2017 summaries of medical benefits and coverage glossary ... · 2017 summaries of medical benefits...
TRANSCRIPT

2017 SUMMARIES OF MEDICAL BENEFITS AND COVERAGE GLOSSARY OF HEALTH COVERAGE AND MEDICAL TERMS

The University of Chicago is required under Health Care Reform to provide a summary of benefits and coverage (or “SBC”) for each medical plan offered and a list of definitions designed to make it easier for you to compare your medical options.
You are receiving this booklet because you are a current employee of the University and currently participating in, or eligible to participate in, the University of Chicago’s medical plans. This information is provided to help you understand and evaluate your medical choices.
The following SBCs summarize important information about all your medical plan options to help you compare your choices before you enroll and understand your coverage after you enroll. They summarize the key features of the medical plans, such as the covered benefits, cost-sharing provisions, and coverage limitations and exceptions. The Glossary of Terms defines some of the most common medical and insurance terms. An example showing how deductibles, co-insurance, and out-of-pocket limits work together in a real-life situation is also included.
This is only a summary. If you want more details about your coverage and costs, you can get the complete terms in the policy or plan document by contacting each medical plan provider:
Maroon Plan: bcbsil.comMaroon Savings Choice: bcbsil.comHMO Illinois: bcbsil.comUCHP: uchp.uchicago.edu
If you need assistance choosing a medical plan, you may visit decisionsupportsuite.com/UChicago17. Simply answer a few questions about your benefit needs. Then in just a few minutes, The Choice Is Yours will suggest the medical plan that is right for you based on your responses. Please contact a Benefit Specialist at 773.702.9634 or [email protected] if you have any questions about this information.
Sincerely,
Maria E. Garcia Director, Health & Welfare and RetirementHuman ResourcesThe University of Chicago
University of Chicago Colleagues:

1 of 8
The University of Chicago: Maroon Plan Coverage Period: 01/01/2017 - 12/31/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: All | Plan Type: PPO
Questions: Call 1-866-390-7772 or visit us at www.bcbsil.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf or call 1-855-756-4448 to request a copy. SBC IL Non-HMO LG-2017
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plandocument by calling 1-866-390-7772 or at
Important Questions Answers Why this Matters:
What is the overall deductible?
For The University of Chicago Medical Center $300 Individual/$600 Family For PPO and Non-PPO $500 Individual/$1,000 Family Doesn't apply to prescription drugs and certain preventative care.
You must pay all the costs up to the deductible amount before this plan begins to pay for covered services you use. Check your policy or plan document to see when the deductible starts over (usually, but not always, January 1st). See the chart starting on page 2 for how much you pay for covered services after you meet the deductible.
Are there other deductibles for specific services?
Yes. $200 deductible for Non-PPO hospital admission. There are no other specific deductibles
You must pay all of the costs for these services up to the specific deductible amount before this plan begins to pay for these services.
Is there an out-of-pocket limit on my expenses?
For The University of Chicago Medical Center $1,750 Individual/$3,500 Family Yes. For PPO and Non-PPO $2,500 Individual/$5,000 Family
The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses.
What is not included in the out-of-pocket limit?
Prescription copay, premiums, balanced-billed charges, and health care this plan doesn’t cover.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Does this plan use a network of providers?
Yes. Visit www.bcbsil.com or call 1-866-390-7772 for a list of PPO providers.
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? No. You can see the specialist you choose without permission from this plan.
Are there services this plan doesn’t cover? Yes. Some of the services this plan doesn’t cover are listed on page 4. See your policy or
plan document for additional information about excluded services.
http://humanresources.uchicago.edu/benefits/healthwelfare/medical/maroon/

2 of 8
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if
the plan’s allowed amount for an overnight hospital stay is $1,000, your coinsurance payment of 20% would be $200. This may change ifyou haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than theallowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay andthe allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use PPO providers by charging you lower deductibles, copayments and coinsurance amounts.
Common Medical Event Services You May Need
Your Cost If You Use an
University of Chicago Medical Center
Provider
Your Cost If You Use a
PPO Provider
Your Cost If You Use a Non-PPO Provider
Limitations & Exceptions
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness 10% coinsurance 20% coinsurance 35% coinsurance ---none---
Specialist visit 10% coinsurance 20% coinsurance 35% coinsurance ---none---
Other practitioner office visit 10% coinsurance 20% coinsurance 35% coinsurance
Limited to 20 visits per condition; muscle manipulations subject to medical necessity review after 20 visits
Preventivecare/screening/immunization No Charge No Charge No Charge ---none---
If you have a test
Diagnostic test (x-ray, blood work) 10% coinsurance 20% coinsurance 35% coinsurance ---none---
Imaging (CT/PET scans, MRIs) 10% coinsurance 20% coinsurance 35% coinsurance ---none---

3 of 8
Common Medical Event Services You May Need
Your Cost If You Use an
University of Chicago Medical Center
Provider
Your Cost If You Use a
PPO Provider
Your Cost If You Use a Non-PPO Provider
Limitations & Exceptions
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.caremark.com or 866-873-8632.
Generic drugs
$10 copay/ prescription for up to a 30 day supply. $20 copay/ prescription for up to a 90 day supply.
$10 copay/ prescription for up to a 30 day supply. $20 copay/ prescription for up to a 90 day supply.
$10 copay/ prescription for up to a 30 day supply. $20 copay/ prescription for up to a 90 day supply
RX Out-of-Pocket Expense Limit: $2,000 Individual/$4,000 Family
Dispensing limits may apply to certain drugs.
Formulary brand drugs
$30 copay/ prescription for up to a 30 day supply. $60 copay/ prescription for up to a 90 day supply.
$30 copay/ prescription for up to a 30 day supply. $60 copay/ prescription for up to a 90 day supply.
$30 copay/ prescription for up to a 30 day supply. $60 copay/ prescription for up to a 90 day supply.
Dispensing limits may apply to certain drugs.
Non-Formulary brand drugs
$45 copay/ prescription for up to a 30 day supply. $90 copay/ prescription for up to a 90 day supply.
$45 copay/ prescription for up to a 30 day supply. $90 copay/ prescription for up to a 90 day supply.
$45 copay/ prescription for up to a 30 day supply. $90 copay/ prescription for up to a 90 day supply.
Dispensing limits may apply to certain drugs.
Specialty drugs
$75 copay/ prescription for up to a 30 day supply.
$75 copay/ prescription for up to a 30 day supply.
$75 copay/ prescription for up to a 30 day supply.
Prior authorization may be required.

4 of 8
Common Medical Event Services You May Need
Your Cost If You Use an
University of Chicago Medical Center
Provider
Your Cost If You Use a
PPO Provider
Your Cost If You Use a Non-PPO Provider
Limitations & Exceptions
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) 10% coinsurance 20% coinsurance 35% coinsurance ---none---
Physician/surgeon fees 10% coinsurance 20% coinsurance 35% coinsurance ---none---
If you need immediate medical attention
Emergency room services 10% coinsurance 20% coinsurance 20% coinsurance ---none--- Emergency medical transportation 20% coinsurance 20% coinsurance 20% coinsurance Limited to local ground or air
transportation. Urgent care 10% coinsurance 20% coinsurance 35% coinsurance ---none---
If you have a hospital stay
Facility fee (e.g., hospital room) 10% coinsurance 20% coinsurance 35% coinsurance $200 deductible per admissionfor Non-PPO providers.
Physician/surgeon fee 10% coinsurance 20% coinsurance 35% coinsurance ---none---
If you have mental health, behavioral health, or substance abuse needs
Mental/Behavioral health outpatient services 10% coinsurance 20% coinsurance 35% coinsurance ---none---
Mental/Behavioral health inpatient services 10% coinsurance 20% coinsurance 35% coinsurance $200 deductible per admission
for Non-PPO providers. Substance use disorder outpatient services 10% coinsurance 20% coinsurance 35% coinsurance ---none---
Substance use disorder inpatient services 10% coinsurance 20% coinsurance 35% coinsurance $200 deductible per admission
for Non-PPO providers.
If you are pregnant
Prenatal and postnatal care No Charge 20% coinsurance 35% coinsurance Covered at 100% afterdeductible at UCMC.
Delivery and all inpatient services No Charge 20% coinsurance 35% coinsurance
Covered at 100% after deductible at UCMC. $200 deductible per admission for Non-PPO providers.

