burden of foodborne diseases - who
TRANSCRIPT

World Health House
Indraprastha Estate,
Mahatma Gandhi Marg,
New Delhi-110002, India
www.searo.who.int
in the South-East Asia Region
foodborne diseasesBurden of
Globally, billions of people are at risk of foodborne diseases (FBDs) and millions
fall ill from these every year. Many die as a result of consuming unsafe food. FBDs
can also affect economic development through the tourism, agricultural and
food export industries. The South-East Asia Region has the second highest
burden of FBDs after the African Region, with more than 150 million cases and
175 000 deaths annually.
The World Health Organization has launched a comprehensive and first of
its kind report to estimate the global and regional burden of FBDs. This report will
support policy-makers in implementing the right strategies to prevent, detect and
manage foodborne risks to improve food safety. It highlights the work of WHO's
Regional Office for South-East Asia with national governments on improving
surveillance of foodborne diseases and meeting unique local challenges.
9 789290 225034
ISBN 978-92-9022-503-4


Burden of foodborne diseasesin the South-East Asia Region

© World Health Organization 2016
All rights reserved.
Requests for publications, or for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – can be obtained from SEARO Library, World Health Organization, Regional Office for South-East Asia, Indraprastha Estate, Mahatma Gandhi Marg, New Delhi 110 002, India (fax: +91 11 23370197; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
This publication does not necessarily represent the decisions or policies of the World Health Organization.
Printed in India
WHO Library Cataloguing-in-Publication data
World Health Organization, Regional Office for South-East Asia.
Burden of foodborne diseases in the South-East Asia Region.
1. Foodborne Diseases 2. Epidemiology 3. Food contamination
ISBN 978-92-9022-503-4 (NLM classification: WC 268)

iiiBurden of foodborne diseases in the South-East Asia Region
Acronyms ............................................................................................................... v
Introduction: Foodborne diseases ..........................................................................1
Foodborne infections ..................................................................................................2
Chemicals and toxins in food ......................................................................................3
Food allergy ...............................................................................................................4
Global burden of foodborne diseases .....................................................................5
Objectives ..................................................................................................................5
Methodology ..............................................................................................................6
Gaps and limitations ...................................................................................................9
Foodborne diseases in the WHO South-East Asia Region.......................................11
Foodborne diseases in under-five children ................................................................13
Conclusions and action points ...............................................................................17
Annexes
1. Classification of foodborne diseases ..............................................................21
2 A guide to national burden of foodborne disease study .................................42
3 Categorization of subgroups under WHO regions .........................................47
Contents


vBurden of foodborne diseases in the South-East Asia Region
Acronyms
CA Codex Alimentarius
DALY disability-adjusted life-year
ETEC enterotoxigenic Escherichia coli
EPEC enteropathogenic Escherichia coli
FAO Food and Agriculture Organization of the United Nations
FBDs foodborne diseases
FERG Foodborne Disease Burden Epidemiology Reference Group
GEMS Global Environmental Monitoring System
HAV hepatitis A virus
IHR (2005) International Health Regulations (2005)
INFOSAN International Food Safety Authorities Network
NTS non-typhoidal Salmonella enterica
POPs persistent organic pollutants
sp., spp. species (sing. and plural)
WHO World Health Organization


1Burden of foodborne diseases in the South-East Asia Region
Introduction: Foodborne diseases
Food is an essential requirement for humans but it can also be a vehicle of disease transmission if contaminated with harmful microbes (bacteria, viruses or parasites) or chemicals/toxins. Globally, billions of people are at risk of foodborne diseases (FBDs) and millions fall ill every year. Many also die as a result of consuming unsafe food.
Foodborne illnesses are mainly caused due to food contamination with harmful bacteria, viruses, parasites, toxins or chemicals. Microbial and chemical risks could be introduced at the farm level (e.g. using water contaminated by industrial waste or poultry farm waste for irrigation of crops). Similarly, such risks may emerge during processing, transportation or storage of food and food products.
While many FBDs may be self-limiting, some can be very serious and even result in death. These diseases may be more serious in children, pregnant women and those who are older or have a weakened immune system. Children who survive some of the more serious FBDs may suffer from delayed physical and mental development, impacting their quality of life permanently. Food allergy is another emerging problem. A brief description of major FBDs of public health importance is presented in Annex 1.
FBDs are more critical in developing countries due to various reasons, such as use of unsafe water for cleaning and processing of food, poor food production processes and food handling, absence of adequate food storage infrastructure, and inadequate or poorly enforced regulatory standards. The tropical climate in many countries in the Region also favours the proliferation of pests and naturally occurring toxins and increase the risk of contracting parasitic diseases including worm infestations.
FBDs can also affect economic development through the tourism, agriculture and food export industries. In a globalized world, FBDs do not recognize borders. A local incident can quickly become an international emergency due to the speed and range of product distribution, impacting health, international relations and trade. A brief description of foodborne diseases is presented in Annex 1.

2Burden of foodborne diseases in the South-East Asia Region
Foodborne infections
When certain disease-causing microbes (bacteria, viruses or parasites) contaminate food, they can cause foodborne illness, often called “food poisoning”. Foods that are contaminated may not look, taste or smell any different from foods that are safe to eat. Salmonella, Campylobacter, Shigella and Escherichia coli (also called E. coli) are the common bacteria that cause foodborne illnesses. Salmonella is the most common cause of foodborne illnesses and meat, egg and seafood are common food sources for much illnesses. Some foodborne bacteria like Listeria monocytogenes can even grow inside the refrigerator in ready-to-eat food. Staphylococcus aureus bacteria grow in food and produce toxins that cause staphylococcal food poisoning. Viruses that commonly cause foodborne illnesses are norovirus and hepatitis A virus (HAV), which can be transmitted through contaminated water as well as contaminated surfaces.
Foodborne bacteria are often naturally present in food and under the right conditions, a single bacterium can grow into millions of bacteria in a few hours. These bacteria multiply rapidly on foods with lots of protein or carbohydrates when food temperature is between 5 °C and 60 °C, which is often known as the “food danger zone”. Therefore, most foodborne illnesses and outbreaks are reported during the summer months.
Bacteria grow and multiply on some types of food more easily than on others. The types of foods that bacteria prefer include meat, poultry, dairy products, eggs, seafood, cooked rice, prepared fruit and salads. These foods are more likely to be infected by foodborne bacteria but other foods could also be infected or cross-contaminated by them if appropriate food safety measures are not taken during preparation, storage, transportation and handling .
The symptoms of FBDs range from mild and self-limiting (nausea, vomiting and diarrhoea with or without blood) to debilitating and life-threatening (such as kidney and liver failure, brain and neural disorders, paralysis and potentially cancers) leading to long periods of absenteeism from work and premature death. After eating tainted food, abdominal cramps, diarrhoea and vomiting can start as early as one hour or within three days depending on the foodborne pathogen, type of toxin and level of food contamination.

3Burden of foodborne diseases in the South-East Asia Region
Chemicals and toxins in food
Food adulteration and falsification are still a problem in countries of the WHO South-East Asia Region where informal food production and distribution systems are deeply entrenched at the community level. Adulteration of food is normally observed in its most crude form where prohibited substances are either added or used to partly or wholly substitute healthy ingredients or to artificially create the impression of freshness in stale food. Adulterants may be in solid form, of chemicals, or liquid and made up of colouring substances. Poisonous colouring agents like auramine, rhodomine b, malachite green and Sudan red are applied on food items for colouring, brightness and freshness. This can damage the liver and kidneys sometimes. These agents also cause stomach cancer, asthma and bladder cancer. Colouring agents such as chrome, tartazine and erythrosine are used in spices, sauces, juices, lentils and oils, causing cancer, allergy and respiratory problems. The calcium carbide of industrial grade used for fruit ripening by unscrupulous traders may contain toxic impurities such as traces of arsenic and phosphorous, which can be quite harmful for the health and can lead to various ailments..
Dioxins are byproducts of industrial processes but could also result from natural phenomena such as volcanic eruptions and forest fires. Human exposure is primarily through food – mainly meat and dairy products, fish and shellfish. These toxins accumulate in humans, especially in body fat. Dioxins are toxic to the thyroid gland and inhibit sperm production, and prolonged exposure leads to accumulation in the body. The dioxin concentration in breast milk fat directly reflects its concentration in body fat.
Mycotoxins are a group of naturally occurring chemicals produced by certain moulds or fungi. They can grow on a variety of different crops and foodstuffs including cereals, nuts, spices and dried fruits. Mycotoxins are produced by several fungi in foodstuffs and these feed during production, storage and transportation, often under warm and humid conditions. Mycotoxins of most concern from a food safety perspective include the aflatoxins, ochratoxin A, fumonisins, trichothecenes and zearalenone. Aflatoxins are most commonly found in maize and peanuts, and feed as contaminants, and these can also be found in the milk of animals that are fed aflatoxin-contaminated feed in the form of aflatoxin M1.
Most natural toxins found in fish are produced by species (spp.) of naturally occurring marine algae. They accumulate in fish when they feed on the algae or on other fish that have fed on the algae. Ciguatera fish poisoning is associated with consumption of toxin-contaminated subtropical and tropical reef fish. Unfortunately,
4Burden of foodborne diseases in the South-East Asia Region
these toxins are not destroyed by normal cooking or processing. Naturally occurring cyanogenic glycosides are found in raw or unprocessed cassava (Manihot esculenta), which can cause nerve damage or death if consumed in quantity.
Food poisoning from the consumption of poisonous wild mushrooms has been reported frequently during the monsoon season in countries of the South-East Asia Region. In some episodes, whole families have lost their lives due to consumption of poisonous wild mushrooms. The majority of fatal mushroom poisoning occurs due to ingestion of Amanita phalloides – the death cap – due to its high content of Amatoxin, a potent cytotoxin. Fatal poisoning is usually associated with delayed onset of symptoms, which are very severe and have a toxic effect on the liver, kidney and nervous system. Unfortunately, cases remain undiagnosed, under-reported and unpublished as these happen in rural communities.
Food allergy
Food allergy is an abnormal response to a food triggered by the body’s immune system. Individuals with food allergies develop symptoms by eating foods that for the vast majority of the population are part of a healthy diet. Food allergy is a growing problem. The prevalence of food allergies in the general population has been roughly estimated to be around 1–3% in adults and 4–6% in children.
Peanut or groundnut allergy occurs early in life (<five years of age) and is believed to be lifelong. Egg and milk allergies are most common food allergies among infants but are often outgrown. More than 70 foods have been described as causing food allergies. Several studies indicate that 75% of allergic reactions among children are due to a limited number of foods, namely egg, peanuts, milk, fish and nuts. Fruits, vegetables, nuts and peanuts are responsible for most allergic reactions among adults.
Food allergies are a concern for both the allergic individual and also all involved in supplying and preparing food, including family and friends, caterers, restaurants and the food industry. There is no cure for food allergies, so it is important to avoid the food that cause the allergy. Having the correct information to eat, order food and shop wisely can make a big difference. People with food allergies have to be extremely careful about what they eat. Eating away from home is often risky for an allergic person. Food allergic individuals need to know what to avoid eating. They are dependent on reliable and easy-to-find information about the ingredients of the foods they buy. Food labelling is, therefore, very important to those with food allergies as there can be potentially serious consequences.

5Burden of foodborne diseases in the South-East Asia Region
Global burden of foodborne diseases
Foodborne diseases (FBDs) are an important cause of illness and death around the world. However, the extent and cost of unsafe food, and especially the burden due to chemical and parasitic contaminants in food, is still not fully known. Epidemiological data on FBDs and laboratory capacity to detect the cause of FBDs are not available widely, particularly in the developing world. As a result, many foodborne outbreaks often go unrecognized, unreported or uninvestigated.
A major problem in addressing food safety concerns is the lack of accurate data/information regarding the extent and cost of FBDs. Lack of comprehensive data and information on the burden of FBDs makes it challenging for policy-makers to set public health priorities and allocate resources. Therefore, the World Health Organization (WHO) has taken an initiative to carry out an estimation of the global burden of FBDs and generation of evidence-based data and information that will enable policy-makers to prioritize and allocate resources for food safety.
Objectives
WHO Department of Food Safety, Zoonoses and Foodborne Diseases together with its partners launched the initiative to estimate the global burden of FBDs in 2006. The primary goal of the initiative is to enable policy-makers and other stakeholders to set appropriate, evidence-based priorities in the area of food safety. After an initial consultation, WHO established a Foodborne Disease Burden Epidemiology Reference Group (FERG) in 2007 to lead the initiative. These objectives were to:
• strengthen the capacity of Member States to conduct the burden of foodborne disease assessments and to increase the number of Member States that have undertaken a burden of foodborne disease study;

6Burden of foodborne diseases in the South-East Asia Region
• provide estimates on the global burden of FBDs according to age, sex and regions for a defined list of causative agents of microbial, parasitic and chemical origin;
• increase awareness and commitment among Member States for the implementation of food safety standards; and
• encourage Member States to use burden of foodborne disease estimates for cost-effective analyses of prevention, intervention and control measures.
Methodology
These objectives were addressed through the establishment of six task forces, each pursuing on groups of hazards or select aspects of the methodology. Together with the WHO Secretariat, these task forces commissioned systematic reviews and other studies to provide the data from which burden estimates could be calculated.
According to WHO, it was important to provide estimates of foodborne disease at as localized a level as possible because not all foodborne hazards affect every country equally. On account of gaps in the information available from certain countries (especially developing countries), subregional estimates are considered more robust as they build on the data from several countries in each Region.
The six WHO regions were divided into 14 subregions as shown in Figure 1, based on five categories considering child and adult mortality rates, as follows:
• Category A: very low child and adult mortality
• Category B: low child mortality and very low adult mortality
• Category C: low child mortality and high adult mortality
• Category D: high child and adult mortality
• Category E: high child mortality and very high adult mortality

