bc practice support program: end of life care module ... · end of life care module facilitating...
TRANSCRIPT
10/18/2012
1
www.pspbc.ca
BC Practice Support Program: End of Life Care Module
Facilitating Practice Change
International Primary Palliative Care Research GroupOctober 2012
Dr. Cathy Clelland
2
� Catherine A. Clelland, BMedSc, MD, CCFP, FCFP� Executive Director, Society of General Practitioners of BC
� Chair, EOL PSP Module Development Working Group� GP Services Committee Staff Support
� There is no corporate or other potential conflict of
interest in relation to this program/presentation
Conflict Disclosure Information
10/18/2012
2
4
� Background to the British Columbia (BC) provincial Practice Support module in End-of-Life (EOL) care.
� Clarify the components of a provincial model integrating home care, palliative care services with services being provided in General practitioners offices.
� Demonstrate the utility of the EOL algorithm
� Review the Early Evaluation findings
Objectives

10/18/2012
3
Practice Support Program:
6
� Created to help family physicians in BC network with colleagues & learn how to integrate new ways of doing things into their clinical practices via a peer-to-peer teaching model.
� Expanding to include specialist physicians.
� Supported by the GP Services Committee, Specialist Services Committee & Shared Care Committee (partnerships between the Ministry of Health Services and the BC Medical Association, including the Society of General Practitioners) and Regional Health Authorities.
BC Practice Support Program (PSP)

10/18/2012
4
7
� Overall goal: To give participants tools they can use in their practice to improve care and to support them as they try to use these tools.
� Structure:
› Pre-work
› 3 Learning sessions:
� Half day sessions with GP/MOA teams, Specialists and Community Allied Health Professionals (possibly NGOs in some communities)
› 2 Action Periods:
� Change concepts are implemented during the periods between learning sessions.
� Not CME, but eligible for CME Credits for both GPs and Specialists.
Structured Learning Collaborative
8
Role: To teach content/ change concepts to their peers at a local level.
Qualifications: Those who
� Enjoy teaching in an interactive & informal context
� Are passionate about the clinical topic area.
Supports for role:
� Champions are reimbursed for their time spent doing PSP work.
� Experienced PSP coordinators
GP Champions
� Champion
[def’n]: A peer
who has special
experience or
skills and mentors others
� Principle: A teacher as similar
to the student as
possible

