bilateral spontaneous pnuemothoraces with pleuro pleural communication
TRANSCRIPT
BILATERAL SPONTANEOUS PNUEMOTHORACES WITH
PLEURO-PLEURAL COMMUNICATION
Dr. Nabajyoti Hazarika,
Dept of Cardiothoracic & Vascular Surgery,Gauhati Medical College Hospital
Under guidance of Prof. & HODDr. A. Rai Baruah, CTVS Deptt.,
GMCH
INTRODUCTION Simultaneous spontaneous bilateral
pneumothoraces, the presentation of separate right and left pneumothoraces together, is a rare event.
The pleural cavities in humans are separated completely and the only previous reports of pleuropleural communication have been associated with major invasive thoracic procedures, specifically mediastinal surgery.
The term “buffalo chest” has been coined for the condition on the basis that the buffalo or bison has a single pleural cavity, one of the few mammals to do so.
This proved a disadvantage for the North American buffalo, as a single arrow strike from a Native American into the buffalo's chest would probably cause both lungs to collapse, rendering the animal incapacitated
A Turkish surgeon Şerafeddin Sabuncuoğlu (1385–1468), endorsed an early description of traumatic pneumothorax secondary to rib fractures appears in Imperial Surgery, which was also recommends a method of simple aspiration.
Itard and Laennec reIn 1803 by Jean Marc Gaspard Itard, a student of René Laennec, who provided an extensive description of the clinical picture in 1819 in regards to Pneumothorax
Itard and Laennec recognized that some cases were not due to tuberculosis (then the most common cause), the concept of spontaneous pneumothorax in the absence of tuberculosis (primary pneumothorax).
History
Reintroduced it by the Danish physician Hans Kjærgaard in 1932.
In 1941, the surgeons Tyson and Crandall introduced pleural abrasion for the treatment of pneumothorax.
Prior to the advent of anti-tuberculous medications, pneumothoraces were intentionally caused by healthcare providers in people with tuberculosis in an effort to collapse a lobe, or entire lung, around a cavitating lesion.
This was known as "resting the lung". It was introduced by the Italian surgeon Carlo Forlanini in 1888, and publicized by the American surgeon John Benjamin Murphy in the early 20th century (after discovering the same procedure independently).
Murphy used the (then) recently discovered X-ray technology to create pneumothoraces of the correct size.
The surface of the inner wall of lung is lined by a serous membrane.
Consists of a single layer of flat epithelium with a thin underlying propria.
The visceral pleura covers the outer surface of the lung.
THE PLEURA & PLEURAL CAVITY
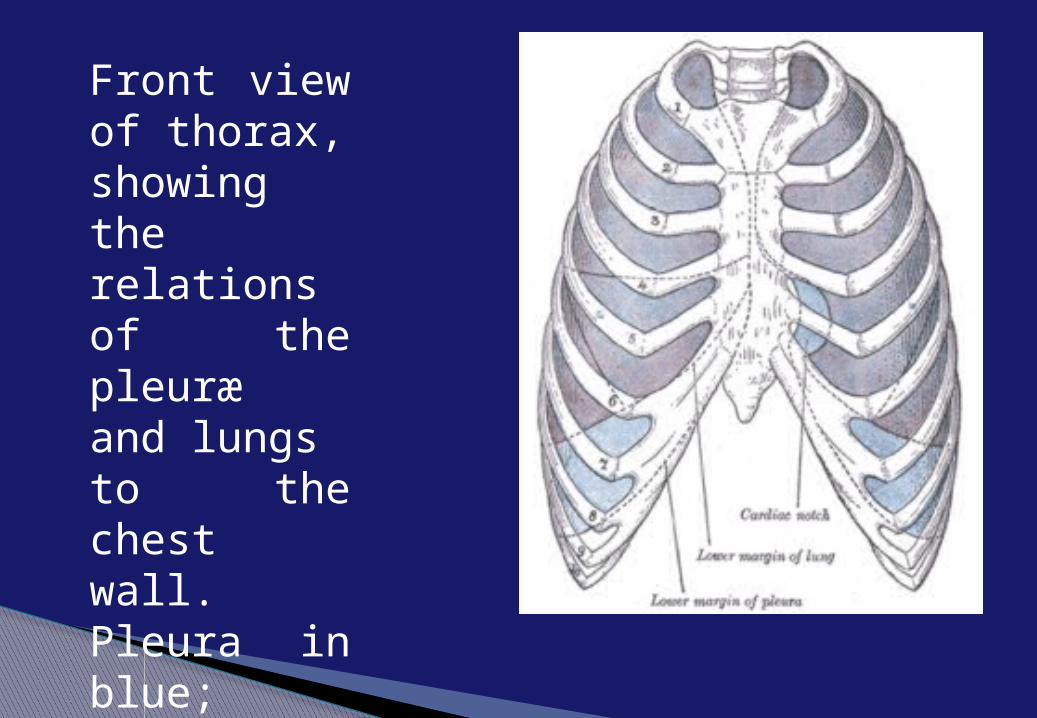
Front view of thorax, showing the relations of the pleuræ and lungs to the chest wall. Pleura in blue; lungs in purple.
