assessment of the skeletal pattern and its relevance in treatment planning
DESCRIPTION
OrthodonticsTRANSCRIPT
Assessment of the skeletal pattern and its relevance in treatment planning
“Knowing how to see”Leonardo da Vinci
“We only treat what we are educated to see. The more we see, the better the treatment we render our patients”
Arnett and Bergman AJODO 1993
Terms of reference
• Frankfort plane• Zero meridian• True vertical (plumb line)• Mandibular plane• Maxillary plane• Horizontal(Transverse) 1/5ths • Vertical 1/3rds• Midline(s)• Dentoalveolar compensation
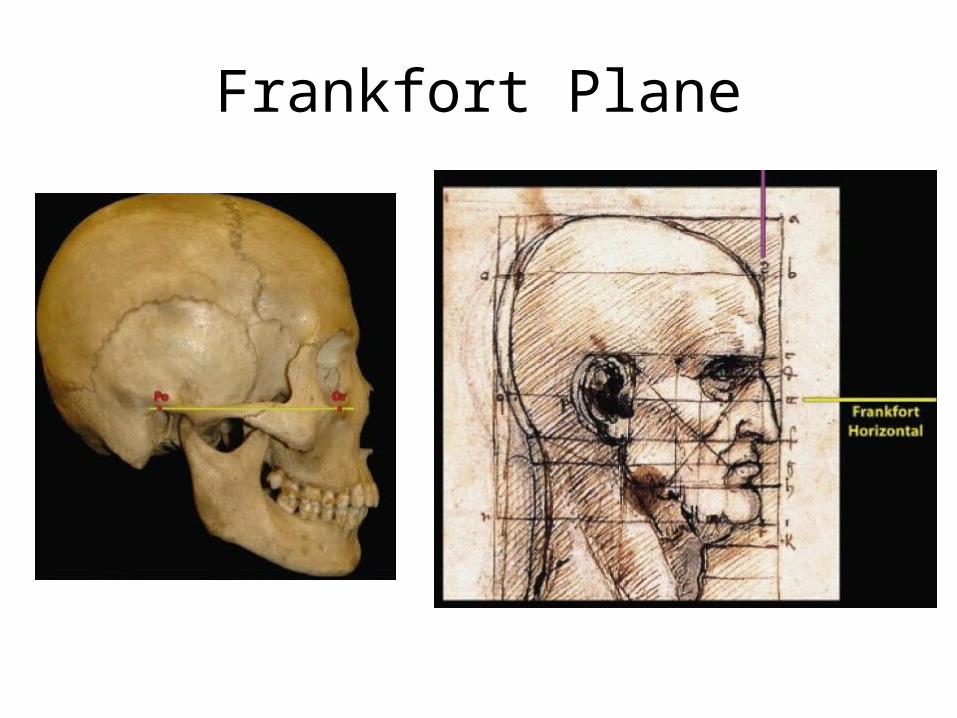
Frankfort Plane
Skeletal Class I, II or III?
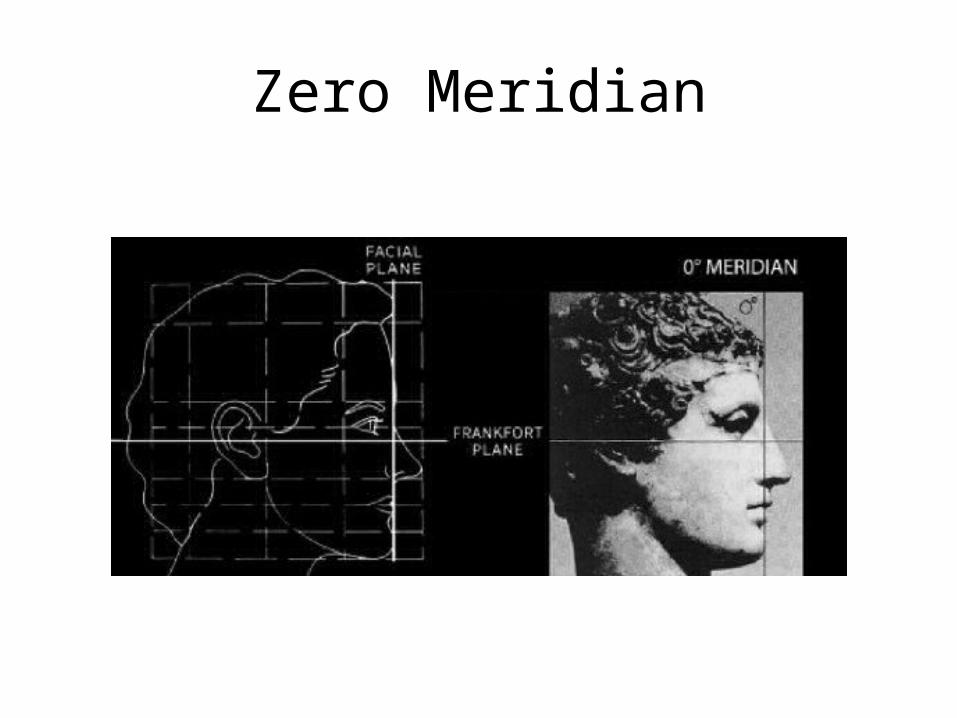
Zero Meridian
True Vertical
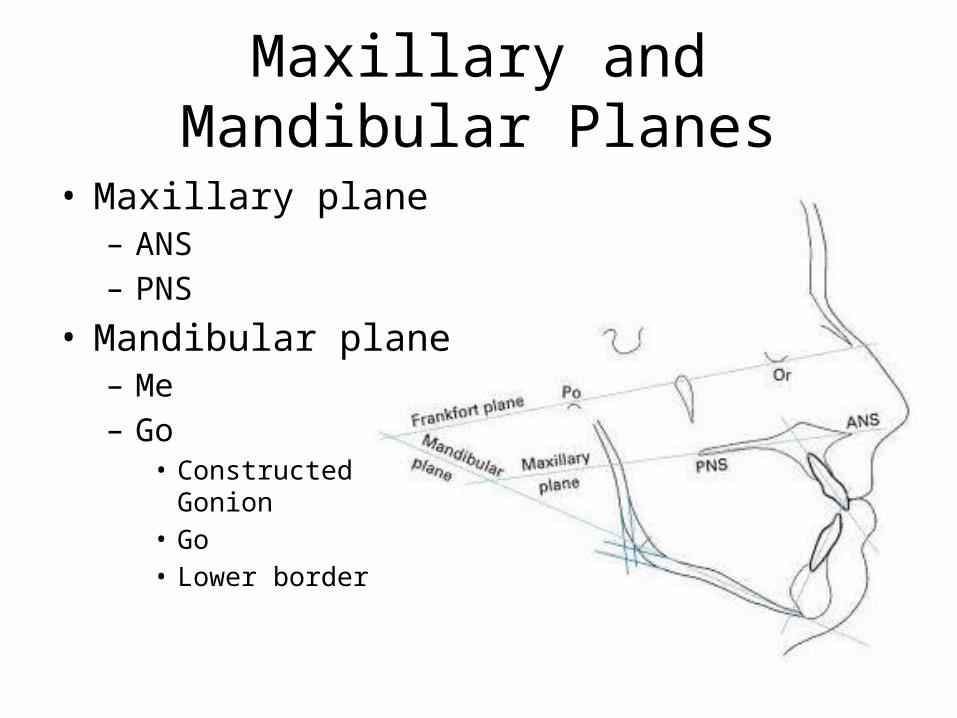
Maxillary and Mandibular Planes
• Maxillary plane– ANS– PNS
• Mandibular plane– Me– Go
• Constructed Gonion• Go• Lower border
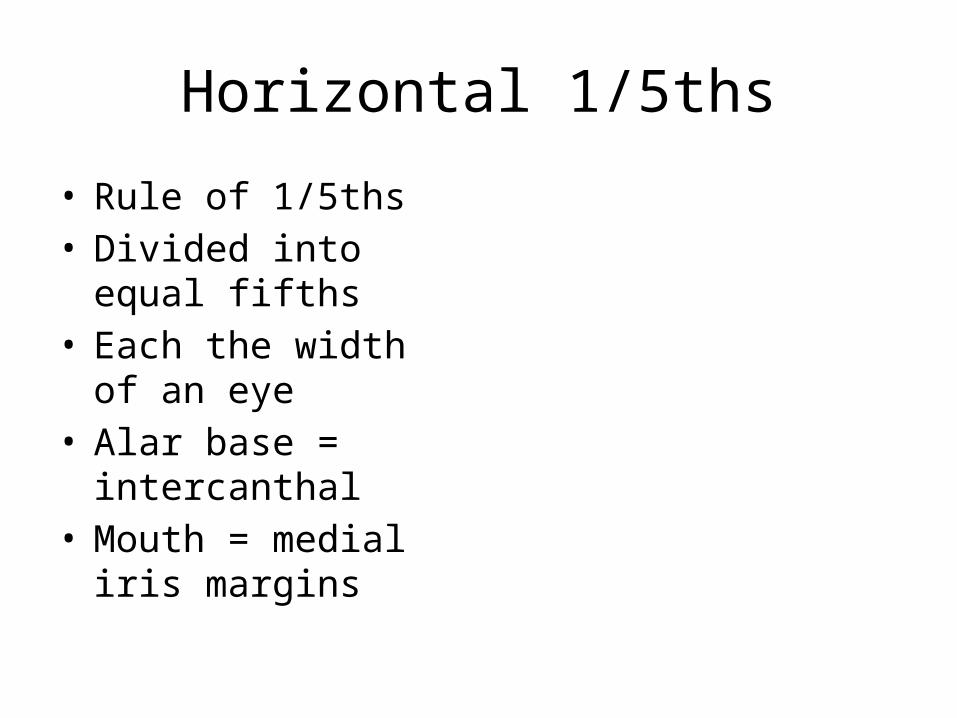
