your registration form - medical marijuana services · pdf fileyour registration form...
TRANSCRIPT
YOUR REGISTRATION FORMApplication to Become a Client
Your Registration FormVersion: 11 / 14©Tweed Inc.
Page 1
INSTRUCTIONS:Thank you for choosing Tweed as your trusted source for premium medical marijuana. Our team will do everything we can to make your experience with Tweed memorable for all the right reasons.
To register as a client for the purchase of medical marijuana, you must complete and sign this Registration Form and send it to us by fax, email, or regular mail to any of the following:
Fax: 888-977-2595Email: [email protected]
Address: ATTN: Tweed Care Centre1 Hershey Dr.Smiths Falls, ONK7A 0A8
If you have any problems completing the application, give us a call and we will happily walk through each step of the appli-cation with you.
To complete your registration, Tweed will also need an original version of your Medical Document, completed by your healthcare practitioner. We can accept this document by fax only directly from your doctor’s office. Otherwise you or your doctor will need to mail us the original paper version. If you need assistance with this, Tweed would be pleased to arrange for the collection of your forms and/or to provide you with a self-addressed prepaid envelope upon request.
For More Information: Tel: 855-558-9333 Email: [email protected]
www.tweed.com
Secure ePortal Fax Line:888-977-2595
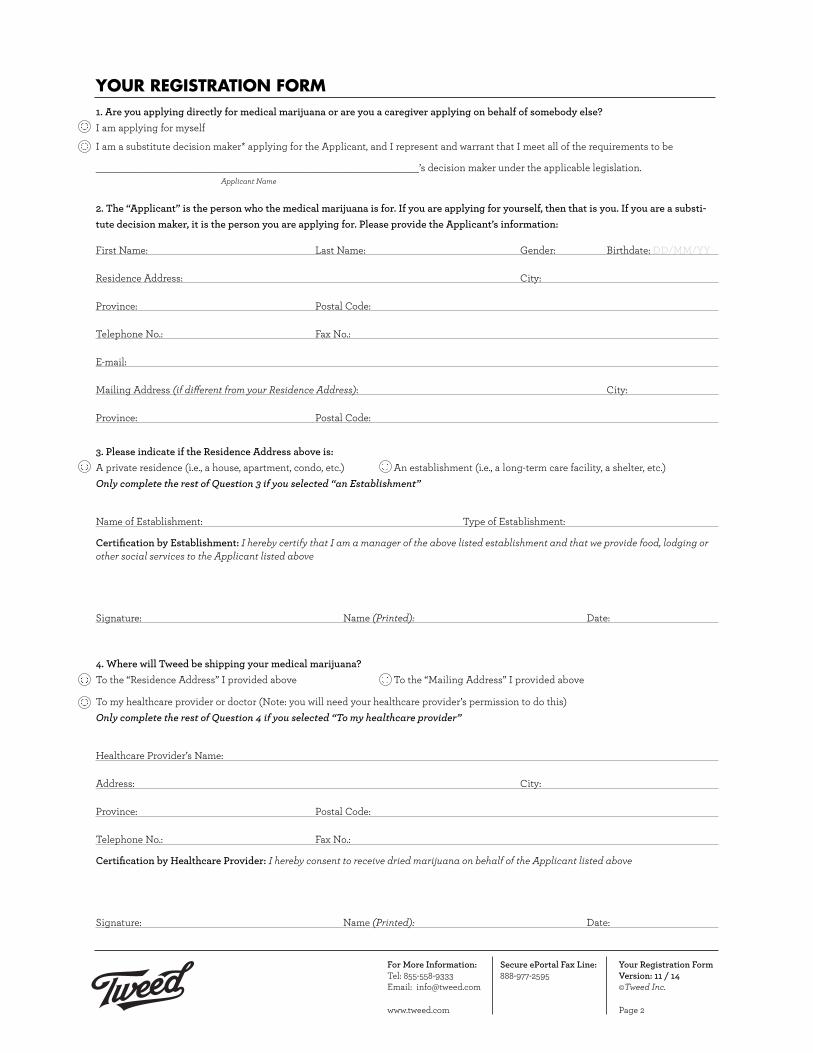
YOUR REGISTRATION FORM1. Are you applying directly for medical marijuana or are you a caregiver applying on behalf of somebody else?I am applying for myself
I am a substitute decision maker* applying for the Applicant, and I represent and warrant that I meet all of the requirements to be
___________________________________________________________’s decision maker under the applicable legislation.Applicant Name
2. The “Applicant” is the person who the medical marijuana is for. If you are applying for yourself, then that is you. If you are a substi-tute decision maker, it is the person you are applying for. Please provide the Applicant’s information:
First Name: Last Name: Gender: Birthdate: DD/MM/YY
Residence Address: City:
Province: Postal Code:
Telephone No.: Fax No.:
