2012 algorithm for management of advanced ovarian cancer bradley j. monk, md, facs, facog professor...
TRANSCRIPT

2012 ALGORITHM FOR MANAGEMENT OF ADVANCED OVARIAN CANCER
Bradley J. Monk, MD, FACS, FACOG
Professor and DirectorDivision of Gynecologic Oncology
Department of Obstetrics and GynecologyCreighton University School of Medicine atSt. Joseph’s Hospital and Medical Center,
a Member of Catholic Healthcare WestPhoenix, Arizona USA

Newly Diagnosed Advanced Ovarian Cancer

Ovarian Carcinoma: Incidence and Mortality
• Incidence in US women
– 21,880 cases in 2010
– Eighth most common cancer
– Second most common gynecologic cancer
– 1.5% lifetime risk of getting ovarian cancer
• Mortality in US women
– 14,850 deaths in 2010
– Fifth most common cause of cancer death
– Most common cause of death due to gynecologic cancer
– 1.0% lifetime risk of dying of ovarian cancer
ACS. Available at: http://www.cancer.org/

Cancer in the United Sates of America
ACS. Available at: http://www.cancer.org/
First-line Therapy Global Standard Treatment
IV Platinum + Taxane Chemotherapy(Carboplatin + Paclitaxel) x 6
2004 Consensus Statements on the Management of Ovarian Cancer:Final Document of the 3rd International GCIG Ovarian Cancer Consensus Conference (GCIG OCCC 2004).
Annals Of Oncology 16 (Supplement 8) Viii7–viii12, 2005
Surgery with maximum cytoreduction effort
Basis for Current Standard: Systemic Therapy
• Studies showing paclitaxel/cisplatin superior to cyclophosphamide/cisplatin – GOG Protocol 111[1]
– EORTC-NCIC OV 10[2]
• Studies showing paclitaxel/carboplatin at least equivalent to paclitaxel/cisplatin in efficacy– AGO Trial[3]
– GOG Protocol 158[4]
1. McGuire WP, et al. N Eng J Med .1996;334:1-6. 2. Piccart MJ, et al. J Natl Cancer Inst. 2000;92:699-708.3. DuBois A, et al. J Natl Cancer Inst. 2003;95:1320-1329. 4. Ozols RF, et al. J Clin Oncol. 2003;21:3194-3200.
1. Docetaxel instead of paclitaxel2. Neoadjuvant chemotherapy3. Intraperitoneal Chemotherapy4. Weekly dosing5. Adding a targeted agent (e.g. bevacizumab)6. Maintenance or consolidation chemotherapy after
complete remission
First-line Therapy: Acceptable but Uncommon

1. Docetaxel instead of paclitaxel2. Neoadjuvant chemotherapy3. Intraperitoneal Chemotherapy4. Weekly dosing5. Adding a targeted agent (e.g. bevacizumab)6. Maintenance or consolidation chemotherapy after
complete remission
First-line Therapy: Acceptable but Uncommon
IGCS Meeting October 25th 2009 BangkokN Engl J Med. 2010 Sep 2;363(10):943-53

Randomization
Ovarian, tubal or peritonal cancerFIGO stage IIIc-IV (n = 718)
Primary Debulking Surgery
Neoadjuvant chemotherapy
3 x Platinum based CT
Interval debulking (not obligatory)
Interval debulking if no PD
3 x Platinum based CT
> 3 x Platinum based CT > 3 x Platinum based CT
Primary Endpoint: Overall survival
Secondary endpoints: Progression Free Survival, Quality of Life, Complications
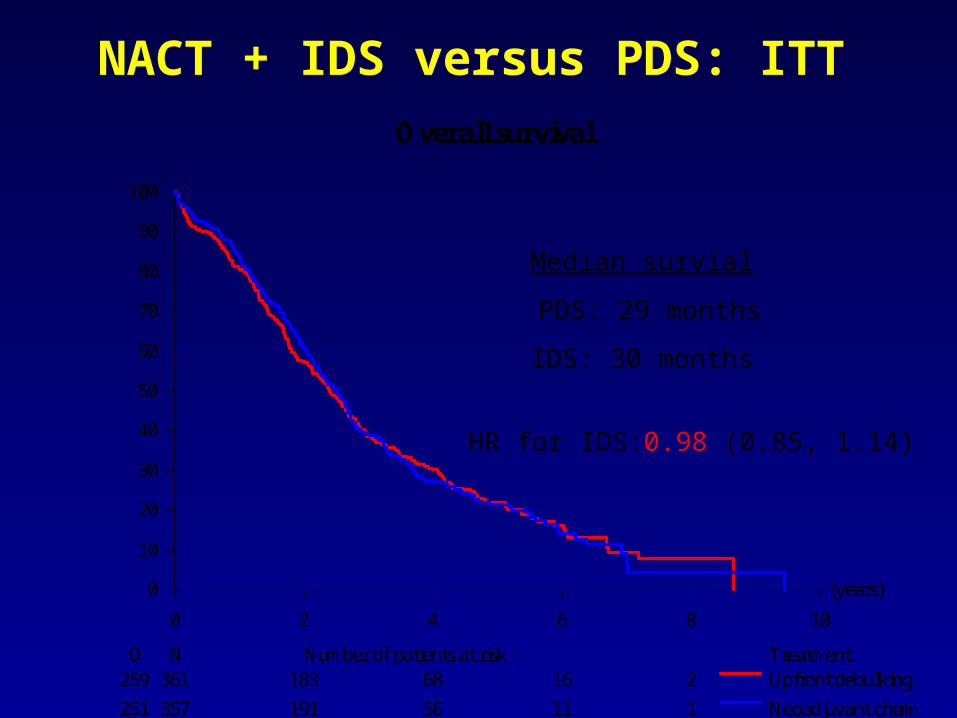
NACT + IDS versus PDS: ITT
(years)
0 2 4 6 8 10
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment259 361 183 68 16 2
251 357 191 56 11 1
Upfront debulking surgery
Neoadjuvant chemotherapy
Overall survival
Median survial
PDS: 29 months
IDS: 30 months
HR for IDS:0.98 (0.85, 1.14)

1. Docetaxel instead of paclitaxel2. Neoadjuvant chemotherapy3. Intraperitoneal Chemotherapy4. Weekly dosing5. Adding a targeted agent (e.g. bevacizumab)6. Maintenance or consolidation chemotherapy after
complete remission
First-line Therapy: Acceptable but Uncommon

Role of IP Chemotherapy for Optimally Debulked Advanced-Stage Ovarian Cancer
GOG 1041
Improved outcome in CP-treated patients when cisplatin administered IP (relative risk, 0.76)
GOG 1142
Improved outcome in TP-treated patients when cisplatin administered IP (relative risk, 0.78)
GOG 1723
Improved outcome in TP-treated patients when paclitaxel and cisplatin administered IP
(relative risk, 0.73)
CP =Cyclophosphamide and cisplatin; IP = Intraperitoneal; TP = Paclitaxel and cisplatin.1. Alberts DS, et al. N Engl J Med. 1996;335:1950-1955. 2. Markman M, et al. J Clin Oncol. 2001;19:1001-1007. 3. Armstrong DK et al. N Engl J Med. 2006;354:34-43.Reprinted with permission from Memorial Sloan-Kettering Cancer Web site. Available at: www.mskcc.org/patient_education/html/ 41495.cfm. Accessed March 9, 2006.

