breast conserving therapy/ krūts saaudzējošā terapija
TRANSCRIPT

Breast conserving therapy (BCT)
Maksims Tjurins
LU MF 5th year
INTRODUCTION
• Breast conserving therapy (BCT) refers to breast conserving surgery (BCS), followed by moderate-dose radiation therapy (RT) to eradicate any microscopic residual disease.
• The goals of BCT are to provide the survival equivalent of mastectomy, a cosmetically acceptable breast, and a low rate of recurrence in the treated breast.

PATIENT SELECTION FOR BCT
—Although BCT provides an acceptable alternative to mastectomy for the treatment of invasive breast cancer, it is not applicable to all patients

The following issues are emphasized in the appropriate selection of patients for BCT:
• A complete history and physical examination prior to treatment.
• Tissue biopsy with core needle sampling to provide conclusive proof of malignancy. Needle biopsy is preferred over surgical biopsy to reduce unnecessary surgery and avoid scars that may complicate the placement of the subsequent lumpectomy incision.
The following issues are emphasized in the appropriate selection of patients for BCT:
• Accurate histologic assessment of the primary tumor, including histologic subtype, hormone receptor status, and HER2 status
• Once the diagnosis of cancer is made, multidisciplinary coordination among breast and reconstructive surgeons, radiation and medical oncologists, and radiologists and pathologists facilitates treatment planning and streamlines patient care. In some cases, neoadjuvantchemotherapy is warranted to decrease the tumor size and improve the success rate of breast conservation.

The following issues are emphasized in the appropriate selection of patients for BCT:
• Preoperative breast imaging, to define the extent of disease and identify multifocal or multicentric cancer that could preclude breast conservation or potential difficulty in achieving clear surgical margins. Imaging typically includes a combination of bilateral mammographic evaluation, with appropriate magnification views, and ultrasound, if appropriate.
• The tumor size should be included in the mammographic report, as well as documentation of associated microcalcifications, and the extent of the calcifications within and outside the mass.

• Some surgeons may incorporate breast magnetic resonance imaging (MRI) in the work-up of patients considering BCT, however the use of routine MRI in this setting is not indicated.
The following issues are emphasized in the appropriate selection of patients for BCT:

Selection criteria for BCT
• Histologic subtypes other than invasive ductal carcinoma (eg, invasive lobular cancer) are not associated with an increased risk of breast cancer recurrence; these women are candidates for BCT if the tumor distribution is not diffuse and it can be excised with negative margins.

• The presence of an extensive intraductal component (EIC) is an indicator that disease extent may be greater than clinically suspected but is not a contraindication to BCT by itself. Patients with negative margins are still acceptable candidates for BCT.
• Lymph node positivity is a marker of worse prognosis, but positive lymph nodes are not a contraindication for BCT, as BCT and mastectomy have equivalent outcomes independent of nodal metastases.
Selection criteria for BCT

• Tumor location should not influence the choice of treatment. Tumors in a superficial subareolar location may require resection of the nipple-areolar complex to achieve negative margins; oncologic outcomes will not be affected, but the cosmetic result may be.
Selection criteria for BCT
• A family history of breast cancer is not a contraindication to BCT;

Special consideration
Tumor size — Tumor size relative to breast size is an important consideration in selecting patients for BCT. A large tumor in a small breast is a relative contraindication, since an adequate resection would result in significant cosmetic alteration.
Role of neoadjuvant treatment — Neoadjuvant treatment with chemotherapy or hormonal therapy can reduce tumor size significantly and allow for breast conservation

Contraindications
• Multicentric disease with two or more primary tumors in separate quadrants of the breast such that they cannot be encompassed in a single excision.

Contraindications
• Diffuse malignant microcalcifications on mammography.
Contraindications
• A history of prior therapeutic RT that included a portion of the affected breast, which when combined with the proposed treatment, would result in an excessively high total radiation dose to the chest wall.