7Burden of foodborne diseases in the South-East Asia Region
Figure 1: Categorization of subgroups under WHO regions for estimation of global burden of foodborne diseases
Source: FERG Report (2015)
The list of countries that were divided into 14 subregions is available in Annex 3. A country can obtain national estimates by referring to estimates for the subregion to which it belong.
In addition to providing global and regional estimates, the initiative also sought to promote actions at a national level. This involved capacity-building through national foodborne disease burden studies, and encouraging the use of information on the burden of disease in setting evidence-informed policies. A suite of tools and resources were created to facilitate national studies on the burden of foodborne diseases and pilot studies were conducted in four countries (Albania, Japan, Thailand and Uganda).
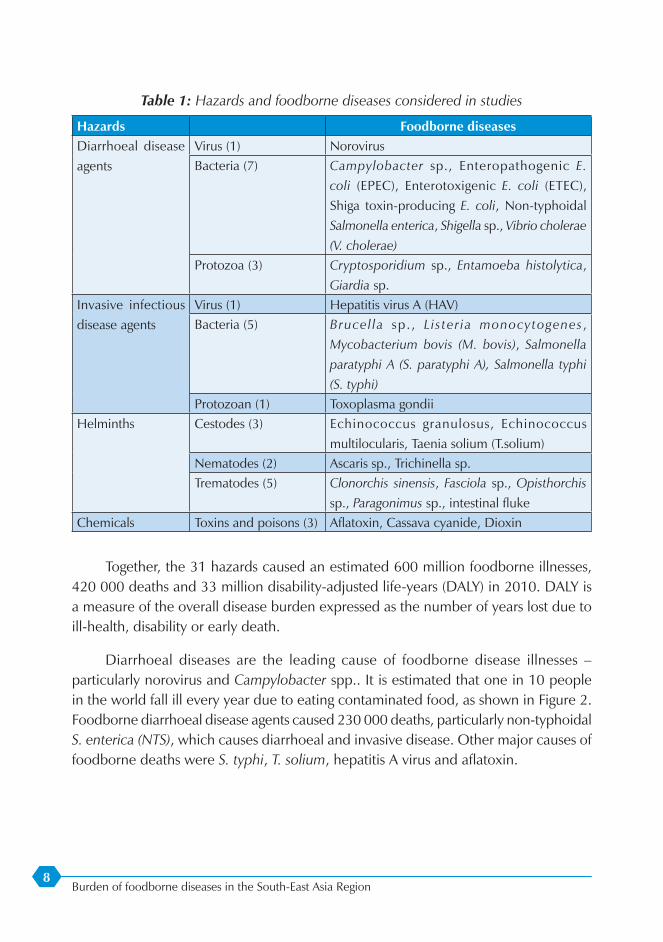
Thirty-one foodborne hazards causing 32 diseases with 11 diarrhoeal disease agents (1 virus, 7 bacteria and 3 protozoa), 7 invasive infectious disease agents (1 virus, 5 bacteria and 1 protozoa), 10 helminths and 3 chemicals are included (as shown in Table 1).
8Burden of foodborne diseases in the South-East Asia Region
Table 1: Hazards and foodborne diseases considered in studies
Hazards Foodborne diseasesDiarrhoeal disease agents
Virus (1) NorovirusBacteria (7) Campylobacter sp., Enteropathogenic E.
coli (EPEC), Enterotoxigenic E. coli (ETEC), Shiga toxin-producing E. coli, Non-typhoidal Salmonella enterica, Shigella sp., Vibrio cholerae (V. cholerae)
Protozoa (3) Cryptosporidium sp., Entamoeba histolytica, Giardia sp.
Invasive infectious disease agents
Virus (1) Hepatitis virus A (HAV)Bacteria (5) Brucel la sp. , Lister ia monocytogenes ,
Mycobacterium bovis (M. bovis), Salmonella paratyphi A (S. paratyphi A), Salmonella typhi (S. typhi)
Protozoan (1) Toxoplasma gondiiHelminths Cestodes (3) Echinococcus granulosus, Echinococcus
multilocularis, Taenia solium (T.solium) Nematodes (2) Ascaris sp., Trichinella sp.Trematodes (5) Clonorchis sinensis, Fasciola sp., Opisthorchis
sp., Paragonimus sp., intestinal flukeChemicals Toxins and poisons (3) Aflatoxin, Cassava cyanide, Dioxin
Together, the 31 hazards caused an estimated 600 million foodborne illnesses, 420 000 deaths and 33 million disability-adjusted life-years (DALY) in 2010. DALY is a measure of the overall disease burden expressed as the number of years lost due to ill-health, disability or early death.
Diarrhoeal diseases are the leading cause of foodborne disease illnesses – particularly norovirus and Campylobacter spp.. It is estimated that one in 10 people in the world fall ill every year due to eating contaminated food, as shown in Figure 2. Foodborne diarrhoeal disease agents caused 230 000 deaths, particularly non-typhoidal S. enterica (NTS), which causes diarrhoeal and invasive disease. Other major causes of foodborne deaths were S. typhi, T. solium, hepatitis A virus and aflatoxin.

9Burden of foodborne diseases in the South-East Asia Region
Figure 2: Burden of foodborne illness
1 in 10 people in the world fall ill every year due to eating contaminated food
Source: FERG Report (2015)
The global burden of FBDs is considerable with marked regional variations. The burden of FBDs is borne by individuals of all ages, but particularly children under five years of age and persons living in low-income regions of the world. Nearly 40% of the foodborne disease burden was among children under five years of age with 18 million DALY lost due to foodborne diarrhoeal disease agents, particularly NTS and EPEC. Other foodborne hazards with a substantial contribution to the global burden included S. typhi and T. solium.
Gaps and limitations
Estimates are based on the best available data at the time of reporting. Identified data gaps were filled using imputation, assumptions and other methods.
Data gaps were a major hurdle to making estimates of the foodborne disease burden in these national studies. The global and regional estimates provided by FERG offer an interim solution until improved surveillance and laboratory capacity is developed.
It is likely that the true number of illnesses and deaths resulting from FBDs worldwide is even higher because:
• many cases of food poisoning go unrecognized and untreated,
• there are gaps in the collection and reporting of data (especially in developing countries) on the burden of FBDs,
• there are other causes beyond the 31 hazards included in this report, especially in the chemical domain,
• for certain foodborne hazards, there is still considerable uncertainty regarding their clinical impact. Current estimates only included symptoms for which sufficient evidence existed.

10Burden of foodborne diseases in the South-East Asia Region
WHO is focusing its efforts on supporting national policy-makers and governments in improving surveillance of FBDs to obtain a clearer picture of the unique local challenges and implement the right strategies to prevent, detect and manage foodborne risks.
The report prepared by the WHO Foodborne Disease Burden Epidemiology Reference Group provides the first estimates of global foodborne disease in terms of incidence, mortality and disease burden in the form of DALY. This report is the outcome of 10 years of monumental work by WHO and its donors and partners as well as a number of individuals contributing to this initiative from around the world. The report is an essential part of WHO’s efforts to facilitate global prevention, detection and response to public health threats associated with unsafe food. It is a continuation of WHO activities dedicated to driving food safety as highlighted during World Health Day 2015.
An important goal of the FERG initiative and the next step in the process is to encourage and support countries in undertaking foodborne burden of disease studies, using consistent WHO tools and processes. Therefore, a guide to national burden of foodborne diseases study has been briefly mentioned in Annex 2.

11Burden of foodborne diseases in the South-East Asia Region
Foodborne diseases in the WHO South-East Asia Region
Home to a quarter of the world’s population, the WHO South-East Asia Region has the second highest burden of FBDs per population among WHO regions. It has more than half of the global infections and deaths due to typhoid fever or hepatitis A.
Based on data (2010) from the FERG report, the annual burden of FBDs in the South-East Asia Region includes more than:
• 150 million illnesses
• 175 000 deaths
• 12 million DALYs.
Figure 3: Top 10 causes of foodborne illnesses in the WHO South-East Asia Region
0 5 million 10 million 15 million 20 million 25 million
Salmonella typhi
Ascaris species
Entamoeba histolytica
Hepatitis A virus
Enteropathogenic E. coli
Norovirus
Non-typhoidal S. enterica
Enterotoxigenic E. coli
Shigella species
Campylobacter species
Source: FERG Report (2015)

12Burden of foodborne diseases in the South-East Asia Region
As shown in Figure 3, Campylobacter sp. was the leading cause of foodborne illness with an estimated more than 20 million cases every year in the Region. This was followed by Shigella sp. and enterotoxigenic Escherichia coli with more than 19 million cases each. At the fourth spot, NTS was estimated to cause more than 16 million infections.
In aggregate terms, E. coli and S. spp. were the leading causes of foodborne illnesses. Norovirus and hepatitis A virus also caused significant diseases in the Region. Amoebiasis caused by Entamoeba histolytica and worm infestation by Ascaris sp. were the leading parasitic causes of illness due to contaminated food.
Figure 4: Top 10 causes of deaths due to foodborne illnesses in the WHO South-East Asia Region
0 5 000 10 000 15 000 20 000 25 000 30 000 35 000
Campylobacter spp.
Taenia solium
Salmonella paratyphi A
Vibrio cholerae
Enterotoxigenic E. coli
Enteropathogenic E. coli
Non-typhoidal S. enterica
Hepatitis A virus
Norovirus
Salmonella typhi
Source: FERG Report (2015)
As shown in Figure 4, the leading cause of death due to foodborne diseases in the Region was S. typhi (more than 32 000 deaths), followed by norovirus (nearly 19 000 deaths) and hepatitis A virus (nearly 18 000 deaths) respectively. NTS at fourth position was responsible for nearly 16 000 deaths in the Region. EPEC and ETEC caused more than 15 000 and 10 000 deaths respectively. Cholera (caused by V. cholerae) and paratyphoid fever (caused by S. paratyphi A) were estimated to have caused more than 7600 and nearly 7500 deaths respectively.
Among the parasites, the pork tapeworm (T. solium) was estimated to cause more than 6800 deaths annually. Despite being the leading cause of foodborne illness in the Region, Campylobacter sp. caused only 6700 deaths here.

13Burden of foodborne diseases in the South-East Asia Region
Going by the estimated burden of FBDs in terms of DALYs in the Region as shown in Figure 5, S. typhi is the leading cause of ill-health, disability or early death and leads to the highest number of DALYs (nearly 2.3 million). S. paratyphi A that causes a similar illness was also estimated to be responsible for more than half a million DALYs every year.
Figure 5: Top 10 causes of DALYs due to foodborne illnesses in the WHO South-East Asia Region
0 0.5 million 1 million 1.5 million 2 million 2.5 million
Salmonella paratyphi A
Vibrio cholerae
Campylobacter spp.
Taenia solium
Enterotoxigenic E. coli
Hepatitis A virus
Non-typhoidal S. enterica
Enteropathogenic E. coli
Norovirus
Salmonella typhi
Source: FERG Report (2015)
Viral causes of foodborne diseases – norovirus and hepatitis A virus were estimated to be responsible for nearly 1.3 million and 870 000 DALYs every year.
Interestingly, non-typhoidal S. enterica continued to occupy the fourth position among the top 10 causes of DALYs and was estimated to be responsible for more than a million DALYs. EPEC and ETEC were responsible for nearly 1.2 million and 760 000 DALYs respectively.
The pork tapeworm was responsible for nearly 670 000 DALY and Campylobacter sp. and cholera led to 600 000 and 530 000 DALY respectively.
Foodborne diseases in under-five children
The burden of FBDs in children under five years of age is quite high in the Region as compared with other WHO regions. As shown in Figure 6, three out of 10 children suffer from diarrhoea in South-East Asia.

14Burden of foodborne diseases in the South-East Asia Region
Figure 6: Under-five children suffering from diarrhoea in the WHO South-East Asia Region
3 in 10 children under five years of age suffer from diarrhoea
Source: FERG Report (2015)
The Region contributes to one third of the global deaths due to diarrhoea in children under five years of age that could be prevented.
Figure 7: Top 10 causes of foodborne illnesses in children under five years of age in the South-East Asia Region
0 2 million 4 million 6 million 8 million 10 million 12 million
Entamoeba histolytica
Hepatitis A virus
Giardia spp.
Ascaris spp.
Non-typhoidal S. enterica
Norovirus
Shigella spp.
Campylobacter spp.
Enteropathogenic E. coli
Enterotoxigenic E. coli
Source: FERG Report (2015)
In children under five years of age (as shown in Figure 7), the top three causes of foodborne illnesses were ETEC (nearly 11 million cases), EPEC (nearly 7.3 million cases) and Campylobacter sp. (nearly 7 million cases).
Shigella sp., norovirus and NTS caused 5.2, 5 and 4.4 million illnesses respectively and hepatitis A virus caused nearly 1.4 million cases in children under five years of age.
Among parasitic infections in under-five children, round worm (Ascaris sp.), giardiasis (Giardia sp.) and amoebiasis (Entamoeba histolytica) caused nearly 3, 1.8 and 1 million illnesses respectively.
15Burden of foodborne diseases in the South-East Asia Region
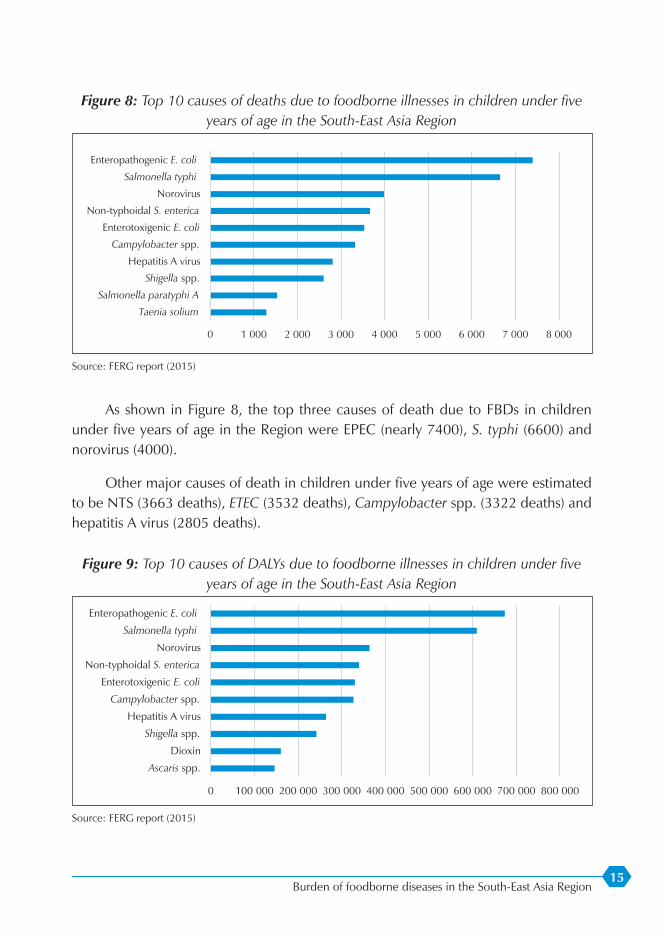
Figure 8: Top 10 causes of deaths due to foodborne illnesses in children under five years of age in the South-East Asia Region
0 1 000 2 000 3 000 4 000 5 000 6 000 7 000 8 000
Taenia solium
Salmonella paratyphi A
Shigella spp.
Hepatitis A virus
Campylobacter spp.
Enterotoxigenic E. coli
Non-typhoidal S. enterica
Norovirus
Salmonella typhi
Enteropathogenic E. coli
Source: FERG report (2015)
As shown in Figure 8, the top three causes of death due to FBDs in children under five years of age in the Region were EPEC (nearly 7400), S. typhi (6600) and norovirus (4000).
Other major causes of death in children under five years of age were estimated to be NTS (3663 deaths), ETEC (3532 deaths), Campylobacter spp. (3322 deaths) and hepatitis A virus (2805 deaths).
Figure 9: Top 10 causes of DALYs due to foodborne illnesses in children under five years of age in the South-East Asia Region
0 100 000 200 000 300 000 400 000 500 000 600 000 700 000 800 000
Ascaris spp.
Dioxin
Shigella spp.
Hepatitis A virus
Campylobacter spp.
Enterotoxigenic E. coli
Non-typhoidal S. enterica
Norovirus
Salmonella typhi
Enteropathogenic E. coli
Source: FERG report (2015)

