29 cfr part 1904 - cbia...• in-patient hospitalization of 1or more employee(s) an amputation is...
TRANSCRIPT

1
29 CFR Part 1904Recording and Reporting
Occupational Injuries and Illnesses
OSHA Recordkeeping29 CFR 1904
Grayson Gregory, Associate Research Analyst [email protected](860) 263-6912
Catherine Zinsser, Occupational Safety Training [email protected](860) 263-6942

2
OSHA vs. CONN-OSHA
• CONN-OSHA– Compliance Coverage
• Since 1978 Public Sector only• 169 Cities/Towns • Public Schools• Police, Career/Volunteer Fire Departments• State of Connecticut
• Consultation Coverage– Public Sector– Private Sector
● Federal OSHA Compliance Coverage
Purpose of Recordkeeping Rule
• To require employers to record and report work-related fatalities, injuries and illnesses
• OSHA injury and illness recordkeeping and Workers’ Compensation are Independent of each other
WC OSHA
Mississippi River

3
5
29 CFR 1904
Reporting requirements…“who and when do you call…”
Recording requirements…
Reporting RequirementsAll employers must…
• 1904.39, Reporting fatalities, hospitalization incidents, loss of eye, amputations
• 1904.41, Electronic submission of injury and illness records
• 1904.42, BLS Annual Survey (if specifically requested to do so by BLS)
Private Sector Employers that are partially exempt from the recordkeeping requirements because of their size or industry must continue to comply with 1904.42

4
Within 24 hours you must report• amputations• the loss of an eye• in-patient hospitalization of 1or more employee(s)An amputation is defined as the traumatic loss of a limb or other external body part. Amputations include a part, that has been severed, cut off, amputated (either completely or partially); fingertip amputations with or without bone loss; medical amputations resulting from irreparable damage; and amputations of body parts that have since been reattached.
Reporting Requirements for allEmployers
Within 8 hours you must report fatalities
Public Sector Exemptions
There are none for reporting…or recording

5
9
Private Sector Exemptions from Recording
• 1904.1 – Small employer partial exemptions
• 1904.2 – Private Industry partial exemptions
• 1904.3 – Keeping records for other Federal agencies
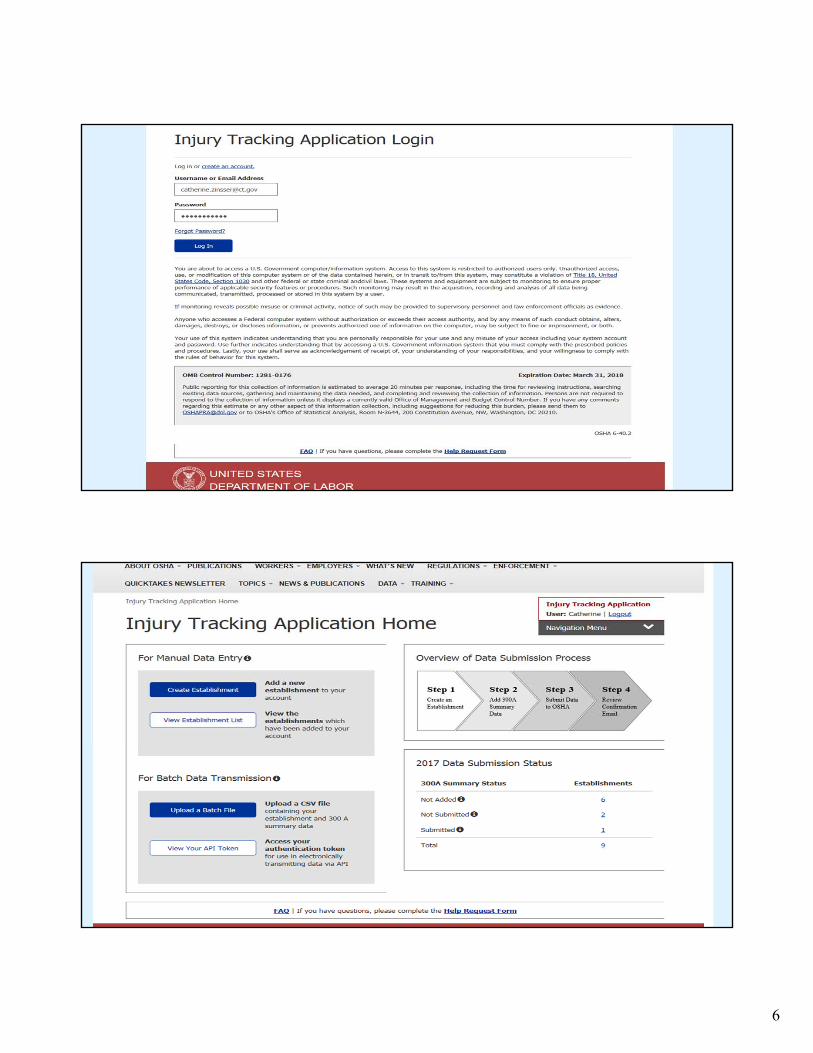
Establishments with 250 or more employees in industries covered by the recordkeeping regulation must submit information from their 2017 Form 300A by July 1, 2018. (300’s and 301’s are not being accepted at this time).
Beginning in 2019 and every year thereafter, covered establishments must submit the information by March 2.
Establishments with 20-249 employees in certain high-risk industries and public sector employers must submit information from their 2017 Form 300A by July 1, 2018.
1904.41 Electronic Submission of Injury and Illness Data Private Sector employers
https://www.osha.gov/injuryreporting/index.html
Public Sector employers- All must submit
6

7
You should subscribe to OSHA Quick Takeshttps://www.osha.gov/

8
U.S. OSHA Reporting:Hartford Area Office- 860-240-3152Bridgeport Area Office- 203-579-558124-Hour hot line 1-800-321-6742Online: www.osha.gov/report online
CONN-OSHA Reporting:Fatality & hospitalization reporting:Regular Business hours: 860-263-6946After Hours- 1-866-241-4060

9

10
OSHA Recordkeeping Guidelines
&
Temporary Employees
What if….
1. A salesman, who works out of his private home, slips and falls on ice in his driveway. The employee states he was carrying company property at the time of his fall. Is this work-related?