10/18/2012
5
9
� Support content development
� Support physicians during action
periods to ensure the role is manageable and not disruptive to clinical responsibilities.
� Facilitate communication among local
providers/practice peers and care delivery across the continuum
� Ongoing support for practices with practice change and action periods
� Monthly phone calls
� List-serve to share learning as it happens
PSP Coordinators
Team Functions:
Knowledgeable, local support available in all three domains: Clinical, Practice Management, & IMIT
1
Clinical
2 3 4
1 2 3 4
IMIT
1 2 3 4
Practice Management
10
What are we trying toaccomplish?
How will we know that achange is an improvement?
What changes can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
10/18/2012
6
Practice Support Program:End-of-Life Module
12
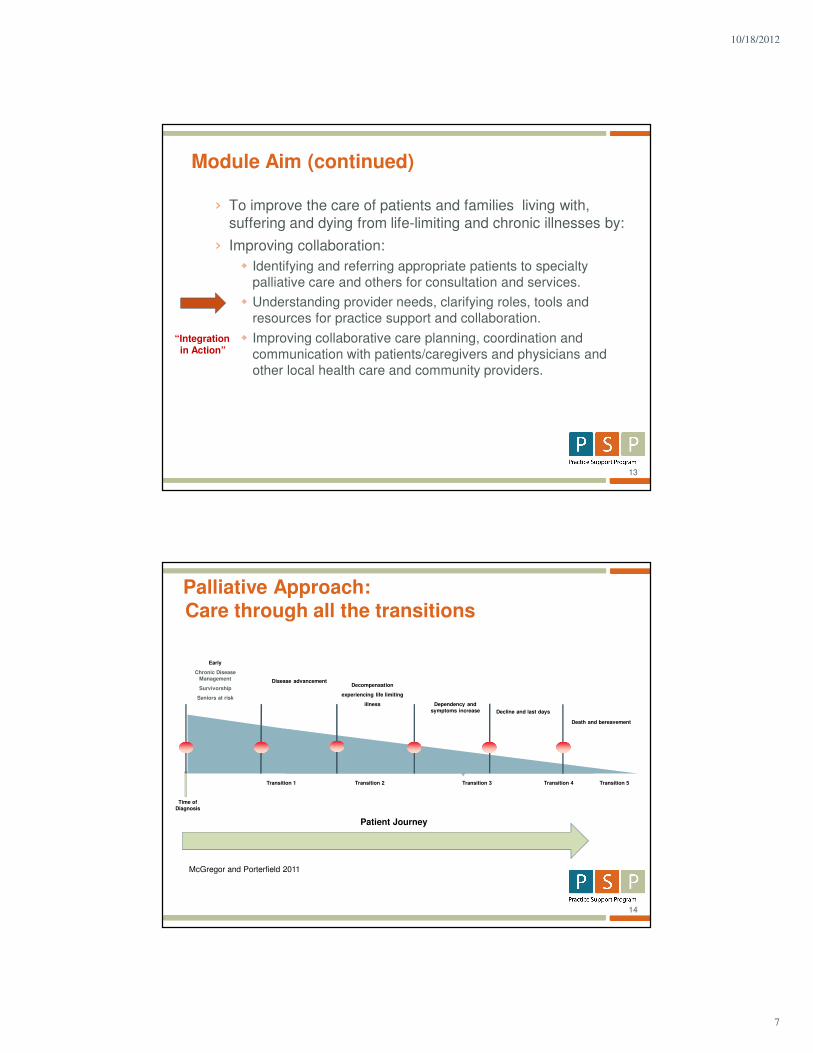
� Improve the care of patients and families living with,
suffering and dying from life-limiting and chronic
illnesses by:
› Early Identification (Registry Building)
› Enhance and Improve physician confidence related to End of
Life care (e.g. care planning, forms, communication, resources)
› Improve Collaboration (clarity of roles, appropriate resource
referrals, network of community resources, etc)
› Improve the experience of the patient, family, physician, MOA and healthcare providers in End of Life care.
Module Aim
10/18/2012
7
13
› To improve the care of patients and families living with,
suffering and dying from life-limiting and chronic illnesses by:
› Improving collaboration:
� Identifying and referring appropriate patients to specialty
palliative care and others for consultation and services.
� Understanding provider needs, clarifying roles, tools and
resources for practice support and collaboration.
� Improving collaborative care planning, coordination and
communication with patients/caregivers and physicians and
other local health care and community providers.
“Integration in Action”
Module Aim (continued)
14
Palliative Approach: Care through all the transitions
Patient Journey
McGregor and Porterfield 2011
Time of
Diagnosis
Decompensation
experiencing life limiting
illness
Decline and last days
Dependency and
symptoms increase
Death and bereavement
Transition 1 Transition 5Transition 4Transition 3Transition 2
Early
Chronic Disease
Management
Survivorship
Seniors at risk
Disease advancement
10/18/2012
8
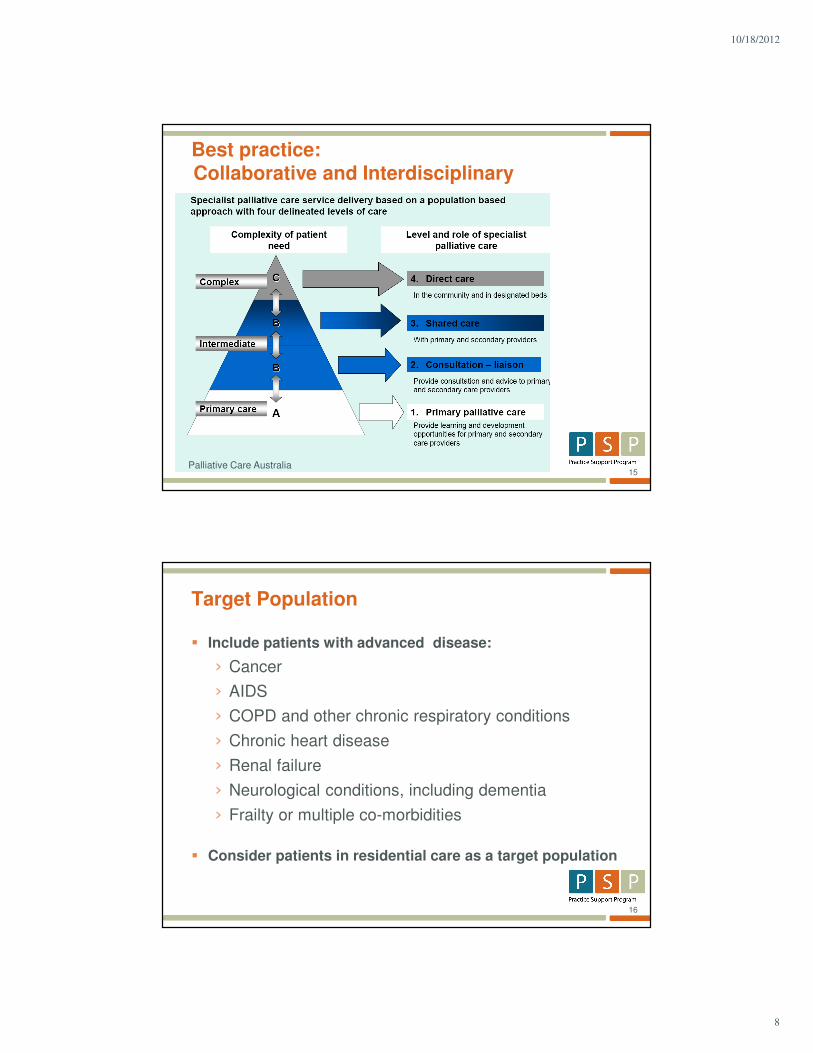
15
Best practice: Collaborative and Interdisciplinary
Palliative Care Australia
16
� Include patients with advanced disease:
› Cancer
› AIDS
› COPD and other chronic respiratory conditions
› Chronic heart disease
› Renal failure
› Neurological conditions, including dementia
› Frailty or multiple co-morbidities
� Consider patients in residential care as a target population
Target Population