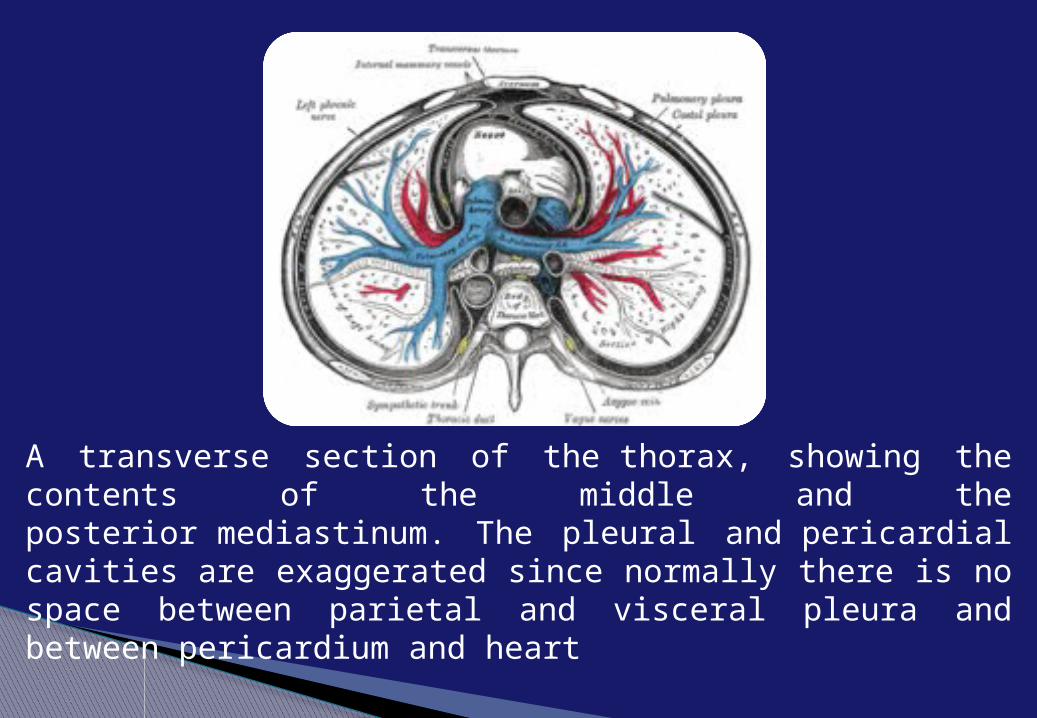
A transverse section of the thorax, showing the contents of the middle and the posterior mediastinum. The pleural and pericardial cavities are exaggerated since normally there is no space between parietal and visceral pleura and between pericardium and heart
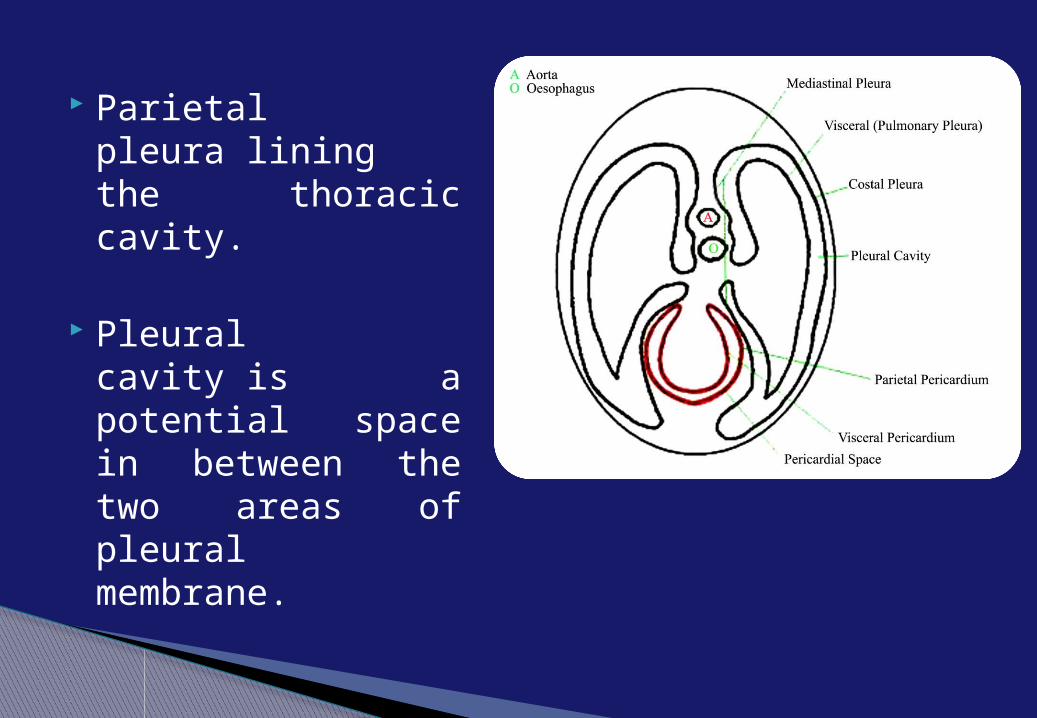
Parietal pleura lining the thoracic cavity.
Pleural cavity is a potential space in between the two areas of pleural membrane.
A pleura is a smooth membrane folded over itself to create a two-layered membrane with a space in between known as the pleural cavity.
During inhalation and exhalation, the pleurae easily slide against each other with the aid of the slippery fluid in the pleural cavity, allowing for optimal functioning of the lungs.
The surface tension created by the pleurae also keep the lungs' surfaces close to the chest wall, allowing the alveoli to take in more air when breathing.
What is the function of the pleura?
The pleurae normally secrete small amounts of pleural fluid that act as a lubricant for the lungs.
Protections to the lung is also one of the very much important function of the pleura.
Negative Pressure that is crucial for keeping the lungs from collapsing after an exhale.
The importance of pleural membranes can be seen in instances when the membrane is pierced.
This results in the air entering the space between the two pleural membranes.
The lung is not held in their proper place, recoils and cannot expand anymore, thus breathing in this lung stops.
This condition is called pneumothorax, and the treatment for this condition is to seal the hole in the pleural membrane.
Louisiana State University Medical School states that there are two areas of muscles that expand the chest cavity, and thus the lungs, decreasing their internal