5 of 8
Common Medical Event Services You May Need
Your Cost If You Use an
University of Chicago Medical Center
Provider
Your Cost If You Use a
PPO Provider
Your Cost If You Use a Non-PPO Provider
Limitations & Exceptions
If you need help recovering or have other special health needs
Home health care No Charge No Charge No Charge Limited to 120 visits per benefit period; precertification required.
Rehabilitation services 10% coinsurance 20% coinsurance 35% coinsurance Limited to 20 visits per condition; subject to medical necessity review after 20 visits. Habilitation services 10% coinsurance 20% coinsurance 35% coinsurance
Skilled nursing care No Charge No Charge No Charge Limited to 120 days per benefit period; precertification required.
Durable medical equipment 10% coinsurance 20% coinsurance 35% coinsurance
Benefits are limited to items used to serve a medical purpose. DME benefits are provided for both purchase and rental equipment (up to the purchase price).
Hospice service No Charge No Charge No Charge ---none---
If your child needs dental or eye care
Eye exam Not Covered Not Covered Not Covered ---none---
Glasses Not Covered Not Covered Not Covered ---none---
Dental check-up Not Covered Not Covered Not Covered ---none---
Excluded Services & Other Covered Services:
Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture Cosmetic Surgery Dental Care (Adult)
Hearing Aids Long Term Care Routine Eye Care (Adult)
Routine Foot Care (with the exception ofperson with diagnosis of diabetes)
Weight Loss Programs

6 of 8
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Bariatric Surgery Chiropractic Care
Infertility Treatment Most coverage provided outside the
United States. See www.bcbsil.com
Non-Emergency Care When TravelingOutside the U.S.
Private Duty Nursing (with the exceptionof inpatient private duty nursing)
Your Rights to Continue Coverage: If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply. For more information on your rights to continue coverage, contact the plan at 1-866-390-7772. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact Blue Cross and Blue Shield of Illinois at 1-866-390-7772 or visit www.bcbsil.com, or contact the U.S Department of Labor's Employee Benefits Security Administration at 1-866-444-EBSA (3272) or visit www.dol.gov/ebsa/healthreform. Additionally, a consumer assistance program can help you file your appeal. Contact the Illinois Department of Insurance at (877) 527-9431 or visit http://insurance.illinois.gov.
Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Language Access Services:Spanish (Español): Para obtener asistencia en Español, llame al 1-866-390-7772. Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-866-390-7772. Chinese (中文): 如果需要中文的帮助,请拨打这个号码1-866-390-7772.Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-866-390-7772.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––

7 of 8
Having a baby (normal delivery)
Managing type 2 diabetes (routine maintenance of
a well-controlled condition)
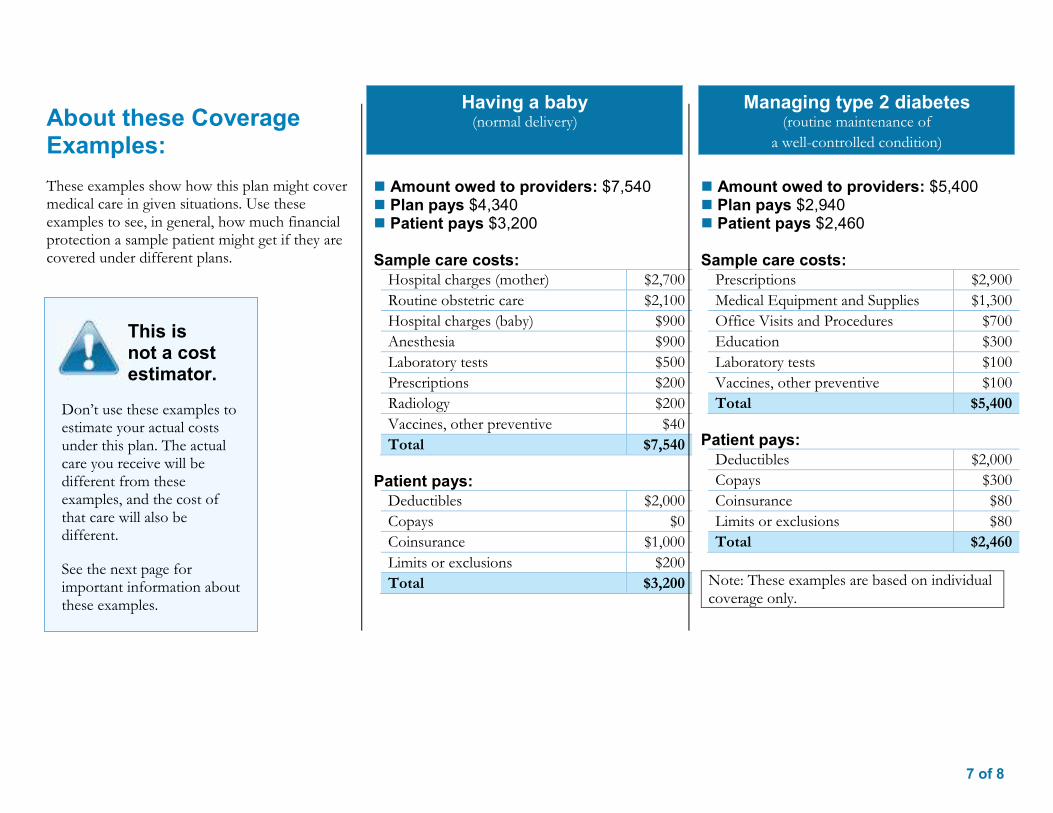
About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays $5,030 Patient pays $2,010
Sample care costs: Hospital charges (mother) $2,700 Routine obstetric care $2,100 Hospital charges (baby) $900 Anesthesia $900 Laboratory tests $500 Prescriptions $200 Radiology $200 Vaccines, other preventive $40 Total $7,540
Patient pays: Deductibles $500 Copays $10 Coinsurance $1,350 Limits or exclusions $200 Total $2,010
Amount owed to providers: $5,400 Plan pays $4,120 Patient pays $1,280
Sample care costs: Prescriptions $2,900 Medical Equipment and Supplies $1,300 Office Visits and Procedures $700 Education $300 Laboratory tests $100 Vaccines, other preventive $100 Total $5,400
Patient pays: Deductibles $500 Copays $300 Coinsurance $400 Limits or exclusions $80 Total $1,280
Note: These examples are based on individual coverage only.
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.

8 of 8 Questions: Call 1-866-390-7772 or visit us at www.bcbsil.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf or call 1-855-756-4448 to request a copy.
Questions and answers about the Coverage Examples:
What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S.Department of Health and HumanServices, and aren’t specific to aparticular geographic area or health plan.
The patient’s condition was not anexcluded or preexisting condition.
All services and treatments started andended in the same coverage period.
There are no other medical expenses forany member covered under this plan.
Out-of-pocket expenses are based onlyon treating the condition in the example.
The patient received all care from in-network providers. If the patient hadreceived care from out-of-networkproviders, costs would have been higher.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples.The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not costestimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary ofBenefits and Coverage for other plans,you’ll find the same Coverage Examples.When you compare plans, check the“Patient Pays” box in each example. Thesmaller that number, the more coveragethe plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premiumyou pay. Generally, the lower yourpremium, the more you’ll pay in out-of-pocket costs, such as copayments,deductibles, and coinsurance. Youshould also consider contributions toaccounts such as health savings accounts(HSAs), flexible spending arrangements(FSAs) or health reimbursement accounts(HRAs) that help you pay out-of-pocketexpenses.

1 of 8
The University of Chicago: Maroon Savings Choice HSA Plan Coverage Period: 01/01/2017 - 12/31/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: All | Plan Type: HSA
Questions: Call 1-866-390-7772 or visit us at www.bcbsil.com . If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf or call 1-855-756-4448 to request a copy. SBC IL Non-HMO LG-2017
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plandocument by calling 1-866-390-7772 or at
Important Questions Answers Why this Matters:
What is the overall deductible?
For PPO $2,000 Individual/ $4,000 Family For Non-PPO $4,000 Individual/ $8,000 Family Doesn't apply to prescription drugs and certain preventative care.
You must pay all the costs up to the deductible amount before this plan begins to pay for covered services you use. Check your policy or plan document to see when the deductible starts over (usually, but not always, January 1st). See the chart starting on page 2 for how much you pay for covered services after you meet the deductible.
Are there other deductibles for specific services?
Yes. $200 deductible for Non-PPO hospital admission. There are no other specific deductibles
You must pay all of the costs for these services up to the specific deductible amount before this plan begins to pay for these services.
Is there an out-of-pocket limit on my expenses?
Yes. For PPO $3,000 Individual/ $6,000 Family For Non-PPO $6,000 Individual/ $12,000 Family
The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses.
What is not included in the out-of-pocket limit?
Premiums, balanced-billed charges, and health care this plan doesn’t cover.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Does this plan use a network of providers?
Yes. Visit www.bcbsil.com or call 1-866-390-7772 for a list of PPO providers.
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? No. You can see the specialist you choose without permission from this plan.
Are there services this plan doesn’t cover? Yes. Some of the services this plan doesn’t cover are listed on page 5. See your policy or plan
document for additional information about excluded services.
http://humanresources.uchicago.edu/benefits/healthwelfare/medical/maroonsavingschoice/

2 of 8
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if
the plan’s allowed amount for an overnight hospital stay is $1,000, your coinsurance payment of 20% would be $200. This may change ifyou haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than theallowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay andthe allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use PPO providers by charging you lower deductibles, copayments and coinsurance amounts.
Common Medical Event Services You May Need
Your Cost If You Use an
PPO Provider
Your Cost If You Use an Non-PPO Provider
Limitations & Exceptions
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness 20% coinsurance 35% coinsurance ---none---
Specialist visit 20% coinsurance 35% coinsurance ---none---
Other practitioner office visit 20% coinsurance 35% coinsurance Limited to 20 visits per condition; muscle manipulations subject to medical necessity review after 20 visits.
Preventive care/screening/immunization No Charge No Charge ---none---
If you have a test Diagnostic test (x-ray, blood work) 20% coinsurance 35% coinsurance ---none---
Imaging (CT/PET scans, MRIs) 20% coinsurance 35% coinsurance ---none---

