bellflower unified open enrollment - busd benefits
TRANSCRIPT
BELLFLOWER UNIFIED SCHOOL DISTRICT
OPEN ENROLLMENT
2011-2012
MANUAL ENROLLMENT ONLY (On Line Enrollment is NOT available)
8:00 a.m. August 15, 2011 thru 4:30 p.m. September 9, 2011
PLEASE NOTE: THIS IS YOUR ONLY OPEN ENROLLMENT FOR SCHOOL YEAR 2011-2012.
HEALTH INSURANCE
OPT OUT ENROLLMENT
FLEX PLAN – IRC 125
VOLUNTARY LIFE INSURANCE
ELIGIBLE EMPLOYEES BELLFLOWER UNIFIED SCHOOL DISTRICT
OPEN ENROLLMENT FOR HEALTH INSURANCE
Forms may be obtained from www.busdbenefits.com
Open enrollment is the only time during the year when eligible employees may change medical or dental plans. If you choose to mail in your enrollment forms you may mail them anytime as long as they reach the District office by 4:30 on September 9, 2011. All changes will go into effect October 1, 2011. A brief summary of all available medical and dental plans is included with this packet. If you would like to make changes to your coverages you may obtain forms on line at www.busdbenefits.com and download the appropriate form. If you have specific questions, attend our Open Enrollment meeting. You will have the opportunity to meet representatives from our providers, as well as ask questions. You will also have the opportunity to be educated about various health issues, and your specific insurance benefits. There will be representatives from our Health Insurance Office. The Open Enrollment Meeting will be held on:
Tuesday, August 30, 2011
From 10:30 a.m. to 4:00 p.m. Ramona Multipurpose Room
If you are unable to attend this meeting, the Insurance Help-Desk is available to answer questions during this time as well as during the rest of the school year. If you have any questions, please contact Char Lambert at 310-609-1917 ext. 222 or 562-866-9011 ext. 3123, email at [email protected] or Kim Soder at [email protected] Fax: 310-609-1877. Information is also available on the web at www.busdbenefits.com. Please note: ALL pages of your confirmation statement must be turned into the Health Insurance Office with any additional data required. All documents are date stamped. It is your responsibility to make sure your information is turned before the deadline.
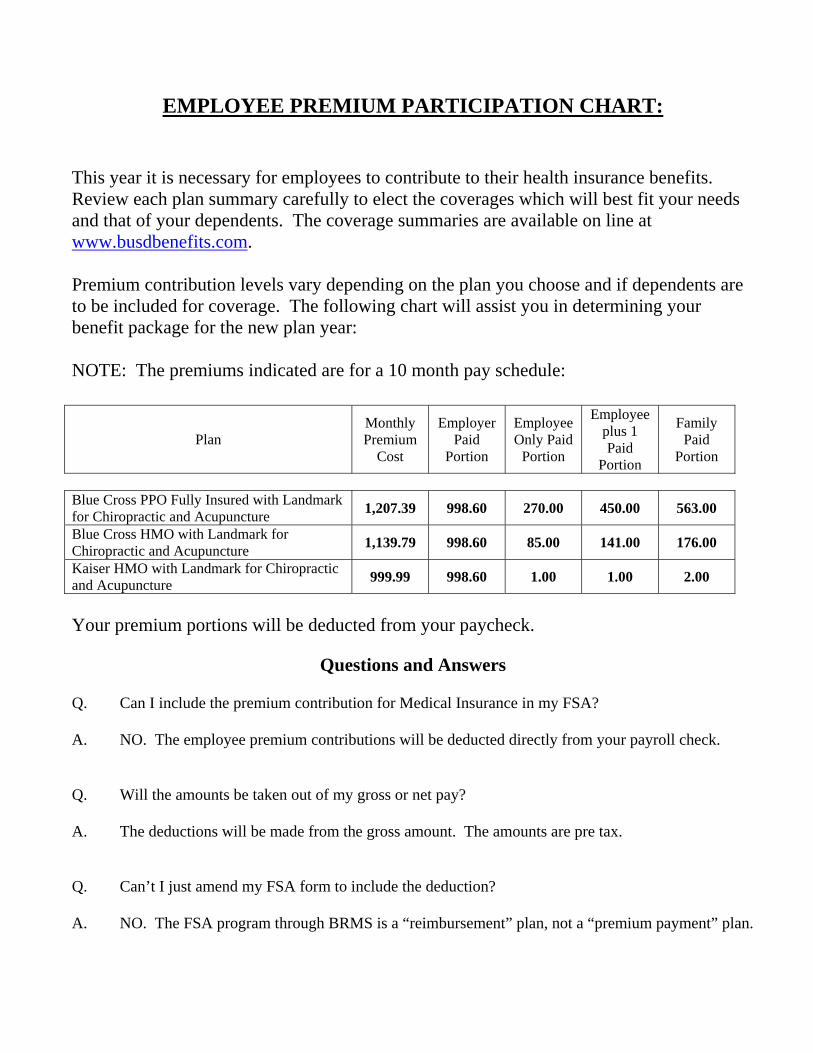
EMPLOYEE PREMIUM PARTICIPATION CHART:
This year it is necessary for employees to contribute to their health insurance benefits. Review each plan summary carefully to elect the coverages which will best fit your needs and that of your dependents. The coverage summaries are available on line at www.busdbenefits.com. Premium contribution levels vary depending on the plan you choose and if dependents are to be included for coverage. The following chart will assist you in determining your benefit package for the new plan year: NOTE: The premiums indicated are for a 10 month pay schedule:
Plan Monthly Premium
Cost
Employer Paid
Portion
Employee Only Paid
Portion
Employee plus 1 Paid
Portion
Family Paid
Portion
Blue Cross PPO Fully Insured with Landmark for Chiropractic and Acupuncture 1,207.39 998.60 270.00 450.00 563.00
Blue Cross HMO with Landmark for Chiropractic and Acupuncture 1,139.79 998.60 85.00 141.00 176.00
Kaiser HMO with Landmark for Chiropractic and Acupuncture 999.99 998.60 1.00 1.00 2.00
Your premium portions will be deducted from your paycheck.
Questions and Answers
Q. Can I include the premium contribution for Medical Insurance in my FSA? A. NO. The employee premium contributions will be deducted directly from your payroll check. Q. Will the amounts be taken out of my gross or net pay? A. The deductions will be made from the gross amount. The amounts are pre tax. Q. Can’t I just amend my FSA form to include the deduction? A. NO. The FSA program through BRMS is a “reimbursement” plan, not a “premium payment” plan.