E-mail:
Mailing Address (if different from your Residence Address): City:
Province: Postal Code:
3. Please indicate if the Residence Address above is:A private residence (i.e., a house, apartment, condo, etc.) An establishment (i.e., a long-term care facility, a shelter, etc.) Only complete the rest of Question 3 if you selected “an Establishment”
Name of Establishment: Type of Establishment:
Certification by Establishment: I hereby certify that I am a manager of the above listed establishment and that we provide food, lodging or other social services to the Applicant listed above
Signature: Name (Printed): Date:
4. Where will Tweed be shipping your medical marijuana?To the “Residence Address” I provided above To the “Mailing Address” I provided above
To my healthcare provider or doctor (Note: you will need your healthcare provider’s permission to do this) Only complete the rest of Question 4 if you selected “To my healthcare provider”
Healthcare Provider’s Name:
Address: City:
Province: Postal Code:
Telephone No.: Fax No.:
Certification by Healthcare Provider: I hereby consent to receive dried marijuana on behalf of the Applicant listed above
Signature: Name (Printed): Date:
Your Registration FormVersion: 11 / 14©Tweed Inc.
Page 2
For More Information: Tel: 855-558-9333 Email: [email protected]
www.tweed.com
Secure ePortal Fax Line:888-977-2595

5. Only complete Question 5 if you are a substitute decision maker applying on behalf of the Applicant. Please provide your information:
First Name: Last Name: Gender: Birthdate:
Certification by substitute decision maker: I certify that I am responsible for the Applicant listed above
Signature: Name (Printed): Date:
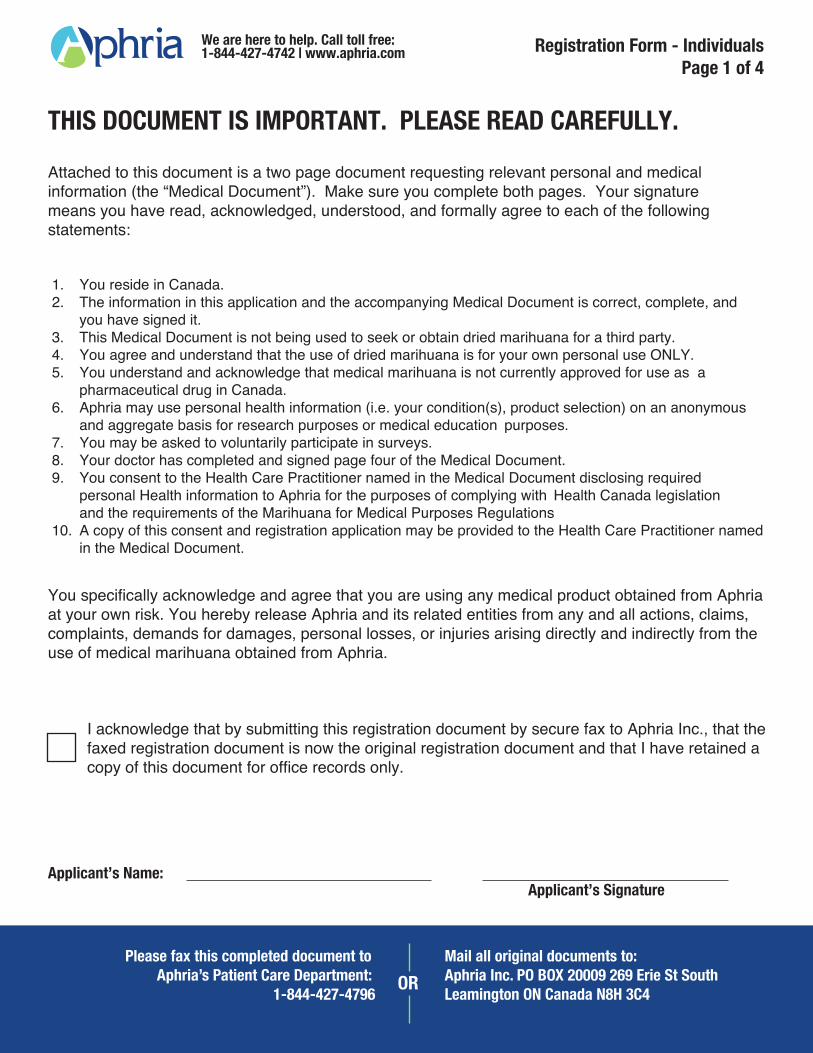
6. That’s it. Whether you are the Applicant or the substitute decision maker, we need you to sign this registration form certifying that:
a) The Applicant is ordinarily resident in Canada;b) The information in this application and the accompanying medical document is accurate and complete;c) The medical document is not being used to seek or obtain dried marijuana from another source;d) The valid medical document accompanies this application; ande) The applicant will use dried medical marijuana only for their own medical purposes.
