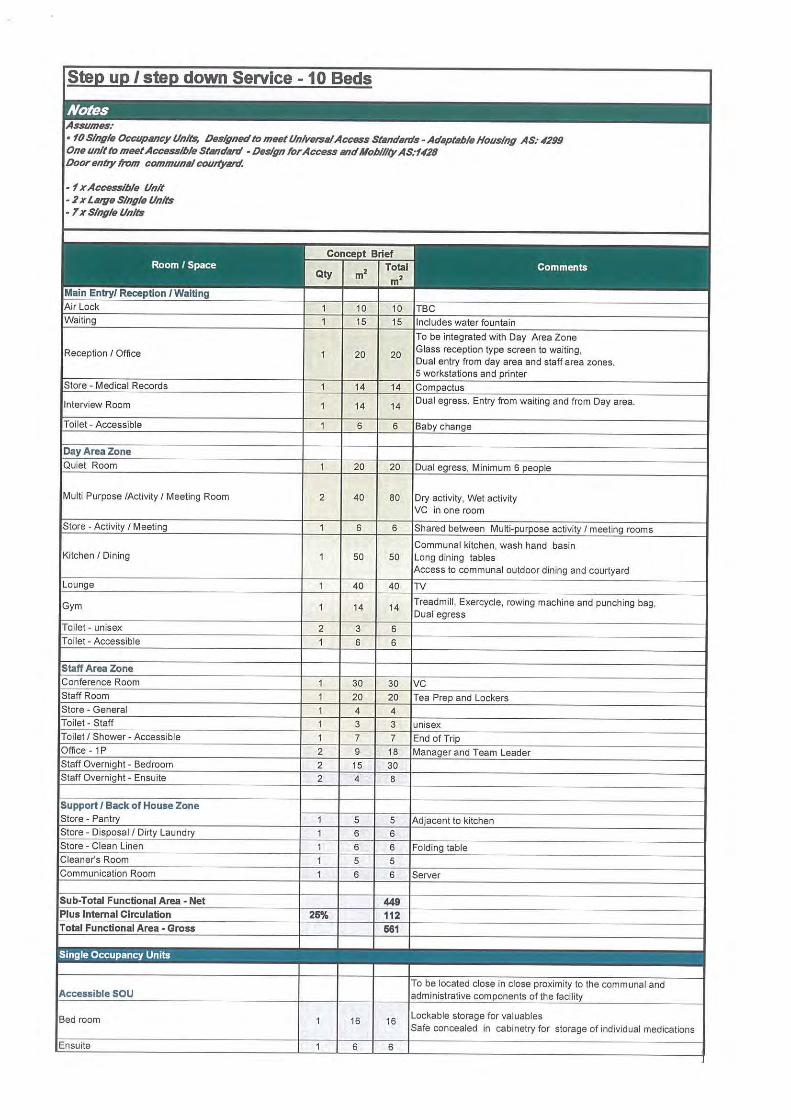
Step up/ step down Service -10 Beds
Assumes: • fO Sing!• Occupancy Units, Designed tr, mHt Un/ver.;a/ Access Standards -Adaptll/J/11 Housing AS: ,1299 On• unit tr, mHI Access/bl• Standard - D•slgn for Access and No/J/1/ty AS:U28 Door •ntry from communal cou,tyanl.
• f X Access//J/11 Unit • 2 x J.a11111 S/ng/(I Units • 7 x Single Units
Concept Brief Room/ Space
mz Total Comments
Qty mz Main Entry/ Reception/ Waiting Air Lock 1 10 10 TBC Waiting 1 15 15 Includes water fountain
To be integrated with Day Area Zone
Reception / Office 1 20 20 Glass reception type screen to waiting, Dual entry from day area and staff area zones. 5 workstations and printer
Store - Medical Records 1 14 14 Compactus
Interview Room 1 14 14 Dual egress. Entry from waiting and from Day area.
Toilet - Accessible 1 6 6 Baby change
Day Area Zone Quiet Room 1 20 20 Dual egress, Minimum 6 people
Multi Purpose /Activity/ Meeting Room 2 40 80 Dry activity, Wet activity VC in one room
Store - Activity / Meeting 1 6 6 Shared between Multi-purpose activity/ meeting rooms
Communal kitchen, wash hand basin Kitchen / Dining 1 50 50 Long dining tables
Access to communal outdoor dining and courtyard
Lounge 1 40 40 TV
Gym 1 14 14 Treadmill, Exercycle, rowing machine and punching bag, Dual egress
Toilet - unisex 2 3 6 Toilet - Accessible 1 6 6
Staff Area Zone Conference Room 1 30 30 vc Staff Room 1 20 20 Tea Prep and Lockers Store - General 1 4 4 Toilet - Staff 1 3 3 unisex Toilet/ Shower - Accessible 1 7 7 End of Trip Office - 1 P 2 9 18 Manager and Team Leader Staff Overnight - Bedroom 2 15 30 Staff Overnight - Ensuite 2 4 8
Support / Back of House Zone Store - Pantry 1 5 5 Adjacent to kitchen Store - Disposal / Dirty Laundry 1 6 6 Store - Clean Linen 1 6 6 Folding table Cleaner's Room 1 5 5 Communication Room 1 6 6 Server
Sub-Total Functional Area - Net 449 Plus Internal Circulation 26% 112 Total Functional Area • Gross 661
Single Occupancy Units
Accessible SOU To be located close in close proximity to the communal and administrative components of the facility
