osteomyelitis & septic arthritis jay green november 23, 2006
TRANSCRIPT
Osteomyelitis & Septic Arthritis
Jay Green
November 23, 2006
Outline Both
Risk factors, mechanism of infection, pathogens
Osteomyelitis Septic Arthritis
Case 61y.o. M, ↑R leg pain, fever, H/A, fatigue PMH: DMII, CAD, smoker, COPD Recent # R tibia ORIF Post-op exacerbation of COPD still tx
Question What are some risk factors for bone/joint
infections?
Who gets bone/joint infections?
Risk Factors IV drug users AIDS Post-sx – prosthetic implants Iatrogenic immune suppression Sickle cell anemia Diabetes Alcoholism Pre-existing joint disease
Bone/Joint Infection – Fast Facts Bimodal age distribution
<20 y.o. and >50 y.o.
Occur in healthy kids or adults with RF Mortality (OM)
Pre-antibiotic era 20% Today <5%
1% incidence in inpatients
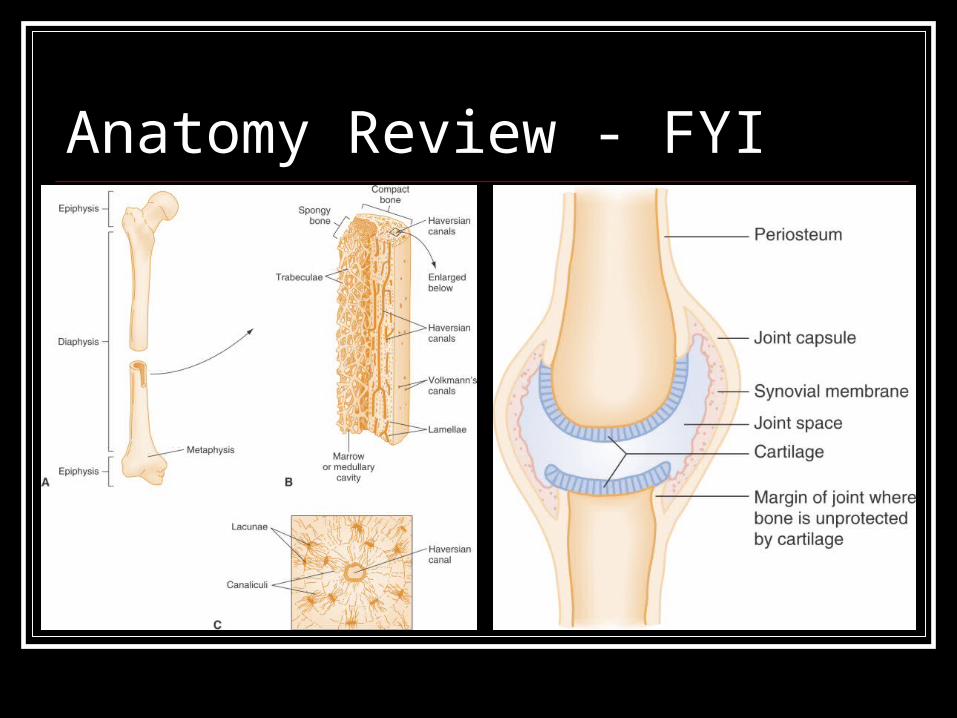
Anatomy Review - FYI
Case 51y.o. M, swollen, tender R knee Seen in ED 2 weeks ago fluid taken off Last 2 weeks ↑↑pain/redness/swelling knee Using ice, ibuprofen with some relief Now fever, fatigue, nausea, myalgias
Question By what mechanisms can a bone/joint
become infected?
Mechanism of Infection Hematogenous spread Contiguous spread Direct inoculation
Penetrating trauma Joint aspiration
Predisposed sites Long bone metaphysis, vertebral body
What bug? 12F from Angola
TB 23M sexually active
N. gonorrhea 68M with DMII and foot ulcer
S. aureus, Anaerobes, enterobacteriaceae 12F bit by her cat
Pasteurella 21M bouncer bitten by drunk on elbow
Eikenella 51M stepped on nail
Pseudomonas
Pathogens *Bacterial* Viral Fungal Parasitic
Depends on host/environmental factors
Pathogens – Key Points S. aureus = #1 (except neonates – GBS) H. influenzae B gone N. gonorrhea <30y.o. Gram –ve in elderly Polymicrobial – DM, post-trauma, chronic
Pathogens – Key Points Pseudomonas – puncture wound to foot,
prosthetic implants, IV drug users
Pasteurella multocida – animal bites
Fungal – increasingly common
Case 9F ↑ing pain R tibia x 4 days Malaise, H/A, fatigue, anorexia No fever at home, no trauma O/E:
Vitals: 375, 98/75, 88, 18 Gen: looks well R leg: erythema, swelling, ++tender, warm
?Osteomyelitis?