Horizontal 1/5ths
• Rule of 1/5ths• Divided into equal fifths• Each the width of an
eye• Alar base = intercanthal• Mouth = medial iris
margins
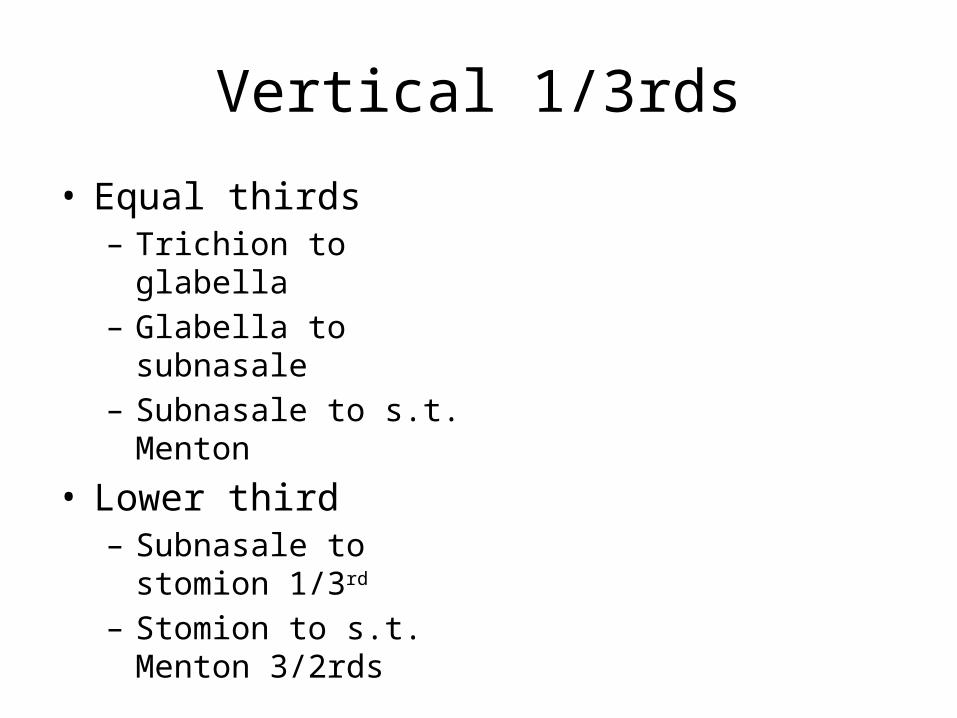
Vertical 1/3rds
• Equal thirds– Trichion to glabella– Glabella to subnasale– Subnasale to s.t. Menton
• Lower third– Subnasale to stomion
1/3rd
– Stomion to s.t. Menton 3/2rds
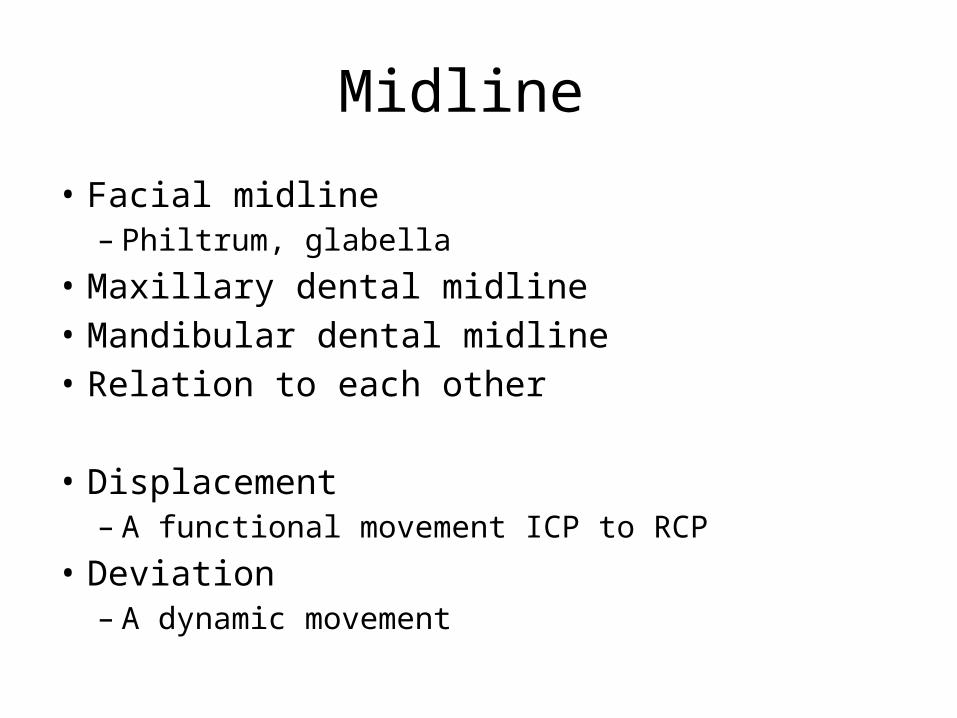
Midline
• Facial midline– Philtrum, glabella
• Maxillary dental midline• Mandibular dental midline• Relation to each other
• Displacement– A functional movement ICP to RCP
• Deviation – A dynamic movement
Dentoalveolar compensation
• A mechanism where the position of the teeth has altered in an attempt to maintain a normal inter-arch relationship
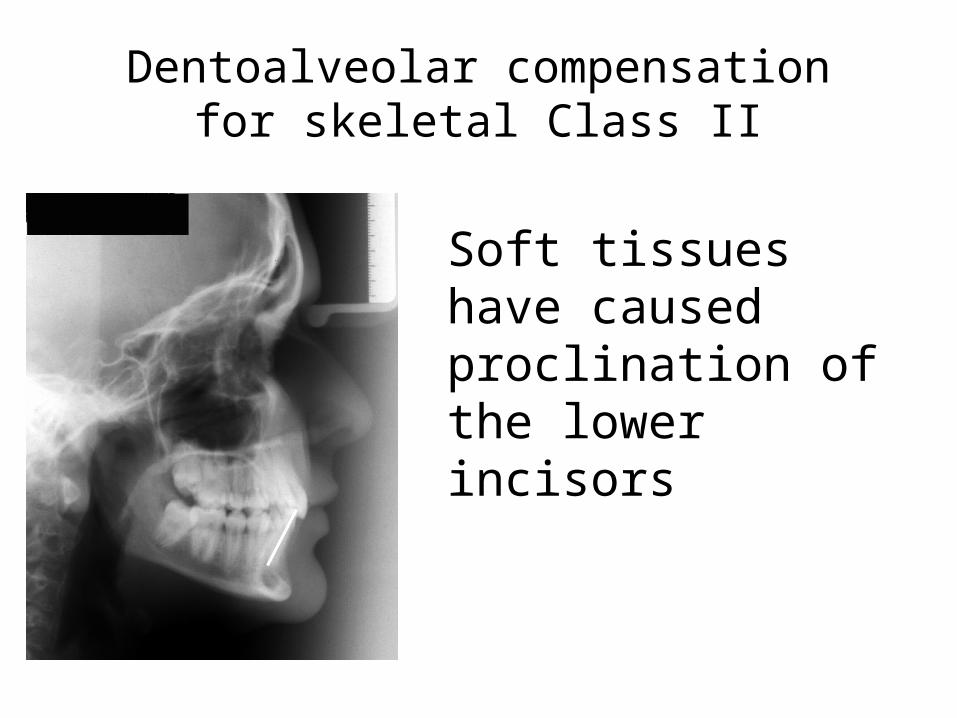
Dentoalveolar compensation for skeletal Class II
Soft tissues have caused proclination of the lower incisors
Aetiology
• 95% Complex interaction– Genetic– Environmental influence
