antibiotics
TRANSCRIPT

-DR.AKIF A.B

1) Erythromycin is given in intestinal hypomotility:
A Because it binds to motilin receptors
B Increases gastric acid secretion
C Improves digestion
D None

Ans. A Because it binds to motilin receptors
Macrolides a group of versatile antibiotics with motilin receptor activating property shared by all the member of the group.
Erythromycin is however most potent and is hence most commonly used for this purpose.
Erythromycin is used in diabetic gastroperesis and dyspepsia for its motilinreceptor activating activity.
Motilin receptor is a G protein coupled receptor.

-It inhibits Translocation of tRNA by acting on 50S Ribosome.
-Erythromycin
-Azithromycin
-Clarithromycin
-Telithromycin
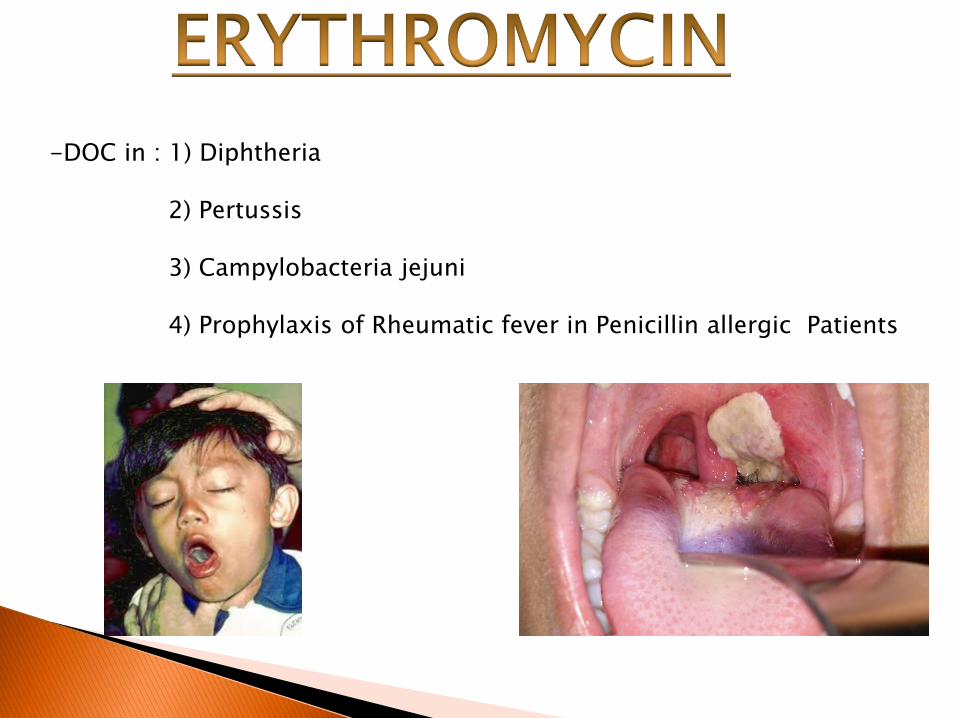
-DOC in : 1) Diphtheria
2) Pertussis
3) Campylobacteria jejuni
4) Prophylaxis of Rheumatic fever in Penicillin allergic Patients


-DOC in : 1) Legionella
2) Chancroid
3) Mycoplasma pneumoniae

M - Motilin receptors : Diarrhea
A - Allergy
C - Cholestasis
R
O
Reversible Ototoxicity

30S
50S
Tetracyclines
Aminoglycosides
Spectinomycin
Oxazolidinediones
Macrolides
Lincosamides
Chloramphenicol

2) All are true except: (DNB Dec 2011)
A Cefoperazone is antipseudomonas
B Cefoxitin has no anti anaerobic activity
C Ceftazidime is Group III cephalosporin
D Cephalosporin act by inhibiting cell wall synthesis
Ans. B cefoxitin has no anti-anerobic activity.
This is answer by exclusion.
Cephalosporin; similar to penicillins act by inhibiting the cell wall synthesis.
Ceftazidime is III generation cephalosporin which has strong anti-pseudomonal activity similar to cefoperazone.
One of the important feature of II generation compounds – some drugs like cefoxitin are having activity against the anaerobes like B. fragilis. Thus this statement is false.