Signature: Name (Printed): Date:
7. The small print: The Applicant acknowledges that he/she has read and agrees to Tweed’s Terms of Service and Privacy Policy, available at tweed.com. The Applicant further acknowledges that medical marijuana is not approved for use as a drug in Canada, that its indications, safety and risks have not been adequately studied and the appropriate dosage is unclear. The applicant acknowledges and agrees that he or she is using any medical marijuana product obtained from Tweed Inc. at his or her own risk, and releases Tweed Inc. from any and all ac-tions, claims, complaints and demands for damages, loss, liability or injury whatsoever arising directly or indirectly as a consequence of the use of medical marijuana obtained from Tweed Inc. Tweed Inc. makes no representations and gives no warranties or conditions, whether ex-press, implied, statutory, or otherwise, including, without limitation, any warranties or conditions of merchantability, merchantable quality, durability, or fitness for a particular purpose, all of which are hereby disclaimed. That said, Tweed takes it product quality very seriously, as well as its obligations under the MMPR to investigate all customer complaints. If at any time you have an issue with your Tweed medicine, we encourage you to get in touch with us.
8. Interacting with Tweed: By signing this registration form, you give Tweed permission to send medical marijuana and your registration information to the Shipping Address provided. You also give us permission to communicate with you at your listed email address so that we can provide you with information related to your account and purchases. If you do not provide an email address, we will be happy to assist you with placing an order over the phone.
Please indicate if we may also contact you:
By Phone By mail at your Residence Address By mail at your Mailing Address (if applicable)
Please indicate if we may email you regarding product availability or to provide other important updates: Yes No
9. Compassionate Pricing Promise: Tweed offers customers a Compassionate Pricing Promise to help ensure those in need can better afford their medicine. Eligibility terms can be found on our website or within your Information Package. If you would like to apply for this Program, please check the box below and make sure to provide supporting documentation.
I have included proof that I receive income support from an eligible provincial or federal program or meet the low income threshold of Tweed.
10. Direct Billing for Canadian Forces Veterans:In order for Tweed to bill Veterans Affairs Canada directly for the cost of your medicine, we require the following information:
a) Your doctor MUST provide a diagnosis on your medical document b) Your Veterans Affairs Canada Health Benefit Card number:_____________________ c) A completed Veteran’s Consent to Disclose form (available on our website)
** Direct billing is subject to approval by Veterans Affairs Canada
Your Registration FormVersion: 11 / 14©Tweed Inc.
Page 3
*A substitute decision-maker is a person authorized to consent, on behalf of an individual, to disclose personal health information about the individual under PHIPA or the applicable health information legislation in the jurisdiction in which the applicant resides.