3 of 8
Common Medical Event Services You May Need
Your Cost If You Use an
PPO Provider
Your Cost If You Use an Non-PPO Provider
Limitations & Exceptions
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at caremark.com
Generic drugs
$10 copay/ prescription for up to a 30 day supply.
$20 copay/ prescription for up to a 90 day supply.
$10 copay/ prescription for up to a 30 day supply.
$20 copay/ prescription for up to a 90 day supply.
RX Out-of-Pocket Expense Limit $3,000 Individual/ $6,000 Family combined with medical.
Copay for Preventative Drugs before and after Deductible is met. Copay for Non-Preventative Drurgs only after Deductible is met. Dispensing limits may apply to certain drugs.
Formulary brand drugs
$30 copay/ prescription for up to a 30 day supply.
$60 copay/ prescription for up to a 90 day supply.
$30 copay/ prescription for up to a 30 day supply.
$60 copay/ prescription for up to a 90 day supply.
Copay for Preventative Drugs before and after Deductible is met. Copay for Non-Preventative Drurgs only after Deductible is met. Dispensing limits may apply to certain drugs.
Non-Formulary brand drugs
$45 copay/ prescription for up to a 30 day supply.
$90 copay/ prescription for up to a 90 day supply.
$45 copay/ prescription for up to a 30 day supply.
$90 copay/ prescription for up to a 90 day supply.
Copay for Preventative Drugs before and after Deductible is met. Copay for Non-Preventative Drurgs only after Deductible is met. Dispensing limits may apply to certain drugs.
Specialty drugs $75 copay/ prescription for up to a 30 day supply.
$75 copay/ prescription for up to a 30 day supply.
Prior authorization may be required.
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) 20% coinsurance 35% coinsurance ---none---
Physician/surgeon fees 20% coinsurance 35% coinsurance ---none---

4 of 8
Common Medical Event Services You May Need
Your Cost If You Use an
PPO Provider
Your Cost If You Use an Non-PPO Provider
Limitations & Exceptions
If you need immediate medical attention
Emergency room services 20% coinsurance 20% coinsurance ---none---
Emergency medical transportation 20% coinsurance 20% coinsurance Limited to local ground or airtransportation.
Urgent care 20% coinsurance 35% coinsurance ---none---
If you have a hospital stay
Facility fee (e.g., hospital room) 20% coinsurance 35% coinsurance $200 deductible per admission forNon-PPO providers.
Physician/surgeon fee 20% coinsurance 35% coinsurance ---none---
If you have mental health, behavioral health, or substance abuse needs
Mental/Behavioral health outpatient services 20% coinsurance 35% coinsurance ---none---
Mental/Behavioral health inpatient services 20% coinsurance 35% coinsurance $200 deductible per admission forNon-PPO providers.
Substance use disorder outpatient services 20% coinsurance 35% coinsurance ---none---
Substance use disorder inpatient services 20% coinsurance 35% coinsurance $200 deductible per admission forNon-PPO providers.
If you are pregnant Prenatal and postnatal care 20% coinsurance 35% coinsurance ---none---
Delivery and all inpatient services 20% coinsurance 35% coinsurance $200 deductible per admission forNon-PPO providers.
If you need help recovering or have other special health needs
Home health care No Charge No Charge Limited to 120 visits per benefit period; precertification required.
Rehabilitation services 20% coinsurance 35% coinsurance Limited to 20 visits per condition; subject to medical necessity review after 20 visits. Habilitation services 20% coinsurance 35% coinsurance
Skilled nursing care No Charge No Charge Limited to 120 days per benefit period; precertification required.
Durable medical equipment 20% coinsurance 35% coinsurance
Benefits are limited to items used to serve a medical purpose. DME benefits are provided for both purchase and rental equipment (up to the purchase price).
Hospice service No Charge No Charge ---none---

5 of 8
Common Medical Event Services You May Need
Your Cost If You Use an
PPO Provider
Your Cost If You Use an Non-PPO Provider
Limitations & Exceptions
If your child needs dental or eye care
Eye exam Not Covered Not Covered ---none---
Glasses Not Covered Not Covered ---none---
Dental check-up Not Covered Not Covered ---none---
Excluded Services & Other Covered Services:
Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture Cosmetic Surgery Dental Care (Adult)
Hearing Aids Long Term Care Routine Eye Care (Adult)
Routine Foot Care (with the exception ofperson with diagnosis of diabetes)
Weight Loss Programs
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Bariatric Surgery Chiropractic Care
Infertility Treatment Most coverage provided outside the
United States. See www.bcbsil.com
Non-Emergency Care When TravelingOutside the U.S.
Private Duty Nursing (with the exceptionof inpatient private duty nursing)
Your Rights to Continue Coverage: If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply.For more information on your rights to continue coverage, contact the plan at 1-866-390-7772. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.