pressure. These include the diaphragm and the muscles that draw the ribs up and out. The diaphragm is a sheet of muscle between the organs of the chest and abdomen that lowers during inhalation. The diaphragm is the primary muscle powering inhalation. In both cases, inhalation requires that the muscles contract actively, while exhalation is caused by the relaxation of both the rib muscles and the diaphragm in quiet breathing. In forced breathing, such as during heavy exercise, other muscles cause exhalation to occur faster. These include the abdominal muscles, which decrease the abdominal volume, and opposing rib muscles, which quickly decrease the volume of the chest cavity. In either case, as with inhalation, exhalation is accomplished through changing the air pressure in the lungs relative to the surrounding air pressure
CASE REPORT A 72 yr male presented to emergency
department recent sudden onset breathlessness (6 hrs) with chest pain on deep inspiration
He had a past history of tuberculosis more than 30-40 yrs back . No recent history of hospital visit ever since .
A retired military officer with no previous history of trauma , surgery or smoking .
On initial examination the patient was distressed ,fatigued and pale , unable to speak due to respiratory distress (RR-50-55/min), drowsy despite oxygen mask support of 8-10 L//h. .
On auscultation left hemithorax air entry was significantly reduced both anteriorly and posteriorly . Right hemithorax air entry was present only in lower anterior / posterior regions
CASE REPORT
Portable saturation monitor measurements were sp02 70-72% , HR 140 /m
Chest radiograph suggested bilateral pnuemothoraces with partial collapse of both left lobes , tracheal shifting to right side of midline , complete collapse of right upper lobe .