Bed room 1 16 16 Lockable storage for valuables Safe concealed in cabinetry for storage of individual medications
Ensuite 1 6 6
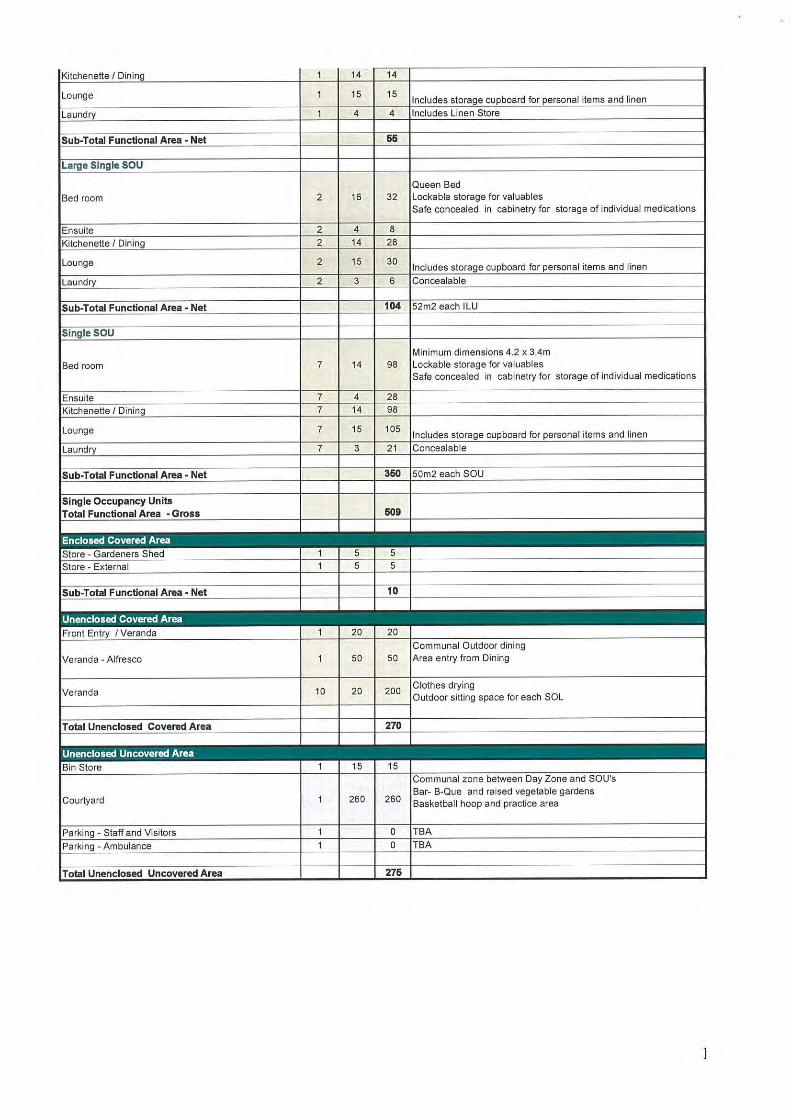
Kitchenette/ Dining 1 14 14
Lounge 1 15 15 Includes storage cupboard for personal items and linen
Laundry 1 4 4 Includes Linen Store
Sub-Total Functional Area• Net 66
Large Single SOU
Queen Bed Bed room 2 16 32 Lockable storage for valuables
Safe concealed in cabinetry for storage of individual medications
Ensuite 2 4 8
Kitchenette/ Dining 2 14 28
Lounge 2 15 30 Includes storage cupboard for personal items and linen
Laundry 2 3 6 Concealable
Sub-Total Functional Area• Net 104 52m2 each ILU
Single SOU
Minimum dimensions 4.2 x 3.4m
Bed room 7 14 98 Lockable storage for valuables Safe concealed in cabinetry for storage of individual medications
Ensuite 7 4 28 Kitchenette / Dining 7 14 98
Lounge 7 15 105 Includes storage cupboard for personal items and linen
Laundry 7 3 21 Concealable
Sub-Total Functional Area• Net 360 50m2 each SOU
Single Occupancy Units Total Functional Area • Gross 609
Enclosed Covered Area Store - Gardeners Shed 1 5 5
Store - External 1 5 5
Sub-Total Functional Area • Net 10
Unenclosed Covered Area Front Entry / Veranda 1 20 20
Communal Outdoor dining
Veranda - A lfresco 1 50 50 Area entry from Dining
Veranda 10 20 200 Clothes drying Outdoor sitting space for each SOL
Total Unenclosed Covered Area 270
Unenclosed Uncovered Area Bin Store 1 15 15
Communal zone between Day Zone and SOU's
Courtyard 1 260 260 Bar- B-Que and raised vegetable gardens Basketball hoop and practice area
Parking - Staff and Visitors 1 0 TBA
Parking - Ambulance 1 0 TBA
Total Unenclosed Uncovered Area 275

2' <
\ \
\ ~
~ :;..\
~ "t,.
t t>
\
--. --sa•
pRf111t,fE \ GAAJEN
\.-i \ •
\ ·
-
,.__ . -.-,
24 -- '"\
.;,
GERALDTON HEALTH SERVICE · STEP UP STEP DOV\'N MENTAL HEALTH UNIT EASTERN ROAD, GERALDTON SITE PLAN - OPTION 1 (10 BED)
JOB: 3081 DATE: 27110/17 SC.t.LE: 1 500~A3
LEGEND
SSOU • STANOi\RDSflGI.E OCCUP"-'CY UNIT LSOO • LARGE SINGLE OCCUPANCY UNIT ASOO · ACCESSIBLE SINGLE OCClPANCY UNIT
Q) _.,;
SK01IA