Question What would you like to order?
Labs? Imaging?
Osteomyelitis - History 5 cardinal signs of inflammation
Pain, erythema, swelling, warmth, ↓ function
±Fever Systemic symptoms
H/A, fatigue, malaise, anorexia
Osteomyelitis – Physical Exam General
Not ill
Inspection Erythema, swelling
Palpation Point tenderness, warmth ±involucrum, ±sequestrum
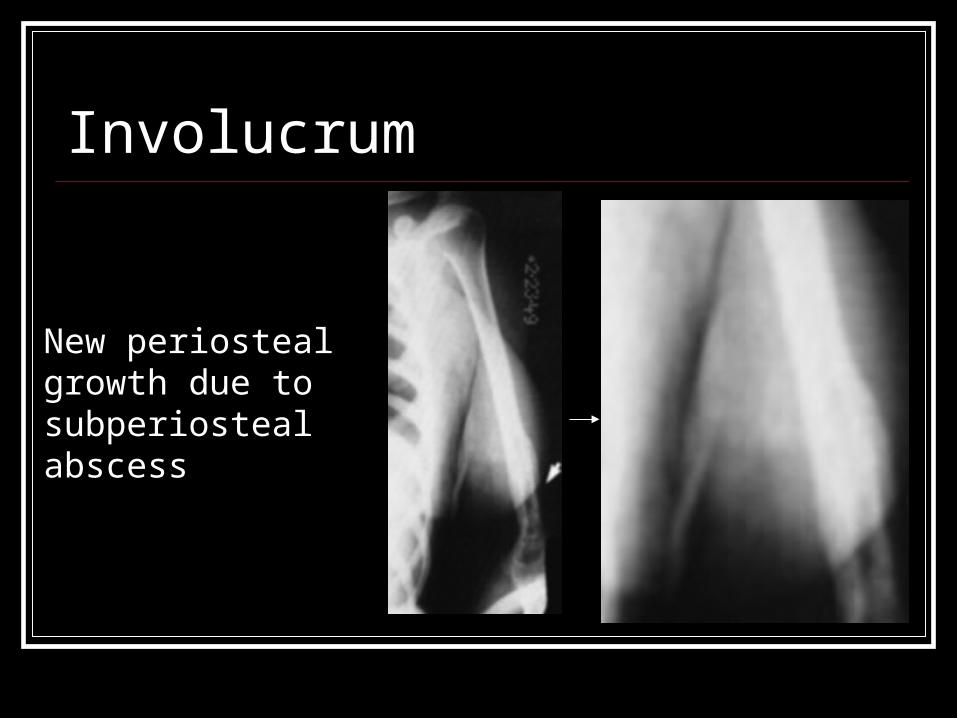
Involucrum
New periosteal growth due to subperiosteal abscess

Sequestrum
Disengaged ischemic segments of bone
Return to case WBC 12,000 ESR 80mm/hr Plain x-ray – N (confirmed by radiology)
What do you think of her ESR?
Investigations Labs typically unhelpful
±↑WBC (N – 15,000) ↑ESR more sensitive
Mean ESR = 70 <8% have ESR < 15
Imaging Start with plain films May miss acute presentation
<1/3 have abN x-ray if <10d of symptoms Lucent areas 30-50% bone mineral lost
Features? Lytic lesions, periosteal reaction, sequestra, involucrum Soft tissue – deep swelling, distorted fascial planes,
altered fat interfaces
Question WBC 12,000, ESR 80, plain film normal What would you like to do now?