CASE REPORT
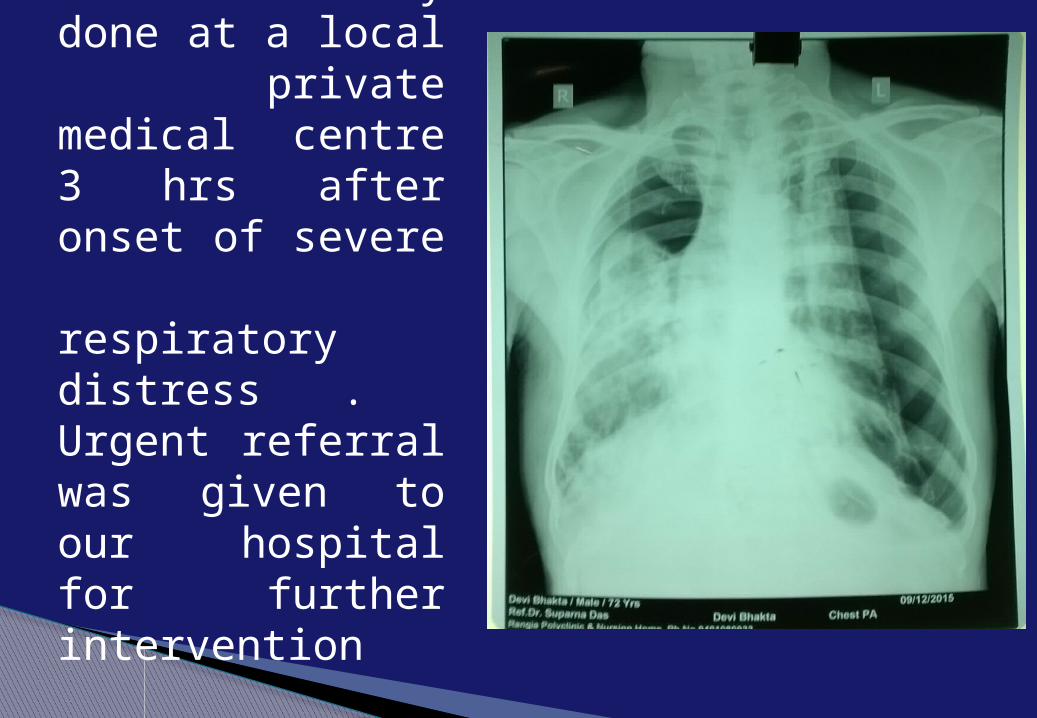
Chest x ray done at a local private medical centre 3 hrs after onset of severe respiratory distress . Urgent referral was given to our hospital for further intervention
Urgent chest tube insertion was warranted in this patient and it was decided to first improve patient saturation by left sided chest tube insertion.
A size 32 French Inter-coastal drainage cathether (non –trocar) was inserted via the 6th intercoastal space in Mid-axiallary line under local aneasthesia (lignocaine 2%) and connected to a under water-seal drainage container .
Continuous Negative suctioning of container was done @ 5-10 mm hg .
CASE REPORT
Post chest tube insertion there was dramatic recovery of patient saturation and consciousness .
Patient was managed in medical high dependency unit for correction of respiratory acidosis ,saturation monitoring, 4 hrly nebulisation with bronchodilators and 8 hrly analgesics
CASE REPORT
AN UNEXPECTED FINDING!!!!! New chest radiograph revealed expanded left lung with
minimal expansion of right upper lobe ,an unexpected finding . Right side chest tube insertion was withheld due to demonstrable resolution of bilateral pneumothoraces .
Vigourous physiotherapy and deep breathing exercises were initiated in hopes of complete re-expansion of remaining collapsed right upper lobe
Patient was shifted to general ward on the second day after stablisation ,improvement in vitals .
Ambulation was initiated from the second day with support .