For More Information: Tel: 855-558-9333 Email: [email protected]
www.tweed.com
Secure ePortal Fax Line:888-977-2595
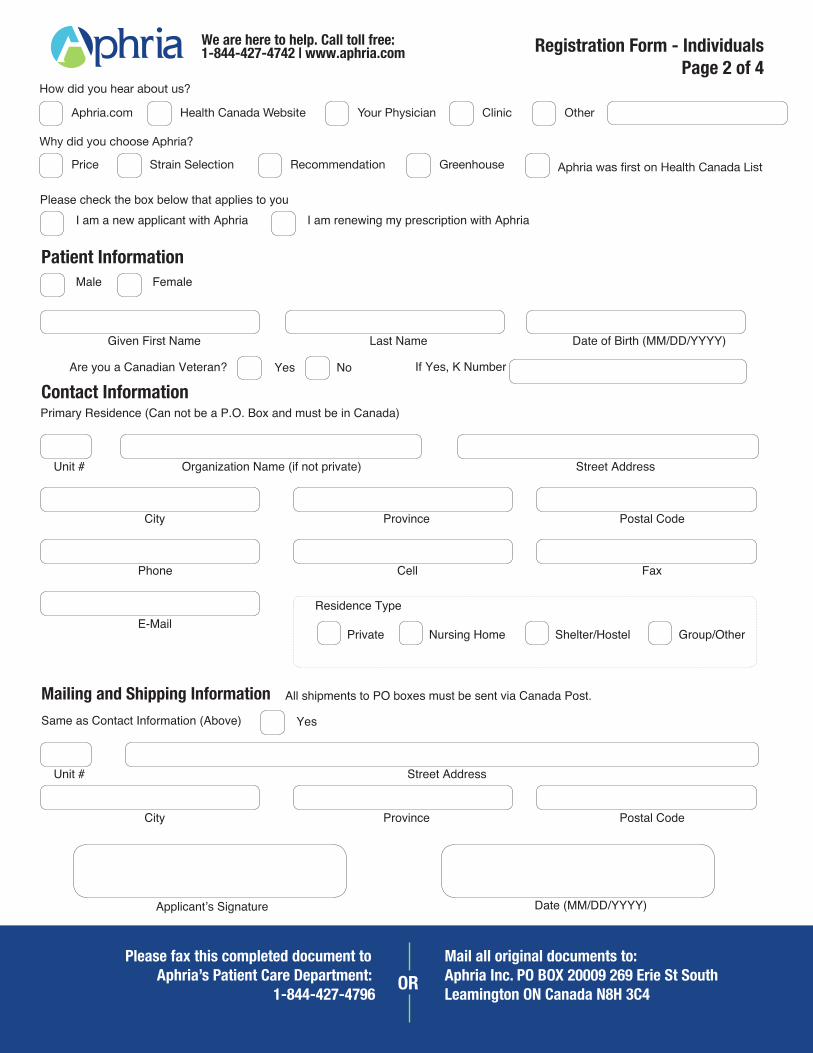
How did you hear about us?
Why did you choose Aphria?
Aphria.com
Price Strain Selection Recommendation Greenhouse Aphria was first on Health Canada List
Health Canada Website Your Physician Clinic Other

Bedrocan.ca | Application Form ‘A’ Page 1 of 2
Registration Amendment Form Complete This Form To Amend Your Registration Information
Questions? Call: 1-855-420-7887 or Email: [email protected] Mail or Courier Completed Documents To:
Bedrocan Canada 250A Eglinton Ave. East
PO BOX 89589, Toronto, ON M4P 3E1
SECTION 1 – Applicant New Information
Full Name:
Date of Birth: Gender: Male
Female
Reason for
Amendment:
New
Information:
SECTION 2 – Caregiver / Individual’s Responsibe For Applicant New Information
Caregiver
Name:
Caregiver Gender: Male
Date of Birth: Female
Caregiver / Person Responsible Declaration:
I am responsible for
Caregiver Signature:
Given First Name(s)
Unique Client ID Number Day / Month / Year
/ /
Caregiver / Person Responsible Full Name Applicant’s Full Name
Given First Name(s) Surname (Last Name)
Day Month Year
/ /
Date: Day / Month / Year
/ /
Surname (Last Name)
Change Residence /
Shipping Address
Name
Change
Gender
Change
Date of Birth
Change
Healthcare
Practitioner
Change
Caregiver
Change
Bedrocan.ca | Application Form ‘A’ Page 2 of 2
Registration Amendment Form Complete This Form To Amend Your Registration Information
Questions? Call: 1-855-420-7887 or Email: [email protected]
Mail or Courier Completed Documents To:
Bedrocan Canada 250A Eglinton Ave. East
PO BOX 89589, Toronto, ON M4P 3E1
SECTION 3 – New Health Care Practitioner Information
Name:
Profession: Clinic Name:
License #:
Office
Address:
Contact:
Consent to Receive Dried Marijuana on Behalf of Applicant
I consent to receive marijuana on behalf of
Unit # Street Address 1 Street Address 2 (If Applicable)
City Province Postal Code
Title Given First Name(s) Surname (Last Name)
Practitioner Phone (required)
( ) Practitioner Fax (required)
( )
Day / Month / Year
/ / Applicant/Individual
Responsible Signature:
The Undersigned Applicant or Person Responsible Hereby Agrees and Warrants That: The Applicant ordinarily resides in Canada.