6 of 8
Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact Blue Cross and Blue Shield of Illinois at 1-866-390-7772 or visit www.bcbsil.com, or contact the U.S Department of Labor's Employee Benefits Security Administration at 1-866-444-EBSA (3272) or visit www.dol.gov/ebsa/healthreform. Additionally, a consumer assistance program can help you file your appeal. Contact the Illinois Department of Insurance at (877) 527-9431 or visit http://insurance.illinois.gov.
Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Language Access Services:Spanish (Español): Para obtener asistencia en Español, llame al 1-866-390-7772.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-866-390-7772.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码1-866-390-7772.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-866-390-7772. ––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––
7 of 8
Having a baby (normal delivery)
Managing type 2 diabetes (routine maintenance of
a well-controlled condition) About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays $4,340 Patient pays $3,200
Sample care costs: Hospital charges (mother) $2,700 Routine obstetric care $2,100 Hospital charges (baby) $900 Anesthesia $900 Laboratory tests $500 Prescriptions $200 Radiology $200 Vaccines, other preventive $40 Total $7,540
Patient pays: Deductibles $2,000 Copays $0 Coinsurance $1,000 Limits or exclusions $200 Total $3,200
Amount owed to providers: $5,400 Plan pays $2,940 Patient pays $2,460
Sample care costs: Prescriptions $2,900 Medical Equipment and Supplies $1,300 Office Visits and Procedures $700 Education $300 Laboratory tests $100 Vaccines, other preventive $100 Total $5,400
Patient pays: Deductibles $2,000 Copays $300 Coinsurance $80 Limits or exclusions $80 Total $2,460
Note: These examples are based on individual coverage only.
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.
8 of 8 Questions: Call 1-866-390-7772 or visit us at www.bcbsil.com . If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf or call 1-855-756-4448 to request a copy.
Questions and answers about the Coverage Examples:
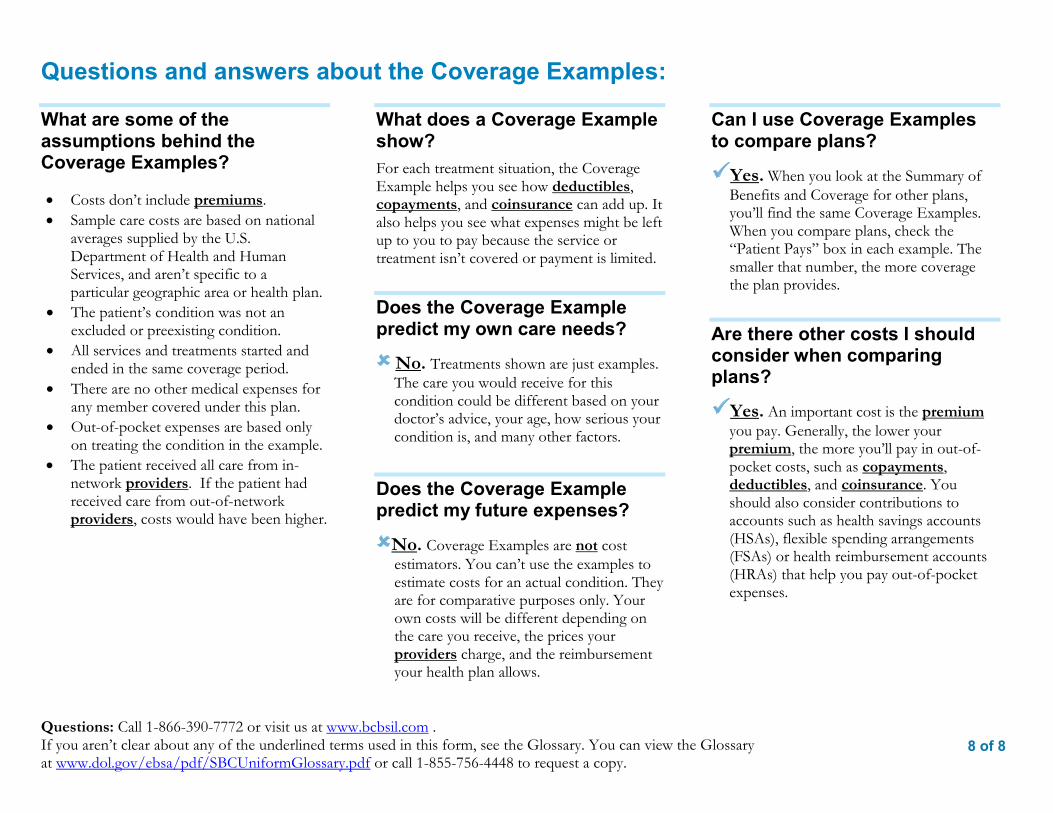
What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S.Department of Health and HumanServices, and aren’t specific to aparticular geographic area or health plan.
The patient’s condition was not anexcluded or preexisting condition.
All services and treatments started andended in the same coverage period.
There are no other medical expenses forany member covered under this plan.
Out-of-pocket expenses are based onlyon treating the condition in the example.
The patient received all care from in-network providers. If the patient hadreceived care from out-of-networkproviders, costs would have been higher.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples.The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not costestimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary ofBenefits and Coverage for other plans,you’ll find the same Coverage Examples.When you compare plans, check the“Patient Pays” box in each example. Thesmaller that number, the more coveragethe plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premiumyou pay. Generally, the lower yourpremium, the more you’ll pay in out-of-pocket costs, such as copayments,deductibles, and coinsurance. Youshould also consider contributions toaccounts such as health savings accounts(HSAs), flexible spending arrangements(FSAs) or health reimbursement accounts(HRAs) that help you pay out-of-pocketexpenses.
1 of 8
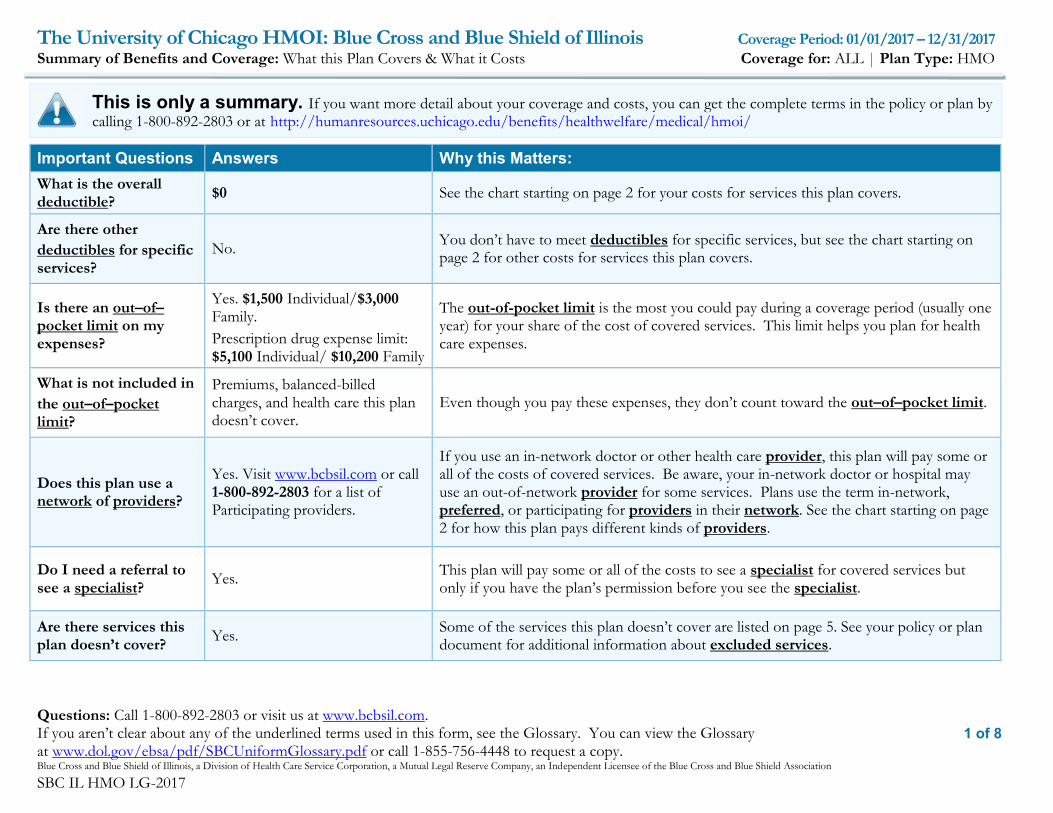
The University of Chicago HMOI: Blue Cross and Blue Shield of Illinois Coverage Period: 01/01/2017 – 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: ALL | Plan Type: HMO
Questions: Call 1-800-892-2803 or visit us at www.bcbsil.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf or call 1-855-756-4448 to request a copy. Blue Cross and Blue Shield of Illinois, a Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association
SBC IL HMO LG-2017
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan bycalling 1-800-892-2803 or at
Important Questions Answers Why this Matters: What is the overall deductible? $0 See the chart starting on page 2 for your costs for services this plan covers.
Are there other deductibles for specific services?
No. You don’t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
Is there an out–of–pocket limit on my expenses?
Yes. $1,500 Individual/$3,000 Family. Prescription drug expense limit: $5,100 Individual/ $10,200 Family
The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses.
What is not included in the out–of–pocket limit?
Premiums, balanced-billed charges, and health care this plan doesn’t cover.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Does this plan use a network of providers?
Yes. Visit www.bcbsil.com or call 1-800-892-2803 for a list of Participating providers.
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? Yes. This plan will pay some or all of the costs to see a specialist for covered services but
only if you have the plan’s permission before you see the specialist.
Are there services this plan doesn’t cover? Yes. Some of the services this plan doesn’t cover are listed on page 5. See your policy or plan
document for additional information about excluded services.
http://humanresources.uchicago.edu/benefits/healthwelfare/medical/hmoi/

2 of 8
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if
the plan’s allowed amount for an overnight hospital stay is $1,000, your coinsurance payment of 20% would be $200. This may change ifyou haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than theallowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay andthe allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use Participating providers by charging you lower deductibles, copayments and coinsurance amounts.
Common Medical Event Services You May Need
Your Cost If You Use a Participating
Provider
Your Cost If You Use a
Non-Participating Provider
Limitations & Exceptions
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness $25 copay/visit Not Covered
Services or supplies that are not ordered by your Primary Care Physician or Women’s Principal Health Care Provider, except emergency and routine vision exams, are not covered.
Specialist visit $45 copay/visit Not Covered Referral required.
Other practitioner office visit $25 copay/visit Not Covered Referral required.
Preventive care/screening/immunization No Charge Not Covered ---none---
If you have a test Diagnostic test (x-ray, blood work) No Charge Not Covered Referral required.
Imaging (CT/PET scans, MRIs) No Charge Not Covered Referral required.

3 of 8
Common Medical Event Services You May Need
Your Cost If You Use a Participating
Provider
Your Cost If You Use a
Non-Participating Provider
Limitations & Exceptions
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.bcbsil.com.
Generic drugs
$10 copay / prescription for up to a 34 day supply. $20 copay / prescription for up to a 90 day supply.
Not Covered Dispensing limit may apply to certain drugs.
Certain women’s preventative services will be covered with no cost to the member. For a full list of these prescriptions and/or services, please contact Customer Service.
34 day retail / 90 day mail.
RX Out-of-Pocket Expense Limit: $5,100 Individual/ $10,200 Family
Formulary brand drugs
$30 copay / prescription for up to a 34 day supply. $60 copay / prescription for up to a 90 day supply.
Not Covered
Non-Formulary brand drugs
$45 copay / prescription for up to a 34 day supply. $90 copay / prescription for up to a 90 day supply.
Not Covered
Specialty drugs $75 copay/ prescription for up to a 34 day supply.
Not Covered Coverage based on group policy. Prior authorization may be required.
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) No Charge Not Covered Referral required.
Physician/surgeon fees No Charge Not Covered Referral required.
If you need immediate medical attention
Emergency room services $125 copay/visit $125 copay/visit Copay waived if admitted.
Emergency medical transportation No Charge No Charge Ground transportation only.
Urgent care $25 copay/visit Not Covered Must be affiliated with member’s chosen medical group or referral required.