RETIREMENT Questions & Answers
Q. If I choose to retire, will my benefits cease? A. If you are eligible for insurance benefits at your retirement age and under the age of 65, your Medical plan coverages will continue until you reach the age of 65 (Medical, Chiropractic & Acupuncture.) Q. Will the District continue the Dental and Vision coverages? A. No, but you will receive a COBRA kit which will give you the option to continue these coverages under COBRA for a limited time. The kit and letter will also let you know the costs involved. The cost will not be covered by the District. Q. When would the Medical Coverages cease? A. When you reach age 65, benefits will cease for you, your spouse/partner and any other covered dependents . Your eligible Spouse/Partner when they reach age 65, if it is before you reach age 65 Other eligible dependents until they reach age 26, or you reach age 65, whichever occurs first Q. What will the cost be for my medical coverages? A. This will depend on the plan you select and the number of dependents to be included. (refer to the Employee Premium Participation Chart) Q. How can I obtain coverage after I turn 65? A. Retirees and/or their dependents turning age 65 should apply for Medicare.
Medicare Part A (Hospital Coverage) helps pay for inpatient hospital charges. Medicare Part A may be earned through Social Security payroll deductions. If not earned, once an individual reaches age 65 they may purchase Medicare Part A through the Social Security Administration office.
Medicare Part B (Medical Coverage) helps pay for physician charges, outpatient x-ray and laboratory charges and many other medical services. Medicare Part B cannot be earned through Social Security payroll deductions. Once an individual reaches age 65 they may purchase Medicare Part B through the Social Security Administration office.

