ajcc 7 th edition of gastric cancer: good enough? deon chong north district hospital
TRANSCRIPT
AJCC 7th Edition of Gastric Cancer:good enough?
Deon ChongNorth District Hospital

Ideal cancer staging - Aim
• Treatment planning• Assessing prognosis• Stratifying patients for therapeutic studies• Evaluating the results of treatment• Facilitating communication
Ideal cancer staging - Aim
• Treatment planning• Assessing prognosis• Stratifying patients for therapeutic studies• Evaluating the results of treatment• Facilitating communication

TNM Staging - History
1943-1952
TNM
Pierre Denoix UICC
1968
1st Ed TNM
1987
4th Ed TNM
UICC + AJCC
1974 1978
2nd EdTNM
3rd EdTNM
2009
7th EdTNM
5th,6th Ed
Does the 7th Ed for gastric cancer meet the aim of staging?

Outline
• Changes in AJCC 7th Ed for gastric cancer:– T stage– N stage– M stage
Meet the aim?

Outline
• Changes in AJCC 7th Ed for gastric cancer:– T stage– N stage– M stage
Meet the aim?

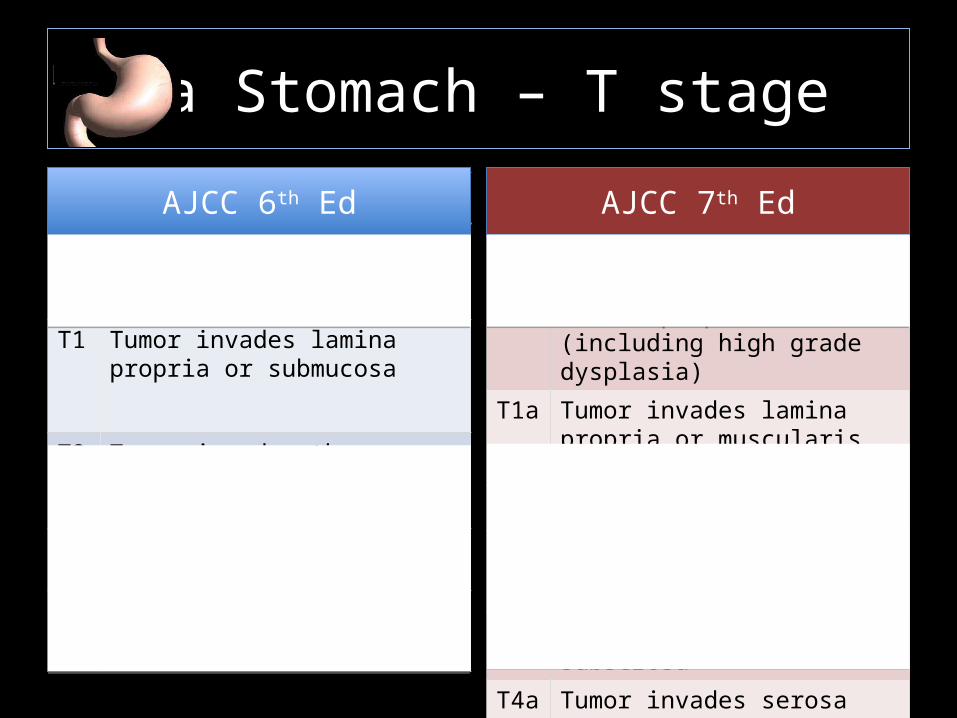
Ca Stomach – T stage
Tis Intraepithelial tumor without invasion of the lamina propria
T1 Tumor invades lamina propria or submucosa
T2 Tumor invades the muscularis propria or subserosa
T3 Tumor invades serosa
T4 Tumor invades adjacent strutures
AJCC 6th Ed
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria
T3 Tumor penetrates the subserosa
T4a Tumor invades serosa
T4b Tumor invades adjacent stuctures
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed

Ca Stomach – T stage
Tis Intraepithelial tumor without invasion of the lamina propria
T1 Tumor invades lamina propria or submucosa
T2 Tumor invades the muscularis propria or subserosa
T3 Tumor invades serosa
T4 Tumor invades adjacent strutures
AJCC 6th Ed
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria
T3 Tumor penetrates the subserosa
T4a Tumor invades serosa
T4b Tumor invades adjacent stuctures
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed
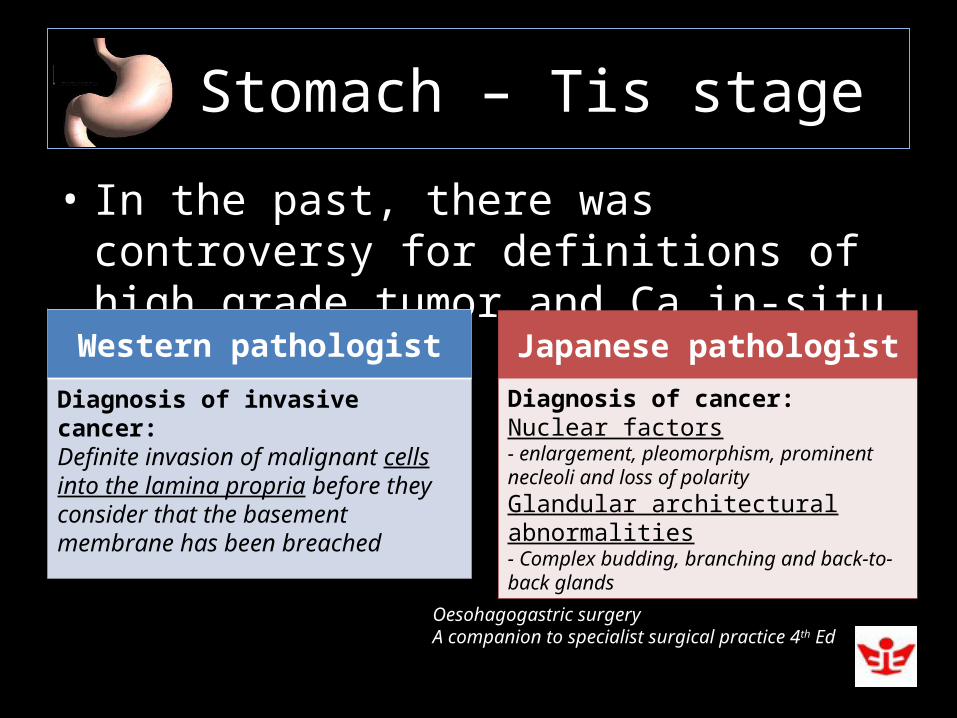
Ca Stomach – Tis stage
• In the past, there was controversy for definitions of high grade tumor and Ca in-situ
Western pathologist
Diagnosis of invasive cancer:Definite invasion of malignant cells into the lamina propria before they consider that the basement membrane has been breached
Japanese pathologist
Diagnosis of cancer:Nuclear factors- enlargement, pleomorphism, prominent necleoli and loss of polarityGlandular architectural abnormalities- Complex budding, branching and back-to-back glands
Oesohagogastric surgeryA companion to specialist surgical practice 4th Ed

Ca Stomach – Tis stage
• Consensus conferences:- Vienna classification
Category 1Negative for neoplasia/dysplasiaCategory 2Indefinite for neoplasia/dysplasiaCategory 3Non invasive neoplasia, low gradeCategory 4Non-invasive neoplasia, high grade4.1 High grade adenoma/dysplasia4.2 Non-invasive carcinoma (carcinoma in situ)4.3 Suspicious for invasive carcinomaCategory 5Invasive neoplasia5.1 Intramucosal carcinoma5.2 submucosal carcinoma
Category 1Negative for neoplasia/dysplasiaCategory 2Indefinite for neoplasia/dysplasiaCategory 3Non invasive neoplasia, low gradeCategory 4Non-invasive neoplasia, high grade4.1 High grade adenoma/dysplasia4.2 Non-invasive carcinoma (carcinoma in situ)4.3 Suspicious for invasive carcinomaCategory 5Invasive neoplasia5.1 Intramucosal carcinoma5.2 submucosal carcinoma Gut 2000;47:251-5

Ca Stomach – Tis stage
• This new Tis staging solves the controversy • Implies a less conservative management
towards high grade dysplasia
Ca Stomach – T stage
Tis Intraepithelial tumor without invasion of the lamina propria
T1 Tumor invades lamina propria or submucosa
T2 Tumor invades the muscularis propria or subserosa
T3 Tumor invades serosa
T4 Tumor invades adjacent strutures
AJCC 6th Ed
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria
T3 Tumor penetrates the subserosa
T4a Tumor invades serosa
T4b Tumor invades adjacent stuctures
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed

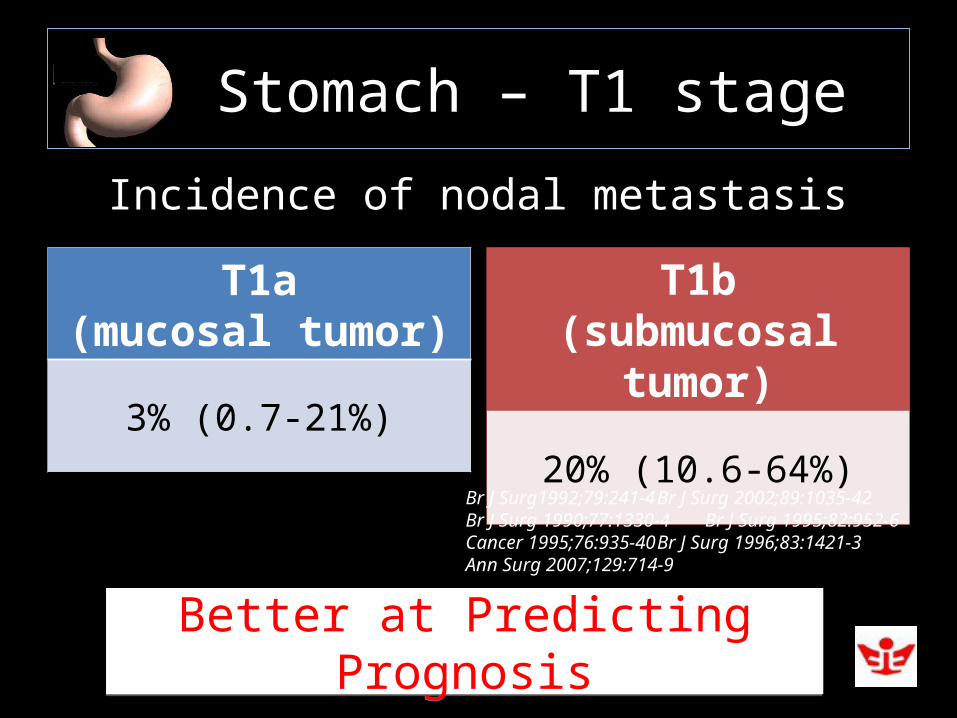
Ca Stomach – T1 stage
T1a(mucosal tumor)
3% (0.7-21%)
T1b(submucosal tumor)
20% (10.6-64%)
Incidence of nodal metastasis
Br J Surg1992;79:241-4 Br J Surg 2002;89:1035-42Br J Surg 1990;77:1330-4 Br J Surg 1995;82:952-6Cancer 1995;76:935-40 Br J Surg 1996;83:1421-3Ann Surg 2007;129:714-9
Ca Stomach – T1 stage
T1a(mucosal tumor)
3% (0.7-21%)
T1b(submucosal tumor)
20% (10.6-64%)
Incidence of nodal metastasis
Br J Surg1992;79:241-4 Br J Surg 2002;89:1035-42Br J Surg 1990;77:1330-4 Br J Surg 1995;82:952-6Cancer 1995;76:935-40 Br J Surg 1996;83:1421-3Ann Surg 2007;129:714-9
Better at Predicting PrognosisBetter at Predicting Prognosis

Ca Stomach – T1 stage
• Recent advances in EMR and ESD:
Suitable tumor:Elevated or flat lesions <2cm sizeDepressed lesions <1cm without ulcerationMucosal invasionWell differentiated No lymphatic permeation
Suitable tumor:Elevated or flat lesions <2cm sizeDepressed lesions <1cm without ulcerationMucosal invasionWell differentiated No lymphatic permeation
Oesohagogastric surgeryA companion to specialist surgical practice 4th Ed

Ca Stomach – T1 stage
• Recent advances in EMR and ESD:
Suitable tumor:Elevated or flat lesions <2cm sizeDepressed lesions <1cm without ulcerationMucosal invasionWell differentiated No lymphatic permeation
Suitable tumor:Elevated or flat lesions <2cm sizeDepressed lesions <1cm without ulcerationMucosal invasionWell differentiated No lymphatic permeation
Guide Our Treatment PlanGuide Our Treatment Plan

