arthroscopy: management of chronic septic arthritis
TRANSCRIPT
MANAGEMENT OF CHRONIC SEPTIC
ARTHRITIS:- POST ARTHROSCOPY
Case Presentation
By: Chrystal Lynch
First Year Physical Therapy Student
OBJECTIVES
• To provide a brief overview of the anatomy of the knee.
• To define septic arthritis.
• To provide a brief incidence of septic arthritis.
• To explain the aetiology and pathology of septic arthritis.
• To provide the signs and symptoms of septic arthritis.
• To describe the medical and surgical management.
• Introduction of patient’s case.
• To describe the physical therapy management
ANATOMY OF THE KNEE JOINT
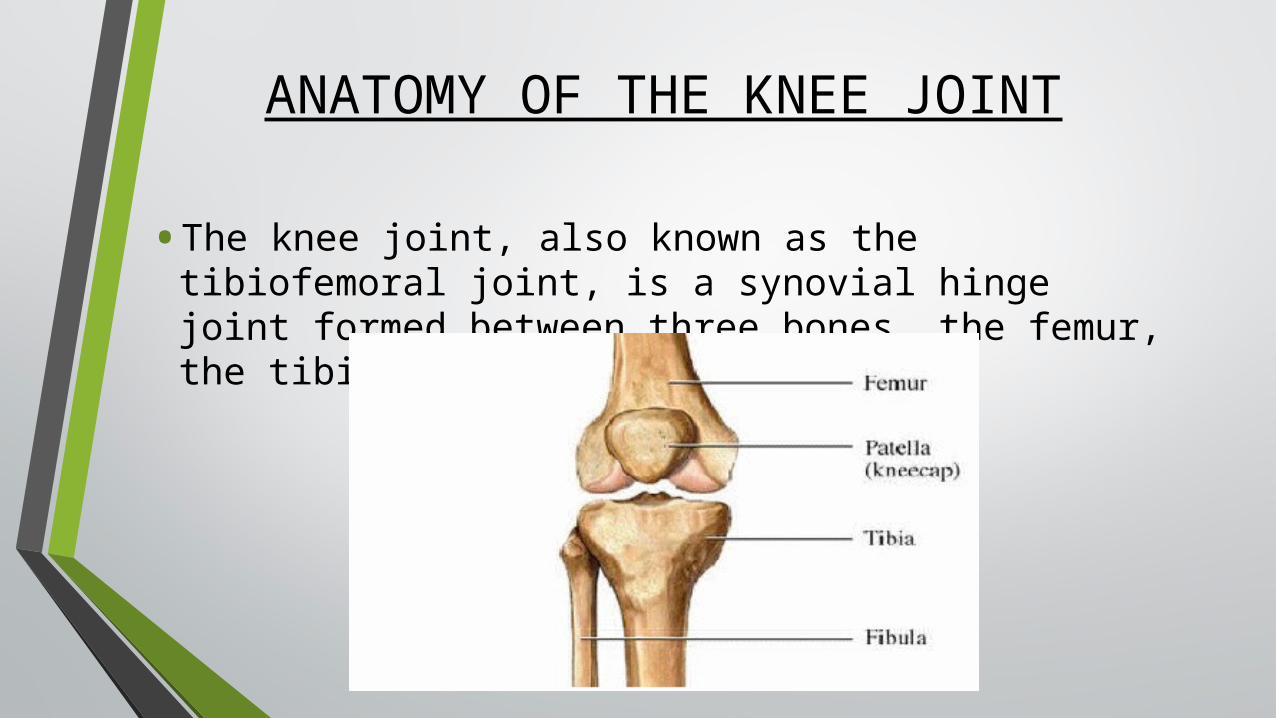
• The knee joint, also known as the tibiofemoral joint, is a synovial hinge joint formed between three bones, the femur, the tibia and the patella.

