b-complex vitamins - university of baghdad · b-complex vitamins thiamine (vitamin b1 ... human...
TRANSCRIPT

- 1 -
BIOCHEMISTRY
Lec:4 : 2nd stage شيماء سبتي.د.م
B-COMPLEX VITAMINS
THIAMINE (VITAMIN B1)
Synonyms: Antiberiberi factor, antineuritic vitamin, aneurin.
►Biosynthesis: Synthesized by plants, yeasts and bacteria. Not synthesized by
human beings, hence should be supplied in diet. Intestinal bacterial flora can
synthesize the vitamin.
►Metabolism
Absorption: Free thiamine is absorbed readily from the small intestine, but the
pyrophosphate (ester-form) is not. Bulk of the dietary vegetable thiamine is in the
“free” form. In tissues, it is actively phosphorylated to form Thiamine
pyrophosphate (TPP) in Liver, and to a lesser extent in other tissues like muscle,
brain and nucleated RB Cells.
- 2 -
►Plasma/blood level: Present in plasma and CS fluid in the “free” form, approx.
1 μg/100 ml. Blood cells contain 6 to 12 μg/100 ml where occurs as TPP.
►Storage: Capacity to store is limited. It is present in both free and combined
forms in heart (highest concentration), Liver and kidneys. In lower concentration in
skeletal muscle and brain. Total amount of Thiamine in body is approx. 25 mg.
►Excretion: If normal amount of thiamine is taken in the diet:
• About 10 per cent is excreted in the urine
• The remainder is (a) Partly phosphorylated and is used as coenzyme, and (b)
Partly degraded to neutral sulphur compounds and inorganic SO4 which are
excreted in urine.
►Occurrence and Food Sources
• Plant source: Widely distributed in plant kingdom. In cereal grains, it is
concentrated in outer germ/bran layers (e.g. rice polishings) (Richest source).
Other good sources are peas, beans, whole cereal grains, bran, nuts, prunes, etc.
Whole white bread is a good source.
• Animal source: Thiamine is present in most animal tissues. Liver, meat and eggs
supply considerable amounts. Ham/pork meats are particularly rich. Milk has low
concentration, but a good source as large quantities are consumed.
►METABOLIC ROLE
Biological active form is Thiamine pyrophosphate (TPP). Acts as a coenzyme in
several metabolic reactions.
• Acts as coenzyme to the enzyme pyruvate dehydrogenase complex (PDH) which
converts pyruvic acid to acetyl-CoA (oxidative decarboxylation) PDH Pyruvate
Acetyl-CoA TPP
Pyruvate PDH Acetyl-CoA
TPP
• TPP acts as the coenzyme (Co-carboxylase) of pyruvate carboxylase in yeasts for
the non-oxidative decarboxylation of pyruvate to acetaldehyde.

- 3 -
►CLINICAL ASPECT
DEFICIENCY MANIFESTATIONS: Beriberi
The deficiency of thiamine produces a condition called beriberi. It is characterised
by the following manifestations.
1- CV manifestations: These include palpitation, dyspnoea, cardiac hypertrophy
and dilatation, which may progress to congestive cardiac failure.
2- Neurological manifestations: These are predominantly those of ascending,
symmetrical, peripheral polyneuritis. These neurological features may be
accompanied occasionally by an acute haemorrhagic polioencephalitis which is
then called as Wernicke’s encephalopathy.
3- GI symptoms: Amongst these, anorexia is an early symptom. There may be
gastric atony, with diminished gastric motility and nausea; fever and vomiting
occur in advanced stages.
Dry beriberi: When it is not associated with oedema.
Wet beriberi: Oedema is associated. It is probably in part to congestive cardiac
failure and in part to protein malnutrition (Low plasma albumin).
►Biochemical Features in Thiamine Deficiency
1- Decreased level of thiamine and TPP in blood and urine. Determination of
amount of thiamine excreted in 4 hours urine is used.
2- Accumulation of pentose sugars in RB cells due to retardation of transketolation
reaction.
3- Increased level of pyruvic acid and lactic acid in blood, due to retardation of
oxidative decarboxylation of pyruvic acid. – LA/PA ratio: Abnormal blood LA/PA
ratio is said to be more specific indicator of B1 deficiency.
4- Catatorulin effect: Decreased uptake of O2 by thiamine-deficient brain in vitro;
reversible by addition of thiamine.