The information submitted in this Application & Medical Document is correct and complete.
The medical document is not being used to seek or obtain dried marijuana from another source.
The original of the Medical Document accompanies the Application.
The Applicant will use dried marijuana only for his or her own medical purposes.
The Applicant understands and acknowledges that medical marijuana is not currently approved for use as a drug in Canada and that its safety and risks
have not been fully studied and the appropriate dosage is unclear.
The Applicant acknowledges and agrees that he or she is using any medical marijuana product obtained from Bedrocan Canada at his or her own risk,
and releases Bedrocan Canada (and its partners, providers, officers, directors and staff) from any and all actions, claims, complaints and demands for
damages, loss or injury whatsoever arising directly or indirectly from the use of medical marijuana obtained from Bedrocan Canada.
The Applicant consents to Bedrocan Canada collecting and disclosing necessary personal information in order to process this registration and fulfill
orders for medicinal cannabis in accordance with Bedrocan Canada’s privacy policy (www.Bedrocan.ca/privacy)
The Applicant consents to the health care practitioner named in this document disclosing required personal health information to Bedrocan Canada for
the purposes of complying with the requirements of the Marijuana for Medical Purposes Regulations (MMPR). The Applicant understands and agrees
that a copy of this consent & registration application may be provided to the health care practitioner named herein.
Medical License Number
Ship Dried Marijuana
to My Office
Health Care Practitioner Name Applicant Name
Day / Month / Year
/ / Health Care
Practitioner Signature:
(required if you are consenting to receive dried marijuana on behalf of Applicant)
Practitioner Email
Province Licensed to Practice
Send Dried Marijuana to
Shipping Address in Section 3
SECTION 4 – *IMPORTANT* – PLEASE READ AND SIGN BELOW
Reg
istr
atio
n A
pplic
atio
n - F
orm
A -
FOR
IND
IVID
UALS
| Pa
ge 1
Use primary address as my shipping address.
MedReleaf.com | Application Form A | Doc # 002 | Revision #004 | Effective Date 01/02/2015
SECTION 2 - CONTACT & SHIPPING INFORMATION
Primary Residence
Residence Type
ContactInfo
Unit # Street Address 1 Street Address 2 (If Applicable)
City Province Postal Code
If Other, Please Specify Name of Establishment (if not private residence)
Phone Number Fax Number
Private Residence Nursing/Care Home Shelter Hostel Group Home Other
Primary Residence, must be In Canada
www.MedReleaf.com
We’re here to help!Email: [email protected]
Phone: 1.855.4.RELEAF (473.5323)
Questions?
SECTION 1 - APPLICANT / PATIENT INFORMATIONPatient’s name
License # (If Yes)
MaleFemale
Gender
Given First Name(s) Surname (Last Name)
Email Address
DOB (DD/MM/YY)
YesNo
Do you possess a valid Authorization To Possess licence (ATP)
More establishment info (if necessary)
Confirm Email Address
ALTERNATE ADDRESS
ShippingAddress:
Unit # Street Address 1 Street Address 2 (If Applicable)
City Province Postal Code
Applicable ONLY if your primary residence has no postal service.
This form may be filled out electronically or printed and completed by hand.
Reg
istr
atio
n A
pplic
atio
n - F
orm
A -
FOR
IND
IVID
UALS
| Pa
ge 2
MedReleaf P.O. Box 3040 Markham Industrial Park Markham ON, Canada L3R 6G4
Please send both this completed document ANDyour ORIGINAL Medical Document to us at:
MedReleaf.com | Application Form A | Doc # 002 | Revision #004 | Effective Date 01/02/2015
www.MedReleaf.com
We’re here to help!Email: [email protected]
Phone: 1.855.4.RELEAF (473.5323)
Questions?