• In-between the distal femur and proximal tibia, is a fibrocartilage called the meniscus.
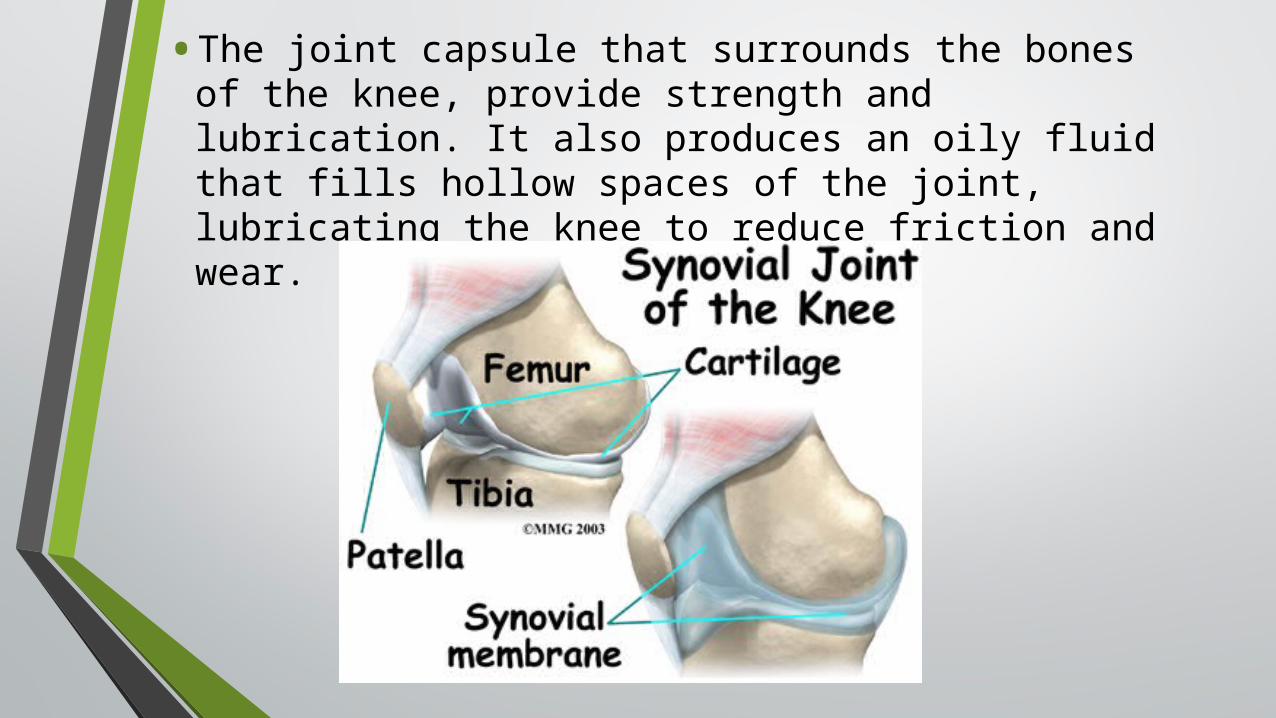
• The joint capsule that surrounds the bones of the knee, provide strength and lubrication. It also produces an oily fluid that fills hollow spaces of the joint, lubricating the knee to reduce friction and wear.
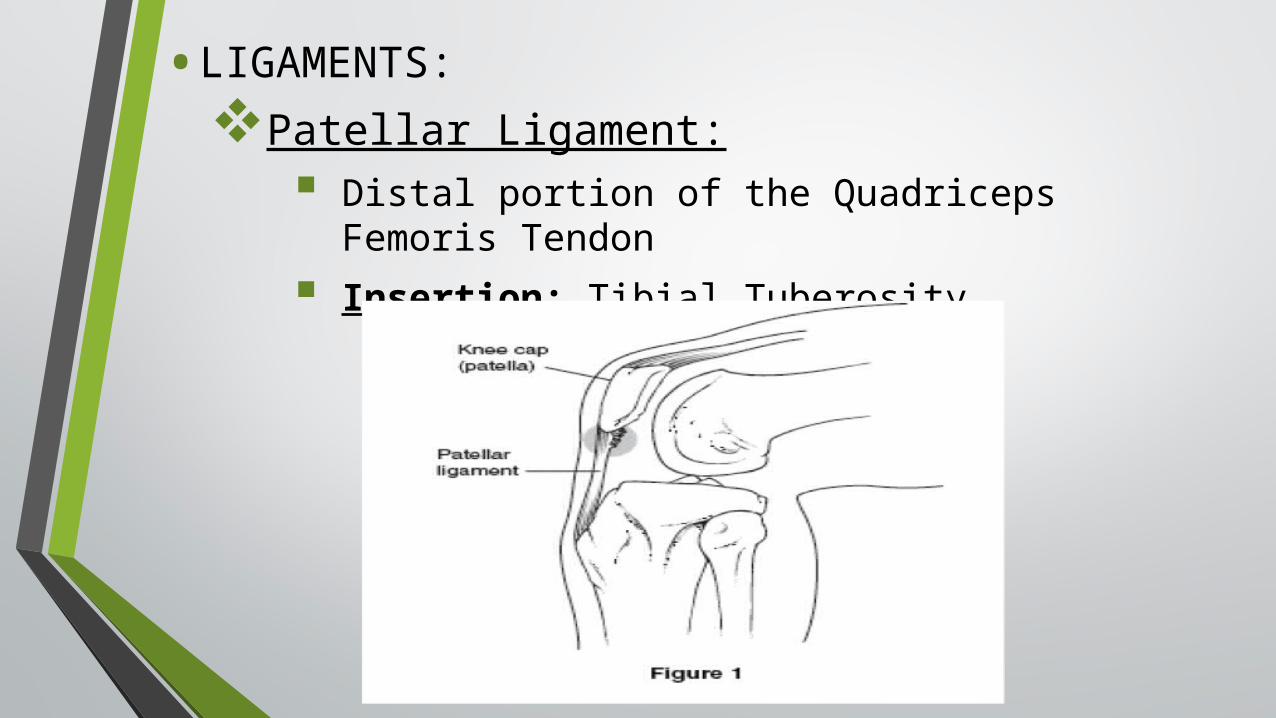
• LIGAMENTS:
Patellar Ligament:
Distal portion of the Quadriceps Femoris Tendon
Insertion: Tibial Tuberosity

