5 february 2011 interns hour. general data 2 month old male calamba, laguna born term via lt cs,...
TRANSCRIPT
5 FEBRUARY 2011
Interns Hour

General Data
2 month old maleCalamba, LagunaBorn term via LT CS, twin pregnancy

Chief complaint
Right scrotal mass

History of Present Illness
At 3 weeks of age – noted to have a right inguinal mass, prominent when patient is crying. Mass is reducible when patient is relaxed. No changes in bowel movement, no abdominal distention, no diifficulty urinating. Patient had good suck and activity.
Consult was done at a local hospital and was advised surgery once the patient is older.
At 2 months of age – persistence of above symptoms with noted extension of the mass to the scrotal area. Mass was reducible when palpated. No tenderness, no changes in color noted. No changes in bowel movement, no difficulty urinating, no abdominal distention. Patient had good appetite.

Few hours prior to consult, patient was noted to be crying. Scrotal mass was noted to be enlarged with deviation of the penis to the left side. Noted tenderness. No discoloration noted. No vomiting, no changes in bowel movement, no difficulty urinating. Patient was noted to have poor appetite. Patient was immediately brought to PGH. Hence consult.

Review of systems
• (-) fever, weight loss• (+) rashes, inguinal area, (-) jaundice, pallor• (-) eye pain/discharge, (-) nasoaural discharge• (-) dyspnea, hemoptysis• (-) cyanosis• (-) abdominal pain, diarrhea/constipation• (-) dysuria, hematuria, nocturia• (-) seizures
Prenatal History
Born to a 25 year old motherNo known maternal illnessNo intake of medicationsRegular monthly prenatal check-up at (6x)
LHC

Birth History
Born term via LTCS due to twin pregnancy at St. John Hospital
No known fetomaternal complicationsGood suck, good cry and goo activity

Feeding history
Breastfed up to 1 month of ageStarted drinking formula milk at 1 month of
age (2 cups/ 80ml bottle) Feeds ~8 times a dayNo food preferences

Developmental History
Social smile at 1 month of age

Past Medical History
(+) vaccinations: DPT1, Hepa B1, BCG, OPV1No known illnessesNo allergies to food/drugs

Family Medical History
(+) heart disease(+) similar inguinal mass – twin sibling(-) hypertension(-) PTB(-) Diabetes(-) Bronchial asthma

Personal/Social History
Eldest of twinsLives with parents and grandparents in
bungalow type of house with 2 bedrooms and 1 comfort room
PHYSICAL EXAMINATION

Vital Signs & Anthropometric Measurements
Vital Signs Measures
Heart Rate136 bpm
Length 58 cm
Respiratory Rate
34 cpm Weight 5.41 kg
Temperature 36.8Head
Circumference
37 cm
Abdominal Circumferen
ce37 cm
Chest Circumferen
ce39 cm

Physical Findings

Physical Findings

Primary Working Impression
Inguinoscrotal hernia, incarcerated

Differential DIAGNOSIS

Differential Diagnosis
Findings
Hydrocele (communicating)
Cystic swellingIncrease in size when upright or when intra-abdominal pressure increasesUsually congenitalTransilluminates
Hydrocele (noncommunicatin
g)
Cystic swellingDoes not change in size with changes in position of intra-abdominal pressureOften a simultaneous scrotal abnormality (eg, tumor, epididymitis)Transilluminates
Spermatocele Cystic mass at the upper pole of the testis, adjacent to epididymisTransilluminates

Differential Diagnosis
Findings
Inguinal hernia
Increases in size when upright or when intra-abdominal pressure increasesMay disappear when recumbent or be reducible or compressiblePossibly bowel soundsAbsence of normal spermatic cord structures above the massPossibly palpable in the inguinal canal
Varicocele Palpable when standing, feeling like a bag of wormsUsually on left sidePossibly pain and fullness when standingPossibly testicular atrophy
Hematocele Tender swellingRisk factors (eg, trauma, surgery, bleeding disorder or use of anticoagulants)
Testicular cancer
Mass attached to or part of testisIs solid or does not transilluminatePossibly dull, aching pain or acute pain due to hemorrhage