- 4 -
5- Saturation test (thiamine loading test): A lower urinary excretion of thiamine
and TPP after administration of a test-dose occurring in thiamine-deficient as
compared to normal subjects.
►Daily Requirements
• Adult: 0.5 mg for each 1000 calories; 1.0 to 1.5 mg for diets providing 2000 to
3000 C. Minimum requirement is 1.0 mg. Actual requirement is related more
directly to carbohydrates content of diet than to calorie value of diet.
• Children: Ranges from 0.4 mg for infants to 1.3 mg for preadolescents (10 to 12
years of age). Requirements Increases in Anoxia-shock and haemorrhage,
Serious illness and injury, During prolonged administration of broadspectrum oral
antibiotics, Increased calorie expenditure like fever, hyperthyroidism, Increased
carbohydrate intake, Increased alcohol intake, and pregnancy and in lactation.
RIBOFLAVIN (VITAMIN B2)
Synonyms: Lactoflavin, ovoflavin, hepatoflavin.

- 5 -
►Biological Active Forms
The biological active forms, in which riboflavin serves as the prosthetic group (as
coenzyme) of a number of enzymes are the phosphorylated derivatives.
Two main derivatives are:
1- FMN (Flavin mononucleotide): In this the phosphoric acid is attached to
ribityl alcoholic group in position 5 ( Flavin-Ribityl-PO4).
2- FAD (Flavin adenine dinucleotide): It may be linked to an adenine nucleotide
through a pyrophosphate linkage to form FAD (Flavin-ribityl-P-P-ribose-Adenine)
Thus, FMN and FAD are two coenzymes of this vitamin.
The acidic properties given by phosphoric acid group influence their capacity for
combining with proteins apoenzyme-forming flavoproteins (Holoenzyme). Thus,
FP (holoenzyme) = FMN/FAD + Protein
(coenzyme) (Apoenzyme)
FP may also unite with metals like Fe and Mo thus forming Metalloflavoproteins.
►Biosynthesis
All higher plants can synthesize riboflavin. In nature, it occurs both as “free form”
and also as “nucleotide” form or as flavoproteins. Human beings and animals
cannot synthesise and hence solely dependent on dietary supply. In man,
considerable amounts can be synthesised by intestinal bacteria, but the quantity
absorbed is not adequate to maintain normal nutrition.

- 6 -
Metabolism ►Absorption: Flavin nucleotides are readily absorbed in small intestine. Free
riboflavin undergoes phosphorylation, a prerequisite for absorption.
►Blood/Plasma level: Human blood plasma contains 2.5 to 4.0 μgm%, two-third
as FAD and bulk of remainder as FMN. Concentration in RB cells-15 to 30 μg/100
gm. Leucocytes and platelets-250 μg/100 gm. These values remain quite constant
even in severe riboflavin deficiency, hence determination of riboflavin in blood is
not useful. Riboflavin present in all tissues as nucleotides bound to proteins (FP),
highest concentration in liver and kidney.
►Excretion: Daily urinary excretion 0.1 to 0.4 mg (10 to 20% of intake).
• Milk: Riboflavin is secreted in milk, 40 to 80 per cent in ‘free’ form.
• Faeces: Free and nucleotides tend to remain quite constant, 500 to 750 μg daily,
largely from the unabsorbed bacterial synthesis.
►Occurrences and Food Sources
Widely distributed in nature, present in all plant and animal cells.
• Plant sources: High concentration occurs in yeasts. Appreciable amount present
in whole grains, dry beans and peas, nuts, green vegetable. Germinating seeds, e.g.
grams/Dals are very good source.
• Animal source: Liver (2–3 mg/100 gm), kidney, milk, eggs, Crab meat has high
content.