• 5% Specific cause– In-utero disturbances– Syndromes– Trauma– Growth disturbances
Importance
• Greater genetic component: worse prognosis
• Mode of treatment– Interceptive– Camouflage– Orthognathic
Skeletal pattern
• Antero-Posterior• Vertical• Transverse
• Clinical assessment• Radiographic assessment
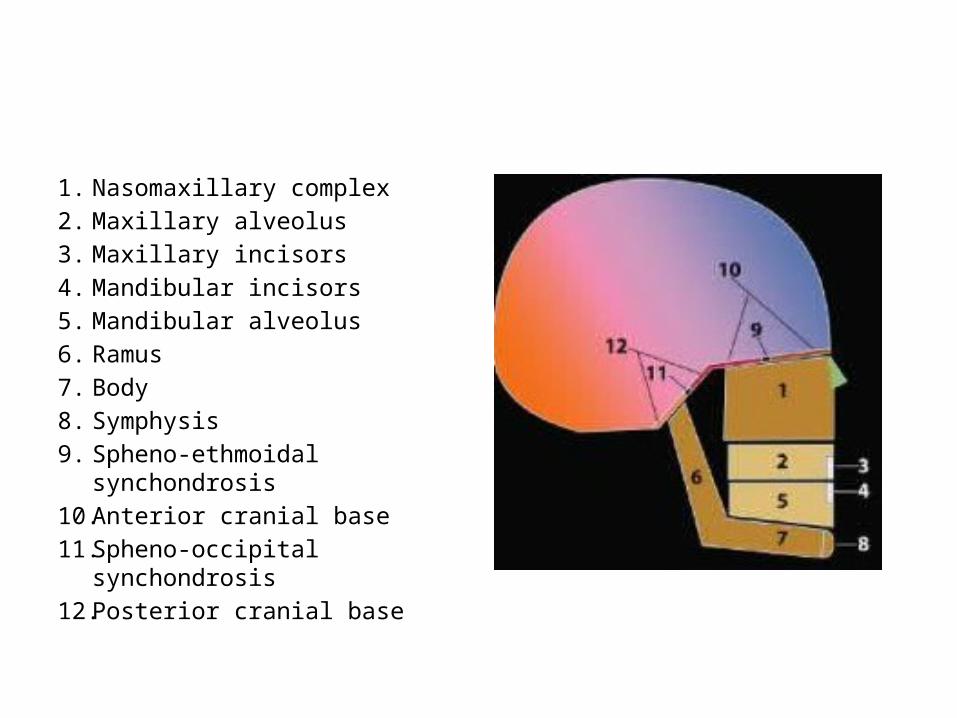
1. Nasomaxillary complex2. Maxillary alveolus3. Maxillary incisors4. Mandibular incisors5. Mandibular alveolus6. Ramus7. Body8. Symphysis9. Spheno-ethmoidal
synchondrosis10. Anterior cranial base11. Spheno-occipital synchondrosis12. Posterior cranial base
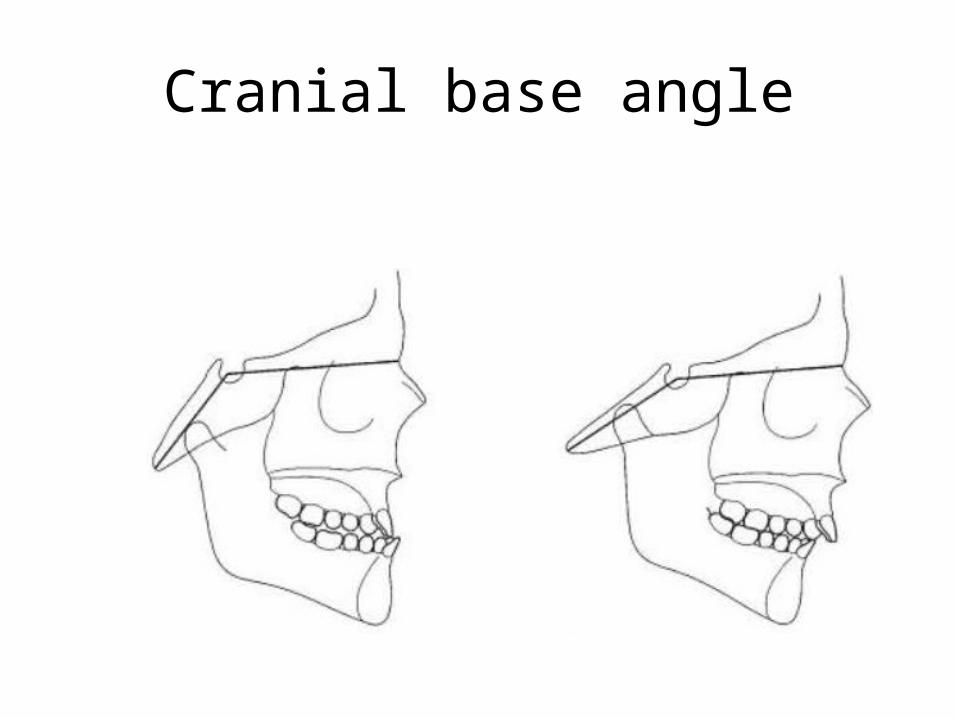
Cranial base angle
CLINICAL ASSESSMENT
Clinical assessment: How
• Sat upright in chair– Why? Class I, II or III– Natural Head Position(NHP)• Standard reproducible( 2°) head orientation• Relaxed• Looking at distant object or own eyes in mirror• Individual variation• Frankfort plane may not be horizontal
