blood groups,
TRANSCRIPT

BLOOD GROUPS, BLOOD COMPONENTS
AND ALTERNATIVES TO
TRANSFUSION- Dr. Praneeth Kumar Koduru

• Many lives are saved throughout the world each year through the use of blood transfusions, by preventing death from loss of blood due to trauma, and by allowing performance of surgical procedures which would otherwise be impossible.
• However, it was not until the early nineteen hundreds that routine blood transfusion between humans became possible, following the discovery that genetically determined differences exist between the blood of different individuals.
• These differences must be identified and compatibility ensured before transfusions can be safely carried out.
INTRODUCTION

• Many genetic systems controlling blood groups in humans are known, and they have been of considerable importance in understanding genetics.
• The most important and most commonly used of these is the ABO system.
BLOOD GROUPS

• Patients are grouped by serological testing into either group A, B, AB or O.
• Patients of all groups have a common H antigen on the red cell membrane surface, which is coded for by the H gene on chromosome 19.
• This H antigen may then be acted upon by further enzymes, depending on the presence of ABO genes on chromosome 9.
• Each person inherits two ABO genes.
• The O gene is non-functional so that if an individual has not inherited A and B gene, then the H antigen alone is detected on the red cell surface. Such individuals are group O.
ABO blood groups

• If an individual has inherited A or B gene, then each codes for a specific enzyme which adds a specific sugar to the H gene product producing either the A, B or AB phenotype.
ABO blood groups cont…
Genotype AO or AA BO or BB AB OO

• People form antibodies to any of the ABO antigens that they lack.
• These antibodies appear during the first few months of life due to the exposure to ABH-like antigens in the environment.
• The ABO system is significant because these antibodies are of the IgM type and thus are capable of complete activation of complement through to red cell lysis.
• Therefore, if a mismatched blood is transfused into a patient, a potentially fatal reaction may occur.
ABO blood groups cont…

• The Rh or Rhesus system (discovered in Rhesus monkeys) is a complex system of 45 antigens encoded on chromosome 1.
• The most important is the Rh D antigen, which is highly immunogenic and 90% of individuals exposed to Rh D - positive blood by transfusion will produce anti-D antibodies, which are of IgG type.
The Rh blood group system

• Rh D-negative women may also become sensitized and form anti-D by an Rh D-positive foetus at times when feto-maternal haemorrhage occurs, e.g. at delivery.
• Anti-D is important as it can not only cause a delayed haemolytic transfusion reaction if Rh D-positive blood is transfused, but anti-D antibodies can also cross the placenta.
The Rh blood group system cont…Haemolytic disease of newborn

• Therefore, if a Rh D-negative woman has anti -D and she carries a Rh D-positive baby, anti-D may attach to the foetal red cells and cause haemolysis.
• This may cause either haemolytic disease of the newborn or even death of the foetus due to hydrops fetalis.
• Therefore, a Rh D-negative woman of childbearing age must always receive Rh D-negative blood.
The Rh blood group system cont…Haemolytic disease of newborn

• It is impossible to provide 'identical' or fully matched red cells for transfusion.
• In practice, ABO and Rh D identical blood is provided and in addition, all patients are tested to determine if they have any antibodies to other clinically significant red cell antigens.
• If so, antigen negative blood must be provided to prevent a delayed haemolytic transfusion reaction from occurring.
• Red cell antibodies occur in 3.8 percent of patients.
Other blood group systems

• A patient is tested before each transfusion episode to screen for the presence of antibodies, i.e. a group and screen (G&S) test, by incubating the patient's plasma with two different fully antigen typed 'screening' red cells which are known to possess all the blood group antigens which matter clinically.
• If the antibody screen is negative, any blood which is ABO- and Rh D-compatible could be given. If the antibody screen is positive, the antibody(s) must be identified using a large panel of red cells of known antigen types.
• As antibodies can develop 2 days to 20 weeks after a transfusion episode, a new blood sample is required for antibody screening if the patient has been transfused recently.
Other blood group systems cont…

• The patient's plasma is incubated with the donor red cells from units of blood selected for transfusion to double check that the patient has no antibodies present which could react with antigens on the donor's red cells to cause a delayed haemolytic transfusion reaction.
• Blood is normally reserved for a particular patient for 48 hours.
Crossmatch

• For operations where blood is used in less than a third of procedures, if a patient's group and screen test shows no antibodies are present, a crossmatch is not performed.
• This is safe as in the event of an unexpected bleeding emergency, as no antibodies are present, ABO- and Rh D compatible blood can be provided within 10 minutes.
• However, if a patient's group and screen does show an antibody, a full crossmatch must be done before surgery.
• A maximum surgical blood ordering schedule (MSBOS) is normally compiled by agreement between surgeons, anaesthetists and haematologists and is individually tailored to each hospital, taking into account the procedures performed, operators, logistical arrangements of the blood bank, etc.
Maximum surgical blood ordering schedule (MSBOS)

Maximum surgical blood ordering schedule cont...