GOG172: Ovarian (optimal III)GOG172: Ovarian (optimal III)GOG172: Ovarian (optimal III)GOG172: Ovarian (optimal III)
Cisplatin 75 mg/m2
Paclitaxel 135 mg/m2 (24 h)
Cisplatin 100 mg/m2 IP d1Paclitaxel 135 mg/m2 (24 h) IV d1Paclitaxel 60 mg/m2 IP d8
• Epithelial Ovarian CancerEpithelial Ovarian Cancer• Optimal Stage IIIOptimal Stage III• No prior therapyNo prior therapy• Elective Second-LookElective Second-Look
Open:Open: 23-Mar-9823-Mar-98Closed:Closed: 29-Jan-0129-Jan-01Accrual:Accrual: 416 pts (evaluable)416 pts (evaluable)
I
II
Armstrong, et al. Armstrong, et al. NEJMNEJM 354:34-43, 2006 354:34-43, 2006
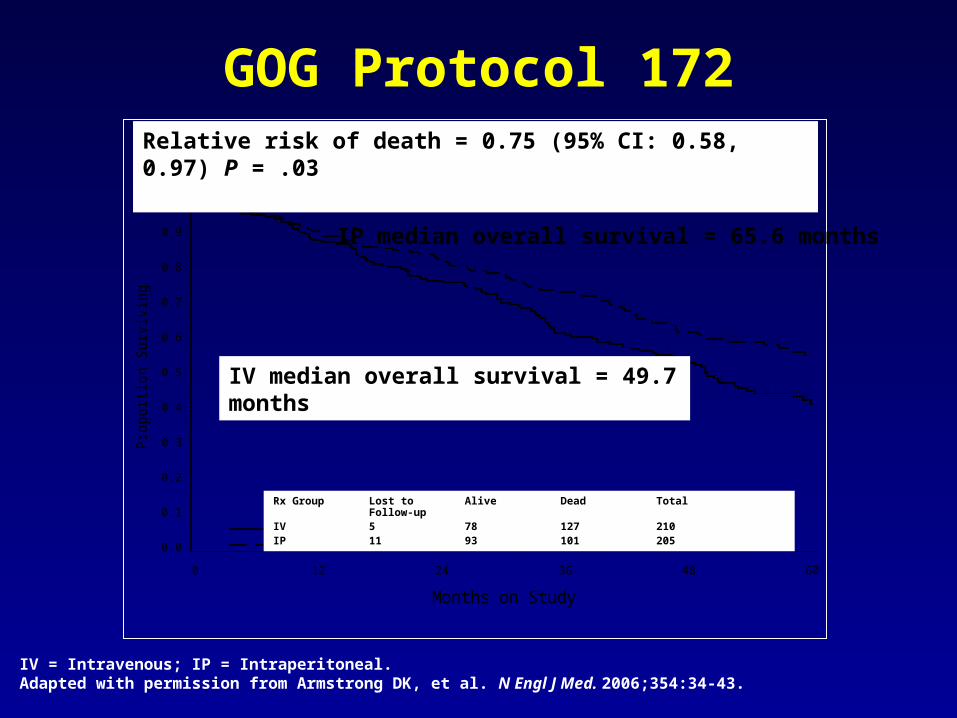
GOG Protocol 172
By Treatment GroupP
ropo
rtion
Sur
vivi
ng
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Months on Study0 12 24 36 48 60
Rx Group Alive Dead Total IV 93 117 210
Alive Dead Total
IP 117 88 205
IV median overall survival = 49.7 months
IP median overall survival = 65.6 months
Relative risk of death = 0.75 (95% CI: 0.58, 0.97) P = .03
IV = Intravenous; IP = Intraperitoneal.Adapted with permission from Armstrong DK, et al. N Engl J Med. 2006;354:34-43.
Rx Group Lost to Alive Dead TotalFollow-up
IV 5 78 127 210IP 11 93 101 205

GOG Protocol 172 Toxicity
No difference in QOL at 12 months
IV = Intravenous; IP = Intraperitoneal; GI = Gastrointestinal; QOL = Quality of life.Armstrong DK, et al. N Engl J Med. 2006;354:34-43.
IV, %(N = 210)
IP, %(N = 201)
G3/4 Leukopenia* 64 76
G3/4 Platelet 4 12
G3/4 GI* 24 46
G3/4 Renal* 2 7
G3/4 Neurologic Event* 9 19
G3/4 Fatigue* 4 18
G3/4 Infection* 6 16
G3/4 Metabolic* 7 27
G3/4 Pain* 1 11
*P ≤ 0.05

GOG 252:Stage II/III Disease: Small Volume Residual
GOG 252:Stage II/III Disease: Small Volume Residual
Carboplatin AUC=6 (IV)Paclitaxel 80 mg/m2 (d1, 8, 15 3h)Bevacizumab (C2+ C22) x 21 days
Cisplatin 75 mg/m2 (IP d2)Paclitaxel 135 mg/m2 (d1, 3h)Paclitaxel 60 mg/m2 (d8, IP)Bevacizumab (C2+ C22) x 21 days
• Epithelial Ovarian Cancer• Optimal Stage III• No prior therapy
• Phase III• PFS primary endpoint
Open: 27 Jul 2009Closed: 30 Nov 2011Accrual: 1100Study Chair: J Walker
I
III
IICarboplatin AUC=6 (IP)Paclitaxel 80 mg/m2 (d1, 8, 15 3h)Bevacizumab (C2+ C22) x 21 days
ClinicalTrials.gov Identifier: NCT00951496
1. Docetaxel instead of paclitaxel2. Neoadjuvant chemotherapy3. Intraperitoneal Chemotherapy4. Weekly dosing5. Docetaxel instead of paclitaxel6. Maintenance or consolidation chemotherapy after
complete remission
First-line Therapy: Acceptable but Uncommon

JGOG: Dose-Dense Weekly PaclitaxelJGOG: Dose-Dense Weekly PaclitaxelJGOG: Dose-Dense Weekly PaclitaxelJGOG: Dose-Dense Weekly Paclitaxel
Paclitaxel 180 mg/m2 Carbolatin AUC = 6
Carbolatin AUC = 6Paclitaxel 80 mg/m2/w x3
• Epithelial Ovarian or PeritonealEpithelial Ovarian or Peritoneal
• Stage II - IVStage II - IV
• No prior therapyNo prior therapy
• Stratfied: residual disease, Stratfied: residual disease, stage, and histologystage, and histology
• Primary endpoint: PFSPrimary endpoint: PFS
• Secondary endpoint: OSSecondary endpoint: OS
• Epithelial Ovarian or PeritonealEpithelial Ovarian or Peritoneal
• Stage II - IVStage II - IV
• No prior therapyNo prior therapy
• Stratfied: residual disease, Stratfied: residual disease, stage, and histologystage, and histology
• Primary endpoint: PFSPrimary endpoint: PFS
• Secondary endpoint: OSSecondary endpoint: OS
Accrual: 637 pts (intent-to-treat)Accrual: 637 pts (intent-to-treat)
I
II
Isonishi S, et al. Isonishi S, et al. J Clin OncolJ Clin Oncol. 2008; 26:A5506.. 2008; 26:A5506.
x6-9
x6-9
• Dose-dense paclitaxel associated with greater hematologic toxicity, and fewer Dose-dense paclitaxel associated with greater hematologic toxicity, and fewer patients completed all protocol therapypatients completed all protocol therapy
• Improved PFS with dose-dense weekly paclitaxelImproved PFS with dose-dense weekly paclitaxel
• Dose-dense paclitaxel associated with greater hematologic toxicity, and fewer Dose-dense paclitaxel associated with greater hematologic toxicity, and fewer patients completed all protocol therapypatients completed all protocol therapy
• Improved PFS with dose-dense weekly paclitaxelImproved PFS with dose-dense weekly paclitaxel
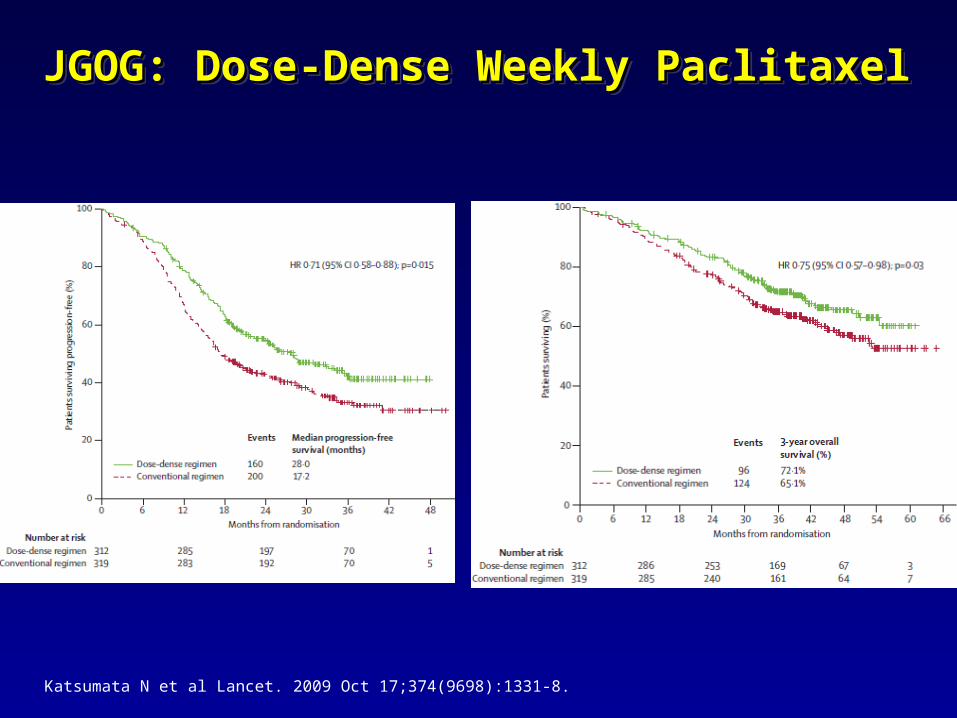
JGOG: Dose-Dense Weekly PaclitaxelJGOG: Dose-Dense Weekly PaclitaxelJGOG: Dose-Dense Weekly PaclitaxelJGOG: Dose-Dense Weekly Paclitaxel
Katsumata N et al Lancet. 2009 Oct 17;374(9698):1331-8.