Fazol (Cefazoline) is a lorry driver (Cefloridine) . He works very hard and has become thin(Cephalothin) . He has Red watch (CephRadine) and Lux soap ( CephaLexine) . He wears green Drawer (Cefodroxine)
-Main activity against Gram +ve organism and mild activity against Gram –veand anaerobes (except bacteroides)

1) Cefixime
2) Ceftriaxone
3) Ceftazidime
4) Ceftazoxime
5) Ceftibuten
6) Cefoperazone
7) Cefpodoxime
Me
One
Ten
3rd generation
Except Cefuroxime which is a 2nd
generation
-More active against Gram -ve
-Ceftoperazone and ceftazidime are active againstPseudomonas. Rest of 3rd gen. is not active.

-Cefuroxime
-Cefotetan
-Cefoxitin
-Cefmetazole
-Cefomendole
-Active against Gram –ve and anaerobesbut less active against Gram +ve
Cefipime
Cefpirome
Pi = 4th generation
Ceftibiprole
Ceftaroline
Rol = 5th generation
C - CarbepenamsColistimCiprofloxacinCephalosporins ; 3rd gen.: Ceftazidime and Cefoperazone
4th generation5th geneartion
A -Aminoglycosides
P -Penicillins : 1) Piperacillin2) Azlocillin3) Mazlocillin4) Carbenicillin5) Ticarcillin


PSEUDOMONAS

PSEUDOMONAS

3. Which cephalosporins can be used in ↓GFR
A CefuroximeB CeftriaxoneC CeftazidimeD Cefoperazone

Ans. D Cefoperazone
Cefoperazone is almost totally eliminated by bile.
Therefore, it could be used in case of reduced GFR.
Ceftrixone too can be used, but has partial elimination by bile.
Hence, if we are to choose one option between these, we shall choose cefoperazone
Cefoperazone is one of the drug of choice for pseudomonas infection.

4. Patients is given tacrolimus. The antibiotic not given is all except
A Gentamycin
B Cisplatin
C Rifampicin
D Vancomycin

Ans. C Rifampicin
Rifampin is a potent enzyme inducer.
The drug has the chance of inducing the metabolism.
This might reduce the efficacy of tacrolimus.
Rest of the drugs have nephro or ototoxicity.
Though, these too have the potential to interact with tacrolimus but with rifampin such interaction is more likely.

5. A girl on sulphonamides developed abdominal pain and presented to emergency with seizure. What is the probable cause?
A Acute intermittent porphyriaB Congenital erythropoietic porphyriaC Infectious mononucleosis D Kawasaki’s disease

Ans. A Acute intermittent porphyria
a. Acute intermittent porphyria is an autosomal dominant disorder.
b. Acute intermittent porphyria, which causes abdominal pain and neurologic symptoms, is the most common acute porphyria.
c. Sulmonamides and barbuitures are most common agents precipitating acute intermittent porphyria.
d. Acute intermittent porphyria is due to a deficiency of the enzyme porphobilinogen deaminase (also known as hydroxymethylbilane synthase) that leads to accumulation of the heme precursors delta-aminolevulinicacid and porphobilinogen initially in the liver.
f. Abdominal pain is the most common symptom, is usually steady and poorly localized, but may be cramping.