4 of 8
Common Medical Event Services You May Need
Your Cost If You Use a Participating
Provider
Your Cost If You Use a
Non-Participating Provider
Limitations & Exceptions
If you have a hospital stay
Facility fee (e.g., hospital room) $350 copay/ admission Not Covered Referral required.
Physician/surgeon fee No Charge Not Covered Referral required.
If you have mental health, behavioral health, or substance abuse needs
Mental/Behavioral health outpatient services $25 copay/visit Not Covered Unlimited visits.
Referral required.
Mental/Behavioral health inpatient services $350 copay/admission Not Covered Unlimited days.
Referral required.
Substance use disorder outpatient services $25 copay/visit Not Covered Use a plan provider only. Referral required.
Substance use disorder inpatient services $350 copay/ admission Not Covered Unlimited days.
Referral required.
If you are pregnant Prenatal and postnatal care $25 copay/visit Not Covered Copay applies for the 1st prenatal
visit only.
Delivery and all inpatient services $350 copay/ admission Not Covered ---none---
If you need help recovering or have other special health needs
Home health care No Charge Not Covered Referral required. Rehabilitation services $25 copay/visit Not Covered 60 treatments combined for all
therapies. Referral required. Habilitation services $25 copay/visit Not Covered
Skilled nursing care $350 copay/ admission Not Covered Excludes custodial care.
Referral required.
Durable medical equipment No Charge Not Covered
Referral required. Benefits are limited to items used to serve a medical purpose. DME benefits are provided for both purchase and rental equipment (up to the purchase price).
Hospice service $350 copay/ admission Not Covered Inpatient copay may apply.
Referral required.
5 of 8
Common Medical Event Services You May Need
Your Cost If You Use a Participating
Provider
Your Cost If You Use a
Non-Participating Provider
Limitations & Exceptions
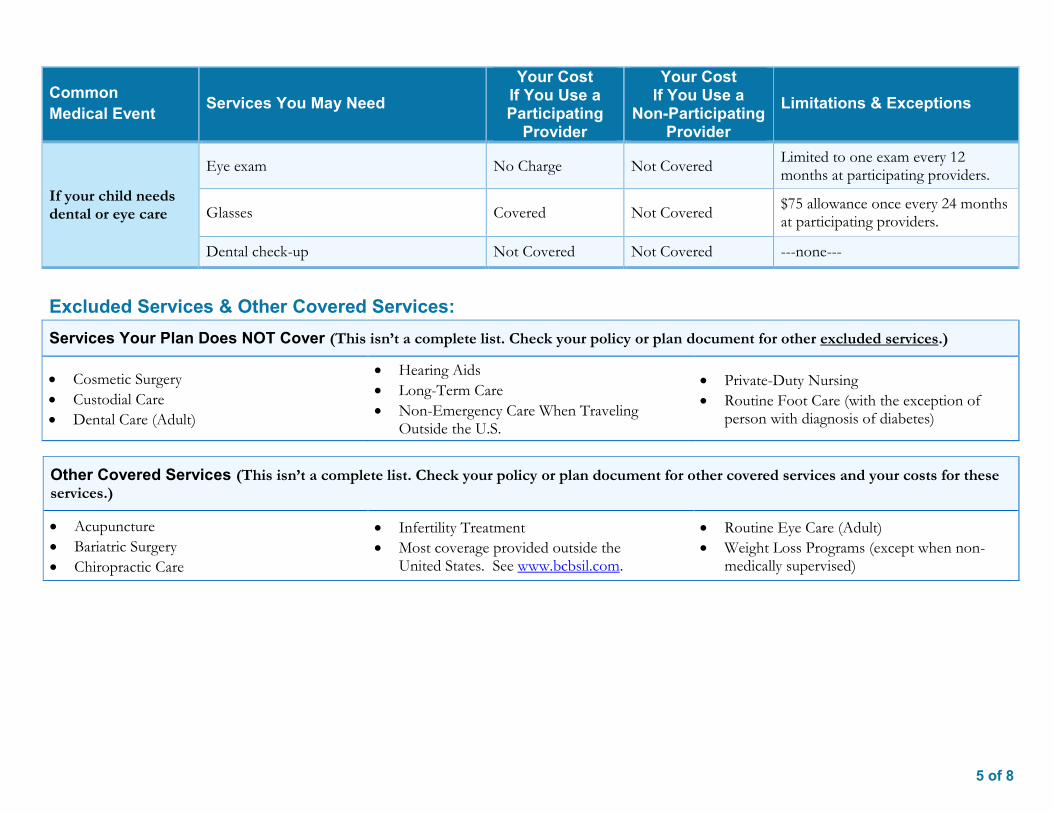
If your child needs dental or eye care
Eye exam No Charge Not Covered Limited to one exam every 12 months at participating providers.
Glasses Covered Not Covered $75 allowance once every 24 months at participating providers.
Dental check-up Not Covered Not Covered ---none---
Excluded Services & Other Covered Services: Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Cosmetic Surgery Custodial Care Dental Care (Adult)
Hearing Aids Long-Term Care Non-Emergency Care When Traveling
Outside the U.S.
Private-Duty Nursing Routine Foot Care (with the exception of
person with diagnosis of diabetes)
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Acupuncture Bariatric Surgery Chiropractic Care
Infertility Treatment Most coverage provided outside the
United States. See www.bcbsil.com.
Routine Eye Care (Adult) Weight Loss Programs (except when non-
medically supervised)

6 of 8
Your Rights to Continue Coverage: If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply.
For more information on your rights to continue coverage, contact the plan at 1-800-892-2803. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa, or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact Blue Cross and Blue Shield of Illinois at 1-800-892-2803 or visit www.bcbsil.com, or contact the U.S Department of Labor's Employee Benefits Security Administration at 1-866-444-EBSA (3272) or visit www.dol.gov/ebsa/healthreform. Additionally, a consumer assistance program can help you file your appeal. Contact the Illinois Department of Insurance at (877) 527-9431 or visit http://insurance.illinois.gov.
Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Language Access Services:Spanish (Español): Para obtener asistencia en Español, llame al 1-800-892-2803.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-800-892-2803.
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-800-892-2803.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-800-892-2803.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––

7 of 8
Having a Baby (normal delivery)
Managing Type 2 Diabetes (routine maintenance of
a well-controlled condition)
gener
About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays $6,640 Patient pays $900
Sample care costs: Hospital charges (mother) $2,700 Routine obstetric care $2,100 Hospital charges (baby) $900 Anesthesia $900 Laboratory tests $500 Prescriptions $200 Radiology $200 Vaccines, other preventive $40 Total $7,540
Patient pays: Deductibles $0 Copays $700 Coinsurance $0 Limits or exclusions $200 Total $900
Amount owed to providers: $5,400 Plan pays $4,620 Patient pays $780
Sample care costs: Prescriptions $2,900 Medical Equipment and Supplies $1,300 Office Visits and Procedures $700 Education $300 Laboratory tests $100 Vaccines, other preventive $100 Total $5,400
Patient pays: Deductibles $0 Copays $700 Coinsurance $0 Limits or exclusions $80 Total $780
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.

8 of 8 Questions: Call 1-866-390-7772 or visit us at www.bcbsil.com . If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf or call 1-855-756-4448 to request a copy.
Questions and answers about the Coverage Examples:
What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S.Department of Health and HumanServices, and aren’t specific to aparticular geographic area or health plan.
The patient’s condition was not anexcluded or preexisting condition.
All services and treatments started andended in the same coverage period.
There are no other medical expenses forany member covered under this plan.
Out-of-pocket expenses are based onlyon treating the condition in the example.
The patient received all care from in-network providers. If the patient hadreceived care from out-of-networkproviders, costs would have been higher.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples.The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not costestimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary ofBenefits and Coverage for other plans,you’ll find the same Coverage Examples.When you compare plans, check the“Patient Pays” box in each example. Thesmaller that number, the more coveragethe plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premiumyou pay. Generally, the lower yourpremium, the more you’ll pay in out-of-pocket costs, such as copayments,deductibles, and coinsurance. Youshould also consider contributions toaccounts such as health savings accounts(HSAs), flexible spending arrangements(FSAs) or health reimbursement accounts(HRAs) that help you pay out-of-pocketexpenses.