– Asymmetry; from above
Clinical assessment:ANTERO-POSTERIOR
• Soft tissue point A: Soft tissue point B• Kettle’s method• Soft tissue pogonion to zero-meridian• Profile convexity
• Sat upright in chair• Natural Head Position• Frankfort plane horizontal
Soft tissue point A: soft tissue point B
• Class I; 2-3mm
• Class II; Mandible retrusive to maxilla
• Class III; Mandible protrusive to maxilla
A
B
Kettle’s Method
Zero Meridian
Profile contour
• Straight• Convex– II
• Max excess• Mand def• combination
• Concave– III
• Max def• Mand excess• combination
• Upper facial plane; Glabella to Subnasale
• Lower facial plane; Subnasale to Pogonion
Clinical assessment:VERTICAL
• FMPA• Vertical 1/3rds – LAFH
Clinical assessment:Transverse
• Vertical 1/3rds• Horizontal 1/5ths• Ask pt to bite on a spatula
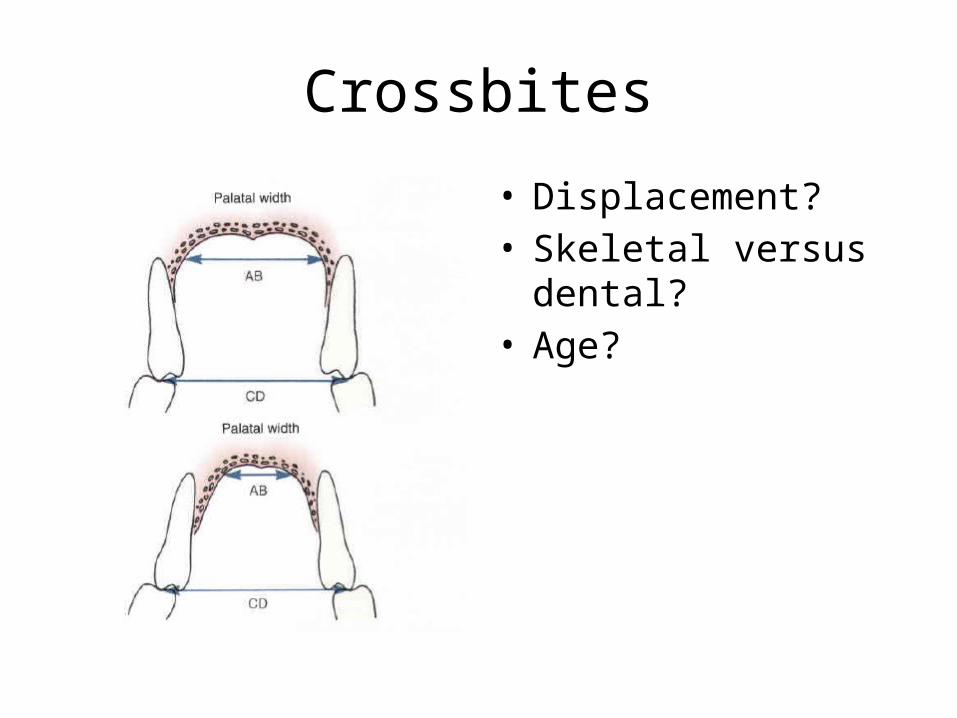
Crossbites
• Displacement?• Skeletal versus dental?• Age?