GOG 262: Stage III/IV Disease: Large Volume Residual
Paclitaxel 80 mg/m2 IV every week + Carboplatin AUC 6 IV every 3 weeks x 6 cycles with optional Bevacizumab 15 mg/kg IV starting with cycle 2 until disease progression
RANDOMIZE
N = 625Primary Endpoint = Progression free survivalActivated: Sep 27 2010Study Chair: J Chan
Paclitaxel 175 mg/m2 IV + Carboplatin AUC 6 IV every 3 weeks x 6 cycles with optional Bevacizumab 15 mg/kg IV starting with cycle 2 until disease progression
ClinicalTrials.gov Identifier: NCT01167712
1. Docetaxel instead of paclitaxel2. Neoadjuvant chemotherapy3. Intraperitoneal Chemotherapy4. Weekly dosing5. Adding a targeted agent (e.g. bevacizumab)6. Maintenance or consolidation chemotherapy after
complete remission
First-line Therapy: Acceptable but Uncommon
23
Phase III Trial of Bevacizumab in the Primary Treatment of Advanced Epithelial Ovarian,
Primary Peritoneal, or Fallopian Tube Cancer: A Gynecologic Oncology Group (GOG) Study
R.A. Burger,R.A. Burger,11 M.F. Brady, M.F. Brady,22 M.A. Bookman, M.A. Bookman,33
J.L. Walker,J.L. Walker,44 H.D. Homesley, H.D. Homesley,55 J. Fowler, J. Fowler,66 B.J. Monk,B.J. Monk,77 B.E. Greer, B.E. Greer,88 M. Boente, M. Boente,99 S.X. Liang S.X. Liang1010
11Fox Chase Cancer Center, Philadelphia, PA; Fox Chase Cancer Center, Philadelphia, PA; 22Gynecologic Oncology Group Gynecologic Oncology Group Statistical and Data Center, Roswell Park Cancer Institute, Buffalo, NY; Statistical and Data Center, Roswell Park Cancer Institute, Buffalo, NY;
33University of Arizona Cancer Center, Tucson, AZ; University of Arizona Cancer Center, Tucson, AZ; 44University of Oklahoma University of Oklahoma Health Sciences Center, Oklahoma City, OK; Health Sciences Center, Oklahoma City, OK; 55Brody School of Medicine, Brody School of Medicine,
Greenville, NC; Greenville, NC; 66James Cancer Hospital at the Ohio State University, Hilliard, James Cancer Hospital at the Ohio State University, Hilliard, OH; OH; 77University of California, Irvine Medical Center, Orange, CA; University of California, Irvine Medical Center, Orange, CA; 88Seattle Cancer Seattle Cancer Care Alliance, Seattle, WA; Care Alliance, Seattle, WA; 99Minnesota Oncology and Hematology, Minneapolis, Minnesota Oncology and Hematology, Minneapolis,
MN; MN; 1010State University of New York at Stony Brook, Stony Brook, NY, USAState University of New York at Stony Brook, Stony Brook, NY, USA
J Clin Oncol 28:18s, 2010 (suppl; abstr LBA1)J Clin Oncol 28:18s, 2010 (suppl; abstr LBA1)N Engl J Med. 2011 Dec 29;365(26):2473-83.
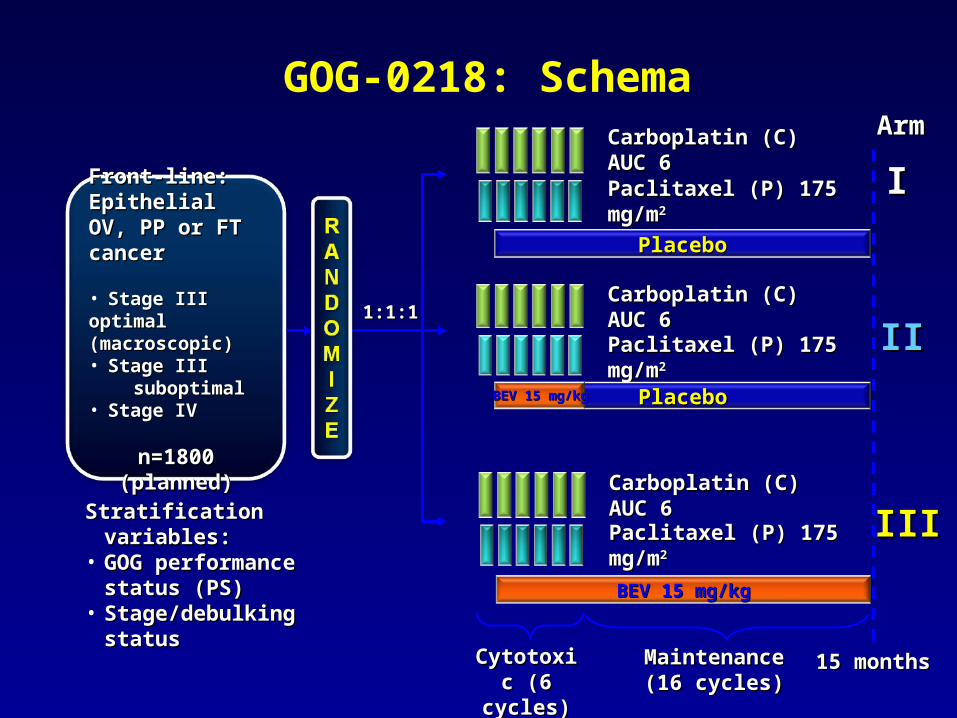
GOG-0218: Schema
Front-line: Front-line: Epithelial OV, PP Epithelial OV, PP or FT canceror FT cancer
• Stage III optimal Stage III optimal (macroscopic)(macroscopic)
• Stage III Stage III suboptimalsuboptimal• Stage IVStage IV
n=1800 (planned)n=1800 (planned)
Carboplatin (C) AUC 6Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/mPaclitaxel (P) 175 mg/m22
PlaceboPlaceboBEV 15 mg/kgBEV 15 mg/kg
IIII
Stratification variables:Stratification variables:• GOG performance status GOG performance status
(PS)(PS)• Stage/debulking statusStage/debulking status
1:1:11:1:1
15 months15 months
Paclitaxel (P) 175 mg/mPaclitaxel (P) 175 mg/m22
Carboplatin (C) AUC 6Carboplatin (C) AUC 6
PlaceboPlacebo
II
ArmArm
Cytotoxic Cytotoxic (6 cycles)(6 cycles)
BEV 15 mg/kgBEV 15 mg/kg
Carboplatin (C) AUC 6Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/mPaclitaxel (P) 175 mg/m22IIIIII
MaintenanceMaintenance(16 cycles)(16 cycles)

