“being ill makes me sad” huon gray national clinical director for cardiac care, nhs england...
TRANSCRIPT

“Being ill makes me sad”
Huon GrayNational Clinical Director for Cardiac Care, NHS England
Consultant Cardiologist, University Hospital of Southampton
‘Valuing physical & mental health equally’Parity of Esteem ConferenceStadium of Light, Sunderland
14th October 2014

Outline
• Why is CVD important?• Relationship between CVD & Mental Health• CVD Outcomes Strategy• Conclusions

Outline
• Why is CVD important?• Relationship between CVD & Mental Health• CVD Outcomes Strategy• Conclusions

BHF Heart Stats (2012) http://www.bhf.org.uk/publications/view-publication.aspx?ps=1002097
CVD Mortality in England (all <75 yrs)

Source: www.statistics.gov.uk/ statbase/Product.asp?vlnk=6725
Causes of Death (England, <75 yrs) (Source: ‘Living Well for Longer’ [ONS data], 2013)

CVD………..
• 200k deaths pa (1:3 of all)• 4.9m adults have CVD (11.7% of population)• 1.4m hospital admissions in 2010/11
• 65% were patients under 75 yrs• >50% were emergencies
• Prevalence increases with deprivation - Inequalities• CVD costs NHS & UK economy £30bn pa.
“Services for the prevention of CV Disease”NICE Commissioning Guide 45. March 2012

Deaths by Disease & Deprivation (England <75 yrs)

Global Burden of Disease Study. Lancet 2013;381:997-1020
UK causes of Years of Life Lost (both sexes, all ages) 1990-2010

Global Burden of Disease Study. Lancet 2013;381:997-1020 UK causes of Years of Life Lost (both sexes, all ages) 1990-2010
259 diseases and injuries & 67 risk factors

Global Burden of Disease Study. Lancet 2013;381:997-1020
DALYs Attributable to 20 Risk Factors (UK)

Outline
• Why is CVD important?• Relationship between CVD & Mental Health• CVD Outcomes Strategy• Conclusions

INTERHEART: Risk of AMI with Multiple Risk Factors (52 countries, n≈30,000)
Yusuf et al. Lancet 2004;364:937-52

Yusuf et al. Lancet 2004;364:937-52
INTERHEART: Risk of AMI with Multiple Risk Factors (52 countries, n≈30,000)

Yusuf et al. Lancet 2004;364:937-52
INTERHEART: Risk of AMI with Multiple Risk Factors (52 countries, n≈30,000)

http://www.instituteofhealthequity.org
2011
2013

JAMA Psychiatry 2014; October 8th

…”people having a first schizophrenia spectrum episode were significantly more likely to show a host of cardiovascular and endocrinologic risk factors than the general population of a similar age.”
…”among relatively young patients enrolled (mean age 24) – half were overweight or obese, nearly 60% had abnormal lipid levels, half have had raised BP, and 13% had metabolic syndrome”
…”some of these findings likely related to antipsychotic Rx, but the illness itself and associated unhealthy lifestyles also played major roles”
JAMA Psychiatry 2014; October 8th

Pyschosocial Factors & CVD
• Promotion of atherosclerosis [Circulation. 1999;99(16):2192]
– Direct effects (endothelium, platelets)– Indirect via usual risk factors
• Depression and anger increase risk of angina & MI [Normative Aging Study 1998-2000]
• Depression in 20-40% of people having CABG, and poorer outcomes [Circulation. 2005;111(3):271]
• AHA (2004) recommends depression screening for those with CHD [Circulation. 2008;118(17):1768]

Pyschosocial Factors & CVD
• EPIC-Norfolk UK Prospective cohort study [Am J Psychiatry 2008;165(4):515]
– 19,000 people with major depressive disorder in year before enrolment
– initially free of CHD– Median F/U 8.5 years
• Those with depression 2.7 more likely to die from IHD even after adjustment for traditional & other socio-demographic risk factors

Outline
• Why is CVD important?• Relationship between CVD & Mental Health• CVD Outcomes Strategy• Conclusions


“The performance of the UK in terms of premature mortality….is below the mean of the EU15+…….further progress will require improved public health, prevention, early intervention and treatment activities……and deserves an integrated and strategic response”