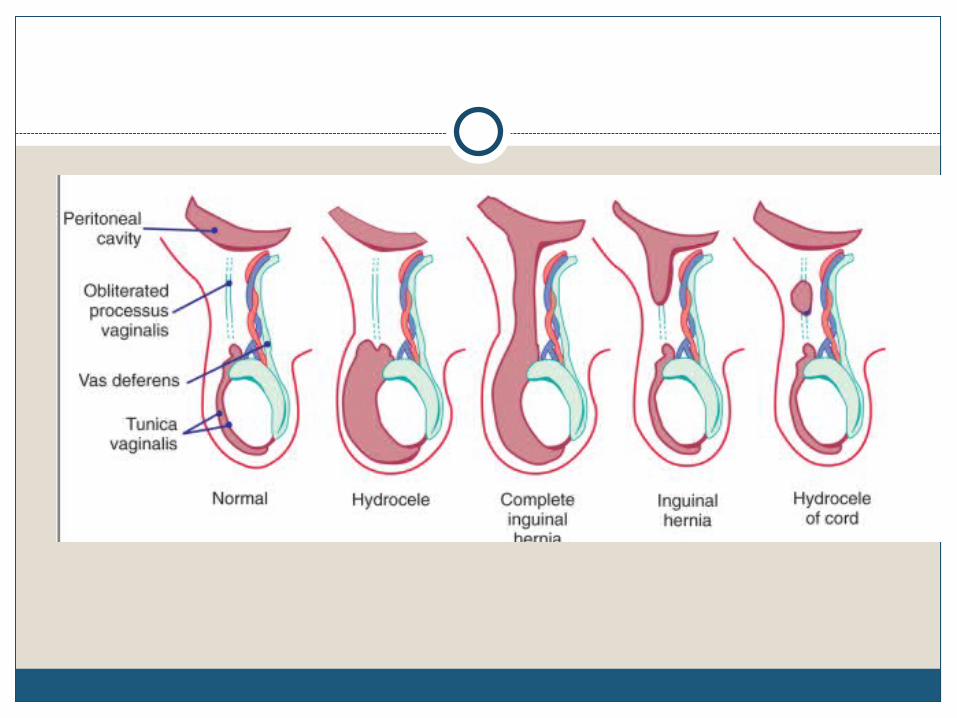
Hydrocele
accumulation of fluid within the tunica vaginalis
nontendertransilluminates

Hernia
indirect inguinal hernia
Bulge that appears on straining
Bowel sounds may be heard over the hernia
(-) transillumination test

Hematocele
Blood in the tunica vaginalis
Swelling resembles a hydrocele
(-) transillumination test
(+) history of trauma

Spermatocele
painless fluid-filled sac with sperm that is often located above and posterior to the testicle
(+) transillumination test

Inguinal Hernias

Inguinal Hernias
Usually indirect (99%)High incidence in premature infants (30%)Risk for incarceration and strangulation
highest in the 1st year of life (30-40%)
Inguinal hernias
Intra-abdominal contents enter the inguinal region through the patent processus vaginalis
Usually congenital, due to a patent processus vaginalis
Twice as common on the right side

Predisposing Factors
PREMATURITY UROGENITAL Cryptorchidism Exstrophy of the bladder
or cloaca Ambiguous genitalia Hypospadius/epispadius
INCREASED PERITONEAL FLUID
Ascites Ventriculoperitoneal
shunt Peritoneal dialysis
catheter
INCREASED INTRA-ABDOMINAL PRESSURE
Repair of abdominal wall defects
Severe ascites (chylous) Meconium peritonitis CHRONIC RESPIRATORY
DISEASE Cystic fibrosis CONNECTIVE TISSUE
DISORDERS Ehlers-Danlos syndrome Hunter-Hurler syndrome Marfan syndrome Mucopolysaccharidosis

bulge in the inguinal region or extending through the inguinal region into the scrotum or in the upper portion of the labia majora.
most visible at times of irritability or increased intra-abdominal pressure
smooth, firm mass that emerges through the external inguinal ring lateral to the pubic tubercle and enlarges with increased intra-abdominal pressure
“silk glove sign” as the layers of the hernia sac (processus vaginalis) slide over the spermatic cord structures