- 7 -
►METABOLIC ROLE
FMN and FAD act as coenzymes in various H-transfer reactions in metabolism.
The hydrogen is transported by reversible reduction of the coenzyme by two
hydrogen atoms added to the ‘N’ at positions 1 and 10, thus forming dihydro or
leucoriboflavin. The principal enzyme reactions catalysed are as shown below:
FMN FAD
• Cytochrome-C-reductase • Xanthine oxidase (Xanthine → uric acid)
• D-amino acid oxidase • L-amino acid oxidase • Aldehyde oxidase
►CLINICAL ASPECT Deficiency Manifestations
There is no definite disease entity. Deficiency is usually associated with
deficiencies in other B-vitamins. In human beings lesions of the mouth, tongue,
nose, skin and eyes with weakness, and lassitude reported. They include:
• Lips: Redness and shiny appearance of lips.
• Cheilosis: Lesions at the mucocutaneous junction at the angles of the
mouth leading to painful fissures are characteristic.
• Tongue: Painful glossitis, the tongue assuming a red-purple (magenta)
colour.
• Seborrhoeic dermatitis: Scaly, greasy, desquamation chiefly about the
ears, nose and naso-labial folds.
• Eyes: May lead to corneal vascularisation and inflammation with
cloudiness of cornea, watering, burning of eyes, photophobia, scleral
congestion and cataract has also been reported.
• Protein synthesis: This is impaired in severe riboflavin deficiency; since
protein malnutrition interferes with utilisation and retention of riboflavin.
- 8 -
►Daily Requirement