GOG-0218: Investigator-Assessed PFS
Arm I CP
(n=625)
Arm IICP + BEV(n=625)
Patients with event, n (%)423
(67.7)418
(66.9)
Median PFS, months 10.3 11.2
Stratified analysis HR (95% CI)
0.908(0.759–1.040)
One-sided p-value (log rank) 0.080*
+ BEV (Arm II)+ BEV (Arm II)CP (Arm I)CP (Arm I)
*p-value boundary = 0.0116*p-value boundary = 0.0116
+ BEV → BEV maintenance (Arm III)+ BEV → BEV maintenance (Arm III)Pro
po
rtio
n s
urv
ivin
g p
rog
ress
ion
fre
eP
rop
ort
ion
su
rviv
ing
pro
gre
ssio
n f
ree
Months since randomizationMonths since randomization
1.01.0
0.90.9
0.80.8
0.70.7
0.60.6
0.50.5
0.40.4
0.30.3
0.20.2
0.10.1
0000 1212 2424 3636
Arm IIICP + BEV BEV
(n=623)
360 (57.8)
14.1
0.717 (0.625–0.824)
<0.0001*

Hazard ratio
Experimental arm (CP + BEV BEV;
Arm III) betterControl arm
(CP; Arm I) better
Stage 3 optimal (n=434) 0.618
Stage 3 suboptimal (n=496) 0.763
Stage 4 (n=318) 0.698
PS 0 (n=616) 0.710
PS 1/2 (n=632) 0.690
Age <60 years (n=629) 0.680
Age 60–69 years (n=409) 0.763
Age 70 years (n=210) 0.678
0.33 0.5 0.67 1.0 1.5 2.0 3.0
GOG-0218: Subgroup Analyses of PFSCP + BEV BEV (Arm III) vs CP (Arm I)
Treatment hazard ratioTreatment hazard ratio

2727
ICON7: a phase III Gynaecologic Cancer InterGroup (GCIG) trial of adding bevacizumab
to standard chemotherapy in women with newly diagnosed epithelial ovarian, primary peritoneal
or fallopian tube cancerTim Perren, Ann Marie Swart, Jacobus Pfisterer, Jonathan Tim Perren, Ann Marie Swart, Jacobus Pfisterer, Jonathan
Ledermann, Alain Lortholary, Gunnar Kristensen, Mark Carey, Ledermann, Alain Lortholary, Gunnar Kristensen, Mark Carey, Philip Beale, Andreas Cervantes, Amit Oza Philip Beale, Andreas Cervantes, Amit Oza
on behalf of GCIG ICON7 collaborators on behalf of GCIG ICON7 collaborators (MRC/NCRI, AGO-OVAR, GINECO, NSGO, ANZGOG, (MRC/NCRI, AGO-OVAR, GINECO, NSGO, ANZGOG,
GEICO, NCIC-CTG)GEICO, NCIC-CTG)ESMOESMO
2010N Engl J Med. 2011 Dec 29;365(26):2484-96.2010N Engl J Med. 2011 Dec 29;365(26):2484-96.

ICON7: Study Design
Stratification variables: Stratification variables: • Stage/surgeryStage/surgery• Time since surgeryTime since surgery• GCIG groupGCIG group *Might vary based on GCIG group*Might vary based on GCIG group
****Omit cycle 1 bevacizumab if <4 weeks from surgeryOmit cycle 1 bevacizumab if <4 weeks from surgery
Paclitaxel 175 mg/mPaclitaxel 175 mg/m22
Carboplatin AUC Carboplatin AUC 6*6*
AVASTINAVASTIN
Carboplatin AUC 6*Carboplatin AUC 6*
Paclitaxel 175 mg/mPaclitaxel 175 mg/m22
Arm A
Arm A
ArmArm BB
12 months12 months
Front-line EOC, Front-line EOC, PP or FT cancerPP or FT cancer
• Stage I-IIA (Gr 3 Stage I-IIA (Gr 3 or CC) or CC)
• Stage IIB/CStage IIB/C• Stage IIIStage III• Stage IVStage IV
n=1528 n=1528
Bevacizumab 7.5 mg/kgBevacizumab 7.5 mg/kg****
Primary endpoints: Primary endpoints: PFSPFS
Secondary Secondary endpoints: OS, RR, endpoints: OS, RR, safety, QOL, safety, QOL, cost-effectiveness,cost-effectiveness,translationaltranslational
No IRC presentNo IRC present
Perren, et al. ESMO 2010

Number at riskCP 764 723 693 556 464 307 216 143 91 50 25CPB7.5+ 764 748 715 647 585 399 263 144 73 36 19
Number at riskCP 764 723 693 556 464 307 216 143 91 50 25CPB7.5+ 764 748 715 647 585 399 263 144 73 36 19
1.00
0.75
0.50
0.25
0
1.00
0.75
0.50
0.25
0
Pro
po
rtio
n a
live
wit
ho
ut
pro
gre
ssi
on
Pro
po
rtio
n a
live
wit
ho
ut
pro
gre
ssi
on
Time (months)Time (months)
0 3 6 9 12 15 18 21 24 27 300 3 6 9 12 15 18 21 24 27 30
CP CPB7.5+
Events, n (%) 392 (51) 367 (48)
Median, months 17.3 19.0
Log-rank test p=0.0041
HR (95% CI) 0.81 (0.70–0.94)
17.3 19.0
CPCPB7.5+
ICON 7 PFS Benefit: Academic Analysis
Perren, et al. ESMO 2010

ICON 7 Subgroups
No. of events/no. of patients
Origin of cancer Research Control HR
Age <60 202/449 210/450 0.84
60–69 134/242 142/237 0.76
≥70 31/73 40/77 0.82
ECOG PS 0 154/334 145/358 1.01
1 175/366 210/354 0.66
2 27/45 31/43 0.78
Histology Serous 274/525 278/529 0.85
Mucinous 12/19 10/15 0.77
Endometroid 26/60 25/57 0.81
Clear cell 22/67 22/60 0.90
FIGO I 6/54 9/65 0.73
II 14/83 19/80 0.72
III 277/523 290/522 0.79
IV 70/104 74/97 0.69
Residual disease
Optimal (≤1 cm) 226/559 233/552 0.87
Suboptimal (>1cm) 131/192 145/195 0.68
Grade Grade 1 10/41 16/56 0.76
Grade 2 86/175 77/142 0.77
Grade 3 267/538 294/556 0.81
Hazard ratio (fixed)
0 1 20.5 1.5
CP better
Age: Trend p=0.69, interaction p=0.83; ECOG: Trend p=0.027, interaction p=0.022Histology: Interaction test p=0.085; FIGO: Trend p=0.71, interaction p=0.91Residual disease: Trend p=0.10; Grade: Trend p=0.76, interaction p=0.95 CPB7.5+ better
Perren, et al. ESMO 2010

1. Docetaxel instead of paclitaxel2. Neoadjuvant chemotherapy3. Intraperitoneal Chemotherapy4. Weekly dosing5. Adding a targeted agent (e.g. bevacizumab)6. Maintenance or consolidation chemotherapy after
complete remission
First-line Therapy: Acceptable but Uncommon