Sulfadoxine -Longest acting
- Used along with Artesunate and Pyrimethamine in ChloroquineResistant Malaria
Sulfadiazine -Used along with Pyrimethamine in Toxoplasmosis
Sulfasalazine -Used in 1) Ulcerative colitis2) Rheumatoid Arthritis
-Sulfadiazine- Silver Sulfadiazine is used in BURNS

B - Bone marrow suppression
I - Insoluble in Urine (Crystalluria)
K - Kernicterus in Newborn
A - Aplastic Anemia
S - Steven Johnson Sx
H - Hemolysis in G6PD deficient patient

Steven Johnson Sx

-Sulfamethoxazole + Trimethoprim in ratio of 5;1 in tablet
-But in circulation ratio changes to 1:20
-DOC in : 1) Nocardiosis
2) Pneumocystitis

6. CELL wall synthesis is inhibited by? (DNB Dec 2010)
A Erythromycin
B Lomefloxacin
C Cefipime
D Tetracycline

C) Cefipime
Cell wall Synthesis Inhibition
Protein synthesis Inhibition
Cell metabolism Inhibition
DNA Synthesis Inhibition
Penicillin Aminoglycosides Sulfonamides Quinolones
Cephalosporins Macrolides Trimethoprim
Vancomycin Tetracyclines
Carbapenems Linezolid
Cycloserine Chloramphenicol
Fosfomycin

7. Which of the following drug is not used for Methicillin Resistant Staph. Aureus (MRSA).?
A Cefaclor
B Cotrimoxazole
C Ciprofloxacin
D Vancomycin

Ans. A Cefaclor
Drugs used for MRSA:
VancomycinChloramphenicolLinezolidMinocyclineDoxycyclineTrimethoprim - sulfamethoxazoleFluoroquinolones

Narrow spectrumPenicillins
Wide spectrumPenicillins
Penicillin G
Penicillin V
PenicillinaseResistantPenicillins
Aminopenicillins
Carboxypeniccillins
Ureidopenicillins

-Oldest Penicillin
-It is lipid soluble drug and thus has RAPID oral absorption
-It is rapidly destructed by acid
-After parenteral administration, It is rapidly eliminated due to tubular secretions by pumps. Hence it is very short acting drug.
-To increase its duration of action, one of following are added:
1) Probenicid : It inhibits tubular pumps
2) Procaine
3) Benzathine
Makes penicillin water soluble and thus slows its release fromsite

Q. Longest Acting Penicillin
Ans. Penicillin G
-Duration of action of 28days
-Hence is a drug of choice for Prophylaxis Of Rheumatic fever given once in a month.

PENICILLIN G is DOC for following conditions
B Bacillus Anthrax
L Leptospirosis
A Actinomyces
S Streptococcus
T Treponema pallidum(Syphilis)
My Meningococcus
Penicillin Pertenue(Yaws)
G Gas gangrene
Benzathine Penicillin is used for all stages of Syphilis except NeurosyphilisWhere Aqueous Penicillin is used.

Cutaneous Anthrax Syphilis

-Acid stable
-Uses similar to Penicillin G
-It is an oral substitute of Penicillin G

ACID STABLE ACID LABILE
Oxacillin Methicillin
Dicloxacillin Nafcicillin
Cloxacillin
Given orally Given parenteral
DRUG SIDE EFFECT
Oxacillin Liver toxicity
Methicillin Interstitial Nephritis
Nafcicillin Agranulocytosis(Neutropenia)

DOC : Penicilin Penicillin Resistance
Penicillinase ResistantPenicillins
MRSADOC : Vancomycin
VRSADOC : Daptomycin

Aminopenicillins Carboxypeniciilins Ureidopenicillins
Amoxycillin Carbenicillin Mazlocillin
Ampicillin Ticarcillin Azlocillin
Piperacillin
-all have good oral absorption

MC S/E = Hypersensitivity
JARISCH HERSCHEIMER REACTION-Acute febrile reaction to Treponemal antigens released due to destruction of
Bacteria By penicillin treatment.
-C/F: 1) Fever
2) Myalgia
3) Arthralgia
4) Worsening of cutaneous lesions