Bone scan
Imaging – Nuclear Medicine Bone scan
Can detect OM within 48-72h 99mTc MDP 3-phase scan
Flow – within 60sec Pool – 5-15min Delayed – 2-4hrs
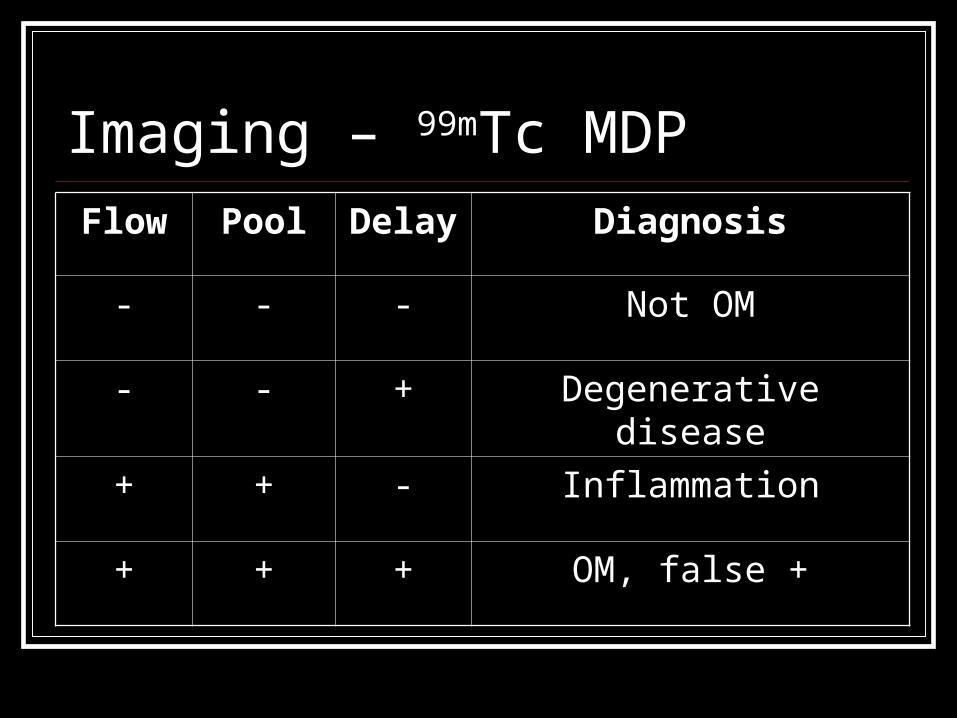
Imaging – 99mTc MDPFlow Pool Delay Diagnosis
- - - Not OM
- - + Degenerative disease
+ + - Inflammation
+ + + OM, false +
Imaging – 99mTc MDP SN > 90% FP rate ~65%
Trauma, surgery, tumor, chronic soft tissue infection, healing fracture
Other radionuclides 67Ga citrate 111In oxine 99Tc hexamethylpropyleneamine oxime
?Useful in ED All have 24-48h wait time
CT Scan May miss acute presentation Better for:
Sternum, vertebrae, pelvic bones, calcaneus
Useful post-bone scan, guides sx/bx
MRI Comparable SN to bone scan Better resolution IV gadolinium
Bone vs. soft tissue infection Normal vs. devitalized bone
Availability limited ?Replace bone scan altogether?
Question How do we find the bug? In ED
Blood culture+ in 50%– always if chronic
NOT cultures from fistulae/sinus Not in ED
Biopsy – needle, resection
Find bug in 80-90%
Question WBC 12, ESR 80, x-ray N, bone scan + What would you like to do doctor?