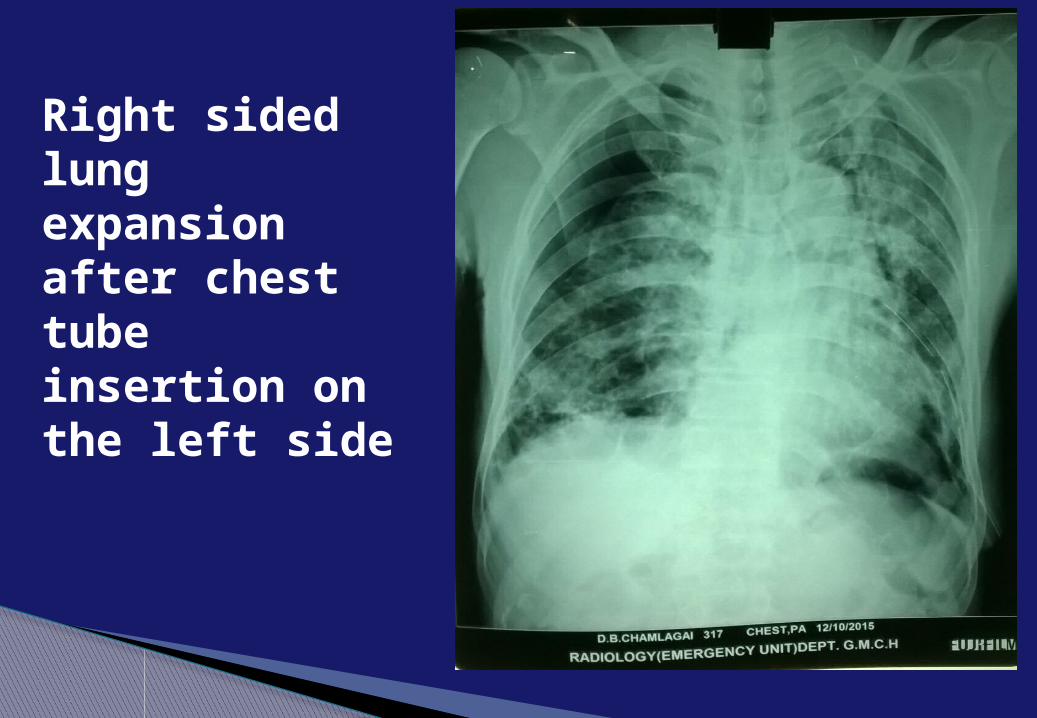
Right sided lung expansion after chest tube insertion on the left side
On the fifth day after chest tube insertion a fresh chest radiograph was obtained after a initial assessment of patient for satisfactory bi-lateral air entry and container for absent column movement .
Container fluid level remained at nil till chest tube removal . The chest radiograph demonstrated bi lateral expanded lungs
and complete resolution pneumothoraces with a single left sided chest tube catheter .
Pleura– pleural communication was demonstrated by drainage of right pneumothorax via the left chest tube .
CASE REPORT
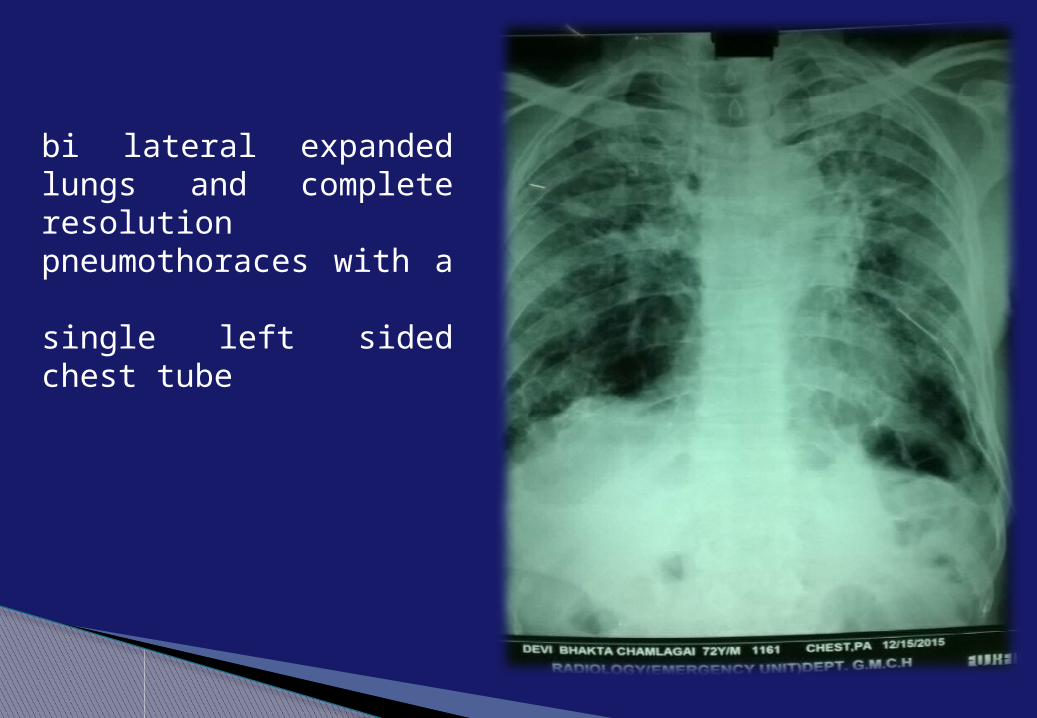
bi lateral expanded lungs and complete resolution pneumothoraces with a single left sided chest tube
On sixth day , 24 hrs since absent column movement of the container decision to remove the chest tube was taken .
