atlas of dermatological manifestations of gastrointestinal disease || churg–strauss syndrome:...
TRANSCRIPT

115G.Y. Wu et al. (eds.), Atlas of Dermatological Manifestations of Gastrointestinal Disease, DOI 10.1007/978-1-4614-6191-3_48, © Springer Science+Business Media New York 2013
Clinical signs and features include: Systemic and pulmonary small and medium vessel vascu-• litis, tissue and peripheral hypereosinophilia, and extravas-cular granulomas, which occur in the presence of severe asthma Diagnosis usually made at about age 50 with an incidence • of 1.3–6.8 per million of the general population [ 1 ] and an incidence of 34.6–67 per million in asthmatics [ 2 ] Stage I (prodromal) begins in the second or third decade • of life with allergic rhinitis, nasal polyposis, sinusitis, and asthma Stage II (eosinophilic phase) increased peripheral eosino-• phils that in fi ltrate the organs (eosinophilic pneumonia, eosinophilic gastroenteritis) Stage III (vasculitic) systemic vasculitis • Most frequently involved systems involve peripheral ner-• vous system in 65–76%, lungs in 51–65%, and skin in 52–57% [ 1 ] Skin changes occur in one half to two thirds of patients • and include nonthrombocytopenic palpable purpura (most common), occasional nodules, papules, petechiae, urti-
caria, and livedo of the extremities/trunk [ 2 ] (see Fig. 48.1 ) Peripheral nervous system disease is usually mononeuri-• tis multiplex but symmetrical peripheral neuropathy can develop
Pathogenesis of this disease involves: Unknown although strong association with asthma, atopy, • eosinophilia, heightened T-cell immunity, and positive antineutrophil cytoplasmic antibodies (ANCA) suggests autoimmune disorder is likely [ 3 ] Appears as though infectious, foreign, or autoantigen ini-• tiates the Th-2 response, leading to rhinosinusitis, asthma, then eosinophilic in fi ltration of vessels and organs [ 2 ] Strong association with anti-asthma medications particu-• larly anti-leukotriene receptor antagonists [ 2 ] Controversial whether asthma medications cause Churg–• Strauss syndrome (CSS) or whether these medications make it possible to taper steroid doses, thus unmasking CSS [ 3 ] Forty percent are positive ANCA and 90% of those with • positive ANCA are perinuclear ANCA; those with posi-tive ANCA are more likely to have a vasculitis pattern with greater incidence of renal involvement, neuropathy, alveolar hemorrhage, and fi brinoid degeneration/necro-sis; heart and lung disease (excluding alveolar hemor-rhage) are more likely in ANCA-negative patients [ 2 ]
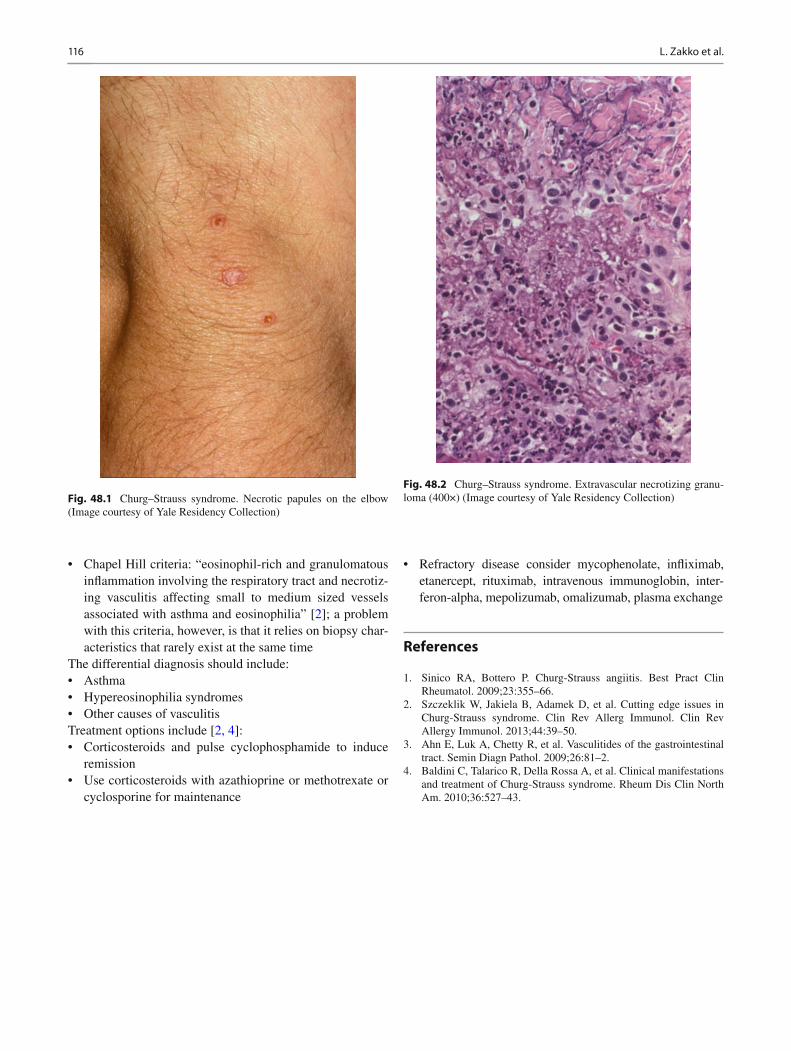