RADIOGRAPHIC ASSESSMENT
Indications for radiographs
• BOS Guidelines
Radiographic assessment:Antero-posterior
• ANB• Eastman correction• Wits analysis• Ballard conversion
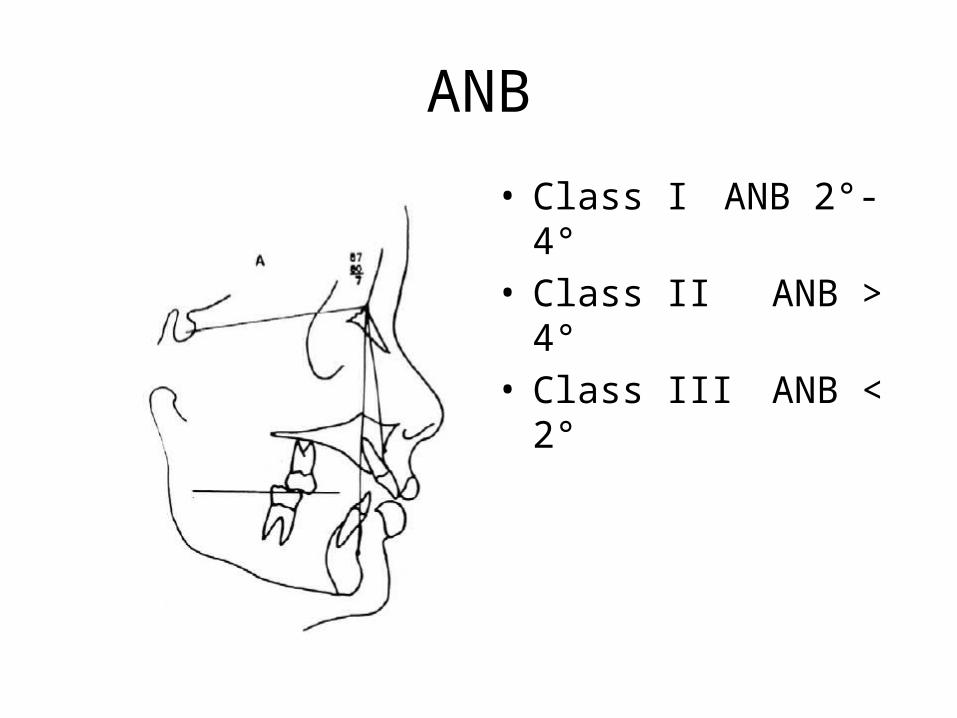
ANB
• Class IANB 2°-4°• Class II ANB > 4°• Class III ANB < 2°
Eastman Correction
• ANB assumes – SN is reliable– Points A and B reflect basal bone– Variation in position of Nasion affects SNA, SNB
and therefore ANB• Providing SN-Max plane is within 5-11°– For every degree SNA >81°, subtract 0.5° from
ANB– For every degree SNA <81°, add 0.5° to ANB
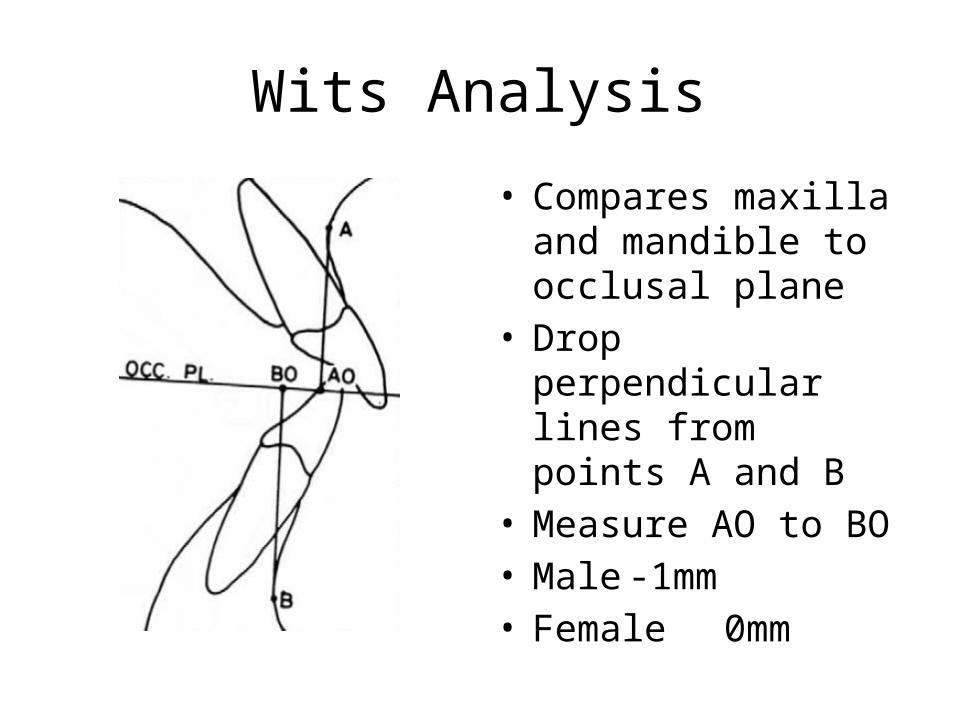
Wits Analysis
• Compares maxilla and mandible to occlusal plane
• Drop perpendicular lines from points A and B
• Measure AO to BO• Male -1mm• Female 0mm
Ballard Conversion
• Rotate the upper incisors to 109°• Rotate lower incisors to 120 – MMPA• Residual OJ reflects underlying skeletal pattern
Radiographic assessment:Vertical
• MMPA• LAFH:TAFH• Posterior face height: Anterior face height
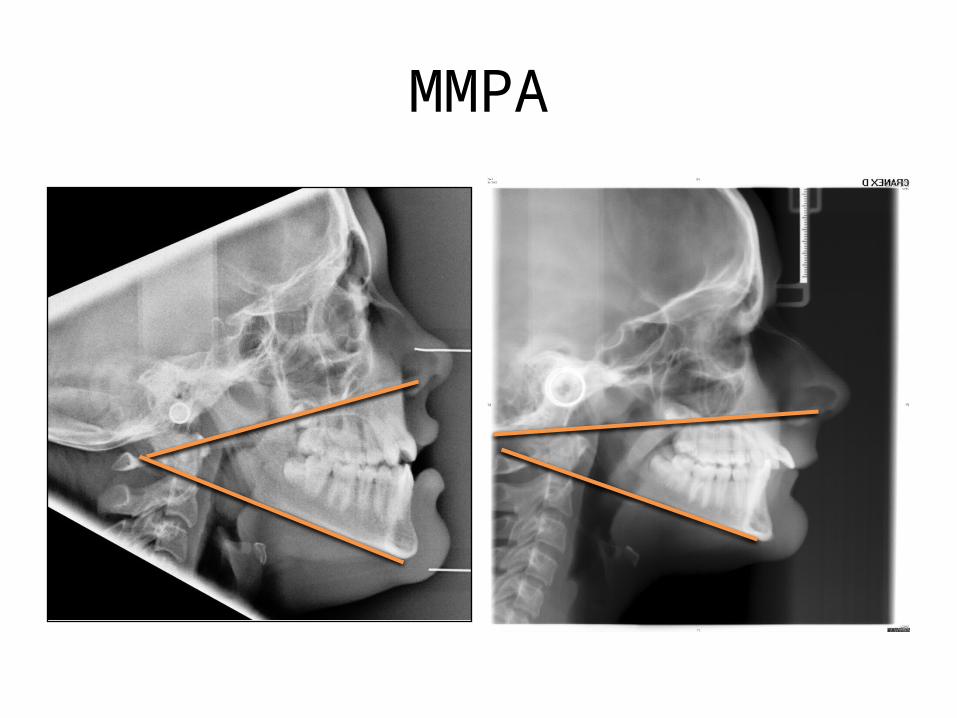
MMPA
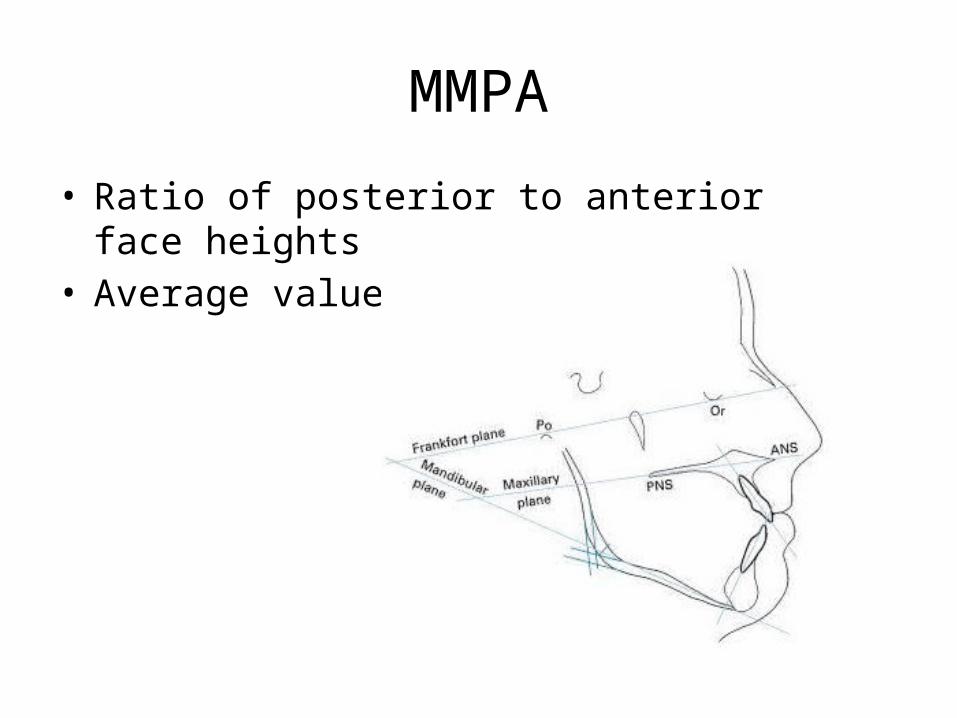
MMPA
• Ratio of posterior to anterior face heights• Average value 27° +/- 4°
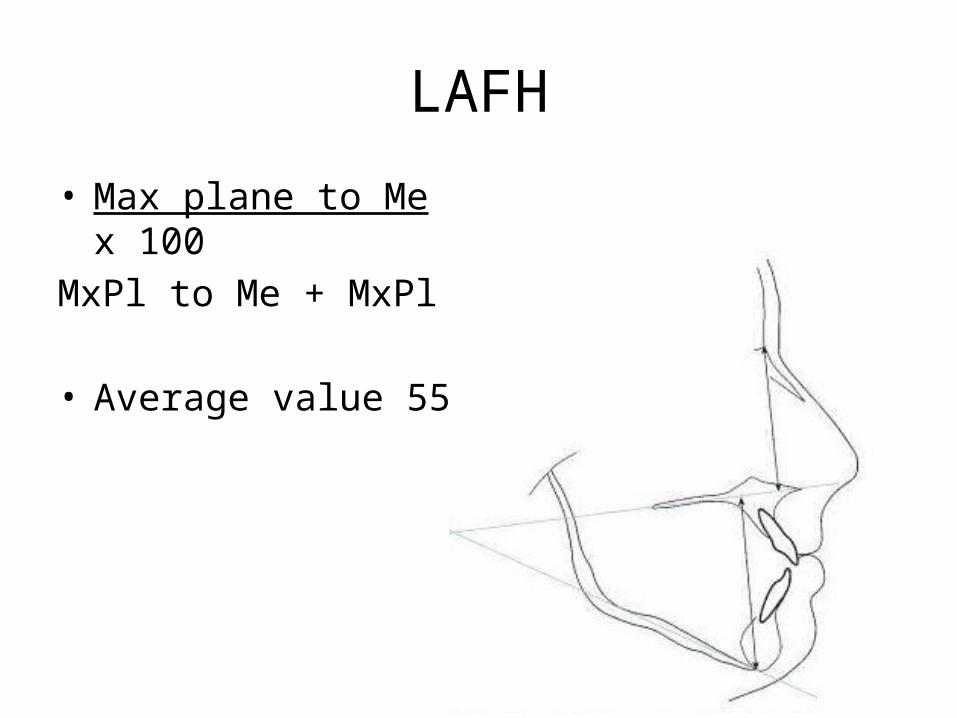
LAFH
• Max plane to Me x 100MxPl to Me + MxPl to N
• Average value 55%
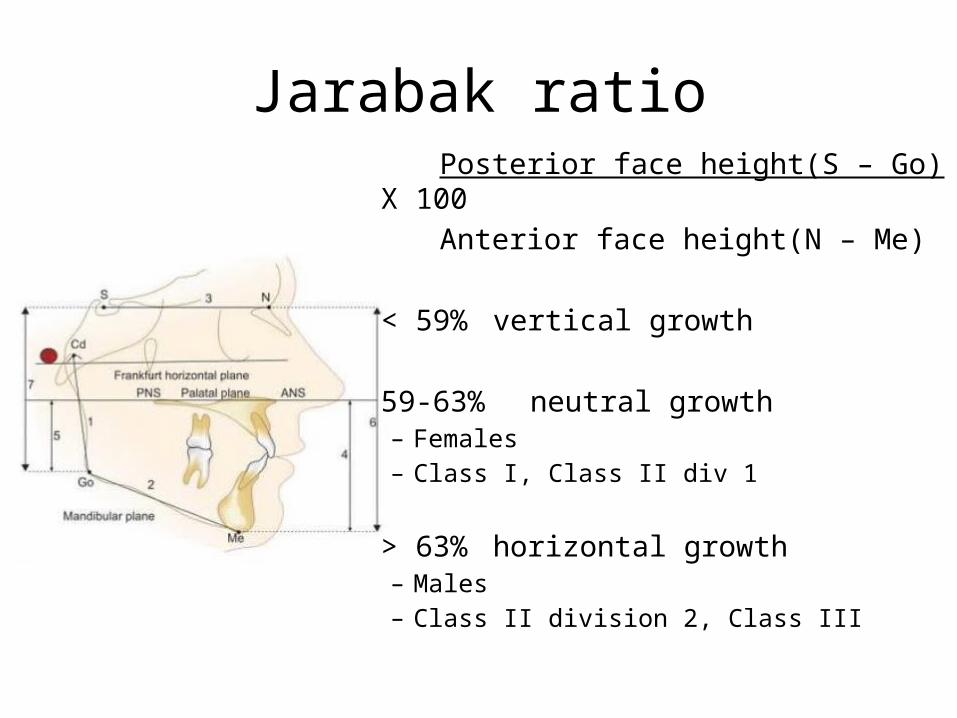
Jarabak ratio Posterior face height(S – Go) X 100 Anterior face height(N – Me)
< 59% vertical growth
59-63% neutral growth– Females– Class I, Class II div 1