1 of 8
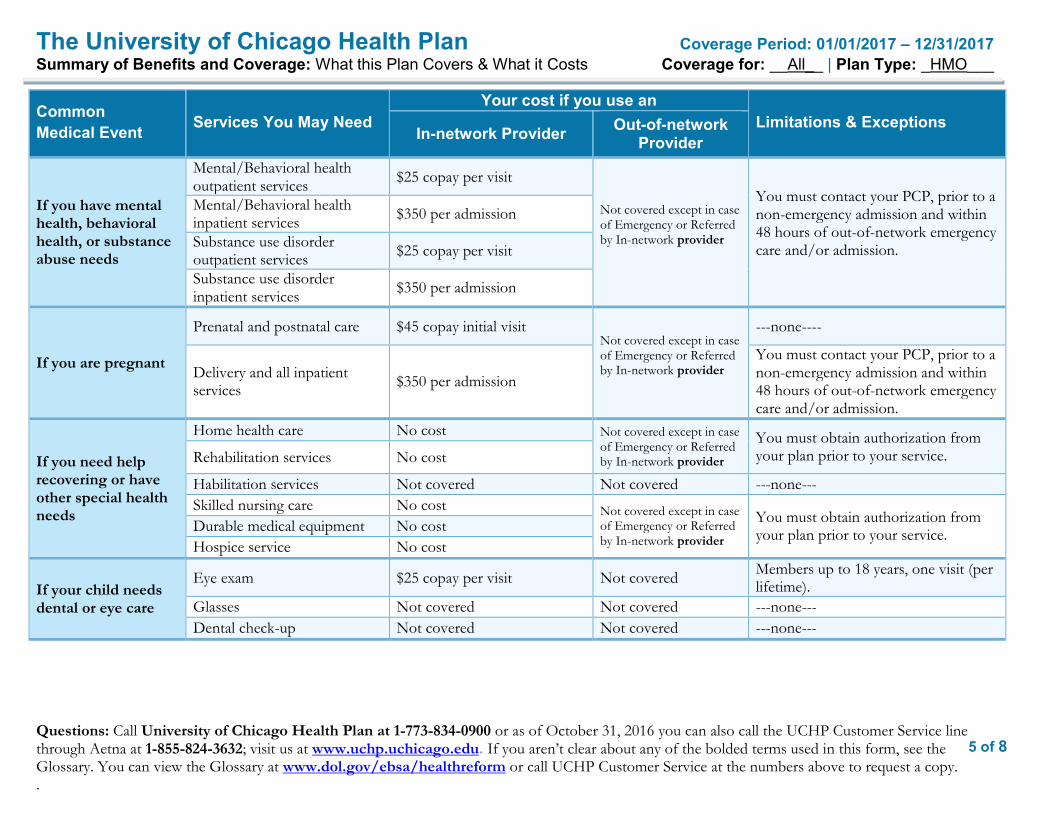
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: __All__ | Plan Type: _HMO___
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plandocument at www.uchp.uchicago.edu .or by calling 1-773-834-0900. Effective January 1, 2017, UCHP will contract with Aetna to administer the UCHP benefits. As the UCHP administrator, Aetna will provide customer service and medical management services on behalf of UCHP. Starting October 31, 2016 you can also reach the UCHP Customer Service line through Aetna at 1-855-824-3632.
Important Questions Answers Why this Matters: What is the overall deductible? $0.00 See the chart starting on Page 2 for your costs for services this plan covers.
Are there other deductibles for specific services?
No You don’t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for service the plan covers.
Is there an out–of–pocket limit on my expenses?
Yes There is a limit for out of pocket expenses for in-network services of $1,500 for an individual and $3,000 for a family.
What is not included in the out–of–pocket limit?
Out of pocket expenses for out of network services.
Obtaining Authorized Covered services from in-network providers will minimize your out of pocket expenses.
Is there an overall annual limit on what the plan pays?
No The chart starting on page 2 describes any limits on what the plan will pay for specific covered services, such as office visits.
Does this plan use a network of providers?
Yes. For the list of University of Chicago Physicians, see www.uchospitals.edu or call 773-834-0900 or the UCHP Customer Service line through Aetna at 1-855-824-3632
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? Yes This plan will pay some or all of the costs to see a specialist for covered services but only
if you have plan’s permission before you see the specialist. Are there services this plan doesn’t cover? Yes Some of the services that this plan doesn’t cover are listed on page 6. See your policy or
plan document for additional information about excluded services.

2 of 8
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: __All__ | Plan Type: _HMO___
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Co-payments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Co-insurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if
the plan’s allowed amount for an overnight hospital stay is $1,000, your co-insurance payment of 20% would be $200. This may change ifyou haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than theallowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay andthe allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use in-network providers by charging you lower deductibles, co-payments and co-insurance amounts.
Common Medical Event Services You May Need
Your cost if you use an Limitations & Exceptions
In-network Provider Out-of-network Provider
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness $25 copay per visit
Not covered except in case of Emergency or Referred by In-network provider
----none----
Specialist visit $45 copay per visit Not covered except in case of Emergency or Referred by In-network provider
You must obtain authorization from your plan prior to visiting a specialist.
Other practitioner office visit Not covered Not covered
Preventivecare/screening/immunization No cost
Not covered except in case of Emergency or Referred by In-network provider
Prior authorization must be obtained before screening can be performed by out-of-network provider.
If you have a test
Diagnostic test (x-ray, blood work) No cost
Not covered except in case of Emergency or Referred by In-network provider
Prior authorization must be obtained before testing can be performed by out-of-network provider.
Imaging (CT/PET scans, MRIs) No cost
Not covered except in case of Emergency or Referred by In-network provider
Prior authorization must be obtained before testing can be performed by out-of-network provider.

3 of 8
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: __All__ | Plan Type: _HMO___
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Common Medical Event Services You May Need
Your cost if you use an Limitations & Exceptions
In-network Provider Out-of-network Provider
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.uchp.uchicago.edu
Generic drugs
$5 copay/prescription for 30 day order at DCAM. $10 copay/prescription for 30 day order at a retail pharmacy (i.e. CVS). $10 copay/prescription for 90 day order at DCAM. $20 copay/prescription for 90 day order with CVS Caremark Mail Order.
Not covered except in case of Emergency or Referred by In-network provider
Members filling orders at a retail pharmacy (CVS) will receive two prescription fills at the copayment amount.
The third fill the member’s cost will 50% of the medication cost.
Preferred brand drugs
$15 copay/prescription for 30 day order at DCAM. $30 copay/prescription for 30 day order at a retail pharmacy (i.e. CVS). $30 copay/prescription for 90 day order at DCAM. $60 copay/prescription for 90 day order with CVS Caremark Mail Order.
Not covered except in case of Emergency or Referred by In-network provider
Non-preferred brand drugs
$30 copay/prescription for 30 day order at DCAM. $45 copay/prescription for 30 day order at a retail pharmacy (i.e. CVS). $60 copay/prescription for 90 day order at DCAM. $90 copay/prescription for 90 day order with CVS Caremark Mail Order.
Not covered except in case of Emergency or Referred by In-network provider
Specialty drugs $75 copay/prescription for 30 day order
Not covered except in case of Emergency or Referred by In-network provider
Drugs used for treatment of infertility, impotence and smoking deterrents have plan limitations.
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) No cost
Not covered except in case of Emergency or Referred by In-network provider
You must obtain authorization from your plan prior to your service.
Physician/surgeon fees No cost

4 of 8
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: __All__ | Plan Type: _HMO___
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Common Medical Event Services You May Need
Your cost if you use an Limitations & Exceptions
In-network Provider Out-of-network Provider
If you need immediate medical attention
Emergency room services $125 copay per visit (copay waived if admitted)
$125 copay per visit (copay waived if admitted)
Out of network emergency care is eligible with an urgent condition or for a life threatening or severe emergency condition. Contact your PCP after any emergency room visit.
Emergency medical transportation No cost
Not covered except in case of Emergency or Referred by In-network provider
None
Urgent care $45 copay per visit $45 copay per visit
Both in network and out of network urgent care is eligible with an urgent condition. In network providers include, University of Chicago Hospitals or CVS Minute Clinics located within the 10 County Chicago Metropolitan Area and Northwest Indiana (Lake, Porter, LaPorte Counties). For both in network and out of network urgent care,.you or your representative must contact your PCP prior to seeking services or within 24 hours if prior notification is not feasible.
If you have a hospital stay
Facility fee (e.g., hospital room) $350 per admission
Not covered except in case of Emergency or Referred by In-network provider
Prior to your non-emergency inpatient admission, your attending physician should obtain approval from UCHP. For out-of-network emergency care and/or inpatient admission you or your representative must contact your PCP within 48 hours of out-of-network emergency care and/or admission.
Physician/surgeon fee No cost
5 of 8
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: __All__ | Plan Type: _HMO___
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Common Medical Event Services You May Need
Your cost if you use an Limitations & Exceptions
In-network Provider Out-of-network Provider
If you have mental health, behavioral health, or substance abuse needs
Mental/Behavioral health outpatient services $25 copay per visit
Not covered except in case of Emergency or Referred by In-network provider
You must contact your PCP, prior to a non-emergency admission and within 48 hours of out-of-network emergency care and/or admission.
Mental/Behavioral health inpatient services $350 per admission
Substance use disorder outpatient services $25 copay per visit
Substance use disorder inpatient services $350 per admission
If you are pregnant
Prenatal and postnatal care $45 copay initial visit Not covered except in case of Emergency or Referred by In-network provider
---none----
Delivery and all inpatient services $350 per admission
You must contact your PCP, prior to a non-emergency admission and within 48 hours of out-of-network emergency care and/or admission.
If you need help recovering or have other special health needs
Home health care No cost Not covered except in case of Emergency or Referred by In-network provider
You must obtain authorization from your plan prior to your service. Rehabilitation services No cost
Habilitation services Not covered Not covered ---none--- Skilled nursing care No cost Not covered except in case
of Emergency or Referred by In-network provider
You must obtain authorization from your plan prior to your service. Durable medical equipment No cost
Hospice service No cost
If your child needs dental or eye care
Eye exam $25 copay per visit Not covered Members up to 18 years, one visit (per lifetime).
Glasses Not covered Not covered ---none--- Dental check-up Not covered Not covered ---none---