• Adults: 1.5 to 1.8 mg • Women in later half of pregnancy: 2.0 mg
• During lactation: 2.5 mg • Infants: 0.6 mg
• Children: 1.0 to 1.8 mg • Adolescence: 2.0 to 2.5 mg
Requirement increases After severe injury/burns, etc. during acute illness and
during convalescence, during increased protein utilization, in pregnancy and
actation, during oral broad spectrum antibiotic therapy.
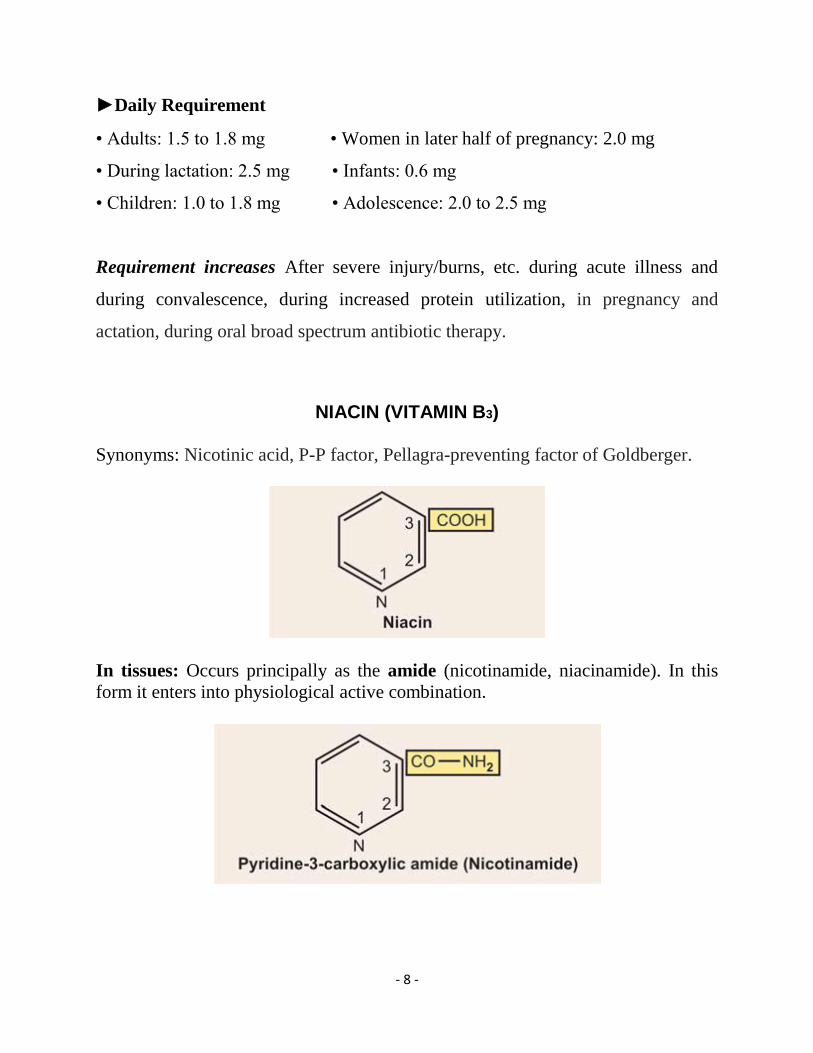
NIACIN (VITAMIN B3)
Synonyms: Nicotinic acid, P-P factor, Pellagra-preventing factor of Goldberger.
In tissues: Occurs principally as the amide (nicotinamide, niacinamide). In this
form it enters into physiological active combination.
- 9 -
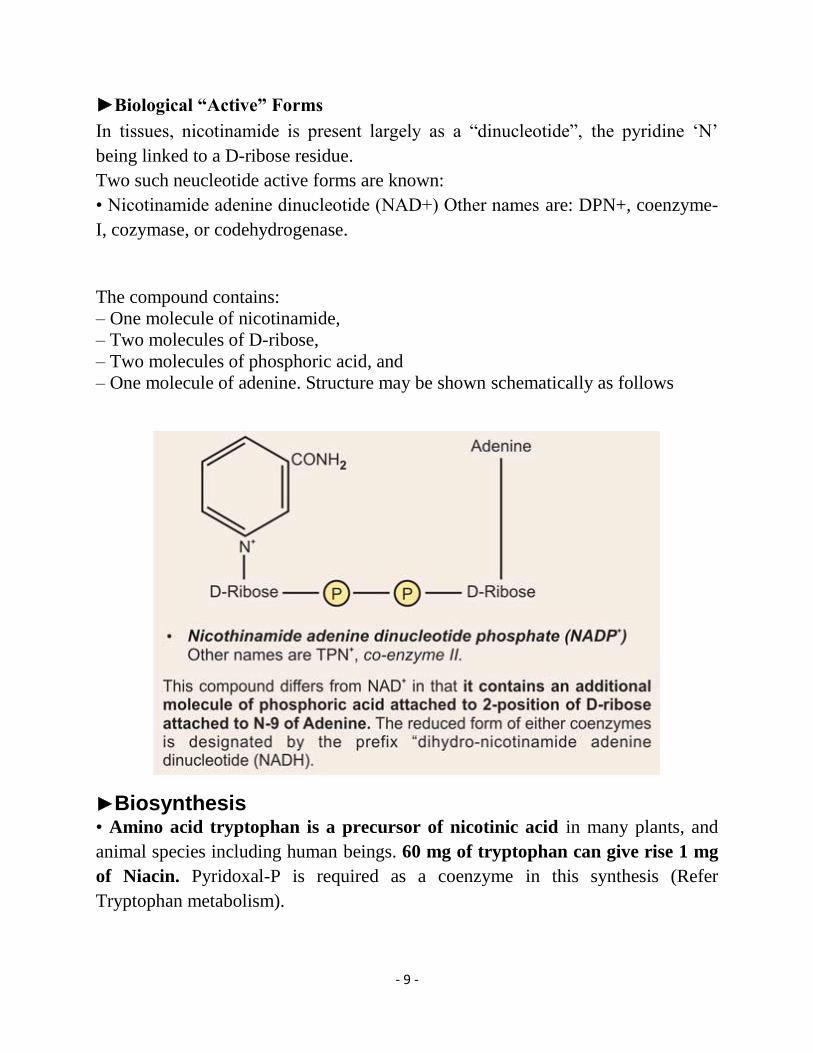
►Biological “Active” Forms
In tissues, nicotinamide is present largely as a “dinucleotide”, the pyridine ‘N’
being linked to a D-ribose residue.
Two such neucleotide active forms are known:
• Nicotinamide adenine dinucleotide (NAD+) Other names are: DPN+, coenzyme-
I, cozymase, or codehydrogenase.
The compound contains:
– One molecule of nicotinamide,
– Two molecules of D-ribose,
– Two molecules of phosphoric acid, and
– One molecule of adenine. Structure may be shown schematically as follows
►Biosynthesis
• Amino acid tryptophan is a precursor of nicotinic acid in many plants, and
animal species including human beings. 60 mg of tryptophan can give rise 1 mg
of Niacin. Pyridoxal-P is required as a coenzyme in this synthesis (Refer
Tryptophan metabolism).