DEPENDENTS CHECKLIST: Definition: Each of the following would be considered a “dependent” under your medical benefits:
- Spouse - Domestic Partner - Child up to age 26
The following documentation must be on file with the District for dependents:
Marriage Certificate To add a spouse
Divorce Decree
To delete a spouse
Domestic Partner Filing To add a same sex domestic partner
Children:
Birth certificate to add a child Adoption Confirmation Court legal guardianship papers to add a child, other than your own, who you are
legally responsible for Special Note: Failure to provide the required documentation will result in ineligibility and your dependent will not be able to be enrolled in the health plan. It is your responsibility to notify the District if a dependent is no longer eligible for coverage. Failure to do so will result in charge back to you for the cost of claims, retroactive premiums of medical, dental and vision coverages and reinstatement fees that may have been incurred during the ineligible period.
MEDICAL
HEALTH
INSURANCE
(Enrollment Forms are included)

Special Notice
Effective October 1, 2011, the self funded PPO plan will no longer be available.
If you are currently covered under Option 2, you must re-enroll in the Blue Cross PPO plan, the Blue
Cross HMO plan or the Kaiser HMO plan.

You have THREE choices of MEDICAL PLANS:
Blue Cross PPO Kaiser or Blue Cross HMO
BLUE CROSS – Fully Insured PPO - You may use in-network or out-of-network providers at any given time. (refer to plan summary)
PREFERRED PROVIDER ORGANIZATION OPTION (PPO) – this option allows you to select the services of a Blue Cross Prudent Buyer provider without obtaining a referral from a Primary Care Physician. After satisfying an individual deductible of $250, the plan pays 80% of most services. (See insert) OUT-OF-NETWORK OPTION – this option allows you to select services of a physician not in the Blue Cross Prudent Buyer Network. After satisfying an individual deductible of $500, the plan pays 60%. RETAIL PRESCRIPTIONS co-pay $10.00 generic, $25.00 formulary and $40.00 brand name, then 80%. MAIL ORDER is also available.
KAISER – HMO – You use the services and physicians at a Kaiser Medical Center. There is a $10 co-payment cost per visit, 100% hospitalization and $10 charge per prescription. (refer to plan summary) BLUE CROSS – HMO – You use the services and physicians contracted with Blue Cross. There is a $15 co-payment cost per office visit. Prescriptions are $10.00 for generic, $20.00 for formulary and $25.00 for brand name. (refer to plan summary) SPECIAL NOTE: The individual plan summaries available on line at www.busdbenefits.com.