Histopathological features include: Eosinophilic in fi ltrates within the dermis • Extravascular granulomas ( see Fig. • 48.2 ) Leukocytoclastic vasculitis involving small and medium • sized vessels ( see Fig. 48.2 )
The diagnosis is made using a combination of [ 2 ] : New onset of four of the following: asthma, peripheral • blood eosinophilia (>10% of total leukocyte count), mono- or polyneuropathy, paranasal sinus abnormalities, eosinophilia in tissues on biopsy, migratory pulmonary in fi ltrates
Churg–Strauss Syndrome: Dermatological Features
Liam Zakko , Justin Finch, Marti J. Rothe , and Jane M. Grant-Kels
48
L. Zakko (*) Yale Department of Internal Medicine , 20 York Street , Yale New Haven Hospital , New Haven , CT 06510 , USA e-mail: [email protected]
J. Finch • M. J. Rothe • J. M. Grant-Kels Department of Dermatology , University of Connecticut Health Center , 21 South Road , Farmington , CT 06030 , USA e-mail: fi [email protected]; [email protected]; [email protected]
116 L. Zakko et al.
Chapel Hill criteria: “eosinophil-rich and granulomatous • in fl ammation involving the respiratory tract and necrotiz-ing vasculitis affecting small to medium sized vessels associated with asthma and eosinophilia” [ 2 ] ; a problem with this criteria, however, is that it relies on biopsy char-acteristics that rarely exist at the same time
The differential diagnosis should include: Asthma • Hypereosinophilia syndromes • Other causes of vasculitis •
Treatment options include [ 2, 4 ] : Corticosteroids and pulse cyclophosphamide to induce • remission Use corticosteroids with azathioprine or methotrexate or • cyclosporine for maintenance
Refractory disease consider mycophenolate, in fl iximab, • etanercept, rituximab, intravenous immunoglobin, inter-feron-alpha, mepolizumab, omalizumab, plasma exchange
References
1. Sinico RA, Bottero P. Churg-Strauss angiitis. Best Pract Clin Rheumatol. 2009;23:355–66.
2. Szczeklik W, Jakiela B, Adamek D, et al. Cutting edge issues in Churg-Strauss syndrome. Clin Rev Allerg Immunol. Clin Rev Allergy Immunol. 2013;44:39–50.
3. Ahn E, Luk A, Chetty R, et al. Vasculitides of the gastrointestinal tract. Semin Diagn Pathol. 2009;26:81–2.
4. Baldini C, Talarico R, Della Rossa A, et al. Clinical manifestations and treatment of Churg-Strauss syndrome. Rheum Dis Clin North Am. 2010;36:527–43.
Fig. 48.1 Churg–Strauss syndrome. Necrotic papules on the elbow (Image courtesy of Yale Residency Collection)
Fig. 48.2 Churg–Strauss syndrome. Extravascular necrotizing granu-loma (400×) (Image courtesy of Yale Residency Collection)