11
2. Does the form 300A need to be mailed to OSHA by a certain date? If so, when is this date? Where should it be mailed to?
What if…. ( new reporting requirements)
What if….
3. An employee works for a certain location and visits different locations of his company during his day's work. During such a visit, he is injured in a location which is other than his home location. In such a case, should the injury be reported (in the OSHA 300 log) for the home location or the location where the employee was actually injured?

12
What if…
4. Since a tetanus immunization is a preventative medication and is not considered medical treatment for recordkeeping purposes, are other preventative medications first aid or medical treatment?
For example if a person is bitten by a dog and the Physician gives prescription antibiotics as a preventive measure, is the case recordable?
What if…
5. An employee is bitten on the arm by a patient and the skin is slightly broken with little bleeding present. No medical treatment (beyond first aid) was needed and the case did not involve any days away or restrictions. Is this recordable?

13
What if…
6. An employee was injured on 9/21. He went to the Urgent Care doctor, who sent him to the hospital for an MRI. The doctor required the employee to return to him the next day to interpret the results of the MRI. The MRI was good, but the employee could not get in to see the doctor until the afternoon of 9/22. By the time this doctor had released him to work, his shift had already ended. Does this count as a lost work day?
What if…7. An employee arrives for work. As she is walking across the parking lot prior to the start of her shift, she is bitten by a wasp/bee and has an allergic reaction. She is taken to the doctor where she is given an injection and a prescription. Is this case recordable?

14
27
What if…
8. An employee is hired from a local union hall for a short duration. If the employee suffers a lost time injury, but the job is finished days later and the employee is laid off due to a lack of work, does the employer have to continue counting the days away from work until the employee is returned to full duty status by the treating physician?
9. On Record Keeping form 300A, what is the definition of "Company Executive"? Specifically, does a Manager of Safety, Health, & Environment meet the criteria of Company Executive if he/she is responsible for the safety and health of employees at a plant location for which the form is being completed?
What if…

15
10. Do I have to give my employees and their representative's access to the OSHA injury and illness records?
What if…..
11. I am getting the OSHA 300A forms ready for posting the next year and I have a question on how many employees to put down. We have several establishments, and they all need to post their own log. All together, the company has about 150 employees, but each branch location only has 5-8 employees. For the annual average # of employees and the hours worked, do I put the total for the company or just the for each location.
What if…..

16
12. We have an employee who had a job related injury, which resulted in work restrictions. As is required by our Company, he had to submit to a post injury drug test, and the drug test came back positive. Do we still need to record this on our 301 log, even though it did result in a positive drug test?
What if…..
13. How do I record a case in which the employee was prescribed restricted work activity and we made it available, but the employee decides on his own, to refuse the restricted work and stays home instead?
What if…..

17
14. Are work-related cases involving chipped or broken teeth recordable?
What if…..
34
Resources• OSHA’s Recordkeeping Page
http://www.osha.gov/recordkeeping/index.html
• State Plan – CONN-OSHA 860-263-6900

18
Questions?

CONN-OSHA Connecticut Occupational Safety and Health Administration
OSHA Recordkeeping Guidelines
Questions Regarding This Form? Call the Office of Research at 860-263-6272 or e-mail [email protected]
Overview The Occupational Safety and Health Administration (OSHA) Standard 29 CFR Part 1904 Recording and Reporting Occupational Injuries and Illnesses require employers to record and report work-related fatalities, injuries and illnesses. This handout is a general overview of OSHA recordkeeping. It does not address all the rules and regulations of OSHA recordkeeping, which are periodically updated.
You are responsible for upholding all OSHA regulations regarding the reporting and recording of occupational injuries and illnesses.
Recordkeeping Reminders Upon request, government representatives must be provided copies of OSHA records
within 4 business hours.
Enter OSHA recordable cases on your OSHA 300 Log within 7 calendar days.
Post your completed OSHA Form 300A from February 1st through April 30th.
Retain forms for the past 5 years, updating the OSHA Form 300 as needed.
Days Away, Restricted, or Transferred (DART) Rate calculation DART Rate = (Column H + Column I) x 200,000 Total Hours Worked.
Websites Downloadable OSHA Recordkeeping forms in PDF or Excel format are available at
U.S. OSHA’s Recordkeeping website: www.osha.gov/recordkeeping
For the complete recordkeeping standard, Google “OSHA Standard Part 1904” and follow the first link to: www.osha.gov/pls/oshaweb/owastand.display_standard_group?p_toc_level=1&p_part_number=1904
Last updated: January 2017