Management IV antibiotics
Typically empiric to begin 4-6 weeks
Surgery Debridement often necessary Can avoid in kids with acute hematogenous OM
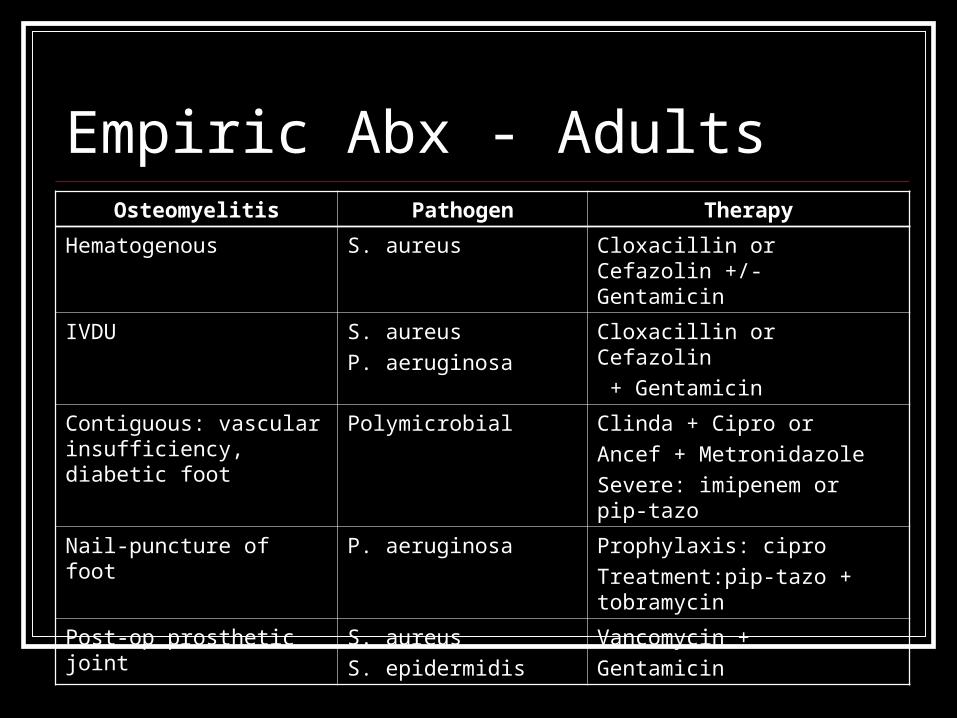
Empiric Abx - AdultsOsteomyelitis Pathogen Therapy
Hematogenous S. aureus Cloxacillin or Cefazolin +/- Gentamicin
IVDU S. aureus
P. aeruginosa
Cloxacillin or Cefazolin
+ Gentamicin
Contiguous: vascular insufficiency, diabetic foot
Polymicrobial Clinda + Cipro or
Ancef + Metronidazole
Severe: imipenem or pip-tazo
Nail-puncture of foot P. aeruginosa Prophylaxis: cipro
Treatment:pip-tazo + tobramycin
Post-op prosthetic joint S. aureus
S. epidermidis
Vancomycin +
Gentamicin
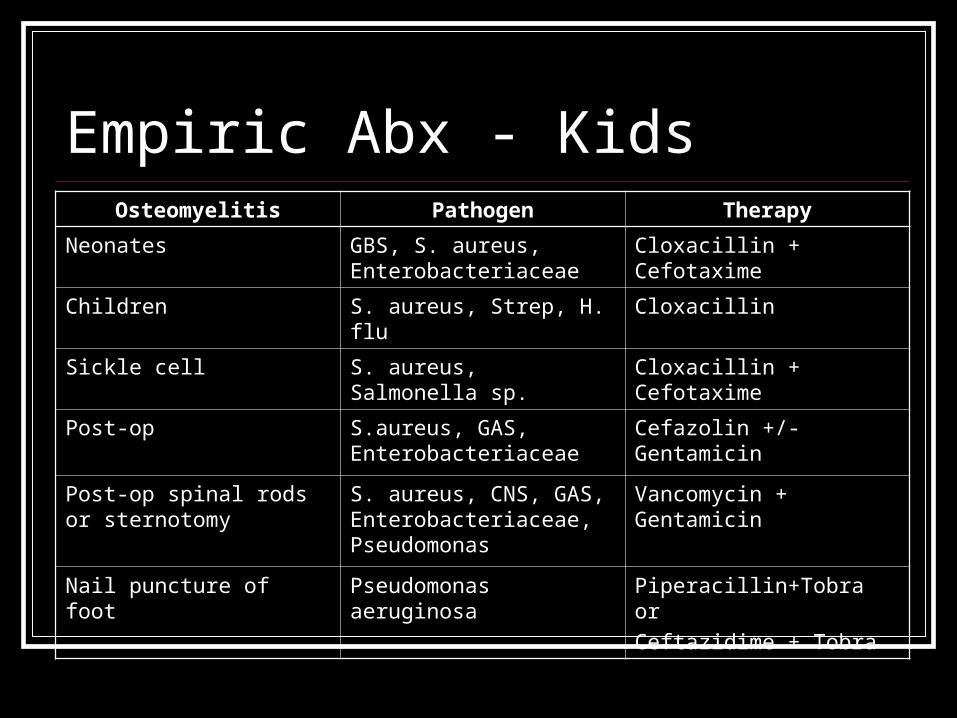
Empiric Abx - KidsOsteomyelitis Pathogen Therapy
Neonates GBS, S. aureus, Enterobacteriaceae
Cloxacillin + Cefotaxime
Children S. aureus, Strep, H. flu Cloxacillin
Sickle cell S. aureus, Salmonella sp. Cloxacillin + Cefotaxime
Post-op S.aureus, GAS, Enterobacteriaceae
Cefazolin +/- Gentamicin
Post-op spinal rods or sternotomy
S. aureus, CNS, GAS, Enterobacteriaceae, Pseudomonas
Vancomycin + Gentamicin
Nail puncture of foot Pseudomonas aeruginosa Piperacillin+Tobra or
Ceftazidime + Tobra
Case 77M DMII, ankle ulcer x 1 yr Draining pus, occasionally ↑pain/redness Several courses of abx over past year
Question Are imaging or cultures of the pus useful in
chronic osteomyelitis?