• Routine samples are tested in batches, so normally, a G&S requires approximately half a working day to complete, but if the antibody screen is positive, an additional half a working day or more is required.
• Therefore a G&S or crossmatch sample should be sent 24 hours before surgery to ensure that blood can be provided if the patient has an antibody.
• It is safe practice to perform a G&S test on these samples and freeze the plasma until a few days before surgery, then crossmatch blood if required using this sample.(if patient not transfused in last 6 months).
• If a patient has been transfused in recent 6 months, a new sample is required before transfusion can be given.
TIMING OF GROUP AND SCREEN OR CROSSMATCH SAMPLES BEFORE ELECTIVE SURGERY
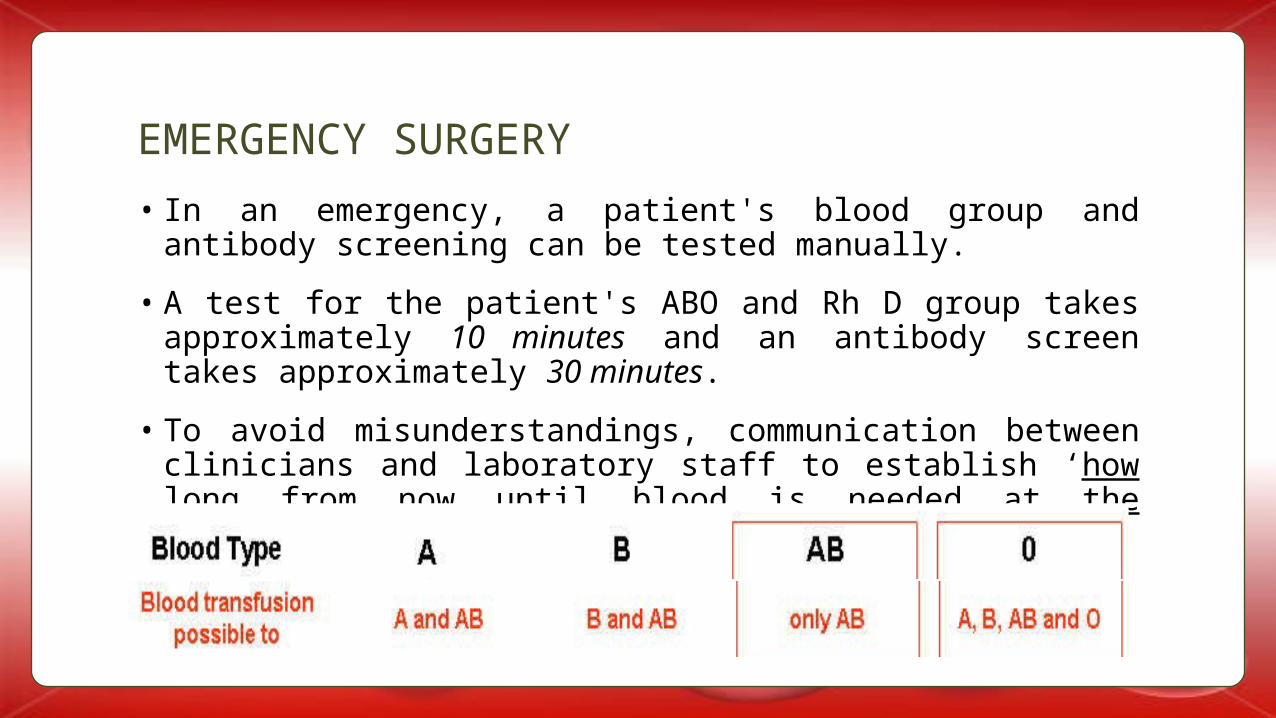
• In an emergency, a patient's blood group and antibody screening can be tested manually.
• A test for the patient's ABO and Rh D group takes approximately 10 minutes and an antibody screen takes approximately 30 minutes.
• To avoid misunderstandings, communication between clinicians and laboratory staff to establish ‘how long from now until blood is needed at the bedside‘ is crucial.
EMERGENCY SURGERY