- 2 -
Recording Criteria Decision Tree To determine if an OSHA recordable case has occurred, answer these four questions: 1. Has an injury or illness occurred? Yes Continue to question 2. No An injury or illness has not occurred. Do not record this on your OSHA log. 2. Is the injury or illness work-related?
Work-relatedness is presumed for injuries and illnesses occurring in the work environment. Assume the injury or illness is work-related unless it is specifically addressed in the exceptions listed below.
Yes Continue to question 3. No A recordable injury/illness has not occurred. Do not record this on your OSHA log.
Exceptions. The case is not considered work-related if it falls into one of these categories: ◊ Present as a member of the general public. ◊ Symptoms arise in workplace but are solely due to non-work related event or exposure. ◊ Voluntary participation in a wellness program. ◊ Eating, drinking, or preparing food or drink for personal consumption. ◊ Personal tasks outside assigned working hours. ◊ Personal grooming, self-medication for non-work-related conditions, or intentionally self-
inflicted injuries. ◊ Motor vehicle accident occurring in a parking lot or access road during a normal
commute to or from work. ◊ Common cold or flu. ◊ Mental illness, unless employee voluntarily provides a medical opinion from a physician or
licensed health care professional (PLHCP) that affirms the mental illness is work-related. 3. Is the injury or illness a new case?
If an employee has recovered completely from a previous injury or illness, and an event or exposure in the work environment causes the symptoms to re-appear, the injury or illness is a new case.
Yes Continue to question 4. No Do not record a new case. If necessary, update the previously recorded injury or illness entry.
4. Does the injury or illness meet the general recording criteria? Remember to check for rules that
apply to special cases. Yes A recordable injury/illness has occurred. Record this as a case on your OSHA log. No A recordable injury/illness has not occurred. Do not record this on your OSHA log.
General recording criteria. A case is recordable if it involves one or more of the following: All fatalities occurring in the United States and her territories Occupational injuries and illnesses that resulted in:
◊ days away from work, restricted work or job transfer ◊ medical treatment (see page four) ◊ loss of consciousness
Other serious or significant cases diagnosed by a PLHCP Occupational injuries and illnesses that meet special recording criteria:
◊ needlestick and sharps injuries ◊ medical removal under OSHA standards ◊ occupational hearing loss

- 3 -
Completing the OSHA Log - Form 300 New OSHA 300 Forms were established on January 1, 2004. The new form lists Column K as Number of Days Away from Work and has a Hearing Loss category in Column M. If you need a new form, please contact our office or visit www.osha.gov/recordkeeping to download a form. For every case recorded on your log, you must also complete OSHA Form 301: Injury and Illness Incident Report. All fields are required: date of birth, date hired, time employee began work, time of event, etc. You may substitute an equivalent form, such as the Connecticut Workers’ Compensation First Report of Injury, if it includes all of the information requested on the OSHA Form 301. Column G: Death Each year, nearly five thousand U.S. workers lose their lives to work injuries. All employers, regardless of size or industry, are required to report these deaths. Reporting and recording deaths are separate actions – a reportable death may not be a recordable case. Consult the decision tree to determine if a death should be recorded on your OSHA log. Reporting
◊ Within 8 hours, you must report any work fatality to OSHA. This includes fatal heart attacks and other incidents that may not be recordable on the OSHA Log.
◊ Report to your local OSHA office. If after business hours, call 1-800-321-OSHA (1-800-321-6742). ◊ You are not required to report:
highway or public street motor vehicle accidents unless they are in a construction work zone. commercial airplane, boat, train, subway, or bus accidents.
◊ You are also required to report within 24 hours amputations, loss of eye, and hospitalizations. Recording
◊ If appropriate, record the case on your OSHA 300 Log with a check in Column G: Deaths. Do not record any days away from work related to the death (see example on page six).
◊ Transportation fatalities occurring outside of an employee’s normal commute are recordable, even if you have not reported them.
Column H: Days Away from Work When an injury or illness involves one or more days away from work, you must record the case on your OSHA 300 Log with a check in Column H: Cases with Days Away from Work. If a job restriction or transfer is recommended, but the employer cannot offer restricted work or a job
transfer, the case will be counted as a days away from work case. ◊ Example: A doctor recommends 3 days of light duty for Gina. There is no light work available, so the employer
tells her to stay home instead. This is a recordable case with 3 days away from work.
If a case has both days away and job transfer/restriction days, record the case once and only once in Column H: Cases with Days Away from Work. Leave Column I: Cases with Job Transfer or Restriction blank. This is true even when the job transfer/restriction days exceed the number of days away from work. ◊ Example: Rob falls from an extension ladder to a concrete patio and breaks his arm. He is out of work for 7
days and on restricted duty for 10 days. Check Column H, record 7 days in Column K and 10 days in Column L. Leave Column I blank (see example on page six).
Column I: Job Transfer or Restriction If a work injury or illness prevents an employee from performing one or more routine functions of his or her job, the case involves days of job restriction or transfer. If the case does not have any days away from work, record the case in Column I: Cases with Job Transfer or Restriction. A routine function is defined as a task performed at least once per week.
◊ Example: Every Friday, Cindy moves 15-40 lb delivery boxes. A work-related injury prohibits her from lifting over 20 lbs. for five days. The injury is recordable with 5 days of restriction.
◊ Example: The doctor tells Aaron not to lift anything over 40 lbs. His normal workweek does not require any lifting over 15 lbs. The restriction is not recordable.
If an employee is kept from working a full workday, the days are counted as restrictions. ◊ Example: Todd is injured at work and is told to work only four-hour shifts for 2 days. The injury is recordable
with 2 days of restriction.