GOG 178—Investigating Paclitaxel as Consolidation
CR = Complete response.Markman M, et al. J Clin Oncol. 2003;21:2460-2465.
RANDOMIZE
277 stage III/IV patients in completeclinical remission
Paclitaxel 175 mg/m2 every 28 days × 3 months
Paclitaxel 175 mg/m2 every 28 days × 12 months
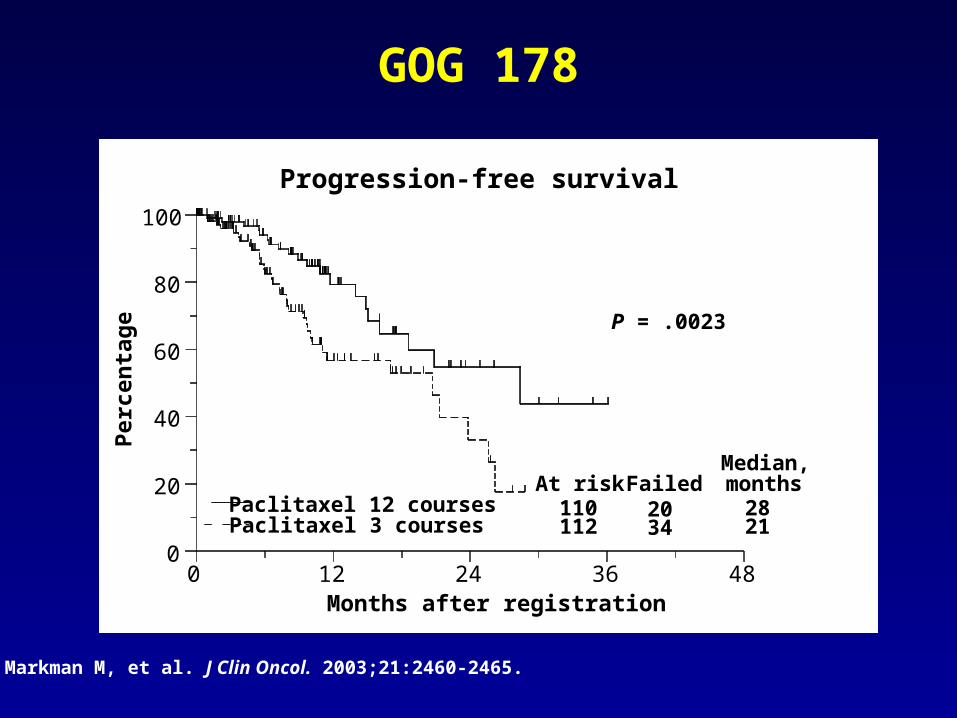
GOG 178
Progression-free survival
0
20
40
60
80
100
0 12 24 36 48Months after registration
Paclitaxel 12 coursesPaclitaxel 3 courses
110At risk
112
Failed2034
Median,months
2821
P = .0023
Pe
rcen
tag
e
Markman M, et al. J Clin Oncol. 2003;21:2460-2465.

GOG-0212Phase III Maintenance Therapy Trial
Primary endpoint: survivalSecondary endpoints: PFS, toxicity, QoL
www.clinicaltrials.gov/ct2/show/NCT00108745.
Macromolecular complexMacromolecular complex of paclitaxel poliglumexof paclitaxel poliglumex
Patients with stage III/IV epithelial ovarian or primary peritoneal cancer, GOG PS ≤ 2, and complete response after surgery plus taxane and carboplatin
(Planned N = 1400-1550)
Paclitaxel Every 28 days for up to 12 courses
No treatment
Paclitaxel poliglumex Every 28 days for up to 12 courses

Recurrent Disease
CHEMOTHERPAY

Population Study Treatment PFS
Optimal Stage 3 GOG 114 IV Carb & Pac, IP Cis 28 mos
GOG 172 IV Pac, IP Cis & Pac 24 mos
GOG 158 IV Pac & Carb 21 mos
GOG 114 IV Pac & Cis 22 mos
GOG 158 IV Pac & Cis 19 mos
GOG 172 IV Pac & Cis 18 mos
Suboptimal 3 & 4 GOG 111 IV Pac & Cis 18 mos
GOG 162 IV Pac Cis 12 mos
GOG 152 IV Pac Cis 11 mos
All Stage 3 & 4 GOG 182 IV Pac/Carbo x 8 16 mos
When Does Advanced Ovarian Cancer Recur?
Carb = carboplatin; Cis = cisplatin; Doc = docetaxel; GOG = Gynecologic Oncology Group; IP = intraperitoneal; Pac = paclitaxel.

Treatment Considerations and Goals:Recurrent Ovarian Cancer
• Treatment considerations in the management of recurrent ovarian cancer – Disease-free interval– Existing toxicities remaining due to the 1st-line therapy – Volume of disease at the time of relapse– Serologic relapse (CA-125)
• Primary goals of therapy for the treatment of recurrent ovarian cancer– Progression-free survival (PFS)– Increased survival– Prevention of symptoms– Palliation of symptoms– Quality of life (QoL)

Ovarian Cancer Treatment Considerations
First-Line Treatment Recurrent Disease
Cure Goal Palliation
High Toxicity Acceptance
Low
Less Important Convenience More Important

Recurrence After First-line Chemotherapy
PlatinumPlatinumSensitiveSensitive
> 6 Months> 6 Months
ChemotherapyChemotherapyDoubletDoublet
Platinum Platinum Refractory/ResistantRefractory/Resistant
< 6 Months< 6 Months
Non-PlatinumNon-PlatinumSingle AgentSingle Agent
The Traditional Treatment Paradigm

FDA-Approved Drugs in Ovarian Cancer
1978
Cis
plat
in
Car
bopl
atin
Altr
etam
ine
Pac
litax
elTo
pote
can
Lipo
som
al d
oxor
ubic
in (P
LD)
(acc
eler
ated
)Li
poso
mal
dox
orub
icin
(ful
l)
Gem
cita
bine
(with
car
bopl
atin
)
2006
1989
1990
1992
1996
1999
2005
2009
Trab
ecte
din;
EU
onl
y
(with
PLD
)
1964
Mel
phal
anD
oxor
ubic
in
1974

OCEANS
Stratification variables: Stratification variables: • Time to recurrenceTime to recurrence• Cytoreductive surgeryCytoreductive surgery
Gemcitabine 1000 mg/mGemcitabine 1000 mg/m22 d1/8d1/8
Carboplatin AUC 4Carboplatin AUC 4
Carboplatin AUC 4Carboplatin AUC 4
Gemcitabine 1000 mg/mGemcitabine 1000 mg/m22 d1/8d1/8
Arm A
Arm A
Arm BArm B
Placebo to progressionPlacebo to progression
Bevacizumab 15 mg/kg to progressionBevacizumab 15 mg/kg to progression
Platinum-Platinum-sensitive, sensitive, recurrentrecurrent
OC, PP, FTCOC, PP, FTC
No prior No prior bevacizumabbevacizumab
n=480n=480
Primary endpoint: Primary endpoint: PFSPFS
Secondary Secondary endpoints:endpoints:ORR, OS, DR, safetyORR, OS, DR, safety
Exploratory Exploratory endpoints:endpoints:IRC, CA 125 IRC, CA 125 response, ascitesresponse, ascites
IRC presentIRC present
ClinicalTrials.gov Identifier: NCT00434642

242242 177177 4545 1111 33 00CG + PLCG + PL
OCEANS: Primary analysis of PFSCG + PL(n=242)
CG + BV(n=242)
Events, n (%) 187 (77) 151 (62)
Median PFS, months (95% CI)
8.4(8.3–9.7)
12.4(11.4–12.7)
Stratified analysis HR (95% CI)Log-rank p-value
0.484 (0.388–0.605)
<0.0001
MonthsMonthsNo. at riskNo. at risk
242242 203203 9292 3333 1111 00CG + BVCG + BV
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
Pro
po
rtio
n p
rog
res
sio
n f
ree
Pro
po
rtio
n p
rog
res
sio
n f
ree
00 66 1212 1818 2424 3030
ASCO 2011