PROVISION OF
BLOOD IN AN
EMERGENCY

• Whole blood may be split into various components, to allow for efficient use of donated blood…
BLOOD COMPONENTS

• Whole blood is rarely used in modern clinical practice: red cell concentrates, which have had plasma removed for other products, are used in preference.
• Each unit is estimated to raise the Hb concentration in an adult by 1 g/dL.
• Donated blood is collected into a pack containing the anticoagulant citrate phosphate dextrose (CPD) and then after centrifugation, transferred to a pack containing saline-adenine-glucose-mannitol (SAGM) medium suitable for optimal red cell storage.
• Red cells are then stored at 4°C for up to 35 days to minimize proliferation of any contaminant bacteria.
Red cell transfusions

• Blood should be given when the potential benefits outweigh the risks.
• Most hospitals have policies addressing the use of blood and components, as agreed among surgeons and haematologists and based on national guidelines.
• The British Committee for Safety in Haematology guidelines, The clinical use of red cell transfusion, published in 2001, provides useful guidance on when to transfuse patients.
INDICATIONS FOR TRANSFUSION

ACUTE BLOOD LOSS
• Patients with acute massive loss should ideally be managed by experienced clinicians in a suitable setting.
• A blood sample should be sent for the urgent provision of blood according to hospital policy.
• As it is often difficult in such circumstances to estimate blood loss, a classification system is used as a guide to measure hypovolaemic shock.
British Committee for Safety in Haematologyguidelines 2001


According to the British Committee for Safety in Haematology (BCSH) guidelines:
• 15 percent loss of volume (750 mL in an adult or estimate the circulating blood volume by 75 x weight in kg) : No need for blood transfusion unless blood loss is superimposed on pre-existing anaemia or when the patient is unable to compensate for this loss due to pre-existing cardiac or respiratory disease.
• 15-30 percent loss of volume (800-1500 mL in an adult): Need to transfuse crystalloids or colloids.
Requirement for transfusion based on an estimation ofblood loss

The need for red cells is unlikely unless the patient has pre-existing anaemia, reduced cardiorespiratory reserve or if blood loss continues.
• 30-40 percent loss of blood volume (1500-2000 mL): Rapid volume replacement is required with crystalloid or synthetic colloids, and red cell transfusion will probably be required.
• 40 percent loss of blood volume (> 2000 mL) rapid volume replacement including red cells is required.
Requirement for transfusion based on an estimation ofblood loss cont...

• Red cell transfusion is not indicated when estimates of actual and anticipated haemoglobin concentrations are > 10 g/dL.
• Red cell transfusion is indicated when the rate of concentration is < 7 g/ dL. Red cells should be given in relation to ongoing red cell loss.
• If the patient is otherwise stable, two units of red cells should be transfused in adults and then the clinical situation and haemoglobin concentration should be reassessed.
• The correct strategy for transfusion of patients with haemoglobin concentrations between 7 and 10 g/dL is less clear.
Requirements for red cell transfusion based onhaemoglobin concentration

• Clinicians often transfuse red cells, although the available evidence suggests this is not often justified.
• In patients who may tolerate anaemia poorly, e.g. patients over the age of 65 and patients with cardiovascular disease, consider adopting a higher haemoglobin level at which transfusions are indicated.
• These guidelines provide a framework for clinical transfusion, but the decision to transfuse should be based on the individual patient's circumstances.
Requirements for red cell transfusion based onhaemoglobin concentration cont...

• Plasma is separated from whole blood by centrifugation and frozen to -30°C within six hours of its collection.
• Thawing of FFP takes about 30 minutes from the time of request and should be used within two hours for it to maintain its optimal clinical effectiveness.
• It cannot be refrozen for further storage.
• Shelf life – 1 year
• Dose – 12 to 15 ml/kg
• FFP should be ABO-compatible to avoid a mild haemolytic reaction due to anti-A or anti-B in the FFP.
Fresh frozen plasma
• FFP is not crossmatched, but the patient needs to have had a G&S test.
• A small amount of red cell contamination may be present in FFP so women of childbearing age should therefore receive Rh D-compatible FFP to prevent possible sensitization.
• In an emergency situation if Rh-positive FFP has to be issued to Rh D-negative women, i.m. anti-D can be administered to prevent immunization.
INDICATIONS
• National BCSH guidelines give recommendations for the use of FFP -
Fresh frozen plasma cont...