- 4 -
Other Recordable Cases vs. First Aid
Column J: Other Recordable Cases If a case falls into one of the categories below, it is OSHA recordable. If the employee did not have days away from work (Column H), job transfer or restriction (Column I), the case is recorded in Column J: Other Recordable Cases. You must also record the appropriate category under Column M: Injury and Illness Types. Medical treatment beyond First Aid: ◊ Prescription medication. The use of non-prescription medication at prescription strength as recommended
by a physician or licensed health care professional (PLHCP) is considered prescription medication. ◊ Immunizations (except tetanus) such as hepatitis B or rabies vaccines. ◊ Wound-closing devices such as surgical glue, sutures, staples, etc. ◊ Any device with rigid stays or other systems designed to immobilize parts of the body. ◊ Physical therapy or chiropractic treatment. ◊ Removal of foreign material that is embedded in the eye. ◊ Any treatment not specifically defined as First Aid (listed below)
Significant Diagnosed Injury or Illness: Any serious or significant work-related disorder that is diagnosed by a PLHCP or identified by a positive medical test. These include cases of cancer, chronic irreversible disease, a fractured or cracked bone or tooth, or a punctured eardrum. Specific guidelines on recordable hearing loss injuries may be found online @ www.osha.gov/recordkeeping
Needlestick injuries and cuts from sharp objects that are contaminated with another person’s blood or other potentially infectious materials. Potentially infectious materials include human bodily fluids, tissues and organs, and materials infected with the HIV or hepatitis B virus.
An OSHA standard requires medical removal of an employee for medical surveillance.
Loss of consciousness from a work-related injury or illness is recordable. Loss of consciousness due solely to personal health conditions (diabetes, epilepsy, narcolepsy, etc.) is not recordable.
Not Recordable If a case is limited to First Aid treatment AND there are no days away from work, job transfer, or job restriction, do not include the case on your OSHA 300 Log. The case is not OSHA recordable, even if the First Aid treatment is administered at a health clinic, emergency room, hospital, or other medical treatment facility. First Aid treatment is defined as: Visits to a PLHCP solely for observation or
counseling. Diagnostic procedures, such as x-rays and blood
tests, including the administration of prescription medications solely for diagnostic purposes (e.g., eye drops to dilate pupils).
Using non-prescription medications at non-prescription strength (per box instructions).
Cleaning, flushing or soaking wounds on the surface of the skin.
Using wound coverings such as bandages, Band-Aids, gauze pads, butterfly bandages, Steri-Strips, and other similar coverings (Note: wound closing devices listed above are medical treatment).
Using any non-rigid means of support such as elastic bandages, wraps, non-rigid back belts, etc.
Using temporary immobilization devices while transporting an accident victim (e.g., splints, slings, neck collars, back boards, etc.).
Drilling of fingernail or toenail to relieve pressure, or draining fluid from a blister.
Removing splinters or foreign material from areas other than the eyes by irrigation, tweezers, cotton swabs or other simple means.
Removing foreign bodies from the eye using only irrigation or a cotton swab.
Using eye patches or finger guards. Non-therapeutic massages (spa treatment). Using hot or cold therapy. Drinking fluids for relief of heat disorder. Tetanus immunizations.
Examples Sue cuts her hand and goes to the emergency room. A nurse cleans and covers the wound with a
Band-Aid and sends Sue back to work. This is not a recordable case. Henry has a piece of metal embedded in his eye. A doctor removes it and sends him back to work.
This case should be recorded in Column J: Other Recordable Cases. Joan falls at work, bruising her leg. She does not receive medical treatment but the doctor tells her
to stay home for two days before returning to work. This case should be recorded in Column H: Cases with Days Away from Work.

- 5 -
Number of Days & Injury or Illness Types Columns K & L: Number of Days Start counting with the day after the injury and count calendar days. Count all the days the
person is unable to work, or work with restrictions/transfer, even if the person is not scheduled to work on those days. ◊ Example: An employee’s workweek is Monday through Friday. The employee is injured on Thursday
morning and goes home for the rest of the day. She stays home on Friday and Monday, but returns to full duty Tuesday morning. This case involves lost time and should be recorded in Column H: Cases with Days Away from Work. Also record 4 days (Friday, Saturday, Sunday, and Monday) in Column K: Number of Days Away From Work.
◊ Example: On Monday morning, an employee punches in at 8:05 a.m. and is injured at 8:15 a.m. He goes home for the rest of the day but returns on Tuesday to work a complete shift without restrictions/transfer. This injury does not involve lost time. If the injury required treatment beyond First Aid, you would record it in Column J: Other Recordable Cases.
A case has days away from work that continue into the next year. Record the case and all related days on the log for the year the injury or illness occurred. ◊ Example: An employee is injured on December 23, 2012, and does not return to work until January
27, 2013. The case and the 34 days away from work would be recorded on the 2012 log. Do not include the case or lost days on the 2013 log.
If an individual case has a large amount of lost time, you may stop counting at 180 days. ◊ Example: An employee is injured and stays home for 150 days, followed by 120 days of job transfer.
You may record 150 days in Column K: Number of Days Away From Work and 30 days in Column L: Number of Days of Transfer or Restriction for a total of 180 days.
If a person leaves your company for reasons unrelated to the injury or illness, stop counting the number of days. ◊ Example: A clerk typist falls in the parking lot and breaks her leg. The doctor recommends she stay
home for two weeks. After one week, she accepts a clerk typist position at a company with better benefits. Record the case in Column H: Cases with Days Away from Work and 7 days in Column K: Number of Days Away From Work.
◊ Example: A carpenter’s leg is amputated after suffering a work-related accident and will be out of work for 120 days. The carpenter decides to pursue a safer career and leaves the company. Record the case in Column H: Cases with Days Away from Work. Since he left because of the injury, the full 120 days are recorded in Column K: Number of Days Away From Work.
Column M: Injury and Illness Types For every case entered in columns G, H, I, and J, there must be a corresponding checkmark in Column M: Injury and Illness Type. The total number of cases (G+H+I+J) must equal the total for Column M (1+2+3+4+5+6). Examples of each category are provided below. Injuries
◊ M1 Injuries: Amputations, animal and insect bites, broken bones, burns, concussions, electrocutions, heat stroke, hernias, lacerations, muscle strains and sprains, etc.
Illnesses ◊ M2 Skin Disorders: dermatitis, rosacia, psoriasis, poison ivy, etc. ◊ M3 Respiratory Conditions: avian or swine flu, sinusitis, emphysema, asthma, tuberculosis, etc. ◊ M4 Poisonings: carbon monoxide, lead, or cadmium poisoning, medical removal due to an OSHA
standard, etc. ◊ M5 Hearing Loss: Specific guidelines may be found online @ www.osha.gov/recordkeeping ◊ M6 All Other Illnesses: Repetitive motion illnesses such as carpal tunnel syndrome or tendonitis,
mental illness, varicose veins, chicken pox, etc.