SECTION 3 - AUTHORIZATION OF APPLICANTBy signing below the applicant acknowledges that they have read, understood and agree that:
Applicant’s or Caregiver’s Signature
DateSigned
(DD/MM/YY)
How did you hear about MedReleaf? (optional)
The Applicant ordinarily resides in Canada.
The information in this application and the accompanying Medical Document is correct and complete.
The Medical Document is not being used to seek or obtain dried cannabis from another source.
The original Medical Document or one of the original Personal Use Production License (PUPL) or Designated Person Production License (DPPL) MUST be received by MedReleaf Corp. in order for MedReleaf Corp. to complete the patient registration.
The Applicant will use dried cannabis only for its own medical purposes.
The Applicant understands and acknowledges that medical cannabis is not currently approved for use as a pharmaceutical drug in Canada.
The Applicant acknowledges and agrees that he or she is using any medical cannabis product obtained from MedReleaf Corp. at his or her own risk, and releases MedReleaf Corp. (and its partners, providers, officers, directors and staff) from any and all actions, claims, complaints and demands for damages, loss or injury whatsoever arising directly or indirectly from the use of medical cannabis obtained from MedReleaf Corp.
The Applicant consents to MedReleaf Corp. collecting and disclosing necessary personal information in order to process this registration and to fulfill orders for medical cannabis in accordance with the MedReleaf Corp. privacy policy (www.MedReleaf.com/privacy.php).
By signing below the applicant acknowledges that they have read, understood and agree that: MedReleaf may from time to time use personal health information (i.e. your condition(s), product selection) on an anonymous and aggregate basis for research and/or medical educational purposes. We may also ask you to complete surveys that we use for research purposes, these are optional. MedReleaf is committed to helping both patients and doctors better understand the benefits and utility of Cannabis as a medical tool, for a variety of ailments. We use voluntary, aggregated, and anonymous health data as a part of that research program. As a MedReleaf client you are under no obligation to participate and if you would like your data to be excluded from this research program, you can opt-out or opt-in. If you would like more information about our research program, please feel free to contact us.
The Applicant consents to their health care practitioner named in the Medical Document disclosing required personal health information to MedReleaf Corp. for the purposes of complying with the requirements of the Cannabis for Medical Purposes Regulations (MMPR). The Applicant understands and agrees that a copy of this consent & registration application may be provided to the health care practitioner.
•
•
•
•
•
•
•
•
•
•
METTRUM REGISTRATION APPLICATION – LAST REVISED MAR, 2015
Mettrum Ltd. PO BOX 68 Bowmanville, Bowmanville, Ontario L1C 3K8 1-844-638-8786 | Fax 1-888-344-3620 | [email protected] | All forms available for download at mettrum.com
Name
First NameLast Name
Month / Day / Year
Date of Birth Gender Male Female
APPLICANT’S INFORMATION
PRE-EXISTING LICENSE
Does the applicant have a pre-existing Personal-Use Production License or Designated-Person Production License?
License NumberYes No
Registration Application
CONTACT ADDRESS
I would like you to leave a message on my voicemail if I am not home: Yes No
Is your ‘Mailing Address’ the same as your ‘Contact Address’? Yes No
Is your ‘Shipping Address’ the same as your ‘Contact Address’? Yes No
Address 1
Address 2
City
Telephone Fax Email
Province Postal Code
NOTE: If the applicant is without a permanent address and receives services from an institution, please complete ‘Appendix A2’ available at http://www.mettrum.com/register/AppendixA2
NOTE: If you answered ‘No’ to either of the questions above, please complete ‘Appendix A3’ available at http://www.mettrum.com/register/AppendixA3
NOTE: If you are completing this document on behalf of the applicant (responsible individual), please complete ‘Appendix A1’ available at http://www.mettrum.com/register/AppendixA1
Before registering a client, the Mettrum Client Service Department must obtain this application in full from the client or an individual who is responsible for the client.