Definite
• thrombotic thrombocytopenic purpura (TTP);
• acute disseminated intravascular coagulation (DIC);
• immediate reversal of warfarin effect;
• replacement of single coagulation deficiencies where a specific or combined concentrate is unavailable;
• vitamin K deficiency;
• C1 esterase inhibitor deficiency.
Fresh frozen plasma cont...

Disseminated intravascular coagulation
• Disseminated intravascular coagulation leads to deficiencies in coagulation factors particularly V, VIII and fibrinogen, and platelets.
• In patients who are actively bleeding and in whom laboratory tests indicate DIC.., FFP, platelets and cryoprecipitate are often required.
• Subsequent therapy should be based on repeat coagulation tests and with the guidance of haematological colleagues.
• In chronic DIC or DIC without haemorrhage, there is no indication for FFP just to normalize laboratory results.
Fresh frozen plasma cont...

Vitamin K deficiency
• Patients who present to surgical teams with biliary obstruction may have impaired absorption of the fat soluble vitamin K and therefore have a deficiency of vitamin K-dependent coagulation factors.
• If immediate correction is required, e.g. for haemorrhage or imminent surgery, FFP is indicated.
Fresh frozen plasma cont...

Reversal of warfarin effect
• In an emergency, FFP (or prothrombin complex concentrate) can be used to reverse warfarin effects.
• In elective surgery, the risks of potential adverse effects of FFP must be balanced against the urgency of the surgery, and should be discussed with the patient, before deciding whether to reverse the effect of warfarin or postpone the elective surgery to allow the warfarin to be stopped ahead of surgery.
• Recommendations from the BCSH guidelines -
Fresh frozen plasma cont...

Fresh frozen plasma cont...

Conditional use of fresh frozen plasma
• In cases of massive transfusion (> 5 L in 24 hours), dilution of clotting factors may occur.
• In patients who are hypotensive or septic, DIC may also complicate cases of massive transfusion.
• In most hospitals, the first dose of FFP (12-15 mL/kg) is given empirically as laboratory coagulation results take at least 25 minutes to obtain, but subsequent use of FFP should be based on the results of repeated coagulation screens.
• Platelet and fibrinogen levels may also be required. The platelet count should be kept above 50 x 109/L. If the fibrinogen level is < 0.8 g/L, cryoprecipitate should be given.
Fresh frozen plasma cont...

Liver disease
• Patients who have liver disease may need FFP if they have bleeding associated with a coagulopathy.
• They may have significantly expanded plasma volumes (due to ascites and/or oedema) and the coagulopathy may be difficult to correct with FFP alone.
• If six to eight units of FFP fail to correct the coagulation tests in a bleeding patient, pro thrombin complex concentrate may be indicated, in spite of the associated increased risk of thrombosis.
Fresh frozen plasma cont...

Fresh frozen plasma is not indicated in the following:
• hypovolaemia;
• immunodeficiency;
• nutritional support/protein loss states;
• plasma exchange procedures, unless there is an underlying coagulopathy.
Fresh frozen plasma cont...

• This is a product rich in factor VIII and fibrinogen and is made by thawing fresh frozen plasma overnight at 4-8°C. It is stored at -300C and shelf-life is 2 years.
• Each unit provides -
• Fibrinogen 150-250mg
• Factor VIII 80-150 U
• Von willebrand factor 100-150 U
• Factor XIII 50-75 U
• It also contains Fibronectin, but there are no clear indications for fibronectin replacement.
CRYOPRECIPITATE

• Indications for cryoprecipitate include
• treatment of DIC, where the fibrinogen is < 1 g/L and
• in rare cases of fibrinogen deficiency
• Haemophilia
• Von willebrand disease
• Uremic bleeding tendency
• Massive hemorrhage
CRYOPRECIPITATE cont...

Platelet collection and storage
• Platelet concentrates (contain 250 x 109 / L) are produced either by pooling platelets derived from four separate donations of whole blood or as single donor platelets which are obtained by apheresis.
• For optimal platelet function, platelets, unlike red cells, are stored under conditions of gentle agitation (to prevent clumping) at a temperature of 22 ± 2°C.
• However, the shelf-life is limited to five days because of the risk of bacterial proliferation at this storage temperature.
PLATELETS

• Sepsis secondary to platelet transfusion is more common than red cell infusion and therefore platelets should only be used when necessary.
• In the ENT setting, if patients have mild oral haemorrhage, the antifibrinolytic agent tranexamic acid may be a valuable alternative either as tablets or as an effective mouthwash suspension.
Indications for platelet transfusion
• The cause of thrombocytopenia should be established as soon as possible so that the most appropriate treatment can be given and so that platelets are not given in conditions where they could cause harm.
• Serious spontaneous haemorrhage due to a low platelet count alone is unlikely to occur at platelet count > 10 x 109/L.
PLATELETS cont...