- 6 -
Log Example, Privacy Concerns & Healthcare Recommendations
Log Example For your reference, a sample OSHA 300 Log is provided below. Notice that each case has one and only one check mark in columns G-J.
Privacy Concerns If you wish to share your OSHA records with unauthorized persons, you must first remove the employees’ names from the records. Authorized persons include representatives from OSHA, Workers’ Compensation, Public Health, law enforcement agencies, insurance auditors, or consultants.
Privacy concern cases require the removal of an employee’s name and identifying information from OSHA Forms. Instead of the person’s name, list “privacy concern”. You must keep a separate, confidential list identifying the case number and employee name. Privacy concern cases are:
Injury or illness to an intimate body part Injury or illness resulting from a sexual assault Mental illness HIV infection, hepatitis, tuberculosis Needlestick and sharps injuries that are contaminated with another person’s blood or other potentially
infectious material Employee requests to keep name off of an illness case
Healthcare Recommendations You are not required to obtain the recommendation of a physician or licensed health care professional (PLHCP). However, if a recommendation is available, you must record the case accordingly. This is true even if the employee does not follow the recommendation.
Example: George is injured at work and is told not to lift anything over 30 lbs for five days, but he immediately resumes his full job duties. The injury is a recordable case with five days of restriction.
Example: Carl slips and falls at work. The plant nurse instructs him to return to work, but he stays at home for two days. The injury is not recordable.
Fell from extension ladder onto concrete patio. Fractured lower arm. Cut hand on rotary table saw. Received stitches and returned to work. Strained lower back lifting 80lb bags of concrete-no lifting over 50lbs for 2 weeks.
Carpal tunnel in wrists due to daily typing.
Rash on arm from exposure to cutting oil – prescription meds Carbon monoxide poisoning-hospitalized 2 weeks before death.
X
X
X
X
X
X
-- --
-- --
-- --
7 10
30 15
14 --
x x x
x x
x