Contraindications
Pregnancy is an absolute contraindication to the use of breast irradiation; however, it may be possible to perform breast-conserving surgery in the third trimester, deferring breast irradiation until after delivery.
Contraindications
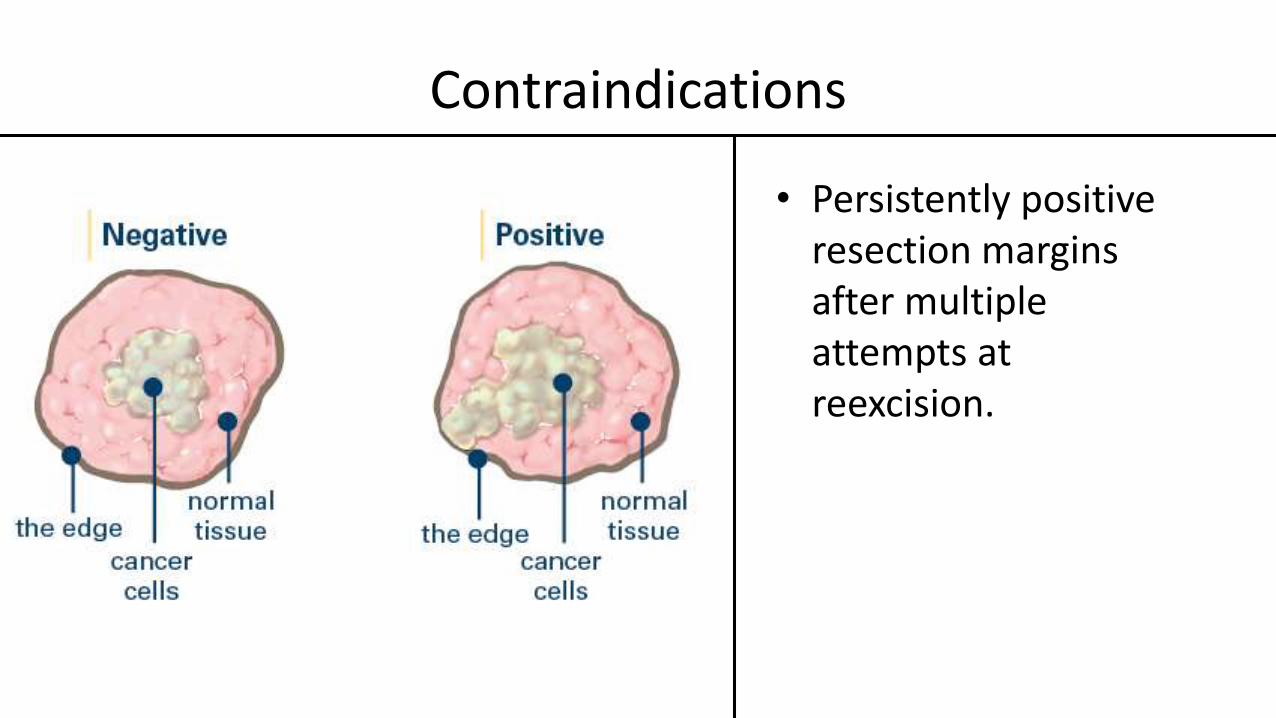
• Persistently positive resection margins after multiple attempts at reexcision.
PREOPERATIVE PREPARATION
• Antibiotics
• Deep venous thrombosis prophylaxis

SURGICAL TECHNIQUE
• The type and location of the incision is important for several reasons. It is imperative to remember that any patient who undergoes lumpectomy may ultimately require a mastectomy, and incisions should be planned with possible mastectomy incisions in mind
• The incision should be placed close to the tumor to avoid extensive tunneling

SURGICAL TECHNIQUE
• In the upper part of the breast, incisions should be curvilinear or transverse and follow the natural skin creases (Langer's lines).

SURGICAL TECHNIQUE
• In the lower part of the breast, the choice of a curvilinear or radial incision is dependent upon the contour of the breast, the distance from the skin to the tumor, and the amount of breast tissue to be resected.
• At the completion of the procedure, the incision should be closed with a subcuticular suture to avoid cross-hatching of the skin.

Evaluation of the axilla
• Evaluation of the axilla provides information for treatment decisions in patients with invasive breast cancer. Sentinel node biopsy is the standard initial approach for patients with a clinically negative axillary examination.

Margins of resection
Microscopic resection margins are the major selection factor for breast conserving therapy (BCT), because of their marked influence on local recurrence. Women with negative excision margins have low rates of local recurrence following BCT, while positive resection margins (ie, carcinoma at the inked margin) are associated with a higher risk of local recurrence.
Indications for wider excision of margins
• The indication for a wider excision following breast conserving surgery is a histologically positive tumor margin identified on the surgical specimen. A positive margin implies a potentially incomplete resection. Patients with a positive tumor margin have an at least twofold increase in ipsilateral local breast cancer recurrence.

Cosmetic outcome
• Many surgical factors will play a role in the ultimate cosmetic appearance of the breast. These include the size and placement of the incision, management of the lumpectomy cavity, and the extent of axillary dissection if necessary.

Cosmetic outcome
• Excellent: The treated and untreated breast are almost identical
• Good: Minimal differences between the treated and untreated breasts
• Fair: Obvious differences between the treated and untreated breasts
• Poor: Major aesthetic sequelae in the treated breast

POSTOPERATIVE COMPLICATIONS
• Seroma
• Infection
• Arm morbidity

Seroma
• Seroma formation occurs in virtually all patients after breast and axillary surgery, and should be considered a transient side effect rather than a major long-lasting complication of these procedures.
• Although all patients will have some serous fluid collect at the surgical site, seromas are not clinically significant in most cases.
• A clinically significant seroma can be defined as a postoperative fluid collection that requires one or more aspirations or subsequent drain placement.

Breast cellulitis and abscess
• Breast cellulitis is an emerging problem in women undergoing breast conserving therapy (BCT)

Arm morbidity
• Arm morbidity is common after breast cancer treatment and can include– arm swelling,– arm pain, – arm numbness, – arm stiffness, – shoulder stiffness, – shoulder pain, – nerve injury.
Arm problems are less common after BCT as compared to mastectomy.

Elderly
• Risk of postoperative complications increases with increasing age as well as associated comorbid illnesses.

Thank you for your attention