Ca Stomach – T stage
Tis Intraepithelial tumor without invasion of the lamina propria
T1 Tumor invades lamina propria or submucosa
T2 Tumor invades the muscularis propria or subserosa
T3 Tumor invades serosa
T4 Tumor invades adjacent strutures
AJCC 6th Ed
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria
T3 Tumor penetrates the subserosa
T4a Tumor invades serosa
T4b Tumor invades adjacent stuctures
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed

Ca Stomach – T2-4 stage
• Depth of tumor invasion is one of the most important predictors for prognosis
Ann Surg 1998;228:449-61Surg Gynrcol Obstet 1986;162(3):229-34Lancet 2003;362:305-15Ann Surg 2005;241:27-39

Ca Stomach – T2-4 stage
• Serosal invasion correlates with early recurrence and short survival period
• Transcoelomic dissemination and direct infiltration of adjacent structures may occur as a result of serosal involvement
Cancer 1992;70:1030-7Cancer 2000;89:255-61Cancer 1996;77:2445-8
Br J Surg 1990;77:436-9

Ca Stomach – T stage
T2 Tumor invades the muscularis propria or subserosa
T3 Tumor invades serosa
T4 Tumor invades adjacent strutures
AJCC 6th Ed
T2 Tumor invades the muscularis propria
T3 Tumor penetrates the subserosa
T4a Tumor invades serosa
T4b
Tumor invades adjacent stuctures
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed
Better at Predicting PrognosisBetter at Predicting Prognosis

Ca Stomach – T stage
The new T staging is better stratified to predict prognosis and guide our treatment
The new T staging is better stratified to predict prognosis and guide our treatment

Outline
• Changes in AJCC 7th Ed for gastric cancer:– T stage– N stage– M stage
Meet the aim?

Ca Stomach – N stage
• LN status is the most important prognostic indicator
Berlin: Springer.1995,47-64Ann Surg 1998;228:449-61

Ca Stomach – N stage
• N stage of 4th Ed of AJCC was based on anatomical location of the involved LN, according to the Japanese Classification of Gastric Cancer (JCGC)

Ca Stomach – N stage
• Japanese believe that tumor growth inside the regional LN could reflect tumor aggressiveness
Ann Surg Oncol 2000;7:750-7


NOT SIMPLENOT SIMPLE

NOT EASILY REPRODUCIBLENOT EASILY REPRODUCIBLE

Ca Stomach – N stage
• NOT EASILY REPRODUCIBLE:For Surgeons
D2/3 lymphadenectomy should be performed in order to complete the nodal stagingD2/3 lymphadenectomy should be performed in order to complete the nodal staging

Ca Stomach – N stage
• NOT EASILY REPRODUCIBLE:For Pathologist
Assessment of the distance to edge of primary tumor may be variable due to shrinking of the tumor free gastric wall after resection and formalin fixation
Assessment of the distance to edge of primary tumor may be variable due to shrinking of the tumor free gastric wall after resection and formalin fixation

Ca Stomach – N stage
• In 1997, UICC/AJCC used the number of met LN in N staging for a more uniform and comparable system for western and Japanese
5th Ed AJCC Staging5th Ed AJCC Staging

Ca Stomach – N stage
• 5th AJCC N staging was more simple, reproducible and sensitive in the prognostic evaluation than the JCGC N staging
Cancer 2000;88:1796-800Br J Surg 1994;81:414-4Surg Gynecol Obstet 1990;170:488-94Ai Zheng 2005;24:596-9Arch Surg 1992;127:290-4
Retained in 6th EdRetained in 6th Ed

Ca Stomach – N stage
• 5th/6th Ed N staging was criticized for inappropriate cut-off of the N number, especially in N1, for homogeneity and prediction of prognosis
Ann Surg Oncol 2009;16:61-7J Surg Oncol 2006;94:274-80Dig Surg 2003;20:148-53Gut 1996;38:525-7J Clin Oncol 1993;11:1894-900Chin Med J 2007;120:2268-70

Ca Stomach – N stage
Nx Regional LN cannot be assessed
N0 No regional LN mets
N1 Mets in 1-6 regional LN
N2 Mets in 7-15 regional LN
N3 Mets in >15 regional LN
AJCC 6th Ed
Nx Regional LN cannot be assessed
N0 No regional LN mets
N1 Mets in 1-2 regional LN
N2 Mets in 3-6 regional LN
N3a Mets in 7-15 regional LN
N3b Mets in ≥ 16 regional LN
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed

• Univariate analysis: 7th Ed N stage, 5th/6th Ed N stage and JCGC N stage were associated with overall survival
• Multivariate analysis, only 7th Ed N stage is an independent factor
• Using case control matched fashion, 7th Ed N stage is also superior in prognostic prediction

Ca Stomach – N stage
• 7th Ed N stage still has the same limitation as in 5th/6th Ed
Stage MigrationStage Migration

Ca Stomach – N stage
• 7th Ed N stage still has the same limitation as in 5th/6th Ed
Stage MigrationStage Migration
Instances in which evaluation of an inadequate number of LN leads to understaging and subsequent underestimation of disease severity
Ca Stomach – N stage
• 7th Ed N stage still has the same limitation as in 5th/6th Ed
Stage MigrationStage Migration
Observed in about 10-15% of cases, especially in less extensive lymphadenctomy
Ann Surg Oncol 2002;9:775-84Ann Surg Oncol 2003;10:1077-85J Clin Oncol 1995;13:19-25N Engl J Med 1985;312:1604-8Arch Surg 1988;123:1023-4

Ca Stomach – N stage
• 7th Ed N stage still has the same limitation as in 5th/6th Ed
Stage MigrationStage Migration
In an analysis of US SEER data from 1973-1999, the median number of LN examined was 8 and <25% of patients had ≥15 nodes examined
J Clin Oncol 2005;23:7114-24

Ca Stomach – N stage
• 7th Ed N stage still has the same limitation as in 5th/6th Ed
Stage MigrationStage Migration
Mets LN RatioMets LN Ratio

Ca Stomach – N stage
• LN ratio:- number of positive LN over the number of examined LN

Ca Stomach – N stage
• LN ratio is minimally influenced by:- the extent of the lymphadenectomy - the pathologist’s accuracy in looking for an adequate number of nodes
BMC Cancer 2007;7:200J Clin Oncol 1995;13:19-25Cancer 1999;86:553-8Cancer 1998;82:621-31Br J Surg 1991;78:825-7

Ca Stomach – N stage

Ca Stomach – N stage
D2 or D3D2 or D3

Ca Stomach – N stage
• Limitations of LN ratio:- cut off of LN ratio intervals- present studies compared with 5th/6th Ed
Future studies requiredFuture studies required

Ca Stomach – N stage
The new N staging is better than 6th Ed in prognosis prediction but controversy is
still present
The new N staging is better than 6th Ed in prognosis prediction but controversy is
still present

Outline
• Changes in AJCC 7th Ed for gastric cancer:– T stage– N stage– M stage
Meet the aim?

Ca Stomach – M stage
Mx Distant mets cannot be assessed
M0 No distant mets
M1 Distant mets- Non regional or distant LN- Peritoneal surfaces- Other organs
AJCC 6th Ed
M0 No distant mets
M1 Distant mets- Positive peritoneal cytology- Non regional or distant LN- Peritoneal surfaces- Other organs
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed

Ca Stomach – M stage
Mx Distant mets cannot be assessed
M0 No distant mets
M1 Distant mets- Non regional or distant LN- Peritoneal surfaces- Other organs
AJCC 6th Ed
M0 No distant mets
M1 Distant mets- Positive peritoneal cytology- Non regional or distant LN- Peritoneal surfaces- Other organs
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed
Ca Stomach – M stage
• Mx is deleted in 7th Ed- Lack of information about metastatic status is considered inappropriate

Ca Stomach – M stage
• Use of Mx could jeopardize:- results of apparently curative surgery- reliability of evaluation of response after neoadjuvant/adjuvant therapy- reliability of follow-up programs
Ann Surg Oncol 2010 Sept 29

Ca Stomach – M stage
Mx Distant mets cannot be assessed
M0 No distant mets
M1 Distant mets- Non regional or distant LN- Peritoneal surfaces- Other organs
AJCC 6th Ed
M0 No distant mets
M1 Distant mets- Positive peritoneal cytology- Non regional or distant LN- Peritoneal surfaces- Other organs
AJCC 6th EdAJCC 6th Ed AJCC 7th EdAJCC 7th Ed