The Medial Collateral Ligament:
Origin: Medial Epicondyle of Femur.
Insertion: Medial surface of the body of the tibia.
Function: Prevents excessive abduction of the knee.
The Lateral Collateral Ligament:
Origin: Lateral Epicondyle of Femur.
Insertion: Head of Fibula.
Function: Prevents excessive adduction of the knee.


Anterior Cruciate Ligament:
Origin: Anterior part of the tibial plateau
Insertion: Posteromedial aspect of the lateral femoral condyle.
Function: Prevents excessive posterior movement of the femur on the tibia.

The Posterior Cruciate Ligament:
Origin: Posterior part of the tibial intercondylar area
Insertion: Anterior lateral aspect of the medial femoral condyle
Function: Prevents excessive anterior movement of the femur on the tibia.

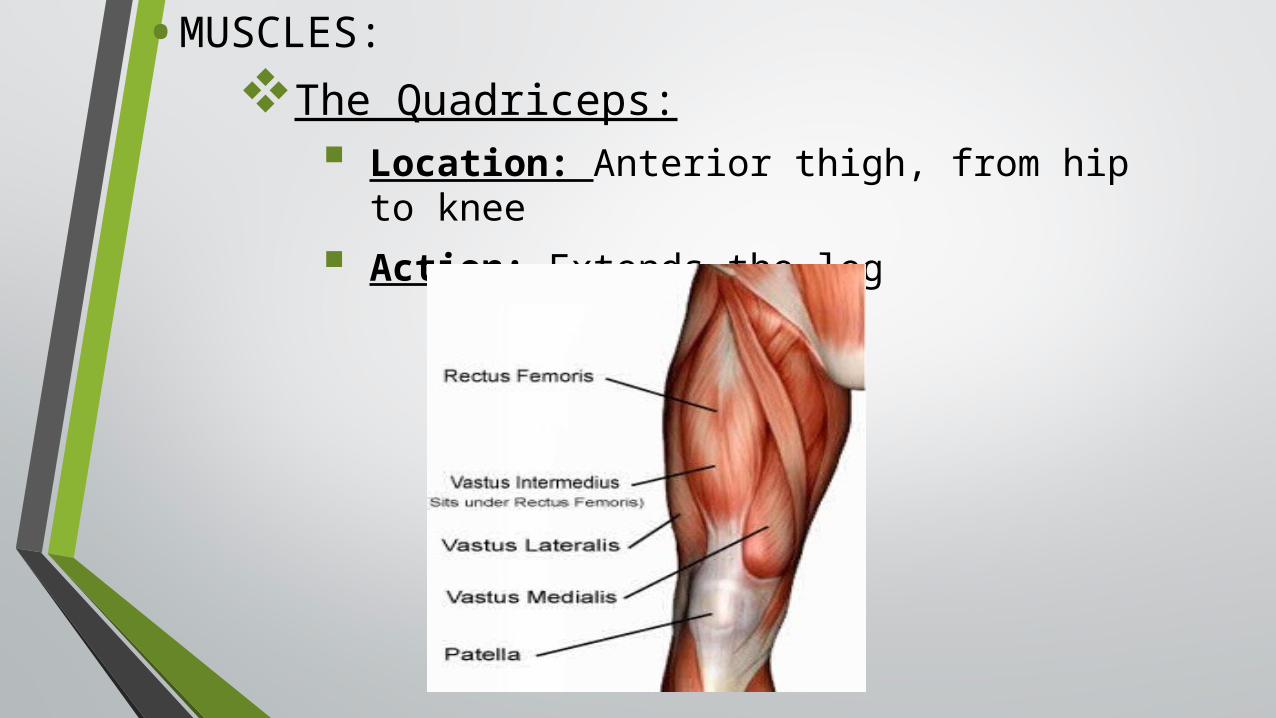
•MUSCLES:
The Quadriceps:
Location: Anterior thigh, from hip to knee
Action: Extends the leg
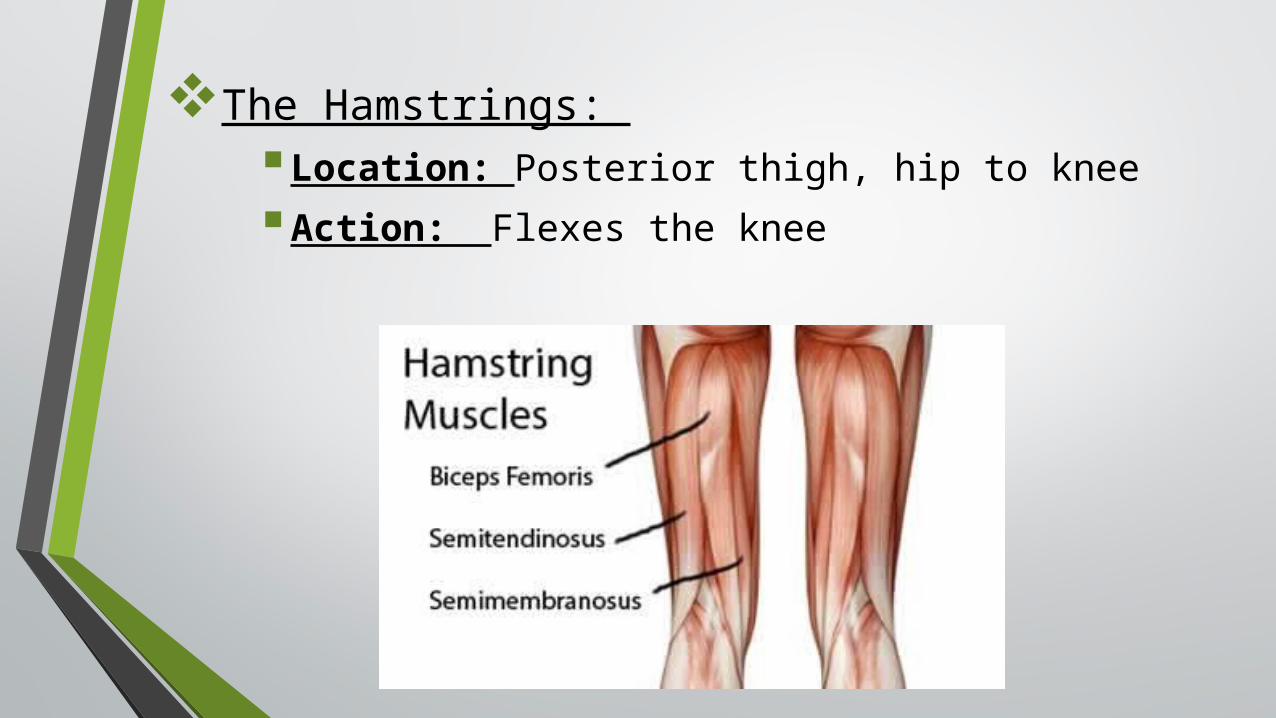
The Hamstrings:
Location: Posterior thigh, hip to knee
Action: Flexes the knee

Gastrocnemius:
Origin: Lateral condyle of femur (lateral head) and Medial condyle of femur (Medial head).
Insertion: Posterior surface of the calcaneus as the Achilles Tendon
Action: Flexes the Knee