Will IV/PO antibiotics be sufficient?
Chronic Osteomyelitis Usually complication of post-traumatic OM,
surgery, diabetic foot infection Recurrent course Sequestra Chronic draining sinus/fistulae Polymicrobial, commonly anaerobes
Chronic OM - Investigations Bone scan – limited use Cultures of tracts not reliable Need bone bx
Chronic OM - Management Surgery
Antibiotic-containing beads Bone grafts
±HBO Seems to be effective in case-series and non-
randomized studies for DM foot osteomyelitis
Case 28 y.o. M Ped-MVC while biking to work Spinal precautions Tachycardic, BP 90/65 GCS = 11 Multiple abrasions, open # R tibia
Question How can we prevent OM in his R leg?
OM Prophylaxis In Open # Cut away surrounding clothing Pour sterile NS/water over bone Cover with moist sterile gauze Surface cultures?
Not predictive of future pathogens Manipulate?
Only if severe vascular compromise Early Abx
Ancef ± G- coverage
Case 4y.o. M, R hip pain x 2d, refusing to walk No trauma Cough, runny nose, sore throat last week O/E:
Vitals normal (T = 37.5°C) Refusing to walk, knee/ankle normal R leg in flexion, slight abd, slight ER Pain at end range of IR
Question What would you like to order doctor?
Investigations Labs
WBC 11.2, ESR 14 Imaging
Plain films “?R hip effusion, suggest U/S”
U/S – effusion present
Ideas?
Transient Synovitis Diagnosis of exclusion Most common cause of hip pain in kids Typically ages 3-6yrs Usually affects hip>knee Pain can be referred to knee/thigh U/S – effusion present in 60-70%
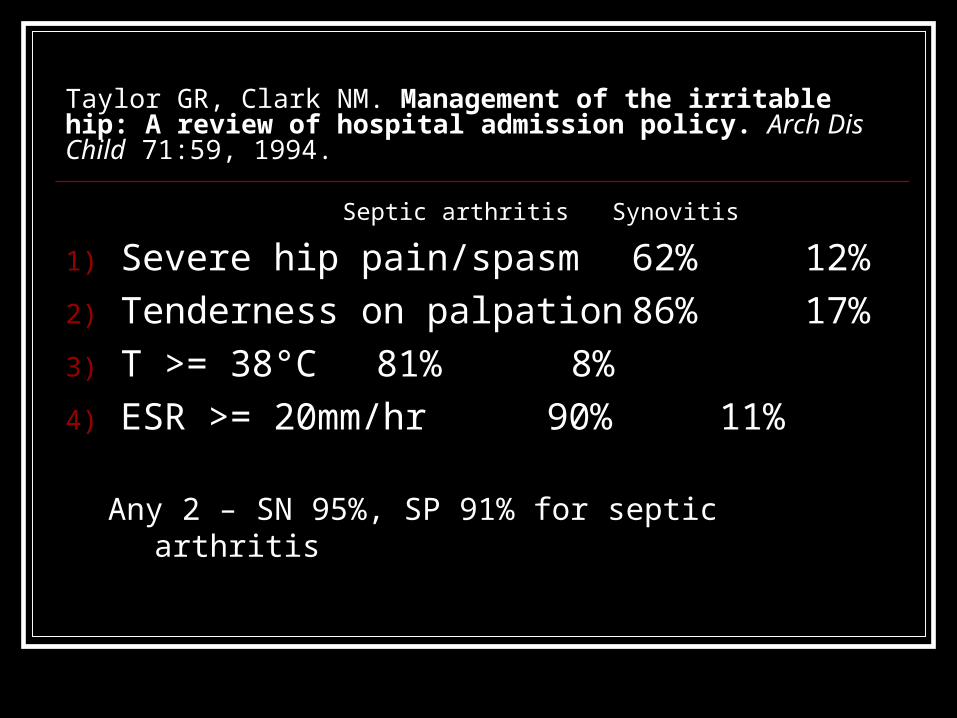
Taylor GR, Clark NM. Management of the irritable hip: A review of hospital admission policy. Arch Dis Child 71:59, 1994.