Duration of response CG + PL (n=139)
CG + BV (n=190)
Median, months 7.4 10.4
HR (95% CI) 0.534(0.408–0.698)
p<0.0001a
OCEANS: Objective Response
100
80
60
40
20
0
100
80
60
40
20
0
%%
78.5
57.4 PR = 61
PR = 48
CR = 17CR = 9
Difference: 21.1% p<0.0001
aCompared for descriptive purposes only
CG + PL (n=242)
CG + BV (n=242)
ASCO 2011
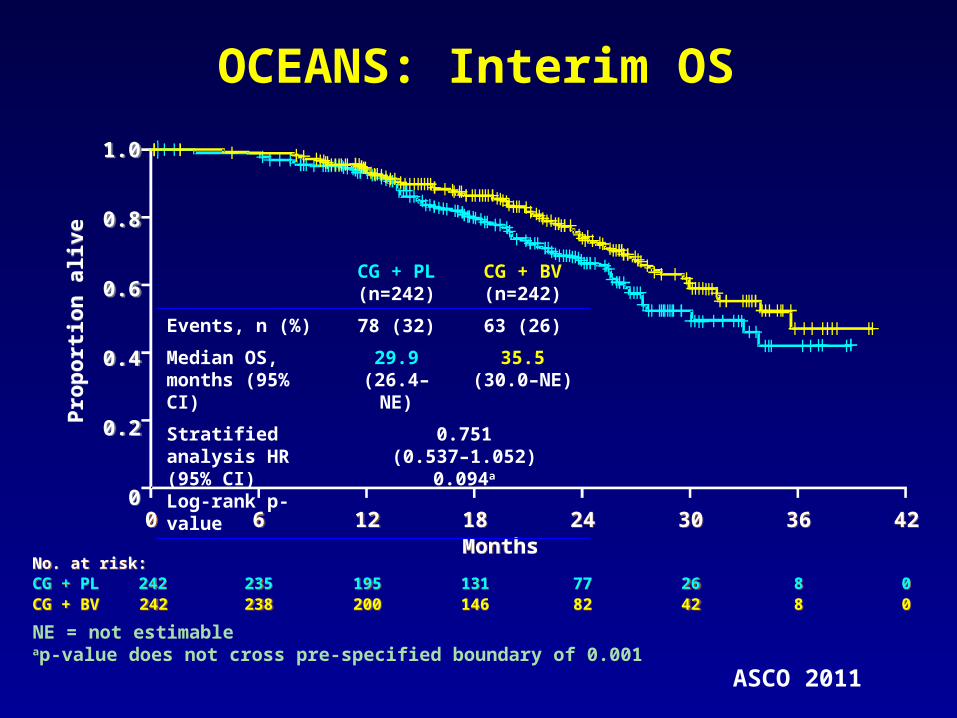
OCEANS: Interim OS
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
Pro
po
rtio
n a
live
Pro
po
rtio
n a
live
00MonthsMonths
66 1212 3030 3636 4242
No. at risk:No. at risk:
1818 2424
242242 235235 195195 2626 88 00CG + PLCG + PL 131131 7777242242 238238 200200 4242 88 00CG + BVCG + BV 146146 8282
CG + PL(n=242)
CG + BV(n=242)
Events, n (%) 78 (32) 63 (26)
Median OS, months (95% CI)
29.9(26.4–NE)
35.5(30.0–NE)
Stratified analysis HR (95% CI)Log-rank p-value
0.751(0.537–1.052)
0.094a
NE = not estimableap-value does not cross pre-specified boundary of 0.001
ASCO 2011
Summary and Looking Towards the Future
Unanswered Questions Regarding Bevacizumab in Ovarian Cancer1.Best clinical setting (frontline vs recurrence)
2.Single agent or combination
3.Dose
4.Duration
5.Continuation beyond progression
6.Cost effectiveness
7.Impact on patient reported outcomes (PRO or QOL)
•Other agents that effect angiogenesis and the tumor vasculature active and in late stage development

NCCN “ Preferred” Agents in“Platinum Resistant” Ovarian Cancer
Level IIA
•Docetaxel•Etoposide, oral•Gemcitabine•PLD•Weekly paclitaxel•Topotecan•Bevacizumab
National Comprehensive Cancer Network (NCCN)www.nccn.org

Summary and Conclusions
• Advanced ovarian cancer is very lethal despite many active medicines
• IV carboplatin and paclitaxel standard adjuvant front-line therapy
• Little survival benefit in recurrent setting• No approved targeted agent• No agent approved since 2006

2012:Phase III Registration Studies in Ovarian Cancer*
Front-line added to chemotherapy then as Maintenance1. BIBF 1120 (OVAR 12)2. AMG 386 (with Carboplatin or Paclitaxel)
Maintenance alone1. Polyglutamate paclitaxel (GOG 212)2. Pazopanib (OVAR 16)
Platinum-resistant recurrent ovarian cancer 1. Karenitecin2. Bevacizumab (with chemotherapy - AURELIA)3. AMG 386 (with PLD or Paclitaxel)4. EC-145 (with PLD)
Platinum-sensitive recurrent ovarian cancer1. Bevacizumab (with chemotherapy - OCEANS, GOG 213)2. Trabectedin (with PLD)3. Cediranib (with chemotherapy - ICON7)4. Farletuzumab (with Carboplatin or Paclitaxel)5. Water soluble formulation of Paclitaxel *Phase II studies of PARP inhibitors, NKTR-102 and
XL-184 may lead to FDA approval
PLD = Pegylated Liposomal Doxorubicin

• Histologically or cytologically confirmed non-mucinous epithelial ovarian cancer including primary peritoneal or fallopian tube malignancies
• Measurable disease by CT or MRI scan
• Relapse within < 6 months after first-line platinum/taxane chemotherapy
• Up to 4 prior lines of therapy• Neurologic function: neuropathy
(sensory and motor) ≤CTCAE Grade 1
ClinicalTrials.gov Identifier: NCT00738699 (FAR122)
Co-Primary Endpoints = Progression-free survival and Overall survivalN = 550
Weekly paclitaxel (80mg/m2) x 12then 3 out of 4 weekswith placebo MORAb-003 2.5 mg/kg(N=367)
Weekly paclitaxel (80mg/m2) x 12then 3 out of 4 weekswith placebo (N=183)
RRAANNDDOOMMIIZZEE
Farletuzumab (MORAb-003): Phase II Farletuzumab (MORAb-003): Phase II Platinum Resistant PatientsPlatinum Resistant Patients

• November 28, 2011– Study stopped by IDMC for futility– 40% of OS events = 161 deaths– HR boundaries PFS > 0.9 and OS > 1.00– Corresponding conditional power < 1% and
one sided P value was > 0.1985 for PFS and > 0.5000 for OS
– No new safety issues identified
Farletuzumab (MORAb-003): Phase II Farletuzumab (MORAb-003): Phase II Platinum Resistant PatientsPlatinum Resistant Patients
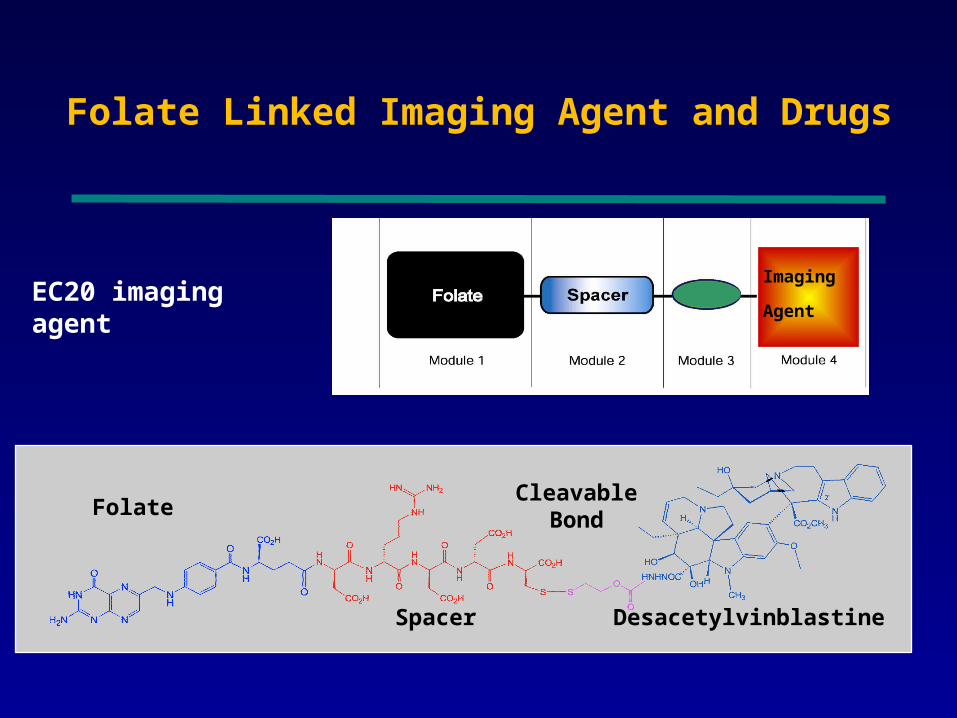
Imaging
AgentEC20 imaging agent
EC145 therapeutic
Folate Linked Imaging Agent and Drugs
Desacetylvinblastine
Folate
Spacer
Cleavable Bond