U.S. Department of LaborOccupational Safety and Health Administration
OSHA’s Form 300 (Rev. 01/2004) Year 20__ __Log of Work-Related Injuries and IllnessesYou must record information about every work-related death and about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer,days away from work, or medical treatment beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed healthcare professional. You must also record work-related injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR Part 1904.8 through 1904.12. Feel free touse two lines for a single case if you need to. You must complete an Injury and Illness Incident Report (OSHA Form 301) or equivalent form for each injury or illness recorded on thisform. If you’re not sure whether a case is recordable, call your local OSHA office for help.
Form approved OMB no. 1218-0176
Page ____ of ____
Skin
dis
orde
r
Res
pira
tory
cond
ition
Pois
onin
g
Hea
ring
loss
All
othe
rill
ness
es
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Page totals
Establishment name ___________________________________________
City ________________________________ State ___________________
Inju
ry
Enter the number ofdays the injured orill worker was:
Check the “Injury” column orchoose one type of illness:
month/day
month/day
month/day
month/day
month/day
month/day
month/day
month/day
month/day
month/day
month/day
month/day
month/day
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to reviewthe instructions, search and gather the data needed, and complete and review the collection of information. Persons are not requiredto respond to the collection of information unless it displays a currently valid OMB control number. If you have any commentsabout these estimates or any other aspects of this data collection, contact: US Department of Labor, OSHA Office of StatisticalAnalysis, Room N-3644, 200 Constitution Avenue, NW, Washington, DC 20210. Do not send the completed forms to this office.
(A) (B) (C) (D) (E) (F)
(M)
(K) (L)(G) (H) (I) (J)
DeathDays awayfrom work
On jobtransfer orrestriction
Awayfromwork
Attention: This form contains information relating toemployee health and must be used in a manner thatprotects the confidentiality of employees to the extentpossible while the information is being used foroccupational safety and health purposes.
CHECK ONLY ONE box for each casebased on the most serious outcome forthat case:
Job transferor restriction
Other record-able cases
Remained at Work
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
❑
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
(1) (2) (3) (4) (5) (6)
(1) (2) (3) (4) (5) (6)
Skin
dis
orde
r
Res
pira
tory
cond
ition
Pois
onin
g
Hea
ring
loss
All
othe
rill
ness
es
Inju
ry
Identify the person Describe the case Classify the case
Case Employee’s name Job title Date of injury Where the event occurred Describe injury or illness, parts of body affected,
of illness or made person ill (
no. or onset and object/substance that directly injured
e.g., Second degree burns on
e.g., Welder e.g., Loading dock north end
right forearm from acetylene torch
( ) ( )
)
_____ ________________________ ____________ ______/__________ ______________________ ___________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ___________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ___________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ___________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ___________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ___________________ ____________________________________________________ ____ ____
_____ ________________________ ____________ ______/__________ ______________________ ____________________________________________________ ____ ____
days days
days days
days days
days days
days days
days days
days days
days days
days days
days days
days days
days days
days days
U.S. Department of LaborOccupational Safety and Health Administration
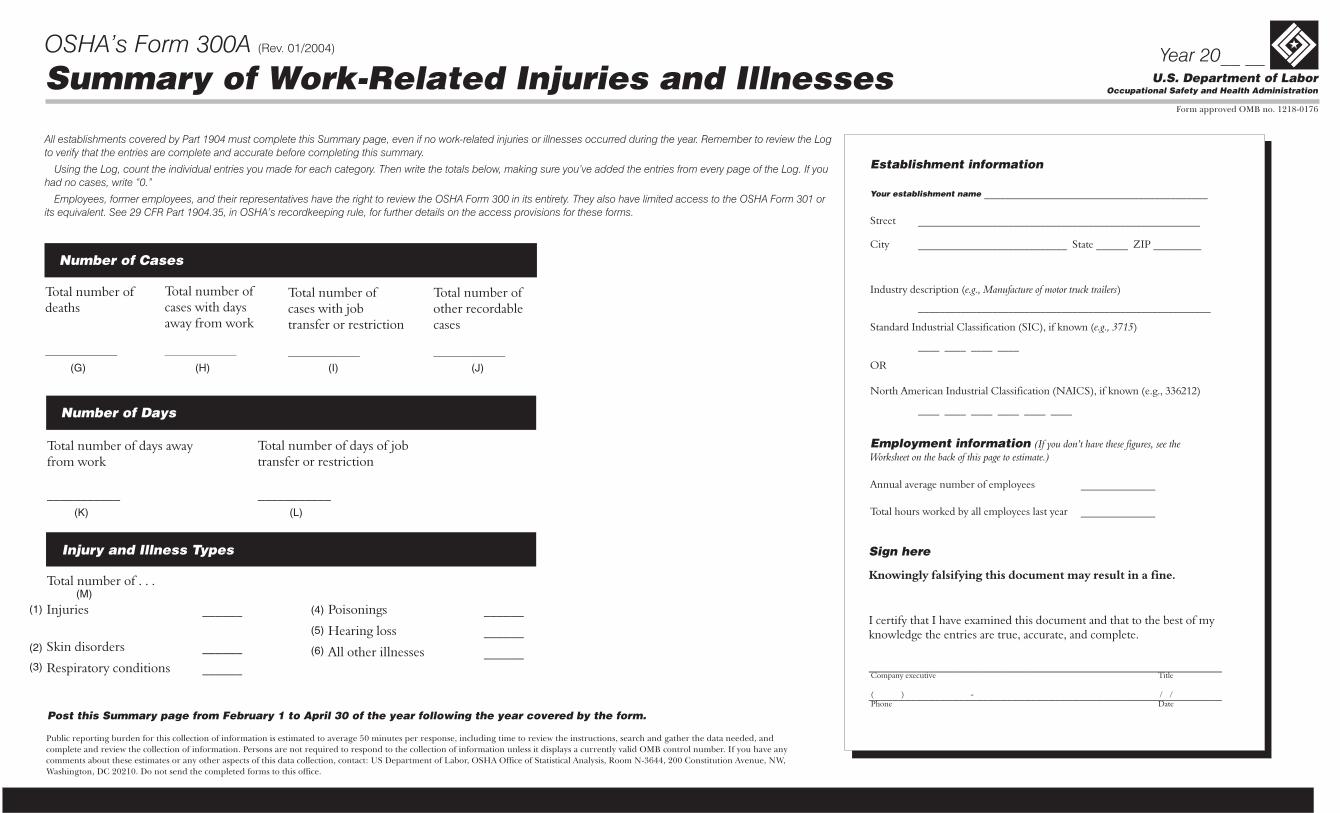
OSHA’s Form 300A (Rev. 01/2004) Year 20__ __Summary of Work-Related Injuries and Illnesses
Form approved OMB no. 1218-0176
Total number ofdeaths
__________________
Total number ofcases with daysaway from work
__________________
Number of Cases
Total number of days awayfrom work
___________
Total number of days of jobtransfer or restriction
___________
Number of Days
Post this Summary page from February 1 to April 30 of the year following the year covered by the form.
All establishments covered by Part 1904 must complete this Summary page, even if no work-related injuries or illnesses occurred during the year. Remember to review the Logto verify that the entries are complete and accurate before completing this summary.
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you’ve added the entries from every page of the Log. If youhad no cases, write “0.”