8. Drug effective in pseudomonas infection is
A Piperacillin
B Amoxicillin
C Tetracycline
D Vancomycin

A Piperacillin
C - CarbepenamsColistimCiprofloxacinCephalosporins ; 3rd gen.: Ceftazidime and Cefoperazone
4th generation5th geneartion
A -Aminoglycosides
P -Penicillins : 1) Piperacillin2) Azlocillin3) Mazlocillin4) Carbenicillin5) Ticarcillin

9. All of the following are TRUE about Penicillin G EXCEPT (AIIME Nov 2009)
A Can be given orally B Main mechanism of action is cell wall synthesis inhibition C Probenecid decreases its secretion D Effective against Gram-positive bacteria

Ans. A Can be given orally
a. Antibacterial spectrum: PcG is a narrow spectrum antibiotic; activity is limited primarily to Gram-positive bacteria and few others.
b. Penicillin G is acid labile—destroyed by gastric acid. So it is not given orally
c. The pharmacokinetics of PnG is dominated by very rapid renal excretion; about 10% by glomerular filtration and the rest by tubular secretion.
d. Tubular secretion of PnG can be blocked by probenecid; higher and longer lasting plasma concentrations are achieved.
e. Penicillin act by inhibiting cell wall synthesis.
f. They are bactericidal drugs.

10. Which of the following is nephrotoxic?
A Streptomycin
B Ciprofloxacin
C Piperacillin
D Cefotaxime

Ans. A Streptomycin
Common properties of aminoglycoside antibiotics:
a. All are used as sulfate salts, which are highly water soluble; solutions are stable for months.
b. They ionize in solution; are not absorbed orally; distribute only extracellularly; do not penetrate brain or CSF.
c. All are excreted unchanged in urine by glomerular filtration.
d. All are bactericidal and more active at alkaline pH. They act by interfering with bacterial protein synthesis.
e. All are active primarily against aerobic Gram-negative bacilli and do not inhibit anaerobes.
g. They have relatively narrow margin of safety.
h. All exhibit ototoxicity and nephrotoxicity.

-Active only against Gram –ve organisms
-They require ATP and Oxygen for its function. Hence not effective againstAnaerobes (Bacteroides)
-Water soluble drugs, Hence has poor oral absorption
-Inhibits 30S Ribosomes.


DOC : Plague and Tularaemia
Used in Inhalational route for Treatment of Pseudomonas associatedWith Cystic Fibrosis

-DOC = Rifaximin
-Neomycin can also be used for it.

Auditory Toxicity Vestibulotoxic
K- Kanamycin Gentamycin
A- Amikacin Streptomycin
N - Neomycin
- In hindi ear is called as KAN
-Nephrotoxicity : Max. with Neomycin
-Neuromuscular toxicity : Max. with Neomycin
-Ototoxicity : Damage to Outer Hair Cell
-Accidental Intraocular administration of Gentamicin can cause Maculopathy.
12. Which of the following antibiotics inhibit protein synthesis?
A Doxycycline
B Nitrofurantoin
C Cephalosporin
D Penicillin

Ans. A Doxycycline
Mechanism of action of various antibiotics
a. Inhibit cell wall synthesis: Penicillin’s, Cephalosporins, Cycloserine, Vancomycin and Bacitracin.
b. Inhibit protein synthesis: Tetracyclines, Chloramphenicol, Erythromycin, Clindamycin and Linezolid.
f. 5 Inhibit DNA gyrase: Fluoroquinolones, ciprofloxacin and others.
g. Interfere with DNA function: Rifampin metronidazole.
h. Interfere with intermediary metabolism: Sulfonamides, sulfones, PAS, trimethoprim, pyrimethamine, ethambutol.

DRUGS FEATURES
Tetracyclines Resistance is being developed
Doxycycline
Demeclocyclines -Maximum Photosensitivity
-Maximum Diabetes Insipidus
Oxytetracyclines
Chlortetracyclines
Minocyclines Maximum vestibular toxicity

K - Kidney failure
A -Anti anabolic
P - Photosensitivity
I - Diabetes Insipidus
L - Liver failure
D -Pigmentation of Dentition and bone
E - Expired drugs can cause Fanconi Sx
V - Vestibulotoxicity
- C.I in pregnancy and childrens.