Septic arthritis Synovitis
1) Severe hip pain/spasm 62% 12%
2) Tenderness on palpation 86% 17%
3) T >= 38°C 81% 8%
4) ESR >= 20mm/hr 90% 11%
Any 2 – SN 95%, SP 91% for septic arthritis
Question You’re convinced this is TS…
How would you like to treat this child?
Transient Synovitis - Management Outpatient F/U exam in 12-24hrs ± 2wks Rest
Initial non-weight bearing Gradual return to activity
NSAIDs
Transient Synovitis - Outcome 75% - 2 weeks 88% - 4 weeks 12% - persistent pain x 8 weeks
These should have U/S for ?persistent effusion
Long-term Relapse, asymptomatic coxa magna, mild cystic
changes of femoral neck, LCP disease
Case 51y.o. M, swollen, tender R knee Seen in ED 2 weeks ago fluid taken off Last 2 weeks ↑↑pain/redness/swelling knee Using ice, ibuprofen with some relief Now fever, fatigue, nausea, myalgias
Question What would you like to do?
Labs? Imaging? Tap joint?
?Septic Arthritis?
Septic Arthritis – The Bad, The Ugly Infection effusion decreased nutrients
into jt dormant m/o resistance to abx
PMN enzymes degrade cartilage Hyaline cartilage cannot re-grow
Other structures at risk Bursae, tendons, bone
Septic Arthritis - History Joint pain, refusal to use limb
Minimal in immunocomp/steroids
Fever 40% adults, 80% kids
±Constitutional symptoms Weakness, malaise, anorexia, nausea, myalgias
Risk factors
Septic Arthritis – Physical Exam General
Fever, other vitals N ±Focus (skin, nose, ears, pharynx) ±Referred pain
Inspection Motionless limb, slight flexion Swelling, erythema
Palpation Warmth Tenderness Joint movement ++painful
Investigations Labs
Not consistently helpful ↑WBC in 50% ↑ESR in 90% +BC in 25-50% ±Culture of focus