PRECEDENT – A Randomized Phase II Trial of PLD ± EC145 in Platinum-Resistant Ovarian Cancer (EC-FV-04)
PLD 50 mg/m2 q 28 daysEC145 2.5 mg/m2 q MWF every other wk
PLD 50 mg/m2RRAANNDDOOMMIIZZEE
Recurrent EOC1st or 2nd Relapse
< 6 mo platinum based therapy
N = 149
2:1 Randomization
1° EndpointPFSHR 0.68 at 95 events2° EndpointORR and OSCorrelate EC 20 scan and response
Optional EC20 Scan
n = 94
Naumann RW, et al. ASCO 2011. Abstract 5045.
PLD= Pegylated liposomal doxorubicin
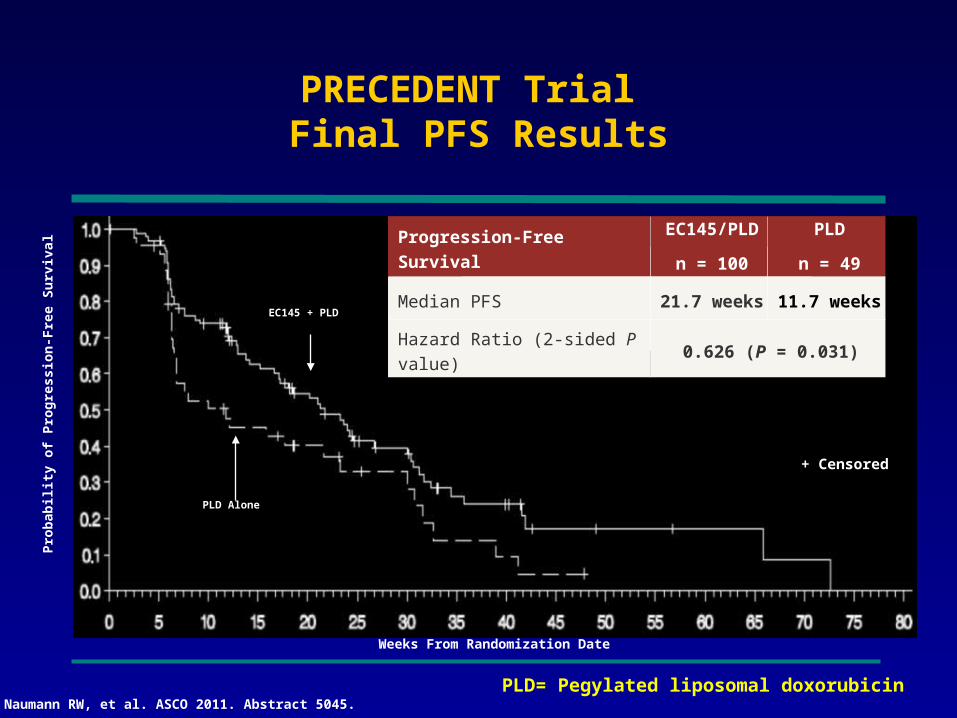
+ Censored
Progression-Free SurvivalEC145/PLD
n = 100
PLD
n = 49
Median PFS 21.7 weeks 11.7 weeks
Hazard Ratio (2-sided P value) 0.626 (P = 0.031)
EC145 + PLD
PLD Alone
Pro
bab
ility
of
Pro
gre
ssio
n-F
ree
Su
rviv
al
Weeks From Randomization Date
PRECEDENT Trial Final PFS Results
Naumann RW, et al. ASCO 2011. Abstract 5045.PLD= Pegylated liposomal doxorubicin
EC145 + PLD
PLD Alone
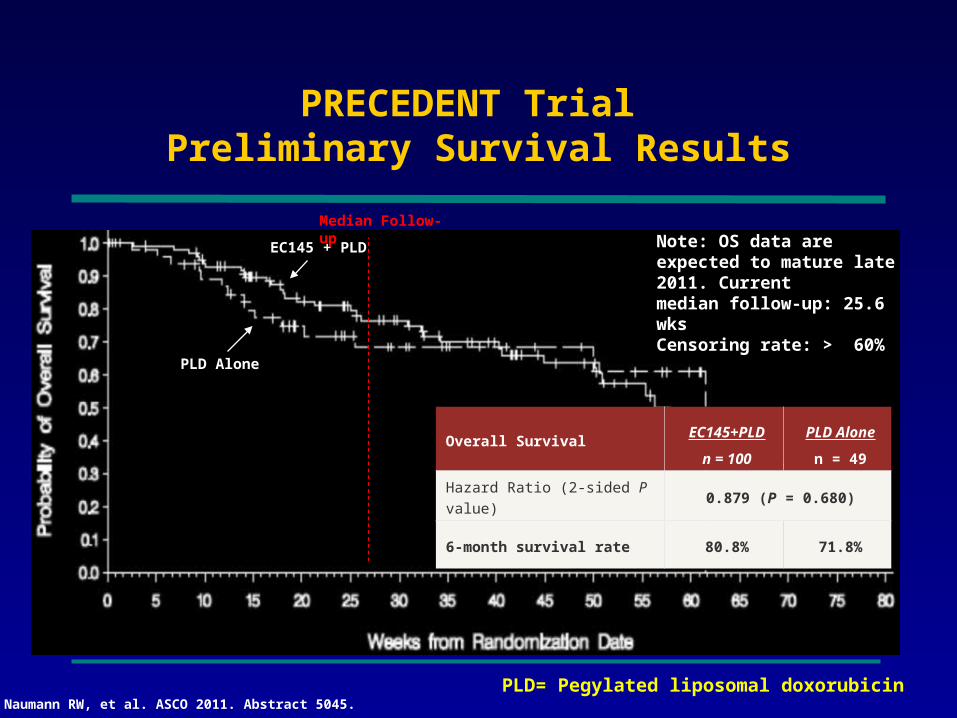
Note: OS data are expected to mature late 2011. Current median follow-up: 25.6 wksCensoring rate: > 60%
Overall SurvivalEC145+PLD
n = 100
PLD Alone
n = 49
Hazard Ratio (2-sided P value) 0.879 (P = 0.680)
6-month survival rate 80.8% 71.8%
PRECEDENT Trial Preliminary Survival Results
Median Follow-up
Naumann RW, et al. ASCO 2011. Abstract 5045.PLD= Pegylated liposomal doxorubicin
Disappointing Mature Overall Survival (OS)
Press Release - Dec 13, 2011•The median OS in the EC145 study arm = 14.1 months• The median OS in the PLD control = 16.9 months•HR = 1.099 intent-to-treat
http://www.endocyte.com/wp-content/uploads/2011/04/2011.12.13_EU-Supplemental-Analysis.pdf