> 63% horizontal growth– Males– Class II division 2, Class III
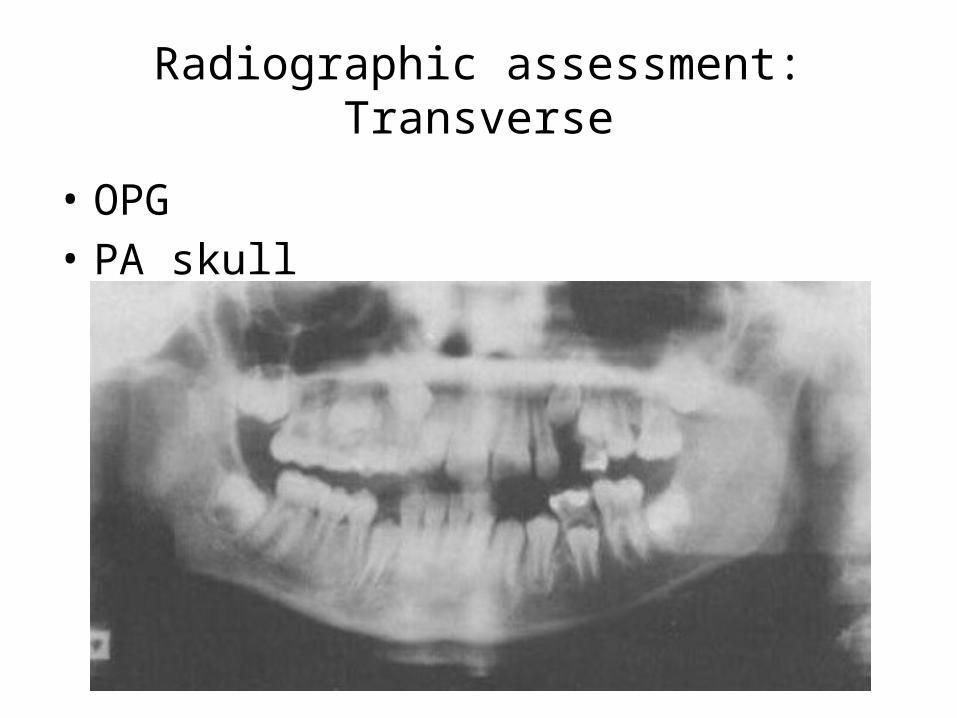
Radiographic assessment:Transverse
• OPG• PA skull

TREATMENT
Treatment planning
• Facial concerns• Dentoalveolar compensation• Influence of soft tissues• Mechanics– Compensation– High/low angle
• Growth– Expected future growth– Influence it?
Skeletal Class I
• Treatable• Be aware of vertical and transverse problems• Eliminate any unfavourable soft tissue influences• Soft tissue profile• Dentoalveolar assessment– Degree of crowding– Incisor protrusion
• A-Pog line (Raleigh Williams)• Aesthetic not for stability(Houston and Edler)• Lower labial segment position (Mills)
Skeletal Class II• Where is the problem?
– Prominent maxilla– Retrognathic mandible– Combination
• Mild, moderate or severe?• Influence of the soft tissues• Anchorage requirements
– Look at A-P position of canines and molars• Degree of dentoalveolar compensation
– Compensated Class II• Retroclined upper incisors• Proclined lower incisors• Both
Skeletal Class II
• Mild, treatable• Moderate – Growth modification– Camouflage– Associated vertical or transverse problems?
• Severe– Usually orthodontic/surgical treatment
Class II; Growth Modification
• Ideal class II functional case– Growing patient– Non xl with well-aligned arches– Skeletal mandibular retrusion– MM angle reduced or average– Increased overbite– Maxillary incisors proclined– Mandibular incisors retroclined
Class II; Camouflage