- 10 -
• It can be synthesized also by intestinal bacteria. Bacteria in addition to
synthesis from tryptophan, can also synthesize from other amino acids, e.g.
glutamic acid, proline, ornithine and glycine.
• In human beings:
– In addition to dietary source,
– It is synthesised in tissues from amino acid tryptophan, and
– To a limited extent supplemented by bacterial synthesis in intestine.
Applied Aspect
In high corn diet, requirement of dietary niacin increases, as synthesis from
tryptophan cannot take place. The reason is the maize protein Zein lacks the amino
acid tryptophan. Hence pellagra is more common in persons whose staple diet is
maize.
Metabolism
►Absorption: Nicotinic acid and its amide are absorbed from the small intestine.
►Blood/plasma level
• Whole blood: 0.2 to 0.9 mg/100 ml (average 0.6 mg%)
• RB cells: 1.3 mg%
• Plasma-total activity: 0.025 to 0.15 mg% (average 0.075 mg%)
Note
1. Most of the nicotinic acid and its amide in the blood is in RB cells, presumably
as coenzyme.
2. Values in the blood are not altered significantly even in severe Niacin
deficiency. Hence its determination is of no value in the detection of clinical
deficiency states.

- 11 -
►Excretion
In urine, it is excreted as follows:
• As nicotinic acid and nicotinamide: Normal adults on normal diet excretes both
nicotinic acid and its amide in urine.
Nicotinic acid: 0.25 to 1.25 mg daily. Nicotinamide: 0.5 to 4 mg daily.
• As N’-methyl nicotinamide: Major urinary metabolite is a methylated derivative-
N’-methyl nicotinamide. The methylation occurs in liver, by the enzyme
niacinamide methyl transferase.

- 12 -
►Occurrence and Food Sources:
1. Both nicotinamide and coenzyme forms are distributed widely in plants and
animals.
2. Important food sources are:
• Animal source: Liver, kidney, meat, fish
• Vegetable source: Legumes (peas, beans, lentils), nuts, certain green vegetables,
coffee and tea. Nicotinamide is present in highest concentration in germ and
pericarp (bran) in cereal grains. Yeast also particularly rich. Poor sources are:
Fruits, milk and eggs.
Metabolic Role • The coenzymes NAD+ and NADP+ operate as hydrogen and electron transfer
agents by virtue of reversible oxidation and reduction.
• Function of NADP+ is similar to that of NAD+ in hydrogen and electron
transport.
• The two coenzymes are interconvertible.

- 13 -
►CLINICAL ASPECT
Deficiency Manifestations
Pellagra: Nicotinic acid deficiency produces a disease called Cardinal features
described as “3 D’s” are • Dermatitis, • Diarrhoea, and • Dementia.
Precipitating factors are: (a) High-corn diet and (b) Alcoholism
Clinical Features
(a) Skin lesions: Typically involves areas of skin exposed to sunlight and
subjected to pressure, heat or other types of trauma or/irritation. The skin becomes
reddened, later brown, thickened and scaly.
(b) GI manifestations: Include
1- anorexia, nausea, vomiting, abdominal pain, with alternating constipation/
diarrhea, Diarrhoea becomes intractable later.
2- Gingivitis and stomatitis with reddening of the tip and margin of the tongue,
which become swollen and cracked.
3- Achlorhydria present in about 40% cases.
4- Thickening and inflammation of the colon, with cystic lesions of the
mucosa, which later becomes atrophic and ulcerated.
(c) Cerebral manifestations: These include headache, insomnia, depression and
other mental symptoms ranging from mild psychoneuroses to severe psychosis.
(d) General effects: These include:
1-Inadequate growth,
2-loss of weight and strength,
3-anaemia which may be due to associated deficiency of other vitamins.
4-dehydration and its consequences resulting from diarrhoea.

- 14 -
Daily Requirement
• In adult: 17 to 21 mg daily
• Infants: 6 mg
• Pre-adolescence: 17 mg
Requirement Increases in:
Increased calorie intake or expenditure, acute illness or early convalescence, after
severe injury, infection and burns, high corn or Maize diet, pregnancy and
lactation.
• Effect on plasma Lipids: Nicotinic acid and NOT amide have been found to
reduce the plasma lipid concentration in certain cases of hyperlipidaemia. Large
doses of Nicotinic acid from 3 to 6 Grams per day have been found to reduce the
levels of cholesterol, β-lipoproteins and TG in
blood.
• Niacin toxicity: Excessive dosage can produce toxic effects:
– Dilatation of blood vessels and flushing.
– Skin irritation
– Can produce liver damage.