bug bites & stings · local reactions normal reaction to an insect bite is an inflammatory...
TRANSCRIPT

BUG BITES & STINGS
Emily Coluccio, PA-S

OUCH!● Insect bites & stings can be mild, but they also have the
ability to transmit insect-borne illnesses and cause severe allergic reactions
● Bites vs. Stings○ Bites consist of punctures made by the mouthparts of the organism○ Stings involve the injection of venom and may cause reactions ranging
from local irritation to life-threatening allergic reactions
● Lesions from arthropod bites (mosquitoes, ticks, kissing bugs, bed bugs, black flies, etc.) usually result from the host's immune reactions to the insect’s salivary secretions or venom

TYPES OF REACTIONS

LOCAL REACTIONS● Normal reaction to an insect bite is an
inflammatory reaction at the site, appearing within minutes, and usually involves pruritic erythema and edema
● Treatment○ Wash with soap and water○ Ice or cold packs may help with swelling○ Topical creams, gels, and lotions (Calamine
or Pramoxine) may help with itching○ Oral antihistamines (Cetirizine or
Fexofenadine) preferred in small children to help with troublesome itching

PAPULAR URTICARIA● Hypersensitivity disorder in
which insect bites (most commonly fleas, mosquitoes, or bed bugs) lead to recurrent and sometimes chrony itchy papules on exposed areas of skin
● Reported predominantly in young children (typically 2-10 years old)○ Diaper area, genital, perianal, and
axillary areas are spared
PAPULAR URTICARIA● There may be a delay between the inciting bite and the onset
of lesions, and new lesions may appear sporadically● Renewed itching may reactivate older lesions, and the
disorder may last from months to years● Treatment
○ Selective and limited use of non-sedating antihistamines for itching○ Mid-potency corticosteroids
● Resolves spontaneously
SYSTEMIC ALLERGIC REACTIONS● Uncommon, widespread activation of mast cells with
prominent flushing and hypotension● Treatment
○ Rapid administration of Epinephrine

TYPES OF BUG BITES & STINGS

MOSQUITOES● Most commonly occurring insect bites● Results in local pain, pruritus, and
erythema● Immediate “wheal-and-flare” response that
peaks at about 20 minutes and/or an indurated pruritic papule that peaks at 2-3 days and resolves over days-weeks
● “Skeeter syndrome”: Dramatic swelling surrounding the bite, heat, redness, itching and pain, which may be accompanied by low-grade fever occurring particularly in young children○ Managed prophylactically with antihistamines
● In rare cases, patients can develop anaphylaxis

MOSQUITOES● Disease Transmission
○ United States - West Nile virus, St. Louis encephalitis, Eastern equine encephalitis, and La Crosse encephalitis
○ Worldwide - Malaria, Yellow fever, Dengue fever, etc.
● Prevention○ Apply insect repellents that contain ingredients such as DEET○ Wear long sleeves and pants when in an environment where mosquitoes
are prevalent
WEST NILE VIRUS● Mosquito-borne illness that can lead to a wide range of
clinical symptoms ranging from asymptomatic disease to severe meningitis and encephalitis
● Seasonal epidemic, with peak around mid-August to early September
● ~1 in 4 people who become infected will become ill and only ~1 in 230 who become infected develops severe symptoms
● Risk factors include advancing age, malignancy, organ transplantation, and genetic factors

WEST NILE VIRUS - CLINICAL MANIFESTATIONS● Most commonly asymptomatic● West Nile fever
○ Self-limited illness, which is indistinguishable from dengue fever and other viral syndromes
○ Abrupt onset of fever, headache, malaise, back pain, myalgias and anorexia
○ Occasionally rash found on chest, back and arms
● Neuroinvasive disease○ Fever in conjunction with meningitis, encephalitis, flaccid
paralysis, or mixed pattern○ Encephalitis more common in older age groups and meningitis more
common in children

TICKS● Primary concern is disease transmission
○ Lyme disease■ Tick-borne illness caused primarily by the
Borrelia burgdorferi species transmitted by ticks in the U.S.
■ Broad spectrum of clinical manifestations which depend on the stage of the illness
○ Rocky Mountain spotted fever (RMSF)● Rarely, tick paralysis and allergic reactions may
occur○ Tick paralysis occurs after a tick has been attached
for 4-7 days. Symptoms include paresthesias, fatigue, and weakness.
○ Some tick bites can sensitize patients to allergens that are found in certain foods such as red meat

LYME DISEASE - EARLY LOCALIZED DISEASE IN CHILDREN● Occurs within the first 2-3 weeks of
infection● Erythema migrans
○ Rash that appears as a red macule at the site of the tick bite, usually within 7-14 days after the bite
○ Most likely to occur on the head or neck in younger children and on the extremities in older children
○ May be pruritic or burning, but rarely painful

LYME DISEASE - EARLY DISSEMINATED & LATE DISEASE● Early Disseminated Disease
○ Occurs weeks to several months after the tick bite
○ Multiple erythema migrans○ Cranial nerve palsy (especially facial nerve
palsy)○ Meningitis○ Carditis○ Fever, fatigue, headache and arthralgia common
● Late Disease○ Occurs weeks to months after the initial
infection if not treated effectively○ Arthritis - usually monoarticular or
oligoarticular, affecting primarily the knee

ROCKY MOUNTAIN SPOTTED FEVER● Caused by infection with Rickettsia rickettsii via
tick-bite● More common in rural and suburban locations● Infected patients become symptomatic 2-14 days after
being bitten