Scope“To improve outcomes for people with, or at risk of developing, CVD”
Context Increased Government focus on “the outcomes that matter
most to people” Evidence based & cost neutral or saving Need to create a joined-up approach to CVD across the three outcomes
frameworks (with shared implementation)
CVD Outcomes Strategy (2012-13)
NHS Public Health Adult Social Care

NHS Outcomes Framework
Preventing people from
dying prematurely
Enhancing quality of life
for people with long-
term conditions
Helping people to
recover from episodes of ill
health or following
injury
Ensuring people have a positive experience of care
Treating and caring for people in a safe environment and protecting them from avoidable
harm
Domain 1 Domain 2 Domain 3
Domain 4
Domain 5
Effectiveness
Experience
Safety

NHS Outcome Indicators
25
3Overarching indicators
Improvement areas
Helping people to recover from episodes of ill health or following injury
3a Emergency admissions for acute conditions that should not usually require hospital admission3b Emergency readmissions within 30 days of discharge from hospital* (PHOF 4.11)
Improving outcomes from planned treatments3.1 Total health gain as assessed by patients for elective procedures
i Hip replacement ii Knee replacement iii Groin hernia iv Varicose veins v Psychological therapies
Preventing lower respiratory tract infections (LRTI) in children from becoming serious3.2 Emergency admissions for children with LRTI
Improving recovery from injuries and trauma3.3 Proportion of people who recover from major trauma
Improving recovery from stroke3.4 Proportion of stroke patients reporting an improvement in activity/lifestyle on the Modified Rankin Scale at 6 months
Improving recovery from fragility fractures3.5 Proportion of patients recovering to their previous levels of mobility/walking ability at i 30 and ii 120 days
Helping older people to recover their independence after illness or injury3.6 i Proportion of older people (65 and over) who were still at home 91 days
after discharge from hospital into reablement/ rehabilitation service*** (ASCOF 2B) ii Proportion offered rehabilitation following discharge from acute or community hospital
Enhancing quality of life for people with long-term conditions2
Overarching indicator
2 Health-related quality of life for people with long-term conditions** (ASCOF 1A)
Improvement areas
Ensuring people feel supported to manage their condition2.1 Proportion of people feeling supported to manage their condition**
Improving functional ability in people with long-term conditions2.2 Employment of people with long-term conditions** * (ASCOF 1E PHOF 1.8)
Reducing time spent in hospital by people with long-term conditions2.3 i Unplanned hospitalisation for chronic ambulatory care sensitive
conditions (adults) ii Unplanned hospitalisation for asthma, diabetes and epilepsy in under
19s
Enhancing quality of life for carers2.4 Health-related quality of life for carers** (ASCOF 1D)
Enhancing quality of life for people with mental illness2.5 Employment of people with mental illness **** (ASCOF 1F & PHOF 1.8)
Enhancing quality of life for people with dementia2.6 i Estimated diagnosis rate for people with dementia* (PHOF 4.16)
ii A measure of the effectiveness of post-diagnosis care in sustaining independence and improving quality of life*** (ASCOF 2F)
Preventing people from dying prematurely1Overarching indicators
1a Potential Years of Life Lost (PYLL) from causes considered amenable to healthcare
i Adults ii Children and young people1b Life expectancy at 75
i Males ii Females
Improvement areas
Reducing premature death in people with serious mental illness1.5 Excess under 75 mortality rate in adults with serious mental illness* (PHOF 4.9)
Reducing deaths in babies and young children1.6 i Infant mortality* (PHOF 4.1)
ii Neonatal mortality and stillbirthsiii Five year survival from all cancers in children
Reducing premature mortality from the major causes of death1.1 Under 75 mortality rate from cardiovascular disease* (PHOF 4.4)1.2 Under 75 mortality rate from respiratory disease* (PHOF 4.7)1.3 Under 75 mortality rate from liver disease* (PHOF 4.6)1.4 Under 75 mortality rate from cancer* (PHOF 4.5)
i One- and ii Five-year survival from all cancersiii One- and iv Five-year survival from breast, lung and colorectal cancer
Reducing premature death in people with a learning disability1.7 Excess under 60 mortality rate in adults with a learning disability
4Overarching indicators
Ensuring that people have a positive experience of care
4a Patient experience of primary carei GP services ii GP Out of Hours services iii NHS Dental Services
4b Patient experience of hospital care4c Friends and family test
Improvement areas
Improving people’s experience of outpatient care4.1 Patient experience of outpatient services
Improving hospitals’ responsiveness to personal needs4.2 Responsiveness to in-patients’ personal needs
Improving access to primary care services4.4 Access to i GP services and ii NHS dental services
Improving women and their families’ experience of maternity services4.5 Women’s experience of maternity services
Improving the experience of care for people at the end of their lives4.6 Bereaved carers’ views on the quality of care in the last 3 months of life
Improving experience of healthcare for people with mental illness4.7 Patient experience of community mental health services
Improving children and young people’s experience of healthcare4.8 An indicator is under development
Improving people’s experience of accident and emergency services4.3 Patient experience of A&E services
Improving people’s experience of integrated care 4.9 An indicator is under development *** (ASCOF 3E)
Reducing the incidence of avoidable harm5.1 Incidence of hospital-related venous thromboembolism (VTE)5.2 Incidence of healthcare associated infection (HCAI)
i MRSAii C. difficile
5.3 Incidence of newly-acquired category 2, 3 and 4 pressure ulcers5.4 Incidence of medication errors causing serious harm
Improving the safety of maternity services5.5 Admission of full-term babies to neonatal care
Delivering safe care to children in acute settings5.6 Incidence of harm to children due to ‘failure to monitor’
Treating and caring for people in a safe environment and protect them from avoidable harm5
Overarching indicators
5a Patient safety incidents reported5b Safety incidents involving severe harm or death 5c Hospital deaths attributable to problems in care
Improvement areas
NHS OutcomesFramework 2013/14
at a glance
Alignment across the Health and Social Care System
* Indicator shared with Public Health Outcomes Framework (PHOF)** Indicator complementary with Adult Social Care Outcomes
Framework (ASCOF)*** Indicator shared with Adult Social Care Outcomes Framework**** Indicator complementary with Adult Social Care Outcomes
Framework and Public Health Outcomes Framework
Indicators in italics are placeholders, pending development or identification