Patient was asked to hold breath before rapid withdrawal of
chest tube and purse string suture tightening to seal the incision .
6hrs after chest tube removal a chest radiograph was done to investigate for collapse of lung . Patient was encouraged to continue physiotherapy and deep breathing exercises . Bronchodilators were continued .
After a 24 hrs observation for respiratory distress ,patient was discharged on the the morning of the seventh day of admission
CASE REPORT
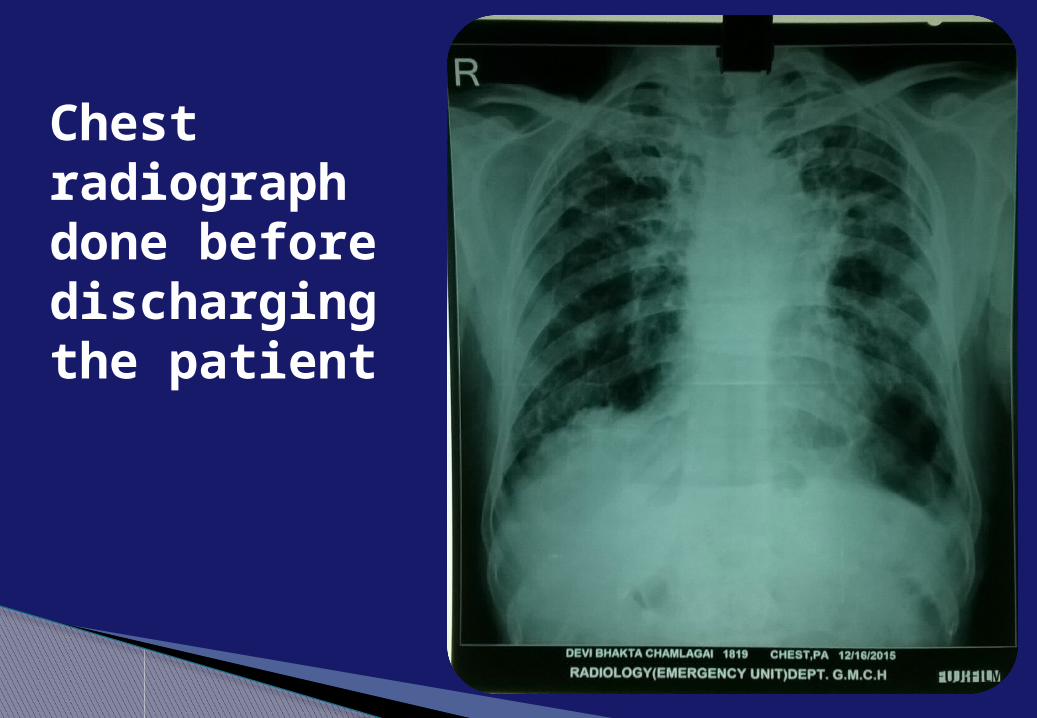
Chest radiograph done before discharging the patient
SIMILAR CASE REPORTS WORLDWIDE1.Case of the month: Buffalo chest: a case of
bilateral pneumothoraces due to pleuropleural communication...Emerg Med J v.23(6); 2006 Jun PMC256435
Charles_M._Russell_-_The_Buffalo_Hunt_No_39_-_1919-818x539
2.Simultaneous bilateral spontaneous pneumothorax with congenital pleuro-pleural communication ….J Thorac Dis. 2013 Feb; 5(1): 87–89.
3.Simultaneous bilateral spontaneous pneumothorax with pleural window communicating with bilateral pleural spaces. Yamada S1, Yoshino K, Inoue H. Ann Thorac Surg. 2008 Apr;85(4):1434
Conclusion and discussion There are currently very few articles published
of this rarest of the rare chest anomaly with a incidence of nine cases reported worldwide .