Study for Women With Platinum Resistant Ovarian Cancer Evaluating EC145 in Combination With Doxil®
(PROCEED)
• Placebo IV days 1,3,5 and15,17,19 of a 4-week cycle
• PLD 50 mg/m2 (IBW) every4 weeks.
• EC145 IV days 1,3,5 and15,17,19 of a 4-week cycle
• PLD 50 mg/m2 (IBW) every4 weeks.
RANDOMIZE
ClinicalTrials.gov Identifier: NCT01170650
Estimated Enrollment: 500
Study Start Date: September 2010
Estimated Study Completion Date: July 2014
Estimated Primary Completion Date: August 2012
Primary Endpoint: PFS
Secondary Endpoints: OS, toxicity
• Primary or secondary platinum-resistant ovarian cancer.
• Measurable disease (RECIST v1.1-defined)
• Prior platinum-based chemotherapy for management of primary regimens
PLD= Pegylated liposomal doxorubicin
Phase II study of the oral PARP inhibitor olaparib (AZD2281) versus liposomal doxorubicin in ovarian cancer patients with BRCA1 and/or
BRCA2 mutations
Stan Kaye,Stan Kaye,11 Bella Kaufman, Bella Kaufman,2 2 Jan Lubinski,Jan Lubinski,3 3
Ursula Matulonis,Ursula Matulonis,44 Charlie Gourley, Charlie Gourley,55 Beth Karlan, Beth Karlan,6 6
Dianna Taylor,Dianna Taylor,77 Mark Wickens, Mark Wickens,77 James Carmichael James Carmichael77
1. Royal Marsden Hospital, Sutton, Surrey, UK1. Royal Marsden Hospital, Sutton, Surrey, UK
2. Chaim Sheba Medical Center, Tel Hashomer, Israel 2. Chaim Sheba Medical Center, Tel Hashomer, Israel
3. Pomeranian Medical University, Szczecin, Poland3. Pomeranian Medical University, Szczecin, Poland
4. Dana-Farber Cancer Institute, Boston, MA, USA4. Dana-Farber Cancer Institute, Boston, MA, USA
5. University of Edinburgh Cancer Research Centre, Western General Hospital, Edinburgh, UK5. University of Edinburgh Cancer Research Centre, Western General Hospital, Edinburgh, UK
6. Cedars-Sinai Medical Center, Los Angeles, CA, USA6. Cedars-Sinai Medical Center, Los Angeles, CA, USA
7. AstraZeneca, Alderley Park, Macclesfield, UK7. AstraZeneca, Alderley Park, Macclesfield, UK
Clinicaltrials.gov number, NCT00628251
ESMO 2010ESMO 2010
Kaye S, et al. Ann Oncol. 2010;21(suppl 8). Abstract 9710.
Randomized
1:1:1
Olaparib 200 mg bid in 28-day cycles
PLD 50 mg/m2 IV every 4 weeks
PD or withdrawal from treatment for
other reason
As above or max lifetime cumulative
dose reached
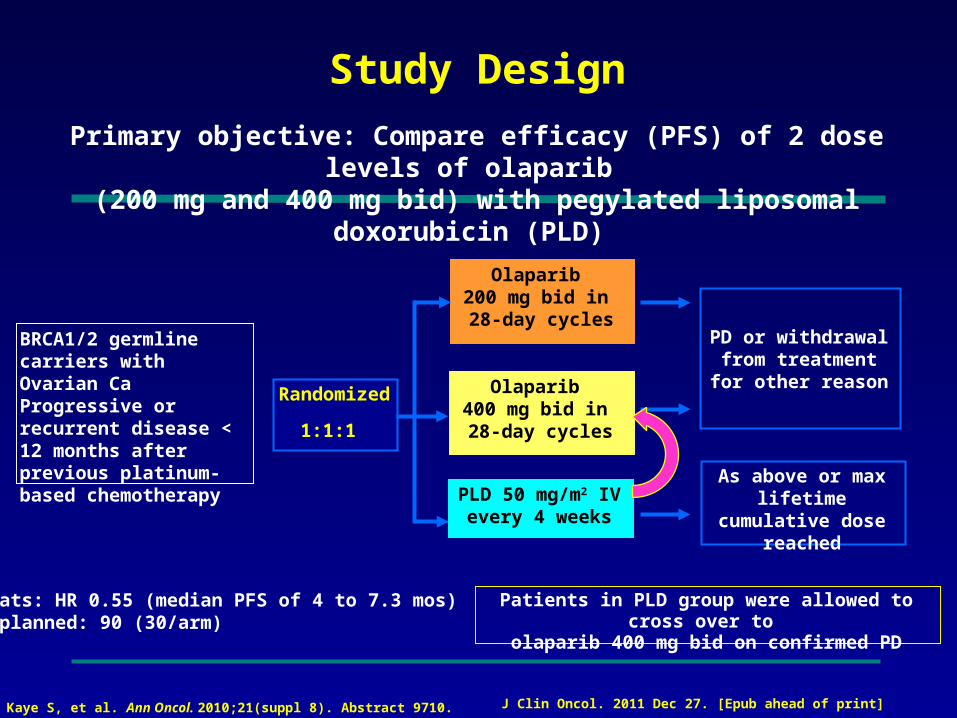
Primary objective: Compare efficacy (PFS) of 2 dose levels of olaparib (200 mg and 400 mg bid) with pegylated liposomal doxorubicin (PLD)
Study Design
Olaparib 400 mg bid in 28-day cycles
BRCA1/2 germline carriers with Ovarian CaProgressive or recurrent disease < 12 months after previous platinum-based chemotherapy
Patients in PLD group were allowed to cross over to
olaparib 400 mg bid on confirmed PD
Stats: HR 0.55 (median PFS of 4 to 7.3 mos)N planned: 90 (30/arm)
Kaye S, et al. Ann Oncol. 2010;21(suppl 8). Abstract 9710. J Clin Oncol. 2011 Dec 27. [Epub ahead of print]

Progression-Free Survival
Olaparib 200 mg: 6.5 (5.6-8.0) months
Median PFS (80% CI)
Olaparib 400 mg: 8.8 (6.3-9.2) months
PLD 50 mg/m2: 7.1 (5.5-7.8) months
HR* vs PLD (80% CI)
Olaparib 200 mg: 0.91 (0.60-1.39); P = 0.78
Olaparib 400 mg: 0.86 (0.56-1.30); P = 0.63
Olaparib 200 mg + 400 mg: 0.88 (0.62-1.28); P = 0.66
Time From Randomization (months)
Pro
po
rtio
n o
f P
atie
nts
Pro
gre
ssio
n F
ree
0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0 12108642
*HR < 1 favors olaparib.
32 03813212432 011217212833 038151825
Number of patients at risk:
Olaparib 200 mg
Olaparib 400 mg
PLD
Stats: HR 0.55 (median PFS of 4 to 7.3 mos)N planned: 90 (30/arm)
Olaparib 400 mg
Olaparib 200 mg
PLD
Kaye S, et al. Ann Oncol. 2010;21(suppl 8). Abstract 9710. J Clin Oncol. 2011 Dec 27. [Epub ahead of print]

Phase II randomized placebo-controlled study of olaparib (AZD2281) in patients
with platinum-sensitive relapsed serous ovarian cancer
Jonathan A. Ledermann
J Clin Oncol 29: 2011 (suppl; abstr 5003)

Maintenance Olaparib:Study design
Placebo(n=129)
Olaparib400mg bid,
orally(n=136)
Patients
•Platinum-sensitive high-grade serous ovarian cancer
•≥2 previous platinum regimens
•Maintained PR or CR following last platinum regimen
Ledermann et al. J Clin Oncol 2011;29 (suppl; abstr 5003)
Primary endpoint
PFS by RECIST
Secondary endpoints
TTP by CA-125 (GCIG criteria) or RECIST, OS, safety
Randomized 1:1
82 sites in 16 countries
Lederman J et al J Clin Oncol 29: 2011 (suppl; abstr 5003)

Progression-free survival
0
Time from randomization (months)
136 104 51 23 6 0 0
129 72 23 7 1 0 0
At risk (n)
Olaparib
Placebo
0.6
0.8
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
3 6 9 12 15 18
No. of events: Total patients (%)
Median PFS (months)
Olaparib60:136 (44.1)
8.4
Placebo93:129 (72.1)
4.8
Hazard ratio 0.35 (95% CI, 0.25–0.49)P<0.00001
Olaparib 400 mg bidPlacebo
Randomized treatmentPro
po
rtio
n o
f p
atie
nts
p
rog
ress
ion
fre
e
Lederman J et al J Clin Oncol 29: 2011 (suppl; abstr 5003)

Olaparib:Another PARP Inhibitor Abandoned in
Ovarian Cancer
Press Release - Dec 20, 2011•The previously reported progression free survival benefit is unlikely to translate into an overall survival benefit, the definitive measure of patient benefit in ovarian cancer•Attempts to identify a suitable tablet dose for use in Phase III studies have not been successful.
http://www.astrazeneca.com/Media/Press-releases/Article/20111220-az-updates-olaparib-TC5214-development