• BCSH guidelines suggest in stable thrombocytopenia, a threshold of 10 x 109/L for platelet transfusion, in the absence of any additional risk factors, e.g. sepsis, antibiotic use or other abnormalities of haemostasis.
Recommendations for platelets as surgical prophylaxis
The platelet count should be kept above > 50 x 109/L for:
• lumbar puncture;
• epidural anaesthesia;
• gastroscopy and biopsy;
• insertion of indwelling lines;
PLATELETS cont...
• transbronchial biopsy;
• liver biopsy;
• laparotomy or similar procedures.

• For operations at critical sites such as the eye and brain, the platelet count should be kept > 100 x 109/L.
• Prior to a procedure, it is essential to repeat the platelet count after platelets have been transfused to ensure an adequate increment has been achieved.
• Platelets may be required in massive transfusion or in acute DIC and in each the platelets should be kept > 50 x 109/L.
• Again repeated platelet counts are invaluable in acting as a guide to therapy.
• In chronic DIC, platelet transfusion is not routinely given to correct the thrombocytopenia.
PLATELETS cont...

Contraindications to platelet transfusion -
Heparin induced thrombocytopenia (HIT). In such cases, platelet transfusion has been associated with acute arterial thrombosis.
Thrombotic thrombocytopenic purpura (TTP). Platelet infusions are contraindicated as they have been associated with TTP exacerbation: FFP is the treatment of choice.
PLATELETS cont...

In spite of stringent measures to minimize bacterial contamination of donated blood, bacterial contamination still rarely occurs.
Therefore, all platelets in particular, should be checked at all stages, including at the bedside, for any possible leak or damage to the bag.
Any change of colour or turbidity must be regarded as suspicious of contamination and discussed with the transfusion laboratory.
MEASURES TO AVOID TRANSMISSION OF BACTERIAL INFECTION VIA BLOOD COMPONENTS -

Strict eligibility criteria are applied to prevent harm to either the patient or the donor as a result of blood donation.
• Blood is taken from healthy adult donors aged between 17 and 70 years.
Blood donation is voluntary so that there are no incentives for donors to withhold information about their health and put patients or themselves at risk.
The avoidance of the transmission of infection to the recipient of blood products is of paramount importance in transfusion medicine.
Donors at high risk of infections are excluded.
Donors are therefore questioned extensively before donation proceeds.
BLOOD DONATION -

• Collection of 450 mL of blood is by strict aseptic technique.
• Blood is currently tested for a number of markers of infection but there is a 'window period' for each, when the donor may have recently acquired an infection but the marker will not yet be detected
BLOOD DONATION cont...