Question What are you looking for on the x-ray?
Imaging Plain films
Effusion Bone erosions
Synovial attachment, subchondral Concurrent OM Air
Imaging Bone scan
Only if diagnostic uncertainty May risk further damage
U/S Effusion, help with aspiration
CT/MRI Better anatomy, ?used in ED
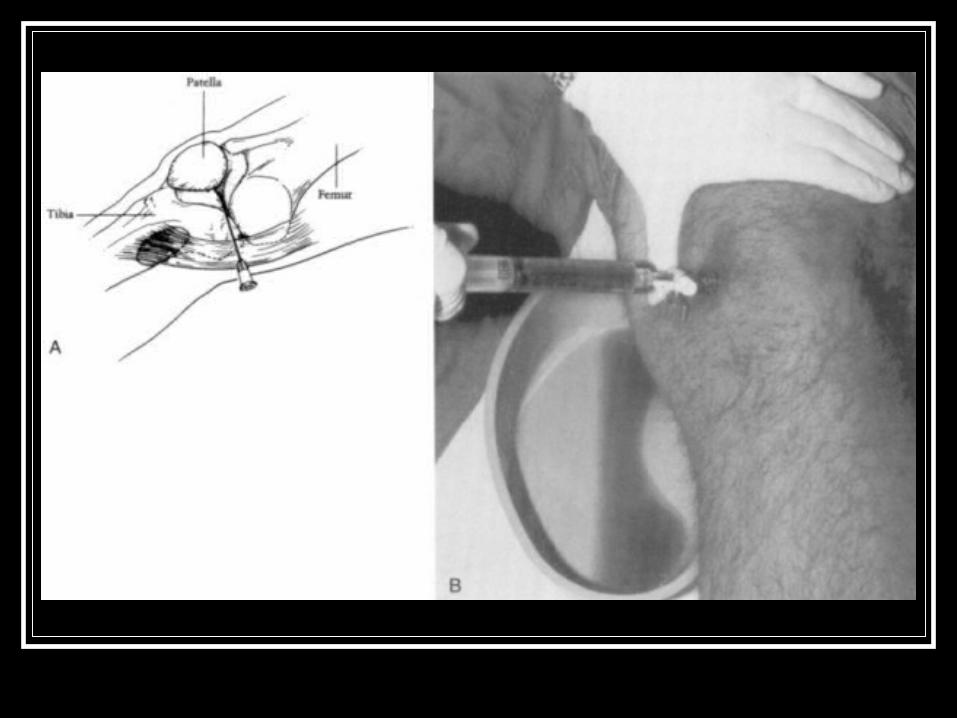
Joint Aspiration - Technique Anteromedial Approach
Position: knee in full extension or 20° flexion with towel under knee
18-ga needle, 60cc syringe Middle/superior portion of the medial patella 1 cm medial to the anteromedial patellar edge Direct needle posteriorly ±elevate patella Can milk suprapatellar pouch
Investigations Joint aspiration
Definitive test – culture Gram stain, smear Cell count/diff
WBC > 50,000 (90% have S.A.), PMN’s Fasting fluid/serum glucose < 1:2 (or ↓fluid glu) WBC < 10,000 and glucose N S.A. unlikely Priority – culture, smear, Gram stain, cell count,
glucose
Question Your labs and joint aspiration results point
you towards septic arthritis…
What would you like to do doctor?
Management Early IV antibiotics Admission Medical vs. surgical decompression
No RCT’s Animal evidence – surgical > medical Definitely surgery in:
Septic hip (esp. kids), ±shoulder Infected prosthesis
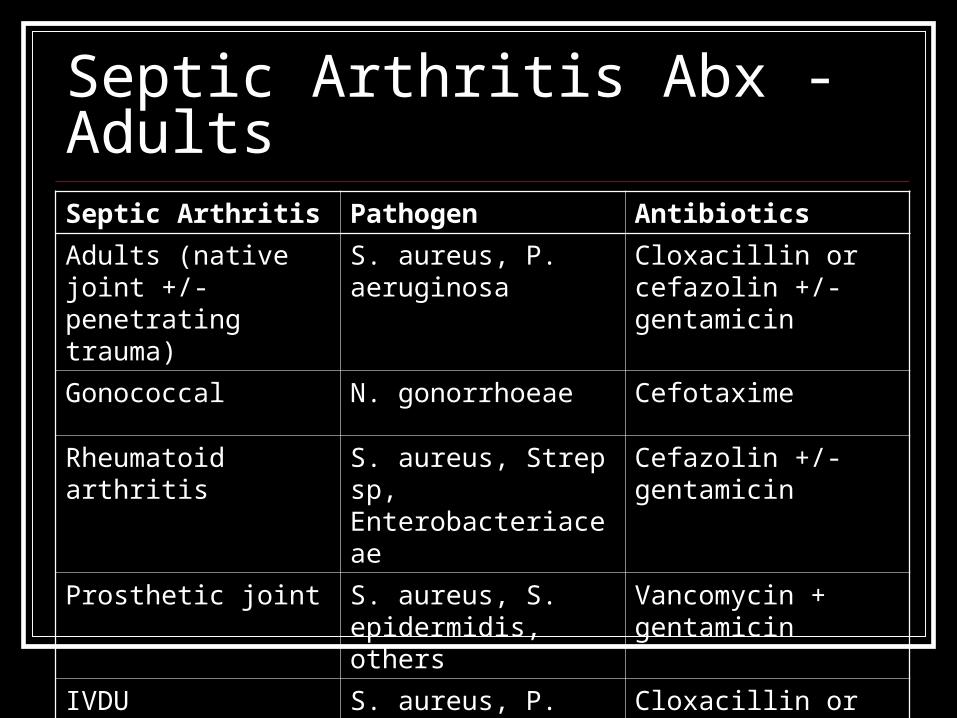
Septic Arthritis Abx - AdultsSeptic Arthritis Pathogen Antibiotics
Adults (native joint +/- penetrating trauma)
S. aureus, P. aeruginosa
Cloxacillin or cefazolin +/- gentamicin
Gonococcal N. gonorrhoeae Cefotaxime
Rheumatoid arthritis S. aureus, Strep sp, Enterobacteriaceae
Cefazolin +/- gentamicin