Congenital and iatrogenic eitiology has been demonstrated in all the earlier reported presentations . This is the first case with a spontaneous occurance in a elderly patient
Conclusion and discussion It is a miracle that earlier pulmonary
tubercular disease had led to right lower lobe adhesions to chest wall thus preventing the complete bilateral lung collapse ,in which case the patient might not have survived without urgent ventilatory support .
It still remains a mystery as to which side was the air leak initially from ?
Conclusion and discussion There has been a report of demonstrated
pleuro - pleural communication by CT and thoracoscopy at posterior mediastenal space between heart and eosophagous which might be also most likely site in this elderly patient .
Although post recovery CT scan did not demonstrate any communication probably due to hyperinflated ,expanded lungs


A primary spontaneous pneumothorax (PSP) tends to occur in a young adult without underlying lung problems, and usually causes limited symptoms. Chest pain and sometimes mild breathlessness are the usual predominant presenting features. People who are affected by PSPs are often unaware of potential danger and may wait several days before seeking medical attention. PSPs more commonly occur during changes in atmospheric pressure, explaining to some extent why episodes of pneumothorax may happen in clusters. It is rare for PSPs to cause tension pneumothoraces.Secondary spontaneous pneumothoraces (SSPs), by definition, occur in individuals with significant underlying lung disease. Symptoms in SSPs tend to be
more severe than in PSPs, as the unaffected lungs are generally unable to replace the loss of function in the affected lungs. Hypoxemia (decreased blood-oxygen levels) is usually present and may be observed as cyanosis(blue discoloration of the lips and skin). Hypercapnia (accumulation of carbon dioxide in the blood) is sometimes encountered; this may cause confusion and - if very severe - may result in comas. The sudden onset of breathlessness in someone with chronic obstructive pulmonary disease (COPD), cystic fibrosis, or other serious lung diseases should therefore prompt investigations to identify the possibility of a pneumothorax. Traumatic pneumothorax most commonly occurs when the chest wall is pierced, such as when a stab
wound or gunshot woundallows air to enter the pleural space, or because some other mechanical injury to the lung compromises the integrity of the involved structures. Traumatic pneumothoraces have been found to occur in up to half of all cases of chest trauma, with only rib fractures being more common in this group. The pneumothorax can be occult (not readily apparent) in half of these cases, but may enlarge - particularly if mechanical ventilation is required. They are also encountered in patients already receiving mechanical ventilation for some other reason. Upon physical examination, breath sounds (heard with a stethoscope) may be diminished on the
affected side, partly because air in the pleural space dampens the transmission of sound. Measures of the conduction of vocal vibrations to the surface of the chest may be altered. Percussion of the chest may be perceived as hyperresonant (like a booming drum), and vocal resonance and tactile fremitus can both be noticeably decreased. Importantly, the volume of the pneumothorax can show limited correlation with the intensity of the symptoms experienced by the victim, and physical signs may not be apparent if the pneumothorax is relatively small.
Although multiple definitions exist, a tension pneumothorax is generally considered to be present when a pneumothorax (primary spontaneous, secondary spontaneous, or traumatic) leads to significant impairment of respiration and/or blood circulation. Tension pneumothorax tends to occur in clinical situations such as ventilation, resuscitation, trauma, or in patients with lung disease. The most common findings in people with tension pneumothorax are chest pain and respiratory distress, often with an increased heart rate (tachycardia) and rapid breathing (tachypnea) in the initial stages. Other findings may include quieter breath sounds on one side of the chest, low oxygen levels and blood pressure, and displacement of the trachea away from the affected side. Rarely, there may be cyanosis (bluish discoloration of the skin due to low oxygen levels), altered level of consciousness, a hyperresonant percussion note on examination of the affected side with reduced expansion and decreased movement, pain in the epigastrium (upper abdomen), displacement of the apex beat (heart impulse), and resonant sound when tapping the sternum.
TENSION PNEUMOTHORAX
This is a medical emergency and may require immediate treatment without further investigations.
Tension pneumothorax may also occur in someone who is receiving mechanical ventilation, in which case it may be difficult to spot as the person is typically receiving sedation; it is often noted because of a sudden deterioration in condition. Recent studies have shown that the development of tension features may not always be as rapid as previously thought. Deviation of the trachea to one side and the presence of raised jugular venous pressure (distended neck veins) are not reliable as clinical signs.