16Burden of foodborne diseases in the South-East Asia Region
In terms of DALY due to FBDs in children under five years of age (as shown in Figure 9), the leading cause was EPEC (nearly 674 000 DALY), followed by S. typhi (610 000 DALY) and norovirus (nearly 364 000 DALY).
Other causes of DALYs include NTS, ETEC, Campylobacter sp. hepatitis A virus, Shigella sp. and dioxin. Interestingly, dioxin was estimated to have a significant impact in children under five years of age in the Region with more than 160 000 DALYs. It was based on the result of breast milk testing for a persistent organic pollutants (POPs) study carried out in India under the Global Environmental Monitoring System (GEMS).

17Burden of foodborne diseases in the South-East Asia Region
Conclusions and action points
The most comprehensive report to date on the impact of contaminated food on health and well-being is titled ‘Estimates of the Global Burden of Foodborne Diseases’. These estimates are the result of a decade of work, including inputs from more than 100 experts from around the world. Based on what we know now, it is apparent that the global burden of FBDs is considerable. The FERG report highlights the global threat posed by FBDs in the context of globalization of the food trade. Unsafe food endangers everyone and billions of people are at risk.
The global burden of FBDs is considerable with marked regional variations. The burden of FBDs is borne by individuals of all ages, and particularly children under five years of age and persons living in low-income regions of the world. These estimates are conservative; further studies are needed to address the data gaps and limitations of this study. The considerable difference in the burden of foodborne disease between low- and high-income regions suggests that a major proportion of the current burden is avoidable and that control methods do exist.
The report highlights that action to reduce illnesses and deaths from FBDs must be tailored according to regional and national needs as the types of contaminants and reasons for their prevalence differ across the world. The report will support policy-makers in implementing the right strategies to prevent, detect and manage foodborne risks to improve food safety.
The report will enable governments achieve the Sustainable Development Goal 2 for food security and nutrition (target 2.1: “By 2030, end hunger and ensure access by all people, in particular the poor and people in vulnerable situations, including infants, to safe, nutritious and sufficient food all year round”). The achievement of Goal 3 (Ensure healthy lives and promote well-being for all at all ages); Goal 1 (End Poverty in all its forms everywhere) and Goal 8 (Promote sustained, inclusive and sustainable

18Burden of foodborne diseases in the South-East Asia Region
economic growth, full and productive employment and decent work for all) will also be cited through promoting the safety of food supply domestically and internationally.
The report also reinforces the need for governments, the food industry and individuals to do more to make food safe and prevent foodborne illnesses and intoxications. Safe drinking water, good hygienic practices and improved sanitation are keys for preventing foodborne illnesses and intoxications.
The majority of FBDs and deaths are preventable. Food safety is a public health priority and governments should develop policies and regulatory frameworks to establish and implement effective food safety systems. Food safety systems should ensure that food producers and suppliers along the whole food chain operate responsibly and supply safe food to consumers.
Food safety is a shared responsibility. All food operators and consumers should understand the roles they must play to protect their health and that of the wider community. All stakeholders can contribute to improvements in food safety throughout the food chain by incorporating these estimates into policy development at the national and international levels.
Think globally, act locally: while there is no single, global solution to the problem of FBDs, a strengthened food safety system in one country will positively impact the safety of food in other countries. There is need for coordinated, cross-border action across the entire food supply chain.
Coordinated action at the global, regional and national levels is needed to address risks of FBDs and ensure food safety. Education and training are needed on prevention of FBDs among food producers, suppliers, handlers and the general public, including women and school children.
Key action points towards ensuring food safety in the Region include the conduct of national studies on the burden of FBDs, strengthening of laboratory capacity to be able to detect FBDs, and strengthening the surveillance of FBDs, including the collation of local data to validate regional estimates and translation of estimates of FBDs into food safety policy.
The International Health Regulations (IHR 2005) is a legally binding instrument to ensure global health security. It calls upon WHO Member States to build core capacities for implementation of IHR (2005), including food safety events. The evaluation of IHR self-assessment done by 11 Member States of the WHO South-East Asia Region in

19Burden of foodborne diseases in the South-East Asia Region
2015 clearly illustrates that most Member States have limited capacity for surveillance, assessment and management of priority food safety events. Therefore, the WHO Regional Office for South-East Asia is providing technical support to Member States to evaluate existing national foodborne disease surveillance systems, including risk assessment and the management of food safety events, and to identify action plans to improve surveillance, assessment and management of priority FBDs and food safety events.
WHO is working with governments and partners to reduce the level of food contamination throughout different stages of the food-chain. These stages include the point of final consumption to the levels at which the exposure to pathogens and contaminants does not pose significant risks for human health.
WHO promotes the use of international platforms such as the joint WHO-FAO (Food and Agriculture Organization of the United Nations) International Food Safety Authorities Network (INFOSAN) to ensure effective and rapid communication during food safety emergencies. WHO also works closely with other international organizations to ensure food safety along the entire food-chain, from production to consumption, in line with the Codex Alimentarius (CA). CA is a collection of international food standards, guidelines and codes of practice covering all main foods and steps in the food supply chain.
FBDs are preventable. WHO is promoting the important role that everyone can play to promote food safety through systematic disease prevention and awareness programmes. WHO’s Five Keys to Safer Food explains the basic principles that each individual should know all over the world to prevent FBDs:
(1) Keep clean
– thoroughly wash raw fruits and vegetables with tap water.
– keep clean hands, kitchen and chopping board all the time.
(2) Separate raw and cooked food
– do not mix raw food and ready-to-eat food.
– do not mix raw meat, fish and raw vegetables.
(3) Cook thoroughly
– thoroughly cook all meat, poultry and seafood, especially shellfish.
– reheat all leftovers until they are steaming hot.

20Burden of foodborne diseases in the South-East Asia Region
(4) Keep food at safe temperatures
– refrigerate cooked food within two hours of preparation.
– never defrost food at room temperature; defrost frozen food in the refrigerator, cold water or the microwave.
(5) Use safe water and raw materials
– use safe drinking water for food preparation.
– check use-by dates and labels while buying packed food.

21Burden of foodborne diseases in the South-East Asia Region
Anne
x 1
Cla
ssifi
catio
n of
food
born
e di
seas
es1
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
1. In
itial
or m
ajor
sig
ns a
nd s
ympt
oms
of th
e up
per d
iges
tive
trac
ts (n
ause
a, v
omiti
ng)
1.1
Incu
batio
n pe
riod
tend
s to
be
less
than
1 h
our
Fung
al a
gent
s
Poiso
ning
by
mus
hroo
ms o
f the
gr
oup
that
cau
ses
gastr
oint
estin
al ir
ritat
ion
Poss
ibly
resin
-type
su
bsta
nces
foun
d in
som
e ty
pes o
f m
ushr
oom
s
From
30
min
utes
to
2 h
ours
Nau
sea,
vom
iting
, re
tchi
ng, d
iarrh
oea,
ab
dom
inal
pai
ns
Man
y va
rietie
s of
wild
mus
hroo
ms
Vom
itIn
gesti
on o
f unk
now
n to
xic
varie
ties o
f m
ushr
oom
s, th
roug
h co
nfus
ion
with
oth
er
edib
le v
arie
ties
Chem
ical
age
nts
Antim
ony
poiso
ning
Antim
ony
in
enam
elle
d iro
n ut
ensil
s
From
a fe
w
min
utes
to 1
hou
rVo
miti
ng, a
bdom
inal
pa
ins,
diar
rhoe
aVe
ry a
cid
food
and
be
vera
ges
Vom
it, st
ool a
nd
urin
eU
se o
f ute
nsils
that
co
ntai
n an
timon
y, sto
rage
of v
ery
acid
fo
od in
ena
mel
led
iron
uten
sils
Cadm
ium
poi
soni
ngCa
dmiu
m in
pla
ted
uten
sils
From
15
to 3
0 m
inut
esN
ause
a, v
omiti
ng,
abdo
min
al p
ains
, di
arrh
oea,
shoc
k
Very
aci
d fo
ods
and
drin
ks, c
andi
es
and
othe
r cak
e de
cora
tions
Vom
it, st
ool,
urin
e an
d bl
ood
Use
of u
tens
ils th
at
cont
ain
cadm
ium
, sto
rage
of v
ery
acid
fo
od in
con
tain
ers t
hat
cont
ain
cadm
ium
, in
gesti
on o
f foo
ds th
at
cont
ain
cadm
ium
2
1 Ad
apte
d an
d m
odifi
ed fr
om In
stitu
to P
anam
eric
ano
de P
rote
cció
n de
Alim
ento
s y Z
oono
sis (I
NPP
AZ) –
Pan
Am
eric
an H
ealth
Org
aniz
atio
n W
HO
2
Sam
ples
shou
ld b
e co
llect
ed fr
om a
ny o
f the
liste
d fo
ods t
hat h
ave
been
inge
sted
durin
g th
e in
cuba
tion
perio
d of
the
dise
ase.

22Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Copp
er p
oiso
ning
Copp
er in
pip
es
and
uten
sils
From
a fe
w
min
utes
to a
few
ho
urs
Met
allic
taste
, na
usea
, vom
iting
(g
reen
vom
it),
abdo
min
al p
ains
, di
arrh
oea
Very
aci
d fo
od a
nd
beve
rage
sVo
mit,
gas
tric
lava
ge, u
rine
and
bloo
d
Stor
age
of v
ery
acid
fo
od in
cop
per u
tens
ils
or u
se o
f cop
per t
ubin
g in
serv
ing
very
aci
d be
vera
ges,
defe
ctiv
e va
lves
on
devi
ces
to p
reve
nt re
flux
(in
disp
ense
rs)
Fluo
ride
poiso
ning
(fl
uoro
sis)
Sodi
um fl
uorid
e in
in
sect
icid
esFr
om a
few
m
inut
es to
2 h
ours
Salty
or s
oapy
ta
ste, n
umbn
ess
in th
e m
outh
, vo
miti
ng, d
iarrh
oea,
ab
dom
inal
pai
ns,
pallo
ur, c
yano
sis,
dila
ted
pupi
ls,
spas
ms,
colla
pse,
sh
ock
Any
acci
dent
ally
co
ntam
inat
ed
food
, par
ticul
arly
dr
y fo
od su
ch a
s po
wde
red
milk
, flo
ur, b
akin
g po
wde
r and
cak
e m
ixes
Vom
it an
d ga
stric
la
vage
sSt
orag
e of
inse
ctic
ides
in
the
sam
e pl
ace
as fo
od,
conf
usio
n of
pes
ticid
es
with
pow
dere
d fo
ods
Lead
poi
soni
ngLe
ad c
onta
ined
in
earth
enw
are
pots,
pe
stici
des,
pain
ts,
plas
ter a
nd p
utty
30 m
inut
es o
r m
ore
Met
allic
taste
, bu
rnin
g in
the
mou
th, a
bdom
inal
pa
ins,
milk
y vo
mit,
bl
ack
stool
or
pres
ence
of b
lood
, ba
d br
eath
, sho
ck,
blue
line
at t
he e
dge
of g
ums (
"lead
line
")
Very
aci
d fo
od
and
beve
rage
s sto
red
in v
esse
ls co
ntai
ning
lead
, an
y ac
cide
ntal
ly
cont
amin
ated
food
Vom
it, g
astri
c la
vage
s, sto
ol,
bloo
d an
d ur
ine
Use
of v
esse
ls co
ntai
ning
le
ad, s
tora
ge o
f ver
y ac
id fo
od in
ves
sels
cont
aini
ng le
ad, s
tora
ge
of p
estic
ides
in th
e sa
me
plac
e as
food
Tin
poiso
ning
Tin
in ti
n ca
nsFr
om 3
0 m
inut
es
to 2
hou
rsSw
ellin
g, n
ause
a,
vom
iting
, abd
omin
al
pain
s, di
arrh
oea,
he
adac
he
Very
aci
d fo
ods a
nd
beve
rage
sVo
miti
ng, s
tool
, ur
ine
and
bloo
dSt
orag
e of
aci
d fo
ods i
n un
lined
tin
cont
aine
rs
Zinc
poi
soni
ngZi
nc in
gal
vani
zed
cont
aine
rsFr
om a
few
m
inut
es to
2 h
ours
Mou
th a
nd
abdo
min
al p
ains
, na
usea
, vom
iting
, di
zzin
ess
Very
aci
d fo
od a
nd
beve
rage
sVo
mit,
gas
tric
lava
ges,
urin
e,
bloo
d an
d sto
ol
Stor
age
of v
ery
acid
food
in
gal
vani
zed
tins

23Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
1.2
Incu
batio
n pe
riod
of 1
to 6
hou
rs
Bact
eria
l age
nts
Baci
llus c
ereu
s ga
stroe
nter
itis (
type
em
etic
)
Exoe
nter
otox
in o
f B.
cer
eus
From
½ to
5 h
ours
Nau
sea,
vom
iting
, oc
casio
nally
di
arrh
oea
Cook
ed o
r frie
d ric
e an
d pl
ates
of
rice
with
mea
t
Vom
it an
d sto
olSt
orag
e of
coo
ked
food
at
war
m te
mpe
ratu
res,
food
coo
ked
in la
rge
cont
aine
rs, fo
od
prep
ared
seve
ral h
ours
befo
re se
rvin
g
Stap
hylo
cocc
al fo
od
poiso
ning
Exoe
nter
otox
ins
A, B
, C, D
and
E
of S
taph
yloco
ccus
au
reus
. St
aphy
loco
cci f
rom
th
e no
se, s
kin,
and
le
sions
of i
nfec
ted
peop
le a
nd a
nim
als,
and
infe
cted
udd
ers
of c
ows
From
1 to
8 h
ours,
av
erag
e of
2 to
4
hour
s
Nau
sea,
vom
iting
, re
tchi
ng, a
bdom
inal
pa
ins,
diar
rhoe
a,
pros
tratio
n
Ham
, bee
f or
poul
try p
rodu
cts,
crea
m-fi
lled
pastr
ies,
food
mix
es
and
lefto
ver f
ood
Patie
nt: v
omit,
sto
ol, r
ecta
l sw
ab.
Carri
er: n
asal
sw
abs,
swab
s fro
m le
sion,
and
re
ctal
swab
s
Inad
equa
te re
frige
ratio
n,
hand
ler t
ouch
ed c
ooke
d fo
od, p
repa
ratio
n of
fo
od se
vera
l hou
rs be
fore
serv
ing,
ha
ndle
rs w
ith p
urul
ent
infe
ctio
ns, f
ood
kept
at
war
m te
mpe
ratu
res
(bac
teria
l inc
ubat
ion)
, fe
rmen
tatio
n of
food
s ab
norm
ally
low
in a
cids
Chem
ical
age
nts 3
Nitr
ite p
oiso
ning
Nitr
ites o
r nitr
ates
us
ed a
s com
poun
ds
to c
ure
mea
t, or
w
ater
from
shal
low
w
ells
From
1 to
2 h
ours
Nau
sea,
vom
iting
, cy
anos
is, h
eada
che,
di
zzin
ess,
wea
knes
s, lo
ss o
f co
nsci
ousn
ess,
choc
olat
e-co
lour
ed
bloo
d
Cure
d m
eats,
an
y ac
cide
ntal
ly
cont
amin
ated
fo
od a
nd e
xpos
ure
to e
xces
sive
nitri
ficat
ion
Bloo
dU
se o
f exc
essiv
e qu
antit
ies
of n
itrite
s or n
itrat
es to
cu
re fo
od o
r con
ceal
spoi
lage,
con
fusio
n of
ni
trite
s with
com
mon
salt,
an
d ot
her c
ondi
men
ts,
inad
equa
te re
frige
ratio
n,
exce
ssive
nitr
ifica
tion
in
ferti
lized
food
3 Ca
rbon
mon
oxid
e po
isoni
ng c
an re
sem
ble
som
e of
the
dise
ases
incl
uded
in th
is ca
tego
ry. P
atie
nts w
ho h
ave
been
insid
e a
clos
ed a
utom
obile
with
the
mot
or ru
nnin
g or
who
hav
e be
en in
hea
ted
room
s with
poo
r ve
ntila
tion
are
at ri
sk o
f exp
osur
e to
car
bon
mon
oxid
e.

24Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Dia
rrhea
l she
llfish
po
isoni
ng (D
SP)
Oka
daic
o ac
id
and
othe
r tox
ins
prod
uced
by
dino
flage
llate
s of
the
Din
ophy
sis sp
p.
From
1/2
to 1
2 ho
urs,
usua
lly 4
ho
urs
Dia
rrhoe
a, n
ause
a,
abdo
min
al p
ains
Mus
sels,
cla
ms,
oyste
rsG
astri
c rin
seSh
ellfi
sh c
augh
t in
wat
er
with
hig
h co
ncen
tratio
n of
Dyn
ophy
sis sp
p.
1.3
Incu
batio
n pe
riod
usua
lly fr
om 7
to 1
2 ho
urs
Fung
al a
gent
s
Poiso
ning
cau
sed
by
mus
hroo
ms o
f the
cy
clop
eptid
e an
d G
irom
itra
grou
ps
Cycl
opep
tides
an
d gy
rom
itrin
e fo
und
in c
erta
in
mus
hroo
ms
From
6 to
24
hour
sAb
dom
inal
pai
ns,
feel
ing
of fu
llnes
s, vo
miti
ng, p
rolo
nged
di
arrh
oea,
loss
of
stre
ngth
, th
irst,
mus
cle
cram
ps, r
apid
an
d w
eak
pulse
, co
llaps
e, ja
undi
ce,
som
nole
nce,
dila
ted
pupi
ls, c
oma,
dea
th
Aman
ita p
hallo
ides
, A.
ver
na, G
aler
ina
autu
mna
lis.
Escu
lent
a gi
rom
itra
(false
col
men
illa)
an
d sim
ilar s
pp. o
f m
ushr
oom
s
Urin
e, b
lood
, vo
mit
Inge
stion
of c
erta
in
spp.
of A
man
ita,
Gal
erin
a an
d G
irom
itra
mus
hroo
ms,
inge
stion
of
unk
now
n va
rietie
s of
mus
hroo
ms,
conf
usio
n of
toxi
c m
ushr
oom
s with
ed
ible
var
ietie
s
Vira
l age
nt
Nor
oviru
s (N
orw
alk-
like
viru
ses)
Nor
oviru
s viru
ses
are
rela
tivel
y sta
ble
in th
e en
viro
nmen
t an
d ca
n su
rviv
e fre
ezin
g an
d he
atin
g to
60°
C
12 to
48
hour
sVo
miti
ng, w
ater
y, no
n-bl
oody
di
arrh
oea
with
ab
dom
inal
cra
mps
, lo
w-g
rade
feve
r, m
yalg
ia, m
alai
se,
head
ache
Cont
amin
ated
food
or
wat
erSt
ool s
peci
men
s ta
ken
with
in
48 to
72
hour
s af
ter o
nset
of
sym
ptom
s
Dire
ct p
erso
n-to
-per
son
spre
ad o
r fae
cally
co
ntam
inat
ed fo
od o
r w
ater
, tou
chin
g su
rface
s or
obj
ects
cont
amin
ated
w
ith n
orov
irus,
noro
viru
ses c
an a
lso
spre
ad v
ia a
dro
plet
ro
ute
from
vom
itus.

25Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Smal
l rou
nd v
iruse
s, pr
oduc
tive
of
gastr
oent
eriti
s
Incl
udes
ad
enov
irus,
coro
navi
rus,
rota
viru
s, pa
rvov
irus,
and
astro
viru
s
½ to
3 d
ays,
usua
lly 3
6 ho
urs
Nau
sea,
vom
iting
, di
arrh
oea,
ab
dom
inal
pai
n,
mya
lgia
, hea
dach
e,
light
feve
r. D
urat
ion:
36
hou
rs
Shel
lfish
from
co
ntam
inat
ed w
ater
Stoo
l, bl
ood
in a
cute
and
co
nval
esce
nt
phas
es
Infe
cted
peo
ple
who
to
uch
food
read
y fo
r co
nsum
ptio
n, h
arve
st of
shel
lfish
from
co
ntam
inat
ed w
ater
s, im
prop
er d
ispos
al
of w
aste
s, us
e of
co
ntam
inat
ed w
ater
2. M
anife
stat
ion
of p
hary
ngiti
s an
d re
spira
tory
sig
ns a
nd s
ympt
oms
2.1
Incu
batio
n pe
riod
less
than
1 h
our
Chem
ical
age
nts
Calc
ium
chl
orid
e po
isoni
ngFr
eezi
ng m
ixtu
res o
f ca
lciu
m c
hlor
ide
for
freez
ing
dess
erts
A fe
w m
inut
esBu
rnin
g in
the
tong
ue, m
outh
, and
th
roat
, vom
iting
Froz
en d
esse
rtsVo
mit
Cont
amin
atio
n of
po
psic
les d
urin
g fre
ezin
g, p
erm
ittin
g th
e in
trodu
ctio
n of
cal
cium
ch
lorid
e in
the
syru
p
Sodi
um h
ydro
xide
po
isoni
ngSo
dium
hyd
roxi
de
(cau
stic
soda
) in
com
poun
ds u
sed
to w
ash
bottl
es,
dete
rgen
t, dr
ain
clea
ners,
hai
r-re
laxa
nts
A fe
w m
inut
esBu
rnin
g of
the
lips,
mou
th a
nd th
roat
; vo
miti
ng, a
bdom
inal
pa
ins,
diar
rhoe
a
Bottl
ed b
ever
ages
Vom
itIm
prop
er ri
nsin
g of
bo
ttles
was
hed
with
ca
ustic
subs
tanc
es
2.2
Incu
batio
n pe
riod
from
18
to 7
2 ho
urs
Bact
eria
l age
nts
Infe
ctio
ns b
y be
ta-
haem
olyt
ic st
rept
ococ
ciSt
rept
ococ
cus
pyog
enes
of t
he
thro
at a
nd le
sions
of
infe
cted
peo
ple
From
1 to
3 d
ays
Phar
yngi
tis, f
ever
, na
usea
, vom
iting
, rh
inor
rhoe
a,
som
etim
es ra
sh
Raw
milk
, foo
ds
cont
aini
ng e
ggPh
aryn
geal
swab
s, vo
mit
Wor
kers
who
touc
hed
cook
ed fo
od, w
orke
rs w
ith p
urul
ent i
nfec
tions
, in
adeq
uate
refri
gera
tion,
im
prop
er c
ooki
ng o
r re
heat
ing,
pre
para
tion
of fo
od se
vera
l hou
rs be
fore
serv
ing

26Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
2.3
Incu
batio
n pe
riod
from
3 to
30
days
Rick
ettsi
al a
gent
Q F
ever
Coxi
ella
bur
netii
2-3
wee
ks (3
-30
days
)Ch
ills,
head
ache
, m
alai
se, m
yalg
ia a
nd
swee
ts
Raw
milk
from
in
fect
ed c
attle
or
goat
s, di
rect
con
tact
w
ith c
onta
min
ated
m
ater
ials
Seru
mCo
nsum
ptio
n of
raw
m
ilk, d
irect
con
tact
w
ith a
borte
d m
ater
ials,
in
adeq
uate
disi
nfec
tion
and
disp
osal
of a
borte
d m
ater
ials
3. In
itial
or m
ajor
sig
ns a
nd s
ympt
oms
of th
e lo
wer
dig
estiv
e tr
act (
abdo
min
al p
ains
, dia
rrho
ea)
3.1
Incu
batio
n pe
riod
usua
lly fr
om 7
to 1
2 ho
urs
Bact
eria
l age
nts
Gas
troen
terit
is by
Bac
illus
cer
eus
(dia
rrhea
l typ
e)
Exoe
nter
otox
in o
f B.
cere
us, o
rgan
isms i
n th
e so
il
From
8 to
16
hour
s (av
erag
e of
12
hou
rs)
Nau
sea,
abd
omin
al
pain
s, di
arrh
oea
Food
s mad
e fro
m g
rain
s, ric
e,
custa
rd, s
auce
s, m
eatb
alls,
saus
ages
, co
oked
veg
etab
les,
dehy
drat
ed o
r re
cons
titut
ed
prod
ucts
Stoo
lIn
adeq
uate
refri
gera
tion,
sto
rage
of f
ood
at w
arm
te
mpe
ratu
res (
bact
eria
l in
cuba
tion)
, pre
para
tion
of fo
od se
vera
l hou
rs be
fore
serv
ing,
impr
oper
re
heat
ing
of le
ftove
rs
Gas
troen
terit
is ca
used
by
Clo
strid
ium
pe
rfrin
gens
Endo
ente
roto
xin
form
ed d
urin
g th
e sp
orul
atio
n of
C.
perfr
inge
ns in
the
inte
stine
s, th
e bo
dy, i
n hu
man
or
anim
als f
aece
s or i
n th
e so
il
From
8 to
22
hour
s (av
erag
e of
10
hou
rs)
Abdo
min
al p
ains
, di
arrh
oea
Cook
ed b
eef o
r po
ultry
, bro
ths,
sauc
es a
nd so
ups
Stoo
lIn
adeq
uate
refri
gera
tion,
sto
rage
of f
ood
at w
arm
te
mpe
ratu
res (
bact
eria
l in
cuba
tion)
, pre
para
tion
of fo
od se
vera
l hou
rs be
fore
serv
ing,
impr
oper
re
heat
ing
of le
ftove
r fo
od

27Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
3.2
Incu
batio
n pe
riod
usua
lly fr
om 1
8 to
72
hour
s
Bact
eria
l age
nts
Dia
rrhea
l dise
ases
ca
used
by
Aero
mon
asAe
rom
onas
hy
drop
hila
1 to
2 d
ays
Wat
ery
diar
rhoe
a,
abdo
min
al p
ain,
na
usea
, hea
dach
e
Fish
, she
llfish
, sn
ails,
wat
erSt
ool
Cont
amin
atio
n of
food
in
sea
or su
rface
wat
er
Cam
pylo
bact
er
Infe
ctio
nCa
mpy
loba
cter
je
juni
2 to
7 d
ays u
sual
ly
betw
een
3 an
d 5
Abdo
min
al p
ains
, di
arrh
oea
(freq
uent
ly
with
muc
us a
nd
bloo
d), h
eada
che,
m
yalg
ia, f
ever
, an
orex
ia, n
ause
a,
vom
iting
. Seq
uella
e:
Gui
llian
-Bar
re
synd
rom
e
Raw
milk
, bee
f liv
er, r
aw c
lam
s St
ool o
r rec
tal
swab
s, bl
ood
Drin
king
raw
milk
, ha
ndlin
g ra
w p
rodu
cts,
eatin
g ra
w o
r un
derc
ooke
d po
ultry
, in
adeq
uate
coo
king
or
paste
uriz
atio
n, c
ross
-co
ntam
inat
ion
with
raw
m
eat
Chol
era
Endo
ente
roto
xin
of
V. c
hole
rae
clas
sical
an
d El
Tor
bio
type
s, fro
m fa
eces
of
infe
cted
per
sons
From
1 to
3 d
ays
Seve
re, w
ater
y di
arrh
oea
(rice
wat
er
stool
s), v
omiti
ng,
abdo
min
al p
ains
, de
hydr
atio
n, th
irst,
colla
pse,
loss
of
skin
tone
, shr
ivel
led
finge
rs, su
nken
eye
s
Raw
fish
and
sh
ellfi
sh, f
ood
was
hed
or
prep
ared
with
co
ntam
inat
ed
wat
er, w
ater
Stoo
lH
arve
sting
of f
ish a
nd
shel
lfish
from
wat
er
cont
amin
ated
with
se
wag
e in
end
emic
ar
eas,
poor
per
sona
l hy
gien
e, in
fect
ed
hand
lers
who
touc
hed
food
, ina
dequ
ate
cook
ing,
use
of
cont
amin
ated
wat
er in
w
ashi
ng o
r rin
sing
food
, im
prop
er d
ispos
al o
f w
aste
wat
er, u
se o
f was
te
from
latri
nes a
s fer
tiliz
er

28Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Gas
troen
terit
is ca
used
by
cho
lera
like
vib
rioCh
oler
a lik
e vib
rioFr
om 5
to 4
8 ho
urs,
aver
age
from
10
to 2
4 ho
urs
Abdo
min
al p
ains
, di
arrh
oea,
nau
sea,
vo
miti
ng, f
ever
, ch
ills,
head
ache
, m
yalg
ia
Vario
us fo
ods,
wat
erSt
ool,
rect
al
swab
sIn
fect
ed h
andl
ers w
ho
touc
h fo
od, i
nsuf
ficie
nt
cool
ing,
inco
mpl
ete
cook
ing,
impr
oper
cl
eani
ng a
nd d
isinf
ectio
n of
equ
ipm
ent
Dia
rrhoe
al
dise
ases
cau
sed
by
Ente
roha
emor
rhag
ic
Esch
eric
hia
coli
E. c
oli O
157:
H7,
O
26, O
111,
O11
5,
O11
3
1 to
10
days
us
ually
2 to
5 d
ays
Wat
ery
diar
rhoe
a fo
llow
ed b
y bl
oody
di
arrh
oea,
seve
re
abdo
min
al p
ain,
bl
ood
in th
e ur
ine.
Seq
uela
e:
Hae
mol
ytic
ure
mic
sy
ndro
me
(HU
S)
Ham
burg
er, r
aw
milk
, sau
sage
s, yo
gurt,
lettu
ce,
wat
er
Stoo
l, re
ctal
sw
abs
Ham
burg
er m
ade
from
mea
t of i
nfec
ted
anim
als,
cons
umpt
ion
of ra
w m
eat a
nd m
ilk,
inad
equa
te c
ooki
ng,
cros
s-co
ntam
inat
ion,
in
fect
ed p
eopl
e to
uchi
ng fo
od re
ady
for
cons
umpt
ion,
impr
oper
de
sicca
tion
and
ferm
enta
tion
of m
eats
Dia
rrhoe
a ca
used
by
Ent
eroi
nvas
ive
Esch
eric
hia
coli
Stra
ins o
f En
tero
inva
sive
E. c
oli
½ to
3 d
ays
Seve
re a
bdom
inal
pa
in, f
ever
, wat
ery
diar
rhoe
a, (u
sual
ly
with
muc
us a
nd
bloo
d pr
esen
t) te
nesm
us
Sala
ds a
nd o
ther
fo
od th
at a
re n
ot
subs
eque
ntly
tre
ated
, wat
er
Stoo
l, re
ctal
sw
abs
Inad
equa
te c
ooki
ng,
infe
cted
per
sons
to
uchi
ng fo
od re
ady
for c
onsu
mpt
ion,
not
w
ashi
ng h
ands
afte
r de
feca
tion,
stor
ing
food
at
room
tem
pera
ture
, sto
ring
food
in th
e re
frige
rato
r in
larg
e co
ntai
ners,
pre
parin
g fo
od se
vera
l hou
rs be
fore
serv
ing,
impr
oper
re
heat
ing
of fo
od

29Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Dia
rrhoe
a ca
used
by
ETEC
St
rain
s of E
TEC
½ to
3 d
ays
Prof
use
wat
ery
diar
rhoe
a (w
ithou
t m
ucus
or b
lood
) ab
dom
inal
pa
in, v
omiti
ng,
pros
tratio
n,
dehy
drat
ion,
ligh
t fe
ver
Sala
ds a
nd o
ther
fo
od th
at a
re n
ot
subs
eque
ntly
th
erm
ally
trea
ted,
fre
sh c
hees
es,
wat
er
Stoo
l, re
ctal
sw
abs
Inad
equa
te c
ooki
ng,
infe
cted
peo
ple
touc
hing
food
read
y fo
r con
sum
ptio
n, n
ot
was
hing
han
ds a
fter
defe
catio
n, st
orag
e of
food
at r
oom
te
mpe
ratu
re, k
eepi
ng
food
in th
e re
frige
rato
r in
larg
e co
ntai
ners,
pr
epar
ing
food
seve
ral
hour
s bef
ore
serv
ing,
im
prop
er re
heat
ing
of
food
, use
of r
aw m
ilk in
m
akin
g ch
eese
Ente
ritis
by P
lesio
mon
asPl
eiso
mon
as
shig
eloi
des
1 to
2 d
ays
Dia
rrhoe
a w
ith
muc
us a
nd b
lood
in
the
stool
Wat
erSt
ool,
rect
al
swab
sIn
adeq
uate
coo
king
Salm
onel
losis
Vario
us se
roty
pes
of S
alm
onel
la fr
om
faec
es o
f inf
ecte
d pe
ople
and
ani
mal
s
From
6 to
72
hour
s, av
erag
e fro
m 1
8 to
36
hour
s
Abdo
min
al p
ains
, di
arrh
oea,
chi
lls,
feve
r, na
usea
, vo
miti
ng, m
alai
se
Beef
and
pou
ltry
and
thei
r by-
prod
ucts,
egg
pr
oduc
ts, o
ther
fo
ods c
onta
min
ated
w
ith sa
lmon
ella
e
Stoo
l, re
ctal
sw
abs
Inad
equa
te re
frige
ratio
n,
stora
ge o
f foo
d at
w
arm
tem
pera
ture
s (b
acte
rial i
ncub
atio
n),
inad
equa
te c
ooki
ng a
nd
rehe
atin
g, p
repa
ratio
n of
food
seve
ral h
ours
befo
re se
rvin
g, c
ross
-co
ntam
inat
ion,
impr
oper
cl
eani
ng o
f equ
ipm
ent,
infe
cted
han
dler
s who
to
uch
cook
ed fo
od,
acqu
isitio
n of
food
from
co
ntam
inat
ed so
urce
s.

30Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Shig
ello
sisSh
igel
la fl
exne
ri,
S. d
ysen
teria
e, S
. so
nnei
and
S. b
oydi
i
From
½ to
7 d
ays,
usua
lly fr
om 1
to
3 da
ys
Abdo
min
al p
ains
, di
arrh
oea,
muc
oid
faec
es w
ith b
lood
pr
esen
t, fe
ver
Any
food
read
y fo
r con
sum
ptio
n th
at b
ecom
es
cont
amin
ated
, fre
quen
tly sa
lads
, w
ater
Stoo
l, re
ctal
sw
abs
Infe
cted
han
dler
s to
uchi
ng th
e fo
od,
inad
equa
te re
frige
ratio
n,
impr
oper
coo
king
and
re
heat
ing
Gas
troen
terit
is ca
used
by
V. p
arah
aem
olyt
icus
V. p
arah
aem
olyt
icus
fro
m se
a w
ater
or
mar
ine
prod
ucts
From
2 to
48
hour
s, av
erag
e 12
ho
urs
Abdo
min
al p
ains
, di
arrh
oea,
nau
sea,
vo
miti
ng, f
ever
, ch
ills,
head
ache
Raw
or
cont
amin
ated
sea
food
, she
llfish
Stoo
l, re
ctal
sw
abs
Inad
equa
te c
ooki
ng,
inad
equa
te re
frige
ratio
n,
cros
s-co
ntam
inat
ion,
im
prop
er c
lean
ing
of
equi
pmen
t, us
e of
sea
wat
er in
pre
parin
g fo
od
Dia
rrhoe
a ca
used
by
yers
inio
sisYe
rsin
ia
ente
roco
litic
a1
to 7
day
sAb
dom
inal
pai
ns
(can
sim
ulat
e ap
pend
iciti
s), li
ght
feve
r, he
adac
he,
disc
omfo
rt, a
nore
xia,
na
usea
, vom
iting
Raw
milk
, wat
erSt
ool,
rect
al
swab
sIn
adeq
uate
coo
king
or
pas
teur
izat
ion,
cr
oss-
cont
amin
atio
n,
cont
amin
ated
in
gred
ient
s or w
ater
Vira
l age
nts
Vira
l gas
troen
terit
isEn
teric
viru
ses
(ech
oviru
s, co
xsac
kiev
irus,
reov
irus,
aden
oviru
s)
From
3 to
5 d
ays
Dia
rrhoe
a, fe
ver,
vom
iting
, abd
omin
al
pain
s, so
met
imes
re
spira
tory
sy
mpt
oms
Food
read
y fo
r co
nsum
ptio
nSt
ool
Poor
per
sona
l hyg
iene
, in
fect
ed w
orke
rs to
uchi
ng fo
od, i
mpr
oper
co
okin
g an
d re
heat
ing
3.3
Incu
batio
n pe
riod
from
a fe
w d
ays
to s
ever
al w
eeks
Para
sitic
age
nts
Asca
riasis
Asca
ris lu
mbr
icoi
des
14 to
20
days
Stom
ach
diso
rder
s, cr
amps
, vom
iting
, fe
ver
Vege
tabl
es a
nd
wat
erSt
ool
Inad
equa
te w
aste
di
spos
al, p
oor h
ygie
ne in
fo
od h
andl
ing

31Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Amoe
bic
dyse
nter
y (a
moe
bias
is)En
tam
oeba
hi
stolyt
ica
From
a fe
w d
ays
to se
vera
l mon
ths
usua
lly b
etw
een
2 an
d 4
wee
ks
Abdo
min
al p
ains
, co
nstip
atio
n or
di
arrh
oea
with
blo
od
and
muc
us
Vege
tabl
es a
nd ra
w
fruits
Stoo
lPo
or p
erso
nal h
ygie
ne,
infe
cted
han
dler
s to
uchi
ng th
e fo
od,
impr
oper
coo
king
and
re
heat
ing
Gia
rdia
sisG
iard
ia la
mbl
ia
from
faec
es o
f in
fect
ed p
eopl
e
From
1 to
6 w
eeks
Abdo
min
al p
ains
, di
arrh
oea
with
m
ucus
, fat
ty st
ools
Raw
frui
ts an
d ve
geta
bles
, wat
erSt
ool
Poor
per
sona
l hyg
iene
, in
fect
ed h
andl
ers
touc
hing
food
, im
prop
er
cook
ing,
impr
oper
was
te
wat
er d
ispos
al
Cryp
tosp
orid
iosis
Cryp
tosp
orid
ium
pa
rvum
1 to
12
days
, us
ually
7 d
ays
Prof
use
wat
ery
diar
rhoe
a,
abdo
min
al p
ain,
an
orex
ia, v
omiti
ng,
light
feve
r
Appl
e ci
der,
wat
erSt
ool,
inte
stina
l bi
opsy
Impr
oper
disp
osal
of
ani
mal
was
tes,
cont
amin
atio
n fro
m th
e an
imal
env
ironm
ent,
inad
equa
te fi
lterin
g of
w
ater
Hyd
atid
osis
(uni
locu
lar
or m
ultil
ocul
ar)
Echi
noco
ccus
gr
anul
osus
, Ec
hino
cocc
us
mul
tiloc
ular
is
Mon
ths t
o ye
ars
Abdo
min
al p
ain,
ab
norm
al a
bdom
inal
te
nder
ness
, he
pato
meg
aly
with
an
abd
omin
al m
ass,
jaun
dice
, fev
er
Food
or w
ater
co
ntam
inat
ed w
ith
faec
es o
f inf
ecte
d do
g, fo
x
Biop
sy o
r ser
umCo
nsum
ptio
n of
raw
ve
geta
bles
or w
ater
co
ntam
inat
ed w
ith
faec
es o
f inf
ecte
d do
g or
fox
Live
rfluk
e (F
asci
olia
sis)
Fasc
iola
hep
atic
aFr
om 4
to 6
wee
ksD
yspe
psia
, fev
er,
right
upp
er q
uadr
ant
pain
, ano
rexi
a,
hepa
tom
egal
y, sp
leno
meg
aly,
asci
tes,
urtic
aria
, re
spira
tory
sy
mpt
oms,
and
jaun
dice
Aqua
tic p
lant
s or
plan
ts w
ith h
igh
moi
sture
con
tent
Stoo
l, tis
sue
biop
syEa
ting
raw
aqu
atic
pl
ants,
inef
ficie
nt
disp
osal
of h
uman
and
an
imal
was
tes i
n po
nd o
r w
ater
bod
ies
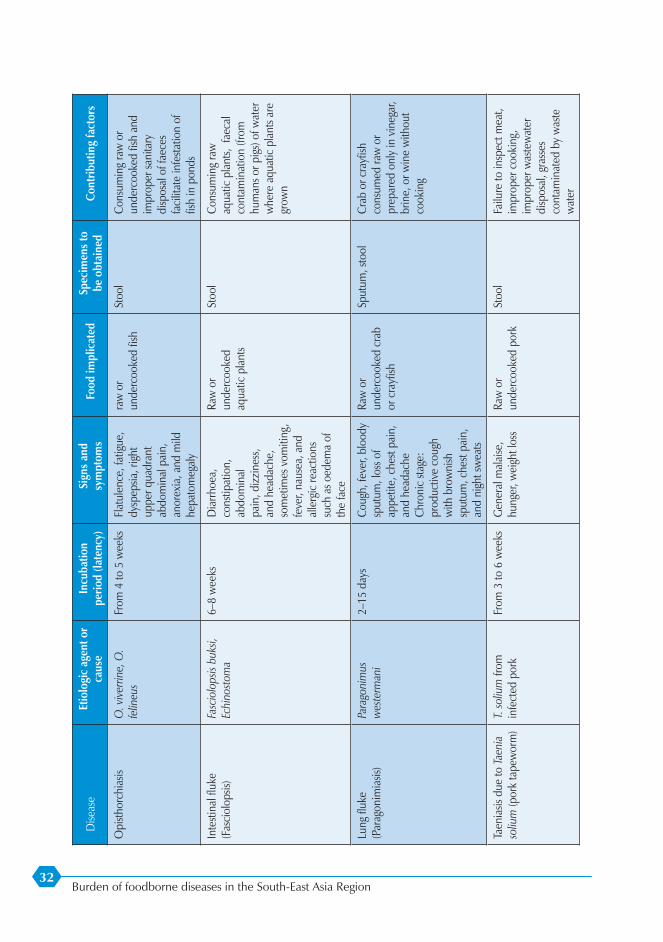
32Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Opi
sthor
chia
sisO
. vive
rrine
, O.
felin
eus
From
4 to
5 w
eeks
Flat
ulen
ce, f
atig
ue,
dysp
epsia
, rig
ht
uppe
r qua
dran
t ab
dom
inal
pai
n,
anor
exia
, and
mild
he
pato
meg
aly
raw
or
unde
rcoo
ked
fish
Stoo
lCo
nsum
ing
raw
or
unde
rcoo
ked
fish
and
impr
oper
sani
tary
di
spos
al o
f fae
ces
faci
litat
e in
festa
tion
of
fish
in p
onds
Inte
stina
l flu
ke
(Fas
ciol
opsis
)Fa
scio
lops
is bu
ksi,
Echi
nosto
ma
6–8
wee
ksD
iarrh
oea,
co
nstip
atio
n,
abdo
min
al
pain
, diz
zine
ss,
and
head
ache
, so
met
imes
vom
iting
, fe
ver,
naus
ea, a
nd
alle
rgic
reac
tions
su
ch a
s oed
ema
of
the
face
Raw
or
unde
rcoo
ked
aqua
tic p
lant
s
Stoo
lCo
nsum
ing
raw
aq
uatic
pla
nts,
faec
al
cont
amin
atio
n (fr
om
hum
ans o
r pig
s) of
wat
er
whe
re a
quat
ic p
lant
s are
gr
own
Lung
fluk
e (P
arag
onim
iasis
)Pa
rago
nim
us
wes
term
ani
2–15
day
sCo
ugh,
feve
r, bl
oody
sp
utum
, los
s of
appe
tite,
che
st pa
in,
and
head
ache
Ch
roni
c sta
ge:
prod
uctiv
e co
ugh
with
bro
wni
sh
sput
um, c
hest
pain
, an
d ni
ght s
wea
ts
Raw
or
unde
rcoo
ked
crab
or
cra
yfish
Sput
um, s
tool
Crab
or c
rayf
ish
cons
umed
raw
or
prep
ared
onl
y in
vin
egar
, br
ine,
or w
ine
with
out
cook
ing
Taen
iasis
due
to Ta
enia
so
lium
(por
k ta
pew
orm
)T.
soliu
m fr
om
infe
cted
por
kFr
om 3
to 6
wee
ksG
ener
al m
alai
se,
hung
er, w
eigh
t los
sRa
w o
r un
derc
ooke
d po
rkSt
ool
Failu
re to
insp
ect m
eat,
impr
oper
coo
king
, im
prop
er w
aste
wat
er
disp
osal
, gra
sses
co
ntam
inat
ed b
y w
aste
w
ater

33Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Taen
iasis
due
to
Taen
ia sa
gina
ta (b
eef
tape
wor
m)
T. sa
gina
ta fr
om
mea
t fro
m m
eat o
f in
fect
ed c
attle
From
8 to
14
wee
ksG
ener
al m
alai
se,
hung
er, w
eigh
t los
s, ab
dom
inal
pai
ns
Raw
or
unde
rcoo
ked
mea
tSt
ool
Failu
re to
insp
ect m
eat,
impr
oper
coo
king
, im
prop
er w
aste
wat
er
disp
osal
, pas
ture
co
ntam
inat
ed b
y w
aste
w
ater
Anisa
kias
isAn
isaki
s ps
eudo
terra
nova
From
4 to
6 w
eeks
Stom
ach
pain
, na
usea
, vom
iting
, ab
dom
inal
pai
n
Rock
fish
, her
ring,
co
d, sa
lmon
, squ
id,
sush
i
Stoo
lIn
gesti
on o
f raw
or
unde
rcoo
ked
fish
Dip
hyllo
botri
asis
(fish
ta
pew
orm
infe
ctio
n)D
iphy
llobo
thriu
m
latu
m fr
om fl
esh
of
infe
cted
fish
From
3 to
6 w
eeks
Und
efin
ed
gastr
oint
estin
al
disc
omfo
rt, a
naem
ia
may
occ
ur
Raw
or
unde
rcoo
ked
fresh
w
ater
fish
Stoo
lIn
adeq
uate
coo
king
, im
prop
er w
aste
wat
er
disp
osal
, lak
es
cont
amin
ated
by
was
te
wat
er
Spar
gano
sisSp
irom
etra
spp.
pain
ful o
edem
a,
seiz
ures
, he
mip
ares
is, a
nd
head
ache
s
Cont
amin
ated
w
ater
, con
sum
ing
raw
fles
h of
frog
or
snak
e
Biop
syD
rinki
ng w
ater
co
ntam
inat
ed w
ith
infe
cted
cop
epod
s or
con
sum
ing
raw
or
unde
r-coo
ked
flesh
of
frog
or sn
ake
4. M
anife
stat
ion
of n
euro
logi
cal s
igns
and
sym
ptom
s (v
isua
l dis
orde
rs, t
ingl
ing,
par
alys
is)
4.1
Incu
batio
n pe
riod
tend
s to
be
less
than
1 h
our
Fung
al a
gent
s
Mus
hroo
m p
oiso
ning
fro
m th
e gr
oup
that
co
ntai
ns ib
oten
ic a
cid
Ibot
enic
and
m
usci
mol
foun
d in
ce
rtain
mus
hroo
ms
From
30
to 6
0 m
inut
esSo
mno
lenc
e an
d sta
te o
f int
oxic
atio
n,
conf
usio
n, m
uscu
lar
spas
ms,
delir
ium
, vi
sual
diso
rder
s
Aman
ita
mus
caria
, A.
pant
herin
a, a
nd
rela
ted
spp.
of
mus
hroo
ms
In
gesti
on o
f Am
anita
m
usca
ria a
nd re
late
d sp
p. o
f mus
hroo
ms,
inge
stion
of u
nkno
wn
varie
ties o
f mus
hroo
ms,
conf
usio
n of
toxi
c m
ushr
oom
s with
edi
ble
varie
ties

34Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Poiso
ning
cau
sed
by m
ushr
oom
s of
the
grou
p th
at
cont
ains
mus
carin
e (m
usca
rinism
)
Mus
carin
e fo
und
in
certa
in m
ushr
oom
s15
min
utes
to a
fe
w h
ours
Exce
ssiv
e sa
liva-
tion,
per
spira
tion,
la
crim
atio
n, d
rop
in b
lood
pre
ssur
e,
irreg
ular
pul
se,
cont
ract
ion
of th
e pu
pils,
blu
rred
visio
n, a
sthm
atic
br
eath
ing
Clito
cybe
dea
l-ba
ta, C
. riv
ulos
e,
and
man
y sp
p. o
f In
ocyb
e an
d Bo
le-
tus m
ushr
oom
s
Vom
itIn
gesti
on o
f A.
mus
caria
and
rela
ted
spp.
, con
sum
ptio
n of
unk
now
n va
rietie
s of
mus
hroo
ms,
cons
umpt
ion
of to
xic
mus
hroo
ms b
y m
istak
e
Chem
ical
age
nts
Org
anop
hosp
horu
s po
isoni
ngO
rgan
opho
spho
rus
inse
ctic
ides
, suc
h as
par
athi
on, T
EPP,
diaz
inon
, mal
athi
on
From
a fe
w
min
utes
to a
few
ho
urs
Nau
sea,
vom
iting
, ab
dom
inal
pa
ins,
diar
rhoe
a,
head
ache
, ne
rvou
snes
s, bl
urre
d vi
sion,
che
st pa
ins,
cyan
osis,
con
fusio
n,
spas
mod
ic
cont
ract
ion,
co
nvul
sions
Any
acci
dent
ally
co
ntam
inat
ed fo
odBl
ood,
urin
e,
adip
ose
tissu
e (fo
r bi
opsy
)
Spra
ying
of c
rops
im
med
iate
ly b
efor
e ha
rves
t, sto
rage
of
inse
ctic
ides
in th
e sa
me
plac
e as
food
, con
fusio
n of
pes
ticid
es w
ith fo
od in
po
wde
red
form
Carb
amat
e po
isoni
ngCa
rbar
yl (s
evin
), Te
mik
(ald
icar
b)½
hou
rEp
igas
tric
pain
, vo
miti
ng, a
bnor
mal
sa
livat
ion,
co
ntra
ctio
n of
th
e pu
pils,
lack
of
mus
cula
r co
ordi
natio
n
Any
acci
dent
ally
co
ntam
inat
ed fo
odBl
ood,
urin
eIm
prop
er a
pplic
atio
n to
cro
ps, s
tora
ge in
the
sam
e ar
eas a
s foo
d,
mist
aken
as f
ood
in
pow
dere
d fo
rm

35Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Din
ofla
gella
tes
Para
lytic
She
llfish
Po
isoni
ngSa
xito
xin
and
othe
r din
ofla
gella
te
toxi
ns o
f the
spp.
Al
exan
driu
m a
nd
Gym
nodi
nium
Seve
ral m
inut
es to
30
min
utes
Ting
ling,
bur
ning
, an
d nu
mbn
ess
arou
nd th
e lip
s an
d th
e tip
s of t
he
finge
rs, d
izzy
spel
ls,
inco
here
nt sp
eech
, re
spira
tory
par
alys
is
Mus
sels
and
clam
sG
astri
c la
vage
Har
vesti
ng sh
ellfi
sh
from
wat
er w
ith h
igh
conc
entra
tions
of
dino
flage
llate
s of t
he
spp.
Ale
xand
rium
and
G
ymno
dini
um
Tetro
doto
xism
(te
traod
on p
oiso
ning
)Te
trodo
xin
foun
d in
th
e in
testi
nes a
nd
gona
ds o
f puf
fer f
ish
(blo
wfis
h, g
lobe
fish)
From
10
min
utes
to
3 h
ours
Sens
atio
n of
tin
glin
g in
the
finge
rs an
d to
es,
dizz
ines
s, pa
llor,
num
bnes
s of t
he
mou
th a
nd li
mbs
, ga
stroi
ntes
tinal
sy
mpt
oms,
haem
orrh
age
and
flaki
ng o
f the
skin
, fix
atio
n of
the
eyes
, spa
smod
ic
cont
ract
ion,
pa
raly
sis, c
yano
sis
Fish
of t
he p
uffe
r fis
h fa
mily
Sto
olIn
gesti
on o
f fish
of
the
puffe
r fish
fam
ily,
cons
umpt
ion
of su
ch
fish
with
out e
xtra
ctin
g in
testi
nes a
nd g
onad
s
Poiso
nous
pla
nts
Jimso
nwee
d (th
orn
appl
e) p
oiso
ning
Trop
ane
alka
loid
s fo
und
in D
atur
a str
amon
ium
Less
than
1 h
our
Abno
rmal
thirs
t, ph
otop
hobi
a,
disto
rted
visio
n,
diffi
culty
spea
king
, de
liriu
m, f
acia
l flu
shin
g, d
eliri
um,
com
a, ra
pid
pulse
he
art a
ttack
.
Any
part
of th
e he
rb, t
omat
oes
grow
n w
ith g
rafts
Urin
eCo
nsum
ptio
n of
any
pa
rt of
the
Jimso
n w
eed
or c
onsu
mpt
ion
of
tom
atoe
s gro
wn
with
gr
afts

36Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Wat
er h
emlo
ck
poiso
ning
Resin
or c
icut
oxin
fo
und
in w
ater
he
mlo
ck
From
15
to 6
0 m
inut
esEx
cess
ive
saliv
atio
n,
naus
ea, v
omiti
ng,
stom
ach
pain
s, fro
thin
g at
the
mou
th, i
rregu
lar
brea
thin
g,
conv
ulsio
ns,
resp
irato
ry p
aral
ysis
Root
of w
ater
he
mlo
ck (C
icut
a vi
rosa
and
C.
mas
cula
ta)
Urin
eIn
gesti
on o
f wat
er
hem
lock
; con
fusio
n of
the
root
of w
ater
he
mlo
ck w
ith w
ild
parsn
ip, s
wee
t pot
ato,
or
car
rot
4.2
Incu
batio
n pe
riod
usua
lly b
etw
een
1 an
d 6
hour
s
Chem
ical
age
nts
Chlo
rinat
ed
hydr
ocar
bon
poiso
ning
Inse
ctic
ides
co
ntai
ning
ch
lorin
ated
hy
droc
arbo
n, su
ch
as a
ldrin
, chl
orda
ne,
DD
T, d
ield
rin,
endr
in, l
inda
ne,
and
toxa
phen
e
From
30
min
utes
to
6 h
ours
Nau
sea,
vom
iting
, pa
resth
esia
, di
zzin
ess,
mus
cula
r w
eakn
ess,
anor
exia
, w
eigh
t los
s, co
nfus
ion
Any
acci
dent
ally
co
ntam
inat
ed fo
odBl
ood,
urin
e,
stool
, gas
tric
lava
ges
Stor
age
of in
sect
icid
es in
th
e sa
me
plac
e as
food
, co
nfus
ion
of p
estic
ides
w
ith fo
od in
pow
dere
d fo
rm
Mar
ine
plan
kton
Cigu
ater
a po
isoni
ngCi
guat
oxin
from
th
e in
testi
nes,
roe,
go
nads
, and
fles
h of
tro
pica
l mar
ine
fish
From
3 to
5 h
ours,
so
met
imes
mor
eTi
nglin
g an
d nu
mbn
ess a
roun
d th
e m
outh
, met
allic
ta
ste, d
ryne
ss
of th
e m
outh
, ga
stroi
ntes
tinal
sy
mpt
oms,
wat
ery
stool
, mya
lgia
, di
zzin
ess,
dila
ted
pupi
ls, b
lurre
d vi
sion,
pro
strat
ion,
pa
raly
sis
Num
erou
s var
ietie
s of
trop
ical
fish
In
gesti
on o
f liv
er,
inte
stine
s, ro
e, g
onad
s, or
fles
h of
trop
ical
reef
fis
h; in
gen
eral
the
larg
e re
ef fi
sh a
re m
ore
likel
y to
be
toxi
c

37Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
4.3
Incu
batio
n pe
riod
usua
lly fr
om 1
2 to
72
hour
s
Bact
eria
l age
nts
Botu
lism
Exon
euro
toxi
ns
A, B
, E a
nd F
fro
m C
lostr
idiu
m
botu
linum
. The
sp
ores
are
foun
d in
soil
and
anim
al
inte
stine
s
From
2 h
ours
to 8
da
ys, a
vera
ge fr
om
18 to
36
hour
s
Verti
go, d
oubl
e or
blu
rred
visio
n,
dryn
ess o
f the
m
outh
, diff
icul
ty in
sw
allo
win
g, sp
eaki
ng
and
brea
thin
g;
desc
endi
ng
flacc
id p
aral
ysis,
co
nstip
atio
n,
dila
tion
or fi
xatio
n of
the
pupi
ls,
resp
irato
ry p
aral
ysis.
G
astro
inte
stina
l sy
mpt
oms c
an
prec
ede
neur
olog
ical
sy
mpt
oms.
Is fre
quen
tly fa
tal
Hom
e-ca
nned
fo
ods w
ith lo
w
acid
con
tent
, va
cuum
-pac
ked
fish;
ferm
ente
d ro
e,
fish
and
mar
ine
mam
mal
s, fis
h th
at
have
not
bee
n gu
tted
Bloo
d, st
ool,
gastr
ic la
vage
Impr
oper
pre
para
tion
of c
anne
d fo
od
and
smok
ed fi
sh,
unco
ntro
lled
ferm
enta
tion
4.4
Incu
batio
n pe
riod
high
er th
an 7
2 ho
urs
Chem
ical
age
nts
Mer
cury
poi
soni
ngEt
hyl a
nd m
ethy
l co
mpo
unds
of
mer
cury
in
indu
stria
l was
te a
nd
orga
nic
mer
cury
in
fung
icid
es
1 w
eek
or m
ore
Num
bnes
s, w
eakn
ess o
f the
legs
, sp
astic
par
alys
is,
dete
riora
tion
in th
e vi
sion,
blin
dnes
s, co
ma
Gra
ins t
reat
ed
with
fung
icid
es
that
con
tain
m
ercu
ry; p
ork,
fis
h, a
nd sh
ellfi
sh
expo
sed
to m
ercu
ry
com
poun
ds
Urin
e, b
lood
, hai
rFi
sh c
augh
t in
wat
ers
cont
amin
ated
with
m
ercu
ry c
ompo
unds
, an
imal
s fed
with
gra
ins
treat
ed w
ith fu
ngic
ides
co
ntai
ning
mer
cury
, in
gesti
on o
f mer
cury
, in
gesti
on o
f gra
ins
treat
ed w
ith m
ercu
ry o
r m
eat f
rom
ani
mal
s fed
w
ith th
ose
grai
ns

38Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Trio
rthoc
resy
l ph
osph
ate
poiso
ning
Trio
rthoc
resy
l ph
osph
ate
used
as
an
extra
ct o
r as
a su
bstit
ute
for
kitc
hen
oil
From
5 to
21
days
, av
erag
e 10
day
sG
astro
inte
stina
l sy
mpt
oms,
pain
s in
the
legs
, ver
y ac
cent
uate
d eq
uine
ga
it, li
mpn
ess o
f fee
t an
d w
rist
Cook
ing
oils,
ex
tract
s and
ot
her f
oods
tuffs
co
ntam
inat
ed
with
trio
rthoc
resy
l ph
osph
ate
Biop
sy o
f the
ga
stron
emiu
s m
uscl
e
Use
of t
he c
ompo
und
as a
n ex
tract
or a
s oil
for
cook
ing
or fo
r sal
ads
5. M
anife
stat
ion
of s
igns
and
sym
ptom
s of
gen
eral
ized
infe
ctio
n (fe
ver,
chill
s, d
isco
mfo
rt, p
ains
)
5.1
Incu
batio
n pe
riod
betw
een
12-7
2 ho
urs
Bact
eria
l age
nts
Infe
ctio
n ca
used
by
Vibr
io v
ulni
ficus
Vibr
io v
ulni
ficus
16 h
ours
Sept
icae
mia
, fev
er,
mal
aise
, pro
strat
ion,
ty
pica
l of c
ases
w
ith p
revi
ous l
iver
pr
oble
ms
Oys
ters
and
raw
cl
ams
Bloo
dPe
ople
with
live
r pr
oble
ms
Anth
rax
Baci
llus a
nthr
acis
From
3 to
5 d
ays
Gas
troen
terit
is,
vom
iting
, ha
emor
rhag
ic
depo
sitio
ns
Mea
t fro
m si
ck
anim
als
Stoo
l, vo
miti
ngCl
inic
al m
anife
statio
ns
afte
r con
sum
ptio
n of
m
eat f
rom
sick
ani
mal
s
Stre
ptoc
occu
s sui
s in
fect
ion
Stre
ptoc
occu
s sui
s3
hour
s to
14 d
ays
Hea
dach
e, fe
ver,
vom
iting
, men
ingi
tis,
sept
icae
mia
, en
doca
rditi
s, to
xic
shoc
k sy
ndro
me,
ar
thrit
is, a
cute
de
afne
ss
Infe
cted
pig
s or
cont
amin
ated
por
kCS
F or
blo
od
sam
ples
Dire
ct c
onta
ct w
ith
infe
cted
or c
onta
min
ated
m
ater
ials,
pro
cess
ing
or
cons
umin
g un
cook
ed
or p
artia
lly c
ooke
d po
rk
prod
ucts

39Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
5.2
Incu
batio
n pe
riod
long
er th
an 1
wee
k
Bact
eria
l age
nts
Bruc
ello
sisBr
ucel
la a
bortu
s, B.
m
elite
nsis,
and
B.
suis
in ti
ssue
s and
m
ilk o
f inf
ecte
d an
imal
s
From
7 to
21
days
Feve
r, ch
ills,
swea
ts,
wea
knes
s, m
alai
se,
head
ache
, mya
lgia
an
d ar
thra
lgia
, w
eigh
t los
s
Raw
milk
, goa
t ch
eese
mad
e w
ith
raw
milk
Bloo
dU
npas
teur
ized
milk
, liv
esto
ck in
fect
ed b
y br
ucel
losis
, con
tact
with
ab
orte
d m
ater
ials
Tube
rcul
osis
Myc
obac
teriu
m
bovis
4–12
wee
ksLu
ng le
sions
ba
sical
ly b
ut a
lso in
ki
dney
s, liv
er, s
plee
n an
d co
rresp
ondi
ng
node
s
Raw
milk
and
mea
tCu
lture
from
se
cret
ions
or
tissu
es
Cons
umpt
ion
of ra
w
milk
, con
sum
ptio
n of
ra
w in
fect
ed m
eat f
rom
do
mes
tic o
r wild
ani
mal
s
Liste
ria in
fect
ion
Liste
ria
mon
ocyt
ogen
es3
to 7
0 da
ys,
usua
lly 4
to 2
1 da
ys
Feve
r, he
adac
he,
naus
ea, v
omiti
ng,
abor
tion,
men
ingi
tis,
ence
phal
itis,
and
seps
is
Milk
, fre
sh c
hees
e,
proc
esse
d m
eats
Bloo
d, u
rine
Impr
oper
coo
king
, non
-pa
steur
izat
ion
of m
ilk,
prol
onge
d co
olin
g
Typh
oid
and
para
typh
oid
feve
rS.
ent
eric
a Se
roty
pe
typh
i fou
nd in
fa
eces
of i
nfec
ted
peop
le, o
ther
se
roty
pes (
as
para
typh
i A, c
hole
ra
suis)
for c
ases
of
para
typh
oid,
faec
es
of h
uman
s and
an
imal
s
From
7 to
28
days
, av
erag
e 14
day
sM
alai
se, h
eada
che,
fe
ver,
coug
h,
naus
ea, v
omiti
ng,
cons
tipat
ion,
ab
dom
inal
pai
ns,
chill
s, ro
se sp
ots,
bloo
dy st
ool
Shel
lfish
, foo
d co
ntam
inat
ed b
y ha
ndle
rs, ra
w m
ilk,
chee
se, w
ater
cres
s, w
ater
Stoo
l, re
ctal
sw
abs,
bloo
d in
ear
ly p
art o
f th
e ac
ute
phas
e,
urin
e in
the
acut
e ph
ase
Infe
cted
han
dler
s to
uchi
ng fo
od, p
oor
perso
nal h
ygie
ne,
impr
oper
coo
king
, in
adeq
uate
refri
gera
tion,
im
prop
er w
aste
wat
er
disp
osal
, acq
uisit
ion
of
food
from
con
tam
inat
ed
sour
ces,
harv
estin
g of
sh
ellfi
sh fr
om w
ater
s co
ntam
inat
ed w
ith
sew
age

40Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Vira
l age
nts
Hep
atiti
s AH
epat
itis A
viru
s fo
und
in th
e fa
eces
, ur
ine,
or b
lood
of
infe
cted
peo
ple
and
othe
r inf
ecte
d no
n-hu
man
prim
ates
From
10
to 5
0 da
ys, a
vera
ge 2
5 da
ys
Feve
r, m
alai
se,
lass
itude
, ano
rexi
a,
naus
ea, a
bdom
inal
pa
ins,
jaun
dice
Shel
lfish
, any
food
co
ntam
inat
ed w
ith
hepa
titis
viru
s, w
ater
Stoo
l, ur
ine,
bl
ood
Infe
cted
han
dler
s to
uchi
ng fo
od, p
oor
perso
nal h
ygie
ne,
impr
oper
coo
king
, ha
rves
ting
shel
lfish
from
w
ater
s con
tam
inat
ed
with
sew
age,
impr
oper
di
spos
al o
f was
tew
ater
Hep
atiti
s EH
epat
itis E
viru
sFr
om 1
5 to
65
days
usu
ally
35
to 4
0
Sim
ilar t
o ab
ove
(hig
h m
orta
lity
for
preg
nant
wom
en)
Shel
lfish
, any
food
co
ntam
inat
ed w
ith
hepa
titis
viru
s, w
ater
Stoo
l, ur
ine,
bl
ood
Infe
cted
han
dler
s to
uchi
ng fo
od, p
oor
perso
nal h
ygie
ne,
impr
oper
coo
king
, ha
rves
ting
shel
lfish
from
w
ater
s con
tam
inat
ed
with
sew
age,
impr
oper
di
spos
al o
f was
te w
ater
Para
sitic
age
nts
Angi
ostro
ngy-
liasis
(Eos
inop
hilic
m
enin
goen
ceph
aliti
s)
Angi
osgt
rong
ylus
cant
onen
sis (l
ung-
wor
m o
f rat
s) fo
und
in ro
dent
dro
ppin
gs
and
the
soil
From
14
to 1
6 da
ysG
astro
ente
ritis,
he
adac
he, s
tiffn
ess
of th
e ne
ck a
nd
back
, low
-gra
de
feve
r
Crab
s, pr
awns
, slu
gs, s
hrim
p, ra
w
snai
ls
Bloo
dIm
prop
er c
ooki
ng
Toxo
plas
mos
isTo
xopl
asm
a go
ndii
foun
d in
tiss
ues a
nd
mea
t of i
nfec
ted
anim
als
From
10
to 1
3 da
ysFe
ver,
head
ache
, m
yalg
ia, c
utan
eous
ra
sh
Raw
or
unde
rcoo
ked
mea
tLy
mph
nod
es (f
or
biop
sy),
bloo
dIm
prop
er c
ooki
ng o
f m
utto
n, p
ork,
bee
f or
veal