METTRUM REGISTRATION APPLICATION – LAST REVISED MAR, 2015
Mettrum Ltd. PO BOX 68 Bowmanville, Bowmanville, Ontario L1C 3K8 1-844-638-8786 | Fax 1-888-344-3620 | [email protected] | All forms available for download at mettrum.com
HEALTH CARE PRACTITIONER INFORMATION
Address 1
Name
Address 2
Profession
City
Telephone Fax Email
Province Postal Code
Please provide contact information for the Health Care Practitioner that provided the medical document.NOTE: The applicant must include the original medical document with this application.
As applicant or a responsible individual you acknowledge, attest, agree and consent to the following:(a) the applicant is permanent resident in Canada;(b) the information in the application and the medical document is correct and complete;(c) the medical document is not being used to seek or obtain dried marihuana from another source;(d) the original of the medical document accompanies the application; and(e) the applicant will use dried marihuana only for their own medical purposes
The applicant acknowledges that dried marihuana is not an approved therapeutic product and cannabis has not been authorized through the standard Health Canada drug approval process because the available scientific evidence does not establish the safety and efficacy of cannabis to the extent required by the Food and Drug Regulations for marketed drugs in Canada.
The applicant acknowledges that they are using any medical marihuana or related product obtained from Mettrum Ltd. at their own risk. The applicant also specifically releases Mettrum Ltd. (and its service providers, officers, directors and staff) from any and all actions, claims, complaints and demands for damages, loss or injury whatsoever, whether arising directly or indirectly as a consequence of the use of Mettrum’s products or services.
In order to receive our products and services, the applicant or authorized person gives consent to Mettrum Ltd. to disclose the nec-essary personal information to Mettrum’s service providers, including the health care practitioner named in this registration, in accor-dance with Mettrum’s Privacy Policy (www.mettrum.com/privacy/).
The applicant and/or authorized person consents to the health care practitioner named in this registration application disclosing to Mettrum Ltd. the applicant’s personal health information by phone, physical means or digital means (including Mettrum’s online portal or SFax secure system) for the purposes of processing this registration (which may include the submission of my Medical Document by digital means), client service and complying with the requirements of the Marihuana for Medical Purposes Regulations. The applicant understands and agrees that a copy of this consent and registration application may be provided to the health care practitioner named in this registration.
AUTHORIZATION OF APPLICANT
Month / Day / Year
Applicant Signature Date
NOTE: If you are completing this document on behalf of the applicant (responsible individual), please complete ‘Appendix A1’ available at http://www.mettrum.com/register/AppendixA1
I consent to Mettrum sending me e-mail communication Yes No
Client Registration Form
Thank you for choosing OrganiGram as your medical marijuana provider. Before we can begin filling your prescription, you will need to complete your application. If you are a Caregiver for the person obtaining medical marijuana, use our Caregiver Registration Form*
To register as a client for the purchase of medical marijuana, you must
a) complete and sign TWO COPIES of this application, leaving one original copy at your doctor’s
office so we have your consent to verify your information
b) mail the second copy together with your medical documents to:
OrganiGram, Inc. 35 A English Dr. Moncton,NBE1E 3X3
Important, Please Read & Sign Below:
- The information contained in the registration document and medical document is correct and complete.
- The applicant is ordinarily a resident of Canada.
- The medical document is not being used to seek or obtain dried marihuana from another source.
- The original of the medical document accompanies the application.
- The applicant will use dried marihuana for their own medical purposes.
- The applicant consents to their health care practitioner named in the Medical Document disclosing required personal health information to OrganiGram Inc for the purposes of complying with the requirements of the Marihuana for Medical Purposes Regulation (MMPR), in accordance with OrganiGram’s Privacy Policy (www.organigram.ca/privacy-policy)
If you have any questions or concerns, please call us at 1-855-961-9420 or email [email protected]
*Caregiver Registration Form is available on our website at www.organigram.ca/forpatients
Client Registration Form
First Name:
Last Name:
Email Address:
Mailing Address: Unit# Street
City Province Postal Code
Shipping Address: Unit# Street
(if different from mailing) City Province Postal Code
Phone Number:
Date of Birth (D,M,Y) :
Gender:
Signature of Patient: Date:
If you have any questions or concerns, please call us at 1-855-961-9420 or email [email protected]
*Caregiver Registration Form is available on our website at www.organigram.ca/forpatients
Male Female