NHS Outcomes Framework:Domain 1 – Potential years of life lost from causes considered amenable to healthcare – Life expectancy at 75 (males/females) – Under 75 mortality rate from cardiovascular diseaseDomain 3 – Indicator to be derived based on proportion of stroke patients reporting improvement in activity/lifestyle on the Modified Rankin Scale at 6 months
Public Health Outcomes Framework:Domain 2 – recorded diabetes – take up of NHS health checkDomain 4 – mortality from all cardiovascular diseases (including heart disease & stroke)
Adult Social Care Outcomes Framework:Domain 2 – permanent admissions to residential & nursing homes, per 1000
population – proportion of older people (65 & over) still at home 91 days
after discharge from hospital into reablement/rehab services – Delayed transfer of care from hospital, and those which are
attributable to adult social care
CVD-related indicators

March 5th, 2013
https://www.gov.uk/government/publications/improving-cardiovascular-disease-outcomes-strategy

Contents

Recommended ActionsIntegration

Vascular Disease – One Event Leads to Another (REACH Registry; 69,000 patients, 44 countries)
Original Event = Stroke MI Risk • 2-3 x greater risk2* Stroke Risk• 9 x greater risk3
Original Condition = PAD MI Risk• 4 x greater risk4**Stroke Risk• 2-3 x greater risk3++
Original Event = MI MI Risk• 5-7 x greater risk1+
Stroke Risk• 3-4 x greater risk2++
Diabetes (type 2)Because of the increased risk associated with diabetes, it should be considered a cardiovascular risk equivalent to a non-diabetic patient with previous MI
*Includes angina and sudden death. Sudden death defined as death documented within 1 hour and attributed to coronary heart disease (CHD) **Includes only fatal heart attack and other CHD death; does not include non-fatal heart attack, + Includes death ++Includes TIA
1. Adult Treatment Panel II. Circulation 1994; 89:1333–63. 2. Kannel WB. J Cardiovasc Risk 1994; 1: 333–9.
3. Wilterdink JI, Easton JD. Arch Neurol1992; 49: 857–63. 4. Criqui MH et al. N Engl J Med 1992; 326: 381–6.
Data is increased risk vs general population (%)
CKDMI Risk• 2 x greater
riskStroke risk• Up 50%