• Cytomegalovirus (CMV) negative components are only provided for patients at risk of developing severe manifestations of CMV, e.g. neonates, pregnant women, bone marrow transplant patients.
• Testing for malaria and Trypanosoma cruzi is also undertaken where appropriate.
• There is no evidence at present to suggest that Creutzfeldt-Jakob disease (CJD) or variant CJD (vCJD) is transmissible to humans via blood products.
BLOOD DONATION cont...
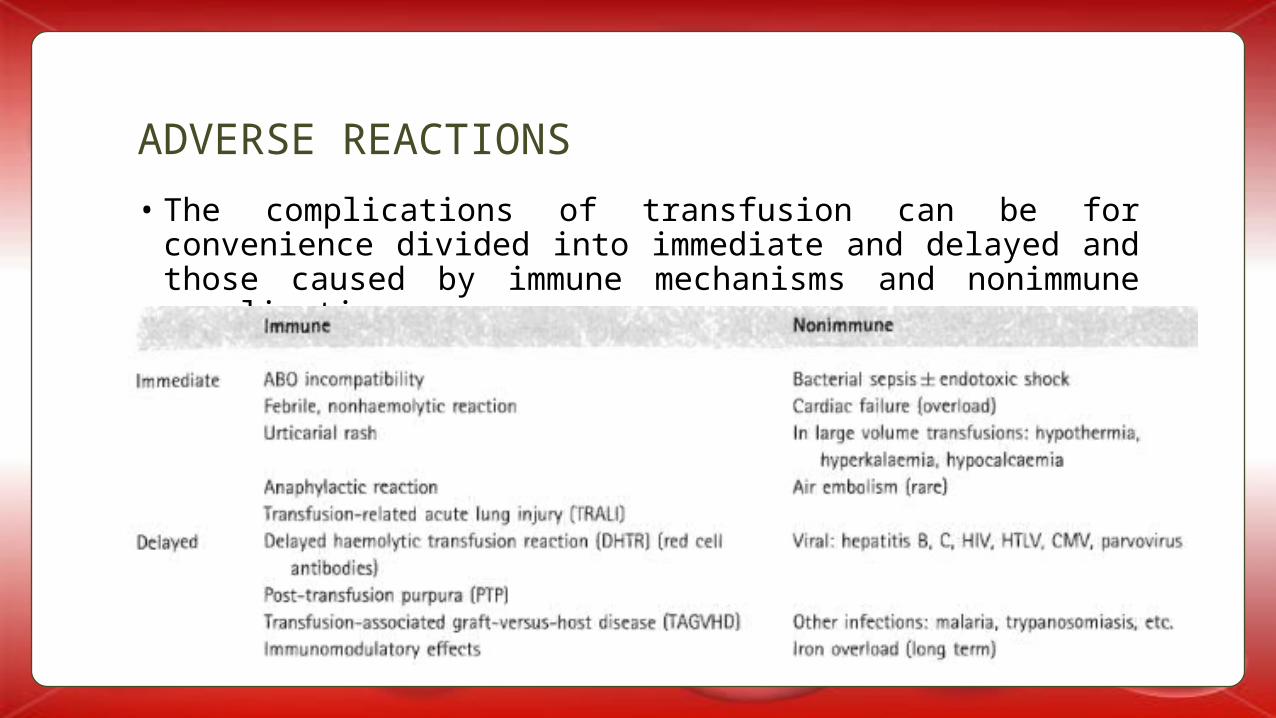
• The complications of transfusion can be for convenience divided into immediate and delayed and those caused by immune mechanisms and nonimmune complications -
ADVERSE REACTIONS

Immediate transfusion reactions -
ABO INCOMPATIBILITY
• This is the most dangerous of transfusion reactions and can prove fatal.
• The reaction often starts within the first hour of the transfusion and monitoring the patient's observations is important in detecting a reaction early.
• ABO mismatch is totally preventable and mostly are due to human error in checking the patient's identity at the bedside before transfusion begins.
• In addition, errors in labelling of crossmatch or G&S samples can be prevented by labelling the sample at the bedside, from the patient's wristband only.
ADVERSE REACTIONS cont...

• Mortality in cases of intravascular lysis secondary to ABO incompatibility is significant and of the order of 10 percent.
• From the annual Serious Hazards of Transfusion (SHOT) reporting scheme in the UK, two to four patients die each year and a further five to ten have serious morbidity (e.g. require renal dialysis or admission to the intensive therapy unit (ITU)) as a result of 'wrong blood' errors.
• A further 25-30 have the wrong blood given, but with no adverse effect, e.g. because they receive group O in error.
• Clinically, the patient experiences headache, lumbar back pain, chest tightness, nausea or facial flushing.
ADVERSE REACTIONS cont...

• Examination of the patient may reveal tachycardia and hypotension.
• Fever and rigors typically follow.
• Microscopic or in severe cases macroscopic haematuria may be seen.
Treatment consists of stopping the transfusion, giving i.v. fluids, resuscitation and management of renal failure.
The blood unit and further samples for G&S, full blood count, coagulation screen, biochemistry and a urine for haemoglobinuria should be sent to the laboratory and discussed with a haematologist.
ADVERSE REACTIONS cont...

BACTERIAL INFECTION
• Very similar symptoms of fever, tachycardia and hypotension also occur with infected blood components being transfused.
• Antibiotics need to be given before a definitive diagnosis is made.
• This should be done in accordance with the hospital's current antibiotic protocol.
• Management of the patient is again by resuscitation and plain fluids and treatment of any renal failure.
ADVERSE REACTIONS cont...

FEBRILE, NON HAEMOLYTIC TRANSFUSION REACTIONS
• Patients may develop a fever and sometimes rigors during transfusions.
This is thought to be due to release of cytokines during storage, but has not been prevented totally by leukodepletion.
These reactions are harmless but clinicians must make sure that severe reactions, e.g. bacterial sepsis or wrong blood reactions are not mistaken for these.
ADVERSE REACTIONS cont...
ALLERGIC REACTIONS
• These may occur when a blood component contains a plasma protein to which the patient is allergic and has IgE antibodies and occur in about 1 percent of transfusions.
• They often result in mild urticarial reactions and are usually treated with an antihistamine with or without hydrocortisone.
• However, severe reactions may rarely occur leading to anaphylaxis. These may be seen in patients who are deficient in IgA, who may make anti-IgA antibodies, which can react with IgA normally present in blood components, causing anaphylaxis.
ADVERSE REACTIONS cont...