Ca Stomach – M stage
• Prognosis of patients with positive peritoneal cytology is very poor:- 5 year survival rate is less than 5%
Hepatoenterol 2001;48:892-4J Surg Oncol 2009;99:324-8Ann Surg Oncol 2001;8:215-21
Better at Predicting PrognosisBetter at Predicting Prognosis

Ca Stomach – M stage
• Imply the systematic use of staging laparoscopy + evaluation of peritoneal lavage fluid?
Alter Our Staging Process?Alter Our Staging Process?
Ca Stomach – M stage
The new M staging is better in predicting prognosis and possibly alter our staging process
The new M staging is better in predicting prognosis and possibly alter our staging process

AJCC 7th Edition of Gastric Cancer:good enough?
Conclusion:• This new TNM Staging is superior in assessing prognosis. • T stage guides our treatment and the M stage may alter our staging process. • N stage still remains controversial.


THE END
OGJ Tumor
• In AJCC 6th Ed: No clear statement on whether we should stage OGJ tumor as Ca eso or ca stomach- ie: it could be staged as either Ca eso or Ca stomach- since the N stages were different, the prognostic groupings were different
• In AJCC 7th Ed: It is now staged under Ca eso- harmonised!
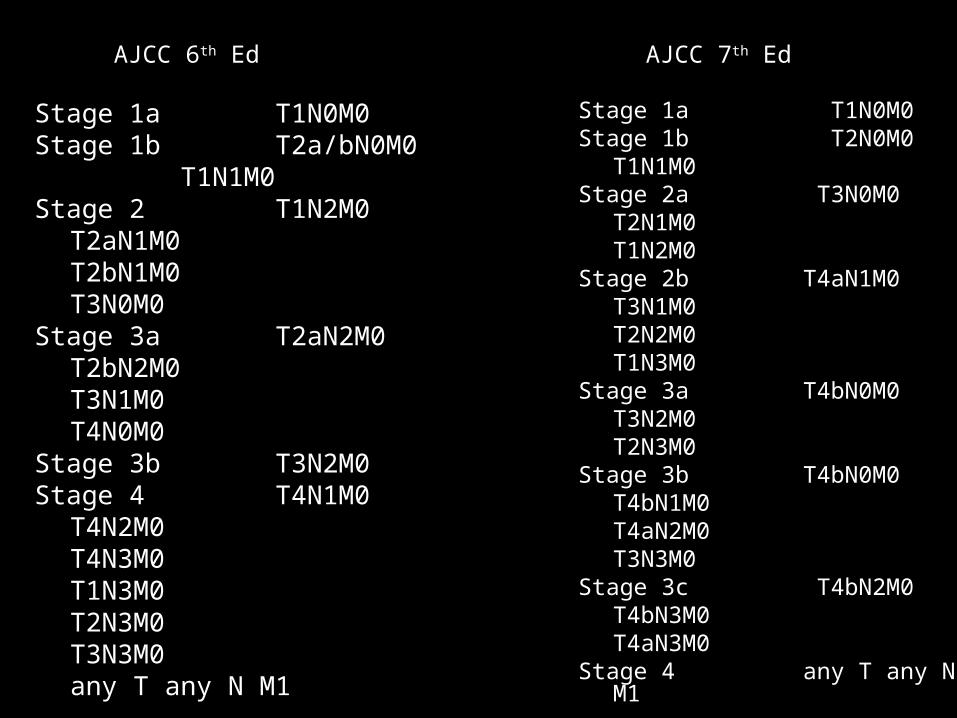
Stage 1a T1N0M0Stage 1b T2a/bN0M0
T1N1M0Stage 2 T1N2M0
T2aN1M0T2bN1M0T3N0M0
Stage 3a T2aN2M0T2bN2M0T3N1M0T4N0M0
Stage 3b T3N2M0Stage 4 T4N1M0
T4N2M0T4N3M0T1N3M0T2N3M0T3N3M0any T any N M1
Stage 1a T1N0M0Stage 1b T2N0M0
T1N1M0Stage 2a T3N0M0
T2N1M0T1N2M0
Stage 2b T4aN1M0T3N1M0T2N2M0T1N3M0
Stage 3a T4bN0M0T3N2M0T2N3M0
Stage 3b T4bN0M0T4bN1M0T4aN2M0T3N3M0
Stage 3c T4bN2M0T4bN3M0T4aN3M0
Stage 4 any T any N M1
AJCC 6th Ed AJCC 7th Ed