• Retraction of upper incisors– Relative prominence of nose– Nasolabial angle– Palatal bone to retract into to achieve edge centroid
• Proclination of lower incisors– Labial bony support and gingival recession– Stability
• Use of class II elastics• Facial profile considerations
Common xl patterns
• Finish to Class I molars– Upper 4s– Lower 5s
• Finish to Class II molars– Upper 4s– Lower non-xl
Class II; Orthognathic
• OJ > 10mm• Short mandible• Proclined lower incisors• Long face
Skeletal III
• Mild, treatable especially if simple interceptive treatment• GROWTH BEWARE. Can be very unpredictable• Refer early for growth monitoring• Treat once growth has slowed• Treat upper only?• Degree of dentoalveolar compensation– Compensated Class III
• Proclined upper incisors• retroclined lower incisors• both
Class III; Growth modification
• Facemask therapy• Mandell 2011– Early class III protraction HG in patients under
10years is skeletally and dentally effective in short term and does not result in TMD
– 70% successful, positive OJ– No clinically significant psychosocial benefit
• Awaiting results of long term follow up
Class III; Camouflage
• Less successful than Class II camouflage• Proclination of upper incisors• Retroclination of lower incisors– If excessive, increases chin prominence
• Use of class III elastics• Achieve edge to edge
Common extraction patterns
• Finish to Class I molars– Upper 5s– Lower 4s
• Possibility of future orthognathic treatment– LOWER non-XL?