TRANSFUSION-RELATED ACUTE LUNG INJURY
• This is a rare but often severe complication. During, or soon after transfusion, particularly of FFP or platelets, patients became markedly hypoxic, dyspnoeic and may require ventilation and it is sometimes fatal.
• Transfusion related acute lung injury (TRALI) is caused by anti leukocyte (or neutrophil) antibodies in the donor's plasma, which match the specificity of the patient's white blood cells (WBC) causing aggregation of WBC in the patient's lung vasculature, causing tissue destruction.
FLUID OVERLOAD
• This can be avoided by giving a diuretic with alternate units of blood if necessary.
ADVERSE REACTIONS cont...

LARGE VOLUME TRANSFUSION
• Hypothermia may occur and can be minimized by infusing blood via a blood warmer.
• Hyperkalaemia, due to a large volume of stored blood, in which red cells have leaked some potassium, does not usually require treatment but electrocardiogram (ECG) monitoring is advisable.
• Hypocalcaemia, due to citrate anti-coagulant in stored blood, does not usually require treatment.
ADVERSE REACTIONS cont...

Delayed haemolytic transfusion reactions
PREMATURE DESTRUCTION OF TRANSFUSED RED CELLS
• Transfused red cells are destroyed prematurely (normal red cell life span 120 days) due to the presence of antibodies in the patient’s plasma which are directed at antigens on the donor’s RBC.
• Such reactions usually occur between 7-10 days post-transfusion and may manifest as a mild anaemia, a rise in serum bilirubin level and often an accompanying fever.
• The drop in haemoglobin is proportional to the quantity of red cells transfused, i.e. larger volume transfusions manifest with a greater drop in haemoglobin.
• Occasionally, transfusion reactions occur within 24 hours of the transfusion.
ADVERSE REACTIONS cont...

POST-TRANSFUSION PURPURA
• Profound thrombocytopenia (<10) associated with purpura and occasionally severe bleeding, may occur about 7-10 days post-transfusion and is caused by the presence of antiplatelet antibodies, usually antiHPA 1a in the recipient.
• The resulting platelet destruction occurs in both autologous and transfused platelets due to cross-reaction or by the formation of immune complexes.
• Intravenous immunoglobulin is the treatment of choice.
• Platelet transfusion is unhelpful and not warranted unless life-threatening bleeding occurs. The differential diagnosis postoperatively often includes heparin-induced thrombocytopenia.
ADVERSE REACTIONS cont...

TRANSFUSION-ASSOCIATED GRAFT-VERSUS-HOST DISEASE
• Transfusion-associated graft-versus-host disease (TAGVHD) occurs in severely immunosuppressed patients or could occur in those receiving blood from first-degree relatives.
• It is caused by viable T lymphocytes in the donor’s blood which attack the patient’s tissues causing a skin rash, liver failure, severe diarrhoea and bone marrow failure and is uniformly fatal.
• It is preventable by irradiating blood components for susceptible patients.
ADVERSE REACTIONS cont...

IMMUNOMODULATORY EFFECTS
• Transfusion may be associated with an increase in post- operative sepsis (away from the wound site) and increased tumour recurrence rates (e.g. in cancer of the colon), but there are conflicting results and the same results are apparent whenever allogeneic (donor) blood or autologous blood is used. Further studies are needed to clarify this.
ADVERSE REACTIONS cont...

IRON OVERLOAD
Repeated transfusions in some patients, such as those with thalassaemia or sickle cell disease, may result in the gradual accumulation of iron with subsequent organ deposition (heart, pancreas, etc.).
Such patients are managed with iron-chelating agents.
Any patient with a haemoglobinopathy, who is due to undergo surgery, should be discussed jointly with both the haematologist and anaesthetist well in advance of any procedure.
ADVERSE REACTIONS cont...