10/18/2012
9
17
18
� Patient, family and informal network
� Family physician
� Specialist Physician (Oncology, IM)
� Community pharmacist
� Home Health / Community Care
› Nurses/rehab/home support
� Nurse practitioners, community RT
� Disease specific consultants / services
� Hospice palliative care consult teams
Who is the patient’s care team?

10/18/2012
10
19
� Participation of Home and Community Care
at Learning Sessions and Train the Trainer
Sessions
� Creation of regionally-specific Integration
material where applicable
� Development of learning objectives and
action period activities for Home and Community Care
staff
� Evaluation includes the input from Home and
Community Care /Palliative Care staff
Collaboration with Home and Community Care/Palliative Care
20
� 500 GPs with MOAs (recent approval to
increase to 900)
� 100 H&CC/palliative care staff ~
1H&CC/PC: 5 GPs
� 30 - 50 specialist physicians
� 40-50 PSP Coordinators
Who is involved in the PSP EOL module?
10/18/2012
11
21
Through the
past year…
Evaluation: Early Learnings

10/18/2012
12
23
� Two Surveys
› Baseline to April 30, 2012 (administered at beginning of LS1)
› End-of-Module to August 31, 2012 (administered at end of LS3)
� Three groups of survey respondents
› GPs� Baseline: N=308, response rate = 72.5%
� End-of-Module: N=155, response rate = 48.7%
› MOAs� Baseline: N=180, response rate = 62.9%
� End-of-Module: N=67, response rate = 36.4%
› Home and Community Care and Palliative Care (HCC/PC) nurses� Baseline: N=27, response rate = 23.4%
� End-of-Module: N=7, response rate = 10.4%
Evaluation: Early Learnings
Satisfaction with the EOL Module
97.4
89.0
71.2
94.197.0 98.5
9.113.6
89.6
69.2
90.8
85.7
100.0
28.6 28.6
100.0
91.0
29.0
34.8
0
20
40
60
80
100
The material was
clear and
informative.
The facilitators
were well
informed and
knowledgeable.
Pacing of
sessions was
too slow.
Respondent
already knew
much of the
material.
Networking and
sharing of
information was
helpful.
Required action
period activities
could be
completed in
time allocated.
Respondent
learned
something new
that he/she
incorporated into
his/her practice.
%R
esp
on
de
nts
wh
o A
gre
ed
or
Str
on
gly
Ag
ree
d
GPs (N=155) MOAs (N=67) HCC/PC Nurses (N=7)
* Responses for questions with N<7 are not shown
10/18/2012
13
25
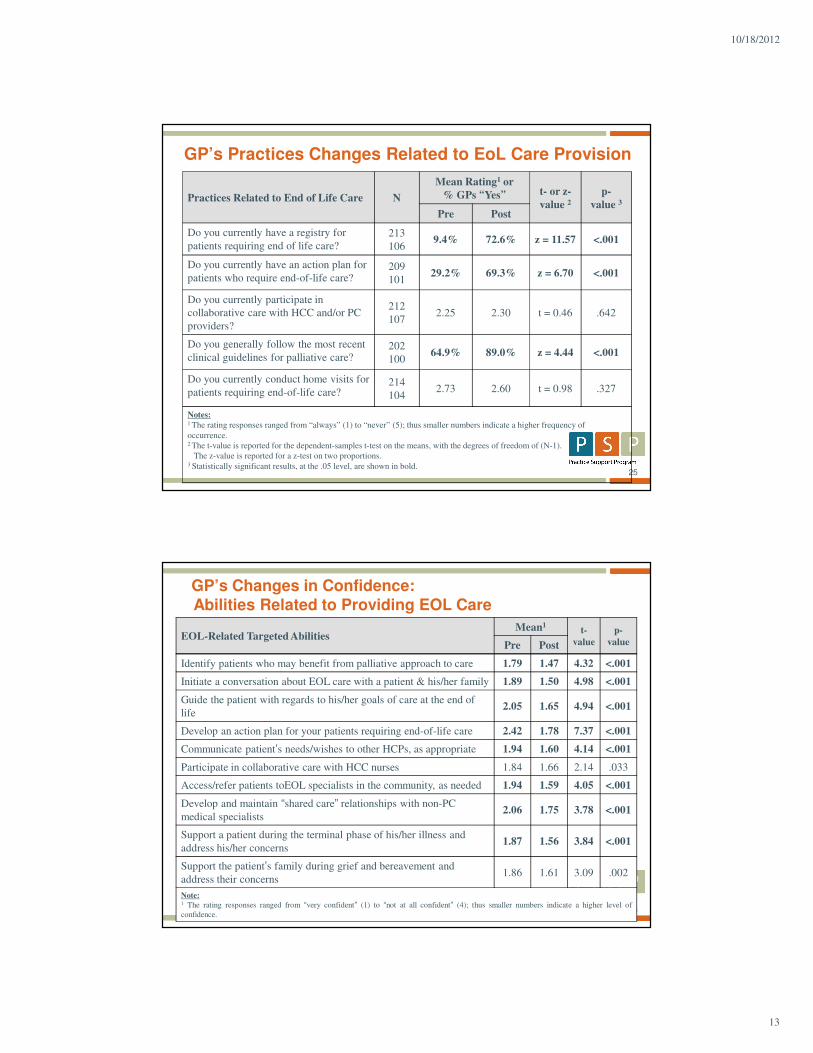
Practices Related to End of Life Care N
Mean Rating1 or
% GPs “Yes” t- or z-
value 2p-
value 3
Pre Post
Do you currently have a registry for
patients requiring end of life care?
213
1069.4% 72.6% z = 11.57 <.001