6 of 8
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: __All__ | Plan Type: _HMO___
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Excluded Services & Other Covered Services: Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture Chiropractic care Cosmetic surgery Dental care (adult & children)
Habilitation services Hearing aids Long term care Non-emergency care when traveling outside of the U.S.
Private duty nursing Routine foot care Weight loss programs
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Infertility Bariatric surgery
Your Rights to Continue Coverage: If you lose coverage under the plan, then, depending upon circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue may also apply.
For more information on your rights to continue coverage, contact the plan at 1-773-834-0900 or as of October 31, 2016 the UCHP Customer Service line through Aetna at 1-855-824-3632. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa, or the U.S. Department of Health and Human Services at 1-877-267-2323 x 61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact: Customer Service Representative at 1-773-834-0900 or as of October 31, 2016 the UCHP Customer Service line through Aetna at 1-855-824-3632.
Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage”. This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Language Access Services: Spanish (Español): Para obtener asistencia en Español, llame al 1-773-834-0900, o llame al 1-855-824-3632. For all other language access needs call 1-773-834-0900 or as of October 31, 2016 the UCHP Customer Service line through Aetna at 1-855-824-3632.
–––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––
7 of 8
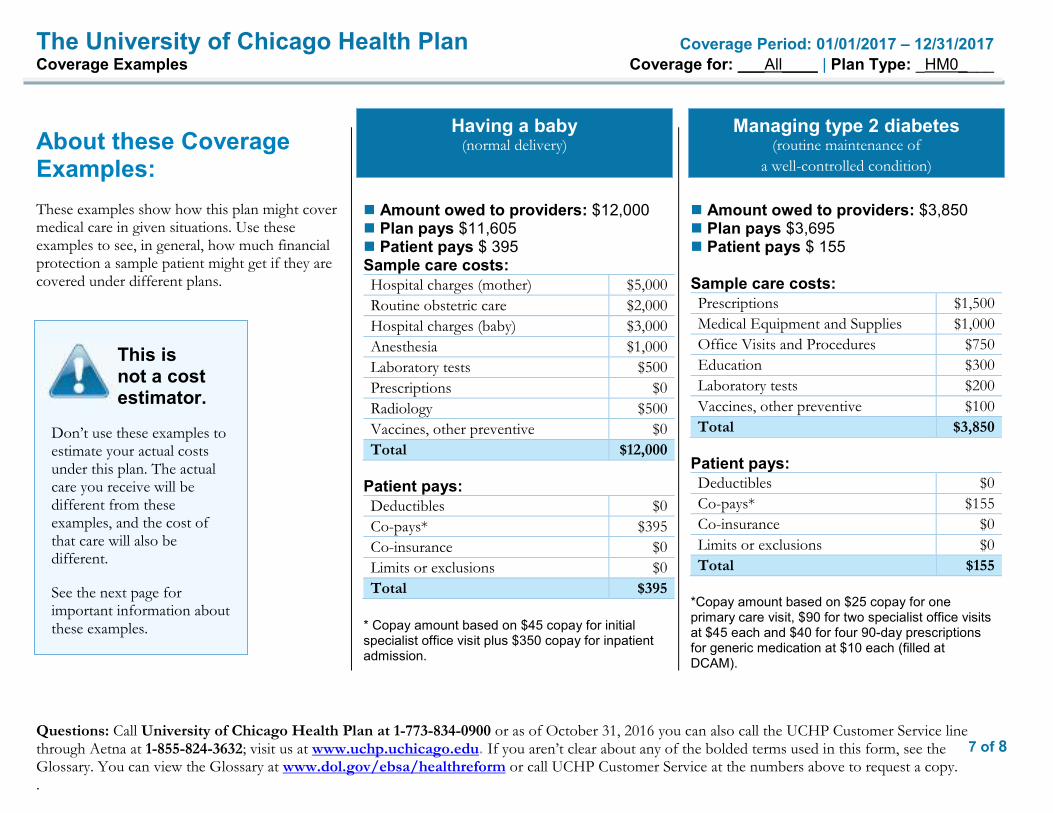
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017 Coverage Examples Coverage for: ___All____ | Plan Type: _HM0____
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Having a baby (normal delivery)
Managing type 2 diabetes (routine maintenance of
a well-controlled condition)
About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $12,000 Plan pays $11,605 Patient pays $ 395 Sample care costs: Hospital charges (mother) $5,000 Routine obstetric care $2,000 Hospital charges (baby) $3,000 Anesthesia $1,000 Laboratory tests $500 Prescriptions $0 Radiology $500 Vaccines, other preventive $0 Total $12,000
Patient pays: Deductibles $0 Co-pays* $395 Co-insurance $0 Limits or exclusions $0 Total $395
* Copay amount based on $45 copay for initial specialist office visit plus $350 copay for inpatient admission.
Amount owed to providers: $3,850 Plan pays $3,695 Patient pays $ 155
Sample care costs: Prescriptions $1,500 Medical Equipment and Supplies $1,000 Office Visits and Procedures $750 Education $300 Laboratory tests $200 Vaccines, other preventive $100 Total $3,850
Patient pays: Deductibles $0 Co-pays* $155 Co-insurance $0 Limits or exclusions $0 Total $155
*Copay amount based on $25 copay for one primary care visit, $90 for two specialist office visits at $45 each and $40 for four 90-day prescriptions for generic medication at $10 each (filled at DCAM).
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.

8 of 8
The University of Chicago Health Plan Coverage Period: 01/01/2017 – 12/31/2017 Coverage Examples Coverage for: ___All____ | Plan Type: _HM0____
Questions: Call University of Chicago Health Plan at 1-773-834-0900 or as of October 31, 2016 you can also call the UCHP Customer Service line through Aetna at 1-855-824-3632; visit us at www.uchp.uchicago.edu. If you aren’t clear about any of the bolded terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthreform or call UCHP Customer Service at the numbers above to request a copy. .
Questions and answers about the Coverage Examples: What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S. Department of Health and Human Services, and aren’t specific to a particular geographic area or health plan.
The patient’s condition was not an excluded or preexisting condition.
All services and treatments started and ended in the same coverage period.
There are no other medical expenses for any member covered under this plan.
Out-of-pocket expenses are based only on treating the condition in the example.
The patient received all care from in-network providers. If the patient had received care from out-of-network providers, costs would have been higher.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, co-payments, and co-insurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples. The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not cost estimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary of Benefits and Coverage for other plans, you’ll find the same Coverage Examples. When you compare plans, check the “Patient Pays” box in each example. The smaller that number, the more coverage the plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premium you pay. Generally, the lower your premium, the more you’ll pay in out-of-pocket costs, such as co-payments, deductibles, and co-insurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses.

Glossary of H
ealth Coverage and M
edical Term
s Page 1
of 4
Glossary
of Health C
overageand M
edical Terms
•T
his glossary has many com
monly used term
s, but isn’t a full list. These glossary term
s and definitions are intended to be educational and m
ay be different from the term
s and definitions in your plan. Some of these term
s also m
ight not have exactly the same m
eaning when used in your policy or plan, and in any such case, the policy or plan
governs. (See your Summ
ary of Benefits and Coverage for inform
ation on how to get a copy of your policy or plan
document.)
•Bold blue text indicates a term
defined in this Glossary.
•See page 4 for an exam
ple showing how
deductibles, co-insurance and out-of-pocket limits w
ork together in a real life situation.
Allow
ed Am
ount M
aximum
amount on w
hich payment is based for
covered health care services. This m
ay be called “eligible expense,” “paym
ent allowance" or "negotiated rate." If
your provider charges more than the allow
ed amount, you
may have to pay the difference. (See Balance Billing.)
Appeal
A request for your health insurer or plan to review
a decision or a g rievance again.
Balance Billing W
hen a provider bills you for the difference between the
provider’s charge and the allowed am
ount. For example,
if the provider’s charge is $100 and the allowed am
ount is $70, the provider m
ay bill you for the remaining $30.
A preferred provider m
ay not balance bill you for covered services.
Co-insurance
Your share of the costs
of a covered health care service, calculated as a percent (for exam
ple, 20%
) of the allowed
amount for the service.
You pay co-insurance
plus any deductibles you ow
e. For example,
if the health insurance or plan’s allowed am
ount for an office visit is $100 and you’ve m
et your deductible, your co-insurance paym
ent of 20% w
ould be $20. The health
insurance or plan pays the rest of the allowed am
ount.
Com
plications of Pregnancy C
onditions due to pregnancy, labor and delivery that require m
edical care to prevent serious harm to the health
of the mother or the fetus. M
orning sickness and a non-em
ergency caesarean section aren’t complications of
pregnancy.
Co-paym
ent A
fixed amount (for exam
ple, $15) you pay for a covered health care service, usually w
hen you receive the service. T
he amount can vary by the type of covered health care
service.
Deductible
The am
ount you owe for
health care services your health insurance or plan covers before your health insurance or plan begins to pay. For exam
ple, if your deductible is $1000, your plan w
on’t pay anything until you’ve m
et your $1000 deductible for covered health care services subject to the deductible. T
he deductible may not apply
to all services.
Durable M
edical Equipment (D
ME)
Equipment and supplies ordered by a health care provider
for everyday or extended use. Coverage for D
ME m
ay include: oxygen equipm
ent, wheelchairs, crutches or
blood testing strips for diabetics.
Emergency M
edical Condition
An illness, injury, sym
ptom or condition so serious that a
reasonable person would seek care right aw
ay to avoid severe harm
.
Emergency M
edical Transportation
Am
bulance services for an emergency m
edical condition.
Emergency R
oom C
are Em
ergency services you get in an emergency room
.
Emergency Services
Evaluation of an emergency m
edical condition and treatm
ent to keep the condition from getting w
orse.
(See page 4 for a detailed example.)
Jane pays 20%
H
er plan pays 80%
(See page 4 for a detailed example.)
Jane pays 100%
H
er plan pays 0%
OM
B C
ontrol Num
bers 1545-2229, 1210-0147, and 0938-1146