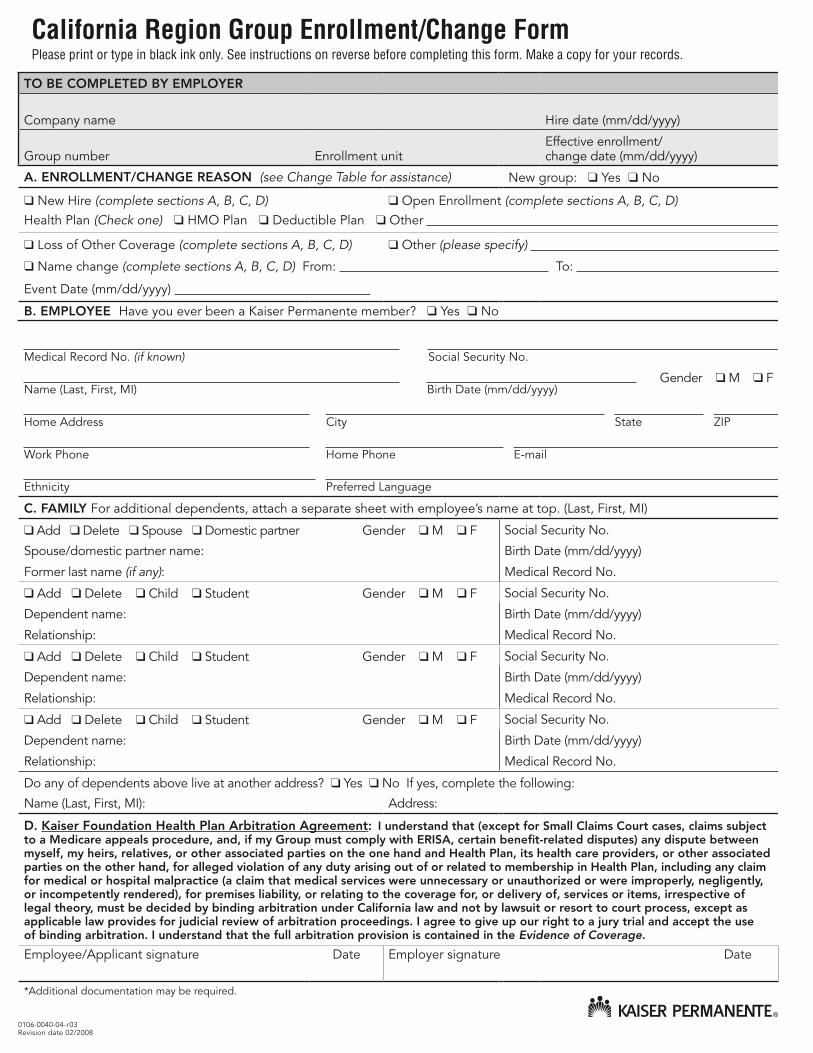
California Region Group Enrollment/Change Form Please print or type in black ink only. See instructions on reverse before completing this form. Make a copy for your records.
0106-0040-04-r03Revision date 02/2008
TO BE COMPLETED BY EMPLOYER
Company name Hire date (mm/dd/yyyy)
Group number Enrollment unitEffective enrollment/ change date (mm/dd/yyyy)
A. ENROLLMENT/CHANGE REASON (see Change Table for assistance) New group: ❑ Yes ❑ No
❑ New Hire (complete sections A, B, C, D) ❑ Open Enrollment (complete sections A, B, C, D) Health Plan (Check one) ❑ HMO Plan ❑ Deductible Plan ❑ Other
❑ Loss of Other Coverage (complete sections A, B, C, D) ❑ Other (please specify)
❑ Name change (complete sections A, B, C, D) From: To:
Event Date (mm/dd/yyyy)
B. EMPLOYEE Have you ever been a Kaiser Permanente member? ❑ Yes ❑ No
Medical Record No. (if known) Social Security No.
Name (Last, First, MI) Birth Date (mm/dd/yyyy) Gender ❑ M ❑ F
Home Address City State ZIP
Work Phone Home Phone E-mail
Ethnicity Preferred Language
C. FAMILY For additional dependents, attach a separate sheet with employee’s name at top. (Last, First, MI)
❑ Add ❑ Delete ❑ Spouse ❑ Domestic partner Gender ❑ M ❑ F Social Security No.
Spouse/domestic partner name: Birth Date (mm/dd/yyyy)
Former last name (if any): Medical Record No.
❑ Add ❑ Delete ❑ Child ❑ Student Gender ❑ M ❑ F Social Security No.
Dependent name: Birth Date (mm/dd/yyyy)
Relationship: Medical Record No.
❑ Add ❑ Delete ❑ Child ❑ Student Gender ❑ M ❑ F Social Security No.
Dependent name: Birth Date (mm/dd/yyyy)
Relationship: Medical Record No.
❑ Add ❑ Delete ❑ Child ❑ Student Gender ❑ M ❑ F Social Security No.
Dependent name: Birth Date (mm/dd/yyyy)
Relationship: Medical Record No.
Do any of dependents above live at another address? ❑ Yes ❑ No If yes, complete the following:
Name (Last, First, MI): Address:
D. Kaiser Foundation Health Plan Arbitration Agreement: I understand that (except for Small Claims Court cases, claims subject to a Medicare appeals procedure, and, if my Group must comply with ERISA, certain benefit-related disputes) any dispute between myself, my heirs, relatives, or other associated parties on the one hand and Health Plan, its health care providers, or other associated parties on the other hand, for alleged violation of any duty arising out of or related to membership in Health Plan, including any claim for medical or hospital malpractice (a claim that medical services were unnecessary or unauthorized or were improperly, negligently, or incompetently rendered), for premises liability, or relating to the coverage for, or delivery of, services or items, irrespective of legal theory, must be decided by binding arbitration under California law and not by lawsuit or resort to court process, except as applicable law provides for judicial review of arbitration proceedings. I agree to give up our right to a jury trial and accept the use of binding arbitration. I understand that the full arbitration provision is contained in the Evidence of Coverage.
Employee/Applicant signature Date Employer signature Date
*Additional documentation may be required.