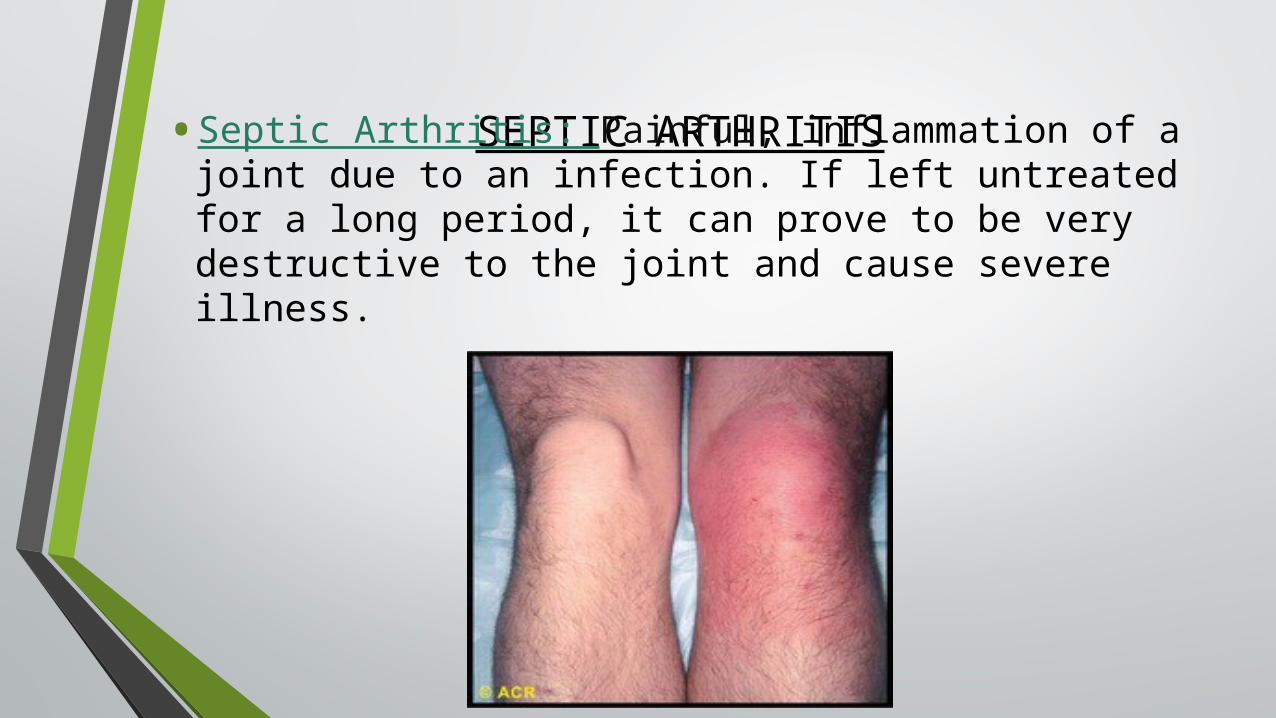
SEPTIC ARTHRITIS• Septic Arthritis: Painful, inflammation of a joint due to an
infection. If left untreated for a long period, it can prove to be very destructive to the joint and cause severe illness.

AETIOLOGY
• Septic Arthritis can be caused by bacteria that comes from another area of the body or from a bacterial infection, that is resulting from an open wound or opening from a surgical procedure.
•Most cases of acute septic arthritis is caused by bacteria such as staphylococcus aureus or streptococcus
• Chronic septic arthritis caused by organisms such as mycobacterium tuberculosis and candida albicans.

PATHOLOGY
• The most common route for the bacterial spread is hematogenuous.
• An inflammatory reaction is produced rapidly when the bacteria enters the joint and deposits in the synovial membrane.
• The inflammation results in an increase of white blood cells in the synovial fluid.
• The longer septic arthritis is left untreated, the more destruction to the joint occurs due to the microorganism/s.