Employees, former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 orits equivalent. See 29 CFR Part 1904.35, in OSHA’s recordkeeping rule, for further details on the access provisions for these forms.
Establishment information
Employment information
Your establishment name __________________________________________
Street _________________________ _______
City ____________________________ State ______ ZIP _________
Industry description ( )
_______________________________________________________
Standard Industrial Classification (SIC), if known ( )
____ ____ ____ ____
North American Industrial Classification (NAICS), if known (e.g., 336212)
e.g., Manufacture of motor truck trailers
e.g., 3715
(I ee theWorksheet on the back of this page to estimate.)
_____________________
OR
____ ____ ____ ____ ____ ____
Annual average number of employees ______________
Total hours worked by all employees last year ______________
f you don’t have these figures, s
Sign here
Knowingly falsifying this document may result in a fine.
I certify that I have examined this document and that to the best of myknowledge the entries are true, accurate, and complete.
___________________________________________________________
___________________________________________________________
Company executive Title
Phone Date( ) - / /
Public reporting burden for this collection of information is estimated to average 50 minutes per response, including time to review the instructions, search and gather the data needed, andcomplete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have anycomments about these estimates or any other aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room N-3644, 200 Constitution Avenue, NW,Washington, DC 20210. Do not send the completed forms to this office.
Total number of . . .
Skin disorders ______
Respiratory conditions ______
Injuries ______
Injury and Illness Types
Poisonings ______
Hearing loss
All other illnesses ______
______
(G) (H) (I) (J)
(K) (L)
(M)(1)
(2)
(3)
(4)
(5)
(6)
Total number ofcases with jobtransfer or restriction
__________________
Total number ofother recordablecases
__________________
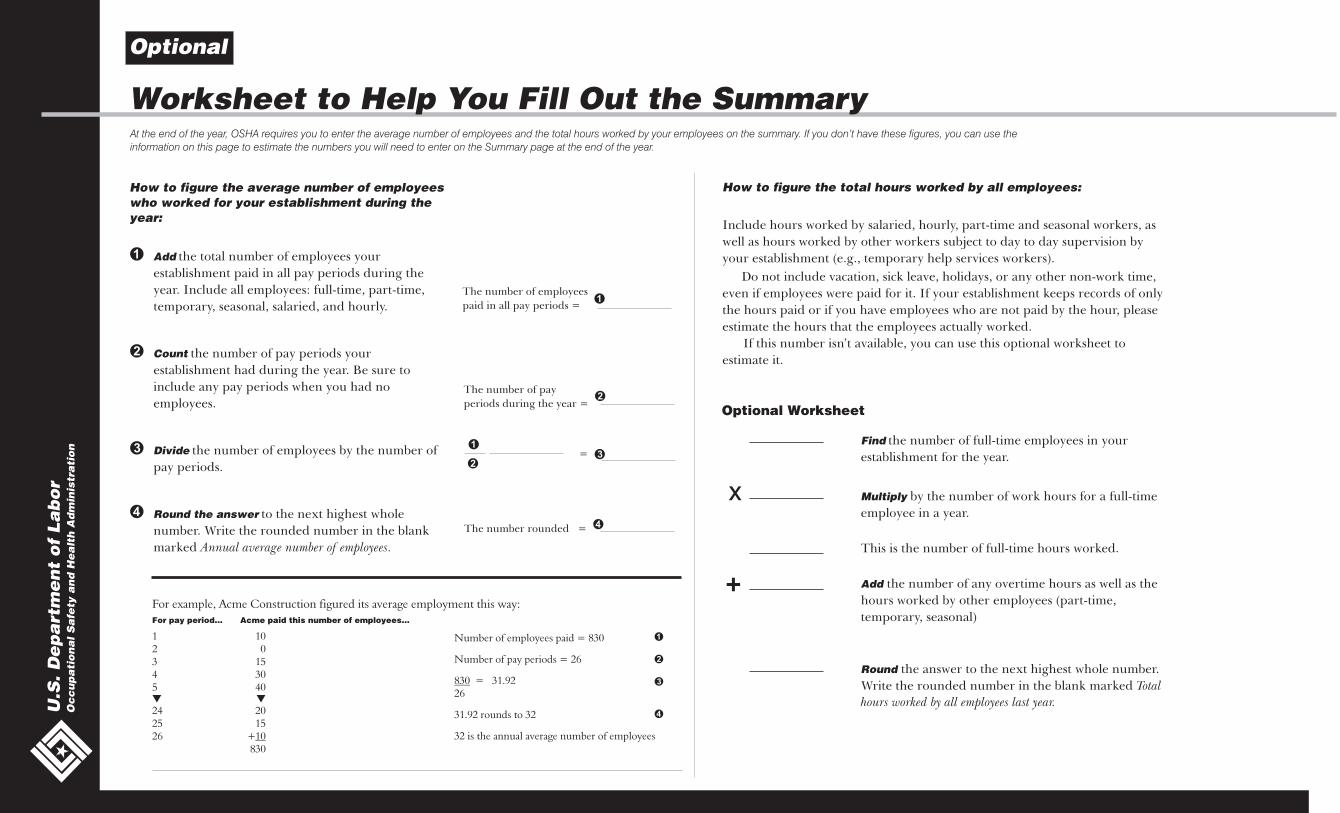
At the end of the year, OSHA requires you to enter the average number of employees and the total hours worked by your employees on the summary. If you don’t have these figures, you can use theinformation on this page to estimate the numbers you will need to enter on the Summary page at the end of the year.
For example, Acme Construction figured its average employment this way:For pay period… Acme paid this number of employees…
1 102 03 154 305 40
24 2025 1526 +
830
▼ ▼
10
How to figure the average number of employeeswho worked for your establishment during theyear:
�
�
�
�
Add
Count
Divide
Round the answer
the total number of employees your
establishment paid in all pay periods during the
year. Include all employees: full-time, part-time,
temporary, seasonal, salaried, and hourly.
the number of pay periods your
establishment had during the year. Be sure to
include any pay periods when you had no
employees.
the number of employees by the number of
pay periods.
to the next highest whole
number. Write the rounded number in the blank
marked Annual average number of employees.
The number of employees
paid in all pay periods =
The number of pay
periods during the year =
=
The number rounded =
�
�
�
�
How to figure the total hours worked by all employees:
Include hours worked by salaried, hourly, part-time and seasonal workers, as
well as hours worked by other workers subject to day to day supervision by
your establishment (e.g., temporary help services workers).
Do not include vacation, sick leave, holidays, or any other non-work time,
even if employees were paid for it. If your establishment keeps records of only
the hours paid or if you have employees who are not paid by the hour, please
estimate the hours that the employees actually worked.
If this number isn’t available, you can use this optional worksheet to
estimate it.
Optional
Worksheet to Help You Fill Out the Summary
U.S
. D
ep
art
me
nt
of
La
bo
rO
cc
up
ati
on
al S
afe
ty a
nd
He
alt
h A
dm
inis
tra
tio
n Find
Multiply
Add
Round
the number of full-time employees in your
establishment for the year.
by the number of work hours for a full-time
employee in a year.
This is the number of full-time hours worked.
the number of any overtime hours as well as the
hours worked by other employees (part-time,
temporary, seasonal)
the answer to the next highest whole number.
Write the rounded number in the blank marked Total
hours worked by all employees last year.
x
+
Optional Worksheet
Number of employees paid = 830
Number of pay periods = 26
= 31.9226
31.92 rounds to 32
32 is the annual average number of employees
830