S - SIADH (Demeclocycline)
R - Rickketsia (DOC)
I - Inguinale Granuloma
L - LGV (DOC)
A - Atypical Pneumonia ( DOC : Macrolides)
N -None
K - Cholera (DOC)
A - Amoebiasis
- Also a DOC for Pleurodesis and Pericardiodesis

-Acts on 50S ribosome
-S/E :
1) Bone marrow suppression
2) Grey baby Syndrome



13. TRUE about the Side-effects of Tetracycline include all of the following EXCEPT
A Can cause Pseudotumor cerebriB NOT teratogenic if used during pregnancy C Discoloration of teeth may occur D Superinfection can occur

Ans. B NOT teratogenic if used during pregnancy
Adverse effects of tetracyclinea. Irritative effects: Tetracyclines can cause epigastric pain, nausea, vomiting and diarrhea by their irritant property.b. Dose related toxicityi. Liver damage: Fatty infiltration of liver and jaundice occurs occasionally.ii. Kidney damage: A reversible Fanconi syndromeiii. Phototoxicityiv. Teeth and bones: Given during late pregnancy or childhood, tetracyclinescan cause temporary suppression of bone growth. The ultimate effect on stature is mostly insignificant, but deformitiesv. and reduction in height are a possibility with prolonged use.vi. Anti anabolic effectvii. Increased intracranial pressureviii. Diabetes insipidusix. Vestibular toxicityc. Hypersensitivityd. Superinfection
14. A patient on antimicrobial therapy develops the following signs andsymptoms that ultimately are found to be drug-induced ; cough , dyspnea,
and pulmonary infiltrates ; neutropenia and bleeding tendencies; andparesthesias. Which of the following is the most likely cause of this patient’ssymptoms?
A Amoxicillin
B Azithromycin
C Ciprofloxacin
D Nitrofurantoin

Ans. D Nitrofurantoin
a. Although several of the antimicrobial agents listed here can cause one of the adverse responses noted here, nitrofurantoin is the most likely cause.b. GI side effects (anorexia, nausea, vomiting) are the most common side effects caused by this drug, which is still widely used for managing acute lower urinary tract infections (e.g., many strains of E. coli, staphylococci streptococci, Neisseria, Bacteroides).c. Acute pulmonary reactions to nitrofurantoin are an uncommon side effect of therapy and can cause minor or life-threatening pulmonary dysfunction.d. Symptoms include fever, chills, cough, pleuritic chest pain, dyspnea. Rarely, pleural effusion and/or pulmonary hemorrhage may occur.e. Diagnosis is made by clinical suspicion and exclusion of other causes of respiratory compromise. Chronic toxicity ofd drug presents as pulmonary infiltrates after an year or so of the drig treatment.f. It should promptly be discontinued. If this is not sufficient, then the condition should be treated by corticosterioids.g. The drug can also cause acute or subacute pulmonary reaction such as those described: e.g. various hematologic reactions (in particular, leukopenia and thrombocytopenia) and peripheral sensory and motor neuropathies.
-Causes Pseudomembranous Colitis
-Secreted in Bile
-Used for Anaerobic bacterial Infection
-DOC for Pseudomembranous colitis : Metronidazole > Vancomycin
-Orally not effective except in Pseudomembranous colitis
-I.V - Histamine = Red Man Sx
-S/E : Nephrotoxic
Ototoxic
-Not effective against Pseudomonas
-Uses : 1) DOC in MRSA
2) Pseudomembranous colitis

-MC cause = 3rd generation Cephalosporins > Clindamycin
-Max. risk with = Clindamycin
-MC bacteria cause = Clostridium difficile
-DOC for Pseudomembranous colitis : Metronidazole > Vancomycin
15. A patient requires an antibiotic that is most effective against P. aeruginosa.Which of the following is the quinolone of choice?
A Ciprofloxacin
B Enoxacin
C Lomefloxacin
D Norfloxacin

Ans. A Ciprofloxacin
Ciprofloxacin is highly effective against P. aeruginosa.
Others in the fluoroquinolone class have less activity toward P. aeruginosa, although they are effective against many other common gram-negative organisms.
It is a potent enzyme inhibitor and participates in several of the clinically significant drug interactions.