Recommended ActionsIntegration


CVDOS Recommended Actions• Seeing CVD as one condition (‘family of diseases’)• Integration of services
• Risk factors • Case finding in 10 care• Better management in, and support for, 10 Care• Inherited cardiac conditions (incl. FH)• Improve survival from OHCA (CPR, AEDs, First Responders,
Education, Registry)• Raising awareness• 24 x 7 CV Services• Care planning (phys & psych support, self care, EOL care)• Information (CVIN, Benchmarking – those at risk and quality of care)
• Researchhttps://www.gov.uk/government/publications/improving-cardiovascular-disease-outcomes-strategy

CVDOS Recommended Actions• Seeing CVD as one condition (‘family of diseases’)• Integration of services
• Risk factors, NHS Health Check• Case finding in 10 care• Better management in, and support for, 10 Care• Inherited cardiac conditions (incl. FH)• Improve survival from OHCA (CPR, AEDs, First Responders,
Education, Registry)• Raising awareness• 24 x 7 CV Services• Care planning (phys & psych support, self care, EOL care)• Information (CVIN, Benchmarking – those at risk and quality of care)
• Researchhttps://www.gov.uk/government/publications/improving-cardiovascular-disease-outcomes-strategy

NHS Health Checks
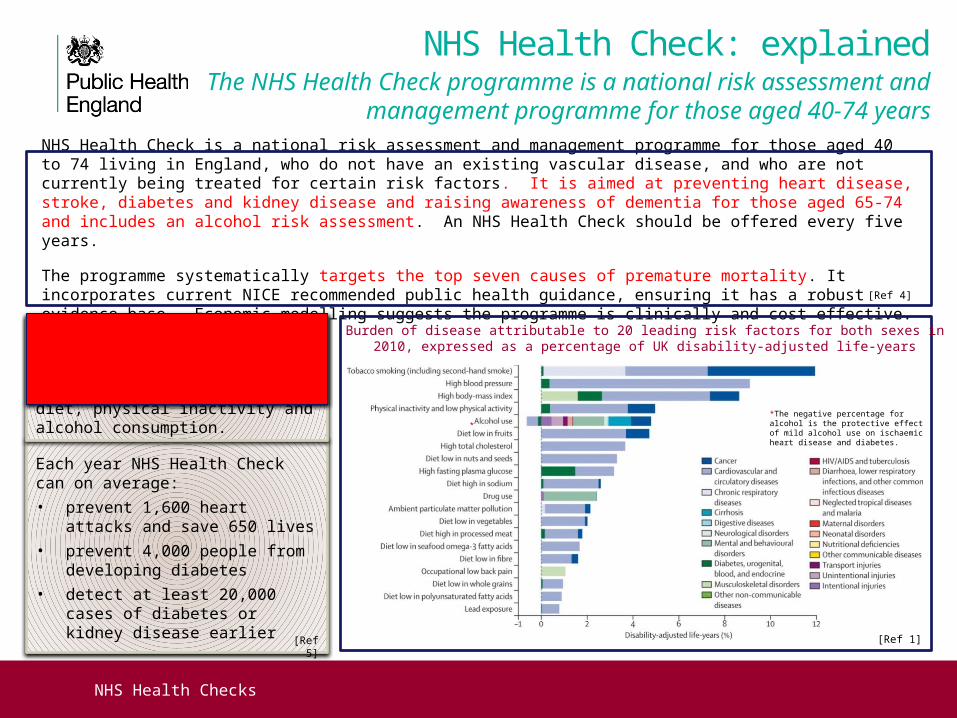
NHS Health Check: explainedThe NHS Health Check programme is a national risk assessment
and management programme for those aged 40-74 years
NHS Health Check is a national risk assessment and management programme for those aged 40 to 74 living in England, who do not have an existing vascular disease, and who are not currently being treated for certain risk factors . It is aimed at preventing heart disease, stroke, diabetes and kidney disease and raising awareness of dementia for those aged 65-74 and includes an alcohol risk assessment. An NHS Health Check should be offered every five years.
The programme systematically targets the top seven causes of premature mortality. It incorporates current NICE recommended public health guidance, ensuring it has a robust evidence base. Economic modelling suggests the programme is clinically and cost effective.
Each year NHS Health Check can on average:
• prevent 1,600 heart attacks and save 650 lives
• prevent 4,000 people from developing diabetes
• detect at least 20,000 cases of diabetes or kidney disease earlier
Burden of disease attributable to 20 leading risk factors for both sexes in 2010, expressed as a percentage of UK disability-adjusted life-years
*The negative percentage for alcohol is the protective effect of mild alcohol use on ischaemic heart disease and diabetes.
*
[Ref 4]
[Ref 5]
Top seven causes of preventable mortality: high blood pressure, smoking, cholesterol, obesity, poor diet, physical inactivity and alcohol consumption.
[Ref 1]
NHS Health Checks
NHS Health Check: explainedThe NHS Health Check programme is a national risk assessment
and management programme for those aged 40-74 years
NHS Health Check is a national risk assessment and management programme for those aged 40 to 74 living in England, who do not have an existing vascular disease, and who are not currently being treated for certain risk factors . It is aimed at preventing heart disease, stroke, diabetes and kidney disease and raising awareness of dementia for those aged 65-74 and includes an alcohol risk assessment. An NHS Health Check should be offered every five years.
The programme systematically targets the top seven causes of premature mortality. It incorporates current NICE recommended public health guidance, ensuring it has a robust evidence base. Economic modelling suggests the programme is clinically and cost effective.
Each year NHS Health Check can on average:
• prevent 1,600 heart attacks and save 650 lives
• prevent 4,000 people from developing diabetes
• detect at least 20,000 cases of diabetes or kidney disease earlier
Burden of disease attributable to 20 leading risk factors for both sexes in 2010, expressed as a percentage of UK disability-adjusted life-years
*The negative percentage for alcohol is the protective effect of mild alcohol use on ischaemic heart disease and diabetes.
*
[Ref 4]
[Ref 5]
Top seven causes of preventable mortality: high blood pressure, smoking, cholesterol, obesity, poor diet, physical inactivity and alcohol consumption.
[Ref 1]