Glossary of H
ealth Coverage and M
edical Term
s Page 2
of 4
Excluded Services H
ealth care services that your health insurance or plan doesn’t pay for or cover.
Grievance
A com
plaint that you comm
unicate to your health insurer or p lan.
Habilitation Services
Health care services that help a person keep, learn or
improve skills and functioning for daily living. Exam
ples include therapy for a child w
ho isn’t walking or talking at
the expected age. These services m
ay include physical and occupational therapy, speech-language pathology and other services for people w
ith disabilities in a variety of inpatient and/or outpatient settings.
Health Insurance
A contract that requires your health insurer to pay som
e or all of your health care costs in exchange for a prem
ium.
Hom
e Health C
are H
ealth care services a person receives at home.
Hospice Services
Services to provide comfort and support for persons in
the last stages of a terminal illness and their fam
ilies.
Hospitalization
Care in a hospital that requires adm
ission as an inpatient and usually requires an overnight stay. A
n overnight stay for observation could be outpatient care.
Hospital O
utpatient Care
Care in a hospital that usually doesn’t require an
overnight stay.
In-network C
o-insurance T
he percent (for example, 20%
) you pay of the allowed
amount for covered health care services to providers w
ho contract w
ith your health insurance or plan. In-network
co-insurance usually costs you less than out-of-network
co-insurance.
In-network C
o-payment
A fixed am
ount (for example, $15) you pay for covered
health care services to providers who contract w
ith your health insurance or plan. In-netw
ork co-payments usually
are less than out-of-network co-paym
ents.
Medically N
ecessary H
ealth care services or supplies needed to prevent, diagnose or treat an illness, injury, condition, disease or its sym
ptoms and that m
eet accepted standards of m
edicine.
Netw
ork T
he facilities, providers and suppliers your health insurer or plan has contracted w
ith to provide health care services.
Non-Preferred Provider
A provider w
ho doesn’t have a contract with your health
insurer or plan to provide services to you. You’ll pay
more to see a non-preferred provider. C
heck your policy to see if you can go to all providers w
ho have contracted w
ith your health insurance or plan, or if your health insurance or plan has a “tiered” netw
ork and you must
pay extra to see some providers.
Out-of-netw
ork Co-insurance
The percent (for exam
ple, 40%) you pay of the allow
ed am
ount for covered health care services to providers who
do not contract with your health insurance or plan. O
ut-of-netw
ork co-insurance usually costs you more than in-
network co-insurance.
Out-of-netw
ork Co-paym
ent A
fixed amount (for exam
ple, $30) you pay for covered health care services from
providers who do not contract
with your health insurance or plan. O
ut-of-network co-
payments usually are m
ore than in-network co-paym
ents.
Out-of-Pocket Lim
it T
he most you pay during a
policy period (usually a year) before your health insurance or plan begins to pay 100%
of the allowed
amount. T
his limit never
includes your premium
, balance-billed charges or health care your health insurance or plan doesn’t cover. Som
e health insurance or plans don’t count all of your co-paym
ents, deductibles, co-insurance paym
ents, out-of-network paym
ents or other expenses tow
ard this limit.
Physician Services H
ealth care services a licensed medical physician (M
.D. –
Medical D
octor or D.O
. – Doctor of O
steopathic M
edicine) provides or coordinates.
(See page 4 for a detailed example.)
Jane pays 0%
H
er plan pays 100%

Glossary of H
ealth Coverage and M
edical Term
s Page 3
of 4
Plan A
benefit your employer, union or other group sponsor
provides to you to pay for your health care services.
Preauthorization A
decision by your health insurer or plan that a health care service, treatm
ent plan, prescription drug or durable m
edical equipment is m
edically necessary. Sometim
es called prior authorization, prior approval or precertification. Y
our health insurance or plan may
require preauthorization for certain services before you receive them
, except in an emergency. Preauthorization
isn’t a promise your health insurance or plan w
ill cover the cost.
Preferred Provider A
provider who has a contract w
ith your health insurer or plan to provide services to you at a discount. C
heck your policy to see if you can see all preferred providers or if your health insurance or plan has a “tiered” netw
ork and you m
ust pay extra to see some providers. Y
our health insurance or plan m
ay have preferred providers who are
also “participating” providers. Participating providers also contract w
ith your health insurer or plan, but the discount m
ay not be as great, and you may have to pay
more.
Premium
T
he amount that m
ust be paid for your health insurance or plan. Y
ou and/or your employer usually pay it
monthly, quarterly or yearly.
Prescription Drug C
overage H
ealth insurance or plan that helps pay for prescription drugs and m
edications.
Prescription Drugs
Drugs and m
edications that by law require a prescription.
Primary C
are Physician A
physician (M.D
. – Medical D
octor or D.O
. – Doctor
of Osteopathic M
edicine) who directly provides or
coordinates a range of health care services for a patient.
Primary C
are Provider A
physician (M.D
. – Medical D
octor or D.O
. – Doctor
of Osteopathic M
edicine), nurse practitioner, clinical nurse specialist or physician assistant, as allow
ed under state law
, who provides, coordinates or helps a patient
access a range of health care services.
Provider A
physician (M.D
. – Medical D
octor or D.O
. – Doctor
of Osteopathic M
edicine), health care professional or health care facility licensed, certified or accredited as required by state law
.
Reconstructive Surgery
Surgery and follow-up treatm
ent needed to correct or im
prove a part of the body because of birth defects, accidents, injuries or m
edical conditions.
Rehabilitation Services
Health care services that help a person keep, get back or
improve skills and functioning for daily living that have
been lost or impaired because a person w
as sick, hurt or disabled. T
hese services may include physical and
occupational therapy, speech-language pathology and psychiatric rehabilitation services in a variety of inpatient and/or outpatient settings.
Skilled Nursing C
are Services from
licensed nurses in your own hom
e or in a nursing hom
e. Skilled care services are from technicians
and therapists in your own hom
e or in a nursing home.
Specialist A
physician specialist focuses on a specific area of m
edicine or a group of patients to diagnose, manage,
prevent or treat certain types of symptom
s and conditions. A
non-physician specialist is a provider who
has more training in a specific area of health care.
UC
R (U
sual, Custom
ary and Reasonable)
The am
ount paid for a medical service in a geographic
area based on what providers in the area usually charge
for the same or sim
ilar medical service. T
he UC
R
amount som
etimes is used to determ
ine the allowed
amount.
Urgent C
are C
are for an illness, injury or condition serious enough that a reasonable person w
ould seek care right away, but
not so severe as to require emergency room
care.

Glossary of Health Coverage and Medical Terms Page 4 of 4
How You and Your Insurer Share Costs - ExampleJane’s Plan Deductible: $1,500 Co-insurance: 20% Out-of-Pocket Limit: $5,000
Jane reaches her $1,500 deductible, co-insurance beginsJane has seen a doctor several times and paid $1,500 in total. Her plan pays some of the costs for her next visit.
Office visit costs: $75 Jane pays: 20% of $75 = $15 Her plan pays: 80% of $75 = $60
Jane pays 20%
Her plan pays 80%
Jane pays 100%
Her plan pays 0%
Jane hasn’t reached her $1,500 deductible yetHer plan doesn’t pay any of the costs.
Office visit costs: $125 Jane pays: $125 Her plan pays: $0
January 1st
Beginning of CoveragePeriod
December 31st
End of Coverage Period
morecosts
morecosts
Jane reaches her $5,000 out-of-pocket limitJane has seen the doctor often and paid $5,000 in total. Her plan pays the full cost of her covered health care services for the rest of the year.
Office visit costs: $200 Jane pays: $0 Her plan pays: $200
Jane pays 0%
Her plan pays 100%


How to Contact the Benefits Office Address: 6054 South Drexel Avenue, Chicago, Illinois 60637 Phone: 773.702.9634 Fax: 773.834.0996 Email: [email protected] Web: humanresources.uchicago.edu
Office hours: 8:30 a.m.–4:30 p.m., weekdays
HRS-3001-17
The University of Chicago does not discriminate on the basis of race,color, religion, sex, sexual orientation, gender identity, national or ethnicorigin, age, status as an individual with a disability, protected veteranstatus, genetic information, or other protected classes under the law. Formore information and resources, visit equalopportunity.uchicago.edu.