General instructions
1. Please print firmly and legibly in black ink.
2. To enroll, the subscriber must reside or work within one of the ZIP codes listed on the enclosed sheet.
3. The employer must complete the first section titled “To be completed by employer.”
4. The employer is responsible for confirming all information prior to submitting, especially effective dates, as these affect your Health Plan dues.
5. The employee/subscriber must complete Sections A and B. See right column for detailed instructions.
6. Be sure to sign and date the bottom of the form.
7. Once the form is complete (including employer section), the subscriber should make a copy for his or her records, and to use as a temporary ID card, after the effective date.
8. All changes to accounts, including effective dates and child or student status, will be made in accordance with the contractual agreement between the purchaser and Kaiser Permanente.
Instructions for completing employer and new enrollment sections and sections A through D:To be completed by employer: The employer must complete all fields to ensure we have correct account and enrollment information.
Section A: The subscriber must complete this section.
Section B: The subscriber must always complete this section. Use the Change Table (below) for assistance.
Section C: The subscriber must indicate the requested change to the account and complete all fields for any dependents being enrolled. We will verify the eligibility of these dependents during the enrollment process. Be sure to include any former last names for both spouses and dependents. Also indicate the appropriate role. The student role should be marked only if the dependent qualifies as an “overage dependent” attending school. Please contact your employer regarding rules for overage dependent students. A completed Student Certification form may be required.
Section D: The subscriber must sign and date this section.
Change Table
Add dependent Event date
Acquired student status* Student status date
Family adoption* Adoption date
Loss of coverage Coverage loss date
New spouse (marriage) Marriage date
Moved into service area Move date
Newborn addition Birth date
Open enrollment Open enrollment effective date
Delete dependent Event date
Loss of student status Status change date
Divorce Divorce date
Member deceased* Death date
Delete dependent(s) Dependent termination date
Open enrollment Open enrollment effective date
Demographic Change Event date
Address change, telephone number change Status change date
Demographic (name, birthdate, social security number) change Status change date
*Additional documentation may be required.
0106-0040-04-r03Revision date 02/2008
California Region Group Enrollment/Change Form

DENTAL
VISION
CHIROPRACTIC
(Enrollment Forms for Delta Care and Delta Dental are included
VSP and Chiropractic Services do not need
enrollment form)

You have two choices of DENTAL PLANS: DELTA DENTAL OR DELTACARE PMI
DELTA DENTAL (PPO) – You select your own dentist. The plan pays 70% of the cost during the first year and each year increases 10% until 100% is reached, if you visit the dentist at least once a year. Maximum benefit per calendar year is $1,500 per person (increases to $2,000 when using a DPO). No orthodontia coverage DELTACARE PMI (HMO)- You select a dentist from the Plan’s Dental Group. The plan pays 100% of most charges. Some orthodontia coverage
The VISION PLAN offered is: VSP – Vision Service Plan
VISION SERVICE – You are automatically enrolled in Vision Service Plan with each medical plan. This plan provides a yearly examination and glasses if needed for a $10 deductible payment, and discounted prices for Laser Vision Correction.
The Acupuncture and Chiropractic Plan offered is: LANDMARK HEALTHCARE
ACUPUNCTURE AND CHIROPRACTIC SERVICES: You are automatically enrolled in Landmark Healthcare with each medical plan. This plan provides you 40 Chiropractic visits and unlimited Acupuncture visits per year for a $7 co-payment. Treatment beyond the initial visits must be medically necessary. All services must be performed by a Landmark provider.



OPT OUT PLAN
(Enrollment Form is Included)