NHS Health Checks
NHS Health Check: explainedThe NHS Health Check programme is a national risk assessment
and management programme for those aged 40-74 years
NHS Health Check is a national risk assessment and management programme for those aged 40 to 74 living in England, who do not have an existing vascular disease, and who are not currently being treated for certain risk factors . It is aimed at preventing heart disease, stroke, diabetes and kidney disease and raising awareness of dementia for those aged 65-74 and includes an alcohol risk assessment. An NHS Health Check should be offered every five years.
The programme systematically targets the top seven causes of premature mortality. It incorporates current NICE recommended public health guidance, ensuring it has a robust evidence base. Economic modelling suggests the programme is clinically and cost effective.
Each year NHS Health Check can on average:
• prevent 1,600 heart attacks and save 650 lives
• prevent 4,000 people from developing diabetes
• detect at least 20,000 cases of diabetes or kidney disease earlier
Burden of disease attributable to 20 leading risk factors for both sexes in 2010, expressed as a percentage of UK disability-adjusted life-years
*The negative percentage for alcohol is the protective effect of mild alcohol use on ischaemic heart disease and diabetes.
*
[Ref 4]
[Ref 5]
Top seven causes of preventable mortality: high blood pressure, smoking, cholesterol, obesity, poor diet, physical inactivity and alcohol consumption.
[Ref 1]

CVDOS Recommended Actions• Seeing CVD as one condition (‘family of diseases’)• Integration of services
• Risk factors, NHS Health Check• Case finding in 10 care• Better management in, and support for, 10 Care• Inherited cardiac conditions (incl. FH)• Improve survival from OHCA (CPR, AEDs, First Responders,
Education, Registry)
• Raising awareness• 24 x 7 CV Services• Care planning (phys & psych support, self care, EOL care)
• Information (CVIN, Benchmarking – those at risk, quality of care)
• Researchhttps://www.gov.uk/government/publications/improving-cardiovascular-disease-outcomes-strategy

Conclusions
• CVD still important cause of premature mortality• CVD increases risk of mental illness• CVD is common in those with SMI• Risk factors for CVD in people with SMI are
similar to those of people without SMI• CVDOS highlights what can be done• CVD health of those with SMI deserves attention