INCIDENCE
Septic Arthritis:
• In Western Europe:
4-10 cases per 100,000 patient-years per year
• In Industrialized Countries:
6 per 100,000 of population per year
• Patients with underlying joint disease or prosthetic joint:
30 – 60 per 100,000 of population per year

• Persons at Risk for Septic Arthritis:
Young children, adolescents and the elderly.
Patients with diabetes, diabetes or any other pre-existing conditions.
Patients on haemodialysis.
Intravenous drug users.
Persons whose immune system is weakened
Chronic Arthritis
History of steroid injections into the joint
History of previous surgeries on the joint
Infection in another part of body
SIGNS AND SYMPTOMS
• Chills
• Joint is warm to touch
• Joint is red
• Fatigue and generalized weakness
• Fever
• Inability to move the limb of the affected joint
• Severe pain of the affected joint
• Swelling

MEDICAL AND SURGICAL MANAGEMENT
oAntibiotics
• Intravenously
• Tablets
oNSAIDs
oAntifungal Medication
oResting the Joint

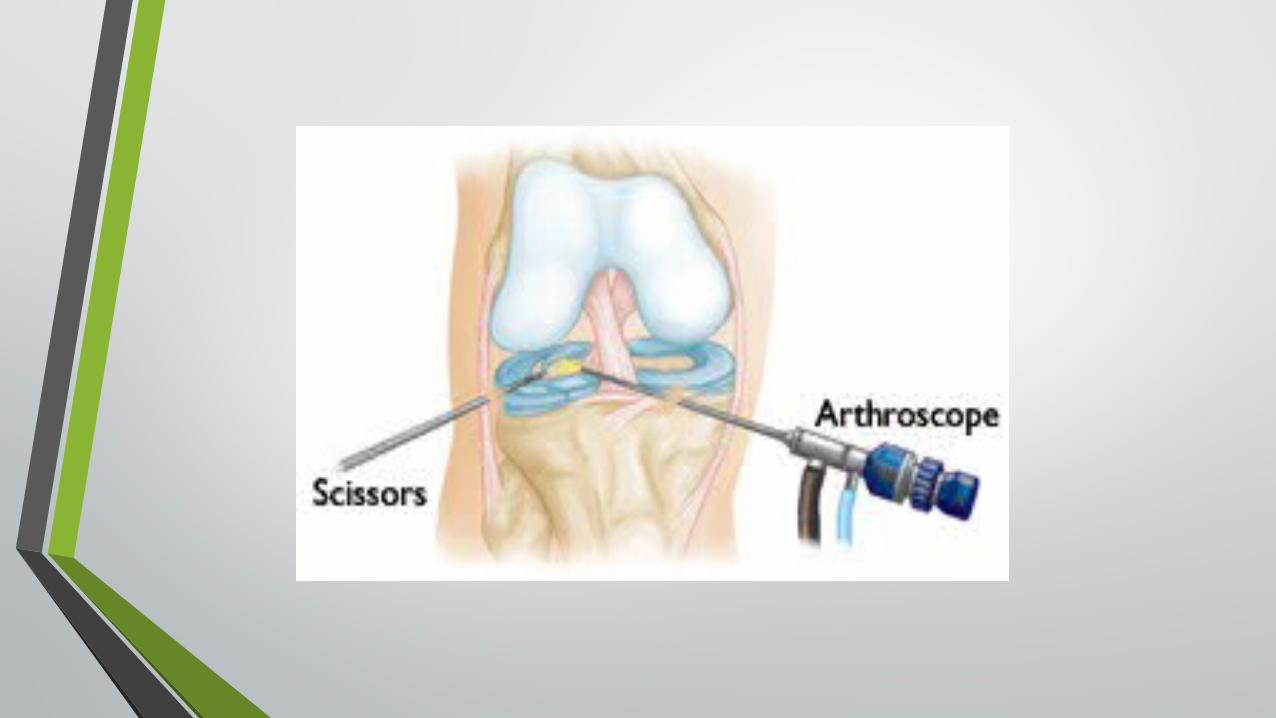
oArthroscopy: this a surgical orthopedic procedure performed on a joint, where the joint is viewed using a small camera. It is done through small incisions into the joint. – The American Orthopedic Society for Sports
Medicine.

oArthroscopic Lavage: clear sterile solution used to fill joint and rinse away any cloudy contents (blood, fluids or loose debris). It is usually combined with arthroscopic debridement. – Ontario Health Technology Advisory Committee Recommendations: Arthroscopic Lavage and Debridement for Osteoarthritis of the Knee

• Girth Measurements:
RIGHT LEFT33.5cm 10cm above
superior border of the patella
34.5cm
31cm Superior border of Patella
33.5cm
36.1cm 10cm below superior border of the patella
37.5cm