Information about the employee
Information about the physician or other health careprofessional
Full name
Street
City State ZIP
Date of birth
Date hired
Male
Female
Name of physician or other health care professional
If treatment was given away from the worksite, where was it given?
Facility
Street
City State ZIP
Was employee treated in an emergency room?
Yes
No
Was employee hospitalized overnight as an in-patient?
Yes
No
_____________________________________________________________
________________________________________________________________
______________________________________ _________ ___________
______ / _____ / ______
______ / _____ / ______
__________________________
________________________________________________________________________
_________________________________________________________________
_______________________________________________________________
______________________________________ _________ ___________
�
�
�
�
�
�
U.S. Department of LaborOccupational Safety and Health Administration
OSHA’s Form 301Injury and Illness Incident Report
Form approved OMB no. 1218-0176
This is one of the
first forms you must fill out when a recordable work-
related injury or illness has occurred. Together with
the and the
accompanying these forms help the
employer and OSHA develop a picture of the extent
and severity of work-related incidents.
Within 7 calendar days after you receive
information that a recordable work-related injury or
illness has occurred, you must fill out this form or an
equivalent. Some state workers’ compensation,
insurance, or other reports may be acceptable
substitutes. To be considered an equivalent form,
any substitute must contain all the information
asked for on this form.
According to Public Law 91-596 and 29 CFR
1904, OSHA’s recordkeeping rule, you must keep
this form on file for 5 years following the year to
which it pertains.
If you need additional copies of this form, you
may photocopy and use as many as you need.
Injury and Illness Incident Report
Log of Work-Related Injuries and Illnesses
Summary,
Information about the case
Case number from the
Date of injury or illness
Time employee began work
Time of event Check if time cannot be determined
Date of death
Log _____________________ (Transfer the case number from the Log after you record the case.)
______ / _____ / ______
____________________
____________________
______ / _____ / ______
AM / PM
AM / PM �
What was the employee doing just before the incident occurred?
What happened?
What was the injury or illness?
What object or substance directly harmed the employee?
If the employee died, when did death occur?
Describe the activity, as well as the
tools, equipment, or material the employee was using. Be specific. “climbing a ladder while
carrying roofing materials”; “spraying chlorine from hand sprayer”; “daily computer key-entry.”
Tell us how the injury occurred. “When ladder slipped on wet floor, worker
fell 20 feet”; “Worker was sprayed with chlorine when gasket broke during replacement”; “Worker
developed soreness in wrist over time.”
Tell us the part of the body that was affected and how it was affected; be
more specific than “hurt,” “pain,” or sore.” “strained back”; “chemical burn, hand”; “carpal
tunnel syndrome.”
“concrete floor”; “chlorine”;
“radial arm saw.”
Examples:
Examples:
Examples:
Examples:
If this question does not apply to the incident, leave it blank.
Completed by
Title
Phone Date
_______________________________________________________
_________________________________________________________________
(________)_________--_____________ _____/ ______ / _____
Public reporting burden for this collection of information is estimated to average 22 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Persons are not required to respond to the
collection of information unless it displays a current valid OMB control number. If you have any comments about this estimate or any other aspects of this data collection, including suggestions for reducing this burden, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room N-3644, 200 Constitution Avenue, NW,
Washington, DC 20210. Do not send the completed forms to this office.
10)
11)
12)
13)
14)
15)
16)
17)
18)
1)
2)
3)
5)
6)
7)
8)
9)
4)
Attention: This form contains information relating toemployee health and must be used in a manner thatprotects the confidentiality of employees to the extentpossible while the information is being used foroccupational safety and health purposes.