• The fact that blood transfusion is not a zero risk intervention has led to attempts to introduce alternative therapies which reduce the need for allogeneic blood components.
• Such technologies may be useful for individual patients who decline transfusion on the grounds of religious teachings and beliefs.
ALTERNATIVES TO TRANSFUSION

Autologous transfusion
PREOPERATIVE AUTOLOGOUS DEPOSIT
• Preoperative autologous deposit (PAD) is of use only in those patients who have planned elective surgical procedures.
• Patients who are fit enough to donate blood, can take oral iron supplements and donate one unit (450 mL) of blood at weekly intervals in the four weeks leading up to surgery, provided their haemoglobin recovers adequately between weekly donations.
• In practice, patients donate two or three units at most. These donations are then subject to the same storage and handling procedures as for other donated units but kept solely for the use of the donor at a subsequent time. Such a procedure requires considerable planning and liaison between surgical firms and the local blood service.
ALTERNATIVES TO TRANSFUSION cont...

• The other pitfall of autologous donation in clinical practice, is that as the amount of blood that can be used from autologous donation is limited, complications at the time of the planned procedure may mean that allogeneic transfusion may be needed in addition.
• Although regarded as safer than allogeneic transfusion from the point of view of viral transmission, it does not eliminate the risk of bacterial contamination or receiving the ‘wrong blood’.
• Autologous transfusion in clinical practice is also limited by the five-week shelf-life of red cells so that if surgery is postponed, the blood expires.
ALTERNATIVES TO TRANSFUSION cont...
• Many clinicians now prefer to ensure that patients are not anaemic before surgery, allow patients to run a lower haemoglobin postoperatively before requiring transfusion and give patients iron supplements.
ACUTE NORMOVOLAEMIC HAEMODILUTION
• Just before induction of anaesthesia at operation, 0.5–1 L (one to two units) of a patient’s blood can be removed, using a blood collection pack containing anticoagulant, and replaced with crystalloid fluid to maintain normovolaemia.
• Following blood loss during surgery, the patient’s own blood can be returned. This technique has very limited use as the amount of blood that can be removed is limited, the patient must be fit enough to withstand this and often, allogeneic blood is still needed in addition to the patient’s own.
ALTERNATIVES TO TRANSFUSION cont...

CELL SALVAGE
Blood lost can be salvaged either
• (1)during surgery: intraoperative cell salvage, which requires expensive equipment to suction, anticoagulate, wash, centrifuge and filter the blood or
• (2) after surgery: postoperative cell salvage, which requires just a modified drain, in which blood is collected for six hours then simply filtered and reinfused.
• These techniques can be used in a variety of surgical operations, but generally, intraoperative cell salvage is used only where >1 L blood loss is likely and neither is appropriate where the surgical field is bacterially contaminated.
ALTERNATIVES TO TRANSFUSION cont...

RECOMBINANT ERYTHROPOIETIN
• Recombinant erythropoietin (rEpo) is currently widely used in a number of chronic and malignant conditions, such as chronic renal failure and multiple myeloma,
to avoid repeated transfusions and the complications that accompany them.
• It can be used in the weeks prior to surgery in patients in whom transfusion with allogeneic blood would be a problem (e.g. Jehovah’s witnesses).
• Other alternative treatments to avoid the use of allogeneic blood are directed at reducing blood loss.
Other methods to reduce red blood cell transfusion

FIBRIN GLUE
• One syringe containing calcium and human thrombin and another containing human fibrinogen are mixed directly when injected simultaneously at the point of bleeding.
• Subsequent reaction leads to the formation of fibrin clot achieving haemostasis.
• This ‘glue’ is now widely used in accident and emergency departments and at minor injury clinics for the treatment of minor cutaneous bleeds.
Other methods to reduce red blood cell transfusion cont...

TRANEXAMIC ACID
• Tranexamic acid is an antifibrinolytic agent and can be used for the treatment of minor bleeds, such as bleeds in the oral cavity.
HAEMOGLOBIN SUBSTITUTES
• There are available acellular preparations of human haemoglobin.
• Such products are interesting prospects in that they would remove the risk of bacterial, viral and prion transfusion.
• Unfortunately, at the present time, such preparations are of limited clinical use in areas of acute trauma resuscitation mainly became of their relatively short half-life of around 24 hours.
• Such preparations are only currently on limited licences in the United States and South Africa.
Other methods to reduce red blood cell transfusion cont...

SYNTHETIC OXYGEN CARRIERS
• O2-carrying synthetic compounds such as perfluorocarbons (PFC) require high flow oxygen available to the patient for them to be of any significant value to the patient.
• Therefore, their application in the clinical arena is limited to situations such as intensive therapy where patients can be highly monitored.
• Their half-life is very short.
Other methods to reduce red blood cell transfusion cont...
SAVE LIVES