Prosthetic joint S. aureus, S. epidermidis, others
Vancomycin + gentamicin
IVDU S. aureus, P. aeruginosa
Cloxacillin or cefazolin +/- gentamicin
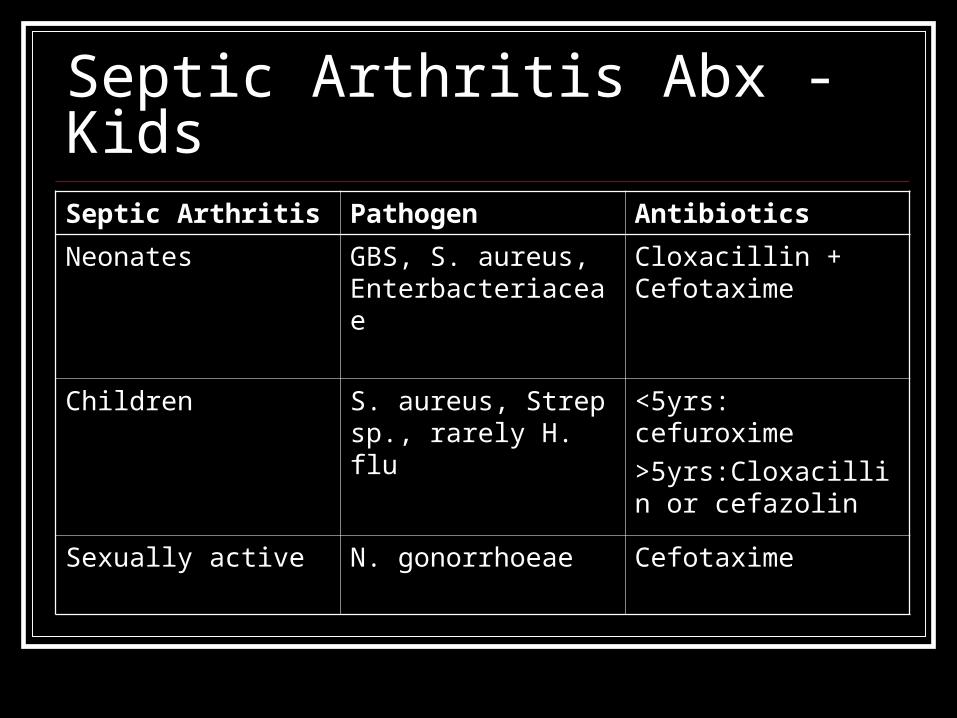
Septic Arthritis Abx - KidsSeptic Arthritis Pathogen Antibiotics
Neonates GBS, S. aureus, Enterbacteriaceae
Cloxacillin + Cefotaxime
Children S. aureus, Strep sp., rarely H. flu
<5yrs: cefuroxime
>5yrs:Cloxacillin or cefazolin
Sexually active N. gonorrhoeae Cefotaxime
Case 8y.o. F Your dx: R shoulder septic arthritis Pt being admitted, on IV abx
Mom asks: Is this going to lead to any short or long term
problems doctor?
Complications Local
Epiphyseal damage Impaired growth, length discrepancy
Tissue damage Bursae, tendons, ligaments, muscles
Ankylosis
Systemic Sepsis – elderly, immunocompromised
Question Mom says:
Wow, you seem so smart, can you tell me what my child’s chance of a full recovery is?
Prognosis Complete recovery
66% Tx initiated within 1 week of onset
Long-term complications 33% ↓mobility, ankylosis, pain, chronic infection, sepsis, death Delay in dx/tx, RA, polyarticular, +BC
Question Any questions?
References Le Saux et al. Shorter courses of parenteral antibiotic therapy do not
appear to influence response rates for children with acute hematogenous ostermyelitis: a systematic review. BMC Inf Disease. 2:16, 2002.
Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 6th ed., Copyright © 2006 Mosby, Inc.
Roberts: Clinical Procedures in Emergency Medicine, 4th ed., Copyright © 2004 Saunders, An Imprint of Elsevier
Taylor GR, Clark NM. Management of the irritable hip: A review of hospital admission policy. Arch Dis Child 71:59, 1994.