Do you currently have an action plan for
patients who require end-of-life care?209
10129.2% 69.3% z = 6.70 <.001
Do you currently participate in
collaborative care with HCC and/or PC
providers?
212
1072.25 2.30 t = 0.46 .642
Do you generally follow the most recent
clinical guidelines for palliative care?202
10064.9% 89.0% z = 4.44 <.001
Do you currently conduct home visits for
patients requiring end-of-life care?214
1042.73 2.60 t = 0.98 .327
Notes:1 The rating responses ranged from “always” (1) to “never” (5); thus smaller numbers indicate a higher frequency of
occurrence.2 The t-value is reported for the dependent-samples t-test on the means, with the degrees of freedom of (N-1).
The z-value is reported for a z-test on two proportions.3 Statistically significant results, at the .05 level, are shown in bold.
GP’s Practices Changes Related to EoL Care Provision
26
GP’s Changes in Confidence: Abilities Related to Providing EOL Care
EOL-Related Targeted AbilitiesMean1
t-
value
p-
valuePre Post
Identify patients who may benefit from palliative approach to care 1.79 1.47 4.32 <.001
Initiate a conversation about EOL care with a patient & his/her family 1.89 1.50 4.98 <.001
Guide the patient with regards to his/her goals of care at the end of
life2.05 1.65 4.94 <.001
Develop an action plan for your patients requiring end-of-life care 2.42 1.78 7.37 <.001
Communicate patient’s needs/wishes to other HCPs, as appropriate 1.94 1.60 4.14 <.001
Participate in collaborative care with HCC nurses 1.84 1.66 2.14 .033
Access/refer patients toEOL specialists in the community, as needed 1.94 1.59 4.05 <.001
Develop and maintain “shared care” relationships with non-PC
medical specialists2.06 1.75 3.78 <.001
Support a patient during the terminal phase of his/her illness and
address his/her concerns1.87 1.56 3.84 <.001
Support the patient’s family during grief and bereavement and
address their concerns1.86 1.61 3.09 .002
Note:1 The rating responses ranged from “very confident” (1) to “not at all confident” (4); thus smaller numbers indicate a higher level of
confidence.

10/18/2012
14
27
� All groups of participants were satisfied with the EOL learning module
� The EOL module has had a positive impact on GP practices and patients
� GPs’ and MOAs’ confidence in addressing the concerns of EOL patients has increased, compared with baseline measures
� Preliminary results show that the relationships between general practices and the home and community care providers are improving, but there are opportunities to strengthen these further
Conclusion
28
Thank You