Date: 2011-2012 Plan Year To: All Bellflower Unified School District Employees Re: Cash Opt Out Program Bellflower Unified School District is offering a Cash Opt Out plan to our active employees and eligible retirees effective October 1, 2011. This plan is designed for those employees and retirees that have other health coverage through their spouse’s employer (including BUSD) or another credible insurance provider. Effective October 1, 2011, if you elect the Cash Opt Out plan, your group medical health coverages through the District will terminate. The termination of coverage would include Chiropractic and Acupuncture. You will continue to receive dental and vision benefits without interruption. You can also elect to Opt Out of the Medical coverages AND Dental and Vision coverages. In this case, all of your health benefits will be terminated. The District is offering employees a cash payment of $250.00 paid out 10 times per fiscal year for a total of $2,500 to Opt Out of the Medical plans and an additional monthly amount of $30.00 or $300.00 yearly for Dental and Vision plans. Employees are required to re-enroll in the Cash Opt Out program for each benefit year. The due date for submitting the election form for open enrollment is September 9, 2011. Your election form must include a photocopy of an insurance ID card from the other insurance company. Enrollment forms not accompanied by a photocopy of the ID card will not be accepted. You must ALSO return all pages of the signed open enrollment confirmation statement. The District reserves the right to contact the other carrier to confirm your coverage and benefits. The decision as to whether this other coverage is a credible alternative remains with the District and your election could be denied. A general Q&A of the Cash Opt Out plan is included for your information. If you have any questions regarding this option, then please contact the Insurance Help Desk at (562) 866-9011, Extension 3123, or our District Consultant at (310) 609-1917. Insurance Help Desk
Cash Opt Out Plan Description What is a Cash Opt Out Plan? An Opt Out plan is offered to employees or eligible retirees who have other coverage, usually through a spouse (including BUSD employees). The District establishes a fixed cash alternative to participation in the group health plans. In school Districts this cash alternative is typically $1,500 to $2,000 per year. Why is an Opt Out plan a good option? In some families both spouses are provided family coverage in an HMO or PPO. As a result the employers are paying the premium so the insured employee can have their $5 to $15 co-payments reimbursed. By offering cash in lieu of benefits, the employee can pocket the difference between the employer cash and any out of pocket from the spouses plan. How does the Opt Out plan work? An employee or eligible retiree enrolls in the Opt Out plan instead of a District offered health plan. This is done through an enrollment form that includes a waiver of medical benefits. The District pays a specific amount per year or a percentage of the lowest health plan premium. The compensation is paid out through the regular payroll system. What is other Credible Coverage? This would include a spouse’s health plan; another employers plan if an early retiree, or military retirement. This includes coverage under a spouse who is also a District employee. The determination of credible coverage will be at the sole discretion of the District. If other coverage is not clear, the District’s insurance help desk will contact the other insurer and verify credibility. What happens if my spouse loses his/her coverage? The employee could elect COBRA through the spouse’s employer or re-enroll into the District plan due to the qualifying event. What is Bellflower Unified School District offering me to Opt Out? The District is offering employees a cash payment of $250.00 paid out 10 times per fiscal year for a total of $2,500 to Opt Out of the Medical plans and an additional monthly amount of $30.00 or $300.00 yearly for Dental and Vision plans. Employees will be required to re-enroll in the Cash Opt Out program for each benefit year. This amount is significantly higher than any other District in the region. Will I lose my Dental and Vision coverage? The Opt Out plan covers health benefits, which includes medical (Rx) and chiropractic. However, you also have the option to Opt Out of the Dental and Vision plans. If I elect to keep my Dental and Vision coverages, will I still receive the $280? No, the annual Opt Out reimbursement would be $2,500 or $250 paid tenthly during the plan year.

BELLFLOWER UNIFIED SCHOOL DISTRICT
MEDICAL INSURANCE “OPT-OUT” PROGRAM
ELECTION FORM
I, __________________________________, hereby acknowledge that I am currently covered (Print Name) as either a subscriber or dependent on a medical insurance plan enabling me to participate in the “Opt-Out” Program. I understand that the provisions of the “Opt-Out” Program require that I provide evidence of the insurability on the above referenced plan in the form of a bona fide copy of the enrollment document or current identification card adding me to the plan. I also understand that in opting out of the Medical Plan I am not eligible for Chiropractic. By participating in the “Opt-Out” program I fully understand that once this election is made I will be unable to participate in the medical insurance benefits during the plan year unless there is a qualifying event. A qualifying event means loss of the other coverage, change in legal marital status or termination of employment. I also understand that I must re-enroll in the “Opt-Out” program at open-enrollment each year and provide new evidence of other coverage. Check your current District plan: None Currently Opting Out
Blue Cross PPO Self Funded Blue Cross HMO Kaiser HMO
I also wish to Opt out of Dental & Vision plans Yes No (a box must be checked)
__________________________________________________ _________________ Signature Date
__________________________________________________ _________________ Printed Name Marital Status
__________________________________________________ _________________ Phone Number Ext. # Social Security #
____________________________________________________________________
____________________________________________________________________
Mailing address, including city, state and zip code NOTE: Incomplete forms will NOT be accepted.

FLEX PLAN
IRC 125
(Enrollment Form is Included)

VOLUNTARY
LIFE INSURANCE
Reliance Standard policy is available to all employees
Sun Life policy is available to confidential and
management employees only
Employee will pay the premiums thru payroll deductions
(Enrollment Form is included)