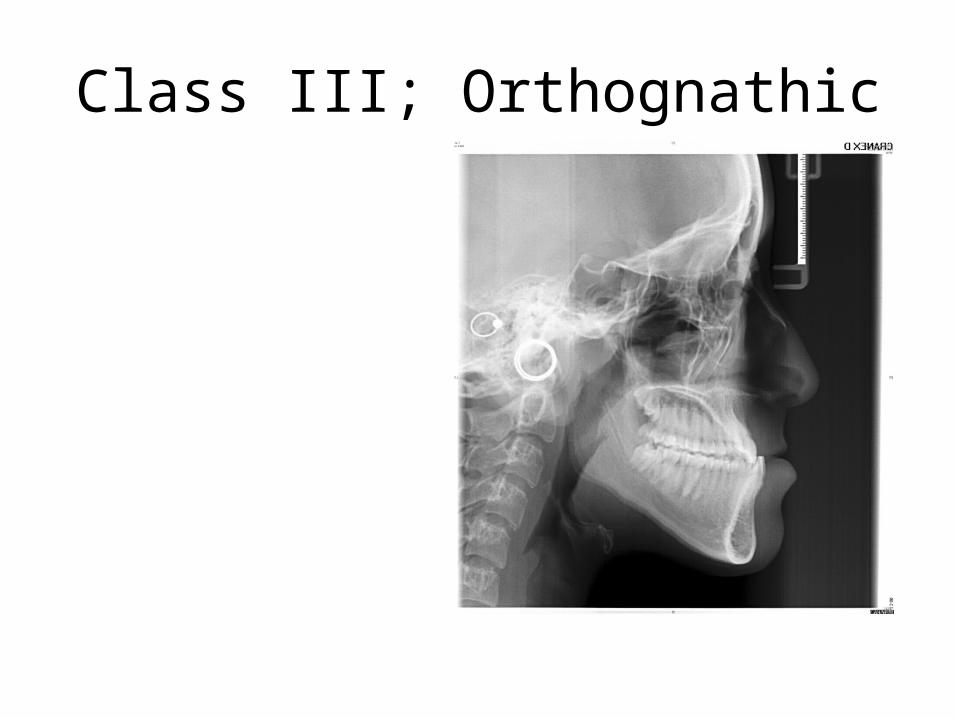
Class III; Orthognathic
Kerr; Limits for Class III
• ANB below -4°• Holdaway angle below 3.5°• Lower incisors retroclined more than 78.5°
Vertical; Low MMPA
• Reduced anterior face height• Increased OB• Forward rotation of mandible• Excessive eruption of lower incisor teeth• Extractions avoided as space closure retracts
lower labial segment and worsens OB
Vertical; High MMPA
• Increased anterior face height• Reduced OB and mild AOB, treat• Anchorage rapidly lost but ?stability?• Increased AOB, orthognathic• Care with excessive eruption of posterior teeth– High pull headgear– Buccal bite blocks– microscrews
VME
Transverse problems
• Displacement? – Eliminate
• True mandibular asymmetry– Refer– Growth potential– Accept?– Surgical approach
Tx options
• Grinding premature contact in deciduous dentition• Asymmetric XLs• URA• QH• RME• SARPE• Functional• Headgear• Fixed• Orthognathic surgery
Growth
Growth rotations;– reflection of differential growth between anterior and
posterior face heights(Bjork 1955, 1969)• Backward– Type I– Type II
• Forward– Type I– Type II– Type III
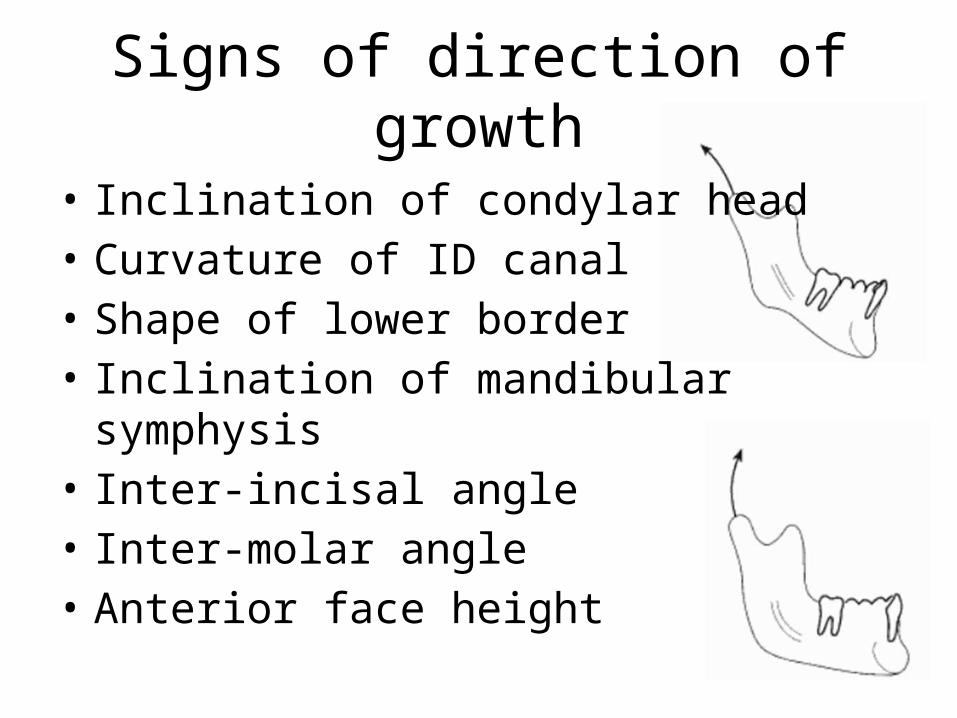
Signs of direction of growth
• Inclination of condylar head• Curvature of ID canal• Shape of lower border• Inclination of mandibular symphysis• Inter-incisal angle• Inter-molar angle• Anterior face height
Proffit; Limitations for camouflage
Acceptable results likely• Average/short facial pattern• Mild A-P discrepancy• Crowding < 4-6mm• Normal soft tissues• No transverse skeletal
discrepancies
Poor results likely• Long vertical facial pattern• Moderate or severe A-P
skeletal discrepancy• Crowding >4-6mm• Exaggerated facial features• Transverse skeletal
discrepancies
Summary
Camouflage• Too old for successful
growth modification• Mild/Moderate Class II• Mild Class III• Good alignment• Average vertical proportions
Avoid camouflage• Still potential for growth
modification• Severe Class II or Class III• Significant vertical
discrepancy• Severe crowding and
protrusion• Adults better managed with
orthognathic surgery