ROCKY MOUNTAIN SPOTTED FEVER - CLINICAL MANIFESTATIONS● Classic symptoms include fever, severe
headache, and rash● Rash usually develops between the third
and fifth days of illness○ Blanching erythematous rash with macules
that become petechial over time ○ Usually begins on the ankles and wrists and
spreads to the trunk○ Rash that appears on the palms and soles is
highly characteristic of RMSF, but usually occurs in later-stage disease
● Other symptoms may include flu-like illness, muscle and joint pain, nausea and vomiting, and abdominal pain

PREVENTION OF TICK BITES & DISEASE● Transmission most likely to occur from May
through October, with a peak in June in northeastern states
● Wear protective clothing● Use repellents that contain DEET or
permethrin● Avoid areas of high vegetation with tall
grass● Carefully examine gear and pets for ticks● Place dry clothes in dryers on high heat for
short period of time after outdoor activities
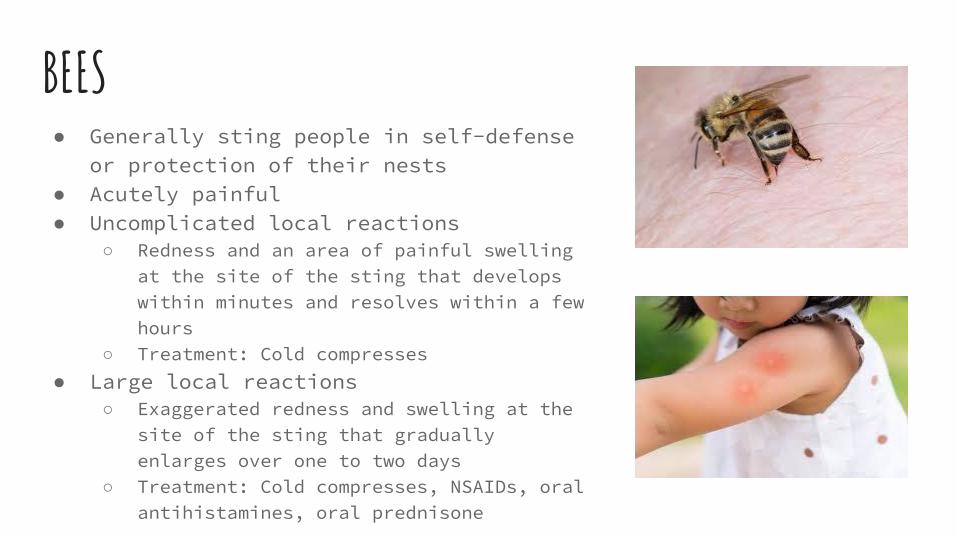
BEES● Generally sting people in self-defense
or protection of their nests● Acutely painful● Uncomplicated local reactions
○ Redness and an area of painful swelling at the site of the sting that develops within minutes and resolves within a few hours
○ Treatment: Cold compresses● Large local reactions
○ Exaggerated redness and swelling at the site of the sting that gradually enlarges over one to two days
○ Treatment: Cold compresses, NSAIDs, oral antihistamines, oral prednisone

BEES● Systemic allergic
reactions/Anaphylaxis○ Can develop at any age, but more
severe in adults○ Develops rapidly○ Generalized urticaria, flushing,
angioedema○ Respiratory symptoms (hoarse
voice, upper airway obstruction)○ Cardiovascular symptoms
(lightheadedness, hypotension)○ Management: IM Epinephrine
● Prevention

LICE● Tiny parasitic insects that can infest
the skin, and live on people’s head● Head lice are very contagious -
spreading by close body contact and shared clothes and other personal items
● Seen mostly in child-care settings and among school-aged children
● Most common symptom is itching, especially at night
● Lice or their eggs (nits) can typically be seen on the hair, behind the ears, or on the neck

LICE● Treatment depends on the symptoms and severity of the
condition● Very treatable - includes applying a medicated cream
rinse or shampoo to your child's hair ● Treatment may also include removing nits from wet hair
with a comb, soaking combs and brushes in hot water and the shampoo, and checking other household members
● Children can return to school or daycare the day after their first treatment for head lice
REFERENCES● Eisen, R. Prevention of Lyme Disease. In: UpToDate, Waltham, MA, 2020.● Freeman, T. Bee, yellow jacket, wasp, and other Hymenoptera stings: Reaction types and
acute management. In: UpToDate, Waltham, MA, 2020.● Freeman, T. Patient education: Bee and insect stings (Beyond the Basics). In:
UpToDate, Waltham, MA, 2020.● Goddard, J. Insect and other arthropod bits. In: UpToDate, Waltham, MA, 2020.● Head Lice in Children - Stanford Children's Health. (n.d.). Retrieved from
https://www.stanfordchildrens.org/en/topic/default?id=lice-90-P01908● Petersen, LR. Clinical manifestations and diagnosis of West Nile virus infection. In:
UpToDate, Waltham, MA, 2020.● Petersen, LR. Patient education: West Nile virus infection (Beyond the Basics). In:
UpToDate, Waltham, MA, 2020.● Sexton, DJ. Clinical manifestations and diagnosis of Rocky Mountain spotted fever. In:
UpToDate, Waltham, MA, 2020.● Shapiro, ED. Lyme disease: Clinical manifestations in children. In: UpToDate, Waltham,
MA, 2020.