41Burden of foodborne diseases in the South-East Asia Region
Dise
ase
Etio
logi
c ag
ent o
r ca
use
Incu
batio
n pe
riod
(late
ncy)
Sign
s an
d sy
mpt
oms
Food
impl
icat
ed
Spec
imen
s to
be
obt
aine
dCo
ntrib
utin
g fa
ctor
s
Tric
hino
sisTr
ichi
nella
sp
iralis
foun
d in
po
rk a
nd b
ear m
eat
From
4 to
28
days
, av
erag
e 9
days
Gas
troen
terit
is, fe
ver,
oede
ma
arou
nd th
e ey
es, m
yalg
ia, c
hills
, pr
ostra
tion,
diff
icul
ty
brea
thin
g
Pork
, bea
r, w
alru
sM
uscl
e tis
sue
(for
biop
sy)
Inge
stion
of
unde
rcoo
ked
pork
or
bear
mea
t, im
prop
er
cook
ing
or te
mpe
ratu
res,
feed
ing
pigs
with
ga
rbag
e th
at h
as n
ot
been
coo
ked
or p
rope
rly
treat
ed w
ith h
eat
6. A
llerg
ic s
ympt
oms
and
sign
s (fl
ushi
ng a
nd it
chin
g of
the
face
)
Incu
batio
n pe
riod
less
than
1 h
our
Bact
eria
l age
nts (
and
anim
als)
Scom
broi
d po
isoni
ng
(Hist
amin
e Po
isoni
ng)
Hist
amin
e-lik
e su
bsta
nces
pr
oduc
ed
by P
rote
us sp
p.
or o
ther
hist
idin
e ba
cter
ia fo
und
in
the
flesh
of f
ish
From
a fe
w
min
utes
to 1
hou
rH
eada
che,
diz
zine
ss,
naus
ea, v
omiti
ng,
pepp
ery
taste
, bu
rnin
g in
the
thro
at, f
acia
l sw
ellin
g an
d flu
shin
g, c
olic
, itc
hing
Tuna
fish
, blu
e m
acke
rel,
Paci
fic
dolp
hin,
che
ese
Vom
itIn
adeq
uate
refri
gera
tion
of sc
ombr
oid
fish,
im
prop
er c
urin
g of
ch
eese
Chem
ical
age
nts
Mon
osod
ium
glu
tam
ate
poiso
ning
Exce
ssiv
e qu
antit
y of
mon
osod
ium
gl
utam
ate
From
a fe
w
min
utes
to 1
hou
rBu
rnin
g se
nsat
ion
in
the
back
of t
he n
eck,
fo
rear
ms a
nd c
hest;
tig
htne
ss, t
ingl
ing,
fa
cial
flus
hing
, di
zzin
ess,
head
ache
, na
usea
Food
seas
oned
w
ith m
onos
odiu
m
glut
amat
e
U
se o
f exc
essiv
e qu
antit
ies o
f m
onos
odiu
m g
luta
mat
e to
enh
ance
flav
our.
Onl
y so
me
indi
vidu
als a
re
sens
itive
to th
e M
SG
Nic
otin
ic a
cid
poiso
ning
(nia
cin)
Sodi
um n
icot
inat
e us
ed a
s col
our
pres
erva
tive
From
a fe
w
min
utes
to a
n ho
urRe
dden
ing,
hot
fla
shes
, itc
hing
, ab
dom
inal
pai
ns,
swel
ling
of th
e fa
ce
and
knee
s
Mea
t or o
ther
food
to
whi
ch so
dium
ni
cotin
ate
has b
een
adde
d
U
se o
f sod
ium
nic
otin
ate
to p
rese
rve
colo
ur
42Burden of foodborne diseases in the South-East Asia Region
Annex 2 A guide to national burden of foodborne disease study
The FERG’s report on the global burden of foodborne diseases highlights the worldwide threat of FBDs and emphasizes the need for all national governments, the food industry and individuals to work together to make food safe and prevent FBDs. The report also highlights that action to reduce the impact, illnesses and deaths due to FBDs needs to be adapted based on national needs as the types of food contaminants and reasons for their prevalence differ in various regions and countries.
While there is no single, global solution to the problem of FBDs, a strengthened food safety system in one country is likely to positively impact the food safety in other countries. There is need for coordinated action across the entire food supply chain in all countries. WHO is working with national governments to improve surveillance of FBDs to obtain a clear picture of unique local challenges in all countries.
The objectives of individual country studies are to:
• deliver burden of disease estimates in the area of FBDs;
• contribute to strengthening the capacity of countries in conducting burden of foodborne disease assessments, including knowledge translation capacity development within the country; and
• provide results that are translated into food safety policy for the country involved.
The anticipated uses of the results from the burden of foodborne disease studies are:
(1) prioritization of food safety as an issue within a country.
(2) prioritization of specific food safety issues within a country.
(3) provision of a baseline against which to evaluate future food safety interventions,
(4) providing assistance with harmonization of international trade and regulatory standards,

43Burden of foodborne diseases in the South-East Asia Region
(5) assessment of equivalence of food safety controls for import and export risk assessments (e.g. within the context of Codex Alimentarius).
Country studies involve two important parallel activities:
• The collection and analysis of data on the incidence of health effects caused by food hazards so that the burden of disease can be aggregated into the DALY metric using calculation methodology developed by FERG; and
• A situation analysis/context mapping exercise followed by knowledge translation, which facilitates the use of burden information to develop food safety policy in a country.
The following tools and documents, developed by the FERG, shall help national governments in undertaking the studies to estimate the disease burden of FBDs in countries.
1. Online WHO tool
This has been developed to help policy-makers identify the most prevalent FBDs in their regions based on which they could develop appropriate actions to address them in their countries. By looking at the burden of foodborne diseases in different regions of the world, the report may also help countries identify relevant lessons on how to control certain FBDs. The regional burden shall also help prioritize foodborne risks in countries of the SEA Region and the need for further national studies needed to quantify them accurately.
2. Burden of FBDs: appraisal of methodology and development of protocols; burden of foodborne disease: methodology protocol for country studies (WHO-FERG project: written by Haagsma JA, Polinder S and Havelaar AH); August 2011
This document describes a protocol for the measurement of the burden of FBDs and provides information on DALY calculations. It also provides a detailed description of how incidence data may be derived from different data sources and underreporting and under-ascertainment, as sources of uncertainty, are explained in detail. Researchers aiming to undertake the burden of foodborne disease studies in their countries can use this protocol developed under the framework of FERG.

44Burden of foodborne diseases in the South-East Asia Region
3. FERG priority setting tool (WHO, 2012)
This prioritization tool is intended to assist with the identification of agents relevant to the national burden of foodborne disease study. Agents that will be addressed by the FERG in its global and regional burden of foodborne disease studies have been categorized into two groups: (i) global agents of importance in all countries (should be considered by all national burden studies), and (ii) local agents, which are of importance in some specific countries or regions, especially in the case of parasitic hazards.
The tool provides key questions to help countries in determining which foodborne hazards are relevant for their national burden of FBDs study. The list of local agents may be complemented by additional local agents not addressed by FERG but which may still be relevant to the national study.
The list of priority pathogens for a specific national burden of foodborne disease study consists of all “global” and a selection of the “local” agents addressed by FERG and possibly complemented with other agents that are of particular relevance to the country.
4. Data sources checklist (Country Studies Task Force: WHO, 2012)
As a part of the FBDs burden protocol to be used in country studies, this guidance document provides a checklist for participating countries to take stock of existing data required for the national study and is intended to be an aid to data gathering. However, it is neither comprehensive nor exhaustive.
The following information is required for a national FBDs burden study:
(1) Demographic baseline
– Total population for the selected time period, stratified by age and sex;
– Total number of pregnant women and the total number of live births, stillbirths and abortions for the selected time period;
– Local life expectancy table for the selected time period, stratified by sex.
(2) Epidemiological data
– Years of life lost (YLL) parameters: disease mortality, stratified by age and sex;
– Chemicals and toxins: levels in human samples, stratified by age and sex.

45Burden of foodborne diseases in the South-East Asia Region
(3) Food consumption and contamination data
– Qualitative and quantitative description of food consumption;
– Qualitative and quantitative description of food contamination.
This guidance document contains four appendices, which contain additional useful information for the countries undertaking a national burden of foodborne disease study:
Appendix 1: Task Force data sheets
Each of the three agent-specific task forces has generated a list of specific information needed for its priority agents and corresponding data sources. These task force data sheets may guide countries in their data collection process.
Appendix 2: Databases and search engines
Relevant online databases and search engines for scientific and grey literature and online survey catalogues.
Appendix 3: Food consumption atlas data sources
The data sources, identified by the Source Attribution Task Force, will be used for the compilation of a global Food Consumption Atlas. These specific data sources can contribute to the assessment of national food consumption patterns.
Appendix 4: Age groups for estimation of FBDs burden
Where possible, estimates will be made for five-year age groups and separately for males and females. The recommended age groups presented in this appendix coincide with the age groups in the Global Burden of Diseases 2010.
5. Situation analysis/knowledge translation/risk communication manual (FERG, 2013)
This manual addresses the situation analysis/context mapping exercise. The objective is to provide countries undertaking a national burden of foodborne disease study with a guide to situation analysis/context mapping and knowledge translation to support the use of burden of disease information in policy-making.

46Burden of foodborne diseases in the South-East Asia Region
6. FERG workplan matrix for the Country Study Monitoring Matrix (WHO, 2013)
This is a matrix to assist the countries to monitor the progress of their studies and is intended to be customized and adapted based on specific country workplans. The country study monitoring matrix consists of two main sections: content and process of the monitoring exercise. The content section consists of five items – activity, specific tasks, activity leader, timelines and final deliverable/output; and the process section consists of four items – monitoring lead, dates for monitoring and reporting, target audience and comments.
7. National Foodborne Burden of Disease Study: final report draft outline (FERG Country Studies Task Force; WHO, 2013)
This is a draft outline to assist countries to prepare a final report of the country study to estimate the burden of FBDs.

47Burden of foodborne diseases in the South-East Asia Region
Annex 3: Categorization of subgroups under WHO regionsSubregion WHO Member States
AFR D Algeria; Angola; Benin; Burkina Faso; Cameroon; Cape Verde; Chad; Comoros; Equatorial Guinea; Gabon; Gambia; Ghana; Guinea; Guinea-Bissau; Liberia; Madagascar; Mali; Mauritania; Mauritius; Niger; Nigeria; Sao Tome and Principe; Senegal; Seychelles; Sierra Leone; Togo.
AFR E Botswana; Burundi; Central African Republic; Congo; Cote d'Ivoire; Democratic Republic of the Congo; Eritrea; Ethiopia; Kenya; Lesotho; Malawi; Mozambique; Namibia; Rwanda; South Africa; Swaziland; Uganda; United Republic of Tanzania; Zambia; Zimbabwe.
AMR A Canada; Cuba; United States of America.
AMR B Antigua and Barbuda; Argentina; Bahamas; Barbados; Belize; Brazil; Chile; Colombia; Costa Rica; Dominica; Dominican Republic; El Salvador; Grenada; Guyana; Honduras; Jamaica; Mexico; Panama; Paraguay; Saint Kitts and Nevis; Saint Lucia; Saint Vincent and the Grenadines; Suriname; Trinidad and Tobago; Uruguay; Venezuela (Bolivarian Republic of).
AMR D Bolivia (Plurinational State of); Ecuador; Guatemala; Haiti; Nicaragua; Peru.
EMR B Bahrain; Iran (Islamic Republic of); Jordan; Kuwait; Lebanon; Libyan Arab Jamahiriya; Oman; Qatar; Saudi Arabia; Syrian Arab Republic; Tunisia; United Arab Emirates.
EMR D Afghanistan; Djibouti; Egypt; Iraq; Morocco; Pakistan; Somalia; South Sudan; Sudan; Yemen.
EUR A Andorra; Austria; Belgium; Croatia; Cyprus; Czech Republic; Denmark; Finland; France; Germany; Greece; Iceland; Ireland; Israel; Italy; Luxembourg; Malta; Monaco; Netherlands; Norway; Portugal; San Marino; Slovenia; Spain; Sweden; Switzerland; United Kingdom.
EUR B Albania; Armenia; Azerbaijan; Bosnia and Herzegovina; Bulgaria; Georgia; Kyrgyzstan; Montenegro; Poland; Romania; Serbia; Slovakia; Tajikistan; The Former Yugoslav Republic of Macedonia; Turkey; Turkmenistan; Uzbekistan.
EUR C Belarus; Estonia; Hungary; Kazakhstan; Latvia; Lithuania; Republic of Moldova; Russian Federation; Ukraine.
SEAR B Indonesia; Sri Lanka; Thailand.
SEAR D Bangladesh; Bhutan; Democratic People's Republic of Korea; India; Maldives; Myanmar; Nepal; Timor-Leste.
WPR A Australia; Brunei Darussalam; Japan; New Zealand; Singapore.
WPR B Cambodia; China; Cook Islands; Fiji; Kiribati; Lao People's Democratic Republic; Malaysia; Marshall Islands; Micronesia (Federated States of); Mongolia; Nauru; Niue; Palau; Papua New Guinea; Philippines; Republic of Korea; Samoa; Solomon Islands; Tonga; Tuvalu; Vanuatu; Viet Nam.

48Burden of foodborne diseases in the South-East Asia Region
Notes:
(1) The subregions are defined on the basis of child and adult mortality as described by Ezzati et al.4 Stratum A = very low child and adult mortality; Stratum B = low child mortality and very low adult mortality; Stratum C = low child mortality and high adult mortality; Stratum D = high child and adult mortality; and Stratum E = high child mortality and very high adult mortality. The use of the term subregion here and throughout the text does not identify an official grouping of WHO Member States and the subregions are not related to the six official WHO regions, which are AFR = African Region; AMR = Region of the Americas; EMR = Eastern Mediterranean Region; EUR = European Region; SEAR = South-East Asia Region; WPR = Western Pacific Region.
(2) South Sudan was re-assigned to the WHO African Region in May 2013. As this study relates to time periods prior to this date, estimates for South Sudan were included in the WHO Eastern Mediterranean Region.
4 Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, Comparative Risk Assessment Collabo- rating Group (2002) Selected major risk factors and global and regional burden of disease. Lancet 360 (9343):1347–1360. PMID: 12423980.

World Health House
Indraprastha Estate,
Mahatma Gandhi Marg,
New Delhi-110002, India
www.searo.who.int
in the South-East Asia Region
foodborne diseasesBurden of
Globally, billions of people are at risk of foodborne diseases (FBDs) and millions
fall ill from these every year. Many die as a result of consuming unsafe food. FBDs
can also affect economic development through the tourism, agricultural and
food export industries. The South-East Asia Region has the second highest
burden of FBDs after the African Region, with more than 150 million cases and
175 000 deaths annually.
The World Health Organization has launched a comprehensive and first of
its kind report to estimate the global and regional burden of FBDs. This report will
support policy-makers in implementing the right strategies to prevent, detect and
manage foodborne risks to improve food safety. It highlights the work of WHO's
Regional Office for South-East Asia with national governments on improving
surveillance of foodborne diseases and meeting unique local challenges.
9 789290 225034
ISBN 978-92-9022-503-4