4. shock dr. sinhasan- mdzah
TRANSCRIPT

Impaired tissue perfusion

1. Septic Shock (Endotoxic Shock:: Gram –ve )
2. Cardiogenic Shock:: Myocardial failure, Arrhythmia,
Embolism
3. Hypovoluemic Shock:: Blood loss, Burns
4. Others:: Neurogenic Shock, Anaphylactic Shock
CATEGORIES OF SHOCK

Final event to lethal clinical conditions like::
Severe hemorrhage,
Extensive trauma,
Burns,
Large MI,
Massive Pulmonary Embolism,
Sepsis.
Initially Shock Reversible injury ..Later Irreversible Injury
SHOCK… is syndrome

Cells switch from aerobic to anaerobic metabolism
lactic acid production
Cell function ceases & swells
membrane becomes more permeable
electrolytes & fluids seep in & out of cell
Na+/K+ pump impaired
mitochondria damage
cell death
PATHOPHYSIOLOGY OF SHOCK SYNDROME

70% are due to endotoxin producing Gram –ve bacilli infection
Endotoxins contain Lipopolysacharides
Most common cause of death in ICU
25 to 50% mortality
More technology.. More high risk patients.!!!!
Spread and expansion of initial localized infection
PATHOGENESIS OF SEPTIC SHOCK

LPS contains toxic fatty acid Lipid A and complex
polysaccharide coat
Free LPS binds to LPS binding protein
Binds to receptors on vascular wall, leukocytes and initiate
cytokine cascade
Effects of cytokines is to isolate organisms & trigger innate
immunity
Effect depends on dosage of LPS
PATHOGENESIS OF SEPTIC SHOCK

Same cytokines & mediators at higher levels
Systemic vasodilatation
Diminished Myocardial contraction
Widespread endothelial injury
Alveolar damage .. ARDS
DIC activation
VERY HIGH LPS.. SEPTIC SHOCK
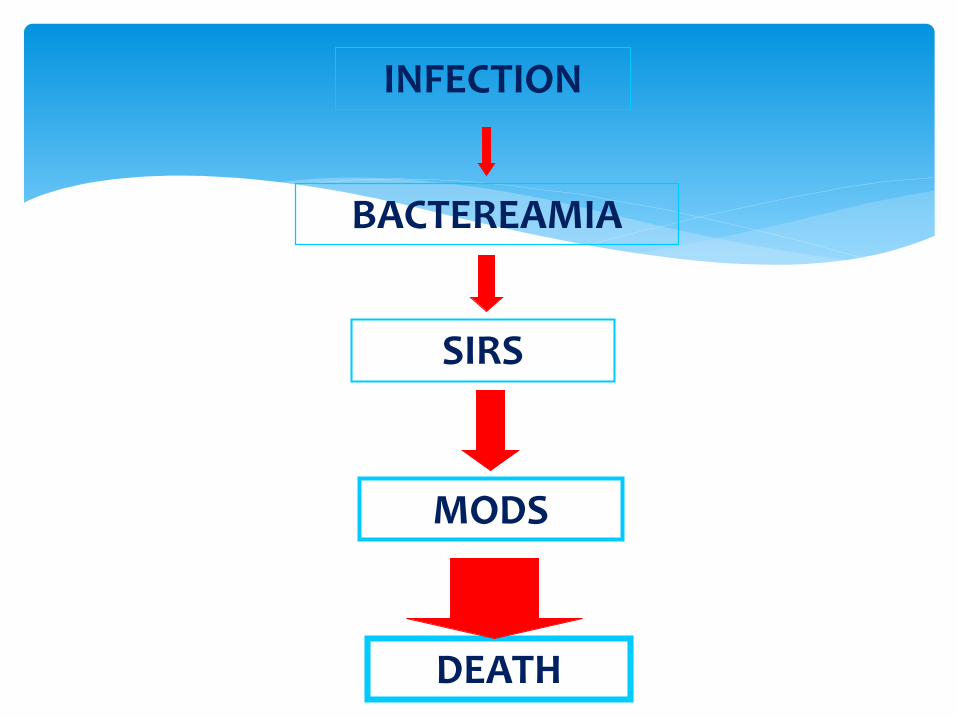
INFECTION
BACTEREAMIA
SIRS
MODS
DEATH
Septic Shock SIRSBacteremia
Infn

Any two or more of the following constitutes SIRS:::
Body temperature > 38° C or < 36° C
Heart rate > 90 / min
Hyperventilation >20 /min
WBC count >12,000/mm³ or < 4000/mm³
SIRS can lead to Septic Shock and MODS
SIRS CRITERIA

1. Non Progressive stage:: Reflex compensatory
mechanisms are activated
2. Progressive stage:: Tissue hypoperfusion, metabolic
imbalance, acidosis
3. Irreversible stage:: Severe Cellular & tissue injury,
Survival is not possible
STAGES OF SHOCK

Changes are those of Hypoxic Injury
Brain:: Ischemic Encephalopathy
Heart:: Coagulative necrosis, Subendocardial hemorrhage.
Kidneys:: Acute Tubular Necrosis
Lungs:: Diffuse alveolar damage Shock Lung
MORPHOLOGY OF SHOCK

Adrenals:: Adrenal cortex lipid depletion:
“Waterhouse Frederickson syndrome”
GIT:: Patchy mucosal hemorrhages “Hemorrhagic
enteropathy”
Liver:: fatty change, Central hemorrhagic necrosis

Tachycardia and tachypnea
Weak pulses
Hypotension
Skin cool & clammy
Mental status changes
Decreased urine output: dark & concentrated

Loss of circulating volume “Empty tank ”
decrease tissue perfusion—Hypovoluemic shock.
ETIOLOGY:
Body Fluid loss-- Nausea & vomiting, diarrhea, massive diuresis, extensive burns.
Most common causes:
Hemorrhage
Dehydration

Clinical Signs of hypovoluemic Shock
% Blood loss Clinical Signs
< 15 Slightly increased heart rate, local
swelling, bleeding
15-30 Increased heart rate, increased
diastolic blood pressure, prolonged
capillary refill
30-50 Above findings plus: hypotension,
confusion, acidosis, decreased urine
output
> 50 Refractory hypotension, refractory
acidosis, death

The impaired ability of the heart to pump blood
Most common cause is LV MI
Occurs when > 40% of ventricular mass damage
Mortality rate of >80 %.

Antigen exposure
Body stimulated to produce IgE antibodies specific to antigen
drugs, bites, contrast, blood, foods, vaccines
Re-exposure to antigen
IgE binds to mast cells and basophils
Anaphylactic response

A type of distributive shock that results from the loss
or suppression of sympathetic tone
Most common etiology: Spinal cord injury above T6
Neurogenic is the rarest form of shock!

COLLABORATIVE MANAGEMENT
Prevention !!!
Find and kill the source of
the infection
Fluid Resuscitation
Vasoconstrictors
Inotropic drugs
Maximize O2 delivery Support
Nutritional Support
Comfort & Emotional support

Hypovoluemia: Blood/ fluid transfusion
Sepsis: Antibiotics, ? steroids
Neurogenic: Steroids
Anaphylactic: Adrenalin
Electrolyte/acid base imbalance
Specific measures