-DNA Gyrase Inhibitor
-Bactericidal
-Effective orally
-Wide spectrum
-Effective against MRSA and Pseudomonas
-Excreted in Kidneys except Pefloxacin and Moxifloxacin .
Hence C.I in Renal failure

DRUGS FEATURES
Norfloxacin Used in UTI
Gatifloxacin Causes Dysglycemia( Withdrwan from market)
Sparfloxacin Longest acting
Travofloxacin Hepatotoxic
Moxifloxacin -longest acting
-Safe in Renal failure
-Respiratory FQs
-Effective against Anaerobes

SIDE EFFECT FEATURE
Tendinitis Common in elderly
Nausea and Vomiting MC S/E
Pseudomembranous colitis
Cartilage defect Hence C.I in pregnancy and Children
QT Prolongation Maximum with Sparfloxacin
Photosensitivity ExceptP - PefloxacinM - MoxyfloxacinT - Trovafloxacin

Oh - Ofloxacin
My - Moxifloxacin
God - Gatifloxacin
Love - Levofloxacin

QT3
Q - Quinidine
T - Thioridazine
T - TCAs
3 - Class 3 AntiArrhythmics ; Amiodarone/ Procainamide/Diisopyramide
1) Polymyxin- B
2) Polymyxin – E (Colistin)
3) Daptomycin : DOC for VRSA

Minimum Inhibitory Concentration
Lowest concentration of drug which inhibits visible growth after 24hrs of Incubation.
Time dependent Killing(TDK)
Effects persist only for the time for which concentration of drug is above MIC.Hence has short Post antibiotic effect
Beta lactams
Vancomycin
Concentration dependent killing (CDK)
It depends only on concentration but not on MIC.So effect is seen even after drug concentration is below MIC.Hence it has prolonged post antibiotic effect.
Fluoroquinolones
Aminoglycosides
Both CDK & TDK Beta lactamsFQsAminoglycosidesMacrolides

17) Streptomycin and other aminoglycosides inhibit bacterial protein synthesis by binding to which of the following?
A 30S ribosomal particles B DNA C mRNA D RNA polymerase

Ans. A 30S ribosomal particles
a. The bactericidal activity of streptomycin and other aminoglycosidesinvolves a direct action on the 30S ribosomal subunit, the site at which these agents both inhibit protein synthesis and diminish the accuracy of translation of the genetic code.
b. Proteins containing improper sequences of amino acids (known as nonsense proteins) are often nonfunctional. Streptomycin is used in treatment rhinoscleroma, pelvic inflmmatory diseases, brucella and resistant tuberlosis.

19. Which of the following drugs is primarily used in pneumonia caused by P. carcinii? (AIIMS May 2010)
A CarbenicillinB MetronidazoleC NifurtimoxD Pentamidine

Ans. D Pentamidine
Both trimethoprim-sulfamethoxazole and pentamidine are effective in pneumonia caused by P carinii. This protozoal disease usually occurs in immunodeficient patients, such as those with AIDS.
Nifurtimox is effective in trypanosomiasis and metronidazole in amebiasisand leishmaniasis, as well as in anaerobic bacterial infections.
Penicillins are not considered drugs of choice for this particular disease state.
21. Compared with most other cephalosporins, the administration of cefoperazone, or cefotetan is associated with a higher incidence of which of the following? (AIPG 2009)
A Acute heart failure B Acute renal failure C Bleeding tendencies in patients taking warfarinD Hypertension