Incarcerated hernia cannot be reduced into the abdominal cavity small bowel, appendix, omentum, colon, Meckel
diverticulum ovary, fallopian tube irritability, pain in the groin and abdomen, abdominal
distention, and vomiting
Strangulated hernia hernia contents have become ischemic or gangrenous






MANAGEMENT

DIAGNOSTICS

DAIGNOSTIC STRATEGIES
diagnosis of IH in an overwhelming majority of cases is clinical history and examination
If diagnosis cannot be made immediately, the child needs to be re-examined over a period of time to make a definitive diagnosis

Comparative Sp and Sn
TechniqueSensitivi
tySpecificit
y
Physical Exam 74.5 96.3
Ultrasound 92.7 81.5
MRI 94.5 86.3

IMAGING TECHNIQUES
imaging studies are generally not indicatedUltrasonography- can confirm IH in selected
patients not the gold standard for diagnosing IH in children

Gold Standard
Laparoscopy - considered the final means of determining the true groin pathology

Pre-Operation Labs
Complete blood count with differential countblood urea, creatinine, serum electrolytes -
helpful in cases of strangulation and obstruction

Available Labs
Ultrasound: Both testicles are normal with fine homegenous
echogencity, epididymis not dilated No fluid collection in scrotal sac, no mass density
demonstrated Omental structures seen in widened left inguinal
canal with descent upon valsalva

Available Labs
Blood Typing: B PositiveComplete Blood Count
Hemoglobin 107 Hematocrit 0.333
Platelet 443 WBC 15.93
Neutrophils 0.185 Lymphocytes
0.653
Monocyte 0.130 Eosinophils 0.029
Basophils 0.003
Electrolytes Na 142 K 4.4 Cl 102
BUN 5.4 CREA 37

SURGICAL MANAGEMENT


MANAGEMENT
Inguinal hernias do not spontaneously heal and must be surgically repaired because of the risk of incarceration.
Surgical consultation should be made at the time of diagnosis, and repair (on an elective basis) should be performed very soon after the diagnosis is confirmed.
Application of gentle pressure on the bulge of an inguinal hernia to prevent incarceration until the elective operative repair is performed.

MANAGEMENT: Surgical
Elective herniorrhaphy Involves closing of the patent processus vaginalis indicated to prevent incarceration and subsequent
strangulation Controversy exists regarding the role for exploration
of an asymptomatic opposite side in a child with an inguinal hernia.
Explore only under certain conditions such as in premature infants or in patients in whom incarceration is present.

Management of Incarcerated Hernia
Manual reduction should be attempted if the patient has no signs of systemic toxicity like: leukocytosis, severe tachycardia, abdominal
distention, bilious vomiting, and discoloration of the entrapped viscera
If the patient appears toxic, emergent surgical exploration is necessary.

Management of Incarcerated Hernia
Successful reduction of an incarcerated inguinal hernia results in immediate patient comfort, relief of obstruction, and prevention of strangulation.
Immediate surgery is performed if the reduction is unsuccessful; otherwise, elective operation is scheduled within 24-72 hours after reduction because recurrent incarceration is quite common.

Management of Hernia Strangulation
reduction without operative intervention is not possible
significant swelling from the compromised bowel, the presence of intestinal ischemia secondary to incarceration precludes the possibility of reducing the hernia back into the peritoneal cavity
immediate operative intervention is indicated, and the viability of the intestine must be carefully assessed at the time of surgery
If necrosis has developed, resect the affected segment of bowel

Course of the Patient
Prepared for OR: (maintained on NPO) IVF: D5 IMB @ 23CC/HR started on Cefuroxime (100) 190 mg Q8 Metronidazole (30) 60 mg Q8H
Underwent herniotomy, L under GA High ligation of the hernia sac
Discharge the next day….Take home meds:
1) Paracetamol 0.6 ml every 6H X 2days 2)Amoxicillin 2 drops (100mg/ml) Q6H X 7 days

PROGNOSIS
Inguinal hernias in children recur in less than 1 percent of patients, and recurrences usually result from missed hernia sacs at the fisrt procedure, a direct hernia, or missed femoral hernia.
Overall prognosis is excellent; most patients do extremely well after operative repair of their inguinal hernia.
Mortality is extremely rare but, unfortunately, continues to be reported as a consequence of delayed recognition of an incarcerated and strangulated inguinal hernia.

END