Ans. C Bleeding tendencies in patients taking warfarin
a. Cefmetazole and cefotetan, both second-generation cephalosporins, and cefoperazone (third generation) can interfere with hepatic vitamin K metabolism, leading to what amounts to a deficiency ot vitamin K-dependent clotting factor activity.b. Because this is the general mechanism by which warfarin exerts its anticoagulant effects, combined use of one of these cephalosporins can cause further (and potentially dangerous) prolongations of the International Normalized Ratio (or prothrombin time); the clinical consequence can be spontaneous, prolonged, or excessive bleeding.c. One should also be cautious when these cephalosporins are given to patients taking aspirin or other antiplatelet drugs (e.g., clopidogrel) or thrombolytics.d. Although most cephalosporins are excreted unchanged by the kidneys, renal failure (especially severe and acute) seldom occurs with these or other cephalosporins.

22. The Amikacin differs from gentamicin mainly in that it: (AIIME Nov 2012)
A Does not require monitoring of blood levels during therapy B Exerts significant bactericidal effects against anaerobes too C Has broadest spectrum against gram-negative bacilli D Lacks ototoxic potential

Ans. C Has broadest spectrum against gram-negative bacilli
a. Amikacin stands out among all the aminoglycosides in two main ways: it has the broadest spectrum against gram-negative bacilli, and it is least susceptible to bacterial enzymes that inactivate aminoglycosides and lead to resistance.

23. Resistance to Methicillin in the microorganism given in picture is due to
A. Beta lactamase
B. Efflux
C. Altered Penicillin binding protein
D. Mec A gene

C) Altered Penicillin binding protein
-Grape like clusters in gram stain is due to Staphylococcus aureus,in which resistance is seen due to Penicillinase production
-But in Penicillinase Resistant penicillin like Methicillin , Resistance is due to Altered penicillin binding protein.

24. DOC for the given condition is
A. Ceftriaxone
B. Piperacillin
C. Carbapenems
D. Ceftazidime
D. Ceftazidime
-This condition is known as Green Nail Syndrome caused By Pseudomonas
- DOC ; Ceftazidime

Q. DOC for condition given below
A.DoxycyclineB.GentamycinC.ErythromycinD.Penicillin G

Ans. C) Erythromycin
-This is Diphtheria
-DOC for Diphtheria is : Erythromycin

NEMATODES DRUG OF CHOICE
Round worm Albendazole
Hook worm Albendazole
Whipworm Albendazole
Trichinella spiralis Albendazole
Enterobius vermicularis Albendazole
Dracunculiasis Albendazole
Threadworm Ivermectin
Onchocerca volvulus Ivermectin
Filariasis DEC
Loa loa DEC

CESTODES DRUG OF CHOICE
Neurocysticercosis Albendazole
Echinococcus Albendazole
T.Solium Praziquantel > Niclosamide
T.Saginata Praziquantel > Niclosamide
Hymenolepsis nana Praziquantel > Niclosamide
Diphylobothrium latum Praziquantel > Niclosamide

TREMATODES DRUG OF CHOICE
Liver fluke Triclabendazole
Lung fluke Praziquantel
Schistosoma Praziquantel

Cutaneous Leishmaniasis Visceral Leishmaniasis( Kala Azar)
Sodium stibogluconate(DOC)
Amphotericin B (DOC)
Amphotericin B Miltefosine
Paromomycin Sodium stibogluconate
Pentamidine Pentamidine
Paromomycin
Sitamaquine

TRYPANOSOMIASIS
LATEEFLORNITHINE
BENZNIDAZOLE (DOC)
EARLYPENTAMIDINE
LATEMelarsoprol
EARLYSURAMIN
WESTEAST
AMERICAN(CHAGAS DISEASE)
AFRICAN SLEEPING SICKNESS

VREDaptomycin (DOC)
Vancomycin (DOC)
Ampicillin (DOC)
FaeciumFaecalis
ENTEROCOCCUS
Vancomycin (DOC)
